Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
|
|
|
- Osborne Wood
- 6 years ago
- Views:
Transcription
1 Steroids in ARDS: if, when, how much? John Fowler, MD, FACEP Dept. of Emergency Medicine Kent Hospital, İzmir, Türkiye
2 Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem (hydrocortisone mg/day for 7 d) Septic shock (sepsis + fluids + vasopressors) Eosinophilic pneumonia Pneumocystis pneumonia Adrenocortical insufficiency Steroids are not indicated for routine prophylaxis or treatment of ARDS
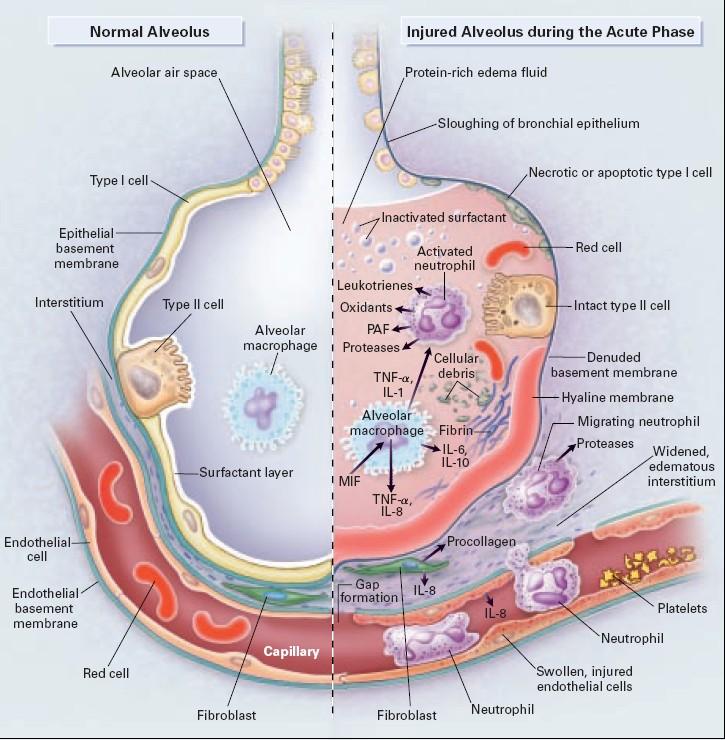
3 Why might steroids make sense? Pathophysiology of ARDS = neutrophil activation and endothelial injury after pulmonary insult: after extrapulmonary insult: Pneumonia, gastric aspiration, fat emboli, inhalation injury, fat emboli, lung contusion Sepsis, multiple trauma, CABG, pancreatitis, burns, drug overdose, blood transfusion Increased risk of ARDS with predisposing medical disorders, alcohol abuse, COPD, acidemia
4 Why might steroids make sense? Pathophysiology of ARDS = neutrophil activation and endothelial injury after pulmonary and extrapulmonary insults = many, many inflammatory molecules Interleukin-6, -8, -10, -1ß Tumor necrosis factor (TNF-α) Interferon-γ

5 Extracellular effects of corticosteroids b

6 Intracellular effects of corticosteroids b
7 Time course of ARDS
8

9 Proliferative and fibrosis phases of ARDS
10 Definition of ARDS (Berlin, 2012) Within one week of insult Bilateral opacities not explained by effusions, lobar collapse, or nodules Respiratory failure not explained by cardiac failure or fluid overload (assess objectively to exclude hydrostatic edema; for example, with echocardiography) Oxygenation: Mild: with PEEP or CPAP 5 cm H2O, 200< PaO2/FiO2 300 Moderate: with PEEP 5 cm H2O, 100< PaO2/FiO2 200 Severe: with PEEP 5 cm H2O, PaO2/FiO2 100
11 Steroids given for prevention of ARDS All studies done in the 1980 s Steroids: More patients developed ARDS More patients died
12 Randomized controlled trials using steroids in ARDS High-dose steroids given early for ARDS: No benefit Increased rate of infectious complications 1985 Arch Surg. Early steroid therapy for respiratory failure NEJM. High-dose corticosteroids in patients with the adult respiratory distress syndrome.
13 Randomized controlled trials using steroids in ARDS High-dose steroids given early for ARDS: No benefit Increased rate of infectious complications 1985 Arch Surg. Early steroid therapy for respiratory failure NEJM. High-dose corticosteroids in patients with the adult respiratory distress syndrome.
14 Steroids given for the treatment of established ARDS Some studies had very few patients results were very variable
15 Randomized controlled trials using steroids in ARDS Steroids given late in ARDS: Survival benefit (24 patients) No survival benefit (180 patients) 1998 JAMA. Effect of prolonged methylprednisolone therapy in unresolving acute respiratory distress syndrome NEJM. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome.
16 Randomized controlled trials using steroids in ARDS 2006 NEJM. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome N=180, all with ARDS for at least 7 days No difference in mortality at 60 days or at 180 days Steroid group had better oxygenation, more ventilatorfree days Steroid group had more neuromyopathy, more hyperglycemia If given after 14 days, steroids increased mortality
17 Randomized controlled trials using steroids in ARDS 2006 NEJM. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome N=180, all with ARDS for at least 7 days No difference in mortality at 60 days or at 180 days Steroid group had better oxygenation, more ventilatorfree days Steroid group had more neuromyopathy, more hyperglycemia If given after 14 days, steroids increased mortality
18 Randomized controlled trials using steroids in ARDS 2006 NEJM. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome N=180, all with ARDS for at least 7 days No difference in mortality at 60 days or at 180 days Steroid group had better oxygenation, more ventilatorfree days Steroid group had more neuromyopathy, more hyperglycemia If given after 14 days, steroids increased mortality
19 Randomized controlled trials using steroids in ARDS 2006 NEJM. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome N=180, all with ARDS for at least 7 days No difference in mortality at 60 days or at 180 days Steroid group had better oxygenation, more ventilatorfree days Steroid group had more neuromyopathy, more hyperglycemia If given after 14 days, steroids increased mortality
20 Randomized controlled trials using steroids in ARDS 2007 Methylprednisolone infusion in early severe ARDS N=91, sepsis in 66%, steroids started within 72 hrs Survival was not a primary outcome (!) Primary outcomes were decrease in lung injury score and C-reactive protein levels
21 Randomized controlled trials using steroids in ARDS 2007 Methylprednisolone infusion in early severe ARDS
22 Randomized controlled trials using steroids in ARDS 2007 Methylprednisolone infusion in early severe ARDS At 28 days, the difference in survival was not significantly different. p=0.20
23 Randomized controlled trials using steroids in ARDS 2011 Early Corticosteroids in Severe Influenza A/H1N1 Pneumonia and ARDS Retrospective study of 208 pts with ARDS and influenza A/H1N1 No steroids n=125 Steroids n=83 Steroid group More deaths (34% vs 17%) More ICU-acquired infections (45% vs 35%) More ICU-acquired pneumonia (41% vs 26%)
24 Randomized controlled trials using steroids in ARDS 2011, retrospective, multicenter, 245 patients 90-day mortality 58% steroids 27% no steroids Steroid group more superinfections longer ICU stay
25 ARDS caused by inhalational injury Only 13 studies (mostly animal) found for a metaanalysis No benefit in the acute phase Harm if given in the late phase No data exists for corticosteroid treatment of patients with inhalational exposures
26 ARDS caused by aspiration of gastric contents One randomized trial no difference in outcomes Case-control study No difference in mortality Ventilator days fewer in steroid group More gram-negative pneumonia in steroid group = steroids are not recommended in these patients
27 Steroids in ARDS: conclusion Give low-dose steroids if indicated for another problem (hydrocortisone mg/day for 7 d) Septic shock (sepsis + fluids + vasopressors) Eosinophilic pneumonia Pneumocystis pneumonia Adrenocortical insufficiency Steroids are not indicated for routine prophylaxis or treatment of ARDS

28 2013: an interesting question:
29 If you decide to give steroids Do not give etomidate Do not give neuromuscular blockers Taper the steroids s-l-o-w-l-y
30 If not steroids, what can we do for ARDS pts? FiO2 <0.6 Tidal volume 6 ml/kg (predicted body weight) Plateau pressures <30 cm H2O Recruitment maneuvers / PEEP (individualized) Fluid restriction, restricted transfusion protocols [Prone positioning, inhaled nitric oxide, neuromuscular blockers] [High-freq. oscillatory ventilation, ECMO]
 Plateau pressures <30 cm H2O Recruitment maneuvers / PEEP (individualized) Fluid restriction [Prone")
31 If not steroids, what can we do for ARDS pts? FiO2 <0.6 Tidal volume 6 ml/kg (predicted body weight) Plateau pressures <30 cm H2O Recruitment maneuvers / PEEP (individualized) Fluid restriction [Prone positioning, inhaled nitric oxide, neuromuscular blockers] [High-freq. oscillatory ventilation, ECMO]
32 An ideal study design for steroids in ARDS: Who: worsening or unresolving ARDS, despite receiving optimal supportive therapy Abx, source control of infxn, lung-protective ventilation, fluid restriction, restrictive blood transfusion protocols When: during the first week Design: randomized, double-blind, placebo-controlled Stratify randomization according to shock and vasopressor use Endpoints: mortality, ICU length of stay, long-term functional outcomes, adverse events

33 Conclusion: The use of low-dose corticosteroids was associated with improved mortality and morbidity outcomes without increased adverse reactions. The consistency of results in both study designs and all outcomes suggests that they are an effective treatment for ALI or ARDS. The mortality benefits in early ARDS should be confirmed by an adequately powered randomized trial. Crit Care Med 2009; 37:
34 2011: Even Dr. Meduri admits The balance of the available data has a moderate degree of heterogeneity and provides weak evidence (grade 2B) for a survival benefit. Treatment decisions involve a tradeoff between benefits and risk, as well as costs.
35 Recent ongoing studies related to ARDS Dexamethasone, cisatracurium, statins, omega-3 fatty acids, lipid emulsions, corticotropin injection, anticoagulants, aspirin, pentoxifylline, stem cells Intrapleural steroids ECMO PEEP / fluids / prone positioning / high-freq. oscillating vent., IL-6 removal by hemoperfusion
36 Recent ongoing studies related to ARDS Bevacizumab, dexamethasone, cisatracurium, statins, omega-3 fatty acids, lipid emulsions, corticotropin injection Intrapleural steroids ECMO PEEP / fluids / prone positioning / high-freq. oscillating vent., IL-6 removal by hemoperfusion Biomarkers (many), electrical impedance tomography monitoring


37 Questions? Comments?
ACUTE RESPIRATORY DISTRESS SYNDROME
 ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
ACUTE RESPIRATORY DISTRESS SYNDROME Angel Coz MD, FCCP, DCE Assistant Professor of Medicine UCSF Fresno November 4, 2017 No disclosures OBJECTIVES Identify current trends and risk factors of ARDS Describe
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill
 Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Back to the Future: Updated Guidelines for Evaluation and Management of Adrenal Insufficiency in the Critically Ill Joe Palumbo PGY-2 Critical Care Pharmacy Resident Buffalo General Medical Center Disclosures
Steroids for ARDS. Clinical Problem. Management
 Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Steroids for ARDS James Beck Clinical Problem A 60 year old lady re-presented to ICU with respiratory failure. She had previously been admitted for fluid management and electrolyte correction having presented
Landmark articles on ventilation
 Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
Landmark articles on ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity ARDS AECC DEFINITION-1994 ALI Acute onset Bilateral chest infiltrates PCWP
ARDS and Lung Protection
 ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
ARDS and Lung Protection Kristina Sullivan, MD Associate Professor University of California, San Francisco Department of Anesthesia and Perioperative Care Division of Critical Care Medicine Overview Low
Acute Lung Injury/ARDS. Disclosures. Overview. Acute Respiratory Failure 5/30/2014. Research funding: NIH, UCSF CTSI, Glaxo Smith Kline
 Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Disclosures Acute Respiratory Failure Carolyn S. Calfee, MD MAS UCSF Critical Care Medicine and Trauma CME May 30, 2014 Research funding: NIH, UCSF CTSI, Glaxo Smith Kline Medical advisory boards: Cerus
Acute Respiratory Distress Syndrome (ARDS) An Update
 An Update") Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
Acute Respiratory Distress Syndrome (ARDS) An Update Prof. A.S.M. Areef Ahsan FCPS(Medicine) MD(Critical Care Medicine) MD ( Chest) Head, Dept. of Critical Care Medicine BIRDEM General Hospital INTRODUCTION
ARDS: an update 6 th March A. Hakeem Al Hashim, MD, FRCP SQUH
 ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
ARDS: an update 6 th March 2017 A. Hakeem Al Hashim, MD, FRCP SQUH 30M, previously healthy Hx: 1 week dry cough Gradually worsening SOB No travel Hx Case BP 130/70, HR 100/min ph 7.29 pco2 35 po2 50 HCO3
Best of Pulmonary Jennifer R. Hucks, MD University of South Carolina School of Medicine
 Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Best of Pulmonary 2012-2013 Jennifer R. Hucks, MD University of South Carolina School of Medicine Topics ARDS- Berlin Definition Prone Positioning For ARDS Lung Protective Ventilation In Patients Without
Breathing life into new therapies: Updates on treatment for severe respiratory failure. Whitney Gannon, MSN ACNP-BC
 Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Breathing life into new therapies: Updates on treatment for severe respiratory failure Whitney Gannon, MSN ACNP-BC Overview Definition of ARDS Clinical signs and symptoms Causes Pathophysiology Management
Outcomes From Severe ARDS Managed Without ECMO. Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016
 Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
Outcomes From Severe ARDS Managed Without ECMO Roy Brower, MD Johns Hopkins University Critical Care Canada Forum Toronto November 1, 2016 Severe ARDS Berlin Definition 2012 P:F ratio 100 mm Hg Prevalence:
ARDS: The Evidence. Topics. New definition Breaths: Little or Big? Wet or Dry? Moving or Still? Upside down or Right side up?
 ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS: The Evidence Todd M Bull MD Professor of Medicine Division of Pulmonary Sciences and Critical Care Division of Cardiology Director Pulmonary Vascular Disease Center Director Center for Lungs and
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013
 ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
ARDS and Ventilators PG26 Update in Surgical Critical Care October 9, 2013 Pauline K. Park MD, FACS, FCCM University of Michigan School of Medicine Ann Arbor, MI OVERVIEW New Berlin definition of ARDS
Sub-category: Intensive Care for Respiratory Distress
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Acute Respiratory Distress
THE ACUTE RESPIRATORY DISTRESS SYNDROME. Daniel Brockman, DO
 THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
THE ACUTE RESPIRATORY DISTRESS SYNDROME Daniel Brockman, DO Objectives Describe the history and evolution of the diagnosis of ARDS Review the diagnostic criteria for ARDS Discuss the primary interventions
7/4/2015. diffuse lung injury resulting in noncardiogenic pulmonary edema due to increase in capillary permeability
 Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
Leanna R. Miller, RN, MN, CCRN-CMC, PCCN-CSC, CEN, CNRN, CMSRN, NP Education Specialist LRM Consulting Nashville, TN Objectives Identify the 5 criteria for the diagnosis of ARDS. Discuss the common etiologies
DAILY SCREENING FORM
 DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
DAILY SCREENING FORM Patient s initials: Date of admission: Time of admission: Gender: M F Year of Birth: Type of admission: Medical/Surgical/Postoperative (elective) Days Date Mechanical ventilation Lung
Subclinical Problems in the ICU:
 Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
Subclinical Problems in the ICU: Corticosteroid Insufficiency C. S. Cutillar, M.D., FPCP, FPSEM Associate Professor Cebu Institute of Medicine H-P-A Axis during Critical Illness CRH ACTH H-P-A Axis during
Management of Severe ARDS: Current Canadian Practice
 Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
Management of Severe ARDS: Current Canadian Practice Erick Duan MD FRCPC Clinical Scholar, Department of Medicine, Division of Critical Care, McMaster University Intensivist, St. Joseph's Healthcare Hamilton
What is Acute Respiratory Distress Syndrome? Acute Respiratory Distress Syndrome (ARDS)
") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) What is Acute Respiratory Distress Syndrome?
 What is Acute Respiratory Distress Syndrome?") Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
Acute Respiratory Distress Syndrome (ARDS) Sonal Pannu, MD Clinical Assistant Professor Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University
ARDS Management Protocol
 ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS Management Protocol February 2018 ARDS Criteria Onset Within 1 week of a known clinical insult or new or worsening respiratory symptoms Bilateral opacities not fully explained by effusions, lobar/lung
ARDS: MANAGEMENT UPDATE
 ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
ARDS: MANAGEMENT UPDATE Tanıl Kendirli, Assoc. Prof. Ankara University School of Medicine, Pediatric Critical Care Medicine The AECC Definition Timing Acute onset, within 48-72 hours Oxygenation ALI PaO2/FiO2
Part 2 of park s Ventilator and ARDS slides for syllabus
 Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
Part 2 of park s Ventilator and ARDS slides for syllabus Early Neuromuscular Blockade Question 4 The early use of cis-atracurium in severe ARDS is: A. Contraindicated in patients with diabetes B. Associated
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate. Carolyn Calfee, MD MAS Mark Eisner, MD MPH
 ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
ECMO for Severe Hypoxemic Respiratory Failure: Pro-Con Debate Carolyn Calfee, MD MAS Mark Eisner, MD MPH June 3, 2010 Case Presentation Setting: Community hospital, November 2009 29 year old woman with
9/5/2018. Conflicts of Interests. Pediatric Acute Respiratory Distress Syndrome. Objectives ARDS ARDS. Definitions. None
 Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Pediatric Acute Respiratory Distress Syndrome Conflicts of Interests Diane C Lipscomb, MD Director Inpatient Pediatric Medical Director Mercy Springfield Associate Clerkship Clinical Director University
Acute Respiratory Distress Syndrome
 Acute Respiratory Distress Syndrome ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications Clinical Manifestations Related to systemic inflammatory
Acute Respiratory Distress Syndrome ARDS Lung complication resulting in dangerously low blood oxygen ARDS is often a result of other health complications Clinical Manifestations Related to systemic inflammatory
Acute Respiratory Distress Syndrome
 Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Colloquium series on Integrated Systems Physiology: from molecule to function to disease Series Editors: D. Neil Granger & Joey Granger Acute Respiratory Distress Syndrome Marie Carmelle Elie Donna Carden
Acute respiratory distress syndrome
 20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
20 Acute respiratory distress syndrome Introduction i Key points Acute respiratory distress syndrome is triggered by injury to the alveolar capillary barrier from any of a variety of causes, resulting
Surviving Sepsis Campaign. Guidelines for Management of Severe Sepsis/Septic Shock. An Overview
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview Mechanical Ventilation of Sepsis-Induced ALI/ARDS ARDSnet Mechanical Ventilation Protocol Results: Mortality
Difficult Ventilation in ARDS Patients
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure.
 Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
Yuanlin Song, M.D. Clinical syndrome of severe dyspnea of rapid onset, hypoxemia, and diffuse pulmonary infiltrates leading to respiratory failure. Pneumonia Trauma SARS PaO2/fiO2
The Berlin Definition: Does it fix anything?
 The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
The Berlin Definition: Does it fix anything? Gordon D. Rubenfeld, MD MSc Professor of Medicine, University of Toronto Chief, Program in Trauma, Emergency, and Critical Care Sunnybrook Health Sciences Centre
Ventilatory Management of ARDS. Alexei Ortiz Milan; MD, MSc
 Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Ventilatory Management of ARDS Alexei Ortiz Milan; MD, MSc 2017 Outline Ventilatory management of ARDS Protected Ventilatory Strategy Use of NMB Selection of PEEP Driving pressure Lung Recruitment Prone
Nutrition and Sepsis
 Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
Nutrition and Sepsis Todd W. Rice, MD, MSc Associate Professor of Medicine Vanderbilt University 2017 DNS Symposium June 2, 2017 Case 55 y.o. male COPD, DM, HTN, presents with pneumonia and septic shock.
New Strategies in the Management of Patients with Severe Sepsis
 New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
New Strategies in the Management of Patients with Severe Sepsis Michael Zgoda, MD, MBA President, Medical Staff Medical Director, ICU CMC-University, Charlotte, NC Factors of increases in the dx. of severe
PEEP recruitment maneuver
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF Case 1: 40 yo Male restrained driver high speed MVA P 140, RR 40 labored, BP 100/70, O 2 sat 70 Chest wheeze, crackles
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: The National Heart, Lung, and Blood Institute Acute Respiratory
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: The National Heart, Lung, and Blood Institute Acute Respiratory
Management of refractory ARDS. Saurabh maji
 Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Management of refractory ARDS Saurabh maji Refractory hypoxemia as PaO2/FIO2 is less than 100 mm Hg, inability to keep plateau pressure below 30 cm H2O despite a VT of 4 ml/kg development of barotrauma
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE
 Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Fluids in Sepsis: How much and what type? John Fowler, MD, FACEP Kent Hospital, İzmir Eisenhower Medical Center, USA American Hospital Dubai, UAE In critically ill patients: too little fluid Low preload,
Biomarkers for ARDS not so simple. John Laffey. Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA
 Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Biomarkers for ARDS not so simple John Laffey Critical Illness and Injury Research Centre St Michael s Hospital, University of Toronto, CANADA Berlin ARDS definition - 2012 Mild Moderate Severe Acute Onset
Surviving Sepsis. Brian Woodcock MBChB MRCP FRCA FCCM
 1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
1 Surviving Sepsis Brian Woodcock MBChB MRCP FRCA FCCM 2 Disclosures No conflicts of interest 3 Sepsis Principles of management of septic shock in the operating room "Surviving Sepsis" guidelines 4 Add-on
Oxygenation Failure. Increase FiO2. Titrate end-expiratory pressure. Adjust duty cycle to increase MAP. Patient Positioning. Inhaled Vasodilators
 Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Oxygenation Failure Increase FiO2 Titrate end-expiratory pressure Adjust duty cycle to increase MAP Patient Positioning Inhaled Vasodilators Extracorporeal Circulation ARDS Radiology Increasing Intensity
Pneumonia in the Hospitalized
 Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
Pneumonia in the Hospitalized Patient: Use of Steroids Nicolette Myers, MD Pulmonary/Sleep/Critical Care November 9, 2018 Park Nicollet Clinic Facts About Pneumonia CAP is the 8 th most common cause of
ARDS and treatment strategies
 ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
ARDS and treatment strategies Geoff Bellingan Medical Director University College Hospital ARDS: Definitions History of predisposing condition Refractory hypoxaemia of acute onset PaO 2 /FiO 2 ratio:
Intravenous Vitamin C. Severe Sepsis Acute Lung Injury
 Intravenous Vitamin C Severe Sepsis Acute Lung Injury Alpha A. (Berry) Fowler, III, MD Professor of Medicine VCU Pulmonary Disease and Critical Care Medicine I Have No Disclosures Bacterial Sepsis Approximately
Intravenous Vitamin C Severe Sepsis Acute Lung Injury Alpha A. (Berry) Fowler, III, MD Professor of Medicine VCU Pulmonary Disease and Critical Care Medicine I Have No Disclosures Bacterial Sepsis Approximately
Steroid in Paediatric Sepsis. Dr Pon Kah Min Hospital Pulau Pinang
 Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
Steroid in Paediatric Sepsis Dr Pon Kah Min Hospital Pulau Pinang Contents Importance of steroid in sepsis Literature Review for adult studies Literature Review for paediatric studies Conclusions. Rationale
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE)
") Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE) John Laffey, Giacomo Bellani, Tai Pham, Eddy Fan, Antonio Pesenti on behalf of the LUNG SAFE Investigators
Large observational study to UNderstand the Global impact of Severe Acute respiratory FailurE (LUNG-SAFE) John Laffey, Giacomo Bellani, Tai Pham, Eddy Fan, Antonio Pesenti on behalf of the LUNG SAFE Investigators
Kansas City, MO 2 University of Missouri-Kansas City, MO 3 University of Kansas School of Pharmacy,
 in Acute Respiratory Distress Syndrome Joshua R. Howitt, Pharm.D. 1,2,3, John D. Hill, Pharm.D. Candidate 2, Trenton D. Nauser, M.D. 1,4 1 Department of Veterans Affairs, Kansas City, MO 2 University of
in Acute Respiratory Distress Syndrome Joshua R. Howitt, Pharm.D. 1,2,3, John D. Hill, Pharm.D. Candidate 2, Trenton D. Nauser, M.D. 1,4 1 Department of Veterans Affairs, Kansas City, MO 2 University of
Critical Care Medicine Update for Non-Intensivists 2015
 27 March 2015 Boca Raton Critical Care Medicine Update for Non-Intensivists 2015 MARGARET M. JOHNSON, MD CHAIR, DIVISION OF PULMONARY MEDICINE MAYO CLINIC FLORIDA Critical Care Medicine Update for The
27 March 2015 Boca Raton Critical Care Medicine Update for Non-Intensivists 2015 MARGARET M. JOHNSON, MD CHAIR, DIVISION OF PULMONARY MEDICINE MAYO CLINIC FLORIDA Critical Care Medicine Update for The
The GOLD Study. Goal of Open Lung Ventilation in Donors. Michael A. Matthay M.D. and Lorraine B. Ware, MD. Disclosures
 The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
The GOLD Study Goal of Open Lung Ventilation in Donors Michael A. Matthay M.D. and Lorraine B. Ware, MD Disclosures Research grants from the NHLBI, FDA & Industry - R37 HL51856 - R01 HL126176 - HL 110969
The use of proning in the management of Acute Respiratory Distress Syndrome
 Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
Case 3 The use of proning in the management of Acute Respiratory Distress Syndrome Clinical Problem This expanded case summary has been chosen to explore the rationale and evidence behind the use of proning
4/5/2018. Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY. I have no financial disclosures
 Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Update on Sepsis NIKHIL JAGAN PULMONARY AND CRITICAL CARE CREIGHTON UNIVERSITY I have no financial disclosures 1 Objectives Why do we care about sepsis Understanding the core measures by Centers for Medicare
Endocrine and Metabolic Complications in the ICU
 Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
Endocrine and Metabolic Complications in the ICU Linda Liu, M.D. Associate Professor UCSF Department of Anesthesia UC SF 1 New Progress Discovery of complex neuro-endocrine adaptation to critical illness
towards early goal directed therapy
 Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Paediatric Septic Shock- towards early goal directed therapy Elliot Long Paediatric Acute Care 2011 Conference Outline Emergency Department Rivers Protocol (EGDT) ACCM Sepsis Protocol Evidence Barriers
Evidence-Based. Management of Severe Sepsis. What is the BP Target?
 Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
Evidence-Based Management of Severe Sepsis Michael A. Gropper, MD, PhD Professor and Vice Chair of Anesthesia Director, Critical Care Medicine Chair, Quality Improvment University of California San Francisco
The new ARDS definitions: what does it mean?
 The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
The new ARDS definitions: what does it mean? Richard Beale 7 th September 2012 METHODS ESICM convened an international panel of experts, with representation of ATS and SCCM The objectives were to update
Pro: Early use of VV ECMO for ARDS
 Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Pro: Early use of VV ECMO for ARDS Kyle J. Rehder, MD, FCCP Associate Professor Division of Pediatric Critical Care Medicine Department of Pediatrics Duke Children s Hospital The ventilator is slowly killing
Form "EAST Multicenter Study Proposal" Study Title. Primary investigator / Senior researcher. of Primary investigator / Senior researcher
 Form "EAST Multicenter Study Proposal" Study Title Primary investigator / Senior researcher Email of Primary investigator / Senior researcher Co-primary investigator Use this area to briefly (1-2 paragraphs
Form "EAST Multicenter Study Proposal" Study Title Primary investigator / Senior researcher Email of Primary investigator / Senior researcher Co-primary investigator Use this area to briefly (1-2 paragraphs
Is ARDS Important to Recognize?
 Is ARDS Important to Recognize? Lorraine B. Ware MD Vanderbilt University Financial Disclosures: research funding from Boehringer Ingelheim, Global Blood Therapeutics Why diagnose ARDS? -initiate specific
Is ARDS Important to Recognize? Lorraine B. Ware MD Vanderbilt University Financial Disclosures: research funding from Boehringer Ingelheim, Global Blood Therapeutics Why diagnose ARDS? -initiate specific
Introduction Definition Etiology Epidemiology Lung injury prediction score. Pathophysiology Diagnosis Clinical presentation Management Conclusion
 Introduction Definition Etiology Epidemiology Lung injury prediction score Pathophysiology Diagnosis Clinical presentation Management Conclusion During the 1960s, a distinct type of a life threatening
Introduction Definition Etiology Epidemiology Lung injury prediction score Pathophysiology Diagnosis Clinical presentation Management Conclusion During the 1960s, a distinct type of a life threatening
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials
 Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
Critical Care in Obstetrics: An Innovative and Integrated Model for Learning the Essentials Respiratory Distress Syndrome and Pulmonary Edema Sonya S. Abdel-Razeq, MD Maternal-Fetal Medicine Surgical Critical
ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE
 ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE Acute respiratory distress syndrome: challenges for translational research and opportunities
ACUTE RESPIRATORY DISTRESS SYNDROME CHALLENGES FOR TRANSLATIONAL RESEARCH AND OPPORTUNITIES FOR PRECISION MEDICINE Acute respiratory distress syndrome: challenges for translational research and opportunities
Noninvasive Ventilation: Non-COPD Applications
 Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Noninvasive Ventilation: Non-COPD Applications NONINVASIVE MECHANICAL VENTILATION Why Noninvasive Ventilation? Avoids upper A respiratory airway trauma system lacerations, protective hemorrhage strategy
Adjunct Therapies for Pediatric ARDS: Where are the Data?
 Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Adjunct Therapies for Pediatric ARDS: Where are the Data? Alexandre T. Rotta, MD, FCCM Professor of Pediatrics, Linsalata Family Endowed Chair in Pediatric Critical Care and Emergency Medicine Rainbow
Ventilator ECMO Interactions
 Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Ventilator ECMO Interactions Lorenzo Del Sorbo, MD CCCF Toronto, October 2 nd 2017 Disclosure Relevant relationships with commercial entities: none Potential for conflicts within this presentation: none
Surgery Grand Rounds. Non-invasive Ventilation: A valuable tool. James Cromie, PGY 3 8/24/09
 Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
Surgery Grand Rounds Non-invasive Ventilation: A valuable tool James Cromie, PGY 3 8/24/09 History of mechanical ventilation 1930 s: use of iron lung 1940 s: First NIV system (Bellevue Hospital) 1950 s:
How ARDS should be treated in 2017
 How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
How ARDS should be treated in 2017 2017, Ostrava Luciano Gattinoni, MD, FRCP Georg-August-Universität Göttingen Germany ARDS 1. Keep the patient alive respiration circulation 2. Cure the disease leading
Objectives. Pathophysiology of Steroids. Question 1. Pathophysiology 3/1/2010. Steroids in Septic Shock: An Update
 Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
Objectives : An Update Michael W. Perry PharmD, BCPS PGY2 Critical Care Resident Palmetto Health Richland Hospital Review the history of steroids in sepsis Summarize the current guidelines for steroids
Year in Review: Critical Care Medicine
 Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Year in Review: Critical Care Medicine No disclosures Eric J. Seeley, M.D. Assistant Professor of Medicine Division of Pulmonary and Critical Care Medicine Why I Selected These Studies High quality studies
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
UPDATE IN HOSPITAL MEDICINE
 UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
UPDATE IN HOSPITAL MEDICINE FLORIDA CHAPTER ACP MEETING 2016 Himangi Kaushal, M.D., F.A.C.P. Program Director Memorial Healthcare System Internal Medicine Residency DISCLOSURES None OBJECTIVES Review some
Application of Lung Protective Ventilation MUST Begin Immediately After Intubation
 Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
Conflict of Interest Disclosure Robert M Kacmarek Managing Severe Hypoxemia!" 9-28-17 FOCUS Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts I disclose
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS
 REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
REPORT OF TRANSFUSION ADVERSE REACTION TO BLOOD CENTERS INSTRUCTIONS: Send the form to ALL blood centers that provided blood components to this patient. Timely reporting is important, so that, if appropriate,
Immunomodulation and Sepsis in Oncological Patients. Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC
 Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
Immunomodulation and Sepsis in Oncological Patients Imad Haddad, M.D. Medical Director, PICU Banner Children s Hospital at BDMC 1 Objectives Immune dys-regulation in oncological septic patients Implementation
The Use of Metabolic Resuscitation in Sepsis
 The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
The Use of Metabolic Resuscitation in Sepsis Jennifer M. Roth, PharmD, BCPS, BCCCP Critical Care Clinical Specialist - Surgical Trauma ICU Baylor University Medical Center Disclosures No conflicts of interest
Polmoniti: Steroidi sì, no, quando. Alfredo Chetta Clinica Pneumologica Università degli Studi di Parma
 Polmoniti: Steroidi sì, no, quando Alfredo Chetta Clinica Pneumologica Università degli Studi di Parma Number of patients Epidemiology and outcome of severe pneumococcal pneumonia admitted to intensive
Polmoniti: Steroidi sì, no, quando Alfredo Chetta Clinica Pneumologica Università degli Studi di Parma Number of patients Epidemiology and outcome of severe pneumococcal pneumonia admitted to intensive
No conflicts of interest
 Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Robert M. Rodriguez, MD FAAEM Clinical Professor of Medicine and Emergency Medicine, UCSF No conflicts of interest Major Points Most ICU patients start in ED Chain of critical care starting in field and
Surviving Sepsis Campaign
 Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
Surviving Sepsis Campaign Guidelines for Management of Severe Sepsis/Septic Shock An Overview By professor Ahmad Alaysh BMC-MICU 1 Surviving Sepsis A global program to Reduce mortality rates in severe
The Effect of Comorbidity on the Prognosis of Acute Lung Injury and Acute Respiratory Distress Syndrome
 ORIGINAL ARTICLE The Effect of Comorbidity on the Prognosis of Acute Lung Injury and Acute Respiratory Distress Syndrome Katsutoshi Ando 1, Tokuhide Doi 2, Sandra Y. Moody 3, Yoshihiro Ohkuni 1, Sachiko
ORIGINAL ARTICLE The Effect of Comorbidity on the Prognosis of Acute Lung Injury and Acute Respiratory Distress Syndrome Katsutoshi Ando 1, Tokuhide Doi 2, Sandra Y. Moody 3, Yoshihiro Ohkuni 1, Sachiko
Objectives. Management of Septic Shock. Definitions Progression of sepsis. Epidemiology of severe sepsis. Major goals of therapy
 Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Objectives Management of Septic Shock Review of the Evidence and Implementation of Pediatric Guidelines at Christus Santa Rosa Manish Desai, M.D. PL 5 2 nd year Pediatric Critical Care Fellow Review of
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI)
") Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Fluid Resuscitation in Critically Ill Patients with Acute Kidney Injury (AKI) Robert W. Schrier, MD University of Colorado School of Medicine Denver, Colorado USA Prevalence of acute renal failure in Intensive
Does proning patients with refractory hypoxaemia improve mortality?
 Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
Does proning patients with refractory hypoxaemia improve mortality? Clinical problem and domain I selected this case because although this was the second patient we had proned in our unit within a week,
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Update in Critical Care Medicine
 Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Update in Critical Care Medicine Michael A. Gropper, MD, PhD Professor and Executive Vice Chair Department of Anesthesia and Perioperative Care Director, Critical Care Medicine UCSF Disclosure None Update
Index. Note: Page numbers of article titles are in boldface type
 Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Index Note: Page numbers of article titles are in boldface type A Acute coronary syndrome, perioperative oxygen in, 599 600 Acute lung injury (ALI). See Lung injury and Acute respiratory distress syndrome.
