Cancer-Related Fatigue (CRF) Management During and Following Cancer Treatment: Moving the Evidence into Practice
|
|
|
- Priscilla Roberts
- 5 years ago
- Views:
Transcription
1 Cancer-Related Fatigue (CRF) Management During and Following Cancer Treatment: Moving the Evidence into Practice Sandra A. Mitchell, PhD, CRNP, AOCN, FAAN Research Scientist and Program Director; Outcomes Research Branch; Division of Cancer Control and Population Sciences and Oncology Nurse Practitioner; Experimental Transplantation and Immunology Branch National Cancer Institute Rockville, MD March 11, 2016
2 Disclosures Nothing to disclose
3 Objectives At the end of this session, the participant will be able to: Describe the strength of the evidence for three interventions to manage fatigue during and following stem cell transplantation Identify two instruments that can be used for screening or outcomes assessment in patients or survivors with cancer-related fatigue Name two evidence-based guidelines that can be used to improve clinical outcomes for patients at risk for or experiencing fatigue
4 Scope of the Problem Prevalence of fatigue during and following transplant: 35% of respondents had moderate/severe fatigue immediately pretransplant and Day % have moderate to severe fatigue at nadir 30-50% bothered a lot or extremely by fatigue at 6, 12 and 24 months post transplant 5 years post-transplant fatigue was significantly higher than age- and gender-matched healthy comparison samples Fatigue has consequences for physical, vocational, cognitive and social functioning; mood; treatment adherence, psychological and spiritual distress, and possibly for long-term survival outcomes
5 Scope of the Problem Single item assessments of fatigue are common in the literature; comparatively fewer prospective studies using multi-dimensional fatigue measures Variety of self-report measures used makes comparisons between studies difficult Strong correlations between measures of fatigue and depression Small convenience samples; high rates of missing data Identifying the biologic factors contributing to fatigue across the transplant trajectory is challenging 5



6 Fatigue Definition Cancer related fatigue (CRF) is a multifaceted condition characterized by an usual, persistent and subjective sense of tiredness that is not proportional to recent activity and interferes with usual functioning May be accompanied by generalized weakness, diminished mental concentration, insomnia or hypersomnia, and emotional reactivity 6
7 ICD-10 Criteria for Cancer-Related Fatigue 1 A. Six (or more) of the following symptoms have been present every day or nearly every day during the same two-week period in the past month, and at least one of the symptoms is significant fatigue (A1) A1. Significant fatigue, diminished energy, or increased need to rest, disproportionate to any recent change in activity level A2. Complaints of generalized weakness or limb heaviness A3. Diminished concentration or attention A4. Decreased motivation or interest to engage in usual activities A5. Insomnia or hypersomnia A6. Experience of sleep as unrefreshing or nonrestorative A7. Perceived need to struggle to overcome inactivity A8. Marked emotional reactivity (e.g. sadness, frustration, irritability) to feeling fatigued A9. Difficulty completing daily tasks attributed to feeling fatigued A10. Perceived problems with short-term memory A11. Postexertional malaise lasting several hours 1. Cella, D., Davis, K., Bretibart, W., Curt, G. (2001). Cancer-related fatigue: Prevalence of proposed diagnostic criteria in a United States sample of cancer survivors. Journal of Clinical Oncology; 19 (14),
8 ICD-10 Criteria for Cancer-Related Fatigue B. The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning C. There is evidence from the history, physical examination, or laboratory findings that the symptoms are a consequence of cancer or cancer therapy D. The symptoms are not primarily a consequence of comorbid psychiatric disorders such as major depression, somatization disorder, somatoform disorder, or delirium 8
9 Features Clinical expression of CRF is multidimensional Fatigue may be experienced and reported differently by each individual May occur as an isolated symptom or as one component within a cluster (pain, fatigue, depression, sleep disturbances) Qualitative studies of fatigue show: CRF experience is unlike other fatigue Unpredictability and refractoriness to self-management contributes to distress Personality and coping style may also influence the experience of CRF 9
10 Variability in Manifestations of CRF Central features: loss of efficiency, mental fogginess, inertia, and sleep that is not restorative Peripheral features: excessive need to rest, an inability to recover promptly from exertion, muscle heaviness and weakness Variable features of fatigue? Fatigue subtypes? Cause or sequelae of fatigue? Challenging to distinguish CRF from depression, cognitive dysfunction, or asthenia Overlapping symptoms? Shared neurophysiologic mechanisms? 10
11 What do we need to be doing better? Studies suggest: fatigue screening and evaluation is suboptimal fatigue is undertreated health care professionals may not fully appreciate the degree of distress and functional loss that fatigue produces Fatigue communication barriers: Inadequate knowledge of effective treatments, including nonpharmacologic treatments which some patients may prefer Tendency to be stoic about fatigue in order to avoid being labeled as a complainer 11
12 Etiology and Risk Factors Inconsistent relationships to treatment-related variables (chemotherapy, radiation therapy, anemia, neutropenia, and time since treatment completion) Inconsistent relationships with age, gender, marital status and employment status 12
13 Etiology and Risk Factors Advanced/metastatic disease or cancer recurrence Cancer treatment (chemotherapy, radiation, surgery, biologic agents, hormonal agents, molecularly targeted agents) Anemia Neutropenia Hypothyroidism Adrenal Insufficiency Hypogonadism Infection Malnutrition Depletion of vitamins B1, B 6 and B12 Electrolyte disturbances (calcium, magnesium, phosphorus) Cardiopulmonary, hepatic or renal dysfunction Sarcopenia, asthenia, deconditioning 13
14 Etiology and Risk Factors Proinflammatory cytokine expression/generalized inflammation Medications with sedating side effects (e.g. narcotics, anxiolytics, antiemetics, antidepressants), or medications with fatigue as part of the side effects profile (e.g. beta-blockers) of medications Concurrent symptoms (e.g. pain, dyspnea, nausea, diarrhea) Impaired sleep quality Psychological distress (depression, anxiety) Accumulating evidence also suggests a role for gene polymorphisms, altered circadian rhythmicity, immune dysregulation, abnormal cortisol secretion, elevated body mass index, and metabolic syndrome In any one individual, the etiology of CRF likely involves the interaction of several physiologic and psychobehavioral mechanisms 14
15 Psychophysiologic Models of CRF Energy Balance/Energy Analysis Models energy intake metabolism and expenditure are major explanatory variables Fatigue as a Stress Response Models tiredness, fatigue, and exhaustion represent a continuum of stress response Neuro-Endocrine Based Regulatory Fatigue Models fatigue explained by neuro-immuno-endocrine dysregulation 15
, Personalized Approach to Cancer Survivorship.")
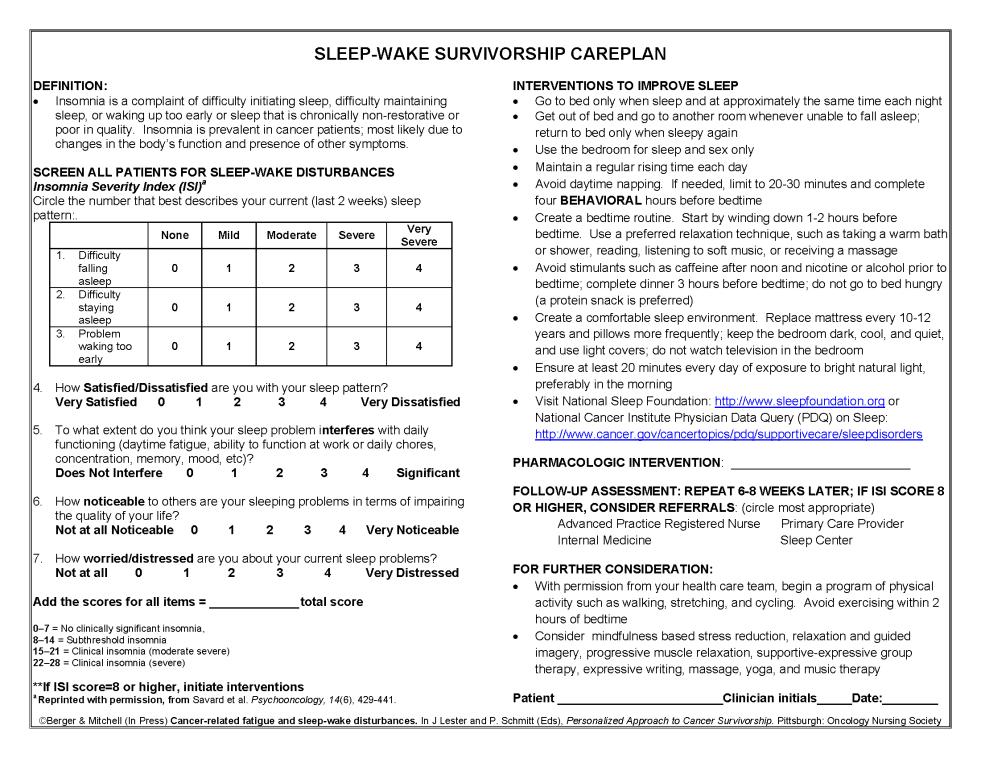
16 Organizing Framework for Understanding Cancer-Related Fatigue Berger & Mitchell (2011) Cancer-related fatigue and sleep-wake disturbances. In J Lester and P. Schmitt (Eds), Personalized Approach to Cancer Survivorship. Pittsburgh: Oncology Nursing Society Press. 16
17 Approaches to Measuring Cancer-Related Fatigue Single items that gauge fatigue severity Single items or subscales that measure relevant aspects of the fatigue experience that have been drawn from measures of quality of life (e.g. FACIT-Fatigue), psychosocial adjustment, mood, or self-reported health status (e.g. vigor, vitality) Instruments designed specifically to evaluate CRF from a multidimensional perspective (e.g. Multidimensional Fatigue Inventory; Piper Fatigue Scale; PROMIS Fatigue Measures) Neurophysiologic and performance-based measurements of fatigue, including muscle force, endurance time, muscle reserve, neuromuscularjunction impulse propagation, and functional performance 17
18 Measurement Considerations Fatigue is a multidimensional construct: sensory dimension (fatigue severity, persistence) physiologic dimension (e.g. leg weakness, diminished mental concentration) affective dimension (sadness, depression, fear) behavioral dimension (reduction in the performance of needed or valued activities) Multidimensional measures provide information about this full range of characteristics beyond fatigue presence and intensity Weakness, tiredness or the absence of vigor or vitality, may not necessarily be equated with fatigue 18
19 Measurement Considerations for Research Purposes Reliability, validity, specificity, sensitivity to change, and recall period Respondent burden, translation in multiple languages, the complexity of scoring algorithms, and the availability of normative values and other interpretive guidance (e.g. minimal clinically important difference) Should possess the capacity to discriminate cases from non-cases with an acceptable level of sensitivity and specificity 19
20 Measurement Considerations for Research Purposes Contemporary advances: item-banks, computerized-adapted testing, and other digital formats will improve efficiency, precision, and ease of interpretation of screening measures for CRF (e.g. PROMIS) Ecological momentary assessment elicits a repeated, real-time measurement of behaviors or experiences as they occur in the naturalistic setting of an individual s day to day life may overcome methodologic limitations including recall bias and the influence of current context on self-report of fatigue 20
21 Fatigue Screening and Evaluation in the HSCT Recipient Screening Brief measures to screen for fatigue are sensitive, and they can be applied efficiently in the clinic to identify individuals who would benefit from more systematic evaluation Every patient be screened for the presence of fatigue at regular intervals. If present, fatigue should be assessed quantitatively on a 0-10 scale (0= no fatigue and 10= worst fatigue imaginable) Those with a severity of more than 4 should be further evaluated by history and physical examination.
22 Evaluation of the HSCT Recipient with Fatigue>4 presence, intensity, and pervasiveness of fatigue course over time factors that exacerbate or relieve fatigue impact of fatigue on functioning and level of distress impact on self-esteem, mood, and the ability to perform activities of daily living, fulfill important roles as parent, spouse and worker, and relate to family and friends self-management interventions the patient has tried for fatigue and their effectiveness can be helpful in tailoring recommendations for fatigue management
23 Etiologic Factors That May Amplify Fatigue Hypothyroidism Hypogonadism Adrenal insufficiency Cardiomyopathy Pulmonary dysfunction Infection Anemia, neutropenia Sleep disturbances Malnutrition Sarcopenia, asthenia Inactivity and deconditioning Fluid and electrolyte imbalances Emotional distress (anxiety, depression) Uncontrolled concurrent symptoms Disease progression or recurrence 23
24 Medication Side Effects Profile May Intensify Fatigue Medications that may produce daytime sleepiness and fatigue opioid analgesics, sedative-hypnotics, benzodiazepines, anxiolytics antidepressants, antiemetics, antihistamines, and anticonvulsant agents cardiac medications such as beta-blockers may contribute to fatigue by causing bradycardia corticosteroids may cause fatigue by disrupting sleep or generating proximal muscle weakness 24
25 General Principles of CRF Management Typically several different causes in any one patient, treatment plan must be multidimensional and individually tailored Work with the patient and family to improve the assessment of fatigue and identify management strategies Open communication among patient, family, and health care team will facilitate discussion about the experience of fatigue and its effects on daily life General supportive care recommendations: Optimize nutritional status and prevent weight loss Balance rest with physical activity Encourage attention restoring activities such as exposure to natural environments and pleasant distractions like music 25
26 Interventions for Cancer Related Fatigue General Principles More than 300 empiric studies of pharmacologic and non-pharmacologic interventions to reduce or manage CRF, and more than 75 meta-analyses or systematic reviews For some interventions, there is strong and consistent evidence to support effectiveness, while for other interventions only preliminary data are available Many of the interventions for fatigue have not been studied in HSCT recipients or long-term survivors of HSCT 26
27 Exercise Recommended for Practice Exercise is effective in managing fatigue during and following cancer treatment in patients with breast, prostate or colorectal cancer, patients undergoing chemotherapy, radiation or HSCT; survivors with solid tumor or hematologic malignancy, and following HSCT Possible mechanisms: Improves aerobic capacity, and ameliorates muscle loss and deconditioning Favorable effects on sleep, mood, self-efficacy, body composition, and the immune system and cytokine Exercise modalities differ in: content (walking, cycling, swimming, resistive exercise, or combined exercise) frequency (ranging from two times per week to two times daily) intensity degree of supervision (fully supervised group versus self-directed exercise) duration (from two weeks up to one year) 27
28 Exercise Referral to a rehabilitation professional such as a physiatrist or physical therapist can be helpful in providing specific and detailed recommendations about the type, intensity, and frequency of exercise in which the patient should engage Ongoing follow-up by rehabilitation professionals contributes to strengthening motivation and adherence, and to advancing the exercise program as functional capacity improves Research is needed to: Recommended for Practice systematically assess the safety of exercise (both aerobic exercise and strength training) tailor the intensity, frequency, duration and type of exercise prescribed for different sub-populations of patients (e.g. tumor types, phase of treatment and follow-up) 28
29 Likely to Be Effective Screen for potential etiologic factors and manage as appropriate Experts recommend that patients with fatigue be screened for the following treatable etiologic factors and managed as indicated: Concurrent distressing symptoms including pain, nausea and depression Hypothyroidism Hypogonadism Cardiomyopthathy Adrenal insufficiency Pulmonary dysfunction Anemia Sleep disturbance Fluid and electrolyte imbalances Emotional distress Sedation secondary to specific classes of medications (e.g. opiates, antidepressants, antiemetics, antihistamines) or due to drug-drug interactions, and manage as indicated 29
30 Energy Conservation and Activity Management Likely to Be Effective A nurse-delivered intervention focused on energy conservation and activity management (a multi-component intervention designed to help patients develop skills in planning, delegating, setting priorities, pacing, resting, and planning high-energy use activities at times of peak energy) had a modest but significant effect in a large, multi-site randomized clinical trial with patients (mostly breast cancer) initiating chemotherapy or radiation Education/Information Provision Four meta-analyses and 12 RCTs indicate that educational interventions (including teaching, counseling, support, anticipatory guidance about fatigue patterns, coping skills training, and coaching in fatigue self- management have a role in supporting positive coping in patients with fatigue, and contribute to reductions in fatigue levels Interventions incorporate anticipatory guidance about fatigue patterns, the importance of exercise and sleep, and coaching and emotional support to promote goal setting and enhance self-efficacy 30
31 Likely to Be Effective Measures to Optimize Sleep Quality Studies indicate a multi-component cognitive-behavioral intervention designed to optimize sleep quality may also improve fatigue Cognitive behavioral intervention generally includes: relaxation training sleep consolidation strategies (avoiding long or late afternoon naps, limiting time in bed to actual sleep time) stimulus control therapy go to bed only when sleepy, use bed/bedroom for sleep and sexual activities only consistent time to lie down and get up, avoid caffeine and stimulating activity in the evening) reducing cognitive-emotional arousal keep at least an hour to relax before going to bed establish a pre-sleep routine to be used every night 31
32 Relaxation Likely to Be Effective In six RCTs, progressive muscle relaxation training or relaxation breathing and yoga-like positioning delivered in a series of sessions to patients with cancer were found to be effective in lowering fatigue scores Yoga Practices Significantly improved fatigue outcomes in breast cancer Effects of yoga on fatigue outcomes has not been established across a wide range of cancer patient populations High risk of bias across studies with respect to sampling, inconsistent methods, blinding of participants and outcomes assessors and duration of follow-up 32
33 Structured Multidimensional Rehabilitation Likely to Be Effective Eight RCTs in patients with a range of solid tumors, including advanced disease Structured combination of physical training, psychoeducation, and nutritional counselling, mudpacks, massage and manual lymph drainage Some therapies delivered during an inpatient hospital stay Improves fatigue as well as mood, physical function and nutritional status Mindfulness-Based Stress Reduction and Cognitive-Behavioral Stress Mgmt Significantly improved fatigue outcomes in 5 RCTs in breast cancer, and one RCT in patients with mixed tumor sites Three other RCTs however showed no effects on fatigue outcomes 33
34 Likely to Be Effective Cognitive-Behavioral Therapy (CBT) for Fatigue, Depression and Pain Six RCTs in patients with a range of solid tumors and severely fatigue survivors and patients with advanced cancers Consistently favorable effects on fatigue outcomes Management of Concurrent Symptoms Including Pain, SOB, Insomnia and Depression APN intervention to systematically evaluate and manage symptoms Palliative care clinic consultation to address concurrent symptoms 34
35 Correction of Anemia Benefits Balanced With Harms Seven recent meta-analyses or systematic reviews suggest that patients receiving erythropoiesis stimulating agents to correct anemia less than 10 g/dl may experience increased vigor and diminished fatigue There is only limited evidence that ESAs improve fatigue when anemia is less severe Data suggest that a target hemoglobin level of 11 to 12 g/dl will produce the greatest gains in fatigue and other quality of life outcomes Use of these agents specifically for fatigue is relatively contraindicated due to safety issues: Increased risk of thrombotic events, hypertension Epoietin may support or extend tumor growth in certain tumor types National practice guidelines (NCCN, 2010) and FDA guidance should direct patient management including Decisions about monitoring Treatment thresholds Dose reductions and treatment discontinuation Use of supplemental iron; transfusion support instead of ESAs FDA mandated a risk evaluation and mitigation strategy (REMS) requiring all prescribers of ESAs to register and receive training 35
36 Low-dose Dexamethasone Benefits Balanced With Harms Dexamethasone 4 mg BID x 2 weeks improved CRF in advanced cancer in a small randomized, placebo-controlled trial Adverse events were comparable in dexamethasone and placebo groups Caveat: systemic corticosteroids may have prominent adverse effects in specific subpopulations (e.g. at end of life) 36
37 Acupuncture, acupressure and self-acupuncture 6 meta-analyses of randomized trials published in the last 2 years Many studies demonstrate a positive effect on fatigue outcomes Interventions are feasible, well-accepted and safe Interpretation of study outcomes is complicated by high risk of bias including short duration of follow-up, single acupuncturists and non-blinding of outcome assessors All reviews urge additional study using rigorous trial designs Morning exposure to bright light Small RCT showed positive effects in terms of preventing fatigue during chemotherapy for breast cancer and in cancer survivors with mixed diagnoses Evidence suggests that exposure to bright light may protect recipients from circadian rhythm desynchronization during cancer treatment Qigong or Tai Chi Effectiveness Not Established Three RCTs showed favorable effects of Qigong on fatigue outcomes Tai chi improved fatigue In a small single arm trial Recent meta-analysis concluded that study results should be interpreted cautiously 37
38 Nutritional Supplements and Herbal Remedies Effectiveness Not Established Agents studied include vitamin supplements, levocarnitine, lectin-standardized misteltoe, omega-3 fatty acid, guarana, valerian, and Chinese herbal medicines Many studied as part of a multi-component regimen Improvements in fatigue endpoints was inconsistent High risk of bias given the open label, non-randomized study designs, small samples, and testing of multiple secondary endpoints Massage and biofield therapies such as Reiki, healing touch Multiple small RCTs or quasi-experimental studies Modalities examined as single interventions or as part of a multicomponent intervention Preliminary evidence suggests these may be effective, although efficacy results are mixed, and studies have a high risk of bias Continued testing and refinement is needed Complementary Approaches Expressive writing, art, music, dance, or animal-assisted therapy, exposure to nature and green space, distraction-virtual reality immersion, and aromatherapy with lavender foot soak and reflexology Open label and/or uncontrolled study designs and small sample sizes make it difficult to 38 draw conclusions
39 Paroxetine Effectiveness Not Established Evidence of effectiveness in treating fatigue during and following cancer treatment is mixed In two large randomized trials, paroxetine 20 mg po daily did not have an effect on fatigue, although improvements in depression and overall mood were noted in the paroxetine treatment group Two small trials show a possible benefit for paroxetine in treating fatigue in women with hot flashes and in patients receiving interferon alpha Methylphenidate Several small open label, single arm trials and 3 RCTs have reported improvements in fatigue in most of their participants as a result of the methylphenidate (5-10 mg BID) intervention Donepezil Donepezil (5 mg every morning) evaluated in a blinded RCT and two single arm open label trials RCT showed no benefit on fatigue outcomes; fatigue was improved in the open label trials 39
40 Bupropion Sustained Release Effectiveness Not Established Bupropion Sustained Release (dose of mg/day) evaluated in an uncontrolled, open-label trial in 15 patients with marked fatigue Most participants reported an improvement in their level of fatigue within two to four weeks of therapy Controlled trials needed to establish the efficacy of this intervention, and to determine whether this effect of bupropion is separate from its action as an antidepressant Modafinil Several trials also suggest that modafinil at a dose of 100 mg BID may be effective in treating fatigue and improving daytime wakefulness and cognitive function in patients during and following cancer treatment 40
41 Venlafaxine Effectiveness Not Established Small RCT (n=57) showed no improvement in fatigue outcomes Sertraline Large RCT (n=189) in patients with advanced cancer showed not significant effect on fatigue in the absence of depression 41
42 Expert Opinion Work with patient and family caregivers to improve assessment of fatigue and identify management strategies Promote open communication between patient, family and caregiving team to facilitate discussions about the experience of fatigue and its effects on daily life Consider attention restoring activities such as exposure to natural environments, and pleasant distractions such as music Encourage a balanced diet with adequate intake of fluid, calories, protein, carbohydrates, fat, vitamins, minerals 42
43 Case Study Beatrice M is a 54 year old high school art teacher with AML in 1 st remission. She is day +45 status post related allogeneic HSCT with her course complicated by acute GVHD of upper GI tract (nausea and anorexia), and pruritic erythematous skin rash She continues on immunosuppression with tacrolimus and is on a tapering dose of steroids. Due to poor oral intake, she has continued to lose weight (BMI now 22), and she requires daily visits to the day hospital for fluids and magnesium supplementation She has mild anemia which she tearfully admits causes her some concern about her remission status, however donor chimerism is 100% On review of systems she has periodic waves of nausea, a limited appetite, and has been sleeping poorly for more than month since starting steroids. She often cat-naps throughout the day and early evening, with the result that she finds it difficult to sleep at night. In addition to the cutaneous findings for acute GVHD of the skin, on examination she has mild proximal muscle weakness 43
44 Your Approach Screen for fatigue using a 0-10 scale Fatigue is a 5 Evaluate for contributing fatigue contributing factors: Anemia Emotional distress Proximal muscle weakness Sarcopenia and weight loss Concurrent symptoms (pruritis, nausea, anorexia) Poor sleep quality Dehydration/electrolyte imbalances 44
45 Your Approach Anticipatory guidance about possible reasons for fatigue (anemia, proinflammatory cytokine activity with acute GVHD, sarcopenia, proximal muscle weakness, concurrent symptoms, sleep quality) and options for selfmanagement Teach energy conservation strategies Refer to physical therapy for proximal muscle strengthening and a gentle exercise program Supportive therapy to help manage anxiety Nutrition consultation to attenuate weight loss Multiple vitamin supplement; folic acid Consider medication to improve sleep quality Topical agents to relieve pruritis 45
46 Case Study Gina M.is a married, 56 year old African American female who is 2 1/2 years post matched-unrelated donor hematopoietic stem cell transplantation for acute lymphocytic leukemia (ALL). She was conditioned with Bu/Cy/TBI. Her posttransplant course has been complicated by chronic graft-versus-host disease (GVHD) requiring treatment with immunosuppressants, including prednisone 40 mg daily Comorbidities include neuropathic pain (NP), depression, weight gain, and osteoporosis. She has been post-menopausal since her remission induction chemotherapy Gina has returned to part- time work, with adjusted responsibilities due to her physical and cognitive fatigue and to allow her to keep frequent medical appointments. However she is worried these accommodations will not be offered to her indefinitely Although Gina was prepared to feel fatigue for at least a year post-transplant, she has become very discouraged by its persistence, and she is tearful as she discusses her concerns 46
47 Case Study Due to multiple psychological stresses as well as neuropathy, she has difficulty falling asleep most nights, and often lies awake due to pain. Although she has had trouble sleeping for several years, this has worsened with the initiation of prednisone. She rates her fatigue severity as 6 or 8 on a 0-10 scale and is fatigued on most days. Her muscles feel weak and she frequently experiences daytime sleepiness, difficulty concentrating, and short term memory problems. These have all caused her to limit her social interaction and recreational pursuits. She often goes straight to bed after work, spending the evening napping and watching TV On examination she is obese with a BMI of 32; CBC and basic metabolic panel are normal 47
48 Your Approach Comprehensive assessment of fatigue and sleep-wake patterns Evaluate for contributing factors such as hypothyroidism (given conditioning with TBI) TSH and reduced free-t4 consistent with hypothyroidism You also note depression, sarcopenia, and suboptimal management of neuropathic pain. She is not engaged in a program of regular exercise 48
49 Your Approach Pharmacotherapy to address pain, depression, and hypothyroidism Referral to physical therapy to improve strength, aerobic conditioning, and muscle mass Amitriptyline hydrochloride at hs is selected for painful neuropathy, and its sedating side-effects may also have a beneficial impact on sleep To improve sleep quality you also recommend progressive muscle relaxation with imagery behavioral measures including regular bedtime and get-up times, using the bedroom only for sleep and sexual activity, and initiating a calming pre-sleep routine 49
50 Your Approach You discuss with Gina several causes of her fatigue during survivorship and how chronic GVHD and its treatment with corticosteroids may amplify her fatigue and sleep problems through an altered cytokine milieu and disrupted immune-neuro-endocrine stress response You also provide coaching to encourage goal setting and self-management. At the weekly team conference you suggest administering prednisone in the morning to limit the effects on sleep and/or moving to an every-other day steroid dosing, as tapering proceeds At her follow-up appointment 8 weeks later, Gina rates her fatigue as a 3 (0-10) and reports her sleep and daytime functioning are gradually improving The team encourages her to continue the positive steps she has taken to reduce her symptom distress and recommends follow-up assessments every month to modify the care plan and consider referrals 50
51 Implications for Practice Ongoing periodic screening is an essential component of care quality 10 point scale for screening is efficient and sensitive; moderate to severe fatigue 4-10 (on 10 point scale) warrants further evaluation and treatment Use national guidelines (NCCN and ONS-PEP) to: Examine your practice and expand the repertoire of interventions recommended for a specific patient based on efficacy Emphasis has been on fatigue in patients with solid tumors who are on treatment and cancer survivors 51
52 Implications for Practice Attention to treating comorbidities (e.g. deconditioning, impaired sleep quality, concurrent symptoms, mood disturbances) Multimodal approach addressing both central and peripheral fatigue: exercise psychoeducational interventions to optimize fatigue self-management manage concurrent symptoms (especially depression, pain and stress) improve sleep quality judicious use of medications such as modafinil, methylphenidate to improve daytime dysfunction complementary therapies such as relaxation, massage, healing touch, or acupuncture 52
53 Implications for Practice Screen for correctable contributing factors: anemia, thyroid dysfunction, hypogonadism, cardiomyopathy, adrenal insufficiency, pulmonary dysfunction, sleep disturbances, fluid and electrolyte imbalances Provide patients with anticipatory information about fatigue prior to initiation of treatment, and as they transition to survivorship phase Develop plan to prevent/manage fatigue Systematic evaluation of fatigue at baseline and prospectively, to evaluate outcome of intervention 53
54 Recommendations for Cancer-Related Fatigue in Adults: National Guidelines Interventions Identified as Recommended for Practice by NCCN, ONS, CPAC/CAPO, ASCO Address Treatable Contributors to Fatigue Manage Concurrent Symptoms Physical Activity/Exercise Comprehensive rehabilitation Psychoeducational Interventions, including Energy Conservation Meditation, mindfulness-based stress reduction, cognitive-behavioral stress management Relaxation Cognitive-behavioral therapy for fatigue, depression, and pain Cognitive-behavioral therapy for sleep Yoga 54

55 55
56 Implications for Research Many of the fatigue interventions have had only limited study- many were uncontrolled trials or pilot work Few interventions have been tested in transplant recipients and survivors Randomized trials are indicated Further development of interventions that have shown promise (eg. massage, rehabilitation) Evaluate therapies where there were mixed results (eg. accupuncture, methylphenidate; modafinil) to develop more tailored indications for use 56


57
Why am I so Tired? Cancer Related Fatigue. Rose Bell, PhD, ARNP, AOCNP Northwest Medical Specialties
 Why am I so Tired? Cancer Related Fatigue Rose Bell, PhD, ARNP, AOCNP Northwest Medical Specialties Cancer Related Fatigue (CRF) Significantly different in quality and severity Unrelieved by sleep or rest
Why am I so Tired? Cancer Related Fatigue Rose Bell, PhD, ARNP, AOCNP Northwest Medical Specialties Cancer Related Fatigue (CRF) Significantly different in quality and severity Unrelieved by sleep or rest
CANCER-RELATED Fatigue. Nelson Byrne, Ph.D., C.Psych. Krista McGrath, MRT(T), HBSc.
