Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University
|
|
|
- Blaise Cameron Lucas
- 5 years ago
- Views:
Transcription



1 Wanchai Wongkornrat Cardiovascular Thoracic Surgery Siriraj Hospital Mahidol University
2 Assess adequacy of ventilation and oxygenation Aids in establishing a diagnosis and severity of respiratory failure Assess changes in acid- base homeostasis Helps in management of ICU patients
3 4 Steps in ABG analysis 1. ABG or VBG 2. Oxygenation 3. Ventilation 4. Acid-Base disorder

4 ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l VBG ph PvO mmhg PvCO mmhg O2 sat % HCO3 24 ± 2 meq/l O2 sat from ABG = O2 sat from pulse oximetry O2 sat from VBG



5 Usually this in patients with shock Should doubt when PO2 is significantly lower than O2 sat from pulse oximetry draw venous blood to check comparison redraw arterial blood
 3.")
6 1. PaO2 (room air, FiO2=0.2) 2. A-a gradient (room air, FiO2=0.2) 3. PaO2 / FiO2

 Severe (severe arrhythmias, brain")
7 Normal room air PaO mmhg Normal room air PaO2 = 100 Age/4 Hypoxemia (room air, FiO2 = 0.2) PaO2 (mmhg) O2 sat (%) Mild Moderate (tachycardia, hypertension, cool extremities) Severe (severe arrhythmias, brain injury, death) < 40 <75




8 A = Alveoli a = arterial A-a gradient = PAO2 PaO2 PAO2 = 713 FiO2 PaCO2/0.8 Normal room air A-a gradient = 5 25 mmhg Normal room air A-a gradient = Age/4 Wide A-a gradient = lung parenchymal disease
I = (PaO2/FiO2)II O2 flow (L/min) FiO2 Room air - 0.")
9 Normal PaO2/FiO2 = 100/0.2 = 500 PaO2 / FiO2 < 300 = lung pathology (PaO2/FiO2)I = (PaO2/FiO2)II O2 flow (L/min) FiO2 Room air O2 nasal cannula O2 mask O2 mask with bag
10

11 ARDS is characterized by an acute onset within 1 week, bilateral radiographic pulmonary infiltrates, respiratory failure not fully explained by heart failure or volume overload, and a PaO2/FiO2 ratio < 300 severity PaO2 / FiO2 ratio Mild ARDS Moderate ARDS < Severe ARDS
12 Hypoxemia Normal A-a gradient (FiO2=0.2) Normal PaO2/FiO2 (FiO2>0.2) Wide A-a gradient (FiO2=0.2) Low PaO2/FiO2 (FiO2>0.2) Decreased FiO2 FiO2 Hypoventilation minute ventilation (TV, RR) V/Q mismatch Dead space (PE, PHT) Intrapulmonary shunt (pneumonia, atelectasis) Extrapulmonary shunt (cyanotic heart disease, pulmonary AVF) Diffusion defect (defect at alveolar capillary membrane, pulmonary fibrosis, interstitial lung disease ) Low SvO2 Low O2 delivery (shock, anemia) High O2 consumption (fever, shivering, convulsion) 100% O2 Thrombolytic, anticoagulant, pulmonary vasodilator PEEP, inverse I:E ratio, prone position Disease specific treatment 100% O2 Disease specific treatment
13 30 YO male Fever RR 12/min Room air ph 7.28 PaO2 = 65 mmhg PaCO2 = 55 mmhg HCO3 = 27 meq/l Mild hypoxemia (PaO mmhg) PAO2 = 713 FiO2 PaCO2/0.8 = 713x0.2 55/0.8 = A-a gradient = PAO2 PaO2 = = 8.85 Normal A-a gradient = Age/4 = /4 = 10 No lung parenchymal disease PaCO2 > 45 mmhg = Hypoventilation Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
14 30 YO male Pneumonia RR 28/min Room air ph 7.50 PaO2 70 mmhg PaCO2 25mmHg HCO3 19 meq/l Mild hypoxemia (PaO mmhg) PAO2 = 713 FiO2 PaCO2/0.8 = 713x0.2 25/0.8 = A-a gradient = PAO2 PaO2 = = Normal A-a gradient = Age/4 = /4 = lung parenchymal disease (V/Q mismatch) PaCO2 < 35 mmhg = Hyperventilation Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
15 ARDS, FiO2 = 1.0 O2 sat 100%, PaO2 = 100 mmhg O2sat 90%, PaO2 =?, FiO2 =? O2sat 90%, PaO2 = 60 mmhg (PaO2/FiO2)I = (PaO2/FiO2)II (100/1) = (60/FiO2) FiO2 = 0.6


I = (PaCO2 x")

16 Normal PaCO mmhg PaCO2 < 35mmHg = Hyperventilation PaCO2 > 45 mmhg = Hypoventilation (PaCO2 x TV x RR)I = (PaCO2 x TV x RR)II PaCO2 = 0.8 x CO2 production RR (TV Dead space)
17 Normal PaCO mmhg PaCO2 < 35mmHg = Hyperventilation PaCO2 > 45 mmhg = Hypoventilation PaCO2 = 0.8 x CO2 production RR ( TV Dead space)
18 Normal PaCO mmhg PaCO2 < 35mmHg = Hyperventilation PaCO2 > 45 mmhg = Hypoventilation PaCO2 = 0.8 x CO2 production RR ( TV Dead space) Cut the ET tube shorter Longer expiratory time ( decrease auto PEEP )
19 Pneumonia, FiO2=0.6 TV=400 ml, RR=15/min, PaCO2=50 mmhg PaCO2=40 mmhg, TV=?, RR=? (PaCO2 x TV x RR)I = (PaCO2 x TV x RR)II 50x400x15 = 40xTVxRR TVxRR = 7500 ml/min (minute ventilation) TV, keep inspiratory < 35 mmhg RR, beware air trapping
 4.")
20 1. Metabolic acidosis 2. Metabolic alkalosis 3. Respiratory acidosis (acute, chronic) 4. Respiratory alkalosis (acute, chronic)


21 1. In seconds: buffer systems 2. In minutes: CO2 excretion by the lungs 3. In hours to days: renal excretion of H+, reabsorption of HCO3
 Wide anion gap (>16) metabolic acidosis Lactic acidosis Ketoacidosis (diabetic, starvation, alcoholic)")

22 H HCO3 RR PaCO2 Predicted PaCO2 = 1.5 HCO3 + 8 ± 2 Anion gap = Na Cl HCO3 Normal AG = 12 ± 4 AG (Corrected) = AG (4 Albumin) Wide anion gap (>16) metabolic acidosis Lactic acidosis Ketoacidosis (diabetic, starvation, alcoholic) Uremia Rhabdomyolysis Drug intoxication (salicylate, ethanol, ethylene glycol) Normal anion gap (<16) metabolic acidosis Diarrhea Renal tubular acidosis Early renal insufficiency Excessive saline loading Amino acid infusion ureterosigmoidostomy

23 HCO3 H RR PaCO2 Predicted PaCO2 = 0.7 HCO ± 2
24 Hypoventilation PaCO2 H kidney HCO3 Respiratory acidosis PaCO2 Predicted HCO3 Predicted ph acute 10 mmhg 1 meq/l 0.08 chronic 10 mmhg 4 meq/l 0.03
25
26 Hyperventilation PaCO2 H kidney HCO3 Respiratory alkalosis PaCO2 Predicted HCO3 Predicted ph acute 10 mmhg 2 meq/l 0.08 chronic 10 mmhg 5 meq/l 0.03
27

28 ph = 7.20 PaCO2 = 20 mmhg HCO3 = 8 meq/l Acidosis (ph<7.40) Metabolic (HCO3 < 22 ) Predicted PaCO2 = 1.5 HCO3 + 8 ± 2 = 20 ± 2 Pure metabolic acidosis Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
29 ph = 7.15 PaCO2 = 30 mmhg HCO3 = 8 meq/l Acidosis (ph<7.40) Metabolic (HCO3 < 22 ) Predicted PaCO2 = 1.5 HCO3 + 8 ± 2 = 20 ± 2 Metabolic acidosis + Respiratory acidosis Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
30 ph = 7.25 PaCO2 = 15 mmhg HCO3 = 8 meq/l Acidosis (ph<7.40) Metabolic (HCO3 < 22 ) Predicted PaCO2 = 1.5 HCO3 + 8 ± 2 = 20 ± 2 Metabolic acidosis + Respiratory alkalosis Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
31 ph = 7.50 PaCO2 = 42 mmhg HCO3 = 30 meq/l alkalosis (ph>7.40) Metabolic (HCO3 > 26 ) Predicted PaCO2 = 0.7 HCO ± 2 = 41 ± 2 Pure metabolic alkalosis Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
32 ph = 7.45 PaCO2 = 50 mmhg HCO3 = 30 meq/l alkalosis (ph>7.40) Metabolic (HCO3 > 26 ) Predicted PaCO2 = 0.7 HCO ± 2 = 41 ± 2 Metabolic alkalosis + Respiratory acidosis Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
33 ph = 7.60 PaCO2 = 35 mmhg HCO3 = 30 meq/l alkalosis (ph>7.40) Metabolic (HCO3 > 26 ) Predicted PaCO2 = 0.7 HCO ± 2 = 41 ± 2 Metabolic alkalosis + Respiratory alkalosis Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
34 ph = 7.24 PaCO2 = 60 mmhg HCO3 = 28 meq/l acidosis (ph<7.40) respiratory (PaCO2 > 45 ) Respiratory acidosis Acute (ph ) Predicted HCO3 = (24 ± 2) + (60-40)/10 = 26 ± 2 Pure acute respiratory acidosis Respiratory acidosis PaCO2 Predicted HCO3 Predicted ph acute 10 mmhg 1 meq/l 0.08 chronic 10 mmhg 4 meq/l 0.03 Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
35 ph = 7.18 PaCO2 = 60 mmhg HCO3 = 22 meq/l acidosis (ph<7.40) respiratory (PaCO2 > 45 ) Respiratory acidosis Acute (ph ) Predicted HCO3 = (24 ± 2) + (60-40)/10 = 26 ± 2 + Metabolic acidosis Respiratory acidosis PaCO2 Predicted HCO3 Predicted ph acute 10 mmhg 1 meq/l 0.08 chronic 10 mmhg 4 meq/l 0.03 Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
36 ph = 7.30 PaCO2 = 60 mmhg HCO3 = 32 meq/l acidosis (ph<7.40) respiratory (PaCO2 > 45 ) Respiratory acidosis Acute (ph ) Predicted HCO3 = (24 ± 2) + (60-40)/10 = 26 ± 2 + Metabolic alkalosis Respiratory acidosis PaCO2 Predicted HCO3 Predicted ph acute 10 mmhg 1 meq/l 0.08 chronic 10 mmhg 4 meq/l 0.03 Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
37 ph = 7.56 PaCO2 = 20 mmhg HCO3 = 18 meq/l alkalosis (ph>7.40) respiratory (PaCO2 < 35 ) Respiratory alkalosis Acute (ph ) Predicted HCO3 = (24 ± 2) (40-20)2/10 = 20 ± 2 Pure acute respiratory alkalosis Respiratory alkalosis PaCO2 Predicted HCO3 Predicted ph acute 10 mmhg 2 meq/l 0.08 chronic 10 mmhg 5 meq/l 0.03 Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
38 ph = 7.50 PaCO2 = 20 mmhg HCO3 = 12 meq/l alkalosis (ph>7.40) respiratory (PaCO2 < 35 ) Respiratory alkalosis Acute (ph ) Predicted HCO3 = (24 ± 2) - (40-20)2/10 = 20 ± 2 + Metabolic acidosis Respiratory alkalosis PaCO2 Predicted HCO3 Predicted ph acute 10 mmhg 2 meq/l 0.08 chronic 10 mmhg 5 meq/l 0.03 Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
 respiratory (PaCO2 < 35 ) Respiratory alkalosis Acute (ph ) Predicted HCO3 = (24 ± 2) - (40-20)2/10 = 20 ± 2 + Metabolic alkalosis Respiratory alkalosis PaCO2 Predicted HCO3 Predicted ph acute")
39 ph = 7.62 PaCO2 = 20 mmhg HCO3 = 25 meq/l alkalosis (ph>7.40) respiratory (PaCO2 < 35 ) Respiratory alkalosis Acute (ph ) Predicted HCO3 = (24 ± 2) - (40-20)2/10 = 20 ± 2 + Metabolic alkalosis Respiratory alkalosis PaCO2 Predicted HCO3 Predicted ph acute 10 mmhg 2 meq/l 0.08 chronic 10 mmhg 5 meq/l 0.03 Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
40 ph = 7.40 PaCO2 = 15 mmhg HCO3 = 12 meq/l Acidosis? Alkalosis? (ph =7.40) Metabolic acidosis (HCO3 < 22) Respiratory alkalosis (PaCO2 < 35 ) Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l
41 ph = 7.40 PaCO2 = 60 mmhg HCO3 = 36 meq/l Acidosis? Alkalosis? (ph =7.40) Metabolic alkalosis (HCO3 > 26) Respiratory acidosis (PaCO2 > 45 ) Normal ABG ph PaO mmhg PaCO mmhg O2 sat % HCO3 24 ± 2 meq/l

42 Thank you
43
44 40 YO male, IE at AV S/P AVR and Ao root replacement for 2 days Post op pneumonia On ET tube, VCV mode, FiO2=0.8, TV=400ml, RR 18/min ph=7.14, PaCO2=50 mmhg, PaO2=60 mmhg Na=140, K=5.5, Cl=102, HCO3=15 meq/l BUN 50, Cr 3.0 CXR - bilateral pulmonary infiltration ABP 90/50 mmhg, P100/min regular Low dose inotropic drug CVP 8 mmhg, PA pressure 30/15 mmhg Oxygenation Ventilation Acid-Base disorder Management
45 40 YO male, IE at AV S/P AVR and Ao root replacement for 2 days Post op pneumonia On ET tube, VCV mode, FiO2=0.8, TV=400ml, RR 18/min ph=7.14, PaCO2=50 mmhg, PaO2=60 mmhg Na=140, K=5.5, Cl=102, HCO3=15 meq/l BUN 50, Cr 3.0 CXR - bilateral pulmonary infiltration ABP 90/50 mmhg, P100/min regular Low dose inotropic drug CVP 8 mmhg, PA pressure 30/15 mmhg Oxygenation FiO2=0.8, PaO2=60 mmhg, O2 sat 90% PO2/FiO2 = 60/0.8 = 75 severe ARDS FiO2 X, PEEP, inverse I:E ratio, prone position Ventilation PaCO2=50 mmhg, RR 18/min, hypoventilation? severe pneumonia mild form pneumonia hyperventilation, acute respiratory alkalosis) PEEP Acid-Base disorder Acidosis (ph<7.40) Metabolic (HCO3 < 22 ) Predicted PaCO2 = 1.5 HCO3 + 8 ± 2 = 30.5 ± 2 Metabolic acidosis + Respiratory acidosis Anion gap = Na Cl HCO3 = = 23 Wide anion gap (>16) metabolic acidosis Lactic acidosis, sepsis, ARF treatment
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Outline. ABG Interpretation: A Respirologist s approach. Acid-Base Disturbances. What use is an ABG? Acid-Base Disturbances. Alveolar Ventilation
 Outline ABG Interpretation: A Respirologist s approach Dr. Shane Shapera Division of Respirology University Health Network October 2014 A quick review of acidbase physiology The 8 steps to ABG interpretation
Outline ABG Interpretation: A Respirologist s approach Dr. Shane Shapera Division of Respirology University Health Network October 2014 A quick review of acidbase physiology The 8 steps to ABG interpretation
Arterial Blood Gas Analysis
 Arterial Blood Gas Analysis L Lester www.3bv.org Bones, Brains & Blood Vessels Drawn from radial or femoral arteries. Invasive procedure Caution must be taken with patient on anticoagulants ph: 7.35-7.45
Arterial Blood Gas Analysis L Lester www.3bv.org Bones, Brains & Blood Vessels Drawn from radial or femoral arteries. Invasive procedure Caution must be taken with patient on anticoagulants ph: 7.35-7.45
SIMPLY Arterial Blood Gases Interpretation. Week 4 Dr William Dooley
 SIMPLY Arterial Blood Gases Interpretation Week 4 Dr William Dooley Plan Structure for interpretation 5-step approach Works for majority of cases Case scenarios Some common concerns A-a gradient BE Anion
SIMPLY Arterial Blood Gases Interpretation Week 4 Dr William Dooley Plan Structure for interpretation 5-step approach Works for majority of cases Case scenarios Some common concerns A-a gradient BE Anion
OXYGENATION AND ACID- BASE EVALUATION. Chapter 1
 OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
Arterial Blood Gases. Dr Mark Young Mater Health Services
 Arterial Blood Gases Dr Mark Young Mater Health Services Why do them? Quick results Bedside test Range of important information Oxygenation Effectiveness of gas exchange Control of ventilation Acid base
Arterial Blood Gases Dr Mark Young Mater Health Services Why do them? Quick results Bedside test Range of important information Oxygenation Effectiveness of gas exchange Control of ventilation Acid base
PICU Resident Self-Study Tutorial Interpreting Blood Gases
 Christopher Carroll, MD INTRODUCTION Blood gases give us a huge amount of information regarding the patient s physiologic condition and are the best method available to assess a patient s oxygenation and
Christopher Carroll, MD INTRODUCTION Blood gases give us a huge amount of information regarding the patient s physiologic condition and are the best method available to assess a patient s oxygenation and
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Physiological Causes of Abnormal ABG s
 Physiological Causes of Abnormal ABG s Major Student Performance Objective 1 1. The student will be able to discuss causes for various types of blood gas results. 2. They will also be required to discuss
Physiological Causes of Abnormal ABG s Major Student Performance Objective 1 1. The student will be able to discuss causes for various types of blood gas results. 2. They will also be required to discuss
Interpretation of Arterial Blood Gases. Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB)
") Interpretation of Arterial Blood Gases Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB) Before interpretation of ABG Make/Take note of Correct puncture
Interpretation of Arterial Blood Gases Prof. Dr. W. Vincken Head Respiratory Division Academisch Ziekenhuis Vrije Universiteit Brussel (AZ VUB) Before interpretation of ABG Make/Take note of Correct puncture
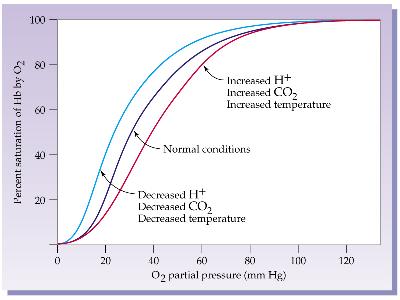
Carbon Dioxide Transport. Carbon Dioxide. Carbon Dioxide Transport. Carbon Dioxide Transport - Plasma. Hydrolysis of Water
 Module H: Carbon Dioxide Transport Beachey Ch 9 & 10 Egan pp. 244-246, 281-284 Carbon Dioxide Transport At the end of today s session you will be able to : Describe the relationship free hydrogen ions
Module H: Carbon Dioxide Transport Beachey Ch 9 & 10 Egan pp. 244-246, 281-284 Carbon Dioxide Transport At the end of today s session you will be able to : Describe the relationship free hydrogen ions
i. Zone 1 = dead space ii. Zone 2 = ventilation = perfusion (ideal situation) iii. Zone 3 = shunt
 iii. Zone 3 = shunt") Respiratory Review I. Oxygen transport a. Oxygen content of blood i. Dissolved oxygen =.003 x PaO 2, per 100 ml plasma 1. Henry s Law ii. Oxygen on hemoglobin = 1.34 ml x sat x Hgb iii. CaO 2 = Dissolved
Respiratory Review I. Oxygen transport a. Oxygen content of blood i. Dissolved oxygen =.003 x PaO 2, per 100 ml plasma 1. Henry s Law ii. Oxygen on hemoglobin = 1.34 ml x sat x Hgb iii. CaO 2 = Dissolved
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Arterial Blood Gas Interpretation Routine Assessment Inspection Palpation Auscultation Labs Na 135-145 K 3.5-5.3 Chloride 95-105 CO2 22-31 BUN 10-26 Creat.5-1.2 Glu 80-120 Arterial Blood Gases WBC 5-10K
Arterial Blood Gas Interpretation Routine Assessment Inspection Palpation Auscultation Labs Na 135-145 K 3.5-5.3 Chloride 95-105 CO2 22-31 BUN 10-26 Creat.5-1.2 Glu 80-120 Arterial Blood Gases WBC 5-10K
RESPIRATORY SYSTEM and ACID BASE
 RESPIRATORY SYSTEM and ACID BASE Arif HM Marsaban Rudyanto Sedono Department of Anesthesiology and Intensive Therapy Faculty of medicine University of Indonesia Dr Cipto Mangunkusumo General Hospital Jakarta
RESPIRATORY SYSTEM and ACID BASE Arif HM Marsaban Rudyanto Sedono Department of Anesthesiology and Intensive Therapy Faculty of medicine University of Indonesia Dr Cipto Mangunkusumo General Hospital Jakarta
Arterial Blood Gases Interpretation Definition Values respiratory metabolic
 Arterial Blood Gases Interpretation Definition A blood gas test measures the amount of oxygen and carbon dioxide in the blood. It is also useful in determining the ph level of the blood. The test is commonly
Arterial Blood Gases Interpretation Definition A blood gas test measures the amount of oxygen and carbon dioxide in the blood. It is also useful in determining the ph level of the blood. The test is commonly
9/14/2017. Acid-Base Disturbances. Goal. Provide an approach to determine complex acid-base disorders
 Acid-Base Disturbances NCNP October 10, 2017 Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine Goal Provide an approach to determine complex acid-base disorders
Acid-Base Disturbances NCNP October 10, 2017 Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine Goal Provide an approach to determine complex acid-base disorders
Basic facts repetition Regulation of A-B balance. Pathophysiology of clinically important disorders
 In The name of God Acid base balance Basic facts repetition Regulation of A-B balance Pathophysiology of clinically important disorders Acid-Base Balance Physiology - The ph of ECF is tightly regulated
In The name of God Acid base balance Basic facts repetition Regulation of A-B balance Pathophysiology of clinically important disorders Acid-Base Balance Physiology - The ph of ECF is tightly regulated
3. Which of the following would be inconsistent with respiratory alkalosis? A. ph = 7.57 B. PaCO = 30 mm Hg C. ph = 7.63 D.
 Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
Pilbeam: Mechanical Ventilation, 4 th Edition Test Bank Chapter 1: Oxygenation and Acid-Base Evaluation MULTIPLE CHOICE 1. The diffusion of carbon dioxide across the alveolar capillary membrane is. A.
3/17/2017. Acid-Base Disturbances. Goal. Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine
 Acid-Base Disturbances Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine Goal Provide an approach to determine complex acid-base disorders Discuss the approach
Acid-Base Disturbances Eric Magaña, M.D. Presbyterian Medical Center Department of Pulmonary and Critical Care Medicine Goal Provide an approach to determine complex acid-base disorders Discuss the approach
Mechanical Ventilation. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
1. What is the acid-base disturbance in this patient?
 /ABG QUIZ QUIZ 1. What is the acid-base disturbance in this patient? Presenting complaint: pneumonia 1 point Uncompensated metabolic alkalosis Partially compensated respiratory alkalosis Mixed alkalosis
/ABG QUIZ QUIZ 1. What is the acid-base disturbance in this patient? Presenting complaint: pneumonia 1 point Uncompensated metabolic alkalosis Partially compensated respiratory alkalosis Mixed alkalosis
Acid/Base Disorders 2015
 Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
Objectives - 2 1. Identify acid/base disorders 2. Discuss etiologies for 1 0 acid/base disorders (will not include mixed disorders) 3. Interpret acid/base disorders by interpreting arterial blood gas &
Blood Gases 2: Acid-Base and Electrolytes Made Simple. Objectives. Important Fact #1
 Blood Gases 2: Acid-Base and Electrolytes Made Simple Gary L. Horowitz, MD Beth Israel Deaconess Medical Center Boston, MA Objectives Identify the 4 major acid-base disturbances, giving typical values
Blood Gases 2: Acid-Base and Electrolytes Made Simple Gary L. Horowitz, MD Beth Israel Deaconess Medical Center Boston, MA Objectives Identify the 4 major acid-base disturbances, giving typical values
Identification and Treatment of the Patient with Sleep Related Hypoventilation
 Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Identification and Treatment of the Patient with Sleep Related Hypoventilation Hillary Loomis-King, MD Pulmonary and Critical Care of NW MI Munson Sleep Disorders Center X Conflict of Interest Disclosures
Acid-Base Balance Workshop. Dr. Najla Al Kuwaiti Dr. Abdullah Al Ameri Dr. Amar Al Shibli
 Acid-Base Balance Workshop Dr. Najla Al Kuwaiti Dr. Abdullah Al Ameri Dr. Amar Al Shibli Objectives Normal Acid-Base Physiology Simple Acid-Base Disorders Compensations and Disorders The Anion Gap Mixed
Acid-Base Balance Workshop Dr. Najla Al Kuwaiti Dr. Abdullah Al Ameri Dr. Amar Al Shibli Objectives Normal Acid-Base Physiology Simple Acid-Base Disorders Compensations and Disorders The Anion Gap Mixed
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Critical Care Monitoring. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Respiratory Pathophysiology Cases Linda Costanzo Ph.D.
 Respiratory Pathophysiology Cases Linda Costanzo Ph.D. I. Case of Pulmonary Fibrosis Susan was diagnosed 3 years ago with diffuse interstitial pulmonary fibrosis. She tries to continue normal activities,
Respiratory Pathophysiology Cases Linda Costanzo Ph.D. I. Case of Pulmonary Fibrosis Susan was diagnosed 3 years ago with diffuse interstitial pulmonary fibrosis. She tries to continue normal activities,
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Interpretation of Arterial Blood Gases (ABG)
") Interpretation of Arterial Blood Gases (ABG) Prof. Dr. W. Vincken Head Respiratory Division Universitair Ziekenhuis Brussel (UZ Brussel) Vrije Universiteit Brussel (VUB) 29-3-2015 W Vincken - UZ Brussel
Interpretation of Arterial Blood Gases (ABG) Prof. Dr. W. Vincken Head Respiratory Division Universitair Ziekenhuis Brussel (UZ Brussel) Vrije Universiteit Brussel (VUB) 29-3-2015 W Vincken - UZ Brussel
Dr. Suzana Voiculescu
 Dr. Suzana Voiculescu AB balance parameters Extracellular ph (plasmatic ph)= 7.35-7.45 < 7.35= acidosis >7.45= alkalosis Kassirer-Bleich equation [H+] = 24 PCO2/ [HCO3-] predicts that the ratio of dissolved
Dr. Suzana Voiculescu AB balance parameters Extracellular ph (plasmatic ph)= 7.35-7.45 < 7.35= acidosis >7.45= alkalosis Kassirer-Bleich equation [H+] = 24 PCO2/ [HCO3-] predicts that the ratio of dissolved
Acids, Bases, and Salts
 Acid / Base Balance Objectives Define an acid, a base, and the measure of ph. Discuss acid/base balance, the effects of acidosis or alkalosis on the body, and the mechanisms in place to maintain balance
Acid / Base Balance Objectives Define an acid, a base, and the measure of ph. Discuss acid/base balance, the effects of acidosis or alkalosis on the body, and the mechanisms in place to maintain balance
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Biochemistry of acid-base disorders. Alice Skoumalová
 Biochemistry of acid-base disorders Alice Skoumalová Main topics of the lecture: Measurement of acid-base dysbalance Classification of the acid-base disorders 4 basic acid-base disorders and their compensaiton
Biochemistry of acid-base disorders Alice Skoumalová Main topics of the lecture: Measurement of acid-base dysbalance Classification of the acid-base disorders 4 basic acid-base disorders and their compensaiton
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
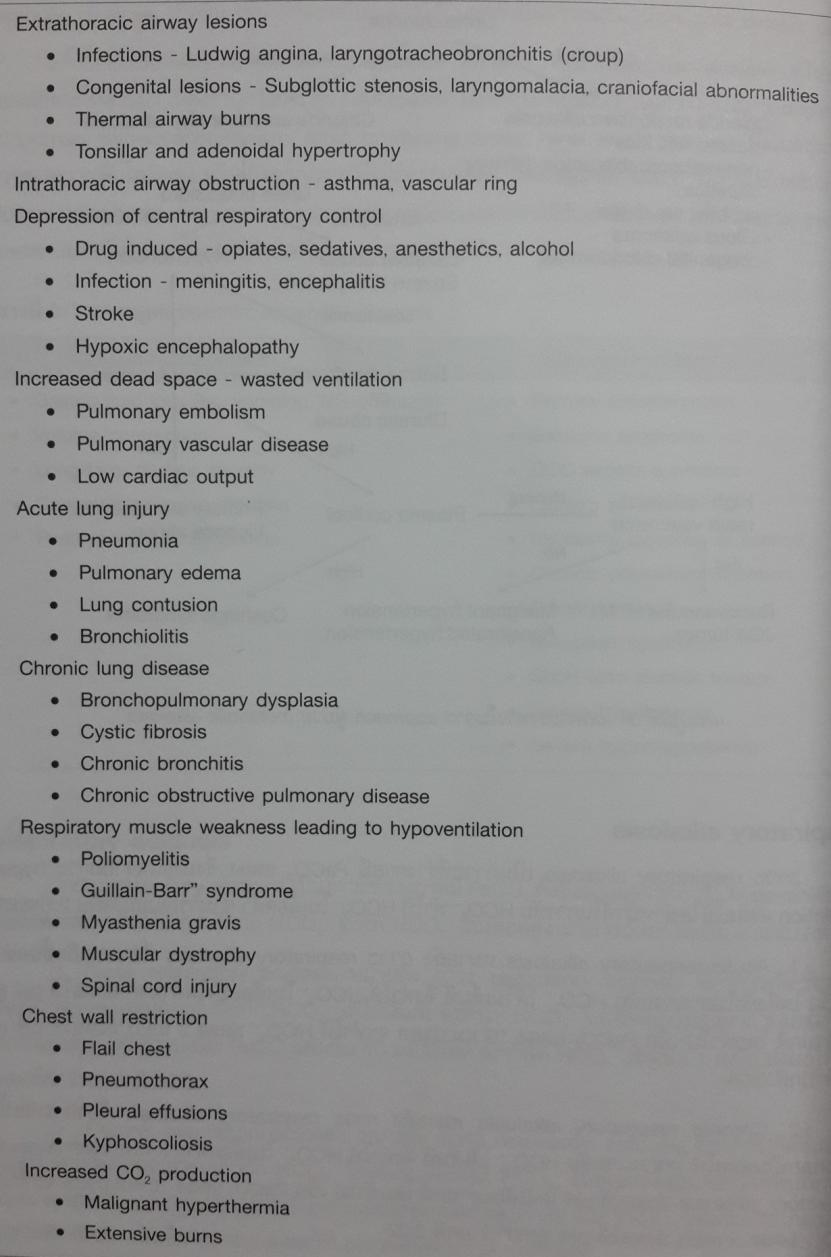
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
The relationship between H+,PaCO₂ and HCO₃ are expressed in the equation of:
 [Acid-Base Balance] [Dr. Bashir Khasawneh] [5 th February 2012] Acid-Base Basic Concepts: The relationship between H+,PaCO₂ and HCO₃ are expressed in the equation of: Which is modified from Henderson-Hasselbach
[Acid-Base Balance] [Dr. Bashir Khasawneh] [5 th February 2012] Acid-Base Basic Concepts: The relationship between H+,PaCO₂ and HCO₃ are expressed in the equation of: Which is modified from Henderson-Hasselbach
There are number of parameters which are measured: ph Oxygen (O 2 ) Carbon Dioxide (CO 2 ) Bicarbonate (HCO 3 -) AaDO 2 O 2 Content O 2 Saturation
 Carbon Dioxide (CO 2 ) Bicarbonate (HCO 3 -) AaDO 2 O 2 Content O 2 Saturation") Arterial Blood Gases (ABG) A blood gas is exactly that...it measures the dissolved gases in your bloodstream. This provides one of the best measurements of what is known as the acid-base balance. The body
Arterial Blood Gases (ABG) A blood gas is exactly that...it measures the dissolved gases in your bloodstream. This provides one of the best measurements of what is known as the acid-base balance. The body
/ABG. It covers acid-base disturbance, respiratory failure, and a small summary for some other derangements. Causes of disturbance
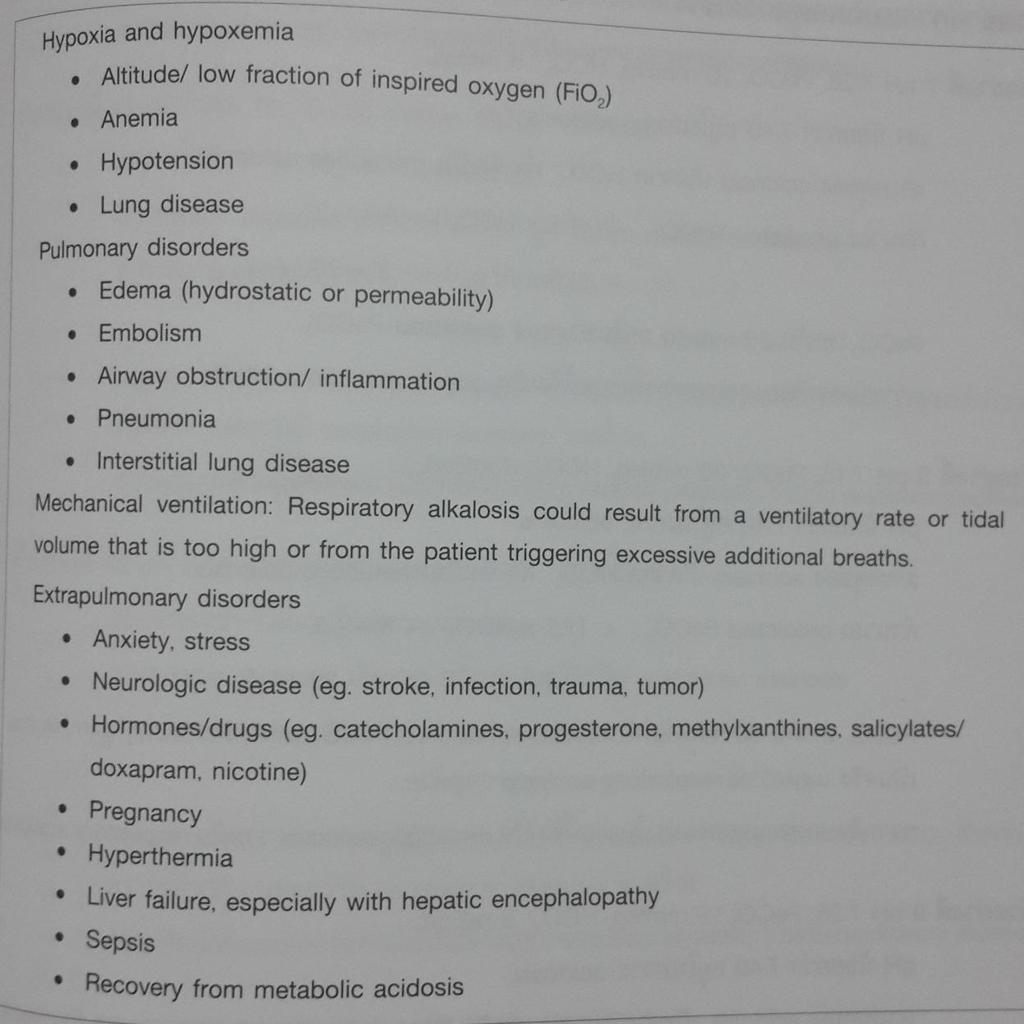
 /ABG This page focuses on providing some possible causes for the various disturbances that may be seen on an ABG. Although not an exhaustive list, it attempts to outline the main headings for possible
/ABG This page focuses on providing some possible causes for the various disturbances that may be seen on an ABG. Although not an exhaustive list, it attempts to outline the main headings for possible
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Objective 2/9/2012. Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. VENOARTERIAL CO2 GRADIENT
 Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
Blood Gas Analysis In The Univentricular Patient: The Need For A Different Perspective. Gary Grist RN CCP Chief Perfusionist The Children s Mercy Hospitals and Clinics Kansas City, Mo. Objective The participant
UNIT VI: ACID BASE IMBALANCE
 UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4
 INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
Acute Respiratory Failure
 Acute Respiratory Failure יובל לאונוב ? Respiratory failure? Respiratory a o y failure Hypoxic Hypercapnic Hypoxemic Respiratory Failure (type I) Hypercapnic Respiratory Failure (type II) Hypercapnic Respiratory
Acute Respiratory Failure יובל לאונוב ? Respiratory failure? Respiratory a o y failure Hypoxic Hypercapnic Hypoxemic Respiratory Failure (type I) Hypercapnic Respiratory Failure (type II) Hypercapnic Respiratory
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
ACID-BASE BALANCE. It is important to remember that more than one of the above processes can be present in a patient at any given time.
 ACID-BASE BALANCE Epidemiology/Pathophysiology Understanding the physiology of acid-base homeostasis is important to the surgeon. The two acid-base buffer systems in the human body are the metabolic system
ACID-BASE BALANCE Epidemiology/Pathophysiology Understanding the physiology of acid-base homeostasis is important to the surgeon. The two acid-base buffer systems in the human body are the metabolic system
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Are you ready to have fun?
 Arterial Blood Gas INTERPRETATION By Nena Bonuel, MSN, RN, CCRN, CNS, ACNS-BC Nurse Specialist, Center for Professional Excellence Are you ready to have fun? 1. Yes! 2. I rather go shopping 3. I still
Arterial Blood Gas INTERPRETATION By Nena Bonuel, MSN, RN, CCRN, CNS, ACNS-BC Nurse Specialist, Center for Professional Excellence Are you ready to have fun? 1. Yes! 2. I rather go shopping 3. I still
to optimize By Jin Xiong Lian, BSN, RN, CNS
 Using ABGs to optimize By Jin Xiong Lian BSN RN CNS AN ARTERIAL BLOOD GAS (ABG) analysis can tell you about the patient s oxygenation (via PaO 2 and SaO 2 ) acid-base balance pulmonary function (through
Using ABGs to optimize By Jin Xiong Lian BSN RN CNS AN ARTERIAL BLOOD GAS (ABG) analysis can tell you about the patient s oxygenation (via PaO 2 and SaO 2 ) acid-base balance pulmonary function (through
Slide 1. Slide 2. Slide 3. Learning Outcomes. Acid base terminology ARTERIAL BLOOD GAS INTERPRETATION
 Slide 1 ARTERIAL BLOOD GAS INTERPRETATION David O Neill MSc BSc RN NMP FHEA Associate Lecturer (Non Medical Prescribing) Cardiff University Advanced Nurse Practitioner Respiratory Medicine Slide 2 Learning
Slide 1 ARTERIAL BLOOD GAS INTERPRETATION David O Neill MSc BSc RN NMP FHEA Associate Lecturer (Non Medical Prescribing) Cardiff University Advanced Nurse Practitioner Respiratory Medicine Slide 2 Learning
Acid-Base Tutorial 2/10/2014. Overview. Physiology (2) Physiology (1)
 Physiology (1)") Overview Acid-Base Tutorial Nicola Barlow Physiology Buffering systems Control mechanisms Laboratory assessment of acid-base Disorders of H + ion homeostasis Respiratory acidosis Metabolic acidosis Respiratory
Overview Acid-Base Tutorial Nicola Barlow Physiology Buffering systems Control mechanisms Laboratory assessment of acid-base Disorders of H + ion homeostasis Respiratory acidosis Metabolic acidosis Respiratory
Acid and Base Balance
 Acid and Base Balance 1 2 The Body and ph Homeostasis of ph is tightly controlled Extracellular fluid = 7.4 Blood = 7.35 7.45 < 7.35: Acidosis (acidemia) > 7.45: Alkalosis (alkalemia) < 6.8 or > 8.0: death
Acid and Base Balance 1 2 The Body and ph Homeostasis of ph is tightly controlled Extracellular fluid = 7.4 Blood = 7.35 7.45 < 7.35: Acidosis (acidemia) > 7.45: Alkalosis (alkalemia) < 6.8 or > 8.0: death
Pulmonary Problems of the Neonate. Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA
 Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Interpretation of ABG. Chandra Shekhar Bala, FCPS( Medicine) Junior Consultant NINS and Hospital, Dhaka
 Junior Consultant NINS and Hospital, Dhaka") Interpretation of ABG Chandra Shekhar Bala, FCPS( Medicine) Junior Consultant NINS and Hospital, Dhaka ABG analysis of Ms Rubi Ms. Rubi, 20 year-old lady PH 7.29 presented with breathlessness. She had
Interpretation of ABG Chandra Shekhar Bala, FCPS( Medicine) Junior Consultant NINS and Hospital, Dhaka ABG analysis of Ms Rubi Ms. Rubi, 20 year-old lady PH 7.29 presented with breathlessness. She had
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Introduction. Invasive Hemodynamic Monitoring. Determinants of Cardiovascular Function. Cardiovascular System. Hemodynamic Monitoring
 Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Introduction Invasive Hemodynamic Monitoring Audis Bethea, Pharm.D. Assistant Professor Therapeutics IV January 21, 2004 Hemodynamic monitoring is necessary to assess and manage shock Information obtained
Case discussion Acute severe asthma during pregnancy. J.G. van der Hoeven
 Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Case discussion Acute severe asthma during pregnancy J.G. van der Hoeven Case (1) 32-year-old female - gravida 3 - para 2 Previous medical history - asthma Pregnant (33 w) Acute onset fever with wheezing
Blood Gases, ph, Acid- Base Balance
 Blood Gases, ph, Acid- Base Balance Blood Gases Acid-Base Physiology Clinical Acid-Base Disturbances Blood Gases Respiratory Gas Exchange Chemical Control of Respiration Dyshemoglobins Oxygen Transport
Blood Gases, ph, Acid- Base Balance Blood Gases Acid-Base Physiology Clinical Acid-Base Disturbances Blood Gases Respiratory Gas Exchange Chemical Control of Respiration Dyshemoglobins Oxygen Transport
Dr. Suzana Voiculescu Discipline of Physiology and Fundamental Neurosciences Carol Davila Univ. of Medicine and Pharmacy
 Dr. Suzana Voiculescu Discipline of Physiology and Fundamental Neurosciences Carol Davila Univ. of Medicine and Pharmacy AB balance parameters Extracellular ph (plasmatic ph)= 7.35-7.45 < 7.35= acidosis
Dr. Suzana Voiculescu Discipline of Physiology and Fundamental Neurosciences Carol Davila Univ. of Medicine and Pharmacy AB balance parameters Extracellular ph (plasmatic ph)= 7.35-7.45 < 7.35= acidosis
ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017
 ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017 WHAT INFORMATION DOES AN ABG GIVE US? ph = measure of hydrogen ion concentration (acidity or alkalinity) PaCO2 = partial pressure
ARTERIAL BLOOD GASES PART 1 BACK TO BASICS SSR OLIVIA ELSWORTH SEPT 2017 WHAT INFORMATION DOES AN ABG GIVE US? ph = measure of hydrogen ion concentration (acidity or alkalinity) PaCO2 = partial pressure
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Acid-Base Imbalance-2 Lecture 9 (12/4/2015) Yanal A. Shafagoj MD. PhD
 Yanal A. Shafagoj MD. PhD") AcidBase Imbalance2 Lecture 9 (12/4/2015) Yanal A. Shafagoj MD. PhD Introduction Disturbance in acidbase balance are common clinical problem that range in severity from mild to life threatening, the acute
AcidBase Imbalance2 Lecture 9 (12/4/2015) Yanal A. Shafagoj MD. PhD Introduction Disturbance in acidbase balance are common clinical problem that range in severity from mild to life threatening, the acute
Chapter 21. Flail Chest. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Flail Chest 1 Figure 21-1. Flail chest. Double fractures of three or more adjacent ribs produce instability of the chest wall and paradoxical motion of the thorax. Inset, Atelectasis, a common
Chapter 21 Flail Chest 1 Figure 21-1. Flail chest. Double fractures of three or more adjacent ribs produce instability of the chest wall and paradoxical motion of the thorax. Inset, Atelectasis, a common
For more information about how to cite these materials visit
 Author(s): John G. Younger, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Author(s): John G. Younger, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
UNIT 9 INVESTIGATION OF ACID-BASE DISTURBANCES
 UNIT 9 INVESTIGATION OF ACIDBASE DISTURBANCES LEARNING OBJECTIVES At the end of this chapter, students must be able to: 1. Describe the main parametres that define the acidbase equilibrium 2. Identify
UNIT 9 INVESTIGATION OF ACIDBASE DISTURBANCES LEARNING OBJECTIVES At the end of this chapter, students must be able to: 1. Describe the main parametres that define the acidbase equilibrium 2. Identify
Case scenario V AV ECMO. Dr Pranay Oza
 Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
Case scenario V AV ECMO Dr Pranay Oza Case Summary 53 y/m, k/c/o MVP with myxomatous mitral valve with severe Mitral regurgitation underwent Mitral valve replacement with mini thoracotomy Pump time nearly
i-stat Alinity v Utilization Guide
 istat Alinity v Utilization Guide The istat Alinity v delivers blood gas, acidbase, electrolyte, chemistry, and hematology measurements in a completely portable, handheld package. Accuracy is ensured by
istat Alinity v Utilization Guide The istat Alinity v delivers blood gas, acidbase, electrolyte, chemistry, and hematology measurements in a completely portable, handheld package. Accuracy is ensured by
Lung Wit and Wisdom. Understanding Oxygenation and Ventilation in the Neonate. Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital
 Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
Acute respiratory failure
 Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Chronic Obstructive Pulmonary Disease
 136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
Inter Inter Pretation of Acid Base Disturbance in Critically ill Patients. By :-: Dr. Vinay Bhomia M.D.
 Inter Inter Pretation of Acid Base Disturbance in Critically ill Patients. By :-: Dr. Vinay Bhomia M.D. Normal Blood PH 7.35 to 7.45 Crucial importance to maintain homeostatic function of Body. Any Significant
Inter Inter Pretation of Acid Base Disturbance in Critically ill Patients. By :-: Dr. Vinay Bhomia M.D. Normal Blood PH 7.35 to 7.45 Crucial importance to maintain homeostatic function of Body. Any Significant
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
Blood Gases / Acid-Base
 Blood Gases / Acid-Base Neonatal Ventilation Workshop June 2010 Dr. Julian Eason Consultant Neonatologist Why are blood gases performed? Diagnostic assessment of oxygenation capacity of lungs Therapeutic
Blood Gases / Acid-Base Neonatal Ventilation Workshop June 2010 Dr. Julian Eason Consultant Neonatologist Why are blood gases performed? Diagnostic assessment of oxygenation capacity of lungs Therapeutic
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Acute Liver Failure: Supporting Other Organs
 Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acute Liver Failure: Supporting Other Organs Michael A. Gropper, MD, PhD Professor of Anesthesia and Physiology Director, Critical Care Medicine University of California San Francisco Acute Liver Failure
Acid Base Balance by: Susan Mberenga RN, BSN, MSN
 Acid Base Balance by: Susan Mberenga RN, BSN, MSN Acid Base Balance Refers to hydrogen ions as measured by ph Normal range: 7.35-7.45 Acidosis/acidemia: ph is less than 7.35 Alkalosis/alkalemia: ph is
Acid Base Balance by: Susan Mberenga RN, BSN, MSN Acid Base Balance Refers to hydrogen ions as measured by ph Normal range: 7.35-7.45 Acidosis/acidemia: ph is less than 7.35 Alkalosis/alkalemia: ph is
Effects of PPV on the Pulmonary System. Chapter 17
 Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
Effects of PPV on the Pulmonary System Chapter 17 Pulmonary Complications Lung Injury Gas distribution Pulmonary blood flow VAP Hypoventilation Hyperventilation Air trapping Oxygen toxicity WOB Patient-Ventilator
BUFFERING OF HYDROGEN LOAD
 BUFFERING OF HYDROGEN LOAD 1. Extracellular space minutes 2. Intracellular space minutes to hours 3. Respiratory compensation 6 to 12 hours 4. Renal compensation hours, up to 2-3 days RENAL HYDROGEN SECRETION
BUFFERING OF HYDROGEN LOAD 1. Extracellular space minutes 2. Intracellular space minutes to hours 3. Respiratory compensation 6 to 12 hours 4. Renal compensation hours, up to 2-3 days RENAL HYDROGEN SECRETION
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
9/13/2015. Laboratory. HPI and PE
 Critical Care HPI and PE 74 yo male confused SBP 90/20 MAP50, P 122, RR 34 Ox1 w/o nuchal rigidity S1S2 wo m RLL reduced breath sounds Skin warm dry Laboratory» WBC 15,600 Hgb 8.4 HCt 23%, Plts 95000,
Critical Care HPI and PE 74 yo male confused SBP 90/20 MAP50, P 122, RR 34 Ox1 w/o nuchal rigidity S1S2 wo m RLL reduced breath sounds Skin warm dry Laboratory» WBC 15,600 Hgb 8.4 HCt 23%, Plts 95000,
Carver College of Medicine University of Iowa
 October 15, 2010 Deborah J. DeWaay MD Assistant Professor of Medicine Associate Vice Chair i of Education Department of Internal Medicine Medical University of South Carolina Joel A. Gordon, MD Professor
October 15, 2010 Deborah J. DeWaay MD Assistant Professor of Medicine Associate Vice Chair i of Education Department of Internal Medicine Medical University of South Carolina Joel A. Gordon, MD Professor
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
ACVECC Small Animal Benchmark, May 2012
 ACVECC Small Animal Benchmark, May 2012 A 25 kg, 9 y MC Labrador Retriever presents with a 2-day history of cough and tachypnea. Physical exam revealed T 101.7 F, HR 120 BPM, pulses strong and synchronous,
ACVECC Small Animal Benchmark, May 2012 A 25 kg, 9 y MC Labrador Retriever presents with a 2-day history of cough and tachypnea. Physical exam revealed T 101.7 F, HR 120 BPM, pulses strong and synchronous,
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE
 VAPOTHERM POCKET GUIDE") Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Tissue Hypoxia and Oxygen Therapy
 Tissue Hypoxia and Oxygen Therapy ก ก ก ก ก ก 1. ก ก 2. ก ก 3. tissue hypoxia 4. ก ก ก 5. ก ก ก 6. ก กก ก 7. ก ก tissue hypoxia ก ก ก ก 1. Pathway of oxygen transport 2. Causes of tissue hypoxia 3. Effect
Tissue Hypoxia and Oxygen Therapy ก ก ก ก ก ก 1. ก ก 2. ก ก 3. tissue hypoxia 4. ก ก ก 5. ก ก ก 6. ก กก ก 7. ก ก tissue hypoxia ก ก ก ก 1. Pathway of oxygen transport 2. Causes of tissue hypoxia 3. Effect
ICU management and referral guidelines for severe hypoxic respiratory failure
 Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory
Aim: ICU management and referral guidelines for severe hypoxic respiratory failure 1) To provide a concise management plan Non ventilatory Ventilatory 2) Timeline for referring patient with refractory