National Opioid Treatment Guideline Dr. Ronald Lim
|
|
|
- Edith Park
- 5 years ago
- Views:
Transcription
1 National Opioid Treatment Guideline Dr. Ronald Lim (MD, CCFP, DFASAM, ABAM(D), FISAM, CCSAM, MRO) Clinical Assistant Professor, Department of Psychiatry and Family Practice Cumming School of Medicine University of Calgary Disclosure No connection to pharmaceutical companies Not Paid for this presentation I was external reviewer for the BC Opioid Treatment Guideline and current reviewer for the National Guidelines All information today is referenced to the BC guidelines and their references which as the template for the National Treatment Guidelines Overview Introduction and defining problem Opioid Treatment Guidelines Withdrawal Management Opioid Agonist Therapy SROM (slow release oral morphine) Psychosocial and Residential Treatment Harm Reduction Stepped, Integrated care and Tapering Summary of Recommendations 1
2 2

 quality of evidence (study design, risk-benefit ratios, potential biases, scope")

3 Evidence Selection and Review 180 references structured review of the literature meta-analyses of randomized clinical trials individual clinical trials, observational reports expert opinion Grading of Recommendations Assessment, Development and Evaluation (GRADE) quality of evidence (study design, risk-benefit ratios, potential biases, scope and consistency of results) Rated low, moderate or high Strength of Recommendation Rated weak or strong Committee recommendation, Internal and External Review of experts and stakeholders 3
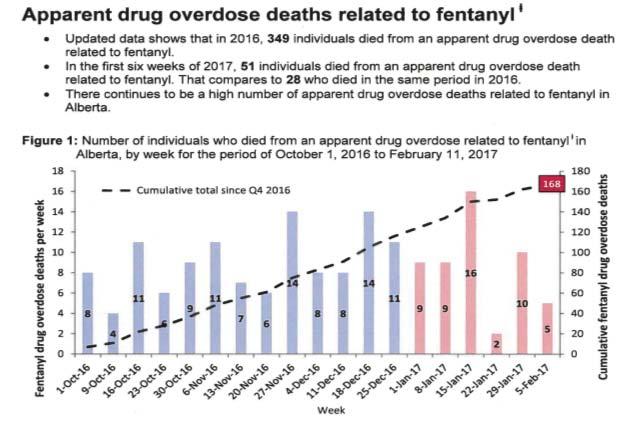
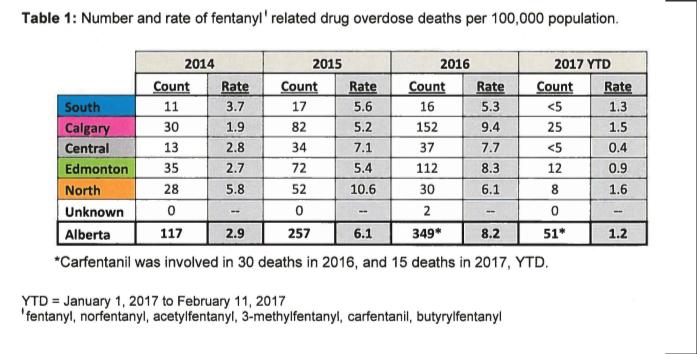
4 Introduction and background Opioid Use Disorder ~ 2% prevalence in US Recent increase in OD and deaths Increasing potency of street opioids Fentanyl and carfentanyl Public health concern Treatment for OUD remains inadequate No consistent approach Withdrawal management only Abstinence programs (outpatient and inpatient) Methadone maintenance vs buprenorphine/naloxone Naltrexone Withdrawal management Withdrawal management alone is not an effective treatment for opioid use disorder regardless of method used. Traditional rapid inpatient withdrawal (<7days) for other substances to reduce withdrawal complications like alcohol withdrawal seizures and DTs does not apply to opioids Rates of dropout and relapse to opioid use are high Loss of tolerance and relapse to current high potency opioids (fentanyl and its derivatives) results in increased overdose risk and deaths HIV and hepatitis C transmission, are higher for individuals who have recently completed withdrawal management compared to individuals who receive no treatment Treatment OAT recommended as first line WITHDRAWAL MANAGEMENT Opioid withdrawal management should be a bridge to treatment, access to long-term opioid agonist treatment (preferred) intensive outpatient treatment or residential treatment with OAT Intensive outpatient or residential treatment without OAT should be started immediately Patients who request withdrawal management alone Should be provided with clear, concise information about the known risks to personal and public safety, Engaged in supportive, constructive discussion about safer treatment options Provided with harm reduction supplies and information consider initiating buprenorphine/naloxone treatment to address withdrawal symptoms And then slowly tapering under outpatient supervision. Individuals who are unsuccessful with this approach may be offered agonist therapy again For individuals resistant or inappropriate for OAT, long term outpatient slow tapering is less disruptive 4
5 PSYCHOSOCIAL TREATMENT INTERVENTIONS PROVIDED WITH OPIOID WITHDRAWAL MANAGEMENT Psychosocial treatment interventions may be beneficial adjuncts Insufficient evidence to favor any specific psychosocial treatment modality Currently limited evidence due to small study sample sizes and varying assessment and outcome measurements If withdrawal management alone is pursued, psychosocial treatment interventions likely do not protect against the elevated risk of HIV infection or fatal overdose Opioid agonist treatments opioid agonist treatments are superior to withdrawal management alone retention in treatment, sustained abstinence from opioid use reduced risk of morbidity and mortality choice of agonist treatment (methadone vs Buprenorphine/naloxone) depends on comorbidities (liver disease, prolonged QTc interval) drug drug interactions, treatment preference, and Previous response prescriber experience and appropriate authorization Opioid agonist treatments should Incorporate provider-led counselling long-term substance use monitoring regular assessment, follow-up urine drug tests comprehensive preventive and primary care Harm reduction strategies psychosocial treatment interventions psychosocial supports specialist care as required 5
6 Methadone Methadone more effective than non-pharmacological outpatient treatment Mattick RP, Breen C, Kimber J, Davoli M. Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence. Cochrane Database Syst Rev. 2009(3):CD higher doses ( mg) more effective than lower doses treatment retention reducing heroin higher methadone doses (> 75 mg/day) can be protective against overdose reduce injection risk behaviors, hepatitis C and HIV increased adherence to antiretroviral therapy Methadone concerns Unique pharmacological properties narrow therapeutic index, long elimination half-life interactions with alcohol and other drugs increase risk of toxicity and adverse events Methadone related emergency room visits occur 6 and 23 x higher than other prescription opioids In US methadone identified > 1/3 of prescription-opioid-related overdose deaths BC methadone identified in ~ 25% of prescription-opioid-related deaths Overall increase risk of overdose during initiation and stabilization Strict provincial standards and guidelines and requirement of daily dosing Methadone Pharmacokinetics High oral bioavailability Tissue binding once absorbed Peak plasma 2-4 hours, oral administration ½ life of hours 6
, USA (2002), Canada (2010) Partial opioid agonist with a high affinity and slow dissociation for")
7 Methadone Steady State Courtesy of Dr. Peter Lawlor TIME Buprenorphine Synthetic opioid for the treatment of opioid addiction France (1996), USA (2002), Canada (2010) Partial opioid agonist with a high affinity and slow dissociation for mu receptor Ceiling effect greater safety (low risk of respiratory depression) Precipitated withdrawal because of high affinity for receptor Degree of physical dependence and withdrawal syndrome less severe. Less abuse potential but possible. Easier to switch from buprenorphine/naloxone to methadone, 20 Buprenorphine Available as sublingual tablets combo with naloxone (Suboxone) There is low oral bioavailability Sublingual buprenorphine has adequate bioavailability Addition of naloxone decreases abuse potential for tablets (decreased iv use) Sublingually Buprenorphine will be well absorbed Naloxone absorption will be minimal Intravenously Naloxone is 100% bioavailable Precipitated withdrawal occurs in opioid-maintained patients MMT Introductory Workshop September


8 Fig. 3. Competitive binding data for opioid drugs. Symbols represent mean ± SE of three wells. Solid line is the nonlinear fit of the binding data. Donna A. Volpe, Grainne A. McMahon Tobin, R. Daniel Mellon, Aspandiar G. Katki, Robert J. Parker, Thomas Colatsky, Timothy J. Kropp, S. Leigh Verbois Uniform assessment and ranking of opioid Mu receptor binding constants for selected opioid drugs Regulatory Toxicology and Pharmacology, Volume 59, Issue 3, 2011, Buprenorphine effectiveness Retention in Treatment Doses greater than 2 mg/day > placebo Compared to methadone, Low doses ( 6 mg/day) < low doses of methadone ( 40 mg/day) Medium doses (7 16 mg/day) and = medium doses methadone (40 85 mg/day) High doses ( 16 mg/day) = high doses methadone ( 85 mg/day). Reducing illicit opioid use Buprenorphine (>16 mg) = methadone Recent meta-analysis comparing buprenorphine and methadone for prescription opioid dependence reached similar conclusions Older trials had not shown this due to low buprenorphine doses and slow induction rates. Newer studies show sublingual buprenorphine achieves equivalent outcomes to methadone when a sufficient dose, appropriate induction rate and flexible dosing are used 8
9 Buprenorphine safety Buprenorphine preferable in terms of reduced overdose potential. UK study over 6 years 19 million prescription buprenorphine was 6X safer than methadone for overdose risk Marteau D, McDonald R, Patel K. The relative risk of fatal poisoning by methadone or buprenorphinewithin the wider population of England and Wales. BMJ Open. 2015;5(5):e Methadone has a 4X higher risk of fatal overdose 71. Bell JR, Butler B, Lawrance A, Batey R, Salmelainen P. Comparing overdose mortality associated with methadone and buprenorphine treatment. Drug Alcohol Depend. 2009;104(1 2): Luty J, O Gara C, Sessay M. Is methadone too dangerous for opiate addiction? BMJ. 2005;331(7529): Buprenorphine has a lower potential for respiratory depression Standard doses are well below the threshold lethal dose for opioid-naïve adults compared to standard methadone doses, which often exceed the threshold lethal dose. methadone has higher potential for adverse drug drug interactions with many common medications (e.g., antibiotics, antidepressants, antiretroviral) and increased risk of cardiac arrhythmias as a result of QT prolongation Buprenorphine disadvantages May not be appropriate for all patients Intolerable symptoms during the partial opioid withdrawal that is required for initiation Risk of precipitated withdrawal Inpatient detoxification and treatment facility for more intensive monitoring, support and symptom management for patients with challenging inductions Potentially higher risk of drop-out Doses may be suboptimal for individuals with high opioid tolerance At high doses, may block the analgesic effect of concurrent opioid medications for pain SLOW-RELEASE ORAL MORPHINE Since November 2014, slow-release oral morphine (24-hour formulation, brand name Kadian ) has been approved by Health Canada s Non-Insured Health Benefits (NIHB) Program for the treatment of opioid use disorder Health Canada and Express Scripts Canada. NIHB Newsletter (Fall2014):1 4.Non-InsuredHealth Benefits (NIHB)Program.Released Fall2014.Availableat: health.chiefs-ofontario.org/sites/default/files/files/ Health Canada NIHB Pharmacy Newsletter Fall 2014.pdf. Accessed 13 Jan2015 Cochrane review three randomized trials no difference in treatment retention to other OAT higher incidence of adverse events compared to methadone low number of studies included in the review limited conclusions Collectively less evidence regarding slow-release oral morphine in comparison to other opioid agonist therapies important to note that only the once-daily, 24-hour formulation of slowrelease oral morphine has been studied for the treatment of opioid use disorder Other formulations of oral morphine have not been empirically studied and are not recommended for treatment of opioid use disorder 9
10 SLOW-RELEASE ORAL MORPHINE Providers should have Section 56 exemption from the Controlled Drugs and Substances Act to prescribe methadone Specialist consultation should be sought Practitioner who lacks experience prescribing slow-release oral morphine must consult a specialist Strict policies to prevent misuse, diversion and to ensure patient safety are required Regular scheduled and random urine drug testing required with GCMS/LCMS Daily witness dosing required and take home not recommended Psychosocial Treatment Interventions and Supports Clinicians should provide medical management, general support and unstructured counselling Clinicians should be familiar with the principles of trauma-informed practice Consider undertaking cultural safety training for Indigenous clients Attention to assessing, treating and monitoring emotional and mental health is an essential component of care high prevalence of concurrent medical and mental health diagnoses in substance use disorders Evidence that inclusion of psychosocial treatment interventions can improve outcomes for individuals with concurrent and other mental health disorders There are limited number of controlled studies of psychosocial treatment interventions for substance use disorders Psychosocial Treatment Interventions and Supports The addition of psychosocial supports helpful in supporting overall recovery in terms of improving individuals psychosocial circumstances and survival needs. Although no systematic reviews have examined the impact of providing supports for various social needs (e.g., housing support, vocational and skills training, social supports, financial assistance), previous studies have demonstrated housing and other survival needs may have a significant impact on opioid agonist treatment outcomes. Benefit for opioid use disorder care being offered in interdisciplinary care teams that are equipped to address above needs. Where patients have struggled to engage in care, intensive case management, peer navigation and outreach may also be effective at improving retention in addictions treatment. 10
11 Harm reduction strategies Harm reduction refers to policies, programs and practices reduce the adverse health, social and economic consequences of licit and illicit substance use needle/syringe distribution programs, overdose prevention with take-home naloxone supervised injection or consumption services No evidence that participation in any of the above services leads to increased opioid use or initiation of injection use Substantial evidence that harm reduction services decreases in substance-related harms and risky behaviors, HIV and hepatitis C infection, and overdose deaths Harm reduction services is not treatment and can promote entry into addiction treatment which should be concurrently offered and encouraged Residential Treatment No systematic reviews or meta-analyses on residential treatment programs for opioid use disorder and no large clinical trials comparing to other interventions Overall lack of evidence does not mean residential treatment is ineffective, but understudied Observational cohort studies in the UK have found that relapse is relatively common following discharged from residential treatment for opioid use disorder Smyth et al. (2010) reported after six-week residential treatment program in Ireland 80% relapse within one month 59% relapsed within one week National Treatment Outcome Research Study (NTORS) 57% heroin use within 30 days 31% relapsing to regular heroin use at 1-year follow-up NTORS at 4 5 years follow-up, injecting rates dropped from 61% at intake to 29% abstinence increased from 23.2% to 48.6% improvements in safer injection practices, psychological and physical health, and reductions in criminal behavior Residential treatment US data varied results One randomized trial in treatment outcomes for residential treatment < 7 weeks no difference compared to no treatment > 7 weeks, improved outcomes increased likelihood of employment or enrolment in school, decreased likelihood of criminal conviction or incarceration, and decreased likelihood of heroin use An additional study found 4 week residential treatment decreased maladaptive cognitive and behavioral patterns that may contribute to ongoing substance use problems in adults with opioid use disorder Another randomized clinical trial found that a combination of community reinforcement and family training was associated with improved retention in treatment and reductions in opioid and other drug use providers should be aware of risks associated with loss of tolerance for patients who attend residential treatment programs when not using opioid agonist therapy (risk is 2 x) 11
12 naltrexone Naltrexone is an opioid receptor antagonist May increase the risk of overdose for patients who stop taking the medication and relapse to opioid use, non-randomized study of naltrexone-associated mortality rates in Australia 3 to 7 X higher than methadone-related mortality rates Oral naltrexone (currently the only formulation available in Canada), have limited benefits over placebo 2011 meta-analysis found no statistically significant differences in retention or abstinence rates for oral naltrexone compared to placebo or no treatment Across studies, treatment retention rates were low with oral naltrexone treatment However, there are some circumstances where oral naltrexone may be an appropriate option individuals who wish to avoid OAT who are highly motivated to stay abstinent, including individuals in safety sensitive positions that prohibit opioid agonist treatment Several randomized controlled trials have found that injectable naltrexone is superior to placebo in terms of improved retention in treatment, increased abstinence rates and decreased opioid cravings Combination approaches and movement between approaches residential treatment facilities and opioid agonist treatment programs have often operated independently excluding participants on stable opioid agonist treatment from residential treatment create barriers Best approach is the integration of both strategies particularly for polysubstance users STEPPED CARE STRATEGY (comparing initiation on buprenorphine/naloxone and escalation to methadone if necessary) vs standard methadone treatment relatively superior safety profile of buprenorphine/naloxone (in the absence of concurrent alcohol or benzodiazepine use) ease of transitioning from buprenorphine/naloxone to methadone Improved cost of buprenorphine due to reduced need for daily dosing Result stepped care approach was equally efficacious compared to optimally delivered methadone treatment Conclusion that due to safety profile of buprenorphine that it be used as first-line treatment for opioid use disorder 12
13 TAPERING limited evidence to guide strategies for transitioning off agonist therapies majority of tapers from methadone treatment appear to be unsuccessful (approximately 87%) increased odds of success when doses are reduced gradually with longer periods Voluntary taper as shared decision more successful than forced tapering Large gap in evidence in this area and relies heavily in practitioner and patient relationship and evaluation of bio-psycho-social-spiritual stability Go slow and continually monitor Summary and recommendations 1. Withdrawal management alone (detoxification without immediate transition to longterm addiction treatment) is not recommended 2. Initiate OAT with buprenorphine/naloxone whenever feasible 3. Initiate OAT with methadone when treatment with buprenorphine/naloxone is not preferable 4. If withdrawal management is pursued, for most patients, this can be provided more safely in an outpatient rather than inpatient setting. During withdrawal management, patients should be immediately transitioned to long-term addiction treatment to assist in preventing relapse and associated harms 5. For individuals responding poorly to buprenorphine/naloxone, consider transition to methadone 6. For individuals responding poorly to methadone, or with successful and sustained response to methadone desiring treatment simplification, consider transition to buprenorphine/naloxone 7. For individuals with a successful and sustained response to OAT taper, consider slow taper (e.g., 12 months) Summary of Recommendations 8. Psychosocial treatment interventions and supports should be routinely offered in conjunction with pharmacological treatment 9. For patients wishing to avoid long-term OAT, provide supervised slow (> 1 month) rather than rapid (< 1 week) inpatient opioid agonist taper During withdrawal management, patients should be transitioned to long-term addiction treatment to prevent relapse and associated harms Oral naltrexone can also be considered as an adjunct upon cessation of opioid use 10. For patients who have been unsuccessful with first- and second-line treatment options, opioid agonist treatment with slow-release oral morphine (prescribed as once-daily witnessed doses) can be considered 11. Harm reduction Information and referral to take-home naloxone programs and other harm reduction services should be routinely offered as part of standard care for opioid use disorder 13
14 Thank You 14
OAT Transitions - focus on microdosing. Mark McLean MD MSc FRCPC CISAM DABAM
 OAT Transitions - focus on microdosing Mark McLean MD MSc FRCPC CISAM DABAM Disclosures No pharmaceutical industry or other financial conflicts of interest Study Physician for research funded by Canadian
OAT Transitions - focus on microdosing Mark McLean MD MSc FRCPC CISAM DABAM Disclosures No pharmaceutical industry or other financial conflicts of interest Study Physician for research funded by Canadian
Buprenorphine as a Treatment Option for Opioid Use Disorder
 Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Building capacity for a CHC response to Ontario's Opioid Crisis
 Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Buprenorphine: An Introduction. Sharon Stancliff, MD Harm Reduction Coalition September 2008
 Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Medication Assisted Treatment. Nicole Gastala, MD
 Medication Assisted Treatment Nicole Gastala, MD Objectives Training Goals: To enhance the understanding of the participants in use of medication assisted therapy To increase the knowledge of participants
Medication Assisted Treatment Nicole Gastala, MD Objectives Training Goals: To enhance the understanding of the participants in use of medication assisted therapy To increase the knowledge of participants
FY17 SCOPE OF WORK TEMPLATE. Name of Program/Services: Medication-Assisted Treatment: Buprenorphine
 FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
a Guideline for the Clinical Management of Opioid Addiction
 a Guideline for the Clinical Management of Opioid Addiction Published 2015 This page left intentionally blank for double-sided printing. Vancouver Coastal Health & Providence Health Care Opioid Use Disorder
a Guideline for the Clinical Management of Opioid Addiction Published 2015 This page left intentionally blank for double-sided printing. Vancouver Coastal Health & Providence Health Care Opioid Use Disorder
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines
 The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets. Risk Evaluation and Mitigation Strategy (REMS) Program
 Program") SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations
 Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medications for Opioid Use Disorder. Charles Brackett, MD, MPH General Internal Medicine, DHMC
 Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine
 [Patient-focused, evidence-based addiction treatment] Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine BrightView Health All Rights Reserved www.brightviewhealth.com
[Patient-focused, evidence-based addiction treatment] Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine BrightView Health All Rights Reserved www.brightviewhealth.com
NALTREXONE DAVID CRABTREE, MD, MPH UNIVERSITY OF UTAH HEALTH, 2018
 NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT)
") Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) What has changed? Effective January 16, 2018, Coordinated Care will change the requirement for form HCA 13-333 Medication
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) What has changed? Effective January 16, 2018, Coordinated Care will change the requirement for form HCA 13-333 Medication
Rule Governing the Prescribing of Opioids for Pain
 Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Optimizing Opioid Dependence Treatment A Guideline for Pharmacists
 Optimizing Opioid Dependence Treatment A Guideline for Pharmacists Module 3: Optimal Use of Methadone F e b r u a r y 2 0 1 5 Learning Objectives To know and understand the pathophysiology of substance
Optimizing Opioid Dependence Treatment A Guideline for Pharmacists Module 3: Optimal Use of Methadone F e b r u a r y 2 0 1 5 Learning Objectives To know and understand the pathophysiology of substance
Medication-Assisted Treatment (MAT) Overview
 Overview") Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT)
") Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) For Apple Health clients served Fee-for-Service and through contracted Medicaid Managed Care Organizations Updated January
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) For Apple Health clients served Fee-for-Service and through contracted Medicaid Managed Care Organizations Updated January
OPIOID SUBSTITUTION THERAPY RISKS & BENEFITS
 OPIOID SUBSTITUTION THERAPY RISKS & BENEFITS LEO O. LANOIE, MD, MPH, FCFP, CCSAM, ABAM, FISAM, MRO Dr. Leo Lanoie, 2017 DISCLAIMER In the past year I have accepted funds from Purdue for speaking OPIOID
OPIOID SUBSTITUTION THERAPY RISKS & BENEFITS LEO O. LANOIE, MD, MPH, FCFP, CCSAM, ABAM, FISAM, MRO Dr. Leo Lanoie, 2017 DISCLAIMER In the past year I have accepted funds from Purdue for speaking OPIOID
Agenda. 1 Opioid Addiction in the United States. Evidence-based treatments for OUD. OUD Treatment: Best Practices. 4 Groups: Our Model
 Agenda 1 Opioid Addiction in the United States 2 Evidence-based treatments for OUD OUD Treatment: Best Practices 4 Groups: Our Model 2 Groups is a national network of clinics providing affordable, evidencebased
Agenda 1 Opioid Addiction in the United States 2 Evidence-based treatments for OUD OUD Treatment: Best Practices 4 Groups: Our Model 2 Groups is a national network of clinics providing affordable, evidencebased
Opioid Agonists. Natural derivatives of opium poppy - Opium - Morphine - Codeine
 Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Opioid Step Policy. Description. Section: Prescription Drugs Effective Date: April 1, 2018
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Opioid Step Policy Page: 1 of 6 Last Review Date: March 16, 2018 Opioid Step Policy Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Opioid Step Policy Page: 1 of 6 Last Review Date: March 16, 2018 Opioid Step Policy Description
Noel Schenk MD. Davis Behavioral Health
 Noel Schenk MD Davis Behavioral Health Michael Botticelli Director of National Drug Control Policy What is Addiction? Addiction is defined as a chronic, relapsing brain disease that is characterized by
Noel Schenk MD Davis Behavioral Health Michael Botticelli Director of National Drug Control Policy What is Addiction? Addiction is defined as a chronic, relapsing brain disease that is characterized by
Opiate Dependency bka Opioid Addiction
 Opiate Dependency bka Opioid Addiction GP CME Dunedin July 2012 Doug Sellman Professor of Psychiatry and Addiction Medicine Director, National Addiction Centre University of Otago, Christchurch What this
Opiate Dependency bka Opioid Addiction GP CME Dunedin July 2012 Doug Sellman Professor of Psychiatry and Addiction Medicine Director, National Addiction Centre University of Otago, Christchurch What this
Methadone Maintenance 101
 Methadone Maintenance 101 OTP/DAILY DOSING CLINICS - ANDREW PUTNEY MD Conflicts of Interest - Employed by Acadia HealthCare 1 Why Methadone? At adequate doses methadone decreases opioid withdrawal symptoms
Methadone Maintenance 101 OTP/DAILY DOSING CLINICS - ANDREW PUTNEY MD Conflicts of Interest - Employed by Acadia HealthCare 1 Why Methadone? At adequate doses methadone decreases opioid withdrawal symptoms
HARM REDUCTION & TREATMENT. Devin Reaves MSW
 HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
Methadone Maintenance
 Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT
 and acute pain management on MAT") An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
Acute General Medical and Surgical Admission:
 Acute General Medical and Surgical Admission: Managing Substance Use Disorders in Patients Who are Severely Ill Scott Grantham, MD Executive Director, Behavioral Health Saint Francis Health System By the
Acute General Medical and Surgical Admission: Managing Substance Use Disorders in Patients Who are Severely Ill Scott Grantham, MD Executive Director, Behavioral Health Saint Francis Health System By the
Management Options for Opioid Dependence:
 Management Options for Opioid Dependence: Policy Implications and Recommendations Dan Ollendorf, PhD Sarah Jane Reed, MSc New England CEPAC Goal: To improve the application of evidence to guide practice
Management Options for Opioid Dependence: Policy Implications and Recommendations Dan Ollendorf, PhD Sarah Jane Reed, MSc New England CEPAC Goal: To improve the application of evidence to guide practice
Buprenorphine pharmacology
 Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Faculty/Presenter Disclosure
 Provincial Guidelines for the Clinical Management of Opioid Use Disorder Leslie Lappalainen MD Family and Addiction Medicine Medical Lead for Addiction Medicine, Interior Health, Mental Health and Substance
Provincial Guidelines for the Clinical Management of Opioid Use Disorder Leslie Lappalainen MD Family and Addiction Medicine Medical Lead for Addiction Medicine, Interior Health, Mental Health and Substance
Medication Assisted Treatment of an Opioid Use Disorder. J. Craig Allen, MD. Medical Director, Rushford
 Medication Assisted Treatment of an Opioid Use Disorder J. Craig Allen, MD. Medical Director, Rushford Learning objectives At the conclusion of this activity, participants will be able to: Understand
Medication Assisted Treatment of an Opioid Use Disorder J. Craig Allen, MD. Medical Director, Rushford Learning objectives At the conclusion of this activity, participants will be able to: Understand
MAT in the Corrections Setting
 MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
Arizona s Opioid Epidemic
 Arizona s Opioid Epidemic Rise in Heroin Addiction and the Dangers of Fentanyl Sara Salek, MD Chief Medical Officer Shana Malone, MS Clinical Initiatives Project Manager 1 Disclosures None The National
Arizona s Opioid Epidemic Rise in Heroin Addiction and the Dangers of Fentanyl Sara Salek, MD Chief Medical Officer Shana Malone, MS Clinical Initiatives Project Manager 1 Disclosures None The National
Buprenorphine is the most effective office-based treatment available for heroin and prescription opioid addiction
 Buprenorphine is the most effective office-based treatment available for heroin and prescription opioid addiction The Problem The overdose death rate in Missouri and in the country has been rising for
Buprenorphine is the most effective office-based treatment available for heroin and prescription opioid addiction The Problem The overdose death rate in Missouri and in the country has been rising for
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Drug Misuse: opiate detoxification of drug misusers in the community, hospital and prison. 1.1 Short title Drug misuse detoxification
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Drug Misuse: opiate detoxification of drug misusers in the community, hospital and prison. 1.1 Short title Drug misuse detoxification
Buprenorphine Prescribing as a Patient- Centered Medical Home Enhancement
 Buprenorphine Prescribing as a Patient- Centered Medical Home Enhancement TANNER NISSLY DO, BOB LEVY MD FASAM, MICHELE MANDRICH MSW, CMPE AS YOU ENTER, PLEASE SET UP TO PARTICIPATE IN OUR POLL EVERYWHERE
Buprenorphine Prescribing as a Patient- Centered Medical Home Enhancement TANNER NISSLY DO, BOB LEVY MD FASAM, MICHELE MANDRICH MSW, CMPE AS YOU ENTER, PLEASE SET UP TO PARTICIPATE IN OUR POLL EVERYWHERE
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE
 LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
Should buprenorphine be covered for maintenance treatment in opioid dependent persons?
 Prepared by: Silvia Pregno May 13,2012 Patients: people with opioid dependence Should buprenorphine be covered for maintenance treatment in opioid dependent persons? Intervention: buprenorphine Comparison:
Prepared by: Silvia Pregno May 13,2012 Patients: people with opioid dependence Should buprenorphine be covered for maintenance treatment in opioid dependent persons? Intervention: buprenorphine Comparison:
Pharmacotherapy for opioid addiction. Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco
 Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Opioid Dependence and Buprenorphine Management
 Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Prepublication Requirements
 Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Academic Medical School: Implementing Curriculum in Chronic Pain and Opioid Misuse. Jill M Williams, MD
 Academic Medical School: Implementing Curriculum in Chronic Pain and Opioid Misuse Pain, Pain Management and the Opioid Epidemic Symposium Jill M Williams, MD Professor Psychiatry Director, Division Addiction
Academic Medical School: Implementing Curriculum in Chronic Pain and Opioid Misuse Pain, Pain Management and the Opioid Epidemic Symposium Jill M Williams, MD Professor Psychiatry Director, Division Addiction
Buprenorphine for Family Medicine. Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17
 + Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
+ Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
Models of good practice in drug treatment in Europe. Project group
 Models of good practice in drug treatment in Europe ( moretreat 2006329 ) Project group Hamburg, London, Rome, Stockholm, Vienna, Warsaw, Zurich Project duration: 17 months from April 2006 August 2008
Models of good practice in drug treatment in Europe ( moretreat 2006329 ) Project group Hamburg, London, Rome, Stockholm, Vienna, Warsaw, Zurich Project duration: 17 months from April 2006 August 2008
OST. Pharmacology & Therapeutics. Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO
 OST Pharmacology & Therapeutics Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO Disclaimer In the past two years I have received no payment for services from any agency other than government or academic.
OST Pharmacology & Therapeutics Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO Disclaimer In the past two years I have received no payment for services from any agency other than government or academic.
Opioid Review and MAT Clinic CDC Guidelines
 1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings
 Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Understanding and Combating the Heroin Epidemic
 Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
Addiction to Opioids. Marvin D. Seppala, MD Chief Medical Officer
 Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
RECOMMENDATIONS FOR HEALTH CARE PROVIDERS
 Ending Addiction Changes Everything RECOMMENDATIONS FOR HEALTH CARE PROVIDERS CRITICAL ADDICTION PREVENTION, TREATMENT AND MANAGEMENT SERVICES TO INCLUDE IN ROUTINE HEALTH CARE PRACTICE JULY 2013 In the
Ending Addiction Changes Everything RECOMMENDATIONS FOR HEALTH CARE PROVIDERS CRITICAL ADDICTION PREVENTION, TREATMENT AND MANAGEMENT SERVICES TO INCLUDE IN ROUTINE HEALTH CARE PRACTICE JULY 2013 In the
HARM REDUCTION & THE OPIOID EPIDEMIC. CHELSEA RAINWATER Co-Founder & Executive Director No Overdose Baton Rouge
 HARM REDUCTION & THE OPIOID EPIDEMIC CHELSEA RAINWATER Co-Founder & Executive Director No Overdose Baton Rouge NO OVERDOSE BATON ROUGE Formed in late 2013 Community education Naloxone distribution Syringe
HARM REDUCTION & THE OPIOID EPIDEMIC CHELSEA RAINWATER Co-Founder & Executive Director No Overdose Baton Rouge NO OVERDOSE BATON ROUGE Formed in late 2013 Community education Naloxone distribution Syringe
The CARA & Buprenorphine Prescribing for APNs & PAs
 The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Drug Misuse: opiate detoxification of drug misusers in the community, hospital and prison. 1.1 Short title Drug misuse detoxification
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Drug Misuse: opiate detoxification of drug misusers in the community, hospital and prison. 1.1 Short title Drug misuse detoxification
2/19/18. Today s talk. Today s talk. The Role of Behavioral Interventions in Buprenorphine Treatment of Opioid Use Disorders
 The Role of Behavioral Interventions in Buprenorphine Treatment of Opioid Use Disorders Roger D. Weiss, MD Chief, Division of Alcohol and Drug Abuse, McLean Hospital, Belmont, MA Professor of Psychiatry,
The Role of Behavioral Interventions in Buprenorphine Treatment of Opioid Use Disorders Roger D. Weiss, MD Chief, Division of Alcohol and Drug Abuse, McLean Hospital, Belmont, MA Professor of Psychiatry,
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates
 and Medication Assisted Treatment (MAT) for Opiates") Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
ONTARIO S STRATEGY TO PREVENT OPIOID ADDICTION AND OVERDOSE. Dr. David Williams Chief Medical Officer of Health
 ONTARIO S STRATEGY TO PREVENT OPIOID ADDICTION AND OVERDOSE Dr. David Williams Chief Medical Officer of Health National opioid-related mortality data, 2016 (Health Canada) Provincial Overdose Coordinator
ONTARIO S STRATEGY TO PREVENT OPIOID ADDICTION AND OVERDOSE Dr. David Williams Chief Medical Officer of Health National opioid-related mortality data, 2016 (Health Canada) Provincial Overdose Coordinator
Opioid dependence and buprenorphine treatment
 Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
9/13/2017. Buprenorphine Treatment (Suboxone) Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare
 Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare") Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Closing the Loop in Treating Opioid Addiction:
 Closing the Loop in Treating Opioid Addiction: Integrating MAT into Prison and Jail Health Systems May 9, 2018 Webinar Housekeeping All lines are muted This session will be recorded To ask a question:
Closing the Loop in Treating Opioid Addiction: Integrating MAT into Prison and Jail Health Systems May 9, 2018 Webinar Housekeeping All lines are muted This session will be recorded To ask a question:
Opioids Research to Practice
 Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Brief History of Methadone Maintenance Treatment
 METHADONE Brief History of Methadone Maintenance Treatment Methadone maintenance treatment was on the cusp of the social revolution in the sixties. Doctors and public health workers had concluded what
METHADONE Brief History of Methadone Maintenance Treatment Methadone maintenance treatment was on the cusp of the social revolution in the sixties. Doctors and public health workers had concluded what
Appendix F Federation of State Medical Boards
 Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
CDC Guideline for Prescribing Opioids for Chronic Pain. Centers for Disease Control and Prevention National Center for Injury Prevention and Control
 CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
Opioid use disorder is one of the most challenging forms
 VULNERABLE POPULATIONS CPD Management of opioid use disorders: a national clinical practice guideline Julie Bruneau MD MSc, Keith Ahamad MD, Marie-Ève Goyer MD MSc, Ginette Poulin MD, Peter Selby MBBS
VULNERABLE POPULATIONS CPD Management of opioid use disorders: a national clinical practice guideline Julie Bruneau MD MSc, Keith Ahamad MD, Marie-Ève Goyer MD MSc, Ginette Poulin MD, Peter Selby MBBS
Public Policy Statement on the Regulation of Office-Based Opioid Treatment
 Public Policy Statement on the Regulation of Office-Based Opioid Treatment Background Office-based opioid treatment (OBOT) commonly refers to outpatient treatment services provided outside of licensed
Public Policy Statement on the Regulation of Office-Based Opioid Treatment Background Office-based opioid treatment (OBOT) commonly refers to outpatient treatment services provided outside of licensed
Dr Alistair Dunn. General Practitioner Whangarei
 Dr Alistair Dunn General Practitioner Whangarei 1982 Temgesic = Buprenorphine Sublingual opiate analgesic 0.2 mg Popular drug of abuse 1991 Temgesic NX = Bup & Nalxone Nalxone added to deter abuse 1999
Dr Alistair Dunn General Practitioner Whangarei 1982 Temgesic = Buprenorphine Sublingual opiate analgesic 0.2 mg Popular drug of abuse 1991 Temgesic NX = Bup & Nalxone Nalxone added to deter abuse 1999
Clinical Guidelines for the Pharmacologic Treatment of Opioid Use Disorder
 Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of Opioid Dependence Abbreviated Version
 Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of Opioid Dependence Abbreviated Version Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of
Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of Opioid Dependence Abbreviated Version Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of
Disclosures. Topics of today s training 4/24/2017. Evolving Treads in Medication Assisted Treatment. Christopher J Davis D.O.
 Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Medication Assisted Treatment:
 Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
ADVANCED BEHAVIORAL HEALTH, INC. Clinical Level of Care Guidelines
 The Clinical Level of Care Guidelines contained on the following pages have been developed as a guide to assist care managers, physicians and providers in making medical necessity decisions about the least
The Clinical Level of Care Guidelines contained on the following pages have been developed as a guide to assist care managers, physicians and providers in making medical necessity decisions about the least
Revised 9/30/2016. Primary Care Provider Pain Management Toolkit
 Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
METHADONE TO BUPRENORPHINE TRANSFERS TRANSITIONING FROM METHADONE MAINTENANCE TO BUPRENORPHINE/NALOXONE
 METHADONE TO BUPRENORPHINE TRANSFERS TRANSITIONING FROM METHADONE MAINTENANCE TO BUPRENORPHINE/NALOXONE Work with methadone clinic staff to coordinate the methadone taper, with the transition to buprenorphine/naloxone:
METHADONE TO BUPRENORPHINE TRANSFERS TRANSITIONING FROM METHADONE MAINTENANCE TO BUPRENORPHINE/NALOXONE Work with methadone clinic staff to coordinate the methadone taper, with the transition to buprenorphine/naloxone:
MEDICALLY ASSISTED TREATMENT IN PROBLEMATIC OPIOID Punta Cana 2018
 MEDICALLY ASSISTED TREATMENT IN PROBLEMATIC OPIOID USE @joelbordman Punta Cana 2018 Copyright 2017 by Sea Courses Inc All rights reserved. No part of this document may be reproduced, copied, stored, or
MEDICALLY ASSISTED TREATMENT IN PROBLEMATIC OPIOID USE @joelbordman Punta Cana 2018 Copyright 2017 by Sea Courses Inc All rights reserved. No part of this document may be reproduced, copied, stored, or
Opioid Management of Chronic (Non- Cancer) Pain
 Pain") Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Public Health Association of British Columbia
 October 30 th, 2017 Open Letter to the Government of British Columbia: BC Needs an OPIOID ACTION PLAN Since April, 2016 when the epidemic of opioid overdose deaths was declared a Public Health Emergency
October 30 th, 2017 Open Letter to the Government of British Columbia: BC Needs an OPIOID ACTION PLAN Since April, 2016 when the epidemic of opioid overdose deaths was declared a Public Health Emergency
Management of Opioid Use Disorder in Primary Care
 1 Northwest ATTC presents Management of Opioid Use Disorder in Primary Care Joseph O. Merrill, MD, MPH University of Washington Associate Professor of Medicine 4/26/2018 Today s Presenter 2 Joseph Merrill,
1 Northwest ATTC presents Management of Opioid Use Disorder in Primary Care Joseph O. Merrill, MD, MPH University of Washington Associate Professor of Medicine 4/26/2018 Today s Presenter 2 Joseph Merrill,
The role of behavioral interventions in buprenorphine treatment of opioid use disorders
 The role of behavioral interventions in buprenorphine treatment of opioid use disorders Roger D. Weiss, MD Harvard Medical School, Boston, MA, McLean Hospital, Belmont, MA, USA Today s talk Review of studies
The role of behavioral interventions in buprenorphine treatment of opioid use disorders Roger D. Weiss, MD Harvard Medical School, Boston, MA, McLean Hospital, Belmont, MA, USA Today s talk Review of studies
Medication-Assisted Treatment (MAT) for Opioid Use Disorders
 for Opioid Use Disorders") Medication-Assisted Treatment (MAT) for Opioid Use Disorders Sybil Marsh MA MD FASAM Department of Family Medicine and Community Health Case Western Reserve University/UHCMC Learning Objective 1 Following
Medication-Assisted Treatment (MAT) for Opioid Use Disorders Sybil Marsh MA MD FASAM Department of Family Medicine and Community Health Case Western Reserve University/UHCMC Learning Objective 1 Following
Proposed Revision to Med (i)
") Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
6/6/2018. Objectives. Outline. Rethinking Medication Treatment for Opioid Use Disorder
 Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
The Opioid Crisis: What Can Physicians Do About It?
 The Opioid Crisis: What Can Physicians Do About It? Richard S. Schottenfeld, M.D. Professor and Chair, Department of Psychiatry and Behavioral Sciences 2018 Louis J. Kolodner Memorial Lecture Disclosures
The Opioid Crisis: What Can Physicians Do About It? Richard S. Schottenfeld, M.D. Professor and Chair, Department of Psychiatry and Behavioral Sciences 2018 Louis J. Kolodner Memorial Lecture Disclosures
How Can Injectable Hydromorphone and Pharmaceutical-Grade Heroin be Used to Treat Opioid Use Disorder?
 How Can Injectable Hydromorphone 0 and Pharmaceutical-Grade Heroin be Used to Treat Opioid Use Disorder? Dr. Eugenia Oviedo-Joekes University of British Columbia Dr. Martin Schechter University of British
How Can Injectable Hydromorphone 0 and Pharmaceutical-Grade Heroin be Used to Treat Opioid Use Disorder? Dr. Eugenia Oviedo-Joekes University of British Columbia Dr. Martin Schechter University of British
Methadone and Pregnancy
 Methadone and Pregnancy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Charissa Patricelli, MD, CCFP, ABAM Clinical Associate Professor, Dept. of Family Practice UBC American Board of Addiction Medicine
Methadone and Pregnancy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Charissa Patricelli, MD, CCFP, ABAM Clinical Associate Professor, Dept. of Family Practice UBC American Board of Addiction Medicine
Medication-assisted opioid addiction treatments: OB/GYN
 5/13/16se Medication-assisted opioid addiction treatments: OB/GYN In October 2002, the Food and Drug Administration (FDA) approved buprenorphine monotherapy product, Subutex, and a buprenorphine/naloxone
5/13/16se Medication-assisted opioid addiction treatments: OB/GYN In October 2002, the Food and Drug Administration (FDA) approved buprenorphine monotherapy product, Subutex, and a buprenorphine/naloxone
Special Populations health complications of Substance Use Anthony Dekker DO, OMED 2018 San Diego
 Special Populations health complications of Substance Use Anthony Dekker DO, OMED 2018 San Diego 1 Disclosure Anthony Dekker DO has presented numerous programs on Chronic Pain Management and Addiction
Special Populations health complications of Substance Use Anthony Dekker DO, OMED 2018 San Diego 1 Disclosure Anthony Dekker DO has presented numerous programs on Chronic Pain Management and Addiction