Medication-Assisted Treatment (MAT) for Opioid Use Disorders
|
|
|
- Augustus Patrick
- 5 years ago
- Views:
Transcription

1 Medication-Assisted Treatment (MAT) for Opioid Use Disorders Sybil Marsh MA MD FASAM Department of Family Medicine and Community Health Case Western Reserve University/UHCMC
2 Learning Objective 1 Following this presentation, participants will be able to name 3 medications useful in the treatment of opiate use disorder, and describe for each : indications mechanism of action dosing common side effects effectiveness 2
3 Learning Objective 2 Review some fears and misconceptions about medication-assisted treatment (MAT) that can interfere with its appropriate use Appreciate evidence for the statement that opioid substitution treatment is effective in suppressing illicit opioid use and reducing all cause an overdose mortality (Sordo, BMJ, 2017) 3
4 Learning Objective 3 Discuss strategies to more fully integrate MAT into existing mental health, medical and substance use disorder services 4
5 5
6 6
7 7
8 CDC

9 Ohio needs effective ways to prevent overdose deaths and other costs of OUD 9

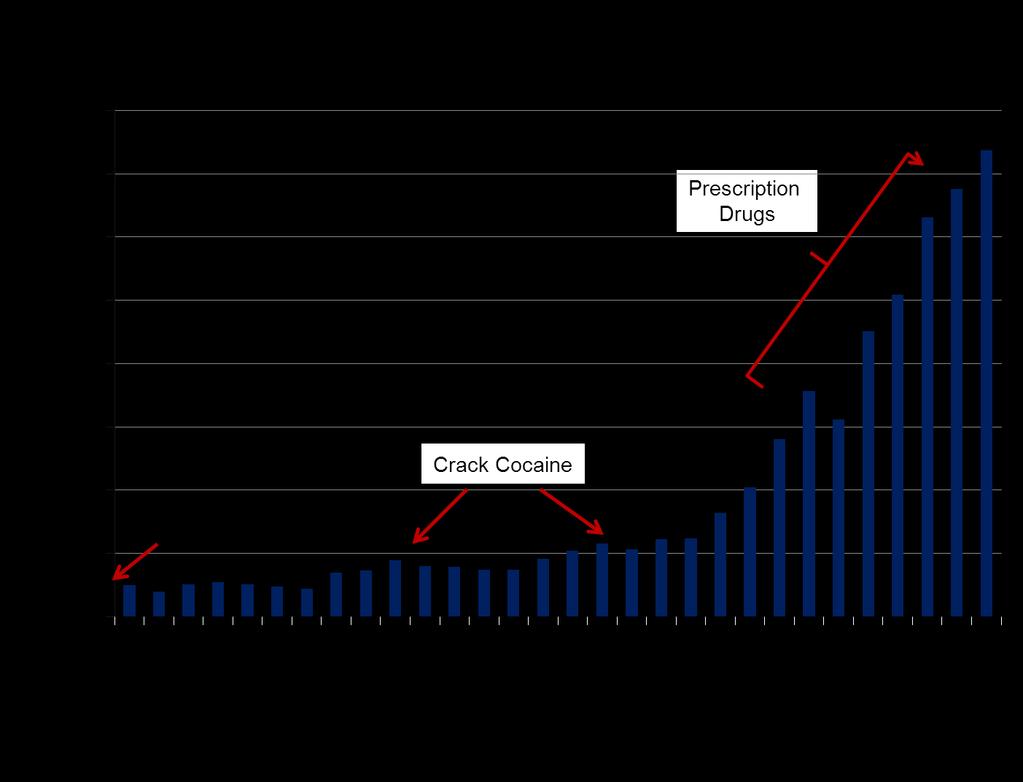
10 OD deaths- prescription vs other opioids 10
11 What does it mean? Even though doses of prescribed opioids and overdose deaths related to them have declined over time, the percentage of deaths due to other opioids has increased Total deaths by opioid overdose have increased over recent years, and the major source is illicit Opioids from every source are deadly They re not going away We need to prevent first use and We need effective treatment for people with opioid use disorder, including long-term relapse prevention 11
12 Is MAT effective? MAT, particularly with opioid agonist medications, has been found to reduce morbidity and mortality, decrease overdose deaths, reduce transmission of infectious disease, increase treatment retention, improve social functioning, and reduce criminal activity. National and international health organizations, such as the American Society of Addiction Medicine (ASAM), and the World Health Organization, consider MAT an evidence-based best practice for treating opioid use disorder. SAMHSA Advisory
13 Indications for MAT medications Methadone and buprenorphine (or buprenorphine/ naloxone) are approved to treat opioid dependence Extended-release injectable naltrexone is approved for prevention of relapse to opioid use Short acting oral naltrexone reduces craving and binging on alcohol Naloxone treats opioid overdose (temporarily) 13
14 Indications for MAT medications Successful use of MAT requires: Medically-assisted withdrawal for naltrexone and ` buprenorphine ( detox )- NOT for methadone Adequate medical care for life threatening disease (infections, liver disease, cardiovascular, psychiatric disease) Willingness to engage in counselling, behavioral therapies, outpatient psychosocial treatment including mutual help groups like NA and AA Resources that facilitate treatment for as long as necessary Informed consent as for other medications 14
15 Mechanism of MAT medications Methadone agonist Fills opiate receptors Same effects as other opiates- but slower and flatter, prevents craving, can cause sedation, but not euphoria Buprenorphine partial agonist Fills opiate receptors imperfectly Partial opiate effect and a ceiling dose- Naltrexone antagonist Blocks opiate receptors NO opiate effect 15
16 Effect of MAT on Opioid Receptors 16
17 Methadone Opiate agonist for treatment of severe opiate use disorder Well-studied and effective (BMJ, 2017) Normalizes function/return to work, decreases crime/violence, reduces HIV and Hepatitis C exposure Dose is individualized to stop craving, avoid sedation Goal is lowest dose that prevents withdrawal, minimizes craving and blocks high caused by opiates Not a stand-alone but a program of treatment Enhanced services improve outcomes Counseling, medical, behavioral, social/vocational services, etc. 17
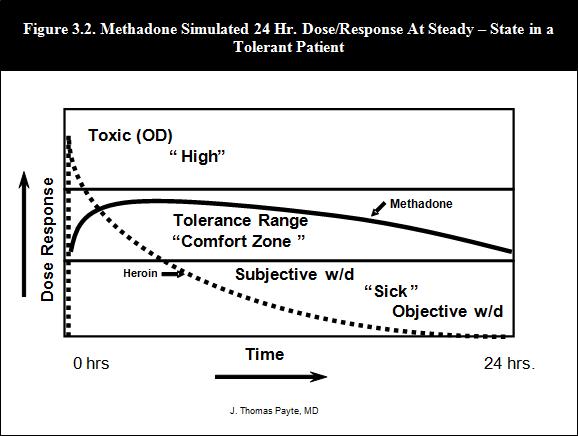
18 Methadone
19 Methadone dosing Usually taken once a day to suppress withdrawal for 24 to 36 hours Usually given in liquid form or wafer by MAT Program Induction phase no more than 30 to 40 mg on the first day of treatment Dose changes usually occur once a week (every 5-7 days) More rapid dose increases can cause overdose because of rise in blood level with each dose till dose #5 Maintenance phase usually mg, sometimes less Sometimes more for high tolerance, CP 450-inducing medications (like Depakote) 19
20 Methadone side effects and hazards Common side effects Sweating, constipation, decreased libido, mild anorexia/nausea, weight gain, water retention, dry mouth Adverse effects Cardiac rhythm abnormalities Prolongation of QTc (usually seen with very high doses, mean of 350mg daily) Oversedation at excessive dose- different from being high Potential interaction with risk of oversedation with ALCOHOL, BENZODIAZEPINES, BARBITURATES 20
