Drunk When You re Not A 67 year old male presents with feeling off balance
|
|
|
- Arlene Sophia Holt
- 5 years ago
- Views:
Transcription
1 Drunk When You re Not A 67 year old male presents with feeling off balance Kiera McElrone, DO Internal Medicine/Pediatrics Residency Maine Medical Center September 2017 ACP Bar Harbor Meeting
2 Chief Complaint NOVEMBER 2015 Telephone call to primary care office. 67 year old has been feeling off balance for awhile but starting to feels worse. When he walks, he feels like he is drunk.
3 History of Present Illness NOVEMBER 2015 Balance and coordination issues since 2013 after right hip surgery Plays tennis and cannot swing well Multiple falls Occasional slurred speech Developed nighttime urinary incontinence (normal prostate exam in May 2015)
4 Past Medical History Past Medical History Rheumatoid Arthritis REM Sleep Disorder- since around 2011 Erectile Dysfunction: diagnosed in 2014 Obesity Degenerative Joint Disease Past Surgical History Right hip replacement in 2013 with difficult intubation
5 Past Medical History Family History Cardiovascular Disease: Myocardial Infarctions (brother and mother), Type 2 Diabetes (brother) No neurological, autoimmune family history Social History Married with 3 adult children Small business owner 1-2 glasses of wine nightly, no smoking
6 Physical Exam Vitals: General: NAD HEENT: mmm Cardiac: RRR, no murmurs Lungs: CTAB Abdomen: obese, NT, ND Extremities: without atrophy Neurologic: CN 2-12 intact, but with mild dysarthria. No word finding difficulties. No tremor with rest, action, or posture. Rocks to stand. 5/5 upper and lower extremity strength Negative Romberg. Finger to nose, heel to shin with mild right>left dysmetria bilaterally. Gait: slightly wide base, decreased arm swing bilaterally, stooped posture Medications: sildenafil, plaquenil
7 Investigations Labs B 12, TSH, CPK all WNL
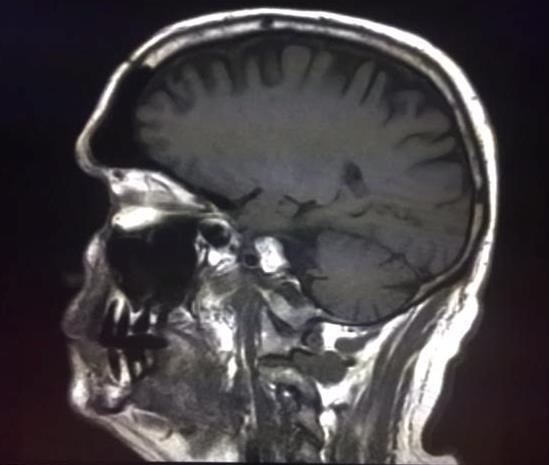
8 MRI 11/15 Investigations
9 Investigations JANUARY 2016: NEUROLOGY CONSULT Additional Clinical Information: Decreased Blink Frequency EMG: normal Referral to Movement Disorders Clinic
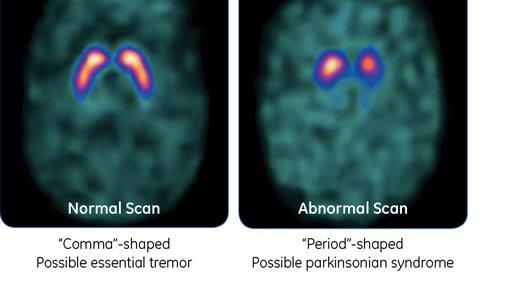
10 Investigations DaT- SPECT scan (Dopamine Transport Imaging with Single-Photon Emission Computed Tomography) Radioligands attach to the dopamine transporter (DaT), a protein on the presynaptic membrane which serves as a portal for dopamine update. Detects abnormal signal update in the striatum in patients with PD and other disease with nigrostriatal deficits
11 Investigations

12 DaT Scan- June 2016 Abnormal size, shape and activity both basal ganglia. Prominent decreased activity both putamen. Moderate decreased activity both caudate nuclei

13
14 Differential Diagnosis Parkinson s Disease Motor Neuron Disease Atypical Parkinson s Multiple System Atrophy Lewy Body Dementia
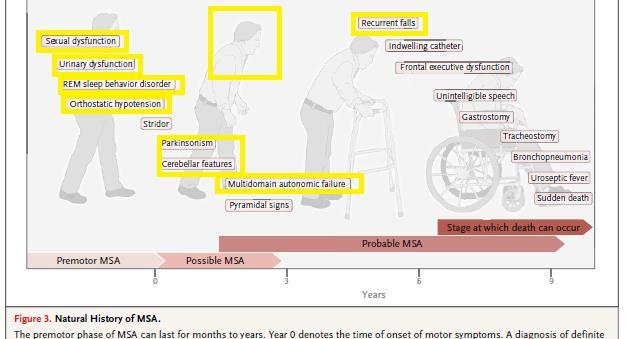
15 Clinical Update MAY 2017 Sudden leg weakness Unable to get out of bed Orthostatic, with standing SBP 70 Now choking with meals Started on fludrocortisone
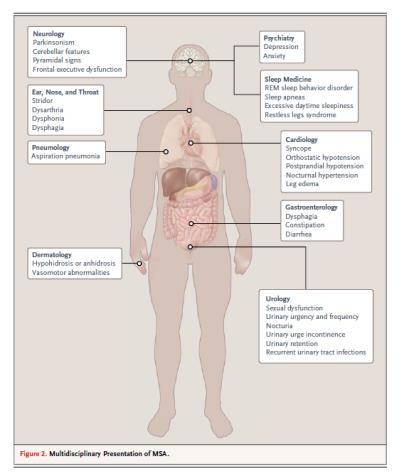
16 Multiple System Atrophy Progressive fatal neurodegenerative disease characterized by Progressive autonomic failure Parkinsonian features Cerebellar and Pyramidal Features Major diagnostic challenge with relevance in: Cardiology GI ENT Urology Sleep Medicine
17 History 1969: combined three neurologic entities: Olivopontocerebellar atrophy Shy-Drager syndrome Striatonigral degeneration
18 Diagnosis Definite MSA Postmortem Diagnosis Alpha synuclein positive glial cytoplasmic inclusions Neurodegenerative changes in striatonigral or olivopontocerebellar region Probable Sporadic, progressive disease in adults after 30 yr characterized by autonomic failure, including urinary incontinence (with ED in men), or an orthostatic hypotension plus either Parkinsonian or cerebellar features
19 Epidemiology Rare orphan disease Incidence : 100,000 Prevalence: : 100,000 2 forms MSA- P: Parkinsonian features, more common in North America and Europe MSA- C: cerebellar features, more common in Japan Disease Onset: usually sixth decade with both sexes affected equally Survival: 6-10 years
20 Causes Unknown Sporadic Some families genetics Loss of function mutation COQ2 in some Japanese and sporadic cases Loss of copy number of SHC 2 in monozygotic twins and Japanese patients with sporadic MSA Mutations, duplications, and triplications of SNCA may cause Parkinson s disease with features similar to MSA
21 Neuropathological Features Variable degrees of olivopontocerebellar atrophy cerebellar syndrome striatonigral degeneration poorly levodopa responsive parkinsonism Degeneration of brain stem and medullary autonomic nuclei multidomain autonomic failure Oligodendroglialopathy Histology: Proteinaceous oligodendroglial cytoplasmic inclusions (Papp-Lantos bodies) Misfolded alpha-synuclein, normally found in neuronal axons and synapses
22 Clinical Presentation Prodromal premotor phase Sexual dysfunction Urinary urge incontinence Orthostatic Hypotension Inspiratory Stridor Rapid Eye Movement Sleep Behavior Disorder
23 REM Sleep Behavior Disorder (RBD) Abnormal behaviors during REM sleep Vocalizations and complex motor ranging from aggressive to pleasurable. Dream enactment behavior Polysomnography- loss of skeletal muscle atonia during REM sleep 50% with spontaneous RBD develop parkinsonism 1817 An Essay on Shaking Palsy : Case VI demonstrated a violent parasomnia 81-90% develop a neurodegenerative disorder Most reveal alpha synuclein abnormalities post mortem
24 Clinical Presentation Motor Features Multiple System Atrophy- Parkinsonism (MSA-P) Slowness of movements, rigidity, fall tendency Lack of pill rolling tremor Irregular postural and action tremor with superimposed jerks (50%) Degeneration of striatum poor response to levodopa though transient response can be seen in 40% of patients
25 Clinical Presentation Motor Features Multiple System Atrophy- Cerebellar Cerebellar ataxia Wide based gait, uncoordinated limb movements, action tremor, downbeat nystagmus Lack of spasticity Can see hyperreflexia in 30-50% of cases Abnormal posturing: bent spine and antecollis Dysphonia, dysarthria, dysphagia Recurrent falls
26 Clinical Presentation Nonmotor Features Autonomic dysfunction hallmark of disease Erectile Dysfunction Urinary Dysfunction Often misdiagnosed as BPH in men or perineal laxity in women Orthostatic Hypotension Syncope, dizziness, weakness, nausea, pain in neck and shoulder region
27 Clinical Presentation Nonmotor Features Respiratory disturbances Inspiratory stridor in 50% of patients especially in advanced disease This can occur with sleep apnea together Risk factor for sudden death Autonomic Failure Constipation, Thermoregulatory Problems
28 Clinical Presentation Nonmotor Features Dementia and hallucinations are not a part of the disease Frontal lobe dysfunction can occur- emotional incontinence, behavioral changes Depression, anxiety, and suicidal ideation are more common
29
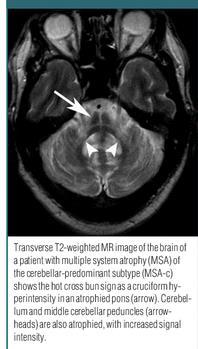
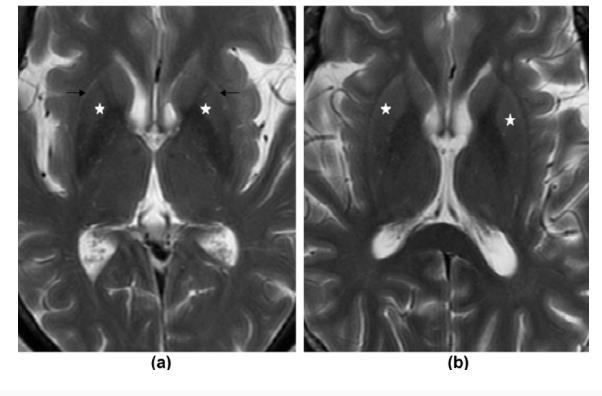
30 Radiographic Signs MRI MSA-P: atrophy of putamen, middle cerebellar peduncle, pons or cerebellum putaminal rim sign- hyperintense signal of the dorsolateral border of putamen plus putaminal hypointensity in T 2 weighted sequences MSA- C Atrophy of putamen, middle cerebellar peduncle, or pons Hot cross bun sign (Cruciform hyperintensity in the pons) in T 2 weighted sequences Putaminal rim sign and hot cross bun signs are specific but not sensitive
31
32
33 Disease Progression Worsening of symptoms over 10 year period 50%: walking aids within 3 years 60%: wheelchair by 5 years 6-8 years: bedridden Causes of death: Pneumonia, Sepsis secondary to UTI, Sudden Death due to bilateral vocal cord paralysis or disruption of brainstem cardiorespiratory drive Poor prognostic indicators: older age, parkinsonian phenotype, and early development of severe autonomic failure
34 Disease Progression
35 Treatments Symptomatic therapy with low evidence Motor Features Slow increase in levodopa- 40% responsive at first
36 Treatments Nonmotor Features Neurogenic bladder: screen regularly for UTIs Urge incontinence: antimuscarinic agents, with caution Sildenafil for ED ; intracavernous injections of prostaglandins may be an alternative Orthostatic hypotension Fludrocortisone or midodrine Behavioral changes Inspiratory Stridor or Sleep Apnea CPAP or botox injection in vocal cord adductors Glycopyrrolate or botox of salivary glands for drooling, impaired swallowing
37 Acknowledgements Thank you to: Dr. William Medd Dr. Sarah Dodwell Dr. Erich Russell Dr. Stephen Hayes
38 References Fanciulli A, Wenning GK. Multiple-System Atrophy. N Engl J Med 2015; 372: Howell, MJ, Schenck CH. Rapid Eye Movement Sleep Behavior Disorder and Neurodegenerative Disease. JAMA Neurology 2015; 72 (6); Quinn, Niall. Multiple System Atrophy- the nature of the beast. Journal of Neurology, Neurosurgery, and Psychiatry. Special Supplement. 1989: Bega, D, Gonzalez-Latapi, P, Zadikoff, C, et al. Is there a role for DAT-SPECT imaging in a Specialty Movement Disorders Practice? Neurodegener Dis 2015; 15:

39
DIFFERENTIAL DIAGNOSIS SARAH MARRINAN
 Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Parkinson s Academy Registrar Masterclass Sheffield DIFFERENTIAL DIAGNOSIS SARAH MARRINAN 17 th September 2014 Objectives Importance of age in diagnosis Diagnostic challenges Brain Bank criteria Differential
Evaluation of Parkinson s Patients and Primary Care Providers
 Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
Evaluation of Parkinson s Patients and Primary Care Providers 2018 Movement Disorders Half Day Symposium Elise Anderson MD Medical Co-Director, PBSI Movement Disorders 6/28/2018 1 Disclosures GE Speaker,
III./3.1. Movement disorders with akinetic rigid symptoms
 III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
III./3.1. Movement disorders with akinetic rigid symptoms III./3.1.1. Parkinson s disease Parkinson s disease (PD) is the second most common neurodegenerative disorder worldwide after Alzheimer s disease.
Pietro Cortelli. IRCCS Istituto delle Scienze Neurologiche di Bologna DIBINEM, Alma Mater Studiorum - Università di Bologna
 Pietro Cortelli IRCCS Istituto delle Scienze Neurologiche di Bologna DIBINEM, Alma Mater Studiorum - Università di Bologna HYSTORY 1900 description of OPCA (Dejerine, Thomas) 1960 description of Shy-Drager
Pietro Cortelli IRCCS Istituto delle Scienze Neurologiche di Bologna DIBINEM, Alma Mater Studiorum - Università di Bologna HYSTORY 1900 description of OPCA (Dejerine, Thomas) 1960 description of Shy-Drager
MULTI SYSTEM ATROPHY: REPORT OF TWO CASES Dipu Bhuyan 1, Rohit Kr. Chandak 2, Pankaj Kr. Patel 3, Sushant Agarwal 4, Debjanee Phukan 5
 MULTI SYSTEM ATROPHY: REPORT OF TWO CASES Dipu Bhuyan 1, Rohit Kr. Chandak 2, Pankaj Kr. Patel 3, Sushant Agarwal 4, Debjanee Phukan 5 HOW TO CITE THIS ARTICLE: Dipu Bhuyan, Rohit Kr. Chandak, Pankaj Kr.
MULTI SYSTEM ATROPHY: REPORT OF TWO CASES Dipu Bhuyan 1, Rohit Kr. Chandak 2, Pankaj Kr. Patel 3, Sushant Agarwal 4, Debjanee Phukan 5 HOW TO CITE THIS ARTICLE: Dipu Bhuyan, Rohit Kr. Chandak, Pankaj Kr.
Niall Quinn. Professor of Clinical Neurology UCL IoN & NHNN Queen Square London UK
 Niall Quinn Professor of Clinical Neurology UCL IoN & NHNN Queen Square London UK Decade of the basal ganglia 1960 Shy Drager syndrome 1961 Striatonigral degeneration 1961 Birkmeyer & Hornykiewicz; Barbeau
Niall Quinn Professor of Clinical Neurology UCL IoN & NHNN Queen Square London UK Decade of the basal ganglia 1960 Shy Drager syndrome 1961 Striatonigral degeneration 1961 Birkmeyer & Hornykiewicz; Barbeau
Multiple System Atrophy
 Multiple System Atrophy This document has been prepared to help you become more informed about Multiple System Atrophy. It is designed to answer questions about the condition and includes suggestions on
Multiple System Atrophy This document has been prepared to help you become more informed about Multiple System Atrophy. It is designed to answer questions about the condition and includes suggestions on
A guide to Multiple System Atrophy for: General Practitioners
 Introduction Prevalence Duration Initial presentation Red flags and symptoms Key management problems GP support The MSA Trust A guide to Multiple System Atrophy for: General Practitioners This document
Introduction Prevalence Duration Initial presentation Red flags and symptoms Key management problems GP support The MSA Trust A guide to Multiple System Atrophy for: General Practitioners This document
Atypical parkinsonism
 Atypical parkinsonism Wassilios Meissner Service de neurologie et CMR atrophie multisystématisée, CHU de Bordeaux Institut des Maladies Neurodégénératives, Université Bordeaux 2, CNRS UMR 5293 Parkinsonism?
Atypical parkinsonism Wassilios Meissner Service de neurologie et CMR atrophie multisystématisée, CHU de Bordeaux Institut des Maladies Neurodégénératives, Université Bordeaux 2, CNRS UMR 5293 Parkinsonism?
Evolution of a concept: Apraxia/higher level gait disorder. ataxia v. apraxia gait = limb apraxia. low, middle, high gait disturbance levels
 Case #1 81-year-old woman Gait Imbalance: Two Unusual Cases in Older Patients February 2008: 3 years of gradually progressive gait imbalance no vertigo, dizziness or paresthesias etiology unclear on examination
Case #1 81-year-old woman Gait Imbalance: Two Unusual Cases in Older Patients February 2008: 3 years of gradually progressive gait imbalance no vertigo, dizziness or paresthesias etiology unclear on examination
Overview. Overview. Parkinson s disease. Secondary Parkinsonism. Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits
 Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Overview Overview Parkinsonism: Motor symptoms associated with impairment in basal ganglia circuits The differential diagnosis of Parkinson s disease Primary vs. Secondary Parkinsonism Proteinopathies:
Sleep-Disordered Breathing and Risk of Sudden Death in Multiple System Atrophy
 Sleep-Disordered Breathing and Risk of Sudden Death in Multiple System Atrophy Lisa Cutchen MD Sleep Medicine Fellow University of New Mexico Sleep Disorders Center New Mexico Thoracic Society February
Sleep-Disordered Breathing and Risk of Sudden Death in Multiple System Atrophy Lisa Cutchen MD Sleep Medicine Fellow University of New Mexico Sleep Disorders Center New Mexico Thoracic Society February
Early Clinical Features of Parkinson s Disease and Related Disorders. Dr. Alastair Noyce
 1 Specialist Registrar in Neurology, London Deanery Parkinson s UK Doctoral Research Fellow Project lead for PREDICT-PD Declarations Salary: Parkinson's UK, Barts and the London NHS Trust Grants: Parkinson's
1 Specialist Registrar in Neurology, London Deanery Parkinson s UK Doctoral Research Fellow Project lead for PREDICT-PD Declarations Salary: Parkinson's UK, Barts and the London NHS Trust Grants: Parkinson's
Parkinson s Disease in the Elderly A Physicians perspective. Dr John Coyle
 Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Parkinson s Disease in the Elderly A Physicians perspective Dr John Coyle Overview Introduction Epidemiology and aetiology Pathogenesis Diagnosis and clinical features Treatment Psychological issues/ non
Joint Session with ACOFP and Mayo Clinic. Parkinson's Disease: 5 Pearls. Jay Van Gerpen, MD
 Joint Session with ACOFP and Mayo Clinic Parkinson's Disease: 5 Pearls Jay Van Gerpen, MD Parkinson s Disease: 5 Pearls J.A. van Gerpen, MD Sections of Movement Disorders and Clinical Neurophysiology
Joint Session with ACOFP and Mayo Clinic Parkinson's Disease: 5 Pearls Jay Van Gerpen, MD Parkinson s Disease: 5 Pearls J.A. van Gerpen, MD Sections of Movement Disorders and Clinical Neurophysiology
Parkinson Disease. Lorraine Kalia, MD, PhD, FRCPC. Presented by: Ontario s Geriatric Steering Committee
 Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
Parkinson Disease Lorraine Kalia, MD, PhD, FRCPC Key Learnings Parkinson Disease (L. Kalia) Key Learnings Parkinson disease is the most common but not the only cause of parkinsonism Parkinson disease is
:{ic0fp'16. Geriatric Medicine: Blood Pressure Monitoring in the Elderly. Terrie Ginsberg, DO, FACOI
 :{ic0fp'16 ACOFP 53 rd Annual Convention & Scientific Seminars Geriatric Medicine: Blood Pressure Monitoring in the Elderly Terrie Ginsberg, DO, FACOI Blood Pressure Management in the Elderly Terrie B.
:{ic0fp'16 ACOFP 53 rd Annual Convention & Scientific Seminars Geriatric Medicine: Blood Pressure Monitoring in the Elderly Terrie Ginsberg, DO, FACOI Blood Pressure Management in the Elderly Terrie B.
Parkinson s Disease. Prevalence. Mark S. Baron, M.D. Cardinal Features. Clinical Characteristics. Not Just a Movement Disorder
 Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
Prevalence Parkinson s Disease Mark S. Baron, M.D. Associate Professor of Neurology Movement Disorders Section VCU School of Medicine Common disorder Approaching 1% by 65 yrs of age, 2% by 80 yrs of age
International Journal of Health Sciences and Research ISSN:
 International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Multiple System Atrophy-Cerebellar Type (MSA-C): A Case Report Mohd Abbas Ilyas, Pramod Shaha, Kulamani Sahoo,
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report Multiple System Atrophy-Cerebellar Type (MSA-C): A Case Report Mohd Abbas Ilyas, Pramod Shaha, Kulamani Sahoo,
Movement Disorders. Psychology 372 Physiological Psychology. Background. Myasthenia Gravis. Many Types
 Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Background Movement Disorders Psychology 372 Physiological Psychology Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Early Studies Found some patients with progressive weakness
Non-Motor Symptoms of Parkinson s Disease
 Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
Non-Motor Symptoms of Parkinson s Disease Samantha Holden, MD University of Colorado Movement Disorders MOTOR SYMPTOMS Rigidity Bradykinesia Tremor Gait Imbalance NON-MOTOR SYMPTOMS Dementia Urinary frequency
Differential Diagnosis of Hypokinetic Movement Disorders
 Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Differential Diagnosis of Hypokinetic Movement Disorders Dr Donald Grosset Consultant Neurologist - Honorary Professor Institute of Neurological Sciences - Glasgow University Hypokinetic Parkinson's Disease
Parkinson s Disease Initial Clinical and Diagnostic Evaluation. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
Parkinson s Disease Initial Clinical and Diagnostic Evaluation J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even when supported
The PSP Association. Presentation on the symptoms, care and support of patients with PSP.
 The PSP Association Presentation on the symptoms, care and support of patients with PSP. 1 Presented by: Kathy Miller-Hunt Development Officer Southwest Other names Steele Richardson Olszewski Syndrome
The PSP Association Presentation on the symptoms, care and support of patients with PSP. 1 Presented by: Kathy Miller-Hunt Development Officer Southwest Other names Steele Richardson Olszewski Syndrome
Parkinson s Disease Update. Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s
 Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Parkinson s Disease Update Presented by Joanna O Leary, MD Movement disorder neurologist Providence St. Vincent s What is a movement disorder? Neurological disorders that affect ability to move by causing
Subthalamic Nucleus Deep Brain Stimulation (STN-DBS)
") Subthalamic Nucleus Deep Brain Stimulation (STN-DBS) A Neurosurgical Treatment for Parkinson s Disease Parkinson s Disease Parkinson s disease is a common neurodegenerative disorder that affects about
Subthalamic Nucleus Deep Brain Stimulation (STN-DBS) A Neurosurgical Treatment for Parkinson s Disease Parkinson s Disease Parkinson s disease is a common neurodegenerative disorder that affects about
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features. J. Timothy Greenamyre, MD, PhD
 Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
Parkinson s Disease: initial diagnosis, initial treatment & non-motor features J. Timothy Greenamyre, MD, PhD Involuntary tremulous motion, with lessened muscular power, in parts not in action and even
The Parkinson s You Can t See
 The Parkinson s You Can t See We principally see the motor phenomena of Parkinson's disease, but is there an early stage without visible features? Might this provide a window for disease-modifying therapy?
The Parkinson s You Can t See We principally see the motor phenomena of Parkinson's disease, but is there an early stage without visible features? Might this provide a window for disease-modifying therapy?
Parts of the motor circuits
 MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
MOVEMENT DISORDERS Parts of the motor circuits cortical centers: there are centers in all the cortical lobes subcortical centers: caudate nucleus putamen pallidum subthalamical nucleus (Luys) nucleus ruber
Multiple choice questions: ANSWERS
 Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Multiple choice questions: ANSWERS Chapter 1. Redefining Parkinson s disease 1. Common non-motor features that precede the motor findings in Parkinson s disease (PD) include all of the following except?
