PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
|
|
|
- Angela Day
- 5 years ago
- Views:
Transcription
1 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
2 TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted therapy -RT -Hormone
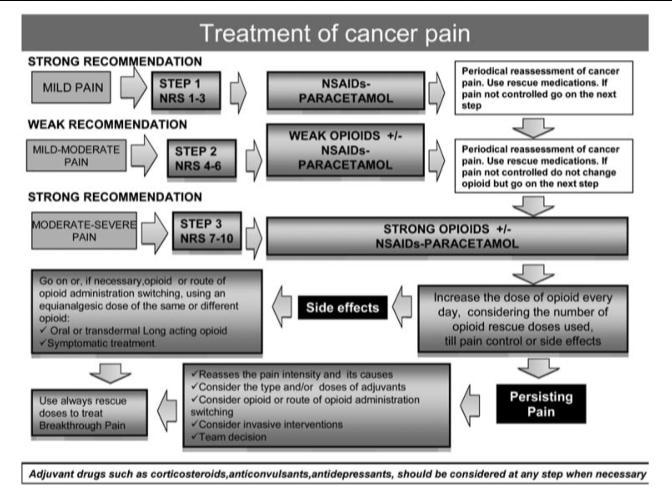
3 TREATMENT IN ONCOLOGY Palliative treatment : quality of life, prolong life, relieve symptom -CMT, Targeted therapy -RT -Sx -Others -BSC
4 Treatment outline of early or locally advanced cancer Early or locally advanced cancer Primary treatment: surgery Neoadjuvant chemotherapy/ radiotherapy Adjuvant chemotherapy / radiotherapy Unresectable Surveillance Recurrent disease In remission
5 Treatment outline of advanced or metastatic cancer Advanced or metastatic cancer Resectable Unresectable Surgery Postoperative Chemotherapy/ radiotherapy Palliative chemotherapy/ radiotherapy Response Second-line Not response/ Too toxic Best supportive care
6 ASSESSMENT BY ONCOLOGY TEAM Benefits/Burdens of anticancer therapy - Natural of specific tumor - Potential for response to further treatment - Potential for treatment-related toxicities - Patient s understanding of disease prognosis - Goal and meaning of anticancer therapy for patient/family/caregivers - Impairment of vital organs - Performance status - Serious comorbid conditions
7 ASSESSMENT BY ONCOLOGY TEAM Patient/family/caregivers goals/values/expectations/priorities - Shared decision-making with patient/family/caregivers - Advance care planning - Goals and meaning of anticancer therapy - Quality of life
8 ASSESSMENT BY ONCOLOGY TEAM Symptom management - Pain - Dyspnea - Anorexia/cachexia - Nausea/vomiting - Constipation - Diarrhea - Etc.
9
10
11
12
13
14
15 DOMAINS FOR PAIN MANAGEMENT OUTCOME : 4 A s Analgesia Activities of Daily Living Adverse Events Aberrant Drug-Taking Behaviors
16
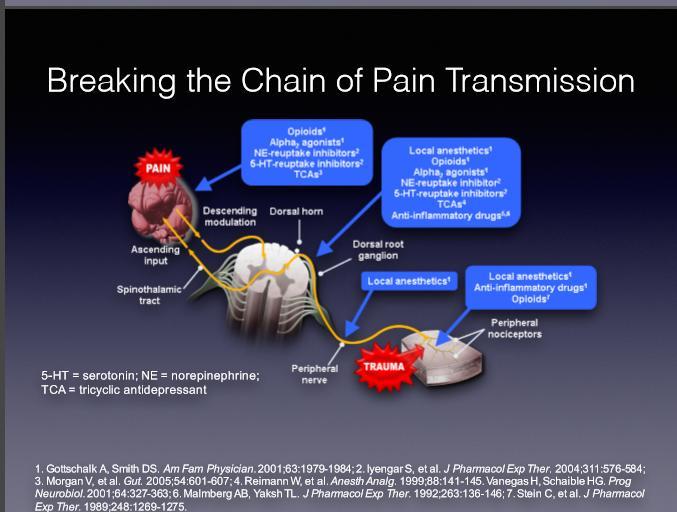
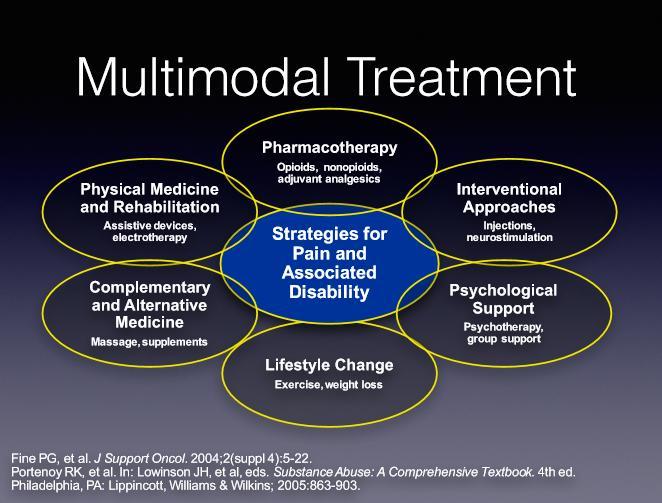
17 CANCER PAIN MANGEMENT STRATEGIES Pharmacologic strategies - Nonopioid analgesics - Acetaminophen - Nonsteroidal anti-inflammatory drugs - Opioid analgesics - Coanalgesics (adjuvant analgesics) Psychological strategies - Hypnosis or relaxation with imagery - Cognitive-behavioral methods
18 CANCER PAIN MANGEMENT STRATEGIES Physical strategies - Massage - Exercise - Transcutaneous electrical nerve stimulation (TENS) - Acupucture Nerve blocks Radiation therapy Chemotherapy
19 OPIOID ANALGESICS : CANCER PAIN Used most often in the management of severe pain : - Effectiveness - Ease of titration - Favorable risk-to-benefit ratio Routes of administration - Oral - Transdermal - Intraspinal : epidural or intrathecal
20
21 OPIOID FORMULATIONS TYPE OF DRUG Pure µ-opioid receptor agonists Dual mechanism opioids Rapid onset (transmucosal) Immediate release Modified release (long acting) Available with co-analgesic Only available with co-analgesic EXAMPLES Morphine, hydromorphone, fentanyl, oxycodone Tramadol, tapentadol Fentanyl, alfentanil, sufentanil, diamorphine Tramadol, oxycodone Morphine, methadone, oxycodone Oxycodone, tramadol, codeine Hydrocodone
22
23

24 Codeine natural opioid ADR : Constipation Onset Duration Dosage Ceiling dose Shift when 30 mins 4-6 hrs mg PO q 4-6 hrs 120 mg/dose not response at 60 mg q 4 hrs


25 Tramadol synthetic opioid Action: MOPr and SNRI ADR : N/V, Dizziness Onset Duration 1 hr 8 hrs Dosage Ceiling dose Shift when mg PO q 6-8 hrs 100 mg/dose not response at 400 mg/day



26 Morphine natural opioid Injection Oral Immediate release Controlled release Onset : IV < 5 mins MO IR min MST 1 hr Kapanol 2-4 hr PotencyOral = 1/3 IV (1 st pass metabolism effect) Sustained release MST 10, 30 mg Extended release Kapanol 20, 50 mg


27 Oxycodone semisynthetic opioid Onset 15 min for IR, Stable over 12 hr for CR Initial dose 5 15 mg PO q 4-6 h (IR) 10 mg PO q 12 h (CR) Dosage mg PO q 4-6 h (titrate up 25% q 12 hr for CR)


28 Fentanyl synthetic opioid Highly lipid soluble Onset Duration Prep hrs 72 hrs/patch 12, 25, 50 mcg/hr Initiation Naïve to opioid mcg/hr Do not forget to prescribe bridging analgesics in first hr
29 ADVERSE DRUG REACTION OF OPIOID ANALGESIC DRUGS







30 Skin Neuro GI ADVERSE REACTION of opioids usage Sedation Confusion Myoclonus Respiratory depression Nausea / Vomiting Constipation Itching Histamine release Dry lips Urinary retention
31 NEUROLOGICAL ADR of opioids usage Sedation Confusion Myoclonus Reduce 25% Methylphenidate IR Light Exposure T Reduce 25 % TCA LT ADR Baclofen, Valium Respiratory depression Naloxone 0.2 mg IV push q 2-3 min Dry mouth NaHCO 3 mouthwash 3-4 times/day T Urinary retention Foley s cath T. T = Tolerable ADR

32 GASTROINTESTINAL ADR of opioids usage Nausea / Vomiting Co-administration antiemetics Constipation Stimulant laxative Stool softener *** AVOID bulk forming *** T T = Tolerable ADR
33 OPIOID SWITCHING Opioid rotation ( or switching) is a change in opioid drug or route of administration with the goal of improving outcomes. Opioid therapy for acute or chronic pain requires individualization of the dose, with the objective of identifying a favorable balance between analgesia and side effects.
34 INDICATIONS FOR SWITCHING Occurrence of intolerable adverse effects during dose titration Poor analgesic efficacy despite aggressive dose titration Problematic drug-drug interactions Preference or need for a different route of administration Change in clinical status (e.g. concern about drug abuse) or clinical setting that suggests benefit from an opioid with different pharmacokinetic properties Financial or drug-availability considerations

 MO (IV) Oxycontin Codeine")

35 STEP 1 : EFFICACY OPIOID ROTATION Calculate Equianalgesic dose (the dose in steady state provide the same analgesic response) Require special consideration MO (PO) MO (IV) Oxycontin Codeine Tramadol Fentanyl TTS Methadone IV 30 mg 10 mg 15 mg 200 mg 250 mg 12 mcg/hr 8 mg Methadone Oral 16 mg 1 x 1.5 x 20 x 25 x 1.2 x 0.8 x x 2.

36 STEP 2 : SAFETY Pathogenesis : Variation of MOPr subtype in different person Identified Automatic Dose Reduction Windows ~ % due to incomplete cross-tolerance 25 % in General population 50 % in currently on High dose Elderly/Frailty

37 STEP 3 : INDIVIDUALIZED Re-assessment Titration up 25% if inadequate Rescue dosing prescription % (1/6 of total daily dose)
38 EXAMPLE A 56 years old female who has advance stage CA breast which currently on Kapanol (50) 2 tab PO at 8PM MST (10) 2 tab PO at 8AM MO IR (10) 2 3 tab per day Kapanol was sold out from hospital. So you need to change it to another drugs
39 EXAMPLE Step 1: Calculate MEDD [(100+20) 3] + [10x3 3] mg of MO IV per day Step 2 : calculate ADRW
40 EXAMPLE Switch to Oxycontin 37.5 x 1.5 = mg Order Oxycontin (30) 1 tab PO q 12 h
 1 tab PO prn q 4-6h Reassessment If not")
41 EXAMPLE Step 3: Breakthrough : 6.25 mg MO IR (10) 1 tab PO prn q 4-6h Reassessment If not adequate +25% (~9-10 MO equivalence)
42 Jirawat Thanestada, M.D. SUMMARY
43
44

45
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Opioid Conversion Guidelines
 Opioid Conversion Guidelines March 2015 Gippsland Region Palliative Care Consortium Clinical Practice Group Title Keywords Ratified Opioid, Conversion, Drug, Therapy, Palliative, Guideline, Palliative,
Opioid Conversion Guidelines March 2015 Gippsland Region Palliative Care Consortium Clinical Practice Group Title Keywords Ratified Opioid, Conversion, Drug, Therapy, Palliative, Guideline, Palliative,
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
Opioid Case Studies. Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN. September 29, MFMER slide-1
 Opioid Case Studies Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN September 29, 2016 2015 MFMER slide-1 Disclosures Relevant Financial Relationship(s) None Off Label and/or
Opioid Case Studies Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN September 29, 2016 2015 MFMER slide-1 Disclosures Relevant Financial Relationship(s) None Off Label and/or
1/21/14. Cancer Related Pain: Case-Based Pharmacology. Conflicts of Interest. Learning Objective
 Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Pain Management in Hospice and Palliative Care
 Pain Management in Hospice and Palliative Care A Case-based Approach JoAnne Nowak, M.D. Merrimack Valley Hospice Revised November 2011 Objectives Use a case study approach to stimulate discussion and illustrate
Pain Management in Hospice and Palliative Care A Case-based Approach JoAnne Nowak, M.D. Merrimack Valley Hospice Revised November 2011 Objectives Use a case study approach to stimulate discussion and illustrate
Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management
 Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management Eric Roeland, MD GI Oncology Palliative Medicine Pancreatic Cancer Patient Tool Belt Chemotherapy Surgery Pain & Symptom
Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management Eric Roeland, MD GI Oncology Palliative Medicine Pancreatic Cancer Patient Tool Belt Chemotherapy Surgery Pain & Symptom
Review of Pain Management with Clinical and Regulatory Updates
 Review of Pain Management with Clinical and Regulatory Updates Palliative Care Collaborative: 8 th Annual Regional Conference October 10, 2014 Michael Stellini, M.D.,M.S. Medical Director, Hospice and
Review of Pain Management with Clinical and Regulatory Updates Palliative Care Collaborative: 8 th Annual Regional Conference October 10, 2014 Michael Stellini, M.D.,M.S. Medical Director, Hospice and
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
Equianalgesic Dosing: Making Opioid Interchange Easier. Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine
 Equianalgesic Dosing: Making Opioid Interchange Easier Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine 1 Why Change Opioids? Side Effects Insufficient Pain
Equianalgesic Dosing: Making Opioid Interchange Easier Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine 1 Why Change Opioids? Side Effects Insufficient Pain
Analgesia. This is widely used in palliative care. It has antipyretic and analgesic effects but no anti-
 Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Pain management. Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD
 Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Narcotic Analgesics. Jacqueline Morgan March 22, 2017
 Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Management of Cancer Pain
 Management of Cancer Pain Mihir M. Kamdar, MD Associate Director, Palliative Care Director, MGH Cancer Pain Clinic Depts of Anesthesia Pain/Palliative Care Massachusetts General Hospital None Disclosures
Management of Cancer Pain Mihir M. Kamdar, MD Associate Director, Palliative Care Director, MGH Cancer Pain Clinic Depts of Anesthesia Pain/Palliative Care Massachusetts General Hospital None Disclosures
Opioid Pearls and Acute Pain Management
 Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
FDA hormone replacement therapy Web site 6
 TABLE OF CONTENTS Caring for pain at UIMCC 1-5 FDA hormone replacement therapy Web site 6 P&T Committee Formulary Action - September 2003 6 Caring for pain at UIMCC The International Association for the
TABLE OF CONTENTS Caring for pain at UIMCC 1-5 FDA hormone replacement therapy Web site 6 P&T Committee Formulary Action - September 2003 6 Caring for pain at UIMCC The International Association for the
Long Term Care Formulary HCD - 08
 1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline
 GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
GG&C Chronic Non Malignant Pain Opioid Prescribing Guideline Background Persistent pain is common, affecting around five million people in the UK. For many sufferers, pain can be frustrating and disabling,
Pain management in Paediatric Palliative Care. Dr Jane Nakawesi 14 th August 2017
 Pain management in Paediatric Palliative Care Dr Jane Nakawesi 14 th August 2017 Content Management of pain in children Non pharmacological Pharmacological Exit level outcomes The participants will: Know
Pain management in Paediatric Palliative Care Dr Jane Nakawesi 14 th August 2017 Content Management of pain in children Non pharmacological Pharmacological Exit level outcomes The participants will: Know
Dose equivalent of fentanyl patch to oxycontin
 Dose equivalent of fentanyl patch to oxycontin 10-3-2018 Detailed dosage guidelines and administration information for OxyContin (oxycodone hydrochloride). Includes dose adjustments, warnings and precautions.
Dose equivalent of fentanyl patch to oxycontin 10-3-2018 Detailed dosage guidelines and administration information for OxyContin (oxycodone hydrochloride). Includes dose adjustments, warnings and precautions.
Opioid Rotation. Dr Bruno Gagnon, M.D., M.Sc.
 Opioid Rotation Dr Bruno Gagnon, M.D., M.Sc. Associate Professor Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval Consultant in Palliative Medicine CHU de Québec-Université
Opioid Rotation Dr Bruno Gagnon, M.D., M.Sc. Associate Professor Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval Consultant in Palliative Medicine CHU de Québec-Université
10 mg hydrocodone equals how much oxycodone
 Cari untuk: Cari Cari 10 mg hydrocodone equals how much oxycodone Posts about dilaudid 8 vs oxycodone 30 written by buyprescriptionmedication. Can you help me with the conversion of Oxycodone IR (5mg tab)
Cari untuk: Cari Cari 10 mg hydrocodone equals how much oxycodone Posts about dilaudid 8 vs oxycodone 30 written by buyprescriptionmedication. Can you help me with the conversion of Oxycodone IR (5mg tab)
Interprofessional Webinar Series
 Interprofessional Webinar Series Opioids in the Medically Ill: Principles of Administration Russell K. Portenoy, MD Chief Medical Officer MJHS Hospice and Palliative Care Director MJHS Institute for Innovation
Interprofessional Webinar Series Opioids in the Medically Ill: Principles of Administration Russell K. Portenoy, MD Chief Medical Officer MJHS Hospice and Palliative Care Director MJHS Institute for Innovation
RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM ACPE UAN: 107-000-14-016-L05-P Activity Type: Application-Based 0.1 CEU/1.0 hr Learning Objectives for
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM ACPE UAN: 107-000-14-016-L05-P Activity Type: Application-Based 0.1 CEU/1.0 hr Learning Objectives for
PAIN. TREATMENT TABLES Analgesics. NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose
 Duration Initial Dose") NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly
 Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
Drug Information Common to the Class of Extended-Release and Long-Acting Opioid Analgesics (ER/LA opioid analgesics) Avinza Butrans
 Avinza Butrans") FDA Blueprint for Prescriber Education for Extended-Release and Long-Acting Opioid Analgesics 7/9/2012 Drug Information Common to the Class of Extended-Release and Long-Acting Opioid Analgesics (ER/LA
FDA Blueprint for Prescriber Education for Extended-Release and Long-Acting Opioid Analgesics 7/9/2012 Drug Information Common to the Class of Extended-Release and Long-Acting Opioid Analgesics (ER/LA
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015
 Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Opioid Conversions Mixture of Science and Art
 Opioid Conversions Mixture of Science and Art Matthew J. Pingree, MD Assistant Professor Division of Pain Medicine Physical Medicine and Rehabilitation and Anesthesiology Mayo Clinic, Rochester Pingree.Matthew@Mayo.edu
Opioid Conversions Mixture of Science and Art Matthew J. Pingree, MD Assistant Professor Division of Pain Medicine Physical Medicine and Rehabilitation and Anesthesiology Mayo Clinic, Rochester Pingree.Matthew@Mayo.edu
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Pain is a more terrible Lord of mankind than even death itself.
 CHRONIC OPIOID RX FOR NON-MALIGNANT PAIN Gerald M. Aronoff, M.D., DABPM Med. Dir., Carolina Pain Assoc Charlotte, North Carolina, USA Pain Pain is a more terrible Lord of mankind than even death itself.
CHRONIC OPIOID RX FOR NON-MALIGNANT PAIN Gerald M. Aronoff, M.D., DABPM Med. Dir., Carolina Pain Assoc Charlotte, North Carolina, USA Pain Pain is a more terrible Lord of mankind than even death itself.
Cancer Pain: A Clinical Overview. Linda A. King, MD Section of Palliative Care and Medical Ethics
 Cancer Pain: A Clinical Overview Linda A. King, MD Section of Palliative Care and Medical Ethics Objectives Define Palliative Care Review prevalence of cancer pain Know barriers to cancer pain management
Cancer Pain: A Clinical Overview Linda A. King, MD Section of Palliative Care and Medical Ethics Objectives Define Palliative Care Review prevalence of cancer pain Know barriers to cancer pain management
Analgesics: Management of Pain In the Elderly Handout Package
 Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
E-Learning Module N: Pharmacological Review
 E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
Fighting the Good Fight: How to Convert Opioids Just Right!
 Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Module 2 Pain Management. Handouts. Pain Is... Please click the links button under the video. You can print and/or save the handouts.
 E L N E C End-of-Life Nursing Education Consortium SuperCore Curriculum Module 2 Pain Management Handouts Please click the links button under the video. You can print and/or save the handouts. Pain Is...
E L N E C End-of-Life Nursing Education Consortium SuperCore Curriculum Module 2 Pain Management Handouts Please click the links button under the video. You can print and/or save the handouts. Pain Is...
PAIN MANAGEMENT COMPETENCY
 PAIN MANAGEMENT COMPETENCY What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Pain is always subjective.
PAIN MANAGEMENT COMPETENCY What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Pain is always subjective.
Pancreatic cancer Palliative Care
 Pancreatic cancer Palliative Care Snežana Bošnjak Institute for Oncology and Radiology of Serbia Dept. Supportive Oncology & Pall Care Serbia, Belgrade Pancreatic Cancer: Palliative Care Abdominal / epigastric
Pancreatic cancer Palliative Care Snežana Bošnjak Institute for Oncology and Radiology of Serbia Dept. Supportive Oncology & Pall Care Serbia, Belgrade Pancreatic Cancer: Palliative Care Abdominal / epigastric
THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT
 1 THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT Jaegtvolden 4-5 June 2012 14. 12. 2012 2 1 3 WHO ANALGESIC LADDER (1996) NSAID +/- Adjuvant STEP II OPIODS Opids for mild to moderate
1 THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT Jaegtvolden 4-5 June 2012 14. 12. 2012 2 1 3 WHO ANALGESIC LADDER (1996) NSAID +/- Adjuvant STEP II OPIODS Opids for mild to moderate
Pain Management in the Hospital
 E P E C O Pain Management in the Hospital Denise Waugh, MD FACEP FAAHPM Medical Director of Palliative Care Services Scott and White Healthcare 724-6859 Pain is a more terrible lord of mankind than even
E P E C O Pain Management in the Hospital Denise Waugh, MD FACEP FAAHPM Medical Director of Palliative Care Services Scott and White Healthcare 724-6859 Pain is a more terrible lord of mankind than even
B. Long-acting/Extended-release Opioids
 4 Opioid tolerance is assumed in patients already taking fentanyl 25 mcg/hr OR daily doses of the following oral agents for 1 week: 60 mg oral morphine, 30 mg oxycodone, 8 mg hydromorphone, 25 mg of oxymorphone
4 Opioid tolerance is assumed in patients already taking fentanyl 25 mcg/hr OR daily doses of the following oral agents for 1 week: 60 mg oral morphine, 30 mg oxycodone, 8 mg hydromorphone, 25 mg of oxymorphone
Managing Care at End of Life:
 Managing Care at End of Life: Physical Suffering Pain & Dyspnea Verna Sellers, MD, MPH, AGSF Medical Director Centra PACE Lynchburg, Virginia 1 Speaker Disclosures: Dr. Sellers has disclosed that she has
Managing Care at End of Life: Physical Suffering Pain & Dyspnea Verna Sellers, MD, MPH, AGSF Medical Director Centra PACE Lynchburg, Virginia 1 Speaker Disclosures: Dr. Sellers has disclosed that she has
BASICS OF OPIOID PRESCRIBING 10:30-11:45AM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
Slide 1. Slide 2. Slide 3. Opioid (Narcotic) Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists
 Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists") Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Opioid Use in Serious Illness
 Opioid Use in Serious Illness Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Opioid Use in Serious Illness Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Po dilaudid versus iv dilaudid
 Po dilaudid versus iv dilaudid Search IM/IV/SC 120 mg ratios of morphine to methadone in patients with neuropathic pain versus non-neuropathic an equianalgesic ratio for PO. Dilaudid official prescribing
Po dilaudid versus iv dilaudid Search IM/IV/SC 120 mg ratios of morphine to methadone in patients with neuropathic pain versus non-neuropathic an equianalgesic ratio for PO. Dilaudid official prescribing
Q&A: Opioid Prescribing for Chronic Non-Malignant Pain
 NHS Hastings and Rother Clinical Commissioning Group Chair Dr David Warden Chief Officer Amanda Philpott NHS Eastbourne, Hailsham and Seaford Clinical Commissioning Group Chair Dr Martin Writer Chief Officer
NHS Hastings and Rother Clinical Commissioning Group Chair Dr David Warden Chief Officer Amanda Philpott NHS Eastbourne, Hailsham and Seaford Clinical Commissioning Group Chair Dr Martin Writer Chief Officer
Oxymorphone (Opana ) is indicated for the relief of moderate-to-severe acute pain where the use of an opioid is appropriate.
 is indicated for the relief of moderate-to-severe acute pain where the use of an opioid is appropriate.") Page 1 of 7 Policies Repository Policy Title Policy Number Schedule II Prior Authorization FS.CLIN.16 Application of Pharmacy Policy is determined by benefits and contracts. Benefits may vary based on
Page 1 of 7 Policies Repository Policy Title Policy Number Schedule II Prior Authorization FS.CLIN.16 Application of Pharmacy Policy is determined by benefits and contracts. Benefits may vary based on
15mg oxycodone is equivalent to how much morphine
 15mg oxycodone is equivalent to how much morphine The Borg System is 100 % 15mg oxycodone is equivalent to how much morphine nursing home activity director cover letter 15 mg oxycodone equal to how much
15mg oxycodone is equivalent to how much morphine The Borg System is 100 % 15mg oxycodone is equivalent to how much morphine nursing home activity director cover letter 15 mg oxycodone equal to how much
Berkshire West Area Prescribing Committee Guidance
 Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Objectives: What is your Definition of Pain? 8/16/2017
 Safe Opioid Management for the Seriously Ill Patient Sam Perna, D.O. Objectives: MDB1 1) Participants will understand the way the body s pain system works. 2) Participants will identify the elements of
Safe Opioid Management for the Seriously Ill Patient Sam Perna, D.O. Objectives: MDB1 1) Participants will understand the way the body s pain system works. 2) Participants will identify the elements of
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Acute Pain Management in the Hospital Setting. Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX
 Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Pain and Chemical Dependency Fathy Nasr
 Pain and Chemical Dependency Fathy Nasr Email: fathynasr@lycos.com WEB SITE: profathynasr.com Opioid Receptors Adenosine Guanosine Inositol PHAMACOTHERAPY, Step ladder Analgesic pyramids WHO Nociceptive
Pain and Chemical Dependency Fathy Nasr Email: fathynasr@lycos.com WEB SITE: profathynasr.com Opioid Receptors Adenosine Guanosine Inositol PHAMACOTHERAPY, Step ladder Analgesic pyramids WHO Nociceptive
Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center
 Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Session II. Learning Objectives for Session II. Key Principles of Safe Prescribing. Benefits and Limitations of ER/LA Opioids
 Learning Objectives for Session II Session II Best Practices for How to Start Therapy with ER/LA Opioids, How to Stop, and What to Do in Between Upon completion of this module, the participants will be
Learning Objectives for Session II Session II Best Practices for How to Start Therapy with ER/LA Opioids, How to Stop, and What to Do in Between Upon completion of this module, the participants will be
PAIN MANAGEMENT PGY-1. Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC
 PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Pain management in palliative care. Dr. Stepanie Lippett and Sister Karen Davies-Linihan
 Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Pain control in Cancer patients. Dr Ali Shoeibi, Assistant Professor of Neurology
 Pain control in Cancer patients Dr Ali Shoeibi, Assistant Professor of Neurology More than two thirds of patients with advanced cancer experience cancer pain Almost all pain can be controlled to some extent
Pain control in Cancer patients Dr Ali Shoeibi, Assistant Professor of Neurology More than two thirds of patients with advanced cancer experience cancer pain Almost all pain can be controlled to some extent
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults
 SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults BACKGROUND The justification for developing these guidelines lies
SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults BACKGROUND The justification for developing these guidelines lies
Conversion chart from fentanyl to opana er
 Conversion chart from fentanyl to opana er (e.g., Nucynta). Both opioid products involved in conversion are one of the following: morphine, oxycodone, oxymorphone, hydromorphone (not extended- release),
Conversion chart from fentanyl to opana er (e.g., Nucynta). Both opioid products involved in conversion are one of the following: morphine, oxycodone, oxymorphone, hydromorphone (not extended- release),
J Clin Oncol 23: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 23 NUMBER 22 AUGUST 1 2005 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Rapid Switching Between Transdermal Fentanyl and Methadone in Cancer Patients Sebastiano Mercadante, Patrizia
VOLUME 23 NUMBER 22 AUGUST 1 2005 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Rapid Switching Between Transdermal Fentanyl and Methadone in Cancer Patients Sebastiano Mercadante, Patrizia
NATL. II. Health Net Approved Indications and Usage Guidelines: Diagnosis of cancer AND. Member is on fentanyl transdermal patches AND
 Coverage of drugs is first determined by the member s pharmacy or medical benefit. Please consult with or refer to the Evidence of Coverage document I. FDA Approved Indications: The management of breakthrough
Coverage of drugs is first determined by the member s pharmacy or medical benefit. Please consult with or refer to the Evidence of Coverage document I. FDA Approved Indications: The management of breakthrough
NOVIDADES NO TRATAMENTO COM OPIOIDES. Novelties in therapeutic with opioids. V Congresso National de Cuidados Palliativos Marco 2010, Lisboa
 NOVIDADES NO TRATAMENTO COM OPIOIDES Novelties in therapeutic with opioids V Congresso National de Cuidados Palliativos 11 12 Marco 2010, Lisboa Friedemann Nauck Department Palliative Medicine Center Anesthesiology,
NOVIDADES NO TRATAMENTO COM OPIOIDES Novelties in therapeutic with opioids V Congresso National de Cuidados Palliativos 11 12 Marco 2010, Lisboa Friedemann Nauck Department Palliative Medicine Center Anesthesiology,
The pain of it all. Rod MacLeod MNZM. Hibiscus Hospice, Auckland and University of Auckland
 The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
Opioid Pharmacology. Dr Ian Paterson, MA (Pharmacology), MB BS, FRCA, MAcadMEd. Consultant Anaesthetist Sheffield Teaching Hospitals
, MB BS, FRCA, MAcadMEd. Consultant Anaesthetist Sheffield Teaching Hospitals") Opioid Pharmacology Dr Ian Paterson, MA (Pharmacology), MB BS, FRCA, MAcadMEd Consultant Anaesthetist Sheffield Teaching Hospitals Introduction The available opioids and routes of administration - oral
Opioid Pharmacology Dr Ian Paterson, MA (Pharmacology), MB BS, FRCA, MAcadMEd Consultant Anaesthetist Sheffield Teaching Hospitals Introduction The available opioids and routes of administration - oral
BJF Acute Pain Team Formulary Group
 Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio (740) ~
 ~") 2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio 43130 (740) 687-8000 ~ www.fmchealth.org Introduction The purpose of this module is to reduce the risk of adverse outcomes for adult patients
2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio 43130 (740) 687-8000 ~ www.fmchealth.org Introduction The purpose of this module is to reduce the risk of adverse outcomes for adult patients
Opioid Analgesics. Recommended starting dose for opioid-naïve patients
 Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
Mid Essex Locality Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care
 Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Pain Management Management in Hepatic Hepatic and and Renal Dysfunction
 Pain Management in Hepatic and Renal Dysfunction Review the pharmacologic basis for medications used in pain management Identify pain medications which hshould ldbe avoided in patients with hepatic dysfunction
Pain Management in Hepatic and Renal Dysfunction Review the pharmacologic basis for medications used in pain management Identify pain medications which hshould ldbe avoided in patients with hepatic dysfunction
Cancer Pain. Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center
 Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
Nociceptive Pain. Pathophysiologic Pain. Types of Pain. At Presentation. At Presentation. Nonpharmacologic Therapy. Modulation
 Learning Objectives Effective, Safe Analgesia An Approach to Appropriate Outpatient Chronic Pain Treatment By the end of this presentation, participants will be able to: Identify multiple factors that
Learning Objectives Effective, Safe Analgesia An Approach to Appropriate Outpatient Chronic Pain Treatment By the end of this presentation, participants will be able to: Identify multiple factors that
Postoperative Pain Management. Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt)
") Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt) Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement
Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt) Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement
Narcotic Equivalence Converter Narcotic Route Dose Duration; Select a drug: mg Convert to: mg Adapted from Tarascon Pocket Pharmacopoeia.
 Narcotic Equivalence Converter Narcotic Route Dose Duration; Select a drug: mg Convert to: mg Adapted from Tarascon Pocket Pharmacopoeia. Created: Monday, March 12. Online calculator to convert equianalgesic
Narcotic Equivalence Converter Narcotic Route Dose Duration; Select a drug: mg Convert to: mg Adapted from Tarascon Pocket Pharmacopoeia. Created: Monday, March 12. Online calculator to convert equianalgesic
Opioid rotation or switching may be considered if a patient obtains pain relief with one opioid and is suffering severe adverse effects.
 Dose equivalence and switching between opioids Key Messages Switching from one opioid to another should only be recommended or supervised by a healthcare practitioner with adequate competence and sufficient
Dose equivalence and switching between opioids Key Messages Switching from one opioid to another should only be recommended or supervised by a healthcare practitioner with adequate competence and sufficient
Management of Cancer Pain
 i Management of Cancer Pain ii Management of Cancer Pain iii Management of Cancer Pain iv Management of Cancer Pain v Management of Cancer Pain vi Management of Cancer Pain vii Management of Cancer Pain
i Management of Cancer Pain ii Management of Cancer Pain iii Management of Cancer Pain iv Management of Cancer Pain v Management of Cancer Pain vi Management of Cancer Pain vii Management of Cancer Pain
Sharon A Stephen, PhD, ARNP, ACHPN. September 23, 2014
 Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
Chronic Non Malignant Pain Opioid Guideline
 CLINICAL GUIDELINE Chronic Non Malignant Pain Opioid Guideline A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised
CLINICAL GUIDELINE Chronic Non Malignant Pain Opioid Guideline A guideline is intended to assist healthcare professionals in the choice of disease-specific treatments. Clinical judgement should be exercised
PAIN MANAGEMENT 101. By: Vicki McCulloch RN, NP & DeAnna Looper RN, CHPN, CHPCA
 PAIN MANAGEMENT 101 By: Vicki McCulloch RN, NP & DeAnna Looper RN, CHPN, CHPCA Objectives Identify a step-wise approach to pain management. Identify the WHO Pain Ladder. Identify non-pharmacological pain
PAIN MANAGEMENT 101 By: Vicki McCulloch RN, NP & DeAnna Looper RN, CHPN, CHPCA Objectives Identify a step-wise approach to pain management. Identify the WHO Pain Ladder. Identify non-pharmacological pain
Overcoming challenges in pain management in older patients. David Lussier, MD, FRCP(c) March 21, 2012
 March 21, 2012") Overcoming challenges in pain management in older patients David Lussier, MD, FRCP(c) March 21, 2012 Pain An unpleasant sensory and emotional experience associated with actual or potential tissue damage,
Overcoming challenges in pain management in older patients David Lussier, MD, FRCP(c) March 21, 2012 Pain An unpleasant sensory and emotional experience associated with actual or potential tissue damage,
Pharmacogenetics of Codeine. Lily Mulugeta, Pharm.D Office of Clinical Pharmacology Pediatric Group FDA
 Pharmacogenetics of Codeine Lily Mulugeta, Pharm.D Office of Clinical Pharmacology Pediatric Group FDA 1 Codeine Overview Naturally occurring opium alkaloid Demethylated to morphine for analgesic effect
Pharmacogenetics of Codeine Lily Mulugeta, Pharm.D Office of Clinical Pharmacology Pediatric Group FDA 1 Codeine Overview Naturally occurring opium alkaloid Demethylated to morphine for analgesic effect
Drugs Used In Management Of Pain. Dr. Aliah Alshanwani
 Drugs Used In Management Of Pain Dr. Aliah Alshanwani 1 Drugs Used In Management Of Pain A CASE OF OVERDOSE Sigmund Freud, the father of psychoanalysis His cancer of the jaw was causing him increasingly
Drugs Used In Management Of Pain Dr. Aliah Alshanwani 1 Drugs Used In Management Of Pain A CASE OF OVERDOSE Sigmund Freud, the father of psychoanalysis His cancer of the jaw was causing him increasingly
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
PAIN MANAGEMENT Person established taking oral morphine or opioid naive.
 PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 4000-3 Program Opioid Overutilization Cumulative Drug Utilization Review Criteria Medication Includes all salt forms, single and
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 4000-3 Program Opioid Overutilization Cumulative Drug Utilization Review Criteria Medication Includes all salt forms, single and
WR Fentanyl Symposium. Opioids, Overdose, and Fentanyls
 Opioids, Overdose, and Fentanyls Outline: What are opioids? Why are we experiencing and opioid crisis? Potency, purity, and product How do opioids cause overdose and overdose deaths? What is naloxone and
Opioids, Overdose, and Fentanyls Outline: What are opioids? Why are we experiencing and opioid crisis? Potency, purity, and product How do opioids cause overdose and overdose deaths? What is naloxone and
15 mg morphine 10 mg hydrocodone
 Cari untuk: Cari Cari 15 mg morphine 10 mg hydrocodone 3-2-2013 Convert From CALCULATED MORPHINE EQUIVALENT BY RESOURCE: Average ( mg ) Range ( mg ) Standard Deviation of Sample ( mg ) Hydrocodone. I usually
Cari untuk: Cari Cari 15 mg morphine 10 mg hydrocodone 3-2-2013 Convert From CALCULATED MORPHINE EQUIVALENT BY RESOURCE: Average ( mg ) Range ( mg ) Standard Deviation of Sample ( mg ) Hydrocodone. I usually
OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN
 OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN ANTOINETTE BROWN, RPH LAUREL RAMER, 2019 PHARMD CANDIDATE 2018 WYOMING CONFERENCE ON AGING LARAMIE, WY OCTOBER 3, 2018 OBJECTIVES 1. Understand the
OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN ANTOINETTE BROWN, RPH LAUREL RAMER, 2019 PHARMD CANDIDATE 2018 WYOMING CONFERENCE ON AGING LARAMIE, WY OCTOBER 3, 2018 OBJECTIVES 1. Understand the
Long-Acting Opioid Analgesics
 Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
Market DC Long-Acting Opioid Analgesics Override(s) Prior Authorization Step Therapy Quantity Limit Approval Duration Initial request: 3 months Maintenance Therapy: Additional prior authorization required
Opioids: Use, Abuse and Cause of Death. Jennifer Harmon Assistant Director - Forensic Chemistry Orange County Crime Laboratory
 Opioids: Use, Abuse and Cause of Death Jennifer Harmon Assistant Director - Forensic Chemistry Orange County Crime Laboratory jharmon@occl.ocgov.com Opioid: Any psychoactive chemical that resembles morphine
Opioids: Use, Abuse and Cause of Death Jennifer Harmon Assistant Director - Forensic Chemistry Orange County Crime Laboratory jharmon@occl.ocgov.com Opioid: Any psychoactive chemical that resembles morphine
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
OPIOID- INDUCED NEUROTOXICITY*
 OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS