Prof. P.K. Rajiv Head of Newborn division Amrita Institute of Medical Sciences Kochi, India,
|
|
|
- Roland Hampton
- 5 years ago
- Views:
Transcription
1 CPAP Bedside Application in Newborn Prof. P.K. Rajiv Head of Newborn division Amrita Institute of Medical Sciences Kochi, India,
2 Contents 1. Preface 2. Introduction 3. Applied physiology 4. Effects of CPAP 5. Clinical assessment of respiratory distress 6. Indications and contraindications of CPAP 7. CPAP protocol 8. Optimum CPAP 9. Failure of CPAP 10. CPAP and X-rays 11. Blood gas analysis 12. Strategies in specific disorders 13. Case scenarios 14. CPAP devices 15. Setting up CPAP 16. Troubleshooting 17. Weaning from CPAP 18. Complications of CPAP 19. Certain dictums in CPAP management 20. Product information 21. Bibliography 2
3 FOREWORD CPAP: Bedside application in the newborn by PK Rajiv covers an important aspect of ventilatory management in the newborn infant. The popularity of the application of Continuous Positive airway Pressure in the spontaneously breathing infant has gained momentum since its introduction in Most neonatal centres around the world use it as the first line of treatment in preterm Infants at risk of developing hyaline membrane disease. It is also used frequently when weaning infants from mechanical ventilation. Under the circumstance, the advent of this book is timely. It is a step by step guide which takes the student and the clinician through the introduction of CPAP to the sick newborn infant to its weaning as the infant improves. Dr Rajiv has drawn from his extensive experience in India and overseas to develop his own strategies to achieve the desirable outcome in the infants. A wide range of radiographs and figures are used to illustrate his point. A unique feature of this book is the description of the different types of devices available in India for the provision of CPAP to newborn infants. This is a useful book to have in all nurseries. Elizabeth John MD, DCH, FRACP Emeritus Consultant in Neonatology Westmead Hospital, Westmead, NSW
4 Applied physiology A reasonable understanding of pulmonary physiology is elementary in the understanding the approach and bedside management of respiratory disorders. An attempt has been made to synchronize physiological or pathological deviations with ventilatory management. PHYSIOLOGICAL PRINCIPLES The physiological basis of treating any critical newborn lies in the optimization of ventilation and perfusion. Under ideal conditions, Ventilation and Perfusion are evenly matched and the V/Q ratio = 1. FIGURE 2 V=VENTILATION Q=PERFUSION 4
5 VENTILATION (V): Ventilation applies to a physiological tidal volume, which reaches the alveoli and distends it optimally. If the minute ventilation ( tidal volume X rate ) is optimal, the ideal CO2 will be 35 to 45 mm of Hg. Normal tidal volume in neonate is 4 to 6 ml / kg. PERFUSION (Q): This is maintained by the state of dilatation of the pulmonary arterioles and capillaries supplying the air sac. It is controlled to a large extent by systemic blood pressure (Mean Arterial Blood Pressure). Myocardial pump function determines the systemic blood pressure directly. In addition certain physiological variables have to be taken into consideration. Hb content of the blood State of dilation of the air sac (FRC) Nitric Oxide Metabolism (maintains pulmonary arteriolar dilatation) 5
6 Basic Understanding Of Various Lung Units In Disease States. Three-lobe, three compartment model of the lung with V/Q equal to 1 in A, V/Q equal to infinity in B, and V/Q equal to zero in C. Coming into the pulmonary circuit on the left is blood returning from the body and having a low PaO2 (40mmHg) and a high Pa CO2 (46mm Hg ). Mixed blood returning from the lungs is not fully saturated with O2 because of venous admixture from the low V/Q unit C, where the lack of ventilation leaves the Pa O2 unchanged (40mmHg ); SO2 of 75% at a PaO2 of 40 mmhg, and a Pa O2 of 55 mmhg at a SaO2 of 86% 6
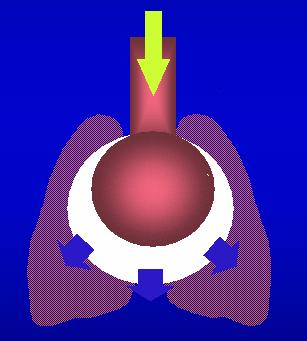
7 (Adapted from Goldsmith : Physiological principles pg 56) Physiological abnormalities in disease states ALVEOLI IS ATELECTATIC The pulmonary arterioles are coiled up leading to less perfusion to those alveoli (Pulmonary hypertension) and if atelectasis is more profound perfusion proportionately is reduced leading to intrapulmonary shunting due to admixture of mixed venous blood into the systemic circulation. The density of the haziness on the X ray is a rough estimate of the blood CO2 levels. V/Q< 1 CO mmhg 7
8 ALVEOLI ARE OPTIMALLY DISTENDED NORMAL LUNG UNDER IDEAL CONDITIONS The pulmonary arterioles unfurl completely and perfuse the alveolar bed completely. V/Q = 1 CO mm Hg ALVEOLAR OVERDISTENTION: 8

9 On the other hand if the alveoli is overdistended due to inappropriate pressures on the ventilator (CPAP), the pulmonary arterioles got stretched to a point where narrowing of their lumen causing pulmonary hypertension leading, to decreased perfusion in the lung and intrapulmonary shunt. The X Ray shows hyperlucent lung fields. V/Q >1 (upto infinity) CO2 =25-30mmHg CONCEPTUAL MODELS OF APPLIED PHYSIOLOGY It would be over simplification of the lung units and the surface area for gas exchange by presenting a model of lung units with 3 generations of alveoli, the collapse of which present with increasing oxygen requirements in atelectatic lung disease. 9
 One generation of alveoli maybe collapsing and it would be")

10 OXYGEN REQUIREMENTS > 40% (FiO2 >0.4) One generation of alveoli maybe collapsing and it would be appropriate to institute assisted ventilation ideally CPAP or IMV at this stage. This would recruit lung volume and optimize gas exchange and prevent morbidity and air leaks. 10
 Two generations of alveoli have collapsed and unless interfered, actively with intubation and ventilation (IMV), air leaks, pulmonary")
 Most generations of alveoli have collapsed and only approximately 1/3 alveolar surface area is available for gas exchange.")
11 OXYGEN REQUIREMENTS > 60% (FiO2 >0.6) Two generations of alveoli have collapsed and unless interfered, actively with intubation and ventilation (IMV), air leaks, pulmonary hypertension and morbidity could occur. OXYGEN REQUIREMENTS > 70-80% (FiO2 > ) Most generations of alveoli have collapsed and only approximately 1/3 alveolar surface area is available for gas exchange. It would be inadvisable to allow a neonate with RDS to progress to this stage. When ventilation (IMV) is resorted to at this stage air leaks, severe pulmonary hypertension and pulmonary hemorrhage could occur. 11
12 From the above discussion it is apparent that EARLY RECRUITMENT OF LUNG VOLUME is essential for optimum ventilation and prevention of morbidity. The early and optimal addition of PEEP or CPAP in lung disease is the sine qua non of ventilatory care and reflects the great variability in morbidity and mortality of various centers dealing in newborn care. A thumb rule in this lung volume recruitment strategy is highlighted below which is basically intended for atelectatic lung disease. FiO2 PEEP CPAP Fi O 2 > 0.4 5cms H2O 6cms Fi O 2 > cms H2O 7-8cms can be tried Fi O 2 > cms H2O Not recommended 12
13 Anatomical considerations The closing volume of alveoli is larger than the FRC until 6-8 years of age. This causes an increased tendency for airway closure at end expiration. Thus, neonates and infants generally benefit from use of continuous positive airway pressure ( CPAP ) in suitable conditions. For the most part, neonates are preferential nose breathers, which easily facilitates the application of nasal CPAP. CPAP is accomplished by inserting nasopharyngeal tubes, affixing nasal prongs, or fitting a nasal mask to the patient. Physiological considerations The application of assisted ventilation requires the basic understanding of a few physiological parameters which are to be assessed in order to optimally ventilate a baby with CPAP Airway resistance Lung compliance 13
 and the stiffness of the lung which is reflected by alveolar collapse (atelectasis) this")
14 The respiratory tract can be simplified into a tube and balloon model to understand the basic concepts of application of CPAP. The baby s ventilation is influenced by the caliber of the air ways (airway resistance) and the stiffness of the lung which is reflected by alveolar collapse (atelectasis) this indicates the lung compliance. Airway resistance 14
15 Lung compliance 15

16 Compliance is defined as the unit change in volume for a given unit change in pressure. In HMD, compliance is extremely low and at the lowest point of the pressure- volume curve. 16

17 Resistance R Resistance of airways Delta P is pressure difference between upper airway and alveoli Delta F is the difference in flow between upper airway and alveoli Airway resistance is directly correlated with the tube length, and divided by the fourth power of tube radius. Inspiratory flow resistance is always less than expiratory flow resistance as the airways dilate during inspiration.in meconium aspiration, the airway resistance is very much increased due to airway debris and bronchospasm., which reduce the cross sectional diameter of the airways significantly. 17
18 Pressure volume loop The work of breathing is best displayed on a pressurevolume curve of one respiratory cycle.the diagram shows the different pathways for inspiration and expiration, known as hysteresis. The total work of breathing of the cycle is the area contained in the loop. 18
 lung which shows minimal change in volume per unit pressure change.")
19 Pressure volume loop in HMD Relationship of lung condition with pressure volume loop The normal lung exhibits good change in volume for a given unit change in pressure. This is in sharp contrast to the atelectatic ( HMD ) lung which shows minimal change in volume per unit pressure change. The direction of arrows show inspiration and expiration respectively. 19
20 The pressure volume curve as it moves towards residual volume (RV) will indicate the severity of atelectasis. The degree of improvement in functional residual capacity (FRC) moves the point towards the middle of the pressure volume curve indicating good change in volume for unit change in pressure. It is evident that as the FRC gets over expanded with excessive CPAP, the change in volume is again reduced for unit change in pressure. TLC denotes total lung capacity CPAP is the major factor determining lung volume. At low CPAP low lung volumes are evidenced as in RDS and compliance is low.at optimum lung 20
21 volumes compliance increases. At still higher volumes (overdistension) compliance again decreases. Optimum FRC results in optimum compliance and the lowest work of breathing. Optimum CPAP is indicative of optimum FRC. Lung volume is also related to airway resistance. At low lung volumes (insufficient CPAP) airway resistance is high and since atelectasis is not resolved, work of breathing is high. At optimum lung volumes airway resistance is low. Thus CPAP can improve distribution of ventilation to optimize FRC and therefore optimize both lung compliance and airway resistance. 21
22 Effects of CPAP The effect of CPAP works on lung mechanics to improve oxygenation (PaO2). The effect on CO2 is only secondary to the primary process of improvement in lung volume and minute ventilation CPAP maintains inspiratory and expiratory pressures above ambient pressure, which should result in an increase in functional residual capacity (FRC) and improvement in static lung compliance and decreased airway resistance in an infant with unstable lung mechanics. This allows a greater volume change per unit of pressure change (i.e., greater tidal volume for a given pressure change) with subsequent reduction in the work of breathing and stabilization of minute ventilation (V E ). The beneficial physiologic effects of CPAP are created by an Increased transpulmonary pressure resulting in an increased functional residual capacity and potentially reduce oxygen demands Stabilization of an unstable chest wall Improves lung compliance ( causes redistribution of fluid in the lungs ) Reduces airway resistance Reduces work of breathing Improvement in ventilation perfusion ratios May expand, or stent, upper airway structures preventing collapse and upper airway obstruction 22
23 Preserves endogenous surfactant. Maintenance of optimal functional residual capacity improves surfactant synthesis and release CPAP and PaO PaO CPAP CPAP PaO2 When CPAP used in RDS (Clinical study from AIMS , Kochi), relationship with PaO 2 is evident and the optimum level of CPAP in preterm appears to be between 7-8cm of H2O CPAP improves oxygenation by an increase in functional residual capacity by recruiting atelectatic alveoli thereby increasing the surface area for gas exchange. The locally vasoconstrited vessels due to underventilation opens up with an increase in functional residual capacity achieved with an appropriate CPAP. These effects decreases 23
24 intrapulmonary shunt and causes a reduction of PaCO2 levels. It stabilizes the chest wall thereby reducing airway resistance. This reduces the work of breathing and improves ventilation perfusion mismatch.the intrapulmonary shunt is reduced. All this add up to cause an increase in PaO2 levels It splints open the upper airway and thus reduces the possibility of obstructive apnea. The application of CPAP increases airway caliber according to their individual compliances lowering the airway resistance.this improves the ventilation of regions of the lung where narrowing of the airway has occurred Application of CPAP stretches the pleura and lungs resulting in stimulation of stretch receptors. This has beneficial effect on mixed and central apnea Alveolar collapse results in a higher consumption of surfactant owing to reduced surface area, and CPAP could conserve surfactant by prevention of collapse or enhancement of surfactant release through a cholinergic mechanism. This may explain why CPAP is more effective when used early in the course of the disease while most alveoli are open. Early application of CPAP is seen to reduce the need for mechanical ventilation 24
25 CPAP PaO2 PaCO2 CPAP in RDS and relationship with PaO 2 and PaCO 2 (Clinical study from AIMS, Kochi ) It appears from this study that CPAP levels beyond 8 cm of H2O should be used cautiously in preterm babies. With high CPAP levels,a reduction in tidal volume occurs resulting in hypercarbia and hypoxemia. A reduction in CPAP level at this point would result in an improvement of ventilation Long term implication Maintaining lung volumes within the optimal range between atelectasis and over distension have been found to decrease the incidence and severity of later chronic lung disease 25
26 Cardiovascular stability High CPAP can have a detrimental effect on the cardiovascular system. The effects include Compression of right sided vessels thereby decreasing cardiac return resulting in decreased cardiac output. Decreased peripheral and regional blood flow Decrease in oxygen available to tissue Increase in pulmonary vascular resistance and thereby increase extrapulmonary shunts Decrease in cardiac output can lead to acidosis, tachycardia and reduced arterial blood pressure. The amount of CPAP that is excessive will produce this effect depends on the lung compliance. If the lung compliance is low ( HMD ), less intra airway pressure will be transmitted to the pleural space and cardiac compromise will be less. Hypovolemia will exacerbate the negative effect of high CPAP. Excessive CPAP may be detected by the development of acidosis, decreased dynamic lung compliance and increased carbon dioxide retention. A trial of lower CPAP or increased intravenous fluids will resolve the problem. However it should be recalled that too low a CPAP will also cause acidosis ( respiratory ) due to atelectasis.. A precise level based on the operators experience would be instrumental before conclusions could be drawn on the level. It would be grave mistake to experiment with CPAP levels in a critically ill baby Sequence of events in excessive CPAP 26
27 Tachycardia increased capillary filling time fall in blood pressure diminished urine output acidosis ( metabolic ). Blood PCO2 may initially fall to rise subsequently over a period due to gas trapping. Renal system CPAP can result in decrease in glomerular filtration rate and thus the urine output. Renal effects are directly proportional to compliance of the chest wall. Decreased renal blood flow results in increased aldosterone and ADH secretion Gastrointestinal tract Abdominal distension can occur in babies on CPAP. It is compounded by presence of immature gut in preterms and decrease in blood flow to the gut. All these together lead to what is called as CPAP belly syndrome. Clinically the baby develops increased abdominal girth and dilated bowel loops, which may cause upward pressure on diaphragm and respiratory compromise. Central nervous system There is increase in intracranial pressure (ICP) with application of CPAP. This, in combination with decrease in arterial pressure, results in decrease in cerebral perfusion pressure (CPP). Increase in ICP is seen more with head box CPAP than with endotracheal CPAP or nasal prongs. High ICP is instrumental in pathogenesis of intraventricular hemorrhage in low birth 27
28 weight babies ventilated for RDS. Head box CPAP is not used currently. The significance of this finding in clinical practice is not evidenced with the current CPAP devices and protocols (Gregory GA. Continuous positive airway pressure. Neonatal Pulmonary care.2 nd ed. Norwalk, CT, Appleton and Lang, p 355) It is evident that when CPAP pressure exceeds 6 cm of H20 and especially when it nears 8 cm of H2O, significant increase in central venous pressure coincides with decreases in PaO2 levels and increased PaCO2 levels. 28
29 OPTIMUM CPAP It is the level of CPAP that results in maximum PaO2 on lowest FiO2 without increase in PaCO2 in the absence of any adverse hemodynamic effects Optimum CPAP CPAP is considered optimum when the baby on CPAP is Comfortable and pink Has normal blood pressure and normal capillary filling time Has no respiratory distress No cyanosis Audible air entry on auscultation SpO2 more than % ABG : PaO / PaCO /p H Optimal chest expansion ( Chest X ray in supine : Post. Intercostal space 7-8 Impovement in air entry is also a good measure of improvement with CPAP expecially in baby more than 1.5 kg. 29
30 Road to Optimum CPAP Optimising CPAP requirement is an art. The decision is based on the underlying lung condition, disease pattern, pressure requirement, opacity of chest X-ray, ABG and the clinical condition. Always increase pressure in increments of 1 cm and observe the effect. In our unit, we start CPAP at 6 cm H2O in atelectatic disorders guided by the clinical status and the degree of opacification on chest X-ray.Clinically there should be an improvement in chest recessions and tachypnea, The degree of expansion of the lungs is assessed by an X-ray is taken within 4-6 hrs after initiation of CPAP. A decrease in FiO2 requirement would suggest an improvement of the oxygenation status. Of all the parameters assessed, objectivity is best maintained with chest X ray and ABG a) Based on Chest X-ray: Presence of 8 posterior intercostals spaces above diaphragm indicates optimum CPAP.Less than 6 intercostal spaces indicates low volume lungs in an inspiratory film.a low lung volume as evidenced by chest X ray may require an increase in CPAP level.presence of more than 8 spaces with flat dome of diaphragm indicates hyperinflation which could be one of the indication to decrease the level of CPAP. b) ABG ABG is done within 20 mins of setting CPAP.ABG is preferable done after any subsequent change of pressure within 15 to 30 minutes. Increasing PaO2 with decreasing FiO2 30