Identification number: TÁMOP /1/A
 Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
Manifestation of Novel Social Challenges of the European Union in the Teaching Material of Medical Biotechnology Master s Programmes at the University of Pécs and at the University of Debrecen Identification
PARKINSON S PRIMER. Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada
 PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
PARKINSON S PRIMER Dr. Kathryn Giles MD, MSc, FRCPC Cambridge, Ontario, Canada COPYRIGHT 2017 BY SEA COURSES INC. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Objectives. Distinguishing Parkinson s disease from other parkinsonian and tremor syndromes. Characteristics. Basal Ganglia Structures
 12:45 1:30 pm PD or not PD? Distinguishing Parkinson s Disease From Other Parkinsonian and Tremor Syndromes SPEAKER Jennifer G. Goldman, MD, MS Presenter Disclosure Information The following relationships
12:45 1:30 pm PD or not PD? Distinguishing Parkinson s Disease From Other Parkinsonian and Tremor Syndromes SPEAKER Jennifer G. Goldman, MD, MS Presenter Disclosure Information The following relationships
Functional Distinctions
 Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
Functional Distinctions FUNCTION COMPONENT DEFICITS Start Basal Ganglia Spontaneous Movements Move UMN/LMN Cerebral Cortex Brainstem, Spinal cord Roots/peripheral nerves Plan Cerebellum Ataxia Adjust Cerebellum
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia
 What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
What if it s not Alzheimer s? Update on Lewy body dementia and frontotemporal dementia Dementia: broad term for any acquired brain condition impairing mental function such that ADLs are impaired. Includes:
PARKINSON S DISEASE. Nigrostriatal Dopaminergic Neurons 5/11/16 CARDINAL FEATURES OF PARKINSON S DISEASE. Parkinson s disease
 5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
5/11/16 PARKINSON S DISEASE Parkinson s disease Prevalence increases with age (starts 40s60s) Seen in all ethnic groups, M:F about 1.5:1 Second most common neurodegenerative disease Genetics role greater
Non-motor symptoms as a marker of. Michael Samuel
 Non-motor symptoms as a marker of progression in Parkinson s s disease Michael Samuel London, UK 1 Definitions and their problems Non-motor symptoms as a marker of progression Non-motor symptoms (NMS)
Non-motor symptoms as a marker of progression in Parkinson s s disease Michael Samuel London, UK 1 Definitions and their problems Non-motor symptoms as a marker of progression Non-motor symptoms (NMS)
Multiple System Atrophy Manifested by Bilateral Vocal Cord Palsy as an Initial Sign
 Korean J Crit Care Med 2015 May 30(2):123-127 / ISSN 2383-4870 (Print) ㆍ ISSN 2383-4889 (Online) Case Report Multiple System Atrophy Manifested by Bilateral Vocal Cord Palsy as an Initial Sign Yuri Seo,
Korean J Crit Care Med 2015 May 30(2):123-127 / ISSN 2383-4870 (Print) ㆍ ISSN 2383-4889 (Online) Case Report Multiple System Atrophy Manifested by Bilateral Vocal Cord Palsy as an Initial Sign Yuri Seo,
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute
 Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Parkinson s Disease Associated Sleep Disturbance Ehsan M. Hadi, MD, MPH. Dignity Health Neurological Institute Parkinson s Disease 2 nd most common neurodegenerative disorder Peak age at onset is 60 years
Movement Disorders: A Brief Overview
 Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Movement Disorders: A Brief Overview Albert Hung, MD, PhD Massachusetts General Hospital Harvard Medical School August 17, 2006 Cardinal Features of Parkinsonism Tremor Rigidity Bradykinesia Postural imbalance
Comprehensive Approach to DLB Management
 Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
Comprehensive Approach to DLB Management Bradley F. Boeve, MD Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Comprehensive Approach to DLB Management Disclosures
Enhanced Primary Care Pathway: Parkinson s Disease
 Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
Enhanced Primary Care Pathway: Parkinson s Disease 1. Focused summary of PD relevant to primary care Parkinson s Disease (PD) and Essential tremor (ET) are two of the most common movement disorders encountered
PARKINS ON CENTER. Parkinson s Disease: Diagnosis and Management. Learning Objectives: Recognition of PD OHSU. Disclosure Information
 OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
OHSU PARKINS ON CENTER Parkinson s Disease: Diagnosis and Management for Every MD Disclosure Information Grants/Research Support: National Parkinson Foundation, NIH, Michael J. Fox Foundation Consultant:
Parkinson s Disease. Sirilak yimcharoen
 Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Parkinson s Disease Sirilak yimcharoen EPIDEMIOLOGY ~1% of people over 55 years Age range 35 85 years peak age of onset is in the early 60s ~5% of cases characterized by an earlier age of onset (typically
Extrapyramidal Motor System. Basal Ganglia or Striatum. Basal Ganglia or Striatum 3/3/2010
 Extrapyramidal Motor System Basal Ganglia or Striatum Descending extrapyramidal paths receive input from other parts of motor system: From the cerebellum From the basal ganglia or corpus striatum Caudate
Extrapyramidal Motor System Basal Ganglia or Striatum Descending extrapyramidal paths receive input from other parts of motor system: From the cerebellum From the basal ganglia or corpus striatum Caudate
Corporate Medical Policy
 Corporate Medical Policy Dopamine Transporter Imaging with Single Photon Emission File Name: Origination: Last CAP Review: Next CAP Review: Last Review: dopamine_transporter_imaging_with_single_photon_emission_computed_tomography
Corporate Medical Policy Dopamine Transporter Imaging with Single Photon Emission File Name: Origination: Last CAP Review: Next CAP Review: Last Review: dopamine_transporter_imaging_with_single_photon_emission_computed_tomography
The PD You Don t See: Cognitive and Non-motor Symptoms
 The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Assistant Professor of Neurology and Psychiatry University of Colorado Denver Goals 1) What are the most common non-motor
The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Assistant Professor of Neurology and Psychiatry University of Colorado Denver Goals 1) What are the most common non-motor
Clinical Characteristics of Patients with Multiple System Atrophy in Singapore
 Original Article 553 Clinical Characteristics of Patients with Multiple System Atrophy in Singapore RDG Jamora, 1 MD, A Gupta, 1 MRCP (UK), AKY Tan, 1 MRCP (UK), FAMS, LCS Tan, 1 FRCP (Edin), FAMS Abstract
Original Article 553 Clinical Characteristics of Patients with Multiple System Atrophy in Singapore RDG Jamora, 1 MD, A Gupta, 1 MRCP (UK), AKY Tan, 1 MRCP (UK), FAMS, LCS Tan, 1 FRCP (Edin), FAMS Abstract
Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy
 Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy Dr Rahul Chakor, Associate Prof and Head Dept of Neurology, Dr Anand Soni, Senior Resident, T N Medical
Dizziness, postural hypotension and postural blackouts: Two cases suggesting multiple system atrophy Dr Rahul Chakor, Associate Prof and Head Dept of Neurology, Dr Anand Soni, Senior Resident, T N Medical
10th Medicine Review Course st July Prakash Kumar
 10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
10th Medicine Review Course 2018 21 st July 2018 Drug Therapy for Parkinson's disease Prakash Kumar National Neuroscience Institute Singapore General Hospital Sengkang General Hospital Singhealth Duke-NUS
CN V! touch! pain! Touch! P/T!
 CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
CN V! touch! pain! Touch! P/T! Visual Pathways! L! R! B! A! C! D! LT! E! F! RT! G! hypothalamospinal! and! ALS! Vestibular Pathways! 1. Posture/Balance!!falling! 2. Head Position! 3. Eye-Head Movements
Neurodegenerative Disease. April 12, Cunningham. Department of Neurosciences
 Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
Neurodegenerative Disease April 12, 2017 Cunningham Department of Neurosciences NEURODEGENERATIVE DISEASE Any of a group of hereditary and sporadic conditions characterized by progressive dysfunction,
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging. Dr. Olav E. Krigolson Lecture 5: PARKINSONS DISEASE
 ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
ASHI691: Why We Fall Apart: The Neuroscience and Neurophysiology of Aging Dr. Olav E. Krigolson krigolson@uvic.ca Lecture 5: PARKINSONS DISEASE The Basal Ganglia Primary motor cortex Execution of movement
Središnja medicinska knjižnica
 Središnja medicinska knjižnica Adamec I., Klepac N., Milivojević I., Radić B., Habek M. (2012) Sick sinus syndrome and orthostatic hypotension in Parkinson's disease. Acta Neurologica Belgica, 112 (3).
Središnja medicinska knjižnica Adamec I., Klepac N., Milivojević I., Radić B., Habek M. (2012) Sick sinus syndrome and orthostatic hypotension in Parkinson's disease. Acta Neurologica Belgica, 112 (3).
Faculty. Joseph Friedman, MD
 Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Faculty Claire Henchcliffe, MD, DPhil Associate Professor of Neurology Weill Cornell Medical College Associate Attending Neurologist New York-Presbyterian Hospital Director of the Parkinson s Institute
Multiple-system atrophy is an adult-onset, fatal neurodegenerative
 Review Article Dan L. Longo, M.D., Editor Multiple-System Atrophy Alessandra Fanciulli, M.D., and Gregor K. Wenning, M.D., Ph.D. Multiple-system atrophy is an adult-onset, fatal neurodegenerative disease
Review Article Dan L. Longo, M.D., Editor Multiple-System Atrophy Alessandra Fanciulli, M.D., and Gregor K. Wenning, M.D., Ph.D. Multiple-system atrophy is an adult-onset, fatal neurodegenerative disease
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
Program Highlights. Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone Medical Center New York, New York
 Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
Program Highlights David Swope, MD Associate Professor of Neurology Mount Sinai Health System New York, New York Michael Pourfar, MD Co-Director, Center for Neuromodulation New York University Langone
VL VA BASAL GANGLIA. FUNCTIONAl COMPONENTS. Function Component Deficits Start/initiation Basal Ganglia Spontan movements
 BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
BASAL GANGLIA Chris Cohan, Ph.D. Dept. of Pathology/Anat Sci University at Buffalo I) Overview How do Basal Ganglia affect movement Basal ganglia enhance cortical motor activity and facilitate movement.
The PD You Don t See: Cognitive and Non-motor Symptoms
 The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
The PD You Don t See: Cognitive and Non-motor Symptoms Benzi M. Kluger, M.D., M.S. Associate Professor of Neurology and Psychiatry Director Movement Disorders Center University of Colorado Denver Goals
Dementia Update. Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota
 Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Dementia Update Daniel Drubach, M.D. Division of Behavioral Neurology Department of Neurology Mayo Clinic Rochester, Minnesota Nothing to disclose Dementia Progressive deterioration in mental function
Date of Referral: Enhanced Primary Care Pathway: Parkinson s Disease
 Specialist LINK Linking Physicians CALGARY AND AREA Patient Name: Date of Birth: Calgary RHRN: PHN / ULI: Date of Referral: Referring MD: Fax: Today s Date: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS:
Specialist LINK Linking Physicians CALGARY AND AREA Patient Name: Date of Birth: Calgary RHRN: PHN / ULI: Date of Referral: Referring MD: Fax: Today s Date: CONFIRMATION: TRIAGE CATEGORY: REFERRAL STATUS:
The NIHSS score is 4 (considering 2 pts for the ataxia involving upper and lower limbs.
 Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Neuroscience case 5 1. Speech comprehension, ability to speak, and word use were normal in Mr. Washburn, indicating that aphasia (cortical language problem) was not involved. However, he did have a problem
Vague Neurological Disorders
 Vague Neurological Disorders Dr. Philip Smalley MD FRCPC SVP & Global Chief Medical Officer RGA International Rose Conference, September 17, 2015 Agenda Vague neurological symptoms associated with: Alzheimer
Vague Neurological Disorders Dr. Philip Smalley MD FRCPC SVP & Global Chief Medical Officer RGA International Rose Conference, September 17, 2015 Agenda Vague neurological symptoms associated with: Alzheimer
Optimizing Clinical Communication in Parkinson s Disease:
 Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
Optimizing Clinical Communication in Parkinson s Disease:,Strategies for improving communication between you and your neurologist PFNCA Symposium March 25, 2017 Pritha Ghosh, MD Assistant Professor of
CONTROL OF MOVEMENT BY THE BRAIN A. PRIMARY MOTOR CORTEX:
 CONTROL OF MOVEMENT BY THE BRAIN A. PRIMARY MOTOR CORTEX: - responsible for - like somatosensory cortex, primary motor cortex show (motor homunculus) - amount of cortex devoted to different parts of body
CONTROL OF MOVEMENT BY THE BRAIN A. PRIMARY MOTOR CORTEX: - responsible for - like somatosensory cortex, primary motor cortex show (motor homunculus) - amount of cortex devoted to different parts of body
Parkinson s Disease Current Treatment Options
 Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
Parkinson s Disease Current Treatment Options Daniel Kassicieh, D.O., FAAN Sarasota Neurology, P.A. PD: A Chronic Neurodegenerative Ds. 1 Million in USA Epidemiology 50,000 New Cases per Year Majority
A. PRIMARY MOTOR CORTEX: - responsible for - like somatosensory cortex, primary motor cortex show (motor homunculus) - amount of cortex devoted to
 - amount of cortex devoted to") CONTROL OF MOVEMENT BY THE BRAIN A. PRIMARY MOTOR CORTEX: - responsible for - like somatosensory cortex, primary motor cortex show (motor homunculus) - amount of cortex devoted to different parts of body
CONTROL OF MOVEMENT BY THE BRAIN A. PRIMARY MOTOR CORTEX: - responsible for - like somatosensory cortex, primary motor cortex show (motor homunculus) - amount of cortex devoted to different parts of body
High Yield Neurological Examination
 High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
High Yield Neurological Examination Vanja Douglas, MD Sara & Evan Williams Foundation Endowed Neurohospitalist Chair Director, Neurohospitalist Division Associate Professor of Clinical Neurology UCSF Department
Brain and Central Nervous System Cancers
 Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Brain and Central Nervous System Cancers NICE guidance link: https://www.nice.org.uk/guidance/ta121 Clinical presentation of brain tumours History and Examination Consider immediate referral Management
Biology 3201 Nervous System # 7: Nervous System Disorders
 Biology 3201 Nervous System # 7: Nervous System Disorders Alzheimer's Disease first identified by German physician, Alois Alzheimer, in 1906 most common neurodegenerative disease two thirds of cases of
Biology 3201 Nervous System # 7: Nervous System Disorders Alzheimer's Disease first identified by German physician, Alois Alzheimer, in 1906 most common neurodegenerative disease two thirds of cases of
FOUNDATION OF UNDERSTANDING PARKINSON S DISEASE
 FOUNDATION OF UNDERSTANDING PARKINSON S DISEASE DEE SILVER M.D MOVEMENT DISORDER SPECIALIST MEDICAL DIRECTOR -- PARKINSON ASSOCIATION OF SAN DIEGO 1980 TO PRESENT SCRIPPS MEMORIAL HOSPITAL, LA JOLLA CA.
FOUNDATION OF UNDERSTANDING PARKINSON S DISEASE DEE SILVER M.D MOVEMENT DISORDER SPECIALIST MEDICAL DIRECTOR -- PARKINSON ASSOCIATION OF SAN DIEGO 1980 TO PRESENT SCRIPPS MEMORIAL HOSPITAL, LA JOLLA CA.
Dizziness: Neurological Aspect
 Dizziness: Neurological Aspect..! E-mail: somtia@kku.ac.th http://epilepsy.kku.ac.th Features between peripheral and central vertigo 1. Peripheral Central 2.! " # $ " Imbalance Mild-moderate Severe 3.!
Dizziness: Neurological Aspect..! E-mail: somtia@kku.ac.th http://epilepsy.kku.ac.th Features between peripheral and central vertigo 1. Peripheral Central 2.! " # $ " Imbalance Mild-moderate Severe 3.!
Parkinsons Disease & Movement Disorder Aug 11-13, Frankfurt l Dr. Geeta Shroff
 USE OF HUMAN EMBRYONIC STEM CELLS IN THE TREATMENT OF PARKINSON S DISEASE Dr. Geeta Shroff Founder and Medical Director, Nutech Mediworld CONDITIONS TREATED Spinal Cord Injury Cell Culture Technology Diabetes
USE OF HUMAN EMBRYONIC STEM CELLS IN THE TREATMENT OF PARKINSON S DISEASE Dr. Geeta Shroff Founder and Medical Director, Nutech Mediworld CONDITIONS TREATED Spinal Cord Injury Cell Culture Technology Diabetes
Multiple system atrophy (MSA) is a sporadic adult-onset
 is a sporadic adult-onset") ORIGINAL RESEARCH E. Matsusue S. Fujii Y. Kanasaki T. Kaminou E. Ohama T. Ogawa Cerebellar Lesions in Multiple System Atrophy: Postmortem MR Imaging Pathologic Correlations BACKGROUND AND PURPOSE: Cerebellar
ORIGINAL RESEARCH E. Matsusue S. Fujii Y. Kanasaki T. Kaminou E. Ohama T. Ogawa Cerebellar Lesions in Multiple System Atrophy: Postmortem MR Imaging Pathologic Correlations BACKGROUND AND PURPOSE: Cerebellar
Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination
 Three-step H.I.N.T.S. eye examination") Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination Head Impulse (right- and leftward) Nystagmus type Test of Skew (cover test for skew deviation) Stroke findings: I.N.F.A.R.C.T.
Acute Vestibular Syndrome (VS or Stroke?) Three-step H.I.N.T.S. eye examination Head Impulse (right- and leftward) Nystagmus type Test of Skew (cover test for skew deviation) Stroke findings: I.N.F.A.R.C.T.
MAXIMIZING FUNCTION IN PARKINSON S DISEASE
 1 MAXIMIZING FUNCTION IN PARKINSON S DISEASE September 13, 2016 End Falls This Falls Conference Jan Goldstein Elman One Step Ahead Mobility Toronto, Ontario Outline An overview of Parkinson s disease (PD):
1 MAXIMIZING FUNCTION IN PARKINSON S DISEASE September 13, 2016 End Falls This Falls Conference Jan Goldstein Elman One Step Ahead Mobility Toronto, Ontario Outline An overview of Parkinson s disease (PD):
MOVEMENT DISORDERS AND DEMENTIA
 MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
MOVEMENT DISORDERS AND DEMENTIA FOCUS ON DEMENTIA WITH LEWY BODIES MADHAVI THOMAS MD NORTH TEXAS MOVEMENT DISORDERS INSTITUTE, INC DEMENTIA de men tia dəˈmen(t)sh(ē)ə/ nounmedicine noun: dementia a chronic
Pathogenesis of Degenerative Diseases and Dementias. D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria)
. M. Path (U. of Alexandria)") Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
Pathogenesis of Degenerative Diseases and Dementias D r. Ali Eltayb ( U. of Omdurman. I ). M. Path (U. of Alexandria) Dementias Defined: as the development of memory impairment and other cognitive deficits
WELCOME. Parkinson s 101 for the Newly Diagnosed. Today s Topic: Parkinson s Basics presented by Cari Friedman, LCSW
 WELCOME Parkinson s 101 for the Newly Diagnosed Today s Topic: Parkinson s Basics presented by Cari Friedman, LCSW Parkinson s Disease 101 Presenter for Today Cari Friedman, LCSW Patient and Family Service
WELCOME Parkinson s 101 for the Newly Diagnosed Today s Topic: Parkinson s Basics presented by Cari Friedman, LCSW Parkinson s Disease 101 Presenter for Today Cari Friedman, LCSW Patient and Family Service
Parkinson s Disease and other related movement disorders a video guide to diagnosis
 Parkinson s Disease and other related movement disorders a video guide to diagnosis Parkinson s Disease Masterclass November 2017 Dr Frank Phelan MidYorkshire Hospitals NHS Trust Ideopathic Parkinson s
Parkinson s Disease and other related movement disorders a video guide to diagnosis Parkinson s Disease Masterclass November 2017 Dr Frank Phelan MidYorkshire Hospitals NHS Trust Ideopathic Parkinson s
ORIGINAL CONTRIBUTION. Brain Magnetic Resonance Imaging in Multiple-System Atrophy and Parkinson Disease
 Brain Magnetic Resonance Imaging in Multiple-System Atrophy and Parkinson Disease A Diagnostic Algorithm ORIGINAL CONTRIBUTION Kirsty Bhattacharya, MD; Daniela Saadia, MD; Barbara Eisenkraft, MD; Melvin
Brain Magnetic Resonance Imaging in Multiple-System Atrophy and Parkinson Disease A Diagnostic Algorithm ORIGINAL CONTRIBUTION Kirsty Bhattacharya, MD; Daniela Saadia, MD; Barbara Eisenkraft, MD; Melvin
14 - Central Nervous System. The Brain Taft College Human Physiology
 14 - Central Nervous System The Brain Taft College Human Physiology Development of the Brain The brain begins as a simple tube, a neural tube. The tube or chamber (ventricle) is filled with cerebrospinal
14 - Central Nervous System The Brain Taft College Human Physiology Development of the Brain The brain begins as a simple tube, a neural tube. The tube or chamber (ventricle) is filled with cerebrospinal
A Hypothesis Driven Approach to the Neurological Exam
 A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
A Hypothesis Driven Approach to the Neurological Exam Vanja Douglas, MD Assistant Clinical Professor UCSF Department of Neurology Disclosures None 1 Purpose of Neuro Exam Screen asymptomatic patients Screen
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O.
 Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
Parkinson s Disease WHERE HAVE WE BEEN, WHERE ARE WE HEADING? CHARLECE HUGHES D.O. Parkinson s Epidemiology AFFECTS 1% OF POPULATION OVER 65 MEAN AGE OF ONSET 65 MEN:WOMEN 1.5:1 IDIOPATHIC:HEREDITARY 90:10
M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz. Parkinson s Disease. A Guide to Medical Treatment
 M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz Parkinson s Disease A Guide to Medical Treatment SEEd srl. All rights reserved Piazza Carlo Emanuele II, 19 10123 Torino, Italy Tel. 011.566.02.58
M. Carranza M. R. Snyder J. Davenport Shaw T. A. Zesiewicz Parkinson s Disease A Guide to Medical Treatment SEEd srl. All rights reserved Piazza Carlo Emanuele II, 19 10123 Torino, Italy Tel. 011.566.02.58
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE
 Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Scott J Sherman MD, PhD The University of Arizona PARKINSON DISEASE LEARNING OBJECTIVES The Course Participant will: 1. Be familiar with the pathogenesis of Parkinson s Disease (PD) 2. Understand clinical
Treatment of Parkinson s Disease: Present and Future
 Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Treatment of Parkinson s Disease: Present and Future Karen Blindauer, MD Professor of Neurology Director of Movement Disorders Program Medical College of Wisconsin Neuropathology: Loss of Dopamine- Producing
Types of involuntary movements
 Tremor Types of involuntary movements Dystonia Chorea Myoclonus Tics Tremor Rhythmic shaking of muscles that produces an oscillating movement Parkinsonian tremor Rest tremor > posture > kinetic Re-emergent
Tremor Types of involuntary movements Dystonia Chorea Myoclonus Tics Tremor Rhythmic shaking of muscles that produces an oscillating movement Parkinsonian tremor Rest tremor > posture > kinetic Re-emergent
Common Forms of Dementia Handout Package
 Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
Common Forms of Dementia Handout Package Common Forms of Dementia 1 Learning Objectives As a result of working through this module, you should be better able to: 1. Describe clinical features of 4 major
8/28/2017. Behind the Scenes of Parkinson s Disease
 BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
BEHIND THE SCENCES IN Parkinson s Disease Behind the Scenes of Parkinson s Disease Anna Marie Wellins DNP, ANP C Objectives Describe prevalence of Parkinson's disease (PD) Describe the hallmark pathologic
Depression & Anxiety. What can I do? What are other possible treatments? What is this? Why does this happen? KEY POINTS
 Depression & Anxiety One set of important protectors from depression is friends and family as much as you can, keep yourself active and engaged with others. Exercise, particularly while outside, may help.
Depression & Anxiety One set of important protectors from depression is friends and family as much as you can, keep yourself active and engaged with others. Exercise, particularly while outside, may help.
Movement Disorders- Parkinson s Disease. Fahed Saada, MD March 8 th, th Family Medicine Refresher Course St.
 Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
Movement Disorders- Parkinson s Disease Fahed Saada, MD March 8 th, 2019 48 th Family Medicine Refresher Course St. Joseph s Health Disclosure ACADIA Pharmaceuticals Objectives Review the classification
Update on functional brain imaging in Movement Disorders
 Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Update on functional brain imaging in Movement Disorders Mario Masellis, MSc, MD, FRCPC, PhD Assistant Professor & Clinician-Scientist Sunnybrook Health Sciences Centre University of Toronto 53 rd CNSF
Basal ganglia Sujata Sofat, class of 2009
 Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Basal ganglia Sujata Sofat, class of 2009 Basal ganglia Objectives Describe the function of the Basal Ganglia in movement Define the BG components and their locations Describe the motor loop of the BG
Dysarthria and Dysphagia: a Neurology Perspective William Meador, MD Assistant Professor of Neurology, UAB
 Dysarthria and Dysphagia: a Neurology Perspective William Meador, MD Assistant Professor of Neurology, UAB 2.11.16 Disclosures I have no relevant conflicts or potential conflicts to disclose regarding
Dysarthria and Dysphagia: a Neurology Perspective William Meador, MD Assistant Professor of Neurology, UAB 2.11.16 Disclosures I have no relevant conflicts or potential conflicts to disclose regarding
Neurological Examination
 Neurological Examination Charles University in Prague 1st Medical Faculty and General University Hospital Neurological examination: Why important? clinical history taking and bedside examination: classical
Neurological Examination Charles University in Prague 1st Medical Faculty and General University Hospital Neurological examination: Why important? clinical history taking and bedside examination: classical
Revised criteria for the clinical diagnosis of dementia with Lewy. Dementia with Lewy bodies. (Dementia with Lewy Bodies)
") Dementia with Lewy bodies First described: Okazaki H, 1961, Diffuse intracytoplasmic ganglionic inclusions (Lewy type) associated with progressive dementia and quadriparesis in flexion. J Neuropathol Exp
Dementia with Lewy bodies First described: Okazaki H, 1961, Diffuse intracytoplasmic ganglionic inclusions (Lewy type) associated with progressive dementia and quadriparesis in flexion. J Neuropathol Exp