Multidisciplinary Management of the Opioid Crisis To Optimize Perinatal Outcome in a Rural Women s Clinic Population
|
|
|
- Constance Collins
- 5 years ago
- Views:
Transcription

1 Multidisciplinary Management of the Opioid Crisis To Optimize Perinatal Outcome in a Rural Women s Clinic Population Dale Robinson MD,FACOG Jennifer Gonzalez RN,BSN
2
3 Surgeon General s Report 2016 Office of the Surgeon General released this first report of its kind The Surgeon General s Report on Alcohol, Drugs, and Health. Report identified addiction the number one public health problem in America. Addiction at the crisis level - 1/3 of total population affected. The Report discusses opportunities to bring substance use disorder treatment and mainstream health care systems into alignment

4 Opioid Addiction
5 Scope of the Problem : Cost Substance misuse and substance use disorders also have serious economic consequences, costing more than $400 billion annually in crime, health, and lost productivity Diabetes by contrast cost the US $245 billion annually A potentially more effective use of healthcare resources should focus on efforts on screening and treating addiction rather than managing outcomes of the disease
6 Opioid Addiction In the 1990 s we were told pain is the 5 th Vital Sign Pleasant sensations cause endorphin production which transiently bind the mu opioid receptor Morphine strongly binds the receptor and produces intense euphoria Attempts have been made to harness positive analgesic effects without side effects or potential for addiction
7 Heroin
8 Heroin Heron was synthesized from morphine in 1874 It was once hoped that heroin would have the analgesic properties of morphine Without the addictive potential Widely abused and banned in the Heroin Act of 1924

9 Codeine Very similar structure (ether) FDA warning against breastfeeding due to potentially rapid conversion to morphine leading to infant toxicity Breastfeeding is encouraged for buprenorphine and methadone although monitoring for CNS depression is always prudent
10 Risk of Addiction Risk of substance use disorder rises after 5 days of use and increases dramatically with prolonged use One in four patients using legal opioids misuses them (continuation of opioids past the point of analgesia) Opioid use has quadrupled over the past decade In million patients abused prescription opioids while abused heroin
11 Risk of Addiction Many heroin users once abused legal narcotics Every 3 minutes a woman of child bearing age seeks care in an ED related to prescription opioid misuse Increased opioid use in pregnant women has increased Neonatal Abstinence Syndrome (NAS) 5 fold and 2/3 of these cases are associated with legally prescribed narcotics
12 Risk of Addiction Addiction in laboratory animals Causes of opioid addiction are multifactorial Clinicians, pharmaceutical companies, accrediting organizations, drug cartels, and public expectations are all involved Changing the way we do business and addressing the crisis in a multidisciplinary fashion is needed to resolve the public health crisis

13
14 How Can We Help Our Community? Community Assessment- current programs available and functionality. Identify Key Stakeholders- School, hospital, clinical practice, Center for Human Development (CHD), Department of Human Services (DHS) and local law enforcement. (AA and DA programs) Federal and State Grants
15 Barriers to Success Timid Population addicts are sensitive and untrusting of non-addicts. They are easily scared away from treatment. Buy in from providers- are the providers on board with a program? Expectations of the providers- is it realistic? Realistic expectations of patients
16 Barriers to Success Cost- Hiring new employees and training current staff Funding for emergent needs for the patients Education to staff and providers
17
18 Healthy Outcomes Healthy outcomes are more likely when women obtain prenatal care early during pregnancy, consistently complete their prenatal visits, receive MAT and participate in counseling. Conversely, poor health outcomes for the baby are more likely when women miss prenatal and neonatal appointments, continue their illicit use of opioids, lack stable housing, and/or do not continue to obtain substance abuse counseling. To reach our goals we have identified 6 key elements for a successful recovery program.
19 6 Key Elements Screening Navigator Home safety assessment Individualized treatment plan Delivery plan Post delivery care
20 REPORTING Oregon law states that all medical personnel are mandatory reporters. The Department of Human Services specifically states that all county health employees are mandatory reporters and are required to report any suspected abuse or neglect. Child Abuse - Child means an unmarried person who is under 18 years of age. Oregon does not recognize the fetus as a child and therefore has no protective rights. However if the maternal patient is using drugs or engaging in an activity that could put her other children at risk that is reportable.
21 Screening Best Practices Screening for alcohol in pregnant women is easier as valid standardized questionnaires are available Screening for drugs is not as simple and there is no universally accepted practice U.S. Preventive Services Task Force insufficient evidence for screening ACOG recommends screening all pregnant women
22 Screening Best Practices: Barriers Legal consequences to a positive screen include: Possible child custody affects Societal stigma Lack of availability of drug treatment and referral options for patients with a positive test
23 Screening Best Practices: Barriers Do we need a questionnaire? Who should administer it? If laboratory tests are done, how reliable are they? State laws limit testing options for patients that don t consent and patients should be aware of possible false positive results and mandatory reporting requirements We do not report rapid drug screens to DHS due to the risk of false positives; only confirmatory tests are reported
24 Screening Best Practices: Legal ACOG: Urine drug testing should be performed with the patient s consent and in compliance with existing state laws. Pregnant women should be informed of the potential consequences of a positive test before performing it, including any mandatory reporting requirements Oregon law requires written consent Clinical vs. forensic testing
25 CHARM Program: Screening Screening occurs when indicated Patients in Medically Assisted Treatment (MAT) get frequent testing Own protection and always voluntary Worrisome clinical picture and high suspicion Oregon Law requires patient consent
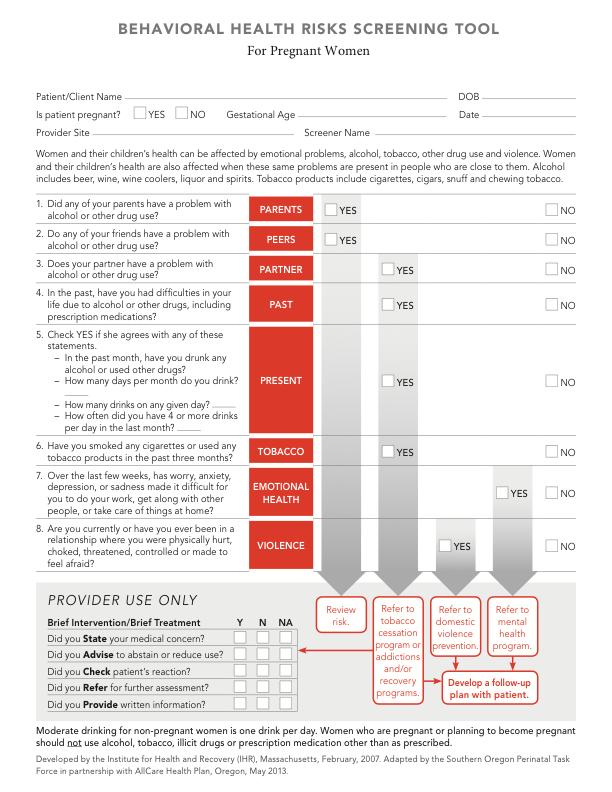
26 Screening Instrument
27 CHARM Program: Screening Role Developed by the Institute for Health and Recovery 2007 Adapted by the Southern Oregon Perinatal Taskforce in partnership with Allcare Health Plan Oregon May P s : parents, peers, partner, past and present Everyone is screened at initial obstetric visit with this form by clinical nurse and appropriate referrals are made

28 Screening Results: Rates of USDTL Clients with High Risk Pregnancies
29 Colorado Positivity Rates of Clients with High Risk Pregnancies A study of the impact of relaxing statewide marijuana laws on maternal marijuana use; Joseph Jones, Clarity in Newborn Toxicology 2016 volume 7 THC positivity rate for all meconium specimens increased from 10.6% to 11.7% from 2012 to 2014 The median concentration of THC in the meconium specimens more than doubled from 108ng to 277ng Neonates following commercialization are exposed to substantially more THC in utero

30 THC Edibles

31 THC Concentrates Continued
32 THC Concentrates Continued Woodstock era marijuana 2% THC vs Colorado 30% Single serving 10 mg and THC lobbies solution Candy cigarettes, Flavored nicotine vapes Nicotine infused Pop-Tarts, Alcohol-infused gummies, or codeine-infused sodas Edibles are 40 percent of the market
33 Marijuana risks in Pregnancy and Lactation ACOG and AAP recommends pregnant and lactating women not use marijuana either medically or recreationally THC remains in breast milk for 6 days or longer Concentrates are concerning and are effectively a new drug Highest concentrate studied is 16 mg; Lancet
34 AAP and Marijuana Observational studies indicate concern for fetal growth and early neonatal behaviors As well as altered long-term neurodevelopmental consequences of prenatal exposure to marijuana. These studies were conducted when marijuana had a much lower potency than today thus the adverse consequences may be much greater than what has been reported to date
35 Case Study Late Screen A maternal patient in her late 20 s arrived to the OB department in early labor at 39 weeks. She is married with a 3 year old at home. A stay at home mom devoted to her family. Had a history of dabbling with drug use in her teens- but nothing since. History of ankle fracture over a year ago that required surgical repair, otherwise very healthy. Changes in the program
36 Navigator Role The navigator is a highly motivated, organized, people person, adept at conflict resolution. It is most beneficial if they have a background in social work. She/he must have access to the EHR and have social services connections. The navigator coordinates medical care, substance abuse treatment, social supports, and nutrition services for CHARM families. She also educates parents about CHARM and requests a signed release of information for families that enroll in the program. She relies on the CHARM meetings to coordinate services for CHARM clients efficiently with other providers.

37 Navigator Role The navigator updates the collaborative team during monthly meetings where CHARM patient updates are provided. The team reviews and assesses the individualized treatment plan of each CHARM patient and family ensuring that all needs are addressed and met.
38 Individualized Treatment Plan Individualized plan of care it is just that. No two people are the same in their daily struggles and no two people will fit into the same cookie cutter plan of care for treatment. In addition to standard prenatal care, each visit includes a urine drug test; monitoring of attendance at prior prenatal visits; substance abuse counseling; home visiting appointments; and ongoing assessment of social support needs, including housing, transportation, and mental health services.
39 Individualized Treatment Plan A Medication Assisted Therapy (MAT) assessment is typically completed at the first CHARM appointment. All CHARM women who receive MAT must also receive substance abuse counseling and non pharmacological substance abuse treatment. Both group and individual treatment are provided to CHARM patients. Collaborative members stress the importance of substance abuse counseling with families and make every effort to keep women engaged and actively participating in this aspect of their treatment.
40 Home Safety Assessment The home safety assessments of families affected by prenatal substance exposure are completed using the same protocol as those used for all families reported to DHS Children Services for any reason. CHARM Collaborative members may share the results of safety assessments and intervention plans with other collaborative members, and all members who are working with a family share their observations regarding the family s progress, success, concerns, and needs.

41 Home Safety Assessment CHD maternal nurse completes the home assessment. This helps to establish a relationship prior to delivery and the nurse can help answer questions the patient may have regarding her pregnancy. Assessment findings are communicated to the navigator who will then communicate to the delivering hospital and collaborative members.
42 Delivery Plan The CHARM navigator alerts all collaborative members and delivery units of expected deliveries at weeks gestation. Labor and delivery protocols are the same for all women delivering at GRH, except that the focus on pain control increases because women taking buprenorphine or methadone often experience higher levels of pain during childbirth.
43 Post-delivery Care GRH continues to provide services to CHARM women for 6 weeks after delivery for follow up care. After that time, the women receive ongoing care from a community based clinic or a primary care provider. Newborns are seen weekly by CHD Babies First a home nursing visit where they measure the baby s weight and size; conducts a physical examination; monitors the infant s growth and development; lactation services are available. A continuation of substance abuse counseling; home visiting appointments; and ongoing assessment of social support needs, including housing, transportation, and mental health.
44 Case-Study Delivery Plan 30+ year old woman with extensive heroin and Oxycontin use. Has 2 older children who were removed by DHS and are being raised by the FOB s family. Has a huge fear of government agencies- DHS and CHD especially- and therefore very reluctant for any interference. After signing into CHARM, she received social support including housing, is involved with therapy, counseling and MAT program. The patient was very successful in her recovery efforts. High concern for relapse due to her extensive drug use history.
45 Best Practices: Can We Use Less Narcotics Without Inadequate Pain Treatment Prevention is Better Than Treatment Are We Overprescribing Narcotics After Delivery? Duration of use is a risk factor for addiction Can we limit Narcotics Use During Inpatient Stay and Still Adequately Treat Pain Alternative Treatments of Postoperative Pain
46 Best Practices: Opioid Prescribing at Hospital Discharge How many oxycodone tablets do we prescribe after vaginal delivery? Cesarean? How many should we? Are there best practices? CDC recommends that 3 days or less will often be sufficient for acute pain and that rarely are more than 7 days necessary? Is this true in obstetrics?
47 Leftover Narcotics Those pills not taken after a legal prescription Pathway to opioid abuse Many individuals abusing narcotics received them from community family or friends Studies in other areas of medicine suggest that more than half of legal narcotics go unused and are not disposed of safely
48 Best Practices: Opioids at Hospital Discharge after Cesarean Delivery Cesarean Delivery is the most common major surgical procedure in the US The risk of developing opioid addiction after CD in opioid naïve patients is low (1/300) but the number of procedures makes this an important public health issue Post-discharge opioid use after Cesarean Delivery was studied by Osmundson and colleagues in Obstetrics and Gynecology July 2017:130:36-41
49 Postdischarge Opioid Use After Cesarean Delivery: Osmundson et al They found that 83% of surgical patients used narcotics after hospital discharge for a median duration of use of 8 days with a interquartile range of 6-13 days 17% used opioids for more than 2 weeks postpartum with the maximum duration being 39 days The average prescription was for 30 tablets and 75 % of patients had unused tablets A median of 10 unused oxycodone tablets were leftover per patient and for every additional 10 tablets of oxycodone prescribed and average of 2 additional extra tablets occurred
50 Post-discharge Opioid Use After Cesarean Delivery: Osmundson et al Only 6 % of patients reported disposing of extra tablets safely so a significant quantity of tablets was leftover Less than 3% had an additional prescription of narcotics filled Higher inpatient use of narcotics made the patient less likely to have leftover narcotics and to report that they were prescribed too few medications The women using the most pills postop were more likely to use tobacco and have public health insurance
51 Postdischarge Opioid Use After Cesarean Delivery: Osmundson et al The patients using the most narcotics in the postoperative period were given more narcotics but the correlation was weak (r=.35); other factors were involved Provider type was an important determinant of prescribing practice with CNM prescribing fewer narcotics than physicians in a faculty practice The authors concluded that more narcotics were apparently needed than the CDC recognized but leftover narcotics was a significant problem; they suggested that, health care providers are not currently considering in hospital opioid use in determining the amount of opioid prescribed at discharge. Instead prescriptions appear to be personalized to health care provider background
52 What is the right number of pills after CD? CDC suggests 3 days or less Osmundson study median 8 days with range 6-13 days 75% of patients had leftover pills Can we lower this number yet meet legitimate postop pain needs Wal-mart in our community
53 What is the right number of pills after CD? A Shared Decision-Making Intervention to Guide Opioid Prescribing After Cesarean Delivery Prabhu et al. Obstet Gynecol 2017; A study was done asking postop c-section patients how many pills they needed Postoperative patients received information concerning typical pain resolution time courses where allowed to choose the number of 5 mg oxycodone tablets
54 A Shared Decision-Making Intervention The median number of tablets was 20 with interquartile range % were satisfied with the analgesia achieved and only 8% required an additional prescription The number of tablets prescribed was significantly less than the institutional average of 40 pills The number of leftover tablets was 4 with an interquartile range of 0 to 8
55 Narcotics after vaginal delivery Does everyone need them? Filled prescriptions for opioids after vaginal delivery Jarlenski and colleagues Obstet Gynecol 2017;129:431-7.
56 Narcotics after vaginal delivery 12% of women filled an opioid prescription within 5 days of delivery 72% of them did not have a laceration, episiotomy or tubal ligation Most women received 3-7 days worth of narcotics but some received up to 30 days worth of medication Smokers and patients with a mental health diagnosis were more likely to receive meds The rate of leftover pills was not recorded
57 Narcotics after vaginal delivery No national guidelines Pennsylvania guidelines; hierarchical approach ACOG in Postpartum Pain Management July 2018 Nonpharmacologic treatment, nonnarcotic treatment Finally only after treatment failure short acting opioid can be used for 5-7 days
58 Best Practices: Opioid Management During Pregnancy Medically supervised withdrawal versus medically assisted treatment Prevention of Neonatal Abstinence Syndrome (NAS) is desirable Goal of treatment is to prevent withdrawal and illicit use of opiates Increased risk of relapse and withdrawal poses a risk to the fetus The risk of maternal relapse and possible fetal risks have limited this approach in most cases and medication assisted treatment is the preferred treatment in most cases
59 Opioid Prescription During Pregnancy: Methadone Studies have been inconsistent in establishing the relationship between methadone dose and NAS incidence and severity: a lower dose is not safer May be better than buprenorphine for women with longstanding poly-substance abuse and previous failed detox attempts Methadone is only routinely available through a federally regulated addiction clinic Both methadone and buprenorphine may be dispensed in a hospital setting by physicians without waivers
60 Opioid Prescription During Pregnancy: Buprenorphine Buprenorphine is a synthetic opioid that produces weaker euphoric effects than methadone or heroin and is a partial antagonist Ceiling effect: shorting acting agonist like fentanyl will provide more analgesia but it will take a higher dose Pregnant women on methadone should not transition to buprenorphine because buprenorphine may precipitate withdrawal due to its partial antagonist action
61 Opioid Prescription During Pregnancy: Buprenorphine Buprenorphine is the only opioid agonist currently approved for the treatment of opioid use disorder by prescription in an office-based setting Increases availability of treatment and may decrease stigma of treatment; currently more than providers in many specialties are approved prescribers Buprenorphine advantage: lower risk of death from an overdose than methadone Suboxone is a combination of buprenorphine with naloxone and is rarely used in pregnant women
62 Buprenorphine : Better Neonatal Outcomes The Maternal Opioid Treatment, Human Experimental Research study which was a multicenter randomized trial comparing buprenorphine with methadone Buprenorphine exposed neonates required 89% less morphine to treat NAS and spent 43% less time in the hospital The total neonatal abstinence syndrome score and the individual signs were higher among methadone exposed neonates Meta-analysis: buprenorphine exposed neonates had greater gestational age and birth weight and were less likely to use illicit opioids near delivery
63
64 Neonatal Abstinence Syndrome Neonatal Abstinence Syndrome- (NAS) is a group of conditions that occurs when the newborn withdrawals from a substance it was exposed to while in the womb. NAS increased 5 fold and 2/3 of cases are associated with legal medications NAS after buprenorphine develop symptoms by 48 hours and peak by hours NAS after methadone: symptoms appear by 3-5 days but may appear as late as a week of age and persist longer All newborns exposed to opioids should be monitored for at least 96 hrs (AAP guideline)
65 Neonatal Abstinence Syndrome How do you counsel patients? NAS incidence variable but high up to 80% Factors that affect the incidence and severity of NAS include CNS agents such as nicotine benzodiazepines, gabapentin, SSRI, THC, and genetic predisposition, gestational age and maternal diet. Role of lactation
66 Neonatal Abstinence Syndrome Do you treat it locally at a CAH? All CHARM babies stay in their mother s room after birth. CHARM mothers are encouraged to use non-pharmacological treatments for withdrawal symptoms in their infants, including skin to skin contact, breastfeeding, and a low stimulus environment for the baby. A low stimulus environment includes low levels of lights, low levels of noise, and few visitors. CHARM infants typically stay in the hospital for 4 6 days for NAS monitoring. Hospital nurses assess all CHARM babies for NAS using a scoring tool based on the Finnegan Neonatal Abstinence Scoring System (Finnegan, 1975). Assessments begin at 2 hours after birth and continuing every 3 to 4 hours for the first 96 hours until discharge.
67 Case Study NAS Patient in her early 20 s with a history of Oxycontin addiction that developed into heroin addiction- anywhere from 2-6 point a day. Committed and completed 30 day inpatient rehab, moved to a new apartment, therapy and counseling 2-3 times a week and MAT program. Planned repeat C-section at 39 weeks. Baby stayed in the hospital for 6 days.

68
The Opioid-Exposed Woman
 The Opioid-Exposed Woman Management Considerations for Labor and Delivery Jane Sublette, MS, RN, CNM, WHNP-BC Fairview Ridges Hospital Objectives Describe opioid-associated risks to the mother and fetus
The Opioid-Exposed Woman Management Considerations for Labor and Delivery Jane Sublette, MS, RN, CNM, WHNP-BC Fairview Ridges Hospital Objectives Describe opioid-associated risks to the mother and fetus
Maternal-fetal Opiate Medical Home (MOMH) Jocelyn Davis DNP,CNM, RN, CEFMM Karen Frantz BSN, RNC
 Jocelyn Davis DNP,CNM, RN, CEFMM Karen Frantz BSN, RNC") Maternal-fetal Opiate Medical Home (MOMH) Jocelyn Davis DNP,CNM, RN, CEFMM Karen Frantz BSN, RNC Objectives 1. Discuss the effects of opiate addiction on mothers and infants. 2. Discuss a Medical Home
Maternal-fetal Opiate Medical Home (MOMH) Jocelyn Davis DNP,CNM, RN, CEFMM Karen Frantz BSN, RNC Objectives 1. Discuss the effects of opiate addiction on mothers and infants. 2. Discuss a Medical Home
4/19/2018. Opioid Use Disorder in Pregnancy OBJECTIVES ANTENATAL TESTING
 Opioid Use Disorder in Pregnancy 2017 Recommendations from ACOG and The Pew Charitable Trust KATHY D. HARTKE, MD, LEGISLATIVE CO-CHAIR AND IMMEDIATE PAST CHAIR, WISCONSIN SECTION OF THE AMERICAN COLLEGE
Opioid Use Disorder in Pregnancy 2017 Recommendations from ACOG and The Pew Charitable Trust KATHY D. HARTKE, MD, LEGISLATIVE CO-CHAIR AND IMMEDIATE PAST CHAIR, WISCONSIN SECTION OF THE AMERICAN COLLEGE
Neonatal Abstinence Syndrome Questions & Answers Webinar #1 (February 9, 2012) Webinar #2 (March 30, 3012)
 Webinar #2 (March 30, 3012)") Neonatal bstinence Syndrome Questions & nswers Webinar #1 (February 9, 2012) Webinar #2 (March 30, 3012) For more information and to download a copy of the NS Clinical Practice Guidelines, please visit
Neonatal bstinence Syndrome Questions & nswers Webinar #1 (February 9, 2012) Webinar #2 (March 30, 3012) For more information and to download a copy of the NS Clinical Practice Guidelines, please visit
THE OPIOID CRISIS 9/19/2018 DEFINING THE CRISIS DEFINING THE CRISIS NUMBER OF OPIOID-RELATED OVERDOSE DEATHS IN ALABAMA
 THE OPIOID CRISIS DEFINING THE CRISIS KATHLEEN DUPPER, MD MEDICAL DIRECTOR, HUNTSVILLE RECOVERY 19 th Annual Perinatal Conference: The Opioid Crisis September 21, 2018 DEFINING THE CRISIS NUMBER OF OPIOID-RELATED
THE OPIOID CRISIS DEFINING THE CRISIS KATHLEEN DUPPER, MD MEDICAL DIRECTOR, HUNTSVILLE RECOVERY 19 th Annual Perinatal Conference: The Opioid Crisis September 21, 2018 DEFINING THE CRISIS NUMBER OF OPIOID-RELATED
MAT IN PREGNANCY KAYLA LIFE STAGE 1: ADOLESCENCE LIFE STAGE 2: EARLY ADULTHOOD. family History of addiction. addiction to oral opioids
 MAT IN PREGNANCY R. COREY WALLER MD, MS PRINCIPAL, HEALTH MANAGEMENT ASSOCIATES FACULTY, INSTITUTE FOR HEALTHCARE INNOVATION (IHI) CHAIR, LEGISLATIVE ADVOCACY COMMITTEE, ASAM KAYLA LIFE STAGE 1: ADOLESCENCE
MAT IN PREGNANCY R. COREY WALLER MD, MS PRINCIPAL, HEALTH MANAGEMENT ASSOCIATES FACULTY, INSTITUTE FOR HEALTHCARE INNOVATION (IHI) CHAIR, LEGISLATIVE ADVOCACY COMMITTEE, ASAM KAYLA LIFE STAGE 1: ADOLESCENCE
Medication Assisted Treatment. MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment
 Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Maternal Substance Abuse: Challenges & Opportunities for Perinatal Nurses Catherine H. Ivory, PhD, RNC-OB October, 2015
 Maternal Substance Abuse: Challenges & Opportunities for Perinatal Nurses Catherine H. Ivory, PhD, RNC-OB October, 2015 Objectives Discuss the current scope of maternal substance use and abuse List examples
Maternal Substance Abuse: Challenges & Opportunities for Perinatal Nurses Catherine H. Ivory, PhD, RNC-OB October, 2015 Objectives Discuss the current scope of maternal substance use and abuse List examples
NOWS The Time Caring for the Infant with Neonatal Opiate Withdrawal Syndrome
 NOWS The Time Caring for the Infant with Neonatal Opiate Withdrawal Syndrome Meghan Howell, MD FAAP Assistant Professor of Pediatrics Clinical Director, Tulane NICU Graduate Clinic Tulane University School
NOWS The Time Caring for the Infant with Neonatal Opiate Withdrawal Syndrome Meghan Howell, MD FAAP Assistant Professor of Pediatrics Clinical Director, Tulane NICU Graduate Clinic Tulane University School
PROJECT DOVE. Improving Maternal and Neonatal Health Through Safer Opioid Prescribing
 PROJECT DOVE Improving Maternal and Neonatal Health Through Safer Opioid Prescribing PARTNERS SUPPORT Bureau of Justice Assistance, Department of Justice Rhode Island Opportunity Non-medical prescription
PROJECT DOVE Improving Maternal and Neonatal Health Through Safer Opioid Prescribing PARTNERS SUPPORT Bureau of Justice Assistance, Department of Justice Rhode Island Opportunity Non-medical prescription
Medication Assisted Treatment
 Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
ADDRESSING THE OPIOID EPIDEMIC. Joint principles of the following organizations representing front-line physicians
 ADDRESSING THE OPIOID EPIDEMIC Joint principles of the following organizations representing front-line physicians American Academy of Family Physicians American Academy of Pediatrics American College of
ADDRESSING THE OPIOID EPIDEMIC Joint principles of the following organizations representing front-line physicians American Academy of Family Physicians American Academy of Pediatrics American College of
Central Appalachia: A Regional Response to an Opioid Epidemic in Pregnancy
 Centers for Disease Control and Prevention Central Appalachia: A Regional Response to an Opioid Epidemic in Pregnancy Jenna Meyer MPH, RNC-MNN, IBCLC Public Health Advisor Therapies for Opioid Dependent
Centers for Disease Control and Prevention Central Appalachia: A Regional Response to an Opioid Epidemic in Pregnancy Jenna Meyer MPH, RNC-MNN, IBCLC Public Health Advisor Therapies for Opioid Dependent
Brief History of Methadone Maintenance Treatment
 METHADONE Brief History of Methadone Maintenance Treatment Methadone maintenance treatment was on the cusp of the social revolution in the sixties. Doctors and public health workers had concluded what
METHADONE Brief History of Methadone Maintenance Treatment Methadone maintenance treatment was on the cusp of the social revolution in the sixties. Doctors and public health workers had concluded what
Child Welfare and MOMS: Building Partnerships to Improve Care
 Child Welfare and MOMS: Building Partnerships to Improve Care Goals Develop collaborative partnerships between MOMS pilot sites and child welfare agencies: Facilitate successful outcomes for clients Jointly
Child Welfare and MOMS: Building Partnerships to Improve Care Goals Develop collaborative partnerships between MOMS pilot sites and child welfare agencies: Facilitate successful outcomes for clients Jointly
Opioid use in pregnancy and Neonatal Abstinence Syndrome
 Opioid use in pregnancy and Neonatal Abstinence Syndrome Morissa Ladinsky, MD Assoc. Professor of Pediatrics Division of General Pediatrics and Adolescent Medicine UAB Objectives 1. Understand the magnitude,
Opioid use in pregnancy and Neonatal Abstinence Syndrome Morissa Ladinsky, MD Assoc. Professor of Pediatrics Division of General Pediatrics and Adolescent Medicine UAB Objectives 1. Understand the magnitude,
Effects of Prenatal Illicit Drug. Use on Infant and Child
 Effects of Prenatal Illicit Drug Use on Infant and Child Development Andrew Hsi, MD, MPH Larry Leeman, MD, MPH Family Medicine MCH Grand Rounds 6 July 2011 Objectives for Presentation At the end of this
Effects of Prenatal Illicit Drug Use on Infant and Child Development Andrew Hsi, MD, MPH Larry Leeman, MD, MPH Family Medicine MCH Grand Rounds 6 July 2011 Objectives for Presentation At the end of this
EI Leadership April 24, 2018
 Early Childhood Community Partnerships to Support Families Struggling with SUD EI Leadership April 24, 2018 Setting the Stage The issue of young children impacted by substance use disorders in families
Early Childhood Community Partnerships to Support Families Struggling with SUD EI Leadership April 24, 2018 Setting the Stage The issue of young children impacted by substance use disorders in families
2/24/2017. Pregnant Women Who Use Drugs: Stigma, Science and Society
 Pregnant Women Who Use Drugs: Stigma, Science and Society Mishka Terplan MD MPH FACOG FASAM Professor Departments Obstetrics and Gynecology and Psychiatry Associate Director Addiction Medicine Virginia
Pregnant Women Who Use Drugs: Stigma, Science and Society Mishka Terplan MD MPH FACOG FASAM Professor Departments Obstetrics and Gynecology and Psychiatry Associate Director Addiction Medicine Virginia
Trends and Challenges: The Kentucky Opioid Crisis. Jason Smith, MD PhD University of Louisville
 Trends and Challenges: The Kentucky Opioid Crisis Jason Smith, MD PhD University of Louisville Brief Introduction I am by no means an expert I have no financial disclosures Jokes are meant to be lighthearted
Trends and Challenges: The Kentucky Opioid Crisis Jason Smith, MD PhD University of Louisville Brief Introduction I am by no means an expert I have no financial disclosures Jokes are meant to be lighthearted
Agenda. 1 Opioid Addiction in the United States. Evidence-based treatments for OUD. OUD Treatment: Best Practices. 4 Groups: Our Model
 Agenda 1 Opioid Addiction in the United States 2 Evidence-based treatments for OUD OUD Treatment: Best Practices 4 Groups: Our Model 2 Groups is a national network of clinics providing affordable, evidencebased
Agenda 1 Opioid Addiction in the United States 2 Evidence-based treatments for OUD OUD Treatment: Best Practices 4 Groups: Our Model 2 Groups is a national network of clinics providing affordable, evidencebased
Medication-Assisted Treatment & Pregnancy. Dave Kneessy, MS, MAC, CAP, LMHC Regional Director Central Florida Treatment Centers
 Medication-Assisted Treatment & Pregnancy Dave Kneessy, MS, MAC, CAP, LMHC Regional Director Central Florida Treatment Centers Addiction/ Substance Use Disorder Addiction is a Biopsychosocial Disease Has
Medication-Assisted Treatment & Pregnancy Dave Kneessy, MS, MAC, CAP, LMHC Regional Director Central Florida Treatment Centers Addiction/ Substance Use Disorder Addiction is a Biopsychosocial Disease Has
Disclosures. Objectives 2/5/2018. Women and opioid use disorder: Optimizing care during pregnancy and beyond
 Women and opioid use disorder: Optimizing care during pregnancy and beyond Susanne Astrab Fogger, DNP, PMHNP-BC, CARN-AP, FAANP Ashley L. Hodges, PhD, CRNP, WHNP-BC Disclosures Dr. Fogger has nothing to
Women and opioid use disorder: Optimizing care during pregnancy and beyond Susanne Astrab Fogger, DNP, PMHNP-BC, CARN-AP, FAANP Ashley L. Hodges, PhD, CRNP, WHNP-BC Disclosures Dr. Fogger has nothing to
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Opioid Step Policy. Description. Section: Prescription Drugs Effective Date: April 1, 2018
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Opioid Step Policy Page: 1 of 6 Last Review Date: March 16, 2018 Opioid Step Policy Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Opioid Step Policy Page: 1 of 6 Last Review Date: March 16, 2018 Opioid Step Policy Description
Methadone and Pregnancy
 Methadone and Pregnancy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Charissa Patricelli, MD, CCFP, ABAM Clinical Associate Professor, Dept. of Family Practice UBC American Board of Addiction Medicine
Methadone and Pregnancy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Charissa Patricelli, MD, CCFP, ABAM Clinical Associate Professor, Dept. of Family Practice UBC American Board of Addiction Medicine
Learning Objectives. Serving Pregnant Women Affected by Substance Use Disorders in Healing to Wellness Court: Sharing Lessons
 Serving Pregnant Women Affected by Substance Use Disorders in Healing to Wellness Court: Sharing Lessons Marianna Corona Jennifer Foley September 12, 2017 Learning Objectives 2017 Improving Family Outcomes
Serving Pregnant Women Affected by Substance Use Disorders in Healing to Wellness Court: Sharing Lessons Marianna Corona Jennifer Foley September 12, 2017 Learning Objectives 2017 Improving Family Outcomes
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opioid Use in Pregnant Women and Prenatal Care. Murray F Dweck MD, FACOG Medical Director/OBGYN Florida Department of Health -Brevard
 Opioid Use in Pregnant Women and Prenatal Care Murray F Dweck MD, FACOG Medical Director/OBGYN Florida Department of Health -Brevard Objectives Summarize contextual and co-morbid factors observed among
Opioid Use in Pregnant Women and Prenatal Care Murray F Dweck MD, FACOG Medical Director/OBGYN Florida Department of Health -Brevard Objectives Summarize contextual and co-morbid factors observed among
Beyond Birth: A Comprehensive Recovery Center serving parenting women
 Beyond Birth: A Comprehensive Recovery Center serving parenting women Session Objectives Highlight Plan of Safe Care Introduce the Beyond Birth Comprehensive Recovery Center Describe Levels of Care The
Beyond Birth: A Comprehensive Recovery Center serving parenting women Session Objectives Highlight Plan of Safe Care Introduce the Beyond Birth Comprehensive Recovery Center Describe Levels of Care The
Opioid Use and Other Trends
 Opioid Use and Other Trends National Overview Across the nation communities are struggling with a devastating increase in the number of people misusing opioid drugs, leading many to identify the current
Opioid Use and Other Trends National Overview Across the nation communities are struggling with a devastating increase in the number of people misusing opioid drugs, leading many to identify the current
Pregnancy, Opioid Addiction, and Care Issues in Virginia
 Pregnancy, Opioid Addiction, and Care Issues in Virginia Mishka Terplan MD MPH FACOG FASAM Professor Departments Obstetrics and Gynecology and Psychiatry Associate Director Addiction Medicine Virginia
Pregnancy, Opioid Addiction, and Care Issues in Virginia Mishka Terplan MD MPH FACOG FASAM Professor Departments Obstetrics and Gynecology and Psychiatry Associate Director Addiction Medicine Virginia
Texas Strategies to Address the Opioid Crisis and Neonatal Abstinence Syndrome
 Texas Strategies to Address the Opioid Crisis and Neonatal Abstinence Syndrome 1 Learning Objectives Become familiar with how the opioid epidemic is impacting Texas women Become familiar with Neonatal
Texas Strategies to Address the Opioid Crisis and Neonatal Abstinence Syndrome 1 Learning Objectives Become familiar with how the opioid epidemic is impacting Texas women Become familiar with Neonatal
9/19/13. Postpartum Counseling for Women in MAT. Katie Clark MSPH, CSAC. A little about Katie. Definitions. MAT: Medication-Assisted Treatment
 Postpartum Counseling for Women in MAT Katie Clark MSPH, CSAC A little about Katie SUD and PH crossroads BA Health Arts and Sciences Goddard College MSPH MCH UNC Project Lazarus, Yale, CHER Solutions LLC
Postpartum Counseling for Women in MAT Katie Clark MSPH, CSAC A little about Katie SUD and PH crossroads BA Health Arts and Sciences Goddard College MSPH MCH UNC Project Lazarus, Yale, CHER Solutions LLC
Johann Hari. Truths 2/29/2016. From the street to the NICU. Treatment works
 From the street to the NICU Richard Christensen, PA, CAS Johann Hari Treatment works Truths Disconnect with pregnant women seeking treatment Disconnect between community and science Medication is not a
From the street to the NICU Richard Christensen, PA, CAS Johann Hari Treatment works Truths Disconnect with pregnant women seeking treatment Disconnect between community and science Medication is not a
Medication for the Treatment of Addiction (MAT)
") Medication for the Treatment of Addiction (MAT) Karol Kaltenbach, PhD Emeritus Professor of Pediatrics Sidney Kimmel Medical College at Thomas Jefferson University Terminology: Words Matter Medication
Medication for the Treatment of Addiction (MAT) Karol Kaltenbach, PhD Emeritus Professor of Pediatrics Sidney Kimmel Medical College at Thomas Jefferson University Terminology: Words Matter Medication
PRESCRIPTION DRUG ABUSE: THE NATIONAL PERSPECTIVE
 PRESCRIPTION DRUG ABUSE: THE NATIONAL PERSPECTIVE September 20, 2013 Association of State and Territorial Health Officials Annual Meeting R. Gil Kerlikowske Director of National Drug Control Policy National
PRESCRIPTION DRUG ABUSE: THE NATIONAL PERSPECTIVE September 20, 2013 Association of State and Territorial Health Officials Annual Meeting R. Gil Kerlikowske Director of National Drug Control Policy National
8/24/2015 ADDICTION AND PREGNANCY. Fear ADDICTION & PREGNANCY ADDICTION & PREGNANCY ADDICTION & PREGNANCY ADDICTION & PREGNANCY ADDICTION & PREGNANCY
 ADDICTION AND PREGNANCY L y n é e B r o w n, M A, C D P & D o n n a L i v i n g s t o n, R N A D A P T E D F R O M J i m W a l s h, M D Objectives: Recognize common fears and myths associated with substance
ADDICTION AND PREGNANCY L y n é e B r o w n, M A, C D P & D o n n a L i v i n g s t o n, R N A D A P T E D F R O M J i m W a l s h, M D Objectives: Recognize common fears and myths associated with substance
SW OREGON OPIOID SUMMIT. Medication Assisted Recovery for Opioid Use Disorder. Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass
 SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
Patient and Family Agreement on Opioids
 Patient and Family Agreement on Opioids We care about our patients and are committed to their recovery and wellness. We offer our patients medications and options for various services to keep them from
Patient and Family Agreement on Opioids We care about our patients and are committed to their recovery and wellness. We offer our patients medications and options for various services to keep them from
Pragmatic and Creative Responses to the Opioid Crisis in Connecticut
 Focusing on Highly Vulnerable Populations Track Pragmatic and Creative Responses to the Opioid Crisis in Connecticut A special thanks to our presenting sponsor: Presenters: Shawn Lang Deputy Director AIDS
Focusing on Highly Vulnerable Populations Track Pragmatic and Creative Responses to the Opioid Crisis in Connecticut A special thanks to our presenting sponsor: Presenters: Shawn Lang Deputy Director AIDS
FDA s Response to the Opioid Crisis and the FDA Safe Use Initiative
 FDA s Response to the Opioid Crisis and the FDA Safe Use Initiative Scott K. Winiecki, MD Professional Affairs and Stakeholder Engagement Staff (PASES) Center For Drug Evaluation and Research (CDER) U.S.
FDA s Response to the Opioid Crisis and the FDA Safe Use Initiative Scott K. Winiecki, MD Professional Affairs and Stakeholder Engagement Staff (PASES) Center For Drug Evaluation and Research (CDER) U.S.
Objectives. Care of the Neonate with Prenatal Opioid Exposure. What is Neonatal Abstinence Syndrome (NAS)? Increasing Incidence of NAS 8/27/2016
? Increasing Incidence of NAS 8/27/2016") Care of the Neonate with Prenatal Opioid Exposure Heather Pratt Chavez, MD Ann Winegardner, MD Objectives Review the latest population data on neonates with prenatal opioid exposure Describe the acute
Care of the Neonate with Prenatal Opioid Exposure Heather Pratt Chavez, MD Ann Winegardner, MD Objectives Review the latest population data on neonates with prenatal opioid exposure Describe the acute
PREVENTION. Carroll County Health Department. Bureau of Prevention, Wellness and Recovery
 PREVENTION Carroll County Health Department Bureau of Prevention, Wellness and Recovery What is Prevention? Prevention is the promotion of constructive lifestyles and norms that discourage drug abuse.
PREVENTION Carroll County Health Department Bureau of Prevention, Wellness and Recovery What is Prevention? Prevention is the promotion of constructive lifestyles and norms that discourage drug abuse.
HHS Priorities and Actions to Support Treatment for Those with Opioid Use Disorder
 HHS Priorities and Actions to Support Treatment for Those with Opioid Use Disorder Brett Giroir, U.S. Department of Health and Human Services Join the conversation at #OUDTreatment #EndTheStigma Expanding
HHS Priorities and Actions to Support Treatment for Those with Opioid Use Disorder Brett Giroir, U.S. Department of Health and Human Services Join the conversation at #OUDTreatment #EndTheStigma Expanding
Successful Prevention Strategies to Address the Opioid Crises
 Successful Prevention Strategies to Address the Opioid Crises Shannon Breitzman, MSW, Principal Denver Office Lindsey Kato, MPH, CHES, Consultant Denver Office 1 LEARNING OBJECTIVES + Find out how to effectively
Successful Prevention Strategies to Address the Opioid Crises Shannon Breitzman, MSW, Principal Denver Office Lindsey Kato, MPH, CHES, Consultant Denver Office 1 LEARNING OBJECTIVES + Find out how to effectively
Prepublication Requirements
 Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Disclosures. Topics of today s training 4/24/2017. Evolving Treads in Medication Assisted Treatment. Christopher J Davis D.O.
 Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Kentucky s Strategic Action Plan. Katherine Marks, Ph.D. August 16, 2018
 Kentucky s Strategic Action Plan Katherine Marks, Ph.D. August 16, 2018 OUTLINE The state & the need The organization of a response The action plan THE STATE AND THE NEED KENTUCKY 4.4 million people 35
Kentucky s Strategic Action Plan Katherine Marks, Ph.D. August 16, 2018 OUTLINE The state & the need The organization of a response The action plan THE STATE AND THE NEED KENTUCKY 4.4 million people 35
Structured Guidance for Postpartum Retention in HIV Care
 An Approach to Creating a Safety Net for Individual Patients and for Programmatic Improvements 1. Problem statement and background: Pregnant women living with HIV (WLH) are a vulnerable population that
An Approach to Creating a Safety Net for Individual Patients and for Programmatic Improvements 1. Problem statement and background: Pregnant women living with HIV (WLH) are a vulnerable population that
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Mental and Behavioral Health
 Mental and Behavioral Health Mental Health Poor mental health is a major source of distress, disability, and social burden. In any given year, as many as one in five adults in the United States have a
Mental and Behavioral Health Mental Health Poor mental health is a major source of distress, disability, and social burden. In any given year, as many as one in five adults in the United States have a
Opioid Task Force Kick-Off Meeting. February 29, 2016
 Opioid Task Force Kick-Off Meeting February 29, 2016 Scope of the Opioid Problem and Data Review Olivia Kasirye, MD, MS County Public Health Officer OVERVIEW The Opioid Epidemic Opioid Task Force Development
Opioid Task Force Kick-Off Meeting February 29, 2016 Scope of the Opioid Problem and Data Review Olivia Kasirye, MD, MS County Public Health Officer OVERVIEW The Opioid Epidemic Opioid Task Force Development
Opioid Use Disorders and Pregnancy. Marcela Smid, MD Maternal-Fetal Medicine
 Opioid Use Disorders and Pregnancy Marcela Smid, MD Maternal-Fetal Medicine UNIVERSITY OF UTAH HEALTH, 2017 OBJECTIVES Definitions Epidemiology Pharmacology Effects on pregnancy Screening Treatment CARE
Opioid Use Disorders and Pregnancy Marcela Smid, MD Maternal-Fetal Medicine UNIVERSITY OF UTAH HEALTH, 2017 OBJECTIVES Definitions Epidemiology Pharmacology Effects on pregnancy Screening Treatment CARE
The Opiate Crisis 4/6/18. April 9, Words are important. If you want to care for something, you call it a flower.
 The Opiate Crisis Presented by Dr. Anahi Ortiz Franklin County Coroner April 9, 2018 Words are important. If you want to care for something, you call it a flower. If you want to kill something, you call
The Opiate Crisis Presented by Dr. Anahi Ortiz Franklin County Coroner April 9, 2018 Words are important. If you want to care for something, you call it a flower. If you want to kill something, you call
Neonatal Abstinence Syndrome (NAS)
") Neonatal Abstinence Syndrome (NAS) Jodi Jackson, MD Neonatologist Children's Mercy Hospital Associate Professor of Pediatrics University of Missouri-Kansas City School of Medicine Medical director NICU
Neonatal Abstinence Syndrome (NAS) Jodi Jackson, MD Neonatologist Children's Mercy Hospital Associate Professor of Pediatrics University of Missouri-Kansas City School of Medicine Medical director NICU
2004-L SEPTEMBER
 BULLETIN INTELLIGENCE Buprenorphine: Potential for Abuse Product No. 2004-L0424-013 SEPTEMBER 2004 U. S. D E P A R T M E N T O F J U S T I C E NDIC Within the past 2 years buprenorphine a Schedule III
BULLETIN INTELLIGENCE Buprenorphine: Potential for Abuse Product No. 2004-L0424-013 SEPTEMBER 2004 U. S. D E P A R T M E N T O F J U S T I C E NDIC Within the past 2 years buprenorphine a Schedule III
Progress Report and 2018 Legislative Opportunities. Maine Opiate Collaborative Recommendations
 Progress Report and 2018 Legislative Opportunities related to the Maine Opiate Collaborative Recommendations April 2018 A. Destigmatize substance use disorders within the law enforcement profession 1.
Progress Report and 2018 Legislative Opportunities related to the Maine Opiate Collaborative Recommendations April 2018 A. Destigmatize substance use disorders within the law enforcement profession 1.
Advancing the Care of Pregnant and Parenting Women with Opioid Use Disorder and their Infants: A Foundation for Clinical Guidance
 Advancing the Care of Pregnant and Parenting Women with Opioid Use Disorder and their Infants: A Foundation for Clinical Guidance Karol Kaltenbach, PhD Emeritus Professor of Pediatrics Sidney Kimmel Medical
Advancing the Care of Pregnant and Parenting Women with Opioid Use Disorder and their Infants: A Foundation for Clinical Guidance Karol Kaltenbach, PhD Emeritus Professor of Pediatrics Sidney Kimmel Medical
Addiction and Pregnancy. Jim Walsh, MD Medical Director Addiction Recovery Service Swedish Medical Center WSADCP October 2018
 Jim Walsh, MD Medical Director Addiction Recovery Service Swedish Medical Center WSADCP October 2018 Fear Shame Commitment Barriers Opportunities Fear Thalidomide induced phocomelia 1957 Fear Fetal Alcohol
Jim Walsh, MD Medical Director Addiction Recovery Service Swedish Medical Center WSADCP October 2018 Fear Shame Commitment Barriers Opportunities Fear Thalidomide induced phocomelia 1957 Fear Fetal Alcohol
Strategies for Federal Agencies
 Confronting Pain Management and the Opioid Epidemic Strategies for Federal Agencies Over the past 25 years, the United States has experienced a dramatic increase in deaths from opioid overdose, opioid
Confronting Pain Management and the Opioid Epidemic Strategies for Federal Agencies Over the past 25 years, the United States has experienced a dramatic increase in deaths from opioid overdose, opioid
MAT in the Corrections Setting
 MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
Strategies to Manage The Opioid Crisis
 Strategies to Manage The Opioid Crisis Matt Feehery, LCDC Senior Vice President & CEO PaRC (Prevention & Recovery Center) Behavioral Health Services February 1, 2018 A Pill for Your Pain But my doctor
Strategies to Manage The Opioid Crisis Matt Feehery, LCDC Senior Vice President & CEO PaRC (Prevention & Recovery Center) Behavioral Health Services February 1, 2018 A Pill for Your Pain But my doctor
Continuing Education Webinar The Pregnancy Opioid Epidemic: An Outpatient Medical Home Approach to Treatment
 Continuing Education Webinar The Pregnancy Opioid Epidemic: An Outpatient Medical Home Approach to Treatment This webinar will be recorded and available on the NPIC/QAS website www.npic.org. Nurse Planner:
Continuing Education Webinar The Pregnancy Opioid Epidemic: An Outpatient Medical Home Approach to Treatment This webinar will be recorded and available on the NPIC/QAS website www.npic.org. Nurse Planner:
Building a Comprehensive, Community-driven Prevention Approach to the Opioid Crisis in Maine
 Building a Comprehensive, Community-driven Prevention Approach to the Opioid Crisis in Maine Scott M. Gagnon, MPP, PS-C Director, AdCare Educational Institute of Maine, Inc. Co-Chair, Prevention & Harm
Building a Comprehensive, Community-driven Prevention Approach to the Opioid Crisis in Maine Scott M. Gagnon, MPP, PS-C Director, AdCare Educational Institute of Maine, Inc. Co-Chair, Prevention & Harm
Submitted to the House Energy and Commerce Committee. Federal Efforts to Combat the Opioid Crisis
 STATEMENT FOR THE RECORD Submitted to the House Energy and Commerce Committee Federal Efforts to Combat the Opioid Crisis October 25, 2017 America s Health Insurance Plans 601 Pennsylvania Avenue, NW Suite
STATEMENT FOR THE RECORD Submitted to the House Energy and Commerce Committee Federal Efforts to Combat the Opioid Crisis October 25, 2017 America s Health Insurance Plans 601 Pennsylvania Avenue, NW Suite
Smoking Cessation in Pregnancy. Jessica Reader, MD, MPH Family Medicine Obstetrics Fellow June 1st, 2018
 Smoking Cessation in Pregnancy Jessica Reader, MD, MPH Family Medicine Obstetrics Fellow June 1st, 2018 Tobacco Cessation in Pregnancy: Objective 1. Overview of the negative effects of tobacco abuse in
Smoking Cessation in Pregnancy Jessica Reader, MD, MPH Family Medicine Obstetrics Fellow June 1st, 2018 Tobacco Cessation in Pregnancy: Objective 1. Overview of the negative effects of tobacco abuse in
MOMS Project Panel Overview
 MOMS Project Panel Overview Rick Massatti, PhD, Ohio Department of Mental Health and Addiction Services Jennifer Bailit, MD, MetroHealth Medical Center Mike Marcotte, MD, Tri-Health Mona Prasad, DO,MPH,
MOMS Project Panel Overview Rick Massatti, PhD, Ohio Department of Mental Health and Addiction Services Jennifer Bailit, MD, MetroHealth Medical Center Mike Marcotte, MD, Tri-Health Mona Prasad, DO,MPH,
Maine s Response to the Opiate Crisis. Christopher Pezzullo, DO State Health Officer Maine DHHS Maine CDC November 12, 2016
 Maine s Response to the Opiate Crisis Christopher Pezzullo, DO State Health Officer Maine DHHS Maine CDC November 12, 2016 Required Disclosure Text Font typically Times New Roman at least 20 point Try
Maine s Response to the Opiate Crisis Christopher Pezzullo, DO State Health Officer Maine DHHS Maine CDC November 12, 2016 Required Disclosure Text Font typically Times New Roman at least 20 point Try
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Public Policy Statement on Substance Use, Misuse, and Use Disorders During and Following Pregnancy, with an Emphasis on Opioids
 Public Policy Statement on Substance Use, Misuse, and Use Disorders During and Following Pregnancy, with an Emphasis on Opioids Background The American Society of Addiction Medicine (ASAM) is deeply committed
Public Policy Statement on Substance Use, Misuse, and Use Disorders During and Following Pregnancy, with an Emphasis on Opioids Background The American Society of Addiction Medicine (ASAM) is deeply committed
2/21/2018. What are Opioids?
 Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Linking Opioid Treatment in Primary Care. Roxanne Lewin M.D.
 Roxanne Lewin M.D. The Facts Fewer than 10 percent of individuals with an alcohol use disorder and only about 20 percent of individuals with an opioid use disorder receive specialty treatment. Many individuals
Roxanne Lewin M.D. The Facts Fewer than 10 percent of individuals with an alcohol use disorder and only about 20 percent of individuals with an opioid use disorder receive specialty treatment. Many individuals
Emerging Populations: Challenges for the Early Childhood System. Presented by Maureen Greer
 Emerging Populations: Challenges for the Early Childhood System Presented by Maureen Greer Early Intervention/Early Childhood Special Interest Group (EIEC SIG) Webinar Series September 26, 2017 Presenter
Emerging Populations: Challenges for the Early Childhood System Presented by Maureen Greer Early Intervention/Early Childhood Special Interest Group (EIEC SIG) Webinar Series September 26, 2017 Presenter
Maternal and Child Health, Substance Abuse Ohio Department of Health, Bureau of Maternal Child and Family Health
 Maternal and Child Health, Substance Abuse Ohio Department of Health, Bureau of Maternal Child and Family Health Columbus, Ohio Assignment Description The rapid advance of the opiate crisis has had far
Maternal and Child Health, Substance Abuse Ohio Department of Health, Bureau of Maternal Child and Family Health Columbus, Ohio Assignment Description The rapid advance of the opiate crisis has had far
From Medicaid Transformation Approved Project Toolkit, June 2017
 From Medicaid Transformation Approved Project Toolkit, June 2017 Domain 3: Prevention and Health Promotion Transformation projects within this domain focus on prevention and health promotion to eliminate
From Medicaid Transformation Approved Project Toolkit, June 2017 Domain 3: Prevention and Health Promotion Transformation projects within this domain focus on prevention and health promotion to eliminate
6/6/2017. First Do No Harm SECTION 1 THE OPIOID CRISIS. Implementing an Opioid Stewardship Program in a HealthCare System OBJECTIVES
 First Do No Harm Implementing an Opioid Stewardship Program in a HealthCare System Phil Chang, MD Kristy Deep, MD Doug Oyler, PharmD June 12, 2017 OBJECTIVES Explain the role of opioid stewardship as a
First Do No Harm Implementing an Opioid Stewardship Program in a HealthCare System Phil Chang, MD Kristy Deep, MD Doug Oyler, PharmD June 12, 2017 OBJECTIVES Explain the role of opioid stewardship as a
REDUCING THE STIGMA OF OPIOID ADDICTION AMONG PERINATAL WOMEN. Lyn Raible, M.D., Ph.D. CMO, Aegis
 REDUCING THE STIGMA OF OPIOID ADDICTION AMONG PERINATAL WOMEN Lyn Raible, M.D., Ph.D. CMO, Aegis ORGANIZATION The Opioid Crisis Breaking the Stigma Neurobiology of Opioid Addiction Treatment of Opioid
REDUCING THE STIGMA OF OPIOID ADDICTION AMONG PERINATAL WOMEN Lyn Raible, M.D., Ph.D. CMO, Aegis ORGANIZATION The Opioid Crisis Breaking the Stigma Neurobiology of Opioid Addiction Treatment of Opioid
Opioid Dependence and Buprenorphine Management
 Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
Implementing the 2017 President s Challenge: Primary, Secondary & Tertiary Prevention of Addiction & Substance Misuse
 Implementing the 2017 President s Challenge: Primary, Secondary & Tertiary Prevention of Addiction & Substance Misuse Jay Butler, MD, President of ASTHO, Chief Medical Officer, Alaska Department of Health
Implementing the 2017 President s Challenge: Primary, Secondary & Tertiary Prevention of Addiction & Substance Misuse Jay Butler, MD, President of ASTHO, Chief Medical Officer, Alaska Department of Health
SUBSTANCE EXPOSED NEWBORNS
 Substance Exposed Newborns 1 SUBSTANCE EXPOSED NEWBORNS STATE OF OKLAHOMA 2012 2 Substance Exposed Newborns The mission of the Oklahoma Department of Human Services is to help individuals and families
Substance Exposed Newborns 1 SUBSTANCE EXPOSED NEWBORNS STATE OF OKLAHOMA 2012 2 Substance Exposed Newborns The mission of the Oklahoma Department of Human Services is to help individuals and families
Anesthetics, Local a / or Anesthesia, Epidural a / or Anesthesia, Obstetrical a / or Pain, Postoperative a / or Postpartum Period a
 Appendix 1. Literature Search Databases Years Search Terms Pubmed 01/1966 1. Analgesics, Opioid a / or Opioid-related Disorders a / PsycINFO EMBASE Cochrane 09/2016 or Heroin a / or Heroin Dependence a
Appendix 1. Literature Search Databases Years Search Terms Pubmed 01/1966 1. Analgesics, Opioid a / or Opioid-related Disorders a / PsycINFO EMBASE Cochrane 09/2016 or Heroin a / or Heroin Dependence a
Addressing Substance Abuse To Improve Well-Being in Child Welfare Systems Current Trends, Continuing Challenges
 Addressing Substance Abuse To Improve Well-Being in Child Welfare Systems Current Trends, Continuing Challenges Three Branch Institute on Child Well-Being July 1, 2014 Sid Gardner, MPA Drugs of the Decades
Addressing Substance Abuse To Improve Well-Being in Child Welfare Systems Current Trends, Continuing Challenges Three Branch Institute on Child Well-Being July 1, 2014 Sid Gardner, MPA Drugs of the Decades
The Prescription Opioid and Heroin Crisis
 The Prescription Opioid and Heroin Crisis Dr. Rachel L. Levine Acting Secretary of Health and Physician General Professor of Pediatrics and Psychiatry Penn State College of Medicine Overdose deaths from
The Prescription Opioid and Heroin Crisis Dr. Rachel L. Levine Acting Secretary of Health and Physician General Professor of Pediatrics and Psychiatry Penn State College of Medicine Overdose deaths from
QUARTERLY PROVIDER MEETING MARCH 9, 2017 SUZANNE BORYS, ED.D.
 2017 State Targeted Response to the Opioid Crisis Grants QUARTERLY PROVIDER MEETING MARCH 9, 2017 SUZANNE BORYS, ED.D. H.R.6-21st Century Cures Act The 21st Century Cures Act is a United States law enacted
2017 State Targeted Response to the Opioid Crisis Grants QUARTERLY PROVIDER MEETING MARCH 9, 2017 SUZANNE BORYS, ED.D. H.R.6-21st Century Cures Act The 21st Century Cures Act is a United States law enacted
Effective Strategies for Addressing the Needs of Substance Exposed Newborns & their Families Dixie L. Morgese, BA, CAP, ICADC.
 Effective Strategies for Addressing the Needs of Substance Exposed Newborns & their Families Dixie L. Morgese, BA, CAP, ICADC Key Issues Significant increase in number of pregnant women addicted to prescription
Effective Strategies for Addressing the Needs of Substance Exposed Newborns & their Families Dixie L. Morgese, BA, CAP, ICADC Key Issues Significant increase in number of pregnant women addicted to prescription
Opioid epidemic and PEHP
 Opioid epidemic and PEHP Agenda Overview of opioid crisis Utah perspective PEHP: clinical interventions Impact of interventions Why are we here? In the 1990s, the medical establishment came to believe
Opioid epidemic and PEHP Agenda Overview of opioid crisis Utah perspective PEHP: clinical interventions Impact of interventions Why are we here? In the 1990s, the medical establishment came to believe
9/5/2011. Outline. 1. Past and Current Trends re: RX Abuse 2. Diversion Methods 3. Regulatory Reporting Requirements 4. Q/A
 Prescription Drug Abuse Crises Outline 1. Past and Current Trends re: RX Abuse 2. Diversion Methods 3. Regulatory Reporting Requirements 4. Q/A 1 1970s 1980s 2 The 1990s OXYCODONE Oxycodone/APAP OxyContin
Prescription Drug Abuse Crises Outline 1. Past and Current Trends re: RX Abuse 2. Diversion Methods 3. Regulatory Reporting Requirements 4. Q/A 1 1970s 1980s 2 The 1990s OXYCODONE Oxycodone/APAP OxyContin
Opioid Use Disorder in Pregnancy. Neonatal Abstinence Syndrome
 Opioid Use Disorder in Pregnancy Neonatal Abstinence Syndrome Opioid Use Disorder and Pregnancy Cont. 4.6 million women (or 3.8 percent) ages 18 and older misused prescription drugs in 2013. One-third
Opioid Use Disorder in Pregnancy Neonatal Abstinence Syndrome Opioid Use Disorder and Pregnancy Cont. 4.6 million women (or 3.8 percent) ages 18 and older misused prescription drugs in 2013. One-third
The Role of Dentists in Preventing Opioid Abuse Tufts Health Care Institute Program on Opioid Risk Management 12 th Summit Meeting March 11-12, 2010
 The Role of Dentists in Preventing Opioid Abuse Tufts Health Care Institute Program on Opioid Risk Management 12 th Summit Meeting March 11-12, 2010 EXECUTIVE SUMMARY It is well documented in multiple
The Role of Dentists in Preventing Opioid Abuse Tufts Health Care Institute Program on Opioid Risk Management 12 th Summit Meeting March 11-12, 2010 EXECUTIVE SUMMARY It is well documented in multiple
Opioid Use Disorder- Pregnancy Principles and Myths. Brian Iriye MD and Farzad Kamyar MD High Risk Pregnancy Center
 Opioid Use Disorder- Pregnancy Principles and Myths Brian Iriye MD and Farzad Kamyar MD High Risk Pregnancy Center History of NAS/NOWS Prior to 1875 infants not thought to be affected Congenital Morphinism
Opioid Use Disorder- Pregnancy Principles and Myths Brian Iriye MD and Farzad Kamyar MD High Risk Pregnancy Center History of NAS/NOWS Prior to 1875 infants not thought to be affected Congenital Morphinism
Care of the Neonate with Prenatal Opioid Exposure. Objectives. What is Neonatal Abstinence Syndrome (NAS)/ Neonatal Opiate Withdrawal Syndrome?
/ Neonatal Opiate Withdrawal Syndrome?") Care of the Neonate with Prenatal Opioid Exposure Heather Pratt Chavez, MD Ann Winegardner, MD Objectives Review the latest population data on neonates with prenatal opioid exposure Describe the acute
Care of the Neonate with Prenatal Opioid Exposure Heather Pratt Chavez, MD Ann Winegardner, MD Objectives Review the latest population data on neonates with prenatal opioid exposure Describe the acute
What is the strategy?
 What is the strategy? Multi-pronged approaches to reducing the health consequences of opioid use, New York City Northeast Epidemiology Conference Public health approach Track drug use and associated health
What is the strategy? Multi-pronged approaches to reducing the health consequences of opioid use, New York City Northeast Epidemiology Conference Public health approach Track drug use and associated health
Table of Contents Interim Report of the OxyContin Task Force, Newfoundland & Labrador, January 30, 2004
 OXYCONTIN TASK FORCE INTERIM REPORT January 30, 2004 Submitted to Hon. Elizabeth Marshall, Minister of Health & Community Services, Government of Newfoundland and Labrador Table of Contents INTRODUCTION
OXYCONTIN TASK FORCE INTERIM REPORT January 30, 2004 Submitted to Hon. Elizabeth Marshall, Minister of Health & Community Services, Government of Newfoundland and Labrador Table of Contents INTRODUCTION
Building capacity for a CHC response to Ontario's Opioid Crisis
 Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
FY17 SCOPE OF WORK TEMPLATE. Name of Program/Services: Medication-Assisted Treatment: Buprenorphine
 FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
Fighting Today s Opioid Epidemic
 Fighting Today s Opioid Epidemic Establish in 1966 as a Public Health Department Location: Rock Falls, IL/Whiteside County Population: Whiteside County 2015--57,079 Serving Rural IL: Primarily Whiteside,
Fighting Today s Opioid Epidemic Establish in 1966 as a Public Health Department Location: Rock Falls, IL/Whiteside County Population: Whiteside County 2015--57,079 Serving Rural IL: Primarily Whiteside,
Opioid Overdose in Oregon Report to the Legislature
 SEPTEMBER 2018 Opioid Overdose in Oregon Report to the Legislature This report summarizes the burden of opioid overdose among Oregonians as required by ORS 432.141. It describes Oregon s progress in reducing
SEPTEMBER 2018 Opioid Overdose in Oregon Report to the Legislature This report summarizes the burden of opioid overdose among Oregonians as required by ORS 432.141. It describes Oregon s progress in reducing
Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention
 The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
Opioid Addiction Statistics
 May 2017 Opioid Addiction Statistics Definitions Heroin Epidemic - As pill mills close, prescribing is becoming tighter, demand among younger users rise, and dealer s profits rise, addicts are turning
May 2017 Opioid Addiction Statistics Definitions Heroin Epidemic - As pill mills close, prescribing is becoming tighter, demand among younger users rise, and dealer s profits rise, addicts are turning