21 Methadone: Still an addict? PHYSICAL DEPENDENCE is not SUBSTANCE USE DISORDER/ ADDICTION Pharmacology of methadone prevents highs and lows common with short-acting drugs and normalizes patient functioning Overuse gives a side effect is sedation, not euphoria The patient is PHYSICALLY DEPENDENT on methadone, so might appear to be drug seeking to avoid withdrawal but no longer displays behaviors consistent with active opiate use disorder and instead shows evidence of improved quality of life Successful methadone treatment results in Severe Opioid Use Disorder in Remission not active addiction Dr. Bob said it best
22 Buprenorphine Approved in U.S. (2002) as office-based treatment (OBOT) as an alternative to methadone clinics Individual doctors may treat up to 30 patients at a time, using an special DEA number After 1 year, may increase to 100 patients Must be addiction medicine/addiction psychiatry certified OR complete 8 hour training Must comply with Federal, State and insurance rules and regulations 22
23 Buprenorphine mechanism Opioid partial agonist with a ceiling effect risk of overdose and abuse potential May precipitate opiate withdrawal in dependent individuals, so must be started carefully with negative urine drug screen- best started in mild to moderate withdrawal Approved for treatment of opiate dependence (severe opiate use disorder) Maintenance dose in the range of 8-16 mg daily, occasionally up to 24 mg Sublingual route of administration Buprenorphine only vs. Buprenorphine +naloxone- preferred! 23


24 Many variations, same mechanism Generic buprenorphine Subutex tabs, films Generic buprenorphine/naloxone Suboxone tabs, film Zubsolv Bunavail Not: Butrans patch (chronic pain) 24
25 Buprenorphine dosing Suboxone, Zubsolv and Bunavail are buprenorphine + naloxone in a 4:1 mixture Treatment agreement- informed consent Not a stand-alone, but a program - patient should begin a log of counselling, 12 step meetings, other recovery-promoting activities Induction phase Day 1: usual dose is 2 mg given every 2-3 hours, up to 8 mg Induction phase Day 2: start with 8mg, can go up to 16mg depending on patient symptoms 25
26 Buprenorphine- side effects and hazards Maintenance phase: usually 8 to 16 mg daily This may vary in clinical practice; 16mg dose covers ~95% of opiate receptors Adjust dose if necessary- consider craving, tolerance, interactions Adverse side effects: Liver abnormality, cytolytic hepatitis Common side effects: generally mild Constipation; dizziness; drowsiness; headache; nausea; sweating; vomiting; Strategies to manage need for full agonist opiates (surgery etc.) Potential interaction with alcohol (avoid), benzodiazepines, barbiturates- (avoid when able, minimize always) 26
27 Naltrexone mechanism Opiate antagonist to treat opiate dependence All effects of opiates are blocked Must undergo medically supervised withdrawal and be opiate-free when starting, or severe withdrawal occurs Blocks opioid receptors that are involved in the rewarding effects of opiates (& alcohol!) Long term effects on endorphins unknown Risk for hepatotoxicity Monitor liver enzymes 27
28 Naltrexone- injected, long acting Brand name is Vivitrol Injection of microspheres provides medication for 30 days Approved for alcoholism in 2006 Approved for opiate dependence Oct 2010 Given monthly, 380 mg appears to have increased efficacy versus 190 mg Reduces craving by occupying receptors and preventing opioid effect 28
29 Naltrexone- oral, short acting Brand name is Revia (oral tablets) Usual dose: 50mg daily Efficacy highest in patients who can abstain for 4 to 7 days before initiating treatment Not proven better than placebo High drop-out rate More compliance when the drug involved is alcohol, not opiate 29
30 Naltrexone side effects and hazards Side effects may include anxiety, nervousness, headache, joint pain, nausea- or none of these Injection requires knowledge of technique to avoid tissue damage May not reduce craving as well as agonists Non-compliance is the main barrier to success Not taking pills Not showing up for injection Most useful for highly motivated patients w/ external circumstances Impaired professionals, parolees, probationers, etc. for whom relapse would bring severe consequences Role in relapse prevention for non-dependent opioid users- think younger, newer users with hazardous use pattern, less physical dependence 30
31 CAUTION- Naltrexone needs aftercare When clients have had opiate receptors blocked for some time, their tolerance is reduced Returning to drug use at the same amount they used before blockade by naltrexone puts the client at INCREASED RISK for overdose and death due to lowered tolerance This information needs to be shared with all clients, who should get naloxone for emergency use Need more research on its long term effects Ongoing assessment and after care are needed to ensure continued USE and EFFECTIVENESS Most vulnerable time is when naltrexone is stopped because: Client attributes symptoms to it, stops with no back-up plan Client feels (or is told he is) ready to get back to normal life, is graduating and will NEVER use drugs again
 with ½ life 1 hour- gone quickly Gives enough time to go to ED")

32 Naloxone Opiate antagonist For overdose: Autoinjector, nasal atomizer routes Fast acting (2 minutes) with ½ life 1 hour- gone quickly Gives enough time to go to ED for naloxone IV drip and other help Many recipients REFUSE to go to ED, do not seek treatment, and may have medical and cognitive consequences of their overdose 32
33 MAT is MORE than MEDICATION Medications work on the opioid receptors to relieve craving and prevent withdrawal symptoms Behavioral treatments educate patients about the conditioning process and teach relapse prevention strategies. Evidence favors using these approaches TOGETHER Greater retention Less risk of relapse and overdose More opportunity for RECOVERY Combining the two types of treatment enables patients to stop using opioids and return to more stable aproductive lives. 33
34 Is MAT Recovery? Recovery status is best defined by factors other than medication status. Neither medication-assisted treatment of opioid addiction nor the cessation of such treatment by itself constitutes recovery. Recovery status instead hinges on broader achievements in health and social functioning with or without medication support. A. Thomas McLellan and William White 34
35 Duration of a MAT program- how long? AS LONG AS THE PATIENT NEEDS IT Mild OUD may respond to behavioral treatment, relapse prevention alone Severe OUD is a chronic relapsing lethal disorder and requires chronic effective treatment Compare it to diabetes Bad medicine: You ve been on insulin long enough! Time to taper it off! You can do it, just keep going to counselling and use the 12 steps! Bad medicine: You ve been in MAT long enough! Time to taper it off! You can do it, just keep going to counseling and use the 12 steps! 35
36 Possible Barriers to using MAT Fear # 1: Medication will eventually replace rehabilitation as the treatment of choice for addiction a pill for every ill Response # 1: Medication may be a useful adjunct to treatment Another tool in your toolbox It increases effectiveness of behavioral treatment because the client can pay attention and participate, and apply lessons without being overpowered by craving 36
37 Possible Barriers to using MAT Fear #2: Medication will distract from the difficult work needed for recovery from substance use disorder makes it too easy to be clean Response # 2: Medication makes withdrawal safer and more humane, and inceases retention in treatment Medication may allow the process of recovery to begin and continue Medication provides a safety net so the patient can take risks to do the difficult work 37
38 Possible Barriers to using MAT Fear # 3: Medication will continue an existing addiction Rationale # 3: Physical dependence to medication may occur, but addiction behavior will decrease MAT addresses co-occurring use disorders behaviorally or by intensifying treatment Some room for harm reduction 12 step approach to medications is clear and compatible with MAT, though some members opinions may not be 38
39 Possible Barriers to using MAT Fear # 4: Medication will cause new addictions Response # 4: Incidence is low because methadone and buprenorphine are not highly reinforcing- not worth it Physical dependence is not addiction 39
40 Possible Barriers to using MAT Fear # 4: Medication will cause new addictions Response # 4: Incidence is low because methadone and buprenorphine are not highly reinforcing- not worth it to use to get high Naltrexone not at all reinforcing Patient self-care includes education about risks of physical dependence and withdrawal prevention strategies 40
41 Other Barriers to MAT? Financial MAT may be an expense and insurance coverage inconsistent Logistical Not enough methadone clinics; not enough slots Many physicians are trained to prescribe buprenorphine, but relatively few are actually prescribing Why?! Usual treatment settings are not set up to provide MAT OBOT (Office Based Opiate Treatment) is time consuming in a primary care office and involves complex decision making Buprenorphine can be diverted and misused Mixed messages to prescribers about OBOT cause anxiety: We need you! We re watching you! 41
42 Helping clients get access to MAT Most patients self refer There are not enough treatment providers- waiting lists and travel Not all providers accept insurance How to help a reluctant client with the idea of starting and staying on MAT? Try some Motivational Interviewing: Listening and Reflection Ask-tell-ask to correct misinformation if I take meds, then I am not really sober What do you know about?.
43 More Motivational Interviewing What are the client s goals? How does medication fit (or not fit) with those goals? What are the pros and cons of the medication available? What are the patient s fears about medication? Use reflective listening What is the patient willing to do right now? Go for assessment? Talk about it some more? Medically supervised withdrawal and IOP or other behavioral interventions while thinking about it? Start with antagonist ( long long-acting injectable naltrexone), moving to agonist treatment if needed?
44 False + due to nutritional supplement/stimulant, so he stopped it* CFS system case closed*no mania on Depakote and a higher than average Suboxone dose* Self-pay, decreased drug screening schedule after 3 negative tests*stopped using heroin and has a job despite chronic pain*in intensive counseling now for mood disorder*kept her job as a dancer, and her 8 year old son*recovering from endocarditis* Got a knee replacement without relapsing*completes treatment for Hepatitis C*Finally getting counseling for life-long anxiety*breastfeeding her baby*didn t relapse when her grandma died and kept taking her meds* Stopping MAT in the spring, with 5 meetings per week*may have thyroid cancer, but hasn t relapsed* Hopes he ll be back for reinduction and COPD treatment post incarceration* Went off MAT and died of heroin overdose* Died of an overdose while in a MAT program* Died of cancer while on methadone, but not because of methadone* Lived another day because of MAT*
45 Discussion What strategies can your setting use to help patients/clients who would benefit get access to MAT? Inpatient and Outpatient AOD and MH Physical and Behavioral health Integrative health Think of a short-term goals (3 to 6 months) and long-term goals (12 to 24 months) that would improve access, use, or integration MAT services for clients who would benefit from them? What further training or support would help your organization meet these goals?

46 Summary MAT is an important tool in the toolkit for treating opioid use disorders- it can be lifesaving! Despite internal and external barriers, MAT can be successfully implemented; antagonist treatment presents fewer barriers More agonist treatment is needed state-wide to increase choice Set short- and long-term goals to support and more fully integrate MAT into your setting
47 Resources and References Center for Evidence Based Practices, Case Western Reserve University, BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Mid-America Addiction Technology Transfer Center. Psychotherapeutic Medications 2011: What Every Counselor Should Know
48 Resources and References Center for Substance Abuse Treatment. Medication Assisted Treatment for Opioid Addiction in Opioid Treatment Programs. Treatment Improvement Protocol (TIP) Series 43. DHHS Publication No. (SMA) Rockville, MD: Substance Abuse and Mental Health Services Administration, 2005 Sordo, Luis et al. Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis of covert studies. BMJ, 2017;357:j1550 SAMHSA Advisory, HHS Publication No. (SMA) ,
Medication-Assisted Treatment (MAT) Overview
 Overview") Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medications for Opioid Use Disorder. Charles Brackett, MD, MPH General Internal Medicine, DHMC
 Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine
 [Patient-focused, evidence-based addiction treatment] Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine BrightView Health All Rights Reserved www.brightviewhealth.com
[Patient-focused, evidence-based addiction treatment] Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine BrightView Health All Rights Reserved www.brightviewhealth.com
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates
 and Medication Assisted Treatment (MAT) for Opiates") Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Buprenorphine: An Introduction. Sharon Stancliff, MD Harm Reduction Coalition September 2008
 Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE
 LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
Serious Mental Illness and Opioid Use Disorder
 Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Understanding Medication in Addiction Treatment for Drug Court Participants
 Understanding Medication in Addiction Treatment for Drug Court Participants Introduction This pocket guide is for drug court participants who may be prescribed or considering medication as a part of addiction
Understanding Medication in Addiction Treatment for Drug Court Participants Introduction This pocket guide is for drug court participants who may be prescribed or considering medication as a part of addiction
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They?
 Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Methadone and Naltrexone ER
 Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Arwen Podesta, MD. ABIHM, ABAM, Forensic Psychiatry
 The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
Buprenorphine as a Treatment Option for Opioid Use Disorder
 Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Disclosures. Topics of today s training 4/24/2017. Evolving Treads in Medication Assisted Treatment. Christopher J Davis D.O.
 Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Agenda. 1 Opioid Addiction in the United States. Evidence-based treatments for OUD. OUD Treatment: Best Practices. 4 Groups: Our Model
 Agenda 1 Opioid Addiction in the United States 2 Evidence-based treatments for OUD OUD Treatment: Best Practices 4 Groups: Our Model 2 Groups is a national network of clinics providing affordable, evidencebased
Agenda 1 Opioid Addiction in the United States 2 Evidence-based treatments for OUD OUD Treatment: Best Practices 4 Groups: Our Model 2 Groups is a national network of clinics providing affordable, evidencebased
FY17 SCOPE OF WORK TEMPLATE. Name of Program/Services: Medication-Assisted Treatment: Buprenorphine
 FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
Methadone and Naltrexone ER
 Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Objectives Review Full Opioid
Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Objectives Review Full Opioid
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Treatment Approaches for Drug Addiction
 Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
MAT in the Corrections Setting
 MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
MEDICATION ASSISTED TREATMENT
 MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Vivitrol Vs. Suboxone
 Vivitrol Vs. Suboxone Vivitrol - Naltrexone Indicated for opiate dependence and alcohol withdrawal pure antagonist 380mg once every 4 weeks IM Peak plasma concentration in 2 hrs, followed by a second peak
Vivitrol Vs. Suboxone Vivitrol - Naltrexone Indicated for opiate dependence and alcohol withdrawal pure antagonist 380mg once every 4 weeks IM Peak plasma concentration in 2 hrs, followed by a second peak
Opioid Use Disorder Treatment Initiation in Diverse Settings
 Opioid Use Disorder Treatment Initiation in Diverse Settings Sarah Wakeman, MD, FASAM Medical Director, Mass General Substance Use Disorder Initiative Assistant Professor, Harvard Medical School Disclosures
Opioid Use Disorder Treatment Initiation in Diverse Settings Sarah Wakeman, MD, FASAM Medical Director, Mass General Substance Use Disorder Initiative Assistant Professor, Harvard Medical School Disclosures
Vivitrol Drug Court and Medication Assisted Treatment
 Vivitrol Drug Court and Medication Assisted Treatment Amy Black, CNP and Judge Fred Moses Court program Self-starters Mission Statement To provide court-managed, medically assisted drug intervention treatment
Vivitrol Drug Court and Medication Assisted Treatment Amy Black, CNP and Judge Fred Moses Court program Self-starters Mission Statement To provide court-managed, medically assisted drug intervention treatment
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines
 The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
Buprenorphine for Family Medicine. Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17
 + Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
+ Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
Opioid Dependence and Buprenorphine Management
 Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
The science of the mind: investigating mental health Treating addiction
 The science of the mind: investigating mental health Treating addiction : is a Consultant Addiction Psychiatrist. She works in a drug and alcohol clinic which treats clients from an area of London with
The science of the mind: investigating mental health Treating addiction : is a Consultant Addiction Psychiatrist. She works in a drug and alcohol clinic which treats clients from an area of London with
Opioid dependence and buprenorphine treatment
 Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
Medication Assisted Treatment
 Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations
 Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Talking with your doctor
 SUBOXONE (buprenorphine and naloxone) Sublingual Film (CIII) Talking with your doctor Opioid dependence can be treated. Talking with your healthcare team keeps them aware of your situation so they may
SUBOXONE (buprenorphine and naloxone) Sublingual Film (CIII) Talking with your doctor Opioid dependence can be treated. Talking with your healthcare team keeps them aware of your situation so they may
Medication Assisted Treatment:
 Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
The Social Worker s Role in Medication Assisted Treatment
 The Social Worker s Role in Medication Assisted Treatment Rocky Ephraim Lucas, LICSW Behavioral Health Consultant, Kanawha City Health Center (Cabin Creek Health Systems) What is Medication-Assisted Treatment
The Social Worker s Role in Medication Assisted Treatment Rocky Ephraim Lucas, LICSW Behavioral Health Consultant, Kanawha City Health Center (Cabin Creek Health Systems) What is Medication-Assisted Treatment
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings
 Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets. Risk Evaluation and Mitigation Strategy (REMS) Program
 Program") SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine. March 10, 2016
 The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine March 10, 2016 Objectives Review current state of opioid crisis in Maine Briefly review physiology of
The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine March 10, 2016 Objectives Review current state of opioid crisis in Maine Briefly review physiology of
7/7/2016 Journal of the American Medical Association,
 1 2 Journal of the American Medical Association, 2008 3 The Clinical Trial 152 Adolescents and Young Adults (Age 15 to 21) randomly assigned to either; 1. 2 weeks of Buprenorphine detox 2. 12 weeks of
1 2 Journal of the American Medical Association, 2008 3 The Clinical Trial 152 Adolescents and Young Adults (Age 15 to 21) randomly assigned to either; 1. 2 weeks of Buprenorphine detox 2. 12 weeks of
Optimizing Suboxone in Opioid Addicts
 Optimizing Suboxone in Opioid Addicts David Chim, D.O. Integrated Substance Abuse Programs Dept. of Psychiatry, UCLA K30 Translational Research Interest March 24, 2009 dchim@mednet.ucla.edu www.uclaisap.org
Optimizing Suboxone in Opioid Addicts David Chim, D.O. Integrated Substance Abuse Programs Dept. of Psychiatry, UCLA K30 Translational Research Interest March 24, 2009 dchim@mednet.ucla.edu www.uclaisap.org
ROSC & MAT II: Opioid Treatment Services
 ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
The CARA & Buprenorphine Prescribing for APNs & PAs
 The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
Medication Assisted Treatment. MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment
 Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
What Is Heroin? Examples of Opioids. What Science Says about Opioid Use Disorder and Its Treatment 6/27/2016
 What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
NALTREXONE DAVID CRABTREE, MD, MPH UNIVERSITY OF UTAH HEALTH, 2018
 NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc.
 Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc. Elements Behavioral Health Diplomate, American Board of Addiction
Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc. Elements Behavioral Health Diplomate, American Board of Addiction
Identification and Treatment of Opioid Use Disorders in Primary Care Settings
 Identification and Treatment of Opioid Use Disorders in Primary Care Settings 17th Annual Primary Care Symposium February 24, 2018 Kelly S. Barth, DO Associate Professor, Psychiatry & Internal Medicine
Identification and Treatment of Opioid Use Disorders in Primary Care Settings 17th Annual Primary Care Symposium February 24, 2018 Kelly S. Barth, DO Associate Professor, Psychiatry & Internal Medicine
Earl Hightower's Remarks 2014 National Rx Drug Abuse Summit Medication Assisted Treatment for Opiate Addiction
 Earl Hightower's Remarks 2014 National Rx Drug Abuse Summit Medication Assisted Treatment for Opiate Addiction Thank you, Chairman Rogers, for holding this important Summit and helping to bring attention
Earl Hightower's Remarks 2014 National Rx Drug Abuse Summit Medication Assisted Treatment for Opiate Addiction Thank you, Chairman Rogers, for holding this important Summit and helping to bring attention
Medication for Addiction Treatment (MAT)
") SBIRT Training Screening, Brief Intervention & Referral to Treatment Medication for Addiction Treatment (MAT) The Faith & Spirituality Integrated SBIRT Network Navigating the Training Welcome! These health
SBIRT Training Screening, Brief Intervention & Referral to Treatment Medication for Addiction Treatment (MAT) The Faith & Spirituality Integrated SBIRT Network Navigating the Training Welcome! These health
GOALS AND OBJECTIVES
 SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
Buprenorphine pharmacology
 Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Methadone Maintenance 101
 Methadone Maintenance 101 OTP/DAILY DOSING CLINICS - ANDREW PUTNEY MD Conflicts of Interest - Employed by Acadia HealthCare 1 Why Methadone? At adequate doses methadone decreases opioid withdrawal symptoms
Methadone Maintenance 101 OTP/DAILY DOSING CLINICS - ANDREW PUTNEY MD Conflicts of Interest - Employed by Acadia HealthCare 1 Why Methadone? At adequate doses methadone decreases opioid withdrawal symptoms
Opioid Use Disorders &Medication Treatment
 Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Opioid Agonists. Natural derivatives of opium poppy - Opium - Morphine - Codeine
 Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine 2.0: I have my waiver, now what? Dr. Ritu Bhatnagar, M.D., M.P.H. Dr. John Ewing, M.D., FASAM. Disclosures
 Buprenorphine 2.0: I have my waiver, now what? Dr. Ritu Bhatnagar, M.D., M.P.H. Dr. John Ewing, M.D., FASAM Disclosures Dr. Bhatnagar: no disclosures to report Dr. Ewing: no disclosures to report 1 Our
Buprenorphine 2.0: I have my waiver, now what? Dr. Ritu Bhatnagar, M.D., M.P.H. Dr. John Ewing, M.D., FASAM Disclosures Dr. Bhatnagar: no disclosures to report Dr. Ewing: no disclosures to report 1 Our
Building capacity for a CHC response to Ontario's Opioid Crisis
 Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
HARM REDUCTION & TREATMENT. Devin Reaves MSW
 HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone
 Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone Alexander Y. Walley, MD, MSc Associate Professor of Medicine Director, Addiction Medicine Fellowship Boston University
Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone Alexander Y. Walley, MD, MSc Associate Professor of Medicine Director, Addiction Medicine Fellowship Boston University
Treating Opioid Addiction
 Treating Opioid Addiction Some people who start taking opioid pain medications eventually have serious problems with them and become addicted. Every day, 68 people die in the US from opioid overdose. More
Treating Opioid Addiction Some people who start taking opioid pain medications eventually have serious problems with them and become addicted. Every day, 68 people die in the US from opioid overdose. More
The Rising Tide of Prescription Opioid Use Disorders and Current Treatment Options
 The Rising Tide of Prescription Opioid Use Disorders and Current Treatment Options Michelle R. Lofwall, MD UK Dept of Psychiatry November 4, 2008 Outline for Today s Talk Past & current state of affairs
The Rising Tide of Prescription Opioid Use Disorders and Current Treatment Options Michelle R. Lofwall, MD UK Dept of Psychiatry November 4, 2008 Outline for Today s Talk Past & current state of affairs
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT
 and acute pain management on MAT") An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
Medication Assisted Treatment. Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs
 Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Medication Assisted Treatment of an Opioid Use Disorder. J. Craig Allen, MD. Medical Director, Rushford
 Medication Assisted Treatment of an Opioid Use Disorder J. Craig Allen, MD. Medical Director, Rushford Learning objectives At the conclusion of this activity, participants will be able to: Understand
Medication Assisted Treatment of an Opioid Use Disorder J. Craig Allen, MD. Medical Director, Rushford Learning objectives At the conclusion of this activity, participants will be able to: Understand
Understanding and Combating the Heroin Epidemic
 Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
Prescription Opioid Addiction
 CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
Medical Assisted Treatment of Opioid
 Medical Assisted Treatment of Opioid Dependence with XR-NTX(Vivitrol) Michael McNamara DO, FACN Medical Director Mental Health Center of Greater Manchester Manchester NH Outline Overview of Opioid Dependence
Medical Assisted Treatment of Opioid Dependence with XR-NTX(Vivitrol) Michael McNamara DO, FACN Medical Director Mental Health Center of Greater Manchester Manchester NH Outline Overview of Opioid Dependence
Addiction to Opioids. Marvin D. Seppala, MD Chief Medical Officer
 Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE
 Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
9/13/2017. Buprenorphine Treatment (Suboxone) Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare
 Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare") Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Opioids. October 29, Addiction Medicine Review Course CSAM, Newport Beach, CA
 Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
2/21/2018. What are Opioids?
 Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI)
") OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI) Case 105- Prep Materials University of Massachusetts Medical School Opioid Conscious Curriculum Learner Prep Objectives The purpose of this prep material
OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI) Case 105- Prep Materials University of Massachusetts Medical School Opioid Conscious Curriculum Learner Prep Objectives The purpose of this prep material
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT)
") Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) What has changed? Effective January 16, 2018, Coordinated Care will change the requirement for form HCA 13-333 Medication
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) What has changed? Effective January 16, 2018, Coordinated Care will change the requirement for form HCA 13-333 Medication
Safe Practices and Action Items
 Safe Practices and Action Items Karen F Marlowe, Pharm D, BCPS Certified Pain Educator Auburn University Harrison School of Pharmacy University of South Alabama School of Medicine Case Study A 58 year
Safe Practices and Action Items Karen F Marlowe, Pharm D, BCPS Certified Pain Educator Auburn University Harrison School of Pharmacy University of South Alabama School of Medicine Case Study A 58 year
Buprenorphine is the most effective office-based treatment available for heroin and prescription opioid addiction
 Buprenorphine is the most effective office-based treatment available for heroin and prescription opioid addiction The Problem The overdose death rate in Missouri and in the country has been rising for
Buprenorphine is the most effective office-based treatment available for heroin and prescription opioid addiction The Problem The overdose death rate in Missouri and in the country has been rising for
Opioid Use Disorders as a Brain Disease Why MAT is so important. Ron Jackson, M.S.W., L.I.C.S.W.
 Opioid Use Disorders as a Brain Disease Why MAT is so important Ron Jackson, M.S.W., L.I.C.S.W. Affiliate Professor School of Social Work University of Washington Organization Name: CareOregon Course Title:
Opioid Use Disorders as a Brain Disease Why MAT is so important Ron Jackson, M.S.W., L.I.C.S.W. Affiliate Professor School of Social Work University of Washington Organization Name: CareOregon Course Title:
4/5/2018 MEDICATION ASSISTED TREATMENT FOR OPIOID USE DISORDERS OBJECTIVES DEFINITION OF ADDICTION APRIL 11, 2018 RITU BHATNAGAR, M.D., M.P.H.
 MEDICATION ASSISTED TREATMENT FOR OPIOID USE DISORDERS APRIL 11, 2018 RITU BHATNAGAR, M.D., M.P.H. MEDICAL DIRECTOR, UNITYPOINT HEALTH MERITER/ NEWSTART ADJUNCT PROFESSOR, UNIVERSITY OF WISCONSIN MADISON
MEDICATION ASSISTED TREATMENT FOR OPIOID USE DISORDERS APRIL 11, 2018 RITU BHATNAGAR, M.D., M.P.H. MEDICAL DIRECTOR, UNITYPOINT HEALTH MERITER/ NEWSTART ADJUNCT PROFESSOR, UNIVERSITY OF WISCONSIN MADISON
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT)
") Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) For Apple Health clients served Fee-for-Service and through contracted Medicaid Managed Care Organizations Updated January
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) For Apple Health clients served Fee-for-Service and through contracted Medicaid Managed Care Organizations Updated January
Overview of Opioid Use Disorder
 Overview of Opioid Use Disorder Doug Burgess, MD Medical Director of Outpatient Services, Truman Medical Centers Assistant Professor of Psychiatry, University of Missouri- Kansas City Objectives History
Overview of Opioid Use Disorder Doug Burgess, MD Medical Director of Outpatient Services, Truman Medical Centers Assistant Professor of Psychiatry, University of Missouri- Kansas City Objectives History
Opioid Treatment in North Carolina SEPTEMBER 13, 2016
 Opioid Treatment in North Carolina SEPTEMBER 13, 2016 Source Where Pain Relievers Were Obtained for Most Recent Nonmedical Use among Past Year Users Aged 12 or Older: 2007 Source Where Respondent Obtained
Opioid Treatment in North Carolina SEPTEMBER 13, 2016 Source Where Pain Relievers Were Obtained for Most Recent Nonmedical Use among Past Year Users Aged 12 or Older: 2007 Source Where Respondent Obtained
Pennsylvania Coordinated Medication Assisted Treatment: A Penn State and Pennsylvania Psychiatric Institute Story
 Pennsylvania Coordinated Medication Assisted Treatment: A Penn State and Pennsylvania Psychiatric Institute Story Sarah Sharfstein Kawasaki, MD Director of Addictions Services, Pennsylvania Psychiatric
Pennsylvania Coordinated Medication Assisted Treatment: A Penn State and Pennsylvania Psychiatric Institute Story Sarah Sharfstein Kawasaki, MD Director of Addictions Services, Pennsylvania Psychiatric
Prepublication Requirements
 Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
MAT - ICAAD 2018 Ron Jackson, MSW, LICSW
 The ATTC Network Ten Regional Centers northwest@attcnetwork.org www.attcnetwork.org/northwest phone. 206-685-4419 1107 NE 45 th St, Ste 120, Seattle, WA 98105 http://attcnetwork.org/northwest U.S. Opioid
The ATTC Network Ten Regional Centers northwest@attcnetwork.org www.attcnetwork.org/northwest phone. 206-685-4419 1107 NE 45 th St, Ste 120, Seattle, WA 98105 http://attcnetwork.org/northwest U.S. Opioid
Vivitrol/Suboxone. Comparison Study Summary
 Vivitrol/Suboxone Comparison Study Summary Lee, J. D., Nunes, E. V., Novo, P., Bachrach, K., Bailey, G. L., Bhatt, S., & King, J. (2017). Comparative effectiveness of extended-release naltrexone versus
Vivitrol/Suboxone Comparison Study Summary Lee, J. D., Nunes, E. V., Novo, P., Bachrach, K., Bailey, G. L., Bhatt, S., & King, J. (2017). Comparative effectiveness of extended-release naltrexone versus
Addiction Medicine: What s new for primary care
 Addiction Medicine: What s new for primary care Dan Vinson, MD Family and Community Medicine How to talk so our patients listen, and listen so our patients talk. 1 2 Comfortably engaging your patient in
Addiction Medicine: What s new for primary care Dan Vinson, MD Family and Community Medicine How to talk so our patients listen, and listen so our patients talk. 1 2 Comfortably engaging your patient in
Discover the Hope: Opiate Treatment and Recovery
 Discover the Hope: Opiate Treatment and Recovery The Continued Struggle to Find and Implement Best Practices Ted Parran JR. M.D. FACP Carter and Isabel Wang Professor of Medical Education CWRU School of
Discover the Hope: Opiate Treatment and Recovery The Continued Struggle to Find and Implement Best Practices Ted Parran JR. M.D. FACP Carter and Isabel Wang Professor of Medical Education CWRU School of
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION
 SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION Naltrexone is used as part of a comprehensive programme of treatment against alcoholism to reduce the
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION Naltrexone is used as part of a comprehensive programme of treatment against alcoholism to reduce the
Opioid Use Disorder Treatment: Buprenorphine Treatment Basics
 Opioid Use Disorder Treatment: Buprenorphine Treatment Basics Daniel Warren, MD Eastern Oregon Coordinated Care Organization Provider Forum on Chronic Noncancer Pain Management Pendleton, OR February 24,
Opioid Use Disorder Treatment: Buprenorphine Treatment Basics Daniel Warren, MD Eastern Oregon Coordinated Care Organization Provider Forum on Chronic Noncancer Pain Management Pendleton, OR February 24,
Management Options for Opioid Dependence:
 Management Options for Opioid Dependence: Policy Implications and Recommendations Dan Ollendorf, PhD Sarah Jane Reed, MSc New England CEPAC Goal: To improve the application of evidence to guide practice
Management Options for Opioid Dependence: Policy Implications and Recommendations Dan Ollendorf, PhD Sarah Jane Reed, MSc New England CEPAC Goal: To improve the application of evidence to guide practice
SUBOXONE TREATMENT PROGRAM
 SUBOXONE TREATMENT PROGRAM What is Suboxone? Suboxone is a medication used for the treatment of addiction to prescription pain medication, heroin addiction, methadone or other opioid dependence. The primary
SUBOXONE TREATMENT PROGRAM What is Suboxone? Suboxone is a medication used for the treatment of addiction to prescription pain medication, heroin addiction, methadone or other opioid dependence. The primary
Anyone Can Become Addicted. Anyone.
 Anyone Can Become Addicted. Anyone. PAStop.org Family Toolkit Seeking Drug Abuse Treatment: Know What to Ask Trying to identify the right treatment programs for a loved one can be a difficult process.
Anyone Can Become Addicted. Anyone. PAStop.org Family Toolkit Seeking Drug Abuse Treatment: Know What to Ask Trying to identify the right treatment programs for a loved one can be a difficult process.
Latest Research on Addiction and Treatment
 Latest Research on Addiction and Treatment Joshua D Lee MD MSc joshua.lee@nyumc.org / @DrJoshuaDLee Associate Professor NYU School of Medicine, Department of Population Health Disclosures, LeeJD Grants:
Latest Research on Addiction and Treatment Joshua D Lee MD MSc joshua.lee@nyumc.org / @DrJoshuaDLee Associate Professor NYU School of Medicine, Department of Population Health Disclosures, LeeJD Grants:
MAT 101: TREATMENT OF OPIOID USE DISORDER
 MAT 101: TREATMENT OF OPIOID USE DISORDER WITH SPECIAL EMPHASIS ON BUPRENORPHINE/NALOXONE ICADD May 22, 2018 Alicia Carrasco, MD Debby Woodall, LCSW, ACADC Magni Hamso, MD, MPH Terry Reilly Health Services
MAT 101: TREATMENT OF OPIOID USE DISORDER WITH SPECIAL EMPHASIS ON BUPRENORPHINE/NALOXONE ICADD May 22, 2018 Alicia Carrasco, MD Debby Woodall, LCSW, ACADC Magni Hamso, MD, MPH Terry Reilly Health Services