RESPIRATORY COMPLICATIONS AFTER SCI
|
|
|
- Cory Scott
- 6 years ago
- Views:
Transcription


1 SHEPHERD.ORG RESPIRATORY COMPLICATIONS AFTER SCI NORMA I RIVERA, RRT, RCP RESPIRATORY EDUCATOR SHEPHERD CENTER 2020 Peachtree Road, NW, Atlanta, GA
2 DISCLOSURE STATEMENT I have no relevant financial or nonfinancial relationships in the products or services described, reviewed, evaluated or compared in this presentation.
3 OBJECTIVES Discuss the effect of SCI on pulmonary physiology Describe two strategies to reduce complications associated with ventilator management in SCI population
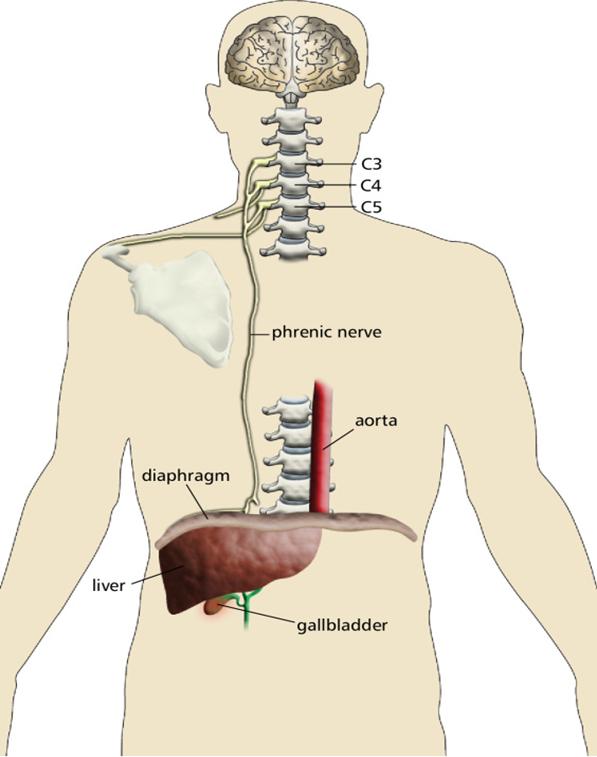
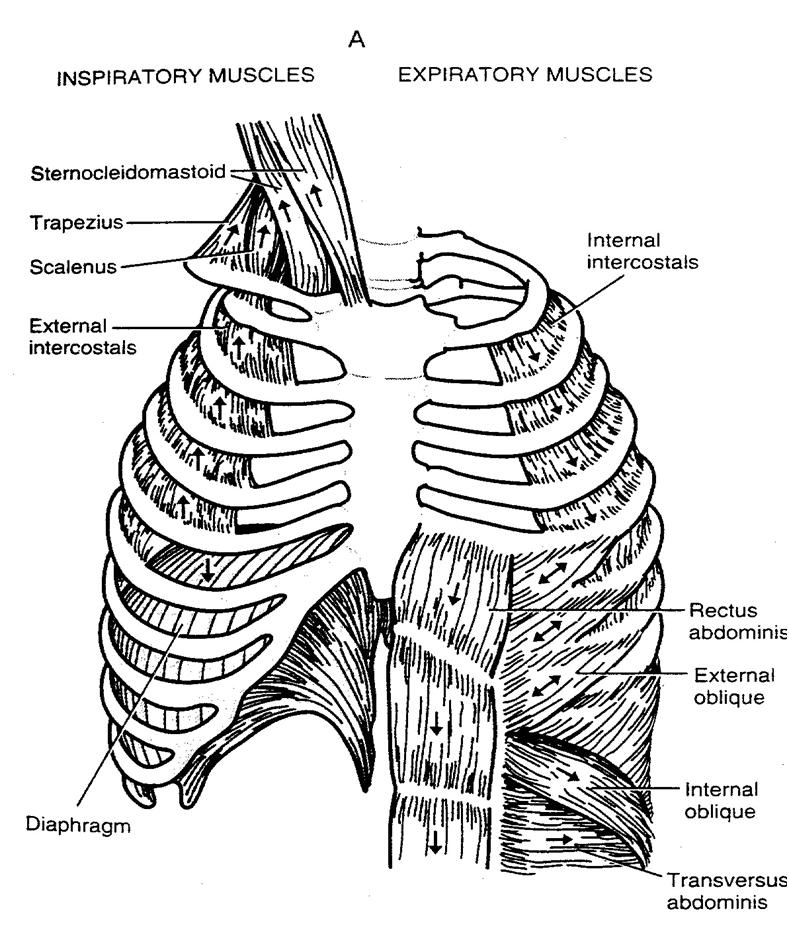
4 INNERVATION OF THE RESPIRATORY NERVES
 C = Incomplete: Motor function is")

5 INTERNATIONAL STANDARDS FOR NEUROLOGICAL CLASSIFICATION OF SCI (ASIA) A = Complete: No motor or sensory function B = Incomplete: Sensory function is preserved below the level of injury ( but no motor function) C = Incomplete: Motor function is preserved below the level of injury; the majority of muscles below the level can have ROM with gravity eliminated D = Incomplete: Motor function is preserved below the level of injury; the majority of muscles below the level can have ROM against gravity E = Normal
 Within 3-5 days after injury Pneumonia can set in 40")
6 FACTS AND RESPIRATORY CONCERNS CATASTROPHIC Number of respiratory complications during initial acute care hospitalization is a more important determinant of length of stay than the level of injury for cervical injuries Respiratory complications are the most prevalent source of morbidity and mortality after SCI (Pneumonia, PE, and Septicemia) Within 3-5 days after injury Pneumonia can set in % of high injury levels will develop atelectasis usually in the LLL

7 FACTS AND RESPIRATORY CONCERNS Most common levels of injury C 4 and C5 and T 11 and T12 Studies found that 51.1% of patients with T1 T6 develop respiratory complications vs.34.5 % of T7 to T12 Neurogenic Pulmonary Edema may occur due to systemic and pulmonary vasoconstriction which can cause left ventricular overload and reduce alveolar ventilation Bronchospasms seen in cervical injuries due to autonomic changes Hypersecretions of mucus increases within 1 hour after an injury caused by loss of sympathetic control

8 FACTS AND RESPIRATORY CONCERNS Effects of Chest Trauma (lung contusion, rib fractures, pneumo s, pleural effusions), MVA s account for 36.5% of SCI Pulmonary emboli / DVT Spinal Shock -à Bradycardia, Hypotension, Hypothermia Occurs minutes post traumatic SCI Unstable Cervical Injury -à Possible worsening of injury Gastric Distention associated with vomiting, aspiration, and decreased lung expansion Dysphagia Preexisting Pulmonary disease (COPD, Smoker, Neuromuscular, Chest wall abnormalities) Sleep Apnea / Obesity

 2.")
 3. Arterial Blood Gas 4. Sputum Sample 5.")
9 RESPIRATORY ASSESSMENT 1. Vital Capacity = Volume measured on complete expiration after a deep inspiration (> 10 to 15 ml/kg body weight or normal 3 5 liters) 2. Negative inspiratory force = measures maximum inspiration pressure (> -20, normal > -60) 3. Arterial Blood Gas 4. Sputum Sample 5. Chest X-Ray 6. EKG 7. Injury Level / Predictable lung function 8. Progress notes from discharged facility

10 Can occur within 1 hour after injury ***HYPERSECRETIONS*** Secretions abnormal in amount and viscosity Imbalance between the sympathetic and parasympathetic systems Beating rate of airway cilia function decreased Mucus will block the inflow of air due to weak or no cough Bronchospasms due to narrowing of the airways Lung compliance is reduced due to airway closure Mucus plug Loss of surfactant due to state of atelectasis All of the above will make it difficult for the patient to breathe, fatigue sets in, and develops respiratory failure. Therefore, keep the lungs expanded and clear!



11 AGGRESSIVE PULMONARY TOILET 9. Switch to manual suctioning technique, avoid inline suction catheters 10. Do use the resuscitator bag and wetting agents (Normal Saline, Sodium Bicarbonate) lavages 11. Implement aggressive pulmonary toilet with assisted coughing techniques 12. If possible use Inexsufflator / Assist Cough Machine 13. Bronchoscopy





12 AGGRESSIVE PULMONARY TOILET

13 CONTRA-INDICATIONS for INEXSUFFLATION ABSOLUTE CONTRA-INDICATIONS Hemoptysis Untreated or recent Pneumothorax Bullous Emphysema Severe COPD Recent Lobectomy Increased intra cranial pressure including ventricular drains Non artificial airway patient with impaired consciousness / inability to communicate RELATIVE CONTRA-INDICATIONS Tachypnea Large Pleural Effusion Unclear cervical spinal injury Hemodynamic instability

14 Tracheostomy tube MECHANICAL VENTILATION Mode of Ventilation / CPAP + PRESSURE SUPPORT Need high volume ventilation between ml/kg 1. Prevents and treats atelectasis 2. Avoids air hunger 3. Compensates for tracheal cuff leaks, monitor cuff pressures (<20cm) Keep peak airway pressures < 35 cm H2O Low PEEP
 X 5 = TV 350) Spontaneous Vital Capacity > 8 ml / kg (70 kg X 8 = VC 560) Minute Ventilation < 10 L / min or 2X normal ( TV 350 X RR/12 = 4.")
.")
15 VENTILATOR WEANING / SPONTANEOUS BREATHING TRAILS - CPAP/PS Spontaneous Tidal Volume > 5 ml / kg (70 kg (154 lbs.) X 5 = TV 350) Spontaneous Vital Capacity > 8 ml / kg (70 kg X 8 = VC 560) Minute Ventilation < 10 L / min or 2X normal ( TV 350 X RR/12 = 4.200) Spontaneous Respiratory Rate < 30 Rapid shallow breathing index < 100 ( RR 12 divide by TV 350 = 34 ) RSBI is the ratio of respiratory rate to tidal volume (f/vt). People on a ventilator who cannot tolerate independent breathing tend to breathe rapidly (high frequency) and shallowly (low tidal volume), and will therefore have a high RSBI CROP index > 13 (Compliance, Rate, Oxygenation, Pressure)



16 CHALLENGERS OF VENTILATOR WEANING Hemodynamically unstable Septic ***Hypersecretion levels *** Depression / Anxiety / Family dynamics Pain / Sedation Airway injury / Artificial airway complications / Aspiration Acquired Brain Injury (inability to follow commands) Sleep Apnea


17 Capnography MAINTAINING VENTILATOR WEANING Sputum monitoring Use intrapulmonary vibrating devices ( Vest, MetNeb, IPV, Flutter Valve ) Bronchodilators Positioning and turning Encourage fluid intake and eating Incentive Spirometer use Education

18 TEAMWORK


19 VENTILATOR DEPENDENT AND HARD TO WEAN PATIENTS NeuRX Diaphragm Pacing System Synapse Biomedical Inc.
20 References Paralyzed Veterans of America Consortium for Spinal Cord Medicine Clinical Practice Guidelines Respiratory Management following Spinal Cord Injury: A clinical Practice Guideline for Health-Care Professionals; January 2005: 5-25 Zadoff A. Pulmonary Issues in Spinal Cord Injuries. Tri State Medical Conference Medical Conference of Thoracic and Pulmonary Healthcare Professionals Mechanical Ventilation and Weaning Protocols Web site. Published February 16, 2016 Lehman, C. Traumatic Injuries: Traumatic Brain Injury and Spinal Cord Injury The Specialty Practice of REHABILITATION NURSING. 7 th ed.; 2015:
Pulmonary Rehabilitation in Acute Spinal Cord Injury. Jatuporn Jatutawanit Physical therapist, Physical therapy unit, Prince of songkla university
 Pulmonary Rehabilitation in Acute Spinal Cord Injury Jatuporn Jatutawanit Physical therapist, Physical therapy unit, Prince of songkla university Causes of spinal cord injury Traumatic injury Motor vehicle
Pulmonary Rehabilitation in Acute Spinal Cord Injury Jatuporn Jatutawanit Physical therapist, Physical therapy unit, Prince of songkla university Causes of spinal cord injury Traumatic injury Motor vehicle
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
COMMISSION ON ACCREDITATION FOR RESPIRATORY CARE TMC DETAILED CONTENT OUTLINE COMPARISON
 A. Evaluate Data in the Patient Record I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 1. Patient history e.g., admission data orders medications progress notes DNR status / advance directives social history
A. Evaluate Data in the Patient Record I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 1. Patient history e.g., admission data orders medications progress notes DNR status / advance directives social history
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
F: Respiratory Care. College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 59
 F: Respiratory Care College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 59 Competency: F-1 Airway Management F-1-1 F-1-2 F-1-3 F-1-4 F-1-5 Demonstrate knowledge and ability
F: Respiratory Care College of Licensed Practical Nurses of Alberta, Competency Profile for LPNs, 3rd Ed. 59 Competency: F-1 Airway Management F-1-1 F-1-2 F-1-3 F-1-4 F-1-5 Demonstrate knowledge and ability
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
H: Respiratory Care. Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 79
 H: Respiratory Care Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 79 Competency: H-1 Airway Management H-1-1 H-1-2 H-1-3 H-1-4 H-1-5 Demonstrate knowledge
H: Respiratory Care Saskatchewan Association of Licensed Practical Nurses, Competency Profile for LPNs, 3rd Ed. 79 Competency: H-1 Airway Management H-1-1 H-1-2 H-1-3 H-1-4 H-1-5 Demonstrate knowledge
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
Therapist Written RRT Examination Detailed Content Outline
 I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 4 7 17 28 A. Review Data in the Patient Record 1 4 0 5 1. Patient history e.g., present illness admission notes respiratory care orders medication history
I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 4 7 17 28 A. Review Data in the Patient Record 1 4 0 5 1. Patient history e.g., present illness admission notes respiratory care orders medication history
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Cough assist T70 for the Tracheostomy Child
 Patient and Family Education Cough assist 70 for the racheostomy Child with or without a ventilator What is a Cough assist device? he Cough assist 70 device removes mucus (secretions) from your child s
Patient and Family Education Cough assist 70 for the racheostomy Child with or without a ventilator What is a Cough assist device? he Cough assist 70 device removes mucus (secretions) from your child s
Weaning guidelines for Spinal Cord Injured patients in Critical Care Units
 RISCI Respiratory Information for Spinal Cord Injury UK Weaning guidelines for Spinal Cord Injured patients in Critical Care Units Introduction It is an unfortunate fact that Spinal Cord Injury Centres
RISCI Respiratory Information for Spinal Cord Injury UK Weaning guidelines for Spinal Cord Injured patients in Critical Care Units Introduction It is an unfortunate fact that Spinal Cord Injury Centres
IPPB via the Servo I Guidelines for use in UCH Critical Care.
 IPPB via the Servo I Guidelines for use in UCH Critical Care. Version 1.3 Document Control Summary Approved by & date Date of publication Review Date Creator & telephone details Distribution/availability
IPPB via the Servo I Guidelines for use in UCH Critical Care. Version 1.3 Document Control Summary Approved by & date Date of publication Review Date Creator & telephone details Distribution/availability
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
Commissioning Policy for Cough Assist Requests
 Commissioning Policy for Cough Assist Requests 1 DOCUMENT CONTROL Reference Number (lead in specific policy area to provide once policy ratified) Version Draft Version 0.3 071015 Status Sponsor(s)/Author(s)
Commissioning Policy for Cough Assist Requests 1 DOCUMENT CONTROL Reference Number (lead in specific policy area to provide once policy ratified) Version Draft Version 0.3 071015 Status Sponsor(s)/Author(s)
AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL
 PROTOCOL") AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL A. Definition of Therapy: 1. Cough machine: 4 sets of 5 breaths with a goal of I:E pressures approximately the same of 30-40. Inhale time = 1 second, exhale
AFCH NEUROMUSCULAR DISORDERS (NMD) PROTOCOL A. Definition of Therapy: 1. Cough machine: 4 sets of 5 breaths with a goal of I:E pressures approximately the same of 30-40. Inhale time = 1 second, exhale
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Neuromuscular diseases (NMDs) include both hereditary and acquired diseases of the peripheral neuromuscular system. They are diseases of the
 include both hereditary and acquired diseases of the peripheral neuromuscular system. They are diseases of the") Neuromuscular diseases (NMDs) include both hereditary and acquired diseases of the peripheral neuromuscular system. They are diseases of the peripheral nerves (neuropathies and anterior horn cell diseases),
Neuromuscular diseases (NMDs) include both hereditary and acquired diseases of the peripheral neuromuscular system. They are diseases of the peripheral nerves (neuropathies and anterior horn cell diseases),
VENTILATOR GRAPHICS ver.2.0. Charles S. Williams RRT, AE-C
 VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
Therapist Multiple-Choice Examination Detailed Content Outline
 I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 12 26 17 55 A. Evaluate Data in the Patient Record 3 5 0 8 1. Patient history, for example, admission data progress notes orders DNR status / advance directives
I. PATIENT DATA EVALUATION AND RECOMMENDATIONS 12 26 17 55 A. Evaluate Data in the Patient Record 3 5 0 8 1. Patient history, for example, admission data progress notes orders DNR status / advance directives
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
North Wales Critical Care Network
 North Wales Critical Care Network Weaning Guidelines for SPINAL CORD INJURED patients in North Wales Critical Care Units NWCCN Spinal Cord Injury Weaning Guidelines_APPROVED February 2014 Page 1 Weaning
North Wales Critical Care Network Weaning Guidelines for SPINAL CORD INJURED patients in North Wales Critical Care Units NWCCN Spinal Cord Injury Weaning Guidelines_APPROVED February 2014 Page 1 Weaning
Problem-solving Respiratory Issues in Children With Neuromuscular Disease. December 13, 2018 Eliezer Be eri, M.D.
 Problem-solving Respiratory Issues in Children With Neuromuscular Disease December 13, 2018 Eliezer Be eri, M.D. About Our Presenter Eliezer Be eri, M.D. Alyn Rehabilitation Hospital Jerusalem, Israel
Problem-solving Respiratory Issues in Children With Neuromuscular Disease December 13, 2018 Eliezer Be eri, M.D. About Our Presenter Eliezer Be eri, M.D. Alyn Rehabilitation Hospital Jerusalem, Israel
The objectives of this presentation are to
 1 The objectives of this presentation are to 1. Review the mechanics of airway clearance 2. Understand the difference between secretion mobilization and secretion clearance 3. Identify conditions that
1 The objectives of this presentation are to 1. Review the mechanics of airway clearance 2. Understand the difference between secretion mobilization and secretion clearance 3. Identify conditions that
RESPIRATORY REHABILITATION
 RESPIRATORY REHABILITATION By: Dr. Fatima Makee AL-Hakak University of kerbala College of nursing CHEST PHYSIOTHERAPY Chest physiotherapy (CPT) includes: 1.Postural drainage. 2.Chest percussion and vibration.
RESPIRATORY REHABILITATION By: Dr. Fatima Makee AL-Hakak University of kerbala College of nursing CHEST PHYSIOTHERAPY Chest physiotherapy (CPT) includes: 1.Postural drainage. 2.Chest percussion and vibration.
Interfacility Protocol Protocol Title:
 Interfacility Protocol Protocol Title: Mechanical Ventilator Monitoring & Management Original Adoption Date: 05/2009 Past Protocol Updates 05/2009, 12/2013 Date of Most Recent Update: March 23, 2015 Medical
Interfacility Protocol Protocol Title: Mechanical Ventilator Monitoring & Management Original Adoption Date: 05/2009 Past Protocol Updates 05/2009, 12/2013 Date of Most Recent Update: March 23, 2015 Medical
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS
 with surfactant in pediatric ARDS") Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Bronchoalveolar lavage (BAL) with surfactant in pediatric ARDS M. Luchetti, E. M. Galassini, A. Galbiati, C. Pagani,, F. Silla and G. A. Marraro gmarraro@picu.it www.picu.it Anesthesia and Intensive Care
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Therapist Multiple-Choice Examination Detailed Content Outline
 I. PATIENT DATA 15 27 8 50 A. Evaluate Data in the Patient Record 4 6 0 10 1. Patient history, for example, history of present illness (HPI) orders medication reconciliation progress notes DNR status /
I. PATIENT DATA 15 27 8 50 A. Evaluate Data in the Patient Record 4 6 0 10 1. Patient history, for example, history of present illness (HPI) orders medication reconciliation progress notes DNR status /
Therapist Multiple-Choice Examination Detailed Content Outline
 I. PATIENT DATA 15 27 8 50 A. Evaluate Data in the Patient Record 4 6 0 10 1. Patient history, for example, history of present illness (HPI) orders medication reconciliation progress notes DNR status /
I. PATIENT DATA 15 27 8 50 A. Evaluate Data in the Patient Record 4 6 0 10 1. Patient history, for example, history of present illness (HPI) orders medication reconciliation progress notes DNR status /
Oxygenation. Chapter 45. Re'eda Almashagba 1
 Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
Oxygenation Chapter 45 Re'eda Almashagba 1 Respiratory Physiology Structure and function Breathing: inspiration, expiration Lung volumes and capacities Pulmonary circulation Respiratory gas exchange: oxygen,
Respiratory Physiology
 Respiratory Physiology Dr. Aida Korish Associate Prof. Physiology KSU The main goal of respiration is to 1-Provide oxygen to tissues 2- Remove CO2 from the body. Respiratory system consists of: Passages
Respiratory Physiology Dr. Aida Korish Associate Prof. Physiology KSU The main goal of respiration is to 1-Provide oxygen to tissues 2- Remove CO2 from the body. Respiratory system consists of: Passages
Respiratory Diseases and Disorders
 Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Chapter 9 Respiratory Diseases and Disorders Anatomy and Physiology Chest, lungs, and conducting airways Two parts: Upper respiratory system consists of nose, mouth, sinuses, pharynx, and larynx Lower
Capnography Connections Guide
 Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Phases of Respiration. Chapter 18: The Respiratory System. Structures of the Respiratory System. Structures of the Respiratory System
 Phases of Respiration Chapter 18: The Respiratory System Respiration Process of obtaining oxygen from environment and delivering it to cells Phases of Respiration 1. Pulmonary ventilation between air and
Phases of Respiration Chapter 18: The Respiratory System Respiration Process of obtaining oxygen from environment and delivering it to cells Phases of Respiration 1. Pulmonary ventilation between air and
7 Initial Ventilator Settings, ~05
 Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Abbreviations (inside front cover and back cover) PART 1 Basic Concepts and Core Knowledge in Mechanical -- -- -- -- 1 Oxygenation and Acid-Base Evaluation, 1 Review 01Arterial Blood Gases, 2 Evaluating
Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600
 Endobronchial valve insertion to reduce lung volume in emphysema Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600 Your responsibility This guidance represents
Endobronchial valve insertion to reduce lung volume in emphysema Interventional procedures guidance Published: 20 December 2017 nice.org.uk/guidance/ipg600 Your responsibility This guidance represents
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Clinical Simulation Examination Detailed Content Outline
 I. PATIENT DATA A. Evaluate Data in the Patient Record 1. Patient history, for example, history of present illness (HPI) orders medication reconciliation progress notes DNR status / advance directives
I. PATIENT DATA A. Evaluate Data in the Patient Record 1. Patient history, for example, history of present illness (HPI) orders medication reconciliation progress notes DNR status / advance directives
Coexistence of confirmed obstruction in spirometry and restriction in body plethysmography, e.g.: COPD + pulmonary fibrosis
 Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
Volumes: IRV inspiratory reserve volume Vt tidal volume ERV expiratory reserve volume RV residual volume Marcin Grabicki Department of Pulmonology, Allergology and Respiratory Oncology Poznań University
Hyperinflation Therapy and the Tools to Accomplish It!! Bill Barnes, RN, RRT Good Shepherd Rehabilitation Network
 Hyperinflation Therapy and the Tools to Accomplish It!! Bill Barnes, RN, RRT Good Shepherd Rehabilitation Network HYPERINFLATION THERAPY Challenges in Post Acute Care Deconditioning Malnutrition Hydration
Hyperinflation Therapy and the Tools to Accomplish It!! Bill Barnes, RN, RRT Good Shepherd Rehabilitation Network HYPERINFLATION THERAPY Challenges in Post Acute Care Deconditioning Malnutrition Hydration
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
10/17/2016 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT COURSE OBJECTIVES COMMON CAUSES OF RESPIRATORY FAILURE
 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Nursing of long-term ventilated SCI-patients - needs, goals and limitations
 Nursing of long-term ventilated SCI-patients - needs, goals and limitations 2016 International SCI Nurse Conference Rome, Italy S. Tiedemann BG Klinikum Hamburg Chief physician: PD Dr. R. Thietje Blohm+Voss
Nursing of long-term ventilated SCI-patients - needs, goals and limitations 2016 International SCI Nurse Conference Rome, Italy S. Tiedemann BG Klinikum Hamburg Chief physician: PD Dr. R. Thietje Blohm+Voss
RESPIRATORY PHYSIOLOGY Pre-Lab Guide
 RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
Moderator: Michael Richardson, MD, FACP Presenters: Toni Chiara, PhD, MHS, MSPT Charles J. Gutierrez, PhD, RRT, FAARC Jim Hunziker, MSN, ARNP
 Moderator: Michael Richardson, MD, FACP Presenters: Toni Chiara, PhD, MHS, MSPT Charles J. Gutierrez, PhD, RRT, FAARC Jim Hunziker, MSN, ARNP 1 CVP may be used with quad cough, or MI/E, with patient in
Moderator: Michael Richardson, MD, FACP Presenters: Toni Chiara, PhD, MHS, MSPT Charles J. Gutierrez, PhD, RRT, FAARC Jim Hunziker, MSN, ARNP 1 CVP may be used with quad cough, or MI/E, with patient in
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014
 Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Mechanical ventilation in the emergency department
 Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
Mechanical ventilation in the emergency department Intubation and mechanical ventilation are often needed in emergency treatment. A ENGELBRECHT, MB ChB, MMed (Fam Med), Dip PEC, DA Head, Emergency Medicine
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Carole Wegner RN, MSN And Lori Leiser CRT
 Airway Clearance Carole Wegner RN, MSN And Lori Leiser CRT Topics Suctioning and suctioning equipment Medications to facilitate t airway clearance Bronchial hygiene modalities Preparing for suctioning
Airway Clearance Carole Wegner RN, MSN And Lori Leiser CRT Topics Suctioning and suctioning equipment Medications to facilitate t airway clearance Bronchial hygiene modalities Preparing for suctioning
Difficult weaning from mechanical ventilation
 Difficult weaning from mechanical ventilation Paolo Biban, MD Director, Neonatal and Paediatric Intensive Care Unit Division of Paediatrics, Major City Hospital Azienda Ospedaliera Universitaria Integrata
Difficult weaning from mechanical ventilation Paolo Biban, MD Director, Neonatal and Paediatric Intensive Care Unit Division of Paediatrics, Major City Hospital Azienda Ospedaliera Universitaria Integrata
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Lower Spinal Cord Injury Management Protocol (for SCI without neurogenic shock, T6 and below)
") Lower Spinal Cord Injury Management Protocol (for SCI without neurogenic shock, T6 and below) Neuro Spinal immobilization and log roll orders Additional imaging as needed Brace per spine recommendations
Lower Spinal Cord Injury Management Protocol (for SCI without neurogenic shock, T6 and below) Neuro Spinal immobilization and log roll orders Additional imaging as needed Brace per spine recommendations
Slide 1. Slide 2. Slide 3 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Objectives: I have nothing to disclose.
 Slide 1 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Maryann M Brogden ND, MSN, RN, APN-C, CCNS, SCRN Slide 2 I have nothing to disclose. Slide 3 Objectives: Identify Criteria for Intubation Differentiate
Slide 1 VENTILATOR MADNESS.. MAKING SENSE OF IT ALL!! Maryann M Brogden ND, MSN, RN, APN-C, CCNS, SCRN Slide 2 I have nothing to disclose. Slide 3 Objectives: Identify Criteria for Intubation Differentiate
C l i n i c a lcpap. Advanced Solutions in Acute Respiratory Care
 C l i n i c a lcpap Advanced Solutions in Acute Respiratory Care This is tex which explains in moderate clinicsal detail, the background and structure of the patient indication for CPAP. This is tex which
C l i n i c a lcpap Advanced Solutions in Acute Respiratory Care This is tex which explains in moderate clinicsal detail, the background and structure of the patient indication for CPAP. This is tex which
BiLevel Pressure Device
 PROCEDURE - Page 1 of 7 Purpose Scope Classes/ Goals Define indications and care settings for acute and chronic initiation of Noninvasive Positive Pressure Ventilation. Identify the role of Respiratory
PROCEDURE - Page 1 of 7 Purpose Scope Classes/ Goals Define indications and care settings for acute and chronic initiation of Noninvasive Positive Pressure Ventilation. Identify the role of Respiratory
The ABC s of Chest Trauma
 The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
The ABC s of Chest Trauma J Bradley Pickhardt MD, FACS Providence St Patrick Hospital What s the Problem? 2/3 of trauma patients have chest trauma Responsible for 25% of all trauma deaths Most injuries
Recent Advances in Respiratory Medicine
 Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Recent Advances in Respiratory Medicine Dr. R KUMAR Pulmonologist Non Invasive Ventilation (NIV) NIV Noninvasive ventilation (NIV) refers to the administration of ventilatory support without using an invasive
Pulmonary Care for Patients with Mitochondrial Disorders
 Pulmonary Care for Patients with Mitochondrial Disorders Rajeev Bhatia, MD, MBBS, DCH, FAAP Pediatric Pulmonologist Assistant Professor of Pediatrics, NEOMED Medical Director, Clinical Exercise Physiology
Pulmonary Care for Patients with Mitochondrial Disorders Rajeev Bhatia, MD, MBBS, DCH, FAAP Pediatric Pulmonologist Assistant Professor of Pediatrics, NEOMED Medical Director, Clinical Exercise Physiology
I Need to Cough Ways to Keep Your Airways Clear
 I Need to Cough Ways to Keep Your Airways Clear 2018 Annual Cure SMA Conference Richard Kravitz, MD Duke University School of Medicine Duke University Medical Center Durham, North Carolina Presenters Jane
I Need to Cough Ways to Keep Your Airways Clear 2018 Annual Cure SMA Conference Richard Kravitz, MD Duke University School of Medicine Duke University Medical Center Durham, North Carolina Presenters Jane
Bergen Community College Division of Health Professions Department of Respiratory Care Fundamentals of Respiratory Critical Care
 Bergen Community College Division of Health Professions Department of Respiratory Care Fundamentals of Respiratory Critical Care Date Revised: January 2015 Course Description Student Learning Objectives:
Bergen Community College Division of Health Professions Department of Respiratory Care Fundamentals of Respiratory Critical Care Date Revised: January 2015 Course Description Student Learning Objectives:
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR
 CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR 801-467-0800 Phone 800-800-HFJV (4358) Hotline TABLE OF CONTENTS Respiratory Care Considerations..3 Physician Considerations
CLINICAL CONSIDERATIONS FOR THE BUNNELL LIFE PULSE HIGH-FREQUENCY JET VENTILATOR 801-467-0800 Phone 800-800-HFJV (4358) Hotline TABLE OF CONTENTS Respiratory Care Considerations..3 Physician Considerations
Neonatal Airway Disorders, Treatments, and Outcomes. Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center
 Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Foundation in Critical Care Nursing. Airway / Respiratory / Workbook
 Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
Foundation in Critical Care Nursing Airway / Respiratory / Workbook Airway Anatomy: Please label the following: Tongue Larynx Epiglottis Pharynx Trachea Vertebrae Oesophagus Where is the ET (endotracheal)
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
Critical Care Therapy and Respiratory Care Section
 Critical Care Therapy and Respiratory Care Section Category: Clinical Section: Bronchial Hygiene Title: Chest Physiotherapy Policy #: 01 Revised: 03/00 1.0 DESCRIPTION 1.1 Definition Chest physiotherapy
Critical Care Therapy and Respiratory Care Section Category: Clinical Section: Bronchial Hygiene Title: Chest Physiotherapy Policy #: 01 Revised: 03/00 1.0 DESCRIPTION 1.1 Definition Chest physiotherapy
OWN THE AIRWAY. Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP. Paramedic Program
 OWN THE AIRWAY Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP The largest detriment to airway management has nothing to do with the patient, but everything to do with you as a provider. PRACTICE..PRACTICE.PRACTICE.
OWN THE AIRWAY Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP The largest detriment to airway management has nothing to do with the patient, but everything to do with you as a provider. PRACTICE..PRACTICE.PRACTICE.
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
COMMUNICATION. Communication and Swallowing post Tracheostomy. Role of SLT. Impact of Tracheostomy. Normal Speech. Facilitating Communication
 Communication and Swallowing post Tracheostomy. Role of SLT 1. 2. 3. Management of communication needs. Management of swallowing issues. Working with the multidisciplinary team to facilitate weaning. Impact
Communication and Swallowing post Tracheostomy. Role of SLT 1. 2. 3. Management of communication needs. Management of swallowing issues. Working with the multidisciplinary team to facilitate weaning. Impact
NIV use in ED. Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH
 NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
NIV use in ED Dr. Khalfan AL Amrani Emergency Resuscitation Symposium 2 nd May 2016 SQUH Outline History & Introduction Overview of NIV application Review of proven uses of NIV History of Ventilation 1940
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Thoracic anaesthesia. Simon May
 Thoracic anaesthesia Simon May Contents Indications for lung isolation Ways of isolating lungs Placing a DLT Hypoxia on OLV Suitability for surgery Analgesia Key procedures Indications for lung isolation
Thoracic anaesthesia Simon May Contents Indications for lung isolation Ways of isolating lungs Placing a DLT Hypoxia on OLV Suitability for surgery Analgesia Key procedures Indications for lung isolation
New Curriculum Content Map NBRC Exam Content Outline
 New Curriculum Content Map NBRC Exam Content Outline Patient Data Evaluation and Recommendations Review Existing Data in the Patient Record Including: 1 Patient history [e.g., present illness, admission
New Curriculum Content Map NBRC Exam Content Outline Patient Data Evaluation and Recommendations Review Existing Data in the Patient Record Including: 1 Patient history [e.g., present illness, admission
Alternative title: Confessions of a Mucus Enthusiast. Mechanical Insufflation Exsufflation for airway secretion clearance and lung expansion therapy
 Mechanical Insufflation Exsufflation for airway secretion clearance and lung expansion therapy Alternative title: Confessions of a Mucus Enthusiast Marty Davig, RRT RCP Philips Respironics Inc. Objectives
Mechanical Insufflation Exsufflation for airway secretion clearance and lung expansion therapy Alternative title: Confessions of a Mucus Enthusiast Marty Davig, RRT RCP Philips Respironics Inc. Objectives
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Non-Invasive Ventilation of the Restricted Thorax: Effects of Ventilator Modality on Quality of Life. The North Study
 Non-Invasive Ventilation of the Restricted Thorax: Effects of Ventilator Modality on Quality of Life The North Study Lorna Cummins RRT, Pat Hanly MD, Andrea Loewen MD, Karen Rimmer MD Raymond Tye RRT,
Non-Invasive Ventilation of the Restricted Thorax: Effects of Ventilator Modality on Quality of Life The North Study Lorna Cummins RRT, Pat Hanly MD, Andrea Loewen MD, Karen Rimmer MD Raymond Tye RRT,
Indian Diploma in Critical Care Nursing
 Indian Diploma in Critical Care Nursing MCQ Section A - Only one answer is correct 1. Four emergency interventions used in resuscitating a patient in cardiac arrest. a. Adrenaline/Atropine/ Amiodarone/Defibrillation
Indian Diploma in Critical Care Nursing MCQ Section A - Only one answer is correct 1. Four emergency interventions used in resuscitating a patient in cardiac arrest. a. Adrenaline/Atropine/ Amiodarone/Defibrillation
Policy Specific Section: October 1, 2010 January 21, 2013
 Medical Policy Bi-level Positive Airway Pressure (BPAP/NPPV) Type: Medical Necessity/Not Medical Necessity Policy Specific Section: Durable Medical Equipment Original Policy Date: Effective Date: October
Medical Policy Bi-level Positive Airway Pressure (BPAP/NPPV) Type: Medical Necessity/Not Medical Necessity Policy Specific Section: Durable Medical Equipment Original Policy Date: Effective Date: October
Presented By : Kamlah Olaimat
 Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Definitions. Definitions. Weaning. Weaning. Disconnection (Discontinuation) Weaning
 Weaning") Definitions 2 Disconnection (Discontinuation) Implies patient no longer needs that form of therapy 80% of patients requiring temporary MVS do not require weaning Definitions 3 Implies some need for MVS
Definitions 2 Disconnection (Discontinuation) Implies patient no longer needs that form of therapy 80% of patients requiring temporary MVS do not require weaning Definitions 3 Implies some need for MVS
Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist. This program has been approved for 1 hour of continuing education credit.
 Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist This program has been approved for 1 hour of continuing education credit. Course Objectives Identify at least four goals of home NIV Identify candidates
Ron Hosp, MS-HSA, RRT Regional Respiratory Specialist This program has been approved for 1 hour of continuing education credit. Course Objectives Identify at least four goals of home NIV Identify candidates
Effects of PPV on the Pulmonary System. Chapter 17
 Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
I. Subject: Therapeutic Bronchoscopy and Bronchoscope Assisted Intubation
 I. Subject: Therapeutic Bronchoscopy and Bronchoscope Assisted Intubation II. Policy: Therapeutic flexible fiberoptic bronchoscopy procedures and bronchoscope assisted intubations will be performed by
I. Subject: Therapeutic Bronchoscopy and Bronchoscope Assisted Intubation II. Policy: Therapeutic flexible fiberoptic bronchoscopy procedures and bronchoscope assisted intubations will be performed by