Community Action Toolkit
|
|
|
- Mervin Spencer Marsh
- 6 years ago
- Views:
Transcription


1 Community Action Toolkit August 2016
2
3 Community Action Toolkit Contents Section 1 Section 2 Section 3 Introduction Community Action Planning and Monitoring CAYAD Projects Using Results Based Accountability Part A: Needs Assessment Part B: Planning your project Part C: Monitoring and Reporting on CAYAD projects Part D: Data Collection Methods Part E: Analysing and Interpreting Data Section 4 Section 5 Section 6 Section 7 Section 8 Section 9 Planning and Monitoring templates CAYAD Media Toolkit Research Evidence Useful to CAYAD work Alcohol and Other Drugs CAYAD Resources and Evaluation Report Summaries Presentation Skills Other Documents/Resources
4
5 Section 1 Introduction
6 Purpose of the Toolkit This Toolkit is a compilation of information and resources developed for CAYAD sites over a number of years. This is a work in progress and is designed to be updated or added to, as new information and needs arise. The CAYAD website provides a lot of information and many reports and resources relevant to CAYAD. This Toolkit is a small but strategically chosen selection of these resources. Any comments, feedback or suggestions for Toolkit content will be gratefully received. s.j.randerson@massey.ac.nz Please August, 2016 The CAYAD National Programme Background The CAYAD programme started in the late 1990s with five sites. In 2016 there were 23 CAYAD sites. The expansion of the programme has been the result of a number of factors: CAYAD practitioners with community credibility, effective community action practice and collaboration at the community level; input, co-ordination and support from the National Co-ordination service; support from CAYAD provider organisations, funders and champions in positions of influence. CAYAD has been fortunate to have been regularly evaluated, and this process and impact data has supported the ongoing resourcing of the programme by the Ministry of Health. There is detailed information on the CAYAD website about the programme and new staff are encouraged to go to Intention and Rationale for CAYAD Programme Health Outcomes Increased community ownership and capability to address alcohol and drug related issues Reduced alcohol and other drug related harm Improved health and wellbeing of New Zealanders CAYAD Programme Outcomes (short to medium term) 1. Increased informed community discussion and debate about issues related to alcohol and other drugs; 2. Effective policies and practices to reduce alcohol and other drug related harm adopted; 3. Increased local capacity to support young people in education, employment and recreation 4. Reduced supply of alcohol and other drugs to young people. Section 1: Introduction Page 2
7 Population Served CAYAD sites serve high need communities in their local region. As a national programme, CAYAD contributes to the following population outcomes: New Zealanders live longer, healthier and more independent lives Maori live longer, healthier and more independent lives New Zealanders have equitable health status In relation to these outcomes, the Ministry of Health monitors specific population indicators: Hazardous drinking score (AUDIT) in past-year drinkers aged 15 years and over Age of onset of alcohol and drug use Rationale It is widely acknowledged that alcohol and other drug use by young people in New Zealand is a major issue impacting the health, education and future employment prospects of young people. The National Drug Policy 2015 to 2020 (Inter-Agency Committee on Drugs, 2015) identifies that the early use of drugs and/or alcohol may interrupt important neurological processes and natural brain maturation, and is a predictor for ongoing problems, including substance use and dependence. One of the key objectives of the National Drug Policy is to delay the uptake of alcohol and other drug use by young people. Over recent years the Government and crown agencies have highlighted the reduction of alcohol and drug related harm in youth as a priority in a number of policy processes: The National Drug Policy 2015 to 2020 The Government s Drivers of Crime initiative (2009) has reducing alcohol related harm as one of four key priorities; The Law Commission s (2010) report Alcohol in Our Lives: Curbing the Harm outlines a range of evidence based strategies to reduce harm from alcohol; The Prime Minister s Youth Mental Health Project 2012 notes that drugs and alcohol play a very important role in youth mental health (New Zealand National Party, 2012); The Prime Minister s Chief Science Advisor, Sir Peter Gluckman s report Improving the Transition: reducing social and psychological in adolescents (2010) calls for stronger measures to restrict access of young people to alcohol and other drugs. The report charts the adverse impact of both alcohol and cannabis on young people s development. The high level of harm and problems associated with youth alcohol and other drug use is strongly supported by New Zealand research evidence. Key findings concerning young people and alcohol include: The Ministry of Health s 2004 Alcohol Use In New Zealand survey (Ministry of Health, 2007) found that 54% of 18 to 24 year old drinkers consume large amounts of alcohol on a typical drinking occasion (more than six drinks for males and more than 4 drinks for females), compared to 25% of the general population. In a study of school students in 2007, 72% of students had tried alcohol and the majority of students (61%) currently drank. About one-third (34%) of students reported they had engaged in binge drinking (5 or more drinks within 4 hours) in the last four weeks (Adolescent Health Research Group, 2008). Section 1: Introduction Page 3
8 A recent national alcohol survey by the SHORE Whariki Research Centre (unpublished) highlighted that since 1999 when the minimum legal purchasing age for alcohol was lowered from 20 to 18, the proportion of young people drinking heavily has sharply increased - particularly for under 18 year olds: Proportion of young people consuming 6+ drinks per occasion by age group: year olds: 14% 25% year olds: 25% 36% 42% year olds: 31% 40% 37% Alcohol consumption by young people is associated with motor vehicle crashes, injuries, deaths, poisonings, crime, violence, mental health problems, sexual risk-taking (Fergusson et al. in Gluckman, 2010), including unsafe and unwanted sex (Adolescent Health Research Group, 2008). Motor vehicle crashes are the leading causes of death among young people. In New Zealand 23% of students reported that at least once during the last month they had been driven by someone who had been drinking (Adolescent Health Research Group, 2008). With regard to addressing alcohol related harm, there is particularly strong evidence of effective policy approaches including increasing excise tax, reducing availability and youth access to alcohol, raising the purchase age, reducing blood alcohol limits and enforcing drink drive laws, restricting or banning alcohol marketing (Babor et al, 2010), and reducing density of liquor outlets (Connor et al, 2010; Huckle et al. 2008). The research evidence supports a community action approach to reducing alcohol related harm (Babor et al, 2010). Key research findings concerning young people and other drug use include: The NZADUS showed that cannabis remains the most widely used illicit drug in New Zealand (Ministry of Health, 2010). By 21 years, about 80% of young people had used cannabis, with 10% developing heavy dependent use (Fergusson et al in Gluckman, 2011) Young people aged years consumed the highest levels of cannabis and are thus most at risk of adverse consequences (Ministry of Health, 2010). One in six past-year users of cannabis reported that their use had an impact on at least one of the following: their financial position; friendships or social life; home life; work, study or employment opportunities; learning difficulties; and legal problems (Ministry of Health, 2010). In reviewing the relationship between cannabis and mental health, Fergusson and Boden found mounting evidence suggesting heavy cannabis users have increased rates of depression, anxiety and suicidal thoughts, with these risks being greater for adolescent users. They also found cannabis use to be associated with increased risks of psychosis/psychotic disorders (Chapter 20, Gluckman, 2010). Brain injury research has shown that frequent heavy users of cannabis experienced marked changes in brain functioning and neuropsychological performance (Gonzalez, 2007). A New Zealand Study of adolescents who used cannabis more than once a week reported significantly Section 1: Introduction Page 4
9 poorer performance on four measures of cognitive function reflecting attention, spatial working memory and learning. (Harvey at al., 2007). A recent New Zealand case control study reports that long term use of cannabis increases the risk of lung cancer in young adults. The risk of lung cancer increased nearly six times in the onethird of young people who smoked most heavily (Aldington, Cox, Beazley et al., 2008). Cannabis continues to be easy or very easy to obtain, as reported by frequent drug users (Wilkins et al., 2011). Particularly in some rural communities in New Zealand, cannabis use is endemic and is supported by a green economy where cannabis is cultivated as a cash crop to provide a primary or supplementary income. Regarding harder drugs, the 2007/08 NZADUS indicated 2.6% of the population used Ecstasy in the past year, and 2.1% used amphetamines other than Ecstasy (including P, meth, ice speed ). Use of both types of drugs was highest in 18 to 24 year olds (Ministry of Health, 2010). Both Ecstasy and Methamphetamine were reported as easy or very easy to obtain by frequent drug users in Auckland, Wellington and Christchurch (Illicit Drug Monitoring System report, Wilkins et al., 2011). Notably the use of Ecstasy continues to increase in NZ (Wilkins et al., 2011). There is an entrenched market for methamphetamine in New Zealand, although use by young people under 20 is not common (Wilkins et al., 2011). The 2007/08 NZADUS indicated that 30% of people who had used amphetamines in their lifetime reported they had experienced a harmful effect from their usage. The most common harmful effects were on friendships and social life (22.5%), home life (20.0%) and financial position (17.1%) (Ministry of Health, 2010). Section 1: Introduction Page 5

10 A public health approach Public health promotes and protects the health of people and the communities where they live, learn, work and play. It focuses on entire populations rather than individuals. These populations can be as small as a local community or as big as an entire country or region of the world. CAYAD aims to introduce prevention measures that will be of benefit to the whole community. In public health the impact on the health of people most at risk of harm is just as important as how wide the effect will be for the whole population. The triangle below shows the focus of CAYAD activities for the whole population, for those at risk and for people already affected by the problem: An example of a population approach at a national level is the recent lowering of the drink driving (blood alcohol) limits. This led to immediate reductions in alcohol consumption. A few years ago, the zero-alcohol limit for youth led to immediate reductions of close to 50% in both drink driving and crashes amongst young people. The evidence for this solution has been clear for many years, but public pressure was important to ensuring the issue also became a priority for the government. So in CAYAD, we have a responsibility to raise community awareness of solutions that have strong supporting evidence, and to help the public generate well-informed submissions that will support effective policy change. We also need to take a population-focused approach in our local communities. You might start with the main places where larger numbers of people in the community get together, like local sports clubs and sports fields. What could be done there to minimise the exposure of young people to excessive drinking and drug Section 1: Introduction Page 6
11 taking? Could more effort go into providing good kai, games and competitions that make it a more familycentred place, and less drinking-centred? Could the families and parents agree not to give drinks to anyone under 18? Later at night, how could you minimise harm? Could there be a roster of sober drivers and a van to get people safely home? Public health organisations Each District Health Board has a Public Health Unit responsible for a large share of public health activity. In addition more than 200 non-government organisations (NGOs) that receive health funding. These providers include: Public health organisations that provide public health services for the general population Maori governed and managed services that provide public health services specifically for Maori or for the general population Pacific governed and managed services that provide public health services for Pacific people What does the public health sector do? The public health sector ensures that potential risks to the health of the population are monitored, managed and promoted by: Health protection - largely led by Public Health Units Monitoring our environment to ensure risks to the health of the public are managed Licensing organisations and premises as required by regulation Enforcing public health legislation, including investigating complaints and taking appropriate action Planning for emergencies, so that if one does happen things can swing into action without delay to protect community health Providing environmental advice for the Government and local bodies on an as required basis Advocating for health policy change at national, regional and local levels Being involved in policy development at national, regional and local levels Raising public awareness of health issues Developing and managing population-based screening programmes Health Promotion Working with communities and the wider health sector to develop and establish public health programmes Assisting schools with the implementation of the Health and Physical Education curriculum and the development of a health promoting environment Working with the media on public health issues interviews, press releases, talk-back radio programmes Advocating for policy change at national, regional and local levels Promoting the development of physical and social environments that will support good health Developing and distributing resources pamphlets, posters, videos, newsletters, teaching kits, interactive websites Training professionals, community workers and educators Section 1: Introduction Page 7
12 Section 1: Introduction Page 8
13 Section 2 Community Action
14 A Community Action Approach To reduce harms from alcohol and other drugs, CAYAD uses a community action approach to engage communities in addressing the conditions and environments in which young people live that increase the risk of their harmful use of alcohol and other drugs. This includes addressing local and other policies and practices, supporting community action to reduce supply of alcohol and other drugs, and facilitating community and system level changes that expand positive opportunities for young people. Evidence on reducing harm from both alcohol and other drugs highlights the importance of multicomponent strategies and utilising a community action approach. There is good evidence to support effectiveness of community action on alcohol (Babor et al 2010). There is also emerging evidence on community action on illegal drugs. A recent international review found that broad based, theory-driven community-based programmes can delay initiation of both alcohol and drug use by young people, as well as having wider positive effects beyond drug and alcohol use. 1 While there is limited research on community action on illicit drugs, key authors in the field assert that the findings from research on community action on alcohol and tobacco can be applied to other drugs 2 Community Action In developing strategies and activities for community action it is vital that all CAYAD staff are familiar with a community action approach. In addition, planning must ensure that CAYAD projects: target systemic change in policies, environments, structures, systems and/or practices are sustained over time have a specific focus (e.g. on alcohol and other drugs) draw on evidence combining research, cultural evidence and local evidence from communities are well coordinated, including outcomes plans, action-reflection and evaluation are collaborative involving selected strategic partners across multiple levels and sectors. 1 Drugs and Public Policy Group Miller et al 2009, Holder Section 2: Community Action Page 10
15 Key Elements of Effective Community Action Engages selected organisations and stakeholders who work together on the issue/project Emphasis is on changing underlying organisational policies, practices, social norms Focus on changing structures and systems means that change can be sustained without on-going effort by stakeholders Is guided by and largely limited to activities/ strategies based on research evidence, local and cultural knowledge Implementation is based on best practice but allows for innovation Specific measurable research based outcomes May focus on a geographic community or communities of interest Encourages engagement in political processes so issue is on policy agenda Focus is on specific issue (e.g. illicit drugs) and problem often defined by government department/ funder A paid co-ordinator specific to the project is important to sustainability and effectiveness A plan of action with short and long term outcomes formally monitored and evaluated On-going research evidence contributed to the project e.g. action research/ formative evaluation A multi-component approach is needed to reduce drug related harm to young people. A focus on only one or two areas of activity (e.g. sport or youth development) does not constitute effective community action 3. The range of strategies used for effective community action includes: Building effective partnerships amongst selected key stakeholders to ensure sustainability of CAYAD supported strategies Supporting community participation in local Council alcohol plans Supporting communities to make submissions on national alcohol and other drug policy Supporting local communities to develop effective alcohol and other drug policies and practice e.g. sports clubs, marae, schools, workplaces etc.; Advocating for community-based policies and initiatives that promote belonging/connecting opportunities for young people Encouraging development of appropriate support systems and youth development initiatives for Maori and non-maori youth Raising awareness of the need for school and community based early intervention for young people experiencing alcohol or other drug related harm Fostering inter-sectoral approaches involving health, education, police and social services to reduce youth alcohol and drug-related harm and manage incidents 3 Greenaway and Witten (2006) Section 2: Community Action Page 11
16 Mobilising resources so that communities and whanau are supported to facilitate their own learning, discovery and action based responses. Publicising of positive achievements by local communities, including young people Organising mass media coverage of community strategies to reduce drug related harm and promote the wellbeing of young people Advocating with education and industry stakeholders for increased, relevant employment and training opportunities for young people Supporting communities who choose to explore economic development opportunities Advocating for diversion and community sentencing programmes for young people involved in illicit drug offences. Ministry of Health requirements for CAYAD sites Needs Assessment Sites will assess community needs periodically and consult with appropriate stakeholders to identify issues for the community in relation to alcohol and other drugs and the harms they cause. CAYAD projects will be informed by the results of the needs assessment and will focus on a range of projects that address both alcohol and other drug related issues. Action Plan Sites will develop a 12 month action plan on the CAYAD Action Plan template provided by the Ministry of Health that specifies what activities will be undertaken for the CAYAD projects and where these activities align to National CAYAD RBA Activities. Reference Group A Reference Group made up of representatives of key stakeholder groups will meet quarterly to provide support and guidance to assist the CAYAD staff in leading the project. Reference Group membership should be identified by CAYAD coordinators in consultation with their manager. Community Action Fund The CAYAD community action fund (CAF) of $5,000 per contracted FTE per annum will be allocated as per the provider s CAF policy to priority community action projects that are clearly linked to the CAYAD objectives. The CAYAD Co-ordinator/s should be enabled to easily access this funding to support CAYAD activities Evaluation Sites will undertake regular evaluative activities to reflect on and improve the effectiveness of the projects. National Coordination CAYAD sites provide one representative per region for the National CAYAD Advisory Group (NCAG), to help support regional and national co-ordination, capability and networking. CAYAD managers and staff engage constructively with the CAYAD National Co-ordination Team (NCT) and National CAYAD Advisory Group (NCAG) representatives. August, 2016 Section 2: Community Action Page 12
17 Section 3 Planning and Monitoring CAYAD Projects Using Results Based Accountability
18 SECTION 3: Planning and Monitoring CAYAD Projects Using Results Based Accountability Part A: Needs Assessment Part B: Planning your project Part C: Monitoring and Reporting on CAYAD Projects Part D: Data Collection Methods Part E: Analysing and interpreting data Appendix A: National CAYAD Measures Appendix B: Evaluation in New Zealand Appendix C: Evaluation standards Section 3: Planning and monitoring CAYAD projects using RBA Page 14
19 Part A: Needs Assessment Purpose This is undertaken to help build a picture of your community, identify any specific issues and priorities (both general and drug-related (including alcohol) that will contribute to informing your project of priorities and potential strategies. This should help provide direction for your Action plan. It can also help build networks and awareness-raising of your project. It should look not just at needs and gaps but also strengths and community visions for the future. Feeding the information back to the community for discussion in a community forum/workshop and/or report will also help mobilise local community support and action on specific initiatives. Avoid paralysis by analysis! You don t need a long and technical research project detailing exact statistics on every type of drug harm; the aim is to identify the known issues that are priorities for the community and move into action on these. It helps to have a short time limit (e.g. 2 months). Step 1: Describe your local community context Develop a brief background history of the area and any unique or special characteristics (often included in local Council reports ask your local librarian). Also include key demographic information (ethnicity, income, employment, education levels, (usually available from your local City/District Council or Stats NZ website. Step 2: Identify CAYAD specific issues and opportunities Using the questions below, interview your reference group (or try the Post Box activity with them; see next page) and other key staff in local organisations i.e. school principal/school guidance counsellor, youth and DHB public health workers, iwi services, marae, social services, police, local clubs and licensing inspectors. Alcohol and other drugs - key questions: 1. What alcohol and other drug related harms are having the biggest impact on wellbeing in your area? 2. Who is being affected? Who is suffering the most harm? What is happening for more vulnerable people/communities? 3. Why? What local factors are contributing most to the problems? 4. Strengths: What local factors are protecting young people from harm from alcohol and other drugs? 5. Policies: Ask key organisations such as schools, marae, clubs, police, (even major employers) about their policies and practices regarding drugs and alcohol. Section 3: Planning and monitoring CAYAD projects using RBA Page 15
20 Include additional information/data where easily available: o Local police data on drug and alcohol apprehensions o Local school data on drug suspension/stand-downs, or truancy data o Local alcohol and drug service/mental health service general information re young people seen issues o Recent media (over last year or so) items re important community issues relating to young people, especially with regard to alcohol and drugs o Use national surveys to get a general indication of what percentage of people are using drugs/alcohol and levels of problems experienced but put it alongside local knowledge and issues for discussion of how it fits the local picture. Education, employment and recreation key questions: 1. What are the needs for young people in education, employment and recreation? 2. Who is most at risk of poor outcomes in education, employment or recreation? 3. Why? In what circumstances are they having difficulty or disengaging? What opportunities or activities are lacking? 4. Strengths: When are people staying engaged and succeeding? What factors are supporting them to achieve? 5. Policies: Ask key organisations such as local councils, iwi organisations and youth networks what policies or strategies they have to support young people to succeed. Include additional information/data where easily available: o Any relevant reports or plans available from local Councils, Safer Community Councils on youth strategies, employment, crime, education, or numbers of young people not in school or training. o Stock-take of local services and amenities for young people (eg social/helping agencies, health, educational, recreation) o Informal simple surveys at public events/shopping centres asking young people questions such as: What do you like about living here? What s not so good about living here? What would make it better? Step 3: Deciding: What will you work on? Your needs assessment could find several competing issues or opportunities to be addressed. To help you and your stakeholders decide where to begin, you can: 1. Ask your stakeholders which issues (and opportunities) are most important A short survey is a good way to ensure the priorities of each of your stakeholders are heard. List the key issues and ask your stakeholders to each rank each as high, medium or low. Repeat the exercise for the opportunities. The results can be discussed as a group. Section 3: Planning and monitoring CAYAD projects using RBA Page 16
21 2. For each priority relevant to CAYAD, ask: o Will it make the community significantly better off (especially young and vulnerable people), if this priority is successfully addressed? o Is it a high priority for your community and stakeholders? o Is it practical to address this priority with the resources you (and your stakeholders) have? This will help you either make a decision, or confirm that first you need to find further information about the issues raised. Post Box Exercise This tool is a creative and fast way to identify local needs and to decide on priorities: 1) Develop three to five key questions 2) Post the questions around the room or use a data projector 3) Hand each participant post it notes one post it for each question 4) Ask them to write their answers to each question 5) Tell participants to post their answers beside each question 6) Divide participants into as many groups as there are questions 7) Participants then collate the answers and present them on a large sheet of paper in a visual format 8) Share findings with the whole group. Section 3: Planning and monitoring CAYAD projects using RBA Page 17
22 Part B: Planning your project The Results Based Accountability method of planning a project, developed by Mark Friedman, involves seven simple questions. This guide to planning your project will help you answer each of these questions and to develop your action plan. Seven performance accountability questions - RBA Q1. Who are our clients? (Customers/Client groups) Q2. How can we measure if our clients are better off? (Customer/Client results) Q3. How can we measure if we are delivering services well? (quality measures) Q4. How are we doing on the most important of these measures (Baseline Data and Story) Q5. Who are the partners that have a role to play in doing better? (Partners) Q6. What works to do better including no-cost and low-cost ideas? (What works) Q7. What do we propose to do? (Action Plan) For CAYAD, we recommend developing an overview of your project at the start. This helps you to explain in brief the nature of your project and what you are aiming to achieve. Project Description Answer these questions to describe your project s objective, which you can enter directly into your CAYAD Action Plan: Project Title 1. Who is the project designed to reach (target group)? 2. What need, issue or concern does your project address? 3. How will your target group be better off as a result of your project? Section 3: Planning and monitoring CAYAD projects using RBA Page 18
23 Example Project Objective: This project is for.. It is designed to address the issue of. As a result of this project. Identify relevant or influential stakeholders With a community action approach it is important to strategically select your key stakeholders. CAYAD sites seldom have the capacity to work with everyone in their communities, so giving thought to the key influencers and major stakeholders is essential. Stakeholders may be: those that can best influence a positive outcome for the project those served by the project those involved in the implementation of the project intended users of the evaluation findings such as policy makers, funding agencies, community groups, other health and social services Section 3: Planning and monitoring CAYAD projects using RBA Page 19
24 Stakeholders for your CAYAD Reference Group or project CAYAD projects work best when they involve people who can bring wide-reaching changes to communities. These might be changes to systems (like youth justice systems) or community institutions (like schools, marae, sports clubs). CAYAD reference groups need to involve the right people, who work in areas that our projects are targeting. We need to keep them engaged and use their strengths, networks and influence to help our projects move forward. Facilitation of the reference group by CAYAD can also strengthen relationships and action between the stakeholder organisations. The activity below will help you assess whether you have the people you need on your reference group or supporting your CAYAD projects. Activity: Identifying Stakeholders Different people can help with different things. To achieve CAYAD outcomes, list the key stakeholders you need for: Advocacy: Who can effectively promote the actions/changes needed at different levels? (e.g. politically, or within local networks/organisations) Delivery: Who can access the people or resources needed to deliver project activities? Positive publicity: Who can put your projects in the spotlight, and increase a project s credibility? Ongoing support: Who can fund/authorise or continue /expand your projects? Section 3: Planning and monitoring CAYAD projects using RBA Page 20
25 Identify environmental and contextual factors Environmental and contextual factors can also impact on the success of your project. Often there is little or no control over these factors. These can be local or national/regional. Local factors may include: Similar initiatives sponsored by other agencies Social norms & conditions that either support or hinder the achievement of outcomes e.g. local attitudes, policies or practices Regional/national factors may include: Government policies that support or hinder your activities Socioeconomic factors of target population Motivations and behaviour of target population You will also have beliefs/assumptions about the way you think your project will work. Some examples of assumptions are: Funding will be secure throughout the project Because we teach information, it will be adopted and used in the way we intended. People will be motivated to attend training sessions Staff with the necessary skills and abilities can be recruited and trained Partnerships can effectively address concerns or reach into areas we cannot Policy adoption leads to behaviour change. Remember, inaccurate or overlooked assumptions could be a reason that your project did not achieve the expected level of success. Section 3: Planning and monitoring CAYAD projects using RBA Page 21
26 Developing project actions: The questions below are essential to developing a set of effective actions to achieve your project objective, and ensuring the right people or groups are involved. 1. What is the story behind the issue? What is causing it? 2. Partners: Who are the partners who could support the development or delivery of the project to achieve its objectives? 3. What works to address this issue, including no-cost or low-cost ideas? (Common sense ideas and research where available)? Question 3 is essential because evidence needs to inform your ideas about the way in which your programme will work. You need to consider the following: Theoretical knowledge from prior research Effectiveness of an existing programme Local knowledge Cultural knowledge Expert knowledge Developing project actions What is the story behind the issue? What is causing it? Partners: Who are the partners who could support the development or delivery of the project? What works to address this issue, including nocost or low-cost ideas? (Common sense ideas and research where available) What do you propose to do? (Action Plan) Tip: Your partners can help you to answer this question, or you may need a plan for gathering further evidence or information. List the key actions you will take to achieve your objective* Section 3: Planning and monitoring CAYAD projects using RBA Page 22
27 *Make sure you consider actions that address the key elements of the Community Action method. Will your project activities: o o o o o o target systemic change in policies, environments, structures, systems and/or practices? focus on specific results that support CAYAD outcomes? focus on a change that can be sustained over time? draw on evidence combining research, cultural evidence and local evidence from communities? include plans for action-reflection and review? Involve collaboration with selected strategic partners, across multiple levels or sectors, and/or does it mobilise the community? ACTIVITY: Transfer the main actions to your CAYAD Action Plan. Try to keep them in a chronological order, to show your step-by-step process. Section 3: Planning and monitoring CAYAD projects using RBA Page 23
28 Part C: Monitoring and Reporting on CAYAD Projects 1. Introduction Purpose There are three fundamental reasons for using RBA and other methods to develop and monitor CAYAD projects: (1) To ensure our activities are clearly aligned to relevant results. (2) To monitor how well our projects are working in order to decide whether or not a project should be continued, expanded, dropped, or improved. (3) To report our efforts and results to the Ministry of Health. RBA Reporting CAYAD sites submit a report on their projects every six months using the RBA process. The RBA report helps us to understand three things: o how much work we are doing (effort) o how well we are doing that work (quality) o whether our effort is helping us to achieve our intended results (impact). RBA is a simple method of reporting, because it focuses on recording just a few carefully selected numbers about your project (quantitative results). Only the most relevant measures of effort, quality and impact are selected. These measures (sometimes called indicators) are like lights on a car dashboard. This is useful for CAYAD providers and for reporting to the Ministry of Health because it: o gives a clear picture nationally of the kind of activities CAYAD is undertaking and the results we are achieving o reduces the need for lengthy written reports o clearly highlights the types of activities and results CAYAD coordinators are accountable for in performing their roles. These quantitative RBA measures are limited because they do not say anything about results or changes which don t fit within the specific CAYAD National Measures. This is why your report also asks for a short complimentary narrative, where you can briefly list other results or downstream changes that have resulted from your project. For instance, after an alcohol and drug policy was introduced in the local sports club, example downstream effects could be a shift in drinking practices in the local community outside the club environment, or improvements in whanau relationships. Project Monitoring If your RBA indicators show your projects aren t going as expected, the RBA approach asks you to work with your stakeholders to investigate why and what could be done to improve the project. A bit like an engine light coming on in a car telling you that it s time to take it to a garage for a closer look under the bonnet. Section 3: Planning and monitoring CAYAD projects using RBA Page 24
29 In CAYAD we are encouraged to try new activities, and so it is also important to look closer at your projects when they are going well, to see what we have learned from trying things out. Is the new approach better than what we had before, and how will we know? Is it better than other options we might have chosen? This involves regular review of your projects, and gathering data from various sources, and making judgements about your project. This practice is called evaluation, and so some tools and principles important to evaluation are included in this manual. 2. Evaluation Both the RBA process and other methods of evaluation start from the moment you begin planning your project and deciding on your actions, rather than when you look at how effective or successful a project has been. For more detailed information about evaluation practice in a New Zealand context, and evaluation standards, see Appendices B and C. Evaluation Ethics Working in community action involves interacting with a range of groups and individuals to develop, implement and evaluate projects. This work requires good ethical practice based on the following ethical principles: Show respect for others Minimise possible harm Informed and voluntary consent Show respect for privacy and confidentiality Research adequacy Avoid deception Avoid conflict of interest Ensure social and cultural sensitivity to age, gender, culture, religion, social class of participants Promote social justice Provide feedback to participants While programme evaluation is generally viewed as a low-risk activity these ethical principles still apply. Ethical review, when necessary, is conducted by institutional ethics committees and Health and Disability Ethics Committees ( that have been established to review research and evaluation. Ethical scrutiny should be proportional to the level of risk of the activity. For example, participants must be fully informed of the purpose of the evaluation, what is expected of them and their rights. Their consent must be gained and findings need to be made accessible to participants. It is also important that you discuss with colleagues, Section 3: Planning and monitoring CAYAD projects using RBA Page 25
30 managers or the National Coordination Team possible ethical issues/concerns at the start of your project. Remember, good ethical evaluation practice: Promotes evaluation Develops trust in the quality of information gathered soundness of evaluative conclusions Increases potential of evaluation to make a positive contribution to programme improvement. Ethical Questions When planning an evaluation the following ethical questions need to be considered: Who has helped to define the evaluation question(s)? Who will benefit? Who will gain knowledge? Is it relevant? Who says so? Are there clearly defined objectives and an appropriate evaluation design to meet the objectives? Who is the evaluator or researcher accountable to? Does this create any conflicts of interest? What parts of the evaluation can I safely conduct myself? What evaluation activities will need to be completed by someone else? Informed consent? How have the participants been prepared? Information provided, opportunity to ask questions? What s in it for participants? How will any sensitive or confidentially information gathered be protected? In the alcohol and other drug sector, you should establish how you will manage information you may be given about illegal activity. Helpful Hints Questions you should ask yourself when making an ethical decision: Have I discussed this with my colleagues, managers or the National Coordination Team? Is it legal? Is it safe? Is it the right thing to do? Will this stand the test of public/community scrutiny? If something terrible were to happen, could I defend my actions? Is it balanced and fair? How will it make me feel about myself? Does this choice lead to the greatest good for the greatest number? Have I incorporated expert advice (eg in questionnaire design) to ensure my evaluation questions and methods will enable high quality data that can increase knowledge? Section 3: Planning and monitoring CAYAD projects using RBA Page 26
 Q2. How can we measure if our clients are better off? (Customer/Client results) Q3. How can we measure if we are delivering services well?")
 Q7. What do we propose to do?")
31 3. CAYAD Reporting and Monitoring Process The CAYAD reporting process is based on the RBA 7 questions approach to performance accountability: Seven performance accountability questions - RBA Q1. Who are our clients? (Customers/Client groups) Q2. How can we measure if our clients are better off? (Customer/Client results) Q3. How can we measure if we are delivering services well? (quality measures) Q4. How are we doing on the most important of these measures (Baseline Data and Story) Q5. Who are the partners that have a role to play in doing better? (Partners) Q6. What works to do better including no-cost and low-cost ideas? (What works) Q7. What do we propose to do? (Action Plan) Fortunately for us, the National CAYAD Measures (Appendix A) define what we need to measure for our projects, including the types of clients we focus on (Q1), and what our performance measures are (Q2 and Q3). Step 1: Choose your measures Look at each action in your plan and choose which of the National CAYAD Measures it aligns with. Remember, not every action needs to align with one of the measures. If there are other activities or results your stakeholders value very highly, you may include those also (see step 2 below). ACTIVITY: Take out the National CAYAD Measures handout and your CAYAD Action Plan. In the Action Plan, complete the Aligned national CAYAD activity column next to each action. Section 3: Planning and monitoring CAYAD projects using RBA Page 27
32 Step 2: What does being better off look like? For projects aligned with National CAYAD Measure Two, you will need to report how many of the project s intended outcomes were achieved. In order to do this, the project group must clearly define two things firstly, what the intended outcomes are; and secondly, the point at which you would all agree that the outcomes have been achieved. The table below will help you clarify your outcomes, define what success looks like, and what data you will need to collect to provide evidence that the project is successful. Working with your stakeholders can help you clearly define what success looks like to them (the middle box). Try to describe practical changes that you will be able to see or measure in some way. Ask if all the changes need to have happened for the main outcome to be achieved, or only some of them? Outcome What success looks like How you will find out (Data collection method) Example: A family friendly environment in the rugby club Less intoxication More meals and non-alcoholic drinks being purchased Kuia and kaumatua attending Parents and children spending time together Observation Manager report/accounts Step 3: Monitoring your project and collecting data During the year, you will need to collect data about your activities at regular intervals: Answer Q4: How well is the project doing on the National CAYAD measures? Gather data on each measure (see guide to different methods in Part D, and detail on analysing any survey data or percentages in Part E, page 44). Gather data for any additional measures you developed with your stakeholders. Review the results with your project group. Work out the story behind the results by talking to key people from the project and reviewing project data or reports. Reflect: Is improvement or change needed? Or more investigation? Section 3: Planning and monitoring CAYAD projects using RBA Page 28

33 ACTIVITY: In your Action Plan, for each action that is aligned with a National CAYAD Measure, complete the data collection method column. Focus on you how you will gather data for the How well measures and the Is anyone better off measures. How will you collect the information? How often will you need to collect it? (for instance, to track changes over time) Try a new tool: Appreciative Inquiry is a helpful tool for monitoring and improving your project. It uses a few simple questions (see page 18) that you can work through with your stakeholders or project team on a regular basis. Step 4: Take action Record the results in your CAYAD report template. Work through the RBA questions 5 to 7: Q5. Who are the partners that have a role to play in doing better? Q6. What works to do better including no-cost and low-cost ideas? Q7. What do we propose to do? Add any new actions to your Action Plan and/or revise the previous activities. Alternatively, if the project is no longer worth pursuing, you may exit the project. Step 5: Deeper Evaluation Using additional methods to evaluate your project can provide a fuller understanding of the benefits of your project and the challenges it encountered. This can help with: identifying ways to improve the project describing other results produced by your project, to include in the complimentary narrative boxes in your CAYAD report making decisions on whether to continue, stop or expand a project identifying key learning to share with others, including funders, community members or other CAYAD sites. Two creative ways to monitor progress towards achieving outcomes are Appreciative Inquiry and the Most Significant Change Technique. These are outlined below. Section 3: Planning and monitoring CAYAD projects using RBA Page 29
34 Appreciative Inquiry The Appreciative Inquiry Process (AI) developed by David Cooperider is a creative way to review, reflect, design and implement initiatives using a positive approach. The whakatauki Me hoki whakamuri, kia ahu whakamua, kaneke looking backwards to the future - we must reflect back to what has been in order to improve, evolve and move forward - fits with the discovery phase of AI. The 4D Appreciative Inquiry Model Using the 4D model can help reflect on and monitor your current CAYAD work as well as imagining or dreaming what else can be achieved. Discover: What are the images and activities at play when your CAYAD work is at its best? Dream: What might be possible with respect to our CAYAD work if we were to imagine a future, ideal community? Design: What are the most compelling actionable ideas and how might we put them into use? Destiny: What will we actually do to bring about the change we envision? How will we track and monitor our progress? Section 3: Planning and monitoring CAYAD projects using RBA Page 30
 stories can be used to describe programme experiences, perceptions and outcomes. Programme participants make sense of the events/experiences after they have happened.")
