VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES
|
|
|
- Abner Campbell
- 5 years ago
- Views:
Transcription
1 VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES REGIMENES TERAPÊUTICOS DE LA HEPATITIS C, INTERFERÓN FREE A Coruña 2 Febrero 2013 Rui Sarmento e Castro Centro Hospitalar do Porto HJU ECS Universidade do Minho
2 Problems associated with current triple therapy Phase III clinical trials have shown that 25-35% of G1 treatment-naïve patients and 50-60% patients who failed a previous treatment do not achieve SVR. New regimens are needed to cure these patients Better tolerability Reduced adverse events Lower number of pills and dosages With efficacy in difficult-to-treat populations
3 Difficulties with new drug development 2ª generation PIs may have cross-resistance with mutations observed in TPV or BOC. Diminished efficacy of the first generation PIs and other drugs in: HIV, Genotype 1a, Blacks, IL28B non-cc, Cirrhotics Side effects of ribavirin are attenuated when taken without IFN but still remain a problem. Ribavirin is needed as part of some oral regimens. Late viral relapse reported Convenience Unexpected side effects suspension of some drugs in development Costs
4 IFN-free clinical trials SOUND C2 - Faldaprevir + BI ± RBV - Daclatasvir + Sofosbuvir ± RBV ELECTRON - Sofosbuvir ± RBV - Sofosbuvir + GS RBV NIH SPARE CO-PILOT PILOT AVIATOR - Sofosbuvir + RBV - ABT-450/r + ABT RBV - ABT-450/r + ABT RBV - ABT-450/r + ABT ABT RBV - Daclatasvir + Asunaprevir + BMS Daclatasvir + Asunaprevir
5 SOUND-C2: BI (Faldaprevir) + BI (NNI) ± RBV intx-naive GT1 Patients phase 2b Stratified by HCV subtype and IL28B genotype Wk 16 Wk 28 Wk 40 BI mg QD + BI mg TID + RBV (n = 81) Tx-naive patients with GT1 HCV (7% to 17% in each group had cirrhosis) (N = 362) BI mg QD + BI mg TID + RBV (n = 80) BI mg QD + BI mg TID + RBV (n = 77) BI mg QD + BI mg BID + RBV (n = 78) 12-wk follow-up for SVR12 BI mg QD + BI mg TID, no RBV (n = 46)* Weight-based RBV dosing ( mg/day). Zeuzem S, et al. EASL Abstract 101. *Randomization to this arm stopped early due to FDA concerns regarding lack of RBV.
6 SOUND-C2: Efficacy According to Study Arm, HCV Subgenotype, and IL28B SVR According to IL28B and HCV Subtype (ITT) 100 All patients 1a non-cc All 1b and 1a-CC SVR12 (%) TID 16 wks RBV TID 28 wks RBV TID 40 wks RBV BID 28 wks RBV 0 TID 28 wks Zeuzem S, et al. EASL Abstract 101.
7 SOUND C 2 Ribavirin was necessary to achieve high SVR rates One relapse after SVR12 Combination relatively well tolerated particularly in arm with BI BID Adverse events (most frequent): GI, skin reactions, hiperbilirubinemia Other outcomes: Pts with compensated cirrhosis SVR12 43 to 50% in genotype 1a 57 to 80% in genotype 1b

8 DCV+GS 7977±RBV Phase 2a
9 Daclatasvir Plus Sofosbuvir ± RBV in Treatment-Naive GT1 or 2/3 Patients No impact of RBV on viral response Wk 1 Wk 24 SVR24, % GT1 GT2/3 Treatment-naive, noncirrhotic patients Sofosbuvir Daclatasvir + Sofosbuvir GT1a or 1b (n = 44) Daclatasvir + Sofosbuvir GT2 or 3 (n = 44) Daclatasvir + Sofosbuvir + RBV Sobosbuvir dosed 400 mg QD. Daclatasvir dosed 60 mg QD. RBV dosed by body weight for GT1 patients ( mg/day); 800 mg/day for GT2/3 patients. Sulkowski MS, et al. AASLD Abstract LB-2.
10 Daclatasvir (NS5A) + Sofosbuvir (GS 7977) ±RBV High sustained virologic response rates in non cirrhotics treatment naive pts. Ribavirin didn t influence the response Low discontinuation AEs: fatigue, headache, nausea No difference across all arms between gen 1a or 1b and between CC or non CC
11 Electron 1 : IFN free arms Impact of Ribavirin and IFN responsiveness Wk 0 Wk 4 Wk 8 Wk 12 SVR 4 n=10 n=10 n=25 n=25 n=10 GS RBV (G2/3 Treatment Naïve) GS 7977 (G2/3 Treatment Naïve) GS RBV (GT 2/3 Treatment Experienced) GS RBV (GT 1 Treatment Naive) GS RBV (GT 1 Null Responders) 100 % 60 % 80 % 88 % 11 % n=19 QUANTUM 2 GS RBV (GT 1 Treatment Naive) 59% 1. Gane E, et al. AASLD 2011 and EASL2012; 2. Gilead press release April 2012
 + RBV Phase")
12 Sofosbuvir (NS5BI) + GS 5885 (NS5AI) + RBV Phase II

13 Sofosbuvir (NS5BI) + GS 5885 (NS5AI) + RBV Gane et al. AASLD 2012 Press Release, 7 January 2013, gilead.com,
 + RBV Phase")
14 Sofosbuvir (NS5BI) + GS 5885 (NS5AI) + RBV Phase II

15 Sofosbuvir (NS5BI) + RBV Phase II Outcomes in Genotypes 2 and 3
16 NIH SPARE: Interim Data on Sofosbuvir and RBV in Difficult-to-Treat GT1 Patients Phase II Patients with poor prognostic indicators: GT1a (70%), male (63%), black (83%), IL28B CT/TT (80%), advanced liver disease (22%) Median BMI: 28; median HCV RNA: 6.4 logs Part 1 (early-stage fibrosis) Wk 24 Viral Response, % EOT SVR4 SVR12 Sofosbuvir + RBV 1000/1200 mg (n = 10) 90* 90* 90* Part 2 (all stages of fibrosis) Sofosbuvir + RBV 600 mg (n = 25) Sofosbuvir + RBV 1000/1200 mg (n = 25) 96* 72* *1 dropout at Wk 3. 3 dropouts by Wk 8. Trend to relapse: high VL, advanced fibrosis, low dose ribavirin Osinusi A, et al. AASLD Abstract LB-4.
17 Co-Pilot: 12-Wk ABT-450/r (PI) + ABT-333 (NNI) + RBV in Tx-Naive and Tx Experienced GT1 Patients Interim analysis of nonrandomized, prospective, open-label phase II trial Wk 12 Treatment-naive patients infected with genotype 1 HCV (n = 33) Treatment-experienced* patients infected with genotype 1 HCV (n = 17) ABT 450/Ritonavir 250/100 mg QD + ABT mg BID + RBV mg QD (n = 19) ABT 450/Ritonavir 150/100 mg QD + ABT mg BID + RBV mg QD (n = 14) ABT 450/Ritonavir 150/100 mg QD + ABT mg BID + RBV mg QD (n = 17) 48 wks of follow up *Previous null response (< 2 log 10 decrease in HCV RNA by Wk 12) or partial response (HCV RNA above limit of detection during treatment) Poordad F, et al. EASL Abstract 1399.
18 Co-Pilot: Virologic Outcomes SVR12 in 94% of treatment-naive and 47% of treatment-experienced patients Responses independent of IL28B genotype Patients (%) RVR ervr SVR4 SVR ABT 450/r 250/100 mg QD + ABT RBV Treatment naive (n = 19) ABT 450/r 150/100 mgqd + ABT RBV Treatment naive (n = 14) ABT 450/r 150/100 mg QD + ABT RBV Nonresponders (n = 17) Poordad F, et al. EASL Abstract 1399.
19 Laboratory Abnormalities of Interest, % Total bilirubin 2 x ULN Creatinine 1.5 ULN* Co-Pilot: Safety Outcomes Most notable laboratory abnormalities: increased bilirubin and creatinine Hyperbilirubinemia consistent with known effect of ABT-450 on OATP1B1 bilirubin transporter Both cases of increased creatinine resolved without ABT-450 or ABT- 333 dose adjustment Tx Naive, ABT-450/r 250/100 mg + ABT RBV (n = 19) Tx Naive, ABT-450/r 150/100 mg + ABT RBV (n = 14) Tx Experienced, ABT-450/r 150/100 mg + ABT RBV (n = 17) 0 CrCl < 50 ml/min* ALT 5 x ULN Poordad F, et al. EASL Abstract 1399.
20 Pilot: ABT-450/r + ABT-072 (NNI) + RBV in Treatment-Naive GT1 HCV, IL28B CC Pts Single-arm, open-label, pilot study: ABT-450/r 150/100 mg QD + ABT mg QD + weightbased RBV mg/day for 12 wks Patients (%) RVR ervr SVR12 SVR24 100% of pts achieved primary endpoint of ervr; 91% went on to SVR12 and SVR24 2 relapses posttherapy 1 at posttreatment Wk 12; resistance variant observed only in protease D168V variant observed in 36% of clones sequenced 1 late relapse at posttreatment Wk 36; resistance variant observed only in polymerase Y448H variant observed in 99% of clones sequenced Lawitz E, et al. EASL Abstract 13.

21
22

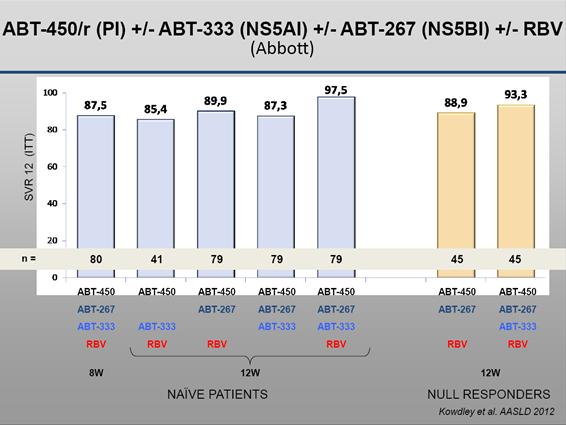
23 AVIATOR: Results by HCV 1 subgenotype

24 AVIATOR: Results by IL28B genotype
 Part 1: Treatment naive noncirrhotic pts with genotype 1 (n=32) Part 2: Treatment naive noncirrhotic pts with")
25 Daclatasvir (NS5AI), Asunaprevir (PI), and BMS (NNI) in treatment naïve genotype 1 Stratified by HCV genotype 1a vs 1b (Phase II a) Part 1: Treatment naive noncirrhotic pts with genotype 1 (n=32) Part 2: Treatment naive noncirrhotic pts with genotype 1
 Group 2 (n=16) 100 94 94 94 100 88 100 94 94 HCV RNA < LDQ (%) 4 12 EOT SVR12 Conclusions:")

26 Daclatasvir (NS5AI), Asunaprevir (PI), and BMS (NNI) in treatment naïve genotype 1 pts Group 1 (n=16) Group 2 (n=16) HCV RNA < LDQ (%) 4 12 EOT SVR12 Conclusions: SVR12 94% with 12 or 24 weeks of treatment High rates of response in difficult to treat populations, including genotype 1a and IL28B non CC Everson GT, et al. AASLD 2012, LB3 Part 2 results not available

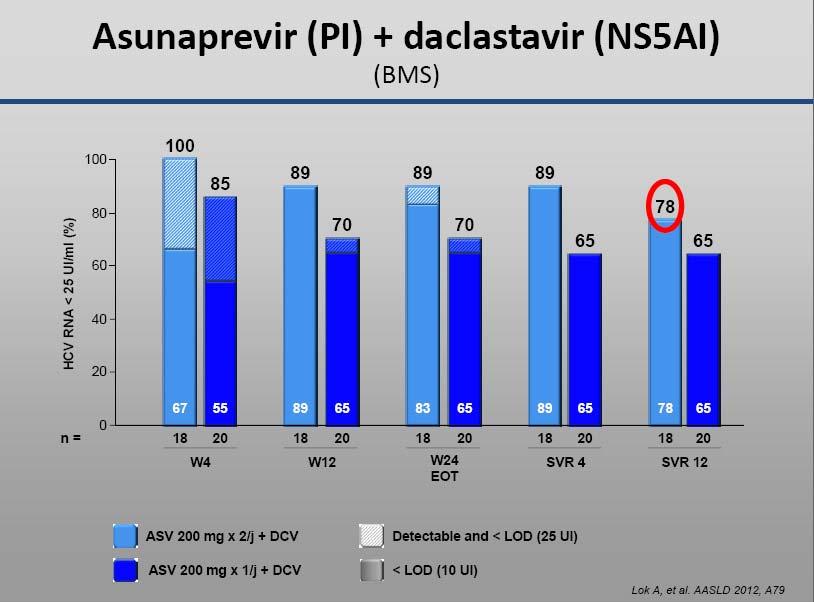
27 Asunaprevir (PI) + Daclatasvir (NS5AI) A1 and A2: G1b Null responders, without cirrhosis n = 21 n = 18 n = 20 n = 22 W24 SVR12 SVR24 SVR48 Lok A, et al. AASLD 2012, A79
28
29 Quad therapy with DCV + ASV + PR Virological response rates Patients achieving endpoint (%) n= 95 * 95 * ASV 200 mg BID + DCV + peg alfa/rbv ASV 200 mg QD + DCV + peg alfa/rbv Solid bars <LOD Hatched bars Detectable and <LLOQ 0 Week 4 Week 12 EOTR (Week 24) SVR 4 *1 patient with missing HCV RNA measurement 1. ASV=asunaprevir; DCV=daclatasvir; EOTR=end of treatment response; LOD=lower limit of detection (~10 IU/mL); LLOQ=lower limit of quantitation (25 IU/mL); peg alfa=pegylated interferon alfa 2a; RBV=ribavirin; SVR=sustained virological response Adapted from Lok A, et al. EASL LB 1415.
30 Previous Null Responders: IFN Free SVR4, 12, or 24 (%) n/ N = Daclatasvir (NS5A) + Asunaprevir (PI) x 24 wks United States [1] 36 4/11 Japan [2] 90 9/10 AASLD 2012* [3] 78 14/18 First IFN-free SVRs in null responders Likely adequate for GT1b but not for GT1a No data in cirrhotics *Includes only asunaprevir BID dosing arm. 1. Lok AS, et al. N Engl J Med. 2012;366: Chayama K, et al. AASLD Abstract LB Lok AS, et al. AASLD Abstract 79.
31 Combination Therapy for Null Responders Daclatasvir (BMS ) QD (NS5A inhibitor) + asunaprevir (BMS ) BID (NS3 protease inhibitor) ± pegifn/rbv for 24 wks US Study [1] Japan Study [2] SVR24 (%) * 1. Lok A, et al. EASL Abstract Chayama K, et al. AASLD Abstract LB-4. N/A Daclatasvir + Asunaprevir Daclatasvir + Asunaprevir + PR *all genotype 1b patients. Adapted from CCO
32 Potent IFN-Free DAA Regimens in Treatment-Naive Genotype 1 Sofosbuvir (Nuc) + daclatasvir (NS5A) + RBV x 24 wks Sofosbuvir (Nuc) + GS 5885 (NS5A) + RBV x 12 wks ABT 450/r (PI) + ABT 333 (NNI) + ABT 267 (NS5A) + RBV x 12 wks Sofosbuvir (Nuc) + daclatasvir (NS5A) x 24 wks Daclatasvir (NS5A) + asunaprevir (PI) + BMS (NNI) x 12 wks SVR4, 12, or 24 (%) n/n = [1] 100 [2] 98 [3] 97 [1] 94 [4] 15/15 25/25 77/79 28/29 15/ DAAs + RBV 2-3 DAAs, No RBV Major caveats: small n, no/few patients with cirrhosis 1. Sulkowski M, et al. AASLD Abstract LB Gane E, et al. AASLD Abstract Kowdley KV, et al. AASLD Abstract LB Everson G, et al. AASLD Abstract LB-3.
33 Previous Null Responders: Quad Therapy Daclatasvir (NS5A) + Asunaprevir (PI) + PegIFN/RBV x 24 wks (Quad) Danoprevir/r (PI) + Mericitabine (Nuc) + PegIFN/RBV x 24 wks (Quad) [3] SVR12 or 24 (%) [1] 88% GT1a 93* [2] n/n = 9/10 38/41 n/n = 62/ *Asunaprevir QD and BID combined. Quad therapy may be a good option for null responders Well tolerated BUT cirrhotics excluded SVR12 (%) % GT1a 1. Lok AS, et al. N Engl J Med. 2012;366: Lok AS, et al. AASLD Abstract Feld JJ, et al. AASLD Abstract
34 Non-GT1: Options Increasing Sofosbuvir (Nuc) + RBV x 12 wks + pegifn x 4 12 wks Sofosbuvir (Nuc) + RBV x 12 wks Sofosbuvir (Nuc) + Daclatasvir (NS5A) ±RBV x 24 wks Sofosbuvir (Nuc) + RBV + pegifn x 24 wks Danoprevir (PI)/ritonavir + pegifn + RBV x wks SVR12 or 24 (%) [1] 100 [1] 96 [2] 68 [1] 20 n/n = 29/29 11/11 27/28 17/25 0 GT2/3 Naive GT2/3 Experienced Major caveat: no patients with cirrhosis included 88 [3] 14/16 GT4/6 Naive 97 [4] 29/30 GT4 Naive 1. Gane EJ, et al. AASLD Abstract Sulkowski M, et al. AASLD Abstract LB Hassanein T, et al. AASLD Abstract Hezode C, et al. AASLD Abstract 760.
35 CONCLUSIONS Several IFN free ongoing trials with promising results Combinations with good efficacy in GT1 patients Some of the new drugs are also active against HCV G2 and G3 Some trials proved that we can make combinations to improve results in difficult to treat patients: HIV/HCV, blacks, G1a, cirrhotics, null responders The majority of the new drugs can be administered once or twice daily RBV must be used in some associations but, in many trials, the drug has no effect on SVR
Highlights of AASLD 2012 CCO Official Conference Coverage of the 2012 Annual Meeting of the American Association for the Study of Liver Diseases
 Highlights of AASLD 12 CCO Official Conference Coverage of the 12 Annual Meeting of the American Association for the Study of Liver Diseases November 9-13, 12 Boston, Massachusetts In partnership with
Highlights of AASLD 12 CCO Official Conference Coverage of the 12 Annual Meeting of the American Association for the Study of Liver Diseases November 9-13, 12 Boston, Massachusetts In partnership with
Evolution of Therapy in HCV
 Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Hepatitis C: Update on New Therapies and AASLD 13 David Bernstein, MD, FACP, AGAF, FACP Professor of Medicine Hofstra North Shore-LIJ School of Medicine Evolution of Therapy in HCV 199 1999 1 13 (%) SVR
Treatments of Genotype 2, 3,and 4: Now and in the future
 Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
The Pipeline of New HCV Therapies: What to Expect in the Next 5 Years. Nancy Reau, MD Associate Professor University of Chicago
 The Pipeline of New HCV Therapies: What to Expect in the Next 5 Years Nancy Reau, MD Associate Professor University of Chicago Learning Objectives Upon completion of this presentation, learners should
The Pipeline of New HCV Therapies: What to Expect in the Next 5 Years Nancy Reau, MD Associate Professor University of Chicago Learning Objectives Upon completion of this presentation, learners should
Clinical Management: Treatment of HCV Mono-infection
 Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Hepatitis C Treatment 2014
 Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Strategies towards cure of HCV infection: a personalized approach. Heiner Wedemeyer Hannover Medical School Hannover, Germany
 Strategies towards cure of HCV infection: a personalized approach Heiner Wedemeyer Hannover Medical School Hannover, Germany 1 Disclosures Honoraria for consulting or speaking (last 5 years): Abbott, Biolex,
Strategies towards cure of HCV infection: a personalized approach Heiner Wedemeyer Hannover Medical School Hannover, Germany 1 Disclosures Honoraria for consulting or speaking (last 5 years): Abbott, Biolex,
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 1)
") Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 1) Goals for Hepatitis C Therapy Compared to PegIFN/RBV, new products should offer: Improved efficacy Efficacy in all patient types including
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 1) Goals for Hepatitis C Therapy Compared to PegIFN/RBV, new products should offer: Improved efficacy Efficacy in all patient types including
Interferon free therapy Are we getting there? Graham R Foster Queen Marys University of London
 Interferon free therapy Are we getting there? Graham R Foster Queen Marys University of London IFN free therapy Disclosures I have received personal and institutional funding from companies that sell drug
Interferon free therapy Are we getting there? Graham R Foster Queen Marys University of London IFN free therapy Disclosures I have received personal and institutional funding from companies that sell drug
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C. Maria Buti Hospital Universitario Valle Hebron Barcelona Spain
 EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
EASL 2013 Interferon Free, All Oral Regimens for Hepatitis C Maria Buti Hospital Universitario Valle Hebron Barcelona Spain The first Results with Oral therapy: a Protease Inhibitor and NS5A inhibitor
New developments in HCV research and their implications for front-line practice
 New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
Bristol-Myers Squibb. HCV Full Development Portfolio Overview. Richard Bertz Int Workshop CP HIV Meeting Amsterdam, Netherlands 24 April 2013
 Bristol-Myers Squibb HCV Full Development Portfolio Overview Richard Bertz Int Workshop CP HIV Meeting Amsterdam, Netherlands 24 April 2013 1 BMS Agents in Clinical Development: DAAs and INF Lambda Lambda
Bristol-Myers Squibb HCV Full Development Portfolio Overview Richard Bertz Int Workshop CP HIV Meeting Amsterdam, Netherlands 24 April 2013 1 BMS Agents in Clinical Development: DAAs and INF Lambda Lambda
Introduction. The ELECTRON Trial
 63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
New Therapeutic Strategies: Polymerase Inhibitors
 New Therapeutic Strategies: Polymerase Inhibitors 6th Paris Hepatitis Conference 14 th - 15 th January, 2013 Stefan Zeuzem Goethe University Hospital Frankfurt, Germany Direct antiviral targets C E1 E2
New Therapeutic Strategies: Polymerase Inhibitors 6th Paris Hepatitis Conference 14 th - 15 th January, 2013 Stefan Zeuzem Goethe University Hospital Frankfurt, Germany Direct antiviral targets C E1 E2
New Treatments for Chronic Hepatitis C. Rafael Esteban Hospital Valle Hebron. Barcelona Spain
 New Treatments for Chronic Hepatitis C Rafael Esteban Hospital Valle Hebron. Barcelona Spain The present: a complex treatment with a better SVR Genotype 1 Genotypes 2 and 3 Triple therapy Boceprevir (BOC)
New Treatments for Chronic Hepatitis C Rafael Esteban Hospital Valle Hebron. Barcelona Spain The present: a complex treatment with a better SVR Genotype 1 Genotypes 2 and 3 Triple therapy Boceprevir (BOC)
Interferon-based and interferon-free new treatment options
 Interferon-based and interferon-free new treatment options White Nights of Hepatology St. Petersburg, 7. June 2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Medizinische Klinik I Frankfurt
Interferon-based and interferon-free new treatment options White Nights of Hepatology St. Petersburg, 7. June 2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Medizinische Klinik I Frankfurt
Hepatitis C en 2013 Tratar o Esperar? Vicente Soriano Servicio de Enfermedades Infecciosas Hospital Carlos III Madrid
 Hepatitis C en 2013 Tratar o Esperar? Vicente Soriano Servicio de Enfermedades Infecciosas Hospital Carlos III Madrid Caveats on hepatitis C therapy decision making We treat persons with a liver. They
Hepatitis C en 2013 Tratar o Esperar? Vicente Soriano Servicio de Enfermedades Infecciosas Hospital Carlos III Madrid Caveats on hepatitis C therapy decision making We treat persons with a liver. They
Future strategies with new DAAs
 Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
SVR Updates from the 2013 EASL
 Updates from the 2013 EASL By Tracy Swan, Treatment Action Group Streamlining HCV Treatment Treatment for hepatitis C virus (HCV) is becoming simpler, shorter, and more effective. All-oral combinations
Updates from the 2013 EASL By Tracy Swan, Treatment Action Group Streamlining HCV Treatment Treatment for hepatitis C virus (HCV) is becoming simpler, shorter, and more effective. All-oral combinations
Interferon Side Effects and The Future of Interferon Sparing Regimens. Todd Wills, MD ETAC Infectious Disease Specialist
 Interferon Side Effects and The Future of Interferon Sparing Regimens Todd Wills, MD ETAC Infectious Disease Specialist HEPATITIS C TREATMENT EXPANSION INITIATIVE MULTISITE CONFERENCE CALL FEBRUARY 15,
Interferon Side Effects and The Future of Interferon Sparing Regimens Todd Wills, MD ETAC Infectious Disease Specialist HEPATITIS C TREATMENT EXPANSION INITIATIVE MULTISITE CONFERENCE CALL FEBRUARY 15,
EASL and The Future of HCV Treatment
 EASL and The Future of HCV Treatment Douglas T. Dieterich, M.D Professor of Medicine Division of Liver Diseases, Gastroenterology and Infectious Diseases Department of Medicine Mount Sinai School of Medicine
EASL and The Future of HCV Treatment Douglas T. Dieterich, M.D Professor of Medicine Division of Liver Diseases, Gastroenterology and Infectious Diseases Department of Medicine Mount Sinai School of Medicine
Associate Professor of Medicine University of Chicago
 Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Feeling right at home
 Feeling right at home Getting to Cure From Cure to Eradication Jordan J. Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto SVR Dramatic Improvements
Feeling right at home Getting to Cure From Cure to Eradication Jordan J. Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto SVR Dramatic Improvements
Direct acting anti-virals: the near future
 Direct acting anti-virals: the near future Heiner Wedemeyer Hannover Medical School Germany Will IFN-free treatment be possible in the near future? Interferon-free regimens to treat hepatitis C What should
Direct acting anti-virals: the near future Heiner Wedemeyer Hannover Medical School Germany Will IFN-free treatment be possible in the near future? Interferon-free regimens to treat hepatitis C What should
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
Pivotal New England Journal of Medicine papers 2014 Phase 3 Trial data
 4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
Special Contribution Highlights of the 2012 American Association for the Study of Liver Diseases Meeting
 Special Contribution Highlights of the 20 American Association for the Study of Liver Diseases Meeting Melissa K. Osborn, MD The American Association for the Study of Liver Diseases (AASLD) held its annual
Special Contribution Highlights of the 20 American Association for the Study of Liver Diseases Meeting Melissa K. Osborn, MD The American Association for the Study of Liver Diseases (AASLD) held its annual
IFN-free for Genotype 1 HCV: the current landscape. Prof. Graham R Foster
 IFN-free for Genotype 1 HCV: the current landscape Prof. Graham R Foster Wonderful new drugs are coming Poordad F, et al. New Engl J Med 2014; online DOI: 10.1056/NEJMoa1402869. 2 The New Drugs Two treatment
IFN-free for Genotype 1 HCV: the current landscape Prof. Graham R Foster Wonderful new drugs are coming Poordad F, et al. New Engl J Med 2014; online DOI: 10.1056/NEJMoa1402869. 2 The New Drugs Two treatment
Treatement Experienced patients without cirrhosis. Rafael Esteban Hospital Universitario Valle Hebron Barcelona
 Treatement Experienced patients without cirrhosis Rafael Esteban Hospital Universitario Valle Hebron Barcelona Agenda With IFN PegIFN+ Ribavirin + Simeprevir PegIFN+ Ribavirin+ Sofosbuvir Without IFN Sofosbuvir
Treatement Experienced patients without cirrhosis Rafael Esteban Hospital Universitario Valle Hebron Barcelona Agenda With IFN PegIFN+ Ribavirin + Simeprevir PegIFN+ Ribavirin+ Sofosbuvir Without IFN Sofosbuvir
What is the Optimized Treatment Duration? To Overtreat versus Undertreat. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
NS5A inhibitors: ideal candidates for combination?
 NS5A inhibitors: ideal candidates for combination? Professor Vasily Isakov, MD, PhD, AGAF Dep.Gastroentrology & Hepatology, ION, Russian Academy of Sciences, Moscow Structure and function of NS5A Meigang
NS5A inhibitors: ideal candidates for combination? Professor Vasily Isakov, MD, PhD, AGAF Dep.Gastroentrology & Hepatology, ION, Russian Academy of Sciences, Moscow Structure and function of NS5A Meigang
The HCV Pipeline Ira M. Jacobson, MD, FACP, FACG, AGAF. Slide Presentation. IFN-free DAA combinations (G1)
") Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
Protease inhibitor based triple therapy in treatment experienced patients
 Protease inhibitor based triple therapy in treatment experienced patients Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Protease inhibitor based triple therapy in treatment experienced patients Universitätsklinikum Leipzig Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber
Update on the Treatment of HCV
 Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Latest Treatment Updates for GT 2 and GT 3 Patients
 Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy
 How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber- und Studienzentrum
How to optimize current therapy for GT1 patients Shortened therapy with IFNa-based therapy Thomas Berg Sektion Hepatologie Klinik und Poliklinik für Gastroenterologie und Rheumatologie Leber- und Studienzentrum
Will difficult-to-treat patients remain difficultto-treat. generation of treatments?
 Will difficult-to-treat patients remain difficultto-treat with the new generation of treatments? Jordan J Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University
Will difficult-to-treat patients remain difficultto-treat with the new generation of treatments? Jordan J Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Ledipasvir-Sofosbuvir (Harvoni)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
I nuovi farmaci per HCV: frequenza della patologia, evidenze di efficacia e sicurezza, strategie di gestione. la pratica clinica
 I nuovi farmaci per HCV: frequenza della patologia, evidenze di efficacia e sicurezza, strategie di gestione La revisione ii delle dll evidenze e indicazioni i iper la pratica clinica Marco Marzioni Segretario
I nuovi farmaci per HCV: frequenza della patologia, evidenze di efficacia e sicurezza, strategie di gestione La revisione ii delle dll evidenze e indicazioni i iper la pratica clinica Marco Marzioni Segretario
The HCV pipeline: Will IFN-free treatment be possible? Heiner Wedemeyer. Hannover Medical School Germany
 : Will IFN-free treatment be possible? Heiner Wedemeyer Hannover Medical School Germany Interferon-free regimens to treat hepatitis C What should be the goal of interferon-free treatment regimens: Sustained
: Will IFN-free treatment be possible? Heiner Wedemeyer Hannover Medical School Germany Interferon-free regimens to treat hepatitis C What should be the goal of interferon-free treatment regimens: Sustained
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
8/5/2014. A new era of HCV clinical management. Direct-Acting Antivirals for Hepatitis C. Goal of HCV treatment is viral cure HIV HBV HCV
 NS5B NS5B 8/5/214 A new era of HCV clinical management Mark Sulkowski, MD Professor of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Disease and Gastroenterology/Hepatology
NS5B NS5B 8/5/214 A new era of HCV clinical management Mark Sulkowski, MD Professor of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Disease and Gastroenterology/Hepatology
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA. Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona
 Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
Experience with pre-transplant antiviral treatment: PEG/RBV and DAA Xavier Forns, MD Liver Unit Hospital Clínic IDIBAPS and CIBREHD Barcelona Interferon-free regimens G1b nulls Asunaprevir (PI) + Daclatasvir
HCV-G3: Sofosbuvir with ledipasvir or daclatasvir?
 HCV-G3: Sofosbuvir with ledipasvir or daclatasvir? Ioannis Goulis, MD Aristotelian University of Thessaloniki XXIII International Hepatitis B & C Meeting of Athens Hadziyannis HCV genotype 3 therapy Chronic
HCV-G3: Sofosbuvir with ledipasvir or daclatasvir? Ioannis Goulis, MD Aristotelian University of Thessaloniki XXIII International Hepatitis B & C Meeting of Athens Hadziyannis HCV genotype 3 therapy Chronic
Update on chronic hepatitis C treatment: current trends, new challenges, what next?
 Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Antiviral agents in HCV
 Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
Antiviral agents in HCV : Upcoming Therapeutic Options Su Jong Yu, M.D., Ph.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Estimated 170 Million
HCV Treatment: Why to Wait
 HCV Treatment: Why to Wait Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital University of Paris-Est
HCV Treatment: Why to Wait Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital University of Paris-Est
CURRENT TREATMENTS. Mitchell L Shiffman, MD Director Liver Institute of Virginia. Richmond and Newport News, VA, USA
 CURRENT TREATMENTS FOR HCV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA Liver Institute of Virginia Education, Research and
CURRENT TREATMENTS FOR HCV Mitchell L Shiffman, MD Director Liver Institute of Virginia Bon Secours Health System Richmond and Newport News, VA, USA Liver Institute of Virginia Education, Research and
HCV In 2015: Maximizing SVR
 HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
Massimo Puoti Dept. of Infectious Diseases AO Ospedale Niguarda Cà Granda
 Massimo Puoti Dept. of Infectious Diseases AO Ospedale Niguarda Cà Granda Innovative strategies in viral hepatitis : Hepatitis C: Interferon and/or Ribavirin free regimens 10th International Workshop on
Massimo Puoti Dept. of Infectious Diseases AO Ospedale Niguarda Cà Granda Innovative strategies in viral hepatitis : Hepatitis C: Interferon and/or Ribavirin free regimens 10th International Workshop on
STATE OF THE ART Update: Treatment Options 2016 Mark Sulkowski, MD
 Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Treating HCV Genotype 2 & 3
 Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
HCV Resistance Clinical Aspects. Sanjay Bhagani Royal Free Hospital/UCL London
 HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
IFN-free therapy in naïve HCV GT1 patients
 IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
Genotype 1 HCV in 2016: Clinical Decision Making in a Time of Plenty
 Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London
 HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
Failure after treatment with DAAs: What to do? Marseille France 2-3 th June 2016
 Failure after treatment with DAAs: What to do? Marc Bourliere, MD White Nights of Hepatology Hôpital Saint Joseph Saint Petersburg Marseille France 2-3 th June 16 Disclosures Board member for : Schering-Plough,
Failure after treatment with DAAs: What to do? Marc Bourliere, MD White Nights of Hepatology Hôpital Saint Joseph Saint Petersburg Marseille France 2-3 th June 16 Disclosures Board member for : Schering-Plough,
Phase 3. Treatment Experienced. Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2. Afdhal N, et al. N Engl J Med. 2014;370:
 Phase 3 Treatment Experienced Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2 Afdhal N, et al. N Engl J Med. 2014;370:1483-93. Ledipasvir-Sofosbuvir +/- Ribavirin in Treatment-Experienced HCV
Phase 3 Treatment Experienced Ledipasvir-Sofosbuvir +/- Ribavirin in HCV Genotype 1 ION-2 Afdhal N, et al. N Engl J Med. 2014;370:1483-93. Ledipasvir-Sofosbuvir +/- Ribavirin in Treatment-Experienced HCV
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 1)
") Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 1) Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 1) Robert S. Brown, Jr., MD, MPH Frank Cardile Professor of Medicine Chief,
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 1) Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 1) Robert S. Brown, Jr., MD, MPH Frank Cardile Professor of Medicine Chief,
ABCs of Hepatitis C: What s New. The Long-Awaited New Era: Protease Inhibitors for HCV Genotype 1
 ABCs of Hepatitis C: What s New ACG Postgraduate Course Washington, DC October 30, 2011 Ira M. Jacobson, M.D. Vincent Astor Professor of Medicine Chief, Division of Gastronterology and Hepatology Medical
ABCs of Hepatitis C: What s New ACG Postgraduate Course Washington, DC October 30, 2011 Ira M. Jacobson, M.D. Vincent Astor Professor of Medicine Chief, Division of Gastronterology and Hepatology Medical
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
HCV: Beyond the current generation of protease inhibitors
 HCV: Beyond the current generation of protease inhibitors Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S. University of Palermo, Italy antonio.craxi@unipa.it Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S. University
HCV: Beyond the current generation of protease inhibitors Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S. University of Palermo, Italy antonio.craxi@unipa.it Antonio Craxì GI & Liver Unit, Di.Bi.M.I.S. University
Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano. Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future
 Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future DAA classes and subclasses Drug Class Subclass Potency
Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future DAA classes and subclasses Drug Class Subclass Potency
Hepatitis C: Aplicaciones Clínicas de la Resistencia. Eva Poveda Division of Clinical Virology INIBIC-Complexo Hospitalario Universitario de A Coruña
 Hepatitis C: Aplicaciones Clínicas de la Resistencia Eva Poveda Division of Clinical Virology INIBIC-Complexo Hospitalario Universitario de A Coruña DAA agents approved or in more advanced stages of clinical
Hepatitis C: Aplicaciones Clínicas de la Resistencia Eva Poveda Division of Clinical Virology INIBIC-Complexo Hospitalario Universitario de A Coruña DAA agents approved or in more advanced stages of clinical
Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos
 Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos Associate Professor of Gastroenterology Academic Department of Gastroenterology
Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos Associate Professor of Gastroenterology Academic Department of Gastroenterology
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
Hepatitis C in Special Populations
 Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Glecaprevir-Pibrentasvir in Cirrhotic Genotype 1, 2, 4, 5, and 6 EXPEDITION-1
 Phase 3 Treatment-Naïve and Treatment-Experienced Glecaprevir-Pibrentasvir in Cirrhotic Genotype 1, 2, 4, 5, and 6 EXPEDITION-1 EXPEDITION-1: Study Features EXPEDITION-1 Trial Design: Open-label, single-arm,
Phase 3 Treatment-Naïve and Treatment-Experienced Glecaprevir-Pibrentasvir in Cirrhotic Genotype 1, 2, 4, 5, and 6 EXPEDITION-1 EXPEDITION-1: Study Features EXPEDITION-1 Trial Design: Open-label, single-arm,
Michael Fried, MD University of North Carolina Chapel Hill, NC. Ira Jacobson, MD Weill Cornell Medical College New York, NY
 Nezam Afdhal, MD Beth Israel Deaconess Medical Center Boston, MA Kim Brown, MD Henry Ford Hospital Detroit, MI Michael Fried, MD University of North Carolina Chapel Hill, NC Jordan Feld, MD Toronto Western
Nezam Afdhal, MD Beth Israel Deaconess Medical Center Boston, MA Kim Brown, MD Henry Ford Hospital Detroit, MI Michael Fried, MD University of North Carolina Chapel Hill, NC Jordan Feld, MD Toronto Western
CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015
 CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015 CCO Official Conference Coverage of the 2015 Annual Meeting of the American Association for the Study of Liver Diseases, November
CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015 CCO Official Conference Coverage of the 2015 Annual Meeting of the American Association for the Study of Liver Diseases, November
HALLMARK-DUAL Study. Daclatasvir + Asunaprevir in Genotype 1b. Hepatitis. Treatment-Naïve and Treatment-Experienced
 Phase 3 Treatment-Naïve and Treatment-Experienced Daclatasvir + Asunaprevir in Genotype 1b HALLMARK-DUAL Study Manns M, et al. Lancet. 2014;384:1597-605. Daclatasvir + Asunaprevir for HCV GT 1b HALLMARK-DUAL:
Phase 3 Treatment-Naïve and Treatment-Experienced Daclatasvir + Asunaprevir in Genotype 1b HALLMARK-DUAL Study Manns M, et al. Lancet. 2014;384:1597-605. Daclatasvir + Asunaprevir for HCV GT 1b HALLMARK-DUAL:
Pegylated interferon based therapy with second-wave direct-acting antivirals in genotype 1 chronic hepatitis C
 Liver International ISSN 1478-3223 REVIEW ARTICLE Pegylated interferon based therapy with second-wave direct-acting antivirals in genotype 1 chronic hepatitis C Nicole M. Welch and Donald M. Jensen University
Liver International ISSN 1478-3223 REVIEW ARTICLE Pegylated interferon based therapy with second-wave direct-acting antivirals in genotype 1 chronic hepatitis C Nicole M. Welch and Donald M. Jensen University
Dr. Siddharth Srivastava
 Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Dr Janice Main Imperial College Healthcare NHS Trust, London
 BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
HCV Case Study. Treat Now or Wait for New Therapies
 HCV Case Study Treat Now or Wait for New Therapies This program is supported by educational grants from Kadmon and Merck Pharmaceuticals. Program Disclosure This activity has been planned and implemented
HCV Case Study Treat Now or Wait for New Therapies This program is supported by educational grants from Kadmon and Merck Pharmaceuticals. Program Disclosure This activity has been planned and implemented
November 2013 AASLD Investor Event 4 November
 November 2013 AASLD Investor Event 4 November Maris Hartmanis, President and CEO Charlotte Edenius, EVP Development Bertil Samuelsson, CSA Rein Piir, EVP Corporate Affairs & IR Corporate presentation,
November 2013 AASLD Investor Event 4 November Maris Hartmanis, President and CEO Charlotte Edenius, EVP Development Bertil Samuelsson, CSA Rein Piir, EVP Corporate Affairs & IR Corporate presentation,
Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors
 Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors Eric Lawitz, MD, AGAF, CPI The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science
Hepatitis C: Management of Treatment Naïve Patients with First Line Protease Inhibitors Eric Lawitz, MD, AGAF, CPI The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science
Treatment of HCV in 2016
 5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
Treatment of Unique Populations Raymond T. Chung, MD
 Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2)
") Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) Goals for Hepatitis C Therapy Compared to PegIFN α/rbv, new treatment regimens for chronic hepatitis C should offer: Improved efficacy Efficacy
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) Goals for Hepatitis C Therapy Compared to PegIFN α/rbv, new treatment regimens for chronic hepatitis C should offer: Improved efficacy Efficacy
Glecaprevir-Pibrentasvir in Non-Cirrhotic Genotype 2 ENDURANCE-2
 Phase 3 Treatment Naïve or Experienced Glecaprevir-Pibrentasvir in Non-Cirrhotic Genotype 2 ENDURANCE-2 *ENDURANCE-2: Study Features ENDURANCE-2 Trial Design: Randomized, double-blind, placebo-controlled
Phase 3 Treatment Naïve or Experienced Glecaprevir-Pibrentasvir in Non-Cirrhotic Genotype 2 ENDURANCE-2 *ENDURANCE-2: Study Features ENDURANCE-2 Trial Design: Randomized, double-blind, placebo-controlled
Hepatitis C: New Therapies in
 Hepatitis C: New Therapies in 216-217 Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Diseases and
Hepatitis C: New Therapies in 216-217 Mark Sulkowski, MD Professor of Medicine Johns Hopkins University School of Medicine Medical Director, Viral Hepatitis Center Divisions of Infectious Diseases and
Hepatitis C Emerging Therapy Update: Reports From the Liver Meeting 2012
 Reports From the Liver Meeting 212 Project ID: 521 Target Audience This activity has been designed to meet the educational needs of gastroenterologists, hepatologists, physician assistants, and nurse practitioners
Reports From the Liver Meeting 212 Project ID: 521 Target Audience This activity has been designed to meet the educational needs of gastroenterologists, hepatologists, physician assistants, and nurse practitioners
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD
 Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD") Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
Individual Optmizaton of therapy. Graham R Foster Professor of Hepatology QMUL
 Individual Optmizaton of therapy Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novarts, Springbank,
Individual Optmizaton of therapy Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novarts, Springbank,
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France
 How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
Saeed Hamid, MD Alex Thompson, MD, PhD
 Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Expert Perspectives: Best of HCV from EASL 2015
 Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
PIB. Next Generation Direct-Acting Antivirals. Collectively: G/P. Pibrentasvir (formerly ABT-530) pangenotypic NS5A inhibitor
 pangenotypic NS5A inhibitor") Surveyor-II, Part 3: Efficacy and Safety of Glecaprevir/Pibrentasvir (Abt-493/Abt-53) in Patients with Hepatitis C Virus Genotype 3 Infection with Prior Treatment Experience and/or Cirrhosis David L. Wyles,
Surveyor-II, Part 3: Efficacy and Safety of Glecaprevir/Pibrentasvir (Abt-493/Abt-53) in Patients with Hepatitis C Virus Genotype 3 Infection with Prior Treatment Experience and/or Cirrhosis David L. Wyles,
The Liver Meeting 2013: The 64th Annual Meeting of the AASLD Washington, DC, November 1 5, 2013 Presentation LB-1
 Phase 2b Study of the Interferon-Free and Ribavirin-Free Combination of Daclatasvir, Asunaprevir, and BMS-791325 for 12 Weeks in Treatment-Naive Patients With Chronic HCV Genotype 1 Infection Everson GT,
Phase 2b Study of the Interferon-Free and Ribavirin-Free Combination of Daclatasvir, Asunaprevir, and BMS-791325 for 12 Weeks in Treatment-Naive Patients With Chronic HCV Genotype 1 Infection Everson GT,
Virological Tools and Monitoring in the DAA Era
 Virological Tools and Monitoring in the DAA Era Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Virological Tools and Monitoring in the DAA Era Prof. Jean-Michel Pawlotsky, MD, PhD National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors
 Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors Fred Poordad, MD The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science Center
Hepatitis C: Management of Previous Non-responders with First Line Protease Inhibitors Fred Poordad, MD The Texas Liver Institute Clinical Professor of Medicine University of Texas Health Science Center
Baseline and acquired viral resistance to DAAs: how to test and manage
 Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline