Chronic Obstructive Pulmonary Disease 1 4/11/20128:52:12 AM
|
|
|
- Elijah White
- 6 years ago
- Views:
Transcription




1 Chronic Obstructive Pulmonary Disease 1 4/11/20128:52:12 AM
2 Table of Contents The Four Stages of COPD. 3 Modified Medical Research Council Dyspnea Scale. 3 Spirometry. 4 Alpha 1 Antitrypsin Deficiency... 4 Smoking Cessation 4 5 Air Quality.. 5 Sleep Apnea.. 5 Anxiety and Depression 5 Nutrition/Weight Loss or Gain. 5 Immunizations. 6 Medications.. 6 Bronchodilators.. 6 Glucocorticosteriods 7 Beta Blockers 7 Oxygen. 7 Miscellaneous Key Points 8 Exacerbations. 8 Indications for Hospital Admission. 9 Pulmonologist Consultation.. 9 Rehabilitation. 9 Benefits of Pulmonary Rehab.. 10 Disease Management Review. 10 Levels of Evidence Used in the GOLD Guidelines.. 11 Pharmacologic Therapy in COPD.. 11 STOP BANG Screening for Obstructive Sleep Apnea.. 12 Clinical Practice Guideline for Treating Tobacco Use and Dependence: 2008 Update.. 13 The 5 A s : Treating Tobacco Dependence as a Chronic Disease Pharmacologic Product Guide: FDA Approved Medications
3 COPD Evidence-Based Summary and Supporting Research The Meridian Health COPD evidence review team studied the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2010 updated clinical guidelines for care. The following points of emphasis were derived for clinician use. This summary highlights only those items the review committee deemed important enough to emphasize. Please access the full document for additional information at global strategy for diagnosis management.html. The four stages of COPD should be used, documented, and communicated consistently across the continuum: Stage 1: Mild FEV1 80% predicted Stage II: Moderate 50% FEV1 < 80% predicted Stage III: Severe 30 % FEV1 < 50% predicted Stage IV: Very Severe: FEV1 < 30% predictor or FEV1 < 50% predicted plus chronic respiratory failure (All with FEV1/FVC < 0.70) The modified medical research council dyspnea scale should be performed annually to assess disease progression. Modified Medical Research Council Dyspnea Scale Grade 0 I only get breathless with strenuous exercise 1 I get short of breath when hurrying on the level or walking up a slight hill 2 I walk slower than people of the same age on the level because of breathlessness or have to stop for breath when walking at my own pace on the level 3 I stop for breath after walking about 100 yards or after a few minutes on the level 4 I am too breathless to leave the house or I am breathless when dressing 3
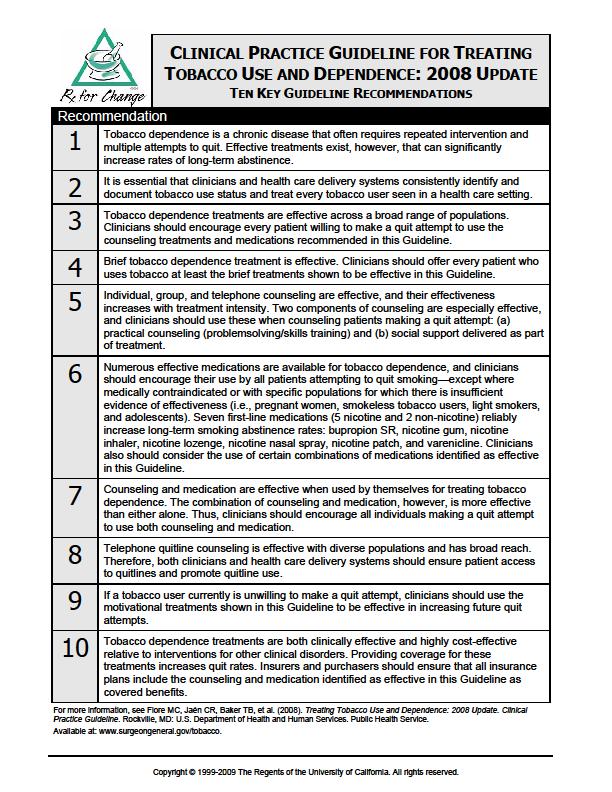
4 Spirometry Spirometry assessment is the gold standard for diagnosing COPD and monitoring its progression. Quality standards in spirometry measurement must be upheld. For patients with moderate disease or worse, full pulmonary function testing with bronchodilator reversibility testing should be performed. Such testing should also be considered in patients of lower stages whose clinical course is more variable and/or spirometry is not reproducible. Neither bronchodilator nor oral gluco cortico steroid reversibility testing predicts disease progression. A patient s decline in lung function is best tracked by spirometry measurements, usually no more than once a year. In Severe COPD An echocardiogram is recommended. ABG measurement while the patient is breathing air is important. Screening less severe cases by pulse oximetry and obtaining ABG if SaO2 is < 92 is reasonable. Alpha-1 Antitrypsin Deficiency In patients of Caucasian descent who develop COPD at a young age, (< 45 years) or who have a strong family history of the disease, it may be valuable to identify coexisting alpha 1 antitrypsin deficiency. Points of Emphasis re: Smoking Cessation Smoking status is critical as this is the single greatest risk factor among U.S. patients. Clinicians must institutionalize the consistent identification, documentation, and treatment of every tobacco user at every visit. ASK; ADVISE; ASSESS; ASSIST; ARRANGE. Use these 5A s (see attached algorithm from Treating Tobacco Use and Dependence: 2008 Update. Quick Reference Guide for Clinicians). Ask every visit. Even a brief (3 minute) period of counseling to urge a smoker to quit may result in smoking cessation rates of 5 10%. Practitioners should instruct patients that it may require multiple attempts to be successful. The quick reference clinician guide may be obtained from Fiore MC, Jaén CR, Baker TB, et al. Treating Tobacco Use and Dependence: 4
5 2008 Update. Quick Reference Guide for Clinicians. Rockville, MD: U.S. Department of Health and Human Services. Public Health Service. April Combination therapy/strategies for smoking cessation are recommended. Smith, S. S., et al. (2009). Comparative effectiveness of 5 smoking cessation pharmacotherapies in primary care clinics, Archives of Internal Medicine, 169(22), Strongly suggested for clinician review are excerpts enclosed: o Clinical Practice Guideline for Treating Tobacco Use and Dependence: 2008 Update Ten Key Guideline Recommendations. o AAFP Pharmacologic Product Guide from the ASK and ACT tobacco cessation program. Air Quality Persons with advanced COPD should monitor air quality announcements and adjust accordingly. Sleep Apnea Decision tools for sleep apnea assessments should be used. Use of the STOP BANG screening tool (enclosed) is recommended as it has high sensitivity and specificity. Abrishami, A., Khajehdehi, A., & Chung, F. (2010). A systematic review of screening questionnaires for obstructive sleep apnea. Canadian Journal of Anesthesiology, 57, Anxiety and Depression Anxiety and depression screening is critical. COPD patients may experience 10x the depression as non COPD patients (NCQA) NCQA. (2009). Insights for improvement: Advancing COPD care through quality measurement. Nutrition/Weight Loss or Gain Both underweight and overweight are a problem. 5
6 A reduction in BMI is an independent risk factor for mortality in COPD (Level A). Advanced COPD patients commonly experience weight loss and this is prognostically important. Immunizations Influenza and pneumococcal vaccination are strongly recommended. Influenza vaccines can reduce serious illness and death in COPD by about 50% (Level A). Pneumococcal polysaccharide vaccine is recommended for COPD patients 65 years and older and has been shown to reduce Community Acquired Pneumonia (CAP) in COPD patients under 65 with FEV1 < 40% predicted (Level B). Medications Pharmacologic management per stage is recommended. See enclosed flow diagram. Bronchodilators Regular treatment with long acting bronchodilators is more effective and convenient than short acting (Level A). Oral therapy is slower in onset and has more side effects than inhaled treatment (Level A). Inhaled products, which are absorbed quicker and possess less enduring side effects, are preferred. Bronchodilator effects of short acting anticholinergics last 8 hours and Tiotropium has a duration of more than 24 hours (Level A). Tiotropium (Spiriva) is preferred. Methylxanthines: Toxicity is dose related, with the therapeutic ratio small and most of the benefit occurs only when near toxic doses are given (Level A). 6
7 Glucocorticosteriods Regular treatment with inhaled glucocorticosteroids has been shown to reduce the frequency of exacerbations and thus improve health status for symptomatic COPD patients at stage III and IV and repeated exacerbations (for example, three in the last three years) (Level A). An inhaled glucocorticosteroid combined with a long acting β2 agonist is more effective than the individual components in reducing exacerbations and improving lung function and health status (Level A). Phosphodiesterase-4 Inhibitors (Roflumilast) This drug is very recently approved for use in the U.S. and has little track record; its role cannot yet be recommended by local experts. Side effects reported have included weight loss, unexpected diarrhea, behavioral disturbances and depression. The widespread use of mucolytic agents cannot be recommended at present (Level D). Beta Blockers Erdman, E. (2009). Safety and tolerability of beta blockers: Prejudices and reality. European Heart Journal Supplements, 11(Supplement A), A21 A25 was reviewed and the following key points of emphasis are significant: o The majority of patients with HF and COPD can safely tolerate beta blocker therapy. o Lung function should be carefully monitored as asthma and COPD may co exist. o Especially in elderly, start low and go slow. o Beta 1 selective therapy is preferred. Oxygen Long term oxygen therapy is introduced in Stage IV with PaO2 55 mm Hg or SaO2 at/below 88% (Level B). Burden vs. benefit should be assessed. Clinical judgment plays a significant role. 7
8 Miscellaneous Key Points Missed days of work should be assessed each visit. Reminder: Regular production of sputum for 3 or more months in 2 consecutive years may signal chronic bronchitis. The presence of wheezing during quiet breathing is a useful pointer to airflow limitation. Wheezing heard only after forced expiration has not been validated as a diagnostic test for COPD. Less prevalent today in the U.S., but still important for initial and annual assessment, is the presence of occupational or environmental contributors to COPD. Determine if the patient can financially cover the costs of their prescriptions/therapies. Routine CT and V P scanning are appropriate only if the patient is going to surgery. Exacerbations There is no current evidence that the use of antibiotics other than for treating infectious exacerbations of COPD and other bacterial infections is helpful (Level A). In the presence of the 3 cardinal signs/indicators, antibiotics of choice are: o Azithromycin 500 mg p.o. daily for 5 days. If on amiodarone therapy, may use one of the following: Bactrim DS 1 tab p.o., twice daily x 7 days Amoxicillin 250mg p.o., three times daily x 7 days Doxycyline 100mg p.o., twice daily x 7 days (Three cardinal signs: increased dyspnea, increased sputum volume, and increased sputum purulence (Level B). The frequency of infections must be assessed.) Areas of emphasis in exacerbations include: o Spirometry and PEF are not accurate during an exacerbation. o Pulse oximetry can be used to evaluate oxygen saturation and the need for supplemental oxygen therapy. o Home management of COPD exacerbations involves increasing the dose and/or frequency of existing short acting bronchodilator therapy, preferable with a beta 2 agonist (Level A). 8
9 o Systemic glucocorticosteroids are beneficial in shortening recovery time, improving lung function and hypoxemia (Level A). Indications for Hospital Admission Include: Marked increase in intensity of symptoms such as sudden development of resting dyspnea Severe underlying COPD Onset of new physical signs such as cyanosis, peripheral edema Failure of exacerbation to respond to initial medical management Significant comorbidities Frequent exacerbations Newly occurring arrhythmias Diagnostic uncertainty Older age Insufficient home support Pulmonologist Consultation Signals for referral to the pulmonologist include but are not limited to: When long term oral steroid use is being entertained Management of alpha 1 antitrypsin deficiency Advanced disease where opioids are needed NIPPV use Surgical management Rehabilitation COPD at all stages of disease appears to benefit from exercise training programs, improving both exercise tolerance and symptoms of dyspnea and fatigue (Level A). Any patient with COPD should be considered for pulmonary rehab. Use of formal rehab services should be encouraged. Where this is not feasible, home exercise should be encouraged. After rehab, guidelines state if exercise is continued at home the patient s health status remains above pre rehab levels (Level B). Nevertheless, the committee noted that attending formal rehab/exercise services does appear to produce social camaraderie and support that promotes adherence. 9
10 Benefits of Pulmonary Rehab 1. A program of exercise training of the muscles of ambulation is recommended as a mandatory component of pulmonary rehabilitation for patients with chronic obstructive pulmonary disease (COPD). Grade of Recommendation 1A 2. Pulmonary rehabilitation improves the symptom of dyspnea in patients with COPD. Grade of Recommendation 1A 3. Pulmonary rehabilitation improves health related quality of life (HRQOL) in patients with COPD. Grade of Recommendation 1A 4. Pulmonary rehabilitation reduces the number of hospital days and other measures of health care utilization in patients with COPD. Grade of Recommendation 2B 5. Pulmonary rehabilitation is cost effective in patients with COPD. Grade of Recommendation 2C Ries AL, Bauldoff GS, Carlin BW, Casaburi R, Emery CF, Mahler DA, Make B, Rochester CL, Zuwallack R, Herrerias C. Pulmonary Rehabilitation: Joint ACCP/AACVPR Evidence Based Clinical Practice Guidelines. Chest 2007 May;131(5 Suppl):4S 42S. Disease Management Review The committee reviewed the evidence (SR) from Lemmens (2008) and the more recent large VA Study by Rice (2010). The committee concurred that there should be an emphasis for the system practitioners in the following: Provider education Patient education/self management Case management across the continuum This triple combination has been showed in meta analysis to reduce the chance of 1 hospitalization as well as improve quality of life. The VA study strongly pointed to a reduction of hospitalizations and ER visits with disease management (DM). As Meridian evolves their COPD DM Services in provider education, patient education and case management, their use should be encouraged. Lemmons, K. M. M., Nieboer, A. P., & Hukjsman, R. (2009). A systematic review of integrated use of disease management interventions in asthma and COPD. Respiratory Care, 103, Rice, K. L., et al. (2010). Disease management program for chronic obstructive pulmonary disease. American Journal of Respiratory Critical Care Medicine, 182, July



11 Levels of Evidence Used in the GOLD Guidelines A Randomized controlled trials with rich body of data. B Randomized controlled trials with limited body of data. C Nonrandomized trials; observational studies. D Panel consensus judgment. Source: University of Pennsylvania, accessed from the page Penn CME/Best Practice 11
12 STOP BANG Screening for Obstructive Sleep Apnea Answer the following questions to find out if you are at risk for Obstructive Sleep Apnea: STOP S (snore) Have you been told that you snore? YES/NO T (tired) Are you often tired during the day? YES/NO O (obstruction) Do you know if you stop breathing or has anyone witnessed you stop breathing while you are asleep? YES/NO P (pressure) Do you have high blood pressure or on medication to control high blood pressure? YES/NO If you answered YES to two or more questions on the STOP portion you are at risk for Obstructive Sleep Apnea. It is recommended that you contact your primary care provider to discuss a possible sleep disorder. To find out if you are at moderate to severe risk of Obstructive Sleep Apnea, complete the BANG questions below. BANG B (BMI) Is your body mass index greater than 30? YES/NO A (age) Are you 50 years old or older? YES/NO N (neck) Do you have a neck circumference greater than 40 cm? YES/NO G (gender) Are you a male? YES/NO The more questions you answer YES to on the BANG portion, the greater your risk of having moderate to severe Obstructive Sleep Apnea. Abrishami, A., Khajehdehi, A., & Chung, F. (2010). A systematic review of screening questionnaires for obstructive sleep apnea. Canadian Journal of Anesthesiology, 57, Ong., T. H., Raudha, S., Fook Chong, S., Lew, N., & Hsu, A. (2010). Simplifying STOP BANG: use of a simple questionnaire to screen for OSA in an Asian population. Sleep Breath. 4(14), 371 6, (Epubl 2010 Apr 26.) 12
13 13



14 From the quick reference guide found at: 14
 myocardial infarction Serious underlying arrhythmias Serious or worsening angina pectoris")
15 PHARMACOLOGIC PRODUCT GUIDE: FDA-APPROVED MEDICATIONS FOR SMOKING CESSATION PRODUCT PRECAUTIONS NICOTINE REPLACEMENT THERAPY (NRT) FORMULATIONS GUM LOZENGE TRANSDERMAL PATCH NASAL SPRAY ORAL INHALER Nicorette 1, Generic OTC 2 mg, 4 mg original, cinnamon, fruit, mint, orange Recent ( 2 weeks) myocardial infarction Serious underlying arrhythmias Serious or worsening angina pectoris Temporomandibular joint disease Pregnancy 3 and breastfeeding Adolescents (<18 years) Nicorette Lozenge, 1 Nicorette Mini Lozenge, 1 Generic OTC 2 mg, 4 mg cherry, mint Recent ( 2 weeks) myocardial infarction Serious underlying arrhythmias Serious or worsening angina pectoris Pregnancy 3 and breastfeeding Adolescents (<18 years) NicoDerm CQ 1, Generic OTC (NicoDerm CQ, generic) Rx (generic) 7 mg, 14 mg, 21 mg (24-hour release) Recent ( 2 weeks) myocardial infarction Serious underlying arrhythmias Serious or worsening angina pectoris Pregnancy 3 (Rx formulations, category D) and breastfeeding Adolescents (<18 years) Nicotrol NS 2 Rx Metered spray 0.5 mg nicotine in 50 mcl aqueous nicotine solution Recent ( 2 weeks) myocardial infarction Serious underlying arrhythmias Serious or worsening angina pectoris Underlying chronic nasal disorders (rhinitis, nasal polyps, sinusitis) Severe reactive airway disease Pregnancy 3 (category D) and breastfeeding Adolescents (<18 years) Nicotrol Inhaler 2 Rx 10 mg cartridge delivers 4 mg inhaled nicotine vapor Recent ( 2 weeks) myocardial infarction Serious underlying arrhythmias Serious or worsening angina pectoris Bronchospastic disease Pregnancy 3 (category D) and breastfeeding Adolescents (<18 years) BUPROPION SR Zyban 1, Generic Rx 150 mg sustained-release tablet Concomitant therapy with medications or medical conditions known to lower the seizure threshold Severe hepatic cirrhosis Pregnancy 3 (category C) and breastfeeding Adolescents (<18 years) Warning: BLACK-BOXED WARNING for neuropsychiatric symptoms 4 Contraindications: Seizure disorder Concomitant bupropion (e.g., Wellbutrin) therapy Current or prior diagnosis of bulimia or anorexia nervosa Simultaneous abrupt discontinuation of alcohol or sedatives/benzodiazepines MAO inhibitor therapy in previous 14 days VARENICLINE Chantix 2 Rx 0.5 mg, 1 mg tablet Severe renal impairment (dosage adjustment is necessary) Pregnancy 3 (category C) and breastfeeding Adolescents (<18 years) Warnings: BLACK-BOXED WARNING for neuropsychiatric symptoms 4 Cardiovascular adverse events in patients with existing cardiovascular disease DOSING 1 st cigarette 30 minutes after waking: 4 mg 1 st cigarette >30 minutes after waking: 2 mg Weeks 1 6: 1 piece q 1 2 hours Weeks 7 9: 1 piece q 2 4 hours Weeks 10 12: 1 piece q 4 8 hours Maximum, 24 pieces/day Chew each piece slowly Park between cheek and gum when peppery or tingling sensation appears (~15 30 chews) Resume chewing when tingle fades Repeat chew/park steps until most of the nicotine is gone (tingle does not return; generally 30 min) Park in different areas of mouth No food or beverages 15 minutes before or during use Duration: up to 12 weeks 1 st cigarette 30 minutes after waking: 4 mg 1 st cigarette >30 minutes after waking: 2 mg Weeks 1 6: 1 lozenge q 1 2 hours Weeks 7 9: 1 lozenge q 2 4 hours Weeks 10 12: 1 lozenge q 4 8 hours Maximum, 20 lozenges/day Allow to dissolve slowly (20 30 minutes for standard; 10 minutes for mini) Nicotine release may cause a warm, tingling sensation Do not chew or swallow Occasionally rotate to different areas of the mouth No food or beverages 15 minutes before or during use Duration: up to 12 weeks >10 cigarettes/day: 21 mg/day x 4 weeks (generic) 6 weeks (NicoDerm CQ) 14 mg/day x 2 weeks 7 mg/day x 2 weeks 10 cigarettes/day: 14 mg/day x 6 weeks 7 mg/day x 2 weeks May wear patch for 16 hours if patient experiences sleep disturbances (remove at bedtime) Duration: 8 10 weeks 1 2 doses/hour (8 40 doses/day) One dose = 2 sprays (one in each nostril); each spray delivers 0.5 mg of nicotine to the nasal mucosa Maximum 5 doses/hour or 40 doses/day For best results, initially use at least 8 doses/day Do not sniff, swallow, or inhale through the nose as the spray is being administered Duration: 3 6 months 6 16 cartridges/day Individualize dosing; initially use 1 cartridge q 1 2 hours Best effects with continuous puffing for 20 minutes Initially use at least 6 cartridges/day Nicotine in cartridge is depleted after 20 minutes of active puffing Inhale into back of throat or puff in short breaths Do NOT inhale into the lungs (like a cigarette) but puff as if lighting a pipe Open cartridge retains potency for 24 hours No food or beverages 15 minutes before or during use Duration: 3 6 months 150 mg po q AM x 3 days, then 150 mg po bid Do not exceed 300 mg/day Begin therapy 1 2 weeks prior to quit date Allow at least 8 hours between doses Avoid bedtime dosing to minimize insomnia Dose tapering is not necessary Can be used safely with NRT Duration: 7 12 weeks, with maintenance up to 6 months in selected patients Days 1 3: 0.5 mg po q AM Days 4 7: 0.5 mg po bid Weeks 2 12: 1 mg po bid Begin therapy 1 week prior to quit date; alternatively, the patient can begin therapy and then quit smoking between days 8 35 of treatment Take dose after eating and with a full glass of water Dose tapering is not necessary Dosing adjustment is necessary for patients with severe renal impairment Duration: 12 weeks; an additional 12-week course may be used in selected patients
16 NICOTINE REPLACEMENT THERAPY (NRT) FORMULATIONS GUM LOZENGE TRANSDERMAL PATCH NASAL SPRAY ORAL INHALER BUPROPION SR VARENICLINE ADVERSE EFFECTS Mouth/jaw soreness Hiccups Dyspepsia Hypersalivation Effects associated with incorrect chewing technique: Lightheadedness Nausea/vomiting Throat and mouth irritation Nausea Hiccups Cough Heartburn Headache Flatulence Insomnia Local skin reactions (erythema, pruritus, burning) Headache Sleep disturbances (insomnia, abnormal/vivid dreams); associated with nocturnal nicotine absorption Nasal and/or throat irritation (hot, peppery, or burning sensation) Rhinitis Tearing Sneezing Cough Headache Mouth and/or throat irritation Cough Headache Rhinitis Dyspepsia Hiccups Insomnia Dry mouth Nervousness/difficulty concentrating Rash Constipation Seizures (risk is 0.1%) Neuropsychiatric symptoms (rare; see PRECAUTIONS) Nausea Sleep disturbances (insomnia, abnormal/vivid dreams) Constipation Flatulence Vomiting Neuropsychiatric symptoms (rare; see PRECAUTIONS) ADVANTAGES Might satisfy oral cravings Might delay weight gain Patients can titrate therapy to manage withdrawal symptoms Variety of flavors are available Might satisfy oral cravings Might delay weight gain Easy to use and conceal Patients can titrate therapy to manage withdrawal symptoms Variety of flavors are available Provides consistent nicotine levels over 24 hours Easy to use and conceal Once daily dosing associated with fewer compliance problems Patients can titrate therapy to rapidly manage withdrawal symptoms Patients can titrate therapy to manage withdrawal symptoms Mimics hand-to-mouth ritual of smoking (could also be perceived as a disadvantage) Easy to use; oral formulation might be associated with fewer compliance problems Might delay weight gain Can be used with NRT Might be beneficial in patients with depression Easy to use; oral formulation might be associated with fewer compliance problems Offers a new mechanism of action for patients who have failed other agents DISADVANTAGES Need for frequent dosing can compromise compliance Might be problematic for patients with significant dental work Patients must use proper chewing technique to minimize adverse effects Gum chewing may not be socially acceptable Need for frequent dosing can compromise compliance Gastrointestinal side effects (nausea, hiccups, heartburn) might be bothersome Patients cannot titrate the dose to acutely manage withdrawal symptoms Allergic reactions to adhesive might occur Patients with dermatologic conditions should not use the patch Need for frequent dosing can compromise compliance Nasal/throat irritation may be bothersome Patients must wait 5 minutes before driving or operating heavy machinery Patients with chronic nasal disorders or severe reactive airway disease should not use the spray Need for frequent dosing can compromise compliance Initial throat or mouth irritation can be bothersome Cartridges should not be stored in very warm conditions or used in very cold conditions Patients with underlying bronchospastic disease must use with caution Seizure risk is increased Several contraindications and precautions preclude use in some patients (see PRECAUTIONS) Patients should be monitored for potential neuropsychiatric symptoms 4 (see PRECAUTIONS) May induce nausea in up to one third of patients Patients should be monitored for potential neuropsychiatric symptoms 4 (see PRECAUTIONS) COST/DAY 5 2 mg or 4 mg: $1.90 $5.49 (9 pieces) 2 mg or 4 mg: $1.89 $4.50 (9 pieces) $1.60 $3.40 (1 patch) $3.58 (8 doses) $6.39 (6 cartridges) $2.71 $6.20 (2 tablets) $5.64 $5.96 (2 tablets) 1 Marketed by GlaxoSmithKline. 2 Marketed by Pfizer. 3 The U.S. Clinical Practice Guideline states that pregnant smokers should be encouraged to quit without medication based on insufficient evidence of effectiveness and theoretical concerns with safety. Pregnant smokers should be offered behavioral counseling interventions that exceed minimal advice to quit. 4 In July 2009, the FDA mandated that the prescribing information for all bupropion- and varenicline-containing products include a black-boxed warning highlighting the risk of serious neuropsychiatric symptoms, including changes in behavior, hostility, agitation, depressed mood, suicidal thoughts and behavior, and attempted suicide. Clinicians should advise patients to stop taking varenicline or bupropion SR and contact a healthcare provider immediately if they experience agitation, depressed mood, and any changes in behavior that are not typical of nicotine withdrawal, or if they experience suicidal thoughts or behavior. If treatment is stopped due to neuropsychiatric symptoms, patients should be monitored until the symptoms resolve. 5 Wholesale acquisition cost from Red Book Online. Thomson Reuters, March Abbreviations: MAO, monoamine oxidase; NRT, nicotine replacement therapy; OTC, over-the-counter (non-prescription product); Rx, prescription product. For complete prescribing information, please refer to the manufacturers package inserts. Copyright The Regents of the University of California. All rights reserved. Updated March 1, 2012.
Smoking cessation therapy
 Appendix 1 Smoking cessation therapy Q. Can a dentist prescribe medications for smoking cessation? A. Yes. Dentists are allowed and are encouraged to help patients with smoking cessation by counseling
Appendix 1 Smoking cessation therapy Q. Can a dentist prescribe medications for smoking cessation? A. Yes. Dentists are allowed and are encouraged to help patients with smoking cessation by counseling
Medication Management to Aid in Smoking Cessation. Rachel Constant, Pharm.D. Baptist Health Corbin Pharmacy Resident 3/22/2019
 Medication Management to Aid in Smoking Cessation Rachel Constant, Pharm.D. Baptist Health Corbin Pharmacy Resident 3/22/2019 1 Learning Objectives: Review the prevalence of tobacco use. Describe tools
Medication Management to Aid in Smoking Cessation Rachel Constant, Pharm.D. Baptist Health Corbin Pharmacy Resident 3/22/2019 1 Learning Objectives: Review the prevalence of tobacco use. Describe tools
My Mask. I keep it all inside. Because I d rather. The pain destroy me. Than everyone else. Anon.
 My Mask KL I keep it all inside Because I d rather The pain destroy me Than everyone else. Anon. 43 K. N. Roy Chengappa, M.D., FRCPC Professor of Psychiatry, University of Pittsburgh School of Medicine,
My Mask KL I keep it all inside Because I d rather The pain destroy me Than everyone else. Anon. 43 K. N. Roy Chengappa, M.D., FRCPC Professor of Psychiatry, University of Pittsburgh School of Medicine,
IMPORTANT POINTS ABOUT MEDICATIONS
 IMPORTANT POINTS ABOUT MEDICATIONS The U.S. Food & Drug Administration (FDA) advises that there are significant health benefits to quitting smoking. The health benefits of quitting smoking include a reduction
IMPORTANT POINTS ABOUT MEDICATIONS The U.S. Food & Drug Administration (FDA) advises that there are significant health benefits to quitting smoking. The health benefits of quitting smoking include a reduction
Cessation Medicine Reference Guide Table of Contents
 Cessation Medicine Reference Guide Table of Contents 1. Patch 2. Nicotine Gum 3. Nicotine Lozenge 4. Inhaler 5. Nasal Spray 6. Bupropion SR (Zyban) 7. Chantix (Varenicline) Patch Typical course of therapy
Cessation Medicine Reference Guide Table of Contents 1. Patch 2. Nicotine Gum 3. Nicotine Lozenge 4. Inhaler 5. Nasal Spray 6. Bupropion SR (Zyban) 7. Chantix (Varenicline) Patch Typical course of therapy
NYSMPEP Smoking Cessation Guidance: Key Message 3
 NYSMPEP Smoking Cessation Guidance: Key Message 3 Key Message 3: All smokers trying to quit should be offered medication (except when contraindicated or for specific populations). The Agency for Healthcare
NYSMPEP Smoking Cessation Guidance: Key Message 3 Key Message 3: All smokers trying to quit should be offered medication (except when contraindicated or for specific populations). The Agency for Healthcare
AIDS for CESSATION PHARMACOTHERAPY. METHODS for QUITTING. NONPHARMACOLOGIC METHODS (cont d) NONPHARMACOLOGIC METHODS
 NONPHARMACOLOGIC METHODS") METHODS for QUITTING AIDS for CESSATION Nonpharmacologic Counseling and other non-drug approaches Pharmacologic FDA-approved medications Counseling and medications are both effective, but the combination
METHODS for QUITTING AIDS for CESSATION Nonpharmacologic Counseling and other non-drug approaches Pharmacologic FDA-approved medications Counseling and medications are both effective, but the combination
5. Offer pharmacotherapy to all smokers who are attempting to quit, unless contraindicated.
 0 11 Key Messages 1. Ask and document smoking status for all patients. 2. Provide brief advice on quit smoking at every visit to all smokers. 3. Use individual, group and telephone counselling approaches,
0 11 Key Messages 1. Ask and document smoking status for all patients. 2. Provide brief advice on quit smoking at every visit to all smokers. 3. Use individual, group and telephone counselling approaches,
AIDS for CESSATION PHARMACOTHERAPY. METHODS for QUITTING. NONPHARMACOLOGIC METHODS (cont d) NONPHARMACOLOGIC METHODS
 NONPHARMACOLOGIC METHODS") METHODS for QUITTING AIDS for CESSATION Nonpharmacologic Counseling and other non-drug approaches Pharmacologic FDA-approved medications Counseling and medications are both effective, but the combination
METHODS for QUITTING AIDS for CESSATION Nonpharmacologic Counseling and other non-drug approaches Pharmacologic FDA-approved medications Counseling and medications are both effective, but the combination
Tobacco Dependence Screening and Treatment in Behavioral Health Settings. Prescribing
 Tobacco Dependence Screening and Treatment in Behavioral Health Settings Prescribing GOAL To build the capacity of prescribing clinicians in behavioral health settings to integrate best practices for prescribing
Tobacco Dependence Screening and Treatment in Behavioral Health Settings Prescribing GOAL To build the capacity of prescribing clinicians in behavioral health settings to integrate best practices for prescribing
Smoking and Nicotine Replacement Therapy (NRT) Lec:5
 Lec:5") Smoking and Nicotine Replacement Therapy (NRT) Lec:5 Tobacco use remains the single largest preventable cause of mortality. Cigarette smoke is a complex mixture of an estimated 4800 compounds. Approximately
Smoking and Nicotine Replacement Therapy (NRT) Lec:5 Tobacco use remains the single largest preventable cause of mortality. Cigarette smoke is a complex mixture of an estimated 4800 compounds. Approximately
Objectives. Disclosure. Prevalence of Tobacco Use. Smoking Cessation Pharmacotherapy 3/2/2016.
 Smoking Cessation Pharmacotherapy Melodie Merzier-Michel PGY-1 Pharmacy Resident Memorial Regional Hospital www.fshp.org Objectives Discuss the prevalence of tobacco use in the United States (U.S.) Describe
Smoking Cessation Pharmacotherapy Melodie Merzier-Michel PGY-1 Pharmacy Resident Memorial Regional Hospital www.fshp.org Objectives Discuss the prevalence of tobacco use in the United States (U.S.) Describe
Pharmacotherapy Summary for the Treatment of Nicotine Withdrawal and Nicotine Dependence 1
 Pharmacotherapy Summary for the Treatment of Nicotine Withdrawal and Nicotine Dependence 1 Compiled by: TOP, in collaboration with Dr. Charl Els and Mr. Ron Pohar: TRaC II (Alberta Medical Association/Primary
Pharmacotherapy Summary for the Treatment of Nicotine Withdrawal and Nicotine Dependence 1 Compiled by: TOP, in collaboration with Dr. Charl Els and Mr. Ron Pohar: TRaC II (Alberta Medical Association/Primary
TREATMENT INTERVENTIONS
 SMOKING CESSATION TREATMENT INTERVENTIONS Smoking and Health Tobacco is the single most preventable cause of death in the world today. kills more than five million people By 2030, the death toll will exceed
SMOKING CESSATION TREATMENT INTERVENTIONS Smoking and Health Tobacco is the single most preventable cause of death in the world today. kills more than five million people By 2030, the death toll will exceed
Smoking Cessation Services Guidance
 Smoking Cessation Services Guidance Alabama Medicaid Tobacco Treatment Coverage Covered Services/Medication 1. Free tobacco cessation counseling is provided through the Alabama Tobacco Quitline. Refer
Smoking Cessation Services Guidance Alabama Medicaid Tobacco Treatment Coverage Covered Services/Medication 1. Free tobacco cessation counseling is provided through the Alabama Tobacco Quitline. Refer
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
SMOKING CESSATION. Recommendations 5As Approach to Smoking Cessation. Stages of Change Assisting the Smoker. Contributor Dr. Saifuz Sulami.
 SMOKING CESSATION 08 Recommendations 5As Approach to Intervention Stages of Change Assisting the Smoker Pharmacotherapy Contributor Dr. Saifuz Sulami Advisor Dr. Audrey Tan 79 nhg_guideline_14102010_1112.indd
SMOKING CESSATION 08 Recommendations 5As Approach to Intervention Stages of Change Assisting the Smoker Pharmacotherapy Contributor Dr. Saifuz Sulami Advisor Dr. Audrey Tan 79 nhg_guideline_14102010_1112.indd
STEP Four: ASSIST with Quitting. STEP One: ASK about Tobacco Use. STEP Two: ADVISE to Quit
 STEP One: ASK about Tobacco Use Suggested Dialogue Do you ever smoke or use any type of tobacco? I take time to talk with all of my patients about tobacco use because it s important. Condition X often
STEP One: ASK about Tobacco Use Suggested Dialogue Do you ever smoke or use any type of tobacco? I take time to talk with all of my patients about tobacco use because it s important. Condition X often
Smoke-free Hospitals. Linda A. Thomas, MS University of Michigan Health System Tobacco Consultation Service
 Smoke-free Hospitals Linda A. Thomas, MS University of Michigan Health System Tobacco Consultation Service Today s Subjects 5A s and Clinician Training and Use with the Hospitalized Patient NRT use in
Smoke-free Hospitals Linda A. Thomas, MS University of Michigan Health System Tobacco Consultation Service Today s Subjects 5A s and Clinician Training and Use with the Hospitalized Patient NRT use in
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: CP.CPA.113 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.CPA.113 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important regulatory
Chantix (Varenicline) and Risk of Cardiovascular Events
 and Risk of Cardiovascular Events") PL Detail-Document #270803 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER August 2011 Chantix (Varenicline)
PL Detail-Document #270803 This PL Detail-Document gives subscribers additional insight related to the Recommendations published in PHARMACIST S LETTER / PRESCRIBER S LETTER August 2011 Chantix (Varenicline)
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
Smoking Cessation and the Pharmacist
 Smoking Cessation and the Pharmacist Jennifer Roberts Assistant Director, Research Pharmacy 1 Objectives Review smoking cessation medication use, based on public health guidelines, as well as contraindications
Smoking Cessation and the Pharmacist Jennifer Roberts Assistant Director, Research Pharmacy 1 Objectives Review smoking cessation medication use, based on public health guidelines, as well as contraindications
See Important Reminder at the end of this policy for important regulatory and legal information.
 Policy: Smoking Cessation Products Reference Number: TCHP.PHAR.18002 Effective Date: 01.01.19 Last Review Date: 10.12.18 Line of Business: Oregon Health Plan Revision Log See Important Reminder at the
Policy: Smoking Cessation Products Reference Number: TCHP.PHAR.18002 Effective Date: 01.01.19 Last Review Date: 10.12.18 Line of Business: Oregon Health Plan Revision Log See Important Reminder at the
Pharmacologic Therapy for Tobacco Use & Dependence
 Pharmacologic Therapy for Tobacco Use & Dependence Thomas Gauvin, MA, TTS Mayo Clinic Nicotine Dependence Center Rochester, MN 2013 MFMER slide-1 Learning Objectives Understand the 7 first line medications
Pharmacologic Therapy for Tobacco Use & Dependence Thomas Gauvin, MA, TTS Mayo Clinic Nicotine Dependence Center Rochester, MN 2013 MFMER slide-1 Learning Objectives Understand the 7 first line medications
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide
 VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
Clearing the Air: What You Need to Know and Do to Prepare to Quit Smoking
 Clearing the Air: What You Need to Know and Do to Prepare to Quit Smoking Getting Ready to Quit Course Creating Success! THINK ABOUT Process of Changing an Addiction Your Pros and Cons of Smoking and Quitting
Clearing the Air: What You Need to Know and Do to Prepare to Quit Smoking Getting Ready to Quit Course Creating Success! THINK ABOUT Process of Changing an Addiction Your Pros and Cons of Smoking and Quitting
Nicotine Replacement Therapy (NRT).
.") Nicotine Replacement Therapy (NRT). Information for smokers 1 What is NRT? The aim of Nicotine Replacement Therapy (NRT) is to reduce the withdrawal symptoms associated with nicotine addiction by replacing
Nicotine Replacement Therapy (NRT). Information for smokers 1 What is NRT? The aim of Nicotine Replacement Therapy (NRT) is to reduce the withdrawal symptoms associated with nicotine addiction by replacing
Pharmacotherapy for Treating Tobacco Dependence
 Pharmacotherapy for Treating Tobacco Dependence Sheila K. Stevens, MSW Education Coordinator Nicotine Dependence Center 2013 MFMER slide-1 Rationale for Pharmacological Therapy Success rate doubles Manage
Pharmacotherapy for Treating Tobacco Dependence Sheila K. Stevens, MSW Education Coordinator Nicotine Dependence Center 2013 MFMER slide-1 Rationale for Pharmacological Therapy Success rate doubles Manage
STEP Four: ASSIST with Quitting. STEP One: ASK about Tobacco Use. STEP Two: Strongly ADVISE to Quit. STEP Three: ASSESS Readiness to Quit
 STEP One: ASK about Tobacco Use Suggested Dialogue Do you, or does anyone in your household, ever smoke or use any type of tobacco? We ask all of our patients about tobacco use, because it can negatively
STEP One: ASK about Tobacco Use Suggested Dialogue Do you, or does anyone in your household, ever smoke or use any type of tobacco? We ask all of our patients about tobacco use, because it can negatively
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Tobacco Cessation The Role of the Dentist/Oral Medicinist
 Tobacco Cessation The Role of the Dentist/Oral Medicinist Jennifer Frustino, DDS PhD Oral Oncology & Maxillofacial Prosthetics Erie County Medical Center Buffalo, NY Statement of Disclosure I have no actual
Tobacco Cessation The Role of the Dentist/Oral Medicinist Jennifer Frustino, DDS PhD Oral Oncology & Maxillofacial Prosthetics Erie County Medical Center Buffalo, NY Statement of Disclosure I have no actual
Nicotine Replacement and Smoking Cessation: Update on Best Practices
 Nicotine Replacement and Smoking Cessation: Update on Best Practices Adrienne Duckworth, MSN, APRN, FNP-C, CTTS Section of Hematology/Oncology WVU Department of Medicine WVU Cancer Institute Objective
Nicotine Replacement and Smoking Cessation: Update on Best Practices Adrienne Duckworth, MSN, APRN, FNP-C, CTTS Section of Hematology/Oncology WVU Department of Medicine WVU Cancer Institute Objective
Tobacco Cessation: Priority for Health Providers. Acknowledgements. Tobacco Cessation: Secondhand Smoke. Smoke-Free Environment & CA
 Acknowledgements Smoking Cessation Leadership Center http://smokingcessationleadership.ucsf.edu/ Rx for Change http://rxforchange.ucsf.edu/ Tobacco Use and Dependence: 2008 Update http://www.surgeongeneral.gov/tobacco
Acknowledgements Smoking Cessation Leadership Center http://smokingcessationleadership.ucsf.edu/ Rx for Change http://rxforchange.ucsf.edu/ Tobacco Use and Dependence: 2008 Update http://www.surgeongeneral.gov/tobacco
Nonprescription Nicotine Replacement Therapy
 Nonprescription Nicotine Replacement Therapy (a one-hour continuing education program) This program covers the nicotine patch, lozenge, and gum, including patient education information and a brief overview
Nonprescription Nicotine Replacement Therapy (a one-hour continuing education program) This program covers the nicotine patch, lozenge, and gum, including patient education information and a brief overview
Pharmacotherapy for Smoking Cessation
 Pharmacotherapy for Smoking Cessation (a one-hour continuing education program) This program provides an overview of all FDA-approved medications for cessation (nicotine patch, lozenge, gum, inhaler, nasal
Pharmacotherapy for Smoking Cessation (a one-hour continuing education program) This program provides an overview of all FDA-approved medications for cessation (nicotine patch, lozenge, gum, inhaler, nasal
PHARMACOTHERAPY OF SMOKING CESSATION
 PHARMACOTHERAPY OF SMOKING CESSATION Domenic A. Ciraulo, MD Director of Alcohol Pharmacotherapy Research Center for Addiction Medicine Department of Psychiatry Massachusetts General Hospital Disclosure
PHARMACOTHERAPY OF SMOKING CESSATION Domenic A. Ciraulo, MD Director of Alcohol Pharmacotherapy Research Center for Addiction Medicine Department of Psychiatry Massachusetts General Hospital Disclosure
Nicotine Replacement Therapy, Zyban and Champix. Name of presentation
 Nicotine Replacement Therapy, Zyban and Champix Nicotine Replacement Therapy (NRT) - Rationale for use Nicotine is highly addictive and causes unpleasant withdrawal symptoms which often undermine a quit
Nicotine Replacement Therapy, Zyban and Champix Nicotine Replacement Therapy (NRT) - Rationale for use Nicotine is highly addictive and causes unpleasant withdrawal symptoms which often undermine a quit
Smoking Cessation: Treating Tobacco Dependence
 Smoking Cessation: Treating Tobacco Dependence Pat Folan, RN Center for Tobacco Control Pulmonary Medicine NS-LIJ Health System NYS DOH Tobacco Control Program Treating Tobacco Dependence Center for Tobacco
Smoking Cessation: Treating Tobacco Dependence Pat Folan, RN Center for Tobacco Control Pulmonary Medicine NS-LIJ Health System NYS DOH Tobacco Control Program Treating Tobacco Dependence Center for Tobacco
Effects of Smoking and Methods of Cessation By Chetan Kaher
 Effects of Smoking and Methods of Cessation By Chetan Kaher Cigarette smoking is the leading cause of preventable death in the United States. It accounts or almost 500,000 deaths per year, or one in every
Effects of Smoking and Methods of Cessation By Chetan Kaher Cigarette smoking is the leading cause of preventable death in the United States. It accounts or almost 500,000 deaths per year, or one in every
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services
 Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services SMOKING CESSATION Introduction NICE recommends that Nicotine Replacement Therapy (NRT), bupropion [Zyban ] and
Clinical Guideline / Formulary Document Pharmacy Department Medicines Management Services SMOKING CESSATION Introduction NICE recommends that Nicotine Replacement Therapy (NRT), bupropion [Zyban ] and
Welcome Please stand by. We will begin shortly.
