Pain management. Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD
|
|
|
- Nora Morgan
- 6 years ago
- Views:
Transcription
1 Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD
2 Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX now in remission. 8 years later, presented with right sided chest pain and weight loss.
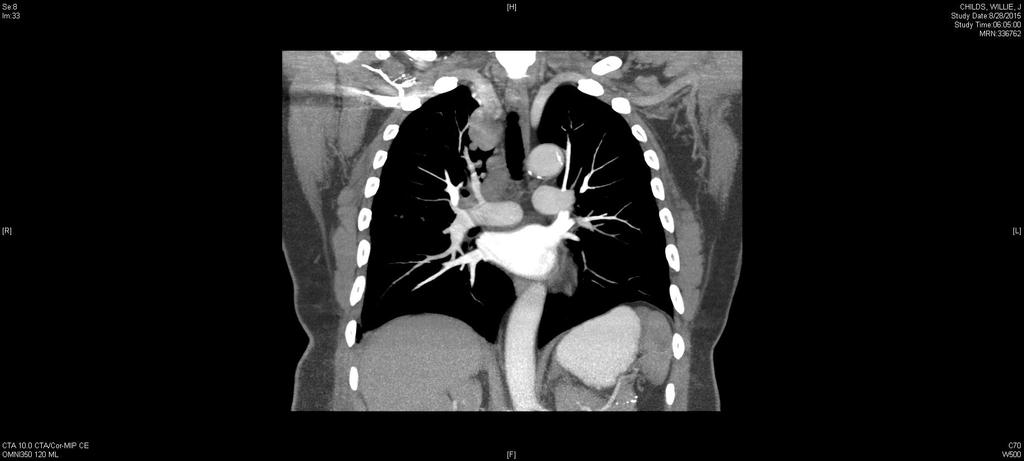
3 Adenocarcinoma
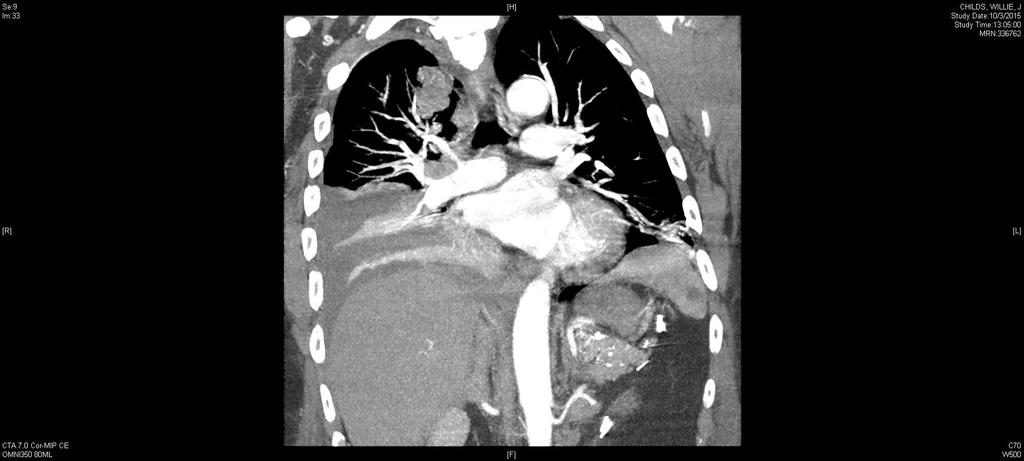
4 Started on chemotherapy (Carboplatin/Pemetrexed) Developed progressive chest pain, respirophasic upper back pain and dyspnea. Meds uptitrated by Oncologist in consultation with pain service Return to ED 3 months after initiation of chemotherapy with severe, uncontrolled pain despite treatment at home. Repeat CT.
5
6 Meds: Fentanyl patch 100mcg/hr q72h Hydromorphone 4mg PO Q3h PRN Gabapentin 600mg PO TID Docusate-senna 1 tab PO BID
7 He has been taking 2-3 of his hydromorphone tabs every 3 hours for the past 18 hours. Before meds: pain 20/10 After meds: pain 10/10 Spending most of time in bed, irritable, can t sleep, no appetite
8 Exam T: 99.3, HR 103, BP 125/81 Brow furrowed, uncomfortable appearing Tender to palpation over entire anterior chest wall; no masses Tachypneic, splinting respirations, decreased breath sounds over lower 1/3 of R lung field Rest benign
9 Acute pain crisis How do you treat this pain crisis? What do you do with his fentanyl? How do you administer the breakthrough meds? Bolus dosing PCA
10 What is this patient s 24 hour oral morphine equivalent (OME)?
11 Our patient Opioid usage Fentanyl 100mcg/hr 200mg oral morphine/24hr Hydromorphone 8mg (2 tabs) PO q3h x 6 (18 hours) 48mg PO hydromorphone 192 mg (48*4) oral morphine TOTAL USAGE: 392 mg oral morphine equivalent (OME)
12 What would you recommend as a starting bolus dose using IV morphine? IV hydromorphone? Dose: 10% of 24 hour usage
13 Acute pain crisis Opioid bolus algorithm Dose: 10% of 24 hour usage Starting bolus dose: 39.2 mg OME 13mg IV morphine 2mg IV hydromorphone Re-assess every mins Rebolus if: Partial control: same dose (50% decrease if SEs) Partial control : decrease in VAS of 2 Uncontrolled (severe): increase by % Uncontrolled : no improvement in pain score
14 Our patient 11:00 AM: Given 2mg IV hydromorphone 11:20 AM: Pain 10/10 Given 4mg IV hydromorphone 11:35 AM: Pain 7/10 Given 4mg IV hydromorphone 11:55 AM: Pain 4/10 ( tolerable ); alert, no SEs
15 Maintenance regimen If you wanted to administer a round-the-clock, hydromoprphone bolus regimen to manage this patient s pain, what dose and frequency would you give? What would your breakthrough dose be?
16 Acute pain crisis Maintenance regimen: Bolus dosing + breakthrough Mild pain, no SEs (Total amount administered) q 4h + 0.1(Total 24-hour dose) q1h PRN No pain OR Ses 0.5(Total amount administered) q4h + 0.1(Total 24-hour dose) q1h PRN EXAMPLE: 10mg IV hydromorphone administered Order: 10mg IV hydromorphone q4h RTC 6mg IV hydromorphone q1h
17 Acute pain crisis Maintenance regimen: PCA What drip do you start? Medication? Dose/Rate? If you are going to give a bolus, what dose do you give? What is the demand dose? What is the frequency?
18 Comparing opioid drips Drug Potency Metabolites Cost* Morphine Active $ Hydromorphone Minimally active $$ Fentanyl Inactive $$ *Note that cost depends on doses used as PCAs are charged per unit
19 Based on your round-the-clock calculation, if you wanted to give this patient a hydromorphone drip, what dose would you choose?
20 Calculating drip rate Calculated total daily dose: Hydromorphone 10mg IV Q4h= 60mg/24h 60/24= IV hydromorphone 2.5mg/hr IV Morphine: ~15mg/hr (2.5*6) IV fentanyl: ~ 160mcg/hr (2.5/15)
21 Acute pain crisis Conversion to PCA If you stop the fentanyl, what drip do you start? Medication? Dose/Rate? What is the demand dose? What is the frequency?
22 If you wanted to convert this regimen to a hydromorphone PCA with a continuous infusion, what would your drip dose be? What would your demand dose be?
23 Acute pain crisis Opioid bolus Calculating the bolus dose 10% of 24 hour rate/hour % of basal rate EXAMPLE: IV hydromorphone 60mg/24hr Breakthrough=6mg/hr (1.5mg q15mins OR 1mg q10mins)
24 Case # 2 50 yo female, former heroin abuse admitted to hospital with increasing abdominal pain and early satiety Home medications: Methadone 60 mg po daily, Tylenol up to 8 grams/day, Aleve prn Pain history: vague, aching, located in mid epigastrum, radiates into her back, 10/10, wakes her up at night, some nausea when severe On exam, ill-appearing and cachetic, stable VS, abdominal is distended and painful to touch, non-tender spine, no fluid wave Labs: LFTs:AST/ALT 300/356, Cr 1.9 (unclear baseline)

25 CT: Metastatic pancreas cancer
26 Questions What options do you have to address her pain? Explain why or why not you would choose certain options. What do we do with the Methadone?


27 Acute pain management for patients on Opioid Agonist Therapy (OAT) for addiction Methadone Buprenorphine
28 Common misconceptions The OAT provides analgesia Use of opioids in these patients may result in addiction relapse Additive effects of opioid analgesics and OAT may cause respiratory and CNS depression The pain complaint may be drug-seeking
29 The truth OAT at once daily dosing to prevent withdrawal (24-48 hrs) not consistent with duration of action for analgesia (4-8 hrs) Opioid tolerance is real patients have less effect and for shorter duration when adding another opioid Opioid-hyperalgesia can occur - latent, due to neuro-plastic changes from long-term exposure Stress from uncontrolled pain more likely to cause relapse than treating the pain with an opioid Tolerance to side effects is high for patients on OAT OAT treatment blocks euphoric effect of other opioids
30 Recommendations - Methadone Continue usual dose of po methadone, but must verify dose with the program If patient cannot take po, give 50% in IV form and divide q 6 or q 8 (example: 60 mg po reduce to 30 mg IV, give 10 mg IV q 8) Add an opioid co-analgesic, higher doses and shorter interval of immediate release with continuous or scheduled dosing Long-acting opioids may cause less euphoric effects Notify methadone program upon discharge of new plan
31 Our patient Methadone and other home meds continued Celiac plexus block on admission: initially brought pain from 10/10 to 3/10, then increased two days later to 10/10 Steroids added decadron 8 mg po qam, plus PPI Started hydromorphone 1 mg IV q 2 which escalated to 2, then 3 mg IV q 2, switched to IV gtt at 2 mg/hr, with increasing pain, despite multiple boluses q 2 and increase in drip rate Question what could be going on?
32 Opioid induced hyperalgesia (OIH) Neuroplastic changes in the peripheral and CNS, sensitization of pronociceptive pathways Central glutaminergic system, NMDA Must be differentiated from tolerance which gets better with increase in opioid Exam often find diffuse, ill-defined pain outside of level of original pain source, allodynia Can mimic opioid withdrawal
33 Our patient Severe abdominal and back pain, 20/10, unable to obtain a comfortable position Renal function declined to 2.5 Non-contrast CT abd/pelvis and Xray no changes OIH leading diagnosis
34 OIH - Treatment Reduce dose of current opioid Opioid rotation (methadone most common) Hydration Select other medications with pain properties (SNRI) Ketamine -uncompetitive antagonist of the phencyclidine binding site of NMDA receptor -usually given in hospital via infusion -dissociative side effects
35 Our patient Reduced hydromorphone Hydration Interventional pain performed second block Once pain and renal function improved she was discharged on LA morphine and back to methadone program
36 Acute pain crisis Opioid side effects Nausea Haldol Sedation Methylphenidate?? Respiratory depression Diluted naloxone Urinary retention Pruritis Myoclonus Opioid induced hyperalgesia
Equianalgesic Dosing: Making Opioid Interchange Easier. Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine
 Equianalgesic Dosing: Making Opioid Interchange Easier Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine 1 Why Change Opioids? Side Effects Insufficient Pain
Equianalgesic Dosing: Making Opioid Interchange Easier Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine 1 Why Change Opioids? Side Effects Insufficient Pain
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat.
 Difficult Pain Syndrome/Intractable/Refractory Pain Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat. Reasonable efforts Differs for specialties/regions/countries
Difficult Pain Syndrome/Intractable/Refractory Pain Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat. Reasonable efforts Differs for specialties/regions/countries
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
Opioid Pearls and Acute Pain Management
 Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
(30689) PROT Pain PCA Adult Patient Controlled Analgesia
 PROT Pain PCA Adult Patient Controlled Analgesia") Diagnosis Allergies Nursing Assess and Document PCA: 1. Assess and document pain rating, sedation level and respiratory rate every 2 hours; assess and document pain rating, sedation level and respiratory
Diagnosis Allergies Nursing Assess and Document PCA: 1. Assess and document pain rating, sedation level and respiratory rate every 2 hours; assess and document pain rating, sedation level and respiratory
4/3/2018. Management of Acute Pain Crises. Five Mistakes I ve made and why you shouldn t
 Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
What to do when you are called to see a patient with... PAIN. Susan Merel, MD Division of General Internal Medicine July 2018
 What to do when you are called to see a patient with... PAIN Susan Merel, MD Division of General Internal Medicine July 2018 Disclosures Susan Merel has no relationships with any entity producing, marketing,
What to do when you are called to see a patient with... PAIN Susan Merel, MD Division of General Internal Medicine July 2018 Disclosures Susan Merel has no relationships with any entity producing, marketing,
Agenda. Case Discussions. Managing Acute & Chronic Pain (requiring opioid analgesics) in Patients on MAT. Daniel Alford, MD Disclosures
 in Patients on MAT. Daniel Alford, MD Disclosures") Managing Acute & Chronic Pain (requiring opioid analgesics) in Patients on MAT Case Discussions August 26, 2014 PCSS MAT Webinar Sponsored by the American Psychiatric Association Daniel P. Alford, MD,
Managing Acute & Chronic Pain (requiring opioid analgesics) in Patients on MAT Case Discussions August 26, 2014 PCSS MAT Webinar Sponsored by the American Psychiatric Association Daniel P. Alford, MD,
1/21/14. Cancer Related Pain: Case-Based Pharmacology. Conflicts of Interest. Learning Objective
 Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Pain and the MGH Promise
 Pain is an unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Our promise to patients we will always: Work as a team to evaluate,
Pain is an unpleasant sensory & emotional experience associated with actual or potential tissue damage or described in terms of such damage Our promise to patients we will always: Work as a team to evaluate,
Fighting the Good Fight: How to Convert Opioids Just Right!
 Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Pain. November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine
 Internal Medicine, Palliative Medicine") Pain November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine Objectives To be able to define pain To be able to evaluate pain To be able to classify types of pain To learn appropriate
Pain November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine Objectives To be able to define pain To be able to evaluate pain To be able to classify types of pain To learn appropriate
Pharmacologic Considerations for Managing Sickle Cell Pain Claire Saadeh, PharmD, BCOP May 5, 2015
 Pharmacologic Considerations for Managing Sickle Cell Pain Claire Saadeh, PharmD, BCOP May 5, 2015 Table 1: Physiologic changes that occur during sickle cell pain crisis 1-3 Phase Description / Complications
Pharmacologic Considerations for Managing Sickle Cell Pain Claire Saadeh, PharmD, BCOP May 5, 2015 Table 1: Physiologic changes that occur during sickle cell pain crisis 1-3 Phase Description / Complications
Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management
 Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management Eric Roeland, MD GI Oncology Palliative Medicine Pancreatic Cancer Patient Tool Belt Chemotherapy Surgery Pain & Symptom
Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management Eric Roeland, MD GI Oncology Palliative Medicine Pancreatic Cancer Patient Tool Belt Chemotherapy Surgery Pain & Symptom
Practical Tools to Successfully Taper Prescription Opioids. Melissa Weimer, DO, MCR
 Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Opioid Case Studies. Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN. September 29, MFMER slide-1
 Opioid Case Studies Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN September 29, 2016 2015 MFMER slide-1 Disclosures Relevant Financial Relationship(s) None Off Label and/or
Opioid Case Studies Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN September 29, 2016 2015 MFMER slide-1 Disclosures Relevant Financial Relationship(s) None Off Label and/or
Use of PCA devices in Difficult Populations
 Use of PCA devices in Difficult Populations Diane M. Santangelo MS RN ANP-C Stony Brook University Medical Center Acute Pain Service September 10, 2011 1 PCA technology? Why Bother? Costly Nurses complain:
Use of PCA devices in Difficult Populations Diane M. Santangelo MS RN ANP-C Stony Brook University Medical Center Acute Pain Service September 10, 2011 1 PCA technology? Why Bother? Costly Nurses complain:
Opioid Conversions Mixture of Science and Art
 Opioid Conversions Mixture of Science and Art Matthew J. Pingree, MD Assistant Professor Division of Pain Medicine Physical Medicine and Rehabilitation and Anesthesiology Mayo Clinic, Rochester Pingree.Matthew@Mayo.edu
Opioid Conversions Mixture of Science and Art Matthew J. Pingree, MD Assistant Professor Division of Pain Medicine Physical Medicine and Rehabilitation and Anesthesiology Mayo Clinic, Rochester Pingree.Matthew@Mayo.edu
Pain Management in Hospice and Palliative Care
 Pain Management in Hospice and Palliative Care A Case-based Approach JoAnne Nowak, M.D. Merrimack Valley Hospice Revised November 2011 Objectives Use a case study approach to stimulate discussion and illustrate
Pain Management in Hospice and Palliative Care A Case-based Approach JoAnne Nowak, M.D. Merrimack Valley Hospice Revised November 2011 Objectives Use a case study approach to stimulate discussion and illustrate
Analgesia for Patients with Substance Abuse Disorders. Lisa Jennings CN November 2015
 Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
Opioids in Serious Medical Illness
 Opioids in Serious Medical Illness Jacob J. Strand, M.D. Assistant Professor of Medicine Medical Director, Palliative Care Clinical Services Mayo Clinic Mayo Clinic Opioid Conference 2013 MFMER slide-1
Opioids in Serious Medical Illness Jacob J. Strand, M.D. Assistant Professor of Medicine Medical Director, Palliative Care Clinical Services Mayo Clinic Mayo Clinic Opioid Conference 2013 MFMER slide-1
PAIN MANAGEMENT PGY-1. Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC
 PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline
 Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline 1. Pharmacist to order Narcotic Withdrawal Scores QH X 4 hours, then per table below: Narcotic Withdrawal Score
Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline 1. Pharmacist to order Narcotic Withdrawal Scores QH X 4 hours, then per table below: Narcotic Withdrawal Score
OPIOID- INDUCED NEUROTOXICITY*
 OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
Opioid use in older adults Is it a good idea? Regional Geriatric Rounds April 26, 2013
 Opioid use in older adults Is it a good idea? Regional Geriatric Rounds April 26, 2013 Allen R. Huang, MDCM, FRCPC, FACP, AGSF Division of Geriatric Medicine allenhuang@toh.on.ca I have no conflict of
Opioid use in older adults Is it a good idea? Regional Geriatric Rounds April 26, 2013 Allen R. Huang, MDCM, FRCPC, FACP, AGSF Division of Geriatric Medicine allenhuang@toh.on.ca I have no conflict of
Analgesics: Management of Pain In the Elderly Handout Package
 Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Opioid Use in Serious Illness
 Opioid Use in Serious Illness Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Opioid Use in Serious Illness Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Long Term Care Formulary HCD - 08
 1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
Opioid Rotation. Dr Bruno Gagnon, M.D., M.Sc.
 Opioid Rotation Dr Bruno Gagnon, M.D., M.Sc. Associate Professor Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval Consultant in Palliative Medicine CHU de Québec-Université
Opioid Rotation Dr Bruno Gagnon, M.D., M.Sc. Associate Professor Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval Consultant in Palliative Medicine CHU de Québec-Université
10 mg hydrocodone equals how much oxycodone
 Cari untuk: Cari Cari 10 mg hydrocodone equals how much oxycodone Posts about dilaudid 8 vs oxycodone 30 written by buyprescriptionmedication. Can you help me with the conversion of Oxycodone IR (5mg tab)
Cari untuk: Cari Cari 10 mg hydrocodone equals how much oxycodone Posts about dilaudid 8 vs oxycodone 30 written by buyprescriptionmedication. Can you help me with the conversion of Oxycodone IR (5mg tab)
BASICS OF OPIOID PRESCRIBING 10:30-11:45AM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
PEDIATRIC SPINE SURGERY POST-OP PLAN - Phase:.
 - Phase:. PHYSICIAN S Diagnosis Weight Allergies DETAILS Patient Care Patient Activity Bedrest Maintain Surgical Drain Maintain JP Drain, Measure Output q12h, and PRN Convert IV to INT when tolerating
- Phase:. PHYSICIAN S Diagnosis Weight Allergies DETAILS Patient Care Patient Activity Bedrest Maintain Surgical Drain Maintain JP Drain, Measure Output q12h, and PRN Convert IV to INT when tolerating
Pain Management Dilemmas. Five Pain Dilemmas. Barriers: Meet Loretta. Daniel Johnson, MD, FAAHPM
 Pain Management Dilemmas Daniel Johnson, MD, FAAHPM Kaiser Permanente University of Colorado Five Pain Dilemmas 1. Barriers to Pain Management 2. Selecting and Titrating Opioids 3. Managing PCAs 4. Using
Pain Management Dilemmas Daniel Johnson, MD, FAAHPM Kaiser Permanente University of Colorado Five Pain Dilemmas 1. Barriers to Pain Management 2. Selecting and Titrating Opioids 3. Managing PCAs 4. Using
PEDIATRIC SPINE SURGERY POST-OP PLAN - Phase: Pediatric Spine Surgery General Orders
 - Phase: Pediatric Spine Surgery General Orders PHYSICIAN S Diagnosis Weight Allergies Patient Care Patient Activity Bedrest Maintain Surgical Drain Maintain JP Drain, Measure Output q12h, and PRN Convert
- Phase: Pediatric Spine Surgery General Orders PHYSICIAN S Diagnosis Weight Allergies Patient Care Patient Activity Bedrest Maintain Surgical Drain Maintain JP Drain, Measure Output q12h, and PRN Convert
Update on Pain: Collaborative Care for the Complex Patient
 Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
Update on Pain: Collaborative Care for the Complex Patient Nirmala R. Abraham, MD Medical Director Sycamore Pain Management Center Kettering Health Network Objectives Standardized approach to patient care
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Managing Pain in Individuals with Serious Illness and Comorbid Substance Use Disorder
 Managing Pain in Individuals with Serious Illness and Comorbid Substance Use Disorder Presented by: Kathleen Broglio, DNP, ANP-BC, ACHPN, CPE, FPCN on December 1, 2016 Webcast Questions and Answers (Answers
Managing Pain in Individuals with Serious Illness and Comorbid Substance Use Disorder Presented by: Kathleen Broglio, DNP, ANP-BC, ACHPN, CPE, FPCN on December 1, 2016 Webcast Questions and Answers (Answers
Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center
 Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Methadone Maintenance
 Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION
 STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
Attach patient label here. Physician Orders ADULT: Palliative Care Plan
 Initiate Orders Phase Care Sets/Protocols/PowerPlans Initiate Powerplan Phase T;N, Phase: Palliative Care Phase, When to Initiate: Palliative Care Phase Admission/Transfer/Discharge Patient Status Initial
Initiate Orders Phase Care Sets/Protocols/PowerPlans Initiate Powerplan Phase T;N, Phase: Palliative Care Phase, When to Initiate: Palliative Care Phase Admission/Transfer/Discharge Patient Status Initial
Session II. Learning Objectives for Session II. Key Principles of Safe Prescribing. Benefits and Limitations of ER/LA Opioids
 Learning Objectives for Session II Session II Best Practices for How to Start Therapy with ER/LA Opioids, How to Stop, and What to Do in Between Upon completion of this module, the participants will be
Learning Objectives for Session II Session II Best Practices for How to Start Therapy with ER/LA Opioids, How to Stop, and What to Do in Between Upon completion of this module, the participants will be
ANSWER # 1 PHARMACOLOGY. Methadone answers Stoltzfus 4/5/2012 METHADONE: WHY GRANDMA S TAKING A DIPHENYLHEPTANE (ANSWERS) JANUARY 26, 2017
 JANUARY 26, 2017") METHADONE: WHY GRANDMA S TAKING A DIPHENYLHEPTANE (ANSWERS) JANUARY 26, 2017 Ky Stoltzfus, MD Assistant Professor, Internal Medicine University of Kansas Medical Center ANSWER # 1 Your response might be
METHADONE: WHY GRANDMA S TAKING A DIPHENYLHEPTANE (ANSWERS) JANUARY 26, 2017 Ky Stoltzfus, MD Assistant Professor, Internal Medicine University of Kansas Medical Center ANSWER # 1 Your response might be
Review of Pain Management with Clinical and Regulatory Updates
 Review of Pain Management with Clinical and Regulatory Updates Palliative Care Collaborative: 8 th Annual Regional Conference October 10, 2014 Michael Stellini, M.D.,M.S. Medical Director, Hospice and
Review of Pain Management with Clinical and Regulatory Updates Palliative Care Collaborative: 8 th Annual Regional Conference October 10, 2014 Michael Stellini, M.D.,M.S. Medical Director, Hospice and
Objectives: What is your Definition of Pain? 8/16/2017
 Safe Opioid Management for the Seriously Ill Patient Sam Perna, D.O. Objectives: MDB1 1) Participants will understand the way the body s pain system works. 2) Participants will identify the elements of
Safe Opioid Management for the Seriously Ill Patient Sam Perna, D.O. Objectives: MDB1 1) Participants will understand the way the body s pain system works. 2) Participants will identify the elements of
UMC Health System Patient Label Here. PHYSICIAN ORDERS Diagnosis
 Diagnosis Weight Allergies Patient Care Vital Signs Per Unit Standards q12h q12h, Temperature Only - Every Shift and PRN Patient Activity Assist as Needed, Bed Position: As Tolerated, elevate to patient
Diagnosis Weight Allergies Patient Care Vital Signs Per Unit Standards q12h q12h, Temperature Only - Every Shift and PRN Patient Activity Assist as Needed, Bed Position: As Tolerated, elevate to patient
@FeliciaJCox. Caring for the person with addiction in the acute pain setting. Felicia Cox FRCN MSc RN
 @FeliciaJCox Caring for the person with addiction in the acute pain setting Felicia Cox FRCN MSc RN Disclosures Editor - British Journal of Pain Associate Editor - Pain Clinical Updates (IASP PAIN Reports)
@FeliciaJCox Caring for the person with addiction in the acute pain setting Felicia Cox FRCN MSc RN Disclosures Editor - British Journal of Pain Associate Editor - Pain Clinical Updates (IASP PAIN Reports)
2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio (740) ~
 ~") 2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio 43130 (740) 687-8000 ~ www.fmchealth.org Introduction The purpose of this module is to reduce the risk of adverse outcomes for adult patients
2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio 43130 (740) 687-8000 ~ www.fmchealth.org Introduction The purpose of this module is to reduce the risk of adverse outcomes for adult patients
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain
 Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
Approach to Acute Pain Management
 Approach to Acute Pain Management Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Approach to Acute Pain Management Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Objectives. Patient Controlled Analgesia (PCA) Management in the Seriously Ill. Discuss principles for opioid dosing and titration for acute pain
 Management in the Seriously Ill. Discuss principles for opioid dosing and titration for acute pain") Patient Controlled Analgesia (PCA) Management in the Seriously Ill Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Associate Director, Colorado
Patient Controlled Analgesia (PCA) Management in the Seriously Ill Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Associate Director, Colorado
Cancer Pain: A Clinical Overview. Linda A. King, MD Section of Palliative Care and Medical Ethics
 Cancer Pain: A Clinical Overview Linda A. King, MD Section of Palliative Care and Medical Ethics Objectives Define Palliative Care Review prevalence of cancer pain Know barriers to cancer pain management
Cancer Pain: A Clinical Overview Linda A. King, MD Section of Palliative Care and Medical Ethics Objectives Define Palliative Care Review prevalence of cancer pain Know barriers to cancer pain management
Opioid Pain Management. John Manfredonia, DO. Disclosures. Dr. Manfredonia discloses his employment as Regional Medical Director for VistaCare
 Opioid Pain Management John Manfredonia, DO Disclosures Dr. Manfredonia discloses his employment as Regional Medical Director for VistaCare VistaCare has provided commercial support for this activity Palliative
Opioid Pain Management John Manfredonia, DO Disclosures Dr. Manfredonia discloses his employment as Regional Medical Director for VistaCare VistaCare has provided commercial support for this activity Palliative
PAIN. TREATMENT TABLES Analgesics. NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose
 Duration Initial Dose") NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Opioid overdose versus opioid toxicity. Dr Colette Reid
 Opioid overdose versus opioid toxicity Dr Colette Reid Overview Asked to discuss and clarify the differences between the two entities Literature searches: opioids and overdose; opioids and toxicity; opioids
Opioid overdose versus opioid toxicity Dr Colette Reid Overview Asked to discuss and clarify the differences between the two entities Literature searches: opioids and overdose; opioids and toxicity; opioids
UMC Health System Patient Label Here PHYSICIAN ORDERS
 Diagnosis Weight Allergies Patient Care Vital Signs Per Unit Standards q12h q12h, Temperature Only - Every Shift and PRN Patient Activity Assist as Needed, Bed Position: As Tolerated, elevate to patient
Diagnosis Weight Allergies Patient Care Vital Signs Per Unit Standards q12h q12h, Temperature Only - Every Shift and PRN Patient Activity Assist as Needed, Bed Position: As Tolerated, elevate to patient
OAT Transitions - focus on microdosing. Mark McLean MD MSc FRCPC CISAM DABAM
 OAT Transitions - focus on microdosing Mark McLean MD MSc FRCPC CISAM DABAM Disclosures No pharmaceutical industry or other financial conflicts of interest Study Physician for research funded by Canadian
OAT Transitions - focus on microdosing Mark McLean MD MSc FRCPC CISAM DABAM Disclosures No pharmaceutical industry or other financial conflicts of interest Study Physician for research funded by Canadian
Tips for Managing Acute Pain
 Tips for Managing Acute Pain Daniel Johnson, MD, FAAHPM Kaiser Permanente University of Colorado Session Outline 1. Pseudoaddiction 2. Opioid Selection 3. PCA Titration 4. Co-Analgesics 5. Breakthrough
Tips for Managing Acute Pain Daniel Johnson, MD, FAAHPM Kaiser Permanente University of Colorado Session Outline 1. Pseudoaddiction 2. Opioid Selection 3. PCA Titration 4. Co-Analgesics 5. Breakthrough
Buprenorphine pharmacology
 Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
UCSF: 150 years in the making
 Securing Hospital Approval for Ketamine use on the Wards: Challenges, Outcomes and Lessons Learned Acknowledgements Mark Schumacher Ph.D.,M.D. Professor and Chief, Division of Pain Medicine Dept. of Anesthesia
Securing Hospital Approval for Ketamine use on the Wards: Challenges, Outcomes and Lessons Learned Acknowledgements Mark Schumacher Ph.D.,M.D. Professor and Chief, Division of Pain Medicine Dept. of Anesthesia
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT
 and acute pain management on MAT") An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program North Sydney April 12, 2018 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program North Sydney April 12, 2018 This speaker has been asked to disclose to the audience any involvement with
Pain Management in the Hospital
 E P E C O Pain Management in the Hospital Denise Waugh, MD FACEP FAAHPM Medical Director of Palliative Care Services Scott and White Healthcare 724-6859 Pain is a more terrible lord of mankind than even
E P E C O Pain Management in the Hospital Denise Waugh, MD FACEP FAAHPM Medical Director of Palliative Care Services Scott and White Healthcare 724-6859 Pain is a more terrible lord of mankind than even
Acute Pain NETP: SEPTEMBER 2013 COHORT
 Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Fairview Southdale Hospital Total Points: 50 RN/LPN Medication Assessment Passing: 45
 Fairview Southdale Hospital Total Points: 50 RN/LPN Medication Assessment Passing: 45 1. Your diabetic patient is to be started on an insulin drip at 8 units/hour. The insulin is supplied: 100 units in
Fairview Southdale Hospital Total Points: 50 RN/LPN Medication Assessment Passing: 45 1. Your diabetic patient is to be started on an insulin drip at 8 units/hour. The insulin is supplied: 100 units in
Tapering Opioids Best Practices*
 Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
Demystifying Opioid Conversion Calculations
 Demystifying Opioid Conversion Calculations Stephanie Cheng, PharmD, MPH, BCGP Clinical Pharmacist Hospice Pharmacy Solutions November 28, 2018 Learning Objectives After this presentation, you should be
Demystifying Opioid Conversion Calculations Stephanie Cheng, PharmD, MPH, BCGP Clinical Pharmacist Hospice Pharmacy Solutions November 28, 2018 Learning Objectives After this presentation, you should be
Acute Pain Management in the Hospital Setting. Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX
 Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Pain management in Paediatric Palliative Care. Dr Jane Nakawesi 14 th August 2017
 Pain management in Paediatric Palliative Care Dr Jane Nakawesi 14 th August 2017 Content Management of pain in children Non pharmacological Pharmacological Exit level outcomes The participants will: Know
Pain management in Paediatric Palliative Care Dr Jane Nakawesi 14 th August 2017 Content Management of pain in children Non pharmacological Pharmacological Exit level outcomes The participants will: Know
RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM ACPE UAN: 107-000-14-016-L05-P Activity Type: Application-Based 0.1 CEU/1.0 hr Learning Objectives for
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM ACPE UAN: 107-000-14-016-L05-P Activity Type: Application-Based 0.1 CEU/1.0 hr Learning Objectives for
Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test
 Analgesia Community Nurses Competency Test") Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test 1 Intraspinal (Neuraxial) Analgesia for Community Nurses Competency Test 1) Name the two major classifications of pain. i. ii. 2) Neuropathic
Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test 1 Intraspinal (Neuraxial) Analgesia for Community Nurses Competency Test 1) Name the two major classifications of pain. i. ii. 2) Neuropathic
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015
 Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Steven Prakken MD Chief, Medical Pain Service Duke Pain Medicine
 Steven Prakken MD Chief, Medical Pain Service Duke Pain Medicine International Association for the Study of Pain "Pain is an unpleasant sensory and emotional experience associated with actual or potential
Steven Prakken MD Chief, Medical Pain Service Duke Pain Medicine International Association for the Study of Pain "Pain is an unpleasant sensory and emotional experience associated with actual or potential
Assessment. Consults & Referrals
 University of Virginia Health System Clinical Pathway: Whipple Enhanced Recovery After () LOS: 4-5 days Date of Origin/Revision: June 29, 2016/September 6, 2017/January 31, 2018 : SAS : : : D1 D2 D 3/
University of Virginia Health System Clinical Pathway: Whipple Enhanced Recovery After () LOS: 4-5 days Date of Origin/Revision: June 29, 2016/September 6, 2017/January 31, 2018 : SAS : : : D1 D2 D 3/
Palliative Emergencies. Ken Stakiw
 Palliative Emergencies Ken Stakiw Disclosure None to disclose for this lecture Have received honoraria from a number of agencies and companies previously Intend to discuss some off label use of medications
Palliative Emergencies Ken Stakiw Disclosure None to disclose for this lecture Have received honoraria from a number of agencies and companies previously Intend to discuss some off label use of medications
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
Disclosures: These presenters have no financial relationships with commercial interests.
 Session: L146 Session: L318 Back Pain in the Painful Patient: Opioid Abuse, Buprenorphine, and Now the Operating Room! Geeta Nagpal, M.D., Vincent M. Tupper, M.D. Northwestern University, Chicago, IL Disclosures:
Session: L146 Session: L318 Back Pain in the Painful Patient: Opioid Abuse, Buprenorphine, and Now the Operating Room! Geeta Nagpal, M.D., Vincent M. Tupper, M.D. Northwestern University, Chicago, IL Disclosures:
Opioid Overdose Best Practices Guideline. Table of Contents. A. General description: B: Typical signs and symptoms:
 Opioid Overdose Best Practices Guideline Table of Contents A. General description B. Typical signs and symptoms C. Expected course D. Making the diagnosis E. Recommended treatment F. Criteria for hospital
Opioid Overdose Best Practices Guideline Table of Contents A. General description B. Typical signs and symptoms C. Expected course D. Making the diagnosis E. Recommended treatment F. Criteria for hospital
Dose equivalent of fentanyl patch to oxycontin
 Dose equivalent of fentanyl patch to oxycontin 10-3-2018 Detailed dosage guidelines and administration information for OxyContin (oxycodone hydrochloride). Includes dose adjustments, warnings and precautions.
Dose equivalent of fentanyl patch to oxycontin 10-3-2018 Detailed dosage guidelines and administration information for OxyContin (oxycodone hydrochloride). Includes dose adjustments, warnings and precautions.
OPIOID MANAGEMENT. Caroline Ha MD. Assistant Professor of Palliative Medicine
 OPIOID MANAGEMENT Caroline Ha MD Assistant Professor of Palliative Medicine None 1. Review how to select an appropriate opioid for patients based on medical and psychosocial information. 2. Review when
OPIOID MANAGEMENT Caroline Ha MD Assistant Professor of Palliative Medicine None 1. Review how to select an appropriate opioid for patients based on medical and psychosocial information. 2. Review when
Multiple Choice Questions
 Multiple Choice Questions 25yo M presents without psychiatric or medical history, with complaint of tremor to the ER. He denies drinking alcohol but his friend at bedside takes you to the side and reports
Multiple Choice Questions 25yo M presents without psychiatric or medical history, with complaint of tremor to the ER. He denies drinking alcohol but his friend at bedside takes you to the side and reports
Management of Cancer Pain
 Management of Cancer Pain Mihir M. Kamdar, MD Associate Director, Palliative Care Director, MGH Cancer Pain Clinic Depts of Anesthesia Pain/Palliative Care Massachusetts General Hospital None Disclosures
Management of Cancer Pain Mihir M. Kamdar, MD Associate Director, Palliative Care Director, MGH Cancer Pain Clinic Depts of Anesthesia Pain/Palliative Care Massachusetts General Hospital None Disclosures
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Medications for the Treatment of Neuropathic Pain
 Medications for the Treatment of Neuropathic Pain February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation Neuropathic Pain Pain, paresthesias, and sensory
Medications for the Treatment of Neuropathic Pain February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation Neuropathic Pain Pain, paresthesias, and sensory
Analgesia is a labeled indication for all of the approved drugs I will be discussing.
 Comparative Opioid Pharmacology Disclosure Analgesia is a labeled indication for all of the approved drugs I will be discussing. I ve consulted with Glaxo (remifentanil), Abbott (remifentanil), Janssen
Comparative Opioid Pharmacology Disclosure Analgesia is a labeled indication for all of the approved drugs I will be discussing. I ve consulted with Glaxo (remifentanil), Abbott (remifentanil), Janssen
morphine 30 mg/ 30 ml (1 mg/ml) Opioid of choice
 Opioid of choice") PATIENT CONTROLLED ANALGESIA (PCA) PLAN Allergies: Medication Selection: morphine 30 mg/ 30 ml (1 mg/ml) Opioid of choice HYDROmorphone (Dilaudid ) 6 mg/ 30 ml (0.2 mg/ml) fentanyl 300 mcg/ 30 ml (10 mcg/ml)
PATIENT CONTROLLED ANALGESIA (PCA) PLAN Allergies: Medication Selection: morphine 30 mg/ 30 ml (1 mg/ml) Opioid of choice HYDROmorphone (Dilaudid ) 6 mg/ 30 ml (0.2 mg/ml) fentanyl 300 mcg/ 30 ml (10 mcg/ml)
Managing Pain in the Patient with Opioid Use Disorder: Inpatient Management. Melissa Weimer, DO, MCR Oregon Health & Science University
 Managing Pain in the Patient with Opioid Use Disorder: Inpatient Management Melissa Weimer, DO, MCR Oregon Health & Science University 1 Educational Objectives At the conclusion of this activity participants
Managing Pain in the Patient with Opioid Use Disorder: Inpatient Management Melissa Weimer, DO, MCR Oregon Health & Science University 1 Educational Objectives At the conclusion of this activity participants
CLINICAL GUIDELINES FOR END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES
 CLINICAL GUIDELINES F END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES OPENING STATEMENT: Insert Facility Name is committed to providing effective end-of-life symptom management to all residents. Symptom
CLINICAL GUIDELINES F END OF LIFE CARE MEDICATIONS IN LONG TERM CARE HOMES OPENING STATEMENT: Insert Facility Name is committed to providing effective end-of-life symptom management to all residents. Symptom
Analgesia. This is widely used in palliative care. It has antipyretic and analgesic effects but no anti-
 Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Disclosures. Ms. Walsh has nothing to disclose Ms. Broglio is on the speaker s bureau for Genentech and Meda Pharmaceuticals
 Anne F. Walsh, MSN, ANP BC, ACHPN, CWOCN Kathleen Broglio, MN, ANP BC, ACHPN, CPE Disclosures Ms. Walsh has nothing to disclose Ms. Broglio is on the speaker s bureau for Genentech and Meda Pharmaceuticals
Anne F. Walsh, MSN, ANP BC, ACHPN, CWOCN Kathleen Broglio, MN, ANP BC, ACHPN, CPE Disclosures Ms. Walsh has nothing to disclose Ms. Broglio is on the speaker s bureau for Genentech and Meda Pharmaceuticals
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin