Dean Olsen, DO Director, Medical Education and Emergency Medicine Residency Nassau University Medical Center Faculty, New York City Poison Control
|
|
|
- Horace Conley
- 5 years ago
- Views:
Transcription


1 Dean Olsen, DO Director, Medical Education and Emergency Medicine Residency Nassau University Medical Center Faculty, New York City Poison Control Center Professor, Toxicology NYIT College of Osteopathic Medicine 1
2 Financial None Conflicts of interest None

3 Define and characterize agitated delirium Identify patients with agitated delirium Understand the complications of agitated delirium Review the data on pharmacologic management of excited delirium Develop a stepwise approach for treatment
4 Excited (or agitated) delirium is characterized by agitation, aggression, acute distress and sudden death Patients are unaware of their surroundings A transient disorder with impairment of attention and cognition. The patient has difficulty focusing, shifting, or sustaining attention. Confusion may fluctuate





5
6 Excited delirium first described in the mid 1800 s Bell s mania Lethal catatonia Acute exhaustive mania Agitated delirium Described first in psychiatric patients Mania Fever Death 75% mortality Sequence of events delirium with agitation (fear, panic, shouting, violence and hyperactivity), sudden cessation of struggle, respiratory arrest and death

7 ACEP Excited Delirium Task Force White. 2009

8 ACEP Excited Delirium Task Force White. 2009
9 Sudden unexpected death is the hallmark of fatal excited delirium. Multiple theories Increased catecholamine levels Increased serotonin levels Increased dopamine levels Hyperthermia Stress cardiomyopathy Arrhythmia / Long QT Positional asphyxia


10 Average Body Temperature 105.2F Forensic Sci Int Sep 10;190(1-3):e13-9.
11 Sudden death Associated with multiple predictable but usually uncontrollable factors Many die at scene and probably can not be saved If they get to the ED alive, don t kill them Respiratory Depression Almost always the result of the treatment

12 Restriction of breathing due to improper positioning of restrained patient SIDS Contributory in sudden death of excited delirium

13


14
15 Psychiatric [Functional] Non-psychiatric [Organic] Medical Toxicologic Approximately 2/3 have organic etiology
16 The most common cause of agitation prehospital and in the ED is drug/alcohol use.
17 Stimulant and Psychostimulant use- drugs that alter dopamine processing, and temperature regulation Alcohol Alcohol withdrawal Cocaine Amphetamines Phencyclodine (PCP) Designer amphetamines Xtc Bath salts Synthetic cannabinoids LSD Anticholinergics

18 Intracranial bleeding Meningitis / encephalitis Stroke Thyroid Storm Hypoglycemia Hypoxia Shock
19 Marzuk P, et al. JAMA. 1998;279:

20 20

21 21
22
 Observation Serial assessment Thanks Bob Hoffman, MD")
23 Restraint (physical and chemical) Oxygen Dextrose Examinations (physical, Temperature, labs ECG) Observation Serial assessment Thanks Bob Hoffman, MD NYCPCC
24 Poorly studied Selection bias Most not representative of true excited delirium Unclear pharmacology Imperfect endpoints Safety monitoring less then perfect
25 Time to sedation? Or Time to rectal temperature Time to iv access Time to fingerstick glucose Time to ecg Time to proper monitoring
26
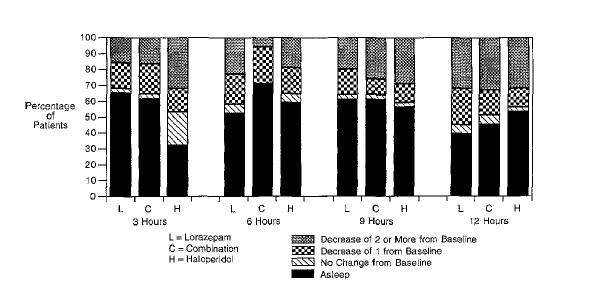
27 Largest blinded study to date (1997) on combination intramuscular Ativan / Haldol therapy in the emergency department Included all patients with psychosis Used multiple doses of both drugs alone and in combination Concluded that combination therapy is more effective than either alone
28
29
30 Problems Excluded all patients with ethanol Excluded patients with delirium!! No objective evaluation of agitated patients Authors used a psychiatric rating scale A minority of patients (10%) had stimulant abuse (not confirmed) Most patients had schizophrenia Long sedation times This was really a study of psychosis patients NOT excited / agitated delirium
31 Lorazepam (Ativan) is should be avoided in intoxicated patients Pharmacodynamics make this drug high risk for use in patients who are intoxicated 15 min peak effect 1-3 min peak effect with midazolam
32 Randomized blinded study of IM administration 5mg Droperidol vs 5mg Midazolam vs 20mg Ziprasidone Primary endpoint was time to sedation Secondary endpoints Disposition Need for rescue medication / additional sedation
33
34 Midazolam sedated patients faster Midazolam patients woke up faster Ziprasidone patients took longer to sedate and remained sedated longer
35 Conclusion more patients remained agitated at 15 minutes with ziprasidone relative to the other agents, and patients receiving midazolam more frequently required additional sedation Population all alcohol intoxication (90%) 1/3 with head injury No temperature Stimulant use underrepresented No QT monitoring No data on dose equivalency Not convinced authors have a clear focus on consequential factors
36 Ann Emerg Med 2006; 47: Double blind trial Midazolam vs Droperidol 5mg intravenous Repeated q5min till sedation Primary outcome time to sedation Secondary outcomes Need for subsequent sedation QT
37
38
39
40
41 Conclusions Midazolam sedated more people at 5 min Drugs are equal at 10 min Midazolam produced a little more respiratory depression Problems No information on baseline agitation No baseline agitation score No temperature Not powered to determine safety

42 Ann Emerg Med. 2010; 56: Randomized blinded study IM therapy 10mg of single agent or 5+5 combo Primary endpoint -time to sedation Secondary endpoints time to additional medication, oxygen desaturation [90%], airway obstruction requiring intervention tracheal intubation cardiac arrhythmias prolonged QT interval, hypotension, extrapyramidal side effects
43
44
45
46 No Adverse Event Adverse Event
47 Time to sedation similar for midazolam and Droperidol Drug related adverse events higher in Midazolam group and sedation times are shorter midazolam, particularly through the intramuscular route, has unpredictable effects and a high rate of adverse reactions in this setting. Basically they are telling us if you give benzos to people who are intoxicated they have airway related events
48 This is mostly a study of belligerent intoxicated patients (75% midaz group) Alcohol intoxicated vs alcohol related Stimulant abuse underrepresented No information on baseline agitation No baseline agitation score No temperature How well does this represent our population? Not powered to determine safety To study adverse event that occurs 1 in 50 would have to have sample size of several hundred
 + droperidol (5mg) intravenous vs. Midazolam + Olanzapine (5mg) Intravenous vs. Midazolam (2.")
49 Ann Emerg Med 2013; 61: Double blind study Midazolam (2.5-5mg) + droperidol (5mg) intravenous vs. Midazolam + Olanzapine (5mg) Intravenous vs. Midazolam (2.5-5mg) alone Primary outcome Time to sedation Proportion of patients sedated at 5 and 10 min Secondary outcome Need for additional drugs Need of re-sedation at and after 60 min Total midazolam dose Qt and adverse events
50
51
52 2 drugs worked faster than one drug of the same dose Droperidol and olanzapine equal at 5 and 10 min Midazolam alone and with droperidol produced slightly more adverse events ECG s were on only gotten on slightly more than half of the patients so we cant say much about qt Data on change of qt not provided
53 No information on baseline agitation No baseline agitation score No temperature Used a small dose of midazolam Many patients were triaged as non critical Long times between triage and when seen by provider No data on qt issue Safety can not be determined
 vs mono therapy of antipsychotics intravenous (10mg) Repeat")
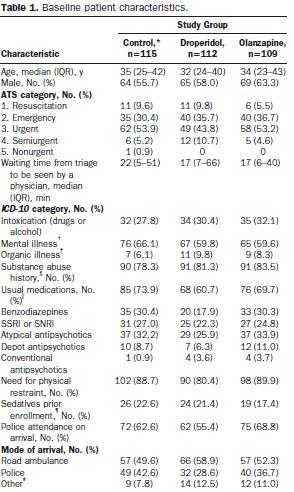
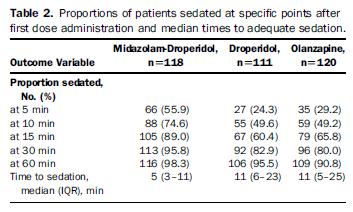
54 [Ann Emerg Med. 2016;-:1-9.] Randomized controlled double blinded trial Combination therapy midazolam-droperidol (5mg/5mg) vs mono therapy of antipsychotics intravenous (10mg) Repeat doses were given Primary endpoint- proportion of patients sedated at 10 min Secondary endpoints Time to sedation Need for more sedation QT
55
56
57
58 Combination drug therapy more effective at rapid sedation and less need for repeat dosing Problems No information on baseline agitation No baseline agitation score No temperature EKG s only done on half the patients No dose equivalency data Long triage times
59

60 [Ann Emerg Med. 2015;66: ] Prospective observational study looking at QT and efficacy of droperidol Over 1000 patients 13 abnormal QT s No torsades de pointes Sampling bias Underpowered to determine association between droperidol and TDP
61 Lower seizure threshold Interfere with the ability to dissipate heat QT prolongation Not good for head injuries Can worsen arrhythmias
62 This is difficult to study rigorously Data are lacking There is more than 1 way to skin a cat Haldol and Ativan has not been studied in agitated delirium Benzos and antipsychotics work either alone or when used together Midazolam works faster All agitated patients are not the same Belligerent alcoholic Psych patient who is haldolopenic Stimulant abuse / etoh withdrawal Newer antipsychotics have not been shown to offer any clear benefit over older ones Benzos + alcohol = respiratory depression
63 Dissociative medication No respiratory depression Problems: Causes catecholamine release Can worsen psychosis


64
65 Ketamine sedation is effective and safe in agitated patients with a psychiatric illness in the aeromedical setting and does not lead to worsening agitation in the subsequent 72-h period. (Emerg Med J 2012;29:335) Article didn t look at excited delirium Retrospective Has nothing to do with excited delirium

66 Case Report Review of Ref 4 Review Case Series Case Report Case Report

67 Unblinded retrospective chart review of paramedic runs where ketamine was used for sedation 53 patients given 4mg/kg IM No baseline characteristics of patients Little information on what happened in the ED with this population Very low quality data [West J Emerg Med. 2014;15(7): ]
:556-62 Prospective observational study unblinded 5mg/kg ketamine IM vs Haldol 10mg IM Primary")
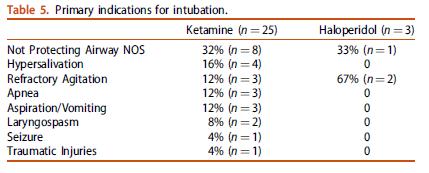
68 Clin Toxicol (Phila) Aug;54(7): Prospective observational study unblinded 5mg/kg ketamine IM vs Haldol 10mg IM Primary Outcome Time to sedation Secondary outcomes Need for repeat dosing Adverse effects Intubation

69 Mean time to sedation Ketamine 5 min Haldol 17 min Adverse Events Ketamine 49% Haldol 5% Intubations Ketamine 39% Haldol 4%
70
71 Ketamine worked faster Almost half of Ketamine patients had adverse events 40% wound up intubated Problems Doses were not equivalent Minority of patients had stimulant use Patients were not severely agitated

72 Data are insufficient to recommend ketamine alone or in combination with other agents at this time in undifferentiated excited delirium Be careful of people who try to suggest otherwise
73 Haloperidol / Lorazepam Haloperidol / Lorazepam / Diphenhydramine Never studied in severe agitation Make little pharmacological sense Admission of a lack of understanding
74 Can you tell the difference between: Psychiatric agitation Cocaine intoxication Alcohol intoxication Alcohol withdrawal
75
76 2/3 die at the scene or during transport by paramedics or police >80% involve alcohol Must direct treatment strategy
 Observation Serial assessment Thanks Bob Hoffman, MD")
77 Restraint (physical and chemical) Oxygen Dextrose Examinations (physical, Temperature, labs ECG) Observation Serial assessment Thanks Bob Hoffman, MD NYCPCC
78 Supine positon Handcuffed Butterfly net or mesh bag Patient may then be rolled to the side facing away from provider to obtain IV Vein in forearm accessible in handcuffed patients

79 Ease and safety vs guaranteed absorption These patients all need IV access anyway Sometimes must start with IM
80 Rapid onset Rapid Peak Rapid offset No prerequisite Safe in undifferentiated cases

81 1. Stimulant or psychostimulant Intoxicated 2. Belligerent alcoholic patient 3. Noncompliant psychiatric patient 4. Agitated and none of the above
82 Psychotic or emotional Antipsychotic Cocaine / amphetamine / psychostimulant / ethanol withdrawal Benzodiazepine Alcohol Intoxication Antipsychotic or maybe ketamine Unknown- Keep it safe Benzodiazepine Dose Midazolam 10mg Haldol 5-10 mg Diazepam 20
83 Agitated delirium can be fatal Drugs and alcohol are a common cause complicating pharmacological management Hyperthermia is common Properly restrain patients Not all agitated patients are the same Tailor your drug therapy to the etiology When you don t know, benzos are probably safest to use

84 Questions Ecstasy causes SIADH Check serum sodium before hydrating these patients If you need help- call the poison center 84
What the s wrong with this person?
 Ketamine for Prehospital Management of Excited Delirium Syndrome: Is it all just a bunch of hype?!? Financial Disclosure Asa M. Margolis, DO, MPH, MS, FACEP Assistant Professor Division of Special Operation
Ketamine for Prehospital Management of Excited Delirium Syndrome: Is it all just a bunch of hype?!? Financial Disclosure Asa M. Margolis, DO, MPH, MS, FACEP Assistant Professor Division of Special Operation
Excited Delirium. Objectives. Case 4/28/2015
 Excited Delirium Patrick Cody, DO, MPH, FACOEP Norman Regional Health System Objectives Review the history of Excited Delirium Syndrome (ExDS) Understand the diagnostic features of this disease Review
Excited Delirium Patrick Cody, DO, MPH, FACOEP Norman Regional Health System Objectives Review the history of Excited Delirium Syndrome (ExDS) Understand the diagnostic features of this disease Review
Management of Severe Agitation
 Management of Severe Agitation Key Points 1. The management of the severely agitated or violent patient embraces psychological, physical and pharmacological approaches. 2. Psychological methods focus on
Management of Severe Agitation Key Points 1. The management of the severely agitated or violent patient embraces psychological, physical and pharmacological approaches. 2. Psychological methods focus on
Management of the Agitated and Violent ED Patient. Lauren Klein, MD, MS Faculty Physician Hennepin County Medical Center Minneapolis, Minnesota
 Management of the Agitated and Violent ED Patient Lauren Klein, MD, MS Faculty Physician Hennepin County Medical Center Minneapolis, Minnesota Conflicts of Interest None A brief preamble Is agitation and
Management of the Agitated and Violent ED Patient Lauren Klein, MD, MS Faculty Physician Hennepin County Medical Center Minneapolis, Minnesota Conflicts of Interest None A brief preamble Is agitation and
Introduction to Emergency Medical Care 1
 Introduction to Emergency Medical Care 1 OBJECTIVES 25.1 Define key terms introduced in this chapter. Slides 13, 36 37 25.2 Recognize behaviors that are abnormal in a given context. Slide 13 25.3 Discuss
Introduction to Emergency Medical Care 1 OBJECTIVES 25.1 Define key terms introduced in this chapter. Slides 13, 36 37 25.2 Recognize behaviors that are abnormal in a given context. Slide 13 25.3 Discuss
Keep Calm and Carry On Management of the Agitated Patient in the ED 29TH ANNUAL UPDATE IN EMERGENCY MEDICINE FEBRUARY 21-24, 2016
 Keep Calm and Carry On Management of the Agitated Patient in the ED 29TH ANNUAL UPDATE IN EMERGENCY MEDICINE FEBRUARY 21-24, 2016 Dr. Jeffrey Tyberg Sunnybrook Health Sciences Centre University of Toronto
Keep Calm and Carry On Management of the Agitated Patient in the ED 29TH ANNUAL UPDATE IN EMERGENCY MEDICINE FEBRUARY 21-24, 2016 Dr. Jeffrey Tyberg Sunnybrook Health Sciences Centre University of Toronto
Psychopharmacology in the Emergency Room. Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan
 Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan Pretest 1. Which of the following conditions is LEAST likely to benefit from emergency
Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan Pretest 1. Which of the following conditions is LEAST likely to benefit from emergency
Care of the Acutely Agitated Patient. Objectives. Agitation Defined
 Care of the Acutely Agitated Patient James C. Hardy, MD Assistant Professor of Emergency Medicine Department of Emergency Medicine, UCSF Dealing with combative patients is one of the most difficult challenges
Care of the Acutely Agitated Patient James C. Hardy, MD Assistant Professor of Emergency Medicine Department of Emergency Medicine, UCSF Dealing with combative patients is one of the most difficult challenges
Emergency Care 3/9/15. Multimedia Directory. Topics. Emergency Care for Behavioral and. Psychiatric Emergencies CHAPTER
 Emergency Care THIRTEENTH EDITION CHAPTER 23 Behavioral and Psychiatric Emergencies and Suicide Multimedia Directory Slide 42 Applications of Mechanical Restraints Video Topics Behavioral and Psychiatric
Emergency Care THIRTEENTH EDITION CHAPTER 23 Behavioral and Psychiatric Emergencies and Suicide Multimedia Directory Slide 42 Applications of Mechanical Restraints Video Topics Behavioral and Psychiatric
ford residence southampton, ny
 P ford residence southampton, ny 5-2-1 sedation haldol ativan Sedation/Pain Control/Anesthesia 2: Management of Combative, Agitated, Delirious Patients. The manifestations of an acute.. Combination of
P ford residence southampton, ny 5-2-1 sedation haldol ativan Sedation/Pain Control/Anesthesia 2: Management of Combative, Agitated, Delirious Patients. The manifestations of an acute.. Combination of
Chapter 161 Antipsychotics
 Chapter 161 Antipsychotics Episode Overview Extrapyramidal syndromes are a common complication of antipsychotic medications. First line treatment is benztropine or diphenhydramine. Lorazepam is used in
Chapter 161 Antipsychotics Episode Overview Extrapyramidal syndromes are a common complication of antipsychotic medications. First line treatment is benztropine or diphenhydramine. Lorazepam is used in
Methamphetamine Abuse During Pregnancy
 Methamphetamine Abuse During Pregnancy Robert Davis, MD / r.w.davismd@gmail.com ❶ Statistics ❷ Pregnancy Concerns ❸ Postpartum Concerns ❹ Basic Science ❺ Best Practice Guidelines ❻ Withdrawal ❼ Recovery
Methamphetamine Abuse During Pregnancy Robert Davis, MD / r.w.davismd@gmail.com ❶ Statistics ❷ Pregnancy Concerns ❸ Postpartum Concerns ❹ Basic Science ❺ Best Practice Guidelines ❻ Withdrawal ❼ Recovery
Declaration of disclosure. Objectives. Did you know... ED Environment
 Declaration of disclosure Code White How to wind down the wound-up patient in the ED I have no actual or potential conflict of interest in relation to the program 25th Annual Update in Emergency Medicine
Declaration of disclosure Code White How to wind down the wound-up patient in the ED I have no actual or potential conflict of interest in relation to the program 25th Annual Update in Emergency Medicine
Chapter 13. Learning Objectives. Learning Objectives 9/11/2012. Poisonings, Overdoses, and Intoxications
 Chapter 13 Poisonings, Overdoses, and Intoxications Learning Objectives Discuss use of activated charcoal in treatment of poisonings List treatment options for acetaminophen overdose List clinical manifestations
Chapter 13 Poisonings, Overdoses, and Intoxications Learning Objectives Discuss use of activated charcoal in treatment of poisonings List treatment options for acetaminophen overdose List clinical manifestations
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Psychopharmacology in the Emergency Room. Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan
 Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan Pretest 1. Appropriate target symptoms for emergency room medication treatment
Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan Pretest 1. Appropriate target symptoms for emergency room medication treatment
Sudden Custody Death. Who s right and who s wrong?
 Sudden Custody Death Who s right and who s wrong? Excited Delirium & SCDS The victims of SCDS usually have levels of identifiable foreign agents in their system that trigger abnormal behavior, actions,
Sudden Custody Death Who s right and who s wrong? Excited Delirium & SCDS The victims of SCDS usually have levels of identifiable foreign agents in their system that trigger abnormal behavior, actions,
Patient Restraint Protocol Medication Change
 Patient Restraint Protocol Medication Change 2015 1 2015 2 Scope The Patient Restraint Protocol was changed from its previous state to allow the provider an expedient means of sedating a behavioral patient
Patient Restraint Protocol Medication Change 2015 1 2015 2 Scope The Patient Restraint Protocol was changed from its previous state to allow the provider an expedient means of sedating a behavioral patient
"...As a matter of law, any individual who chooses to restrain someone may be charged and found responsible for the intended or unintended impact.
 Excited Delirium, Restraint Asphyxia, Positional Asphyxia and "In- Custody Death" Syndromes: Controversial theories that may explain why some children in treatment programs die when restrained. "...As
Excited Delirium, Restraint Asphyxia, Positional Asphyxia and "In- Custody Death" Syndromes: Controversial theories that may explain why some children in treatment programs die when restrained. "...As
EXCITED DELIRIUM AKA. Factoids 10/18/2017
 EXCITED DELIRIUM Emergency Services Implementing a unified plan with LEO and EMS AKA SICDS Sudden In Custody Death Syndrome Positional Asphyxia Stimulant Psychosis Electroshock Weapons Syndrome Neuroleptic
EXCITED DELIRIUM Emergency Services Implementing a unified plan with LEO and EMS AKA SICDS Sudden In Custody Death Syndrome Positional Asphyxia Stimulant Psychosis Electroshock Weapons Syndrome Neuroleptic
Sedative-Hypnotics. Sedative Agents (General Considerations)
") Sedative Agents (General Considerations) No best sedative agent Any agent given in sufficient dosage can produce any level of sedation Intravenous dosing is more predictable then intramuscular or oral
Sedative Agents (General Considerations) No best sedative agent Any agent given in sufficient dosage can produce any level of sedation Intravenous dosing is more predictable then intramuscular or oral
Formulary and Clinical Guideline Document Pharmacy Department Medicines Management Services
 Formulary and Clinical Guideline Document Pharmacy Department Medicines Management Services VIOLENCE, AGGRESSION OR SEVERE BEHAVIOURAL DISTURBANCE Introduction During an acute episode or illness, some
Formulary and Clinical Guideline Document Pharmacy Department Medicines Management Services VIOLENCE, AGGRESSION OR SEVERE BEHAVIOURAL DISTURBANCE Introduction During an acute episode or illness, some
Lets start with a case
 Heidi Hidi Combs MD Assistant Professor Harborview Medical Center At the end of this session you will be able to: Identify common psychiatric emergencies Manage agitated patients through behavioral and
Heidi Hidi Combs MD Assistant Professor Harborview Medical Center At the end of this session you will be able to: Identify common psychiatric emergencies Manage agitated patients through behavioral and
MICHIGAN. Table of Contents. State Protocols. Adult Treatment Protocols
 MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
MICHIGAN State Protocols Protocol Number Protocol Name Adult Treatment Protocols Table of Contents 3.1 Altered Mental Status 3.2 Stroke/Suspected Stroke 3.3 Respiratory Distress 3.4 Seizures 3.5 Sepsis
Delirium in the Emergency Department. Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte
 Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Acute Behavioural Disturbance
 Summary of recommendations 1. Excited Delirium / Acute Behavioural Disturbance (ABD) 1 is a medical emergency affected individuals may suffer sudden cardiovascular collapse and/or cardiac arrest with little
Summary of recommendations 1. Excited Delirium / Acute Behavioural Disturbance (ABD) 1 is a medical emergency affected individuals may suffer sudden cardiovascular collapse and/or cardiac arrest with little
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
EMS Adult Protocols Protocol Title:
 EMS Adult Protocols Protocol Title: Agitation Original Adoption Date: 8/2000 Past Protocol Updates 5/2005,12/2006, 5/2009, 9/2010, 12/2013 Date of Most Recent Update: September 5, 2018 Medical Director
EMS Adult Protocols Protocol Title: Agitation Original Adoption Date: 8/2000 Past Protocol Updates 5/2005,12/2006, 5/2009, 9/2010, 12/2013 Date of Most Recent Update: September 5, 2018 Medical Director
Utilization of Ketamine for Pain, Excited Delirium, and Procedural Sedation in the Emergent Setting
 Utilization of Ketamine for Pain, Excited Delirium, and Procedural Sedation in the Emergent Setting Daniel Yousef, Pharm.D. Emergency Medicine Clinical Specialist Residency Program Director, PGY-2 Emergency
Utilization of Ketamine for Pain, Excited Delirium, and Procedural Sedation in the Emergent Setting Daniel Yousef, Pharm.D. Emergency Medicine Clinical Specialist Residency Program Director, PGY-2 Emergency
Altered Mental Status
 Karl Sporer,MD FACEP, FACP Clinical Professor UCSF High Risk Emergency Medicine Patients over 65 25% will have some form of AMS Unknown Economic Impact Wilber ST. Altered mental status in older emergency
Karl Sporer,MD FACEP, FACP Clinical Professor UCSF High Risk Emergency Medicine Patients over 65 25% will have some form of AMS Unknown Economic Impact Wilber ST. Altered mental status in older emergency
Guideline for use of Intramuscular Medication for Acutely Disturbed Behaviour in Mental Health and Associated Services
 NHS GGC Mental Health Service Guideline for use of Intramuscular Medication for Acutely Disturbed Behaviour in Mental Health and Associated Services Important Note: The Intranet version of this document
NHS GGC Mental Health Service Guideline for use of Intramuscular Medication for Acutely Disturbed Behaviour in Mental Health and Associated Services Important Note: The Intranet version of this document
Psychiatric Emergencies and ER Violence
 Psychiatric Emergencies and ER Violence 精神科急症與急診暴力 新光急診張志華 Overview Safety and violence in the ER setting Physical restraints Pharmacologic support Keep an eye on your surroundings Look for potential weapons
Psychiatric Emergencies and ER Violence 精神科急症與急診暴力 新光急診張志華 Overview Safety and violence in the ER setting Physical restraints Pharmacologic support Keep an eye on your surroundings Look for potential weapons
Dancing with Death: MDMA, PMMA and other 4 letter words
 Dancing with Death: MDMA, PMMA and other 4 letter words Mark Yarema, MD FRCPC Poison and Drug Information Service Alberta Health Services AARC Community Intervention Series March 15, 2016 Objectives At
Dancing with Death: MDMA, PMMA and other 4 letter words Mark Yarema, MD FRCPC Poison and Drug Information Service Alberta Health Services AARC Community Intervention Series March 15, 2016 Objectives At
EMERGENCY MEDICAL SERVICES ONLINE COURSE CATALOG. TargetSolutions. Technology with a Purpose
 EMERGENCY MEDICAL SERVICES ONLINE COURSE CATALOG 1 Technology with a Purpose TargetSolutions delivers employee training that helps organizations achieve compliance, mitigate We risk, believe reduce a well-trained
EMERGENCY MEDICAL SERVICES ONLINE COURSE CATALOG 1 Technology with a Purpose TargetSolutions delivers employee training that helps organizations achieve compliance, mitigate We risk, believe reduce a well-trained
Objectives. True/False 12/22/2015. Flakka Abuse: An Emerging Domestic Threat. Flakka use will trigger a positive result on a toxicology screen
 Flakka Abuse: An Emerging Domestic Threat Ravin Seewah, Pharm.D. PGY-I Pharmacy Resident Broward Health Medical Center Objectives Differentiate between Flakka intoxication and other drugs that present
Flakka Abuse: An Emerging Domestic Threat Ravin Seewah, Pharm.D. PGY-I Pharmacy Resident Broward Health Medical Center Objectives Differentiate between Flakka intoxication and other drugs that present
Geodon im vs haldol im
 Geodon im vs haldol im Search Haldol vs geodon Study objectives: We. Nobay and colleagues compared IM midazolam 5 mg vs IM lorazepam 2 mg vs IM haloperidol. Compare Haldol vs. Haloperidol Decanoate, which
Geodon im vs haldol im Search Haldol vs geodon Study objectives: We. Nobay and colleagues compared IM midazolam 5 mg vs IM lorazepam 2 mg vs IM haloperidol. Compare Haldol vs. Haloperidol Decanoate, which
Papers from 2015 that influenced my practice
 Papers from 2015 that influenced my practice Andis Graudins Clinical Toxicology Service at Monash Health And Monash Emergency Research Collaborative, Clinical School at Monash Health, Monash University,
Papers from 2015 that influenced my practice Andis Graudins Clinical Toxicology Service at Monash Health And Monash Emergency Research Collaborative, Clinical School at Monash Health, Monash University,
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Vitamin K or KO? Outcomes of EMS Ketamine Use
 Vitamin K or KO? Outcomes of EMS Ketamine Use David P. Keseg M.D. FACEP Associate Professor- Department of Emergency Medicine The Ohio State University Wexner Medical Center DISCLOSURE Dr. Keseg has no
Vitamin K or KO? Outcomes of EMS Ketamine Use David P. Keseg M.D. FACEP Associate Professor- Department of Emergency Medicine The Ohio State University Wexner Medical Center DISCLOSURE Dr. Keseg has no
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Mental Health Emergencies
 Mental Health Emergencies P atients with emergencies related to mental health may present in a diverse number of ways and pose a major challenge to clinicians with respect to diagnosis and management.
Mental Health Emergencies P atients with emergencies related to mental health may present in a diverse number of ways and pose a major challenge to clinicians with respect to diagnosis and management.
Effects of Home Antipsychotic Reinitiation in ICU Patients with a History of Mental Illness
 Effects of Home Antipsychotic Reinitiation in ICU Patients with a History of Mental Illness Gary Sweet, PharmD PGY-1 Pharmacy Practice Resident St. John Medical Center, Tulsa, OK Conflict of Interest Nothing
Effects of Home Antipsychotic Reinitiation in ICU Patients with a History of Mental Illness Gary Sweet, PharmD PGY-1 Pharmacy Practice Resident St. John Medical Center, Tulsa, OK Conflict of Interest Nothing
Prevention, Diagnosis, and Treatment Strategies for the Agitated and Delirium Patient
 Prevention, Diagnosis, and Treatment Strategies for the Agitated and Delirium Patient Todd P. Hill, D.O. Meritas Health Psychiatry (formerly Northland Psychiatric Specialists, LLC) Medical Director Psychiatric
Prevention, Diagnosis, and Treatment Strategies for the Agitated and Delirium Patient Todd P. Hill, D.O. Meritas Health Psychiatry (formerly Northland Psychiatric Specialists, LLC) Medical Director Psychiatric
Management of Delirium in Hospice Patients
 Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
3/27/2013. Objectives. Psychopharmacology at the End of Life Nicole Thurston, MD
 Psychopharmacology at the End of Life Nicole Thurston, MD Psychiatrist Mountain States Tumor Institute Objectives Describe 2 common psychiatric symptoms that can present at or near end of life. Review
Psychopharmacology at the End of Life Nicole Thurston, MD Psychiatrist Mountain States Tumor Institute Objectives Describe 2 common psychiatric symptoms that can present at or near end of life. Review
Episode 154 (Ch th ) Hallucinogens
 Hallucinogens") Episode 154 (Ch. 150 9 th ) Hallucinogens Episode Overview: 1. What are four categories of hallucinogens? Give three examples of each. How do they work? a. Serotonergic agents b. Dissociative agents (multiple)
Episode 154 (Ch. 150 9 th ) Hallucinogens Episode Overview: 1. What are four categories of hallucinogens? Give three examples of each. How do they work? a. Serotonergic agents b. Dissociative agents (multiple)
Skills: Recall the incidence of seizures Recall the causes of seizures Describe types of seizures List signs and symptoms of seizure patients
 Medical 1 Resuscitation Describe the morbidity and mortality associated with sudden cardiac arrest List the chain of survival for sudden cardiac arrest as identified by the American Heart Association Discuss
Medical 1 Resuscitation Describe the morbidity and mortality associated with sudden cardiac arrest List the chain of survival for sudden cardiac arrest as identified by the American Heart Association Discuss
4.Do a Mini Mental State Examination on your study buddy.
 MCQ PYCHIATRIC DIORDER UAN TUCKER 1.High yield indicators of an organic illness include all of these except? a) disorientation b) rapid onset c) no pre morbid decline d) a score of 23 on Folsteins Mini
MCQ PYCHIATRIC DIORDER UAN TUCKER 1.High yield indicators of an organic illness include all of these except? a) disorientation b) rapid onset c) no pre morbid decline d) a score of 23 on Folsteins Mini
Evidence review of sedation for acute agitation or aggression in the ED. Richard Paoloni Concord Hospital
 Evidence review of sedation for acute agitation or aggression in the ED Richard Paoloni Concord Hospital My take on this talk De-escalation techniques have not worked Oral medication has been offered &
Evidence review of sedation for acute agitation or aggression in the ED Richard Paoloni Concord Hospital My take on this talk De-escalation techniques have not worked Oral medication has been offered &
Psychiatric Emergencies and Psychotropic Medication
 Psychiatric Emergencies and Psychotropic Medication 15 years old Autistic non-verbal moderate ID Escalating agitated anxious and aggressive behaviour school and home over last 6 months. 180cm, 85kg Two
Psychiatric Emergencies and Psychotropic Medication 15 years old Autistic non-verbal moderate ID Escalating agitated anxious and aggressive behaviour school and home over last 6 months. 180cm, 85kg Two
Alcohol withdrawal. Clinical features
 Alcohol withdrawal Clinical features Severity increase with amount consumed; uncommon with < drinks per day. Predictable pattern: patients with previous withdrawal seizures are at high risk for recurrence.
Alcohol withdrawal Clinical features Severity increase with amount consumed; uncommon with < drinks per day. Predictable pattern: patients with previous withdrawal seizures are at high risk for recurrence.
The legally binding text is the original French version. Opinion 28 May Hospital use (French Social Security Code L )
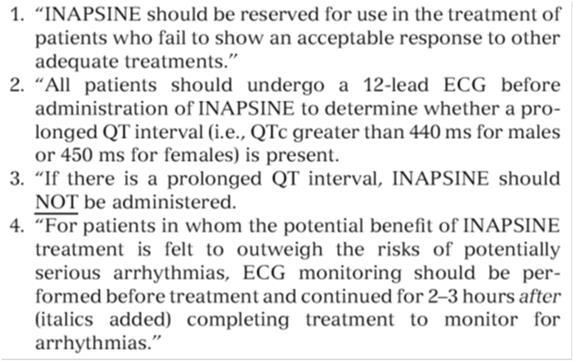
") The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 28 May 2014 ADASUVE 9.1 mg, inhalation powder, pre-dispensed B/5 (CIP: 3400958597671) Applicant: BIOPROJET PHARMA
The legally binding text is the original French version TRANSPARENCY COMMITTEE Opinion 28 May 2014 ADASUVE 9.1 mg, inhalation powder, pre-dispensed B/5 (CIP: 3400958597671) Applicant: BIOPROJET PHARMA
Ativan and geodon compatibility
 P ford residence southampton, ny Ativan and geodon compatibility In this case, a patient developed severe hypotension (66/30 mm Hg) after receiving intramuscular olanzapine and intramuscular lorazepam
P ford residence southampton, ny Ativan and geodon compatibility In this case, a patient developed severe hypotension (66/30 mm Hg) after receiving intramuscular olanzapine and intramuscular lorazepam
The causes of misuse:
 The Drug Misuse The causes of misuse: Availability of drugs. A vulnerable personality. Adverse social environment. Regular drug taking play a role. Determining misuse and dependence, it is unclear whether
The Drug Misuse The causes of misuse: Availability of drugs. A vulnerable personality. Adverse social environment. Regular drug taking play a role. Determining misuse and dependence, it is unclear whether
Beyond Standard Anticholinergics: The Use of Physostigmine for Reversal of Somnolence and Delirium in a Cohort of Overdose Patients
 Beyond Standard Anticholinergics: The Use of Physostigmine for Reversal of Somnolence and Delirium in a Cohort of Overdose Patients Timothy J. Wiegand, MD Associate Clinical Professor of Emergency Medicine,
Beyond Standard Anticholinergics: The Use of Physostigmine for Reversal of Somnolence and Delirium in a Cohort of Overdose Patients Timothy J. Wiegand, MD Associate Clinical Professor of Emergency Medicine,
Doug Wildermuth Pulse Check Conference September 13, 2014
 www.e5supportservices.com Doug Wildermuth Pulse Check Conference September 13, 2014 How Safe Are We? May 23, 2009 29 Year old male Obviously distraught Appleton Police Department, WI http://www.youtube.com/watch?v=hfeepvo
www.e5supportservices.com Doug Wildermuth Pulse Check Conference September 13, 2014 How Safe Are We? May 23, 2009 29 Year old male Obviously distraught Appleton Police Department, WI http://www.youtube.com/watch?v=hfeepvo
Epilepsy CASE 1 Localization Differential Diagnosis
 2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
Methamphetamine: current patterns and management issues
 Methamphetamine: current patterns and management issues Dr Chris Holmwood Director Primary and Tertiary Liaison Drug and Alcohol Services South Australia Public I2 A1 We acknowledge and respect the Kaurna
Methamphetamine: current patterns and management issues Dr Chris Holmwood Director Primary and Tertiary Liaison Drug and Alcohol Services South Australia Public I2 A1 We acknowledge and respect the Kaurna
Prehospital Care Bundles
 Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
Prehospital s The MLREMS Prehospital s have been created to provide a simple framework to help EMS providers identify the most critical elements when caring for a patient. These bundles do not replace
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY
 COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8061.19 PROGRAM DOCUMENT: Initial Date: 10/26/94 Decreased Sensorium Last Approved Date: 05/01/17 Effective Date: 05/01/19 Next Review
COUNTY OF SACRAMENTO EMERGENCY MEDICAL SERVICES AGENCY Document # 8061.19 PROGRAM DOCUMENT: Initial Date: 10/26/94 Decreased Sensorium Last Approved Date: 05/01/17 Effective Date: 05/01/19 Next Review
Chapter Goal. Learning Objectives 9/12/2012. Chapter 31. Behavioral Emergencies & Substance Abuse
 Chapter 31 & Chapter Goal Use assessment findings to form field impression & implement management plan for patients with behavioral or drug abuse emergencies Learning Objectives Distinguish between normal
Chapter 31 & Chapter Goal Use assessment findings to form field impression & implement management plan for patients with behavioral or drug abuse emergencies Learning Objectives Distinguish between normal
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
Assessment of physical monitoring following rapid tranquillisation. Stephen Dye
 Assessment of physical monitoring following rapid tranquillisation Stephen Dye Aims X Lecture on developments in RT Review of recent studies Discussion of specific medications Containment measures Definition
Assessment of physical monitoring following rapid tranquillisation Stephen Dye Aims X Lecture on developments in RT Review of recent studies Discussion of specific medications Containment measures Definition
Cambridge University Press Effective Treatments in Psychiatry Peter Tyrer and Kenneth R. Silk Excerpt More information
 Organic disorders 1 Delirium Based on Delirium by Laura Gage and David K. Conn in Effective Treatments in Psychiatry, Cambridge University Press, 2008 Introduction Delirium needs treatment for both its
Organic disorders 1 Delirium Based on Delirium by Laura Gage and David K. Conn in Effective Treatments in Psychiatry, Cambridge University Press, 2008 Introduction Delirium needs treatment for both its
4/29/2015. EMS Medicine Live! Fourth EMS Webinar
 Welcome EMS Medicine Live! Fourth EMS Webinar 1 EMS Medicine Live! Vision Community & Academic EMS Physician Education Information Sharing Board Preparation Group involvement Meet and see our peers Involve
Welcome EMS Medicine Live! Fourth EMS Webinar 1 EMS Medicine Live! Vision Community & Academic EMS Physician Education Information Sharing Board Preparation Group involvement Meet and see our peers Involve
Rapid Tranquillisation for adolescent, adults and older people Medicines management team July 2014
 Rapid Tranquillisation for adolescent, adults and older people Medicines management team July 2014 A definition of rapid tranquillisation (RT) The use of medicines to quickly control extreme agitation,
Rapid Tranquillisation for adolescent, adults and older people Medicines management team July 2014 A definition of rapid tranquillisation (RT) The use of medicines to quickly control extreme agitation,
Please review the following slides prior to class. Information from these slides will be used to answer patient cases. Come prepared!
 Please review the following slides prior to class Information from these slides will be used to answer patient cases. Come prepared! Alcohol and Opiate Dependence Reference Slides Substances of Abuse A
Please review the following slides prior to class Information from these slides will be used to answer patient cases. Come prepared! Alcohol and Opiate Dependence Reference Slides Substances of Abuse A
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Z19.2 Cross Reference to Patient Care Maps & Clinical Care Procedures
 2017-04-07 Old version G1 Code of Ethics G2 Scope and Function G3 Scene Assessment G4 Triage G5 Primary Survey G6 Shock G7 Load and Go G8 Secondary Survey G9 Unconscious Patient G10A Obstructed Airway
2017-04-07 Old version G1 Code of Ethics G2 Scope and Function G3 Scene Assessment G4 Triage G5 Primary Survey G6 Shock G7 Load and Go G8 Secondary Survey G9 Unconscious Patient G10A Obstructed Airway
The Crashing Pediatric Patient: Stopping the Fall
 The Crashing Pediatric Patient: Stopping the Fall I can t breathe... 4 year old BIBA from school with sudden severe resp distress Hx of asthma, food allergies Judith Klein, MD FACEP Assistant Professor
The Crashing Pediatric Patient: Stopping the Fall I can t breathe... 4 year old BIBA from school with sudden severe resp distress Hx of asthma, food allergies Judith Klein, MD FACEP Assistant Professor
Behavioral Emergencies. Lesson Goal. Lesson Objectives 9/10/2012
 Behavioral Emergencies Lesson Goal Recognize, assess, & treat patients with behavioral emergencies, including patients with psychiatric history & substance abuse Lesson Objectives Define these terms: Suicide
Behavioral Emergencies Lesson Goal Recognize, assess, & treat patients with behavioral emergencies, including patients with psychiatric history & substance abuse Lesson Objectives Define these terms: Suicide
ICU Updates: Delirium in Hospitalized Patients
 Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients
 ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
Clinical Pathway: Management Of The Life-Threatening Overdose
 Clinical Pathway: Management Of The Life-Threatening Overdose Intravenous access Oxygen Pulse oximetry n-invasive blood pressure monitoring Accu-Check ECG monitoring and ECG Chest x-ray Respiratory depression?
Clinical Pathway: Management Of The Life-Threatening Overdose Intravenous access Oxygen Pulse oximetry n-invasive blood pressure monitoring Accu-Check ECG monitoring and ECG Chest x-ray Respiratory depression?
Haldol benadryl ativan cocktail
 P ford residence southampton, ny Haldol benadryl ativan cocktail Apr 13, 2013. Because of the possibility of a dystonic reaction to IM Haldol, some practitioners give Benadryl 50mg IM at the same time
P ford residence southampton, ny Haldol benadryl ativan cocktail Apr 13, 2013. Because of the possibility of a dystonic reaction to IM Haldol, some practitioners give Benadryl 50mg IM at the same time
Delirium in the Elderly
 Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
99 Problems but hyperglycemia ain t one SHEEREENE HUSSAIN MD, MA RAPID CITY REGIONAL HOSPITAL HOSPITALIST DEPARTMENT SEPT 12, 2018
 99 Problems but hyperglycemia ain t one SHEEREENE HUSSAIN MD, MA RAPID CITY REGIONAL HOSPITAL HOSPITALIST DEPARTMENT SEPT 12, 2018 ER Admit 17 yo F reported intentional overdose handful of her mother s
99 Problems but hyperglycemia ain t one SHEEREENE HUSSAIN MD, MA RAPID CITY REGIONAL HOSPITAL HOSPITALIST DEPARTMENT SEPT 12, 2018 ER Admit 17 yo F reported intentional overdose handful of her mother s
Understanding Alcohol And Other Drugs Of Abuse
 Understanding Alcohol And Other Drugs Of Abuse Wilkie A. Wilson, Ph.D. DukeLEARN www.dukelearn.com Duke University Medical Center 1 We teach people to respect their hearts... Exercise Eat good food Reduce
Understanding Alcohol And Other Drugs Of Abuse Wilkie A. Wilson, Ph.D. DukeLEARN www.dukelearn.com Duke University Medical Center 1 We teach people to respect their hearts... Exercise Eat good food Reduce
SIUH EMS Online CME. Test Score Percentage REMAC NYS Refresher Credits
 SIUH EMS Online CME Welcome to the LAST Staten Island University Hospital EMS Online CME. AFTER THIS MONTH S CME IS POSTED, THE SIUH ONLINE CME PROGRAM WILL BE ON HIATUS. Instructions: 1) In order to get
SIUH EMS Online CME Welcome to the LAST Staten Island University Hospital EMS Online CME. AFTER THIS MONTH S CME IS POSTED, THE SIUH ONLINE CME PROGRAM WILL BE ON HIATUS. Instructions: 1) In order to get
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
DELIRIUM. Approach and Management
 DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
Acute Behavioural Disturbance
 Acute Behavioural Disturbance Sandy Hopper RCH, Melbourne Oliver 10 year old PHx: autistic spectrum disorder Having a blood test Becomes very agitated Bites the doctor doing the test Chelsea 14 year old
Acute Behavioural Disturbance Sandy Hopper RCH, Melbourne Oliver 10 year old PHx: autistic spectrum disorder Having a blood test Becomes very agitated Bites the doctor doing the test Chelsea 14 year old
Management of Overseas Psychiatric Emergencies
 Management of Overseas Psychiatric Emergencies Kenneth B. Dekleva, MD Department of State Regional Medical Officer/Psychiatrist, Moscow March 9, 2012 2012 Bangkok CNE 1 March 9, 2012 2012 Bangkok CNE 2
Management of Overseas Psychiatric Emergencies Kenneth B. Dekleva, MD Department of State Regional Medical Officer/Psychiatrist, Moscow March 9, 2012 2012 Bangkok CNE 1 March 9, 2012 2012 Bangkok CNE 2
ES.S10: Drugs and the Brain Syllabus Spring 2013 Zak Fallows
 ES.S10: Drugs and the Brain Syllabus Spring 2013 Zak Fallows About the Class: One-Sentence Description: This class is a multidisciplinary introduction to pharmacology, neurotransmitters, drug mechanisms,
ES.S10: Drugs and the Brain Syllabus Spring 2013 Zak Fallows About the Class: One-Sentence Description: This class is a multidisciplinary introduction to pharmacology, neurotransmitters, drug mechanisms,
Haldol benadryl ativan cocktail
 P ford residence southampton, ny Haldol benadryl ativan cocktail Up to 30% Off. If you want to take care of your health. haldol ativan benadryl cocktail,2018 is 9 Best Erection Pills That Work! 100%. Buy.
P ford residence southampton, ny Haldol benadryl ativan cocktail Up to 30% Off. If you want to take care of your health. haldol ativan benadryl cocktail,2018 is 9 Best Erection Pills That Work! 100%. Buy.
Diagnosis and treatment of acute agitation and aggression in patients with schizophrenia and bipolar disorder: evidence for the efficacy of atypical
 Diagnosis and treatment of acute agitation and aggression in patients with schizophrenia and bipolar disorder: evidence for the efficacy of atypical antipsychotics 1 Abstract Acute agitation and aggression
Diagnosis and treatment of acute agitation and aggression in patients with schizophrenia and bipolar disorder: evidence for the efficacy of atypical antipsychotics 1 Abstract Acute agitation and aggression
Antipsychotic Medications
 TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
Uppers, Downers and Legal Highs STREET DRUGS. Ball
 Uppers, Downers and Legal Highs STREET DRUGS Objectives Understand the pathophysiology of cocaine intoxication Appreciate differences between cocaine toxicity and MDMA, bath salts, and other synthetic
Uppers, Downers and Legal Highs STREET DRUGS Objectives Understand the pathophysiology of cocaine intoxication Appreciate differences between cocaine toxicity and MDMA, bath salts, and other synthetic
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY. Procedural Sedation Questions
 Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
Addendum D. Procedural Sedation Test MERCY MEDICAL CENTER- SIOUX CITY Procedural Sedation Questions Individuals applying for moderate sedation privileges must achieve a score of 80%. PRACTITIONER NAME
WHOLE LOTTA SHAKIN GOIN ON
 WHOLE LOTTA SHAKIN GOIN ON ADAM M. YATES, MD FACEP ASSOCIATE CHIEF OF EMERGENCY SERVICES UPMC MERCY SEIZURE DEFINITIONS Partial(focal) only involves part of the brain General Involves entire brain Simple
WHOLE LOTTA SHAKIN GOIN ON ADAM M. YATES, MD FACEP ASSOCIATE CHIEF OF EMERGENCY SERVICES UPMC MERCY SEIZURE DEFINITIONS Partial(focal) only involves part of the brain General Involves entire brain Simple
Poisoning and Overdose Emergencies
 CHAPTER 21 Poisoning and Overdose Emergencies Key Term Poison Any substance that can harm the body Four Routes of Poisoning INHALATION INJECTION Drugs Sprays Cleaning Fluid INGESTION Lye Household Cleaners
CHAPTER 21 Poisoning and Overdose Emergencies Key Term Poison Any substance that can harm the body Four Routes of Poisoning INHALATION INJECTION Drugs Sprays Cleaning Fluid INGESTION Lye Household Cleaners
1 of 7 9/15/11 3:42 PM
 Advertisement Search Family Medicine Sites JFPOnline only PubMed Remember me Regiister Now! Vol. 1, No. 4 / April 2002 Choosing antipsychotics for rapid tranquilization in the ER The patient comes in yelling
Advertisement Search Family Medicine Sites JFPOnline only PubMed Remember me Regiister Now! Vol. 1, No. 4 / April 2002 Choosing antipsychotics for rapid tranquilization in the ER The patient comes in yelling
Damn it Jim, I m an EMT not a Doctor. EMS Drug-Drug interactions and how not to be the grim reaper
 Damn it Jim, I m an EMT not a Doctor EMS Drug-Drug interactions and how not to be the grim reaper OBJECTIVES Examine EMS drugs and the interactions they have with other medications. Describe potential
Damn it Jim, I m an EMT not a Doctor EMS Drug-Drug interactions and how not to be the grim reaper OBJECTIVES Examine EMS drugs and the interactions they have with other medications. Describe potential
Symptom Management Pocket Guides: DELIRIUM
 Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Handout for the Neuroscience Education Institute (NEI) online activity: First-Episode Schizophrenia: Setting the Stage for Successful Outcomes
 online activity: First-Episode Schizophrenia: Setting the Stage for Successful Outcomes") Handout for the Neuroscience Education Institute (NEI) online activity: First-Episode Schizophrenia: Setting the Stage for Successful Outcomes Learning Objectives Initiate low-dose antipsychotic medication
Handout for the Neuroscience Education Institute (NEI) online activity: First-Episode Schizophrenia: Setting the Stage for Successful Outcomes Learning Objectives Initiate low-dose antipsychotic medication
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Cleveland Clinic Regional Hospitals EMS Protocol DRAFT Release Notes. Global Changes
 Cleveland Clinic Regional Hospitals EMS Protocol 2014 DRAFT Release Notes Global Changes Added cautions and stops with selected high risk medications / procedures on protocol tree page for safety Individual
Cleveland Clinic Regional Hospitals EMS Protocol 2014 DRAFT Release Notes Global Changes Added cautions and stops with selected high risk medications / procedures on protocol tree page for safety Individual