RESPONSIBLE OPIATE PRESCRIBING
|
|
|
- Esther Dean
- 6 years ago
- Views:
Transcription
, including as they apply to Wisconsin state")
1 RESPONSIBLE OPIATE PRESCRIBING CRESTA JONES MD DISCLOSURES No conflicts to report OBJECTIVES Understand the scope and extent of the opiate abuse crisis in the United States Demonstrate appropriate opiate prescribing for both acute and chronic pain Demonstrate appropriate use of prescription data monitoring programs (PDMPs), including as they apply to Wisconsin state law 1


2 THE OPIOID EPIDEMIC : US stats Opioid overuse/abuse is an epidemic Opioids leading cause of injury death Continuing to increase Economic impact $55 billion health and social costs related to prescription opioid abuse per year $20 billion emergency department and inpatient care for opioid poisonings hhs.gov/opioids Just another day in the US ,000 opioid prescriptions dispensed 3900 people initiate nonmedical use prescription opioids 580 people initiate heroin use hhs.gov/opioids 2

3 cdc.gov cdc.gov cdc.gov 3

4 THE OPIOID EPIDEMIC : WI 163,000 opiate use disorder Leading cause of injury deaths in Wisconsin Motor vehicle accidents, suicide, firearms Prescription opioids more overdose deaths than heroin + cocaine dhs.wisconsin.gov/publications/p01129.pdf dhs.wisconsin.gov Who uses opiates? JAMA Psychiatry
5 They started with a prescription...and they are women. HOW DID THIS HAPPEN? Increased prescriptions 5
6 HOW DID THIS HAPPEN? Increased prescriptions 1991: 76 million RX HOW DID THIS HAPPEN? Increased prescriptions 1991: 76 million RX 2014: HOW DID THIS HAPPEN? Increased prescriptions 1991: 76 million RX 2014, 240 million RX = Every US adult - 5 mg hydrocodone every 6 hours for 45 days hhs.gov/opioids 6

7 Opiate use disorder United States 5% of the world population % of the world s opiates! March 2015 HOW DID THIS HAPPEN? Increased social acceptability for use HOW DID THIS HAPPEN? Increased acceptability for use History acute and cancer pain only 1996 extended release for non cancer pain Oxycontin - ER non addictive Based on 1 year addiction rates 1% Postoperative IV narcotics 7



8 HOW DID THIS HAPPEN? Aggressive marketing by pharmaceutical companies SINCE 1999, OPIOID PRESCIPTIONS HAVE QUADRUPLED. BUT REPORTED PAIN REMAINS UNCHANGED! McNett, M Wisconsin Medical Society 8




9 OPIATE PRESCRIBING GUIDELINES OPIATE PRESCRIBING GUIDELINES OPIATE PRESCRIBING GUIDELINES Address acute and chronic pain Chronic longer than 3 months, past expected tissue healing Not for active cancer treatment, end-of-life, palliative care Not designed for pediatric pain 9
10 1. EVALUATING PAIN Pain is subjective Patient reported measures We must accept the patient s report of pain. Commensurate with causative factors? Factors adequately evaluated? Already addressed with non-opioid therapy? 2. TREATMENT OF ACUTE PAIN Consider non-opioid first Opioid START LOW AND GO SLOW! Most less than 3 days (MAX: 5 days) CDC = 7 days Consider med you can refill (APAP/codeine) Consider 2 small Rx, specific refill dates TREATMENT OF ACUTE PAIN Cochrane review acute postoperative pain Number needed to treat (NNT) 50% maximum pain relief 4-6 hours, all types of surgery Medication Number needed to treat Ibuprofen 200mg/APAP 500 mg 1.6 Naproxen 2.7 Oxycodone 5mg/APAP 325 mg 2.7 Oxycodone 15 mg 4.6 Moore et al.,

11 TREATMENT OF ACUTE PAIN Cochrane review acute postoperative pain Number needed to treat (NNT) 50% maximum pain relief 4-6 hours, all types of surgery Medication Number needed to treat Ibuprofen 200mg/APAP 500 mg 1.6 Naproxen 2.7 Oxycodone 5mg/APAP 325 mg 2.7 Oxycodone 15 mg 4.6 Moore et al., 2015 Hill MV, et al, outpatient surgical procedures Partial mastectomies, laparoscopic cholecystectomy, laparoscopic/open inguinal hernia repair Opiate naive patients Hill et al.,
12 Hill et al., 2017 Hill et al., 2017 Hill et al.,

13 Hill et al., % of opioid pills prescribed were NOT taken!! What to do with all those extra meds? Fire safe storage DEA National Drug Take-Back Days April 29, 2017 Sealable plastic bag with water + dirt, cat litter, coffee grounds Away from children Out of home for open house, social events etc. fda.gov 3. IDENTIFY AND TREAT THE CAUSE OF PAIN Address the underlying condition as the primary objective Avoid opiates if unwilling to obtain definitive treatment for condition causing pain Avoid if medical condition present is not reasonably expected to cause pain severe enough for opioids Non-anatomic pain, residual pain at old surgical sites Refer patient if needed 13
14 4. OPIOIDS ARE NOT ALWAYS THE FIRST CHOICE : ACUTE PAIN Evidence for opioids is weak Try first Acetaminophen/NSAIDs Lidocaine gel, biofreeze PT/OT Manipulation, massage Cognitive behavioral therapy If severe enough for opioids, ALWAYS use in combination with other treatments OPIOIDS ARE NOT ALWAYS THE FIRST CHOICE : ACUTE EXTENDED PAIN Look for complications of acute pain: Surgical complication Nonunion of fracture Constipation as side effect of treatment Complication ruled out, transition to non-opioid treatment OPIOIDS ARE NOT ALWAYS THE FIRST CHOICE : ACUTE EXTENDED PAIN Weaning opioids for acute extended pain (more than one week) Decrease 10-25% per week Non-narcotics for acute pain treatment Start treatment for chronic pain refer if indicated 14
15 OPIOIDS ARE NOT ALWAYS THE FIRST CHOICE : CHRONIC PAIN Past expected healing >3 months Studies few benefits, substantial increase mortality 72% INCREASE IN CARDIOVASCULAR MORTALITY No quality evidence to support use > 6 months Already initiated Close monitoring, PDMP Refer for additional treatment Contract no early fills, no other fills, urine drug screen Patient obligations : opiate prescribing I will not increase my dose or use without permission. I will not obtain opioids from other prescribers, or allow them to adjust my dose. I will use the medication exactly as directed. I will never share, sell or allow others access to my medication. I will not receive early refills. I will not abuse other drugs or alcohol during my treatment. I will bring my pills and medication bottles to each appointment. Patient obligations: opiate prescribing I will call the office at least 2 business days before I need a refill. If I miss my appointment, I may not get a refill. I will not call for opioids during evenings, holidays or weekends. I will only use one pharmacy for my opioid prescriptions. I will give a urine drug screen anytime I am asked. I will notify the office as soon as possible of any new medical condition. I will not drive or use heavy machinery while taking opioids. I will follow up as requested. I agree to allow my provider to contact all my other caregivers as needed. 15


16 wisconsinmedicalsociety.org, Opiate CME programming OPIOIDS ARE NOT ALWAYS THE FIRST CHOICE : UNWILLING PATIENT Patient unwilling to accept other treatments Questionable justification for non use nothing else works Intolerance to all other treatments 16
17 5. UTILIZE A SINGLE PROVIDER Dedicated provider primary care, pain specialist Check PDMP before start Ask about existing pain contracts Plan - acute pain outside office hours Call immediately next office day Have ED contact primary prescriber No early refills Fire safe 6. EXACERBATIONS OF CHRONIC PAIN Avoid chronic pain treatment in the emergency dept. Contact chronic pain doctor Avoid IV/IM opiates preferred agent hydromorphone Refer back to primary provider 7. UTILIZING THE PDMP Patient history of controlled substance prescriptions Prescription Data Monitoring Program (PDMP) Currently available in 49 states Prior/ongoing opioid prescriptions Dangerous combinations increasing overdose risk 17


18 WI epdmp training materials, pdmp.wi.gov 18


19 WI epdmp training materials, pdmp.wi.gov WI epdmp training materials, pdmp.wi.gov WI epdmp training materials, pdmp.wi.gov 19



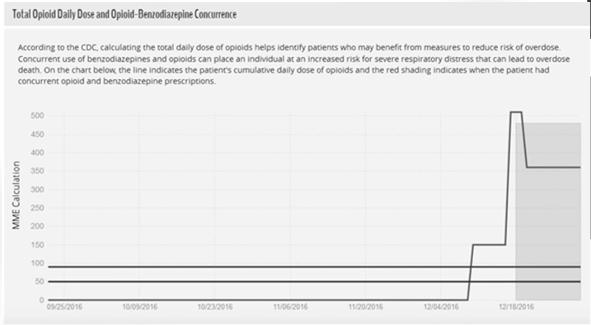
20 WI epdmp training materials, pdmp.wi.gov WI CSB report, Oct 2016 Utilizing the PDMP Red flags: Inconsistent use vs. prescribed Multiple/overlapping prescriptions Dramatic changes in dose Frequent early refills Concurrent opiate and benzo prescribing 20
21 Utilizing the PDMP: WI Act 266 (2015) April 1, 2017 Before prescribing monitored drug Exceptions Hospice 3 days or less prescribed Drug administered directly Emergency situation prevents review of PDMP PDMP not operational, technical issue must notify CSB Act 266 opiate CME prior to license renewal 8. PAIN MANAGEMENT PRIOR TO SURGERY AFFECTS RESULTS Avoid opiates for chronic pain prior to surgery Preop opiate use: Higher complication rates More postoperative narcotics Lower satisfaction rates after surgery Chronic dosing will not address acute postsurgical pain Pain will be perceived as more, but should not last longer 9. BEWARE OF BENZODIAZEPINES AVOID OPIATES + BENZOS 3x increase respiratory depression and annual mortality Neither demonstrates effectiveness more than 2 months Have patient chose, wean the other Concurrent use needs clearly documented rationale Similar effects with alcohol 21
22 Avoid Opiates + Benzos Treatment Increase annualized mortality 100 morphine mg equivalents (MME) 880% 100 MME + benzodiazepines 2640% 200 MME 2400% 200 MME + benzodiazepines 7200% 10. AVOID OXYCODONE No more effective than other oral opioids More qualities that promote addiction to a greater degree 2x euphoria of equivalent doses of oral morphine, hydrocodone Harder to d/c treatment Wightman et al, 2012 AVOID OXYCODONE More abused 16 million >12 yrs age lifetime nonmedical use of oxycodone Illicit value $1/mg ($0.15/mg if acetaminophen added) Most frequently encountered pharmaceutical Rx by law enforcement 2x as potent as morphine Natl Survey on Drug Use and Health,
23 AVOID OXYCODONE Meta-analysis RCTs examining abuse liability 9 studies Oxycodone High subjectiveness attractiveness Increased reinforcing characteristics Increased abuse liability profile Increased vs. oral morphine and oral hydrocodone Wightman et al, 2012 AVOID OXYCODONE the use of oxycodone is discouraged Should not be considered first-line Indications Intolerance of other opioids Evaluated for increased risk of abuse Zachy 2008, Schoedel OPTIMAL TREATMENT OF CHRONIC PAIN FIRST EVALUATE Targeted history/examination signs of abuse Nature/intensity of pain baseline, challenge credibility Current/past treatment, response Co-existing diseases Effect of pain on function Substance abuse history (self and family) Psychiatric disorders bipolar, ADHD, depression Medical indication for opioids documented 23

24 drugabuse.gov 12. OPTIMAL TREATMENT OF CHRONIC PAIN TRIAL OF OPIOIDS Initiation is a trial, NOT a commitment Objective goals symptoms and function prior to start 30% improvement for success Agree on goals before treatment Not met after trial wean/discontinue opioids 13. OPTIMAL TREATMENT OF CHRONIC PAIN RISK/BENEFIT Consider and start and with every refill Reassess risks/benefits Wean/discontinue with increased risk Risk of imminent danger or diverted stop and treat for withdrawal 24
25 OPTIMAL TREATMENT OF CHRONIC PAIN RISK/BENEFIT Exceptions to immediate cessation : Unstable angina Pregnancy 1 st trimester - miscarriage 3 rd trimester preterm labor OPTIMAL TREATMENT OF CHRONIC PAIN Ongoing risk assessment Review of the Prescription Drug Monitoring Program Periodic urine drug testing - at least yearly Periodic pill counts at least yearly Violation review 25
 Hydromorphone Methadone Morphine Oxycodone Time detected in Urine 48 hours 48 hours 2-4 days 3 days 48-72 hours 2-4 days")
26 Urine Drug Screening Medication Used Codeine Heroin (detected as morphine) Hydromorphone Methadone Morphine Oxycodone Time detected in Urine 48 hours 48 hours 2-4 days 3 days hours 2-4 days Healthpartners.com 14. OPTIMAL TREATMENT OF CHRONIC PAIN INFORMED CONSENT Adverse effects of treatment Addiction Overdose Death Treatment agreement Behaviors required of patient to keep them safe from adverse effects 26
27 15. INITIAL OPIOID TREATMENT - SHORT ACTING OPIOIDS Start low, go slow Titrate dose with short acting acute and chronic Consider long acting as majority of dose If stabilized on short acting Chronic therapy No indication for extended release treatment for acute pain 16. INITIAL OPIOID TREATMENT LOWEST EFFECTIVE DOSE Lowest effective dose, shortest duration Convert to morphine milligram equivalents (MME) for risk assessment 50 MME additional precautions 90 MME no evidence for higher doses Must have appropriate documentation to go higher Agencymeddirectors.wa.gov/Files/2015AMDGOpioidGuideline.pdf 27