, HBSc.") CANCER-RELATED Fatigue Nelson Byrne, Ph.D., C.Psych. Krista McGrath, MRT(T), HBSc. Faculty/Presenter Disclosure Faculty: Nelson Byrne, Ph.D., C.Psych. and Krista McGrath, MRT(T), HBSc. with the Mississauga
CANCER-RELATED Fatigue Nelson Byrne, Ph.D., C.Psych. Krista McGrath, MRT(T), HBSc. Faculty/Presenter Disclosure Faculty: Nelson Byrne, Ph.D., C.Psych. and Krista McGrath, MRT(T), HBSc. with the Mississauga
FATIGUE: PHARMACOLOGICAL AND NON-PHARMACOLOGICAL TREATMENT. Fausto Roila Medical Oncology Division, Terni, Italy
 FATIGUE: PHARMACOLOGICAL AND NON-PHARMACOLOGICAL TREATMENT Fausto Roila Medical Oncology Division, Terni, Italy CONFLICT OF INTERESTS NO CONFLICT FATIGUE: DEFINITION (ASCO, NCCN) Cancer-related fatigue
FATIGUE: PHARMACOLOGICAL AND NON-PHARMACOLOGICAL TREATMENT Fausto Roila Medical Oncology Division, Terni, Italy CONFLICT OF INTERESTS NO CONFLICT FATIGUE: DEFINITION (ASCO, NCCN) Cancer-related fatigue
Sunil Nagpal MD Director, Thoracic Oncology West Michigan Cancer Center
 Sunil Nagpal MD Director, Thoracic Oncology West Michigan Cancer Center Disclosures No disclosures Definition of Cancer Related Fatigue Cancer related fatigue is a distressing, persistent, subjective sense
Sunil Nagpal MD Director, Thoracic Oncology West Michigan Cancer Center Disclosures No disclosures Definition of Cancer Related Fatigue Cancer related fatigue is a distressing, persistent, subjective sense
8/29/2013. Discuss Relation of Fatigue to Sleep Disturbance. Assessing and Treating Factors Contributing to Fatigue and Sleep Disturbance
 Timothy Pearman, Ph.D. Director, Supportive Oncology Robert H. Lurie Comprehensive Cancer Center Associate Professor of Medical Social Sciences and Psychiatry Northwestern University Feinberg School of
Timothy Pearman, Ph.D. Director, Supportive Oncology Robert H. Lurie Comprehensive Cancer Center Associate Professor of Medical Social Sciences and Psychiatry Northwestern University Feinberg School of
Managing Fatigue in Bone Marrow Failure Diseases
 Managing Fatigue in Bone Marrow Failure Diseases Lora Thompson, Ph.D. Clinical Psychologist Psychosocial and Palliative Care Program Moffitt Cancer Center Definition of Fatigue a distressing, persistent,
Managing Fatigue in Bone Marrow Failure Diseases Lora Thompson, Ph.D. Clinical Psychologist Psychosocial and Palliative Care Program Moffitt Cancer Center Definition of Fatigue a distressing, persistent,
Symptom Control in Cancer Rehabilitation. Ying Guo, MD Department of Palliative, Rehabilitation and Integrative Medicine UT MD Anderson Cancer Center
 Symptom Control in Cancer Rehabilitation Ying Guo, MD Department of Palliative, Rehabilitation and Integrative Medicine UT MD Anderson Cancer Center Cancer Patients Symptoms Pain- 90% of patients with
Symptom Control in Cancer Rehabilitation Ying Guo, MD Department of Palliative, Rehabilitation and Integrative Medicine UT MD Anderson Cancer Center Cancer Patients Symptoms Pain- 90% of patients with
Fatigue and Myeloma. information sheet
 Fatigue and Myeloma Cancer related fatigue (CRF) is defined as a distressing, persistent and subjective feeling of physical, mental or emotional tiredness related to cancer and/or cancer treatment interfering
Fatigue and Myeloma Cancer related fatigue (CRF) is defined as a distressing, persistent and subjective feeling of physical, mental or emotional tiredness related to cancer and/or cancer treatment interfering
a persistent symptom, a subjective feeling of physical, emotional or cognitive tiredness or exhaustion related to cancer or its treatment that is not
 a persistent symptom, a subjective feeling of physical, emotional or cognitive tiredness or exhaustion related to cancer or its treatment that is not proportional to the recently performed activity, and
a persistent symptom, a subjective feeling of physical, emotional or cognitive tiredness or exhaustion related to cancer or its treatment that is not proportional to the recently performed activity, and
The World Health Organization has developed and has widely accepted an algorithm for treatment of cancer pain. This is described as the three-step lad
 Hello. My name is Cynthia Abarado. I m an Advanced Practice Nurse at the Department of Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. I am going to present to you
Hello. My name is Cynthia Abarado. I m an Advanced Practice Nurse at the Department of Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. I am going to present to you
PAIN MANAGEMENT & MAXIMIZING QUALITY OF LIFE DURING TREATMENT
 PAIN MANAGEMENT & MAXIMIZING QUALITY OF LIFE DURING TREATMENT Brandy Ficek, MD Medical Director of Quality of Life and Palliative Medicine Cancer Treatment Centers of America Rocky Mountain Blood Cancer
PAIN MANAGEMENT & MAXIMIZING QUALITY OF LIFE DURING TREATMENT Brandy Ficek, MD Medical Director of Quality of Life and Palliative Medicine Cancer Treatment Centers of America Rocky Mountain Blood Cancer
Living Well with Bone Marrow Failure Diseases
 Living Well with Bone Marrow Failure Diseases ISABEL SCHUERMEYER, MD DIRECTOR OF PSYCHO-ONCOLOGY CLEVELAND CLINIC JUNE 22, 2013 Overview What do we know about symptoms & quality of life for bone marrow
Living Well with Bone Marrow Failure Diseases ISABEL SCHUERMEYER, MD DIRECTOR OF PSYCHO-ONCOLOGY CLEVELAND CLINIC JUNE 22, 2013 Overview What do we know about symptoms & quality of life for bone marrow
INSOMNIAS. Stephan Eisenschenk, MD Department of Neurology
 INSOMNIAS INSOMNIAS General criteria for insomnia A. Repeated difficulty with sleep initiation, duration, consolidation or quality. B. Adequate sleep opportunity, persistent sleep difficulty and associated
INSOMNIAS INSOMNIAS General criteria for insomnia A. Repeated difficulty with sleep initiation, duration, consolidation or quality. B. Adequate sleep opportunity, persistent sleep difficulty and associated
Caring for the Mind: Managing Depression and Anxiety. Highlights from 2017 ONS Congress
 Caring for the Mind: Managing Depression and Anxiety Highlights from 2017 ONS Congress Mood and Anxiety Disorders: Symptoms of mood disorders Non-reactive mood, worthlessness, guilt, loss of interest,
Caring for the Mind: Managing Depression and Anxiety Highlights from 2017 ONS Congress Mood and Anxiety Disorders: Symptoms of mood disorders Non-reactive mood, worthlessness, guilt, loss of interest,
Beyond Sleep Hygiene: Behavioral Approaches to Insomnia
 Beyond Sleep Hygiene: Behavioral Approaches to Insomnia Rocky Garrison, PhD, CBSM Damon Michael Williams, RN, PMHNP-BC In House Counseling Laughing Heart LLC 10201 SE Main St. 12 SE 14 th Ave. Suite 10
Beyond Sleep Hygiene: Behavioral Approaches to Insomnia Rocky Garrison, PhD, CBSM Damon Michael Williams, RN, PMHNP-BC In House Counseling Laughing Heart LLC 10201 SE Main St. 12 SE 14 th Ave. Suite 10
Fatigue Management in Cancer Care
 Fatigue Management in Cancer Care Overview 1. What is Cancer-Related Fatigue? Causes & symptoms 2. Negative cycles that fuel CRF 3. What are the consequences of CRF 4. Intervention & rehabilitation 5.
Fatigue Management in Cancer Care Overview 1. What is Cancer-Related Fatigue? Causes & symptoms 2. Negative cycles that fuel CRF 3. What are the consequences of CRF 4. Intervention & rehabilitation 5.
Insomnia. Learning Objectives. Disclosure 6/7/11. Research funding: NIH, Respironics, Embla Consulting: Elsevier
 Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Insomnia Teofilo Lee-Chiong MD Professor of Medicine National Jewish Health University of Colorado Denver School of Medicine Learning Objectives Learn about the causes of transient and chronic Learn how
Guideline for Adult Insomnia
 Guideline for Adult Insomnia Exclusions This guideline does not apply to: Children under the age of 18 Pregnant and lactating women Geriatric patients: While the general principles of the diagnosis and
Guideline for Adult Insomnia Exclusions This guideline does not apply to: Children under the age of 18 Pregnant and lactating women Geriatric patients: While the general principles of the diagnosis and
Sleep, Stress, and Fatigue
 Sleep, Stress, and Fatigue Central Washington University E.A.S.E. Cancer Foundation Tim Burnham Ph.D. Interrelated Stress Sleep disturbance Fatigue Stress Stress is YOUR response to a situation Stressor:
Sleep, Stress, and Fatigue Central Washington University E.A.S.E. Cancer Foundation Tim Burnham Ph.D. Interrelated Stress Sleep disturbance Fatigue Stress Stress is YOUR response to a situation Stressor:
SLEEP DISORDERS. Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children
 SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
SLEEP DISORDERS Kenneth C. Sassower, MD Division of Sleep Medicine; Department of Neurology Massachusetts General Hospital for Children Distinctive Features of Pediatric Sleep Daytime sleepiness uncommon
Sleep and Traumatic Brain Injury (TBI)
") Sleep and Traumatic Brain Injury (TBI) A resource for individuals with traumatic brain injury and their supporters This presentation is based on TBI Model Systems research and was developed with support
Sleep and Traumatic Brain Injury (TBI) A resource for individuals with traumatic brain injury and their supporters This presentation is based on TBI Model Systems research and was developed with support
10/8/2014. Quality of Life: On score of 0 (poor) 10 (excellent): MDS average = 5.1. Normal average = 7.7
 10 (excellent): MDS average = 5.1. Normal average = 7.7") What do we know about symptoms & quality of life for bone marrow failure disease patients? Isabel Schuermeyer, MD Director of Psycho-Oncology Cleveland Clinic AA/MDS International Foundation 2014 regional
What do we know about symptoms & quality of life for bone marrow failure disease patients? Isabel Schuermeyer, MD Director of Psycho-Oncology Cleveland Clinic AA/MDS International Foundation 2014 regional
Integrative Medicine at SCCA: A New Program for Survivors
 Integrative Medicine at SCCA: A New Program for Survivors Heather Greenlee, ND, PhD Medical Director, Integrative Medicine Program Associate Member, Fred Hutch Associate Professor, UW School of Medicine
Integrative Medicine at SCCA: A New Program for Survivors Heather Greenlee, ND, PhD Medical Director, Integrative Medicine Program Associate Member, Fred Hutch Associate Professor, UW School of Medicine
Many people with physical
 FACTSHEET How to Sleep Better Many people with physical disabilities suffer from sleep disturbances, and sleep tends to become more disrupted as we get older. Not sleeping well can negatively impact your
FACTSHEET How to Sleep Better Many people with physical disabilities suffer from sleep disturbances, and sleep tends to become more disrupted as we get older. Not sleeping well can negatively impact your
Oncology Nursing Society Registry in Collaboration with CE City 2015 Performance Measure Specifications
 1 ONSQIR 1 Non-PRQS Measure Oncology Nursing Society Registry in Collaboration with CE City 2015 Performance Measure Specifications Performance Measure Name: Symptom Assessment 1-o1a Symptom Assessment
1 ONSQIR 1 Non-PRQS Measure Oncology Nursing Society Registry in Collaboration with CE City 2015 Performance Measure Specifications Performance Measure Name: Symptom Assessment 1-o1a Symptom Assessment
TOP 10 LIST OF SLEEP QUESTIONS. Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children
 TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
TOP 10 LIST OF SLEEP QUESTIONS Kenneth C. Sassower, MD Sleep Disorders Unit Massachusetts General Hospital for Children QUESTION #1: ARE SLEEP ISSUES IN CHILDREN THE SAME AS IN ADULTS? Distinctive Features
Emotional Adaptation after Cancer
 Emotional Adaptation after Cancer Jesse Fann, MD, MPH Department of Psychiatry & Behavioral Sci, UW Clinical Research Division, FHCRC Director, Psychiatry & Psychology Service, SCCA Outline Fear of Recurrence
Emotional Adaptation after Cancer Jesse Fann, MD, MPH Department of Psychiatry & Behavioral Sci, UW Clinical Research Division, FHCRC Director, Psychiatry & Psychology Service, SCCA Outline Fear of Recurrence
YOU REALLY NEED TO SLEEP: Several methods to improve your sleep
 YOU REALLY NEED TO SLEEP: Several methods to improve your sleep Sleep is essential to our well-being. When humans fail to get good sleep over a period of time, numerous problems can occur. CAN T SLEEP!!
YOU REALLY NEED TO SLEEP: Several methods to improve your sleep Sleep is essential to our well-being. When humans fail to get good sleep over a period of time, numerous problems can occur. CAN T SLEEP!!
Sleep Hygiene. William M. DeMayo, M.D. John P. Murtha Neuroscience and Pain Institute Conemaugh Health System Johnstown, PA
 Sleep Hygiene William M. DeMayo, M.D. John P. Murtha Neuroscience and Pain Institute Conemaugh Health System Johnstown, PA Why Is Sleep Important? Symptoms of Sleep Deprivation: Irritability / Poor Stress
Sleep Hygiene William M. DeMayo, M.D. John P. Murtha Neuroscience and Pain Institute Conemaugh Health System Johnstown, PA Why Is Sleep Important? Symptoms of Sleep Deprivation: Irritability / Poor Stress
6/3/2015. Insomnia An Integrative Approach. Objectives. Why An Integrative Approach? Integrative Model. Definition. Short-term Insomnia
 Insomnia An Integrative Approach Jeffrey S. Jump, M.D. Medical Director CHI Memorial Integrative Medicine Associates Objectives Understand the importance of sleep to health Identify patients with insomnia
Insomnia An Integrative Approach Jeffrey S. Jump, M.D. Medical Director CHI Memorial Integrative Medicine Associates Objectives Understand the importance of sleep to health Identify patients with insomnia
Treating Insomnia in Primary Care. Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team
 Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
HEALTH 3--DEPRESSION, SLEEP, AND HEALTH GOALS FOR LEADERS. To educate participants regarding the sleep wake cycle.
 HEALTH 3--DEPRESSION, SLEEP, AND HEALTH GOALS FOR LEADERS Talk about the relationship between depression, sleep, and health problems. To educate participants regarding the sleep wake cycle. To provide
HEALTH 3--DEPRESSION, SLEEP, AND HEALTH GOALS FOR LEADERS Talk about the relationship between depression, sleep, and health problems. To educate participants regarding the sleep wake cycle. To provide
Sleep and mental wellbeing: exploring the links
 Sleep and mental wellbeing: exploring the links Like most physiological functions, the length and quality of sleep is influenced by a host of biological, environmental and lifestyle factors. Across all
Sleep and mental wellbeing: exploring the links Like most physiological functions, the length and quality of sleep is influenced by a host of biological, environmental and lifestyle factors. Across all
WHEN COUNTING SHEEP FAILS: ADMINISTERING SINGLE-SESSION COGNITIVE-BEHAVIORAL THERAPY FOR INSOMNIA IN A GROUP PSYCHOEDUCATIONAL FORMAT
 WHEN COUNTING SHEEP FAILS: ADMINISTERING SINGLE-SESSION COGNITIVE-BEHAVIORAL THERAPY FOR INSOMNIA IN A GROUP PSYCHOEDUCATIONAL FORMAT Kristin E. Eisenhauer, PhD. Trinity University San Antonio, Texas I
WHEN COUNTING SHEEP FAILS: ADMINISTERING SINGLE-SESSION COGNITIVE-BEHAVIORAL THERAPY FOR INSOMNIA IN A GROUP PSYCHOEDUCATIONAL FORMAT Kristin E. Eisenhauer, PhD. Trinity University San Antonio, Texas I
Psychological Sleep Services Sleep Assessment
 Psychological Sleep Services Sleep Assessment Name Date **************************************************** Insomnia Severity Index For each question, please CIRCLE the number that best describes your
Psychological Sleep Services Sleep Assessment Name Date **************************************************** Insomnia Severity Index For each question, please CIRCLE the number that best describes your
Fatigue and Quality of Life. Overview What do we know about symptoms & quality of life for bone marrow failure disease patients?
 Breaking Point: Learning How to Relax, Relate, and Release Isabel Schuermeyer, MD Director of Psycho-Oncology Cleveland Clinic AA/MDS International Foundation 2014 regional conference September 20, 2014
Breaking Point: Learning How to Relax, Relate, and Release Isabel Schuermeyer, MD Director of Psycho-Oncology Cleveland Clinic AA/MDS International Foundation 2014 regional conference September 20, 2014
Article printed from
 What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
Healthy Sleep Tips Along the Way!
 Women and Sleep What You Will Learn The Benefits and Importance of Sleep States and Stages of the Sleep Cycle Unique Physiology of Women s Sleep Common Disorders in Women that Affect Sleep Women s Role
Women and Sleep What You Will Learn The Benefits and Importance of Sleep States and Stages of the Sleep Cycle Unique Physiology of Women s Sleep Common Disorders in Women that Affect Sleep Women s Role
Beyond Cancer Moving On
 Beyond Cancer Moving On Today, people with cancer have a better chance at living a normal life than ever before in history. In fact, there are more than 10 million survivors people who have, or are living
Beyond Cancer Moving On Today, people with cancer have a better chance at living a normal life than ever before in history. In fact, there are more than 10 million survivors people who have, or are living
Survivorship: Life Beyond Cancer Treatment
 Survivorship: Life Beyond Cancer Treatment 1 1 Dear Cancer Survivor, The Cancer Survivorship program at University of Maryland St. Joseph Medical Center s Cancer Institute is designed to help patients
Survivorship: Life Beyond Cancer Treatment 1 1 Dear Cancer Survivor, The Cancer Survivorship program at University of Maryland St. Joseph Medical Center s Cancer Institute is designed to help patients
Sweet Dreams: The Relationship between Sleep Health and Your Weight
 Sweet Dreams: The Relationship between Sleep Health and Your Weight Jason C. Ong, PhD Associate Professor Department of Neurology Center for Circadian and Sleep Medicine Northwestern University Feinberg
Sweet Dreams: The Relationship between Sleep Health and Your Weight Jason C. Ong, PhD Associate Professor Department of Neurology Center for Circadian and Sleep Medicine Northwestern University Feinberg
SECTION 1. Children and Adolescents with Depressive Disorder: Summary of Findings. from the Literature and Clinical Consultation in Ontario
 SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
SECTION 1 Children and Adolescents with Depressive Disorder: Summary of Findings from the Literature and Clinical Consultation in Ontario Children's Mental Health Ontario Children and Adolescents with
Living Well with MDS. Overview. What are the biggest physical and emotional challenges you are facing
 Living Well with MDS Strategies for Optimizing Emotional and Physical Health Isabel Schuermeyer, MD Director, Psycho-Oncology Cleveland Clinic Paul Scribner, LISW Director, Patient Programs and Services
Living Well with MDS Strategies for Optimizing Emotional and Physical Health Isabel Schuermeyer, MD Director, Psycho-Oncology Cleveland Clinic Paul Scribner, LISW Director, Patient Programs and Services
3/5/2018 CANCER ASSOCIATED FATIGUE & PAIN OBJECTIVES CHRONIC PAIN ACUTE PAIN PAIN SCALES
 OBJECTIVES CANCER ASSOCIATED FATIGUE & PAIN SCOT M. SAWYER, PT, DPT BOARD CERTIFIED ELECTROPHYSIOLOGY CLINICAL SPECIALIST EMAIL: SAWYER@CAMPBELL.EDU Recognize the multi-factorial pain response cancer survivors
OBJECTIVES CANCER ASSOCIATED FATIGUE & PAIN SCOT M. SAWYER, PT, DPT BOARD CERTIFIED ELECTROPHYSIOLOGY CLINICAL SPECIALIST EMAIL: SAWYER@CAMPBELL.EDU Recognize the multi-factorial pain response cancer survivors
Chronic Insomnia: DSM - V. Insomnia DSM - V. Patient Symptoms. Insomnia: Assessment and Overview of Management. Insomnia Management in the Digital Age
 Insomnia Management in the Digital Age Dr Anup Desai Sleep & Respiratory Medicine MBBS (syd), PhD (syd), FRACP Senior Staff Specialist, POW Hospital Medical Director, Sydney Sleep Centre Senior Lecturer,
Insomnia Management in the Digital Age Dr Anup Desai Sleep & Respiratory Medicine MBBS (syd), PhD (syd), FRACP Senior Staff Specialist, POW Hospital Medical Director, Sydney Sleep Centre Senior Lecturer,
Weakness & Fatigue. Introduction. Assessment
 Weakness & Fatigue Introduction Fatigue is a persistent, subjective feeling of tiredness, weakness or lack of energy related to advanced chronic illness. It has many contributory causes though the exact
Weakness & Fatigue Introduction Fatigue is a persistent, subjective feeling of tiredness, weakness or lack of energy related to advanced chronic illness. It has many contributory causes though the exact
Fatigue and Chronic Fatigue Syndrome
 Fatigue and Chronic Fatigue Syndrome Introduction Nearly everyone struggles with being overtired or overworked from time to time. Temporary fatigue usually has a specific cause. It is easily treated. Chronic
Fatigue and Chronic Fatigue Syndrome Introduction Nearly everyone struggles with being overtired or overworked from time to time. Temporary fatigue usually has a specific cause. It is easily treated. Chronic
Insomnia treatment. Sleep hygiene education sleep hygiene teaches good sleeping habits. This includes:
 Insomnia treatment INSOMNIA OVERVIEW insomnia is defined as difficulty falling asleep, difficulty staying asleep, or waking up early in the morning and not being able to return to sleep. In general, people
Insomnia treatment INSOMNIA OVERVIEW insomnia is defined as difficulty falling asleep, difficulty staying asleep, or waking up early in the morning and not being able to return to sleep. In general, people
Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice.
 Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice. 25th Annual Palliative Education and Research Days, West Edmonton Mall. Edmonton. 2014 Amanda
Road Blocks in Non-Cancer Palliative Care Obstacles observed from outpatient non-cancer palliative practice. 25th Annual Palliative Education and Research Days, West Edmonton Mall. Edmonton. 2014 Amanda
Chronic Fatigue Syndrome
 Chronic Fatigue Syndrome CFS Toolkit Introduction to the Toolkit Chronic fatigue syndrome (CFS) is a complex and serious illness. The CFS toolkit was prepared to provide a quick and easy-to-use resource
Chronic Fatigue Syndrome CFS Toolkit Introduction to the Toolkit Chronic fatigue syndrome (CFS) is a complex and serious illness. The CFS toolkit was prepared to provide a quick and easy-to-use resource
Index. sleep.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
Note: Page numbers of article titles are in boldface type. A Actigraphy, 475, 485, 496 Adolescents, sleep disorders in, 576 578 Adults, sleep disorders in, 578 580 Advanced sleep phase disorder, 482 Age,
Page 1 of 8. 7 SICKNESS AND HEALTH 7.1. chronic diseases and quality of life
 Page 1 of 8 7 SICKNESS AND HEALTH 7.1. chronic diseases and quality of life Illnesses are classified as either acute or chronic. An acute illness lasts for a short period of time and may go away without
Page 1 of 8 7 SICKNESS AND HEALTH 7.1. chronic diseases and quality of life Illnesses are classified as either acute or chronic. An acute illness lasts for a short period of time and may go away without
2018 OCN Keywords January 22, 2018 Subject Area Weight Keywords
 Subject Area Weight Keywords Care Continuum 19% Care Continuum Coordination of Care Navigation Psychosocial Symptom Management Health Promotion/Screening and Early Detection Disease Prevention High-Risk
Subject Area Weight Keywords Care Continuum 19% Care Continuum Coordination of Care Navigation Psychosocial Symptom Management Health Promotion/Screening and Early Detection Disease Prevention High-Risk
INSOMNIA IN GERIATRICS. Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow
 INSOMNIA IN GERIATRICS Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow Insomnia Insomnia is the inability to fall asleep, the inability to stay asleep, or waking up earlier than desired. To
INSOMNIA IN GERIATRICS Presented By: Sara Kamalfar MD, Geriatrics Medicine Fellow Insomnia Insomnia is the inability to fall asleep, the inability to stay asleep, or waking up earlier than desired. To
WHY CAN T I SLEEP? Deepti Chandran, MD
 WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
Alliance. At Connecticut Fertility Associates Main Street, Suite 306 Bridgeport, CT (203)
") Alliance At Connecticut Fertility Associates 4920 Main Street, Suite 306 Bridgeport, CT 06066 (203) 373-1200 fertility & wellness hand in hand Mind-Body Alliance at CFA Connecticut Fertility Associates'
Alliance At Connecticut Fertility Associates 4920 Main Street, Suite 306 Bridgeport, CT 06066 (203) 373-1200 fertility & wellness hand in hand Mind-Body Alliance at CFA Connecticut Fertility Associates'
ANN BERGER. Key Words. Fatigue Neoplasms Depression Anemia Sleep disorders
 The Oncologist Treating Fatigue in Cancer Patients ANN BERGER Warren Grant Magnuson Clinical Center, National Institutes of Health, Bethesda, Maryland, USA Key Words. Fatigue Neoplasms Depression Anemia
The Oncologist Treating Fatigue in Cancer Patients ANN BERGER Warren Grant Magnuson Clinical Center, National Institutes of Health, Bethesda, Maryland, USA Key Words. Fatigue Neoplasms Depression Anemia
Karen s Ultimate Guide to a Solid Nights Sleep
 Karen s Ultimate Guide to a Solid Nights Sleep Insomnia has reached epidemic proportions. It s estimated to be the #1 health-related problem in America. More than 1/3 of Americans have trouble sleeping
Karen s Ultimate Guide to a Solid Nights Sleep Insomnia has reached epidemic proportions. It s estimated to be the #1 health-related problem in America. More than 1/3 of Americans have trouble sleeping
Ask the. Natural Strategies for Managing Insomnia. A^Insomnia is a sleep disor- DOCTOR
 Natural Strategies for Managing Insomnia ^ / am a 45-year-old woman. Q Although my overall health is ^ood, I have sufferedfromchronic insomnia for more than 15 years. I am concerned that lack of sleep
Natural Strategies for Managing Insomnia ^ / am a 45-year-old woman. Q Although my overall health is ^ood, I have sufferedfromchronic insomnia for more than 15 years. I am concerned that lack of sleep
The Role of Palliative Care in Advanced Lung Disease
 The Role of Palliative Care in Advanced Lung Disease Timothy B. Short, MD, FAAFP, FAAHPM Associate Professor, Palliative Medicine University of Virginia Learning Objectives Describe palliative care s approach
The Role of Palliative Care in Advanced Lung Disease Timothy B. Short, MD, FAAFP, FAAHPM Associate Professor, Palliative Medicine University of Virginia Learning Objectives Describe palliative care s approach
Katherine Anderson, ND FABNO National Director Naturopathic Medicine Cancer Treatment Centers of America
 Katherine Anderson, ND FABNO National Director Naturopathic Medicine Cancer Treatment Centers of America Katherine.Anderson@ctca-hope.com 2013 OSCO Nurses Meeting August 17th, 2013 2008 Rising Tide, Kft.
Katherine Anderson, ND FABNO National Director Naturopathic Medicine Cancer Treatment Centers of America Katherine.Anderson@ctca-hope.com 2013 OSCO Nurses Meeting August 17th, 2013 2008 Rising Tide, Kft.
th Ave NE Suite F Bellevue, WA Phone: (425) Fax: (425) Excessive Daytime Sleepiness
 Fax: (425) Excessive Daytime Sleepiness") 1414 116 th Ave NE Suite F Bellevue, WA 98004 Phone: (425) 451-8417 Fax: (425) 455-4089 Excessive Daytime Sleepiness Nearly everyone has days when they feel sleepy. But for some people, excessive sleepiness
1414 116 th Ave NE Suite F Bellevue, WA 98004 Phone: (425) 451-8417 Fax: (425) 455-4089 Excessive Daytime Sleepiness Nearly everyone has days when they feel sleepy. But for some people, excessive sleepiness
Insomnia. Dr Terri Henderson MBChB FCPsych
 Insomnia Dr Terri Henderson MBChB FCPsych Plan Basics of insomnia Pharmacology Medication CBT Details of insomnia Unsatisfactory sleep that impairs daytime well-being Starts with specific problem or change
Insomnia Dr Terri Henderson MBChB FCPsych Plan Basics of insomnia Pharmacology Medication CBT Details of insomnia Unsatisfactory sleep that impairs daytime well-being Starts with specific problem or change
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) Crain, A. L., Enstad, C. J., Hanson, L. R., Kreitzer, M., Lewis, B. A., & Whitebird, R. R. (2012). Mindfulness-based stress reduction for family caregivers: A randomized
CRITICALLY APPRAISED PAPER (CAP) Crain, A. L., Enstad, C. J., Hanson, L. R., Kreitzer, M., Lewis, B. A., & Whitebird, R. R. (2012). Mindfulness-based stress reduction for family caregivers: A randomized
Who is at risk? What should we do in the clinic?
 Cognitive Changes after Cancer Treatment Patricia A. Ganz, M.D. Professor, UCLA Schools of Medicine & Public Health Director, UCLA-LIVESTRONG Survivorship Center of Excellence Jonsson Comprehensive Cancer
Cognitive Changes after Cancer Treatment Patricia A. Ganz, M.D. Professor, UCLA Schools of Medicine & Public Health Director, UCLA-LIVESTRONG Survivorship Center of Excellence Jonsson Comprehensive Cancer
Cancer and Cognitive Functioning: Strategies for Improvement
 Cancer and Cognitive Functioning: Strategies for Improvement Myron Goldberg, Ph.D., ABPP-CN Clinical Neuropsychologist Director, Neuro-Rehabilitation Program Department of Rehabilitation Medicine University
Cancer and Cognitive Functioning: Strategies for Improvement Myron Goldberg, Ph.D., ABPP-CN Clinical Neuropsychologist Director, Neuro-Rehabilitation Program Department of Rehabilitation Medicine University
Cognitive behavioural therapy for insomnia
 Cognitive behavioural therapy for insomnia Item type Authors Citation Publisher Journal Article Ruth, Alan Ruth A. Cognitive behavioural therapy for insomnia. Nurs Gen Prac 2014 May 29-30, 32 Nursing in
Cognitive behavioural therapy for insomnia Item type Authors Citation Publisher Journal Article Ruth, Alan Ruth A. Cognitive behavioural therapy for insomnia. Nurs Gen Prac 2014 May 29-30, 32 Nursing in
The Integrative Pain Management Program: A Pilot Clinic Serving High-Risk Primary Care Patients with Chronic Pain
 The Integrative Pain Management Program: A Pilot Clinic Serving High-Risk Primary Care Patients with Chronic Pain IM4US CONFERENCE 25 AUGUST 2017 EMILY HURSTAK, MD, MPH, MAS SAN FRANCISCO DEPARTMENT OF
The Integrative Pain Management Program: A Pilot Clinic Serving High-Risk Primary Care Patients with Chronic Pain IM4US CONFERENCE 25 AUGUST 2017 EMILY HURSTAK, MD, MPH, MAS SAN FRANCISCO DEPARTMENT OF
Sophia L. Dollar, MPH Wellness Coach
 Sophia L. Dollar, MPH Wellness Coach Welcome! Today s Outline: Introduction I. Public Health Problem II. The Sleep Cycle III. IV. I. NREM & REM Cycle II. The Right Mix Insomnia I. Causes and Effects II.
Sophia L. Dollar, MPH Wellness Coach Welcome! Today s Outline: Introduction I. Public Health Problem II. The Sleep Cycle III. IV. I. NREM & REM Cycle II. The Right Mix Insomnia I. Causes and Effects II.
CBT in the Treatment of Persistent Insomnia in Patients with Cancer
 CBT in the Treatment of Persistent Insomnia in Patients with Cancer Colin A Espie University of Glasgow Sleep Centre Sackler Institute of Psychobiological Research University of Glasgow Scotland UK Outline
CBT in the Treatment of Persistent Insomnia in Patients with Cancer Colin A Espie University of Glasgow Sleep Centre Sackler Institute of Psychobiological Research University of Glasgow Scotland UK Outline
Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
 COURSES ARTICLE - THERAPYTOOLS.US Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems. Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
COURSES ARTICLE - THERAPYTOOLS.US Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems. Individual Planning: A Treatment Plan Overview for Individuals Sleep Disorder Problems.
Faculty/Presenter Disclosure
 A Little CBT I With My Tea Please: Cognitive Behavioural Therapy for insomnia (CBT I) and Its Use In the Treatment of Sleeplessness W. Jerome Alonso, MD Medical Director, Canadian Sleep Consultants Clinical
A Little CBT I With My Tea Please: Cognitive Behavioural Therapy for insomnia (CBT I) and Its Use In the Treatment of Sleeplessness W. Jerome Alonso, MD Medical Director, Canadian Sleep Consultants Clinical
Managing Insomnia: an example sequence of CBT-based sessions for sleep treatment
 Managing Insomnia: an example sequence of CBT-based sessions for sleep treatment Session 1: Introduction and sleep assessment -Assess sleep problem (option: have client complete 20-item sleep questionnaire).
Managing Insomnia: an example sequence of CBT-based sessions for sleep treatment Session 1: Introduction and sleep assessment -Assess sleep problem (option: have client complete 20-item sleep questionnaire).
Depression. How to Manage Your
 How to Manage Your Depression The recommendations in this guide are based on published evidence and expert consensus. The information in this guide was adapted from the following patient tools: Managing
How to Manage Your Depression The recommendations in this guide are based on published evidence and expert consensus. The information in this guide was adapted from the following patient tools: Managing
Objectives. Conflict of Interest Disclosure. Author Conflict of Interest: The Next Hurdle for Cancer Survivors: Who will manage their Pain?
 The Next Hurdle for Cancer Survivors: Who will manage their Pain? Linda Vanni, MSN, RN-BC, ACNS-BC, NP Nurse Practitioner, Pain Management Providence Hospital Southfield, MI Conflict of Interest Disclosure
The Next Hurdle for Cancer Survivors: Who will manage their Pain? Linda Vanni, MSN, RN-BC, ACNS-BC, NP Nurse Practitioner, Pain Management Providence Hospital Southfield, MI Conflict of Interest Disclosure
Improving Your Sleep Course. Session 1 Understanding Sleep and Assessing Your Difficulties
 Improving Your Sleep Course Session 1 Understanding Sleep and Assessing Your Difficulties Course Information Session Details Sessions Session 1 Session 2 Session 3 Session 4 Optional Review Session 5 Session
Improving Your Sleep Course Session 1 Understanding Sleep and Assessing Your Difficulties Course Information Session Details Sessions Session 1 Session 2 Session 3 Session 4 Optional Review Session 5 Session
Living well with and beyond cancer Information, support and practical advice to help you through treatment and beyond
 Living well with and beyond cancer Information, support and practical advice to help you through treatment and beyond Exceptional healthcare, personally delivered Introduction to this booklet Receiving
Living well with and beyond cancer Information, support and practical advice to help you through treatment and beyond Exceptional healthcare, personally delivered Introduction to this booklet Receiving
Slide 1 EXERCISE AND SLEEP. Slide 2 Sleep and Exercise. Slide 3 Stages of Sleep
 Slide 1 EXERCISE AND SLEEP Slide 2 Sleep and Exercise Sleep and exercise two of the most important elements for health As important as diet So are you surprised that there is a gut connection for both
Slide 1 EXERCISE AND SLEEP Slide 2 Sleep and Exercise Sleep and exercise two of the most important elements for health As important as diet So are you surprised that there is a gut connection for both
Dr Alex Bartle. Sleep Well Clinic
 Dr Alex Bartle Sleep Well Clinic Overview of Sleep Disorders Sleep: Why bother. Effect of Poor Quality or reduced Quantity of Sleep Common Sleep Disorders Management of Insomnia Medication vs CBTi Conclusion
Dr Alex Bartle Sleep Well Clinic Overview of Sleep Disorders Sleep: Why bother. Effect of Poor Quality or reduced Quantity of Sleep Common Sleep Disorders Management of Insomnia Medication vs CBTi Conclusion
CRITICALLY APPRAISED PAPER (CAP)
") CRITICALLY APPRAISED PAPER (CAP) Bower, J. E., Crosswell, A. D., Stanton, A. L., Crespi, C. M., Winston, D., Arevalo, J.,... & Ganz, P. A. (2015). Mindfulness meditation for younger breast cancer survivors:
CRITICALLY APPRAISED PAPER (CAP) Bower, J. E., Crosswell, A. D., Stanton, A. L., Crespi, C. M., Winston, D., Arevalo, J.,... & Ganz, P. A. (2015). Mindfulness meditation for younger breast cancer survivors:
Sleep and Performance: An Integrated Perspective
 Sleep and Performance: An Integrated Perspective Sleep Medical Considerations GETTING THE ATHLETE READY Nutrition Exercise and Conditioning Mental Preparation One Third of your Life Sleep: Using one third
Sleep and Performance: An Integrated Perspective Sleep Medical Considerations GETTING THE ATHLETE READY Nutrition Exercise and Conditioning Mental Preparation One Third of your Life Sleep: Using one third
Pharmacy Benefit Determination Policy
 Policy Subject: CNS Stimulant Medications Policy Number: SHS PBD06 Category: CNS Drugs Policy Type: Medical Pharmacy Department: Pharmacy Product (check all that apply): Group HMO/POS ASO PPO Individual
Policy Subject: CNS Stimulant Medications Policy Number: SHS PBD06 Category: CNS Drugs Policy Type: Medical Pharmacy Department: Pharmacy Product (check all that apply): Group HMO/POS ASO PPO Individual
Psychiatric Treatment of the Concussed Athlete
 Psychiatric Treatment of the Concussed Athlete Eastern Athletic Trainers Association January 11 th, 2015 Alexander S. Strauss, MD Centra, P.C. E-MAIL: DRSTRAUSS@ALEXSTRAUSSMD.COM Evidence Mounts Linking
Psychiatric Treatment of the Concussed Athlete Eastern Athletic Trainers Association January 11 th, 2015 Alexander S. Strauss, MD Centra, P.C. E-MAIL: DRSTRAUSS@ALEXSTRAUSSMD.COM Evidence Mounts Linking
Objectives. Types of Sleep Problems in Developmental Disorders
 Objectives Sleep Problems in the Child with Neurodevelopmental Disorders AACPDM September 11, 2014 BRK-3 Golda Milo-Manson MD, MHSc, FRCP(C) Holland Bloorview Kids Rehabilitation Hospital Toronto, Canada
Objectives Sleep Problems in the Child with Neurodevelopmental Disorders AACPDM September 11, 2014 BRK-3 Golda Milo-Manson MD, MHSc, FRCP(C) Holland Bloorview Kids Rehabilitation Hospital Toronto, Canada
Historical Understandings of Pain
 Gain-Control Theory: A Guide for Pain Relief Nursing: Paul Arnstein, RN, PhD, Director: MGH Cares About Pain Relief 9/24/10 ASPMN 20 th Annual Conference Historical Understandings of Pain Pain is mystical
Gain-Control Theory: A Guide for Pain Relief Nursing: Paul Arnstein, RN, PhD, Director: MGH Cares About Pain Relief 9/24/10 ASPMN 20 th Annual Conference Historical Understandings of Pain Pain is mystical
Pharmacologic and Nonpharmacologic Interventions for Pain
 PUTTING EVIDENCE INTO PRACTICE: IMPROVING ONCOLOGY PATIENT OUTCOMES Pharmacologic and Nonpharmacologic Interventions for Pain Introduction A variety of treatments such as chemotherapy, radiation therapy,
PUTTING EVIDENCE INTO PRACTICE: IMPROVING ONCOLOGY PATIENT OUTCOMES Pharmacologic and Nonpharmacologic Interventions for Pain Introduction A variety of treatments such as chemotherapy, radiation therapy,
Common Side Effects. Fatigue Neuropathy Hot flashes
 Common Side Effects Fatigue Neuropathy Hot flashes Fatigue According to the National Comprehensive Cancer Network (2017), cancer related fatigue is defined as a distressing, persistent, subjective sense
Common Side Effects Fatigue Neuropathy Hot flashes Fatigue According to the National Comprehensive Cancer Network (2017), cancer related fatigue is defined as a distressing, persistent, subjective sense
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Fatigue Bigorio Professor Paddy Stone
 Fatigue Bigorio 2013 Professor Paddy Stone Overview What is fatigue? How can fatigue be assessed? How can fatigue be treated? Guidelines? Fatigue is a subjective, unpleasant symptom which incorporates
Fatigue Bigorio 2013 Professor Paddy Stone Overview What is fatigue? How can fatigue be assessed? How can fatigue be treated? Guidelines? Fatigue is a subjective, unpleasant symptom which incorporates
SLEEP DISORDERS
 SLEEP DISORDERS 17.03.2013 Well this is a problem that is close to my heart, because for most of my life I have had problems sleeping. Many nights I have watched with envy as my husband goes to bed and
SLEEP DISORDERS 17.03.2013 Well this is a problem that is close to my heart, because for most of my life I have had problems sleeping. Many nights I have watched with envy as my husband goes to bed and
Cognitive Behavioral Therapy for Insomnia. Melanie K. Leggett, PhD, CBSM Duke University Medical Center
 Cognitive Behavioral Therapy for Insomnia Melanie K. Leggett, PhD, CBSM Duke University Medical Center Disclosures I have no relevant financial relationship with the manufacturers of any commercial products
Cognitive Behavioral Therapy for Insomnia Melanie K. Leggett, PhD, CBSM Duke University Medical Center Disclosures I have no relevant financial relationship with the manufacturers of any commercial products
PERFORMANCE AFTER HSCT Mutlu arat, md ıstanbul bilim un., dept. hematology ıstanbul, turkey
 PERFORMANCE AFTER HSCT Mutlu arat, md ıstanbul bilim un., dept. hematology ıstanbul, turkey Joint Educational Meeting of the EBMT Severe Aplastic Anaemia, Late Effects and Autoimmune Diseases Working Parties
PERFORMANCE AFTER HSCT Mutlu arat, md ıstanbul bilim un., dept. hematology ıstanbul, turkey Joint Educational Meeting of the EBMT Severe Aplastic Anaemia, Late Effects and Autoimmune Diseases Working Parties
Sue Johnson May Fatigue in Palliative Care
 Sue Johnson May 2017 Fatigue in Palliative Care Why fatigue? Palliative care patients identify fatigue as a significant symptom. Fatigue is one of the most complex symptoms experienced by cancer patients
Sue Johnson May 2017 Fatigue in Palliative Care Why fatigue? Palliative care patients identify fatigue as a significant symptom. Fatigue is one of the most complex symptoms experienced by cancer patients
Insomnia % of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences)
") 10-15% of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences) 30 40% of adults complain of insomnia symptoms only 95% experience insomnia at some time in their
10-15% of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences) 30 40% of adults complain of insomnia symptoms only 95% experience insomnia at some time in their
Biopsychosocial Characteristics of Somatoform Disorders
 Contemporary Psychiatric-Mental Health Nursing Chapter 19 Somatoform and Sleep Disorders Biopsychosocial Characteristics of Somatoform Disorders Unconscious transformation of emotions into physical symptoms
Contemporary Psychiatric-Mental Health Nursing Chapter 19 Somatoform and Sleep Disorders Biopsychosocial Characteristics of Somatoform Disorders Unconscious transformation of emotions into physical symptoms
Managing Sleep Problems after Cancer
 Managing Sleep Problems after Cancer For cancer survivors Read this resource to learn about: What a sleep problem is What causes it What you can do to improve your sleep When to talk to your doctor Please
Managing Sleep Problems after Cancer For cancer survivors Read this resource to learn about: What a sleep problem is What causes it What you can do to improve your sleep When to talk to your doctor Please
7 Secrets for Sweet Sleep. By Annie Barrett, M. A., Educator, Yoga Teacher, Health Coach
 7 Secrets for Sweet Sleep By Annie Barrett, M. A., Educator, Yoga Teacher, Health Coach Hi! I m Annie Barrett. As an educator, yogi and coach, I am a holistic wellness provider trained and practiced in
7 Secrets for Sweet Sleep By Annie Barrett, M. A., Educator, Yoga Teacher, Health Coach Hi! I m Annie Barrett. As an educator, yogi and coach, I am a holistic wellness provider trained and practiced in
Mind-Body Medicine: Enriching Well-being
 Mind-Body Medicine: Enriching Well-being Pamela G. Gebhardt, RN, MS, OCN Clinical Educator, UACC pamela.gebhardt@uahealth.com 520-694-0318 Monthly Educational Series-Promoting Good Health Educational Objectives
Mind-Body Medicine: Enriching Well-being Pamela G. Gebhardt, RN, MS, OCN Clinical Educator, UACC pamela.gebhardt@uahealth.com 520-694-0318 Monthly Educational Series-Promoting Good Health Educational Objectives
Appendix 2 (continued): Recommendations for the management of mild to moderate dementia, dementia with a cerebrovascular component, and for addressing
: Recommendations for the management of mild to moderate dementia, dementia with a cerebrovascular component, and for addressing") a cerebrovascular component, and for addressing ethical issues in dementia (page 1 of 7) Mild to moderate dementia 1. Most patients with dementia can be assessed and managed adequately by their primary
a cerebrovascular component, and for addressing ethical issues in dementia (page 1 of 7) Mild to moderate dementia 1. Most patients with dementia can be assessed and managed adequately by their primary
11. Psychopharmacological Intervention
 11. Psychopharmacological Intervention 11.1 Goals of Psychopharmacology The goal of psychopharmacology is to ensure that patients with more severe forms of depression and those who fail to benefit adequately
11. Psychopharmacological Intervention 11.1 Goals of Psychopharmacology The goal of psychopharmacology is to ensure that patients with more severe forms of depression and those who fail to benefit adequately