Demystifying Buprenorphine Prescribing for Youth With Opioid Use Disorders. Providers Clinical Support System Opioid Therapies (PCSSO) CME 6/21/2017
|
|
|
- Gloria Annis Walters
- 6 years ago
- Views:
Transcription
1 Demystifying Buprenorphine Prescribing for Youth With Opioid Use Disorders Geetha A. Subramaniam MD, DFAACAP, DFAPA National Institute on Drug Abuse June 21, Providers Clinical Support System Opioid Therapies (PCSSO) Grant funded by SAMHSA Coalition of professional organizations Overarching goal: To offer evidence-based trainings on the safe and effective prescribing of opioid medications in the treatment of pain and/or opioid addiction. AAP = 2 Webinars per grant year (6 total) 2 CME CME credit is available for this Webinar upon completion of an evaluation. More information will be provided near the end of this presentation. 3 1
2 Speaker Geetha A Subramaniam MD, DFAACP, DFAPA The speaker has no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or provider(s) of commercial services discussed in this CME activity. Dr Subramaniam does intend to discuss an unapproved/investigative use of a commercial product/device in this presentation. 4 Educational Objectives At the conclusion of this activity participants should be able to: Describe the risk factors for and consequences of non-medical use of opioid medication in the pediatric population. Describe current treatment options for opioid use disorder (OUD) Learn the approach to office-based treatment with buprenorphine for detoxification and maintenance of remission for adolescent OUD. Implement an office-based treatment regimen with buprenorphine for adolescent OUD List factors that impact treatment retention and effectiveness in these patients Review the current training and DEA requirements for prescription of buprenorphine. 5 First Some Basics Terminology: Opium, opiate, opioid 3 OP Receptors: Mu (MOP), Kappa (KOP) & Delta (DOP) Types: Natural: morphine, codeine Semi-synthetic: oxycodone, hydrocodone, heroin, buprenorphine Synthetic: methadone, Fentanyl 6 2

3 Adolescent Brain Development Brain size peaks at 14-15y Increase in white matter (connectivity) Brain blood/oxygen flow in adolescence decreases into adulthood (i.e. the system is getting more energy efficient) Source: National Institute on Drug Abuse; National Institutes of Health; U.S. Department of Health and Human Services. Adapted from slide by James Bjork, PhD 7 During Adolescence: Brain Structures Governing Cognitive Control and Reward Behavior Are still Developing Inhibitory Control Habit Formation Maturation/thinning of frontal cortex is last/delayed relative to other cortical areas Motivation/Drive Reward Salience Memory Adapted from slide by James Bjork, Ph.D 8 Drugs of Abuse Interfere with the Brain s Natural Learning Circuits Addiction could result from the hijacking of learning circuitry Liking Wanting Source: National Institute on Drug Abuse; National Institutes of Health; U.S. Department of Health and Human Services. Drugs may cause the brain to artificially remember (learn) the high too strongly- people may then want the drug even though they no longer like the way it makes them feel. Slide adapted from James Bjork, Ph.D 9 3

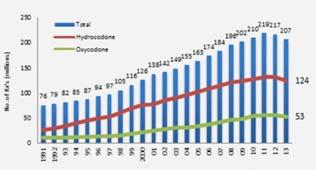


4 At the level of the Receptor _drug_abuse_report_ pdf

5 13 Monitoring the Future (MTF) Study Heroin Non-Heroin Source: Johnston LD, et al., Monitoring the Future National Results on Adolescent Drug Use: Overview of Key Findings, Heroin Admissions in 2015: by gender, age and ethnicity 15 5
6 Non-Heroin Opioid Admissions 2015: by gender, age and ethnicity 16 Age of First Use of Opioids Treatment Episode Dataset (TEDS): (youth treatment admissions for primary Opioid problem) 11 and <11y 12-14y 15-17y 18-20y 63.2 Percentage y 18-20y OAS:SAMHSA. Treatment Episode Data Set -- Admissions (TEDS-A) -- Concatenated, accessed Dec Self-reported Drug of First Choice Subramaniam and Stitzer-Drug Alcohol Depend (2009) 18 6
7 What are the Characteristics of Youth With Opioid Use Disorder Presenting to Treatment? Older teen (> 16 y) Mostly male (but high proportion of female) Predominantly Caucasian (~ 90%) Poor Academic performance, drop out of school Reside in non-urban areas Higher rates of Multiple Substance use (cannabis most common) High rates of Psychiatric Disorders (> 70%) High Injection Drug Use among heroin users (40-70%) Hopfer et al., 2000; Clemmey et al., 2004; Gordon et al., 2004; Marsch et al., 2005; Subramaniam and Stitzer., 2009, Subramaniiam et al, DSM-5 Criteria for Substance Use Disorder 1. Use in larger amounts or for longer periods of time than intended 2. Unsuccessful efforts to cut down or quit. 3. Excessive time spent taking the drug 4. Failure to fulfill major obligations 5. Continued use despite knowledge of problems 6. Important activities given up 7. Recurrent use in physically hazardous situations 8. Continued use despite social or interpersonal problems 9. Tolerance 10. Withdrawal 11. Craving Severity is designated according to the number of symptoms endorsed: 0-1: No diagnosis 2-3: mild SUD 4-5 : moderate SUD 6 or more: Severe SUD Slide courtesy of Sharon Levy, MD, FAAP 20 Physiologic Adaptations: Tolerance and Withdrawal Tolerance is the need for increasing amounts of the substance to achieve the desired effect. Withdrawal is a physiological response to a rapid decline in receptor binding, due to either rapidly decreasing concentrations of the opioid, or presence of a blocking agent. Tolerance and withdrawal alone are not sufficient to make a diagnosis of addiction. Slide courtesy of Sharon Levy, MD, FAAP 21 7
 or similar scale 22 Overview of Treatment for Opioid Use Disorder Non-pharmacologic Residential")
8 Opioid Withdrawal Symptoms Early 6 hours Peak -72hours Dysphoric Mood/Anxiety Nausea/Vomiting Runny nose Diarrhea Muscle aches/cramps Stomach cramps Lacrimation Cravings Sweating Goosebumps Tachycardia Depression Hypertension Typically rated using Clinical Opioid Withdrawal Scale (COWS) or similar scale 22 Overview of Treatment for Opioid Use Disorder Non-pharmacologic Residential Treatment Intensive Outpatient/Partial 12-Step Fellowships Individual or Group Therapy Family Therapy Therapeutic School/Community Pharmacologic Detoxification: buprenorphine, methadone, clonidine, comfort meds Maintenance Agonist Therapy methadone, buprenorphine (partial) Antagonist Therapy naltrexone PO or IM Opioid dependence is a chronic, relapsing neurological condition; patients who remain in long term treatment generally do best. Supportive therapy combined with pharmacologic treatment seems to produce the best outcomes. 23 Comparison of Receptor Activity Level: Full vs. Partial Agonist vs. Antagonist e.g. Methadone e.g. Buprenorphine e.g. Naltrexone Note partial agonists never fully activate the receptor, even at very high doses. Slide Courtesy of Sharon Levy, MD, PCSS-O 24 8


9 Role of Pediatrician: Screen, Identify and Intervene Slide courtesy of Sharon Levy, MD, FAAP 25 Role of Pediatrician: Educate Easy to get from medicine cabinet 62% Available everywhere 52% Not illegal 51% Easy to get through other people s prescriptions 50% Can claim you have a prescription if caught 49% Cheap 43% Safer to use than illegal drugs 35% Less shame attached to using 33% Easy to purchase over the Internet 32% Fewer side effects than street drugs 32% Parents don t care as much if you get caught 21% Slide courtesy of Sharon Levy, MD, FAAP Partnership for Drug-Free Kids. The Partnership Attitude Tracking Study (PATS): Teens in grades 7 through ; May 16, AAP Policy The AAP recommends that pediatricians consider offering pharmacological treatments to their adolescent and young adult patients with moderate/severe opioid use disorders and/or discuss referrals to other providers for this service
10 CTN Study: Buprenorphine for Youth OUD Opioid Positive Urines: 12 weeks Bup vs Detox (Missing = Positive, N=152) DETOX (imputed) BUP (imputed) Group Effect = p<.0001 Time Effect = NS Time X Group = p<.05 Baseline Week 4 Week 8 Week 12 Woody et al., JAMA, Drivers of Treatment Success Abstinence from Opioids: Early abstinence, staying in treatment, receiving additional non-study medications; baseline injection use and having severe medical/ psychiatric problems Retention in Treatment: Early adherence to treatment, early opioid negative urine drug screen, any medication treatment in the month prior to study entry, non-heroin use. Lower retention: Emerging adults (vs. older adults). Daily dosing is associated with lower retention 29 Buprenorphine Formulations Film Strips Brand name only. Combination with naloxone Suboxone sublingual film. Available as 2(.5), 4(1), 8(2) or 12(3) mg Bunavail buccal film. Available as 2.1 (0.3), 4.2 (0.7) or 6.3 (1)mg Dissolve more rapidly than tablets (advantage for observed dosing) Individually wrapped, reduces accidental ingestion by young children CAUTION: Accidental ingestion of buprenorphine by young children may result in over sedation and respiratory suppression. Individually wrapped films may reduce accidental ingestion
11 Buprenorphine Formulations Tablets Available as generic Combo (buprenorphine/naloxone) and mono (buprenorphine) available 2(.5)/8 (2) mg formulations available Newer 1.4(0.36)/5.7(1.4) menthol-flavored Zubsolv tablets (combo) Mono-product has higher misuse potential; indicated only in pregnancy. CAUTION: Accidental ingestion of buprenorphine by young children may result in over sedation and respiratory suppression. Adapted from a slide by Sharon Levy, MD, FAAP 31 Begin with a Comprehensive Initial Evaluation Complete history of substance use, past treatments Medical history and review of systems Current medications and Allergies Brief Psychiatric History - Suicide/Depression/ADHD Psychosocial history including psychosocial support Physical exam OUD Diagnosis DSM 5 criteria Treatment Plan, including medications prescribed Plan for Referral - Psychiatric disorders, Hepatitis-C infection, etc. 32 Opioid Withdrawal Symptoms Early 6 hours Peak -72hours Dysphoric Mood/Anxiety Nausea/Vomiting Runny nose Diarrhea Muscle aches/cramps Stomach cramps Lacrimation Cravings Sweating Goosebumps Tachycardia Depression Hypertension Typically rated using Clinical Opioid Withdrawal Scale (COWS) or similar scale 33 11
12 Withdrawal Management Buprenorphine is started when the patient is in active opioid withdrawal: Plan in advance as patients must be opioid-free for several hours and present in active withdrawal Offer ancillary medications (clonidine, ibuprofen, Peptobismol, Bentyl/other meds for stomach cramps) Use a treatment contract Be available for check-ins and dose adjustments in the first few days of withdrawal management 34 Sample Buprenorphine Contract I agree to stop using all drugs, including opioids, alcohol, marijuana and other street drugs. I will request additional support if I am unable to remain drug free. I understand that it is dangerous to mix buprenorphine with alcohol or other sedatives (such as Valium, Klonopin, Ativan). Mixing could result in accidental overdose, coma or death. I will not use alcohol or sedatives while I am taking buprenorphine. Buprenorphine may make me sleepy. I will not drive a car or operate dangerous machinery while taking buprenorphine until I have been cleared to do so. I agree to cooperate with urine drug testing whenever requested by my doctor to detect whether I have used substances. My doctor will decide how often I should be tested; in most cases I will be tested AT LEAST weekly. I will schedule and keep all recommended appointments. My parent or guardian will accompany me to my appointments until I have been cleared to come by myself. I agree that my parent or guardian will hold my buprenorphine medication. I will never sell, share or otherwise distribute my medication. My parent will provide me one dose at a time and watch me take it. If my medication is accidentally swallowed by a child I will call 911 or Poison Control at I will always take my buprenorphine by placing it under my tongue to d be absorbed. I will never inject buprenorphine because IV use can lead to sudden and severe opioid withdrawal. I will not skip or alter doses without speaking to my doctor. I will give consent for my doctor to communicate with physicians, therapists, probation officers and parents to discuss my treatment and progress, including drug test results. I will report changes in my medical condition to my doctor so that all of my treatment can be coordinated. I will discuss pain management prior to any elective procedure and as soon as possible after an emergency. I agree to participate in counseling to support my medical treatment. I will discuss a counseling plan with my doctor. PATIENT SIGNATURE AND DATE: 35 Induction Ensure that young women are not pregnant Start medication when a COWS indicates moderate withdrawal (>8). Abstinence prior to starting buprenorphine hrs for short-acting opioids (heroin) hrs for sustained-release opioid medications 36 hrs for methadone (30mg x 2 weeks; 15mg x 1 day; no methadone x 1 day; then induce on BUP/NX) Obtain a baseline urine drug screen Adapted from a Slide by Sharon Levy, MD, FAAP 36 12
13 Induction Start with 2-4 mg. Observe the first dose (and demonstrate for parents) Rescore COWS after 45 min If the score has decreased but still indicates moderate withdrawal, administer a second dose Some patients will have withdrawal symptoms controlled with 4 mg; for others consider a second 2-4 mg dose few hours later Advise the patient not to change the dose without speaking to a physician. Titrate dose to suppress withdrawal symptoms and cravings. 37 Buprenorphine Side Effects and Drug Interactions Generally well tolerated when used as prescribed. Common side effects: Headache Nausea/vomiting Constipation Urinary retention/hesitancy Drowsiness Dry mouth Perspiration Sexual dysfunction/decreased libido It is very rare that one has to discontinue meds due to AEs Elevations in liver transaminases possible (rare, but patients with Hep C are at higher risk) Few clinically significant drug interactions; particularly uncommon in adolescents 38 Follow-up See patients frequently while on medication weekly until a stable dose is achieved, and then at least monthly after that. Ask about medication adherence and side effects Evaluate and monitor mental health symptoms. Use patient history, parental report and drug testing to monitor sobriety and medication adherence. For patients on buprenorphine, titrate the dose to balance craving suppression and side effects. Most adolescents will stabilize on a dose between 4 and 16 mg buprenorphine per day. Slide courtesy of Sharon Levy, MD, FAAP 39 13

14 AAP Policy Urine drug testing may have a role in assessing adolescents for substance use disorders in certain circumstances, and in monitoring adolescents in treatment for an identified substance use disorder. Invasive Complex potential for false positive false negative results Confidentiality issues Never be the sole basis for making a diagnosis 40 Maintaining and Terminating Medications The optimal length of time for medication treatment is not known. In adults longer duration of treatment is associated with better abstinence outcomes. There are no long-term studies in youth and the impact of exposure to long term agonists/antagonists on the developing brain are unknown. As a clinical rule of thumb, we recommend avoiding changing medications during periods of stress final exams, summer vacation, high school graduation, etc. Patients who discontinue medications should continue in counseling and should be monitored closely for relapse for an extended period of time. Slide courtesy of Sharon Levy, MD, FAAP 41 Preventing and Managing Relapse Encourage patients to remain abstinent from all substances to minimize the chance of a relapse to opioid use. Advise patients and parents to plan structured time If employed, advise parents to monitor income. Encourage patients and families to continue monitoring over the summer, as substance use tends to increase when kids are out of school. Maintain or increase prosocial/psycho-social activities over the summer: individual counseling, group programs, 12-step meetings, etc

, hypothermia, non-cardiogenic")
15 Psychiatric Care and Psychosocial Support Patients should be evaluated and treated concurrently for co-occurring psychiatric disorders. Integrated care or referral to specialty MH care All patients in treatment for OUD should have regular psychosocial support via individual or group counseling with an experienced counselor. Behavioral treatment options: Motivational Interviewing/MET, Contingency management, CBT, family therapy, 12-step facilitationa 12-step meetings are free and universally available. Another option is SMART recovery 43 Treatment of Opioid Overdose Signs: Respiratory depression usual cause of death Coma, pinpoint pupils (may dilate with hypoxia), hypothermia, non-cardiogenic pulmonary edema Treatment: Naloxone (Narcan) nasal or IV., prn EVZIO autoinjector application If no response, treat for sedative/hypnotic OD Monitor methadone overdose patients for hrs. Single naloxone dose lasts 1-4 hours Naloxone may not work well for buprenorphine because of the higher receptor affinity. Distribution of intranasal naloxone is a major public health initiative that has reduced mortality from opioid overdose. Patients and parents can fill a prescription for naloxone from the treating physician or receive naloxone and training from a local public health department. 44 Diversion and PDMP Diversion refers to giving away or selling or giving a prescribed medication. There are 2 main situations in which diversion occurs: Opioid-dependent individuals illegally purchasing buprenorphine to treat their dependence vs. non-opioid dependent individuals using buprenorphine for euphoria Teens may also sell or trade it for other drugs. Prescription Drug Monitoring Programs (PDMP): are staterun electronic databases used to track the prescribing and dispensing of controlled prescription drugs to patients. As with any other medication, careful prescription monitoring is essential. Monitor lost prescriptions, requests for early refills or increasing dosage
16 Parents Are often aware of the teen s addiction (to opioids) Often benefit from education about opioids, complications, treatment options Can be encouraged play a supportive role ensure adherence to medications, treatment, meetings, etc. May benefit from guidance on how to provide structure, support and positive reinforcement for success Patient confidentiality issues need to be respected Educated about overdose (OD) and OD prevention strategies May benefit from referral for personal treatment 46 Documentation Follow-up Visits (Prescriptions) At Follow-up visits: Self-report of substance use, not limited to opioids Reports of medication adherence, side effects, cravings Participation in school and/or work and establish goals Participation in counseling, support groups Urine drug tests and other lab tests, if indicated Collateral report on progress (from parent or guardian) if available Treatment plan including dose/changes to medications prescribed Prescribers must keep a record of every prescription written for each patient. The DEA periodically audits buprenorphine prescribers to insure best practices are maintained 47 Confidentiality Teens Presenting With Parents In many cases, especially those with OUD, adolescents will present for treatment with the knowledge, and often with the support, of parents. Managing confidentiality is a clinical decision. Consider: Sharing clinical impressions and treatment recommendations. Involve parents if a teen s behavior puts him/her in acute danger. Parents can be taught to effectively monitor and support recovery Avoid sharing details that are not directly relevant to treatment. Parents have access to medical records and may seek information if they desire
17 Confidentiality Laws Rules regarding emancipation or mature minors which allow children under the age of majority (usually 18y) to obtain medical care are dictated by states. Check with a lawyer or other expert regarding local law. In most states, minors can access substance abuse services without parental consent. NOTE: Treating without specific parental consent does not guarantee confidentiality. In fact, protecting confidentiality between adolescent and parent can be particularly difficult. Therefore we recommend involving a parent in treatment whenever possible, though in most cases involving parents is best treated as a treatment goal rather than a requirement. 49 Confidentiality HIPPA and Title 42 CFR Part 2 In a general primary care setting, HIPPA rules guide the confidentiality protection of medical records, including information pertaining to substance use. Records for treatment of OUD should be handled similarly to other confidential information, such as information about substance use in other patients. For substance abuse programs, federal confidentiality regulations ( 42 CFR Part 2 ) supersede HIPPA. If federal confidentiality rules apply, a minor must sign a consent form for a program to release information to his or her parent or guardian. Adapted from a slide from Sharon Levy, MD, FAAP 50 DATA 2000 Waivers to provide office-based opioid dependence treatment (OBOT) Any physician eligible to apply for a waiver to prescribe buprenorphine for opioid dependence after completing 8 hours of waiver training Amendment: Prescribers must limit their practice to the allowable number of buprenorphine patients: up to 30 in the first year, up to 100 after the first year if the provider has obtained a waiver Comprehensive Addiction and Recovery Act (CARA) extends buprenorphine prescribing privileges to qualifying NPs and PAs who complete 24 hours of specific training and apply for waiver To date, few pediatricians have obtained waivers. Some teens may get treatment from adult providers, though there is often a gap in treatment services for younger teens
18 Ready to Get Waivered? Training Opportunities Online Training for AAP Members: Webinar Training: June 28, pm-9:30pm Pacific Half & Half Courses (online & in-person) July 18, pm-5pm Washington, DC pcssmat.org/event/half-and-half-pediatric-mat-waiver-training 52 Or Request a Training in Your Community The AAP can identify a trainer for you. The AAP can help support room rental and AV needs. requests to: substanceuse@aap.org 53 Q & A Please use the chat box to submit a question for the speakers. Obtaining CME After the event, you will receive a link taking you to an evaluation. Upon completion, you will be ed your CME certification. The American Academy of Pediatrics (AAP) is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to provide continuing medical education for physicians. The AAP designates this live activity for a maximum of 1.0 AMA PRA Category 1 Credit(s). Physicians should claim only the credit commensurate with the extent of their participation in the activity. This activity is acceptable for a maximum of 1.0 AAP credits. These credits can be applied toward the AAP CME/CPD Award available to Fellows and Candidate Members of the American Academy of Pediatrics. The American Academy of Physician Assistants (AAPA) accepts certificates of participation for educational activities certified for AMA PRA Category 1 Credit from organizations accredited by ACCME. Physician assistants may receive a maximum of 1.0 hours of Category 1 credit for completing this program. This program is accredited for 1.0 NAPNAP CE contact hours of which 0 contain pharmacology (Rx), (0 related to psychopharmacology) (0 related to controlled substances), content per the National Association of Pediatric Nurse Practitioners (NAPNAP) Continuing Education Guidelines
19 PCSS-O Colleague Support Program and Listserv PCSS-O Colleague Support Program is designed to offer general information to health professionals seeking guidance in their clinical practice in prescribing opioid medications. PCSS-O Mentors comprise a national network of trained providers with expertise in addiction medicine/psychiatry and pain management. Our mentoring approach allows every mentor/mentee relationship to be unique and catered to the specific needs of both parties. The mentoring program is available at no cost to providers. For more information on requesting or becoming a mentor visit: Listserv: A resource that provides an Expert of the Month who will answer questions about educational content that has been presented through PCSS-O project. To join pcss-o@aaap.org. 55 PCSS-O is a collaborative effort led by American Academy of Addiction Psychiatry (AAAP) in partnership with: Addiction Technology Transfer Center (ATTC), American Academy of Neurology (AAN), American Academy of Pain Medicine (AAPM), American Academy of Pediatrics (AAP), American College of Physicians (ACP), American Dental Association (ADA), American Medical Association (AMA), American Osteopathic Academy of Addiction Medicine (AOAAM), American Psychiatric Association (APA), American Society for Pain Management Nursing (ASPMN), International Nurses Society on Addictions (IntNSA), and Southeast Consortium for Substance Abuse Training (SECSAT). For more information visit: For questions pcss-o@aaap.org Funding for this initiative was made possible (in part) by Providers Clinical Support System for Opioid Therapies (grant no. 5H79TI025595) from SAMHSA. The views expressed in written conference materials or publications and by speakers and moderators do not necessarily reflect the official policies of the Department 56 of Health and Human Services; nor does mention of trade names, commercial practices, or organizations imply endorsement by the U.S. Government. 19
Managing Pain in the Patient with Opioid Use Disorder: Inpatient Management. Melissa Weimer, DO, MCR Oregon Health & Science University
 Managing Pain in the Patient with Opioid Use Disorder: Inpatient Management Melissa Weimer, DO, MCR Oregon Health & Science University 1 Educational Objectives At the conclusion of this activity participants
Managing Pain in the Patient with Opioid Use Disorder: Inpatient Management Melissa Weimer, DO, MCR Oregon Health & Science University 1 Educational Objectives At the conclusion of this activity participants
Addiction Prediction: Errors from the bedside hurt patients with pain. Objectives. CDC guideline for prescribing OPIOIDS for Chronic Pain
 Addiction Prediction: Errors from the bedside hurt patients with pain Renee C.B. Manworren, PhD, APRN, BC, PCNS-BC, AP-PMN, FAAN Director of Nursing Research and Professional Practice Posy and Fred Love
Addiction Prediction: Errors from the bedside hurt patients with pain Renee C.B. Manworren, PhD, APRN, BC, PCNS-BC, AP-PMN, FAAN Director of Nursing Research and Professional Practice Posy and Fred Love
Pain Care & Prescription Drug Abuse: Current Topics, Legislation & Policy. Disclosure. Preview
 Providers Clinical Support System for Opioid Therapies (PCSS-O) Webinar March 7, 2017 Pain Care & Prescription Drug Abuse: Current Topics, Legislation & Policy Wade Delk, Government Affairs Director, ASPMN
Providers Clinical Support System for Opioid Therapies (PCSS-O) Webinar March 7, 2017 Pain Care & Prescription Drug Abuse: Current Topics, Legislation & Policy Wade Delk, Government Affairs Director, ASPMN
Buprenorphine as a Treatment Option for Opioid Use Disorder
 Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Opioid Dependence 101 and Medication Assisted Treatment
 Opioid Dependence 101 and Medication Assisted Treatment Dr. Joji Suzuki Director of the Division of Addiction Psychiatry, Brigham & Women s Hospital Assistant Professor of Psychiatry, Harvard Medical School
Opioid Dependence 101 and Medication Assisted Treatment Dr. Joji Suzuki Director of the Division of Addiction Psychiatry, Brigham & Women s Hospital Assistant Professor of Psychiatry, Harvard Medical School
Course Overview Management of Chronic Pain: A Core Curriculum for Primary Care Providers
 Course Overview Management of Chronic Pain: A Core Curriculum for Primary Care Providers Sponsored by PCSS-O American Academy of Addiction Psychiatry Roger Chou, MD 1 About PCSS-O PCSS-O is a national
Course Overview Management of Chronic Pain: A Core Curriculum for Primary Care Providers Sponsored by PCSS-O American Academy of Addiction Psychiatry Roger Chou, MD 1 About PCSS-O PCSS-O is a national
Opioids for Pain Treatment in Persons with Opioid Use Disorder. Patricia Pade, MD Seddon R. Savage, MD, MS Melissa Weimer, DO, MCR
 Opioids for Pain Treatment in Persons with Opioid Use Disorder Patricia Pade, MD Seddon R. Savage, MD, MS Melissa Weimer, DO, MCR 1 Educational Objectives At the conclusion of this activity participants
Opioids for Pain Treatment in Persons with Opioid Use Disorder Patricia Pade, MD Seddon R. Savage, MD, MS Melissa Weimer, DO, MCR 1 Educational Objectives At the conclusion of this activity participants
The CARA & Buprenorphine Prescribing for APNs & PAs
 The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
Medication Assisted Treatment. Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs
 Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Main Results and Clinical Implications of the X:BOT Trial: XR-Naltrexone vs. Buprenorphine-Naloxone Film
 Main Results and Clinical Implications of the X:BOT Trial: XR-Naltrexone vs. Buprenorphine-Naloxone Film July 31 st, 2018 Hosted by John A. Renner, Jr., MD, DLFAPA Professor of Psychiatry Boston University
Main Results and Clinical Implications of the X:BOT Trial: XR-Naltrexone vs. Buprenorphine-Naloxone Film July 31 st, 2018 Hosted by John A. Renner, Jr., MD, DLFAPA Professor of Psychiatry Boston University
PCSS Projects. Kathryn L. Cates-Wessel Executive Director, AAAP PCSS-MAT and PCSS-O PI and Project Director
 PCSS Projects Kathryn L. Cates-Wessel Executive Director, AAAP PCSS-MAT and PCSS-O PI and Project Director 1 Educational Objectives At the conclusion of this activity participants should be able to: Describe
PCSS Projects Kathryn L. Cates-Wessel Executive Director, AAAP PCSS-MAT and PCSS-O PI and Project Director 1 Educational Objectives At the conclusion of this activity participants should be able to: Describe
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Nursing Regulatory Boards Efforts to Provide Guidance to Nurses About Mitigating Prescription Medication Abuse/Diversion
 Nursing Regulatory Boards Efforts to Provide Guidance to Nurses About Mitigating Prescription Medication Abuse/Diversion Cathy Carlson, PhD, APN, FNP-BC Aaron Gilson, MS, MSSW, PhD Authors Conflicts of
Nursing Regulatory Boards Efforts to Provide Guidance to Nurses About Mitigating Prescription Medication Abuse/Diversion Cathy Carlson, PhD, APN, FNP-BC Aaron Gilson, MS, MSSW, PhD Authors Conflicts of
Appendix F Federation of State Medical Boards
 Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
Opioid Use Disorders &Medication Treatment
 Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Pregnancy and Addiction
 Pregnancy and Addiction Carl Christensen, MD, PhD, D-FASAM Clinical Associate Professor, OB Gyn & Psychiatry Wayne State University School of Medicine November 16, 2016 1 Educational Objectives At the
Pregnancy and Addiction Carl Christensen, MD, PhD, D-FASAM Clinical Associate Professor, OB Gyn & Psychiatry Wayne State University School of Medicine November 16, 2016 1 Educational Objectives At the
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Overview of Opioid Use Disorder
 Overview of Opioid Use Disorder Doug Burgess, MD Medical Director of Outpatient Services, Truman Medical Centers Assistant Professor of Psychiatry, University of Missouri- Kansas City Objectives History
Overview of Opioid Use Disorder Doug Burgess, MD Medical Director of Outpatient Services, Truman Medical Centers Assistant Professor of Psychiatry, University of Missouri- Kansas City Objectives History
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets. Risk Evaluation and Mitigation Strategy (REMS) Program
 Program") SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
Opioid Use Disorders as a Brain Disease Why MAT is so important. Ron Jackson, M.S.W., L.I.C.S.W.
 Opioid Use Disorders as a Brain Disease Why MAT is so important Ron Jackson, M.S.W., L.I.C.S.W. Affiliate Professor School of Social Work University of Washington Organization Name: CareOregon Course Title:
Opioid Use Disorders as a Brain Disease Why MAT is so important Ron Jackson, M.S.W., L.I.C.S.W. Affiliate Professor School of Social Work University of Washington Organization Name: CareOregon Course Title:
Medication-Assisted Treatment (MAT) Overview
 Overview") Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Medication Assisted Treatment. MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment
 Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Financing Factors for Implementing Medication-Assisted Treatment
 Financing Factors for Implementing Medication-Assisted Treatment Jeremy Attermann, MSW, National Council for Behavioral Health Nick Szubiak, LCSW, National Council for Behavioral Health Brad DeCamp, MPA,
Financing Factors for Implementing Medication-Assisted Treatment Jeremy Attermann, MSW, National Council for Behavioral Health Nick Szubiak, LCSW, National Council for Behavioral Health Brad DeCamp, MPA,
BUPRENORPHINE and Office-Based Treatment of Opioid Use Disorder
 BUPRENORPHINE and Office-Based Treatment of Opioid Use Disorder Stephen A. Wyatt, DO Anthony Dekker, DO William Morrone, DO Funding for this initiative was made possible (in part) by Providers Clinical
BUPRENORPHINE and Office-Based Treatment of Opioid Use Disorder Stephen A. Wyatt, DO Anthony Dekker, DO William Morrone, DO Funding for this initiative was made possible (in part) by Providers Clinical
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Methadone Maintenance 101
 Methadone Maintenance 101 OTP/DAILY DOSING CLINICS - ANDREW PUTNEY MD Conflicts of Interest - Employed by Acadia HealthCare 1 Why Methadone? At adequate doses methadone decreases opioid withdrawal symptoms
Methadone Maintenance 101 OTP/DAILY DOSING CLINICS - ANDREW PUTNEY MD Conflicts of Interest - Employed by Acadia HealthCare 1 Why Methadone? At adequate doses methadone decreases opioid withdrawal symptoms
Opioid Use in Youth. Amy Yule M.D. March 2,
 Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
STOPPING OPIOIDS. William Morrone, DO MS, FACOFP DABAM DAAPM Deputy Chief Medical Examiner & AOAAM June 24, 2015 Noon ET
 STOPPING OPIOIDS William Morrone, DO MS, FACOFP DABAM DAAPM Deputy Chief Medical Examiner & AOAAM June 24, 2015 Noon ET 1 William Morrone DO, Disclosures William Morrone, DO has presented numerous programs
STOPPING OPIOIDS William Morrone, DO MS, FACOFP DABAM DAAPM Deputy Chief Medical Examiner & AOAAM June 24, 2015 Noon ET 1 William Morrone DO, Disclosures William Morrone, DO has presented numerous programs
Identification and Treatment of Opioid Use Disorders in Primary Care Settings
 Identification and Treatment of Opioid Use Disorders in Primary Care Settings 17th Annual Primary Care Symposium February 24, 2018 Kelly S. Barth, DO Associate Professor, Psychiatry & Internal Medicine
Identification and Treatment of Opioid Use Disorders in Primary Care Settings 17th Annual Primary Care Symposium February 24, 2018 Kelly S. Barth, DO Associate Professor, Psychiatry & Internal Medicine
Serious Mental Illness and Opioid Use Disorder
 Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Module II Opioids 101 Opiate Opioid
 BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module II Opioids 101 Module II Goals of the Module This module reviews the following:! Opioid addiction and the brain!
BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module II Opioids 101 Module II Goals of the Module This module reviews the following:! Opioid addiction and the brain!
GOALS AND OBJECTIVES
 SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
FY17 SCOPE OF WORK TEMPLATE. Name of Program/Services: Medication-Assisted Treatment: Buprenorphine
 FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Building capacity for a CHC response to Ontario's Opioid Crisis
 Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
MEDICATION ASSISTED TREATMENT
 MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
Prescription Opioids
 What are prescription opioids? Prescription Opioids Opioids are a class of drugs naturally found in the opium poppy plant. Some prescription opioids are made from the plant directly, and others are made
What are prescription opioids? Prescription Opioids Opioids are a class of drugs naturally found in the opium poppy plant. Some prescription opioids are made from the plant directly, and others are made
Hospitals Role in Addressing the Opioid Crisis
 Hospitals Role in Addressing the Opioid Crisis Webinar 5: Buprenorphine in the Emergency Department November 14, 2017 Agenda Hospital Based Buprenorphine Initiatives Yngvild Olsen, M.D., Medical Consultant,
Hospitals Role in Addressing the Opioid Crisis Webinar 5: Buprenorphine in the Emergency Department November 14, 2017 Agenda Hospital Based Buprenorphine Initiatives Yngvild Olsen, M.D., Medical Consultant,
The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine. March 10, 2016
 The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine March 10, 2016 Objectives Review current state of opioid crisis in Maine Briefly review physiology of
The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine March 10, 2016 Objectives Review current state of opioid crisis in Maine Briefly review physiology of
Mark Edlund, MD, PhD RTI International. Photo courtesy of The Herb Museum, Vancouver, BC
 Opioid Use Disorders and Their Treatment Mark Edlund, MD, PhD RTI International Photo courtesy of The Herb Museum, Vancouver, BC Acknowledgements Funded by NIDA R01 DA022560-01 NIDA R01 DA034627 NIDA R01
Opioid Use Disorders and Their Treatment Mark Edlund, MD, PhD RTI International Photo courtesy of The Herb Museum, Vancouver, BC Acknowledgements Funded by NIDA R01 DA022560-01 NIDA R01 DA034627 NIDA R01
Pharmacotherapy for opioid addiction. Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco
 Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They?
 Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
SW OREGON OPIOID SUMMIT. Medication Assisted Recovery for Opioid Use Disorder. Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass
 SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
Implementing Buprenorphine Treatment in Opioid Treatment Programs Webinar 2, October 3, 2018
 Implementing Buprenorphine Treatment in Opioid Treatment Programs Webinar 2, October 3, 2018 Judith Martin, MD, Medical Director of Substance Use Services, San Francisco Department of Public Health Webinar
Implementing Buprenorphine Treatment in Opioid Treatment Programs Webinar 2, October 3, 2018 Judith Martin, MD, Medical Director of Substance Use Services, San Francisco Department of Public Health Webinar
Opioid Agonists. Natural derivatives of opium poppy - Opium - Morphine - Codeine
 Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
NORTHWEST AIDS EDUCATION AND TRAINING CENTER. Opioid Use Disorders. Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Opioid Use Disorders Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014 Opioid Use Disorders Importance of opioid use disorders Screening and
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Opioid Use Disorders Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014 Opioid Use Disorders Importance of opioid use disorders Screening and
IntNSA Webinar Series
 BUPRENORPHINE CLINIC: A MULTIDISCIPLINARY MODEL FOR OPIOID MAINTENANCE THERAPY Stephen Strobbe, PhD, RN, NP, PMHCNS-BC, CARN-AP Monday, June 4, 2012 IntNSA Webinar Series Funding for this webinar was made
BUPRENORPHINE CLINIC: A MULTIDISCIPLINARY MODEL FOR OPIOID MAINTENANCE THERAPY Stephen Strobbe, PhD, RN, NP, PMHCNS-BC, CARN-AP Monday, June 4, 2012 IntNSA Webinar Series Funding for this webinar was made
Expanding Access To Medication Assisted Treatment for Opioid Use Disorders to Patients in the Hospital
 Expanding Access To Medication Assisted Treatment for Opioid Use Disorders to Patients in the Hospital August 28, 2018 Hosted by John A. Renner, Jr., MD, DLFAPA Professor of Psychiatry Boston University
Expanding Access To Medication Assisted Treatment for Opioid Use Disorders to Patients in the Hospital August 28, 2018 Hosted by John A. Renner, Jr., MD, DLFAPA Professor of Psychiatry Boston University
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations
 Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT
 and acute pain management on MAT") An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE
 LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
Buprenorphine Prescribing as a Patient- Centered Medical Home Enhancement
 Buprenorphine Prescribing as a Patient- Centered Medical Home Enhancement TANNER NISSLY DO, BOB LEVY MD FASAM, MICHELE MANDRICH MSW, CMPE AS YOU ENTER, PLEASE SET UP TO PARTICIPATE IN OUR POLL EVERYWHERE
Buprenorphine Prescribing as a Patient- Centered Medical Home Enhancement TANNER NISSLY DO, BOB LEVY MD FASAM, MICHELE MANDRICH MSW, CMPE AS YOU ENTER, PLEASE SET UP TO PARTICIPATE IN OUR POLL EVERYWHERE
Opioid Dependence and Buprenorphine Management
 Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
9/13/2017. Buprenorphine Treatment (Suboxone) Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare
 Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare") Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Disclosures. Target Audience 4/28/2015. The Road Less Traveled: Using Buprenorphine-Naloxone to Treat High-Risk Chronic Pain Patients
 The Road Less Traveled: Using Buprenorphine-Naloxone to Treat High-Risk Chronic Pain Patients Patrick Marshalek, MD Jenna Martino, MSN, FNP-C Audrey Royce, MSN, FNP-C Sarah Roy, MSN, RN, CCRN West Virginia
The Road Less Traveled: Using Buprenorphine-Naloxone to Treat High-Risk Chronic Pain Patients Patrick Marshalek, MD Jenna Martino, MSN, FNP-C Audrey Royce, MSN, FNP-C Sarah Roy, MSN, RN, CCRN West Virginia
Buprenorphine: An Introduction. Sharon Stancliff, MD Harm Reduction Coalition September 2008
 Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates
 and Medication Assisted Treatment (MAT) for Opiates") Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Medications for Opioid Use Disorder. Charles Brackett, MD, MPH General Internal Medicine, DHMC
 Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
ROSC & MAT II: Opioid Treatment Services
 ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
Understanding Medication in Addiction Treatment for Drug Court Participants
 Understanding Medication in Addiction Treatment for Drug Court Participants Introduction This pocket guide is for drug court participants who may be prescribed or considering medication as a part of addiction
Understanding Medication in Addiction Treatment for Drug Court Participants Introduction This pocket guide is for drug court participants who may be prescribed or considering medication as a part of addiction
Buprenorphine pharmacology
 Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Prepublication Requirements
 Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Pain Medication and Adolescents: Special Considerations
 Pain Medication and Adolescents: Special Considerations Patricia Cintra Franco Schram, MD Adolescent Substance Abuse Program Boston Children s Hospital Harvard Medical School 1 Educational Objectives At
Pain Medication and Adolescents: Special Considerations Patricia Cintra Franco Schram, MD Adolescent Substance Abuse Program Boston Children s Hospital Harvard Medical School 1 Educational Objectives At
Disclosures. I have no disclosures or commercial interests to report
 Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center Disclosures I have no disclosures or commercial interests to report Medication-Assisted
Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center Disclosures I have no disclosures or commercial interests to report Medication-Assisted
Opioid dependence and buprenorphine treatment
 Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
2/21/2018. What are Opioids?
 Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
SC MAT ACCESS. Medication Assisted Treatment Academic Community Capacity Expansion for Sustainable Success Kathleen Brady, MD, PhD, VPR, MUSC
 SC MAT ACCESS Medication Assisted Treatment Academic Community Capacity Expansion for Sustainable Success Kathleen Brady, MD, PhD, VPR, MUSC Overdose Death Rates from Opiates Most important sign of a
SC MAT ACCESS Medication Assisted Treatment Academic Community Capacity Expansion for Sustainable Success Kathleen Brady, MD, PhD, VPR, MUSC Overdose Death Rates from Opiates Most important sign of a
Buprenorphine for Family Medicine. Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17
 + Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
+ Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center
 Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center Disclosures I have no disclosures or commercial interests to report Addiction
Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center Disclosures I have no disclosures or commercial interests to report Addiction
Suboxone, Zubsolv, Bunavail (buprenorphine with naloxone sublingual tablets and film), Buprenorphine sublingual tablets
, Buprenorphine sublingual tablets") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.32 Subject: Suboxone Drug Class Page: 1 of 7 Last Review Date: June 24, 2016 Suboxone Drug Class Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.32 Subject: Suboxone Drug Class Page: 1 of 7 Last Review Date: June 24, 2016 Suboxone Drug Class Description
Talking with your doctor
 SUBOXONE (buprenorphine and naloxone) Sublingual Film (CIII) Talking with your doctor Opioid dependence can be treated. Talking with your healthcare team keeps them aware of your situation so they may
SUBOXONE (buprenorphine and naloxone) Sublingual Film (CIII) Talking with your doctor Opioid dependence can be treated. Talking with your healthcare team keeps them aware of your situation so they may
2016 American Academy of Neurology
 2016 American Academy of Neurology PCSS-O is a collaborative effort led by American Academy of Addiction Psychiatry (AAAP) in partnership with: Addiction Technology Transfer Center (ATTC), American Academy
2016 American Academy of Neurology PCSS-O is a collaborative effort led by American Academy of Addiction Psychiatry (AAAP) in partnership with: Addiction Technology Transfer Center (ATTC), American Academy
Medication Treatment and Opioid Use Disorder
 Medication Treatment and Opioid Use Disorder Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBOT-B Boston Medical Center Disclosures I have no disclosures
Medication Treatment and Opioid Use Disorder Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBOT-B Boston Medical Center Disclosures I have no disclosures
Opioids. October 29, Addiction Medicine Review Course CSAM, Newport Beach, CA
 Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services
 Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services www.randallwebber.com MAT clients are still addicted Truth: MAT clients will experience withdrawal symptoms if they stop
Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services www.randallwebber.com MAT clients are still addicted Truth: MAT clients will experience withdrawal symptoms if they stop
9/9/2016. Drug Name (select from list of drugs shown) Bunavail Buccal Film (buprenorphinenaloxone) Suboxone Sublingual Film (buprenorphine-naloxone)
 Bunavail Buccal Film (buprenorphinenaloxone) Suboxone Sublingual Film (buprenorphine-naloxone)") 9/9/2016 Prior Authorization Form PASSPORT HEALTH PLAN KENTUCKY MEDICAID Buprenorphine Products This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
9/9/2016 Prior Authorization Form PASSPORT HEALTH PLAN KENTUCKY MEDICAID Buprenorphine Products This fax machine is located in a secure location as required by HIPAA regulations. Complete/review information,
Treatment of Opioid Use Disorder
 Treatment of Opioid Use Disorder Casia Horseman, MD Assistant Professor Department of Psychiatry and Behavioral Health The Ohio State University Wexner Medical Center Objectives Discuss the historical
Treatment of Opioid Use Disorder Casia Horseman, MD Assistant Professor Department of Psychiatry and Behavioral Health The Ohio State University Wexner Medical Center Objectives Discuss the historical
Treatment of Opioid Use Disorder
 Treatment of Opioid Use Disorder Casia Horseman, MD Assistant Professor Department of Psychiatry and Behavioral Health The Ohio State University Wexner Medical Center Objectives Discuss the historical
Treatment of Opioid Use Disorder Casia Horseman, MD Assistant Professor Department of Psychiatry and Behavioral Health The Ohio State University Wexner Medical Center Objectives Discuss the historical
Module 6: Overview Opioid Dependence Treatment with Buprenorphine/Naloxone
 Module 6: Overview Opioid Dependence Treatment with Buprenorphine/Naloxone History of Medical Practice for Opioid Addiction in the U.S. Physicians had been liberal prescribers of morphine in late 1800s/early
Module 6: Overview Opioid Dependence Treatment with Buprenorphine/Naloxone History of Medical Practice for Opioid Addiction in the U.S. Physicians had been liberal prescribers of morphine in late 1800s/early
2015 American Academy of Neurology
 Prescribing Opioids for Pain in the Era of Changing Pain Management Guidelines Miroslav Misha Bačkonja, MD Department of Neurology University of Wisconsin, Madison Department of Neurology University of
Prescribing Opioids for Pain in the Era of Changing Pain Management Guidelines Miroslav Misha Bačkonja, MD Department of Neurology University of Wisconsin, Madison Department of Neurology University of
COMPASS RECOVERY OPIOID REHABILITATION PROGRAM QUESTIONAIRE FOR PROSPECTIVE OPIOID REHABILITATION. Name Birthdate / /
 COMPASS RECOVERY OPIOID REHABILITATION PROGRAM QUESTIONAIRE FOR PROSPECTIVE OPIOID REHABILITATION Name Birthdate / / Home phone ( ) - Cell phone ( ) - Please answer the following questions which will help
COMPASS RECOVERY OPIOID REHABILITATION PROGRAM QUESTIONAIRE FOR PROSPECTIVE OPIOID REHABILITATION Name Birthdate / / Home phone ( ) - Cell phone ( ) - Please answer the following questions which will help
6/6/2018. Objectives. Outline. Rethinking Medication Treatment for Opioid Use Disorder
 Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
Arwen Podesta, MD. ABIHM, ABAM, Forensic Psychiatry
 The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
Tennessee. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Tennessee Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Tennessee Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Now available. A maintenance dose of SUBOXONE mg once daily is clinically effective for most patients*1. Once-daily dosing in a single tablet
 Now available SUBOXONE Once-daily dosing1 12 mg and 16 mg tablets A maintenance dose of SUBOXONE 12-16 mg once daily is clinically effective for most patients*1 Effective maintenance dosing with SUBOXONE
Now available SUBOXONE Once-daily dosing1 12 mg and 16 mg tablets A maintenance dose of SUBOXONE 12-16 mg once daily is clinically effective for most patients*1 Effective maintenance dosing with SUBOXONE
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Opioids Research to Practice
 Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Prescription Opioid Addiction
 CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
Medication Assisted Treatment. Nicole Gastala, MD
 Medication Assisted Treatment Nicole Gastala, MD Objectives Training Goals: To enhance the understanding of the participants in use of medication assisted therapy To increase the knowledge of participants
Medication Assisted Treatment Nicole Gastala, MD Objectives Training Goals: To enhance the understanding of the participants in use of medication assisted therapy To increase the knowledge of participants
Medication Assisted Treatment
 Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
STARTING SUBOXONE IN PRIMARY CARE
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences STARTING SUBOXONE IN PRIMARY CARE MARK DUNCAN MD UNIVERSITY OF WASHINGTON OBJECTIVES 1. Review evidence of how to
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences STARTING SUBOXONE IN PRIMARY CARE MARK DUNCAN MD UNIVERSITY OF WASHINGTON OBJECTIVES 1. Review evidence of how to
Revised 9/30/2016. Primary Care Provider Pain Management Toolkit
 Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Opioids Research to Practice
 Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE
 Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING