Κώστας Τσιούφης Iπποκράτειο Γ.Ν.Α
|
|
|
- Byron Neal
- 6 years ago
- Views:
Transcription


1 Χρόνιες παθήσεις, παράλληλη φαρμακευτική αγωγή και συμμόρφωση στη θεραπεία σε ασθενείς με συννοσηρότητα Ο ρόλος της πολυφαρμακίας και των πολλαπλών θεραπειών. H συμμόρφωση στη θεραπεία του ασθενή με συννοσηρότητες. Κώστας Τσιούφης Iπποκράτειο Γ.Ν.Α
2 Percentage of global deaths for males in 2010 by cause and age Globally, CVD is the most common non-communicable cause of death CV disease Cancer War and disaster Intentional injuries Unintentional injuries Transport injuries Other non-communicable diseases Musculoskeletal disorders Diabetes, urogenital, blood, and endocrine Mental and behavioural disorders Neurological disorders Cirrhosis Chronic respiratory diseases Cardiovascular and circulatory diseases Cancer Other communicable diseases Nutritional deficiencies Neonatal disorders Maternal disorders Neglected tropical diseases and malaria Diarrhoea, lower respiratory infections, and other common infectious diseases HIV/AIDS and tuberculosis Lozano et al. Lancet 2012;380:

3 Hypertension is the main contributor to CVD and all cause mortality

4 In real life, BP control is often suboptimal; globally, BP is controlled in only 32,5% of treated hypertensive patients Chow et al. JAMA 2013;310:959-68




5 Adherence is a difficult issue For every 100 prescriptions written: 30% 50% never make it to the pharmacy 1 34% 52% are filled but never picked up 1 70% 75% are not taken as prescribed 1 Adherence is not a therapeutic parameter that can be described by a single number, as usually reported in the literature Adherence is a dynamic process. It is not the average adherence, but changes in adherence in individuals over time that contribute to visit to visit BP variability 80% 85% are not refilled as prescribed 1
6 Defining patient behaviour to prescribed treatment Medication Adherence: The patient s conformance with the provider s recommendation with respect to timing, dosage, and frequency of medication-taking during the prescribed length of time Compliance: Patient s passive following of provider s orders Persistence: Duration of time patient takes medication, from initiation to discontinuation of therapy Drug Drug holidays : three or more days without taking a drug CQGMedAdherence_FinalReport_ pdf

7 Medication Adherence in United States The World Health Organization estimated that by 2020, the number of Americans affected by at least one chronic condition requiring medication therapy will grow to 157 million Rates of medication adherence drop after first six months Only 51% of Americans treated for hypertension are adherent to their longterm therapy About 25% to 50% of patients discontinue statins within one year of treatment initiation Choudhry 2011, N Engl J Med; Yeaw 2009, J Manag Care Pharm; Script Your Future press release, November 2, 2011; accessed here:

8 When patients are asymptomatic... Non-compliance rates increase dramatically to an estimated 75% percent.


9 BURDEN OF NON-ADHERENCE
10 Non-Adherence Economic Direct cost estimated at $100 billion to $289 billion annually Costs $2000 per patient in physician visits annually Improved self-management of chronic diseases results in an approximate cost-to-savings ratio of 1:10 Cost-related non-adherence reported by 11.4% (~543,000 individuals) of stroke survivors, mostly among the uninsured and younger (45 to 64 years) Ho 2009, Circulation; Levine et al. 2013, Annals of Neurology
11 Non-Adherence Clinical Outcomes High adherence to antihypertensive medication is associated with higher odds of blood pressure control Each incremental 25% increase in proportion of days covered (PDC ) for statins is associated with ~3.8 mg/dl reduction in LDL cholesterol Ho 2009, Circulation

. Nelson MR, et al.")
12 Lower adherence to AHT: worse reported CV outcomes Study description: Cohort study of Australian patients to investigate whether responses to a previously validated 4-item medication adherence questionnaire were associated with CV events (N=4039). Nelson MR, et al. Med J Aust 2006;185:487 9.
13 Non-adherence Mortality, Hospitalizations, ED Visits Non-adherence causes ~30% to 50% of treatment failures and 125,000 deaths annually Non-adherence to statins increased relative risk for mortality (~12% to 25%) Non-adherence to cardioprotective medications increased risk of cardiovascular hospitalizations (10% to 40%) and mortality (50% to 80%) Poor adherence to heart failure medications increased the number of cardiovascular-related emergency department (ED) visits Ho 2009, Circulation; Edmondson 2013, Br J of Health Psychology; George & Shalansky 2006, Br J Clin Phar
14 The issue of non-adherence in CVD/HTN the most effective therapy prescribed by the most careful clinician will control hypertension only if the patient is motivated to take the prescribed medication and to establish and maintain a healthpromoting lifestyle. Meta-analysis of data on 376,162 patients from 20 studies Prescription refill frequency 7 drug classes: aspirin, ACEIs, ARBs, b-blockers, CCBs, thiazides, statins Adherence was 57% after 24 months (50% in primary and 66% in secondary prevention) Adherence decrease by 0.15% points/month Naderi SH et al. Am J Med 2012
15 Assessment of adherence in RHT by toxicological urine analysis 76 patients with uncontrolled HT despite optimal treatment with 4 drugs and after exclusion of secondary HT Urine sample analysis for anti-ht drugs with chromatography-mass spectrometry Analysis performed only when patients confirmed having taken their drugs during the last days prior to clinical visit 47.4% adherent vs 52.6% nonadherent Among the non-adherent, 70% had incomplete adherence: 17.5%: less than 25% of drugs 40%: 26-50% 7.5%: 51-75% 5%: >75% Comparable rates of adherence among drug classes. 87.5% of non-adherent patients eventually admitted not regular drug intake Jung O et al. J Hypertens 2013
16 White coat adherence: another form of the Hawthorne effect Patients tend to improve their adherence before and after clinical visits False clinical impression that acceptable adherence is sustained over time Many drugs have pharmacokinetics that can bring the drug concentration to therapeutic range after ingestion of 1-2 doses White-coat adherence in hypertensive patients receiving once-daily diuretic therapy. Progressive decline in drug adherence over weeks and sudden improvement in drug adherence during the 3 days preceding the medical visit.

17 Barriers to Adherence Five Interacting Dimensions of Non-Adherence Health-care system/team factors Social and economic factors Patient-related factors Condition-related factors Therapy-related factors
18 Health-care Factors Health-care System Health-care Team Access to care Continuity of care Patient education material not written in plain language Stress of health-care visits Discomfort in asking providers questions Patient s belief or understanding Patient s forgetfulness or carelessness Stressful life events Lack of immediate benefit of therapy

19 Provider Factors Communication skills Knowledge of health literacy issues Lack of empathy Lack of positive reinforcement Number of comorbid conditions Number of medications needed per day Types or components of medication Amount of prescribed medications or duration of prescription Source: Haynes RB, Ackloo E, Sahota N, McDonald HP, Yao X. Interventions for enhancing medication adherence. Cochrane Database Syst Rev 2008;(2):CD000011

20 Patient, Condition, and Therapy Factors Patient-related Condition- and therapy-related Physical Complexity of medication Psychological Frequent changes in regimen Treatment requiring mastery of certain techniques Unpleasant side effects Duration of therapy Lack of immediate benefit of therapy Medications with social stigma

21 Economic and Social Factors Economic Social Health insurance Medication cost Limited English proficiency Inability to access or difficulty accessing pharmacy Lack of family or social support Unstable living conditions
22 Greece, adherence and financial crisis Study purpose To record real-world compliance to treatment in a sample of hypertensive patients visiting a Hypertension Unit in Greece. Study design: retrospective analysis of prescribing records Study population: 202 patients with essential hypertension under treatment that are routinely followed (>1 year) in our Hypertension Unit Tsioufis et al, ESH Paris meeting 2016



23 MEDICATION PRESCRIPTION RATIO (MPR) The proportion of days in an observation period that an individual is in possession of medical supply Mean MPR: 78.7% MPR % Tsioufis et al, ESH Paris meeting 2016
24 Adherence-Associations No differences were recorded between men and women. A statistically significant negative effect of age (r=-0.201, p=0.03) was documented in the univariate regression analysis. Presence of comorbidities (obesity, diabetes, hyperlipidemia, CVD, LVH, CKD) did not significantly affect adherence. Patients receiving a fixed combination pill had a higher compliance rate compared to those under separately administered regimens (80.3% vs. 74.8%, p=0.034). Tsioufis et al, ESH Paris meeting 2016
25 Persistence rate after 18 months of follow-up in patients maintained on treatment (atorvastatin) or switched to a generic medication HR=0.574 p= C. Tsioufis et al, ESH, 2017.
 or switched to a generic medication P<0.001 C.")
26 Compliance rate estimated by proprortion days covered in patients maintained on treatment (atorvastatin) or switched to a generic medication P<0.001 C. Tsioufis et al, ESH 2017.
27 What May Providers Do to Overcome These Challenges? Communication is key! Effective interventions Measure medication adherence Ratanawongsa 2012 Arch Intern Med ; Bramley 2006 J Manag Care Pharm 12(3): ; Martin 2011 Am J Health Promot 25(6):

28 Adherence is Improved if a Patient: Takes part in negotiating the treatment plan Understands the disease and treatments Buys into or believes in the treatment plan

29 When patients believe in the Treatment Plan They adhere to the medication regime AND They seek out support for lifestyle changes, like DIET EXERCISE

30 LISTEN to and ADDRESS patients : Fears Lifestyle concerns Social and family issues TEACH patients about: Disease process Medication side effects Providers Need to

31 The role of the physician in adherence Healthcare Provider-Patient Relationship Must be based on mutual respect and trust... Developing open channels of communication Normalizing poor adherence to encourage honest communication for patients Providing high-quality, balanced medical information Implementing patient-specific treatment plans Simplifying treatment regimens E.g. fixed combinations


32 Physicians have many tools available to communicate and educate patients on their overall CV risk


33 Smartphones and wearable sensors could bring personalized healthcare to billions of people
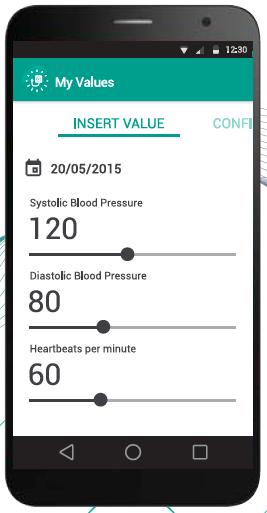


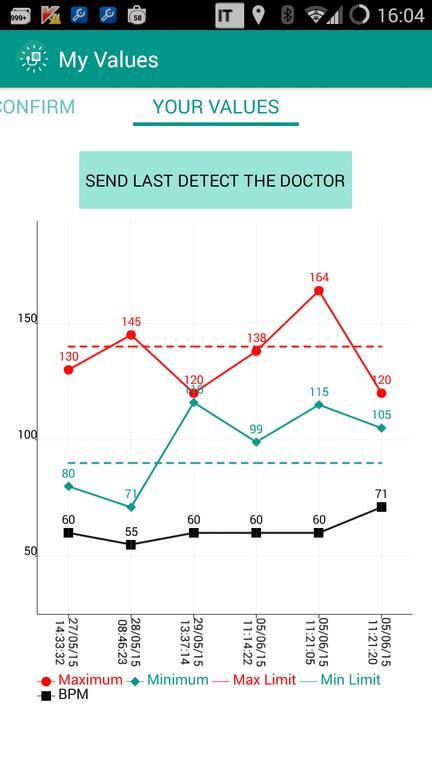

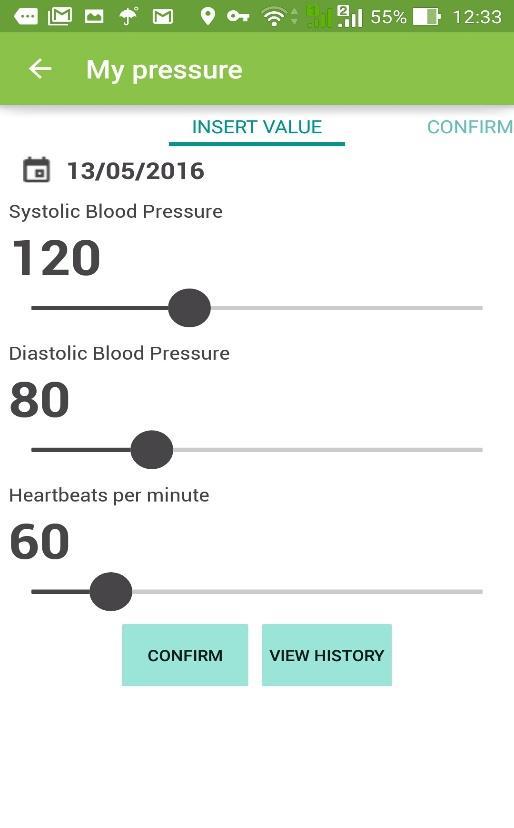
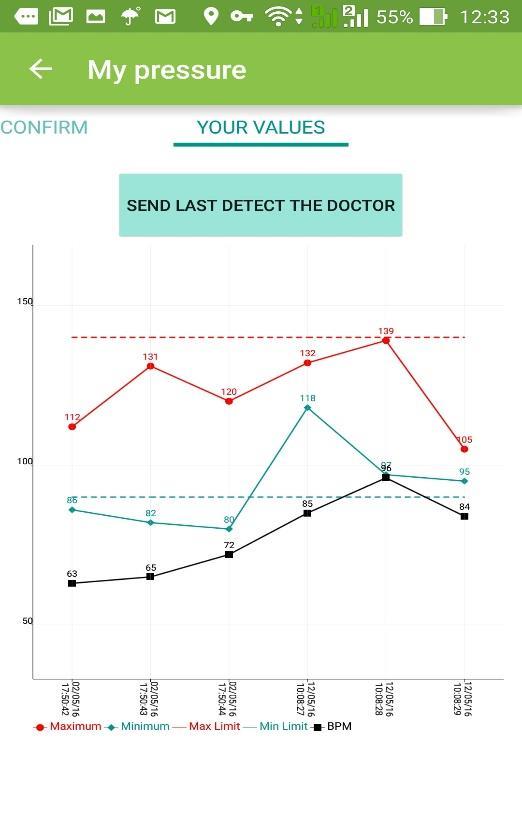

34 MY VALUES
35 The importance of a collaborative approach Each profession should value the unique role that others can play in enhancing patient adherence Specialist (simplifying optimal therapy) Physician Nurse ( building a personal connection to identify a patient s treatment concerns) Pharmacist (Establishing themselves as a primary educator for the patient)
36 How does Medication Non-Adherence compare to Drug Abuse? Non-Adherence Failing to take medications as prescribed Not seen as an ethical breach Poor health outcomes Financial costs to family and society Drug Abuse Taking medications NOT prescribed Seen as an ethical breach Poor health outcomes Financial costs to family and society

37
38 TAKE HOME MESSAGE Physicians and Health care providers must partner together to identify patient beliefs and misunderstandings about medications, and must educate patients appropriately Teamwork presents a more united front and gives patients multiple opportunities to hear critical messages e Health and m-health may contribute significantly in improvement of adherence
Improve the Adherence, Save the Life
 Improve the Adherence, Save the Life Park, Chang Gyu Korea University Guro Hospital Cardiovascular Center Seoul, Korea Modifiable CVD Risk Factors Obesity BMI Hypertension Cholesterol LDL HDL Diabetes
Improve the Adherence, Save the Life Park, Chang Gyu Korea University Guro Hospital Cardiovascular Center Seoul, Korea Modifiable CVD Risk Factors Obesity BMI Hypertension Cholesterol LDL HDL Diabetes
Hypertension and the Challenge of Adherence. Geneva Clark Briggs, Pharm.D., BCPS
 Hypertension and the Challenge of Adherence Geneva Clark Briggs, Pharm.D., BCPS Outline Brief overview of HTN and pharmacologic therapies Role of pharmacists in collaboration with patients and physicians
Hypertension and the Challenge of Adherence Geneva Clark Briggs, Pharm.D., BCPS Outline Brief overview of HTN and pharmacologic therapies Role of pharmacists in collaboration with patients and physicians
To Take or Not To Take?
 To Take or Not To Take? Assessment Question How do the terms adherence & compliance differ? 1. The terms are synonymous 2.Adherence assumes collaboration between patient & provider while compliance suggests
To Take or Not To Take? Assessment Question How do the terms adherence & compliance differ? 1. The terms are synonymous 2.Adherence assumes collaboration between patient & provider while compliance suggests
MEDICATION ADHERENCE: WE DIDN T ASK & THEY DIDN T TELL
 MEDICATION ADHERENCE: WE DIDN T ASK & THEY DIDN T TELL JENNIFER BUSSELL MD FACP INSTITUTE FOR HEALTHCARE IMPROVEMENT 15 TH ANNUAL INTERNATIONAL SUMMIT ON IMPROVING PATIENT CARE IN THE OFFICE PRACTICE AND
MEDICATION ADHERENCE: WE DIDN T ASK & THEY DIDN T TELL JENNIFER BUSSELL MD FACP INSTITUTE FOR HEALTHCARE IMPROVEMENT 15 TH ANNUAL INTERNATIONAL SUMMIT ON IMPROVING PATIENT CARE IN THE OFFICE PRACTICE AND
Getting Hypertension Under Control
 Getting Hypertension Under Control Learning Objectives EXPLAIN the factors involved in patient medication non-adherence. OUTLINE the results of studies focusing on medication adherence issues in patients
Getting Hypertension Under Control Learning Objectives EXPLAIN the factors involved in patient medication non-adherence. OUTLINE the results of studies focusing on medication adherence issues in patients
The Problem of CV Drug Adherence Worldwide
 The Problem of CV Drug Adherence Worldwide Jose M. Castellano Coordinador Investigaciones Clínicas, Centro Nacional de Investigaciones Cardiovascular (CNIC) Instituto de Salud Carlos III, Madrid, Spain
The Problem of CV Drug Adherence Worldwide Jose M. Castellano Coordinador Investigaciones Clínicas, Centro Nacional de Investigaciones Cardiovascular (CNIC) Instituto de Salud Carlos III, Madrid, Spain
Prevention of Heart Failure: What s New with Hypertension
 Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
Prevention of Heart Failure: What s New with Hypertension Ali AlMasood Prince Sultan Cardiac Center Riyadh 3ed Saudi Heart Failure conference, Jeddah, 13 December 2014 Background 20-30% of Saudi adults
The Polypill for Secondary Prevention Is Entering the Cardiovascular Field: Worldwide Interest Based on Better Adherence and Economics
 The Polypill for Secondary Prevention Is Entering the Cardiovascular Field: Worldwide Interest Based on Better Adherence and Economics Jose M. Castellano, MD, PhD Clinical Trials Coordinator, CNIC, Madrid,
The Polypill for Secondary Prevention Is Entering the Cardiovascular Field: Worldwide Interest Based on Better Adherence and Economics Jose M. Castellano, MD, PhD Clinical Trials Coordinator, CNIC, Madrid,
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
OR OTHER RELATIONSHIP(S) DISCLOSURE:
 DISCLOSURE:") Gregory Roth, MD DISCLOSURE DECLARATION Medication Adherence in Cardiovascular Disease: Drugs Don t Work in Patients Who Don t Take Them FINANCIAL OR OTHER RELATIONSHIP(S) DISCLOSURE: St. Charles Medical
Gregory Roth, MD DISCLOSURE DECLARATION Medication Adherence in Cardiovascular Disease: Drugs Don t Work in Patients Who Don t Take Them FINANCIAL OR OTHER RELATIONSHIP(S) DISCLOSURE: St. Charles Medical
Rina Ramirez, MD FACP Teresita Lawson, BSPharm, RPh, CDE
 Rina Ramirez, MD FACP Teresita Lawson, BSPharm, RPh, CDE List three components for CPS Describe how to integrate CPS into the primary care team Explain how CPS aligns with PCMH and Meaningful Use Established
Rina Ramirez, MD FACP Teresita Lawson, BSPharm, RPh, CDE List three components for CPS Describe how to integrate CPS into the primary care team Explain how CPS aligns with PCMH and Meaningful Use Established
Improvement of drug adherence using single pill combinations:
 Improvement of drug adherence using single pill combinations: what is the evidence? Prof. Michel Burnier Service of Nephrology and Hypertension, CHUV, Lausanne, Switzerland Potentialcauses of non-adherence
Improvement of drug adherence using single pill combinations: what is the evidence? Prof. Michel Burnier Service of Nephrology and Hypertension, CHUV, Lausanne, Switzerland Potentialcauses of non-adherence
Hypertension: Global Burden & Barriers
 Hypertension: Global Burden & Barriers A/Prof Clara Chow The George Institute, University of Sydney Dept. of Cardiology, Westmead Hospital Affiliated with the University of Sydney Dr Chow is supported
Hypertension: Global Burden & Barriers A/Prof Clara Chow The George Institute, University of Sydney Dept. of Cardiology, Westmead Hospital Affiliated with the University of Sydney Dr Chow is supported
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Disclosure. Learning Objectives 6/4/2014. Medication Adherence: Challenges and Opportunities
 Medication Adherence: Challenges and Opportunities Jessica W. Skelley, Pharm D., BCACP Assistant Professor of Pharmacy Practice McWhorter School of Pharmacy, Samford University jmwhalen@samford.edu Disclosure
Medication Adherence: Challenges and Opportunities Jessica W. Skelley, Pharm D., BCACP Assistant Professor of Pharmacy Practice McWhorter School of Pharmacy, Samford University jmwhalen@samford.edu Disclosure
Pediatric Adherence for the School Nurse
 Pediatric Adherence for the School Nurse Eve-Lynn Nelson, Ph.D. Assistant Director, Research KU Center for TeleMedicine (913) 588-2413; enelson2@kumc.edu Generously sponsored through a grant from the Health
Pediatric Adherence for the School Nurse Eve-Lynn Nelson, Ph.D. Assistant Director, Research KU Center for TeleMedicine (913) 588-2413; enelson2@kumc.edu Generously sponsored through a grant from the Health
Adherence to therapy. Kamlesh Khunti University of Leicester, UK. William Polonsky University of California San Diego, USA
 Adherence to therapy Kamlesh Khunti University of Leicester, UK William Polonsky University of California San Diego, USA 1 Dualities of interest Kamlesh Khunti: Honoraria for speaking, advising or research
Adherence to therapy Kamlesh Khunti University of Leicester, UK William Polonsky University of California San Diego, USA 1 Dualities of interest Kamlesh Khunti: Honoraria for speaking, advising or research
Improving Medication Adherence through Collaboration between Colleges of Pharmacy and Community Pharmacies
 Improving Medication Adherence through Collaboration between Colleges of Pharmacy and Community Pharmacies Megan Willson, PharmD, BCPS; Catrina Schwartz, PharmD, BS; Jennifer Robinson, PharmD Spokane,
Improving Medication Adherence through Collaboration between Colleges of Pharmacy and Community Pharmacies Megan Willson, PharmD, BCPS; Catrina Schwartz, PharmD, BS; Jennifer Robinson, PharmD Spokane,
Prescription Switching and Reduced LDL-C Goal Attainment
 Prescription Switching and Reduced LDL-C Goal Attainment JoAnne M. Foody, MD, FACC, FAHA Brigham and Women's Hospital, Boston, MA Disclosures Consultant for Merck and Pfizer Why Address Adherence? Increasing
Prescription Switching and Reduced LDL-C Goal Attainment JoAnne M. Foody, MD, FACC, FAHA Brigham and Women's Hospital, Boston, MA Disclosures Consultant for Merck and Pfizer Why Address Adherence? Increasing
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
Improving Adherence to Chronic Medications: The Physicians Role and How 340b Can Help
 Improving Adherence to Chronic Medications: The Physicians Role and How 340b Can Help William Shrank MD MSHS Division of Pharmacoepidemiology & Pharmacoeconomics Harvard Medical School wshrank@partners.org
Improving Adherence to Chronic Medications: The Physicians Role and How 340b Can Help William Shrank MD MSHS Division of Pharmacoepidemiology & Pharmacoeconomics Harvard Medical School wshrank@partners.org
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
High blood pressure (BP) significantly. After the Diagnosis: Adherence and Persistence With Hypertension Therapy REPORTS
 significantly. After the Diagnosis: Adherence and Persistence With Hypertension Therapy REPORTS") After the Diagnosis: Adherence and Persistence With Hypertension Therapy Abstract Poor adherence to therapy is a major reason that a large percentage of patients with hypertension fail to achieve good
After the Diagnosis: Adherence and Persistence With Hypertension Therapy Abstract Poor adherence to therapy is a major reason that a large percentage of patients with hypertension fail to achieve good
Patient persistence with antihypertensive drugs in France, Germany and the UK
 Patient persistence with antihypertensive drugs in France, Germany and the UK B. Ehlken (1), K. Kostev (1), A. Sandberg (2), B. Holz (1), A. M. S. Oberdiek (2) (1) IMS Health Frankfurt / Munich, Germany
Patient persistence with antihypertensive drugs in France, Germany and the UK B. Ehlken (1), K. Kostev (1), A. Sandberg (2), B. Holz (1), A. M. S. Oberdiek (2) (1) IMS Health Frankfurt / Munich, Germany
Potential synergy between lipid-lowering and blood-pressure-lowering, and Single pill benefit in patient s adherence
 Potential synergy between lipid-lowering and blood-pressure-lowering, and Single pill benefit in patient s adherence Park, Chang Gyu Korea University Guro Hospital ASCOT-BPLA and LLA Primary Objectives
Potential synergy between lipid-lowering and blood-pressure-lowering, and Single pill benefit in patient s adherence Park, Chang Gyu Korea University Guro Hospital ASCOT-BPLA and LLA Primary Objectives
Treatment Gaps and Barriers to control of Hypertension
 Treatment Gaps and Barriers to control of Hypertension Dr Clara Chow The George Institute, University of Sydney PHRI, McMaster University Affiliated with the University of Sydney Dr Chow is supported by
Treatment Gaps and Barriers to control of Hypertension Dr Clara Chow The George Institute, University of Sydney PHRI, McMaster University Affiliated with the University of Sydney Dr Chow is supported by
Adherence & Medicaton review
 Adherence & Medicaton review Assoc. Prof. Mitja Kos, Ph.D., M.Pharm. Head, Chair of Social Pharmacy University of Ljubljana, Faculty of Pharmacy, Web: www.ffa.uni-lj.si E-mail: mitja.kos@ffa.uni-lj.si
Adherence & Medicaton review Assoc. Prof. Mitja Kos, Ph.D., M.Pharm. Head, Chair of Social Pharmacy University of Ljubljana, Faculty of Pharmacy, Web: www.ffa.uni-lj.si E-mail: mitja.kos@ffa.uni-lj.si
Long-Term Management Of the ACS Patient: State-of-the-Art. Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA
 Long-Term Management Of the ACS Patient: State-of-the-Art Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA Disclosures I have no disclosures. Case Study 45 y/o male admitted to
Long-Term Management Of the ACS Patient: State-of-the-Art Kim Newlin, CNS, NP-C, FPCNA Sutter Roseville Medical Center Roseville, CA Disclosures I have no disclosures. Case Study 45 y/o male admitted to
Cheshire & Merseyside Cardiovascular Programme
 Cheshire & Merseyside Cardiovascular Programme CVD Prevention and lipids: Are we doing enough? POP-UP UNIVERSITY SESSION Date: Thursday 6 September - Time: 10:45-11:45 Dr Scott W Murray Consultant Cardiologist
Cheshire & Merseyside Cardiovascular Programme CVD Prevention and lipids: Are we doing enough? POP-UP UNIVERSITY SESSION Date: Thursday 6 September - Time: 10:45-11:45 Dr Scott W Murray Consultant Cardiologist
Cost-Effective Process to Improve Drug Adherence for Medicare 5-Star
 Cost-Effective Process to Improve Drug Adherence for Medicare 5-Star HEALTH ALLIANCE PLAN Presented by Vanita K. Pindolia, Pharm.D. VP, Ambulatory Clinical Pharmacy Programs_PCM Medicare 5-Star Rating
Cost-Effective Process to Improve Drug Adherence for Medicare 5-Star HEALTH ALLIANCE PLAN Presented by Vanita K. Pindolia, Pharm.D. VP, Ambulatory Clinical Pharmacy Programs_PCM Medicare 5-Star Rating
Economics of Reducing Out-of-Pocket Costs for Cardiovascular Preventive Services for Patients with High Blood Pressure and High Cholesterol
 s of Reducing Out-of-Pocket Costs for Cardiovascular Preventive Services for Patients with High Blood Pressure and High Cholesterol Summary Evidence Tables Study Author (Year) Bunting (2008) Prepost Incomplete
s of Reducing Out-of-Pocket Costs for Cardiovascular Preventive Services for Patients with High Blood Pressure and High Cholesterol Summary Evidence Tables Study Author (Year) Bunting (2008) Prepost Incomplete
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines. John Potter Professor Ageing & Stroke Medicine University of East Anglia
 Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
The Evolution To Treatment Of Hypertension With Advanced Formulation
 The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
The Evolution To Treatment Of Hypertension With Advanced Formulation Dr. Donald Ang MBChB (UK) FRCP (Edin) MD (UK) CCST Cardiology (UK) FESC (Europe) Consultant Cardiologist Island Hospital Penang High
REDUCING COSTS AND IMPROVING HYPERTENSION MANAGEMENT
 REDUCING COSTS AND IMPROVING HYPERTENSION MANAGEMENT Vida Stankus 1, Brenda Hemmelgarn 2, Norm RC Campbell 2, Guanmin Chen 2, Finlay A McAlister 1, Ross T Tsuyuki 1 1 EPICORE Centre, Department of Medicine,
REDUCING COSTS AND IMPROVING HYPERTENSION MANAGEMENT Vida Stankus 1, Brenda Hemmelgarn 2, Norm RC Campbell 2, Guanmin Chen 2, Finlay A McAlister 1, Ross T Tsuyuki 1 1 EPICORE Centre, Department of Medicine,
Understanding and Addressing Problematic Medication Adherence
 Understanding and Addressing Problematic Medication Adherence William H. Polonsky PhD, CDE November 10, 2017 whp@behavioraldiabetes.org RATES OF VERY POOR GLYCEMIC CONTROL HEDIS data from >1000 health
Understanding and Addressing Problematic Medication Adherence William H. Polonsky PhD, CDE November 10, 2017 whp@behavioraldiabetes.org RATES OF VERY POOR GLYCEMIC CONTROL HEDIS data from >1000 health
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension
 Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
Outcomes and Perspectives of Single-Pill Combination Therapy for the modern management of hypertension Prof. Massimo Volpe, MD, FAHA, FESC, Chair of Cardiology, Department of Clinical and Molecular Medicine
ASSOCIATION MEDICAMENTEUSE ET OBSERVANCE THERAPEUTIQUE: QUOI DE NEUF? Philippe van de Borne Service de cardiologie,hopital Erasme, Bruxelles,Belgique
 ASSOCIATION MEDICAMENTEUSE ET OBSERVANCE THERAPEUTIQUE: QUOI DE NEUF? Philippe van de Borne Service de cardiologie,hopital Erasme, Bruxelles,Belgique Adherence, compliance, persistence: definitions Adherence
ASSOCIATION MEDICAMENTEUSE ET OBSERVANCE THERAPEUTIQUE: QUOI DE NEUF? Philippe van de Borne Service de cardiologie,hopital Erasme, Bruxelles,Belgique Adherence, compliance, persistence: definitions Adherence
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Prescription Pattern of Anti-Hypertensive Drugs in Adherence to JNC- 7 Guidelines
 American Journal of Pharmacology and Toxicology Original Research Paper Prescription Pattern of Anti-Hypertensive Drugs in Adherence to JNC- 7 Guidelines 1 Krishna Murti, 1 M. Arif Khan, 1 Akalanka Dey,
American Journal of Pharmacology and Toxicology Original Research Paper Prescription Pattern of Anti-Hypertensive Drugs in Adherence to JNC- 7 Guidelines 1 Krishna Murti, 1 M. Arif Khan, 1 Akalanka Dey,
Hypertension. Uncontrolled and Apparent Treatment Resistant Hypertension in the United States, 1988 to 2008
 Hypertension Uncontrolled and Apparent Treatment Resistant Hypertension in the United States, 1988 to 2008 Brent M. Egan, MD; Yumin Zhao, PhD; R. Neal Axon, MD; Walter A. Brzezinski, MD; Keith C. Ferdinand,
Hypertension Uncontrolled and Apparent Treatment Resistant Hypertension in the United States, 1988 to 2008 Brent M. Egan, MD; Yumin Zhao, PhD; R. Neal Axon, MD; Walter A. Brzezinski, MD; Keith C. Ferdinand,
Motivating patients to manage their chronic illness
 Motivating patients to manage their chronic illness Bruce G. Bender, Ph.D. Proportional Contribution to Premature Death Genetic predisposition Social circumstances Environmental exposure Health care Behaviors
Motivating patients to manage their chronic illness Bruce G. Bender, Ph.D. Proportional Contribution to Premature Death Genetic predisposition Social circumstances Environmental exposure Health care Behaviors
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Brent M. Egan, MD Professor of Medicine USCSOM Greenville
 Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
Contemporary Management of Uncontrolled and Treatment Resistant Hypertension Brent M. Egan, MD Professor of Medicine USCSOM Greenville Disclosures (past 3 years): Honoraria: BCBSSC, Medtronic Grant Support:
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
INTERNATIONAL RESEARCH JOURNAL OF PHARMACY ISSN Research Article
 INTERNATIONAL RESEARCH JOURNAL OF PHARMACY www.irjponline.com ISSN 2230 8407 Research Article ASSESSMENT OF MEDICATION ADHERENCE AND FACTORS AFFECTING TO MEDIACTION ADHERENCE IN ASTHMA PATIENTS BY CLINICAL
INTERNATIONAL RESEARCH JOURNAL OF PHARMACY www.irjponline.com ISSN 2230 8407 Research Article ASSESSMENT OF MEDICATION ADHERENCE AND FACTORS AFFECTING TO MEDIACTION ADHERENCE IN ASTHMA PATIENTS BY CLINICAL
Transforming Diabetes Care
 Transforming Diabetes Care Barriers to Mealtime Insulin Dosing Mark Peyrot, PhD Loyola University Maryland, Baltimore, MD Faculty Background Principle Investigator DAWN and DAWN2 studies (Novo Nordisk)
Transforming Diabetes Care Barriers to Mealtime Insulin Dosing Mark Peyrot, PhD Loyola University Maryland, Baltimore, MD Faculty Background Principle Investigator DAWN and DAWN2 studies (Novo Nordisk)
MEDICINES ADHERENCE The Role of the Pharmacist
 BROUGHT TO YOU BY MEDICINES ADHERENCE The Role of the Pharmacist Developed by Pfizer 15 May, 2017 This learning module is intended for UK healthcare professionals only. Job code; PP-GEP-GBR-0682. Date
BROUGHT TO YOU BY MEDICINES ADHERENCE The Role of the Pharmacist Developed by Pfizer 15 May, 2017 This learning module is intended for UK healthcare professionals only. Job code; PP-GEP-GBR-0682. Date
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
Management of High Blood Pressure in Adults
 Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Management of High Blood Pressure in Adults Based on the Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC8) James, P. A. (2014, February 05). 2014 Guideline for Management
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
To Do or Not To Do? The Annual Physical- Beyond The PAP And Breast Exam
 1/27/2015 To Do or Not To Do? The Annual Physical- Beyond The PAP And Breast Exam Fleur Sack, M.D., FAAFP Society of General Internal Medicine Cochrane review of 182,000 people followed for 9 years : the
1/27/2015 To Do or Not To Do? The Annual Physical- Beyond The PAP And Breast Exam Fleur Sack, M.D., FAAFP Society of General Internal Medicine Cochrane review of 182,000 people followed for 9 years : the
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8. Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital
 Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
Clinical Updates in the Treatment of Hypertension JNC 7 vs. JNC 8 Lauren Thomas, PharmD PGY1 Pharmacy Practice Resident South Pointe Hospital Objectives Review the Eighth Joint National Committee (JNC
CKD & HT. Anne-Marie Angus
 CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
CKD & HT Anne-Marie Angus Hypertension definitions Persisting BP >140/90 and HBPM >135/85 Stage 1 >140/90 (HBPM >135/85) Stage 2 >160/100 (HBPM >150/90) Severe >180/100 White coat HT Why treat? A major
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
New Antihypertensive Strategies to Improve Blood Pressure Control
 New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
New Antihypertensive Strategies to Improve Blood Pressure Control Antonio Coca, MD, PhD,, FRCP, FESC Hypertension and Vascular Risk Unit Department of Internal Medicine. Hospital Clínic (IDIBAPS) University
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Difficult-to-Control & Resistant Hypertension. Anthony Viera, MD, MPH, FAHA Professor and Chair
 Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Difficult-to-Control & Resistant Hypertension Anthony Viera, MD, MPH, FAHA Professor and Chair Objectives Define resistant hypertension Discuss evaluation strategy for patient with HTN that appears difficult
Module 3.2. Management of hypertension at primary health care
 Module 3.2 Management of hypertension at primary health care What s inside Introduction Learning outcomes Topics covered Competency Teaching and learning activities Background information Introduction
Module 3.2 Management of hypertension at primary health care What s inside Introduction Learning outcomes Topics covered Competency Teaching and learning activities Background information Introduction
Hypertension. Risk of cardiovascular disease beginning at 115/75 mmhg doubles with every 20/10mm Hg increase. (Grade B)
") Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
Practice Guidelines and Principles: Guidelines and principles are intended to be flexible. They serve as reference points or recommendations, not rigid criteria. Guidelines and principles should be followed
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
ASSESS AND ADDRESS RISK OF CARDIOVASCULAR DISEASE
 ASSESS AND ADDRESS RISK OF CARDIOVASCULAR DISEASE Heart diseases and stroke are the top causes of death and disability among people with Type 2 diabetes. In fact, at least 65 percent of people with diabetes
ASSESS AND ADDRESS RISK OF CARDIOVASCULAR DISEASE Heart diseases and stroke are the top causes of death and disability among people with Type 2 diabetes. In fact, at least 65 percent of people with diabetes
The Self-Medication Assessment Tool (SMAT) Training Program
 Training Program") The Self-Medication Assessment Tool (SMAT) Training Program What is the Self-Medication Assessment Tool? The Self-Medication Assessment Tool (SMAT) is a comprehensive instrument intended to screen for
The Self-Medication Assessment Tool (SMAT) Training Program What is the Self-Medication Assessment Tool? The Self-Medication Assessment Tool (SMAT) is a comprehensive instrument intended to screen for
Health System Financing Implications of Chronic Health Conditions: Insights from Sri Lanka
 Health System Financing Implications of Chronic Health Conditions: Insights from Sri Lanka Prioritizing chronicity: An Agenda for Public Health Research on Chronic Disease for sub-saharan Africa and Asia
Health System Financing Implications of Chronic Health Conditions: Insights from Sri Lanka Prioritizing chronicity: An Agenda for Public Health Research on Chronic Disease for sub-saharan Africa and Asia
Adherence in multiple sclerosis: Neurologist s view
 Adherence in multiple sclerosis: Neurologist s view Jaume Sastre-Garriga Unitat de Neuroimmunologia Clínica Centre d Esclerosi Múltiple de Catalunya CEMCat Hospital Universitari Vall d Hebron, Barcelona
Adherence in multiple sclerosis: Neurologist s view Jaume Sastre-Garriga Unitat de Neuroimmunologia Clínica Centre d Esclerosi Múltiple de Catalunya CEMCat Hospital Universitari Vall d Hebron, Barcelona
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventive Cardiology Scientific evidence
 Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
Preventive Cardiology Scientific evidence Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College London Primary prevention
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour
 ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
ABCD and Renal Association Clinical Guidelines for Diabetic Nephropathy-CKD. Management of Dyslipidaemia and Hypertension in Adults Dr Peter Winocour Dr Indranil Dasgupta Rationale No national practical
Pre-ALLHAT Drug Use. Diuretics. ß-Blockers. ACE Inhibitors. CCBs. Year. % of Treated Patients on Medication. CCBs. Beta Blockers.
 Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
Pre- Drug Use % of Treated Patients on Medication 60 50 40 30 20 10 0 1978 Diuretics ß-Blockers ACE Inhibitors Year CCBs CCBs Beta Blockers Diuretics ACE Inhibitors 1980 1982 1984 1986 1988 1990 1992 IMS
LLL Session - Nutrition support in diabetes and dyslipidemia. Dyslipidemia: targeting the management of cardiovascular risk factors. M.
 ESPEN Congress Leipzig 2013 LLL Session - Nutrition support in diabetes and dyslipidemia Dyslipidemia: targeting the management of cardiovascular risk factors M. Leon Sanz (ES) Dyslipidemia: Targeting
ESPEN Congress Leipzig 2013 LLL Session - Nutrition support in diabetes and dyslipidemia Dyslipidemia: targeting the management of cardiovascular risk factors M. Leon Sanz (ES) Dyslipidemia: Targeting
Liability, Informed Consent, and Risk Management 15 Thoughts for Pain Management Physicians
 Liability, Informed Consent, and Risk Management 15 Thoughts for Pain Management Physicians Click to edit Master title style Presented by: Scott Becker, JD, CPA, Partner, Publisher Becker Healthcare 14th
Liability, Informed Consent, and Risk Management 15 Thoughts for Pain Management Physicians Click to edit Master title style Presented by: Scott Becker, JD, CPA, Partner, Publisher Becker Healthcare 14th
Hypertension is among the most prevalent chronic
 Switching Between Different ARBs in Patients With Controlled BP At a Glance Practical Implications e82 Author Information e86 Web Exclusive Original Research Khalid M. Kamal, PhD; Christopher Zacker, RPh,
Switching Between Different ARBs in Patients With Controlled BP At a Glance Practical Implications e82 Author Information e86 Web Exclusive Original Research Khalid M. Kamal, PhD; Christopher Zacker, RPh,
Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study
 Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study Antonio Coca MD, PhD, FRCP, FESC Council on Hypertension. European Society of Cardiology Hypertension and Vascular Risk Unit. Department of
Best Therapy for Resistant Hypertension: The PATHWAY-2 2 Study Antonio Coca MD, PhD, FRCP, FESC Council on Hypertension. European Society of Cardiology Hypertension and Vascular Risk Unit. Department of
Long-Term Care Updates
 Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
Long-Term Care Updates August 2015 By Darren Hein, PharmD Hypertension is a clinical condition in which the force of blood pushing on the arteries is higher than normal. This increases the risk for heart
GSK Medicine: Study Number: Title: Rationale: Study Period: Objectives: Indication: Study Investigators/Centers: Research Methods: Data Source
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Assessing Medication Adherence
 Assessing Medication Adherence Dr. Lauren Hanna and Dr. Delbert Robinson Northwell Health National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental
Assessing Medication Adherence Dr. Lauren Hanna and Dr. Delbert Robinson Northwell Health National Council for Behavioral Health Montefiore Medical Center Northwell Health New York State Office of Mental
Impact of statin adherence on cardiovascular disease and mortality outcomes: a systematic review
 British Journal of Clinical Pharmacology DOI:10.1111/bcp.12339 Impact of statin adherence on cardiovascular disease and mortality outcomes: a systematic review Mary A. De Vera, 1,2 Vidula Bhole, 2 Lindsay
British Journal of Clinical Pharmacology DOI:10.1111/bcp.12339 Impact of statin adherence on cardiovascular disease and mortality outcomes: a systematic review Mary A. De Vera, 1,2 Vidula Bhole, 2 Lindsay
Adherence and persistence with prescribed chronic medications
 RESEARCH Impact of Appointment-Based Medication Synchronization on Existing Users of Chronic Medications David Holdford, RPh, MS, PhD, FAPhA, and Kunal Saxena, BS, MS ABSTRACT BACKGROUND: Appointment-based
RESEARCH Impact of Appointment-Based Medication Synchronization on Existing Users of Chronic Medications David Holdford, RPh, MS, PhD, FAPhA, and Kunal Saxena, BS, MS ABSTRACT BACKGROUND: Appointment-based
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Getting Serious About CVD Prevention What does this mean for Primary Care?
 Getting Serious About CVD Prevention What does this mean for Primary Care? Dr Matt Kearney GP and National Clinical Director for Cardiovascular Disease Prevention NHS England and Public Health England
Getting Serious About CVD Prevention What does this mean for Primary Care? Dr Matt Kearney GP and National Clinical Director for Cardiovascular Disease Prevention NHS England and Public Health England
5.2 Key priorities for implementation
 5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
5.2 Key priorities for implementation From the full set of recommendations, the GDG selected ten key priorities for implementation. The criteria used for selecting these recommendations are listed in detail
Φαρµακευτική θεραπεία υπερτασικών ασθενών. Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική
 Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Φαρµακευτική θεραπεία υπερτασικών ασθενών Δ. Τσιαχρής, Καρδιολόγος, Α Πανεπιστηµαική Καρδιολογική Κλινική A 42-Year-Old Female with True Severe Resistant Hypertension Female, 42 years old, smoker BMI:
Understanding Temporal Patterns in Hypertensive Drug Therapy
 Understanding Temporal Patterns in Hypertensive Drug Therapy 1 Margret Bjarnadottir, 2 Sana Malik, 2 Catherine Plaisant, 3 Eberechukwu Onukwugha 1 Smith School of Business, University of Maryland, College
Understanding Temporal Patterns in Hypertensive Drug Therapy 1 Margret Bjarnadottir, 2 Sana Malik, 2 Catherine Plaisant, 3 Eberechukwu Onukwugha 1 Smith School of Business, University of Maryland, College
Is there a mechanism of interaction between hypertension and dyslipidaemia?
 Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Is there a mechanism of interaction between hypertension and dyslipidaemia? Neil R Poulter International Centre for Circulatory Health NHLI, Imperial College London Daegu, Korea April 2005 Observational
Treatment of hypertension to achieve blood pressure control
 Treatment of hypertension to achieve blood pressure control Item Type Report Authors Peter Mas-Mollinedo Publisher Irish Heart Foundation (IHF) Download date 01/11/2018 18:07:44 Link to Item http://hdl.handle.net/10147/310910
Treatment of hypertension to achieve blood pressure control Item Type Report Authors Peter Mas-Mollinedo Publisher Irish Heart Foundation (IHF) Download date 01/11/2018 18:07:44 Link to Item http://hdl.handle.net/10147/310910
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension)
") Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
Lessons learned from AASK (African-American Study of Kidney Disease and Hypertension) Janice P. Lea, MD, MSc, FASN Professor of Medicine Chief Medical Director of Emory Dialysis ASH Clinical Specialist
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Statins ARE Enough For The Prevention of CVD! Professor Kausik Ray Imperial College London, UK
 1 Disclosures Advisory boards PCSK9- Sanofi/ Regeneron, Amgen, Pfizer, Roche, MSD NLI/ SC member for Odyssey- (Sanofi/ Regeneron), Roche Investigator initiated research grant support (Sanofi/Regeneron/
1 Disclosures Advisory boards PCSK9- Sanofi/ Regeneron, Amgen, Pfizer, Roche, MSD NLI/ SC member for Odyssey- (Sanofi/ Regeneron), Roche Investigator initiated research grant support (Sanofi/Regeneron/
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Modernized Reference Drug Program
 Modernized Reference Drug Program Monitoring Report For the period ending May 31, 2017 Issued: November 2017 Published by: Pharmaceutical Services Division and Health Sector Information, Analysis and Reporting
Modernized Reference Drug Program Monitoring Report For the period ending May 31, 2017 Issued: November 2017 Published by: Pharmaceutical Services Division and Health Sector Information, Analysis and Reporting
Layered Approaches to Studying Drug Responses
 Layered Approaches to Studying Drug Responses Brian B Hoffman, MD Chief of Medicine VA Boston Health Care System Professor of Medicine Harvard Medical School Conflict of Interest: US Federal Grant Funding
Layered Approaches to Studying Drug Responses Brian B Hoffman, MD Chief of Medicine VA Boston Health Care System Professor of Medicine Harvard Medical School Conflict of Interest: US Federal Grant Funding
Primary hypertension in adults
 Primary hypertension in adults NICE provided the content for this booklet which is independent of any company or product advertised Hypertension Welcome NICE published an updated guideline on the diagnosis
Primary hypertension in adults NICE provided the content for this booklet which is independent of any company or product advertised Hypertension Welcome NICE published an updated guideline on the diagnosis
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity