Respiratory Failure in the Pediatric Patient
|
|
|
- Daniella Griffin
- 6 years ago
- Views:
Transcription


1 Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin
2 Objectives Recognize different types of respiratory failure Pathophysiology Management Adjuncts to respiratory support

3 Scope of The Problem
4 Respiratory Failure
5 Anatomy Upper Airway Humidifies inhaled gases Site of most resistances to airflow Lower Airway Conducting airways (anatomic dead space) Site of gas exchange (Resp bronchioles, alveoli)
6 Respiratory Failure Inability of the pulmonary system to meet the metabolic needs of the body not always associated with distress Two crucial metabolic roles Ventilation elimination of CO2 byproduct of cellular respiration Oxygenation-delivery to tissues for utilization 3 forms of respiratory failure Hypoxemic Hypercarbic Mixed
7 Approach to Respiratory Failure Drive issue- patient won t breath CNS (Head injury, Status epilepticus, sedation) Toxin( Drugs) Work issue- patient can t breath because of strength or load Airways (Resistance-UAO, asthma, bronchiolitis) Lungs (Compliance- Pnuemonia) Pump ( Muscle problem- prolonged illness, GBS)
8 Approach to Respiratory Failure Basic mechanism of hypoxemia Ventilation perfusion mismatch most common Diffusion Alveolar hypoventilation Shunt Intra cardiac Extra cardiac (intra- pulmonary) Hypoxia- arterial O2 sat reduced
9 Hypoxemic Respiratory Failure Defined as a PaO2 < 60mmHg Hypoxemic hypoxia Arterial oxygen saturation is reduced Anemic hypoxia SaO2 normal but O2 content reduced by low Hgb inadequate O2 carrying capacity Ischemic hypoxia Blood flow to tissue is low Hgb and O2 concentration normal but cardiac output is low(hypovelemia, myocardial insufficiency) Histotoxic hypoxia Tissue unable to utilize O2,(cyanide or CO poison)
10 Hypercapnic Respiratory Failure Defined as a PaCO2 > 50mmHg Decreased Tidal volume Minute ventilation (volume of air in and out of lung/minute) MV= RR x Tidal volume Shallow breathing, compliance (stiff lungs) airway resistance Decreased Respiratory Rate Drive Increased physiologic dead space Increased carbon dioxide production
11 Categorization of Respiratory Failure Respiratory distress Increased RR by Severity Increased effort (flaring, retractions, use of accessory muscles) Respiratory Failure Clinical state of inadequate oxygenation ventilation or both End stage of respiratory distress
12 Respiratory Distress Intrinsic Pulmonary problem Upper airway obstruction Laryngotracheobronchitis Lower airway obstruction Asthma Bronciolitis Lung parenchyma Pneumonia Pulmonary edema Systemic problem Malaria Shock Dehydration Anemia Heart disease Renal disease

13 Causes of Respiratory Distress Wheeze Crackles Asthma Pneumonia Malaria Treat underlying causes Difficulty breathing Pnuemonia -O2,Abx,Fluids Retractions Asthma-Bronchodilators,Fluids Tachypnea Dehydration- Fluids Anemia-Blood Malaria- Antimalarials, fluids, Anaemia Acidosis Blood film Pallor Acidosis Dehydration Sunken eyes Skin Turgor Acidosis Courtesy Dr B Bevins
14 Management Depends on cause Airway Breathing Circulation
15 Stabilization Airway Clear (unobstructed for normal breathing) Maintainable (simple measures- head tilt, suction) Not maintainable (Advanced interventions)
 MV= RR x Tidal volume Shallow breathing, stiff lungs or airway resistance Lung sounds Pulse")
16 Stabilization Breathing Respiratory rate Effort Nasal flaring Retractions Minute ventilation (volume of air in and out of lung/minute) MV= RR x Tidal volume Shallow breathing, stiff lungs or airway resistance Lung sounds Pulse oximetry
17 Pulse Oximetry The systematic use of pulse oximetry to monitor and treat children in resource-poor developing countries, when coupled with a reliable oxygen supply, improves quality of care and reduces mortality Trevor Duke Annals of Tropical Paediatrics (2009) 29,
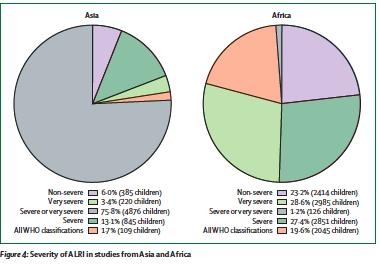
18 Pulse Oximetry Systematic review of 21 published and unpublished articles 16,000 children with acute lower respiratory infection the median hypoxemia prevalence among 13 studies which included children with WHO-defined severe and very severe pneumonia was 13.3% ( %) million children are admitted to hospital each year with Pneumonia, million episodes of hospitalized pneumonia associated with hypoxemia occur in young children globally each year. Annals of Tropical Paediatrics (2009) 29,
19 Scatter diagram showing the correlation between the respiratory rate and oxygen saturation. RR> 60 correlated with low SaO 2 Rajesh V T et al. Arch Dis Child 2000;82: by BMJ Publishing Group Ltd and Royal College of Paediatrics and Child Health
20 Who do you screen? Annals of Tropical Paediatrics (2009) 29,
21
22 Oxygen Availability

23 Oxygen is an essential medicine: a call for international action Hypoxaemia is commonly associated with mortality in developing countries, yet feasible and costeffective ways to address hypoxaemia receive little or no attention in current global Improving access to oxygen and pulse oximetry health strategies.oxygen treatment has been used in medicine for almost 100 years, but in developing countries most seriously ill newborns, children and adults do not have access to oxygen or the simple test that can detect hypoxaemia. Improving access to oxygen and pulse has demonstrated a reduction in mortality from oximetry has demonstrated a reduction in mortality from childhood pneumonia by up to 35% childhood in high-burden child pneumonia settings. by The up cost-effectiveness to 35% in of highburden interventions, child such pneumonia as new vaccines. In settings. addition to its use The in treating cost- acute an oxygen systems strategy compares favourably with other higher profile child survival respiratory illness, oxygen treatment is required for the optimal management of many other conditions effectiveness in adults and children, of an and oxygen is essential for systems safe surgery, strategy anaesthesia and obstetric care. Oxygen concentrators provide the most consistent and least expensive source of oxygen compares in health facilities favorably where power with supplies other are reliable. higher Oxygen concentrators profile are sustainable child survival in developing country interventions, settings if a systematic such approach as new involving nurses, doctors, technicians and administrators is adopted. Improving oxygen vaccines. systems is an entry point for improving the quality of care. For these broad reasons, and for its vital importance in reducing deaths due to lung disease in 2010: Year of the Lung, oxygen deserves a higher priority on the global health agenda. Keywords oxygen; hypoxaemia; pneumonia; lung disease; health systems HYPOXAEMIA is a major cause of morbidity and mortality associated with acute and chronic lung disease in children and adults. Hypoxaemia is a low level of oxygen in the arterial 2010
 Oxygen concentrators work best with nasal cannulas.")
24 Nasal(neonate)C annula Conversion (Gomella-Lange) Flow rate FI02 ¼L 34% ½L 44% ¾L 60% 1L 66% Oxygen Therapy In an adult 1L flow 24% FIO2 FIO2 by 4% for every 1L flow up to 6 L flow (2L 28%) Oxygen concentrators work best with nasal cannulas.


25 Reality we have to deal with Advantage in developed world
26 Using The Tools We Have Monitoring allows the recognition of a patient early in distress or early warning signs of respiratory failure. Tools Physical exam Monitor Cardio-respiratory monitor Pulse oximeter




27 Golden Hour Respiratory Distress Possibly Hours Respiratory Failure Potentially minutes Cardiopulmonary Arrest



28 Early recognition Early Resuscitation Constant Re-assessment Improved Outcome Triage Respiratory rate Retractions Oxygen saturation Emergency Care Oxygen Antibiotics Airway support Ventilation Respiratory Rate Retractions O2 Saturation
29 Adjuncts To Respiratory Support Continuous positive airway pressure(cpap) Non Invasive positive pressure ventilation (NPPV or BIPAP)
30 CPAP or BiPAP Indications Patient who has increased work of breathing despite oxygen support Pneumonia Asthma Gullian barré Syndrome(GBS) Congestive heart failure


31 Non Invasive Mechanical Ventilation(NPV)
32 Contraindication of NPV Respiratory arrest Cardiovascular instability Somnolence High risk of aspiration Craniofacial trauma
33 Non Invasive Mechanical ventilation Advantages Avoids upper airway trauma Leaves airway defenses intact Comfortable Sedation needs less Disadvantages Gastric distention Facial skin necrosis Airleak




34 Bubble CPAP
35 Bubble CPAP Low resistance delivery system Large bore tubing Nasal prongs Fit appropriately and prevent leaks Warm humidified gas Suction 3-4 hrs
36 Bubble CPAP Maintains positive pressure in airway during spontaneous ventilation improves oxygenation Splint the airway, diaphragm Prevents alveolar collapse
37 Bubble CPAP Monitoring Respiratory CVS GI Thermoregulation

38 Summary Systematic approach to a patient in respiratory distress Complete assessment and reassessment of the patient Communication - Interdisciplinary team approach Residents Nursing PATIENT Specialist

39 Team Training building competence to Excellence!
40 Acknowledgement Slides from Dr Vinay Nardkarni Dr Trevor Duke Dr David Hehir Dr Bill Bevins Dr From Mali
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Critical Care Monitoring. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Mechanical Ventilation. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist
 Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
By Mark Bachand, RRT-NPS, RPFT. I have no actual or potential conflict of interest in relation to this presentation.
 By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
ALCO Regulations. Protocol pg. 47
 For the EMT-Basic Objectives Understand ALCO regulations relative to monitoring pulse oximetry by the EMT-B Review the signs and symptoms of respiratory compromise. Understand the importance of adequate
For the EMT-Basic Objectives Understand ALCO regulations relative to monitoring pulse oximetry by the EMT-B Review the signs and symptoms of respiratory compromise. Understand the importance of adequate
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE
 VAPOTHERM POCKET GUIDE") Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
Pediatric Shock. Hypovolemia. Sepsis. Most common cause of pediatric shock Small blood volumes (80cc/kg)
") Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Critical Concepts: Shock Inadequate peripheral perfusion where oxygen delivery does not meet metabolic demand Adult vs Pediatric Shock - Same causes/different frequencies Pediatric Shock Hypovolemia Most
Respiratory Emergencies. Chapter 11
 Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
Respiratory Emergencies Chapter 11 Respiratory System Anatomy and Function of the Lung Characteristics of Adequate Breathing Normal rate and depth Regular breathing pattern Good breath sounds on both sides
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4
 INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Evidence- Based Medicine Fluid Therapy
 Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Evidence- Based Medicine Fluid Therapy Ndidi Musa M.D. Assosciate Professor of Pediatrics Medical College of Wisconsin/ Children s Hospital of Wisconsin Disclosures A. I have no relevant financial relationships
Capnography 101. James A Temple BA, NRP, CCP
 Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Capnography 101 James A Temple BA, NRP, CCP Expected Outcomes 1. Gain a working knowledge of the physiology and science behind End-Tidal CO2. 2.Relate End-Tidal CO2 to ventilation, perfusion, and metabolism.
Tissue Hypoxia and Oxygen Therapy
 Tissue Hypoxia and Oxygen Therapy ก ก ก ก ก ก 1. ก ก 2. ก ก 3. tissue hypoxia 4. ก ก ก 5. ก ก ก 6. ก กก ก 7. ก ก tissue hypoxia ก ก ก ก 1. Pathway of oxygen transport 2. Causes of tissue hypoxia 3. Effect
Tissue Hypoxia and Oxygen Therapy ก ก ก ก ก ก 1. ก ก 2. ก ก 3. tissue hypoxia 4. ก ก ก 5. ก ก ก 6. ก กก ก 7. ก ก tissue hypoxia ก ก ก ก 1. Pathway of oxygen transport 2. Causes of tissue hypoxia 3. Effect
OXYGEN USE IN PHYSICAL THERAPY PRACTICE. Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR
 OXYGEN USE IN PHYSICAL THERAPY PRACTICE Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR Supplemental Oxygen Advantages British Medical Research Council Clinical Trial Improved survival using oxygen 15 hrs/day
OXYGEN USE IN PHYSICAL THERAPY PRACTICE Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR Supplemental Oxygen Advantages British Medical Research Council Clinical Trial Improved survival using oxygen 15 hrs/day
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
Basics of NIV. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Basics of NIV Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Objectives: Definitions Advantages and Disadvantages Interfaces Indications Contraindications
Basics of NIV Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Objectives: Definitions Advantages and Disadvantages Interfaces Indications Contraindications
Training. Continuous Positive Airway Pressure (CPAP)
") Training The training module will follow the national standard curriculum as it relates to the application and use of CPAP. The proposed curriculum will closely resemble the following algorithm utilizing
Training The training module will follow the national standard curriculum as it relates to the application and use of CPAP. The proposed curriculum will closely resemble the following algorithm utilizing
Hyaline membrane disease. By : Dr. Ch Sarishma Peadiatric Pg
 Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients
 Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Bi-Level Therapy: Boosting Comfort & Compliance in Apnea Patients Objectives Describe nocturnal ventilation characteristics that may indicate underlying conditions and benefits of bilevel therapy for specific
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014
 Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
Capnography Connections Guide
 Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
1.1.2 CPAP therapy is used for patients who are suffering from an acute type 1 respiratory failure (Pa02 <8kPa with a normal or low Pac02).
.") Guidelines for initiating and managing CPAP (Continuous Positive Airway Pressure) on a general ward. B25/2006 1.Introduction and Who Guideline applies to 1.1.1 This document provides guidance for Healthcare
Guidelines for initiating and managing CPAP (Continuous Positive Airway Pressure) on a general ward. B25/2006 1.Introduction and Who Guideline applies to 1.1.1 This document provides guidance for Healthcare
OXYGENATION AND ACID- BASE EVALUATION. Chapter 1
 OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Acute respiratory failure
 Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Chapter 13. Respiratory Emergencies
 Chapter 13 Respiratory Emergencies Introduction Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine. Even for physician in
Chapter 13 Respiratory Emergencies Introduction Patients often complain about dyspnea. Shortness of breath Symptom of many different conditions Cause can be difficult to determine. Even for physician in
Oxygenation. Chapter 45. Re'eda Almashagba 1
 Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
3. Which of the following would be inconsistent with respiratory alkalosis? A. ph = 7.57 B. PaCO = 30 mm Hg C. ph = 7.63 D.
 Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
Disclosure. Learning Objectives. Bernadette Zelaya, RRT. Area Clinical Manager
 High Velocity Nasal Insufflation An Important Therapeutic Approach for Use in the Emergency Department Presented by Vapotherm Accredited for 1 CEU by the American Association for Respiratory Care Provider
High Velocity Nasal Insufflation An Important Therapeutic Approach for Use in the Emergency Department Presented by Vapotherm Accredited for 1 CEU by the American Association for Respiratory Care Provider
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Presented By : Kamlah Olaimat
 Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Appendix D An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires:
 Answer Key Appendix D-2 1. An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires: a. oxygen given via nasal cannula b. immediate transport to a medical facility c.
Answer Key Appendix D-2 1. An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires: a. oxygen given via nasal cannula b. immediate transport to a medical facility c.
10/17/2016 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT COURSE OBJECTIVES COMMON CAUSES OF RESPIRATORY FAILURE
 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
Respiratory Distress During RSV Season
 Respiratory Distress During RSV Season Carroll King, MD, FAAP Disclosure : Carroll King, MD, FAAP has nothing to disclose. 1 Objectives At the end of this educational activity, participants should be able
Respiratory Distress During RSV Season Carroll King, MD, FAAP Disclosure : Carroll King, MD, FAAP has nothing to disclose. 1 Objectives At the end of this educational activity, participants should be able
Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning
 CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Indications for Respiratory Assistance. Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer
 Indications for Respiratory Assistance Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer Respiratory Assistance Non-invasive - Nasal specs - Facemask/ Resevoir
Indications for Respiratory Assistance Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer Respiratory Assistance Non-invasive - Nasal specs - Facemask/ Resevoir
Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด
 Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด Noninvasive Mechanical Ventilation Provide support without
Noninvasive Mechanical Ventilation in Children ศ.พญ.อร ณวรรณ พฤทธ พ นธ หน วยโรคระบบหายใจเด ก ภาคว ชาก มารเวชศาสตร คณะแพทยศาสตร โรงพยาบาลรามาธ บด Noninvasive Mechanical Ventilation Provide support without
RESPIRATORY FAILURE. Dr Graeme McCauley KGH
 RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
RESPIRATORY FAILURE Dr Graeme McCauley KGH Definitions Failure to oxygenate-pao2 < 60 Failure to clear CO2-PaCO2 > 50 Acute vs Chronic Hypoxemic failure- type l Hypercapneic failure- type ll Causes of
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Respiratory Emergencies. Lesson Goal. Lesson Objectives 9/10/2012
 Respiratory Emergencies Lesson Goal Assess and provide timely treatment & transport to patients experiencing respiratory emergencies Lesson Objectives List parts of respiratory system and how they work
Respiratory Emergencies Lesson Goal Assess and provide timely treatment & transport to patients experiencing respiratory emergencies Lesson Objectives List parts of respiratory system and how they work
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Anatomy Review. Anatomy Review. Respiratory Emergencies CHAPTER 16
 CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review 1 Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons
CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review 1 Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons
POLICY. Number: Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE. Authorization
 POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
POLICY Number: 7311-60-024 Title: APPLICATION OF NON INVASIVE VENTILATION FOR ACUTE RESPIRATORY FAILURE Authorization [ ] President and CEO [ x ] Vice President, Finance and Corporate Services Source:
Respiratory Emergencies
 CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons for
CHAPTER 16 Respiratory Emergencies Anatomy Review Anatomy Review Pediatric Anatomy Airway structure differences Proportionally larger tongue Smaller, more flexible trachea Abdominal breathers Reasons for
Capnography: The Most Vital Sign
 Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Capnography: The Most Vital Sign Mike McEvoy, PhD, NRP, RN, CCRN Cardiac Surgical ICU RN & Chair Resuscitation Committee Albany Medical Center EMS Coordinator Saratoga County, NY www.mikemcevoy.com CO
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Objectives. Case Presentation. Respiratory Emergencies
 Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Respiratory Emergencies Objectives Describe how to assess airway and breathing, including interpreting information from the PAT and ABCDEs. Differentiate between respiratory distress, respiratory failure,
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Bronchoconstriction is also treated with medications that inhibit bronchiolar constriction such as: Ipratropium (Atrovent)
") Patients with difficulty breathing (dyspnea) may have problems with: Oxygenation due to alveolar problems Ventilation due to bronchiolar problems Oxygenation due to lung perfusion problems Combinations
Patients with difficulty breathing (dyspnea) may have problems with: Oxygenation due to alveolar problems Ventilation due to bronchiolar problems Oxygenation due to lung perfusion problems Combinations
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Oxygen: Is there a problem? Tom Heaps Acute Physician
 Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
ADVANCED ASSESSMENT Respiratory System
 ONTARIO BASE HOSPITAL GROUP QUIT ADVANCED ASSESSMENT Respiratory System 2007 Ontario Base Hospital Group ADVANCED ASSESSMENT Respiratory System AUTHOR(S) Mike Muir AEMCA, ACP, BHSc Paramedic Program Manager
ONTARIO BASE HOSPITAL GROUP QUIT ADVANCED ASSESSMENT Respiratory System 2007 Ontario Base Hospital Group ADVANCED ASSESSMENT Respiratory System AUTHOR(S) Mike Muir AEMCA, ACP, BHSc Paramedic Program Manager
Acute noninvasive ventilation what s the evidence? Respiratory Medicine Update: Royal College of Physicians & BTS Thu 28 th January 2016
 Acute noninvasive ventilation what s the evidence? Respiratory Medicine Update: Royal College of Physicians & BTS Thu 28 th January 2016 Annabel Nickol Consultant in Respiratory Medicine, Sleep & Ventilation
Acute noninvasive ventilation what s the evidence? Respiratory Medicine Update: Royal College of Physicians & BTS Thu 28 th January 2016 Annabel Nickol Consultant in Respiratory Medicine, Sleep & Ventilation
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
3/30/12. Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS
 Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS 1) Define and describe ETCO 2 2) Explain methods of measuring ETCO 2 3) Describe various clinical applications of ETCO 2 4) Describe the relationship
Luke J. Gasowski BS, BSRT, NREMT-P, FP-C, CCP-C, RRT-NPS 1) Define and describe ETCO 2 2) Explain methods of measuring ETCO 2 3) Describe various clinical applications of ETCO 2 4) Describe the relationship
NON-INVASIVE POSITIVE PRESSURE VENTILATION IN THE EMERGENCY DEPARTMENT
 NON-INVASIVE POSITIVE PRESSURE VENTILATION IN THE EMERGENCY DEPARTMENT Developed by J. Osteraas and K. Fuzzard 2001. Reviewed and by K. Maddern 2010 Contents Introduction Assessment Learning Outcomes Background
NON-INVASIVE POSITIVE PRESSURE VENTILATION IN THE EMERGENCY DEPARTMENT Developed by J. Osteraas and K. Fuzzard 2001. Reviewed and by K. Maddern 2010 Contents Introduction Assessment Learning Outcomes Background
Capnography: The Most Vital of Vital Signs. Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017
 Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Capnography: The Most Vital of Vital Signs Tom Ahrens, PhD, RN, FAAN Research Scientist, Barnes-Jewish Hospital, St. Louis, MO May, 2017 Assessing Ventilation and Blood Flow with Capnography Capnography
Chapter 11: Respiratory Emergencies
 29698_CH11_ANS_p001_005 4/12/05 2:02 PM Page 1 Answer Key Chapter 11 1 Chapter 11: Respiratory Emergencies Matching 1. B (page 373) 8. E (page 370) 2. D (page 369) 9. M(page 389) 3. H (page 370) 10. A
29698_CH11_ANS_p001_005 4/12/05 2:02 PM Page 1 Answer Key Chapter 11 1 Chapter 11: Respiratory Emergencies Matching 1. B (page 373) 8. E (page 370) 2. D (page 369) 9. M(page 389) 3. H (page 370) 10. A
Lab 4: Respiratory Physiology and Pathophysiology
 Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be
 1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
1 Chapter 13 Respiratory Emergencies 2 Respiratory Distress Patients often complain about. Shortness of breath Symptom of many different Cause can be difficult to determine. Even for physician in hospital
And Then There is Failure
 Heart Failure And Then There is Failure Heart Failure Brenda Phipps BSN Nurse Educator Minneapolis VA Tina Wright MSN Clinical Nurse Leader Minneapolis VA Symptoms SOB, use of accessory muscles Crackles,
Heart Failure And Then There is Failure Heart Failure Brenda Phipps BSN Nurse Educator Minneapolis VA Tina Wright MSN Clinical Nurse Leader Minneapolis VA Symptoms SOB, use of accessory muscles Crackles,
Appendix E Choose the sign or symptom that best indicates severe respiratory distress.
 Appendix E-2 1. In Kansas EMT-B may monitor pulse oximetry: a. after they complete the EMT-B course b. when the service purchases the state approved pulse oximeters c. when the service director receives
Appendix E-2 1. In Kansas EMT-B may monitor pulse oximetry: a. after they complete the EMT-B course b. when the service purchases the state approved pulse oximeters c. when the service director receives
COPD Challenge CASE PRESENTATION
 Chronic obstructive pulmonary disease (COPD) exacerbations may make up more than 10% of acute medical admissions [1], and they are increasingly recognised as a cause of significant morbidity and mortality
Chronic obstructive pulmonary disease (COPD) exacerbations may make up more than 10% of acute medical admissions [1], and they are increasingly recognised as a cause of significant morbidity and mortality
-Cardiogenic: shock state resulting from impairment or failure of myocardium
 Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Shock chapter Shock -Condition in which tissue perfusion is inadequate to deliver oxygen, nutrients to support vital organs, cellular function -Affects all body systems -Classic signs of early shock: Tachycardia,tachypnea,restlessness,anxiety,
Chapter 10. Objectives. Objectives 01/09/2013. Airway Management, Artificial Ventilation, and Oxygenation
 Chapter 10 Airway Management, Artificial Ventilation, and Oxygenation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
Chapter 10 Airway Management, Artificial Ventilation, and Oxygenation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist. This program has been approved for 1 hour of continuing education credit.
 Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist This program has been approved for 1 hour of continuing education credit. Course Objectives Identify at least four goals of home NIV Identify candidates
Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist This program has been approved for 1 hour of continuing education credit. Course Objectives Identify at least four goals of home NIV Identify candidates
PEDIATRIC RESPIRATORY ILLNESS MADE SIMPLE
 Copyright 2012 Joel Berezow, MD and The Pediatrics for Emergency Physicians Network All rights reserved. Duplication in whole or in part, or electronic transmission in any form, is prohibited THE PEDIATRICS
Copyright 2012 Joel Berezow, MD and The Pediatrics for Emergency Physicians Network All rights reserved. Duplication in whole or in part, or electronic transmission in any form, is prohibited THE PEDIATRICS
Capnography: Not just for confirmation
 Capnography: Not just for confirmation Pennsylvania DOH ALS Protocol 2032-ALS Ernest Yeh, M.D. Division of EMS Department of Emergency Medicine Temple University Hospital and School of Medicine Medical
Capnography: Not just for confirmation Pennsylvania DOH ALS Protocol 2032-ALS Ernest Yeh, M.D. Division of EMS Department of Emergency Medicine Temple University Hospital and School of Medicine Medical
Anaesthetic considerations for laparoscopic surgery in canines
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Anaesthetic considerations for laparoscopic surgery in canines Author : Chris Miller Categories : Canine, Companion animal,
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Anaesthetic considerations for laparoscopic surgery in canines Author : Chris Miller Categories : Canine, Companion animal,
BiLevel Pressure Device
 PROCEDURE - Page 1 of 7 Purpose Scope Classes/ Goals Define indications and care settings for acute and chronic initiation of Noninvasive Positive Pressure Ventilation. Identify the role of Respiratory
PROCEDURE - Page 1 of 7 Purpose Scope Classes/ Goals Define indications and care settings for acute and chronic initiation of Noninvasive Positive Pressure Ventilation. Identify the role of Respiratory
Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study
 D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Condensed version.
 I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
I m Stu 3 Condensed version smcvicar@uwhealth.org Listen 1. Snoring 2. Gurgling 3. Hoarseness 4. Stridor (inspiratory/expiratory) 5. Wheezing 6. Grunting Listen Crackles Wheezing Stridor Absent Crackles
(To be filled by the treating physician)
") CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
CERTIFICATE OF MEDICAL NECESSITY TO BE ISSUED TO CGHS BENEFICIAREIS BEING PRESCRIBED BILEVEL CONTINUOUS POSITIVE AIRWAY PRESSURE (BI-LEVEL CPAP) / BI-LEVEL VENTILATORY SUPPORT SYSTEM Certification Type
Don t let your patients turn blue! Isn t it about time you used etco 2?
 Don t let your patients turn blue! Isn t it about time you used etco 2? American Association of Critical Care Nurses National Teaching Institute Expo Ed 2013 Susan Thibeault MS, CRNA, APRN, CCRN, EMT-P
Don t let your patients turn blue! Isn t it about time you used etco 2? American Association of Critical Care Nurses National Teaching Institute Expo Ed 2013 Susan Thibeault MS, CRNA, APRN, CCRN, EMT-P
Arterial Blood Gas Analysis
 Arterial Blood Gas Analysis L Lester www.3bv.org Bones, Brains & Blood Vessels Drawn from radial or femoral arteries. Invasive procedure Caution must be taken with patient on anticoagulants ph: 7.35-7.45
Arterial Blood Gas Analysis L Lester www.3bv.org Bones, Brains & Blood Vessels Drawn from radial or femoral arteries. Invasive procedure Caution must be taken with patient on anticoagulants ph: 7.35-7.45
Pulmonary Problems of the Neonate. Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA
 Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
New and Future Trends in EMS. Ron Brown, MD, FACEP Paramedic Lecture Series 2018
 New and Future Trends in EMS Ron Brown, MD, FACEP Paramedic Lecture Series 2018 New technologies and protocols DSD Mechanical Compression ITD BiPAP Ultrasound Double Sequential Defibrillation Two defibrillators
New and Future Trends in EMS Ron Brown, MD, FACEP Paramedic Lecture Series 2018 New technologies and protocols DSD Mechanical Compression ITD BiPAP Ultrasound Double Sequential Defibrillation Two defibrillators
Assessing perioperative risk
 Assessing perioperative risk Chronic Obstructive Pulmonary Disease Dr. Michelle Caldecott Respiratory & Sleep Physician Epworth Healthcare Austin Health Impact of COPD on Postoperative Outcomes: Results
Assessing perioperative risk Chronic Obstructive Pulmonary Disease Dr. Michelle Caldecott Respiratory & Sleep Physician Epworth Healthcare Austin Health Impact of COPD on Postoperative Outcomes: Results