It costs you nothing, but gains everything for your patient!
|
|
|
- Daniella Fields
- 5 years ago
- Views:
Transcription


1 It costs you nothing, but gains everything for your patient!

2 Attend the entire presentation Complete and submit the evaluation This session is approved for: ANCC hours CECBEMS hours No partial credit will be awarded
3 Air Evac EMS Inc. believes that part of being a good corporate citizen is supporting the needs of the local communities in which it operates by providing outreach education as a general service. We do not discriminate against attendees all are welcome to attend. The fees we charge are to cover our cost, not to make money, so please accept this service and the information provided in the spirit intended. We have taken care to confirm the accuracy of the information presented, to describe how our company operates (including drug selection and dosage) and to describe generally accepted practices, as we know them. However, in view of ongoing research, changes in government regulation, the constant flow of information in the medical field and simple honest mistakes, the information we present may contain errors, problems or other limitations. Because providing this type of information is not our business, we cannot be responsible for errors or omissions or for any consequences from application of the information presented, and make no warranty, expressed or implied, with respect to the currency, completeness or accuracy of the information. Our presentations are for general information and education purposes, not medical or protocol advice. Application of information we provide in a particular situation remains the professional responsibility of the practitioner, and you should follow local standing orders and protocols established by your medical director and professional governing agency.
4 No influential financial relationships have been disclosed by planners or presenters which would influence the planning of this activity. No commercial support has influenced the planning of the educational objectives and content of this program. There is no endorsement of any product by CECBEMS or ANCC associated with the sessions. Appropriate use and off-label use of products governed by the FDA will be disclosed
5 The learner will be able to describe Apneic Oxygenation (AO) and its implications in Airway Management The learner will be able to demonstrate proper application of AO techniques in a simulated environment The learner will be able to describe the benefits of AO
6 The goal of any airway management episode is to maintain saturation of all available hemoglobin with oxygen to prevent a hypoxemic event. Secondary goals for the intubator is to prevent critical hypoxia and aspiration. The challenge in the emergency environment is to do this rapidly, without harm to the patient.
7 This short program will review and discuss the techniques associated with the preoxygenation and peri-intubation oxygenation phases of airway management.
8 Pre-oxygenation offers the patient a safe condition during airway management. It extends the duration of safe apnea during peri-intubation.
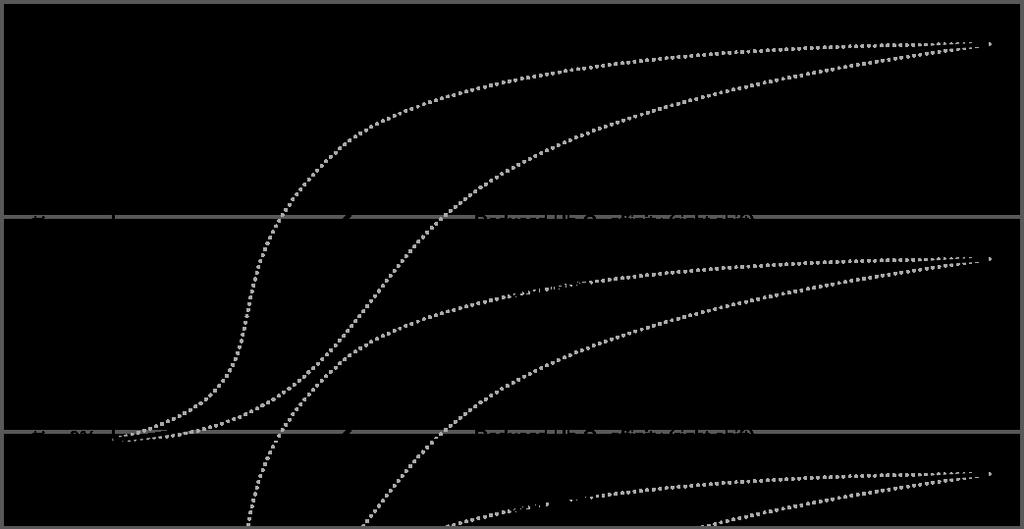
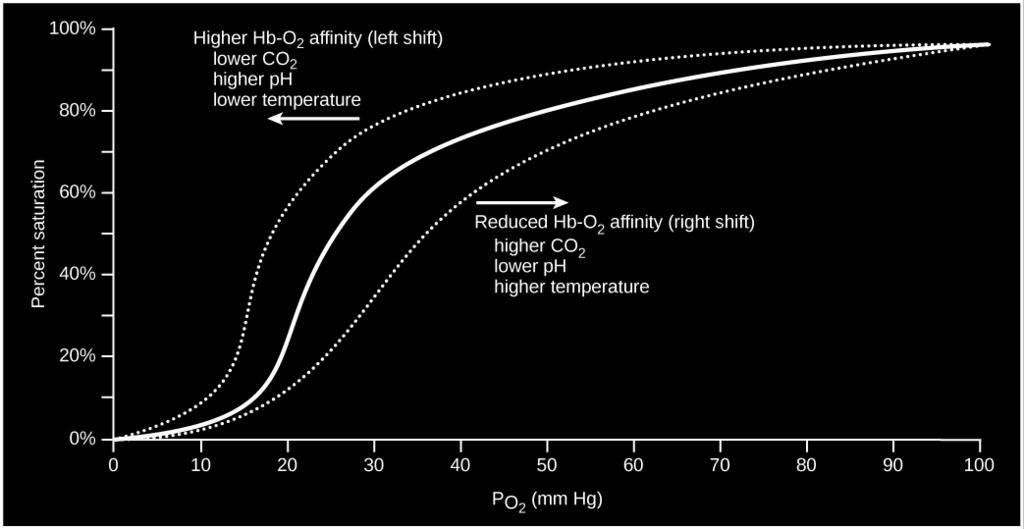
9 In the Emergency Environment, there are 3 goals of pre-oxygenation: 1. Increase the SPO2 to as close to 100% as possible 2. Denitrogenate the lungs which maximizes the patient s natural reservoir 3. Denitrogenate and maximally oxygenate the bloodstream Weingart and Levitan, 2012
10
11 95 91 >90

12 Frumin et al demonstrated in a 1958 research paper that man can sustain safe apnea times of minutes with adequate preoxygenation in the anesthesia environment. Not an anesthesia environment, but you get the point! Frumin, et. al. 1958

13 The challenge is not the time period for preoxygenation. Osborn, 2009; Mort, et. al. 2009

14 The challenge is to deliver a high FiO2 to your patient, to prevent hypoxia

15


16 Earl, 2003
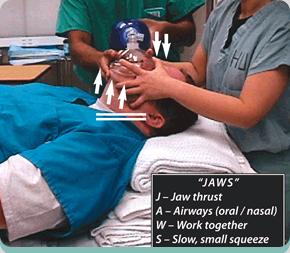
17 Some practitioners opt to utilize a selfinflating bag-valve-mask device to preoxygenate patients.

18 2 person technique is preferred Downside to BVM use- gastric insufflation which increases the risk of vomiting and aspiration. Upside to BVM use- useful for the apneic patient who requires assistance.
19
20 Scenario - Let s assume that your patient has no respiratory disease or shunting. This may be the isolated head injury who is unable to protect their airway, but is spontaneously breathing. How do we manage apneic oxygenation for this patient?


21 The typical approach to apneic oxygenation is to apply a nasal cannula at 6 L/min, then a non-rebreather mask at 15 L/min.

22
23 Allow the patient to breath spontaneously for 3 minutes or 8 maximal vital breaths. Once apnea has been achieved and prior to intubation: 1. increase the nasal cannula flow to at least 15 L/min (near 100% FiO2) NO DESAT! 2. remove mask, but leave nasal cannula in place 3. allow for paralysis to take place then intubate and confirm 4. remove cannula once oxygen therapy has been initiated via airway device

24

25 Why leave the cannula in place for an apneic patient? Levitan, 2013
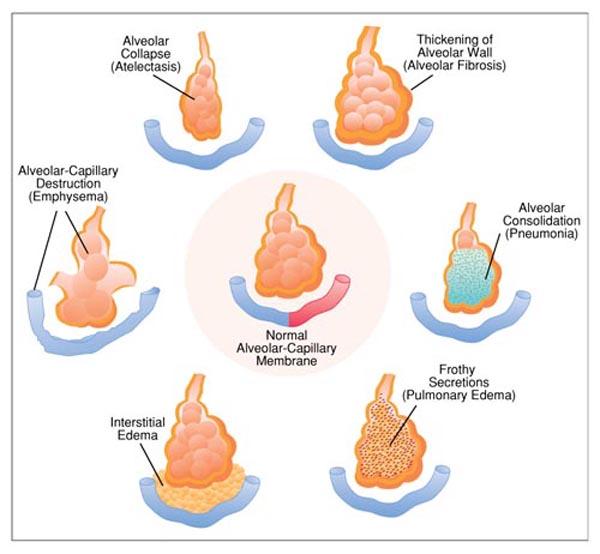
26 What if the patient is unable to be preoxygenated above 93%? Suspect some type of shunt physiology Examples: Obesity Pneumonia Pulmonary Edema
27


28 One of the first maneuvers is to augment the pressure at the alveolar level. Can easily be done by adding a disposable PEEP valve to your BVM for the patient that requires assistance.
29 For the patient who is still breathing but requires PEEP during the preoxygenation phase due to shunting: Non-invasive positive pressure can be applied Note- in critically ill adults with high degrees of shunting, apneic oxygenation may not be helpful without using PEEP and/or positive pressure ventilation.

30

31
32 Supine positioning is not ideal: Difficulty in maximizing ventilations Posterior aspect of lung becomes prone to atelectatic collapse Leads to a reduction in safe apnea time Positioning may be difficult in trauma patients with spinal protection in place. Lane, et. al (2005); Altermatt, et. al. (2005)
; Ramkumar, et al. (2011)")
33 Unless contraindicated, all patients require the head of the bed to be elevated for preoxygenation to at least 20 degrees. Lane, et. al (2005); Ramkumar, et al. (2011)

34 What about the trauma patient that can t have the HOB raised? Reverse Trendelenburg at 30 degrees is effective for the preoxygenation phase.
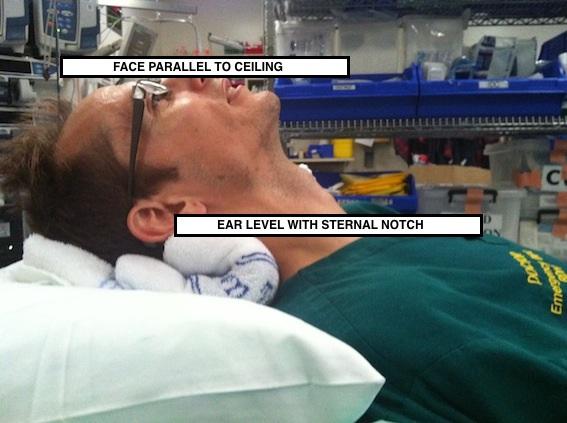
35 One requirement for proper positioning EAR to STERNAL NOTCH positioning Sniffing position Maintain patency of the airway Improves the mechanics of ventilation Lengthens the apneic time period to critical hypoxia Improves direct laryngoscope views

36

37
38

39

40 Leaving the patient flat is not an option! A proper ramping includes loads of linens and plenty of help to elevate the patient. Best to position the patient before laryngoscope attempts. Airwaycam.com
41 What is the primary benefit of Apneic Oxygenation? The creation of a reservoir of oxygen in the alveoli. Why are we concerned about the time to desaturate? ONE episode of hypoxia increases their mortality rate.
42 Benumof, 1999


43 Downside: Poor perfusion status leads to erroneous waveforms Practitioner ability to interpret Lag time seconds Only measures the amount of a gas bound to hemoglobin, it does not tell you which gas it is Useful Device Often called the 5 th Vital Sign Reliable when cardiac output is adequate
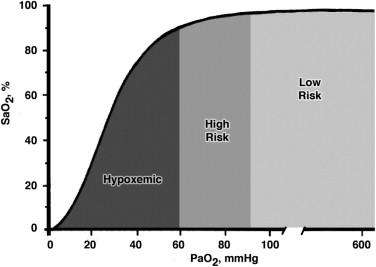
44 LOW RISK SPO % Preoxygenation Period Nonrebreather at 15 L/min Onset of Muscle Relaxant Nonrebreather mask and nasal cannula at 15 L/min Apneic period-no DESAT at 15 L/min Weingart and Levitan, 2012
45 HIGH RISK SPO2 91%-95% Preoxygenation Period-Nonrebreather mask, CPAP or bag-valve-mask device with PEEP. Onset of Muscle Relaxant-Nonrebreather mask, CPAP or bag-valve-mask with PEEP, and NO DESAT at 15 L/min. Apneic Period- NO DESAT at 15 L/min. Weingart and Levitan, 2012
46 HYPOXEMIC SPO2 90% or Less Preoxygenation Period-CPAP or bag-valve-mask device with PEEP. Onset of Muscle Relaxant-CPAP or bag-valve-mask with PEEP, and NO DESAT at 15 L/min. Apneic Period- NO DESAT at 15 L/min. Weingart and Levitan, 2012

47 Preoxygenation Period Weingart and Levitan, 2012
48 Apneic period Weingart and Levitan, 2012
49 Intubation Period Weingart and Levitan, 2012
50 Apneic Oxygenation is not new. Requires little equipment. Preoxygenation can take place in 3-4 min. Ramp all patients to proper position. Leave the cannula on during intubation- NO DESAT! You must recognize and compensate for shunting. The Benefits of AO outweigh any Risk!
51 Altermatt, F. R., Munoz, H. R., Delfine, A. E., et. al. (2005) Br J Anaesth. Pre-oxygenation in the obese patient: Effects of position on tolerance of apnoea. 95: Earl, J.W. (2003) The Science Journal of the American Association for Respiratory Care. Delivery of High FIO2. Abstract Frumin, M.J., et. al. (Nov-Dec 1959) Anesthesiology. Apneic Oxygenation in Man. pp Lane, S, Saunder, D., Shofield A, et. al. (2005) Anaesthesia. A prospective, randomized controlled trial comparing the efficacy of preoxygenation in the 20 degrees head-up vs. supine position. 60: Levitan, R. M. (2010) Emergency Physicians Monthly. NO DESAT!. Retrieved from on 7/15/2014 Mort, T.C., et. al. (2009) Crit Care Med. Extending the preoxygenation period from 4 to 8 mins in critically ill patients undergoing emergency intubation. Retrieved from act on 7/14/2014 Osborn, T. M. (2009) Emergency Medicine. Preoxygenation for Emergency intubation: Longer is not better. Retrieved from on 7/14/2014 Ramkumar, V., et. al. (2011) J Anesth. Preoxygenation with 20 head up tilt provides a longer duration of non-hypoxic apnea than conventional pre-oxygenation in non-obese healthy adults. 25: Weingart, S. D. & Levitan, R. M. (2012) Annals of Emergency Medicine. Preoxygenation and prevention of desaturation during emergency airway management. 59:3 pp
52 Please fill out the evaluation with your comments! If you have questions, please contact our Training Center at
Financial Disclosures. Goal. Overview. Pre-Oxygenation N 2 O 2. Pre-Oxygenation 3/20/2017. Optimizing Intubation. None
 Financial Disclosures None Optimizing Intubation Rahul Bhat, M.D. FACEP Associate Program Director Associate Professor of Emergency Medicine MedStar Georgetown University Hospital MedStar Washington Hospital
Financial Disclosures None Optimizing Intubation Rahul Bhat, M.D. FACEP Associate Program Director Associate Professor of Emergency Medicine MedStar Georgetown University Hospital MedStar Washington Hospital
@airwaycam airwaycam.com
 It s not just about the tube, its the VAPORS & Resuscitation Sequence Intubation What are our lives except a vapor that appears for a little while and vanishes and passes away? James 4:14 Ventilation Acidosis
It s not just about the tube, its the VAPORS & Resuscitation Sequence Intubation What are our lives except a vapor that appears for a little while and vanishes and passes away? James 4:14 Ventilation Acidosis
Tracheal Intubation in ICU: Life saving or life threatening?
 Tracheal Intubation in ICU: Life saving or life threatening? Prof. Sheila Nainan Myatra Department of Anaesthesia, Critical Care & Pain Tata Memorial Hospital Mumbai, India sheila150@hotmail.com Three
Tracheal Intubation in ICU: Life saving or life threatening? Prof. Sheila Nainan Myatra Department of Anaesthesia, Critical Care & Pain Tata Memorial Hospital Mumbai, India sheila150@hotmail.com Three
INTUBATION/RSI. PURPOSE: A. To facilitate secure, definitive control of the airway by endotracheal intubation in an expeditious and safe manner
 Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Manual: LifeLine Patient Care Protocols Section: Adult/Pediatrics Protocol #: AP1-009 Approval Date: 03/01/2018 Effective Date: 03/05/2018 Revision Due Date: 12/01/2018 INTUBATION/RSI PURPOSE: A. To facilitate
Epiglottoscopy, Positioning, The Neglected Orifice, & Passive Oxygenation
 Epiglottoscopy, Positioning, The Neglected Orifice, & Passive Oxygenation Richard M. Levitan, MD Jefferson Medical College Philadelphia PA EPIGLOTTIS: The Anatomic Center of the Airway Start to Finish
Epiglottoscopy, Positioning, The Neglected Orifice, & Passive Oxygenation Richard M. Levitan, MD Jefferson Medical College Philadelphia PA EPIGLOTTIS: The Anatomic Center of the Airway Start to Finish
Preoxygenation and Prevention of Desaturation During Emergency Airway Management
 AIRWAY/REVIEW ARTICLE Preoxygenation and Prevention of Desaturation During Emergency Airway Management Scott D. Weingart, MD, Richard M. Levitan, MD From the Division of Emergency Critical Care, Department
AIRWAY/REVIEW ARTICLE Preoxygenation and Prevention of Desaturation During Emergency Airway Management Scott D. Weingart, MD, Richard M. Levitan, MD From the Division of Emergency Critical Care, Department
yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management
 yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management Overview: Managing a patient s airway may be necessitated due to upper or lower airway obstruction, inadequate
yregion I EMERGENCY MEDICAL SERVICES STANDING MEDICAL ORDERS EMT Basic SMO: Airway Management Overview: Managing a patient s airway may be necessitated due to upper or lower airway obstruction, inadequate
Capnography. Capnography. Oxygenation. Pulmonary Physiology 4/15/2018. non invasive monitor for ventilation. Edward C. Adlesic, DMD.
 Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Capnography Edward C. Adlesic, DMD University of Pittsburgh School of Dental Medicine 2018 North Carolina Program Capnography non invasive monitor for ventilation measures end tidal CO2 early detection
Airway Management & Safety Concerns Experience from Bariatric Surgery
 Airway Management & Safety Concerns Experience from Bariatric Surgery Issues of the Obese Critical Care Patient - Airway Srikantha Rao MBBS MS Associate Professor Department of Anesthesia Aug 2010 Objectives
Airway Management & Safety Concerns Experience from Bariatric Surgery Issues of the Obese Critical Care Patient - Airway Srikantha Rao MBBS MS Associate Professor Department of Anesthesia Aug 2010 Objectives
MAKING RSI SAFER. Nick Taylor ETU THK 2015
 MAKING RSI SAFER Nick Taylor ETU THK 2015 GOALS 1. AIRWAY ASSESSMENT AND PLAN 2. MAXIMALLY PREOXYGENATE 3. HAEMODYNAMIC STABILITY PART 1 : AIRWAY ASSESSMENT AND PLAN LEMON: AIRWAY ASSESS AND PLAN Look
MAKING RSI SAFER Nick Taylor ETU THK 2015 GOALS 1. AIRWAY ASSESSMENT AND PLAN 2. MAXIMALLY PREOXYGENATE 3. HAEMODYNAMIC STABILITY PART 1 : AIRWAY ASSESSMENT AND PLAN LEMON: AIRWAY ASSESS AND PLAN Look
OWN THE AIRWAY. Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP. Paramedic Program
 OWN THE AIRWAY Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP The largest detriment to airway management has nothing to do with the patient, but everything to do with you as a provider. PRACTICE..PRACTICE.PRACTICE.
