NALTREXONE DAVID CRABTREE, MD, MPH UNIVERSITY OF UTAH HEALTH, 2018
|
|
|
- Darleen Crawford
- 5 years ago
- Views:
Transcription

1 NALTREXONE DAVID CRABTREE, MD, MPH
2 TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications (MAT), despite overwhelming evidence of superior outcomes as compared to psychosocial treatment approach All patients should be offered option to be treated with one of the FDA-approved medications, preferably matched to the patient to assure optimal outcome
3 NALTREXONE Antagonist - ligand that binds to the receptor but does not initiate signal transduction Naltrexone & Naloxone act as u-or antagonists Naltrexone binds with the highest affinity of all ligands It will displace all agonists from the receptor It will prevent all agonists from exerting effects At sufficient blood levels, naltrexone fully blocks all opioid effects*
4 NALTREXONE Long acting, high affinity, competitive opioid receptor antagonist with an active metabolite (6-B-naltrexol, also antagonist) Tablet is approved for the blockade of exogenously administered opioids Injection (Extended release) is approved for the prevention of relapse to opioid dependence following opioid detoxification (package insert) May be a good choice for patients seeking withdrawal from all opioids as a first stage of treatment
5 COMPONENTS OF TREATMENT WITH NALTREXONE Behavioral component: blockade of the positive reinforcing effects of opioids leads to gradual extinction of craving and compulsive drug use Patients who use opioids while taking naltrexone experience no euphoric effect and usually stop using opioids Pharmacological component: naltrexone decreases reactivity to drug conditioned cues thereby minimizing pathological responses contributing to relapse (craving) Patients with a good clinical response to naltrexone usually have no urges to use As naltrexone has a different mechanism of action than agonists, it may address limitations related to treatment with agonists, providing another option for patients with OUD
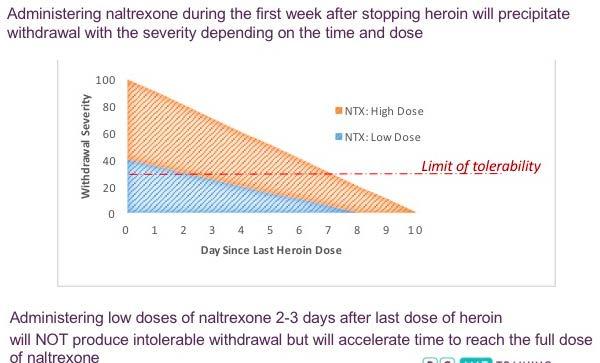
6 LIMITATIONS Requirement of detoxification and a wait period of 7-10 days after the last dose of an opioid before antagonist can be initiated A major barrier for many patients who find difficult to tolerate withdrawal and abstain from opioids Difficulty with the induction due to the possibility of precipitated and protracted withdrawal Patients do not feel well at the beginning of the treatment Requirement of close monitoring XR preparation of naltrexone is a relatively new medication with limited effectiveness research to date
7 BRIEF HISTORY OF NALTREXONE-BASED TREATMENT First introduced in the 1970s (PO)...disappointing results Difficulty with tx initiation, low patient acceptability and poor adherence Reviews concluded that there was no evidence that naltrexone is effective beyond selected patient groups, which discouraged its use New developments in the 1980s Clonidine effective in tx withdrawal Development of naltrexone-assisted withdrawal management protocols Buprenorphine was introduced for withdrawal management which facilitated naltrexone induction
8 BRIEF HISTORY The 1990s-2000s Using antagonists during withdrawal management became an opportunity to continue with naltrexone as a relapse prevention agent Behavioral therapy was developed to improve adherence to oral naltrexone, including elements of MI/CBT/etc Long-acting preparations became available to address non-adherence to PO
9 EFFICACY OF NALTREXONE: PO VS XR INJECTION Retention in treatment rate = 1 outcome Main reason for dropout is relapse Majority retained in treatment are abstinent from opioids Rate in groups tx d with XR preparations is twice that of the PO group, appx 50-70% at 6 months
10 XR VS PLACEBO Trials comparing injection of naltrexone vs placebo showed that patients receiving naltrexone have: Better retention Less opioid use Lower craving of opioids
11 EFFECT OF NALTREXONE: SUMMARY XR preparations of naltrexone are more effective than the PO preparation and should be offered over the oral formulation Adherence is a challenge, but it is better with XR preparation Treatment must emphasize adherence Better treatment retention, lower opioid use, and lower craving as compared to placebo Those retained with XR have low levels of concurrent opioid use No direct evidence yet available comparing efficacy of XR naltrexone vs buprenorphine Indirect comparisons show comparable retention with lower level of ongoing opioid use
12 GOOD CANDIDATES FOR NALTREXONE Patients who are not interested or able to be on agonist med Highly motivated for abstinence from all opioids In professions where treatment w/ agonist med is controversial (health care, pilots, etc) Patients who are abstinent from opioids but remain at risk for relapse Released from a controlled setting (prison, residential program) Moving back to neighborhood w/ greater exposure to drugs Patients who failed prior treatment w/ agonist Continued cravings and use of illicit opioids, non-adherence w/ agonist med, diverting/misusing agonists
13 CONTINUED Less severe forms of OUD Young adults living with involved parents who can supervise tx Young adults unwilling to commit to longer-term agonist therapy Individuals who use opioids sporadically and are at risk or progression to daily use Patients successful on agonist therapy who wish to DC med and seek alternative tx
14 PATIENT-TREATMENT MATCHING No evidence, only clinical experience Good response to PO Naltrexone: Highly motivated pt Older pt w/ long hx of use and multiple relapses Pt w/ long periods of abstinence between relapses
15 IS THE PATIENT READY? Naltrexone WILL precipitate severe and prolonged withdrawal in those who are physically dependent on opioids or have large amount of opioids in their system Always confirm absence of opioids and physical dependence prior to the first dose UDS must be negative for all opioids, but remember not all opioids will be detected (Kratom, loperamiide) Naloxone challenge if unsure of the abstinence and the absence of physiological dependence Patient must understand the risks of precipitated withdrawal if underreporting
16 INITIATING XR-NALTREXONE Give immediately after confirming absence of physical dependence or passing the challenge May give PO challenge ( mg x1) at least 1-2 hours before the injection, to ensure tolerability Alternatively, may do this for a few days, then inject Residential setting Give XR ASAP to minimize risks of non-adherence to PO
17 NALOXONE CHALLENGE Short acting opioid antagonist used to reverse overdose AND to detect physiological dependence Will precipitate withdrawal that usually emerges within 5-10 min and dissipates within 30 min COWS to measure withdrawal Severity of withdrawal proportional to the level of physical dependence and dose of naloxone Any change from baseline = Positive test (wait a day, repeat) Naloxone IM (deltoid) 2 stages to minimize withdrawal: 0.4 mg then 0.8 mg Negative test full dose naltrexone can be started
18 INDUCTION: CLINICAL SCENARIOS Abstinent, after opioid withdrawal XR most easily started this way Not in acute withdrawal, no use of opioids for 7+ days Confirm absence of opioids and physical dependence Administer injection Sporadic use of opioids Individuals who started using after a period of abstinence, high risk intermittent users of opioids Require 2-3 days of abstinence and confirm absence of physical dependence Neg UDS and neg naloxone challenge Administer injection
19 INDUCTION: CLINICAL SCENARIOS Use of daily low amounts Misuse of opioids in the context of pain-treatment (<100 MME) Low amount of heroin (1-3 bags/day) Must complete withdrawal (outpatient w/ daily visits) Confirm absence of physical dependence (neg Utox, neg challenge) Administer injection
20 INDUCTION: CLINICAL SCENARIOS Use of daily large amounts Short or long acting, IN or IV >5 bags heroin, oxycodone, fentanyl, methadone Often use of other substances (etoh, sedatives, simulants) Consider agonist as a first line tx If patient wants naltrexone, consider inpatient withdrawal management (10-14 days) Confirm absence of physical dependence (neg Utox, neg challenge) Administer injection BEFORE discharge
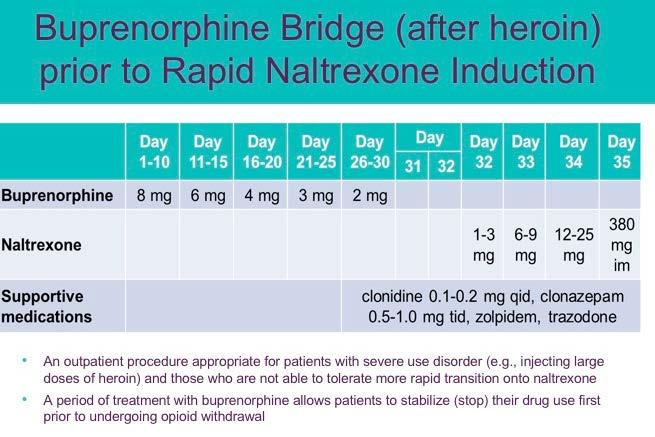
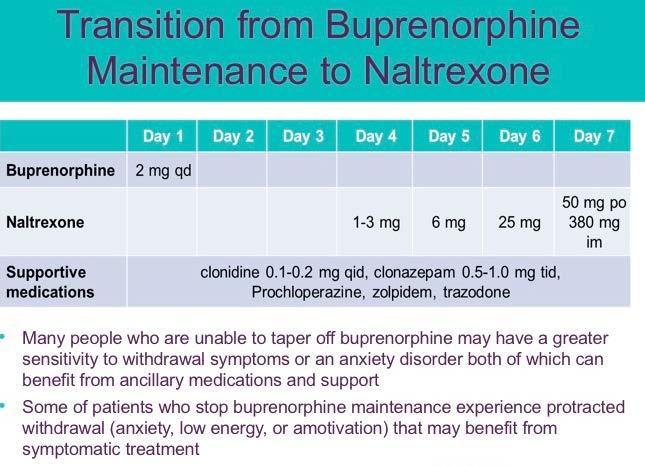
21 THE PATIENT DISCONTINUING METHADONE OR BUPRENORPHINE Those maintained with good response may be considered for transition onto naltrexone Patient should be able to tolerate gradual agonist dose reduction Those on methadone should go onto buprenorphine All should remain stable on buprenorphine 2-4 mg for at least one month before discontinuation Use adjuncts after stopping buprenorphine to alleviate withdrawal Initiate w/ PO followed by XR injection Waiting for neg Utox (bup) is not necessary if starting low naltrexone dose
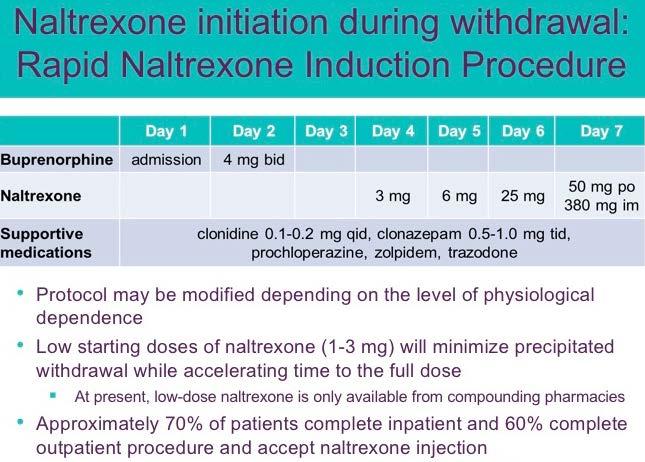
22 OPIOID WITHDRAWAL Approaches, not to be discussed in detail Agonist assisted opioid withdrawal Symptomatic only care Rapid withdrawal using antagonist Naltrexone added 2-3 days after the last dose, start low (3-6 mg), use adjuncts to minimize discomfort Ultra Rapid withdrawal under anesthesia
23
24
25
26
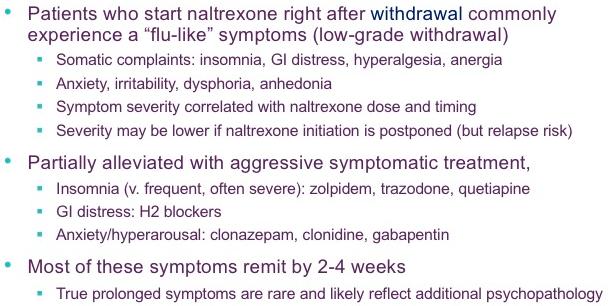
27 NALTREXONE FLU
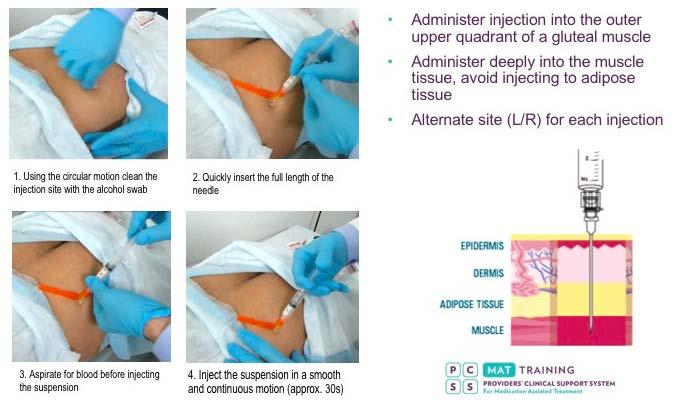
28 SIDE EFFECTS Infrequent, first month, related to withdrawal Nausea, Tiredness, Headache, Dizziness, Vomiting, Decreased Appetite, Painful Joints, Muscle Cramps, Insomnia Injection Site Reactions (inflammation, Tissue Damage) Local tenderness, small bump is common, resolves 1-3 days Serious Site Reaction If Administered Into FAT TISSUE Rare Depressed mood, suicidal behavior Allergic Eosinophilic Pneumonitis Systemic Allergic Reaction

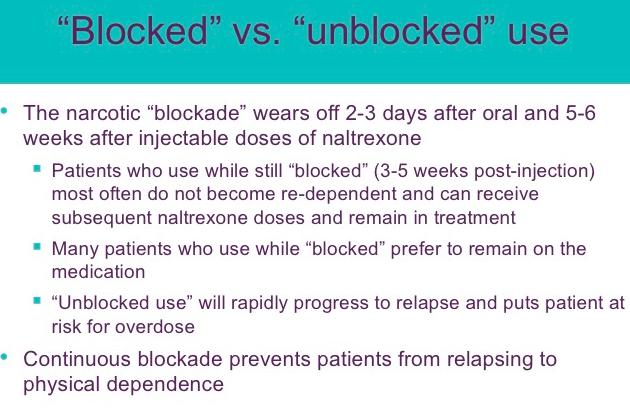
29 CLINICAL CHALLENGES: TESTING THE BLOCKADE
30
31
32

33
34
35
36
37
38
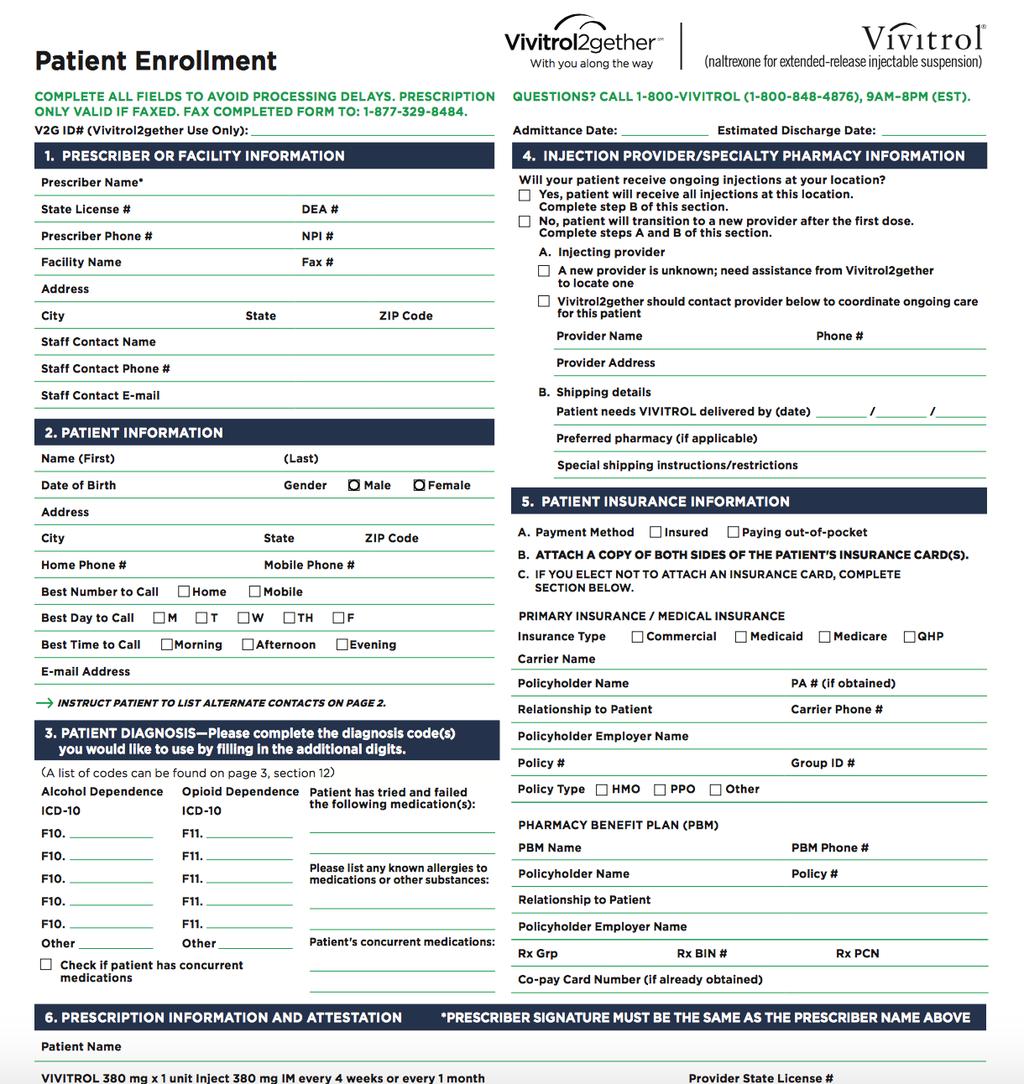
39 INJECTABLE NALTREXONE PRIOR AUTHORIZATION Or Google touchpoints Vivitrol Make sure patient signs consent and opts for co-pay assistance You choose diagnosis and choose length of prescription Fax the form in, expect 2-4 weeks for approval
40
41 REFERENCES
Long term treatment for opioid dependence Antagonist therapy
 Long term treatment for opioid dependence Antagonist therapy Treatment of Opioid Dependence Antagonist treatment Naltrexone Naltrexone (NTX) synthesized in 1965 Eliminate drug carving and prevent relapse
Long term treatment for opioid dependence Antagonist therapy Treatment of Opioid Dependence Antagonist treatment Naltrexone Naltrexone (NTX) synthesized in 1965 Eliminate drug carving and prevent relapse
Medical Assisted Treatment of Opioid
 Medical Assisted Treatment of Opioid Dependence with XR-NTX(Vivitrol) Michael McNamara DO, FACN Medical Director Mental Health Center of Greater Manchester Manchester NH Outline Overview of Opioid Dependence
Medical Assisted Treatment of Opioid Dependence with XR-NTX(Vivitrol) Michael McNamara DO, FACN Medical Director Mental Health Center of Greater Manchester Manchester NH Outline Overview of Opioid Dependence
Methadone and Naltrexone ER
 Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations
 Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Methadone and Naltrexone ER
 Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Objectives Review Full Opioid
Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Objectives Review Full Opioid
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE
 LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
Buprenorphine pharmacology
 Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Buprenorphine as a Treatment Option for Opioid Use Disorder
 Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Opioid Use Disorders &Medication Treatment
 Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
SW OREGON OPIOID SUMMIT. Medication Assisted Recovery for Opioid Use Disorder. Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass
 SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
Guidance for naltrexone prescribing
 Document level: Drug Alcohol (Trustwide) Code: DA7 Issue number: 2 Guidance for naltrexone prescribing Lead executive Authors details Type of document Target audience Document purpose Lead Clinical Director
Document level: Drug Alcohol (Trustwide) Code: DA7 Issue number: 2 Guidance for naltrexone prescribing Lead executive Authors details Type of document Target audience Document purpose Lead Clinical Director
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Building capacity for a CHC response to Ontario's Opioid Crisis
 Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of Opioid Dependence Abbreviated Version
 Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of Opioid Dependence Abbreviated Version Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of
Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of Opioid Dependence Abbreviated Version Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Clinical Guidelines for the Pharmacologic Treatment of Opioid Use Disorder
 Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Prescribing Framework for Naltrexone in Relapse Prevention (Opioid Dependence)
") Hull & East Riding Prescribing Committee Prescribing Framework for Naltrexone in Relapse Prevention (Opioid Dependence) Patients Name: Unit Number: Patients Address:.. G.P s Name:.. Communication We agree
Hull & East Riding Prescribing Committee Prescribing Framework for Naltrexone in Relapse Prevention (Opioid Dependence) Patients Name: Unit Number: Patients Address:.. G.P s Name:.. Communication We agree
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
METHADONE TO BUPRENORPHINE TRANSFERS TRANSITIONING FROM METHADONE MAINTENANCE TO BUPRENORPHINE/NALOXONE
 METHADONE TO BUPRENORPHINE TRANSFERS TRANSITIONING FROM METHADONE MAINTENANCE TO BUPRENORPHINE/NALOXONE Work with methadone clinic staff to coordinate the methadone taper, with the transition to buprenorphine/naloxone:
METHADONE TO BUPRENORPHINE TRANSFERS TRANSITIONING FROM METHADONE MAINTENANCE TO BUPRENORPHINE/NALOXONE Work with methadone clinic staff to coordinate the methadone taper, with the transition to buprenorphine/naloxone:
Medication-Assisted Treatment (MAT) Overview
 Overview") Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
GOALS AND OBJECTIVES
 SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioid dependence: Detoxification
 Opioid dependence: Detoxification What is detoxification? A. Process of removal of toxins from the body? B. Admitting a drug dependent person in a hospital and giving him nutrition? C. Stopping drug use
Opioid dependence: Detoxification What is detoxification? A. Process of removal of toxins from the body? B. Admitting a drug dependent person in a hospital and giving him nutrition? C. Stopping drug use
Agenda. 1 Opioid Addiction in the United States. Evidence-based treatments for OUD. OUD Treatment: Best Practices. 4 Groups: Our Model
 Agenda 1 Opioid Addiction in the United States 2 Evidence-based treatments for OUD OUD Treatment: Best Practices 4 Groups: Our Model 2 Groups is a national network of clinics providing affordable, evidencebased
Agenda 1 Opioid Addiction in the United States 2 Evidence-based treatments for OUD OUD Treatment: Best Practices 4 Groups: Our Model 2 Groups is a national network of clinics providing affordable, evidencebased
Opioids Research to Practice
 Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine
 [Patient-focused, evidence-based addiction treatment] Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine BrightView Health All Rights Reserved www.brightviewhealth.com
[Patient-focused, evidence-based addiction treatment] Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine BrightView Health All Rights Reserved www.brightviewhealth.com
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opioid Agonists. Natural derivatives of opium poppy - Opium - Morphine - Codeine
 Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Addiction to Opioids. Marvin D. Seppala, MD Chief Medical Officer
 Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
ROSC & MAT II: Opioid Treatment Services
 ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
MEDICATION ASSISTED TREATMENT
 MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
Hospitals Role in Addressing the Opioid Crisis
 Hospitals Role in Addressing the Opioid Crisis Webinar 5: Buprenorphine in the Emergency Department November 14, 2017 Agenda Hospital Based Buprenorphine Initiatives Yngvild Olsen, M.D., Medical Consultant,
Hospitals Role in Addressing the Opioid Crisis Webinar 5: Buprenorphine in the Emergency Department November 14, 2017 Agenda Hospital Based Buprenorphine Initiatives Yngvild Olsen, M.D., Medical Consultant,
6/6/2018. Objectives. Outline. Rethinking Medication Treatment for Opioid Use Disorder
 Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
Opioids Research to Practice
 Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
OAT Transitions - focus on microdosing. Mark McLean MD MSc FRCPC CISAM DABAM
 OAT Transitions - focus on microdosing Mark McLean MD MSc FRCPC CISAM DABAM Disclosures No pharmaceutical industry or other financial conflicts of interest Study Physician for research funded by Canadian
OAT Transitions - focus on microdosing Mark McLean MD MSc FRCPC CISAM DABAM Disclosures No pharmaceutical industry or other financial conflicts of interest Study Physician for research funded by Canadian
Opioid Use in Youth. Amy Yule M.D. March 2,
 Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
Naltrexone Overview. Todd Korthuis, MD, MPH ECHO-MAT Conference February 14, 2017
 Naltrexone Overview Todd Korthuis, MD, MPH ECHO-MAT Conference February 14, 2017 Pharmacotherapy for Opioid Use Disorder % Mu Receptor Intrinsic Activity 100 90 80 Full Agonist: Methadone ( How High )
Naltrexone Overview Todd Korthuis, MD, MPH ECHO-MAT Conference February 14, 2017 Pharmacotherapy for Opioid Use Disorder % Mu Receptor Intrinsic Activity 100 90 80 Full Agonist: Methadone ( How High )
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines
 The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
Opioid dependence and buprenorphine treatment
 Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
Mary Ann Ferguson,Pharmacist St Josephs Health Care Concurrent Disorders Inpatient Unit
 Mary Ann Ferguson,Pharmacist St Josephs Health Care Concurrent Disorders Inpatient Unit Fergusom@stjoes.ca Medication should be considered as part of the treatment plan for addictions/substance use disorders:
Mary Ann Ferguson,Pharmacist St Josephs Health Care Concurrent Disorders Inpatient Unit Fergusom@stjoes.ca Medication should be considered as part of the treatment plan for addictions/substance use disorders:
Prescription Opioid Addiction
 CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
VIVITROL (naltrexone for extended-release injectable suspension) A µ-opioid Receptor Antagonist
 A µ-opioid Receptor Antagonist") MECHANISM OF ACTION VIVITROL (naltrexone for extended-release injectable suspension) A µ-opioid Receptor Antagonist VIVITROL is indicated for prevention of relapse to opioid dependence, following opioid
MECHANISM OF ACTION VIVITROL (naltrexone for extended-release injectable suspension) A µ-opioid Receptor Antagonist VIVITROL is indicated for prevention of relapse to opioid dependence, following opioid
6/8/2018. Primary Care Providers Can Treat Opioid Use Disorder and Help End the Epidemic. Disclosures. Outline
 Primary Care Providers Can Treat Opioid Use Disorder and Help End the Epidemic Adam Bisaga M.D. Division on Substance Use Disorders, Department of Psychiatry New York State Psychiatric Institute, New York,
Primary Care Providers Can Treat Opioid Use Disorder and Help End the Epidemic Adam Bisaga M.D. Division on Substance Use Disorders, Department of Psychiatry New York State Psychiatric Institute, New York,
Opioids. October 29, Addiction Medicine Review Course CSAM, Newport Beach, CA
 Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
Vivitrol Vs. Suboxone
 Vivitrol Vs. Suboxone Vivitrol - Naltrexone Indicated for opiate dependence and alcohol withdrawal pure antagonist 380mg once every 4 weeks IM Peak plasma concentration in 2 hrs, followed by a second peak
Vivitrol Vs. Suboxone Vivitrol - Naltrexone Indicated for opiate dependence and alcohol withdrawal pure antagonist 380mg once every 4 weeks IM Peak plasma concentration in 2 hrs, followed by a second peak
EXTENDED-NALTREXONE for the Treatment of OPIOID USE DISORDER:
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences EXTENDED-NALTREXONE for the Treatment of OPIOID USE DISORDER: September 13, 2018 Matt Iles-Shih, MD Acknowledgement:
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences EXTENDED-NALTREXONE for the Treatment of OPIOID USE DISORDER: September 13, 2018 Matt Iles-Shih, MD Acknowledgement:
Overview of Opioid Use Disorder
 Overview of Opioid Use Disorder Doug Burgess, MD Medical Director of Outpatient Services, Truman Medical Centers Assistant Professor of Psychiatry, University of Missouri- Kansas City Objectives History
Overview of Opioid Use Disorder Doug Burgess, MD Medical Director of Outpatient Services, Truman Medical Centers Assistant Professor of Psychiatry, University of Missouri- Kansas City Objectives History
WHEN & HOW TO GET STARTED
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences XR-NALTREXONE for the Treatment of OPIOID USE DISORDER: WHEN & HOW TO GET STARTED Matt Iles-Shih, MD Acting Assistant
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences XR-NALTREXONE for the Treatment of OPIOID USE DISORDER: WHEN & HOW TO GET STARTED Matt Iles-Shih, MD Acting Assistant
Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc.
 Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc. Elements Behavioral Health Diplomate, American Board of Addiction
Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc. Elements Behavioral Health Diplomate, American Board of Addiction
Medication for the Treatment of Alcohol Use Disorder. Pocket Guide
 Medication for the Treatment of Alcohol Use Disorder Pocket Guide Medications are underused in the treatment of alcohol use disorder. According to the National Survey on Drug Use and Health, of the estimated
Medication for the Treatment of Alcohol Use Disorder Pocket Guide Medications are underused in the treatment of alcohol use disorder. According to the National Survey on Drug Use and Health, of the estimated
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT
 and acute pain management on MAT") An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
Medication for Addiction Treatment (MAT)
") SBIRT Training Screening, Brief Intervention & Referral to Treatment Medication for Addiction Treatment (MAT) The Faith & Spirituality Integrated SBIRT Network Navigating the Training Welcome! These health
SBIRT Training Screening, Brief Intervention & Referral to Treatment Medication for Addiction Treatment (MAT) The Faith & Spirituality Integrated SBIRT Network Navigating the Training Welcome! These health
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Medication Assisted Treatment. Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs
 Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Buprenorphine is the most effective office-based treatment available for heroin and prescription opioid addiction
 Buprenorphine is the most effective office-based treatment available for heroin and prescription opioid addiction The Problem The overdose death rate in Missouri and in the country has been rising for
Buprenorphine is the most effective office-based treatment available for heroin and prescription opioid addiction The Problem The overdose death rate in Missouri and in the country has been rising for
Safe Practices and Action Items
 Safe Practices and Action Items Karen F Marlowe, Pharm D, BCPS Certified Pain Educator Auburn University Harrison School of Pharmacy University of South Alabama School of Medicine Case Study A 58 year
Safe Practices and Action Items Karen F Marlowe, Pharm D, BCPS Certified Pain Educator Auburn University Harrison School of Pharmacy University of South Alabama School of Medicine Case Study A 58 year
Arwen Podesta, MD. ABIHM, ABAM, Forensic Psychiatry
 The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
It s Not Just One More Thing! Overcoming Obstacles for Buprenorphine Treatment by Residents, Faculty and Programs
 It s Not Just One More Thing! Overcoming Obstacles for Buprenorphine Treatment by Residents, Faculty and Programs Ken Saffier, MD Maureen Strohm, MD May 7, 2017 Disclosures Ken Saffier, MD, has nothing
It s Not Just One More Thing! Overcoming Obstacles for Buprenorphine Treatment by Residents, Faculty and Programs Ken Saffier, MD Maureen Strohm, MD May 7, 2017 Disclosures Ken Saffier, MD, has nothing
Medications For Alcohol Use Disorder. DATE: October 10, 2017 PRESENTED BY: Alann Weissman-Ward, MD, Addiction Medicine fellow
 Medications For Alcohol Use Disorder DATE: October 10, 2017 PRESENTED BY: Alann Weissman-Ward, MD, Addiction Medicine fellow None DISCLOSURES OBJECTIVES Be able to name 4 medications to treat AUD Describe
Medications For Alcohol Use Disorder DATE: October 10, 2017 PRESENTED BY: Alann Weissman-Ward, MD, Addiction Medicine fellow None DISCLOSURES OBJECTIVES Be able to name 4 medications to treat AUD Describe
Treatment Approaches for Drug Addiction
 Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
MAT - ICAAD 2018 Ron Jackson, MSW, LICSW
 The ATTC Network Ten Regional Centers northwest@attcnetwork.org www.attcnetwork.org/northwest phone. 206-685-4419 1107 NE 45 th St, Ste 120, Seattle, WA 98105 http://attcnetwork.org/northwest U.S. Opioid
The ATTC Network Ten Regional Centers northwest@attcnetwork.org www.attcnetwork.org/northwest phone. 206-685-4419 1107 NE 45 th St, Ste 120, Seattle, WA 98105 http://attcnetwork.org/northwest U.S. Opioid
Latest Research on Addiction and Treatment
 Latest Research on Addiction and Treatment Joshua D Lee MD MSc joshua.lee@nyumc.org / @DrJoshuaDLee Associate Professor NYU School of Medicine, Department of Population Health Disclosures, LeeJD Grants:
Latest Research on Addiction and Treatment Joshua D Lee MD MSc joshua.lee@nyumc.org / @DrJoshuaDLee Associate Professor NYU School of Medicine, Department of Population Health Disclosures, LeeJD Grants:
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They?
 Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT)
") Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) For Apple Health clients served Fee-for-Service and through contracted Medicaid Managed Care Organizations Updated January
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) For Apple Health clients served Fee-for-Service and through contracted Medicaid Managed Care Organizations Updated January
Extended-Release Naltrexone for Opioid Relapse Prevention
 Extended-Release Naltrexone for Opioid Relapse Prevention 1.NYU SOM; Bellevue Hospital Center 2.Brown Univ. 3. Friends Research Institute 4. Columbia Univ. 5. Univ. Pennsylvania 6. Univ. Virginia Funding:
Extended-Release Naltrexone for Opioid Relapse Prevention 1.NYU SOM; Bellevue Hospital Center 2.Brown Univ. 3. Friends Research Institute 4. Columbia Univ. 5. Univ. Pennsylvania 6. Univ. Virginia Funding:
Disclosures. Topics of today s training 4/24/2017. Evolving Treads in Medication Assisted Treatment. Christopher J Davis D.O.
 Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates
 and Medication Assisted Treatment (MAT) for Opiates") Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Medication Assisted Treatment:
 Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services
 Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services www.randallwebber.com MAT clients are still addicted Truth: MAT clients will experience withdrawal symptoms if they stop
Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services www.randallwebber.com MAT clients are still addicted Truth: MAT clients will experience withdrawal symptoms if they stop
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT)
") Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) What has changed? Effective January 16, 2018, Coordinated Care will change the requirement for form HCA 13-333 Medication
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) What has changed? Effective January 16, 2018, Coordinated Care will change the requirement for form HCA 13-333 Medication
Management of Opioid Use Disorder in Primary Care
 1 Northwest ATTC presents Management of Opioid Use Disorder in Primary Care Joseph O. Merrill, MD, MPH University of Washington Associate Professor of Medicine 4/26/2018 Today s Presenter 2 Joseph Merrill,
1 Northwest ATTC presents Management of Opioid Use Disorder in Primary Care Joseph O. Merrill, MD, MPH University of Washington Associate Professor of Medicine 4/26/2018 Today s Presenter 2 Joseph Merrill,
Opioid Use Disorders as a Brain Disease Why MAT is so important. Ron Jackson, M.S.W., L.I.C.S.W.
 Opioid Use Disorders as a Brain Disease Why MAT is so important Ron Jackson, M.S.W., L.I.C.S.W. Affiliate Professor School of Social Work University of Washington Organization Name: CareOregon Course Title:
Opioid Use Disorders as a Brain Disease Why MAT is so important Ron Jackson, M.S.W., L.I.C.S.W. Affiliate Professor School of Social Work University of Washington Organization Name: CareOregon Course Title:
Understanding and Combating the Heroin Epidemic
 Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
7/7/2016 Journal of the American Medical Association,
 1 2 Journal of the American Medical Association, 2008 3 The Clinical Trial 152 Adolescents and Young Adults (Age 15 to 21) randomly assigned to either; 1. 2 weeks of Buprenorphine detox 2. 12 weeks of
1 2 Journal of the American Medical Association, 2008 3 The Clinical Trial 152 Adolescents and Young Adults (Age 15 to 21) randomly assigned to either; 1. 2 weeks of Buprenorphine detox 2. 12 weeks of
Earl Hightower's Remarks 2014 National Rx Drug Abuse Summit Medication Assisted Treatment for Opiate Addiction
 Earl Hightower's Remarks 2014 National Rx Drug Abuse Summit Medication Assisted Treatment for Opiate Addiction Thank you, Chairman Rogers, for holding this important Summit and helping to bring attention
Earl Hightower's Remarks 2014 National Rx Drug Abuse Summit Medication Assisted Treatment for Opiate Addiction Thank you, Chairman Rogers, for holding this important Summit and helping to bring attention
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings
 Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Medications for Opioid Use Disorder. Charles Brackett, MD, MPH General Internal Medicine, DHMC
 Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Vivitrol/Suboxone. Comparison Study Summary
 Vivitrol/Suboxone Comparison Study Summary Lee, J. D., Nunes, E. V., Novo, P., Bachrach, K., Bailey, G. L., Bhatt, S., & King, J. (2017). Comparative effectiveness of extended-release naltrexone versus
Vivitrol/Suboxone Comparison Study Summary Lee, J. D., Nunes, E. V., Novo, P., Bachrach, K., Bailey, G. L., Bhatt, S., & King, J. (2017). Comparative effectiveness of extended-release naltrexone versus
Buprenorphine for Family Medicine. Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17
 + Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
+ Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
Treatment of Youth Opioid Addiction: Approaches to a Modern Epidemic. What should we do with this case? Heroin Addiction History
 Treatment of Youth Opioid Addiction: Approaches to a Modern Epidemic What should we do with this case? 17 M Onset prescription opioids 15, progressing to daily use with withdrawal within 8 months Onset
Treatment of Youth Opioid Addiction: Approaches to a Modern Epidemic What should we do with this case? 17 M Onset prescription opioids 15, progressing to daily use with withdrawal within 8 months Onset
Naltrexone for Opioid Use Disorder. A Project RAMP Resource Adam J. Gordon, MD MPH FACP DFASAM CMRO December 2017
 Naltrexone for Opioid Use Disorder A Project RAMP Resource Adam J. Gordon, MD MPH FACP DFASAM CMRO December 2017 LEARNING OBJECTIVES Be able to inform patients regarding the use and latest literature of
Naltrexone for Opioid Use Disorder A Project RAMP Resource Adam J. Gordon, MD MPH FACP DFASAM CMRO December 2017 LEARNING OBJECTIVES Be able to inform patients regarding the use and latest literature of
National Opioid Treatment Guideline Dr. Ronald Lim
 National Opioid Treatment Guideline Dr. Ronald Lim (MD, CCFP, DFASAM, ABAM(D), FISAM, CCSAM, MRO) Clinical Assistant Professor, Department of Psychiatry and Family Practice Cumming School of Medicine University
National Opioid Treatment Guideline Dr. Ronald Lim (MD, CCFP, DFASAM, ABAM(D), FISAM, CCSAM, MRO) Clinical Assistant Professor, Department of Psychiatry and Family Practice Cumming School of Medicine University
Naltrexone Overview. Todd Korthuis, MD, MPH ECHO-MAT Conference November 7, 2017
 Naltrexone Overview Todd Korthuis, MD, MPH ECHO-MAT Conference November 7, 2017 Disclosure Information Speaker/Planner: Todd Korthuis, MD, has nothing to disclose. 2 Pharmacotherapy for Opioid Use Disorder
Naltrexone Overview Todd Korthuis, MD, MPH ECHO-MAT Conference November 7, 2017 Disclosure Information Speaker/Planner: Todd Korthuis, MD, has nothing to disclose. 2 Pharmacotherapy for Opioid Use Disorder
THE STATE OF MEDICINE IN ADDICTION RECOVERY
 OVERVIEW: Review addiction stats and trends Define addiction Explain neurobiology of addiction Review treatments of addiction Addiction Definition: A Primary, chronic, relapsing disease of brain reward,
OVERVIEW: Review addiction stats and trends Define addiction Explain neurobiology of addiction Review treatments of addiction Addiction Definition: A Primary, chronic, relapsing disease of brain reward,
Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention
 The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
Injectable naltrexone (XR-NTX) A RETROSPECTIVE STUDY OF ITS ACCEPTANCE IN A COMMUNITY RECOVERY SETTING BRIANNE FITZGERALD MSN, PMHNP, CARN-AP
 A RETROSPECTIVE STUDY OF ITS ACCEPTANCE IN A COMMUNITY RECOVERY SETTING BRIANNE FITZGERALD MSN, PMHNP, CARN-AP") Injectable naltrexone (XR-NTX) A RETROSPECTIVE STUDY OF ITS ACCEPTANCE IN A COMMUNITY RECOVERY SETTING BRIANNE FITZGERALD MSN, PMHNP, CARN-AP Overview Gavin Foundation Injectable naltrexone Community report
Injectable naltrexone (XR-NTX) A RETROSPECTIVE STUDY OF ITS ACCEPTANCE IN A COMMUNITY RECOVERY SETTING BRIANNE FITZGERALD MSN, PMHNP, CARN-AP Overview Gavin Foundation Injectable naltrexone Community report
Disclosure Statement. Learning Objectives. American Psychiatric Nurses Association. Christian J. Teter, PharmD, BCPP 1 BUPRENORPHINE UPDATE
 BUPRENORPHINE UPDATE Christian J. Teter, Pharm.D., BCPP Associate Professor, Psychopharmacology College Of Pharmacy, University Of New England Portland, ME E-Mail: cteter@une.edu Image Source: pubchem.ncbi.nlm.nih.gov
BUPRENORPHINE UPDATE Christian J. Teter, Pharm.D., BCPP Associate Professor, Psychopharmacology College Of Pharmacy, University Of New England Portland, ME E-Mail: cteter@une.edu Image Source: pubchem.ncbi.nlm.nih.gov
Implementing Buprenorphine Treatment in Opioid Treatment Programs Webinar 2, October 3, 2018
 Implementing Buprenorphine Treatment in Opioid Treatment Programs Webinar 2, October 3, 2018 Judith Martin, MD, Medical Director of Substance Use Services, San Francisco Department of Public Health Webinar
Implementing Buprenorphine Treatment in Opioid Treatment Programs Webinar 2, October 3, 2018 Judith Martin, MD, Medical Director of Substance Use Services, San Francisco Department of Public Health Webinar
Module II Opioids 101 Opiate Opioid
 BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module II Opioids 101 Module II Goals of the Module This module reviews the following:! Opioid addiction and the brain!
BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module II Opioids 101 Module II Goals of the Module This module reviews the following:! Opioid addiction and the brain!
Pharmacotherapy for opioid addiction. Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco
 Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Supporting Sustained Recovery for Opioid Use Disorder
 Supporting Sustained Recovery for Opioid Use Disorder RCPA Conference Hershey, PA October 3, 2018 Agenda Scope of the opioid epidemic Medication-assisted treatment (MAT) What does MAT involve? What are
Supporting Sustained Recovery for Opioid Use Disorder RCPA Conference Hershey, PA October 3, 2018 Agenda Scope of the opioid epidemic Medication-assisted treatment (MAT) What does MAT involve? What are
Identification and Treatment of Opioid Use Disorders in Primary Care Settings
 Identification and Treatment of Opioid Use Disorders in Primary Care Settings 17th Annual Primary Care Symposium February 24, 2018 Kelly S. Barth, DO Associate Professor, Psychiatry & Internal Medicine
Identification and Treatment of Opioid Use Disorders in Primary Care Settings 17th Annual Primary Care Symposium February 24, 2018 Kelly S. Barth, DO Associate Professor, Psychiatry & Internal Medicine
9/13/2017. Buprenorphine Treatment (Suboxone) Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare
 Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare") Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Medication Assisted Treatment of an Opioid Use Disorder. J. Craig Allen, MD. Medical Director, Rushford
 Medication Assisted Treatment of an Opioid Use Disorder J. Craig Allen, MD. Medical Director, Rushford Learning objectives At the conclusion of this activity, participants will be able to: Understand
Medication Assisted Treatment of an Opioid Use Disorder J. Craig Allen, MD. Medical Director, Rushford Learning objectives At the conclusion of this activity, participants will be able to: Understand