31 requirement indicates that the baby is on road to optimum CPAP.If PaO2 falls with increase of CPAP,it could imply over distension of lungs. This may necessitate decrease of CPAP pressure.paco2 generally increases with increasing pressure. Accept mild CO2 retention if the need is to improve oxygenation with increasing pressures. Measures to maintain optimum CPAP Correctly set up and maintain low resistance delivery circuit Securely attach interface Assure minimal pressure leaks Maintain optimal airway Prevent nasal septal injury Provide meticulous attention to detail Success with CPAP Remaining without ventilatory support for more than 3 days The author feels that experimenting with CPAP levels is dangerous. It should be based on the trend shown in oxygen saturations, the XRay and ABG. 31
32 This is useful only as a guideline in mild to moderate respiratory distress syndrome. It is not useful for severe Respiratory distress syndrome. The numerical projections superimposed on the pressure volume curve is based on the bedside application of CPAP levels in mild to moderate RDS, It is not an absolute value, but will serve as an important guideline to initiate management and titrate the CPAP level with X Rays and blood gas PaO2. 32

33 FiO2 and appropriate blood gas Conceptual Model 0.4 ph pco ph pco2-45 ph pco2-65 FiO2 CPAP 33
34 It is evident that once the CPAP reaches more than optimum for the disease process, an inverse relationship will start establishing between PaO 2 and PaCO 2 (Clinical study from AIMS, Kochi).This is seen when the X-ray expansion crosses 8 spaces. 34
 Expected CO2 50-55 mm Hg CPAP")
35 CXR showing deflation (Posterior ICS of <7spaces) Expected CO mm Hg CPAP 5cmH2O 35
 Expected CO2 30-35 mm Hg CPAP 6-7 Cm H2O")
36 CXR showing adequate chest expansion (Posterior Intercostal spaces of 8 nos) Expected CO mm Hg CPAP 6-7 Cm H2O 36
 Expected CO2 25-28 mm Hg CPAP 8-9 cm")
37 CXR showing over expansion (Posterior ICS of >9 spaces Flattening of diaphragm) Expected CO mm Hg CPAP 8-9 cm H2O 37



38 Hyaline Membrane disease and CPAP Expected CO mm Hg CPAP- 5cm H2O Fig 1 Expected CO mm Hg 38 CPAP 6cm H2O Fig2

39 Expected CO mm Hg CPAP- 7cmH2O Fig 3 CPAP 7 Fig 1 CPAP 6 Fig 2 CPAP 5 Fig


40 Pneumonia and CPAP Expected CO mm Hg CPAP- 5cmH2O Fig 1 Expected CO mm Hg 40 CPAP- 6cmH2O Fig 2

41 Expected CO mm Hg CPAP- 7cmH2O Fig3 Fig 3 Fig 2 Fig 1 41
42 I *It is vital to consider invasive ventilation once the FiO 2 crosses 0.6 as well as the CPAP requirement increases more than 8 cm of H2O. Upper limits of CPAP are still un-defined. But current evidence points on an upper limit of 8 cm of H2O in preterm infants and 9 cm of H2O in term babies. The author opines that the use of so called higher CPAP should not be based on numbers and their restrictions thereof.the clearance of haziness on X-ray should be the end point in the successful application of CPAP within the purview of haemodynamic stability. 42
43 In our unit, we may consider using CPAP within 30 minutes after birth for preterm babies below 28 weeks of gestational age, and for babies above that gestation we start once the clinical features of distress appears. ( refer protocol ) BABY-A: Moderate RDS with Failure of CPAP Preterm 940 gm born to primigravida mother with PIH on nicardia and methyl dopa, No h/o DM, leaking or bleeding PV, delivered by LSCS ( Indication: decrease fetal movements ) with apgar 5 & 7 at 1 and 5 min.baby had tachypnea, Grunt, Inter Costal retractions, sub costal retractions. Baby was put on CPAP 6 (fig 1) and gradually increased to 7 along with FiO2 increased from 0.4 to 0.6 as per protocol. (fig 2) The baby had clinically more retractions with loss of lung volume and hence was electively ventilated, despite bloodgas ph of 7.26 and CO2 of 56mmHg.(fig 3) 43


44 44 Fig 1

45 Fig 2 fig 3 Fig 3 45
46 APNEA OF PREMATURITY: Studies have shown that CPAP has reduced the incidence and severity of Mixed and Obstructive apnea by preventing the collapse of upper airways and pharynx and by splinting the diaphragm. Since the lung in this condition is usually normal, use low to moderate levels of CPAP. Pressures between 4 5 cms of H2O can be used with FiO2 as low as possible to maintain O2 saturation between 88-90% along with medical management. The initial CPAP would be 5 cm of H2O, but if the saturations exceed 95% or the X ray spaces exceed 8, it is worthwhile to reduce the CPAP to 4 cm of H2O. Try to wean off the baby from CPAP once baby is free of apneic episodes for more than 24 hours CPAP 4 to 5 cm of H2O In our unit,we do not use CPAP less than 4 cm of H2O. A CPAP below this level can actually increase the work of breathing since the unphysiological CPAP delivered to the distal airways can lead to collapse Baby-B: Apnea of Prematurity Born by preterm 29wks, Primigravida mother-41yrs of age, Severe PIH on methyl dopa & Nicardia, and Hypothyroidism on eltoxin. 27wks USG and Doppler study showing Utero- Placental insufficiency 46

47 2 doses of Betnesol received, Delivered by LSCS. B.wt 856gms, baby developed apnea and was put on CPAP 5 at FiO which was reduced to CPAP of 4 due to the lung over expansion and bloodgas PCO2 25mmHg. Aminophylline was started after birth. There after baby improved without apnea. 47
48 48
INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2
 2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
2 Effects of CPAP INTRODUCTION The effect of CPAP works on lung mechanics to improve oxygenation (PaO 2 ). The effect on CO 2 is only secondary to the primary process of improvement in lung volume and
Practical Application of CPAP
 CHAPTER 3 Practical Application of CPAP Dr. Srinivas Murki Neonatologist Fernadez Hospital, Hyderabad. A.P. Practical Application of CPAP Continuous positive airway pressure (CPAP) applied to premature
CHAPTER 3 Practical Application of CPAP Dr. Srinivas Murki Neonatologist Fernadez Hospital, Hyderabad. A.P. Practical Application of CPAP Continuous positive airway pressure (CPAP) applied to premature
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION
 DEFINITION") CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) DEFINITION Method of maintaining low pressure distension of lungs during inspiration and expiration when infant breathing spontaneously Benefits Improves oxygenation
Hyaline membrane disease. By : Dr. Ch Sarishma Peadiatric Pg
 Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
Hyaline membrane disease By : Dr. Ch Sarishma Peadiatric Pg Also called Respiratory distress syndrome. It occurs primarily in premature infants; its incidence is inversely related to gestational age and
October Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE
 October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
October 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give
1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation.
 Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
Chapter 1: Principles of Mechanical Ventilation TRUE/FALSE 1. When a patient fails to ventilate or oxygenate adequately, the problem is caused by pathophysiological factors such as hyperventilation. F
APRV Ventilation Mode
 APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
APRV Ventilation Mode Airway Pressure Release Ventilation A Type of CPAP Continuous Positive Airway Pressure (CPAP) with an intermittent release phase. Patient cycles between two levels of CPAP higher
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
Presented By : Kamlah Olaimat
 Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
Presented By : Kamlah Olaimat 18\7\2010 Transient Tachpnea of the Definition:- newborn (TTN) TTN is a benign disease of near term or term infant who display respiratory distress shortly after delivery.
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
AEROSURF Phase 2 Program Update Investor Conference Call
 AEROSURF Phase 2 Program Update Investor Conference Call November 12, 2015 Forward Looking Statement To the extent that statements in this presentation are not strictly historical, including statements
AEROSURF Phase 2 Program Update Investor Conference Call November 12, 2015 Forward Looking Statement To the extent that statements in this presentation are not strictly historical, including statements
Lecture Notes. Chapter 2: Introduction to Respiratory Failure
 Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Lecture Notes Chapter 2: Introduction to Respiratory Failure Objectives Define respiratory failure, ventilatory failure, and oxygenation failure List the causes of respiratory failure Describe the effects
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Simulation 08: Cyanotic Preterm Infant in Respiratory Distress
 Flow Chart Simulation 08: Cyanotic Preterm Infant in Respiratory Distress Opening Scenario Section 1 Type: DM As staff therapist assigned to a Level 2 NICU in a 250 bed rural medical center you are called
Flow Chart Simulation 08: Cyanotic Preterm Infant in Respiratory Distress Opening Scenario Section 1 Type: DM As staff therapist assigned to a Level 2 NICU in a 250 bed rural medical center you are called
Handling Common Problems & Pitfalls During. Oxygen desaturation in patients receiving mechanical ventilation ACUTE SEVERE RESPIRATORY FAILURE
 Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Handling Common Problems & Pitfalls During ACUTE SEVERE RESPIRATORY FAILURE Pravit Jetanachai, MD QSNICH Oxygen desaturation in patients receiving mechanical ventilation Causes of oxygen desaturation 1.
Cardiorespiratory Physiotherapy Tutoring Services 2017
 VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
VENTILATOR HYPERINFLATION ***This document is intended to be used as an information resource only it is not intended to be used as a policy document/practice guideline. Before incorporating the use of
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Surfactant Administration
 Approved by: Surfactant Administration Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual
Approved by: Surfactant Administration Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures Manual
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
Respiratory Physiology
 Respiratory Physiology Dr. Aida Korish Associate Prof. Physiology KSU The main goal of respiration is to 1-Provide oxygen to tissues 2- Remove CO2 from the body. Respiratory system consists of: Passages
Respiratory Physiology Dr. Aida Korish Associate Prof. Physiology KSU The main goal of respiration is to 1-Provide oxygen to tissues 2- Remove CO2 from the body. Respiratory system consists of: Passages
INDEPENDENT LUNG VENTILATION
 INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
INDEPENDENT LUNG VENTILATION Giuseppe A. Marraro, MD Director Anaesthesia and Intensive Care Department Paediatric Intensive Care Unit Fatebenefratelli and Ophthalmiatric Hospital Milan, Italy gmarraro@picu.it
Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor
 Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Mechanical Ventilation Prepared by : Bayan Kaddourah RN,MHM. GICU Clinical Instructor 1 Definition Is a supportive therapy to facilitate gas exchange. Most ventilatory support requires an artificial airway.
Review of Neonatal Respiratory Problems
 Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Review of Neonatal Respiratory Problems Respiratory Distress Occurs in about 7% of infants Clinical presentation includes: Apnea Cyanosis Grunting Inspiratory stridor Nasal flaring Poor feeding Tachypnea
Lecture Notes. Chapter 9: Smoke Inhalation Injury and Burns
 Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lecture Notes Chapter 9: Smoke Inhalation Injury and Burns Objectives List the factors that influence mortality rate Describe the nature of smoke inhalation and the fire environment Recognize the pulmonary
Lung Wit and Wisdom. Understanding Oxygenation and Ventilation in the Neonate. Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital
 Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
Lung Wit and Wisdom Understanding Oxygenation and Ventilation in the Neonate Jennifer Habert, BHS-RT, RRT-NPS, C-NPT Willow Creek Women s Hospital Objectives To review acid base balance and ABG interpretation
Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study
 D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
D-32084-2011 Volume Guarantee Initiation and ongoing clinical management of an infant supported by Volume Guarantee A Case Study Robert DiBlasi RRT-NPS, FAARC Respiratory Care Manager of Research & Quality
Pulmonary Problems of the Neonate. Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA
 Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
Pulmonary Problems of the Neonate Jon Palmer, VMD, DACVIM Chief, Neonatal Intensive Care Service New Bolton Center, University of Pennsylvania, USA Lower Respiratory Diseases Ventilation/Perfusion Abnormalities
ROLE OF EARLY POSTNATAL DEXAMETHASONE IN RESPIRATORY DISTRESS SYNDROME
 INDIAN PEDIATRICS VOLUME 35-FEBRUAKY 1998 ROLE OF EARLY POSTNATAL DEXAMETHASONE IN RESPIRATORY DISTRESS SYNDROME Kanya Mukhopadhyay, Praveen Kumar and Anil Narang From the Division of Neonatology, Department
INDIAN PEDIATRICS VOLUME 35-FEBRUAKY 1998 ROLE OF EARLY POSTNATAL DEXAMETHASONE IN RESPIRATORY DISTRESS SYNDROME Kanya Mukhopadhyay, Praveen Kumar and Anil Narang From the Division of Neonatology, Department
Chronic Obstructive Pulmonary Disease
 136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Ventilator Waveforms: Interpretation
 Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
Respiratory Failure. Causes of Acute Respiratory Failure (ARF): a- Intrapulmonary:
: a- Intrapulmonary:") Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
Respiratory failure exists whenever the exchange of O 2 for CO 2 in the lungs cannot keep up with the rate of O 2 consumption & CO 2 production in the cells of the body. This results in a fall in arterial
RESPIRATORY FAILURE. Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics
 RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
RESPIRATORY FAILURE Michael Kelly, MD Division of Pediatric Critical Care Dept. of Pediatrics What talk is he giving? DO2= CO * CaO2 CO = HR * SV CaO2 = (Hgb* SaO2 * 1.34) + (PaO2 * 0.003) Sound familiar??
SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY
 PS1006 SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY TITLE: NON-INVASIVE VENTILATION FOR THE Job Title of Reviewer: EFFECTIVE DATE: REVISED DATE: Director, Respiratory Care Services 126.685 (neo) 3/26/15
PS1006 SARASOTA MEMORIAL HOSPITAL DEPARTMENT POLICY TITLE: NON-INVASIVE VENTILATION FOR THE Job Title of Reviewer: EFFECTIVE DATE: REVISED DATE: Director, Respiratory Care Services 126.685 (neo) 3/26/15
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
APPENDIX VI HFOV Quick Guide
 APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
APPENDIX VI HFOV Quick Guide Overall goal: Maintain PH in the target range at the minimum tidal volume. This is achieved by favoring higher frequencies over lower P (amplitude). This goal is also promoted
PROCEDURE (TASK): CONTINUOUS DISTENDING PRESSURE THERAPY (CPAP) (NEONATAL/PEDIATRICS)
: CONTINUOUS DISTENDING PRESSURE THERAPY (CPAP) (NEONATAL/PEDIATRICS)") PROCEDURE (TASK): CONTINUOUS DISTENDING PRESSURE THERAPY (CPAP) (NEONATAL/PEDIATRICS) I. KEY PERFORMANCE ELEMENTS Procedural Element (Step): Description of Satisfactory Performance: 5. Obtains baseline
PROCEDURE (TASK): CONTINUOUS DISTENDING PRESSURE THERAPY (CPAP) (NEONATAL/PEDIATRICS) I. KEY PERFORMANCE ELEMENTS Procedural Element (Step): Description of Satisfactory Performance: 5. Obtains baseline
Usefulness of DuoPAP in the treatment of very low birth weight preterm infants with neonatal respiratory distress syndrome
 European Review for Medical and Pharmacological Sciences 2015; 19: 573-577 Usefulness of DuoPAP in the treatment of very low birth weight preterm infants with neonatal respiratory distress syndrome B.
European Review for Medical and Pharmacological Sciences 2015; 19: 573-577 Usefulness of DuoPAP in the treatment of very low birth weight preterm infants with neonatal respiratory distress syndrome B.
PUMANI bcpap GUIDELINES FOR CLINICIANS. An Overview of the Pumani bcpap, Indications for bcpap, and Instructions for Use
 An Overview of the Pumani bcpap, Indications for bcpap, and Instructions for Use What is bcpap? bcpap stands for bubble Continuous Positive Airway Pressure. Sometimes called Continuous Distending Pressure,
An Overview of the Pumani bcpap, Indications for bcpap, and Instructions for Use What is bcpap? bcpap stands for bubble Continuous Positive Airway Pressure. Sometimes called Continuous Distending Pressure,
Mechanical Ventilation 1. Shari McKeown, RRT Respiratory Services - VGH
 Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Mechanical Ventilation 1 Shari McKeown, RRT Respiratory Services - VGH Objectives Describe indications for mcvent Describe types of breaths and modes of ventilation Describe compliance and resistance and
Guidelines and Best Practices for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) NICU POCKET GUIDE
 NICU POCKET GUIDE") Guidelines and Best Practices for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) TM NICU POCKET GUIDE Patient Selection Diagnoses Patient presents with one or more of the following symptoms: These
Guidelines and Best Practices for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) TM NICU POCKET GUIDE Patient Selection Diagnoses Patient presents with one or more of the following symptoms: These
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
NAVA. In Neonates. Howard Stein, M.D. Director Neonatology. Neurally Adjusted Ventilatory Assist. Toledo Children s Hospital Toledo, Ohio
 NAVA Neurally Adjusted Ventilatory Assist In Neonates Howard Stein, M.D. Director Neonatology Toledo Children s Hospital Toledo, Ohio Disclaimers Dr Stein: Is discussing products made by Maquet Has no
NAVA Neurally Adjusted Ventilatory Assist In Neonates Howard Stein, M.D. Director Neonatology Toledo Children s Hospital Toledo, Ohio Disclaimers Dr Stein: Is discussing products made by Maquet Has no
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Chapter 21. Flail Chest. Mosby items and derived items 2011, 2006 by Mosby, Inc., an affiliate of Elsevier Inc.
 Chapter 21 Flail Chest 1 Figure 21-1. Flail chest. Double fractures of three or more adjacent ribs produce instability of the chest wall and paradoxical motion of the thorax. Inset, Atelectasis, a common
Chapter 21 Flail Chest 1 Figure 21-1. Flail chest. Double fractures of three or more adjacent ribs produce instability of the chest wall and paradoxical motion of the thorax. Inset, Atelectasis, a common
Simulation 3: Post-term Baby in Labor and Delivery
 Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
GE Healthcare. Non Invasive Ventilation (NIV) For the Engström Ventilator. Relief, Relax, Recovery
 For the Engström Ventilator. Relief, Relax, Recovery") GE Healthcare Non Invasive Ventilation (NIV) For the Engström Ventilator Relief, Relax, Recovery COPD is currently the fourth leading cause of death in the world, and further increases in the prevalence
GE Healthcare Non Invasive Ventilation (NIV) For the Engström Ventilator Relief, Relax, Recovery COPD is currently the fourth leading cause of death in the world, and further increases in the prevalence
Critical Care Monitoring. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure.
 B. 10 Applied Respiratory Physiology a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure. Intermittent positive pressure ventilation
B. 10 Applied Respiratory Physiology a. Describe the physiological consequences of intermittent positive pressure ventilation and positive end-expiratory pressure. Intermittent positive pressure ventilation
1
 1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
1 2 3 RIFAI 5 6 Dublin cohort, retrospective review. Milrinone was commenced at an initial dose of 0.50 μg/kg/minute up to 0.75 μg/kg/minute and was continued depending on clinical response. No loading
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE
 VAPOTHERM POCKET GUIDE") Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy
 An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
An Overview of Bronchopulmonary Dysplasia and Chronic Lung Disease in Infancy Housekeeping: I have no financial disclosures Learning objectives: Develop an understanding of bronchopulmonary dysplasia (BPD)
Objectives. Apnea Definition and Pitfalls. Pathophysiology of Apnea. Apnea of Prematurity and hypoxemia episodes 5/18/2015
 Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Apnea of Prematurity and hypoxemia episodes Deepak Jain MD Care of Sick Newborn Conference May 2015 Objectives Differentiating between apnea and hypoxemia episodes. Pathophysiology Diagnosis of apnea and
Capnography Connections Guide
 Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Table 1: The major changes in AHA / AAP neonatal resuscitation guidelines2010 compared to previous recommendations in 2005
 Table 1: The major changes in AHA / AAP neonatal guidelines2010 compared to previous recommendations in 2005 Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE 1) Assessment
Table 1: The major changes in AHA / AAP neonatal guidelines2010 compared to previous recommendations in 2005 Resuscitation step Recommendations (2005) Recommendations (2010) Comments/LOE 1) Assessment
Kugelman A, Riskin A, Said W, Shoris I, Mor F, Bader D.
 Heated, Humidified High-Flow Nasal Cannula (HHHFNC) vs. Nasal Intermittent Positive Pressure Ventilation (NIPPV) for the Primary Treatment of RDS, A Randomized, Controlled, Prospective, Pilot Study Kugelman
Heated, Humidified High-Flow Nasal Cannula (HHHFNC) vs. Nasal Intermittent Positive Pressure Ventilation (NIPPV) for the Primary Treatment of RDS, A Randomized, Controlled, Prospective, Pilot Study Kugelman
IRDS, Infantile Respiratory Distress Syndrome
 IRDS, Infantile Respiratory Distress Syndrome - RDS is the leading cause of death in the newborns, and the most common cause of death first 15 years of life (excluding the malformed babies). - RDS is the
IRDS, Infantile Respiratory Distress Syndrome - RDS is the leading cause of death in the newborns, and the most common cause of death first 15 years of life (excluding the malformed babies). - RDS is the
Mechanical Ventilation. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
1 Mechanical Ventilation Assessing the Adequacy of 2 Tissue oxygenation is the end-product of many complex steps - Step 1 3 Oxygen must be made available to alveoli 1 - Step 2 4 Oxygen must cross the alveolarcapillary
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
بسم هللا الرحمن الرحيم
 بسم هللا الرحمن الرحيم Yesterday we spoke of the increased airway resistance and its two examples: 1) emphysema, where we have destruction of the alveolar wall and thus reducing the area available for
بسم هللا الرحمن الرحيم Yesterday we spoke of the increased airway resistance and its two examples: 1) emphysema, where we have destruction of the alveolar wall and thus reducing the area available for
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials
 Certification Preparatory Materials") Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
Neonatal Life Support Provider (NLSP) Certification Preparatory Materials NEONATAL LIFE SUPPORT PROVIDER (NRP) CERTIFICATION TABLE OF CONTENTS NEONATAL FLOW ALGORITHM.2 INTRODUCTION 3 ANTICIPATION OF RESUSCITATION
VENTILATOR GRAPHICS ver.2.0. Charles S. Williams RRT, AE-C
 VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
VENTILATOR GRAPHICS ver.2.0 Charles S. Williams RRT, AE-C Purpose Graphics are waveforms that reflect the patientventilator system and their interaction. Purposes of monitoring graphics: Allow users to
Dr. AM MAALIM KPA 2018
 Dr. AM MAALIM KPA 2018 Journey Towards Lung protection Goals of lung protection Strategies Summary Conclusion Before 1960: Oxygen; impact assessed clinically. The 1960s:President JFK, Ventilators mortality;
Dr. AM MAALIM KPA 2018 Journey Towards Lung protection Goals of lung protection Strategies Summary Conclusion Before 1960: Oxygen; impact assessed clinically. The 1960s:President JFK, Ventilators mortality;
SWISS SOCIETY OF NEONATOLOGY. Supercarbia in an infant with meconium aspiration syndrome
 SWISS SOCIETY OF NEONATOLOGY Supercarbia in an infant with meconium aspiration syndrome January 2006 2 Wilhelm C, Frey B, Department of Intensive Care and Neonatology, University Children s Hospital Zurich,
SWISS SOCIETY OF NEONATOLOGY Supercarbia in an infant with meconium aspiration syndrome January 2006 2 Wilhelm C, Frey B, Department of Intensive Care and Neonatology, University Children s Hospital Zurich,
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal
 Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
Advanced Monitoring of Cardiovascular and Respiratory Systems in Infants Kuwait 2018 Dr. Yasser Elsayed, MD, PhD Director of the Targeted Neonatal Echocardiography, Point of Care and Hemodynamics Program
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Non Invasive Ventilation In Preterm Infants. Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid
 Non Invasive Ventilation In Preterm Infants Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid Summary Noninvasive ventilation begings in the delivery room
Non Invasive Ventilation In Preterm Infants Manuel Sanchez Luna Hospital General Universitario Gregorio Marañón Complutense University Madrid Summary Noninvasive ventilation begings in the delivery room
Nitric Resource Manual
 Nitric Resource Manual OBJECTIVES Describe the biologic basis for inhaled nitric oxide therapy Describe the indications for inhaled nitric oxide therapy Describe the potential hazards, side effects and
Nitric Resource Manual OBJECTIVES Describe the biologic basis for inhaled nitric oxide therapy Describe the indications for inhaled nitric oxide therapy Describe the potential hazards, side effects and
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Respiration Lesson 3. Respiration Lesson 3
 Respiration Lesson 3 and Airway Resistance (key factors affecting air flow) 1) What is the arterial blood pressure in a healthy 18 year old male? 2) What would his venous blood pressure be? 3) What is
Respiration Lesson 3 and Airway Resistance (key factors affecting air flow) 1) What is the arterial blood pressure in a healthy 18 year old male? 2) What would his venous blood pressure be? 3) What is
The Art and Science of Weaning from Mechanical Ventilation
 The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
The Art and Science of Weaning from Mechanical Ventilation Shekhar T. Venkataraman M.D. Professor Departments of Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Some definitions
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
ADVANCED ASSESSMENT Respiratory System
 ONTARIO BASE HOSPITAL GROUP QUIT ADVANCED ASSESSMENT Respiratory System 2007 Ontario Base Hospital Group ADVANCED ASSESSMENT Respiratory System AUTHOR(S) Mike Muir AEMCA, ACP, BHSc Paramedic Program Manager
ONTARIO BASE HOSPITAL GROUP QUIT ADVANCED ASSESSMENT Respiratory System 2007 Ontario Base Hospital Group ADVANCED ASSESSMENT Respiratory System AUTHOR(S) Mike Muir AEMCA, ACP, BHSc Paramedic Program Manager
Paediatric Respiratory Workbook
 2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give you an
2017 Paediatric Respiratory Workbook APCP RESPIRATORY COMMITTEE This workbook is designed to introduce to you the difference between paediatric and adult anatomy and physiology. It will also give you an
BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT
, RPSGT") BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT Modes Continuous Positive Airway Pressure (CPAP): One set pressure which is the same on inspiration and expiration Auto-PAP (APAP) - Provides
BiPAPS/TVAPSCPAPASV???? Lori Davis, B.Sc., R.C.P.T.(P), RPSGT Modes Continuous Positive Airway Pressure (CPAP): One set pressure which is the same on inspiration and expiration Auto-PAP (APAP) - Provides
Neonatal Resuscitation. Dustin Coyle, M.D. Anesthesiology
 Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
Neonatal Resuscitation Dustin Coyle, M.D. Anesthesiology Recognize complications Maternal-fetal factors Maternal DM PIH Chronic HTN Previous stillbirth Rh sensitization Infection Substance abuse/certain
CHEST PHYSIOTHERAPY IN NICU PURPOSE POLICY STATEMENTS SITE APPLICABILITY PRACTICE LEVEL/COMPETENCIES. The role of chest physiotherapy in the NICU
 PURPOSE The role of chest physiotherapy in the NICU POLICY STATEMENTS In principle chest physiotherapy should be limited to those infants considered most likely to benefit with significant respiratory
PURPOSE The role of chest physiotherapy in the NICU POLICY STATEMENTS In principle chest physiotherapy should be limited to those infants considered most likely to benefit with significant respiratory
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Respiratory Management in Pediatrics
 Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Respiratory Management in Pediatrics Children s Hospital Omaha Critical Care Transport Sue Holmer RN, C-NPT Objectives Examine the differences between the pediatric and adults airways. Recognize respiratory
Pulmonary circulation. Lung Blood supply : lungs have a unique blood supply system :
 Dr. Ali Naji Pulmonary circulation Lung Blood supply : lungs have a unique blood supply system : 1. Pulmonary circulation 2. Bronchial circulation 1- Pulmonary circulation : receives the whole cardiac
Dr. Ali Naji Pulmonary circulation Lung Blood supply : lungs have a unique blood supply system : 1. Pulmonary circulation 2. Bronchial circulation 1- Pulmonary circulation : receives the whole cardiac
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Protocol for performing chest clearance techniques by nursing staff
 Protocol for performing chest clearance techniques by nursing staff Rationale The main indications for performing chest clearance techniques (CCT) are to assist in the removal of thick, tenacious secretions
Protocol for performing chest clearance techniques by nursing staff Rationale The main indications for performing chest clearance techniques (CCT) are to assist in the removal of thick, tenacious secretions
ritical Care Review Early Intervention in Respiratory Distress Syndrome Stephen Minton, MD, Dale Gerstmann, MD, Ronald Stoddard, MD
 ritical Care Review CURRENT APPLICATIONS AND ECONOMICS Early Intervention in Respiratory Distress Syndrome Stephen Minton, MD, Dale Gerstmann, MD, Ronald Stoddard, MD Introduction Since its availability
ritical Care Review CURRENT APPLICATIONS AND ECONOMICS Early Intervention in Respiratory Distress Syndrome Stephen Minton, MD, Dale Gerstmann, MD, Ronald Stoddard, MD Introduction Since its availability
5 Million neonatal deaths each year worldwide. 20% caused by neonatal asphyxia. Improvement of the outcome of 1 million newborns every year
 1 5 Million neonatal deaths each year worldwide 20% caused by neonatal asphyxia Improvement of the outcome of 1 million newborns every year International Liaison Committee on Resuscitation (ILCOR) American
1 5 Million neonatal deaths each year worldwide 20% caused by neonatal asphyxia Improvement of the outcome of 1 million newborns every year International Liaison Committee on Resuscitation (ILCOR) American
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4
 INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
TRAINING NEONATOLOGY SILVANA PARIS
 TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
TRAINING ON NEONATOLOGY SILVANA PARIS RESUSCITATION IN DELIVERY ROOM INTRODUCTION THE GLOBAL RESUSCITATION BURDEN IN NEWBORN 136 MILL NEWBORN BABIES EACH YEAR (WHO WORLD REPORT) 5-8 MILL NEWBORN INFANTS
BPD. Neonatal/Pediatric Cardiopulmonary Care. Disease. Bronchopulmonary Dysplasia. Baby Jane
 1 Neonatal/Pediatric Cardiopulmonary Care Disease 2 Bronchopulmonary Dysplasia 3 is a 33-day-old prematurely born girl who weighs 1420 g. At birth, her estimated gestational age was 28 weeks. Her initial
1 Neonatal/Pediatric Cardiopulmonary Care Disease 2 Bronchopulmonary Dysplasia 3 is a 33-day-old prematurely born girl who weighs 1420 g. At birth, her estimated gestational age was 28 weeks. Her initial
Respiratory Failure in the Pediatric Patient
 Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล
 Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล Goal of Mechanical Ventilation Mechanical ventilation is any means in which physical device or machines are
Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล Goal of Mechanical Ventilation Mechanical ventilation is any means in which physical device or machines are