How ARDS should be treated in 2017
|
|
|
- Thomas Allison
- 5 years ago
- Views:
Transcription


1 How ARDS should be treated in , Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany
2 ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading to the syndrome 3. Don t add damage lung body 4. Provide the best environment for lung healing (???)
3 Aim of the respiratory support To buy time with minimal damage Damaging factors Lung Ventilator Baby lung size Homogeneity Recruitability Mechanical power
4 Small, inhomogeneous, recruitable lung VILI comes from
5 Acute Respiratory Distress Syndrome Timing Chest Imaging a Origin of Edema Within 1 week of a known clinical insult or new/worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung collapse, or nodules Respiratory failure not fully explained by cardiac failure or fluid overload; Need objective assessment (e.g., echocardiography) to exclude hydrostatic edema if no risk factor present Mild Moderate Severe 200<PaO 2 /FiO 2 < 300 Oxygenation b with PEEP or CPAP 5 cmh 2 O c 100<PaO 2 /FiO 2 <200 with PEEP 5 cmh 2 O PaO 2 /FiO2<100 with PEEP 5 cmh 2 O a Chest X-ray or CT Scan b If altitude higher than 1000m,correction factor should be made as follows: PaO 2 /FiO 2 x (barometric pressure/760) c This may be delivered non-invasively in the Mild ARDS group JAMA. 2012;307(23):doi: /jama
6 MILD MILD ARDS MODERATE P/F 160 P/F PEEP SEVERE PEEP P/F PEEP 5 cmh 2 O Clinical PEEP PEEP Caironi, et al. CCM 2015
7 Caironi, et al. CCM 2015
8 Baby lung



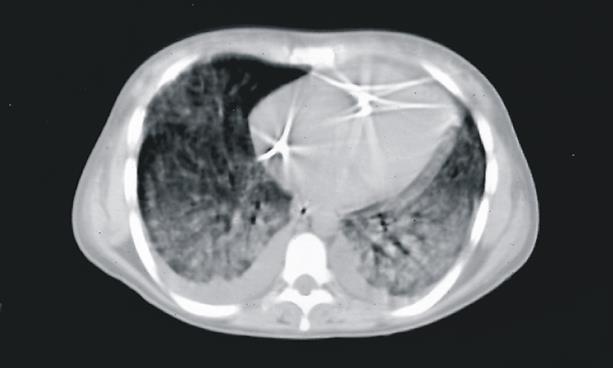
9 Gattinoni L et al. Intensive Care Med (1986) 12:
10 CT numbers frequency (%) Hyperinflated Baby Lung (1987) Normally aerated Poorly aerated Non aerated 50 Normal 40 ARDS CT numbers (Hounsfield Units)
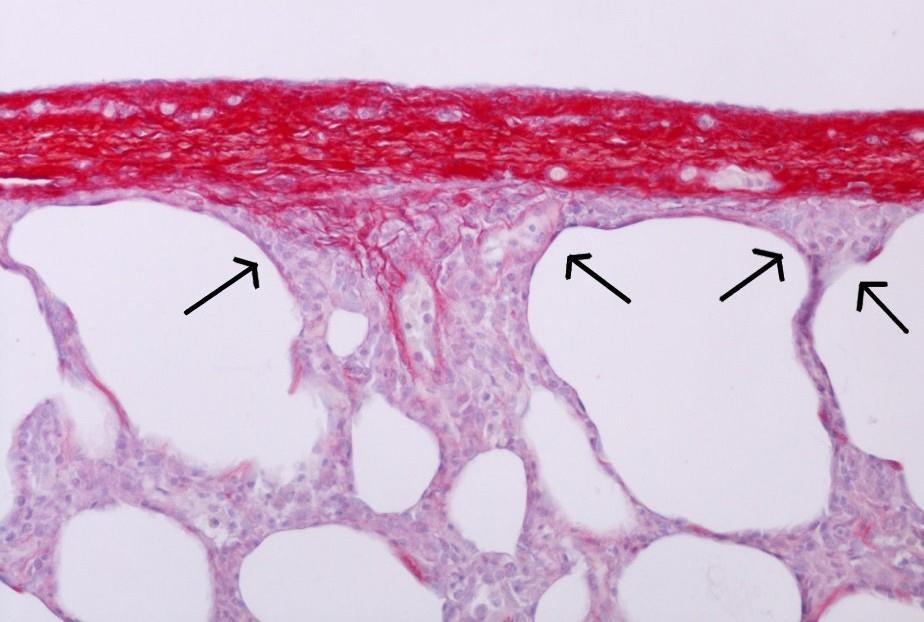
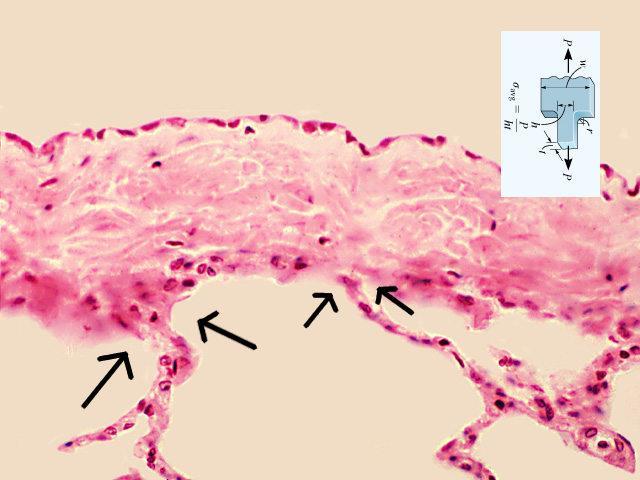
11 Inhomogeneity

12 Voxel Vgas Gas fraction = V gas0 /V voxel Weighted gas ratio = V gas1 /V gas0 * fraction of tissue





13 Average ratio in normal subjects : 1.37±0.15 Healthy subject Moderate ARDS Severe ARDS


14 Ki/lung inhomogeneity interaction and gas/tissue composition MILD MODERATE SEVERE
15 Recruitability
 5 cm H 2 O PaO 2")





16 Morphological response (1986) 5 cm H 2 O PaO 2 : 97 mm Hg 10 cm H 2 O PaO 2 : 103 mm Hg 15 cm H 2 O PaO 2 : 104 mm Hg d. 59% d. 56% 5 cm H 2 O 10 cm H 2 O PaO 2 : 34 mm Hg PaO 2 : 49 mm Hg d. 53% 15 cm H 2 O PaO 2 : 121 mm Hg d. 70% d. 52% d. 32% Intensive Care Med. 1986;12(3):
17 Opening pressures (2001) 6 dogs, Oleic acid % Potential for recruitment 100% inflation recruitment Airway pressure [cmh 2 O] Pelosi et al. Am J Respir Crit Care Med Jul 1;164(1):
18 Recruitment and inflation % 100 Inflation/Recruitment (2001) 5 patients, ALI / ARDS Potential for recruitment 5% Inflation % Recruitment % Paw [cmh 2 O] Crotti et al. Am J Respir Crit Care Med 2001;
19 Frequency [no. of patients] Figure 1 Potential for lung recruitment ± 4% (59 ± 51 grams) lower 21 ± 10% (374 ± 236 grams) higher ALI patients ARDS patients potential for lung recruitment [% total lung weight] Gattinoni L, Caironi P, Cressoni M, Chiumello D, Ranieri VM, Quintel M, Russo S, Cornejo R, Bugedo G, NEJM 2006, 354(17):
20 Recruited lung tissue (g) Opening Pressures Mild ARDS (N=5) Moderate ARDS (N=19) Severe ARDS (N=19) Plateu pressure limit Courtesy of dr. Cressoni M. Pressure (cmh 2 O)
21 Compartments (HU) -1000/ / / / / / / / /-100 0/-100 >0 A: TISSUE PEEP 5 PEEP 15 ** ** * Tissue (g) ** -1000/-900 ** -900/ / / / / / / /-100 0/-100 >0 ** B: GAS Gas (ml) ** ** Chiumello, et al. AJRCCM 2016

22 Aim of the respiratory support To buy time with minimal damage Damaging factors Lung Ventilator Baby lung size Homogeneity Recruitability Mechanical power
23 VILI comes from Excessive power
24 Time course of ventilator induced lung injury Lung Weight (g) Strain (Vt/FRC) Hours of mechanical ventilation 0.5 Protti A. et al. Am J Respir Crit Care Med Feb 4.
25 %Total Lung Capacity Resting Biotrauma Stress at rupture Strain Specific Lung Elastance 12 (cmh 2 O) Transpulmonary pressure (PL cmh 2 O) Agostoni, Mead, Weibel, Gattinoni
26 Stress-strain curve of healthy pigs Stress (PL, cmh2o) Specific Lung Elastance 5.8 cmh 2 O Strain (dvgas/vgas0) Protti A. et al. Am J Respir Crit Care Med Feb 4.
27 Lung Volume TLC FRC VT 100% V PEEP 0% VT 75% V PEEP 25% VT 50% V PEEP 50% VT 25% V PEEP 75% Protti et al. Crit Care Med Feb 4.
28 Mechanical ventilation and VILI 1.Volume 2.Pressure 3.Respiratory Rate 4.Flow 5.Or???
29 ZEEP 600 Total Inspiratory Volume Volume EXAPLES OF ENERGY COMPUTATIONS AT DIFFERENT PRESSURES 0 ZEEP Peak Pressure Pressure Total Inspiratory Volume LOW PEEP Total Inspiratory Volume HIGH PEEP PEEP Volume Volume 600 PEEP Volume Volume PEEP Peak Pressure 0 PEEP Peak Pressure Pressure Pressure
30 Motion equation Total pressure = (E rs V) + (R aw F) + PEEP Distend the lung Move the gas Keep open
31 Mechanical Power Total pressure V RR = Power rs = 0,098 RR V E rs + RR 1 + I: E 60 I: E R aw + V PEEP Distend the lung Move the gas Keep open TIME ENERGY
32 Percent increase power Contributions to Power generation 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% Baseline values RR 20 TV (L) 0,400 Ers 25 I:E 0,5 Raw 10 PEEP 10 Power rs 14,90 RR TV Peep Driving Press 0% 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% Percent increase variable
33 Summary TV Power 2 P aw Power 2 RR Power 1.6 PEEP Power 1
34 Interaction
35 Small, inhomogeneous, recruitable lung VILI comes from Excessive power

36 Chest wall elastance Stiff Soft Soft Stiff EL L Ew EL L Ew 25 5 cmh 2 O E tot E tot
37 Transpulmonary plateau pressue (cmh 2 O) Slope P L /P aw = E w /E tot [ ] A Surgical control group Medical control group B ALI patients ARDS patients Airway plateau pressure (cmh 2 O) Airway plateau pressure (cmh 2 O) Chiumello et al, Am J Respir Crit Care Med. 2008
38 Always consider: V T Baby lung size
39 The ARDS lung is small and not stiff Normal V T FRC = 500 ml 2500 ml = 0.2 ARDS V T FRC = 500 ml 500 ml = 1
40 Always consider: The lung inhomogeneity Stress raisers Atelectrauma
41 Lung expansion/gas-free state Mead J J Appl Physiol May;28(5): V 10 V V 1 V STRESS RAISER=(10/1) 2/3 = 4.64
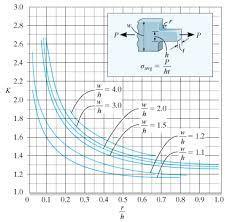

42
43 Lung dishomogeneity and ARDS Mild (N=82) Moderate (N=71) Severe (N=12) P Dishomogeneity 1.49 ± ± ± Dishomogeneity 2/ ± ± ± 0.55 Extent 0.3 ± ± ± Intensity 2.69 ± ± ± Intensity 2/ ± ± ± 0.55 Am J Respir Crit Care Med Jan 15;189(2):149-58
44 Gas / Tissue Ratio The gas/tissue ratio as a function of lung height Normal Supine Normal Prone ARDS Supine ARDS Prone Lung Height (%) Gattinoni L et al. In: Tobin MJ (ed) New York
45 Guerin C. et al. N Engl J Med Jun 6;368(23): Gattinoni L. et al. Minerva Anestesiol Jun;76(6):448-54
46 Atelectrauma
47 Recruitment (g) Opening and closing (1995) Plateau Pressure (cmh 2 O) ± ± ± 1.8 End Expiration End Inspiration 38 ± ± ** ** ** PEEP (cmh 2 O) Gattinoni et al. Am J Respir Crit Care Med 1995;151:
48 Recruited tissue Recruitment-Pressure curve Opening-closing Exp. Exp Pressure
49 Lung protective strategy Less energy + More homogeneous lung
Protective ventilation for ALL patients
 Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Protective ventilation for ALL patients PAOLO PELOSI, MD, FERS Department of Surgical Sciences and Integrated Diagnostics (DISC), San Martino Policlinico Hospital IRCCS for Oncology, University of Genoa,
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS
 Zee and Gommers Critical Care (2019) 23:73 https://doi.org/10.1186/s13054-019-2365-1 REVIEW Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS Philip van der
Zee and Gommers Critical Care (2019) 23:73 https://doi.org/10.1186/s13054-019-2365-1 REVIEW Recruitment Maneuvers and Higher PEEP, the So-Called Open Lung Concept, in Patients with ARDS Philip van der
11 th Annual Congress Turkish Thoracic Society. Mechanical Ventilation in Acute Hypoxemic Respiratory Failure
 11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
11 th Annual Congress Turkish Thoracic Society Mechanical Ventilation in Acute Hypoxemic Respiratory Failure Lluis Blanch MD PhD Senior Critical Care Center Scientific Director Corporació Parc Taulí Universitat
ARDS Assisted ventilation and prone position. ICU Fellowship Training Radboudumc
 ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
ARDS Assisted ventilation and prone position ICU Fellowship Training Radboudumc Fig. 1 Physiological mechanisms controlling respiratory drive and clinical consequences of inappropriate respiratory drive
How the Knowledge Proceeds in Intensive Care: the ARDS Example
 How the Knowledge Proceeds in Intensive Care: the ARDS Example 2016, Antalya Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany INDUCTION: From particular (application) to general (law/theory)
How the Knowledge Proceeds in Intensive Care: the ARDS Example 2016, Antalya Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany INDUCTION: From particular (application) to general (law/theory)
Biomarkers for ARDS not so simple. John Laffey. Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA
 Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services San Francisco General Hospital University of California, San Francisco, Case Study A 39 yo F admitted to SFGH TICU s/p hanging,
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación. Hospital Clinico Universitario Valencia (Spain)
") Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
Analyzing Lung protective ventilation F Javier Belda MD, PhD Sº de Anestesiología y Reanimación Hospital Clinico Universitario Valencia (Spain) ALI/ARDS Report of the American-European consensus conference
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Prone Position in ARDS
 Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Prone Position in ARDS Rich Kallet MS RRT FAARC, FCCM Respiratory Care Services Department of Anesthesia & Perioperative Care University of California, San Francisco, San Francisco General Hospital Case
Tracking lung recruitment and regional tidal volume at the bedside. Antonio Pesenti
 Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
Tracking lung recruitment and regional tidal volume at the bedside Antonio Pesenti Conflicts of Interest Maquet: Received research support and consultation fees Drager: Received research support and consultation
«Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic?
 1936-2005 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic? 1990-2000 Post cardiac arrest First day of mechanical ventilation 1990-1991 No patient
1936-2005 «Best» PEEP? Physiologic? Therapeutic? Optimal? Super? Preferred? Minimal? Right? Protective? Prophylactic? 1990-2000 Post cardiac arrest First day of mechanical ventilation 1990-1991 No patient
Respiratory insufficiency in bariatric patients
 Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
Respiratory insufficiency in bariatric patients Special considerations or just more of the same? Weaning and rehabilation conference 6th November 2015 Definition of obesity Underweight BMI< 18 Normal weight
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Computed tomography in adult respiratory distress syndrome: what has it taught us?
 Eur Respir J, 1996, 9, 155 162 DOI: 1.1183/931936.96.95155 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1996 European Respiratory Journal ISSN 93-1936 SERIES 'CLINICAL PHYSIOLOGY IN RESPIRATORY
Eur Respir J, 1996, 9, 155 162 DOI: 1.1183/931936.96.95155 Printed in UK - all rights reserved Copyright ERS Journals Ltd 1996 European Respiratory Journal ISSN 93-1936 SERIES 'CLINICAL PHYSIOLOGY IN RESPIRATORY
Noninvasive respiratory support:why is it working?
 Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
Noninvasive respiratory support:why is it working? Paolo Pelosi Department of Surgical Sciences and Integrated Diagnostics (DISC) IRCCS San Martino IST University of Genoa, Genoa, Italy ppelosi@hotmail.com
PEEP nuove indicazioni, stesse problematiche
 PEEP nuove indicazioni, stesse problematiche Franco Valenza Department of Pathophysiology and Transplantation Fondazione IRCCS Ca' Granda - Ospedale Maggiore Policlinico Ossigenazione Clearance CO 2 Kats,
PEEP nuove indicazioni, stesse problematiche Franco Valenza Department of Pathophysiology and Transplantation Fondazione IRCCS Ca' Granda - Ospedale Maggiore Policlinico Ossigenazione Clearance CO 2 Kats,
Measuring End Expiratory Lung Volume after cardiac surgery
 (Acta Anaesth. Belg., 2012, 63, 115-120) Measuring End Expiratory Lung Volume after cardiac surgery G. MICHIELS (*), V. MARCHAL (**), D. LEDOUX (*) and P. DAMAS (*) Abstract. Background : The aim of this
(Acta Anaesth. Belg., 2012, 63, 115-120) Measuring End Expiratory Lung Volume after cardiac surgery G. MICHIELS (*), V. MARCHAL (**), D. LEDOUX (*) and P. DAMAS (*) Abstract. Background : The aim of this
Proportional Assist Ventilation (PAV) (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure
 (NAVA) Younes ARRD 1992;145:114. Ventilator output :Triggering, Cycling Control of flow, rise time and pressure") Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Conflict of Interest Disclosure Robert M Kacmarek Unconventional Techniques Using Your ICU Ventilator!" 5-5-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston,
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Transpulmonary pressure measurement
 White Paper Transpulmonary pressure measurement Benefit of measuring transpulmonary pressure in mechanically ventilated patients Dr. Jean-Michel Arnal, Senior Intensivist, Hopital Sainte Musse, Toulon,
White Paper Transpulmonary pressure measurement Benefit of measuring transpulmonary pressure in mechanically ventilated patients Dr. Jean-Michel Arnal, Senior Intensivist, Hopital Sainte Musse, Toulon,
Ventilator ECMO Interactions
 Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilation in Paediatric ARDS: extrapolate from adult studies?
 Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
Ventilation in Paediatric ARDS: extrapolate from adult studies? ASMIC 2014 Dr Adrian Plunkett Consultant Paediatric Intensivist Birmingham Children s Hospital, UK Aims of the presentation Ventilation
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
3/5/14. Disclosures. Background. None. No discussion of non FDA approved products
 Disclosures None No discussion of non FDA approved products Background Who are the patients at risk for severe hypoxemic respiratory failure? ú Acute Lung Injury (ALI) PaO 2 /FIO 2 300 ú Acute Respiratory
Disclosures None No discussion of non FDA approved products Background Who are the patients at risk for severe hypoxemic respiratory failure? ú Acute Lung Injury (ALI) PaO 2 /FIO 2 300 ú Acute Respiratory
Lung CT Scan. Open Access. Paolo Pelosi *.1 and Marcelo Gama de Abreu 2. Gustav Carus, Dresden, Germany
 86 The Open Nuclear Medicine Journal, 2010, 2, 86-98 Lung CT Scan Paolo Pelosi *.1 and Marcelo Gama de Abreu 2 Open Access 1 Department of Ambient, Health and Safety, University of Insubria, Varese, Italy
86 The Open Nuclear Medicine Journal, 2010, 2, 86-98 Lung CT Scan Paolo Pelosi *.1 and Marcelo Gama de Abreu 2 Open Access 1 Department of Ambient, Health and Safety, University of Insubria, Varese, Italy
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Ventilator curves. Fellowonderwijs 2 feb 2012
 Ventilator curves Fellowonderwijs 2 feb 2012 Mechanical ventilation Supported Ventilator affects patients respiratory drive Monitor interaction patient - ventilator Controlled Monitor interatcion patient
Ventilator curves Fellowonderwijs 2 feb 2012 Mechanical ventilation Supported Ventilator affects patients respiratory drive Monitor interaction patient - ventilator Controlled Monitor interatcion patient
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Agenda. Mechanical Ventilation in Morbidly Obese Patients. Paolo Pelosi. ESPCOP, Ostend, Belgium Saturday, November 14, 2009.
 Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Mechanical Ventilation in Morbidly Obese Patients t Paolo Pelosi Department of Ambient, Health and Safety University of Insubria - Varese, ITALY ppelosi@hotmail.com ESPCOP, Ostend, Belgium Saturday, November
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation
 https://doi.org/10.1186/s12938-018-0599-9 BioMedical Engineering OnLine REVIEW Open Access Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation Vincent J. Major
https://doi.org/10.1186/s12938-018-0599-9 BioMedical Engineering OnLine REVIEW Open Access Biomedical engineer s guide to the clinical aspects of intensive care mechanical ventilation Vincent J. Major
Higher PEEP improves outcomes in ARDS patients with clinically objective positive oxygenation response to PEEP: a systematic review and meta-analysis
 Guo et al. BMC Anesthesiology (2018) 18:172 https://doi.org/10.1186/s12871-018-0631-4 RESEARCH ARTICLE Open Access Higher PEEP improves outcomes in ARDS patients with clinically objective positive oxygenation
Guo et al. BMC Anesthesiology (2018) 18:172 https://doi.org/10.1186/s12871-018-0631-4 RESEARCH ARTICLE Open Access Higher PEEP improves outcomes in ARDS patients with clinically objective positive oxygenation
Dr. Yasser Fathi M.B.B.S, M.Sc, M.D. Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah
 BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
BY Dr. Yasser Fathi M.B.B.S, M.Sc, M.D Anesthesia Consultant, Head of ICU King Saud Hospital, Unaizah Objectives For Discussion Respiratory Physiology Pulmonary Graphics BIPAP Graphics Trouble Shootings
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Outline. Basic principles of lung protective ventilation. The challenging areas. Small tidal volumes Recruitment
 ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS beyond 6/kg Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre Outline Basic principles
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
Instellen van beademingsparameters bij de obese pa3ent. MDO Nynke Postma
 Instellen van beademingsparameters bij de obese pa3ent MDO 19-1- 2015 Nynke Postma 1. Altered respiratory mechanics in obese pa@ents 2. Transpulmonary pressure 3. Titra@ng PEEP 4. Titra@ng @dal volume
Instellen van beademingsparameters bij de obese pa3ent MDO 19-1- 2015 Nynke Postma 1. Altered respiratory mechanics in obese pa@ents 2. Transpulmonary pressure 3. Titra@ng PEEP 4. Titra@ng @dal volume
Principles of Mechanical Ventilation
 47 Principles of Mechanical Ventilation Jonathan E. Sevransky, MD, MHS Objectives Understand the indications for treatment with mechanical ventilation Describe ventilator strategies that will minimize
47 Principles of Mechanical Ventilation Jonathan E. Sevransky, MD, MHS Objectives Understand the indications for treatment with mechanical ventilation Describe ventilator strategies that will minimize
High Flow Humidification Therapy, Updates.
 High Flow Humidification Therapy, Updates. Bernardo Selim, M.D. I have no relevant financial relationships to disclose. Assistant Professor, Pulmonary, Critical Care and Sleep Medicine, Mayo Clinic What
High Flow Humidification Therapy, Updates. Bernardo Selim, M.D. I have no relevant financial relationships to disclose. Assistant Professor, Pulmonary, Critical Care and Sleep Medicine, Mayo Clinic What
ARDS: MANAGEMENT UPDATE
 ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
Weaning and extubation in PICU An evidence-based approach
 Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
Weaning and extubation in PICU An evidence-based approach Suchada Sritippayawan, MD. Div. Pulmonology & Crit Care Dept. Pediatrics Faculty of Medicine Chulalongkorn University Kanokporn Udomittipong, MD.
ECMO: a breakthrough in care for respiratory failure. PD Dr. Thomas Müller Regensburg no conflict of interest
 ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
ECMO: a breakthrough in care for respiratory failure? PD Dr. Thomas Müller Regensburg no conflict of interest 1 Overview Mortality of severe ARDS Indication for ECMO PaO 2 /FiO 2 Efficiency of ECMO: gas
C h a p t e r 1 4 Ventilator Support
 C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
C h a p t e r 1 4 Ventilator Support Shirish Prayag Ex. Hon. Asst. Prof of Medicine, BJ Medical College and Sassoon Hospital, Pune; Chief Consultant in Internal Medicine and Critical Care, Shree Medical
Lab 4: Respiratory Physiology and Pathophysiology
 Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
The baby lung became an adult
 Intensive Care Med (2016) 42:663 673 DOI 10.1007/s00134-015-4200-8 REVIEW Luciano Gattinoni John J. Marini Antonio Pesenti Michael Quintel Jordi Mancebo Laurent Brochard The baby lung became an adult Received:
Intensive Care Med (2016) 42:663 673 DOI 10.1007/s00134-015-4200-8 REVIEW Luciano Gattinoni John J. Marini Antonio Pesenti Michael Quintel Jordi Mancebo Laurent Brochard The baby lung became an adult Received:
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal
 Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
Experience with Low Flow ECCO2R device on a CRRT platform : CO2 removal Alain Combes, MD, PhD, Hôpital Pitié-Salpêtrière, AP-HP Inserm UMRS 1166, ican, Institute of Cardiometabolism and Nutrition Pierre
UPMC Critical Care
 UPMC Critical Care www.ccm.pitt.edu Cardiovascular insufficiency with Initiation and Withdrawal of Mechanical Ventilation Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of
UPMC Critical Care www.ccm.pitt.edu Cardiovascular insufficiency with Initiation and Withdrawal of Mechanical Ventilation Michael R. Pinsky, MD, Dr hc Department of Critical Care Medicine University of
Regional overdistension during prone positioning in a patient with acute respiratory failure who was ventilated with a low tidal volume: a case report
 Kotani et al. Journal of Intensive Care (2018) 6:18 https://doi.org/10.1186/s40560-018-0290-z CASE REPORT Regional overdistension during prone positioning in a patient with acute respiratory failure who
Kotani et al. Journal of Intensive Care (2018) 6:18 https://doi.org/10.1186/s40560-018-0290-z CASE REPORT Regional overdistension during prone positioning in a patient with acute respiratory failure who
Ventilator Waveforms: Interpretation
 Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
Ventilator Waveforms: Interpretation Albert L. Rafanan, MD, FPCCP Pulmonary, Critical Care and Sleep Medicine Chong Hua Hospital, Cebu City Types of Waveforms Scalars are waveform representations of pressure,
Potential Conflicts of Interest
 Potential Conflicts of Interest Patient Ventilator Synchrony, PAV and NAVA! Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 4-27-09 WSRC Received research
Potential Conflicts of Interest Patient Ventilator Synchrony, PAV and NAVA! Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 4-27-09 WSRC Received research
Refresher Course MYTHS AND REALITY ABOUT LUNG MECHANICS 5 RC 2. European Society of Anaesthesiologists FIGURE 1 STATIC MEASUREMENTS
 European Society of Anaesthesiologists Refresher Course S AND ABOUT LUNG MECHANICS 5 RC 2 Anders LARSSON Gentofte University Hospital Copenhagen University Hellerup, Denmark Saturday May 31, 2003 Euroanaesthesia
European Society of Anaesthesiologists Refresher Course S AND ABOUT LUNG MECHANICS 5 RC 2 Anders LARSSON Gentofte University Hospital Copenhagen University Hellerup, Denmark Saturday May 31, 2003 Euroanaesthesia
Interpretation of the transpulmonary pressure in the critically ill patient
 Review Article Page 1 of 12 Interpretation of the transpulmonary pressure in the critically ill patient Michele Umbrello 1, Davide Chiumello 1,2 1 UOC Anestesia e Rianimazione, Ospedale San Paolo ASST
Review Article Page 1 of 12 Interpretation of the transpulmonary pressure in the critically ill patient Michele Umbrello 1, Davide Chiumello 1,2 1 UOC Anestesia e Rianimazione, Ospedale San Paolo ASST
Making sense of the pressure of arterial oxygen to fractional inspired oxygen concentration ratio in patients with acute respiratory distress syndrome
 Page 1 of 6 Optimizing Patient Care Making sense of the pressure of arterial oxygen to fractional inspired oxygen concentration ratio in patients with acute respiratory distress syndrome AF Broccard* Abstract
Page 1 of 6 Optimizing Patient Care Making sense of the pressure of arterial oxygen to fractional inspired oxygen concentration ratio in patients with acute respiratory distress syndrome AF Broccard* Abstract
Airway pressure release ventilation (APRV) in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital
 in PICU: Current evidence. Chor Yek Kee Sarawak General Hospital") Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
Airway pressure release ventilation (APRV) in PICU: Current evidence Chor Yek Kee Sarawak General Hospital Outline Brief introduction of APRV History of APRV Common confusion in APRV Features of APRV and
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
ARDS & TBI - Trading Off Ventilation Targets
 ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
ARDS & TBI - Trading Off Ventilation Targets Salvatore M. Maggiore, MD, PhD Rome, Italy smmaggiore@rm.unicatt.it Conflict of interest Principal Investigator: RINO trial o Nasal high-flow vs Venturi mask
Kontroversen in der Intensivmedizin. ARDS gibt es Neues?
 Kontroversen in der Intensivmedizin ARDS gibt es Neues? Disclosure: MQ is a member of International Advisory Boards from Covidien, Gambro, Maquet, Novalung and Pulsion Zürich 22.05.2014 Michael Quintel
Kontroversen in der Intensivmedizin ARDS gibt es Neues? Disclosure: MQ is a member of International Advisory Boards from Covidien, Gambro, Maquet, Novalung and Pulsion Zürich 22.05.2014 Michael Quintel
Lung inhomogeneities, inflation and [ 18 F]2-fluoro-2-deoxy-D-glucose uptake rate in acute respiratory distress syndrome
![Lung inhomogeneities, inflation and [ 18 F]2-fluoro-2-deoxy-D-glucose uptake rate in acute respiratory distress syndrome](/thumbs/88/116222124.jpg "Lung inhomogeneities, inflation and [ 18 F]2-fluoro-2-deoxy-D-glucose uptake rate in acute respiratory distress syndrome") ORIGINAL ARTICLE ACUTE LUNG INJURY AND CRITICAL CARE Lung inhomogeneities, inflation and [ 18 F]2-fluoro-2-deoxy-D-glucose uptake rate in acute respiratory distress syndrome Massimo Cressoni 1, Davide
ORIGINAL ARTICLE ACUTE LUNG INJURY AND CRITICAL CARE Lung inhomogeneities, inflation and [ 18 F]2-fluoro-2-deoxy-D-glucose uptake rate in acute respiratory distress syndrome Massimo Cressoni 1, Davide
1/26/16. Prone Position How does asynchrony impact LPV and how should it be managed? Is there a role for NIV and HFNC in ARDS?
 What is ARDS?: how our understanding changed over time What are the risk factors and major etiologies? How does MV exacerbate or attenuate lung injury? Ventilator managment of ARDS Rich Kallet MS RRT FAARC
What is ARDS?: how our understanding changed over time What are the risk factors and major etiologies? How does MV exacerbate or attenuate lung injury? Ventilator managment of ARDS Rich Kallet MS RRT FAARC
Monitor the patients disease pathology and response to therapy Estimate respiratory mechanics
 Understanding Graphics during Mechanical Ventilation Why Understand Ventilator Graphics? Waveforms are the graphic representation of the data collected by the ventilator and reflect the interaction between
Understanding Graphics during Mechanical Ventilation Why Understand Ventilator Graphics? Waveforms are the graphic representation of the data collected by the ventilator and reflect the interaction between
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
VILI Mechanisms: Are Lung Regions Different? 26 October, 2015 Critical Care Canada Forum Toronto, ON
 VILI Mechanisms: Are Lung Regions Different? 26 October, 2015 Critical Care Canada Forum Toronto, ON Ivor S. Douglas, MD Denver Health Medical Center & U Colorado, Denver idouglas@dhha.org ISD Disclosures
VILI Mechanisms: Are Lung Regions Different? 26 October, 2015 Critical Care Canada Forum Toronto, ON Ivor S. Douglas, MD Denver Health Medical Center & U Colorado, Denver idouglas@dhha.org ISD Disclosures
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018
 ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
ARF, Mechaical Ventilation and PFTs: ACOI Board Review 2018 Thomas F. Morley, DO, FACOI, FCCP, FAASM Professor of Medicine Chairman Department of Internal Medicine Director of the Division of Pulmonary,
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Effects of patient positioning on respiratory mechanics in mechanically ventilated ICU patients
 Review Article Page 1 of 9 Effects of patient positioning on respiratory mechanics in mechanically ventilated ICU patients Mehdi Mezidi 1,2, Claude Guérin 1,2,3 1 Service de réanimation médicale, Hôpital
Review Article Page 1 of 9 Effects of patient positioning on respiratory mechanics in mechanically ventilated ICU patients Mehdi Mezidi 1,2, Claude Guérin 1,2,3 1 Service de réanimation médicale, Hôpital
journal of medicine The new england Lung Recruitment in Patients with the Acute Respiratory Distress Syndrome Abstract
 The new england journal of medicine established in 1812 april 27, 2006 vol. 354 no. 17 Lung Recruitment in Patients with the Acute Respiratory Distress Syndrome Luciano Gattinoni, M.D., F.R.C.P., Pietro
The new england journal of medicine established in 1812 april 27, 2006 vol. 354 no. 17 Lung Recruitment in Patients with the Acute Respiratory Distress Syndrome Luciano Gattinoni, M.D., F.R.C.P., Pietro
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Respiratory failure requiring mechanical ventilation
 Current Issues in Mechanical Ventilation for Respiratory Failure* Neil R. MacIntyre, MD The morbidity and mortality associated with respiratory failure is, to a certain extent, iatrogenic. Mechanical ventilation,
Current Issues in Mechanical Ventilation for Respiratory Failure* Neil R. MacIntyre, MD The morbidity and mortality associated with respiratory failure is, to a certain extent, iatrogenic. Mechanical ventilation,
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS?
 Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
Pulmonary & Extra-pulmonary ARDS: FIZZ or FUSS? Dr. Rajagopala Srinivas Senior Resident, Dept. Pulmonary Medicine, PGIMER, Chandigarh. The beginning.. "The etiology of this respiratory distress syndrome
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Should we titrate positive end-expiratory pressure based on an end-expiratory transpulmonary pressure?
 Perspective Page 1 of 8 Should we titrate positive end-expiratory pressure based on an end-expiratory transpulmonary pressure? John J. Marini Department of Pulmonary and Critical Care Medicine, University
Perspective Page 1 of 8 Should we titrate positive end-expiratory pressure based on an end-expiratory transpulmonary pressure? John J. Marini Department of Pulmonary and Critical Care Medicine, University
The Berlin Definition: Does it fix anything?
 The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
ARDS and treatment strategies
 ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
Patient Ventilator Interactions. Patient-Ventilator Interactions. Assisted vs Controlled MV. Ventilatory Muscle Fatigue Recovery
 Patient Ventilator Interactions Patient-Ventilator Interactions Neil MacIntyre MD Duke Uni versity Medi cal Center Durham NC, USA Newer a pproaches to improving intera ctions Assisted vs Controlled MV
Patient Ventilator Interactions Patient-Ventilator Interactions Neil MacIntyre MD Duke Uni versity Medi cal Center Durham NC, USA Newer a pproaches to improving intera ctions Assisted vs Controlled MV
This bibliography is a literature reference for users and represents selected relevant publications, without any claim to completeness.
 Bibliography Lung recruitment This bibliography is a literature reference for users and represents selected relevant publications, without any claim to completeness. Table of Contents 1 Effect of intensive
Bibliography Lung recruitment This bibliography is a literature reference for users and represents selected relevant publications, without any claim to completeness. Table of Contents 1 Effect of intensive
Lung volumes and lung volume recruitment in ARDS: a comparison between supine and prone position
 https://doi.org/10.1186/s13613-018-0371-0 RESEARCH Open Access Lung volumes and lung volume recruitment in ARDS: a comparison between supine and prone position Hernan Aguirre Bermeo, Marta Turella, Maddalena
https://doi.org/10.1186/s13613-018-0371-0 RESEARCH Open Access Lung volumes and lung volume recruitment in ARDS: a comparison between supine and prone position Hernan Aguirre Bermeo, Marta Turella, Maddalena
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Weaning from Mechanical Ventilation. Dr Azmin Huda Abdul Rahim
 Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Weaning from Mechanical Ventilation Dr Azmin Huda Abdul Rahim Content Definition Classification Weaning criteria Weaning methods Criteria for extubation Introduction Weaning comprises 40% of the duration
Restrictive Pulmonary Diseases
 Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Restrictive Pulmonary Diseases Causes: Acute alveolo-capillary sysfunction Interstitial disease Pleural disorders Chest wall disorders Neuromuscular disease Resistance Pathophysiology Reduced compliance
Physiological Relevance of a Minimal Model in Healthy Pigs Lung
 Physiological Relevance of a Minimal Model in Healthy Pigs Lung Yeong Shiong Chiew*, Thomas Desaive** Bernard Lambermont**, Nathalie Janssen**, Geoffrey M Shaw***, Christoph Schranz****, Knut Möller****,
Physiological Relevance of a Minimal Model in Healthy Pigs Lung Yeong Shiong Chiew*, Thomas Desaive** Bernard Lambermont**, Nathalie Janssen**, Geoffrey M Shaw***, Christoph Schranz****, Knut Möller****,
Recognizing and Correcting Patient-Ventilator Dysynchrony
 2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
2019 KRCS Annual State Education Seminar Recognizing and Correcting Patient-Ventilator Dysynchrony Eric Kriner BS,RRT Pulmonary Critical Care Clinical Specialist MedStar Washington Hospital Center Washington,
Hemodynamic effects of lung recruitment maneuvers in acute respiratory distress syndrome
 Das et al. BMC Pulmonary Medicine (2017) 17:34 DOI 10.1186/s12890-017-0369-7 RESEARCH ARTICLE Open Access Hemodynamic effects of lung recruitment maneuvers in acute respiratory distress syndrome Anup Das
Das et al. BMC Pulmonary Medicine (2017) 17:34 DOI 10.1186/s12890-017-0369-7 RESEARCH ARTICLE Open Access Hemodynamic effects of lung recruitment maneuvers in acute respiratory distress syndrome Anup Das
Institute of Anesthesia and Critical Care, University of Milan, Policlinico IRCCS Hospital, Milan, Italy
 Critical Care October 2004 Vol 8 No 5 Gattinoni et al. Review Bench-to-bedside review: Chest wall elastance in acute lung injury/acute respiratory distress syndrome patients Luciano Gattinoni, Davide Chiumello,
Critical Care October 2004 Vol 8 No 5 Gattinoni et al. Review Bench-to-bedside review: Chest wall elastance in acute lung injury/acute respiratory distress syndrome patients Luciano Gattinoni, Davide Chiumello,
Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care
 28 th ISICEM Brussels, 19 March 2008 Monitoring in respiratory failure Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care Hospital Clinico Universitario
28 th ISICEM Brussels, 19 March 2008 Monitoring in respiratory failure Extravascular lung water reflects pulmonary edema F Javier Belda MD, PhD Dept. Anesthesiology and Critical Care Hospital Clinico Universitario
Dr. AM MAALIM KPA 2018
 Dr. AM MAALIM KPA 2018 Journey Towards Lung protection Goals of lung protection Strategies Summary Conclusion Before 1960: Oxygen; impact assessed clinically. The 1960s:President JFK, Ventilators mortality;
Dr. AM MAALIM KPA 2018 Journey Towards Lung protection Goals of lung protection Strategies Summary Conclusion Before 1960: Oxygen; impact assessed clinically. The 1960s:President JFK, Ventilators mortality;