28 Agencymeddirectors.wa.gov Agencymeddirectors.wa.gov 17. AVOID METHADONE Variable metabolism and sensitivity Days to steady state (accumulation) Drug interactions Stronger respiratory depressant Prolonged QTc effect Increased risk overdose and death Use only with extensive training/experience MAT program 28
29 18. OPIOIDS AND ILLICIT DRUG USE Increase abuse, overdose, death Strongly discouraged Clear and compelling justification 19. INITIAL OPIOID TITRATION Re-evaluation 1-4 weeks Chronic therapy: 3 months or less 20. HOME NALOXONE Indications for use; History of overdose (should be contraindication to prescribe) Opioid dose > 50 MME/day Clinical depression Other measured risk (behaviors, family history, PDMP, UDS) 0.4 IM/intranasal, repeat if needed Can be prescribed to family members Available without prescription in Wisconsin 29

30 HOME NALOXONE Wisconsin Act 200 (2014) Standing naloxone order trained WI Pharmacists Request by individual, family member, friend Screened by pharmacist, pharmacy tech Chronic opioids > 3 months Medication assisted treatment 90 MME/day or higher Medical comorbidities 21. THE RESPONSIBILITIES OF PRESCRIBING Must care for complications Assess for behaviors of opiate use disorder Assist with addiction treatment Providing directly Referring to treatment center Discharging a patient for opioid use disorder alone not acceptable DAST-10 questionnaire (drugabuse.gov) 30

31 22. DISCONTINUING TREATMENT Not effective: Decrease 10% weekly Discontinue at 5-10 MME Increased risk: Decrease 25% weekly Discontinue at 5-10 MME Clonidine 0.2 mg oral twice daily Tizanidine 2 mg oral three times daily Imminent risk of overdose, addiction, or diversion Stop immediately, treat for withdrawal cdc.gov/drugoverdose/pdf/clinical_pocket_guide_tapering-a.pdf Opioid Taper Tips Who should taper? Requests dose reduction No meaningful improvement pain/function (at least 30%) > 50 MME with no benefit Opioids with benzodiazepines Signs of opiate use disorder Early warning signs for overdose : confusion, sedation, slurred speech 31


32 Opioid Taper Tips Adjust the rate and duration of the taper based on reponse Don t reverse the taper Pause or slow and treat withdrawal When reach smallest available dose Extended interval between doses Stop when taken less than once daily Address increased overdose risk if revert to original dose Agencymeddirectors.wa.gov, 2017 cdc.gov, Mar

33 1. Non-opioid treatment preferred chronic pain 2. Establish goals of treatment before starting 3. Review risks, benefits and responsibilities before starting 4. Initiate treatment with immediate release medication 5. Prescribe lowest effective dose 6. Acute pain 3 days typical, 7 days max cdc.gov, Mar Evaluate risk of opiate-related harms start/periodically 8. Re-evaluate benefits and harms 1-4 weeks, at least every 3 mos. 9. Utilize PDMP at start, at least every 3 mos. 10. Urine drug screen at start, at least annually 11. Avoid opiates and benzodiazepines 12. Offer or arrange evidence based treatment if opiate use disorder is diagnosed cdc.gov, Mar 2016 CAN WE MAKE A DIFFERENCE? FLORIDA 2010 Regulated pain clinics No dispensing of prescription opioids from offices Established PDMP 33

 Agenda John Nygren WI Assemblyman")
34 MORE PROOF! NEW YORK 2010: PDMP before prescribing opiates 75% drop in patients with multiple prescribers TENNESSEE 2012: PDMP before prescribing opiates 36% decline in patients with multiple prescribers OREGON Established PDMP, Medicaid pre-auth high-dose methadone, naloxone education and distribution, provider education 38% decrease prescription opioid overdose 58% decrease methadone overdose THE OPIOID EPIDEMIC : WI Heroin, Opiate, Prevention and Education (HOPE) Agenda John Nygren WI Assemblyman 17 pieces of legislation ID to pick up prescriptions (199), drug disposal programs (198), pilot programs for treatment for underserved populations (195) legis.wisconsin.gov 34
35 Special considerations our patients Reproductive plan review Risk of neonatal abstinence Pre-pregnancy consultation Chronic pain Maternal Fetal Medicine Neonatology Effective contraception Conclusion The United States is currently experiencing an unprecedented crisis in opiate use disorders Although there is no easy fix, we can contribute to the solution Progress is made through responsible management of acute and chronic pain Patient and provider education is key to optimal pain management while also minimizing unnecessary opiate prescribing References Ossiander EM. Using textual cause-of-death data to study drug poisoning. Am J Epidemiol Apr 1:179(7). Hill MV, et al. Wide variation and excessive dosage of opioid prescriptions for common general surgical procedures. Ann Surg Apr; 265(4): Manchikanti L et al., Responsible, safe, and effective prescription of opioids for chronic non-cancer pain: American Society of Interventional Pain Physicians (ASIPP) guidelines. Pain Physician 2017 Feb;20(2S): S3-S92. Moore RA et al., Single dose oral analgesics for acute postoperative pain in adults. Cochrane Database of Systematic Reviews, Sept CDC Guideline for Prescribing Opioids for Chronic Pain United States Dowell D et al. JAMA 2016 Apr 19/315(15): Zachny J and Gutierrez S. Subjective, psychomotor, and physiological effects profile of hydrocodone/acetaminophen and oxycodone/acetaminophen combination products. Pain Medicine 2008; 9(4): Schoedel K et al. Positive and negative subjective effects of extended-release oxymorphone versus controlled-release oxycodone in recreational opioid users. J Opioid Manag 2011; 7(3):
36 References Manchikanti et al. Opioid epidemic in the United States. Pain Phys 2012; 15:ES9-ES38 Manchikanti et al. Therapeutic opioids: a 10 year perspective on the complexities and complications of the escalating use, abuse and nonmedical use of opioids. Pain Phys 2008; 11:S63-S88. National Survey on Drug Use and Health. DEA diversion, March Wightman R et al. Likeability and abuse liability of commonly prescribed opiates. J Med Toxicol 2012; 8:
Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline
 Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline: To help providers make informed decisions about acute and chronic pain treatment -pain lasting longer than three months
Wisconsin Opioid Prescribing Guideline Draft Scope and purpose of the guideline: To help providers make informed decisions about acute and chronic pain treatment -pain lasting longer than three months
Opioid Management of Chronic (Non- Cancer) Pain
 Pain") Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Rule Governing the Prescribing of Opioids for Pain
 Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
CDC Guideline for Prescribing Opioids for Chronic Pain. Centers for Disease Control and Prevention National Center for Injury Prevention and Control
 CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Prescription Monitoring Program (PMP)
") 06/15/2018 FACT SHEET Implementation of Enacted Prescribing Limits and Requirements and Relevant Opioid Prescribing Laws and Rules Background: The 2016 law (Chapter 488) makes five major changes to opioid
06/15/2018 FACT SHEET Implementation of Enacted Prescribing Limits and Requirements and Relevant Opioid Prescribing Laws and Rules Background: The 2016 law (Chapter 488) makes five major changes to opioid
Prescribing Opioids in the Opioid Epidemic. Scott Woffinden, PA-C Jason Chapman, JD
 Prescribing Opioids in the Opioid Epidemic Scott Woffinden, PA-C Jason Chapman, JD What's the Problem? http://www.zdoggmd.com/blank-script-taylor-swift-parody/ What's the Problem? CDC 115 Americans die
Prescribing Opioids in the Opioid Epidemic Scott Woffinden, PA-C Jason Chapman, JD What's the Problem? http://www.zdoggmd.com/blank-script-taylor-swift-parody/ What's the Problem? CDC 115 Americans die
SAFE PRESCRIBING: RULES AND REGULATIONS. Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017
 SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017 DISCLOSURES I have no financial disclosures. OBJECTIVES Discuss the significance of the opiate
SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017 DISCLOSURES I have no financial disclosures. OBJECTIVES Discuss the significance of the opiate
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018
 Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Welcome - we will begin the webinar shortly Please read the participation tips below:
 Welcome - we will begin the webinar shortly Please read the participation tips below: All guest phones have been muted: Background noises, conversations, white noise etc., can be disruptive to a webinar.
Welcome - we will begin the webinar shortly Please read the participation tips below: All guest phones have been muted: Background noises, conversations, white noise etc., can be disruptive to a webinar.
MANAGING THE COSTS OF THE OPIOID EPIDEMIC IN WISCONSIN. State Senator Alberta Darling
 MANAGING THE COSTS OF THE OPIOID EPIDEMIC IN WISCONSIN State Senator Alberta Darling A NATIONAL PROBLEM According to the 2014 National Survey on Drug Use and Health: 435,000 Americans have used heroin
MANAGING THE COSTS OF THE OPIOID EPIDEMIC IN WISCONSIN State Senator Alberta Darling A NATIONAL PROBLEM According to the 2014 National Survey on Drug Use and Health: 435,000 Americans have used heroin
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care)
") Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN
 OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN ANTOINETTE BROWN, RPH LAUREL RAMER, 2019 PHARMD CANDIDATE 2018 WYOMING CONFERENCE ON AGING LARAMIE, WY OCTOBER 3, 2018 OBJECTIVES 1. Understand the
OPIOIDS: THE GOOD, THE BAD, AND EVERYTHING IN-BETWEEN ANTOINETTE BROWN, RPH LAUREL RAMER, 2019 PHARMD CANDIDATE 2018 WYOMING CONFERENCE ON AGING LARAMIE, WY OCTOBER 3, 2018 OBJECTIVES 1. Understand the
OPIOID PRESCRIBING RULES. May 17, 2017 Webinar
 OPIOID PRESCRIBING RULES May 17, 2017 Webinar Outline Introduction and Universal Precautions Dr. Levine, Commissioner, Health Department 15 Minutes Acute Pain Dr. Patti Fisher, UVMMC 20 Minutes Chronic
OPIOID PRESCRIBING RULES May 17, 2017 Webinar Outline Introduction and Universal Precautions Dr. Levine, Commissioner, Health Department 15 Minutes Acute Pain Dr. Patti Fisher, UVMMC 20 Minutes Chronic
CDC Guideline for Prescribing Opioids for Chronic Pain
 National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
Subject: Pain Management (Page 1 of 7)
") Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
See Important Reminder at the end of this policy for important regulatory and legal information.
 Effective Date: 04.18 Last Review Date: 04.18 Line of Business: Medicaid- AHCCCS Revision Log See Important Reminder at the end of this policy for important regulatory and legal information. Description
Effective Date: 04.18 Last Review Date: 04.18 Line of Business: Medicaid- AHCCCS Revision Log See Important Reminder at the end of this policy for important regulatory and legal information. Description
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Opioid Analgesics Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 11.17 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the
Clinical Policy: Opioid Analgesics Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 11.17 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the
Opioid Prescribing Guidelines for Patients in the Emergency Department
 Opioid Prescribing Guidelines for Patients in the Emergency Department and Immediate Care Centers These guidelines are meant to assist clinicians in treating patients with acute and chronic pain in the
Opioid Prescribing Guidelines for Patients in the Emergency Department and Immediate Care Centers These guidelines are meant to assist clinicians in treating patients with acute and chronic pain in the
UnitedHealthcare Pharmacy Clinical Pharmacy Programs
 UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 4000-3 Program Opioid Overutilization Cumulative Drug Utilization Review Criteria Medication Includes all salt forms, single and
UnitedHealthcare Pharmacy Clinical Pharmacy Programs Program Number 2018 P 4000-3 Program Opioid Overutilization Cumulative Drug Utilization Review Criteria Medication Includes all salt forms, single and
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 02.18 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this policy
Clinical Policy: Reference Number: HIM.PA.139 Effective Date: 12.01.17 Last Review Date: 02.18 Line of Business: Health Insurance Marketplace Revision Log See Important Reminder at the end of this policy
CLINICAL POLICY Clinical Policy: Extended Release Opioid Analgesics
 Reference Number: AZ.CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.18 Line of Business: Medicaid- AHCCCS Revision Log See Important Reminder at the end of this policy for important regulatory and
Reference Number: AZ.CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.18 Line of Business: Medicaid- AHCCCS Revision Log See Important Reminder at the end of this policy for important regulatory and
Dr. Smith. Roneet Lev, MD FACEP Chief, Emergency Department Scripps Mercy Hospital Chair, San Diego Prescription Drug Abuse Medical Task Force
 Dr. Smith Roneet Lev, MD FACEP Chief, Emergency Department Scripps Mercy Hospital Chair, San Diego Prescription Drug Abuse Medical Task Force 1 1 How We Got Here 2 The Epidemic 3 4 San Diego Death Diaries
Dr. Smith Roneet Lev, MD FACEP Chief, Emergency Department Scripps Mercy Hospital Chair, San Diego Prescription Drug Abuse Medical Task Force 1 1 How We Got Here 2 The Epidemic 3 4 San Diego Death Diaries
6/6/2017. First Do No Harm SECTION 1 THE OPIOID CRISIS. Implementing an Opioid Stewardship Program in a HealthCare System OBJECTIVES
 First Do No Harm Implementing an Opioid Stewardship Program in a HealthCare System Phil Chang, MD Kristy Deep, MD Doug Oyler, PharmD June 12, 2017 OBJECTIVES Explain the role of opioid stewardship as a
First Do No Harm Implementing an Opioid Stewardship Program in a HealthCare System Phil Chang, MD Kristy Deep, MD Doug Oyler, PharmD June 12, 2017 OBJECTIVES Explain the role of opioid stewardship as a
Clinical Policy: Opioid Analgesics Reference Number: CP.PMN.97 Effective Date: Last Review Date: 02.19
 Clinical Policy: Reference Number: CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.19 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.19 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory
The Prescription Review Program and College Expectations. Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM
 The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
Opioid Abuse in Iowa Rx to Heroin. Iowa Governor s Office of Drug Control Policy January 2016
 1 Opioid Abuse in Iowa Rx to Heroin Iowa Governor s Office of Drug Control Policy January 2016 Why Is This Important? 2 3 National Rx Painkiller Trends CDC, 2013 4 National Rx-Heroin Trends NIH, 2015 5
1 Opioid Abuse in Iowa Rx to Heroin Iowa Governor s Office of Drug Control Policy January 2016 Why Is This Important? 2 3 National Rx Painkiller Trends CDC, 2013 4 National Rx-Heroin Trends NIH, 2015 5
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING
 THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
Summary of Recommendations...3. PEG: A Three-Item Scale Assessing Pain (Appendix A) Chronic Pain Flow Sheet Acute Pain Flow Sheet...
 Chronic Pain Flow Sheet Acute Pain Flow Sheet...") Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Opioid Review and MAT Clinic CDC Guidelines
 1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
Clinical Policy: Opioid Analgesics Reference Number: CP.PMN.97 Effective Date: Last Review Date: 02.18
 Clinical Policy: Reference Number: CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory
Clinical Policy: Reference Number: CP.PMN.97 Effective Date: 02.11 Last Review Date: 02.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important regulatory
The Wisconsin Prescription Drug Monitoring Program. WI PDMP Timeline. PDMP Overview. What is a PDMP? PDMPs Across the Nation. Wisconsin.
 The Wisconsin Prescription Drug Monitoring Program Wisconsin Nurses Association Jail Health Care Conference May 21, 2018 WI PDMP Timeline PDMP Overview January 2013 WI PDMP operational April 2017 WI epdmp
The Wisconsin Prescription Drug Monitoring Program Wisconsin Nurses Association Jail Health Care Conference May 21, 2018 WI PDMP Timeline PDMP Overview January 2013 WI PDMP operational April 2017 WI epdmp
October 20, 2016 Scott K. Proescholdbell, MPH. Opioid Overdose and North Carolina s Public Health and Prevention Strategies
 October 20, 2016 Scott K. Proescholdbell, MPH Opioid Overdose and North Carolina s Public Health and Prevention Strategies Deaths per 100,000 population Death Rates* for Three Selected Causes of Injury,
October 20, 2016 Scott K. Proescholdbell, MPH Opioid Overdose and North Carolina s Public Health and Prevention Strategies Deaths per 100,000 population Death Rates* for Three Selected Causes of Injury,
Update on Maine Laws and Associated Rules on Prescribing Opioid Medication
 Update on Maine Laws and Associated Rules on Prescribing Opioid Medication Gordon H. Smith, Esq. Executive Vice President Maine Medical Association 2018 Disclosure There are no significant or relevant
Update on Maine Laws and Associated Rules on Prescribing Opioid Medication Gordon H. Smith, Esq. Executive Vice President Maine Medical Association 2018 Disclosure There are no significant or relevant
Management of Pain - A Comparison of Current Guidelines
 Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Opioids: What You Should Know About Opioid Prescribing. Denis G. Patterson, DO Nevada State Medical Association October 19, 2016
 Opioids: What You Should Know About Opioid Prescribing Denis G. Patterson, DO Nevada State Medical Association October 19, 2016 Contact Information Denis G. Patterson, DO Nevada Advanced Pain Specialists
Opioids: What You Should Know About Opioid Prescribing Denis G. Patterson, DO Nevada State Medical Association October 19, 2016 Contact Information Denis G. Patterson, DO Nevada Advanced Pain Specialists
2. Is this request for a preferred medication? Y N
 Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
The Wisconsin Prescription Drug Monitoring Program
 The Wisconsin Prescription Drug Monitoring Program DHS 2018 WI Opioid Forum April 12, 2018 Learning Objectives 1. How the WI epdmp supports healthcare professionals in making informed prescribing, dispensing
The Wisconsin Prescription Drug Monitoring Program DHS 2018 WI Opioid Forum April 12, 2018 Learning Objectives 1. How the WI epdmp supports healthcare professionals in making informed prescribing, dispensing
Spotlight on Health Policy Beyond the Clinical: The Opioid Epidemic. October 25, 2017
 Spotlight on Health Policy Beyond the Clinical: The Opioid Epidemic October 25, 2017 Disclosures and Disclaimer Neither the Institute for Health Policy and Leadership (IHPL) nor I have any relevant financial
Spotlight on Health Policy Beyond the Clinical: The Opioid Epidemic October 25, 2017 Disclosures and Disclaimer Neither the Institute for Health Policy and Leadership (IHPL) nor I have any relevant financial
WHY GOOD PAIN MANAGEMENT IS GOOD DRUG ABUSE PREVENTION
 WHY GOOD PAIN MANAGEMENT IS GOOD DRUG ABUSE PREVENTION Bob Twillman, Ph.D., FAPM Executive Director Academy of Integrative Pain Management Walking the Tightrope of Pain Management Adverse Events Misuse
WHY GOOD PAIN MANAGEMENT IS GOOD DRUG ABUSE PREVENTION Bob Twillman, Ph.D., FAPM Executive Director Academy of Integrative Pain Management Walking the Tightrope of Pain Management Adverse Events Misuse
Oregon Opioid Overdose Prevention Initiative
 Oregon Opioid Overdose Prevention Initiative Katrina Hedberg, MD, MPH Health Officer & State Epidemiologist Oregon Public Health Division Oregon Association of Hospitals & Health Systems February 2017
Oregon Opioid Overdose Prevention Initiative Katrina Hedberg, MD, MPH Health Officer & State Epidemiologist Oregon Public Health Division Oregon Association of Hospitals & Health Systems February 2017
AHLA. X. Federal Enforcement of Fraud and Abuse Involving Opioid Abuse and Diversion
 Fraud and Compliance Forum, October 2017. Click here to access audio. AHLA X. Federal Enforcement of Fraud and Abuse Involving Opioid Abuse and Diversion Michelle Bergholz Frazier Senior Vice President,
Fraud and Compliance Forum, October 2017. Click here to access audio. AHLA X. Federal Enforcement of Fraud and Abuse Involving Opioid Abuse and Diversion Michelle Bergholz Frazier Senior Vice President,
Prescription Opioid Addiction
 CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
3. Has the patient had a sustained improvement in Pain or Function (e.g. PEG scale with a 30 percent response from baseline)?
?") Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
The Oregon Opioid Initiative. State Pain & Opioid Conference Prescription Drug Monitoring May 2018 Lisa Millet, Public Health Division
 The Oregon Opioid Initiative State Pain & Opioid Conference Prescription Drug Monitoring May 2018 Lisa Millet, Public Health Division Disclosure No disclosures 2 Learning Objectives Learner will be able
The Oregon Opioid Initiative State Pain & Opioid Conference Prescription Drug Monitoring May 2018 Lisa Millet, Public Health Division Disclosure No disclosures 2 Learning Objectives Learner will be able
White Paper on. Prescription Drug Abuse
 White Paper on Prescription Drug Abuse October 22, 2014 Table of Contents: I. Introduction II. Scope of the Problem III. Most Common Drugs Involved in Overdoses IV. Efforts in Tennessee V. Prescription
White Paper on Prescription Drug Abuse October 22, 2014 Table of Contents: I. Introduction II. Scope of the Problem III. Most Common Drugs Involved in Overdoses IV. Efforts in Tennessee V. Prescription
New Guidelines for Opioid Prescribing
 New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
Risk Reduction Strategies in Pain Management
 Risk Reduction Strategies in Pain Management Melissa J. Durham, PharmD, MACM, BCACP, DAAPM Assistant Professor of Clinical Pharmacy USC School of Pharmacy Clinical Pharmacist, The USC Pain Center Learning
Risk Reduction Strategies in Pain Management Melissa J. Durham, PharmD, MACM, BCACP, DAAPM Assistant Professor of Clinical Pharmacy USC School of Pharmacy Clinical Pharmacist, The USC Pain Center Learning
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic
 Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
Opioid Analgesics: Responsible Prescribing in the Midst of an Epidemic Lucas Buffaloe, MD Associate Professor of Clinical Family and Community Medicine University of Missouri Health Care Goals for today
The STOP Measure. Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018
 The STOP Measure Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018 AHIP s Safe, Transparent Opioid Prescribing (STOP) Initiative Methodology
The STOP Measure Safe and Transparent Opioid Prescribing to Promote Patient Safety and Reduced Risk of Opioid Misuse FEBRUARY 2018 AHIP s Safe, Transparent Opioid Prescribing (STOP) Initiative Methodology
CLINICAL POLICY DEPARTMENT: Medical
 IMPTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of currently available generally
IMPTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of currently available generally
Prior Authorization Guideline
 Guideline GL-35952 Opioid Quantity Limit Overrides Formulary OptumRx Formulary Note: Approval Date 7/10/2017 Revision Date 7/10/2017 Technician Note: P&T Approval Date: 2/16/2010; P&T Revision Date: 7/12/2011
Guideline GL-35952 Opioid Quantity Limit Overrides Formulary OptumRx Formulary Note: Approval Date 7/10/2017 Revision Date 7/10/2017 Technician Note: P&T Approval Date: 2/16/2010; P&T Revision Date: 7/12/2011
Objectives. What is pain? 9/27/2017. Pain: Does this Hurt? Fall 2017 Dean Fox, MD, FACP
 Pain: Does this Hurt? Fall 2017 Dean Fox, MD, FACP Photo credit: http://multiple-sclerosis-research.blogspot.com/2013/10/pain-and-unemployment.html Objectives Consider personal goal of pain management
Pain: Does this Hurt? Fall 2017 Dean Fox, MD, FACP Photo credit: http://multiple-sclerosis-research.blogspot.com/2013/10/pain-and-unemployment.html Objectives Consider personal goal of pain management
Michael M. Miller, MD, FASAM, FAPA
 Michael M. Miller, MD, FASAM, FAPA mmiller@rogershospital.org Medical Director, Herrington Recovery Center (HRC) Rogers Memorial Hospital Oconomowoc, Wisconsin Vice Speaker Wisconsin Medical Society Clinical
Michael M. Miller, MD, FASAM, FAPA mmiller@rogershospital.org Medical Director, Herrington Recovery Center (HRC) Rogers Memorial Hospital Oconomowoc, Wisconsin Vice Speaker Wisconsin Medical Society Clinical
DECEMBER 7, 2017 THE OPIOID EPIDEMIC & THE UNIVERSITY S RESPONSE
 DECEMBER 7, 2017 THE OPIOID EPIDEMIC & THE UNIVERSITY S RESPONSE Agenda Welcome & Introductions Trending Articles The Opioid Epidemic Key Updates What are Opioids? Chemically similar to heroin, prescribed
DECEMBER 7, 2017 THE OPIOID EPIDEMIC & THE UNIVERSITY S RESPONSE Agenda Welcome & Introductions Trending Articles The Opioid Epidemic Key Updates What are Opioids? Chemically similar to heroin, prescribed
D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine
 D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine Financial Disclosure I have no relevant financial relationships
D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine Financial Disclosure I have no relevant financial relationships
Literature year in review: Fast take
 Literature year in review: Fast take Fatal opioid overdoses have declined in parts of Eastern Mass. By Catie Edmondson GLOBE CORRESPONDENT AUGUST 11, 2017 EMS program called First Watch: Alert to district
Literature year in review: Fast take Fatal opioid overdoses have declined in parts of Eastern Mass. By Catie Edmondson GLOBE CORRESPONDENT AUGUST 11, 2017 EMS program called First Watch: Alert to district
Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup. Opioid Prescribing Metrics - DRAFT
 Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup Opioid Prescribing Metrics - DRAFT Definitions: Days Supply: The total of all opioid prescriptions dispensed during the calendar quarter
Bree Collaborative AMDG Opioid Prescribing Guidelines Workgroup Opioid Prescribing Metrics - DRAFT Definitions: Days Supply: The total of all opioid prescriptions dispensed during the calendar quarter
Prescription Opioid Overdose in Oregon: A public health perspective
 Prescription Opioid Overdose in Oregon: A public health perspective Katrina Hedberg, MD, MPH Health Officer & State Epidemiologist Oregon Public Health Division Oregon Health Authority All-Cause Mortality,
Prescription Opioid Overdose in Oregon: A public health perspective Katrina Hedberg, MD, MPH Health Officer & State Epidemiologist Oregon Public Health Division Oregon Health Authority All-Cause Mortality,
Unintentional Poisonings: Public Health Response Joint Legislative Health Care Oversight Committee
 Unintentional Poisonings: Public Health Response Joint Legislative Health Care Oversight Committee Dr. Ruth Petersen Chronic Disease and Injury Section Division of Public Health Oct 12, 2010 In 1999, the
Unintentional Poisonings: Public Health Response Joint Legislative Health Care Oversight Committee Dr. Ruth Petersen Chronic Disease and Injury Section Division of Public Health Oct 12, 2010 In 1999, the
Shawn A. Ryan, MD, MBA Assistant Professor, Dept. of Emergency Medicine, University of Cincinnati Chair of Quality & Patient Safety, Jewish
 Shawn A. Ryan, MD, MBA Assistant Professor, Dept. of Emergency Medicine, University of Cincinnati Chair of Quality & Patient Safety, Jewish Hospital-Mercy Health Partners Addiction Specialist, BrightView
Shawn A. Ryan, MD, MBA Assistant Professor, Dept. of Emergency Medicine, University of Cincinnati Chair of Quality & Patient Safety, Jewish Hospital-Mercy Health Partners Addiction Specialist, BrightView
High-Decile Prescribers: All Gain, No Pain?
 High-Decile Prescribers: All Gain, No Pain? Len Paulozzi, MD, MPH National Center for Injury Prevention and Control Centers for Disease Control and Prevention National Center for Injury Prevention and
High-Decile Prescribers: All Gain, No Pain? Len Paulozzi, MD, MPH National Center for Injury Prevention and Control Centers for Disease Control and Prevention National Center for Injury Prevention and
Scope of the Opiate Problem 6/5/18. Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond. Overview.
 Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Opioid Use and Other Trends
 Opioid Use and Other Trends National Overview Across the nation communities are struggling with a devastating increase in the number of people misusing opioid drugs, leading many to identify the current
Opioid Use and Other Trends National Overview Across the nation communities are struggling with a devastating increase in the number of people misusing opioid drugs, leading many to identify the current
Strategies to Manage The Opioid Crisis
 Strategies to Manage The Opioid Crisis Matt Feehery, LCDC Senior Vice President & CEO PaRC (Prevention & Recovery Center) Behavioral Health Services February 1, 2018 A Pill for Your Pain But my doctor
Strategies to Manage The Opioid Crisis Matt Feehery, LCDC Senior Vice President & CEO PaRC (Prevention & Recovery Center) Behavioral Health Services February 1, 2018 A Pill for Your Pain But my doctor
Clinical Policy: Opioid Analgesics Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid
 Clinical Policy: Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: Reference Number: OH.PHAR.PPA.13 Effective Date: 10/2017 Last Review Date: 6/2018 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Prescription for Disaster: Impact of Drugs in our Society
 Prescription for Disaster: Impact of Drugs in our Society What you can do about the epidemic of drug abuse in our communities 1 Florida Poison Information Center-Tampa 10/26/2012 Cynthia R. Lewis-Younger,
Prescription for Disaster: Impact of Drugs in our Society What you can do about the epidemic of drug abuse in our communities 1 Florida Poison Information Center-Tampa 10/26/2012 Cynthia R. Lewis-Younger,
Oregon ACEP Opioid Prescribing Guidelines. Why are we talking about this?
 Oregon ACEP Opioid Prescribing Guidelines Hans Notenboom, M.D. FACEP Current OCEP President Why are we talking about this? Current opioid epidemic 33,000 deaths over half with Rx meds Since 1999 number
Oregon ACEP Opioid Prescribing Guidelines Hans Notenboom, M.D. FACEP Current OCEP President Why are we talking about this? Current opioid epidemic 33,000 deaths over half with Rx meds Since 1999 number
Legal Issues in Opioid Prescribing
 Legal Issues in Opioid Prescribing Joanne L. Martin, J.D. Legal Counsel Mayo Clinic Rochester, Mn 2015 MFMER slide-1 Conflict of Interest I have no relevant financial relationships to disclose I will not
Legal Issues in Opioid Prescribing Joanne L. Martin, J.D. Legal Counsel Mayo Clinic Rochester, Mn 2015 MFMER slide-1 Conflict of Interest I have no relevant financial relationships to disclose I will not
Opioid epidemic and PEHP
 Opioid epidemic and PEHP Agenda Overview of opioid crisis Utah perspective PEHP: clinical interventions Impact of interventions Why are we here? In the 1990s, the medical establishment came to believe
Opioid epidemic and PEHP Agenda Overview of opioid crisis Utah perspective PEHP: clinical interventions Impact of interventions Why are we here? In the 1990s, the medical establishment came to believe
IMPLEMENTATION OF A SHARED MEDICAL APPOINTMENT FOR OPIOID OVERDOSE EDUCATION AND NALOXONE KIT TRAINING FOR VETERANS Kristin A. Tallman, Pharm.
 IMPLEMENTATION OF A SHARED MEDICAL APPOINTMENT FOR OPIOID OVERDOSE EDUCATION AND NALOXONE KIT TRAINING FOR VETERANS Kristin A. Tallman, Pharm.D, BCPS Clinical Pharmacy Specialist Providence Medical Group
IMPLEMENTATION OF A SHARED MEDICAL APPOINTMENT FOR OPIOID OVERDOSE EDUCATION AND NALOXONE KIT TRAINING FOR VETERANS Kristin A. Tallman, Pharm.D, BCPS Clinical Pharmacy Specialist Providence Medical Group
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT
 Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT Learning Objectives Review Opioid Crisis CDC Guidelines for opioid prescribing Discuss Alternatives
Non Opioid Approaches to Pain and Musculoskeletal Disorders KEVIN ODONNELL, DO FLAGSTAFF BONE AND JOINT Learning Objectives Review Opioid Crisis CDC Guidelines for opioid prescribing Discuss Alternatives
1/30/2017 SEISMIC UPGRADE FOR THE OPIOID PARADIGM SHIFT ACPE PRE-TEST QUESTIONS. I have no declarations.
 SEISMIC UPGRADE FOR THE OPIOID PARADIGM SHIFT Traci Hamer, PharmD, MAT Kaiser Permanente Northwest Pain Management Pharmacy Services I have no declarations. ACPE PRE-TEST QUESTIONS True/False: Opioids
SEISMIC UPGRADE FOR THE OPIOID PARADIGM SHIFT Traci Hamer, PharmD, MAT Kaiser Permanente Northwest Pain Management Pharmacy Services I have no declarations. ACPE PRE-TEST QUESTIONS True/False: Opioids
Blue Cross of Idaho Addresses State s Opioid Issue
 Blue Cross of Idaho Addresses State s Opioid Issue BY THE NUMBERS - Opioid Management page 3 THE PROBLEM - How Preventing Pain Hurt Us page 4 THE SOLUTIONS - Idaho State Board Of Pharmacy Prescription
Blue Cross of Idaho Addresses State s Opioid Issue BY THE NUMBERS - Opioid Management page 3 THE PROBLEM - How Preventing Pain Hurt Us page 4 THE SOLUTIONS - Idaho State Board Of Pharmacy Prescription
Naloxone and Combating the Opioid Epidemic
 Objectives Naloxone and Combating the Opioid Epidemic Jeff Jacobson PharmD Southpointe Pharmacy Discuss the current opioid crisis Define the role of Naloxone in opioid overdose Analyze the barriers to
Objectives Naloxone and Combating the Opioid Epidemic Jeff Jacobson PharmD Southpointe Pharmacy Discuss the current opioid crisis Define the role of Naloxone in opioid overdose Analyze the barriers to
New Guidelines for Prescribing Opioids
 New Guidelines for Prescribing Opioids Keeping Your Claimants Safe Presented by: Dr. Mitch Freeman, Pharm.D. Chief Clinical Officer, Pharmacy Solutions Agenda The Opioid Challenge Today How We Got Here
New Guidelines for Prescribing Opioids Keeping Your Claimants Safe Presented by: Dr. Mitch Freeman, Pharm.D. Chief Clinical Officer, Pharmacy Solutions Agenda The Opioid Challenge Today How We Got Here
Prescription Opioids in Vermont A DISCUSSION ABOUT LAWS AND GUIDELINES MICHAEL J. KENOSH, MD
 Prescription Opioids in Vermont A DISCUSSION ABOUT LAWS AND GUIDELINES MICHAEL J. KENOSH, MD Rule(s) Governing the Prescribing of Opioids for Pain KEY rule adopted pursuant to Sections 14(e) and 11(e)
Prescription Opioids in Vermont A DISCUSSION ABOUT LAWS AND GUIDELINES MICHAEL J. KENOSH, MD Rule(s) Governing the Prescribing of Opioids for Pain KEY rule adopted pursuant to Sections 14(e) and 11(e)
Opioid Analgesics. Recommended starting dose for opioid-naïve patients
 Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
Opioid Analgesics Goals: Restrict use of opioid analgesics to OHP-funded conditions with documented sustained improvement in pain and function and with routine monitoring for opioid misuse and abuse. Promote
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: LA.PPA.12 Effective Date: 02/11 Last Review Date: 01/18 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of this policy for
Clinical Policy: Reference Number: LA.PPA.12 Effective Date: 02/11 Last Review Date: 01/18 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of this policy for
The Epidemiology of Opioid Abuse. Thomas Dobbs, MD, MPH Mississippi State Department of Health
 The Epidemiology of Opioid Abuse Thomas Dobbs, MD, MPH Mississippi State Department of Health 1/12/2018 ACKNOWLEDGEMENTS DRUG ABUSE WORKING GROUP MISSISSIPPI STATE DEPARTMENT OF HEALTH Manuela Staneva,
The Epidemiology of Opioid Abuse Thomas Dobbs, MD, MPH Mississippi State Department of Health 1/12/2018 ACKNOWLEDGEMENTS DRUG ABUSE WORKING GROUP MISSISSIPPI STATE DEPARTMENT OF HEALTH Manuela Staneva,
The Prescription Review Program and College Expectations. Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM
 The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM October 13, 2017 Disclosure Relationship with commercial interests: None Professional roles:
The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM October 13, 2017 Disclosure Relationship with commercial interests: None Professional roles:
Opioid Addiction Statistics
 May 2017 Opioid Addiction Statistics Definitions Heroin Epidemic - As pill mills close, prescribing is becoming tighter, demand among younger users rise, and dealer s profits rise, addicts are turning
May 2017 Opioid Addiction Statistics Definitions Heroin Epidemic - As pill mills close, prescribing is becoming tighter, demand among younger users rise, and dealer s profits rise, addicts are turning
Recommendations in Opioid Prescribing Guidelines for Chronic Pain
 Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Recommendations in Opioid Prescribing Guidelines for Chronic Pain The use of opioids for treating chronic pain has been increasing. 1 In 2010, an estimated 20% of patients presenting to physician offices
Managing Narcotics on Workers Comp Claims. Presented By: Craig S. Stern, PharmD, MBA President Pro Pharma Pharmaceutical Consultants, Inc.
 Managing Narcotics on Workers Comp Claims Presented By: Craig S. Stern, PharmD, MBA President Pro Pharma Pharmaceutical Consultants, Inc. October 21, 2014 Outline Rationale Scope list drug list Recommended
Managing Narcotics on Workers Comp Claims Presented By: Craig S. Stern, PharmD, MBA President Pro Pharma Pharmaceutical Consultants, Inc. October 21, 2014 Outline Rationale Scope list drug list Recommended
The Population is Abusing Drugs, but are Drugs Abusing Insurance?
 Image licensed from Shutterstock The Population is Abusing Drugs, but are Drugs Abusing Insurance? 01/30/2018 Gina C. Guzman, MD, DBIM, FALU, FLMI, VP and Chief Medical Director Tim Morant, FSA, MAAA,
Image licensed from Shutterstock The Population is Abusing Drugs, but are Drugs Abusing Insurance? 01/30/2018 Gina C. Guzman, MD, DBIM, FALU, FLMI, VP and Chief Medical Director Tim Morant, FSA, MAAA,
Section I. Short-acting opioid Prior Authorization Criteria
 Request for Prior Authorization for Opioid analgesics Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 Requests for opioid analgesics may be subject to prior authorization
Request for Prior Authorization for Opioid analgesics Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 Requests for opioid analgesics may be subject to prior authorization
AETNA BETTER HEALTH Prior Authorization guideline for Narcotic Analgesic Utilization
 AETNA BETTER HEALTH Prior Authorization guideline for Narcotic Analgesic Utilization Policy applies to all formulary and non-formulary schedules II V opioid narcotics, including tramadol and codeine, as
AETNA BETTER HEALTH Prior Authorization guideline for Narcotic Analgesic Utilization Policy applies to all formulary and non-formulary schedules II V opioid narcotics, including tramadol and codeine, as
Academic Medical School: Implementing Curriculum in Chronic Pain and Opioid Misuse. Jill M Williams, MD
 Academic Medical School: Implementing Curriculum in Chronic Pain and Opioid Misuse Pain, Pain Management and the Opioid Epidemic Symposium Jill M Williams, MD Professor Psychiatry Director, Division Addiction
Academic Medical School: Implementing Curriculum in Chronic Pain and Opioid Misuse Pain, Pain Management and the Opioid Epidemic Symposium Jill M Williams, MD Professor Psychiatry Director, Division Addiction
The Opioid Crisis: Effectiveness of State Responses
 The Opioid Crisis: Effectiveness of State Responses Gordon H. Smith, Esq. Maine Medical Association American Society of Medical Association Counsel Mauna Lani Bay, November 2017 Opioids: the difficult
The Opioid Crisis: Effectiveness of State Responses Gordon H. Smith, Esq. Maine Medical Association American Society of Medical Association Counsel Mauna Lani Bay, November 2017 Opioids: the difficult
Opioid Analgesic Treatment Worksheet
 Opioid Analgesic Treatment Worksheet Aetna Better Health of Louisiana Fax: 1 844 699 2889 www.aetnabetterhealth.com/louisiana/providers/pharmacy LA Legacy Fee for Service (FFS) Medicaid Fax: 1 866 797
Opioid Analgesic Treatment Worksheet Aetna Better Health of Louisiana Fax: 1 844 699 2889 www.aetnabetterhealth.com/louisiana/providers/pharmacy LA Legacy Fee for Service (FFS) Medicaid Fax: 1 866 797
REB CLOSE, MD Community Hospital of the Monterey Peninsula
 REB CLOSE, MD Community Hospital of the Monterey Peninsula The Scope of the Problem 1-5 Opiate use in the US 80% of the world s prescription opiate supply 99% of the world s hydrocodone supply From 1997
REB CLOSE, MD Community Hospital of the Monterey Peninsula The Scope of the Problem 1-5 Opiate use in the US 80% of the world s prescription opiate supply 99% of the world s hydrocodone supply From 1997
Opioid Use: Current Challenges & Clinical Advancements
 Opioid Use: Current Challenges & Clinical Advancements Whitney Bergquist, PharmD, MBA, BCPS Acute Care NPPA Conference February 8, 2017 2017 MFMER slide-1 No Disclosures 2017 MFMER slide-2 Objectives Summarize
Opioid Use: Current Challenges & Clinical Advancements Whitney Bergquist, PharmD, MBA, BCPS Acute Care NPPA Conference February 8, 2017 2017 MFMER slide-1 No Disclosures 2017 MFMER slide-2 Objectives Summarize
Revised 9/30/2016. Primary Care Provider Pain Management Toolkit
 Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Opioid Step Policy. Description. Section: Prescription Drugs Effective Date: April 1, 2018
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Opioid Step Policy Page: 1 of 6 Last Review Date: March 16, 2018 Opioid Step Policy Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Opioid Step Policy Page: 1 of 6 Last Review Date: March 16, 2018 Opioid Step Policy Description
After falls, the leading cause of accidental
 COMMENTARY The National Opioid Epidemic: Local, State, and National Responses Joel M. Prince, MD; William B. Seiden, MD, FACP After falls, the leading cause of accidental death in 2013 among all Wisconsin
COMMENTARY The National Opioid Epidemic: Local, State, and National Responses Joel M. Prince, MD; William B. Seiden, MD, FACP After falls, the leading cause of accidental death in 2013 among all Wisconsin
For female patients only: To the best of my knowledgei am NOT pregnant. Patients Initials:
 Which doctor are you here to see? NAME OF PATIENT: DATE: TO THE PATIENT: As a patient, you have the right to be informed about your condition and the recommended medical or diagnostic procedure or drug
Which doctor are you here to see? NAME OF PATIENT: DATE: TO THE PATIENT: As a patient, you have the right to be informed about your condition and the recommended medical or diagnostic procedure or drug