OWN THE AIRWAY Airway Management Bruce Barry, RN, CEN, CPEN, TCRN, NRP The largest detriment to airway management has nothing to do with the patient, but everything to do with you as a provider. PRACTICE..PRACTICE.PRACTICE.
Appendix D An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires:
 Answer Key Appendix D-2 1. An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires: a. oxygen given via nasal cannula b. immediate transport to a medical facility c.
Answer Key Appendix D-2 1. An unresponsive patient with shallow, gasping breaths at a rate of six per minute requires: a. oxygen given via nasal cannula b. immediate transport to a medical facility c.
Sleep Apnea and ifficulty in Extubation. Jean Louis BOURGAIN May 15, 2016
 Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
Sleep Apnea and ifficulty in Extubation Jean Louis BOURGAIN May 15, 2016 Introduction Repetitive collapse of the upper airway > sleep fragmentation, > hypoxemia, hypercapnia, > marked variations in intrathoracic
10/17/2016 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT COURSE OBJECTIVES COMMON CAUSES OF RESPIRATORY FAILURE
 OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
OXYGEN DELIVERY: INDICATIONS AND USE OF EQUIPMENT J U L I E Z I M M E R M A N, R N, M S N C L I N I C A L N U R S E S P E C I A L I S T E L O I S A C U T L E R, R R T, B S R C C L I N I C A L / E D U C
WSCC EMT CLASS SEVIERVILLE EXAM 1 STUDY GUIDE 1. Describe what is needed for good eye protection. Are prescription eye glasses adequate?
 1. Describe what is needed for good eye protection. Are prescription eye glasses adequate? 2. What kind of report must be given to officially transfer patient care at the hospital? 3. What is subcutaneous
1. Describe what is needed for good eye protection. Are prescription eye glasses adequate? 2. What kind of report must be given to officially transfer patient care at the hospital? 3. What is subcutaneous
Charisma High-flow CPAP solution
 Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Charisma High-flow CPAP solution Homecare PNEUMOLOGY Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support charisma High-flow CPAP solution Evidence CPAP therapy
Appendix E Choose the sign or symptom that best indicates severe respiratory distress.
 Appendix E-2 1. In Kansas EMT-B may monitor pulse oximetry: a. after they complete the EMT-B course b. when the service purchases the state approved pulse oximeters c. when the service director receives
Appendix E-2 1. In Kansas EMT-B may monitor pulse oximetry: a. after they complete the EMT-B course b. when the service purchases the state approved pulse oximeters c. when the service director receives
HeartCode PALS. PALS Actions Overview > Legend. Contents
 HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
HeartCode PALS PALS Actions Overview > Legend Action buttons (round buttons) Clicking a round button initiates an action. Clicking this button, for example, checks the child s carotid pulse. Menu buttons
STATE OF OKLAHOMA 2014 EMERGENCY MEDICAL SERVICES PROTOCOLS
 3K NON-INVASIVE POSITIVE PRESSURE VENTILATION (NIPPV) ADULT EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC Indications: 1. Dyspnea Uncertain Etiology Adult. 2. Dyspnea Asthma Adult. 3. Dyspnea Chronic
3K NON-INVASIVE POSITIVE PRESSURE VENTILATION (NIPPV) ADULT EMT EMT-INTERMEDIATE 85 ADVANCED EMT PARAMEDIC Indications: 1. Dyspnea Uncertain Etiology Adult. 2. Dyspnea Asthma Adult. 3. Dyspnea Chronic
Airway management. Gabriel Blecher
 Airway management Gabriel Blecher Richard Levitan 1: Weingart SD, Levitan RM. Preoxygenation and prevention of desaturation during emergency airway management. Ann Emerg Med. 2012 Mar;59(3):165-75.e1.
Airway management Gabriel Blecher Richard Levitan 1: Weingart SD, Levitan RM. Preoxygenation and prevention of desaturation during emergency airway management. Ann Emerg Med. 2012 Mar;59(3):165-75.e1.
ADVANCED AIRWAY MANAGEMENT
 The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
The Advanced Airway Management protocol should be used on all patients requiring advanced airway management procedures. This protocol is divided into three sections the Crash Airway Algorithm, the Rapid
Where Emergency Medicine Meets Critical Care: Next Level Resuscitation
 Where Emergency Medicine Meets Critical Care: Next Level Resuscitation Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin) Professor, Dalhousie University Departments of Emergency Medicine,Critical Care Medicine
Where Emergency Medicine Meets Critical Care: Next Level Resuscitation Rob Green, BSc, MD, DABEM, FRCPC, FRCP(Edin) Professor, Dalhousie University Departments of Emergency Medicine,Critical Care Medicine
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C
 Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
Advanced Airway Management PRESENTED BY: JOSIAH POIRIER RN, JOHN GRUBER FP-C Advanced Airway Objectives Advanced airway management is a relatively low frequency, high risk intervention. The following education
CONFLICT OF INTEREST NONE
 Airway Dr Albert Buchel MD CCFP EM CAC EM. Assistant Professor, Department of emergency medicine Program Director CCFP EM residency University of Manitoba CONFLICT OF INTEREST NONE AIRWAY TIPS PASSING
Airway Dr Albert Buchel MD CCFP EM CAC EM. Assistant Professor, Department of emergency medicine Program Director CCFP EM residency University of Manitoba CONFLICT OF INTEREST NONE AIRWAY TIPS PASSING
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit
 Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Information Often Given to the Nurse at the Time of Admission to the Postanesthesia Care Unit * Patient s name and age * Surgical procedure and type of anesthetic including drugs used * Other intraoperative
Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill
 Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill Matthew W. Semler, MD; David R. Janz, MD, MSc; Robert J. Lentz, MD; Daniel T. Matthews, MD; Brett C. Norman,
Randomized Trial of Apneic Oxygenation during Endotracheal Intubation of the Critically Ill Matthew W. Semler, MD; David R. Janz, MD, MSc; Robert J. Lentz, MD; Daniel T. Matthews, MD; Brett C. Norman,
Episode 110 Airway Pitfalls Live from EMU 2018
 Episode 110 Airway Pitfalls Live from EMU 2018 With Dr. Scott Weingart Prepared by Anton Helman, May 2018 The last decade has seen a torrent of literature and expert opinion on emergency airway management.
Episode 110 Airway Pitfalls Live from EMU 2018 With Dr. Scott Weingart Prepared by Anton Helman, May 2018 The last decade has seen a torrent of literature and expert opinion on emergency airway management.
Airway Management and The Difficult Airway
 Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
Airway Management and The Difficult Airway Gary McCalla, MD, FACEP Medical Director REACH Air Medical Services Services 1 It is not enough to do your best, unless you have prepared to be the best. -John
County of Santa Clara Emergency Medical Services System
 County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
County of Santa Clara Emergency Medical Services System Policy #700-M12: Continuous Positive Airway Pressure CONTINUOUS POSITIVE AIRWAY PRESSURE Effective: February 8, 2013TBD Replaces: NewFebruary 8,
Joint Theater Trauma System Clinical Practice Guideline
 Page 1 of 7 Joint Theater Trauma System Clinical Practice Guideline TRAUMA AIRWAY MANAGEMENT Original Release/Approval 18 Dec 2004 Note: This CPG requires an annual review. Reviewed: May 2012 Approved:
Page 1 of 7 Joint Theater Trauma System Clinical Practice Guideline TRAUMA AIRWAY MANAGEMENT Original Release/Approval 18 Dec 2004 Note: This CPG requires an annual review. Reviewed: May 2012 Approved:
Emergency Department/Trauma Adult Airway Management Protocol
 Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Emergency Department/Trauma Adult Airway Management Protocol Purpose: A standardized protocol for management of the airway in the setting of trauma in an academic center, with the goal of maximizing successful
Airway Management Adult
 Airway Management Adult Goals: Provide effective oxygenation and ventilation; recognize and alleviate respiratory distress or failure; provide necessary interventions quickly and safely to patients who
Airway Management Adult Goals: Provide effective oxygenation and ventilation; recognize and alleviate respiratory distress or failure; provide necessary interventions quickly and safely to patients who
By Mark Bachand, RRT-NPS, RPFT. I have no actual or potential conflict of interest in relation to this presentation.
 By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
By Mark Bachand, RRT-NPS, RPFT I have no actual or potential conflict of interest in relation to this presentation. Objectives Review state protocols regarding CPAP use. Touch on the different modes that
Study Of Effects Of Varying Durations Of Pre-Oxygenation. J Khandrani, A Modak, B Pachpande, G Walsinge, A Ghosh
 ISPUB.COM The Internet Journal of Anesthesiology Volume 20 Number 1 J Khandrani, A Modak, B Pachpande, G Walsinge, A Ghosh Citation J Khandrani, A Modak, B Pachpande, G Walsinge, A Ghosh.. The Internet
ISPUB.COM The Internet Journal of Anesthesiology Volume 20 Number 1 J Khandrani, A Modak, B Pachpande, G Walsinge, A Ghosh Citation J Khandrani, A Modak, B Pachpande, G Walsinge, A Ghosh.. The Internet
Learning Objectives. 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence
 Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
Learning Objectives 1. Indications versus contra-indications 2. CPAP versus NiVS 3. Clinical evidence Pre-hospital Non-invasive vventilatory support Marc Gillis, MD Imelda Bonheiden Our goal out there
What you need to know about: High flow nasal oxygen therapy
 What you need to know about: High flow nasal oxygen therapy Main introduction Adequate oxygenation is essential in many disorders, and this article will discuss the physiology, practicalities and indications
What you need to know about: High flow nasal oxygen therapy Main introduction Adequate oxygenation is essential in many disorders, and this article will discuss the physiology, practicalities and indications
EPO 2 Evaluation of the preoxygenation in! morbidly obese. Optimal position and ventilation mode!
 EPO 2 Evaluation of the preoxygenation in! morbidly obese. Optimal position and ventilation mode! Antony Carrier-Boucher! PGY 3 Anesthesiology! Laval University! None! Conflict of interest! 2. Anesth Analg
EPO 2 Evaluation of the preoxygenation in! morbidly obese. Optimal position and ventilation mode! Antony Carrier-Boucher! PGY 3 Anesthesiology! Laval University! None! Conflict of interest! 2. Anesth Analg
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Care Unit (FELLOW)
") Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
Facilitating EndotracheaL Intubation by Laryngoscopy technique and Apneic Oxygenation Within the Intensive Data Analysis Plan: Apneic Oxygenation vs. No Apneic Oxygenation Background Critically ill patients
NON INVASIVE LIFE SAVERS. Non Invasive Ventilation (NIV)
") Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
Table 1. NIV: Mechanisms Of Action Decreases work of breathing Increases functional residual capacity Recruits collapsed alveoli Improves respiratory gas exchange Reverses hypoventilation Maintains upper
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014
 Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Capnography for Pediatric Procedural Sedation Learning Module Last revised: February 18, 2014 Capnography 40 Non-invasive device that continually monitors EtCO 2 While pulse oximetry measures oxygen saturation,
Capnography Connections Guide
 Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
Capnography Connections Guide Patient Monitoring Contents I Section 1: Capnography Introduction...1 I Section 2: Capnography & PCA...3 I Section 3: Capnography & Critical Care...7 I Section 4: Capnography
SEMINOLE COUNTY EMS PROVISIONAL EMT SKILLS VERIFICATION
 The following individual has completed the Seminole County EMS Provisional EMT Skills Verification check in the following areas: Oxygen, Airway and Ventilation Skills ALS Assistance Trauma Management Medical
The following individual has completed the Seminole County EMS Provisional EMT Skills Verification check in the following areas: Oxygen, Airway and Ventilation Skills ALS Assistance Trauma Management Medical
Exclusion Criteria 1. Operator or supervisor feels specific intra- procedural laryngoscopy device will be required.
 FELLOW Study Data Analysis Plan Direct Laryngoscopy vs Video Laryngoscopy Background Respiratory failure requiring endotracheal intubation occurs in as many as 40% of critically ill patients. Procedural
FELLOW Study Data Analysis Plan Direct Laryngoscopy vs Video Laryngoscopy Background Respiratory failure requiring endotracheal intubation occurs in as many as 40% of critically ill patients. Procedural
Indications for Respiratory Assistance. Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer
 Indications for Respiratory Assistance Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer Respiratory Assistance Non-invasive - Nasal specs - Facemask/ Resevoir
Indications for Respiratory Assistance Sheba Medical Center, ICU Department Nick D Ardenne St George s University of London Tel Hashomer Respiratory Assistance Non-invasive - Nasal specs - Facemask/ Resevoir
NI 60. Non-invasive ventilation without compromise. Homecare Pneumology Neonatology Anaesthesia. Sleep Diagnostics Service Patient Support
 NI 60 Non-invasive ventilation without compromise Homecare Pneumology Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support NI 60 Non-invasive ventilation without
NI 60 Non-invasive ventilation without compromise Homecare Pneumology Neonatology Anaesthesia INTENSIVE CARE VENTILATION Sleep Diagnostics Service Patient Support NI 60 Non-invasive ventilation without
Competency Title: Continuous Positive Airway Pressure
 Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
Competency Title: Continuous Positive Airway Pressure Trainee Name: ------------------------------------------------------------- Title: ---------------------------------------------------------------
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device
 I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
I. Subject: Continuous Positive Airway Pressure CPAP by Continuous Flow Device II. Policy: Continuous Positive Airway Pressure CPAP by the Down's system will be instituted by Respiratory Therapy personnel
Tissue Hypoxia and Oxygen Therapy
 Tissue Hypoxia and Oxygen Therapy ก ก ก ก ก ก 1. ก ก 2. ก ก 3. tissue hypoxia 4. ก ก ก 5. ก ก ก 6. ก กก ก 7. ก ก tissue hypoxia ก ก ก ก 1. Pathway of oxygen transport 2. Causes of tissue hypoxia 3. Effect
Tissue Hypoxia and Oxygen Therapy ก ก ก ก ก ก 1. ก ก 2. ก ก 3. tissue hypoxia 4. ก ก ก 5. ก ก ก 6. ก กก ก 7. ก ก tissue hypoxia ก ก ก ก 1. Pathway of oxygen transport 2. Causes of tissue hypoxia 3. Effect
Naloxone Intranasal EMT OPTIONAL SKILL. Cell Phones and Pagers. Course Outline 09/2017
 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and Overview
EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and Overview
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist
 Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
Julie Zimmerman, MSN, RN, CCRN Clinical Nurse Specialist Objectives Define capnography vs. end tidal CO2 (EtCO 2 ) Identify what normal vs. abnormal EtCO2 values mean and what to do Understand when to
Subspecialty Rotation: Anesthesia
 Subspecialty Rotation: Anesthesia Faculty: John Heaton, M.D. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation. Recognize and manage upper
Subspecialty Rotation: Anesthesia Faculty: John Heaton, M.D. GOAL: Maintenance of Airway Patency and Oxygenation. Recognize and manage upper airway obstruction and desaturation. Recognize and manage upper
ARTICLE IN PRESS. doi: /j.jemermed PREOXYGENATION, REOXYGENATION, AND DELAYED SEQUENCE INTUBATION IN THE EMERGENCY DEPARTMENT
 doi:10.1016/j.jemermed.2010.02.014 The Journal of Emergency Medicine, Vol. xx, No. x, pp. xxx, 2010 Copyright 2010 Elsevier Inc. Printed in the USA. All rights reserved 0736-4679/10 $ see front matter
doi:10.1016/j.jemermed.2010.02.014 The Journal of Emergency Medicine, Vol. xx, No. x, pp. xxx, 2010 Copyright 2010 Elsevier Inc. Printed in the USA. All rights reserved 0736-4679/10 $ see front matter
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Airway Management in the Multiply Traumatized Patient
 Airway Management in the Multiply Traumatized Patient Toronto Anesthesia Symposium April 18, 2015 Dr. Jeffrey Wassermann Department of Anesthesia St. Michael s Hospital University of Toronto Airway Management
Airway Management in the Multiply Traumatized Patient Toronto Anesthesia Symposium April 18, 2015 Dr. Jeffrey Wassermann Department of Anesthesia St. Michael s Hospital University of Toronto Airway Management
Advanced Airway Management. University of Colorado Medical School Rural Track
 Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
Advanced Airway Management University of Colorado Medical School Rural Track Advanced Airway Management Basic Airway Management Airway Suctioning Oxygen Delivery Methods Laryngeal Mask Airway ET Intubation
POINT Peri-Operative Insufflatory Nasal Therapy
 PINT Peri-perative Insufflatory Nasal Therapy by Armstrong Medical Helping prevent peri-operative pulmonary complications PST-P RECVERY PERATING RMS Hypoxia; a peri-operative risk Pulmonary complications
PINT Peri-perative Insufflatory Nasal Therapy by Armstrong Medical Helping prevent peri-operative pulmonary complications PST-P RECVERY PERATING RMS Hypoxia; a peri-operative risk Pulmonary complications
PROCEDURE (TASK): CONTINUOUS DISTENDING PRESSURE THERAPY (CPAP) (NEONATAL/PEDIATRICS)
: CONTINUOUS DISTENDING PRESSURE THERAPY (CPAP) (NEONATAL/PEDIATRICS)") PROCEDURE (TASK): CONTINUOUS DISTENDING PRESSURE THERAPY (CPAP) (NEONATAL/PEDIATRICS) I. KEY PERFORMANCE ELEMENTS Procedural Element (Step): Description of Satisfactory Performance: 5. Obtains baseline
PROCEDURE (TASK): CONTINUOUS DISTENDING PRESSURE THERAPY (CPAP) (NEONATAL/PEDIATRICS) I. KEY PERFORMANCE ELEMENTS Procedural Element (Step): Description of Satisfactory Performance: 5. Obtains baseline
Transnasal Humidified Rapid Insufflation Ventilatory Exchange (THRIVE): An Optimal Method of Preoxygenation for General Anaesthesia in Obstetrics
: An Optimal Method of Preoxygenation for General Anaesthesia in Obstetrics") Transnasal Humidified Rapid Insufflation Ventilatory Exchange (THRIVE): An Optimal Method of Preoxygenation for General Anaesthesia in Obstetrics Dr E McMaster, Dr E Gent, Dr T Mahendrayogam, Dr A Surendran
Transnasal Humidified Rapid Insufflation Ventilatory Exchange (THRIVE): An Optimal Method of Preoxygenation for General Anaesthesia in Obstetrics Dr E McMaster, Dr E Gent, Dr T Mahendrayogam, Dr A Surendran
Apneic oxygenation during prolonged laryngoscopy in obese patients: a randomized, controlled trial of nasal oxygen administration
 Journal of Clinical Anesthesia (2010) 22, 164 168 Original contribution Apneic oxygenation during prolonged laryngoscopy in obese patients: a randomized, controlled trial of nasal oxygen administration
Journal of Clinical Anesthesia (2010) 22, 164 168 Original contribution Apneic oxygenation during prolonged laryngoscopy in obese patients: a randomized, controlled trial of nasal oxygen administration
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Inselspital Universitätsklinik für Anästhesiologie und Schmerztherapie. 73. Berner Anästhesie-Symposium Mittwoch, 15. November 2017 Kinderanästhesie
 Inselspital Universitätsklinik für Anästhesiologie und Schmerztherapie 73. Berner Anästhesie-Symposium Mittwoch, 15. November 2017 Kinderanästhesie HFNC Von Spontanatmung bis zur apnoischen Oxygenierung
Inselspital Universitätsklinik für Anästhesiologie und Schmerztherapie 73. Berner Anästhesie-Symposium Mittwoch, 15. November 2017 Kinderanästhesie HFNC Von Spontanatmung bis zur apnoischen Oxygenierung
² C Y E N G R E M E ssignac Cardiac Arrest Resuscitation Device uob
 E M E R G E N C Y Boussignac Cardiac Arrest Resuscitation Device ² What is b-card? b-card Boussignac Cardiac Arrest Resuscitation Device has been designed specifically for the treatment of cardiac arrest.
E M E R G E N C Y Boussignac Cardiac Arrest Resuscitation Device ² What is b-card? b-card Boussignac Cardiac Arrest Resuscitation Device has been designed specifically for the treatment of cardiac arrest.
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery. By: Lillian Han
 Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Respiratory Anesthetic Emergencies in Oral and Maxillofacial Surgery By: Lillian Han Background: Respiratory anesthetic emergencies are the most common complications during the administration of anesthesia
Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off.
 1 2 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. 3 4 5 6 Course Outline Introduction
1 2 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. 3 4 5 6 Course Outline Introduction
Chapter 10. Objectives. Objectives 01/09/2013. Airway Management, Artificial Ventilation, and Oxygenation
 Chapter 10 Airway Management, Artificial Ventilation, and Oxygenation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
Chapter 10 Airway Management, Artificial Ventilation, and Oxygenation Prehospital Emergency Care, Ninth Edition Joseph J. Mistovich Keith J. Karren Copyright 2010 by Pearson Education, Inc. All rights
I. Subject: Pressure Support Ventilation (PSV) with BiPAP Device/Nasal CPAP
 with BiPAP Device/Nasal CPAP") I. Subject: Pressure Support Ventilation (PSV) with BiPAP Device/Nasal CPAP II. Policy: PSV with BiPAP device/nasal CPAP will be initiated upon a physician's order by Respiratory Therapy personnel trained
I. Subject: Pressure Support Ventilation (PSV) with BiPAP Device/Nasal CPAP II. Policy: PSV with BiPAP device/nasal CPAP will be initiated upon a physician's order by Respiratory Therapy personnel trained
Oxygen: Is there a problem? Tom Heaps Acute Physician
 Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
How it Works. CO 2 is the smoke from the flames of metabolism 10/21/18. -Ray Fowler, MD. Metabolism creates ETC0 2 for excretion
 CO 2 is the smoke from the flames of metabolism -Ray Fowler, MD How it Works Metabolism creates ETC0 2 for excretion ETC02 and Oxygen are exchanged at the alveolar level in the lungs with each breath.
CO 2 is the smoke from the flames of metabolism -Ray Fowler, MD How it Works Metabolism creates ETC0 2 for excretion ETC02 and Oxygen are exchanged at the alveolar level in the lungs with each breath.
Critical Care Monitoring. Assessing the Adequacy of Tissue Oxygenation. Tissue Oxygenation - Step 1. Tissue Oxygenation
 Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Critical Care Monitoring 1 Assessing the Adequacy of Tissue oxygenation is the end-product of many complex steps 2 - Step 1 Oxygen must be made available to alveoli 3 1 - Step 2 Oxygen must cross the alveolarcapillary
Module 2: Facilitator instructions for Airway & Breathing Skills Station
 Module 2: Facilitator instructions for Airway & Breathing Skills Station 1. Preparation a. Assemble equipment beforehand. b. Make sure that you have what you need and that it is functioning properly. 2.
Module 2: Facilitator instructions for Airway & Breathing Skills Station 1. Preparation a. Assemble equipment beforehand. b. Make sure that you have what you need and that it is functioning properly. 2.
Scenario title. Pear Shaped- prepare for intubation on the ward. Designed for (specific group) ICU MET team. Scenario Design team.
 ICU MET team. Scenario Design team.") Scenario title Pear Shaped- prepare for intubation on the ward Designed for (specific group) ICU MET team Scenario Design team Name Maurice Le Guen Cameron Knott Organisation Austin Hospital Date of creation
Scenario title Pear Shaped- prepare for intubation on the ward Designed for (specific group) ICU MET team Scenario Design team Name Maurice Le Guen Cameron Knott Organisation Austin Hospital Date of creation
Simulation 3: Post-term Baby in Labor and Delivery
 Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
Simulation 3: Post-term Baby in Labor and Delivery Opening Scenario (Links to Section 1) You are an evening-shift respiratory therapist in a large hospital with a level III neonatal unit. You are paged
NON-INVASIVE VENTILATION. Lijun Ding 23 Jan 2018
 NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
NON-INVASIVE VENTILATION Lijun Ding 23 Jan 2018 Learning objectives What is NIV The difference between CPAP and BiPAP The indication of the use of NIV Complication of NIV application Patient monitoring
CPAP. Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device. Charlottesville Albemarle Rescue Squad - CPAP
 CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
CPAP Pre-Hospital Treatment Using The Respironics Whisperflow CPAP Device CPAP What Is It? C ontinuous P ositive A irway P ressure Anatomy Review Anatomy Review Anatomy Review Alveoli Anatomy Review Chest
Respiratory Failure in the Pediatric Patient
 Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
Respiratory Failure in the Pediatric Patient Ndidi Musa M.D. Associate Professor of Pediatrics Medical College of Wisconsin Pediatric Cardiac Intensivist Children s Hospital of Wisconsin Objectives Recognize
How to Predict and Avoid Airway Disasters. Muhammad Umer Ihsan
 How to Predict and Avoid Airway Disasters Muhammad Umer Ihsan Four Key Aspect of Assessing a Difficult Airway Difficult Bag Mask Ventilation Difficult Direct Laryngoscopy Difficult Extra-glottic devices
How to Predict and Avoid Airway Disasters Muhammad Umer Ihsan Four Key Aspect of Assessing a Difficult Airway Difficult Bag Mask Ventilation Difficult Direct Laryngoscopy Difficult Extra-glottic devices
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
No Excellence Without Evidence: The Therapeutic Use of Oxygen
 No Excellence Without Evidence: The Therapeutic Use of Oxygen Penelope S. Benedik PhD, CRNA, RRT Associate Professor of Clinical Nursing UTHealth Houston, Texas Oxygen is a DRUG Oxygen overuse is toxic
No Excellence Without Evidence: The Therapeutic Use of Oxygen Penelope S. Benedik PhD, CRNA, RRT Associate Professor of Clinical Nursing UTHealth Houston, Texas Oxygen is a DRUG Oxygen overuse is toxic
Maintenance of oxygenation during airway
 Apneic Oxygenation: A Method to Prolong the Period of Safe Apnea Matt Pratt, MBA, BSN, BAAS, EMT-P Ann B. Miller, DNP, CRNA, ARNP A difficult intubation poses one of the most challenging tasks for professionals,
Apneic Oxygenation: A Method to Prolong the Period of Safe Apnea Matt Pratt, MBA, BSN, BAAS, EMT-P Ann B. Miller, DNP, CRNA, ARNP A difficult intubation poses one of the most challenging tasks for professionals,
Training. Continuous Positive Airway Pressure (CPAP)
") Training The training module will follow the national standard curriculum as it relates to the application and use of CPAP. The proposed curriculum will closely resemble the following algorithm utilizing
Training The training module will follow the national standard curriculum as it relates to the application and use of CPAP. The proposed curriculum will closely resemble the following algorithm utilizing
Non-invasive Ventilation protocol For COPD
 NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
Prior to applying a nonrebreathing mask on a patient with difficulty breathing, you should:!
 An elderly woman with COPD presents with a decreased level of consciousness, cyanosis to her face and neck, and labored respirations. Her pulse is rapid and weak and her oxygen saturation is 76%. You should:
An elderly woman with COPD presents with a decreased level of consciousness, cyanosis to her face and neck, and labored respirations. Her pulse is rapid and weak and her oxygen saturation is 76%. You should:
Joint Trauma System. Airway Trauma Injury Management
 Joint Trauma System Airway Trauma Injury Management 1 Agenda Contributors Purpose Summary Key Principles of CPG Performance Improvement (PI) Monitoring References List of Appendices in CPG 2 Contributors
Joint Trauma System Airway Trauma Injury Management 1 Agenda Contributors Purpose Summary Key Principles of CPG Performance Improvement (PI) Monitoring References List of Appendices in CPG 2 Contributors
Accident and Emergency Medicine Academic Unit, The Chinese University of Hong Kong, Shatin, Hong Kong
 Clin Exp Emerg Med 2015;2(3):174-178 http://dx.doi.org/10.15441/ceem.15.048 Effects of an elevated position on time to tracheal intubation by novice intubators using Macintosh laryngoscopy or videolaryngoscopy:
Clin Exp Emerg Med 2015;2(3):174-178 http://dx.doi.org/10.15441/ceem.15.048 Effects of an elevated position on time to tracheal intubation by novice intubators using Macintosh laryngoscopy or videolaryngoscopy:
Other methods for maintaining the airway (not definitive airway as still unprotected):
:") Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Page 56 Where anaesthetic skills and drugs are available, endotracheal intubation is the preferred method of securing a definitive airway. This technique comprises: rapid sequence induction of anaesthesia
Causes and Consequences of Respiratory Centre Depression and Hypoventilation
 Causes and Consequences of Respiratory Centre Depression and Hypoventilation Lou Irving Director Respiratory and Sleep Medicine, RMH louis.irving@mh.org.au Capacity of the Respiratory System At rest During
Causes and Consequences of Respiratory Centre Depression and Hypoventilation Lou Irving Director Respiratory and Sleep Medicine, RMH louis.irving@mh.org.au Capacity of the Respiratory System At rest During
Oxygen and Oxygen Equipment
 Oxygen and Oxygen Equipment Policy Number: Original Effective Date: MM.01.008 12/01/2010 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 09/01/2013 Section: DME Place(s) of Service: Home I.
Oxygen and Oxygen Equipment Policy Number: Original Effective Date: MM.01.008 12/01/2010 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST 09/01/2013 Section: DME Place(s) of Service: Home I.
April 2009 Site Code #107200E-1209 The Patient with Dyspnea
 April 2009 Site Code #107200E-1209 The Patient with Dyspnea Prepared by: Bill Hoover, Medical Officer, Wauconda Fire Department Review/revisions by: Sharon Hopkins, RN, BSN, EMT-P To view on the website
April 2009 Site Code #107200E-1209 The Patient with Dyspnea Prepared by: Bill Hoover, Medical Officer, Wauconda Fire Department Review/revisions by: Sharon Hopkins, RN, BSN, EMT-P To view on the website
Provide guidelines for the management of mechanical ventilation in infants <34 weeks gestation.
 Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Page 1 of 5 PURPOSE: Provide guidelines for the management of mechanical ventilation in infants
Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo
 Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Instant dowload and all chapters Test Bank Pilbeam's Mechanical Ventilation Physiological and Clinical Applications 6th Edition Cairo https://testbanklab.com/download/test-bank-pilbeams-mechanical-ventilation-physiologicalclinical-applications-6th-edition-cairo/
Sux Rocs and Roc Suks? Succinocholyne Vs Rocuronium in RSI
 Sux Rocs and Roc Suks? Succinocholyne Vs Rocuronium in RSI Immediately declare a conflict of interest: I am in love with Succinocholyne It 'was a love at first sight. I use it often and, in my clinical
Sux Rocs and Roc Suks? Succinocholyne Vs Rocuronium in RSI Immediately declare a conflict of interest: I am in love with Succinocholyne It 'was a love at first sight. I use it often and, in my clinical
OXYGENATION AND ACID- BASE EVALUATION. Chapter 1
 OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
OXYGENATION AND ACID- BASE EVALUATION Chapter 1 MECHANICAL VENTILATION Used when patients are unable to sustain the level of ventilation necessary to maintain the gas exchange functions Artificial support
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Pearls and Pitfalls of Rapid Sequence Intubation
 Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/pearls-and-pitfalls-of-rapid-sequenceintubation/3829/
Transcript Details This is a transcript of an educational program accessible on the ReachMD network. Details about the program and additional media formats for the program are accessible by visiting: https://reachmd.com/programs/clinicians-roundtable/pearls-and-pitfalls-of-rapid-sequenceintubation/3829/
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients CASE REPORT FORM
 INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM Centre ID number: Patient
INternational observational study To Understand the impact and BEst practices of airway management in critically ill patients Study acronym identifier: INTUBE CASE REPORT FORM Centre ID number: Patient
THRIVE. Dr. med. Alistair McNarry, Consultant anaesthetist, Western General Hospital, Edinburgh (UK)
") Seite 1 von 5 THRIVE Dr. med. Alistair McNarry, Consultant anaesthetist, Western General Hospital, Edinburgh (UK) althegasman@btinternet.com I have been a consultant anaesthetist working in Edinburgh for
Seite 1 von 5 THRIVE Dr. med. Alistair McNarry, Consultant anaesthetist, Western General Hospital, Edinburgh (UK) althegasman@btinternet.com I have been a consultant anaesthetist working in Edinburgh for
Capnography (ILS/ALS)
") Capnography (ILS/ALS) Clinical Indications: 1. Capnography shall be used as soon as possible in conjunction with any airway management adjunct, including endotracheal, Blind Insertion Airway Devices (BIAD)
Capnography (ILS/ALS) Clinical Indications: 1. Capnography shall be used as soon as possible in conjunction with any airway management adjunct, including endotracheal, Blind Insertion Airway Devices (BIAD)