Programme. Why bother? The effects of sleep loss. Common Sleep Disorders, Identification and investigation Treatments
|
|
|
- Dominic Shelton
- 5 years ago
- Views:
Transcription
1
2 Programme. Why bother? The effects of sleep loss. Common Sleep Disorders, Identification and investigation Treatments Brief (but important ) questions.
3 Why bother? The three Pillars of health: - Nutrition - Exercise - SLEEP
4 Why bother? SLEEP impacts on ALL aspects of our lives. - Physically - Cognitively - Behaviouraly
5 PHYSICAL associations with Sleep Disorder Cardiovascular: Hypertension; MI; AF; CVA; CHF; Pulmonary Hypertension; CRP. Endocrine: Obesity; Insulin Resistance; Cortisol; Lipids; Leptin; Libido Cancer: Increased risk (especially breast, also bowel)
6 PHYSICAL associations with Sleep Disorder Urological: Nocturia (may be frequent) Erectile Dysfunction Gastroenterological: GORD; Gastric Ulcer Gynecological: PCO; Menstrual irregularities; Menopause Obstetric: Toxemia; Premature births; Low birth weighs
7 PHYSICAL associations with Sleep Disorder Musculoskeletal: Kyphoscoliosis Genetic: Down s syndrome; Macroglossia etc. Neurodegenerative: Alzheimer's Disease; MS. Respiratory: Obesity-Hypoventilation syndrome.
8 PSYCHOLOGICAL consequences of Sleep Disorder Increased irritability & lower stress tolerance Poor Motivation ( Can t be bothered! ) Faulty Judgment Lapses in Attention and Vigilance Impaired Decision Making & Logical reasoning Depression / Anxiety Personality Change
9 BEHAVOURAL consequences of Sleep Disorder Poor short term memory Risk taking Erratic driving Slower Reaction Time Increased Sensitivity to pain Hyperactivity in Children Accidentally falling asleep!
10 Brief questions: - Do you have any concern about your sleep? - Have you been told that you snore? - Do you wake refreshed in the morning?
11 The most common sleep disorders are associated with:- 1) Shiftwork Up to 20% of the workforce are shiftworkers 2) Insomnia 10 15% of adults suffer from chronic and severe insomnia that affects daytime performance. 3) Snoring and Obstructive Sleep Apnoea (OSA) Snoring up to 60% adults snore regularly OSAS 9% of males, 4% females over 40
 Stress/Anxiety (Hyper-arousal Disorder) Psychiatric Illness Medical disorder Social factors (Unemployed, single,")
12 Insomnia Risk Factors: Female 2:1 (?More likely to report insomnia) Increasing age (? Increased likelihood of medical complaints) Stress/Anxiety (Hyper-arousal Disorder) Psychiatric Illness Medical disorder Social factors (Unemployed, single, physical inactivity) Environmental factors (noisy environment, latitude-sad)
13 Insomnia Treatments: CHEMICAL Herbal Allopathic BEHAVIOURAL (CBTi) Seep hygiene Relaxation therapies Stimulus control Bed Restriction Therapy
14 Insomnia Allopathic Use short acting hypnotics for short term treatment in low dose Use sedating antidepressants in full doses for insomnia associated with depression
15 Brief Questions: Insomnia Evaluation: The three P s - Predisposing Factors Genetics, Personality type, Social Pressures - Precipitating Factors Stressful life event(s). Trigger for insomnia. - Perpetuating Factors. Compensatory strategies. eg Spending longer in bed. Staying in bed. Monitoring sleep. Alcohol use
16 Insomnia Behavioral Treatments CBTi Sleep Hygiene Relaxation therapies / Mindfulness meditation Stimulus Control Sleep (Bed) Restriction Therapy
17 Sleep Hygiene To Provide information about lifestyle, and environment that might interfere with sleep, or promote better sleep. These strategies are important as a baseline, and should be combined with the other treatments. As a sole therapy, it is not effective for the more severe insomnia, but should be addressed in therapy.
18 Sleep Hygiene - Avoid stimulants - Exercise regularly - Caffeine (5-8 hour half life) - Cigarettes - Alcohol (initially sedative, later stimulant) - Psychoactive Drugs - Allow at least 1 hr relaxation time to unwind before bedtime - Bedroom environment should be quiet, dark and comfortable and ~ C - Avoid clock watching
19 Relaxation Therapies - Abdominal breathing - Progressive muscle relaxation - Visualisation - Mindfulness meditation (
20 Stimulus Control for those with insomnia Stimulus Control is based on classical conditioned response to certain stimuli. This involves strengthening the relationship between bed and sleep, and breaking the negative relationship between bed and anxiety and wakefulness Important and Effective
21 STIMULUS CONTROL Go to bed when sleepy Do not watch TV, read, eat or worry while in bed Do not nap during the day Set regular wake up/get up time including weekends Get out of bed if unable to fall asleep in minutes or anxious Return to bed after mins, Repeat as often as necessary
22 Bed Restriction Therapy for those with insomnia Sleep restriction therapy is designed to improve sleep consolidation and sleep efficiency. This is achieved by initially increasing the homeostatic drive to sleep. Sleep efficiency is improved. Time in bed can then be increased The most difficult, but the most effective
23 BED RESTRICTION THERAPY Average the time asleep over 2 weeks Restrict time in bed to that time. (never less than 5hr sleep opportunity) Increase time in bed slowly when sleeping is consolidated to >85%, Stay the same if 80%-85% Reduce time in bed if <80%.
24 Brief Solutions: Insomnia - Journaling - Improve sleep efficiency Later to bed Stimulus Control Bed restriction - Avoid clock-watching - Remove electronic devices from the bedroom - Sleep Diary

25 Tempting! Familiar?
26 Snoring Related Complaints Drives wife from bedroom Girlfriend won t marry me Shakes entire house Ask me to leave movies and church Has had to leave boat so friends could sleep Fall asleep at traffic lights waiting for red light to change
27
28 Consequences of Sleep Apnoea Poor quality Sleep resulting in :- Excessive Daytime Sleepiness.( EDS) Impaired cognitive function. Poor concentration Learning and Memory difficulties Depression Personality changes Hyperactivity in children Road Accidents
29 Risk Factors for Sleep Apnoea Male: Female 2 : 1 Increasing age Body Mass Index > 30 Neck Circumference > 42cm ( M) 38cm (F) Alcohol ( > 2 units) Smoking Post Menopausal Women Sleeping Pills But: 20% of those with sleep apnoea are not overweight
30 Consequences of Sleep Apnoea 1. Daytime fatigue, especially sleepiness 2. Bed partner sleep disturbance 3. Cardiovascular complications
31 History Taking (If Possible With Partner) Sleepy vs non-sleepy (Epworth Sleepiness Scale) Smoking / alcohol Recent weight gain Family history Consistency of snoring Every night Every position Periods of apnoea
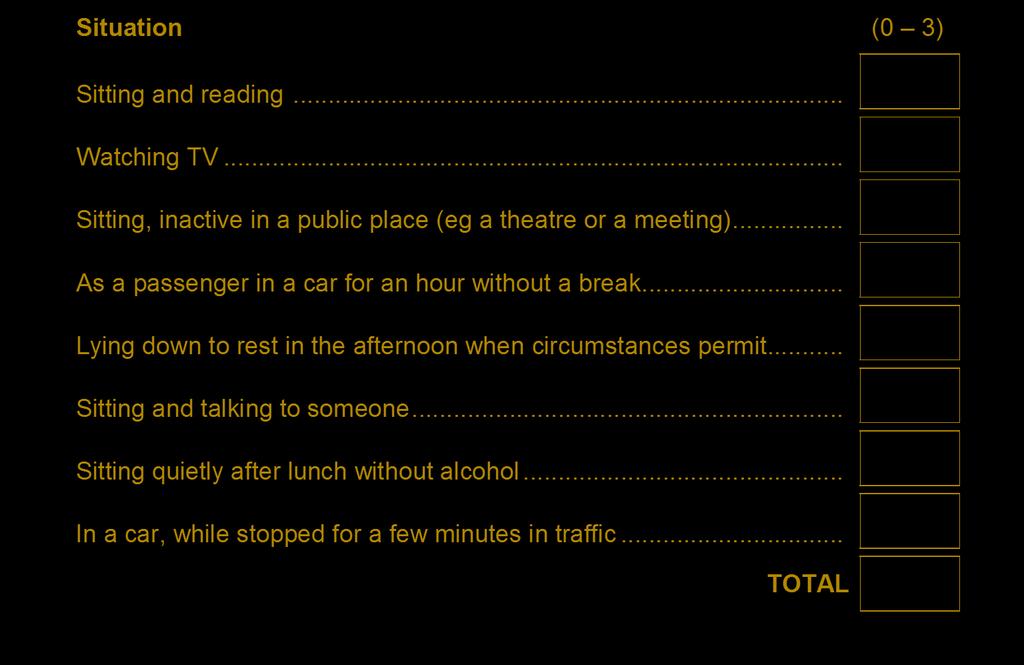
32 The Epworth Sleepiness Scale How likely are you to doze off or fall asleep in the following situations, in contrast to just feeling tired? This refers to your usual way of life in recent times. Even if you have not done some of these things recently, try to work out how they would have affected you. Use the following scale to choose the most appropriate number for each situation: 0 = would never doze 1 = slight chance of dozing 2 = moderate chance of dozing 3 = high chance of dozing
33
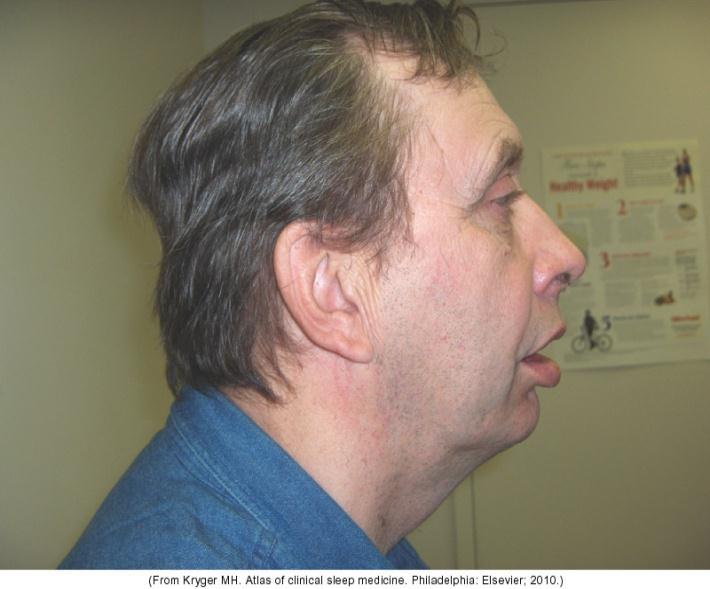
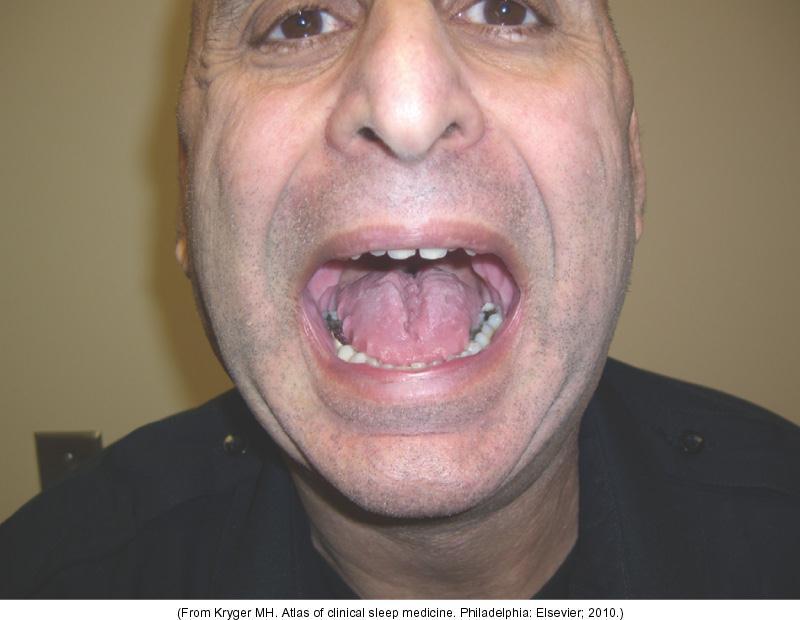
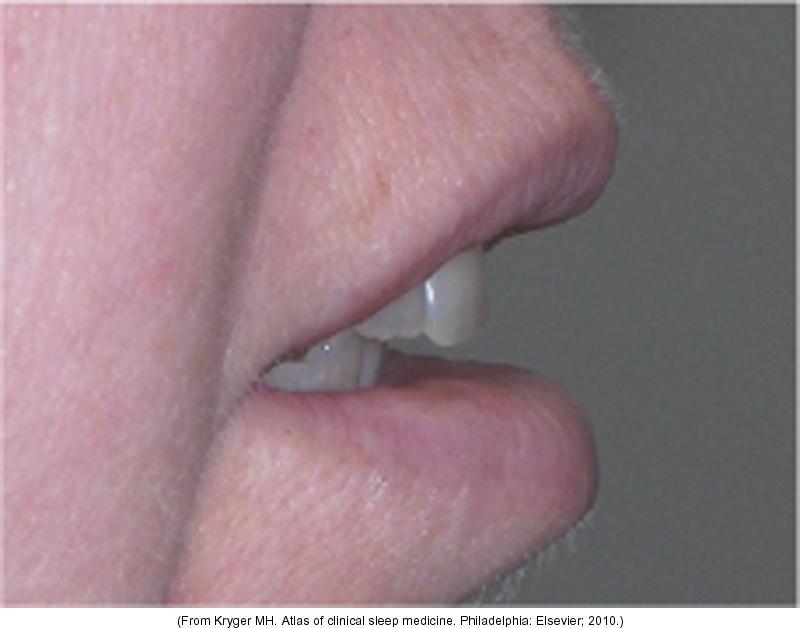
34 Examination BMI Neck circumference Tonsil size (Friedman score) Tongue size (Mallampati Score) Retrognathia / overjet Crossbite / crowded teeth / sufficient number Signs of Bruxism TMJ mobility / ability to protrude the mandible Soft palate/uvula oedema
35 Brief investigation: Snoring/OSA Overweight or Long face Thick neck Oral examination. Teeth/ Tongue/Tonsils Overnight Sleep Study

36 Brief Investigation: Snoring/OSA

37 Brief Investigation: Snoring/OSA c

38 Brief Investigation: Snoring/OSA

39 Brief Investigation: Snoring/OSA
40 Brief questions: STOP-BANG 1. Do you SNORE loudly (louder than talking or loud enough to be heard through closed doors)? 2. Do you often feel TIRED, fatigued, or sleepy during daytime? 3. Has anyone OBSERVED you stop breathing during your sleep? 4. Do you have or are you being treated for high blood PRESSURE? 5. BMI more than 35? 6. AGE over 50 years old? 7. NECK circumference > 42 cms? 8. Male GENDER? 3 yes answers: High-risk for OSA <3 yes answers: Low-risk for OSA
41 Brief questions: - Auckland Sleep Questionnaire This is longer, but covers many aspects of sleep
42 Summary 1. Sleep impacts on virtually all aspects of medical practice. 2. It may be worthwhile setting aside a separate consultation to explore insomnia. Snoring/Sleep Apnoea can be suspected, but investigation is less easy. 3. Just asking about sleep is helpful. 4. Ignore sleep and you ignore 1/3 of life!
43 Thank You Dr Alex Bartle The SLEEP WELL Clinic Throughout New Zealand
Sleep Disorders and their management
 Clinical Stream Sleep Disorders and their management Dr Alex Bartle Programme. What happens in sleep, and why bother? The effects of sleep loss. Common sleep disorders Brief (but important ) questions.
Clinical Stream Sleep Disorders and their management Dr Alex Bartle Programme. What happens in sleep, and why bother? The effects of sleep loss. Common sleep disorders Brief (but important ) questions.
The Agony or the Ecstasy. Familiar?
 The Agony or the Ecstasy Familiar? Snoring Related Complaints Drives wife from bedroom Girlfriend won t marry me Shakes entire house Ask me to leave movies and church Has had to leave boat so friends could
The Agony or the Ecstasy Familiar? Snoring Related Complaints Drives wife from bedroom Girlfriend won t marry me Shakes entire house Ask me to leave movies and church Has had to leave boat so friends could
Dr Alex Bartle. Sleep Well Clinic
 Dr Alex Bartle Sleep Well Clinic Overview of Sleep Disorders Sleep: Why bother. Effect of Poor Quality or reduced Quantity of Sleep Common Sleep Disorders Management of Insomnia Medication vs CBTi Conclusion
Dr Alex Bartle Sleep Well Clinic Overview of Sleep Disorders Sleep: Why bother. Effect of Poor Quality or reduced Quantity of Sleep Common Sleep Disorders Management of Insomnia Medication vs CBTi Conclusion
Insomnia % of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences)
") 10-15% of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences) 30 40% of adults complain of insomnia symptoms only 95% experience insomnia at some time in their
10-15% of adults suffer from chronic and severe insomnia (Complaints of insomnia with daytime consequences) 30 40% of adults complain of insomnia symptoms only 95% experience insomnia at some time in their
Dr Alex Bartle. Director Sleep Well Clinic
 Dr Alex Bartle Director Sleep Well Clinic 1 Fatigue in the Workforce The structure of sleep Fatigue and sleep Consequences of fatigue Management of Shiftwork Conclusion Sleep Architecture REM NREM Rapid
Dr Alex Bartle Director Sleep Well Clinic 1 Fatigue in the Workforce The structure of sleep Fatigue and sleep Consequences of fatigue Management of Shiftwork Conclusion Sleep Architecture REM NREM Rapid
Dr Alex Bartle. Medical Director Sleep Well Clinic Christchurch
 Dr Alex Bartle Medical Director Sleep Well Clinic Christchurch 8:30-9:25 WS #191: Sleep Disorders in The Elderly 9:35-10:30 WS #203: Sleep Disorders in The Elderly (Repeated) REM - Rapid Eye Movement
Dr Alex Bartle Medical Director Sleep Well Clinic Christchurch 8:30-9:25 WS #191: Sleep Disorders in The Elderly 9:35-10:30 WS #203: Sleep Disorders in The Elderly (Repeated) REM - Rapid Eye Movement
PULMONARY & CRITICAL CARE CONSULTANTS OF AUSTIN 1305 West 34 th Street, Suite 400, Austin, TX Phone: Fax:
 Name: Sex: Age: Date: Date of Birth Height Weight Neck size Referring Physician: Primary Care MD: Main Sleep Complaint(s) trouble falling asleep trouble remaining asleep excessive sleepiness during the
Name: Sex: Age: Date: Date of Birth Height Weight Neck size Referring Physician: Primary Care MD: Main Sleep Complaint(s) trouble falling asleep trouble remaining asleep excessive sleepiness during the
Associated Neurological Specialties and Sleep Disorder Center
 Sleep Center Questionnaire Name: Sex: Age: Date: Date of Birth: Height: Weight: Neck Size: Primary Care Physician: Referring Physician: Main Sleep Issues/Complaints Trouble falling asleep Trouble staying
Sleep Center Questionnaire Name: Sex: Age: Date: Date of Birth: Height: Weight: Neck Size: Primary Care Physician: Referring Physician: Main Sleep Issues/Complaints Trouble falling asleep Trouble staying
130 Preston Executive Drive Cary, NC Ph(919) Fax(919) Page 1 of 6. Patient History
 Fax(919) Page 1 of 6. Patient History") 130 Preston Executive Drive Cary, NC 27513 Ph(919)462-8081 Fax(919)462-8082 www.parkwaysleep.com Page 1 of 6 Patient History *Please fill out in dark BLACK INK only. General Information Name Sex: Male
130 Preston Executive Drive Cary, NC 27513 Ph(919)462-8081 Fax(919)462-8082 www.parkwaysleep.com Page 1 of 6 Patient History *Please fill out in dark BLACK INK only. General Information Name Sex: Male
Sleep Questionnaire Name: Sex: Age: Da te: Da te of birth: Height: Weight: Neck siz e: Ref erring Physician: Primary Car e MD:
 www.myvcmf.com 1133 E. Stanley Blvd., Suite 101 Livermore, CA 94550 925 454-4280 5725 W. Las Positas Blvd., Suite 110 Pleasanton, CA 94588 925-416-6767 Sleep Questionnaire Name: Sex: Age: Da te: Da te
www.myvcmf.com 1133 E. Stanley Blvd., Suite 101 Livermore, CA 94550 925 454-4280 5725 W. Las Positas Blvd., Suite 110 Pleasanton, CA 94588 925-416-6767 Sleep Questionnaire Name: Sex: Age: Da te: Da te
SLEEP HISTORY QUESTIONNAIRE
 Date of birth: Today s date: Dear Patient: SLEEP HISTORY QUESTIONNAIRE Thank you for taking the time to fill out a sleep history questionnaire. This will help our healthcare team to provide the best possible
Date of birth: Today s date: Dear Patient: SLEEP HISTORY QUESTIONNAIRE Thank you for taking the time to fill out a sleep history questionnaire. This will help our healthcare team to provide the best possible
Dr Alex Bartle. Medical Director Sleep Well Clinic Christchurch
 Dr Alex Bartle Medical Director Sleep Well Clinic Christchurch 11:00-11:55 WS #113: Circadian Sleep Disorders 12:05-13:00 WS #125: Circadian Sleep Disorders (Repeated) Overview The Structure of Sleep
Dr Alex Bartle Medical Director Sleep Well Clinic Christchurch 11:00-11:55 WS #113: Circadian Sleep Disorders 12:05-13:00 WS #125: Circadian Sleep Disorders (Repeated) Overview The Structure of Sleep
I would like for my patient to be seen in Sleep Medicine consultation and managed by the sleep physician. Yes No
 701 E. COUNTY LINE ROAD, SUITE 207. GREENWOOD, IN. 46143 OFFICE317-887-6400 FAX 317-887-6500 indianasleepcenter.com REFERRAL FOR SLEEP EVALUATION Patient Name:_ Phone: I would like for my patient to be
701 E. COUNTY LINE ROAD, SUITE 207. GREENWOOD, IN. 46143 OFFICE317-887-6400 FAX 317-887-6500 indianasleepcenter.com REFERRAL FOR SLEEP EVALUATION Patient Name:_ Phone: I would like for my patient to be
HOW TO DEAL WITH SLEEP PROBLEMS
 The Handbook on Successful Ageing HOW TO DEAL WITH SLEEP PROBLEMS Up to 50% of the elderly complain of insomnia, but although such complaints are prevalent and are often accompanied by higher rates of
The Handbook on Successful Ageing HOW TO DEAL WITH SLEEP PROBLEMS Up to 50% of the elderly complain of insomnia, but although such complaints are prevalent and are often accompanied by higher rates of
Denver, CO Welcome Packet
 Fax: (303) 957-5414 or 720-542-8699 For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 1210 S Parker Road, Suite 101, Denver,
Fax: (303) 957-5414 or 720-542-8699 For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 1210 S Parker Road, Suite 101, Denver,
Littleton, CO Welcome Packet 8151 Southpark Lane, Suite 200 Littleton, CO 80120
 Littleton, CO Welcome Packet For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 8151 Southpark Lane, Suite 200, Littleton,
Littleton, CO Welcome Packet For any after-hours questions, please call (303) 956-5145 Dear Mountain Sleep Patient, You have been scheduled for a sleep study at 8151 Southpark Lane, Suite 200, Littleton,
WHY CAN T I SLEEP? Deepti Chandran, MD
 WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
WHY CAN T I SLEEP? Deepti Chandran, MD Sleep and Aging How does sleep change as we age? Do we need less sleep as we get older? Can a person expect to experience more sleep problems or have a sleep disorder
Emergency Contact Information Name: Phone: Address: Employer Information Employer Name: Address/Street: City: Zip: Phone: Fax:
 SUNSET SLEEP LABS PATIENT INFORMATION FORM Patient Information Name: Sex: M F Date of Birth: Address/Street: City: Zip: Phone: Alt Phone: Parent/Guardian: Phone: Social Security Number: Drivers License:
SUNSET SLEEP LABS PATIENT INFORMATION FORM Patient Information Name: Sex: M F Date of Birth: Address/Street: City: Zip: Phone: Alt Phone: Parent/Guardian: Phone: Social Security Number: Drivers License:
Patient Adult Information History
 Patient Adult Information History Patient name: Age: Date: What is the main reason for today s evaluation? Infant History Birth delivery: Normal C-section Delayed Epidural Premature: No Yes If yes, how
Patient Adult Information History Patient name: Age: Date: What is the main reason for today s evaluation? Infant History Birth delivery: Normal C-section Delayed Epidural Premature: No Yes If yes, how
Treating Insomnia in Primary Care. Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team
 Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
Treating Insomnia in Primary Care Judith R. Davidson Ph.D., C. Psych. Kingston Family Health Team jdavidson@kfhn.net Disclosure statement Nothing to disclose A ruffled mind makes a restless pillow. ~ Charlotte
Psychological Sleep Services Sleep Assessment
 Psychological Sleep Services Sleep Assessment Name Date **************************************************** Insomnia Severity Index For each question, please CIRCLE the number that best describes your
Psychological Sleep Services Sleep Assessment Name Date **************************************************** Insomnia Severity Index For each question, please CIRCLE the number that best describes your
Maintenance for Wakefulness Testing (MWT)
") SLEEP DISORDERS CENTER St. Joseph Mercy Ann Arbor 5305 Elliott Drive, Ypsilanti, MI 48197 734-712-2276 / Fax 734-712-2967 Maintenance for Wakefulness Testing (MWT) Dear, Your Maintenance for Wakefulness
SLEEP DISORDERS CENTER St. Joseph Mercy Ann Arbor 5305 Elliott Drive, Ypsilanti, MI 48197 734-712-2276 / Fax 734-712-2967 Maintenance for Wakefulness Testing (MWT) Dear, Your Maintenance for Wakefulness
Patient History & Sleep Questionnaire
 Patient History & Sleep Questionnaire Patient Full Name: Nick Name: Birth date: Age: Sex: Height: Current Weight: Weight Five Years Ago: Peak Lifetime Weight: Marital Status: Single Married Divorced Widowed
Patient History & Sleep Questionnaire Patient Full Name: Nick Name: Birth date: Age: Sex: Height: Current Weight: Weight Five Years Ago: Peak Lifetime Weight: Marital Status: Single Married Divorced Widowed
Balboa Island Dentistry (949)
") Do You Snore? Are you always tired? Snoring is no laughing matter! It may be more than an annoying habit. It may be a sign of. How well do you sleep? Just about everyone snores occasionally. Even a baby
Do You Snore? Are you always tired? Snoring is no laughing matter! It may be more than an annoying habit. It may be a sign of. How well do you sleep? Just about everyone snores occasionally. Even a baby
604 NORTH ACADIA ROAD, Suite 210 THIBODAUX, LA SLEEP HISTORY QUESTIONNAIRE
 604 NORTH ACADIA ROAD, Suite 210 THIBODAUX, LA 70301 985-493-4759 SLEEP HISTORY QUESTIONNAIRE DATE: / / NAME: AGE (First) (Middle) (Last) ADDRESS: (Street) (City) (State) (Zip) PHONE: Home( ) Work:( )
604 NORTH ACADIA ROAD, Suite 210 THIBODAUX, LA 70301 985-493-4759 SLEEP HISTORY QUESTIONNAIRE DATE: / / NAME: AGE (First) (Middle) (Last) ADDRESS: (Street) (City) (State) (Zip) PHONE: Home( ) Work:( )
Not Sleepy HO Q1 D2 Q3 Q4 ]5 D6 j7 Q8 Q9 Q10 Extremely Sleepy
![Not Sleepy HO Q1 D2 Q3 Q4 ]5 D6 j7 Q8 Q9 Q10 Extremely Sleepy](/thumbs/96/127246551.jpg "Not Sleepy HO Q1 D2 Q3 Q4 ]5 D6 j7 Q8 Q9 Q10 Extremely Sleepy") Health Benefits Employee Services HBE Preventive Health - Sleep Assessment Form Please bring your completed assessment form to your appointment. To schedule an appointment please call 505 844-HBES (4237).
Health Benefits Employee Services HBE Preventive Health - Sleep Assessment Form Please bring your completed assessment form to your appointment. To schedule an appointment please call 505 844-HBES (4237).
Maintenance for Wakefulness Testing (MWT)
") Maintenance for Wakefulness Testing (MWT) Dear, Your Maintenance for Wakefulness Testing (MWT) will begin on the morning of at 7 a.m. and will end at 5 p.m. ARRIVAL TIME: If you are not able to arrive
Maintenance for Wakefulness Testing (MWT) Dear, Your Maintenance for Wakefulness Testing (MWT) will begin on the morning of at 7 a.m. and will end at 5 p.m. ARRIVAL TIME: If you are not able to arrive
WHAT YOU NEED TO KNOW ABOUT SLEEP APNEA
 WHAT YOU NEED TO KNOW ABOUT SLEEP APNEA Wayne Driscoll Clinical Education Specialist 2 SLEEP APNEA IN THE NEWS Carrie Fisher died from sleep apnea, other factors, coroner says USA Today NJ Transit engineer
WHAT YOU NEED TO KNOW ABOUT SLEEP APNEA Wayne Driscoll Clinical Education Specialist 2 SLEEP APNEA IN THE NEWS Carrie Fisher died from sleep apnea, other factors, coroner says USA Today NJ Transit engineer
Baptist Health Floyd 1850 State Street New Albany, IN Sleep Disorders Center Lung & Sleep Specialists. Date of Birth: Age:
 Page 1 of 7 GENERAL INFORMATION Name: Date of Birth: Age: Social Security #: Sex: Height: Weight: Address: City: State: Zip: Home Phone: Cell Phone: Work Phone: Employer s Name: Marital Status: Married
Page 1 of 7 GENERAL INFORMATION Name: Date of Birth: Age: Social Security #: Sex: Height: Weight: Address: City: State: Zip: Home Phone: Cell Phone: Work Phone: Employer s Name: Marital Status: Married
Sleep History Questionnaire B/P / Pulse: Neck Circum Wgt: Pulse Ox
 2700 Campus Drive, Ste 100 2412 E 117 th Street Plymouth, MN 55441 Burnsville, MN 55337 P 763.519.0634 F 763.519.0636 P 952.431.5011 F 952.431.5013 www.whitneysleepcenter.com Sleep History Questionnaire
2700 Campus Drive, Ste 100 2412 E 117 th Street Plymouth, MN 55441 Burnsville, MN 55337 P 763.519.0634 F 763.519.0636 P 952.431.5011 F 952.431.5013 www.whitneysleepcenter.com Sleep History Questionnaire
Sleep History Questionnaire. Sleep Disorders Center Duke University Medical Center. General Information. Age: Sex: F M (select one)
") Sleep History Questionnaire Sleep Disorders Center Duke University Medical Center Part I: General Information Name: Address: Date: Phone: Age: Sex: F M (select one) Education (years of school): Occupation:
Sleep History Questionnaire Sleep Disorders Center Duke University Medical Center Part I: General Information Name: Address: Date: Phone: Age: Sex: F M (select one) Education (years of school): Occupation:
BMI: Family physician : Neck circumference (cm) Hypertension + 4 cm Snoring + 3 cm Witnessed apnea + 3cm Total
 Hypertension + 4 cm Snoring + 3 cm Witnessed apnea + 3cm Total") Last and first names: F M Date: Date of birth: / / YYYY MM DD Weight: kg /lbs Profession/job: Height: _ cm /ft.in. BMI:_ Family physician : ANC (adjusted neck circumference) : Neck circumference (cm) Hypertension
Last and first names: F M Date: Date of birth: / / YYYY MM DD Weight: kg /lbs Profession/job: Height: _ cm /ft.in. BMI:_ Family physician : ANC (adjusted neck circumference) : Neck circumference (cm) Hypertension
OSA - Obstructive sleep apnoea What you need to know if you think you might have OSA
 OSA - Obstructive sleep apnoea What you need to know if you think you might have OSA Obstructive sleep apnoea, or OSA, is a breathing problem that happens when you sleep. It can affect anyone men, women
OSA - Obstructive sleep apnoea What you need to know if you think you might have OSA Obstructive sleep apnoea, or OSA, is a breathing problem that happens when you sleep. It can affect anyone men, women
Sleep Center. Have you had a previous sleep study? Yes No If so, when and where? Name of facility Address
 Patient Label For office use only Appt date: Clinician: Sleep Center Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 Leading
Patient Label For office use only Appt date: Clinician: Sleep Center Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 Leading
Let s Sleep On It. Session Overview. Let s Sleep On It. Welcome and Introductions Presenter: Rita Piper, VP of Wellness
 Let s Sleep On It Let s Sleep On It Welcome and Introductions Presenter: Rita Piper, VP of Wellness Session Overview Why Sleep is so Important Types of Sleep Common Sleep Disruptors Sleep Disorders Tips
Let s Sleep On It Let s Sleep On It Welcome and Introductions Presenter: Rita Piper, VP of Wellness Session Overview Why Sleep is so Important Types of Sleep Common Sleep Disruptors Sleep Disorders Tips
SLEEP DISORDERS CENTER QUESTIONNAIRE
 Carteret Health Care Patient's name DOB Gender: M F Date of Visit _ Referring physicians: Primary care providers: Please complete the following questionnaire by filling in the blanks and placing a check
Carteret Health Care Patient's name DOB Gender: M F Date of Visit _ Referring physicians: Primary care providers: Please complete the following questionnaire by filling in the blanks and placing a check
A GUIDE TO BETTER SLEEP. Prepared by Dr Grant Willson Director, Sleep and Lifestyle Solutions
 A GUIDE TO BETTER SLEEP Prepared by Dr Grant Willson Director, Sleep and Lifestyle Solutions A GUIDE TO BETTER SLEEP Good sleep is one of life s pleasures. Most people can think of a time when they slept
A GUIDE TO BETTER SLEEP Prepared by Dr Grant Willson Director, Sleep and Lifestyle Solutions A GUIDE TO BETTER SLEEP Good sleep is one of life s pleasures. Most people can think of a time when they slept
HEALTHY LIFESTYLE, HEALTHY SLEEP. There are many different sleep disorders, and almost all of them can be improved with lifestyle changes.
 HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep disorders, and almost all of them can be improved with lifestyle changes. HEALTHY LIFESTYLE, HEALTHY SLEEP There are many different sleep
Get on the Road to Better Health Recognizing the Dangers of Sleep Apnea
 Get on the Road to Better Health You Will Learn About The importance and benefits of sleep Sleep deprivation and its consequences The prevalence, symptoms, and treatments for major sleep problems/ disorders
Get on the Road to Better Health You Will Learn About The importance and benefits of sleep Sleep deprivation and its consequences The prevalence, symptoms, and treatments for major sleep problems/ disorders
SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS
 SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS Laugh and the world laughs with you; snore and you sleep alone. These words by novelist Anthony Vergess ring true with all too many
SNORING AND OBSTRUCTIVE SLEEP APNOEA WAYS TO DEAL WITH THESE PROBLEMS Laugh and the world laughs with you; snore and you sleep alone. These words by novelist Anthony Vergess ring true with all too many
SLEEP SCREENING QUESTIONNAIRE
 Patient Information 433 W. University Dr. Rochester, MI 48307 www.rochesteradvanceddentistry.com +1 248 656-2020 SLEEP SCREENING QUESTIONNAIRE Name: DOB: Age: Address: Employer: SS# Home Phone: Work Phone:
Patient Information 433 W. University Dr. Rochester, MI 48307 www.rochesteradvanceddentistry.com +1 248 656-2020 SLEEP SCREENING QUESTIONNAIRE Name: DOB: Age: Address: Employer: SS# Home Phone: Work Phone:
General Information. Name Age Date of Birth. Address Apt. # City State Zip. Home Phone Work Phone. Social Security Number Marital Status
 Accredited Member Center of The American Academy of Sleep Medicine 400 Riverside Drive, Suite 1500, Bourbonnais, IL 60914 Phone (815) 933-2874 Fax (815) 939-9413 www.riversidemc.net/sleep General Information
Accredited Member Center of The American Academy of Sleep Medicine 400 Riverside Drive, Suite 1500, Bourbonnais, IL 60914 Phone (815) 933-2874 Fax (815) 939-9413 www.riversidemc.net/sleep General Information
Managing Sleep Problems after Cancer
 Managing Sleep Problems after Cancer For cancer survivors Read this resource to learn about: What a sleep problem is What causes it What you can do to improve your sleep When to talk to your doctor Please
Managing Sleep Problems after Cancer For cancer survivors Read this resource to learn about: What a sleep problem is What causes it What you can do to improve your sleep When to talk to your doctor Please
PATIENT NAME: M.R. #: ACCT #: HOME TEL: WORK TEL: AGE: D.O.B.: OCCUPATION: HEIGHT: WEIGHT: NECK SIZE: GENDER EMERGENCY CONTACT: RELATIONSHIP: TEL:
 SLEEP DISORDERS INSTITUTE HOSPITAL: DePaul Building Street Address City, State Zip Tel: (202) 555-1212 Fax: (202) 555-1212 SLEEP QUESTIONNAIRE PATIENT NAME: M.R. #: ACCT #: STREET ADDRESS: CITY: STATE:
SLEEP DISORDERS INSTITUTE HOSPITAL: DePaul Building Street Address City, State Zip Tel: (202) 555-1212 Fax: (202) 555-1212 SLEEP QUESTIONNAIRE PATIENT NAME: M.R. #: ACCT #: STREET ADDRESS: CITY: STATE:
PATIENT DEMOGRAPHICS
 PATIENT DEMOGRAPHICS NPSG CPAP CPAP Retitration Split Night PATIENT INFORMATION: Name: Last First Middle Initial Address: City: State: Zip: Social Security #: DOB: Gender: Age: Phone Number: Cell: Work:
PATIENT DEMOGRAPHICS NPSG CPAP CPAP Retitration Split Night PATIENT INFORMATION: Name: Last First Middle Initial Address: City: State: Zip: Social Security #: DOB: Gender: Age: Phone Number: Cell: Work:
Instructions. If you make a mistake, put an "X" over the checkmark. Then put a checkmark in the correct box and draw a circle around that box.
 SLEEP HEART HEALTH STUDY SLEEP HABITS AND LIFESTYLE QUESTIONNAIRE Instructions Thank you for taking time to fill out the enclosed Sleep Habits Questionnaire. Please fill out the form completely. You may
SLEEP HEART HEALTH STUDY SLEEP HABITS AND LIFESTYLE QUESTIONNAIRE Instructions Thank you for taking time to fill out the enclosed Sleep Habits Questionnaire. Please fill out the form completely. You may
Patient Information. Name: Date of Birth: Address: Number & Street City State Zip Code. Home Number: ( ) Cell Number: ( )
 Cell Number: ( )") Patient Information Name: Date of Birth: Age: Address: Number & Street City State Zip Code Home Number: ( ) Cell Number: ( ) Social Security Number: Marital Status: Religion: Race: Height: Weight: Sex:
Patient Information Name: Date of Birth: Age: Address: Number & Street City State Zip Code Home Number: ( ) Cell Number: ( ) Social Security Number: Marital Status: Religion: Race: Height: Weight: Sex:
Chronic Insomnia: DSM - V. Insomnia DSM - V. Patient Symptoms. Insomnia: Assessment and Overview of Management. Insomnia Management in the Digital Age
 Insomnia Management in the Digital Age Dr Anup Desai Sleep & Respiratory Medicine MBBS (syd), PhD (syd), FRACP Senior Staff Specialist, POW Hospital Medical Director, Sydney Sleep Centre Senior Lecturer,
Insomnia Management in the Digital Age Dr Anup Desai Sleep & Respiratory Medicine MBBS (syd), PhD (syd), FRACP Senior Staff Specialist, POW Hospital Medical Director, Sydney Sleep Centre Senior Lecturer,
THE PERMANENTE MEDICAL GROUP
 Patient label here THE PERMANENTE MEDICAL GROUP Division of Sleep Medicine COMPLETED BY: PARENT/GUARDIAN CHILD/ADOLESCENT Age: Height: Weight: PEDIATRIC SLEEP QUESTIONNAIRE Thank you completing this questionnaire.
Patient label here THE PERMANENTE MEDICAL GROUP Division of Sleep Medicine COMPLETED BY: PARENT/GUARDIAN CHILD/ADOLESCENT Age: Height: Weight: PEDIATRIC SLEEP QUESTIONNAIRE Thank you completing this questionnaire.
New Patient Sleep Intake
 New Patient Sleep Intake Name: Date of Birth: Primary Care Physician: Date of Visit: Referring Physician and/or Other Physicians: Retail Pharmacy: Mail Order Pharmacy: Address: Mail Order Phone #: Phone
New Patient Sleep Intake Name: Date of Birth: Primary Care Physician: Date of Visit: Referring Physician and/or Other Physicians: Retail Pharmacy: Mail Order Pharmacy: Address: Mail Order Phone #: Phone
Beyond Sleep Hygiene: Behavioral Approaches to Insomnia
 Beyond Sleep Hygiene: Behavioral Approaches to Insomnia Rocky Garrison, PhD, CBSM Damon Michael Williams, RN, PMHNP-BC In House Counseling Laughing Heart LLC 10201 SE Main St. 12 SE 14 th Ave. Suite 10
Beyond Sleep Hygiene: Behavioral Approaches to Insomnia Rocky Garrison, PhD, CBSM Damon Michael Williams, RN, PMHNP-BC In House Counseling Laughing Heart LLC 10201 SE Main St. 12 SE 14 th Ave. Suite 10
Sleep Apnoea. Introduction Symptoms Causes Obtaining a Diagnosis Treatment Complications
 The most common forms of sleep apnoea are normally referred to as obstructive sleep apnoea (OSA) and relate to a condition which causes interruptions in breathing during sleep. People with obstructive
The most common forms of sleep apnoea are normally referred to as obstructive sleep apnoea (OSA) and relate to a condition which causes interruptions in breathing during sleep. People with obstructive
Managing Insomnia: an example sequence of CBT-based sessions for sleep treatment
 Managing Insomnia: an example sequence of CBT-based sessions for sleep treatment Session 1: Introduction and sleep assessment -Assess sleep problem (option: have client complete 20-item sleep questionnaire).
Managing Insomnia: an example sequence of CBT-based sessions for sleep treatment Session 1: Introduction and sleep assessment -Assess sleep problem (option: have client complete 20-item sleep questionnaire).
YOU REALLY NEED TO SLEEP: Several methods to improve your sleep
 YOU REALLY NEED TO SLEEP: Several methods to improve your sleep Sleep is essential to our well-being. When humans fail to get good sleep over a period of time, numerous problems can occur. CAN T SLEEP!!
YOU REALLY NEED TO SLEEP: Several methods to improve your sleep Sleep is essential to our well-being. When humans fail to get good sleep over a period of time, numerous problems can occur. CAN T SLEEP!!
Sleep Disorders Diagnostic Center 9733 Healthway Drive, Berlin, MD , ext. 5118
 Sleep Questionnaire *Please complete the following as accurate as possible. Please bring your completed questionnaire, insurance card, photo ID, Pre-Authorization and/or Insurance referral form, and all
Sleep Questionnaire *Please complete the following as accurate as possible. Please bring your completed questionnaire, insurance card, photo ID, Pre-Authorization and/or Insurance referral form, and all
Occupation: Usual Work Hours/Days: Referring Physician: Family Physician (PCP): Marital status: Single Married Divorced Widowed
: Marital status: Single Married Divorced Widowed") Name Social Security No. Last First MI Address Phone No. ( ) City State Zip Secondary No. ( ) Date of Birth Sex (M/F) Race Email County Primary Care Marital Status Single Divorced Married Widowed Employer
Name Social Security No. Last First MI Address Phone No. ( ) City State Zip Secondary No. ( ) Date of Birth Sex (M/F) Race Email County Primary Care Marital Status Single Divorced Married Widowed Employer
SLEEP QUESTIONNAIRE. Name: Sex: Age: Date: DOB: / / SSN: - - Address: Referring Physician: Family Physician: Height: Weight: Neck Size: Phone:
 SLEEP QUESTIONNAIRE Name: Sex: Age: Date: DOB: / / SSN: - - Address: Referring Physician: Family Physician: Height: Weight: Neck Size: Phone: Please fill in the blanks, and check appropriate areas on the
SLEEP QUESTIONNAIRE Name: Sex: Age: Date: DOB: / / SSN: - - Address: Referring Physician: Family Physician: Height: Weight: Neck Size: Phone: Please fill in the blanks, and check appropriate areas on the
Sleep Symptoms & History
 Sleep Symptoms & History In your own words, please tell us what brings you to the sleep clinic today? How long have you been experiencing your sleep problems? yrs. mos. To give us a precise understanding
Sleep Symptoms & History In your own words, please tell us what brings you to the sleep clinic today? How long have you been experiencing your sleep problems? yrs. mos. To give us a precise understanding
Sleep Self-Assessment
 We are pleased you are taking the time to become more aware of your sleep patterns and discover strategies for improving your sleep. You deserve to get a good night s sleep we re here to help! The following
We are pleased you are taking the time to become more aware of your sleep patterns and discover strategies for improving your sleep. You deserve to get a good night s sleep we re here to help! The following
Huron Medical Sleep Center Saad S. Ahmad, MD
 Authorization and Consent for Sleep Testing I authorize the release of any medical information necessary to the durable medical equipment company for therapy, if applicable. I authorize the use of audio
Authorization and Consent for Sleep Testing I authorize the release of any medical information necessary to the durable medical equipment company for therapy, if applicable. I authorize the use of audio
An Introduction to Identifying and Treating Sleep Disorders in Adults
 An Introduction to Identifying and Treating Sleep Disorders in Adults REFERENCES/RESOURCES TOOLS & MEASURES: SLEEP DIARY: Carney, C., et al. (2012). The Consensus Sleep Diary: Standardizing prospective
An Introduction to Identifying and Treating Sleep Disorders in Adults REFERENCES/RESOURCES TOOLS & MEASURES: SLEEP DIARY: Carney, C., et al. (2012). The Consensus Sleep Diary: Standardizing prospective
Sleep Management
 www.working-minds.org.uk Sleep Management Working Minds UK: Dovey Wilday Consultancy Contact: 07941 196379 SLEEP MANAGEMENT Sleep problems occur frequently in people suffering from depression/anxiety.
www.working-minds.org.uk Sleep Management Working Minds UK: Dovey Wilday Consultancy Contact: 07941 196379 SLEEP MANAGEMENT Sleep problems occur frequently in people suffering from depression/anxiety.
THE SLEEP DISORDERS CLINIC Medical Director: Dr Raymond Gottschalk PATIENT QUESTIONNAIRE
 THE SLEEP DISORDERS CLINIC Medical Director: Dr Raymond Gottschalk 55 Frid Street, Unit 7, Hamilton, Ontario L8P 4M3 Phone:905-529-2259 Fax: 905-529-2262 282 Linwell Road, Suite 118, St. Catharines, Ontario
THE SLEEP DISORDERS CLINIC Medical Director: Dr Raymond Gottschalk 55 Frid Street, Unit 7, Hamilton, Ontario L8P 4M3 Phone:905-529-2259 Fax: 905-529-2262 282 Linwell Road, Suite 118, St. Catharines, Ontario
VCU CENTER FOR SLEEP MEDICINE NEW PATIENT QUESTIONNAIRE
 VCU CENTER FOR SLEEP MEDICINE NEW PATIENT QUESTIONNAIRE Name:_ DOB: MR#: Date: Sex: Age: Height: Referring physician: Primary care physician: What is your primary sleep problem? Please explain any strange
VCU CENTER FOR SLEEP MEDICINE NEW PATIENT QUESTIONNAIRE Name:_ DOB: MR#: Date: Sex: Age: Height: Referring physician: Primary care physician: What is your primary sleep problem? Please explain any strange
Sleep and Traumatic Brain Injury (TBI)
") Sleep and Traumatic Brain Injury (TBI) A resource for individuals with traumatic brain injury and their supporters This presentation is based on TBI Model Systems research and was developed with support
Sleep and Traumatic Brain Injury (TBI) A resource for individuals with traumatic brain injury and their supporters This presentation is based on TBI Model Systems research and was developed with support
Sleep Questionnaire. If yes, what? If yes, how would you describe it? Please explain? If yes, what times are these?
 THE ADRENAL THYROID REVOLUTION Professional Mastermind Aviva Romm MD Sleep Questionnaire Sleep is important for musculoskeletal healing and for healthy immune function, mood, cognitive and brain function,
THE ADRENAL THYROID REVOLUTION Professional Mastermind Aviva Romm MD Sleep Questionnaire Sleep is important for musculoskeletal healing and for healthy immune function, mood, cognitive and brain function,
Sleep Medicine Questionnaire
 Please bring this completed questionnaire with you to your sleep medicine appointment. Our sleep medicine staff strives to understand your sleep symptoms, which may be complex in nature. Thank you for
Please bring this completed questionnaire with you to your sleep medicine appointment. Our sleep medicine staff strives to understand your sleep symptoms, which may be complex in nature. Thank you for
WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS
 WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS Prior to your office visit, we request that you complete this questionnaire. It asks questions not only about your sleeping habits and behavior
WELCOME TO THE NORTHSHORE UNIVERSITY HEALTHSYSTEM SLEEP CENTERS Prior to your office visit, we request that you complete this questionnaire. It asks questions not only about your sleeping habits and behavior
Sleep Questionnaire. 2. How long has this problem bothered you? My Main Sleep Complaints: - Trouble sleeping at night For how many months/ years?
 Onslow Medical Specialties Clinic Lung Diseases & Sleep Disorders Clinic Pulmonary Function Test/ CardioPulmonary Exercise Test/ Thoracic Ultrasound Methacholine Challenge Test/ Video-Flexible Laryngoscopy/
Onslow Medical Specialties Clinic Lung Diseases & Sleep Disorders Clinic Pulmonary Function Test/ CardioPulmonary Exercise Test/ Thoracic Ultrasound Methacholine Challenge Test/ Video-Flexible Laryngoscopy/
A good night s sleep
 A good night s sleep Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm A good night
A good night s sleep Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm A good night
Dr Alex Bartle. Director Sleep Well Clinic
 Dr Alex Bartle Director Sleep Well Clinic 1 Sleep Architecture REM NREM Rapid Eye Movement Non-Rapid Eye Movement Stages 1 and 2 light sleep Stages 3 and 4 deep sleep 25% REM, 50% Stage 2 and 25% stages
Dr Alex Bartle Director Sleep Well Clinic 1 Sleep Architecture REM NREM Rapid Eye Movement Non-Rapid Eye Movement Stages 1 and 2 light sleep Stages 3 and 4 deep sleep 25% REM, 50% Stage 2 and 25% stages
Sweet Dreams: The Relationship between Sleep Health and Your Weight
 Sweet Dreams: The Relationship between Sleep Health and Your Weight Jason C. Ong, PhD Associate Professor Department of Neurology Center for Circadian and Sleep Medicine Northwestern University Feinberg
Sweet Dreams: The Relationship between Sleep Health and Your Weight Jason C. Ong, PhD Associate Professor Department of Neurology Center for Circadian and Sleep Medicine Northwestern University Feinberg
Article printed from
 What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
What Are Sleep Disorders? Sleep disorders are conditions that affect how much and how well you sleep. The causes range from poor habits that keep you awake to medical problems that disrupt your sleep cycle.
Humble Dreams Sleep Center. Humble, TX 77339
 Humble Dreams Sleep Center 8901 FM 1960 Bypass West, Ste. 306 Humble, TX 77339 Dear Humble Dreams Sleep Study Patient, Thank you for allowing Humble Dreams Sleep Center to provide your sleep study as requested
Humble Dreams Sleep Center 8901 FM 1960 Bypass West, Ste. 306 Humble, TX 77339 Dear Humble Dreams Sleep Study Patient, Thank you for allowing Humble Dreams Sleep Center to provide your sleep study as requested
Faculty/Presenter Disclosure
 A Little CBT I With My Tea Please: Cognitive Behavioural Therapy for insomnia (CBT I) and Its Use In the Treatment of Sleeplessness W. Jerome Alonso, MD Medical Director, Canadian Sleep Consultants Clinical
A Little CBT I With My Tea Please: Cognitive Behavioural Therapy for insomnia (CBT I) and Its Use In the Treatment of Sleeplessness W. Jerome Alonso, MD Medical Director, Canadian Sleep Consultants Clinical
The Wellbeing Plus Course
 The Wellbeing Plus Course Resource: Good Sleep Guide The Wellbeing Plus Course was written by Professor Nick Titov and Dr Blake Dear The development of the Wellbeing Plus Course was funded by a research
The Wellbeing Plus Course Resource: Good Sleep Guide The Wellbeing Plus Course was written by Professor Nick Titov and Dr Blake Dear The development of the Wellbeing Plus Course was funded by a research
Narendra Kumar, M.D. PC Board Certified ENT Board Certified Sleep Medicine
 Narendra Kumar, M.D. PC Board Certified ENT Board Certified Sleep Medicine PATIENT DEMOGRAPHICS Who is the Physician that referred you to us? Who is the primary care Physician? Date: Do you want this report
Narendra Kumar, M.D. PC Board Certified ENT Board Certified Sleep Medicine PATIENT DEMOGRAPHICS Who is the Physician that referred you to us? Who is the primary care Physician? Date: Do you want this report
Patient Scheduled Letter Thunderbird Internal Medicine Sleep Center 5620 W. Thunderbird Rd., Suite C-1 Glendale, AZ (602)
") Patient Scheduled Letter Thunderbird Internal Medicine Sleep Center 5620 W. Thunderbird Rd., Suite C-1 Glendale, AZ 85306 (602) 938 6960 Dear Patient, Your Doctor has requested you be scheduled for a sleep
Patient Scheduled Letter Thunderbird Internal Medicine Sleep Center 5620 W. Thunderbird Rd., Suite C-1 Glendale, AZ 85306 (602) 938 6960 Dear Patient, Your Doctor has requested you be scheduled for a sleep
Section of Pediatric Sleep Medicine
 Section of Pediatric Sleep Medicine David Gozal, MD Hari Bandla, MD Date: Dear Parent or Caregiver; Thank you for your interest in the Sleep Disorders Program. The sleep clinic s standard assessment procedure
Section of Pediatric Sleep Medicine David Gozal, MD Hari Bandla, MD Date: Dear Parent or Caregiver; Thank you for your interest in the Sleep Disorders Program. The sleep clinic s standard assessment procedure
Original Sleep Hygiene Rules*
 Original Sleep Hygiene Rules* 1. Sleep as much as needed to feel refreshed and healthy during the following day, but not more. Curtailing time in bed a bit seems to solidify sleep; excessively long times
Original Sleep Hygiene Rules* 1. Sleep as much as needed to feel refreshed and healthy during the following day, but not more. Curtailing time in bed a bit seems to solidify sleep; excessively long times
PATIENT REGISTRATION PERSON TO NOTIFY IN CASE OF EMERGENCY. Name: Relationship: Phone:
 PATIENT REGISTRATION Patient's Name (Last, First, MI): Date Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: PERSON TO NOTIFY
PATIENT REGISTRATION Patient's Name (Last, First, MI): Date Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: PERSON TO NOTIFY
Contents. Page. Can t sleep 3. Insomnia 4. Sleep 5. How long should we sleep? 8. Sleep problems 9. Getting a better night s sleep 11
 I Cannot Sleep Contents Page Can t sleep 3 Insomnia 4 Sleep 5 How long should we sleep? 8 Sleep problems 9 Getting a better night s sleep 11 Treatment for insomnia 15 For more information 19 2 Can t sleep
I Cannot Sleep Contents Page Can t sleep 3 Insomnia 4 Sleep 5 How long should we sleep? 8 Sleep problems 9 Getting a better night s sleep 11 Treatment for insomnia 15 For more information 19 2 Can t sleep
PATIENT REGISTRATION PERSON TO NOTIFY IN CASE OF EMERGENCY. Name: Relationship: Phone:
 PATIENT REGISTRATION Patient's Name (Last, First, MI): Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: Employment Status:
PATIENT REGISTRATION Patient's Name (Last, First, MI): Date of Birth: Age: Sex: M / F Social Security Number: Address: Apt. # City: State: Zip: Home Number: Mobile Number: Work Number: Employment Status:
Sleep History Questionnaire
 Sleep History Questionnaire Name: DOB: Phone: Date of Consultation: Consultation is requested by: Primary care provider: _ Preferred pharmacy: Chief complaint: Please tell us why you are here: How long
Sleep History Questionnaire Name: DOB: Phone: Date of Consultation: Consultation is requested by: Primary care provider: _ Preferred pharmacy: Chief complaint: Please tell us why you are here: How long
1960 FP CENTER FOR SLEEP DISORDERS
 1960 FP CENTER FOR SLEEP DISORDERS Sleep Questionnaire Name: Date: Date of Birth: / / Age: Gender: Height: Weight: lbs. Referring Physician: Occupation: Please give a brief description of your sleep problem
1960 FP CENTER FOR SLEEP DISORDERS Sleep Questionnaire Name: Date: Date of Birth: / / Age: Gender: Height: Weight: lbs. Referring Physician: Occupation: Please give a brief description of your sleep problem
Sleeping Well. Tips for students. Presented by: Jeanette Gascho. Campus Wellness
 Sleeping Well Tips for students Presented by: Jeanette Gascho Campus Wellness In this seminar you will learn: Sleep health facts Stats about University of Waterloo students Sleep health tips Campus Wellness
Sleeping Well Tips for students Presented by: Jeanette Gascho Campus Wellness In this seminar you will learn: Sleep health facts Stats about University of Waterloo students Sleep health tips Campus Wellness
Obstructive Sleep Apnea
 Obstructive Sleep Apnea Introduction Obstructive sleep apnea is an interruption in breathing during sleep. It is caused by throat and tongue muscles collapsing and relaxing. This blocks, or obstructs,
Obstructive Sleep Apnea Introduction Obstructive sleep apnea is an interruption in breathing during sleep. It is caused by throat and tongue muscles collapsing and relaxing. This blocks, or obstructs,
Sleep Screening Questionnaire
 Version: SLPQV1 Sleep Screening Questionnaire OFFICE USE Patient ID: NAME: CURRENT DATE: / / DATE OF BIRTH: / / MALE FEMALE Referring Physician: Contact ID: Number Number #1 = the most severe symptom #1
Version: SLPQV1 Sleep Screening Questionnaire OFFICE USE Patient ID: NAME: CURRENT DATE: / / DATE OF BIRTH: / / MALE FEMALE Referring Physician: Contact ID: Number Number #1 = the most severe symptom #1
SLEEP SCREENING QUESTIONNAIRE
 SLEEP SCREENING QUESTIONNAIRE Please answer each question accurately and to the best of your knowledge, to help us obtain an accurate picture of your health and sleep issues, only this way will we be able
SLEEP SCREENING QUESTIONNAIRE Please answer each question accurately and to the best of your knowledge, to help us obtain an accurate picture of your health and sleep issues, only this way will we be able
Rediscover the power of sleep
 Rediscover the power of sleep Patient Copy Apnea solutions for all ages Mobile Sleep Services Who We Are An experienced and well trained team of sleep care professionals consisting of Registered Sleep
Rediscover the power of sleep Patient Copy Apnea solutions for all ages Mobile Sleep Services Who We Are An experienced and well trained team of sleep care professionals consisting of Registered Sleep
Huron Medical Sleep Center Saad S. Ahmad, MD
 Authorization and Consent for Sleep Testing I authorize the release of any medical information necessary to the durable medical equipment company for therapy, if applicable. I authorize the use of audio
Authorization and Consent for Sleep Testing I authorize the release of any medical information necessary to the durable medical equipment company for therapy, if applicable. I authorize the use of audio
Sleep Center New Patient Questionnaire
 For office use only Appt date: Sleep Center Clinician: Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 #1 respiratory hospital
For office use only Appt date: Sleep Center Clinician: Main Campus Highlands Ranch Location 1400 Jackson Street 8671 S. Quebec St., Ste 120 Denver, CO 80206 Highlands Ranch, CO 80130 #1 respiratory hospital
SLEEP STUDY - PATIENT QUESTIONNAIRE
 NOTE: You cannot fill out this form on Mozilla Firefox, please try another browser. You have two options for completing a questionnaire: - Enter the information on the fillable PDF and click Print at the
NOTE: You cannot fill out this form on Mozilla Firefox, please try another browser. You have two options for completing a questionnaire: - Enter the information on the fillable PDF and click Print at the
Sleep & Relaxation. Session 1 Understanding Insomnia Sleep improvement techniques Try a new technique
 Sleep & Relaxation Sleep & Relaxation Session 1 Understanding Insomnia Sleep improvement techniques Try a new technique Session 2 Dealing with unhelpful thoughts Putting these techniques together for better
Sleep & Relaxation Sleep & Relaxation Session 1 Understanding Insomnia Sleep improvement techniques Try a new technique Session 2 Dealing with unhelpful thoughts Putting these techniques together for better
SLEEP QUESTIONNAIRE. Please briefly describe your sleep or sleep problem:
 SLEEP QUESTIONNAIRE Your answers to the following questions will help us to obtain a better understanding of your sleep problems. Please answer every question to the best of your ability. It is helpful
SLEEP QUESTIONNAIRE Your answers to the following questions will help us to obtain a better understanding of your sleep problems. Please answer every question to the best of your ability. It is helpful
Ten tips for a good night s sleep
 Ten tips for a good night s sleep This task set contains: Teacher instructions Reading text Learner response sheet Answer key Marking and feedback to learners When marking the learners' responses please
Ten tips for a good night s sleep This task set contains: Teacher instructions Reading text Learner response sheet Answer key Marking and feedback to learners When marking the learners' responses please
Sleep Health Center. You have been scheduled for an Insomnia Treatment Program consultation to further discuss your
 Sleep Health Center You have been scheduled for an Insomnia Treatment Program consultation to further discuss your sleep. In the week preceding your appointment, please take the time to complete the enclosed
Sleep Health Center You have been scheduled for an Insomnia Treatment Program consultation to further discuss your sleep. In the week preceding your appointment, please take the time to complete the enclosed
WHEN SHOULD I USE SLEEP AIDS IN MY PATIENTS WITH SLEEP DISORDERS... (AND WHEN SHOULD I NOT?)
") Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN SHOULD I USE SLEEP AIDS IN MY PATIENTS WITH SLEEP DISORDERS... (AND WHEN SHOULD I NOT?) CATHERINE MCCALL, MD
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN SHOULD I USE SLEEP AIDS IN MY PATIENTS WITH SLEEP DISORDERS... (AND WHEN SHOULD I NOT?) CATHERINE MCCALL, MD
RESTore TM. Clinician Manual for Single User. Insomnia and Sleep Disorders. A step by step manual to help you guide your clients through the program
 RESTore TM Insomnia and Sleep Disorders Clinician Manual for Single User A step by step manual to help you guide your clients through the program Version 10 July, 2016 Table of Contents Introduction...
RESTore TM Insomnia and Sleep Disorders Clinician Manual for Single User A step by step manual to help you guide your clients through the program Version 10 July, 2016 Table of Contents Introduction...
Intake Questionnaire
 Intake Questionnaire In order to make the best use of your appointment time, please complete this form prior to your initial appointment. What is your name? (Who filled in this form?) (Y= yes N=no DK=
Intake Questionnaire In order to make the best use of your appointment time, please complete this form prior to your initial appointment. What is your name? (Who filled in this form?) (Y= yes N=no DK=