Lung Recruitment Strategies in Anesthesia
 Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
Lung Recruitment Strategies in Anesthesia Intraoperative ventilatory management to prevent Post-operative Pulmonary Complications Kook-Hyun Lee, MD, PhD Department of Anesthesiology Seoul National University
PAEDIATRIC RESPIRATORY FAILURE. Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre
 PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
PAEDIATRIC RESPIRATORY FAILURE Tang Swee Fong Department of Paediatrics University Kebangsaan Malaysia Medical Centre Outline of lecture Bronchiolitis Bronchopulmonary dysplasia Asthma ARDS Bronchiolitis
Controversies in Hospital Medicine: Critical Care. Vasopressors, Steroids, and Insulin Therapy
 Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
Controversies in Hospital Medicine: Critical Care Vasopressors, Steroids, and Insulin Therapy Douglas Fish, Pharm.D. Professor of Pharmacy, University of Colorado Denver Clinical Specialist in Critical
10.2 Strategies to Optimize Parenteral Nutrition and Minimize Risks: Use of lipids May 2015
 10.2 Strategies to Optimize Parenteral Nutrition and Minimize Risks: Use of lipids May 2015 There are no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes
10.2 Strategies to Optimize Parenteral Nutrition and Minimize Risks: Use of lipids May 2015 There are no new randomized controlled trials since the 2009 and 2013 updates and hence there are no changes
ARDS Survival: Building A Roadmap to Achieve Successful Short and Long Term Outcomes
 ARDS Survival: Building A Roadmap to Achieve Successful Short and Long Term Outcomes Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant LLC Director/Ambassador WFCCN
ARDS Survival: Building A Roadmap to Achieve Successful Short and Long Term Outcomes Kathleen Vollman MSN, RN, CCNS, FCCM, FAAN Clinical Nurse Specialist/Educator/Consultant LLC Director/Ambassador WFCCN
Clinical Practice Guidelines for Cases with Pneumonia associated with Pandemic H1N infection As of 7 August 2009
 Clinical Practice Guidelines for Cases with Pneumonia associated with Pandemic H1N1 2009 infection As of 7 August 2009 This Clinical Practice Guideline contains basic information to be considered when
Clinical Practice Guidelines for Cases with Pneumonia associated with Pandemic H1N1 2009 infection As of 7 August 2009 This Clinical Practice Guideline contains basic information to be considered when
Corticosteroids in Severe CAP. Mervyn Mer Department of Medicine & ICU Johannesburg Hospital University of the Witwatersrand
 Corticosteroids in Severe CAP Mervyn Mer Department of Medicine & ICU Johannesburg Hospital University of the Witwatersrand Introduction Much controversy and debate regarding the use of corticosteroids
Corticosteroids in Severe CAP Mervyn Mer Department of Medicine & ICU Johannesburg Hospital University of the Witwatersrand Introduction Much controversy and debate regarding the use of corticosteroids
CLIP: Checklist for Lung Injury Prevention. US Critical Illness and Injury Trials Group: Lung Injury Prevention Study Investigators (USCIITG LIPS)
") CLIP: Checklist for Lung Injury Prevention US Critical Illness and Injury Trials Group: Lung Injury Prevention Study Investigators (USCIITG LIPS) USCIITG-Lung Injury Prevention Group A collaborative research
CLIP: Checklist for Lung Injury Prevention US Critical Illness and Injury Trials Group: Lung Injury Prevention Study Investigators (USCIITG LIPS) USCIITG-Lung Injury Prevention Group A collaborative research
Disclosures. Objectives. Procalcitonin: Pearls and Pitfalls in Daily Practice
 Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Procalcitonin: Pearls and Pitfalls in Daily Practice Sarah K Harrison, PharmD, BCCCP Clinical Pearl Disclosures The author of this presentation has no disclosures concerning possible financial or personal
Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders
![Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders](/thumbs/83/87321224.jpg "Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders") Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders Initial Vent Settings (Single Response) [6360] If no previous orders and no choice made by
Crit Vent Bundle for Mechanical Ventilation (337) [337] Physician - Also, enter Critical Care Admission Orders Initial Vent Settings (Single Response) [6360] If no previous orders and no choice made by
Data Collection Tool. Standard Study Questions: Admission Date: Admission Time: Age: Gender:
 Data Collection Tool Standard Study Questions: Admission Date: Admission Time: Age: Gender: Specifics of Injury: Time of Injury: Mechanism of Injury Blunt vs Penetrating? Injury Severity Score? Injuries:
Data Collection Tool Standard Study Questions: Admission Date: Admission Time: Age: Gender: Specifics of Injury: Time of Injury: Mechanism of Injury Blunt vs Penetrating? Injury Severity Score? Injuries:
15 Years Of Clinical Trials In ARDS: What Progress Have We Made?
 15 Years Of Clinical Trials In ARDS: What Progress Have We Made? Niall D. Ferguson, MD, FRCPC, MSc Head of Critical Care Medicine University Health Network & Mount Sinai Hospital Senior Scientist, Toronto
15 Years Of Clinical Trials In ARDS: What Progress Have We Made? Niall D. Ferguson, MD, FRCPC, MSc Head of Critical Care Medicine University Health Network & Mount Sinai Hospital Senior Scientist, Toronto