 Welcome Please stand by. We will begin shortly. Integrating Medications into Smoking Cessation Treatment: The Basics Tuesday, September 22, 2015 2pm ET (90 minutes) Disclosure Dr. Robin L. Corelli, Dr.
Welcome Please stand by. We will begin shortly. Integrating Medications into Smoking Cessation Treatment: The Basics Tuesday, September 22, 2015 2pm ET (90 minutes) Disclosure Dr. Robin L. Corelli, Dr.
HIV and Aging. Making Tobacco Cessation a Priority in HIV/AIDS Services. Objectives. Tobacco Use Among PLWHA
 HIV and Aging Making Tobacco Cessation a Priority in HIV/AIDS Services June 27, 2008 Amanda Brown, MPH Ruth Tripp, MPH, RN Objectives To explore existing knowledge of the HIV and smoking connection. To
HIV and Aging Making Tobacco Cessation a Priority in HIV/AIDS Services June 27, 2008 Amanda Brown, MPH Ruth Tripp, MPH, RN Objectives To explore existing knowledge of the HIV and smoking connection. To
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE
 MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Smoking Cessation Products LAST REVIEW 5/8/2018 THERAPEUTIC CLASS: Psychiatric Disorders REVIEW HISTORY 5/17, 5/16, 5/15,
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Smoking Cessation Products LAST REVIEW 5/8/2018 THERAPEUTIC CLASS: Psychiatric Disorders REVIEW HISTORY 5/17, 5/16, 5/15,
Dispensing of Nicotine Replacement Therapy (NRT)
") Simcoe Muskoka District Health Unit Print Version Medical Directive Number: Topic: Dispensing of Nicotine Replacement Therapy (NRT) Revised: October 2011 Approved: May 21, 2007 Description Nicotine Replacement
Simcoe Muskoka District Health Unit Print Version Medical Directive Number: Topic: Dispensing of Nicotine Replacement Therapy (NRT) Revised: October 2011 Approved: May 21, 2007 Description Nicotine Replacement
STEP Four: ASSIST with Quitting. STEP One: ASK about Tobacco Use TOBACCO CESSATION COUNSELING GUIDESHEET. STEP Two: Strongly ADVISE to Quit
 STEP One: ASK about Tobacco Use Suggested Dialogue Do you ever smoke or use any type of tobacco? I take time to talk with all of my patients about tobacco use because it s important. Medication X often
STEP One: ASK about Tobacco Use Suggested Dialogue Do you ever smoke or use any type of tobacco? I take time to talk with all of my patients about tobacco use because it s important. Medication X often
Best Practice for Smoking Cessation: Pharmacotherapy. Emma Dean Acting Population Health and Health Promotion Coordinator Lead Pharmacist- Smokefree
 Best Practice for Smoking Cessation: Pharmacotherapy Emma Dean Acting Population Health and Health Promotion Coordinator Lead Pharmacist- Smokefree Why is it so hard to quit? People who smoke aren t weak
Best Practice for Smoking Cessation: Pharmacotherapy Emma Dean Acting Population Health and Health Promotion Coordinator Lead Pharmacist- Smokefree Why is it so hard to quit? People who smoke aren t weak
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Addressing Tobacco Use in Iowa
 Addressing Tobacco Use in Iowa A BRIEF TOBACCO INTERVENTION FOR HEALTHCARE PROVIDERS Lorene Mein Beth Turner Alyssa Reichelt DNP, ARNP, FNP-BC MA, CHES MA Mercy Clinics American Lung Association American
Addressing Tobacco Use in Iowa A BRIEF TOBACCO INTERVENTION FOR HEALTHCARE PROVIDERS Lorene Mein Beth Turner Alyssa Reichelt DNP, ARNP, FNP-BC MA, CHES MA Mercy Clinics American Lung Association American
3. Chantix [package insert]. New York, NY: Pfizer, Inc,; Ramon JM, Morchon S, Baena A, Masuet-Aumatell C. Combining varenicline and nicotine
![3. Chantix [package insert]. New York, NY: Pfizer, Inc,; Ramon JM, Morchon S, Baena A, Masuet-Aumatell C. Combining varenicline and nicotine](/thumbs/87/96607870.jpg "3. Chantix [package insert]. New York, NY: Pfizer, Inc,; Ramon JM, Morchon S, Baena A, Masuet-Aumatell C. Combining varenicline and nicotine") How can there be a warning regarding concomitant use of varenicline with nicotine replacement therapy yet patients can be on varenicline and smoke concurrently? April 20, 2017 The United States (US) Preventive
How can there be a warning regarding concomitant use of varenicline with nicotine replacement therapy yet patients can be on varenicline and smoke concurrently? April 20, 2017 The United States (US) Preventive
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
KAREN MYERS, ARNP Certified Tobacco Training Specialist
 KAREN MYERS, ARNP Certified Tobacco Training Specialist At the conclusion of this talk the learner will be able to: discuss the absorption of nicotine and how it is affected Discuss the addictive properties
KAREN MYERS, ARNP Certified Tobacco Training Specialist At the conclusion of this talk the learner will be able to: discuss the absorption of nicotine and how it is affected Discuss the addictive properties
Chronic Obstructive Pulmonary Disease A breathtaking condition
 1. Jan Crouch JC 2. Diane Cruikshank DC 3. Jillian Millar Drysdale JMD 4. Medical Editor 5. Robert Clarke Article: COPD & smoking.doc Section: Growing Older Family Health: Fall 2008 Chronic Obstructive
1. Jan Crouch JC 2. Diane Cruikshank DC 3. Jillian Millar Drysdale JMD 4. Medical Editor 5. Robert Clarke Article: COPD & smoking.doc Section: Growing Older Family Health: Fall 2008 Chronic Obstructive
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Integrated Cardiopulmonary Pharmacology Third Edition
 Integrated Cardiopulmonary Pharmacology Third Edition Chapter 13 Pharmacologic Management of Asthma, Chronic Bronchitis, and Emphysema Multimedia Directory Slide 7 Slide 12 Slide 60 COPD Video Passive
Integrated Cardiopulmonary Pharmacology Third Edition Chapter 13 Pharmacologic Management of Asthma, Chronic Bronchitis, and Emphysema Multimedia Directory Slide 7 Slide 12 Slide 60 COPD Video Passive
Smoking Cessation Strategies: What Works?
 Smoking Cessation Strategies: What Works? Andrew M. Busch, Ph.D. Centers For Behavioral and Preventive Medicine The Miriam Hospital Department of Psychiatry and Human Behavior Alpert Medical School of
Smoking Cessation Strategies: What Works? Andrew M. Busch, Ph.D. Centers For Behavioral and Preventive Medicine The Miriam Hospital Department of Psychiatry and Human Behavior Alpert Medical School of
Chantix Label Update 2018
 Chantix Label Update 2018 Chantix (varenicline) Prescribing Information Chantix Prescribing Info URL and Disclaimer Please refer to the full Prescribing Information on important treatment considerations
Chantix Label Update 2018 Chantix (varenicline) Prescribing Information Chantix Prescribing Info URL and Disclaimer Please refer to the full Prescribing Information on important treatment considerations
MEDICATION GUIDE WELLBUTRIN (WELL byu-trin) (bupropion hydrochloride) Tablets
 (bupropion hydrochloride) Tablets") Page 25 the 75- or 100-mg tablets. The 100-mg tablet must be administered 4 times daily with at least 4 hours between successive doses, in order not to exceed the limit of 150 mg in a single dose. WELLBUTRIN
Page 25 the 75- or 100-mg tablets. The 100-mg tablet must be administered 4 times daily with at least 4 hours between successive doses, in order not to exceed the limit of 150 mg in a single dose. WELLBUTRIN
Update on SMOKING CESSATION. Supporting the PHO Performance Programme. 38 BPJ Issue 33
 Update on SMOKING CESSATION Supporting the PHO Performance Programme 38 BPJ Issue 33 Key concepts The rate of smoking among New Zealanders is slowly reducing, however more work needs to be done to further
Update on SMOKING CESSATION Supporting the PHO Performance Programme 38 BPJ Issue 33 Key concepts The rate of smoking among New Zealanders is slowly reducing, however more work needs to be done to further
St. Joseph s Health PROVIDER BRIEF. Tobacco Dependence Treatment Guidelines Perinatal and Postpartum Women
 St. Joseph s Health PROVIDER BRIEF Tobacco Dependence Treatment Guidelines Perinatal and Postpartum Women Quitting smoking is perhaps the most important action a pregnant woman can do to ensure the health
St. Joseph s Health PROVIDER BRIEF Tobacco Dependence Treatment Guidelines Perinatal and Postpartum Women Quitting smoking is perhaps the most important action a pregnant woman can do to ensure the health
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable
 THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
SMART STEPS towards a tobacco-free life
 SMART STEPS towards a tobacco-free life Ready to Quit Smoking? You decide when. We ll show you how. Smart steps... Ready to Put Tobacco Behind You? Congratulations on deciding to quit! Quitting tobacco
SMART STEPS towards a tobacco-free life Ready to Quit Smoking? You decide when. We ll show you how. Smart steps... Ready to Put Tobacco Behind You? Congratulations on deciding to quit! Quitting tobacco
ASHP Therapeutic Position Statement on the Cessation of Tobacco Use
 580 ASHP Therapeutic Position Statements ASHP Therapeutic Position Statement on the Cessation of Tobacco Use Position The American Society of Health-System Pharmacists (ASHP) discourages all use of tobacco
580 ASHP Therapeutic Position Statements ASHP Therapeutic Position Statement on the Cessation of Tobacco Use Position The American Society of Health-System Pharmacists (ASHP) discourages all use of tobacco
7 DAY QUIT SMOKING CHALLENGE 7 DAY QUIT SMOKING CHALLENGE 7 DAY QUIT SMOKING PDF YOU CAN QUIT SMOKING. QUIT SMOKING CDC 1 / 5
 7 DAY QUIT SMOKING PDF YOU CAN QUIT SMOKING. QUIT SMOKING CDC 1 / 5 2 / 5 3 / 5 7 day quit smoking pdf 7 Your guide to quitting smoking This guide is for smokers who want to quit and stay quit. Just like
7 DAY QUIT SMOKING PDF YOU CAN QUIT SMOKING. QUIT SMOKING CDC 1 / 5 2 / 5 3 / 5 7 day quit smoking pdf 7 Your guide to quitting smoking This guide is for smokers who want to quit and stay quit. Just like
Over the Road Truck Driver Who Smokes
 Continuing Medical Education Case Presentation 1 CME Credit Physicians Physician Assistants Nurse Practitioners Over the Road Truck Driver Who Smokes RELEASE & REVIEW DATE This activity was last reviewed
Continuing Medical Education Case Presentation 1 CME Credit Physicians Physician Assistants Nurse Practitioners Over the Road Truck Driver Who Smokes RELEASE & REVIEW DATE This activity was last reviewed
Assisting Patients with Tobacco Cessation: A Behavioral Approach
 Assisting Patients with Tobacco Cessation: A Behavioral Approach (a one-hour continuing education program) This one-hour continuing education program provides an overview of behavioral approaches for facilitating
Assisting Patients with Tobacco Cessation: A Behavioral Approach (a one-hour continuing education program) This one-hour continuing education program provides an overview of behavioral approaches for facilitating
Pharmacotherapy for Smoking Cessation
 Pharmacotherapy for Smoking Cessation (a one-hour continuing education program) This program provides an overview of all FDA-approved medications for cessation (nicotine patch, lozenge, gum, inhaler, nasal
Pharmacotherapy for Smoking Cessation (a one-hour continuing education program) This program provides an overview of all FDA-approved medications for cessation (nicotine patch, lozenge, gum, inhaler, nasal
TB and Tobacco: Pharmacotherapy for Tobacco. Cessation. Cathy Cook, LCSW, CTTS
 TB and Tobacco: Pharmacotherapy for Tobacco Cessation Cathy Cook, LCSW, CTTS Objectives 1. Describe the pharmacokinetics of nicotine to aid providers in treating TB patients who use tobacco. 2. List the
TB and Tobacco: Pharmacotherapy for Tobacco Cessation Cathy Cook, LCSW, CTTS Objectives 1. Describe the pharmacokinetics of nicotine to aid providers in treating TB patients who use tobacco. 2. List the
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
Disclaimers. Smoking and Smoking Cessation. Worldwide. Objectives. Statistics at Home. Smoking Epidemic 16/10/2017
 Disclaimers Smoking and Smoking Cessation Dr. Janneke Gradstein CCFP(EM) Yarmouth, NS Received CHA Funding 6 th Annual Ottawa Conference: State of the Art Clinical Approaches to smoking cessation. References
Disclaimers Smoking and Smoking Cessation Dr. Janneke Gradstein CCFP(EM) Yarmouth, NS Received CHA Funding 6 th Annual Ottawa Conference: State of the Art Clinical Approaches to smoking cessation. References
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
TREATMENT OF NICOTINE DEPENDENCE
 TREATMENT OF NICOTINE DEPENDENCE Introduction Most commonly used substance the world over. Largest cause of preventable death worldwide. Leading causes of smoking related death Cardiovascular diseases
TREATMENT OF NICOTINE DEPENDENCE Introduction Most commonly used substance the world over. Largest cause of preventable death worldwide. Leading causes of smoking related death Cardiovascular diseases
Outpatient Tobacco Addiction Treatment Pathway Additional Notes
 Outpatient Tobacco Addiction Treatment Pathway Additional Notes First Line: Varenicline (provide in conjunction with counselling/support, but if such support is refused or is not available, this should
Outpatient Tobacco Addiction Treatment Pathway Additional Notes First Line: Varenicline (provide in conjunction with counselling/support, but if such support is refused or is not available, this should
COPD in primary care: reminder and update
 COPD in primary care: reminder and update Managing COPD continues to be a major feature of primary care, particularly in practices with a high proportion of M ori and Pacific peoples. COPDX clinical practice
COPD in primary care: reminder and update Managing COPD continues to be a major feature of primary care, particularly in practices with a high proportion of M ori and Pacific peoples. COPDX clinical practice
Background. Abstinence rates associated with varenicline
 What are the range of abstinence rates for varenicline for smoking cessation? Do they differ based on treatment duration? Are there any studies utilizing 3-4 months of varenicline treatment? Background
What are the range of abstinence rates for varenicline for smoking cessation? Do they differ based on treatment duration? Are there any studies utilizing 3-4 months of varenicline treatment? Background
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
DRAFT NAVMEDCENPTSVAINST A
 DRAFT --------- NAVMEDCENPTSVAINST 6200.5A NAVMEDCENPTSVA INSTRUCTION 6200.5A Subj: TOBACCO CESSATION PROGRAM POLICY Ref: (a) OPNAVINST 6100.2, Health Promotion Program (b) NAVMEDCENPTSVAINST 6280.1 E,
DRAFT --------- NAVMEDCENPTSVAINST 6200.5A NAVMEDCENPTSVA INSTRUCTION 6200.5A Subj: TOBACCO CESSATION PROGRAM POLICY Ref: (a) OPNAVINST 6100.2, Health Promotion Program (b) NAVMEDCENPTSVAINST 6280.1 E,
Cessation of Smoking By Nicotine Replacement Therapy
 Review Article ISSN: 0974-6943 Mamatha. J et al / Journal of Pharmacy Research 2017,11(5), Available online through http://jprsolutions.info Cessation of Smoking By Nicotine Replacement Therapy Mamatha.
Review Article ISSN: 0974-6943 Mamatha. J et al / Journal of Pharmacy Research 2017,11(5), Available online through http://jprsolutions.info Cessation of Smoking By Nicotine Replacement Therapy Mamatha.
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC)
") DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) Derbyshire Formulary for Nicotine Replacement Therapy (NRT) 1. Supporting Smokers to stop smoking The most effective method to quit smoking is by quitting
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE (JAPC) Derbyshire Formulary for Nicotine Replacement Therapy (NRT) 1. Supporting Smokers to stop smoking The most effective method to quit smoking is by quitting
What else do I need to know about antidepressant medicines?
 MEDICATION GUIDE Bupropion (bue-proe-pee-on) Hydrochloride Extended-Release Tablets (SR), 200 mg Read this Medication Guide carefully before you start taking bupropion hydrochloride extended-release tablets
MEDICATION GUIDE Bupropion (bue-proe-pee-on) Hydrochloride Extended-Release Tablets (SR), 200 mg Read this Medication Guide carefully before you start taking bupropion hydrochloride extended-release tablets
Tobacco use and dependence: an updated review of treatments
 Activity CME Home Page Why should I treat tobacco dependence? How do I treat tobacco users? Ask Advise Assess Assist Arrange Motivational Interviewing Strategies Enhancing Motivation to Quit Tobacco The
Activity CME Home Page Why should I treat tobacco dependence? How do I treat tobacco users? Ask Advise Assess Assist Arrange Motivational Interviewing Strategies Enhancing Motivation to Quit Tobacco The
Health Professional Manual
 Health Professional Manual Session: Smoking Cessation Smoking and COPD Strategies for quitting smoking Adapted from the Living Well with COPD program (2nd edition), Montreal Chest Institute, Canada SESSION
Health Professional Manual Session: Smoking Cessation Smoking and COPD Strategies for quitting smoking Adapted from the Living Well with COPD program (2nd edition), Montreal Chest Institute, Canada SESSION
Kicking the Habit Pharmacological Help for Smokers
 Kicking the Habit Pharmacological Help for Smokers Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant Clinical Assistant Professor, Univ. of Maryland Special Thanks to Teisha Robertson, PharmD
Kicking the Habit Pharmacological Help for Smokers Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant Clinical Assistant Professor, Univ. of Maryland Special Thanks to Teisha Robertson, PharmD
CARE OF THE ADULT COPD PATIENT
 CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
Anyone who smokes and/or has shortness of breath and sputum production could have COPD
 COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
Effective Treatments for Tobacco Dependence
 Effective Treatments for Tobacco Dependence Abigail Halperin MD, MPH Director, University of Washington Tobacco Studies Program Ken Wassum Associate Director of Clinical Development and Support Quit for
Effective Treatments for Tobacco Dependence Abigail Halperin MD, MPH Director, University of Washington Tobacco Studies Program Ken Wassum Associate Director of Clinical Development and Support Quit for
Smoking Cessation CHAPTER 1. Alexander V. Prokhorov, Kentya H. Ford, and Karen Suchanek Hudmon. Overview. Introduction. Smoking and lung cancer
 CHAPTER 1 Smoking Cessation Alexander V. Prokhorov, Kentya H. Ford, and Karen Suchanek Hudmon Overview Tobacco use is a public health issue of enormous importance, and smoking is the primary risk factor
CHAPTER 1 Smoking Cessation Alexander V. Prokhorov, Kentya H. Ford, and Karen Suchanek Hudmon Overview Tobacco use is a public health issue of enormous importance, and smoking is the primary risk factor
COPD/Asthma. Prudence Twigg, AGNP
 COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
Customize Your Quit \ 2 1 / Tailored treatment to help stop smoking. Customize Your Quit. Customize Your Quit
 1 / \ 2 Customize Your Quit McNeil Consumer Healthcare, division of Johnson & Johnson Inc., Markham, Canada L3R 5L2 Johnson & Johnson Inc. 2017 PSNRT15-80E Tailored treatment to help stop smoking 3 / \
1 / \ 2 Customize Your Quit McNeil Consumer Healthcare, division of Johnson & Johnson Inc., Markham, Canada L3R 5L2 Johnson & Johnson Inc. 2017 PSNRT15-80E Tailored treatment to help stop smoking 3 / \
MEDICATION GUIDE WELLBUTRIN (WELL byu-trin) (bupropion hydrochloride) Tablets
 (bupropion hydrochloride) Tablets") MEDICATION GUIDE WELLBUTRIN (WELL byu-trin) (bupropion hydrochloride) Tablets Read this Medication Guide carefully before you start using WELLBUTRIN and each time you get a refill. There may be new information.
MEDICATION GUIDE WELLBUTRIN (WELL byu-trin) (bupropion hydrochloride) Tablets Read this Medication Guide carefully before you start using WELLBUTRIN and each time you get a refill. There may be new information.
People with asthma who smoke. The combination of asthma, a chronic airway disease, and smoking increases the risk of COPD even more.
 COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
WANTED. Pharmacists to Help Patients Quit Smoking: Best practices and updates in cessation treatment. Robin Corelli, PharmD
 WANTED Pharmacists to Help Patients Quit Smoking: Best practices and updates in cessation treatment Robin Corelli, PharmD UCSF School of Pharmacy Karen Hudmon, DrPH, MS, RPh Purdue University College of
WANTED Pharmacists to Help Patients Quit Smoking: Best practices and updates in cessation treatment Robin Corelli, PharmD UCSF School of Pharmacy Karen Hudmon, DrPH, MS, RPh Purdue University College of
Effective date: October 15, 2009
 COLLECTIVE PRESCRIPTION Start According to a protocol: Yes No Effective date: October 15, 2009 Next review date: October 15, 2012 Professionals who can dispense the prescription Community pharmacists working
COLLECTIVE PRESCRIPTION Start According to a protocol: Yes No Effective date: October 15, 2009 Next review date: October 15, 2012 Professionals who can dispense the prescription Community pharmacists working
SECTION 17: NICOTINE REPLACEMENT. Formulary and Prescribing Guidelines
 SECTION 17: NICOTINE REPLACEMENT Formulary and Prescribing Guidelines 17.1 Introduction These guidelines should be used in conjunction with EPUT No Smoking Policy (HRP20) for service users who are 12 years
SECTION 17: NICOTINE REPLACEMENT Formulary and Prescribing Guidelines 17.1 Introduction These guidelines should be used in conjunction with EPUT No Smoking Policy (HRP20) for service users who are 12 years
1. Describe the benefits of smoking cessation. 2. List the withdrawal symptoms of quitting smoking. Cessation
 Time to Butt Out Adil Virani, BSc (Pharm), Pharm D, FCSHP Objectives After this presentation, participants should be able to: 1. Describe the benefits of smoking cessation 2. List the withdrawal symptoms
Time to Butt Out Adil Virani, BSc (Pharm), Pharm D, FCSHP Objectives After this presentation, participants should be able to: 1. Describe the benefits of smoking cessation 2. List the withdrawal symptoms
Wanting to Get Pregnant
 Continuing Medical Education COPD Case Presentation LEARNING OBJECTIVES Those completing this activity will receive information that should allow them to Assist a patient in developing a quit plan; Advise
Continuing Medical Education COPD Case Presentation LEARNING OBJECTIVES Those completing this activity will receive information that should allow them to Assist a patient in developing a quit plan; Advise
Formulary and Prescribing Guidelines
 Formulary and Prescribing Guidelines SECTION 17: NICOTINE REPLACEMENT THERAPY 17.1 Introduction These guidelines should be used in conjunction with SEPT No Smoking Policy (HRP20) and for service users
Formulary and Prescribing Guidelines SECTION 17: NICOTINE REPLACEMENT THERAPY 17.1 Introduction These guidelines should be used in conjunction with SEPT No Smoking Policy (HRP20) and for service users