35 Most Significant Change Technique (Dart, J. 2008) To access the Most Significant Change Technique Manual go to: Most Significant Change (MSC) stories can be used to describe programme experiences, perceptions and outcomes. Programme participants make sense of the events/experiences after they have happened. MSC stories do not stand alone, but contribute to the overall evaluation by providing narratives in participants voices that illustrate change. A ranking and discussion process enables the most significant stories to be selected, what the stories demonstrate and what meanings they hold. The purpose There are several reasons why a wide range of organisations have found MSC monitoring very useful and these include the following. 1. It is a good means of identifying unexpected changes. 2. It is a good way to clearly identify the values that prevail in an organisation and to have a practical discussion about which values are the most important. This happens when people think through and discuss which of the SCs is the most significant. This can happen at all levels of the organisation. 3. It is a participatory form of monitoring that requires no special professional skills. Compared to other monitoring approaches, it is easy to communicate across cultures. There is no need to explain what an indicator is. Everyone can tell stories about events they think were important. 4. It encourages analysis as well as data collection because people have to explain why they believe one change is more important than another. 5. It can build staff capacity in analysing data and describing impact. Section 3: Planning and monitoring CAYAD projects using RBA Page 31
36 6. It can deliver a rich picture of what is happening, rather than an overly simplified picture where organisational, social and economic developments are reduced to a single number. 7. It can be used to monitor and evaluate bottom-up initiatives that do not have predefined outcomes against which to evaluate. Why stories? People tell stories naturally People remember stories Stories can carry difficult messages Stories provide a rich picture Stories provide a basis for discussion MSC stories can help: Identify unexpected changes Capture the voice of those the project is targeting (the participants) Analyse data Facilitate stakeholder engagement Encourage reflection MSC steps You will need to think about stories that will show the changes/differences/impacts that your project has had at whatever level (individuals, community, policy) Your action plan will show the interventions and changes (outcomes) you expect your programme to achieve these are the domains of change which can be: o Changes in the quality of people s lives o Changes in the nature of people s participation in activities o Changes in the sustainability of people s organisations and activities o Any other changes Once you have identified the domains of change, the next step is to decide how often you will collect MSC stories (once a month, three monthly, six monthly). Usually at the start of a new project you would collect stories every month for the first few months and then spread the collection of stories out. It all depends on the length of time you have allocated for your project. Now you are ready to go out and collect MSC stories. It is fairly standard to start with one open-ended question: Looking back over the last month, what do you think was the most significant change that resulted from the CAYAD activities in your community and why is this significant to you? Section 3: Planning and monitoring CAYAD projects using RBA Page 32
37 Once you have collected the MSC stories it is time to begin the analysis. Everybody (key stakeholders, programme staff) reads the stories and assigns stories to domains of change. Then there is an in-depth discussion about which story/ or story to choose in each domain that represents the most significant story of all. It is important to let people who have provided stories know about the process and which story/stories were selected as most significant and why. Keep all stories on record as you may want to do quantify how many stories focused on a similar theme. This can be useful if you have collected a lot of stories. Ethical considerations It is important to get informed consent from story tellers and you need to let them know how the story will be used and whether they want to be named or not. You may also need to consult with others involved in the story to obtain their consent. If children under the age of 16 years are involved you will also need to get parental consent. ACTIVITY: Telling and selecting MSC stories 1. Turn to your neighbour and ask them: What was the most significant change that took place in your CAYAD work this week/month (get the details) 2. Then ask them why they thought this was the most significant. 3. Write down: the story (who, what, where, when) explanation (why is it significant) who documented the story (name, position location, date) 4. Then let your neighbour ask the same questions to you. 5. Come to a decision about which of the two stories you think is most significant, and identify why you both think so. You may have a number of reasons. 6. When asked to, tell a group of eight people the story you chose, and why you did so 7. In your group of eight, decide which of the four stories you think is most interesting, and identify why you all think so. You may have a number of reasons. 8. When asked to, tell the large group people the story you chose, and why you did so. Section 3: Planning and monitoring CAYAD projects using RBA Page 33
38 Part D: Data Collection Methods Introduction Knowing the sorts of information that you need to find out helps you decide what data collection methods you will use. Each method will have a cost for you and often for your stakeholders, so before starting anything you must consider: What questions do you want to answer? What information do you already have? What information do you need? What information gathering techniques would best suit your target audience? (ethically and culturally) Time available to gather information? Who will gather this information, analyse and report it? Here are some general points about quantitative and qualitative methods. Quantitative Methods Qualitative methods find out the numbers of people who did something or thought something quantitative tools have closed questions use a structured format usually have a large number of respondents use numbers and are statistically based can make generalisations to wider group can statistically measure outcomes from a programme or intervention and track changes overtime generally need experts to help used to gain in depth understanding of people s feelings, beliefs and experiences of something use a structured or semi-structured format questions are open-ended usually talk to a smaller number of people but in more depth allows the voices of a range of different groups to be heard can track changes over time requires expertise to develop methods, questions and analyse data Mixed methods Most evaluations include a mix of data collection methods. The use of mixed methods can provide richer data with each of the methods giving you different pictures of the way in which a project operates in practice. When the results from two or three methods are the Section 3: Planning and monitoring CAYAD projects using RBA Page 34
39 same or similar we can be more certain of the findings (Greene, Benjamin, & Goodyear, 2001). As indicated in the table below, a typical design might begin with a qualitative component such as a focus group discussion to inform the evaluator as to issues that could then be further explored in a survey of programme participants. This could then be followed by indepth interviews to clarify some of the survey findings. Methodology: Qualitative Quantitative Qualitative Data collection approach: Exploratory focus Survey Personal Group Interview Helpful Tips There are multiple ways of collecting data and information each with strengths and weaknesses. More detail is given on this in the following section. Mix and match according to the needs of your project (NOT just to your preferences or skills get help if you need it) (Davidson 2003). It s often difficult to establish causal links because there are so many other factors that can influence whether or not outcomes are achieved and whether outcomes are directly related to the programme. This means that you need to be careful about the claims you make about your evaluation findings. Section 3: Planning and monitoring CAYAD projects using RBA Page 35
40 Guidelines for Gathering Data Using Key Informant Interviews, Focus Groups, Feedback Forms and Observation (Partly adapted from Zimmerman, Hurtig & Small (2001). Tools of the Trade: A CWIT guide to participatory evaluation. Center for Research on Women and Gender. Chicago: University of Illinois) Four methods Four information collecting methods are described below. These are key informant interviews, focus groups, feedback forms, and observation. Key informant interview These are one-on-one interviews with opinion leaders or stakeholders - people who know about a particular area that you are trying to find out about. Key informants can be someone who is of a particular rank or position, e.g. head of a trade union or head of the chamber of commerce; they can be people who are informed on a topic because of the work that they do, e.g. people who work with women who experience domestic violence will know about domestic violence in the community; or they can be people who have views on a topic because of their experience, e.g. women who work in factories will have knowledge on what working conditions are like in factories. Key informant interviews are generally carried out fact-to-face. The interviewer usually asks open ended questions that allow the respondents to answer in their own words with the interviewer clarifying unclear responses and probing for details. Benefits of key informant interviews Individual comments are not affected by what other people say because they are conducted in a one on one situation People are able to talk about intimate and personal things relevant to the programme that can aid programme implementation and development Key people with particular skills, roles or knowledge are given an opportunity to talk about their perceptions of a particular issue or topic Some drawbacks of stakeholder interviews Some people may be intimidated or feel uncomfortable being interviewed in a oneto-one situation When conducted face-to-face, these interviews can involve a lot of time in travelling Focus groups This is when a number of people are brought together to talk about a particular issue. Openended questions are asked to encourage discussion among participants on a specific issue. A facilitator takes responsibility for making sure that specific topic areas are covered during discussions and that a group process of open discussion occurs. The specific characteristics of focus groups, such as numbers of people participating and length of discussion, can vary. Section 3: Planning and monitoring CAYAD projects using RBA Page 36
41 Five to eight is a common number of people to participate in a one and a half hour discussion. Benefits of focus groups Can enable you to elicit in-depth information and to explore issues Provide a forum where people can discuss their thoughts, feelings and experiences in an interactive way by meeting in groups Provide insights into what and how people feel about specific issues Some drawbacks of focus groups Are open to peer and social pressure Require a high level of group facilitation skills Can be more involved than individual interviews to analyse What will you need to do a focus group? A quiet place that people will feel welcomed and comfortable Comfortable chairs placed in a circle A tape-recorder and microphone if you decide to record the discussion. Position these on a low table in the centre of the circle Refreshments Name tags it is important that the facilitator knows each person s name so that they can bring them into the conversation easily Questions. This is called an interview schedule. It sets out the topic areas, and/or question-types that you need to cover. The order that the questions or issues are discussed can differ from group to group depending on the direction the conversation takes. Compared to stakeholder interviews an interview schedule for a focus groups needs to include fewer questions. This is because the group members will usually have a range of views, opinions and discussions on a single question. Whom do I include in a group? It is important that you think about this carefully. Since a successful focus group is about people interacting, sharing and discussing ideas you want to make sure that the make-up of a group encourages this. You need to make sure that people are going to be comfortable expressing their views in front of others in the group. Feedback Forms and Surveys Feedback forms can be useful when assessing participants experiences of and learning as a result of attending a workshop or training session. Feedback forms can contain both quantitative and qualitative data collection methods. Rating scales are often used in feedback forms and include: category scales; numerical scales; graphic scales; likert scales; forced-choice instruments; and checklists. Section 3: Planning and monitoring CAYAD projects using RBA Page 37
42 Developing a good feedback form Make the feedback form brief and to the point: Only include questions or scales directly relating to the evaluation. For example there isn t a lot of point asking participants to rate the venue if this was the only available place to accommodate the number of people attending Make the dimensions to be rated clear. For example, if participants were asked to rate their competence, we would expect different people to base their ratings on different factors. One participant might give a particular weight to a particular aspect of competence such as their ability to write well, while another might give weight to being a good communicator. Make clear any standards those doing the rating are expected to use: Words such as superior, good, adequate, and poor imply a standard which the behaviour rated is to be compared: Superior to what, adequate for what? When using likert scales five is the most common number of answer choices, with the middle number being neutral. Some likert scales reduce the number to four by eliminating the middle position. Using open-ended questions to enable participants to add additional information. For example, is there anything else you would like to say? Rating Scales Scales ranging from 1 to 5 are common. Remember to ask people why they have selected the answer they have. For example: How satisfied or dissatisfied are you with the level of training you have received from your current employer? o Very satisfied o Quite satisfied o Neither satisfied nor dissatisfied o Quite dissatisfied o Very dissatisfied Please write down your reasons for how satisfied or dissatisfied you feel: Number ranges can also be used as a scale. For example: How happy are you with your employment conditions? Not at all Neutral Extremely Happy happy Section 3: Planning and monitoring CAYAD projects using RBA Page 38
43 Statements involve getting people to choose the most appropriate statement or statements from a predetermined list. These statements need to cover the broad range of possible responses. In addition, to avoid biasing your results, present an equal number of positive and negative statements. For example: Below is a list of things that could be said about this PICTA monitoring training session. Please circle all those that best fit how you feel about the training session. Too much information Friendly and relaxed Not enough information I feel I know more Very useful information Not enough group work It is also useful to include an other, don t know, and refused category to response options and leave a space to let people elaborate on their answers where appropriate. Observation Observation provides descriptive information about what happens in a programme event, including the environment or context, activities, processes, and discussions. Observation can be as follows: Site visit: the evaluator or another person outside the organisation becomes more familiar with the programme by travelling to the programme site and observing the programme activities as they occur. Staff observation: observations about the programme recorded by staff through reports, record keeping, journal writing or observation notes Participant observation: Observations about the programme reported by those people served by the programme. When to use observation: To determine whether the programme s processes are being implemented as intended To assess whether certain programme outcomes have been met To obtain data about the behaviour of individuals and groups To learn about unanticipated effects of a programme When other types of data collection may be inappropriate or in conflict with the philosophies of the programme When people are unwilling or unable to provide information using other methods Repeated observations of a programme can provide information about changes over time. Section 3: Planning and monitoring CAYAD projects using RBA Page 39
44 Advantages and disadvantages of observation: Advantages Observers document programme activities as they are happening rather than relying on memories of the events Evaluator observation contributes information from a different perspective than that of people participating in the programme and programme staff Disadvantages Confidentiality must be considered Evaluator observation may be intrusive and may influence the event being observed Evaluator observation can be expensive and time-consuming Section 3: Planning and monitoring CAYAD projects using RBA Page 40
45 Design tips for your interview, focus group or survey Key informant interviews Focus groups Surveys Start with an introduction: what it is that you are going to talk about and how you are going to record their responses Begin by asking general questions that are easy for people to answer, then move on to the more specific and personal questions Not too many questions to encourage people to talk freely about issues and give people more time to answer Has the least questions and have a flexible question format so that issues can be discussed as they arise for each group Focus on specific items of information, which often require less time to answer Contain open-ended questions allow people to respond in their own words, rather than choose a response from a list of options. These questions encourage in-depth discussion around people s thoughts, feelings and attitudes, for example: How would you describe how your daily activities have changed? Follow up on any interesting points raised by prompting. This will mean you will have to think on your feet and make up a new question. You probe deeper to find out more information. Contain closed-ended questions limit people s responses to predetermined categories. These are either a list of possible answers from which participants select, or yes/no responses. For example: Who makes the decisions in your household? We make more decisions equally My husband makes most decisions My wife makes most decisions Other Another example: Do you support women with children getting employment? Yes No Don t know Do not use: Words that are hard to understand Two questions in one e.g. do you consider that your household income has increased and what have you spent this extra money on? Questions that are too long and contain a lot of information e.g. in the past many people have thought it more important that boys receive secondary school education. These attitudes have been changing in the past five years with more value placed on girls going to school. Thinking about your attitudes in relation to the education of girls and boys do you think that girls have just as much right to receive secondary schooling as boys? Abbreviations, e.g. information collected by UNDP suggests Double negatives, e.g. do you disagree that there are not more opportunities in urban areas than rural areas? Section 3: Planning and monitoring CAYAD projects using RBA Page 41
46 Pre-testing It is important that the questions you develop for key informant interviews, focus groups or feedback forms are trialled before you use them. This process is called pre-testing. You need to practice using your interview or survey schedules on someone who can give you feedback on whether they work well or not, their suitability and acceptability. Pre-testing enables you to find out whether: The information you collect from the questions are useful to the overall type of information that you are wanting to collect Your questions are being interpreted as you intend them to be The words you use are clearly understood The format of the questions and the instructions are easily understood by both respondents and the interviewer The interview or survey does not take too long to complete. For a survey approximately 10 minutes is a good length of time when interviewing members of the general population. This time can increase if the subject matter is of interest to participants. Key informant interviews and focus groups can run from between 30 minutes to two hours. The following is a checklist that you should run through when pre-testing interview or survey questions. When the interviewer reviews the process, they should ask themselves these questions: Did any of the questions seem to make the respondents uncomfortable? Did you have to repeat any questions? Did the respondents misinterpret any questions? Which questions were the most difficult or awkward for you to read out? Have you come to dislike any specific questions? Why? Did any sections seem to drag? Were there any sections in which you felt that the respondents would have liked the opportunity to say more? Interviewing skills As an interviewer, you will need to know the interview or survey questions well, know how to ask the questions and fill out the questionnaire form, and understand the process of contacting respondents. Skills for key informant questionnaire and focus groups include: covering all the issues or questions and keeping people to the point Clarifying vague statements prompt the respondent so that they provide more information or clarity in their response Creating an atmosphere that encourages open discussion Listening in a positive, unbiased way to what people have to say Presenting yourself as approachable and friendly Section 3: Planning and monitoring CAYAD projects using RBA Page 42
47 Recording information Ideally key informant interviews and focus groups should audio-tape what participants say. Another option is to take written notes at the time of the interview or focus group. Either the interviewer or a colleague writes down word-for-word as much as they can the things that are said. In a focus group situation the person reading out questions and prompting should not write down what is said. There are some problems with writing notes instead of audio-taping information: The note taker is unable to write everything down and the value of the word for word comments is lost. You will never really be able to repeat exactly what a respondent said. As they are writing things down, the note taker will be missing something else that is being said. The process of selecting what to write down affects the results as in doing this they must choose not to write something else. When carrying out face-to-face surveys, interviewers will generally record the respondent s responses by hand there and then. Section 3: Planning and monitoring CAYAD projects using RBA Page 43
48 Part E: Analysing and interpreting data Analysing and reporting on surveys or feedback forms Feedback forms and survey questions can often be analysed by counting and reported in terms of numbers or percentages of people who thought, did or experienced something. Some common ways of analysing and reporting information include: Counting and percentages Adding together how many people responded to each question is a simple way of looking at your information. You can divide the number of people who responded in a particular way to each question by the total number of people asked that question, and then multiply it by 100, to get the percentage of people that had a particular opinion on a question. It is also useful to look at who said what. What types or groups of people responded in some ways and not in others? If you have a small sample (generally less than 30), raw numbers should be used instead of percentages. For example, it may be more meaningful to say, 12 out of 15 people felt a particular way about something than saying 80% felt that. Using percentages with a small sample is often misleading as it can make results appear more or less important than they really are. Graphs and figures Often a useful way of making the information more meaningful, or easier to interpret, is to draw up a table or graph of the information. It can be easier to compare groups and highlight key issues this way. Each graph should have a title and an accompanying paragraph discussing the graphs significance. Open-ended questions in surveys Sometimes open-ended questions are used in surveys when you want people to expand on a response. If you have only a small number of questionnaires, then you can analyse them the same as you would stakeholder interviews or focus groups. With a larger number of questionnaires you may want to transport the participants comments into countable data. To do this you can: Step 1 Write down all the different comments that people make about their level of satisfaction. Each time the same comment is made put a tally mark next to the first one that has been written down. Step 2 Give a general title to each statement that occurs frequently. Step 3 Give each statement that occurs frequently a code number. Then, go back to the questionnaires and write the code number in the margin next to each response as it occurs. Section 3: Planning and monitoring CAYAD projects using RBA Page 44
49 Step 4 When this has been done for all questionnaires start counting the number of times each code occurs. In the end you will be able to say, for example, five out of 50 respondents thought in a particular way, that is 10% of respondents thought this. Analysing and reporting on key informant interviews and focus groups Think about how you want to report the information before you begin the analysis. This way, your analysis becomes part of your report writing process. Step 1 Soon after each interview or discussion, write down on a piece of paper your thoughts on what happened what people thought were key issues and how they responded to some of your questions. This is an overview of the interview. Use your interview schedule as a starting-point for planning your analysis and your report. Your interview schedule will probably have questions set out in topic groups. Under each topic, one or more specific question will have been asked by the interviewer with comments by respondents. So, in your analysis and reporting, Topic 1 may be your first report section and Topic 2 the next and so on. Step 2 Focus on one topic area at one time. Sit down with a photocopy of your transcripts or verbatim notes and either: Cut out from the photocopy, all comments to do with Topic 1. Glue these comments on to a big piece of paper under the heading Topic 1; Or copy and paste from your transcript files into a new file on your work processor. Continue to do this until all your topics have been pasted together and there is nothing that is relevant to the discussion that is left on the original transcripts. Step 3 Now you start looking for the different kinds of things that people said when the first question in this topic was asked. You will soon notice that people often talk about similar issues but use different words. At other times only one or two people might mention a particular issue. Identify sub-topics where people talk about similar or new issues by using different coloured highlighter pens. Step 4 Make sure that everything said (and that is relevant to the topic) is marked in some way. Step 5 Once you have colour-marked everything that goes with Topic 1 you can start reporting this section. Pick a sub-topic and write an introductory sentence and then put in examples or quotations of what people said about that subtopic. Be sure to use quotations which complement the text. Quotations that are concise and to-the-point are preferable. If the quotation makes an excellent point but the language is unclear and hard to follow then it is better to make the point in your own words. Section 3: Planning and monitoring CAYAD projects using RBA Page 45
50 Repeat this process for all topics areas that you have discussed with respondents. A similar process to that described above can be used to analyse in-depth information on your computer. Remember, in-depth methods explore all the different thoughts, feelings and impressions people have about something. Avoid saying how many people thought, felt or did something when reporting this type of information since the number of people who say it just depends on the number of people you included in your study. Section 3: Planning and monitoring CAYAD projects using RBA Page 46
51 Appendix A: National CAYAD Measures Once you have analysed your data you should be able to provide answers to complete how well you are doing against the national RBA measures: National CAYAD Measures # Activity How Many % How Well #/% Is anyone better off 1 Support organisations to develop healthy and sustainable policy and practices to enhance environments to reduce alcohol and other drug related harm. # organisations/commu nity groups supported. % schools supported that are decile 1-4. % marae supported. % organisations/commu nity groups you engaged with who have started the policy development/review process. #/% organisations/community groups with new or improved AOD policies in place as a result of the provider s activity (BC, O). #/% organisations/community groups with new or improved AOD practices in place as a result of the provider s activity (BC, O). Complementary narrative List the organisations/commu nity groups you have supported. Complementary narrative Describe the changes that have occurred as a result of the AOD policy and practices being implemented. Activity How Many % How Well #/% Is anyone better Section 3: Planning and monitoring CAYAD projects using RBA Page 47
52 2 Engage with and support organisations/community groups to plan and deliver community action initiatives to reduce alcohol and other drugs harm in young people 4. # organisations/commu nity groups supported. # community action initiatives supported. Complementary narrative List the organisations/commu nity groups you have supported. % organisations/commu nity groups report they are satisfied or very satisfied with provider s support (ie, rating of 4 or 5 for likert scale of 1 to 5). off #/% outcomes in community action initiatives achieved (CC, O). Complementary narrative Describe the outcomes that have been achieved as a result of provider s support. Activity How Many % How Well #% Is anyone better off 3 Design, deliver and support awarenessraising activities 5 that provide opportunity for informed discussion and debate, increase knowledge 6 and/or # participants # awareness-raising initiatives delivered. % awareness-raising messages are aligned with Government, Ministry of Health and other evidenced based policies/strategies. #/% participants report an increased knowledge of topic and/or increased understanding of key strategies to reducing AOD related harm (SK, S). create behaviour change around the use of alcohol and other drugs. Complementary narrative Complementary narrative Complementary narrative Describe the awareness-raising initiatives. Describe the organisation/commun ity groups that have participated in the awareness-raising initiatives. List the policies/strategies used to inform the awareness-raising initiatives. Describe the behavioural changes as a result of the awareness-raising initiatives. Activity How Many % How Well #% Is anyone better 4 These are initiatives led by the community with CAYAD support or CAYAD led with strong community involvement 5 This can include supporting national campaigns 6 This can include knowledge of evidence-based actions to reduce harm from AOD Section 3: Planning and monitoring CAYAD projects using RBA Page 48
53 4 Support organisations/commu nity groups to increase input into local, regional and national decisionmaking, including engaging in policy/law/by-law development processes and the alcohol licensing process. # organisations/commu nity groups supported to develop a submission. % organisations/commu nity groups that have involved youth in the submission development process. off #/% organisations/commu nity groups report they have put in a submission, including licensing objections, as a result of provider s support (BC, S). #/% organisations/commu nity groups report they have made an oral submission or licensing objection as a result of the provider s support (BC, S). Complementary narrative List the organisations/commu nity groups you have supported. Complementary narrative List the submissions that have been submitted and the outcomes (when available). Section 3: Planning and monitoring CAYAD projects using RBA Page 49
54 Appendix B: Evaluation in New Zealand Evaluation perspectives Just as there are different forms of evaluation, there are also different perspectives on evaluation. The cultural lens that you bring to an evaluation will influence evaluation practice. When conducting evaluations in any community or organisational context, it is critical that evaluators are familiar with their own values, attitudes, beliefs and assumptions about culture as well as being familiar with different cultural perspectives. We think there are a number of concepts that are useful when doing evaluation in the Aotearoa/New Zealand context: Partnerships Participation Flexibility Public good focus Utilisation-focused Capacity building Evidence-based Maori approach to evaluation the hikoi approach Gives a new understanding of evaluation as a Maori empowerment approach Is responsive to situations and people and is reflexive Allows the use of any methodology that supports Maori development Avoids one size fits all How do you do evaluation with Maori? Maori evaluation issues Respect for relationships Shared evaluation kaupapa - working for Maori wellbeing Journey is as important as the outcome Working within or alongside mainstream organisations Iwi issues accountability, ethics Evaluation capacity Relationship based success is being invited back High expectations Evaluators have expert status but we are not experts Pacific approach to evaluation Pacific peoples = many nations Samoa, Cook Islands, Tonga, Niue, Fiji, Tokelau, Tuvalu Other Pacific Tahiti, Solomon Islands, Kiribati, Papua New Guinea, Rotuma One size does not fit all variation across, and variation within Pan-Pacific or ethnic-specific approach Relationships building connection, responsibilities and obligations Reciprocity balance Section 3: Planning and monitoring CAYAD projects using RBA Page 50
55 Formative evaluation Qualitative, formative and process orientation to evaluation - NZ is internationally known for the emphasis placed on formative evaluation techniques. The importance of evaluation being included from the inception of programmes to promote shared understandings and commitments about the role and importance of evaluation An inclusive approach is taken with all stakeholders, appreciating both different perspectives and different types of knowledge, including academic, cultural and social sources. For instance, qualitative methods such as focus groups help to capture alternative perspectives. Ongoing reflection and utilisation of learning are inherent features of formative, process and qualitative evaluation. Reflection processes evaluate both quality of performance and the new learning and knowledge that emerge during the design and implementation of projects. Utility is strongly emphasised. The learning captured during the reflective processes is fed back into the project to improve effectiveness of its design and delivery, and to inform the ongoing evaluation process. Political structure and decision-making cycles Major policy changes can occur very rapidly and evaluators need to be very astute and flexible in order to maximise the use of evaluations The three-year electoral cycle is very short and typically means that new programmes are developed in year one, implemented in year two and evaluated in year two and three with the use of evaluation being affected by the three year election cycle Evaluations tend to focus on shorter term issues and on programmes that produce results fairly quickly Evaluations that produce concrete, safe, specific and immediately useful lessons tend to be favoured over something intangible, and ambiguous and long-term Policy development, funding and evaluation cycles tend to peak at different times which means that evaluations can fail to fit in with key decision making cycles which affects their use The personal effect Process matters a lot particularly due to there being close and often personal relationships between ministers, policy advisers, politicians, programme providers and clients of programmes A lot happens in NZ because of who knows whom and their particular reputations The role of the evaluator is also seen as personal, as opposed to a position of detached observation. It is recognised that the evaluator s role involves a dynamic interaction with the programmes they evaluate, where knowledge and insights are shared and have an impact in both directions. Section 3: Planning and monitoring CAYAD projects using RBA Page 51
56 Appendix C: Evaluation standards The American Evaluation Association Guiding Principles (American Evaluation Association, 2004) also guide evaluation practice. These standards are intended to ensure an evaluation will: Serve the information needs of the intended users Reveal and convey technically adequate information about the features that determining the worth or merit of the programme being evaluated Be realistic, prudent, diplomatic and frugal Be conducted legally and ethically Utility Accuracy Feasibility Propriety Recently the Australia and New Zealand Evaluation Association (ANZEA) has developed Standards. The standards are a set of four high level principles. The core value underpinning the standards is that of evaluation with integrity which means that evaluation needs to consider the following: respectful, meaningful relationships ethic of care responsive methodologies and trustworthy results competence and usefulness. More information on the ANZEA Evaluation Standards can be found here: Section 3: Planning and monitoring CAYAD projects using RBA Page 52
57 Section 4 Planning and Monitoring Templates
58 CAYAD Action Plan Template Project Name: Objective: Key Tasks/Actions Completion Date Aligned National RBA Activity # (where applicable) Data collection method Section 4: Planning and monitoring templates Page 54
59 Writing a Project Objective Project Title 1. Who is the project designed to reach (target group)? 2. What need, issue or concern does your project address? 3. How will your target group be better off as a result of your project? Writing your objective: This project is for.. It is designed to address the issue of. As a result of this project. Section 4: Planning and monitoring templates Page 55
60 Identifying Stakeholders for your CAYAD Reference Group or project List the key stakeholders you need for: Advocacy: Who can effectively promote the actions/changes needed at different levels? (e.g. politically, or within local networks/organisations) Delivery: Who can access the people or resources needed to deliver project activities? Positive publicity: Who can put your projects in the spotlight, and increase a project s credibility? Ongoing support: Who can fund/authorise or continue /expand your projects? Section 4: Planning and monitoring templates Page 56
61 Developing your Actions 4. What is the story behind the issue? What is causing it? 5. Partners: Who are the partners who could support the development or delivery of the project? 6. What works to address this issue, including no-cost or low-cost ideas? (Common sense ideas and research where available) Tip: Your partners can help you to answer this question, or you may need a plan for gathering further evidence or information. 7. What do you propose to do? (Action Plan) List the key actions you will take to achieve your objective Section 4: Planning and monitoring templates Page 57
62 What does being better off look like? Aim: To define (1) your intended outcomes (2) the point you can say they have been achieved. Process: Use the table to clarify your outcomes, to define what success looks like, and to show what data you will need to collect to provide evidence that the project is successful. Tips: Work with your stakeholders to clearly define what success means to them (the middle box) Describe practical changes that you will be able to see and measure Decide if all the changes need to have happened for the outcome to be achieved, or only some of them. Outcome What success looks like How you will find out (Data collection method) Example: A family-friendly environment in the rugby club More meals and non-alcoholic drinks being purchased Less intoxication Kuia and kaumatua attending Parents and children spending more time together in the club Manager report/club accounts Observation in the club Section 5: CAYAD media toolkit Page 58
63 Section 5 CAYAD Media Toolkit
64 FACE THE MEDIA TOOLKIT Prepared by Vienna Richards Section 5: CAYAD media toolkit Page 60
65 SELF-DIAGNOSTIC TOOL Before the Interview This tool is designed to help YOU as a spokesperson ensure you are ready for interviews. Consider the following questions, and fill in the answers. It is best to do this worksheet at least a few hours before your interview (if possible), so that you can do any additional preparation that you may need to. You may not always have all the answers to all of these questions, but if you can t answer several of them, carefully consider whether or not you are prepared for your interview. Questions & Answers 1. To what audience is this interview targeted? 2. Do I have specific message points prepared? What are they? 3. What complex terms, jargon, or topics will I need to explain? Have I prepared simple explanations? 4. What is the format of this interview (e.g., newspaper, radio, television newsmagazine)? 5. Have I prepared specifically for this format (e.g., length, type of questions)? 6. Do I know the reporter s goals, style, and the type of questions that he or she is likely to ask? Section 5: CAYAD media toolkit Page 61
66 7. How will I handle difficult questions? 8. Do I have a quotable sentence or phrase if needed? What is it? 9. What are the things I can t talk about? 10. Who can talk about these things? Section 5: CAYAD media toolkit Page 62
67 AVOIDING MEDIA PITFALLS What To Do When Note: Please role play and practice these responses well before you need to use them! The interviewer expects you to comment on issues beyond your expertise Solution: State firmly, but politely, that you are only prepared to answer questions within your expertise and responsibility Once you ve said that, do not response to any further questions of this nature Transition into key message points If the interviewer persists, say I m sorry, I m unable to answer your question Stick to the substance of your message You are asked a question you don t know the answer to. Solution: Say I don t know. If they ask you again, repeat your answer I don t know. That s outside of my expertise/outside of my role I m sorry that s outside of my area of expertise. I suggest you ask those who do know Never attempt to respond to a question that you don t know the answer to Your credibility will be jeopardized! Offer to find the answer Section 5: CAYAD media toolkit Page 63
68 You ve answered fully, but the interviewer stares at you as if you should say more. Solution: Don t. This is called the pregnant pause. Learn to be comfortable with silence Do not fill in the empty space. Simply stare back at the interviewer and wait for the next question. If the interviewer continues to stare at you expecting more, ask him or her for another question If the interviewer continues to use this technique, make a transition statement, and deliver your key message points A reporter puts down his microphone and says, Let s go off the record Solution: Never go off the record with a reporter. Assume that anything you say in the presence of a reporter will be quoted. Assume that anything you say in the presence of a reporter s equipment will be quoted. The interviewer or guest keeps interrupting you in mid-sentence. Solution: When it happens again, say I will be happy to respond to your comment, but first let me finish with mine Be pleasant, but insist on your right to give complete responses Do not interrupt a questioner! Section 5: CAYAD media toolkit Page 64
69 The interviewer is particularly antagonistic and asks one hostile question after another. Solution: Don t take it personally. Learn to detach from the emotion. Do not become combative Maintain your enthusiasm Do not repeat a negative question Remember, you are well prepared and rehearsed Answer questions with a brief response, then transition to a key message The interviewer wants you to respond to questions with yes or no answers. Solution: Do not fall for this technique If a one-word answer will not do justice to your topic, say that o there is not enough time for a proper answer to the question Offer to provide an answer in writing The interviewer starts questions with hostile or inaccurate comments. This is called the loaded preface. Solution: Don t allow the loaded preface to stand unchallenged. Either correct the comment or state: o I would have to verify that; I m not sure it is correct Quickly dispute the interviewer s comments, and explain why. Then, respond to the question posed, using the answer formula Section 5: CAYAD media toolkit Page 65
70 The interviewer poses an either/or question, and you don t agree with either option. Solution: Don t fall for this old trick If you don t agree with either option, your answer must be neither After you ve responded correctly, explain your response, then develop a transition An interviewer attempts to elicit your endorsement of a legislative proposal or program related to your issue. Solution: Be pleasant, but inform the reporter that your purpose is to provide information, not to make judgments Stress your key message points Develop a transition to get back to your subject During a taped interview, the reporter keeps raising his voice higher and higher. Solution: Don t take it personally Remain calm, and stick to your message Don t respond by raising your voice Each time the reporter raises his voice, lower yours The interviewer is unprepared and asks irrelevant questions. Solution: Take control by reaffirming your expertise Stress your key message points, feeding him questions about your topic Involve the interviewer by asking questions about his experiences and concerns Section 5: CAYAD media toolkit Page 66
71 SELF-DIAGNOSTIC TOOL After the Interview This tool is designed to help YOU as a spokesperson assess your interviews after the fact to identify what went well. In short, what worked, what didn t and lessons to learn. Assess your interview by evaluating the elements in the table below. Interview Assessment What I Did Well Areas for Improvement Key Message Points Tone Action Steps Jargon and Complex Topics Interview Format Scope Difficult Questions and Difficult Interviewer Techniques Were they concise, focused, and appropriately tailored for the audience? Was I open, honest, and empathetic, but not over reassuring? Did I provide specific, positive action steps, as appropriate? Did I avoid the use of jargon? Did I explain scientifically complex topics simply? Was I properly prepared for the format (e.g., had more than a sound bite for a 30- minute interview)? Did I answer only the questions in my scope of expertise and refer the reporter to others as needed? Did I handle these straightforwardly, calmly, and with poise? Section 5: CAYAD media toolkit Page 67
72 Section 5: CAYAD media toolkit Page 68
73 Section 6 Research Evidence Useful to CAYAD: Alcohol & Other Drugs
74 Babor, T., Caetano, R., Casswell, S., Edwards, G., Giesbrecht, N., Graham, K., Grube, J., Hill, L., Holder, H., Homel, R., Livingston, M., Osterberg, E., Rehm, J., Room, R., & Rossow, I. (2010). Alcohol: No Ordinary Commodity Research and Public Policy (2nd
75
76
77
78
79

80 Evidence Based Community Action Strategies to Address Harm from Methamphetamine Intervention model - a systems approach using multiple strategies and levels Proactive Policing in Partnership with Community Require property owners to improve security & conditions of their property & maintain drug free property Work with HNZ & Councils to encourage monitoring of drug activity in their houses Proactive, partnership approach that targets problem places or people Third party policing used - develop agency partnerships which enable local regulations or laws to be used in addressing problem places Available data informs partnership approach & enforcement effort Problem Focused & Third Party Intervention Problem Focused & Third Party Intervention Invisible Law Enforcement Crime Prevention Through Improving Environments Anonymous community reporting Encourage community awareness of drug dealing & market. Encourage anonymous reporting of drug selling via crime stoppers hotline Improve the environment in problem drug locations This may include: Cleaning up run down buildings/areas Improving lighting, security & signage in problem areas Limiting or altering access to problem areas Additional resources from community are leveraged Problem Focused & Third Party Intervention Increase community awareness & galvanize support for more enforcement Community Norms Decrease acceptability & denormalise of meth use WIde approach does not target specific problem areas Police work in partnership with community Ensure community concern increases local support for more meth law enforcement Does not use third party policing strategies Approach is proactive & incorporates: community crime prevention, drug hotline, neighborhood watch groups etc Law enforcement includes knock & talk & patrols Community Wide Policing HELP Encourage and support methamphetamine users, friends or family to access effective help and/or treatment &{MAP_NAME} - 14/06/11 - Mindjet
81 Examples of Evidence Based Strategies to Address Harm from Methamphetamine Proactive Policing in Partnership with Community CAYAD Example; Papakainga Project There was a problem with manufacturing of P in a papakainga and young people getting access to it.cayad was approached by a group of concerned residents who had decided to take action. CAYAD s role was facilitating local meetings and brokering the communities engagement with local police. A Neighborhood Watch roster was set up, a period of amnesty was created for contraband, a charter was developed by the marae committee and P labs were shut down. Problem Focused & Third Party Intervention Invisible Law Enforcement New Zealand & International example The Crime Stoppers Trust has set up an anonymous crime hot line in New Zealand & also in the UK. The purpose of Crime Stoppers is to enable community members to easily and anonymously provide information to the Police about crime in their communities. New Zealand Example Recently Housing New Zealand staff have been trained to recognize the signs of P manufacture in government owned housing. (Herald, Jan, 2010) Problem Focused & Third Party Intervention CAYAD Example Community mural was designed and painted on a wall close to flats where drug selling was happening. Community members also took photos of the mural, and this together with the general public attention the site now got meant that the drug activity ceased in this area Problem Focused & Third Party Intervention Crime Prevention Through Improving Environments International Example In 1996, the Chicago Police Department (CPD) implemented the Municipal Drug and Gang Enforcement (MDGE) pilot program, a multi-agency program designed to combat criminal gang and narcotics activity in Chicago. The program focused on cleaning up gang and drug problem buildings that were known to foster gang and drug crime. International Example: Oakland Beat Health Program This project involved police identifying addresses with repeat calls for police service and developing cooperative relationships with residents and businesses in problem locations. Police worked with city inspectors to improve the physical condition of the affected sites (e.g. enforcement of civil law codes and local regulations). Traditional enforcement methods were also used at the targeted properties. Problem Focused & Third Party Intervention Community Norms CAYAD Example Community members in Murupara launched a campaign to raise awareness of the harms caused by methamphetamine Take the P out of Muru-ara. Bill boards, posters, bumper stickers and the Christmas parade were all used to promote the message and encourage people to stand strong against P. CAYAD Waitakere is working with local wholesalers and retailers of P pre-cursers to encourage safer storage and supply. New Zealand Example Local government based crime prevention teams, New Zealand Police encouraging neighborhood support groups Community Wide Policing New Zealand Example Alcohol and Drug Helpline ( ) is available for calls 10.00am to 10.00pm everyday. HELP provides specific support for methamphetamine users and their friend or family If you want to find the support or treatment services nearest to you go to &{MAP_NAME} - 14/06/11 - Mindjet
82 BOOK SUMMARY doi: /j x Alcohol: No Ordinary Commodity a summary of the second editionadd_ Alcohol and Public Policy Group ABSTRACT This article summarizes the contents of Alcohol: No Ordinary Commodity (2nd edn). The first part of the book describes why alcohol is not an ordinary commodity, and reviews epidemiological data that establish alcohol as a major contributor to the global burden of disease, disability and death in high-, middle- and low-income countries. This section also documents how international beer and spirits production has been consolidated recently by a small number of global corporations that are expanding their operations in Eastern Europe, Asia, Africa and Latin America. In the second part of the book, the scientific evidence for strategies and interventions that can prevent or minimize alcoholrelated harm is reviewed critically in seven key areas: pricing and taxation, regulating the physical availability of alcohol, modifying the drinking context, drink-driving countermeasures, restrictions on marketing, education and persuasion strategies, and treatment and early intervention services. Finally, the book addresses the policy-making process at the local, national and international levels and provides ratings of the effectiveness of strategies and interventions from a public health perspective. Overall, the strongest, most cost-effective strategies include taxation that increases prices, restrictions on the physical availability of alcohol, drink-driving countermeasures, brief interventions with at risk drinkers and treatment of drinkers with alcohol dependence. Keywords Alcohol, alcohol industry, alcohol problems, policy, prevention, treatment. Correspondence to: Thomas F. Babor, University of Connecticut Health Center, 263 Farmington Avenue, Farmington, CT , USA. babor@nso.uchc.edu Submitted 18 January 2010; initial review completed 15 February 2010; final version accepted 15 February 2010 SETTING THE POLICY AGENDA From a public health perspective, alcohol plays a major role in the causation of disability, disease and death on a global scale. With the increasing globalization of alcohol production, trade and marketing, alcohol control policy needs to be understood not only from a national perspective but also from an international purview. The same is true of alcohol science, particularly policy research. In the past 50 years considerable progress has been made in the scientific understanding of the relationship between alcohol and health. Ideally, the cumulative research evidence should provide a scientific basis for public debate and governmental policy making. However, much of the scientific evidence is reported in academic publications and the relevance of this information for alcohol policy often goes unrecognized. To address the need for a policyrelevant analysis of the alcohol research literature, the authors published the first edition of Alcohol: No Ordinary Commodity in 2003, continuing in the tradition of integrative reviews dating back to 1975 [1,2]. The revised, second edition of Alcohol: No Ordinary Commodity [3] reflects the considerable expansion of scientific evidence for effective alcohol policy since the original publication. The second edition also responds to the fact that many parts of the world that have traditionally had relatively low aggregate levels of alcohol consumption and weak alcohol controls (e.g. sub-saharan Africa and parts of Asia) are experiencing an expansion of commercial production and sophisticated marketing campaigns by the alcohol industry. NO ORDINARY COMMODITY Alcoholic beverages are an important, economically embedded commodity. Alcohol provides employment for 1 The Alcohol and Public Policy Group consists of Thomas Babor, Raul Caetano, Sally Casswell, Griffith Edwards, Norman Giesbrecht, Kathryn Graham, Joel Grube, Linda Hill, Harold Holder, Ross Homel, Michael Livingston, Esa Österberg, Jürgen Rehm, Robin Room and Ingeborg Rossow The Author. Journal compilation 2010 Society for the Study of Addiction Addiction, 105,
83 770 Alcohol and Public Policy Group Patterns of drinking Toxic effects* Chronic Disease Intoxication Accidents/Injuries (acute disease) Average volume Dependence Acute Social Problems Chronic Social Problems Figure 1 Why alcohol is no ordinary commodity; relationships among alcohol consumption, mediating factors and alcohol-related consequences (reprinted with permission) people in bars, restaurants and the agricultural sector, brings in foreign currency for exported beverages and generates tax revenues for the government, but the economic benefits connected with the production, sale and use of this commodity come at an enormous cost to society. Three important mechanisms explain alcohol s ability to cause medical, psychological and social harm: (1) physical toxicity, (2) intoxication and (3) dependence. Alcohol is a toxic substance in terms of its direct and indirect effects on a wide range of body organs and systems [4]. With chronic drinking and repeated intoxication a syndrome of interrelated behavioural, physical and cognitive symptoms develops, referred to as alcohol dependence. As illustrated in Fig. 1, the mechanisms of toxicity, intoxication and dependence are related to the ways in which people consume alcohol, referred to as patterns of drinking. Drinking patterns that lead to elevated blood alcohol levels result in problems associated with acute intoxication, such as accidents, injuries and violence. Drinking patterns that promote frequent and heavy alcohol consumption are associated with chronic health problems such as liver cirrhosis, cardiovascular disease and depression. Sustained drinking may also result in alcohol dependence, which impairs a person s ability to control the frequency and amount of drinking. For these reasons, alcohol is not a run-of-the-mill consumer substance. ALCOHOL CONSUMPTION TRENDS AND PATTERNS OF DRINKING Alcohol consumption varies enormously, not only among countries but also over time and among different population groups. Alcohol consumption per capita is highest in the economically developed regions of the world. It is generally lower in Africa and parts of Asia, and is particularly low in the Indian subcontinent and in Moslem countries and communities. Western Europe, Russia and other non-moslem parts of the former Soviet Union now have the highest per capita consumption levels, but levels in some Latin American countries are not far behind [4,5]. With a few exceptions, there has been a levelling-off or decline in drinking in many of the high alcohol consumption countries from the early 1970s to the early 2000s, particularly in the traditional wine-producing countries in Europe and South America [6]. In contrast, increases in per capita consumption have been noted in emerging markets for alcohol in many low- and middle-income countries [5]. As the per capita consumption in a population increases the consumption of the heaviest drinkers also rises, as does the prevalence of heavy drinkers and the rate of alcohol-related harm [7,8]. Much of the variation in alcohol consumption from one part of the world to another is attributable to differences in the proportions of adults who abstain from drinking altogether. This suggests that per capita consumption will increase steeply if the proportion of abstainers declines, particularly in the developing world, where abstention is common. Men are more likely to be drinkers, and women abstainers. Among drinkers, men drink heavily (i.e. to intoxication, or large quantities per occasion) more often than women. Older age groups favour abstinence and infrequent drinking while young adults have higher levels of frequent intoxication [9]. The composition of social and health problems from drinking in any particular country or region is related to the drinking patterns and total amounts consumed in that country or region. These differences may help to explain why prevention and intervention strategies vary from one society to another. However, with the spread of commercial alcohol increasing homogeneity in drinking patterns, alcohol policy needs are likely to become increasingly similar. THE GLOBAL BURDEN OF ALCOHOL CONSUMPTION Alcohol accounts for approximately 4% of deaths worldwide and 4.65% of the global burden of injury and disease, placing it alongside tobacco as one of the leading preventable causes of death and disability [4,10]. In high-income countries, alcohol is the third most detrimental risk factor, whereas in emerging economies such as China alcohol ranks first among 26 examined. Some of the most important individual harms related to alcohol are coronary heart disease, breast cancer, tuberculosis, motor vehicle accidents, liver cirrhosis and suicide. Overall, injuries account for the largest portion of the alcohol-attributable burden. Volume of drinking is linked to most disease outcomes through specific dose response 2010 The Author. Journal compilation 2010 Society for the Study of Addiction Addiction, 105,
84 Alcohol: No Ordinary Commodity 771 relationships. Patterns of drinking also play an important role in the disease burden. Coronary heart disease (CHD), motor vehicle accidents, suicide and other injuries have all been linked to heavy episodic drinking [4]. Moderate drinking has CHD benefits for some individuals, but has also been linked to an increased risk of cancer and other disease conditions. Alcohol consumption is also a risk factor for a wide range of social problems [11]. Although there is plausible evidence for a direct causal link between alcohol consumption and violence [12], the relationship is more complex for problems such as divorce, child abuse and work-related problems. Alcohol consumption can impact negatively people other than the drinker through alcoholrelated crime (e.g. domestic violence), family dysfunction, traffic accidents and problems in the work-place. In sum, alcohol contributes to both social and health burdens. GLOBAL STRUCTURE AND STRATEGIES OF THE ALCOHOL INDUSTRY The alcohol industry is an important but understudied part of the environment in which drinking patterns are learned and practised, especially with the growth of modern industrial production, the proliferation of new products (e.g. caffeinated alcohol energy drinks and alcopops) and the development of sophisticated marketing techniques. At the national level, the industry comprises beer, wine and spirits producers and importers, as well as bars, restaurants, bottle stores and often food stores that sell alcohol to the public. Alcohol is seen as an important contributor to business opportunities and jobs in the hospitality and retail sectors. In recent years the international alcohol market has become dominated by a few large corporations [13,14]. In 2005, 60% of the world s commercially brewed beer was produced by global companies, with 44% made by the largest four: Inbev, Anheuser Busch, SABMiller and Heineken. A similar trend has occurred in the spirits sector, with Diageo and Pernod Ricard now managing some of the world s leading brands. The size and profitability of these companies support integrated marketing on a global scale. Size also allows considerable resources to be devoted, directly or indirectly, to promoting the policy interests of the industry. These developments challenge the public health sector and governments to respond with national and global public health strategies to minimize the health consequences and social harms resulting from the expanding global market in alcoholic beverages. It is often assumed that an industrialized alcohol supply will have positive economic effects in low-income countries, but the evidence for this is equivocal, particularly concerning job creation [15]. Research suggests that alcohol problems increase with economic development [16]. Many developing countries have alcohol laws and policies but often do not have the resources to enforce them adequately. THE INTERNATIONAL CONTEXT OF ALCOHOL POLICY Alcohol control policies at the national and local levels have come increasingly under pressure because of conflict with international trade policies, which tend to treat alcoholic beverages as ordinary commodities such as bread and milk [17]. At the beginning of 2000 there were 127 trade agreements registered at the World Trade Organization, most of which apply to trade in alcoholic beverages. Trade agreements generally require governments to reduce and eventually abolish all tariff and non-tariff barriers to international trade. When alcohol is regarded as an ordinary commodity, these agreements often hamper the effectiveness of alcohol control policies. With the growing emphasis on free trade and free markets, international organizations such as the European Union have pushed to dismantle state alcohol monopolies and other restrictions on the availability of alcoholic beverages, and disputes under trade agreements have resulted in reduced taxes and other increases in availability [18,19]. Nevertheless, the impact of international trade agreements and economic treaties cannot be blamed entirely for the lack of effective alcohol control policies at the national level. Although trade agreements constrain how domestic regulations are designed, they also allow government measures to protect human and environmental health specifically. Policies restricting the supply and marketing of alcohol have been defended successfully against challenge as both necessary and proportionate to achieving a clearly stated government health goal. However, restrictive policies often have an aspect that is protective of local economic interests, which makes them difficult to defend. At the international level, public health considerations concerning alcohol must have precedence over free trade interests [17]. STRATEGIES AND INTERVENTIONS TO REDUCE ALCOHOL-RELATED HARM Alcohol policy is defined broadly as any purposeful effort or authoritative decision on the part of governments to minimize or prevent alcohol-related consequences. Policies may implement a specific strategy with regard to alcohol problems (e.g. increase alcohol taxes or controls on drinking and driving) or allocate resources toward prevention or treatment services. Effective policies are evidence-informed and based upon sound theory, which increases the likelihood that a policy that is effective in one place will be effective in 2010 The Author. Journal compilation 2010 Society for the Study of Addiction Addiction, 105,
85 772 Alcohol and Public Policy Group Table 1 Theoretical assumptions underlying seven broad areas of alcohol policy, and the best practices identified within each policy area. Policy approach Theoretical assumption Best practices a Alcohol taxes and other price controls Regulating physical availability through restrictions on time and place of sales and density of alcohol outlets Altering the drinking context Drink-driving countermeasures Education and persuasion: provide information to adults and young people especially through mass media and school-based alcohol education programmes Regulating alcohol advertising and other marketing Conduct screening and brief intervention in health care settings; increase availability of treatment programmes Increasing economic cost of alcohol relative to alternative commodities will reduce demand Restricting physical availability will increase effort to obtain alcohol, and thereby reduce total volume consumed as well as alcohol-related problems Creating environmental and social constraints will limit alcohol consumption and reduce alcohol-related violence Deterrence, punishment and social pressure will reduce drink driving Health information that increases knowledge and changes attitudes will prevent drinking problems Reducing exposure to marketing which normalizes drinking and links it with social aspirations will slow recruitment of drinkers and reduce heavier drinking by young people Alcohol dependence will be prevented by motivating heavy drinkers to drink moderately; various therapeutic interventions will increase abstinence among people who have developed a dependence on alcohol Alcohol taxes Ban on sales, minimum legal purchase age, rationing, government monopoly of retail sales, hours and days of sale restrictions, restrictions on density of outlets, different availability by alcohol strength Enhanced enforcement of on-premises policies and legal requirements Sobriety checkpoints, random breath testing, lowered BAC limits, administrative licence suspension, low BAC for young drivers ( zero tolerance ), graduated licensing for novice drivers None Legal restrictions on exposure Brief interventions with at-risk drinkers, detoxification, talk therapies, mutual help/self-help organization attendance a Based on consensus ratings of effectiveness, amount of scientific evidence and cross-national testing, these strategies and interventions receivedtwoor more plusses (on a scale of 0 3) in all three categories. BAC: blood alcohol concentration. others. Research has the capacity to indicate which strategies have demonstrated successful achievement of their public health intentions and which have not. Table 1 lists the seven main areas within which alcohol policies have been developed and describes the theoretical assumptions behind each policy approach as well as the specific interventions that have been found to be best practices because of the evidence of effectiveness, amount of research support and extent of testing across diverse countries and cultures. CONTROLLING AFFORDABILITY: PRICING AND TAXATION Governments have long used customs tariffs on alcohol imports and excise duties on domestic production to generate tax revenue and to reduce rates of harm from drinking. Dozens of studies, including a growing number in developing countries, have demonstrated that increased alcohol prices reduce the level of alcohol consumption and related problems, including mortality rates, crime and traffic accidents (see [17,20,21]). The evidence suggests that the effects of pricing apply to all groups of drinkers, including young people and heavy or problem drinkers, who are often the focus of government attention. Some governments have restricted discounted sales or established minimum sale prices for alcoholic beverages. While somewhat limited, the evidence suggests that raising the minimum price of the cheapest beverages is effective in influencing heavy drinkers and reducing rates of harm [22]. Other research [23] shows that alcohol consumption can be reduced by increasing the price of 2010 The Author. Journal compilation 2010 Society for the Study of Addiction Addiction, 105,
86 Alcohol: No Ordinary Commodity 773 drinks (e.g. alcopops) that are designed and marketed in a way that appeals to young adults. Despite its apparent effectiveness, taxation as a method of reducing harm from drinking appears to have been under-used. In recent decades, the real price of alcoholic beverages has decreased in many countries, at a time when other alcohol control measures have been liberalized or abandoned completely [19,24,25]. Prices have declined partly because governments have not increased tax levels in accordance with inflation and rising incomes. In some cases alcohol taxes have been reduced to compete with cross-border imports and smuggling, or to comply with trade dispute decisions. REGULATING THE PHYSICAL AVAILABILITY OF ALCOHOL Restrictions on alcohol availability focus upon regulating the places, times and contexts in which consumers can obtain alcohol, and include both partial and total bans on alcohol sales. There is great variability in regulation of access to alcohol. A number of countries have monopolies for at least some form of retail sale, and many Islamic states and some localities elsewhere practice total prohibition. In contrast, there is concern in many developing countries that cheap, informal-produced and illegal alcohol is largely unregulated [17]. Research indicates strongly that as alcohol becomes more available through commercial or social sources, consumption and alcohol-related problems rise. Conversely, when availability is restricted, alcohol use and associated problems decrease. The best evidence comes from studies of changes in retail availability, including reductions in the hours and days of sale, limits on the number of alcohol outlets and restrictions on retail access to alcohol [16,26 28]. Consistent enforcement of regulations is a key ingredient of effectiveness. Licence suspensions and revocations often provide the most direct and immediate enforcement mechanism. Government ownership of alcohol outlets can regulate alcohol availability in a comprehensive way. There is strong evidence that off-premises monopoly systems limit alcohol consumption and alcohol-related problems if alcohol control is a central goal, and that elimination of those monopolies can increase total alcohol consumption, especially when privatization leads to increased outlets, expanded hours of sale and reductions in the enforcement of policies such as not selling to underage customers [29,30]. For young people, laws that raise the minimum purchase age reduce alcohol sales and problems, if they are enforced at least minimally. This strategy has strong empirical support, with research indicating substantial impacts on traffic and other casualties from changes to the purchase age [23,31,32]. In general, the regulation of availability can have large effects. The cost of restricting physical availability of alcohol is cheap relative to the costs of health consequences related to drinking, especially heavy drinking. The most notable adverse effects of availability restrictions include increases in informal market activities (e.g. home production, illegal imports). Nevertheless, where a legal supply is available, informal market activities can generally be limited by effective enforcement. MODIFYING THE DRINKING CONTEXT Alcohol is consumed in a variety of places. Research suggests that licensed premises provide an opportunity for preventing alcohol-related problems through training bar staff in both responsible beverage service and managing or preventing aggression [33,34]. However, responsible beverage service is only effective if accompanied by enforcement. Enhanced enforcement of laws and regulations by police, liquor licensing, municipal authorities and other methods is likely to have impact through situational deterrents, in particular the threat of suspending or revoking the licence to sell in cases of irresponsible selling and, where laws permit, through holding servers and owners liable for the harms resulting from over-service. Community action programmes, wherein local organizers work with the police, are an effective strategy for reducing problem behaviour when focused upon licensed premises, possibly because these are able to incorporate broad multi-component approaches [35,36]. However, these programmes require extensive resources and longterm commitment, including enhanced and sustained enforcement. DRINK-DRIVING PREVENTION AND COUNTERMEASURES Alcohol is a major risk factor for traffic fatalities and injuries and an issue of great concern in emerging alcohol markets with rapidly expanding ownership of motor vehicles. Traditionally, law enforcement directed at drink-driving has been designed to catch offenders on the assumption that such practices will deter people from driving after drinking. There is limited evidence to support the positive impact of these laws, perhaps because they are enforced inconsistently and the punishment is often delayed. The one punishment that seems to have a consistent impact on drink-driving offences is administrative licence suspension or revocation for drink-driving [37,38] The Author. Journal compilation 2010 Society for the Study of Addiction Addiction, 105,
87 774 Alcohol and Public Policy Group The evidence indicates that laws setting a reasonably low level of blood alcohol concentration (e.g. 0.05%) at which one may drive legally, combined with wellpublicized enforcement, reduces drink-driving and alcohol-related driving fatalities significantly. This is a required first step for effective drink-driving policy [39,40]. The evidence is strong that frequent highly visible, non-selective testing (and selective testing if carried out with sufficient intensity) can have a sustained effect in reducing drink-driving and the associated crashes, injuries and deaths [41,42]. The most effective approach is random breath testing or compulsory breath testing. Sobriety checkpoints also increase the public perception of likelihood of apprehension. Several approaches reduce recidivism of drinkdriving, including counselling or therapy plus licence suspension and ignition interlock devices that prevent a vehicle from being started until the driver passes a breath test [43]. While designated driver and safe ride programmes may have some effect for people who, presumably, would otherwise drive while intoxicated, no overall impact on alcohol-involved accidents has been demonstrated [44]. Effective interventions for young drivers, who are at higher risk for traffic accidents, include a policy of zero tolerance [i.e. setting a blood alcohol concentration (BAC) level as close to 0% as possible] and the use of graduated licensing for novice drivers (i.e. limits on the time and other conditions of driving during the first few years of licensing) [45,46]. Traditional countermeasures such as driver training and school-based education programmes are either ineffective or yield mixed results. RESTRICTIONS ON MARKETING Alcohol marketing is a global industry. Many countries are now subject to unprecedented levels of exposure to sophisticated marketing, through traditional media (e.g. television, radio and print), new media (e.g. internet and cell phones), sponsorships and direct promotions, including branded merchandise and point-of-sale displays. Evidence shows that exposure of young people to alcohol marketing speeds up the onset of drinking and increases the amount consumed by those already drinking. The extent of research available is considerable (e.g.[47 49]), and shows effects consistently with young people. Marketing contributes undoubtedly to the ongoing recruitment of young people to replace older drinkers and to expand the drinking population in emerging markets. Legislation restricting alcohol advertising is a wellestablished precaution used by governments throughout the world, despite opposition from the alcohol industry. However, many bans have been partial, applying only to spirits, to certain hours of television broadcasting or to state-owned media. They have covered only the measured media, which represents only about half the marketing currently in force. These bans often operate alongside codes of industry self-regulation that specify the content of permitted forms of alcohol advertising. Imposing total or partial bans on advertising produce, at best, small effects in the short term on overall consumption in a population, in part because producers and sellers can simply transfer their promotional spending into allowed marketing approaches. The more comprehensive restrictions on exposure (e.g. in France) have not been evaluated. However, the fact that exposure to marketing produces an effect on alcohol consumption puts the question of controls on advertising high on the policy agenda. The extent to which effective restrictions would reduce consumption and related harm in younger age groups remains an open question. The most probable scenario, based upon the theoretical and empirical evidence available, is that extensive restriction of marketing would have an impact. Despite industry claims that they adhere to codes of responsible advertising, the detrimental influences of exposure to marketing messages are not addressed adequately by the voluntary codes on the content of alcohol advertisements adopted by the industry under a self-regulation approach. Self-regulation by means of industry voluntary codes does not seem to prevent the kind of marketing that has an appeal to younger people [17,49,50]. The evidence demonstrating the impact of current levels of marketing on the recruitment of heavierdrinking young people suggests the need for a total ban to restrict exposure to alcohol marketing, one that is able to cross national boundaries. EDUCATION AND PERSUASION STRATEGIES Education and persuasion strategies are among the most popular approaches to the prevention of alcohol-related problems. Some school-based alcohol education programmes have been found to increase knowledge and change attitudes toward alcohol, but drinking behaviour often remains unaffected [51]. Many programmes include both resistance skills training and normative education, which attempts to correct adolescents tendency to overestimate the number of their peers who drink or approve of drinking. Scientific evaluations of these programmes have produced mixed results, with generally modest effects that are short-lived unless accompanied by booster sessions [52]. Some programmes include both 2010 The Author. Journal compilation 2010 Society for the Study of Addiction Addiction, 105,
88 Alcohol: No Ordinary Commodity 775 individual-level education and family- or communitylevel interventions. Evaluations suggest that even these comprehensive programmes may not be sufficient to delay the initiation of drinking, or to sustain a small reduction in drinking beyond the operation of the programme. The strongest effects have been found in programmes directed at high-risk groups, an approach akin to assessment and brief intervention [52 54]. Media campaigns prepared by government agencies and non-governmental organizations (NGOs) that address responsible drinking, the hazards of drinkdriving and related topics are an ineffective antidote to the high-quality pro-drinking messages that appear much more frequently as paid advertisements in the mass media [17]. In sum, the impact of education and persuasion programmes tends to be small, at best. When positive effects are found, they do not persist and a focus upon educating and persuading the individual drinker to change his or her behaviour without changing the broader environment cannot be relied upon as an effective approach. TREATMENT AND EARLY INTERVENTION SERVICES During the past 50 years there has been a steady growth, primarily in high-income countries, in the provision of specialized medical, psychiatric and social services to individuals with alcohol use disorders. Typically, treatment involves a range of services from diagnostic assessment to therapeutic interventions and continuing care. Researchers have identified more than 40 therapeutic approaches evaluated by means of randomized clinical trials [55]. These are delivered in a variety of settings, including freestanding residential facilities, psychiatric and general hospital settings, out-patient programmes and primary health care. More recently, treatment services in some countries have been organized into systems that are defined by linkages between different facilities and levels of care, and by the extent of integration with other types of services, such as mental health, drug dependence treatment and mutual help organizations. Regarding the clinical management of non-dependent high-risk drinkers, the cumulative evidence [56] shows that brief interventions, consisting of one or more sessions of advice and feedback provided by a health professional, can produce clinically significant reductions in drinking and alcohol-related problems. Despite evidence of the benefits of brief interventions, it has been found difficult to persuade practitioners to deliver such care. Specialized or formal treatment consists of detoxification, out-patient counselling and residential care. Detoxification services are directed mainly at patients with a history of chronic drinking (especially those with poor nutrition) who are at risk of experiencing withdrawal symptoms. Administration of thiamine and multivitamins is a low-cost, low-risk intervention that prevents alcohol-related neurological disturbances, and effective medications have been used for the treatment of alcohol withdrawal. Treatment that obviates development of the most severe withdrawal symptoms can be life-saving. Following detoxification, a variety of therapeutic modalities have been incorporated into different service settings to treat the patient s drinking problems, promote abstinence from alcohol and prevent relapse. In most comparative studies, out-patient and residential programmes produce comparable outcomes [57]. The approaches with the greatest amount of supporting evidence are behaviour therapy, group therapy, family treatment and motivational enhancement. Despite advances in the search for a pharmacological intervention that could reduce craving and other precipitants of relapse (alcohol-sensitizing drugs, medications to directly reduce drinking and medications to treat co-morbid psychopathology), the additive effects of pharmacotherapies have been marginal beyond standard counselling and behaviour therapies [58,59]. Mutual help societies composed of recovering alcoholics are inexpensive alternatives and adjuncts to treatment. Mutual help groups based on the Twelve Steps of Alcoholics Anonymous (AA) have proliferated throughout the world. In some countries other approaches, often orientated to the family as well as the drinker, are also flourishing. Research suggests that AA itself can have an incremental effect when combined with formal treatment, and that AA attendance alone may be better than no intervention at all [60]. THE POLICY ARENA Alcohol policies are developed and implemented at many different levels of government. National or subnational laws often establish the legislative framework, including an oversight by the state of production, export and import of commercial alcohol products; control of wholesaling and retailing; legal minimum purchase ages for alcoholic beverages; apprehension of drivers with specified blood alcohol levels; alcohol marketing restrictions; and the support of treatment and prevention services. For this reason, policy systems at the national level are dominated rarely by one decision-making authority, but tend rather to be decentralized, with different aspects of policy delegated to a variety of different and sometimes competing decision-making entities, such as the health ministry and the taxation agency. Public interest groups, often represented by NGOs, contribute to the policy-making process in many countries. More recently, alcohol issues have become increas The Author. Journal compilation 2010 Society for the Study of Addiction Addiction, 105,
89 776 Alcohol and Public Policy Group ingly the concern of health professionals, mirrored by a change in the organization of health and welfare services as well as increasing professionalization in the caring occupations. International agencies, such as the World Health Organization, can also play an important role. In many nations there is a vacuum in advocacy for the public interest. Commercial interests have moved increasingly into this vacuum in the policy arena. Although the alcohol industry is not monolithic in terms of its motives, power or operations, in most instances the industry s producers, retailers and related groups share a common commercial imperative to make a profit. To promote their policy objectives, over the past 25 years the largest alcohol companies have set up more than 30 social aspects organizations, mainly in Europe, the United States and, more recently, in the emerging markets of Asia and Africa [61,62]. Typically, social aspects organizations promote a set of key messages that support ineffective policies for reducing harm [61,63]. Experience suggests that working in partnership with the alcohol industry is likely to lead to ineffective or compromised policy and is best avoided by governments, the scientific community and NGOs [64]. An appreciation of the various players in the alcohol policy arena can heighten our understanding of the following fundamental conclusion: alcohol policy is often the product of competing interests, values and ideologies. ALCOHOL POLICIES: A CONSUMER S GUIDE Table 1 lists 20 best practices that represent the most effective, evidence-based policy approaches to reduce alcohol-related harm. Many of the interventions are universal measures that restrict the affordability, availability and accessibility of alcohol. Alcohol taxes and restrictions limiting the opening hours, locations and density of alcohol outlets have a considerable amount of research support. The enforcement of a minimum purchase age for alcohol is another very effective strategy. Given their broad reach, the expected impact of these measures on public health is relatively high, especially when the informal market and illegal alcohol production can be controlled. Many drink-driving countermeasures received high ratings as well, especially those that increase the likelihood of apprehension and are part of a core alcohol policy mix. Alcohol treatment services have good evidence of effectiveness but they can be expensive to implement and maintain, with the exception of mutual help organizations. At the population level, their impact is limited relative to other policy options, as full treatment for alcohol problems can benefit only those individuals who come to treatment. Nevertheless, these programmes have the potential to impact the heaviest drinkers in a society, and could lower population levels of alcohol consumption and harm if they could be disseminated widely. Although the evidence is limited by the relative lack of research, it is likely that a total ban on the full range of marketing practices could affect drinking by young people, particularly if diversion of the promotional spending to other channels were blocked. There is no evidence that the alcohol industry s favoured alternative to marketing restrictions voluntary self-regulation protects vulnerable populations from exposure to alcohol advertising and other marketing practices. The amount of evidence on the effects of altering the drinking context has been growing, and we now think that strategies in this area can have modest effects. The fact that these strategies are applicable primarily to on-premises drinking in bars and restaurants somewhat limits their public health significance, as a high proportion of alcohol is purchased more cheaply for consumption elsewhere. Despite a growing amount of research using randomized controlled research designs, there is only weak evidence for the effectiveness of programmes that combine alcohol education with more intensive family and community involvement. Similarly, the expected impact is low for mass media responsible drinking campaigns. Although the reach of educational programmes is thought to be excellent, the population impact of these programmes is poor, and effectiveness is limited to several of the more recent college programmes. Policy options are often moulded to existing conditions and are implemented typically over time in a way that is fragmented, piecemeal and uncoordinated, in part because of the range of policy areas covered, in part because different ministries, departments and administrative agencies each have some aspect of alcohol policy under their purview. As a result, most countries do not have a single comprehensive policy towards alcohol but rather fragmented regulations and practices that sometimes are based upon profoundly different assumptions about the role of alcohol in society and the nature of alcohol-related problems. To enhance the likelihood of effectiveness, alcohol policies would benefit from greater public health orientation, integration and coordination. In sum, opportunities for evidence-based alcohol policies that serve the public good more effectively are more available than ever before. However, the policies to address alcohol-related problems are too seldom informed by science, and there are still too many instances of policy vacuums filled by unevaluated or ineffective strategies and interventions. Because alcohol is no ordinary commodity, the public has a right to expect a more enlightened approach to alcohol policy The Author. Journal compilation 2010 Society for the Study of Addiction Addiction, 105,
90 Alcohol: No Ordinary Commodity 777 Acknowledgements The writing of this book was sponsored the UK Society for the Study of Addiction and the Pan American Health Organization (PAHO). The findings and conclusions represent solely the consensus views of its 15 authors, none of whom received either direct or indirect support for their participation from any of the sponsoring organizations or any other organization that might represent a conflict of interest. We are grateful to Jean O Reilly PhD for her assistance with the editorial management of this revision. Declarations of interest JR received financial support to travel to and participate in meetings sponsored in whole or in part by the alcohol industry (ICAP; Association of the American Brewers). JR also received various unrestricted funds for projects by the pharmaceutical industry (Eli Lilly, Schering-Plough Canada). KG has had travel costs paid by the Responsible Hospitality Institute ( org/) and the International Harm Reduction Association. RH received a grant for project development, not research, from Drinkwise Australia in 2008, a body funded by the alcohol industry and at the time also co-funded by the Australian Government a relationship which has now ended. All other authors have no interests to declare. References 1. Bruun K., Edwards G., Lumio M., Mäkelä K., Pan L., Popham R. E. et al. Alcohol Control Policies in Public Health Perspective. Helsinki, Finland: Finnish Foundation for Alcohol Studies; Edwards G., Anderson P., Babor T. F., Casswell S., Ferrence R., Giesbrecht N. et al. Alcohol Policy and the Public Good. Oxford, UK: Oxford University Press; Babor T., Caetano R., Casswell S., Edwards G., Giesbrecht N., Graham K. et al. Alcohol: No Ordinary Commodity Research and Public Policy. Oxford, UK: Oxford University Press; Rehm J., Mathers C., Popova S., Thavorncharoensap M., Teerawattananon Y., Patra J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol use disorders. Lancet 2009; 373: World Health Organization. Global Status Report on Alcohol. Geneva, Switzerland: World Health Organization; Available at: publications/global_status_report_2004_overview.pdf (accessed 12 July 2009). 6. Gual A., Colom J. Why has alcohol consumption declined in countries of southern Europe? Addiction 1997; 92 (Suppl. 1): 21 31S. 7. Skog O.-J. The collectivity of drinking cultures: a theory of the distribution of alcohol consumption. Br J Addict 1985; 80: Skog O.-J. Commentary on Gmel and Rehm s interpretation of the theory of collectivity in drinking culture. Drug Alcohol Rev 2001; 20: Wilsnack R. W., Wilsnack S. C., Kristjanson A. F., Vogeltanz- Holm N. D., Gmel G. Gender and alcohol consumption: patterns from the multinational GENACIS project. Addiction 2009; 104: Ezzati M., Lopez A. D., Rodgers A., Murray C. J. L. Comparative Quantification of Health Risks: Global and Regional Burden of Disease Attributable to Selected Major Risk Factors. Geneva, Switzerland: World Health Organization; Klingemann H., Gmel G. Introduction. Social consequences of alcohol the forgotten dimension? In: Klingemann H., Gmel G., editors. Mapping of Social Consequences of Alcohol Consumption. Dordrecht, the Netherlands: Kluwer; 2001, p Room R., Rossow I. The share of violence attributable to drinking. J Subst Use 2001; 6: Hill L. The alcohol industry. In: Quar S., Heggenhougen H. K., editors. International Encyclopaedia of Public Health. London, UK: Elsevier; 2008, p Jernigan D. H. The global alcohol industry: an overview. Addiction 2009; 104 (Suppl. 1): Baumberg B. The Value of Alcohol Policies: a Review of the Likely Economic Costs and Benefits of Policies to Reduce Alcohol-Related Harm on the Global Level. Background Paper Prepared for the WHO Expert Committee on Problems Related to Alcohol Consumption (second report). Geneva: World Health Organization; Room R., Jernigan D., Carlini-Marlatt B., Gureje O., Mäkelä K., Marshall M. et al. Alcohol in Developing Societies: A Public Health Approach. Helsinki: Finnish Foundation for Alcohol Studies/World Health Organization; World Health Organization (WHO). WHO Expert Committee on Problems Related to Alcohol Consumption (second report). WHO Technical Report Series 944. Geneva: WHO; Anderson P., Baumberg B. Alcohol in Europe: A Public Health Perspective: A Report for the European Commission. Luxembourg: Institute of Alcohol Studies, European Communities; Österberg E., Karlsson T., editors. Alcohol Policies in EU Member States and Norway: A Collection of Country Reports. Helsinki, Finland: STAKES; Wagenaar A. C., Salois M. J., Komro K. A. Effects of beverage alcohol price and tax levels on drinking: a meta-analysis of 1003 estimates from 112 studies. Addiction 2009; 104: Anderson P., Chisholm D., Fuhr D. Effectiveness and costeffectiveness of policies and programmes to reduce the harm caused by alcohol. Lancet 2009; 373: Gruenewald P. J., Ponicki W. R., Holder H. D., Romelsjö A. Alcohol prices, beverage quality, and the demand for alcohol: quality substitutions and price elasticities. Alcohol Clin Exp Res 2006; 30: Toumbourou J. W., Stockwell T., Neighbors C., Marlatt G. A., Sturge J., Rehm J. Interventions to reduce harm associated with adolescent substance use. Lancet 2007; 369: Cook P. J. Paying the Tab: The Economics of Alcohol Policy. Princeton, NJ: Princeton University Press; Leppänen K., Sullström R., Suoniemi I. The Consumption of Alcohol in Fourteen European Countries: A Comparative Econometric Analysis. Helsinki: STAKES; The Author. Journal compilation 2010 Society for the Study of Addiction Addiction, 105,
91 778 Alcohol and Public Policy Group 26. Stockwell T., Chikritzhs T. Do relaxed trading hours for bars and clubs mean more relaxed drinking? A review of international research on the impacts of changes to permitted hours of drinking. Crime Prev Commun Saf 2009; 11: Livingston M., Chikritzhs T., Room R. Changing the density of alcohol outlets to reduce alcohol-related problems. Drug Alcohol Rev 2007; 26: Gruenewald P. J. The spatial ecology of alcohol problems: niche theory and assortative drinking. Addiction 2007; 102: Holder H. D., Kuhlhorn E., Nordlund S., Osterberg E., Romelsjo A., Ugland T. European Integration and Nordic Alcohol Policies. Changes in Alcohol Controls and Consequences in Finland, Norway and Sweden, Aldershot: Ashgate; Holder H., editor. Alcohol Monopoly and Public Health: Potential Effects of Privatization of the Swedish Alcohol Retail Monopoly. Stockholm: Swedish National Institute of Public Health; Voas R. B., Tippetts A. S. Relationship of Alcohol Safety Laws to Drinking Drivers in Fatal Crashes. Washington, DC: National Highway Traffic Safety Administration; Wagenaar A. C., Toomey T. L. Effects of minimum drinking age laws: review and analyses of the literature from J Stud Alcohol 2002; 63: S Graham K. Preventive interventions for on-premise drinking: a promising but underresearched area of prevention. ContempDrugProbl2000; 27: Lee K., Chinnock P. (2006) Interventions in the alcohol server setting for preventing injuries. Cochrane Database Syst Rev Issue 2. Art. no.: CD pub2. DOI: / CD pub Wallin E., Gripenberg J., Andréasson S. Overserving at licensed premises in Stockholm: effects of a community action program. J Stud Alcohol 2005; 66: Warburton A. L., Shepherd J. P. Tackling alcohol related violence in city centres: effect of emergency medicine and police intervention. Emerg Med J 2006; 23: Miller T. R., Lestina D. C., Spicer R. S. Highway crash costs in the United States by driver age, blood alcohol level, victim age, and restraint use. Accid Anal Prev 1998; 30: Wagenaar A. C., Maldonado-Molina M. Effects of drivers license suspension policies on alcohol-related crash involvement: long-term follow-up in forty-six states. Alcohol Clin Exp Res 2007; 31: Homel R. Random breath testing in Australia: getting it to work according to specifications. Addiction 1993; 88 (Suppl. 1): 27 33S. 40. Desapriya E. B. R., Shimizu S., Pike I., Subzwari S., Scime G. Impact of lowering the legal blood alcohol concentration limit to 0.03 on male, female and teenage drivers involved alcohol-related crashes in Japan. Int J Injury Control Saf Prom 2007; 14: Shults R. A., Elder R. W., Sleet D. A., Nichols J. L., Alao M. A., Carande-Kulis V. G. et al. and the Task Force on Community Preventive Services. Reviews of evidence regarding interventions to reduce alcohol-impaired driving. Am J Prev Med 2001; 21: Elder R. W., Shults R. A., Sleet D. A., Nichols J. L., Zaza S., Thompson R. S. Effectiveness of sobriety checkpoints for reducing alcohol-involved crashes. Traffic Injury Prev 2002; 3: Marques P. R. The alcohol ignition interlock and other technologies for the prediction and control of impaired drivers. In: Verster J. C., Pandi-Perumal S. R., Ramaekers J. G., de Gier J. J., editors. Drugs, Driving, and Traffic Safety. Basel: Birkhäuser; 2009, p Ditter S. M., Elder R. W., Shults R. A., Sleet D. A., Compton R., Nichols J. L. and the Task Force on Community Preventive Services. Effectiveness of designated driver programs for reducing alcohol-impaired driving: a systematic review. Am JPrevMed2005; 28: Zwerling C., Jones M. P. Evaluation of the effectiveness of low blood alcohol concentration laws for younger drivers. AmJPrevMed1999; 16 (Suppl. 1): Hartling L., Wiebe N., Russell K., Petruk J., Spinola C., Klassen T. P. (2004) Graduated driver licensing for reducing motor vehicle crashes among young drivers. Cochrane Database Syst Rev Issue 2. Art. no. CD DOI: / CD pub Casswell S. Alcohol brands in young peoples everyday lives: new developments in marketing. Alcohol Alcohol 2004; 6: Snyder L., Milici F., Slater M., Sun H., Strizhakova Y. Effects of advertising exposure on drinking among youth. Arch Pediatr Adolesc Med 2006; 160: Anderson P., de Bruijn A., Angus K., Gordon R., Hastings G. Impact of alcohol advertising and media exposure on adolescent alcohol use: a systematic review of longitudinal studies. Alcohol Alcohol 2009; 44: Booth A., Meier P., Stockwell T., Sutton A., Wilkinson A., Wong R. Independent Review of the Effects of Alcohol Pricing and Promotion. Part A: Systematic Reviews. Sheffield, UK: School of Health and Related Research, University of Sheffield; Available at: (2008) Publichealth/Healthimprovement/Alcoholmisuse/ DH_ (accessed 30 January 2009). 51. Perry C. L., Williams C. L., Veblen-Mortenson S., Toomey T. L., Komro K. A., Anstine P. S. et al. Project Northland: Outcomes of a community-wide alcohol use prevention program during early adolescence. Am J Pub Health 1996; 86: Foxcroft D. R., Ireland D., Lowe G., Breen R. 2002) Primary prevention for alcohol misuse in young people. Cochrane Database Syst Rev Issue 3. Art no. CD DOI: ? CD Johannessen K., Collins C., Mills-Novoa B., Glider P. A. A Practical Guide to Alcohol Abuse Prevention: A Campus Case Study in Implementing Social Norms and Environmental Management Approaches. Tucson, AZ: Campus Health Services, University of Arizona; Perkins H. W., Craig D. W. A Multifaceted Social Norms Approach to Reduce High-Risk Drinking: Lessons from Hobart and William Smith Colleges. Newton, MA: Higher Education Center for Alcohol and other Drug Prevention, Department of Education; Miller W. R., Brown J. M., Simpson T. L., Handmaker N. S., Bien T. H., Luckie L. F. et al. What works? A methodological analysis of the alcohol treatment outcome literature. In: Hester R. K., Miller W. R., editors. Handbook of Alcoholism Treatment Approaches: Effective Alternatives, 2nd edn. Boston, MA: Allyn and Bacon; 1995, p Whitlock E. P., Polen M. R., Green C. A., Orlean T., Klein J. Behavioral counseling interventions in primary care to reduce risky/harmful alcohol use by adults: a summary of the evidence for the US Preventive Services Task Force. Ann Intern Med 2004; 140: The Author. Journal compilation 2010 Society for the Study of Addiction Addiction, 105,
92 Alcohol: No Ordinary Commodity Finney J. W., Hahn A. C., Moos R. H. The effectiveness of inpatient and outpatient treatment for alcohol abuse: the need to focus on mediators and moderators of setting effects. Addiction 1996; 91: Anton R. F., O Malley S. S., Ciraulo D. A., Cisler R. A., Couper D., Donovan D. M. et al. for the COMBINE Study Research Group. Combined pharmacotherapies and behavioral interventions for alcohol dependence: the COMBINE Study: a randomized controlled trial. JAMA 2006; 295: Kranzler H. R., Van Kirk J. Naltrexone and acamprosate in the treatment of alcoholism: a meta-analysis. Alcohol Clin Exp Res 2001; 25: Ouimette P. C., Finney J. W., Gima K., Moos R. H. A comparative evaluation of substance abuse treatment: examining mechanisms underlying patient treatment matching hypotheses for 12-step and cognitive behavioral treatments for substance abuse. Alcohol Clin Exp Res 1999; 23: Anderson P. The beverage alcohol industry s social aspects organizations: a public health warning. Addiction 2005; 99: International Center for Alcohol Policies (ICAP). The Structure of the Beverage Alcohol Industry. ICAP Report 17. Washington, DC: ICAP; Bakke O., Endal D. Alcohol policies out of context: drinks industry supplanting government role in alcohol policies in sub-saharan Africa. Addiction 2010; 105: Stenius K., Babor T. F. The alcohol industry and public interest science. Addiction 2010; 105: The Author. Journal compilation 2010 Society for the Study of Addiction Addiction, 105,
93 bs_bs_banner FOR DEBATE doi: /add A critical first assessment of the new pre-market approval regime for new psychoactive substances (NPS) in New Zealand Chris Wilkins Social and Health Outcomes Research and Evaluation (SHORE), SHORE and Whariki Research Centre, School of Public Health, Massey University, Auckland, New Zealand ABSTRACT Background New Zealand has recently attempted to address the underlying drivers of the escalating new psychoactive substances (NPS) ( legal highs ) problem by establishing the world s first pre-market approval regulatory regime for NPS. NPS products which can be shown with clinical trial data to pose a low risk of harm will be approved for legal manufacture and sale. Aims and method This paper critically assesses the new regime, drawing on experience of the pharmaceutical sector and legal BZP market. Findings A number of characteristics of the recreational use of NPS may not be well addressed by standard medical clinical trials, including binge use, polydrug use, use by vulnerable groups and high-risk modes of administration. The overt advertising and covert promotion of approved NPS products on the internet may make them fairly visible to young people. The black market for unapproved NPS may be difficult to suppress given that unapproved NPS will be physically identical to approved NPS. If the legal market for NPS encourages the use of NPS, alcohol and other drugs there may be an increase in drug-related harm. Alternatively, if the legal NPS market reduces the use of more harmful drugs, there may be a considerable public health benefit. Conclusions The clinical trials required for NPS products should address the characteristics of recreational NPS use. Enforcement resources and technical solutions are required to clearly distinguish legal NPS products. The impact the new NPS regime has on other drug use is a key issue and demands further study. Keywords Drug policy, legal drug market, legal highs, new psychoactive substances (NPS), New Zealand, Psychoactive Substances Act Correspondence to: Chris Wilkins, SHORE and Whariki Research Centre, PO Box 6137, Wellesley Street, Auckland 1010, New Zealand, c.wilkins@massey.ac.nz Submitted 11 September 2013; initial review completed 17 October 2013; final version accepted 7 January 2014 INTRODUCTION A growing number of new or previously obscure psychoactive compounds have emerged over the past 5 years or so, with many sold as so-called legal highs [1 4]. Collectively, they have been termed new psychoactive substances (NPS), and encompass a range of compound classes [5]. They are commonly marketed as legal substitutes for existing illegal drugs, largely because the active compounds are not covered by international drug treaties, although their domestic legal status is often more complex [6]. The policy approach to NPS around the world to date has overwhelmingly been to attempt to prohibit them [7,8]. However, this has proved to be problematic due to the very large number of NPS compounds, the financial cost associated with identifying active ingredients, the slowness of the legislative process to prohibit individual compounds and the speed at which manufacturers can replace newly prohibited compounds with uncontrolled ones [9]. This has led many countries to seek faster means to prohibit psychoactive compounds (i.e. emergency scheduling), adopt broader legislative definitions of psychoactive compounds (i.e. analogue or generic laws) or subject NPS to more nimble regulatory regimes, such as those that apply to medicines or public health [10 13]. Some have argued that these responses do not address the underlying drivers of the NPS problem [9,14]. The onus remains on the government to identify new NPS products, carry out expensive testing and assess the case for scheduling. Meanwhile, the product is free to be 2014 Society for the Study of Addiction Addiction
94 2 Chris Wilkins sold without any restrictions or reliable consumer information, and legal high manufacturers face ongoing incentives to introduce new, possibly more harmful, replacement NPS compounds to replace the ones about to be prohibited. Faster, more comprehensive bans of NPS compounds and commercial activity also raise questions about the arbitrary use of government power (i.e. NPS banned without any prior harm assessment), the proportionality of response (i.e. criminal penalties for NPS that may be less harmful that existing legal drugs) and the banning of whole classes of compounds which may potentially have legitimate uses in other areas [9,14,15]. The New Zealand Government has recently attempted to address these issues by developing the world s first premarket approval regulatory regime for NPS, broadly similar to the regimes which commonly operate for medicines [16,17]. Under the new approach, NPS products which can be shown to pose a low risk of harm will be approved for legal manufacture and sale. Proponents of this approach argue that it will place the onus on manufacturers to show that NPS products are safe in advance of sale, remove high-risk NPS products from legal sale, require the industry rather than the government to bear the financial costs of testing products and subject NPS products to a range of retail restrictions [18,19]. Some proponents have also argued that a regulated legal market for NPS will draw demand away from more harmful illegal drugs. The New Zealand approach has attracted international interest [20], and has even been proposed as a future model for the control of illegal drugs, such as cannabis [21]. The new NPS regime was established with the enactment of the Psychoactive Substances Act (PSA) in mid- July As of December 2013, the regime remains in a transitional phase while supplementary regulations are developed, and no NPS product is yet to be approved. Consequently, aspects of the regime are yet to be fleshed out, and no market for approved NPS is currently available for empirical evaluation. Nevertheless, based on the framework outlined in the PSA, it is possible to raise a number of questions about how effective the new regime will be at addressing the ongoing issues with NPS. This paper discusses these concerns with particular reference to the pharmaceutical sector and the extensive legal market for benzylpiperazine (BZP) party pills which operated in New Zealand from 2000 to 2008 [22,23]. BZP is a piperazine-based central nervous system stimulant with approximately 10% the potency of dexamphetamine [24 27]. An estimated legal BZP pills were sold each month in New Zealand until BZP was prohibited in 2008, generating retail sales of $24 million ($NZ) per year (NZ1$ = $US0.81 = 0.60) [28]. THE PSYCHOACTIVE SUBSTANCE ACT 2013 The PSA creates a regulatory framework whereby NPS products which can be shown with preclinical and clinical trial data to pose no more than a low risk of harm will be approved for legal manufacture and sale subject to regulatory standards [17,29,30]. Product sponsors are responsible for conducting and paying for the required product testing [15] and must also pay an application fee of $NZ per product [31]. A separate application and related test data are required for each finished product, rather than a particular compound, to ensure that testing takes into account the mix and strength of active ingredients and the mode of administration [29,30]. Approved NPS products will be sold subject to a range of retail restrictions, including a minimum purchase age of 18 years and no sales from convenience stores or those that sell alcohol or automobile fuels [18,30]. The advertising of approved NPS products is limited to the pointof-sale only (i.e. no advertising in television, radio or newspapers), must not be visible or audible from outside of premises, must not include themes that are appealing to minors and be limited to objective information about the product and price [18,30]. All NPS products must include a list of ingredients, health warnings and the contact details of the National Poisons Centre [30]. HOW WILL THE STANDARD OF LOW RISK BE APPLIED TO NPS PRODUCTS? The concept of low risk as applied to NPS The PSA establishes low risk as the criteria for product approval [30], but does not include any definition of low risk. The government has previously acknowledged that low risk is not the same as no risk, and some people may be particularly sensitive to specific NPS [15,31]. To this end, the PSA specifically prohibits sellers from advertising an approved product as safe [30]. The experience with BZP legal highs supports this caution. While the vast majority of users reported moderate adverse effects from BZP [22,32], a small number appeared to experience lifethreatening reactions [33]. The question is: how will such a skewed distribution of harm among users be fitted into an overall concept of low risk? Furthermore, what legal recourse will be available to the small number who suffer severe reactions from a government-approved low risk product? NPS harms that cannot be identified in advance of approval Following public concern about the lack of a definition of low risk, six principles were inserted into the PSA 2014 Society for the Study of Addiction Addiction
95 A critical assessment of the new NPS regime in New Zealand 3 which were now required to be considered when evaluating an NPS product (i.e. the toxicological effects, risk to public health, potential to cause death, potential to create dependence, likelihood of misuse and appeal to vulnerable populations ) [30]. There is no guidance in the PSA concerning where in these harm categories the low risk threshold is to be found. Perhaps, more importantly, it seems that many of these risks will only be able to be fully determined after a product is approved and widely used. THE LIMITATIONS OF CLINICAL TESTING AT MINIMIZING NPS HARM A central rationale of the new regime is that by subjecting NPS products to clinical trials and only approving low-risk products it will reduce NPS-related harm [17,21,30]. The clinical tests required for an NPS product have been described previously as broadly similar to those for new medicines [17]. Details of the testing have not been included in the PSA; instead, this task has been left to the regulator. There is no indication as to whether these tests will be required to meet international standards for medicines. The New Zealand Ministry of Health have previously estimated that the cost of testing an NPS product is likely to be NZ$1 2 million per product [15]. However, toxicology testing of an inhalation product under current international pharmaceutical regulation has recently been estimated to cost over ([34], p.78) Assessing all the risks of an NPS product may prove to be challenging, given that the compounds will often be entirely novel [16]. There are a number of further reasons to question whether standard medical clinical trials will be able to fully identify the risks from the recreational use of NPS. High consumption episodes The first complication is that clinical trials of medicines largely examine the side effects of a medicine at the recommended dose [35]. In contrast, recreational drugs are often used during hedonistic social gatherings, which can involve high consumption episodes. The mean number of legal BZP party pills taken on a typical occasion by respondents to a general population survey was 2.6 pills. On an occasion of greatest use, 42% had taken four or more pills, 20% six or more pills and 11% eight or more pills [36]. The dose commonly recommended on partypill product packaging was one to two pills per session [23]. In the same survey, the interviewer explained that binge use of BZP party pills was defined as using BZP continuously for 24 hours or more. Seventeen per cent of those who had used BZP in the previous year reported that they had binged on BZP in this way, with 19% of those having done so 10 or more times in the past year [36]. In a study of BZP use by young people, the legality of BZP party pills was interpreted by young people as indicative that party pills were safe and low strength, beliefs likely to encourage high consumption episodes [23,37]. Polydrug use A second complication is that clinical trials examine the medicine in question in isolation. In contrast, NPS are often used in combination with other legal and illegal psychoactive substances. A national population survey of legal BZP use found that 86% of BZP users combined their use of BZP with another substance [32]. The most popular combinations were alcohol (91%), tobacco (40%), cannabis (22%), 5-HTP (5-hydroxytryptophan) (9%) and ecstasy (5%) [32]. In subsequent analyses, the simultaneous consumption of BZP with cannabis and 5-HTP were both found to increase the risk of adverse effects [32]. Vulnerable populations As NPS products do not purport to address any illness, clinical trials of NPS products are likely to involve healthy young people under supervised conditions. However, we know that the risks of recreational drug use increase when users are from vulnerable groups such as risktaking adolescents, those who are at risk of mental illness and those already dependent on alcohol and drugs. Some synthetic cannabis products have been found to precipitate psychotic symptoms among people with pre-existing risk factors [38 40]. BZP legal highs were surprisingly popular among illegal drugs users in New Zealand. For example, 44% of the frequent methamphetamine users interviewed for a drug monitoring study had used a BZP legal high in 2006 [41]. High-risk modes of administration The health risk of an NPS product will be exacerbated further by risky modes of administration, such as smoking and intravenous use (which may be different from the recommended mode). The injection of mephedrone has been reported in a number of countries with adverse consequences [42]. In New Zealand, 34% of frequent injecting drug users had used a BZP legal high in 2007, of whom 76% had injected it [41]. Long-term adverse effects While toxicology and clinical trials may well be effective at identifying acute risks from an NPS product, establishing long-term effects is considerably more challenging. It is accepted in medicine that even with clinical trials 2014 Society for the Study of Addiction Addiction
96 4 Chris Wilkins some medicines will be approved that are subsequently found to have unforeseen side effects ([43,44], p.151). This is largely because the number of participants in a clinical trial is often too small to identify rare side effects, and trials do not last long enough to identify longer-term effects ([43,44], p.151). A clinical trial may also not identify side effects if they only appear in groups of people different from those in the trial, or if it is a side effect that the study was not designed to look for [35]. THE CHALLENGE OF POST-APPROVAL MONITORING OF NPS PRODUCTS Even after a new medicine has been approved, the patients for whom it is prescribed continue to be monitored for adverse effects (i.e. known as pharmacovigilance) (see [43]). The PSA requires licence holders to report adverse effects from an approved NPS product, and the regulator has the power to withdraw a product [30]. There are a number of instances where pharmacovigilance may fail to identify problems from a medicine, including instances of rare side effects, common complaints which can be easily associated with other illnesses, long time-frames between use and adverse effects and the low profile of a medicine ([44], pp ). Pharmacovigilance may be particularly challenging for NPS, as NPS products will often be combined with alcohol and other drugs, and the resulting hang-over effect may reduce reporting of complaints and complicate further the process of isolating side effects to a specific product. Pharmaceutical companies also have clear obligations to report side effects from their medicines, but in a number of notorious cases (e.g. paroxetine) they failed to do so, with serious health consequences [35,44]. The risk of approving a new medicine is justified on the basis that patients are expected to receive some therapeutic benefit which offsets the risks of side effects [43]. There is no such therapeutic benefit with NPS products, and some commentators have objected to the testing of NPS products on animals for this very reason [45]. However, the new NPS regime could be said to have social benefits, including providing low-risk alternatives to existing drugs and breaking the cycle of the continual introduction of new NPS. WHAT IMPACT WILL THE LEGAL MARKET FOR APPROVED NPS HAVE ON NPS, ALCOHOL AND OTHER DRUG USE? While the new approval process may reduce the health risk of legally available NPS products, any resulting reduction in per unit harm may be offset by any increase in the prevalence of NPS use. Approved NPS products will be certified by the government as low risk, and will be manufactured and sold under government regulatory standards. As a consequence, many people are likely to perceive them as safer and more legitimate than previous products. Perceptions of health risk and social stigma have been found to be important predictors of drug use among young people [46,47]. Legal status, health risk and social stigma have been found to be particularly influential at preventing drug use among more conventional social groups [48 50]. It is also possible that the market for approved NPS will encourage demand for alcohol, tobacco or other drugs if these substances are used in combination with or to mitigate adverse effects from approved NPS use, with a resulting increase in drug-related harm [51]. Alternatively, the market for approved NPS may diminish other drug use if users substitute more harmful substances for NPS, and thereby reduce harm. Indeed, if the availability of approved NPS resulted in reductions in smoking and methamphetamine use, for example, there may be substantial public health gains. HOW EFFECTIVE WILL ADVERTISING RESTRICTIONS OF APPROVED NPS BE? Advertising on dedicated websites As outlined earlier, the PSA restricts the advertising of approved NPS products to the point-of-sale only, and imposes a range of restrictions on advertising at physical locations. However, the PSA permits sales of approved NPS from internet websites set up specifically to sell approved products [30], and consequently advertising is permitted from these sites [30]. Legal highs are sold commonly from websites around the world, and this has been an important driver in their spread [52 54]. The number of online shops selling NPS in Europe increased from 170 in 2010 to 693 in 2012 [55]. Covert promotion on the internet The PSA explicitly prohibits the advertising of approved NPS from the wider internet (i.e. websites not dedicated to selling NPS) but, as has been noted, this is likely to be extremely difficult to enforce [56]. Websites can be hosted in other countries and accessed in New Zealand, a problem which has been encountered with the on-line selling of pharmaceuticals [44]. The internet offers an array of covert ways to promote approved NPS products outside traditional advertising, including utilizing social networking sites and personal blogs. The pharmaceutical industry has developed many covert strategies to market their products despite restrictions on direct-to-consumer advertising in most countries [35,44] Society for the Study of Addiction Addiction
97 A critical assessment of the new NPS regime in New Zealand 5 Age restrictions on dedicated websites The PSA sets a minimum purchase and supply age of 18 years or older for approved NPS products. It is not clear how this age restriction will be enforced in the case of website sales. Will people simply be asked to click a button confirming that they are the required age? TO WHAT EXTENT WILL THE NEW NPS REGIME SUPPRESS THE MARKET FOR UNAPPROVED NPS? An implicit assumption of the new regime is that once the regulated NPS market is established, the vast majority of NPS purchases will be made from the legal market. However, unapproved NPS may be cheaper (as they do not have to comply with the new regulations), be more powerful (as they do have to be low risk) and be perceived as more attractive (as they retain the forbidden fruit appeal) than their approved counterparts. Conversely, approved NPS products have the advantage of legal status, convenience of purchase and some guarantee of safety and quality. To suppress the black market for unapproved NPS, the authorities must be prepared to commit sufficient resources to test imports of chemicals, products available for sale and those found in possession of users. As unapproved NPS will essentially be physically identical to approved NPS (i.e. coloured powders pressed into tablets), particularly when on the outside of packaging, this may be a challenge. Police have, in theory, the power to impose an instant fine for the possession of an unapproved NPS product and confiscate personal supplies [30], but it will be impossible for officers to identify unapproved NPS on the street without further laboratory testing. Legal high manufacturers in New Zealand have already complained of counterfeits undermining the reputation of the legal market. The practical and financial difficulties of identifying unapproved NPS products may mean that those who persist with using unapproved products will largely go unpunished. CONCLUSIONS We have identified a number of characteristics of the recreational use of NPS which may not be well addressed by a standard medical clinical trial. These limitations could be addressed by extending clinical trials for NPS to include the harms from excessive use, polydrug use, risky means of administration and use by vulnerable people. The impact the legal market for approved NPS has on the use of NPS, alcohol and other drugs is a key issue [51]. Depending on whether NPS are substitutes, or complements for other drugs, the new regime could confer considerable public health benefits or additional total harm. This pivotal issue will only be able to be investigated once a market for approved NPS is established. It is entirely possible that different NPS products will have different influences on other drug use (e.g. synthetic cannabis a substitute for cannabis, BZP a complement for alcohol), and this may change over time and be different in different country contexts [57]. The authorities may face challenges in suppressing the black market for unapproved NPS, given that unapproved NPS will look exactly like their approved counterparts. If people can continue to use unapproved NPS products largely without penalty then this will undermine the legal market. There is a chance that legally approved NPS products will simply be more popular. However, unapproved products may be able to offer unique attractions. The task of identifying unapproved NPS products could be enhanced with the development of sophisticated product labelling (e.g. hologram watermarks) and real-time testing technology. A simple confirmatory test could be used to identify approved compounds. Those products which fail would be confiscated and subjected to further more in-depth testing. Supporters of the pre-market approach to NPS may counter that, although the new framework is not perfect at reducing NPS harm, it offers an improvement on the existing unregulated de-facto legal market. However, such a stark policy dichotomy is somewhat misleading. A range of more comprehensive prohibition responses to NPS have emerged in recent years (e.g. generic and emergency scheduling, prohibition of the retail sale of NPS) which are yet to be evaluated [12,13,58]. An evaluation of the prohibition of BZP in New Zealand suggested that the prohibition greatly reduced BZP use, and subsequent levels of replacement legal high use did not match the previous levels of BZP [59]. There are also examples in other countries of prohibition being effective at reducing legal high use [58,60,61]. The application of civil regulatory regimes for medicines, public health and consumer protection to NPS are also yet to be evaluated empirically [11,62]. In New Zealand, the authorities appeared to have reduced the use of nitrous oxide legal highs by simply writing to retailers and pointing out that nitrous oxide is a restricted medicine [59]. More nimble civil regulatory regimes may be able to rapidly address NPS availability without direct resort to either criminal penalties or to creating a new commercial drug industry [51,59,63]. A pressing task for researchers is to provide empirical evaluations of these different approaches to inform future policy responses. Declaration of interests None Society for the Study of Addiction Addiction
98 6 Chris Wilkins References 1. Griffiths P., Sedefov R., Gallegos A., Lopez D. How globalization and market innovation challenge how we think about and respond to drug use: Spice, a case study. Addiction 2010; 105: European Monitoring Centre for Drugs and Drug Addiction (EMCDDA) Annual report on the state of the drugs problem in Europe. Lisbon: European Monitoring Centre for Drugs and Drug Addiction, United Nations Office on Drugs and Crime (UNODC). The challenge of new psychoactive substances. United Nations Office on Drugs and Crime, Available at: (accessed 30 January 2014) (Archived at on 29 January 2014). 4. Davis G. Drug abuse newly emerging trends. Clin Lab Med 2012; 32: European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). New drugs and emerging trends. Annual report 2011: The state of the drugs problem in Europe. Luxembourg: Publications Office of the European Union; 2011: Ramsey J., Dargan P., Smyllie M., Davies S., Button J., Holt D. et al. Buying legal recreational drugs does not mean that you are not breaking the law. Q J Med 2010; 103: Reuter P. Options for regulating new psychoactive drugs: a review of recent experiences: UK Drug Policy Commission (UKDPC). London: UKPDC, Coulson C., Caulkins J. Scheduling of newly emerging drugs: a critical review of decisions over 40 years. Addiction 2011; 106: doi: /j x 9. New Zealand Law Commission. Controlling and Regulating Drugs a Review of the Misuse of Drugs Act Wellington: New Zealand Law Commission; European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). EU Drug Markets Report A Strategic Analysis. Lisbon: European Monitoring Centre for Drugs and Drug Addiction, Hughes B., Winstock A. Controlling new drugs under marketing regulations. Addiction 2012; 107: Hughes B., Connolly J. Ireland passes new law to control head shops and legal highs. DrugNet Europe [serial on the internet]. 2010; 72: 5. Available at: (accessed 13 February 2014) (Archived at on 12 February 2014). 13. Hughes B., Malczewski A. Poland passes new law to control head shops and legal highs. Drugnet Europe [serial on the internet]. 2011; 73: 5. Available at: article12 (accessed 13 February 2014) (Archived at on 12 February 2014). 14. Ministry of Health. Regulatory Impact Statement Government Response to the Law Commission s Report Controlling and Regulating Drugs a review of the Misuse of Drugs Act Wellington: Ministry of Health; 2011, September. 15. Dunne P. Drug law reversing onus of proof on way. 16 July; Available at: drug-law-reversing-onus-proof-way (accessed 24 July 2012) (Archived at on 12 February 2014). 16. Wilkins C., Sheridan J., Adams P., Russell B., Ram S., Newcombe D. The new psychoactive substances regime in New Zealand: a different approach to regulation. J Psychopharmacol 2013; 27: Office of the Associate Minister of Health and Cabinet Social Policy Committee. Regulation of psychoactive substances. Wellington, New Zealand; New Zealand Government Reports. Available at: files/documents/pages/psychoactive_substances-cab-paper _.pdf (accessed 30 January 2014) (Archived at on 29 January 2014). 18. Ministry of Health. Regulatory Impact Statement new regulatory regime for psychoactive substances. Wellington: Ministry of Health; 2012, October. 19. McClay T. Psychoactive Substances Bill Third Reading. Hansard (debates) [serial on the internet]. 2013, 11 July; 692: Available at: psychoactive-substances-bill-%e2%80%94-third-reading (accessed 13 February 2014). 20. Meacher M. Drug policy reform the opportunity presented by legal highs. Psychiatrist 2013; 37: Lees-Galloway I. Psychoactive Substances Bill. Hansard (debates) [serial on the internet]. 2013, 9 April; 689: Available at: debates/50hansd_ _ /psychoactive -substances-bill-%e2%80%94-first-reading (accessed 13 February 2014). 22. Wilkins C., Girling M., Sweetsur P. The prevalence of use, dependency and harms of legal party pills containing benzylpiperazine (BZP) and trifluorophenylmethylpiperazine (TFMPP) in New Zealand. J Subst Use 2007; 12: Sheridan J., Butler R., Wilkins C., Russell B. Legal piperazine-containing party pills a new trend in substance misuse. Drug Alcohol Rev 2007; 26: Bye C., Munro-Faure A., Peck A., Young P. A comparison of the effects of l-benzylpiperazine on human performance tests. Eur J Clin Pharmacol 1973; 6: Campbell H., Cline W., Evans M., Lloyd J., Peck A. Comparison of the effects of dexamethamphetamine and l-benzylpiperazine in former addicts. Eur J Clin Pharmacol 1973; 6: Antia U., Lee H., Kydd R., Tingle M., Russell B. Pharmacokinetics of party pill drug N-benzylpiperazine (BZP) in healthy human participants. Forensic Sci Int 2009; 186: Lin J., Bangs N., Lee H., Kydd R., Russell B. Determining the subjective and physiological effects of BZP on human females. Psychopharmacologia 2009; 207: Wilkins C., Sweetsur P. Differences in harm from legal BZP/TFMPP party pills between North Island and South Island users in New Zealand: a case of effective industry self regulation? Int J Drug Policy 2010; 21: Ministry of Health. Regulatory Impact Statement New regulatory regime for psychoactive substances. Wellington, New Zealand: Ministry of Health; 2012, July. 30. New Zealand Parliament. Psychoactive Substances Act 2013, Public Act 2013 No 53 (2013, 17 July). Available at: DLM html (accessed 30 January 2014) (Archived at on 29 January 2014) Society for the Study of Addiction Addiction
99 A critical assessment of the new NPS regime in New Zealand Office of the Associate Minister of Health, Cabinet Social Policy Committee. Regulation of Psychoactive Substances further policy decisions. Wellington; 2012, October. Cabinet Paper. Available at: files/documents/pages/cabinet-paper-psychoactive -substances-further-decisions.doc (accessed 30 January 2014) (Archived at 6Mzq8uEAI on 29 January 2014). 32. Wilkins C., Sweetsur P., Girling M. Patterns of benzylpiperazine/ trifluoromethylphenylpiperazine (BZP/ TFMPP) party pill use and adverse effects in a population sample in New Zealand. Drug Alcohol Rev 2008; 27: Gee P., Richardson S., Woltersdorf W., Moore G. Toxic effects of BZP-based herbal party pills in humans: a prospective study in Christchurch, New Zealand. NZ Med J [serial on the internet] 2005; 118: U Muller L., Husar E. Preclinical safety testing. In: Griffin J. P., Posner J., Barker G. R., editors. The Textbook of Pharmaceutical Medicine, 7th edn. Oxford: John Wiley & Sons, Ltd; 2013, pp Angell M. The Truth about Drug Companies: How They Deceive Us and What to Do about It. New York: Random House; Wilkins C., Girling M., Sweetsur P., Huckle T., Huakau J. Legal Party Pill Use in New Zealand: Prevalence of Use, Availability, Health Harms and Gateway Effects of Benzylpiperazine (BZP) and Triflourophenylmethylpiperazine (TFMPP). Auckland: Centre for Social and Health Outcomes Research and Evaluation (SHORE) and Te Ropu Whariki, Massey University; 2006, June. 37. Sheridan J., Butler R. They re legal so they re safe, right? What did the legal status of BZP-party pills mean to young people in New Zealand? Int J Drug Policy 2010; 21: Every-Palmer S. Warning: legal synthetic cannabinoidreceptor agonists such as JWH-018 may precipitate psychosis in vulnerable individuals. Addiction 2010; 105: Hermanns-Clausen M., Kneisel S., Szabo B., Auwärter V. Acute toxicity due to the confirmed consumption of synthetic cannabinoids. Addiction 2013; 108: Glue P., Al-Shaqsi S., Hancock D., Gale C., Strong B., Schep L. Hospitalisation associated with use of the synthetic cannabinoid K2. NZ Med J 2013; 126: Wilkins C., Sweetsur P., Smart B., Warne C., Jawalkar S. Recent Trends in Illegal Drug Use in New Zealand: Findings from the 2006, 2007, 2008, 2009, 2010 and 2011 Illicit Drug Monitoring System (IDMS). Auckland: SHORE and Whariki Research Centre, Massey University; Van Hout M., Bingham T. A costly turn on : patterns of use and perceived consequences of mephedrone based head shop products amongst Irish injectors. Int J Drug Policy 2012; 23: Härmark L., van Grootheest A. Pharmacovigilance: methods, recent developments and future perspectives. Eur J Clin Pharmacol 2008; 64: Goldacre B. Bad Pharma: How Drug Companies Mislead Doctors and Harm Patients. London: Fourth Estate; Hague K., Kevin Hague speaks on the committee stage of the Psychoactive Substances Bill. Green Party; Available at: debates/50hansd_ _ /psychoactive -substances-bill- -in-committee (accessed 30 January 2014) (Archived at 6MzshVu70 on 29 January 2014). 46. Bachman J., Johnston L., O Malley P., Humphrey R. Explaining the recent decline in marijuana use: differentiating the effects of perceived risks, disapproval, and general lifestyle factors. J Health Soc Behav 1988; 29: Bachman J., Johnston L., O Malley P. Explaining the recent decline in cocaine use among adults: further evidence that perceived risks and disapproval lead to reduced drug use. J Health Soc Behav 1990; 31: Weatherburn D., Jones C., Donnelly N. Prohibition and cannabis use in Australia: a survey of year olds. Aust NZ J Criminol 2003; 36: MacCoun R. Drugs and the law: a psychological analysis of drug prohibition. Psychol Bull 1993; 113: MacCoun R. Estimation of the Non-Price Effects of Legalization on Cannabis Consumption. Santa Monica, CA: RAND; Wilkins C. A paradigm shift in recreational drug use: the challenge of legal highs in New Zealand [Letter]. NZ Med J 2011; 124: Griffiths P., Evans-Brown M., Sedefov R. Getting up to speed with the public health and regulatory challenges posed by new psychoactive substances in the information age. Addiction 2013; 108: Hillebrand J., Olszewski D., Sedefov R. Legal highs on the internet. Subst Use Misuse 2010; 45: Psychonaut Web Mapping Research Group. Psychonaut Web Mapping Project: final report. London: Institute of Psychiatry, King s College London, European Monitoring Centre for Drugs and Drug Addiction (EMCDDA). New drugs and emerging trends. Annual report 2012: The state of the drugs problem in Europe. Luxembourg: (European Monitoring Centre for Drugs and Drug Addiction), Publications Office of the European Union; 2012: Health Select Committee. Psychoactive Substances Bill. Wellington, New Zealand: House of Representatives, Perrone D., Helgesen R. D., Fischer R. G. United States drug prohibition and legal highs: how drug testing may lead cannabis users to Spice. Drugs Educ Prev Policy 2013; 20: United Nations Office on Drugs and Crime (UNODC). World Drug Report Vienna: United Nations Office on Drugs and Crime; Wilkins C., Sweetsur P. The impact of the prohibition of BZP legal highs on the prevalence of BZP, new legal highs and other drug use in New Zealand. Drug Alcohol Depend 2013; 127: Loeffler G., Craig C. The effect of legal bans on poison control center contacts regarding legal highs. Addiction 2013; 108: Stogner J., Khey D., Griffin O. 3rd, Miller B., Boman J. 4th. Regulating a novel drug: an evaluation of changes in use of Salvia divinorum in the first year of Florida s ban. IntJDrug Policy 2012; 23: Winstock A., Ramsey J. Legal highs and the challenges for policy makers. Addiction 2010; 105: Winstock A., Wilkins C. Legal highs The challenge of new psychoactive substances. Amsterdam: Transnational Institute (TNI), Series on Legislative Reform of Drug Policies no Society for the Study of Addiction Addiction
100 POLICY CASE STUDIES doi: /j x Current status of alcohol marketing policy an urgent challenge for global governanceadd_ Sally Casswell SHORE (Social and Health Outcomes Research and Evaluation), SHORE and Whariki Research Centre, School of Public Health, Massey University, Auckland, New Zealand ABSTRACT Aims To review research literature and available information on the extent and impacts of marketing, current policy response and the interests engaged in the policy debate in order to inform recommendations for policy change on alcohol marketing. Methods Relevant literature, including systematic reviews and publicly available information (websites and participant observation) is reviewed and synthesized. Results Alcohol marketing has expanded markedly in the past 50 years and, while there remains uncertainty about the impact across the population, there is now clear evidence of its impact on the consumption of young people. Few countries have effective policy in place restricting alcohol marketing, and there is a lack of an international response to alcohol marketing which crosses national boundaries. The protection of alcohol marketing has been a major focus for vested interest groups and this has affected governmental response at national and international levels. There has been a lack of non-governmental organization engagement. The policy response to tobacco marketing provides a clear contrast to that of alcohol marketing policy and provides a model for alcohol marketing policy. Conclusion The global exposure of young people to alcohol marketing requires an urgent policy response. The Framework Convention on Tobacco Control provides an appropriate model for global governance to control alcohol marketing. There are extant examples of national level legislation achieving comprehensive bans with France s Loi Evin providing a feasible model. Resources from philanthropic organizations to allow non-governmental organization engagement are urgently required, as is engagement by the governmental sector independent of commercial influence. Keywords Alcohol, alcohol marketing, alcohol policy, framework convention, global governance, review. Correspondence to: Sally Casswell, Centre for Social and Health Outcomes Research and Evaluation (SHORE), Massey University, PO Box 6137, Wellesley Street, Auckland 1141, New Zealand. s.casswell@massey.ac.nz Submitted 22 March 2011; initial review completed 9 May 2011; final version accepted 17 October 2011 INTRODUCTION The issue of alcohol marketing provides a new challenge for the policy arena, in contrast with controls on supply and price, which have been policy tools for millennia. The consolidation and expansion of the alcohol industry, particularly marked over the last two decades, resulted in regular surplus profits which have been ploughed back into what the industry refers to as investment behind brands : marketing to enhance consumers affiliation with particular brands [1]. This expansion of financial resource and marketing skill, a consequence of the consolidation of the global alcohol market, has combined with major technological developments, dramatically increasing the marketing modes available and the sophistication and dispersed nature of the marketing being carried out [2]. It is now estimated that about two-thirds of alcohol marketing is carried out in new media [3]. These are over and above the use of the more traditional and measured media such as television, radio, print and billboards. Alcohol is one of the most heavily marketed products in the world [2]. Alcohol marketing goes beyond national boundaries: it is present on the internet, with company websites providing interactive environments and the dissemination of marketing materials via social networking on the web [4]. Branded screensavers for computers and cellphones are available for download [5,6]. Product placement in films and music [7,8] and the organization of branded events (e.g. Hennessy parties in Asia) are other important 2012 The Author, Addiction 2012 Society for the Study of Addiction Addiction, 107,
101 Current status of alcohol marketing policy 479 marketing tools of global alcohol brands. The media coverage of sponsorship leads to global branding of sports events, despite national efforts to restrict it [9]. These expansions and technological developments occurred at a time when global governance became influenced strongly by the neoliberal ideology that the free market (in all products) was a primary aim, and this undoubtedly contributed to the current lack of adequate alcohol marketing policy. There has been an expansion of alcohol into emerging markets, those with young populations and growing economics and also into the unsaturated segments of the mature markets, women and children in particular [10]. The level of harm recorded in the estimates of disabilityadjusted life years (DALYs) put alcohol on a par with tobacco, and estimates suggest that in high- and middleincome countries more than 1% of gross domestic product purchasing power parity (GDP PPP) is spent on economic costs attributable to alcohol [11]. This makes the lack of control on the marketing of this product an urgent focus for policy action. IMPACTS OF MARKETING The public health research field has struggled to keep up with the speed and extent of these changes in alcohol marketing. For many years the received wisdom in the alcohol research and policy field was that the research on alcohol marketing was inconsistent, with little evidence of effects (e.g. [12]). In part this was a consequence of an early methodological emphasis: on econometric analysis using expenditure on advertising in the measured media (as a proxy for marketing exposure) and relating this to consumption at the population level; and on analysis, at the population level of restrictions (many of them partial) on advertising [10]. While this line of research remains active (e.g. [13]), critiques of this research [3] and a new body of research focused on the impact of marketing among young people and using a range of methodologies, including importantly longitudinal designs [14], structural equation modelling of cross-sectional survey data [15 17] and investigation of naturally occurring regional differences in exposure [18,19], have achieved a major shift in the consensus held by public health researchers. While there is lack of evidence at the population level, the effects of alcohol marketing on the drinking of younger people, with whom most of the research has been carried out, are now widely acknowledged [10,20]. The newer body of alcohol marketing research has reflected a more nuanced understanding of the way in which marketing has its impacts and the size of these. Discourse analysis has revealed how people engage with marketing materials, making meaning in collaboration with their peers, in a wraparound complex of messages about alcohol-mediated fun/cool identity, creating and maintaining what has been described as an intoxigenic environment [21]. The way in which the industry strategically feeds off and builds upon youth culture in the design of marketing campaigns communicating beverage potency, drunkenness and sexual and social success has been documented following the recent disclosure of internal alcohol industry advertising documents [22]. Quantitative methodologies have documented that exposure to alcohol marketing increases positive beliefs about alcohol [23,24], affects young peoples perceptions of how much their friends drink [25] and increases the likelihood of young people drinking and how much they consume when they do drink [14]. Comparison of drinking by young people in US markets with different levels of exposure suggested that each additional dollar spent per capita raised the number of drinks consumed by 3% [18]. Lessons might also be drawn from the numerous case studies of relatively extensive restrictions on tobacco marketing which have accompanied the development of the Framework Convention on Tobacco Control (FCTC). Comprehensive restrictions on tobacco marketing resulted in a decline of 7.4% in cigarette use in Organization for Economic Cooperation and Development (OECD) countries, with some indication that a cumulative effect might occur [26]. Most research has been carried out in high-income countries, but it is likely that marketing s effects are even more pronounced in the emerging alcohol markets with growing economies and high youth populations and which have larger numbers of abstainers and less history of alcohol use [10]. In its 2006 annual report, Diageo reported that following a 28% increase in marketing, sales in emerging markets (outside Europe and the United States) were up 14% compared with 6% world-wide. Marketing s impacts go beyond the immediate effects on the drinker or potential drinker and create a social milieu in which the positive aspects of drinking are dominant and its use is normalized [27]; for example, the drinking responsibly marketing messages widely promulgated by the industry, which have been shown to be understood by young people as being about moderation but also communicating positive messages about alcohol in an approach described as strategically ambiguous by the authors [28]. These messages also promote positive associations with the company conducting the marketing. Such stakeholder marketing, in which the industry associates its brand with good works, including disaster relief [29], international development meetings [30] and sponsorship of all aspects of sporting and cultural life, contribute to the construction of an environment in which alcohol brands become synonymous with many positive values and experiences and in which the 2012 The Author, Addiction 2012 Society for the Study of Addiction Addiction, 107,
102 480 Sally Casswell perception of the industry as a good corporate citizen is enhanced. The extent to which this enhancement of corporate citizenship subsequently influences industry s credibility when providing input to alcohol policy debates is unknown [31]. CURRENT MARKETING POLICY Industry voluntary codes In contrast with the newly emerging situation under the FCTC, many countries in the world have little systematic, stable control of the alcohol marketing to which their populations are exposed. At the national level, many countries rely on voluntary restraints by the industries involved ( self-regulation ) and these have been shown to be fragile and susceptible to economic downturn (for example abandonment, in the mid-1990s at a time of falling whisky sales, of the UK voluntary agreement not to advertise dark spirits in broadcast media); they have also been used as a mechanism to head off legislative action [32]. Such voluntary restrictions are inevitably partial, often taking the form of codes relating to the content of the advertising in the broadcast media or partial restrictions on exposure, applying to specific beverages, media (e.g. no spirits advertisements on TV) or time-periods. In many contexts much of the new media, including and texting, are not covered and nor are point-of-sale or brand-stretching via branded merchandise. Sponsorship has become a major part of alcohol marketing and is also usually excluded from the codes [33]. Following the expansion of self-regulation in the s, co-regulation has developed as response to the critiques of self regulation. An example of coregulation (self-regulation within a regulatory framework) is found in the UK; this has been in existence since 2005 and has shown no positive impact on the nature of the alcohol advertising broadcast [34,35]. In other responses to increased scrutiny of self-regulation elaborate examples of internal auditing have been set up, for example, in Europe [36,37]. Despite a (sometimes implicit) objective of the voluntary action taken by the industries being to protect younger people from marketing s impact by controlling exposure to marketing, or the nature of the message content, or both, there is clear evidence that this is not being achieved by the commonly implemented selfregulation systems and this reflects failure to control both exposure and content. Studies in the United States and Australia have illustrated that exposure to younger people is equivalent to that of older people or is even greater [38 40] and it has been suggested that, given industry access to information about the composition of programme audiences, this may indicate deliberate targeting of younger people [39]. Interpretations of the voluntary codes regarding content do not take into account that alcohol marketing operates at an emotional level and needs only to associate a logo (even a brand colour) with stimuli with associated positive feeling to be effective [41]. Interpretation of the codes of content have been shown to differ markedly between panels set up by the vested interests and samples of general population [42], younger people [43] and media and marketing experts [33], with the vested interest panels consistently less likely to perceive breaches in the codes. In-house revision of the US Beer Code has been shown to give greater scope to the marketers [44]. Research which has demonstrated the impact of alcohol marketing on young people has often investigated the impact of advertising which has been broadcast under the voluntary agreements (e.g. [45]) a further indication of lack of effectiveness of self-regulation regimes. National policy response Legislation or regulation established as a result of a public policy process has generally been found to be stricter than those found in self-regulation regimes [46]. This is the case in alcohol marketing policy, where the often-cited Loi Evin, one of few legislated policies on alcohol marketing, restricted exposure to the less powerful print media and also controlled content, restricting the advertising to a tombstone approach, excluding all life-style elements which have been found, in the research cited above, to be resonant with young people. Unfortunately, although there is published description of the changes following the French legislation in 1991 and expert opinion about the impacts which followed [47], there are no other evaluation data available. Other jurisdictions with relatively comprehensive regulation include Norway, Iceland and Sweden; in many countries, however, restrictions are too partial to have impacts or are circumvented because of loopholes [48]. International policy response There is a marked absence of an international response to alcohol marketing, although national restrictions have been upheld by regional courts, setting important precedents. In Europe the Loi Evin, one of the most restrictive of alcohol marketing policies, has been adjudicated on by the European Court of Justice and found to be justified and proportionate to its purpose of protecting public health [10]. However, the lack of an international policy response means that the situation with regard to access to alcohol marketing materials on the internet is in marked contrast to the absence of tobacco marketing, and young people are increasingly exposed to and responsive to global alcohol marketing communications [2] The Author, Addiction 2012 Society for the Study of Addiction Addiction, 107,
103 Current status of alcohol marketing policy 481 In 2009 an attempt to extend the Loi Evin to cover internet marketing failed [49]. VOICES IN THE DEBATE ON ALCOHOL MARKETING Vested interest groups To defend the right to market alcohol is essential business activity for the vested interests involved. Without marketing there are potentially negative implications for the global alcohol producers in both mature and emerging markets. In mature markets marketing not only serves to reinforce brand choice among committed drinkers, but also to recruit new, potentially heavy, drinkers from the cohorts of young people who enter the drinking market and replace those who are reducing their contribution to the alcohol market as they age or die. Any reduction in consumption among the heavier drinkers will impact significantly on the sales and therefore the profits of the industry. In emerging markets, where drinkers are in the minority, the need to engage in consumer education to build a drinking culture is particularly important [50]. In the case of alcohol marketing, not only are the producers but also the advertising and media industries actively concerned, who stand to lose revenue if alcohol marketing is curtailed, and they have therefore been engaged actively in policy debate with documented cases of conflict of interest leading to failure to represent a public health perspective [51]. It is not surprising, therefore, that at the national level policy development has been slow. Health officials in many countries, with both mature and emerging markets, draw attention to the negative aspects of the continued exposure of new cohorts of young people to alcohol marketing; for many it is described as a priority. However, it is often viewed as the most difficult policy area to address, given the extent of national-level vested interest group lobbying and stakeholder marketing and a related lack of political will. In countries in which the national economy is small relative to the revenues of the alcohol producers, funding via sponsorship can be an important consideration. An example is the contribution made by Lao Beer to the South East Asian [52] games held in Lao in 2009 (one of the poorest economies world-wide) which was perceived to have made hosting the games possible. The relative absence of nongovernmental organizations focused on alcohol means that marketing often remains unchallenged outside the (relatively powerless) health sector. It is noteworthy that the passing of the Loi Evin in France owed much to the role of five medical academics who operated outside the government sector and promoted the new legislation [53]. Vested interest activity at the international level has attempted to influence national level decision-making. The front organization for the largest global alcohol corporations, the Washington-based International Center on Alcohol Policies (ICAP), has actively promoted selfregulation as the appropriate approach to alcohol marketing in a number of work-shops held in regions of the world where the largest and most potentially profitable emerging markets exist [54,55]. In Africa, for example, ICAP worked in collaboration with SAB Miller to conduct a series of national work-shops promoting industryfriendly policy, including self-regulation of advertising [54]. In Asia industry self-regulation has been promoted as best practice leading to a perception among health officials that there is an international convention on alcohol marketing which precludes national action to restrict global corporations marketing their brands [56]. ICAP argues consistently against government regulation to restrict alcohol marketing by regulation [57]. The likelihood of change being affected by the alcohol producers supporting or accepting restriction on their right to alcohol marketing is low. There is a stability in the global alcohol market which generally leads to company preference for transnational self-regulation, giving key producers the ability to ward off national-level government regulation [58]. Whereas the issues which are commonly part of corporate social responsibility, for example human rights and environmental sustainability, can be addressed without threatening company viability, restriction of alcohol marketing would have major effects not only on levels of sales but also industry attempts to normalize and sanitize the product. In this context, it has been concluded by professional groups such as the British Medical Association that national efforts to develop alcohol marketing policy require governments to avoid or withdraw from partnership with industry [20]. Intergovernmental sector Other key players in the global governance arena, the intergovernmental organizations World Trade Organization (WTO) and World Health Organization (WHO), are both relevant to this policy arena. The WTO agreements aim to reduce controls on market access and national restrictions on international trade. There is a requirement for progressive liberalization in successive rounds of negotiations [59]. In relation to alcohol, most of the ways in which trade agreements have influenced public policy and public health have been through requirements to allow import of all products and to reduce and eventually remove tariffs from imported beverages and by challenges to monopoly supply systems [60]. The requirement to allow all products equal access has resulted in Sweden being required to sell Ready to Drinks (spirits plus mixer) 2012 The Author, Addiction 2012 Society for the Study of Addiction Addiction, 107,
104 482 Sally Casswell [61], an important development in marketing alcohol to young people [62]. Apart from the increase in availability of a range of products the WTO system has apparently had no direct involvement in relation to alcohol marketing but may have had a chilling effect by creating a global environment in which threats of action could be taken, particularly in emerging markets [63]. The WHO is the United Nations (UN) agency which has assumed primary responsibility for alcohol. Like all intergovernmental organizations, the influence of their considerable technical expertise and moral standing may be muted by the influence of the big transnational corporations (TNCs) [64,65]. Recent policy development work leading to endorsement of a global strategy to reduce alcohol-related harm illustrates the difficulties surrounding alcohol marketing policy. The process of development of a global strategy involved many levels of consultation, including with the representatives of the commercial interests who urged against across-the-board limitations on alcohol beverage product marketing [66], recommending instead a co-regulatory framework. The Draft Working Paper produced by the Secretariat and commented upon by a number of expert advisers made no mention of a co-regulatory framework, referring instead to a regulatory framework, preferably with a legislative basis, and there was also no reference to a self-regulation option. However, by the time the strategy emerged from the Executive Board in January 2010 the marketing section referred to setting up a regulatory or co-regulatory framework, preferably with a legislative framework and supported when appropriate by self regulatory measures....in addition to the influence of the commercial interests, often expressed through Member States, there is an inherent limitation in the health focus of the WHO, given the range of sectors with interest in curtailing alcohol-related harm (police and justice, for example), and this may explain in part the relative lack of attention paid to alcohol compared, for example, to tobacco. Non-governmental sector Analyses of global governance have highlighted the role of TNCs, non-governmental organizations (NGOs) and the state (including international governmental organizations) in the governance triangle [67]. In relation to alcohol policy there is an imbalance between the resources of the commercial sector and that of both government and NGOs. This suggests the importance of the NGO sector to support and shape the state s response at both national and international level. In the current global environment there has been a major growth in NGOs; there are now world-wide operating internationally [68]. The large number of (well coordinated) NGOs focused on tobacco (the Alliance on Tobacco Control) has been credited with a significant contribution to the development of the FCTC [69]. At a time of relative increase in front organizations funded by the alcohol producers (which operate in an NGO space), the lack of resource for national and international alcohol-specific NGOs is a major concern. However, there are some promising developments with the emergence of a network of regional and a global network [70], increasing interest in and good examples of the establishment of health promotion foundations funded by an earmarked tax on alcohol (e.g. [71]) and increased engagement by the wellorganized non-communicable diseases (NCD) sector [72]. FCTC PRECEDENT FOR GLOBAL GOVERNANCE ON ALCOHOL MARKETING The public health field is facing a global environment in which alcohol marketing and supply drive alcohol demand. This reflects the expansion and consolidation of the alcohol producers, new development in skills and technology of marketing and far-reaching changes in the free trade environment, as well as young people s access to global media and relationship with commodities such as alcohol [2,73]. It is highly unlikely that widespread progress towards healthy policy development will take place at a national level in the absence of supporting global governance. The infrastructure, economic, social and political, which supports and allows alcohol marketing is global in nature and requires a global response. The WHO response to tobacco provides a useful precedent in the formulation of a health treaty, a Framework Convention, which has been found feasible and valuable in controlling tobacco marketing. Such international conventions are important in facilitating the overcoming of domestic vetoes [36] and also providing a source of global information and emulation [64] which otherwise is provided only by the resources of the vested interest groups. There is a general move towards more mandatory mechanisms and increased accountability in relation to the activities of TNCs [64] and the FCTC provides a good global model. While the goals for alcohol consumption (to reduce harm) are different from those for tobacco (to eliminate use) [63] there is nevertheless the need to implement similar policy levers, especially restriction on marketing. The FCTC requires parties to the treaty to implement a comprehensive ban of all tobacco advertising, promotion and sponsorship including a comprehensive ban on cross-border advertising, promotion and sponsorship where this is not in breach of constitutional principles (and in the case of such constitutional difficulties to 2012 The Author, Addiction 2012 Society for the Study of Addiction Addiction, 107,
105 Current status of alcohol marketing policy 483 implement restrictions ) (Article 13) [74]. Under the terms of the Framework Convention countries meet to agree protocols on specific issues such as international collaboration necessary to ban cross-border marketing. The FCTC provides the stimulus for national regulation as well as international collaboration, both of which are urgently required in relation to alcohol marketing. In the meantime, examples of national legislation to restrict alcohol marketing exist and provide good models. These cover sponsorship and promotion and restrict exposure (either by a complete ban in all media or by restriction to adult-orientated print media) and content (by banning life-style advertising). Examples of legislative text are given in the recently published WHO guide to developing effective alcohol legislation [48]. CONCLUSION The contrast between the regulation of tobacco marketing and the unfettered expansion of alcohol marketing cannot be justified when the evidence on harm and the expansion of consumption into younger populations in both mature and emerging markets is acknowledged. A global response to promote restriction of all forms of marketing at national and international level is urgently required. Declarations of interest None. References 1. Hill L. The alcohol industry. In: Heggenhougen K., Quah S., editors. International Encyclopedia of Public Health. San Diego: Academic Press; 2008, p Jernigan D. The extent of global alcohol marketing and its impact on youth. Contemp Drug Probl 2010; 37: Saffer H., Dave D. Alcohol advertising and alcohol consumption by adolescents. Health Econ 2006; 15: Mart S., Mergendoller J., Simon M. Alcohol promotion on facebook. J Glob Drug Policy Pract [serial on the internet] 2009; 3. Available at: 1.php (accessed 10 October 2011). 5. Gordon R. An audit of alcohol brand websites. Drug Alcohol Rev 2011; 30: Center on Alcohol Marketing and Youth. Clicking with kids: alcohol and marketing on the internet. Washington, DC, Hanewinkel R., Tanski S., Sargent J. Exposure to alcohol use in motion pictures and teen drinking in Germany. Int J Epidemiol 2007; 36: Mosher J. Transcendental alcohol marketing: rap music and the youth market. Addiction 2005; 100: Hill L., Casswell S. Alcohol advertising and sponsorship: commercial freedom or control in the public interest? In: Heather N., Stockwell T., editors. The Essential Handbook of Treatment and Prevention of Alcohol Problems. Chichester: John Wiley & Sons; 2004, p Babor T., Caetano R., Casswell S., Edwards G., Giesbrecht N., Graham K. et al. Alcohol: No Ordinary Commodity Research and Public Policy, 2nd edn. Oxford: Oxford University Press; Rehm J., Mathers C., Popova S., Thavorncharoensap M., Teerawattananon Y., Patra J. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet 2009; 373: Smart R. Does alcohol advertising affect overall consumption? A review of empirical studies. J Stud Alcohol 1988; 49: Nelson J., Young D. Effects of youth, price, and audience size on alcohol advertising in magazines. Health Econ 2008; 17: Anderson P., de Bruijn A., Angus K., Gordon R., Hastings G. Impact of alcohol advertising and media exposure on adolescent alcohol use: a systematic review of longitudinal studies. Alcohol Alcohol 2009; 44: Wyllie A., Zhang J. F., Casswell S. Positive responses to televised beer advertisements associated with drinking and problems reported by 18 to 29 year olds. Addiction 1998; 93: Wyllie A., Zhang J. F., Casswell S. Responses to televised alcohol advertisements associated with drinking behaviour of 10 to 17 year-olds. Addiction 1998; 93: Grube J. W., Wallack L. Television beer advertising and drinking knowledge, beliefs and intentions among school children. Am J Public Health 1994; 84: Snyder L., Milici F., Slater M., Sun H., Strizhakova Y. Effects of advertising exposure on drinking among youth. Arch Pediatr Adolesc Med 2006; 160: Saffer H., Dave D. Alcohol consumption and alcohol advertising bans. Appl Econ 2002; 30: British Medical Association. Under the influence: the damaging effect of alcohol marketing on young people. London: British Medical Association; McCreanor T., Moewaka Barnes H., Kaiwai H., Borell S., Gregory A. Creating intoxigenic environments: marketing alcohol to young people in Aotearoa New Zealand. Soc Sci Med 2008; 67: Hastings G. They ll Drink Bucket Loads of the Stuff : An Analysis of Internal Alcohol Industry Advertising Documents. London: Alcohol Education and Research Council; Memorandum by Professor Gerard Hastings, Institute for Social Marketing, University of Stirling and the Open University. 23. Snyder L. B., Blood D. J. Caution: alcohol advertising and the Surgeon General s alcohol warnings may have adverse effects on young adults. J Appl Commun Res 1992; 20: Slater M., Domenech M. M. Alcohol warnings in TV beer advertisements. J Stud Alcohol 1995; 56: Atkin C., Block M. Content and Effects of Alcohol Advertising. Springfield, VA: US National Technical Information Service; Saffer H., Chaloupka F. The effect of tobacco advertising bans on tobacco consumption. J Health Econ 2000; 19: Wallack L. Mass media campaigns in a hostile environment: advertising as anti-health education. J Drug Addict 1983; 28: Smith S., Atkin C., Roznowski J. Are drink responsibly alcohol campaigns strategically ambiguous? Health Commun 2006; 20: The Author, Addiction 2012 Society for the Study of Addiction Addiction, 107,
106 484 Sally Casswell 29. International Organisation of Good Templars International. Money from Misery Available at: org/viewarticle.php?id=330&type=sub&t=home (Archived by WebCite at accessed 12 October 2010). 30. Corporate Watch. Diageo PLC A Corporate Profile Available at: (Archived by WebCite at org/5tqpoyqwv; accessed 12 October 2010). 31. Hastings G., Liberman J. Tobacco corporate social responsibility and fairy godmothers: the Framework Convention on Tobacco Control slays a modern myth. Tob Control 2009; 18: Hill L., Casswell C. Alcohol advertising and sponsorship: commercial freedom or control in the public interest. In: Heather N., Peters T., Stockwell T., editors. International Handbook of Alcohol Dependence and Problems. Chichester: John Wiley & Sons Ltd; 2001, p Jones S., Hall D., Munro G. How effective is the revised regulatory code for alcohol advertising in Australia? Drug Alcohol Rev 2008; 27: Office of Communications (Ofcom). Young people and alcohol advertising: an investigation of alcohol advertising following changes to the advertising code. London: Office of Communications; Gunter B., Hansen A., Touri M. The representation of meaning in alcohol advertising and young people s drinking. Leicester: Department of Media and Communication, University of Leicester; Koenig-Archibugi M. Transnational corporations and public accountability. Gov Oppos 2004; 39: Brewers of Europe. Responsible Beer Advertising Through Self-Regulation Available at: ofeurope.org/docs/flipping_books/responsible_beer_ad_ 2010/index.html (Archived by WebCite at webcitation.org/60kyqfvzx; accessed 21 July 2011). 38. Jernigan D. Alcohol advertising regulation: where to from here [Commentary]. Addiction 2009; 104: Fielder L., Donovan R., Ouschan R. Exposure of children and adolescents to alcohol advertising on Australian metropolitan free-to-air television. Addiction 2009; 104: Chung P., Garfield C., Elliott M., Ostroff J., Ross C., Jernigan D. Association between adolescent viewership and alcohol advertising on cable television. Am J Public Health 2010; 100: Hastings G., Anderson S., Cooke E., Gordon R. Alcohol marketing and young people s drinking: a review of the research. J Public Health Policy 2005; 26: Saunders B., Yap E. Do our guardians need guarding? An examination of the Australian system of self-regulation of alcohol advertising. Drug Alcohol Rev 1991; 10: Jones S., Donovan R. Messages in alcohol advertising targeted to youth. Aust NZ J Public Health 2001; 25: Babor T., Xuan Z., Damon D. Changes in the self-regulation guidelines of the US Beer Code reduce the number of content violations reported in TV advertisements. J Public Aff 2010; 10: Casswell S., Zhang J.-F. Impact of liking for advertising and brand allegiance on drinking and alcohol-related aggression: a longitudinal study. Addiction 1998; 93: Kolk A., van Tulder R., Welters C. International codes of conduct and corporate social responsibility: can transnational corporations regulate themselves? Transnat Corporations 1999; 8: Rigaud A., Craplet M. The Loi Evin : a French exception. Globe 2004; 1&2: World Health Organization (WHO) Western Pacific Region. Addressing the harmful use of alcohol: a guide to developing effective alcohol legislation. Manila: WHO; Braillon A., Dubois G. Public health, politicians decisions, and the citizen. Health Policy 2009; 93: Room R., Jernigan D., Carlini-Marlatt B., Gureje O., Makela K., Marshall M. et al. Alcohol in developing societies: a public health approach. Geneva: Finnish Foundation for Alcohol Studies in collaboration with the World Health Organization Casswell S., Stewart L., Duignan P. The negotiation of New Zealand alcohol policy in a decade of stabilized consumption and political change: the role of research. Addiction 1993; 88: 9S 17S. 52. Buchanan C., Holmbeck G. Measuring beliefs about adolescent personality and behavior. J Youth Adolesc 1998; 27: Sulkunen P. The Public Health Cycle. The Evin Law and the Total Consumption Model in French Alcohol Policy Available at: apa_research_citation/0/2/1/2/9/p21291_index.html (accessed 21 July 2011). 54. Bakke O., Endal D. Vested interests in addiction research and policy alcohol policies out of context: drinks industry supplanting government role in alcohol policies in sub-saharan Africa. Addiction 2010; 105: International Center for Alcohol Policies. Meeting Reports Available at: MeetingReports/tabid/72/Default.aspx (Archived by WebCite at accessed 21 July 2011). 56. Social and Health Outcomes Research and Evaluation (SHORE). Towards sustainable data collection and national alcohol policy development: a cross country collaborative project (unpublished) Report to the World Health Organization. 57. International Center for Alcohol Policies. Self-regulation of beverage alcohol advertising. Washington, DC: International Center for Alcohol Policies; Mugge D. Private public puzzles: inter-firm competition and transnational private regulation. New Polit Econ 2006; 11: Kelsey J. Serving Whose Interests?: The Political Economy of Trade in Services Agreements. Abingdon, UK: Routledge- Cavendish; Gould E. Trade treaties and alcohol advertising policy. J Public Health Policy 2005; 26: Romanus G. Alcopops in Sweden a supply side initiative. Addiction 2000; 94: S Jackson M., Hastings G., Wheeler C., Eadie D., MacKintosh A. Marketing alcohol to young people: implications for industry regulation and research policy. Addiction 2000; 95: S Casswell S., Thamarangsi T. Reducing the harm from alcohol: call to action. Lancet 2009; 373: Koenig-Archibugi M. Understanding the global dimensions of policy. Glob Policy 2010; 1: Roberts I. Corporate capture and Coca-Cola. Lancet 2008; 372: The Author, Addiction 2012 Society for the Study of Addiction Addiction, 107,
107 Current status of alcohol marketing policy World Health Organization (WHO). Report from a Roundtable Meeting with Economic Operators on Harmful Use of Alcohol, Geneva, 6 November Available at: (Archived by WebCite at 5vB55a2MS; accessed 23 December 2010). 67. Abbott K., Snidal D. The governance triangle: regulatory standards institutions and the shadow of the state. In: Matti W., Woods N., editors. The Politics of Global Regulation. Princeton: Princeton University Press; p Sikkink K., Smith J. Infrastructures for change: transnational organizations, In: Khagram S., Riker J., Sikkink K., editors. Restructuring World Politics: Transnational Advocacy Movements, Networks, and Norms. Minneapolis: University of Minnesota Press; 2002, p Lencucha R., Kothari A., Labonte R. The role of nongovernmental organizations in global health diplomacy: negotiating the Framework Convention on Tobacco Control. Health Policy Plan Advance Access published 4 November, doi: /heapol/czq Global Alcohol Policy Alliance (GAPA). Global Alcohol Policy Alliance Available at: (Archived by WebCite at 60KZemb4v; accessed 21 July 2011). 71. Thai Health Promotion. Home. Undated. Available at: (Archived by WebCite at accessed 7 March 2011). 72. Non-Communicable Diseases (NCD) Alliance. Addressing the Harmful Use of Alcohol Is Essential to Realising the Goals of the UN Resolution on Non-communicable Diseases (NCD) Available at: (Archived by WebCite at accessed 21 July 2011). 73. Warde A. Consumption, identity-formation and uncertainty. Sociology 1994; 28: World Health Organization (WHO). WHO Framework Convention on Tobacco Control. Geneva: WHO; The Author, Addiction 2012 Society for the Study of Addiction Addiction, 107,
108
109 Section 7 Key CAYAD Documents & Evaluation Summaries
 Ministry of Health Manat Hauora 1 October")
110 Process and Impact Evaluation Community Action on Youth and Drugs (CAYAD) Ministry of Health Manat Hauora 1 October 2009
111 C A Y A D P R O C E S S A N D I M P A C T E V A L U A T I O N Contents 1. Executive Summary Community Action on Youth and Drugs (CAYAD) Evaluation of CAYAD Implementation of the CAYAD programme The impact of the CAYAD programme Effecting national policy Conclusions Ongoing improvements 6 2. Introduction The CAYAD programme Evaluating the CAYAD programme Evaluation limitations Report terminology CAYAD Implementation at a National Level Alignment of CAYAD with key national strategies National co-ordination of the CAYAD programme Implementation at CAYAD site level Local co-ordination and management of CAYAD Implementation of the National Service Schedule Implementation activities between 2007 and Alignment with community action approach Progression as a national programme CAYAD Outcomes Outcome 1: Increased informed community discussion and debate about issues related to illicit drugs Outcome 2: Effective policies and practices to reduce harm adopted Outcome 3: Increased local capacity to support young people in education, employment and recreation Outcome 4: Reduced supply of drugs to young people Emergence of outcomes across CAYAD sites CAYAD unintended outcomes Effecting national policy Key Evaluation Findings and Improvements 48
112 C A Y A D P R O C E S S A N D I M P A C T E V A L U A T I O N Acknowledgements: Litmus wishes to acknowledge and thank individuals and organisations who contributed to this evaluation. We would especially like to thank the eight CAYAD case study sites for their contribution.
113 C A Y A D P R O C E S S A N D I M P A C T E V A L U A T I O N Executive Summary 1.1 Community Action on Youth and Drugs (CAYAD) Community Action on Youth and Drugs (CAYAD) is a community action programme aligned with the New Zealand National Drug Policy (NDP). The NDP sets out the Government's policy for tobacco, alcohol and other drugs. The NDP aims to minimise the harms from these substances and improve the health and well-being of New Zealanders. The NDP identifies young people as a population group at greater risk of drug-related harms than other New Zealanders, requiring targeted approaches and a strong focus on the prevention of drug-related harm. The CAYAD programme aims to limit the use of drugs and reduce harm from drug use (in line with the NDP s harm minimisation approach). The overall aim of the programme is to improve health outcomes through: increased community ownership and capability to address drug-related issues reduced drug-related harm improved health and well-being of New Zealanders. (Ministry of Health, 2008) CAYAD has four outcomes to address the overall aim of the programme: 1. increased informed community discussion and debate about issues related to illicit drugs 2. effective policies and practices to reduce harm adopted 3. increased local capacity to support young people in education, employment and recreation 4. reduced supply of drugs to young people. The CAYAD programme is focused on 30 communities across New Zealand identified as high-needs. The programme was first piloted in Over the last few years, many CAYAD sites, in response to community need, have expanded their focus to also include reducing demand and controlling supply of alcohol to young people in their communities. 1.2 Evaluation of CAYAD The Ministry of Health (the Ministry) commissioned Litmus Limited to undertake a process and impact evaluation of CAYAD in The objectives of the evaluation were: 1. to describe how CAYAD was implemented between January 2007 and February 2009 to determine whether implementation is proceeding as intended and to identify successes and challenges 2. to identify intended outcomes arising from the implementation of CAYAD, and the underlying factors contributing to or inhibiting their achievement 3. to identify unintended outcomes arising from the implementation of CAYAD 1
114 C A Y A D P R O C E S S A N D I M P A C T E V A L U A T I O N to identify potential improvements to the ongoing implementation of CAYAD that would help bring about the desired outcomes. The evaluation did not consider the costs and benefits of CAYAD. The evaluation findings drew on literature and documentation relating to the CAYAD programme, interviews with key national-level stakeholders, case studies of eight CAYAD sites, and an online survey of the remaining 17 CAYAD providers. 1.3 Implementation of the CAYAD programme The CAYAD programme has a national-level governance and capability building structure of the Ministry of Health, the National Co-ordinator and the National CAYAD Advisory Group (NCAG). The benefits of this structure are clear strategic direction, targeted and effective workforce development, and a mechanism for disseminating knowledge from the 30 CAYAD sites across New Zealand into national-level policy. Overall, the relationship between the Ministry and the National Co-ordinator is working well. NCAG is in its formative stage, and to be effective further clarification of its role and composition is needed. At a local level, each CAYAD site is led by kaimahi supported by their manager. In June 2009, most providers (18 out of 25) have a CAYAD Reference Group made up of community and sector leaders and alcohol and other drug professionals. The kaimahi is pivotal to the success of the CAYAD site. An effective kaimahi: has a community and key stakeholder network understands their community s unique challenges and contexts is knowledgeable about the evidence-base of effective practice in demand reduction and supply control for alcohol and illicit drugs is able to create support and provide leadership for the CAYAD programme locally is culturally competent. The evaluation highlighted that the majority of kaimahi are credible and seen to have the right skills to make an effective difference in their respective communities. At a local level, CAYAD sites move through a number of overlapping cyclical development stages: The establishment phase is for fostering and developing networks and relationships with key stakeholders in a range of community and professional settings. The kaimahi seek to create support for CAYAD s aim and outcomes across a range of stakeholders. It is critical to gain stakeholders active involvement to establish a common voice on drug and alcohol issues, collaborate on specific initiatives and, if appropriate, offer additional resources. This stage takes time to build understanding, relationships and trust. Once created, a local foundation is established on which the CAYAD site can develop strategies to address the community s issues relating to alcohol and illicit drugs. The strategic planning phase is when CAYAD sites, in conjunction with wider stakeholders, identify evidence-based and community-relevant initiatives and activities that align with the aim and desired outcomes of the CAYAD programme. The current CAYAD outcomes are broad and aligned with the NDP. Consequently, kaimahi can 2
115 C A Y A D P R O C E S S A N D I M P A C T E V A L U A T I O N address unique community needs within this framework. Effective CAYAD sites seek to develop a range of initiatives that address each CAYAD outcome from a number of perspectives thus maximising the extent of the change in the community. The implementation phase occurs when the kaimahi works intersectorally to deliver initiatives that align with the four CAYAD outcomes. The box below contains examples of initiatives that have been implemented by CAYAD sites. During the implementation phase, sites reflect on progress by identifying emerging outcomes and using this information to refine networks and action plans. Thus, the cycle commences again. Outcome 1: increased informed community discussion and debate about issues related to illicit drugs Attendance at forums, groups and committees, e.g. Liaison on Alcohol and Other Drug meetings Wider community and stakeholder networking, e.g. drug and alcohol abuse wananga Drug education and resource development and distribution Events and activities, e.g. Youth Expo delivering health messages and services Media, e.g. promotion of CAYAD kaupapa to the community through media and mass events, newsletters, radio shows Outcome 2: effective policies and practices to reduce harm adopted Informing drug and alcohol policies in local community settings, e.g. schools, marae, sports clubs Written submissions and running submission writing seminars, e.g. developing joint submissions on the National Alcohol Action Plan Outcome 3: increased local capacity to support young people in education, employment and recreation Undertaking or supporting other organisations in developing youth leadership and mentoring young people, e.g. setting up a Youth Advisory Group or Youth Council Working with schools and education providers to encourage young people to remain in education and/or enter training courses, e.g. working with local training provider to set up a carpentry course Identifying employment opportunities for young people, e.g. working with local employers Identifying or working with sporting organisations to offer a range of sporting opportunities, e.g. gym, youth basketball Outcome 4: reduced supply of drugs to young people Working with gangs to reduce or stop supply of methamphetamine to young people; supporting communities to report illicit drug sellers Youth hikoi to reduce number of liquor outlets; young people reporting licensees supplying to underage youth or intoxicated young people In summary, CAYAD is a community action approach which addresses two pillars of the NDP: demand reduction and supply control. CAYAD is an iterative process of strategically planned, evidence-based, multi-component initiatives developed and delivered via an intersectoral approach to address community issues about youth s alcohol and illicit drug use across the four CAYAD outcomes. Over the last two years, the CAYAD programme has gone through a period of strengthening. The purpose was to achieve greater consistency in practice across sites in relation to the 3
116 C A Y A D P R O C E S S A N D I M P A C T E V A L U A T I O N CAYAD programme s aim and outcomes, while retaining the ability to respond locally within this overarching framework. The implementation of a National Service Schedule and ongoing capability building has achieved the following results: Development of national and site level programme logic models and action plans (19 out of 25 CAYAD providers have a programme logic model). Although the process was time consuming and challenging, CAYAD providers and key stakeholders found it beneficial. The development of the logic models resulted in a shared and evidencebased direction at site level and a greater consistency of approach across CAYAD sites. The rejuvenation or establishment of Reference Groups. While most Reference Groups are at formative stage, their presence has increased CAYAD s visibility locally. Further, there is evidence that the presence of a Reference Group is resulting in a more collaborative implementation and sharing of local resources (i.e. the adoption of an intersectoral approach). An in-depth understanding of the community action approach. For most CAYAD sites, the implementation of the requirements of the National Service Schedule consolidated and reaffirmed their direction. However, at least two CAYAD sites realised that, while they were active in their community around drug education initiatives, their actions were inconsistent with a community action approach. As a result, the outcomes achieved were limited. Programme logic development therefore enabled these CAYADs to realign their activities and interventions with CAYAD s kaupapa. At the time of this evaluation, it was too early to determine whether the action plans developed will be implemented as intended. These sites will therefore require careful monitoring and constructive feedback over the next year. Increased awareness from CAYAD providers and stakeholders that CAYAD is a national programme. CAYAD sites are increasingly thinking about how to transfer their learnings across sites and how to collaborate regionally. Awareness and presence of the CAYAD brand is high amongst Reference Group members. However, across wider stakeholders CAYAD is less well known. These stakeholders commend the work of the CAYAD provider but do not associate their activities with the CAYAD programme. This lack of awareness has the potential to limit future alliances that may enhance CAYAD s reach and effectiveness. The National Service Schedule introduced two new reporting templates. Across the CAYAD sites, there is confusion about and inconsistent use of these templates. Many CAYAD sites find reporting challenging, particularly in demonstrating the achievements of their CAYAD against outcomes. The development of the programme logic offers an outcome framework against which to report. However, there continues to be a lack of understanding on how to do this. Capability building on outcomes reporting is therefore required. Linked to this reporting, CAYAD sites are seeking more detailed feedback from the Ministry on their progress. CAYAD sites are expected to contribute to the evidence-base of effective demand reduction and supply control initiatives. Consequently, being able to report in a way that is meaningful will contribute to this wider evidence-base is important. Currently, there is no national level reporting on the CAYAD programme, and no national level indicators to demonstrate how CAYAD contributes to national policy. It is acknowledged the latter may be difficult to achieve, given the geographical spread of the CAYAD sites and may be potentially cost prohibitive. However, national reporting is an area, which requires further consideration. 4
117 C A Y A D P R O C E S S A N D I M P A C T E V A L U A T I O N The impact of the CAYAD programme CAYAD is perceived by providers and local and national stakeholders as an effective programme that helps reduce youth demand for alcohol and illicit drugs. This is reflected in the CAYAD programme delivering positive results against three of the four CAYAD outcomes. Increased informed community discussion and debate about issues related to illicit drugs is an outcome clearly being achieved across most CAYAD sites. This increase in discussion has resulted in: wider awareness and knowledge across key alcohol and drug stakeholders and community leaders about the issues relating to illicit drugs and alcohol in the CAYAD communities agreement about how to address these issues and therefore common and consistent messages across the communities agreement across the stakeholders to work together on agreed initiatives collaborative initiatives being actioned. The CAYAD programme has influenced policy about alcohol and drugs both locally and nationally, thus creating systemic and environmental change: Working with schools, marae and sports clubs to introduce or change their drug and alcohol policies has changed alcohol- and drug-related behaviour at that setting level. Collaborative submissions have been made on local council and national policy, including the National Action Alcohol Plan. The CAYAD programme has been very successful in building local capacity to keep young people engaged in education, recreation and employment to reduce the opportunities for drug and alcohol use. This has had further benefits of improved health and well-being through sport, remaining in or returning to education, and/or training or entering the workforce. The CAYAD programme has therefore set many young people onto prosocial life pathways. As a direct result of the CAYAD programme, two unintended outcomes are emerging: CAYAD is having a wider whnau/community effect. Young people s engagement in CAYAD initiatives offers, in some cases, the opportunity to access parents and wider whnau. Some CAYAD sites have reported that wider whnau engagement in CAYAD initiatives is influencing their attitudes and behaviour to drugs and alcohol. Youth crime has reduced significantly in at least four communities due to the work of CAYAD sites. Across the CAYAD sites, only limited activities have been undertaken to reduce the supply of illicit drugs. Many kaimahi acknowledge that supply control initiatives are appropriate for alcohol. However, they struggle to identify initiatives around the supply of illicit drugs, given this tends to be the role of enforcement agencies. One CAYAD site has had positive success in changing some gangs attitudes and behaviour to supplying methamphetamine, although the overall impact on supply is unknown. Others have reported supply activity within the community to the Police which for a visible CAYAD worker has its risks. All CAYAD sites are contributing to the success of the CAYAD programme. However, the extent to which outcomes are emerging varies across the CAYAD sites. Those sites closely 5
118 C A Y A D P R O C E S S A N D I M P A C T E V A L U A T I O N aligned with a broad intersectoral community action approach are more effective at achieving results across the CAYAD outcomes. The few CAYAD sites focusing predominantly on one or two CAYAD outcomes and not embedding an active intersectoral approach were achieving a more limited range of results. This finding therefore supports the use of community action and validates the investment over the last two years of building CAYAD sites understanding of its application. 1.5 Effecting national policy From this evaluation, there is evidence that the CAYAD programme is making a significant difference at a number of national policy levels: Harm minimisation the initiatives of CAYAD sites and their stakeholders have positively changed the lives of numerous young people and their whnau and offered benefits to the wider communities. Evidence-based policy initiatives undertaken by CAYAD sites are based on both research evidence of what works and the local knowledge of communities. Partnership this is integral to the CAYAD programme. Sustainable initiatives are underpinned by a number of strategic relationships. Reducing inequalities many CAYAD sites are located in areas with high Mori and Pacific populations. Iwi-affiliated providers are making a significant difference in their communities and are ensuring access to opportunities and supporting positive outcomes both for young people and for whnau and the wider communities. 1.6 Conclusions Over the last two years, the introduction of a number of national-level initiatives has strengthened CAYAD at both a national and a local level. The CAYAD programme is now becoming more established as a national programme, with greater consistency across sites to CAYAD s aim and outcomes and the use of a community action approach. The CAYAD programme is successfully achieving three of its desired outcomes. The CAYAD programme is not able to demonstrate the same level of success in the reduction of the supply of illicit drugs, although more success is achieved in reducing the supply of alcohol. Two significant unintended outcomes have emerged as a direct result of CAYAD: changes in attitudes and behaviour of the wider whnau to alcohol and drug use and the reduction of youth crime. 1.7 Ongoing improvements Suggestions for improvements focus on ensuring consistency across the CAYAD sites, ongoing strengthening of CAYAD as a national programme, and demonstrating its effect on national policy. The suggested improvements below are organised by key partner groups within the CAYAD programme. More specificity on improvements can be found in sections 3, 4 and 6. 6
119 C A Y A D P R O C E S S A N D I M P A C T E V A L U A T I O N Ministry of Health Identifying the appropriateness of the supply reduction outcome for CAYAD sites, and if appropriate defining and communicating the expected activities. Including in CAYAD s aim and outcomes reference to demand reduction and supply control for alcohol. Clarifying the reporting requirements for the CAYAD sites as detailed in the National Service Schedule. Providing regular feedback to CAYAD sites on their reported progress, particularly for those sites who have realigned with a community action approach. Developing a national reporting framework to quantify and clearly demonstrate how the CAYAD programme is contributing to national policy goals. National Co-ordinator NCAG Ensuring all CAYAD sites have a programme logic model and a functioning Reference Group. A particular focus needs to be placed on the extent to which CAYAD sites programme logic models have intersectoral initiatives that span across all CAYAD s agreed outcomes. Continuing to develop CAYAD sites capability, relative to their development stage, e.g. development of quantitative measures, reporting and policy analysis skills. Clarifying NCAG s role and composition to be an effective conduit between the CAYAD sites and national-level policy. Particular consideration needs to be given to the role of the Ministry and the need for academic rigour within this body in the long-term. CAYAD sites Having a widely agreed programme logic and action plan that is focused across all of the CAYAD outcomes and being able to report meaningfully against it. Having an effective Reference Group that meets regularly. Identifying with partners effective mechanisms on how to transfer community knowledge about effective initiatives to the wider evidence-base. Promoting the CAYAD brand so the kaimahi s work is strongly linked to the national programme. 7
120 What is Community Action? - Some (debatable) distinctions Community Action Focus on achieving change in structures and systems so that change is sustained without significant ongoing effort by stakeholders Emphasis is on changing underlying social norms and organisational policies and practices Focus is on a specific issue eg drugs Activity guided by, and largely limited to, strategies based on research and local evidence Problem often identified by govt/ funder Engagement in political processes is fundamental, so issue is on policy agenda Specific measurable objectives based on research evidence and local knowledge Engages only selected organisations/ stakeholders to work together on issue Either communities of interest and/or geographic communities Often a paid co-ordinator specific to the project Research ongoingly contributed to the project by formative evaluators Action plan developed and progress is formally evaluated using specific indicators Based on best practice + innovation Community Development Relies on sustained input from community members may suffer from competing demands on volunteers Focus is often raising public awareness to change individual attitudes/ behaviour and build capacity of community leaders Multiple issues - as identified by community Community members undertake whatever they believe is needed Problems usually identified by community Engagement in political processes is not necessarily a defining feature Objectives and strategies are left open to be developed by the community Significant numbers of community groups/members involved largely organize themselves Community is usually geographic Co-ordination often by volunteers, or by someone from a local agency Does not necessarily utilise research evidence- may rely on people knowledge Action plans, monitoring and evaluation may be less formal or not prioritised The community knows best ethos

121 Review of CAYAD programme Final Report Report prepared for Ministry of Health by Louise Thornley, Judith Ball, Celia Murphy Quigley and Watts Ltd September
122 Acknowledgements: The authors would like to thank the following for their input and support to the review: The interviewees for their time and expertise SHORE Whariki for advice and assistance locating key documents, and background discussion of the programme New Zealand Drug Foundation (NZDF) for advice on locating key documents Rebecca Kemp, Ministry of Health, for input and advice. 2
123 Executive Summary This report outlines a review of the Community Action Youth and Drugs programme (CAYAD). Quigley and Watts Ltd carried out the review for the Ministry of Health. The review assessed the CAYAD programme s scope in light of the latest evidence on community action, findings on drug-related harm in New Zealand, and interviews with stakeholders. This report summarises the review findings, and presents recommendations. CAYAD programme The CAYAD programme, funded by the Ministry of Health, uses a community action approach to work with key people and organisations to reduce youth drug-related harm. Community action involves facilitating action by groups and agencies, with a focus on changing environments and policies. The CAYAD programme has four intended outcomes: increased informed community discussion and debate about issues related to illegal drugs effective policies and practices to reduce harm adopted increased local capacity to support young people in education, employment and recreation reduced supply of drugs to young people. While the stated outcomes of the CAYAD programme specify harm reduction from illegal drugs to young people, most CAYAD providers also work to reduce alcoholrelated harm. The CAYAD programme was developed and implemented with a focus on evidence and action-reflection. The Ministry funds national coordination to support the CAYAD programme. SHORE and Whariki at Massey University are currently contracted as the National Coordination Team (NCT). The NCT promotes the sharing of best practice amongst CAYAD sites and offers strategic guidance and workforce development. Method The review s objectives were to: 1) Improve CAYAD services by ensuring the CAYAD programme is an effective evidence-based national programme that addresses drugrelated harm for youth, and 2) Determine an appropriate scope for the CAYAD programme by reviewing current service objectives and the definition of drugs that is used. The review was formative in nature as it focused on reviewing the current scope and making suggestions for improvement. It had three strands: 3
124 a) an environmental scan of New Zealand documents and research to describe the issue of youth drug use and drug-related harm b) a review of evidence on community action c) telephone interviews with stakeholders to seek their perspectives and views on the programme. Seventeen stakeholders were interviewed by telephone. They included national-level stakeholders from relevant agencies (eg, Te Puni Kokiri, Ministry of Youth Development, Ministry of Justice, ALAC, New Zealand Drug Foundation), as well as staff directly involved with the CAYAD programme locally and nationally. However, the focus of the review was on the national programme rather than reviewing local sites. The review was limited by a small budget, which restricted the number of interviews and necessitated a rapid rather than comprehensive literature review. Findings The review confirmed the CAYAD programme s direction and approach is consistent with the latest available evidence (Holder 2010, 2009, Alcohol and Public Policy Group 2010, Drugs and Public Policy Group 2010). There is a sound evidence base to support the effectiveness of community action on alcohol, and emerging, but relatively less, research available for illegal drugs (Drugs and Public Policy Group 2010, Miller et al 2009). The CAYAD programme has been subject to three evaluations, with positive results particularly in short and medium-term outcomes (Litmus 2009, SHORE Whariki 2006). The review found the scope is still broadly appropriate, but there is a need for some changes. These include clarifying the focus on alcohol and other drugs, strengthening communication and cohesion across the programme, and building stronger collaboration with national stakeholder organisations. The review s other findings include: stakeholders identified various success factors for the programme, including the coordination at local and national levels, the use of a community action model with a focus on policy-level strategies, and applying learning and evidence in local communities. A stand-out success factor was the particular skills, leadership, experience and credibility of the local CAYAD programme coordinators or kaimahi, which stakeholders saw as vital to success stakeholders were broadly supportive of the current service objectives, but there was debate and concern from some over Objective 4 (to reduce supply of drugs to young people) the main challenges were difficulties with collaboration at a national level, the high workload and expectations on CAYAD programme coordinators, including pressure in some cases from local communities to do work outside the programme s scope. 4
125 The review suggests a need for a clearer focus on alcohol as well as other drugs - so retaining a focus on illegal drugs. It also supports a focus on strategies to reduce both demand and supply. While the balance of strategies to reduce supply verses demand should be decided at a community level, this review suggests a need to consider strengthening the focus on: a) reducing alcohol supply and b) reducing demand for illegal drugs. This is based on the available evidence and concerns raised by some stakeholders about expectations for CAYAD s role in supply reduction work on illegal drugs, especially safety concerns. Based on the interviews and the research literature, we suggest the following range of strategies to improve the delivery and structure of the CAYAD programme. We recommend that: 1. the CAYAD programme has an explicit focus on both alcohol and other drugs (including illegal drugs and harmful legal products). We recommend: using the term alcohol and other drugs because it is used by the Ministry of Health and other national stakeholders retaining a focus on illegal drugs (while making alcohol more explicit) retaining flexibility and local autonomy to decide the most appropriate balance of work 2. the CAYAD programme has a focus on both demand and supply reduction initiatives The particular balance of work for each site needs to be decided locally, depending on local circumstances and context. However, in light of this review the CAYAD programme could consider taking a stronger focus on a) reducing alcohol supply and b) reducing demand for illegal drugs. Potentially, this could be clarified by rewording Objective 4 to Reduced demand for and supply of alcohol and other drugs to young people with a majority of work on supply reduction of alcohol and demand reduction of illegal drugs. 3. the Ministry and SHORE Whariki further develop the national coordination and consistency of the CAYAD programme by: working with the few sites/providers that are doing programme delivery more than community action, and support them to shift to genuine community action strategies 5
126 reviewing the NCAG function and membership to ensure it is providing strategic leadership at a national level. For example, consider changing the membership to be a combination of managers and kaimahi. Another option would be to select members based on particular expertise or experience 4. SHORE Whariki to consider ways to improve communication and sharing of learning: between the National Coordination Team (NCT) and local CAYAD sites. Ensure that all CAYAD staff and reference groups are aware of the NCT role and the ways to make links across the programme s various levels (eg, national and regional hui, online groups etc.) between CAYAD sites eg, allow additional time at national hui for CAYAD sites to discuss with each other what s working and why 5. the Ministry strengthen CAYAD s strategies for cross-sectoral collaboration by: developing or advocating for more collaborative funding and contracting models, such as integrated contracts between the Ministry of Health and Ministries of Social and Youth Development strengthening relationships and increasing collaboration with key national stakeholders, especially in the alcohol and drug sector, such as NZDF and ALAC. This could include formal agreement/memorandum of Understanding to work collaboratively, joint projects and communication between CAYAD sites and national stakeholder organisations ensuring the CAYAD programme is represented on the existing relevant interagency network/s at a national level eg, the Drivers of Crime Initiative, Youth Justice Advisory Group or Reducing Youth Offending further develop formal relationships/links at a national level between the CAYAD programme and key national stakeholders such as Police and MSD 6. the Ministry and SHORE Whariki encourage and support CAYAD sites to: work in partnership with Police and others (such as managers of nightclubs) to encourage greater enforcement on alcohol and other drugs link more with community-level crime prevention initiatives such as Crime Prevention Through Environmental Design and Safer Communities. Research suggests changes in physical environments and community crime prevention approaches are important in addressing illegal drugs such as methamphetamine. 6
127 & Oxford University Press and Community Development Journal All rights reserved. For permissions, please doi: /cdj/bsi053 Advance Access publication 11 March 2005 Meta-analysing community action projects in Aotearoa New Zealand Alison Greenaway and Karen Witten Abstract The current Labour Government in Aotearoa 1 New Zealand has overseen a revival of interest in devolved community decision-making and a burgeoning of locality-based community action and community development projects. This paper reports on a meta-analysis of ten community action projects. The activation, consolidation and transition or completion stages of the projects were examined to identify commonalities in structures and processes that either enhanced or impeded the projects meeting their objectives for social change. The importance of processes for critical reflection, the analysis of power dynamics between stakeholders, and recognition of the social, cultural and historical context of a project s genesis will be discussed. Introduction Community action, a strategy for creating community-based change towards social and environmental policy objectives, is growing in popularity with governments internationally and in Aotearoa New Zealand (Casswell, 2001; Social Exclusion Unit, 2001; Allen, Kilvington and Horn, 2002; Wood, 2002). Devolution to community-based decision-making has been a policy response in light of evidence that social service provision initiated purely within central government has not adequately addressed many social and environmental needs (Department of Internal Affairs, 2002). Community 2 involvement in initiatives to address community need is being heralded as a more effective way of addressing these needs (Cabinet Office, 2000). 1 Aotearoa is the Maori name for New Zealand. 2 The focus on the role of the community raised questions about who and what is the community. Issues of representation are raised as well as notions of communities of interest (see Panelli, 2001, or Valentine, 2001, for useful discussion on this). Community Development Journal Vol 41 No 2 April 2006 pp
128 144 Alison Greenaway and Karen Witten Community action is an approach to addressing specific social and/or environmental needs on a scale that is local and accessible to the participants. While being inherently interconnected, community action projects can be distinguished from community development projects by the very specific focus taken (e.g., improving river water quality or school suspension rates). Actions are aimed at changing particular behaviours, practices and or policies through a participatory and educational process involving a range of community, voluntary sector and central and local government stakeholders. Community development is more focused on enabling the wider community to address a broad range of issues in a holistic manner community development increases the likelihood that community action may take place around specific topics in a community (Ministry of Health, 2003). A key feature of community action projects is developing the skills and analysis within the community so that there can be fundamental and long-term change to problematic systems and structures (McCreanor, Moewaka Barnes and Mathews, 1998; Holder, 2000). This approach to social change has the potential to create activities that are responsive to the diverse needs of community sectors and to changing circumstances (Casswell and Stewart, 1989; Moewaka Barnes, 2000). Aspects that enhance community projects have been identified by Laverack (2001) and Labonte (1990). Laverack provides a useful overview of the operational domains of community empowerment. He highlights participation, leadership, organizational structures, problem assessment, resource mobilization, asking why questions, links with other people and organizations, and programme management. When viewed as practices these domains suggest key process indicators that can be explored as projects develop, for example, building leadership, creating participation, or assessing problems. Knowledge of these process indicators or effective change practices can be incorporated into community action projects through the use of community action research. The Public Health field in Aotearoa New Zealand draws on community action research to enhance projects through the use of formative evaluation. This form of evaluation assists in the establishment, implementation, monitoring and review of community projects by feeding knowledge of best practice into the project as it develops (Conway et al., 2000). The evaluator takes on the roles of critical friend, mentor and broker. Informed by this area of growing knowledge, researchers at the Centre for Social and Health Outcomes Research and Evaluation (SHORE) 3 set out to question whether effective components of community action research were 3 Massey University, Auckland, Aotearoa New Zealand.
129 Meta-analysing community action projects in Aotearoa New Zealand 145 evident across a diverse array of community-based projects. This investigation, the meta-analysis of community action research projects in Aotearoa New Zealand 4 aimed to identify the barriers and enhancers to achieving specific social and environmental change objectives through community action research projects. Ten diverse projects were selected and the commonalities and differences in the practices adopted by these projects were examined. Our use of the term practices incorporates activities and structures used to form projects, as well as processes used to develop projects. This paper describes the qualitative meta-analysis methodology used in the study, discusses the findings structured under the projects phases of activation, consolidation and completion or transition, and proposes a set of key principles found to be fundamental to the success or failure of the ten community action projects studied. Meta-analysis as a way of building knowledge about community action Meta-analysis at the most general level is a research method to compare, combine or synthesize the results of previous research. Hunter and Schmidt (1990) termed meta-analysis the analysis of analyses. It is undertaken so that more rigorous conclusions can be drawn than those based on the findings of individual studies. It usually, but not always implies a statistical approach to reviewing and summarizing existing research findings (Florax, de Groot and de Mooij, 2002; Cochrane Collaboration, 2003). Nijkamp and Pepping (1998) describe meta-analysis as essentially a mode of thinking and may comprise a multiplicity of different methods and technique (p. 1488). In adopting the term meta-analysis for the research described in this paper the intent was to undertake a rigorous and systematic analysis of past community action research projects. In addition to identifying and analysing the practices that enhance or hinder community action, the meta-analysis provided an opportunity to examine the varied practices for supporting and funding community action across government sectors in Aotearoa New Zealand. We were able to explore the matrix of relationships, both the vertical relationships within projects (of funder, fund holder, evaluator and community project team) and the horizontal relationships across projects (between funders, fund holders, evaluators, and community project members) that influence community action projects. Our analysis of dynamics, barriers and 4 The project was funded for the period September 2001 to July 2003 by a New Zealand government funding scheme for research that would build knowledge across government sectors. See for a copy of the full report.
130 146 Alison Greenaway and Karen Witten enhancers to change took into account community discourses as well as social and political contextual factors influencing community policy and funding practices in Aotearoa New Zealand. Case studies to explore how change is facilitated through community action Representatives of seven 5 government ministries were involved in selecting the ten community action research projects that would become the case studies. To ensure a diverse set of case studies were selected, the following two-tiered selection criteria were developed: First tier criteria 1 The project was community based with a research/evaluation component. 2 The formative evaluation was well documented. 3 Projects had been running for more than two years or had reached completion. 4 Community representatives, the researchers and funder were available, willing to participate, and knowledgeable about the history of the project. 5 Of the ten case studies, three were Maori specific and three were Pacific specific. Second tier criteria 1 The case studies spanned sectors ( funders), population groups and issues. 2 The case studies represented urban/rural localities and were geographically spread. 3 Diverse models for community action research were represented (e.g., community initiated/government agency initiated, departmental evaluation/external evaluation, single/multiple funders, projects shaped by different political and socioenvironmental contexts). In hindsight the criteria appear naively optimistic. Despite assurances from the representatives of the government ministries that numerous projects had been funded that met the criteria, delving into the details of project histories indicated otherwise. Few projects incorporated formative evaluation and well-documented examples were rare. 5 The Interdepartmental Reference Group was comprised of representatives from the Ministries of Health, Pacific Island Affairs, and Social Development; Te Puni Kokiri; and the Departments of Conservation, Internal Affairs, and Child, Youth and Family.
131 Meta-analysing community action projects in Aotearoa New Zealand 147 Additionally, in the course of the selection process it became evident that ministry representatives held a range of understandings about community action and formative evaluation. It eventuated that we were unable to identify ten community action research projects that had involved formative evaluation and even fewer with a documented evaluative record of the challenges faced, actions taken and outcomes achieved. Most evaluation reports documented what happened but not the context and basis of the decisions taken to create those actions, and thus gave little insight into the reasons why one path was taken and not another. Attempts to trace key personnel within the funding agencies also revealed a high turnover of staff in this role in government ministries. In the absence of enough documented community action research projects we revised the criteria and selected ten community action projects that had incorporated some form of reflective practice. The implications of this were that we were no longer able to focus on the documented lessons learned from incorporating the knowledge of best practice into projects via a formative evaluation process. It became an analysis of lessons learned through a variety of reflective practices (documented and oral). Consequently the primary research question driving the metaanalysis How is change facilitated through community action research projects? became How is change facilitated through community action projects? The ten projects selected are listed in Table 1. Although the criteria relating to the evaluation of projects were not met for all projects, other criteria were met. The case studies were diverse in terms of location, the focus of the projects, ethnicity, and the government sectors that funded them. Seven of the ten had some form of documented evaluation. Methods The meta-analysis used a multiple methods approach drawing on grounded theory techniques. Theory developed from a continuous interplay between analysis and the data (Strauss and Corbin, 1994, p. 273). Data were gathered and analysed and returned to participants for feedback in a series of iterative stages. For each case study relevant project and evaluation documents were collated and semi-structured face-to-face interviews were undertaken with project members, evaluators and funders. 6 The interviews with research participants gathered data on the history of projects, the local 6 The case studies developed for the meta-analysis are informative, providing a useful account of the historical, environmental and social context in which the community action projects operated (Greenaway et al., 2003a, 2003b).
132 148 Alison Greenaway and Karen Witten Table 1 Community action case studies Name of project Initial focus Demographic Sector Moerewa Community Project Alcohol and the Rural, Maori Public Health community Waitomo Papkainga Tracker Youth development Rural, Maori, Social Welfare Project Youth Pacifica Healthcare Community garden Urban, Pacific Public Health Peaceful Waves/Matangi Male Education for Urban, Pacific Public Health non-violence Whaingaroa Catchment Integrated Catchment Rural Environment Management Project management He Rangihou New Day Alcohol, drugs and Rural, Maori, Public Health Project of Opotiki Safer Communities Council young people Youth Roughcut Youth Development Project Employment training Rural, Youth Community Development Christchurch Youth Project Young people and crime Urban, Youth Police and Local Government TAIERI Trust River Catchment and Rural Environment and Catchment Project PACIFICA community health Governance and management Nationwide, Pacific Public Health Employment contexts, the practices used by groups to document their decision-making and actions, and the reflective practices 7 used to establish if and how change had occurred through their projects. We also facilitated a workshop with evaluators from the projects and liaised with peer advisors to the research project as our analysis developed. Factors that enabled or limited community change were identified in each case study. Common and contrasting practices used in the projects phases of activation, consolidation, and completion or transition were then examined across case studies and the common barriers and enhancers to change identified. This was a qualitative meta-analysis based on the review of documentation and post fact interviews and was not designed to make causal extrapolations about the practices that led to particular actions or outcomes. The scope or boundary of the analysis was quite clear in order not to attempt a meta-evaluation. 8 We did not undertake an evaluation of the projects, nor evaluate the project evaluations, or attempt to assess the impacts or outcomes of the projects. 7 See Sankaran et al. (2001), Smith, Willms and Johnson (1997), plus Reason and Bradbury (2001) for discussion on reflective practices in action research. 8 See for a good discussion on meta-evaluation.
133 Meta-analysing community action projects in Aotearoa New Zealand 149 In order to answer the question How is change facilitated through community action projects? we addressed a number of lower level research questions. The findings section is structured as responses to these research questions. Findings: How change was facilitated through ten community action projects in Aotearoa New Zealand To address our research question we identified the practices that projects had used to meet their objectives for change, and the barriers and enhancers to effecting these practices during the phases of activation, consolidation and completion/transition of the projects. We also identified how the trajectories of projects were influenced by the formation of critical relationships and coalitions, and by the approaches adopted to reflect on and review a project s progress. From this analysis we were able to conclude that there are key practices and principles that facilitate change through community action projects. What processes and activities did the projects utilize to create change? While diversity is an inherent feature of projects working to create change through community-based decision-making, there are practices and perspectives common to them all. Effective community action identified in this meta-analysis required:. building skilled leadership;. accessing adequate resourcing;. enabling infrastructural development;. creating committed strategic support and advocacy from both government agencies and community organizations;. enabling effective coordination;. vision building;. skilled facilitation of people and processes;. networking to build relationships, communication and knowledge;. accessing mentors;. effective planning; and. making opportunities for critical reflection. Projects benefited from the support of people with community development expertise and the skills to foster a project environment in which the above practices are nurtured. This expertise and skill was accessed from people in a variety of roles, including: community development advisors, fund contract managers, mentors from an umbrella organization, project coordinators, evaluators, advisors from a fund-holding organization, and trustees.
134 150 Alison Greenaway and Karen Witten What were the barriers and enhancers to creating change? Activation phase The activation phase of the project was hindered by a lack of clear purpose. When the objectives of the project and processes for working together had not been clarified across all stakeholders and clearly communicated, projects struggled with confused understandings and misinterpreted actions. Involving all key stakeholders at an early stage led to greater ongoing stakeholder support for the project. Useful activities undertaken in the activation phase included stakeholder and needs analyses, community profiling, visioning, plus strategic and action planning. Informal and formal partnerships or networks were formed and opportunities for collaborative work identified. Most projects appointed a paid coordinator and formed governance, management and/or advisory group structures. Important questions for projects to reflect upon during this phase included:. How have the needs or issues been identified, who was involved in identifying them?. What is the history and context that created the issues?. How have the issues been tackled in the past? What makes now the right time to address the issues again?. What administration structures are most appropriate for the project?. What are the most appropriate tools for planning and review?. How will stakeholders know when and if the objectives of the project have been achieved? Consolidation phase The consolidation phase involved identifying the skills and information required to make desired social/environmental changes. Building a resource and knowledge base on matters pertinent to the various projects objectives was critical to this phase. Activities and processes that developed skills, built interest and participation in the project, managed conflict and fostered a project culture were also critical. Consistent with international findings the projects were limited by shortterm funding (Blaxter, Farnell and Watts, 2003) and by funder reporting mechanisms that did not enable critical reflection or the telling of the project s story. An additional challenge projects faced was that of balancing long-term planning and strategy development with short-term action to give a project a profile within the community. Activities found to be effective during this phase included: shoulder tapping movers and shakers to get them involved in the project; planning communication pathways; forming subgroups or work streams; clarifying
135 Meta-analysing community action projects in Aotearoa New Zealand 151 tasks and roles; involving the funding organization in ongoing planning; using other organizations networks to share information; involving local talent to give the project a profile; and finding mentors, advocates and training opportunities. Some important questions for project members to reflect on in this phase were:. Are a variety of practices being used to enable diverse groups of people to participate?. What barriers are there to communication and how can these be addressed?. Where can community development skills and knowledge be accessed?. How could the project become sustainable in the longer term? Completion/transition phase The end of a funding cycle was challenging for all case studies and no project had a clear strategy for sustaining the project in the longer term. A few projects ended but most transitioned into an alternative organizational form. 9 Where projects had prioritized and planned for multistakeholder collaboration, opportunities for combined resourcing of initiatives sometimes eventuated, opening pathways for sustaining the work of the project. It was evident in all the projects that the individuals and organizations involved had developed new ways of relating and/or new skills and knowledge for addressing the issues at hand. Skills and knowledge gained through the case study projects was applied in community initiatives beyond the immediate project (community capacity building). In a few instances the projects had influenced the policy agendas of participating government agencies. Activities found useful for the transition or completion of the project included: organizing an event to commemorate the transition or completion; ensuring all stakeholders were aware of any imminent cessation, down-sizing or review of the project; and planning for closure or transition well ahead of time to manage the community implications of the change in status. Some key points for reflection at this phase included:. How do stakeholders know if the objectives of the project have been achieved?. What are some implications for policy arising out of the project? 9 Some became purely service providers and others became broader community development projects.
136 152 Alison Greenaway and Karen Witten. How will organizations sustain and build on the skills and knowledge that have been developed from participation in the project?. What new directions and opportunities are there for the project and its members? How did the relationships between evaluators, funders and community groups create change? Fundamental to all ten projects was the importance of building relationships that are transformative (Ledwith, 1997), that is, relationships between individuals and organizations that enable existing understandings and ways of working to be challenged and which required new ways to be trialed and adopted. 10 Projects were enhanced when the power dynamics influencing the relationships between stakeholders were acknowledged and addressed throughout the course of the project. 11 This analysis strongly supports arguments that the development of community capacity requires changing the dynamics of relationships between and across governmental and non-governmental organizations. Where government agencies had strong and effective relationships and worked together on particular issues, major enhancement for the community action projects was evident. Some members of projects struggled with notions of accountability when the project s funder or members of the fund-holding body held different perspectives of the issues being addressed than those held by project members. Some projects had multiple levels of accountability and drew on diverse forms and notions of community. A continuous process of negotiating power imbalances between groups or people and within and across organizations was common to most of the case study projects. Something I have a real difficulty with is around community accountability, how we keep faith with the grassroots people we work with while satisfying the people in positions of power that we are also accountable to. It s not such an issue with our major funders as with the local authority which sponsors our umbrella organization. Some of the councillors believe strongly that ratepayers money should not be spent on social issues, so they don t support our work... they also believe we re doing nothing because they don t understand what we re doing or see that it s making any change. Within a local geographical community there 10 See also Blaxter, Farnell and Watts (2003) for further detail on the skills required for this to occur. 11 Although often ignored in recent debates about community capacity building, a range of practices have been developed for analysing the power structures that influence communities. These generally draw from the work of Freire (1972).
137 Meta-analysing community action projects in Aotearoa New Zealand 153 are so many different communities with different cultures and subcultures, different and conflicting interests and different degrees of power (Interview Project Coordinator). Projects benefited where funding organizations acted as a project advocate, committed to achieving the outcomes of the project. Negotiating the funding contract and setting project objectives as part of an open process, led to realistic expectations being set for the projects. It also increased the likelihood of points of connection being found between the philosophies and practices of the community organization and the goals of the funding agency. In some instances members of community organizations rejected funding or strongly stated their terms of engagement with a project in order to ensure their vision was honoured. Complex funding structures created complex relationships within the projects. In some cases there was a fund-holding organization that played an intermediary role between the funding agency and the project leaders. The capacity of this organization to manage the funds as well as maintain credibility with both the government agencies and the community organization was critical. Projects were greatly enhanced when there was a skilled project or contract manger in the fund-holding agency who had formed strong relationships and was able to advocate for and advise the members of the project team. Projects were enhanced by the presence of people with knowledge of community development processes, information to share about the experiences of other projects, skills in visioning, planning, and negotiation with key stakeholders, and effective relationship-building practices. Knowledge and skill levels varied. However, there were key roles identified as important, including the evaluator or researcher, a mentor in an umbrella organization, and the funding advisor or project coordinator. Projects struggled when there was not ready access to skilled people. The presence of a skilled person in at least one of these roles enabled the transfer of knowledge between the funding organization and the project members. It also enhanced networking and collegial support of the project. One of the things that I ve understood is that it takes an awful lot of time to get from the starting point to the strategic action plan...the first lesson is patience, trust the process, people get there in the end if the right people are involved, but there are no shortcuts (Interview funding official). Two common statements from various informants were you have to trust the process and you ve got to know when the timing is right. Almost all of the meta-analysis participants approached community action as a developmental process. However some of the funding officials acknowledged that
138 154 Alison Greenaway and Karen Witten this perspective often sits uncomfortably alongside their focus on outcomes tailored to the three-year political cycle. Trusting the process infers a need to understand that community projects go through cycles and that significant moments or opportunities occur at a time and pace determined by the dynamics of a project. Prescribing particular actions and timeframes at the outset may not be as effective as working through a flexible though focused process. So what I started to understand... when you re funding community action, is you are actually purchasing a process... Community action contracts are always fairly light on content. They are just focused on process goals or process timelines (Interview funding official). To build and operate on a basis of trust was upheld as an ideal by numerous project stakeholders. For funding agencies this required trusting developmental processes, trusting the accountability mechanisms that community organizations had instigated, and respecting and acknowledging the skills and professionalism of community workers. Evaluators also had to trust the process of engaging with community workers, particularly in situations where evidence-based strategies were unknown. The evaluators role became one of supporting and evaluating the effectiveness of innovative strategies as a knowledge base accumulated. What were the reflective practices utilized in the ten selected projects? Reflective practices, where used, contributed significantly to the development of community action projects and to building knowledge in the communities and organizations involved. Reflective practice was used effectively in day-to-day problem solving, planning, gathering of information for decision-making, reviewing work already undertaken, documenting how the work is being done, and to question why certain decisions were made. Various forms of action reflection cycles were integrated into project planning. These included participatory research processes, formative evaluation, informal review discussions, and story telling. In several community projects an action research model was used whereby problem solving incorporated the deliberate practice of moving through cycles of reflection informed by action, and action informed by reflection (Lewin, 1952). Other projects incorporated a clear research strand that helped to inform the decision-making and planning of the project (in one case this was a formative evaluation). Other projects developed distinctive cultures of reflection leading to action through less formalized means, such as regular review meetings with key people in the community to ask questions about what is working, what is not working, and why.
139 Meta-analysing community action projects in Aotearoa New Zealand 155 For the Maori-specific projects, reflective practice was driven by a holistic worldview consistent with concepts of connection between the past, present and future. Story telling enabled spiritual, cultural, mental and physical aspects of a project to be incorporated into a reflective process. The storytelling process located project issues clearly in the context of the community and also helped to identify, prepare for, and address the impact of these issues on the community. The Maori-based projects in the study consistently reflected on dealing with the effects of colonization on a culture and people, the results of powerlessness, and general alienation from inherent cultural strengths. When we looked across the matrix of relationships involved in the three phases of community action projects the importance of organizational learning at the institutional level was emphasized. In order to facilitate community action and community action research, government funding organizations needed to develop their own institutional capacity (knowledge and resources). There was also a need for cross-fertilization of evaluation practice and the opportunity for evaluators to discuss and critique evaluation methods, especially where they operated as sole practitioners. How did these reflective practices inform the actions taken in the course of the project? The utility of reflective practices was apparent not only in the cases where it was particularly strong but in the cases where it was absent. Where reflective practice was not used, projects could lack focus, the project logic could be unclear to participants, and it became difficult for members to plan and act strategically. This lack of clarity created confusion and tension and in some cases made it difficult to communicate the vision of the project to potential stakeholders. Projects where little attention had been given to identifying measures of success struggled to build their funding base or the collaborative relationships required to take the project beyond its initial funding term. Critical reflection enabled questions to be asked throughout the life of the project about who will benefit and who will be disadvantaged by the actions taken. It also assisted the setting of realistic goals in light of the constraints they faced and the existing opportunities. Through reflective processes the context and history of the issues projects were addressing could be understood, kept to the fore and strategically accounted for in the planning of projects. Structured opportunities to meet and share experiences with other community action projects were highly valued. Such meetings were seen to provide support, motivation, the chance to reflect on the project by telling the project s story to others, and the opportunity to learn new strategies.
140 156 Alison Greenaway and Karen Witten Reflections on doing a meta-analysis of community action projects The meta-analysis was designed on the premise that it was possible to identify commonality of enhancers and barriers across community action projects. This commonality was of process and not of activities. The processes that enabled change through the community projects created a myriad of different activities, but similar outcomes (such as relationship building, participation, and increased social cohesion). Consequently, commonality of process does not mean that there are predictable paths (activities or planning) that all community projects should take. While identifying commonalities was a key objective, we were wary of missing the cases where difference was apparent and important. We constantly questioned ourselves about where differences lay across the projects. Our gaze on difference was primarily in the area of ethnic difference. Differences between Maori-specific, Pacific-specific and mixed ethnicity projects existed more in priorities and form rather than in the type of processes that were important for creating change. For example, it was evident that clarity of purpose and a common understanding of how actions related to objectives were critical to the success of all projects. As the Maori projects in the meta-analysis gained strength it was apparent that practices increasingly drew on the local context, experiences, cultural values and tikanga 12 in order to reinforce identity and provide a strong and consistent sense of purpose. Conclusion The meta-analysis of community action projects revealed overarching principles and practices critical to the development of effective community action projects. The achievement of specific social and environmental change objectives through community action required power dynamics between stakeholders to be recognized and relationships between individuals, groups and organizations to be transformed. Transformation involved creating structures for collaborative action and learning, along with power sharing and fostering of developmental practices. These structures and practices created the conditions within which change could occur. Critical reflection was necessary to achieve clarity in the project s purpose, and for the logic of actions with respect to objectives to be clear to participants. This practice also enabled the history, social and political context of issues to be addressed and factored into the design of projects. 12 Tikanga are Maori customs and traditions.
141 Meta-analysing community action projects in Aotearoa New Zealand 157 The meta-analysis method proved to be a useful tool for elevating our analysis of community action projects beyond the case study level to reveal insights not only about the project themselves but common factors that enhance or inhibit community action projects at the various levels of funding, evaluation and coordination. Acknowledgements We would like to thank the representatives of the ten community projects who contributed their time so generously to the project. We are also grateful for the support and advice of Kim Conway, Sharon Milne, Wendy Henwood and Lanuola Asiasiga at SHORE and Whariki; Will Allen and colleagues at Landcare Research; and Cynthia Maling and Adrian Portis at the Ministry of Health. We would also like to acknowledge the involvement of the Ministries of Health, Pacific Island Affairs, and Social Development; Te Puni Kōkiri; and the Departments of Conservation, Internal Affairs, and Child, Youth and Families, as members of the Interdepartmental Reference Group involved in the setting up of the meta-analysis project. The research on which the paper is based was funded by the Cross Departmental Research Pool and administered by the Ministry of Health, New Zealand. Alison Greenaway and Karen Witten work at the Centre for Social and Health Outcomes Research and Evaluation, Massey University, Auckland, Aotearoa/New Zealand. Address for correspondence: Karen Witten, Centre for Social and Health Outcomes Research and Evaluation (SHORE), Massey University, PO Box 6137, Wellesley Street, Auckland, New Zealand; k.witten@massey.ac.nz References Allen, W., Kilvington, M. and Horn, C. (2002) Using participatory and learning-based approaches for environmental management to help achieve constructive behaviour change (Landcare Research Contract Report LC0102/057 Prepared for Ministry for the Environment), May, Landcare, Lincoln. Blaxter, L., Farnell, R. and Watts, J. (2003) Difference, ambiguity and the potential for learning local communities working in partnership with local government, Community Development Journal, 38, Cabinet Office (2000) Stronger Communities Action Fund, Cabinet Paper EXG (00)118. November, Department of the Prime Minister and Cabinet, Wellington, New Zealand. Casswell, S. (2001) Community capacity building and social policy what can be achieved? Social Policy Journal of New Zealand, 17,
142 158 Alison Greenaway and Karen Witten Casswell, S. and Stewart, L. (1989) A community action project on alcohol: community organization and its evaluation, Community Health Studies, 13, Cochrane Collaboration (2003) Structure of a Cochrane Review, Cochrane Collaboration, 18 March 2004, available at Conway, K., Tunks, M., Henwood, W. and Casswell, S. (2000) Te Whanau Cadillac A Waka for Change, Health Education and Behaviour, 27, Department of Internal Affairs (2002) A Framework for Developing Sustainable Communities, Department of Internal Affairs, Wellington, New Zealand, available at Florax, R., de Groot, H. and de Mooij, R. (2002) Meta-Analysis: A Tool for Upgrading Inputs of Macroeconomic Policy Models, Tinbergen Institute Discussion Paper TI /3, Tinbergen Institute, Amsterdam, available at Friere, P. (1972) Pedagogy of the Oppressed, Penguin, Harmondsworth. Greenaway, A., Milne, S., Henwood, W., Asiasiga, L. and Witten, K. (2003a) A Meta Analysis of Community Action Projects, Vol. I, Centre for Social and Health Outcomes Research and Evaluation (SHORE), Massey University, Auckland, available at Greenaway, A., Milne, S., Henwood, W., Asiasiga, L. and Witten, K. (2003b) A Meta Analysis of Community Action Projects, Vol. II, Centre for Social and Health Outcomes Research and Evaluation (SHORE), Massey University, Auckland, available at Holder, H. D. (2000) Community prevention of alcohol problems, Addictive Behaviors, 25, Hunter, J. and Schmidt, F. (1990) Methods of integrating findings across studies, in Methods of Meta-Analysis: Correcting Error and Bias in Research Findings, Sage, Newbury Park, pp Labonte, R. (1990) Empowerment: notes on professional and community dimensions, Canadian Review of Social Policy, 26, Laverack, G. (2001) An identification and interpretation of organizational aspects of community improvement, Community Development Journal, 36, Ledwith, M. (1997) Participating in Transformation: Towards a Working Model of Community Empowerment, Ventura Press, Birmingham. Lewin, K. (1952) Field Theory in Social Science: Selected Theoretical Papers, edited by Dorwin Cartwright Tavistock, London. McCreanor, T., Moewaka Barnes, H. and Mathews, T. (1998) Limited Impact Evaluation for the Waikato Rural Drink Drive Project, Alcohol & Public Health Research Unit, Auckland. Ministry of Health (2003) Community Project Indicators Framework (CPIF) Its Use in Community Projects (Working draft), Ministry of Health, Wellington, New Zealand. Moewaka Barnes, H. (2000) Collaboration in community action: A successful partnership between indigenous communities and researchers, Health Promotion International, 15, Nijkamp, P. and Pepping, G. (1998) A meta-analytic evaluation of sustainable city initiatives, Urban Studies, 35,
143 Meta-analysing community action projects in Aotearoa New Zealand 159 Panelli, R. (2001) Narratives of community and change in a contemporary rural setting: the case of Duaringa, Queensland, Australian Geographical Studies, 39, Reason, P. and Bradbury, H. (2001) Handbook of Action Research, Sage Publications Ltd., London. Sankaran, S., Dick, B., Passfield, R. and Swepson, P. (eds) (2001) Effective Change Management Using Action Learning and Action Research: Concepts, Frameworks, Processes, Applications. Southern Cross University Press, Lismore. Smith, S., Willms, D. and Johnson, N. (1997) Nurtured by Knowledge: Learning to Do Participatory Action Research, The Apex Press, New York. Social Exclusion Unit (2001) A New Commitment to Neighbourhood Renewal: National Strategy for Action, ODPM Publications, Wetherby, West Yorkshire, available at index.htm Strauss, A. and Corbin, J. (1994) Grounded theory methodology, in N. K. Denzin and Y. Lincoln, eds, The Handbook of Qualitative Research, Sage Publications, Thousand Oaks, pp Valentine, G. (2001) Social Geographies: Space and Society, Pearson Education, Harlow, Essex. Wood, M. (2002) Resident Participation in Urban and Community Renewal, Australian Housing and Urban Research Institute UNSW/UWS Research Centre, Melbourne, available at social_housing/items/00003-upload pdf
144
145 Section 8 Presentation Skills
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
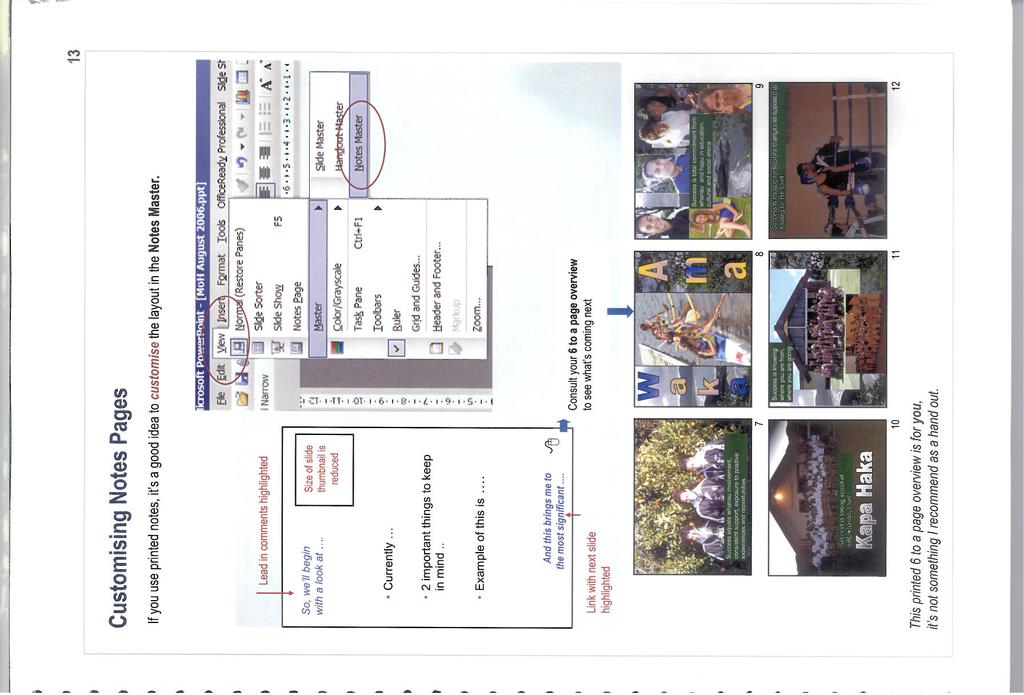
162
163
164
165
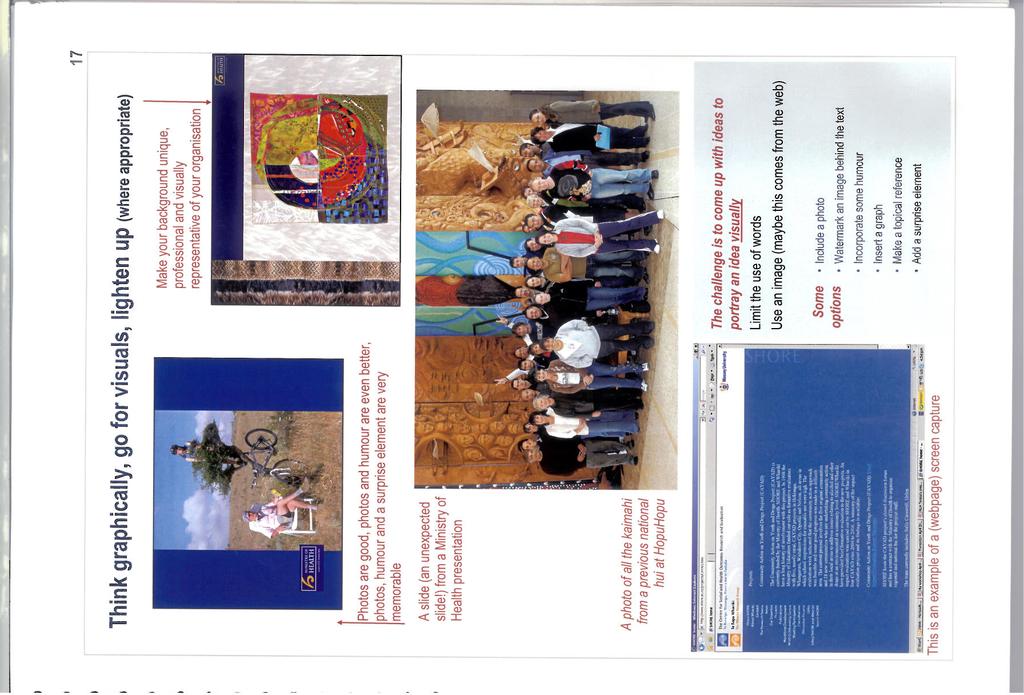
166
Cancer Control Council Evaluation and Monitoring Framework
 Cancer Control Council Evaluation and Monitoring Framework Table of contents 1. Purpose...1 2. Background...1 3. Clarification of key tasks...2 4. International evaluation and monitoring frameworks...3
Cancer Control Council Evaluation and Monitoring Framework Table of contents 1. Purpose...1 2. Background...1 3. Clarification of key tasks...2 4. International evaluation and monitoring frameworks...3
The Vision. The Objectives
 The Vision Older people participate to their fullest ability in decisions about their health and wellbeing and in family, whānau and community life. They are supported in this by co-ordinated and responsive
The Vision Older people participate to their fullest ability in decisions about their health and wellbeing and in family, whānau and community life. They are supported in this by co-ordinated and responsive
Recommendations from the Report of the Government Inquiry into:
 Recommendations from the Report of the Government Inquiry into: mental health addiction. Easy Read Before you start This is a long document. While it is written in Easy Read it can be hard for some people
Recommendations from the Report of the Government Inquiry into: mental health addiction. Easy Read Before you start This is a long document. While it is written in Easy Read it can be hard for some people
Health and Wellbeing Strategy 2016 to 2021 Summary Document
 Health and Wellbeing Strategy 2016 to 2021 Summary Document 1 Health and Wellbeing Strategy 2016-2021 Summary document Introduction The Doncaster Health and Wellbeing Board is a formal Board which was
Health and Wellbeing Strategy 2016 to 2021 Summary Document 1 Health and Wellbeing Strategy 2016-2021 Summary document Introduction The Doncaster Health and Wellbeing Board is a formal Board which was
Hertfordshire Young People s Substance Misuse Strategic Plan
 Hertfordshire Young People s Substance Misuse Strategic Plan 2014 15 1 1. Introduction and context Young people misusing substances can cause harm to our communities through crime and antisocial behaviour,
Hertfordshire Young People s Substance Misuse Strategic Plan 2014 15 1 1. Introduction and context Young people misusing substances can cause harm to our communities through crime and antisocial behaviour,
Guidelines for the development of. Alcohol Accords
 Guidelines for the development of Alcohol Accords Guidelines for the development of Alcohol Accords 3 Three key messages If you are interested in a proven and practical way to make alcohol consumption
Guidelines for the development of Alcohol Accords Guidelines for the development of Alcohol Accords 3 Three key messages If you are interested in a proven and practical way to make alcohol consumption
STRATEGIC PLAN 2014 to 2017
 STRATEGIC PLAN 2014 to 2017 September 2014 1 P a g e KHNZ s STRATEGIC PLAN Contents Page 1. Introduction to the Strategic Plan 3 2. About Kidney Health New Zealand 4 3. The Challenges 6 4. Strategic Context
STRATEGIC PLAN 2014 to 2017 September 2014 1 P a g e KHNZ s STRATEGIC PLAN Contents Page 1. Introduction to the Strategic Plan 3 2. About Kidney Health New Zealand 4 3. The Challenges 6 4. Strategic Context
An evidence rating scale for New Zealand
 Social Policy Evaluation and Research Unit An evidence rating scale for New Zealand Understanding the effectiveness of interventions in the social sector Using Evidence for Impact MARCH 2017 About Superu
Social Policy Evaluation and Research Unit An evidence rating scale for New Zealand Understanding the effectiveness of interventions in the social sector Using Evidence for Impact MARCH 2017 About Superu
Local Healthwatch Quality Statements. February 2016
 Local Healthwatch Quality Statements February 2016 Local Healthwatch Quality Statements Contents 1 About the Quality Statements... 3 1.1 Strategic context and relationships... 5 1.2 Community voice and
Local Healthwatch Quality Statements February 2016 Local Healthwatch Quality Statements Contents 1 About the Quality Statements... 3 1.1 Strategic context and relationships... 5 1.2 Community voice and
Co-ordinated multi-agency support for young carers and their families
 Practice example Co-ordinated multi-agency support for young carers and their families What is the initiative? A partnership between a young carers service and a council Who runs it? Off The Record s Young
Practice example Co-ordinated multi-agency support for young carers and their families What is the initiative? A partnership between a young carers service and a council Who runs it? Off The Record s Young
SLIGO CITY ALCOHOL STRATEGY. Prevent & Reduce Alcohol Related Harm
 SLIGO CITY ALCOHOL STRATEGY Prevent & Reduce Alcohol Related Harm 2018 2023 Foreword The Sligo Healthy Ireland Project in conjunction with the HSE North West Regional Drug & Alcohol Task Force has developed
SLIGO CITY ALCOHOL STRATEGY Prevent & Reduce Alcohol Related Harm 2018 2023 Foreword The Sligo Healthy Ireland Project in conjunction with the HSE North West Regional Drug & Alcohol Task Force has developed
Working Together Protocol for the Strategic Partnership Boards in Somerset
 Health and Wellbeing Working Together Protocol for the Strategic Partnership Boards in Contents 1. Statement of commitment... 1 2. Collective responsibilities... 1 3. Individual Partnership Board Responsibilities...
Health and Wellbeing Working Together Protocol for the Strategic Partnership Boards in Contents 1. Statement of commitment... 1 2. Collective responsibilities... 1 3. Individual Partnership Board Responsibilities...
The functions of the LSCB prescribed in the Local Safeguarding Children Boards Regulations 2006 are as follows:
 Draft Joint Working Protocol between Barnet s Health and Wellbeing Board, Local Safeguarding Children Board and Local Safeguarding Adults Board July 2014 1. Introduction There are three statutory boards
Draft Joint Working Protocol between Barnet s Health and Wellbeing Board, Local Safeguarding Children Board and Local Safeguarding Adults Board July 2014 1. Introduction There are three statutory boards
Youth Justice National Development Team. Youth Justice National Development Team Annual Report. Fiona Dyer
 Youth Justice National Development Team 2012-2013 Youth Justice National Development Team Annual Report Fiona Dyer National Development Team April 2013 0 Annual Report April 2012 March 2013 Youth Justice
Youth Justice National Development Team 2012-2013 Youth Justice National Development Team Annual Report Fiona Dyer National Development Team April 2013 0 Annual Report April 2012 March 2013 Youth Justice
NHS Grampian. Job Description RP10253
 NHS Grampian Job Description RP10253 SECTION 1 JOB IDENTIFICATION Job Title: Aberdeenshire Smoking Cessation Co-ordinator Department(s): Aberdeenshire CHP Public Health Location: Based at Inverurie Hospital
NHS Grampian Job Description RP10253 SECTION 1 JOB IDENTIFICATION Job Title: Aberdeenshire Smoking Cessation Co-ordinator Department(s): Aberdeenshire CHP Public Health Location: Based at Inverurie Hospital
1. Introduction. Background
 Glasgow City Alcohol and Drug Partnership Prevention and Recovery Strategy 2011-2014 1. Introduction 1.1 Glasgow City needs to take action to address major issues around alcohol and drug misuse. The City
Glasgow City Alcohol and Drug Partnership Prevention and Recovery Strategy 2011-2014 1. Introduction 1.1 Glasgow City needs to take action to address major issues around alcohol and drug misuse. The City
Partnership between the government, municipalities, NGOs and the industry: A new National Alcohol Programme in Finland
 Partnership between the government, municipalities, NGOs and the industry: A new National Alcohol Programme in Finland The structure and the aims of the National Alcohol Programme Marjatta Montonen, Programme
Partnership between the government, municipalities, NGOs and the industry: A new National Alcohol Programme in Finland The structure and the aims of the National Alcohol Programme Marjatta Montonen, Programme
Te Kökiri. Mental Health and Addiction Action Plan
 Te Kökiri The Mental and Addiction Action Plan 2006 2015 Citation: Minister of. 2006. Te Kökiri: The Mental and Addiction Action Plan 2006 2015. Wellington:. Published in August 2006 by the, PO Box 5013,
Te Kökiri The Mental and Addiction Action Plan 2006 2015 Citation: Minister of. 2006. Te Kökiri: The Mental and Addiction Action Plan 2006 2015. Wellington:. Published in August 2006 by the, PO Box 5013,
The Children and Social Work Act The role of voluntary sector CSE services in new safeguarding arrangements
 THE INTERNATIONAL CENTRE: RESEARCHING CHILD SEXUAL EXPLOITATION, VIOLENCE AND TRAFFICKING The Children and Social Work Act The role of voluntary sector CSE services in new safeguarding arrangements January
THE INTERNATIONAL CENTRE: RESEARCHING CHILD SEXUAL EXPLOITATION, VIOLENCE AND TRAFFICKING The Children and Social Work Act The role of voluntary sector CSE services in new safeguarding arrangements January
Norfolk and Suffolk NHS Foundation Trust. Suicide Prevention Strategy,
 Norfolk and Suffolk NHS Foundation Trust Suicide Prevention Strategy, 2017-2022 Foreword It is likely that we will know someone, directly or indirectly, who has died by suicide. It may also be possible
Norfolk and Suffolk NHS Foundation Trust Suicide Prevention Strategy, 2017-2022 Foreword It is likely that we will know someone, directly or indirectly, who has died by suicide. It may also be possible
What can NHS Health Scotland do to reduce health inequalities? Questions for applying the Health Inequalities Action Framework
 What can NHS Health Scotland do to reduce health inequalities? Questions for applying the Health Inequalities Action Framework Introduction Definition: health inequalities are the differences in health
What can NHS Health Scotland do to reduce health inequalities? Questions for applying the Health Inequalities Action Framework Introduction Definition: health inequalities are the differences in health
Question: I m worried my child is using illegal drugs, what should I do about it?
 Question: I m worried my child is using illegal drugs, what should I do about it? Answer: Many parents worry about whether their son or daughter is using illegal drugs and what they should do about it.
Question: I m worried my child is using illegal drugs, what should I do about it? Answer: Many parents worry about whether their son or daughter is using illegal drugs and what they should do about it.
A proposal for collaboration between the Psychometrics Committee and the Association of Test Publishers of South Africa
 A proposal for collaboration between the Psychometrics Committee and the Association of Test Publishers of South Africa 27 October 2015 Table of contents Introduction... 3 Overview of the Association of
A proposal for collaboration between the Psychometrics Committee and the Association of Test Publishers of South Africa 27 October 2015 Table of contents Introduction... 3 Overview of the Association of
Assessing the Risk: Protecting the Child
 Assessing the Risk: Protecting the Child Impact and Evidence briefing Key findings is an assessment service for men who pose a sexual risk to children and are not in the criminal justice system. Interviews
Assessing the Risk: Protecting the Child Impact and Evidence briefing Key findings is an assessment service for men who pose a sexual risk to children and are not in the criminal justice system. Interviews
POLICY ANALYST JOB DESCRIPTION
 POLICY ANALYST JOB DESCRIPTION August 2010 Location: Hours of Work: Responsible to: National Office, Auckland 30 hours per week Executive Director The NZAF has an expectation that all staff will: Demonstrate
POLICY ANALYST JOB DESCRIPTION August 2010 Location: Hours of Work: Responsible to: National Office, Auckland 30 hours per week Executive Director The NZAF has an expectation that all staff will: Demonstrate
HEALTHWATCH AND HEALTH AND WELLBEING BOARDS
 HEALTHWATCH AND HEALTH AND WELLBEING BOARDS INTRODUCTION In April 2013 local Healthwatch organisations came into being. The national body, Healthwatch England, with clear responsibilities and powers, was
HEALTHWATCH AND HEALTH AND WELLBEING BOARDS INTRODUCTION In April 2013 local Healthwatch organisations came into being. The national body, Healthwatch England, with clear responsibilities and powers, was
PROMOTION AND MAINTENANCE OF NEW ZEALAND SIGN LANGUAGE
 Office of the Minister for Disability Issues Chair Cabinet Social Policy Committee PROMOTION AND MAINTENANCE OF NEW ZEALAND SIGN LANGUAGE Proposal 1 This paper proposes the establishment of an advisory
Office of the Minister for Disability Issues Chair Cabinet Social Policy Committee PROMOTION AND MAINTENANCE OF NEW ZEALAND SIGN LANGUAGE Proposal 1 This paper proposes the establishment of an advisory
Research for Development Impact Network
 Research for Development Impact Network Mid-term Review of Research for Development Impact (RDI) Network Program Executive Summary and Management Response Submitted: 11 July 2017 This report has been prepared
Research for Development Impact Network Mid-term Review of Research for Development Impact (RDI) Network Program Executive Summary and Management Response Submitted: 11 July 2017 This report has been prepared
Worcestershire's Autism Strategy
 Worcestershire Health and Well-being Board Worcestershire's Autism Strategy 2014-17 Fulfilling and Rewarding Lives for adults with autism spectrum conditions Find out more online: www.worcestershire.gov.uk/healthandwellbeingboard
Worcestershire Health and Well-being Board Worcestershire's Autism Strategy 2014-17 Fulfilling and Rewarding Lives for adults with autism spectrum conditions Find out more online: www.worcestershire.gov.uk/healthandwellbeingboard
Performance Management Framework Outcomes for Healthwatch Kent June 2016
 Performance Management Framework Outcomes for Healthwatch Kent June 2016 A. Making a difference locally Outcome Statutory Function Examples of Good Outcomes/ 1. Local Healthwatch investigations bring added
Performance Management Framework Outcomes for Healthwatch Kent June 2016 A. Making a difference locally Outcome Statutory Function Examples of Good Outcomes/ 1. Local Healthwatch investigations bring added
Peer Support Association. Strategic Plan and Development Strategy
 Peer Support Association Strategic Plan and Development Strategy Outcomes of the Strategic Development Day for Peer Supporters 29 th November 2014 Hosted by CoMHWA and Carers WA Executive Summary This
Peer Support Association Strategic Plan and Development Strategy Outcomes of the Strategic Development Day for Peer Supporters 29 th November 2014 Hosted by CoMHWA and Carers WA Executive Summary This
Monitoring and Evaluation Framework for the Tackling Indigenous Smoking Programme
 Monitoring and Evaluation Framework for the Tackling Indigenous Smoking Programme 30 June 2016 Introduction... 3 Context the TIS programme... 4 2.1 TIS programme objectives... 5 2.2 The delivery of the
Monitoring and Evaluation Framework for the Tackling Indigenous Smoking Programme 30 June 2016 Introduction... 3 Context the TIS programme... 4 2.1 TIS programme objectives... 5 2.2 The delivery of the
Hounslow Safeguarding Children Board. Training Strategy Content.. Page. Introduction 2. Purpose 3
 Hounslow Safeguarding Children Board. Training Strategy 2018-2020. Content.. Page Introduction 2 Purpose 3 What does the Training Strategy hope to achieve?. 4 Review.. 4 Local context.. 4 Training sub
Hounslow Safeguarding Children Board. Training Strategy 2018-2020. Content.. Page Introduction 2 Purpose 3 What does the Training Strategy hope to achieve?. 4 Review.. 4 Local context.. 4 Training sub
Model the social work role, set expectations for others and contribute to the public face of the organisation.
 AMHP Competency PCF capability mapping: Experienced level social worker. 1. Professionalism: Identify and behave as a professional social worker, committed to professional development: Social workers are
AMHP Competency PCF capability mapping: Experienced level social worker. 1. Professionalism: Identify and behave as a professional social worker, committed to professional development: Social workers are
Drug Prevention Policy in Jamaica
 Drug Prevention Policy in Jamaica Like all international and regional efforts, Jamaica s efforts at drug control are premised on the adoption and articulation of three main United Nations Drug Control
Drug Prevention Policy in Jamaica Like all international and regional efforts, Jamaica s efforts at drug control are premised on the adoption and articulation of three main United Nations Drug Control
Engaging with our stakeholders
 Engaging with our stakeholders Report to: Board Date: 27 June 2014 Report by: Report No: Jenny Copland, Senior Communications Adviser Agenda Item: 6.3 PURPOSE OF REPORT To propose a format and processes
Engaging with our stakeholders Report to: Board Date: 27 June 2014 Report by: Report No: Jenny Copland, Senior Communications Adviser Agenda Item: 6.3 PURPOSE OF REPORT To propose a format and processes
Report-back on the Alcohol and Other Drug Treatment Court Pilot and other AOD-related Initiatives
 In confidence Office of the Minister of Justice Office of the Minister of Cabinet Social Policy Committee Report-back on the Alcohol and Other Drug Treatment Court Pilot and other AOD-related Initiatives
In confidence Office of the Minister of Justice Office of the Minister of Cabinet Social Policy Committee Report-back on the Alcohol and Other Drug Treatment Court Pilot and other AOD-related Initiatives
WHY DO WE NEED TO ENGAGE WITH OUR COMMUNITIES?
 WHY DO WE NEED TO ENGAGE WITH OUR COMMUNITIES? Our communities have a central role to play in influencing and shaping what happens in Barnsley. In our corporate plan we recognise that our role as a local
WHY DO WE NEED TO ENGAGE WITH OUR COMMUNITIES? Our communities have a central role to play in influencing and shaping what happens in Barnsley. In our corporate plan we recognise that our role as a local
Alcohol Consumption and Alcohol-related Health Outcomes
 Alcohol Consumption and Alcohol-related Health Outcomes Key points Total alcohol consumption per person has decreased 25 percent since 1980, although there has been a slight increase in the past year.
Alcohol Consumption and Alcohol-related Health Outcomes Key points Total alcohol consumption per person has decreased 25 percent since 1980, although there has been a slight increase in the past year.
Community Innovation Fund. Guidelines
 Community Innovation Fund Guidelines 02 February 2015 1 Community Innovation Fund (CIF)- Guidance Notes 1. Introduction The purpose of the Community Innovation Fund (CIF) is to support the strategic aim
Community Innovation Fund Guidelines 02 February 2015 1 Community Innovation Fund (CIF)- Guidance Notes 1. Introduction The purpose of the Community Innovation Fund (CIF) is to support the strategic aim
ADVOCACY IN ACTION TO ACHIEVE GENDER EQUALITY AND THE SUSTAINABLE DEVELOPMENT GOALS IN KENYA
 ADVOCACY IN ACTION TO ACHIEVE GENDER EQUALITY AND THE SUSTAINABLE DEVELOPMENT GOALS IN KENYA Wherever inequality lives, there stands a girl or woman able to turn the tide of adversity into a tidal wave
ADVOCACY IN ACTION TO ACHIEVE GENDER EQUALITY AND THE SUSTAINABLE DEVELOPMENT GOALS IN KENYA Wherever inequality lives, there stands a girl or woman able to turn the tide of adversity into a tidal wave
Services. Related Personal Outcome Measure: Date(s) Released: 21 / 11 / / 06 /2012
 Released: 21 / 11 / / 06 /2012") Title: Individual Planning Autism Services Type: Services Policy / Procedure Details Related Personal Outcome Measure: I choose Personal Goals Code: 1.1 Original Details Version Previous Version(s) Details
Title: Individual Planning Autism Services Type: Services Policy / Procedure Details Related Personal Outcome Measure: I choose Personal Goals Code: 1.1 Original Details Version Previous Version(s) Details
Communications and engagement for integrated health and care
 Communications and engagement for integrated health and care Report for Northern CCG Committee Mary Bewley STP Communications Lead 6 th September 2018 Background Aims Objectives Challenges Collaborative
Communications and engagement for integrated health and care Report for Northern CCG Committee Mary Bewley STP Communications Lead 6 th September 2018 Background Aims Objectives Challenges Collaborative
Birmingham Homelessness Prevention Strategy 2017+
 Birmingham Homelessness Prevention Strategy 2017+ 24 August - 5 October 2017 Consultation Summary Birmingham Homelessness Prevention Strategy 2017+ 24 August 5 October 2017 What are we trying to achieve?
Birmingham Homelessness Prevention Strategy 2017+ 24 August - 5 October 2017 Consultation Summary Birmingham Homelessness Prevention Strategy 2017+ 24 August 5 October 2017 What are we trying to achieve?
CRIMINAL JUSTICE SECTOR. Strategic Intent YEAR PLAN
 CRIMINAL JUSTICE SECTOR Strategic Intent 2018 4-YEAR PLAN A safe, fair and prosperous society Trust in the criminal justice system 2 3 What we aim for WHERE WE WANT TO BE IN THE NEXT 4 YEARS Our vision
CRIMINAL JUSTICE SECTOR Strategic Intent 2018 4-YEAR PLAN A safe, fair and prosperous society Trust in the criminal justice system 2 3 What we aim for WHERE WE WANT TO BE IN THE NEXT 4 YEARS Our vision
Bradford District Community Advice Network (CAN)
") Bradford District Community Advice Network (CAN) March 2015 Nick Hodgkinson, Project Co-ordinator The CAN in a nutshell registered charity, association CIO since Oct 2014, with organisational (not individual)
Bradford District Community Advice Network (CAN) March 2015 Nick Hodgkinson, Project Co-ordinator The CAN in a nutshell registered charity, association CIO since Oct 2014, with organisational (not individual)
Cannabis Legalization August 22, Ministry of Attorney General Ministry of Finance
 Cannabis Legalization August 22, 2018 Ministry of Attorney General Ministry of Finance Federal Cannabis Legalization and Regulation The federal Cannabis Act received Royal Assent on June 21, 2018 and will
Cannabis Legalization August 22, 2018 Ministry of Attorney General Ministry of Finance Federal Cannabis Legalization and Regulation The federal Cannabis Act received Royal Assent on June 21, 2018 and will
Part 1: Introduction & Overview
 Part 1: Introduction & Overview We envision a collaborative, participative partnership around IDU that: Provides all relevant and interested stakeholders with a voice and role. Promotes awareness of the
Part 1: Introduction & Overview We envision a collaborative, participative partnership around IDU that: Provides all relevant and interested stakeholders with a voice and role. Promotes awareness of the
POSITION DESCRIPTION
 POSITION DETAILS: POSITION DESCRIPTION TITLE: Mental Health Smoke Free Coordinator REPORTS TO: Nurse Director Mental Health & Addiction Directorate LOCATION: Across the Directorate AUTHORISED BY: Nurse
POSITION DETAILS: POSITION DESCRIPTION TITLE: Mental Health Smoke Free Coordinator REPORTS TO: Nurse Director Mental Health & Addiction Directorate LOCATION: Across the Directorate AUTHORISED BY: Nurse
Primary Health Networks
 Primary Health Networks Drug and Alcohol Treatment Activity Work Plan 2016-17 to 2018-19 South Eastern Melbourne PHN When submitting this Activity Work Plan 2016-2018 to the Department of Health, the PHN
Primary Health Networks Drug and Alcohol Treatment Activity Work Plan 2016-17 to 2018-19 South Eastern Melbourne PHN When submitting this Activity Work Plan 2016-2018 to the Department of Health, the PHN
Our Pledge to Children in Care and Care Leavers
 Our Pledge to Children in Care and Care Leavers 1 Designed and printed by Bristol City Council, Bristol Design OCTOBER 15 BD7047 Bristol Corporate Parenting Strategy The Bristol Pledge The pledge is a
Our Pledge to Children in Care and Care Leavers 1 Designed and printed by Bristol City Council, Bristol Design OCTOBER 15 BD7047 Bristol Corporate Parenting Strategy The Bristol Pledge The pledge is a
The National perspective Public Health England s vision, mission and priorities
 The National perspective Public Health England s vision, mission and priorities Dr Ann Hoskins Director Children, Young People and Families Public Health England May 2013 Mission Public Health England
The National perspective Public Health England s vision, mission and priorities Dr Ann Hoskins Director Children, Young People and Families Public Health England May 2013 Mission Public Health England
Working Better Together on Safeguarding: Annual Reports of the Bradford Safeguarding Children Board (BSCB) and the Safeguarding Adults Board (SAB)
 and the Safeguarding Adults Board (SAB)") Report of the Director of Health and Wellbeing and the Director of Children s Services to the meeting of Bradford and Airedale Health and Wellbeing Board to be held on 29 th November 2016. Subject: O Working
Report of the Director of Health and Wellbeing and the Director of Children s Services to the meeting of Bradford and Airedale Health and Wellbeing Board to be held on 29 th November 2016. Subject: O Working
ACHIEVING SMOKEFREE AOTEAROA BY2025
 ACHIEVING SMOKEFREE AOTEAROA BY2025 Monitoring and evaluation plan CONTENTS Acknowledgements 1 Introduction 2 Logic model 3 Sources of information 4 Monitoring progress towards the SFA 2025 goal 4 System
ACHIEVING SMOKEFREE AOTEAROA BY2025 Monitoring and evaluation plan CONTENTS Acknowledgements 1 Introduction 2 Logic model 3 Sources of information 4 Monitoring progress towards the SFA 2025 goal 4 System
Mental Health & Wellbeing Strategy
 getting it right for e ery child in Aberdeenshire Mental Health & Wellbeing Strategy 2016-2019 NHS Grampian 2 Our vision is that all children and young people are mentally flourishing! Introduction and
getting it right for e ery child in Aberdeenshire Mental Health & Wellbeing Strategy 2016-2019 NHS Grampian 2 Our vision is that all children and young people are mentally flourishing! Introduction and
CORPORATE REPORT Communication strategy
 CORPORATE REPORT Communication Strategy 2014-17 1 Introduction This strategy sets out the Commission s goals and objectives in relation to its communication activities for the next three years. It has
CORPORATE REPORT Communication Strategy 2014-17 1 Introduction This strategy sets out the Commission s goals and objectives in relation to its communication activities for the next three years. It has
Meeting The Needs Of Vulnerable People: Finalist
 Meeting The Needs Of Vulnerable People: Finalist LinkLiving: SmartLiving Peer Education Project Summary SmartLiving is a peer education project which seeks to support young people aged 16-24 in sustaining
Meeting The Needs Of Vulnerable People: Finalist LinkLiving: SmartLiving Peer Education Project Summary SmartLiving is a peer education project which seeks to support young people aged 16-24 in sustaining
Developing a drug monitoring system for New Zealand: IDMS
 Developing a drug monitoring system for New Zealand: IDMS 2006-2016 NDEWS webinar "Examining Global Drug Early Warning Systems 26 th September 2017 Chris Wilkins SHORE & Whariki Research Centre College
Developing a drug monitoring system for New Zealand: IDMS 2006-2016 NDEWS webinar "Examining Global Drug Early Warning Systems 26 th September 2017 Chris Wilkins SHORE & Whariki Research Centre College
Reducing harms from alcohol in our communities
 Reducing harms from alcohol in our communities Position statement Counties Manukau Health (CM Health) cares about the achievement of equitable health and wellbeing for the population we serve. Alcohol-related
Reducing harms from alcohol in our communities Position statement Counties Manukau Health (CM Health) cares about the achievement of equitable health and wellbeing for the population we serve. Alcohol-related
Guidelines for Developing a School Substance Use Policy. Table of Contents
 Guidelines for Developing a School Substance Use Policy Table of Contents Introduction 2 Why a policy on Substance Use?.2 What is a Substance Use Policy and how is it developed? 3 STEP 1: Establish a core
Guidelines for Developing a School Substance Use Policy Table of Contents Introduction 2 Why a policy on Substance Use?.2 What is a Substance Use Policy and how is it developed? 3 STEP 1: Establish a core
You said, We did. How your comments and feedback have helped us to add value and improve local services
 ,. How your comments and feedback have helped us to add value and improve local services A lot of our members have advised that although the CCG spends a lot of time engaging with stakeholders, it does
,. How your comments and feedback have helped us to add value and improve local services A lot of our members have advised that although the CCG spends a lot of time engaging with stakeholders, it does
Community alcohol detoxification in primary care
 Community alcohol detoxification in primary care 1. Purpose The purpose of this primary care enhanced service is to improve the health and quality of life of people whose health may be compromised by their
Community alcohol detoxification in primary care 1. Purpose The purpose of this primary care enhanced service is to improve the health and quality of life of people whose health may be compromised by their
Working in Partnership to meet the Childcare Need A Toolkit to support schools and providers / childminders in the provision of out of school care
 ACTION FOR CHILDREN Working in Partnership to meet the Childcare Need A Toolkit to support schools and providers / childminders in the provision of out of school care This toolkit is designed as a step
ACTION FOR CHILDREN Working in Partnership to meet the Childcare Need A Toolkit to support schools and providers / childminders in the provision of out of school care This toolkit is designed as a step
PUBLIC HEALTH INTERVENTION GUIDANCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE PUBLIC HEALTH INTERVENTION GUIDANCE 1 Guidance title SCOPE Interventions delivered in primary and secondary schools to prevent and/or reduce alcohol
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE PUBLIC HEALTH INTERVENTION GUIDANCE 1 Guidance title SCOPE Interventions delivered in primary and secondary schools to prevent and/or reduce alcohol
Tobacco-Control Policy Workshop:
 Tobacco-Control Policy Workshop: Goal: to introduce Mega-Country leaders to an effective policy framework for tobacco control and to develop skills to promote policy implementation. Objectives: As a result
Tobacco-Control Policy Workshop: Goal: to introduce Mega-Country leaders to an effective policy framework for tobacco control and to develop skills to promote policy implementation. Objectives: As a result
Meeting of Bristol Clinical Commissioning Group Governing Body
 Meeting of Bristol Clinical Commissioning Group Governing Body To be held on Tuesday 24 February 2015 commencing at 13:30 at the Vassall Centre, Gill Avenue, Bristol, BS16 2QQ Title: OFSTED Report Agenda
Meeting of Bristol Clinical Commissioning Group Governing Body To be held on Tuesday 24 February 2015 commencing at 13:30 at the Vassall Centre, Gill Avenue, Bristol, BS16 2QQ Title: OFSTED Report Agenda
CONSTITUTION SOUTHAMPTON CHILDREN & YOUNG PEOPLE S TRUST PARTNERSHIP
 CONSTITUTION SOUTHAMPTON CHILDREN & YOUNG PEOPLE S TRUST PARTNERSHIP 1. AIMS To unify and co-ordinate services for children, young people and families in line with the Children Act 2004 To oversee the
CONSTITUTION SOUTHAMPTON CHILDREN & YOUNG PEOPLE S TRUST PARTNERSHIP 1. AIMS To unify and co-ordinate services for children, young people and families in line with the Children Act 2004 To oversee the
Equally Well framework for collaborative action
 Equally Well framework for collaborative action How we work and what actions we can take to improve the physical health of people who experience mental health and addiction problems Phase 3: 2015 Contents
Equally Well framework for collaborative action How we work and what actions we can take to improve the physical health of people who experience mental health and addiction problems Phase 3: 2015 Contents
An Active Inclusive Capital. A Strategic Plan of Action for Disability in London
 An Active Inclusive Capital A Strategic Plan of Action for Disability in London Angus Robertson Director of Operations, London Sport In 2015, London s Blueprint for a Physically Active City was launched,
An Active Inclusive Capital A Strategic Plan of Action for Disability in London Angus Robertson Director of Operations, London Sport In 2015, London s Blueprint for a Physically Active City was launched,
Multi-agency Safeguarding Training Strategy
 Wandsworth Safeguarding Children Board Multi-agency Safeguarding Training Strategy 2017-18 Foreword This strategy sets out our framework and direction for ensuring that all staff and volunteers working
Wandsworth Safeguarding Children Board Multi-agency Safeguarding Training Strategy 2017-18 Foreword This strategy sets out our framework and direction for ensuring that all staff and volunteers working
Welcome to Pathways. - Auckland - Information about Pathways services in the Auckland region.
 Welcome to Pathways - Auckland - Information about Pathways services in the Auckland region. Alongside you in your recovery journey Welcome to Pathways. We re here to support you in your journey to being
Welcome to Pathways - Auckland - Information about Pathways services in the Auckland region. Alongside you in your recovery journey Welcome to Pathways. We re here to support you in your journey to being
HC 963 SesSIon november Department of Health. Young people s sexual health: the National Chlamydia Screening Programme
 Report by the Comptroller and Auditor General HC 963 SesSIon 2008 2009 12 november 2009 Department of Health Young people s sexual health: the National Chlamydia Screening Programme 4 Summary Young people
Report by the Comptroller and Auditor General HC 963 SesSIon 2008 2009 12 november 2009 Department of Health Young people s sexual health: the National Chlamydia Screening Programme 4 Summary Young people
Tenant & Service User Involvement Strategy
 Tenant & Service User Involvement Strategy Policy No: HM 07 Page: 1 of 9 Tenant & Service User Involvement Strategy 1. Introduction 1.1 Loreburn's Mission Statement is "Delivering Excellence" and we see
Tenant & Service User Involvement Strategy Policy No: HM 07 Page: 1 of 9 Tenant & Service User Involvement Strategy 1. Introduction 1.1 Loreburn's Mission Statement is "Delivering Excellence" and we see
State of the Nation A stocktake of how New Zealand is dealing with the issue of drugs
 State of the Nation 2018 A stocktake of how New Zealand is dealing with the issue of drugs Published: January 2019 Tēnā koe The New Zealand Drug Foundation s vision is for an Aotearoa free from drug harm.
State of the Nation 2018 A stocktake of how New Zealand is dealing with the issue of drugs Published: January 2019 Tēnā koe The New Zealand Drug Foundation s vision is for an Aotearoa free from drug harm.
SCS topic headings: Partnership Working, Home Safety, Safety of Vulnerable Groups, Personal Safety
 Title: The Leeds Distraction Burglary Initiative Authors: Stuart Lister, David Wall and Jane Bryan (Centre for Criminal Justice Studies, University of Leeds) Date published: 2004 Funding body: Home Office
Title: The Leeds Distraction Burglary Initiative Authors: Stuart Lister, David Wall and Jane Bryan (Centre for Criminal Justice Studies, University of Leeds) Date published: 2004 Funding body: Home Office
Report to Renfrewshire Child Protection Committee. Dorothy Hawthorn, Head of Child Care and Criminal Justice
 Report to Renfrewshire Child Protection Committee Date: 25th March 2015 From: Subject: Dorothy Hawthorn, Head of Child Care and Criminal Justice Child Sexual Exploitation 1. Purpose of report To furnish
Report to Renfrewshire Child Protection Committee Date: 25th March 2015 From: Subject: Dorothy Hawthorn, Head of Child Care and Criminal Justice Child Sexual Exploitation 1. Purpose of report To furnish
Mapping A Pathway For Embedding A Strengths-Based Approach In Public Health. By Resiliency Initiatives and Ontario Public Health
 + Mapping A Pathway For Embedding A Strengths-Based Approach In Public Health By Resiliency Initiatives and Ontario Public Health + Presentation Outline Introduction The Need for a Paradigm Shift Literature
+ Mapping A Pathway For Embedding A Strengths-Based Approach In Public Health By Resiliency Initiatives and Ontario Public Health + Presentation Outline Introduction The Need for a Paradigm Shift Literature
Alberta Alcohol and Drug Abuse Commission. POSITION ON ADDICTION AND MENTAL HEALTH February 2007
 Alberta Alcohol and Drug Abuse Commission POSITION ON ADDICTION AND MENTAL HEALTH POSITION The Alberta Alcohol and Drug Abuse Commission (AADAC) recognizes that among clients with addiction problems, there
Alberta Alcohol and Drug Abuse Commission POSITION ON ADDICTION AND MENTAL HEALTH POSITION The Alberta Alcohol and Drug Abuse Commission (AADAC) recognizes that among clients with addiction problems, there
Community Development Division: Funding Process Study Update
 Community Development Division: Funding Process Study Update Background and Context Two key research studies the Race to Equity Report and a study of Madison s Social Sector by Joiner Sandbrook LLC--highlighted
Community Development Division: Funding Process Study Update Background and Context Two key research studies the Race to Equity Report and a study of Madison s Social Sector by Joiner Sandbrook LLC--highlighted
Engaging People Strategy
 Engaging People Strategy 2014-2020 Author: Rosemary Hampson, Public Partnership Co-ordinator Executive Lead Officer: Richard Norris, Director, Scottish Health Council Last updated: September 2014 Status:
Engaging People Strategy 2014-2020 Author: Rosemary Hampson, Public Partnership Co-ordinator Executive Lead Officer: Richard Norris, Director, Scottish Health Council Last updated: September 2014 Status:
DOING IT YOUR WAY TOGETHER S STRATEGY 2014/ /19
 DOING IT YOUR WAY TOGETHER S STRATEGY 2014/15 2018/19 Why is Together s role important? Experiencing mental distress is frightening and can lead to long-term disadvantage. Mental illness still carries
DOING IT YOUR WAY TOGETHER S STRATEGY 2014/15 2018/19 Why is Together s role important? Experiencing mental distress is frightening and can lead to long-term disadvantage. Mental illness still carries
Joint Mental Health Commissioning Strategy for Adults
 Joint Mental Health Commissioning Strategy for Adults 2014-2019 Summary Developed in partnership with: NHS Ipswich and East Suffolk CCG, NHS West Suffolk CCG, Suffolk Constabulary and Suffolk County Council
Joint Mental Health Commissioning Strategy for Adults 2014-2019 Summary Developed in partnership with: NHS Ipswich and East Suffolk CCG, NHS West Suffolk CCG, Suffolk Constabulary and Suffolk County Council
HEALTH AND SPORT COMMITTEE AGENDA. 14th Meeting, 2018 (Session 5) Tuesday 1 May 2018
 Tuesday 1 May 2018") HS/S5/18/14/A HEALTH AND SPORT COMMITTEE AGENDA 14th Meeting, 2018 (Session 5) Tuesday 1 May 2018 The Committee will meet at 10.00 am in the James Clerk Maxwell Room (CR4). 1. Scottish Health Council Review:
HS/S5/18/14/A HEALTH AND SPORT COMMITTEE AGENDA 14th Meeting, 2018 (Session 5) Tuesday 1 May 2018 The Committee will meet at 10.00 am in the James Clerk Maxwell Room (CR4). 1. Scottish Health Council Review:
State of Support for the Healthwatch network
 The Rt Hon Jeremy Hunt MP Secretary of State Department of Health Richmond House 79 Whitehall London SW1A 2NS 04 December 2017 Dear Secretary of State, State of Support for the Healthwatch network Please
The Rt Hon Jeremy Hunt MP Secretary of State Department of Health Richmond House 79 Whitehall London SW1A 2NS 04 December 2017 Dear Secretary of State, State of Support for the Healthwatch network Please
An Overview of the Government of Canada s Approach to Legalize, Regulate and Restrict Access to Cannabis. February 2018
 An Overview of the Government of Canada s Approach to Legalize, Regulate and Restrict Access to Cannabis February 2018 I m here today to provide 1 2 3 Context for the Government of Canada s plan to legalize,
An Overview of the Government of Canada s Approach to Legalize, Regulate and Restrict Access to Cannabis February 2018 I m here today to provide 1 2 3 Context for the Government of Canada s plan to legalize,
National Inspection of services that support looked after children and care leavers
 National Inspection of services that support looked after children and care leavers Introduction Children and young people that are looked after and those leaving care need the best support possible. Support
National Inspection of services that support looked after children and care leavers Introduction Children and young people that are looked after and those leaving care need the best support possible. Support
Barnsley Youth Justice Plan 2017/18. Introduction
 Barnsley Youth Justice Plan 2017/18 Introduction Barnsley s Youth Justice Service sits within the Local Authority s Targeted Youth Support Service. The governance of the provision has changed in 2016/17.
Barnsley Youth Justice Plan 2017/18 Introduction Barnsley s Youth Justice Service sits within the Local Authority s Targeted Youth Support Service. The governance of the provision has changed in 2016/17.
Hobsons Bay City Council Submission: Review of the Liquor Control Reform Act 1998
 14 December 2016 Office of Liquor, Gaming and Racing Email: lcra.review@justice.vic.gov.au Ask for: Phone: Our Ref: Kathleen McClusky 9932 1004 A2515449 To whom it may concern, Hobsons Bay City Council
14 December 2016 Office of Liquor, Gaming and Racing Email: lcra.review@justice.vic.gov.au Ask for: Phone: Our Ref: Kathleen McClusky 9932 1004 A2515449 To whom it may concern, Hobsons Bay City Council
Message From the Minister
 May 2002 Message From the Minister A basic principle of the health and social services system is that people have a responsibility to maintain their own health. The Department of Health and Social Services
May 2002 Message From the Minister A basic principle of the health and social services system is that people have a responsibility to maintain their own health. The Department of Health and Social Services
CSSIW Participation Plan. Working Together to Improve Social Care Services
 CSSIW Participation Plan Working Together to Improve Social Care Services Printed on recycled paper Print ISBN 978 0 7504 8280 6 Digital ISBN 978 0 7504 8281 3 Crown copyright 2012 WG16698 Introduction
CSSIW Participation Plan Working Together to Improve Social Care Services Printed on recycled paper Print ISBN 978 0 7504 8280 6 Digital ISBN 978 0 7504 8281 3 Crown copyright 2012 WG16698 Introduction
Workforce Analysis: Children and Young People s Mental Health and Wellbeing Wider system
 Workforce Analysis: Children and Young People s Mental Health and Wellbeing Wider system This questionnaire is aimed at any member of the workforce supporting the mental health and wellbeing for children
Workforce Analysis: Children and Young People s Mental Health and Wellbeing Wider system This questionnaire is aimed at any member of the workforce supporting the mental health and wellbeing for children
YOUTH HOMELESSNESS IN AUSTRALIA
 YOUTH HOMELESSNESS IN AUSTRALIA Numbers Resources Drivers The numbers. Australia has a population of about 23 million. On the last census count there were over 104,000 homeless and about 5,000 rough sleepers.
YOUTH HOMELESSNESS IN AUSTRALIA Numbers Resources Drivers The numbers. Australia has a population of about 23 million. On the last census count there were over 104,000 homeless and about 5,000 rough sleepers.
Evaluation of Satellite Clubs: FINAL REPORT
 Sport England Evaluation of Satellite Clubs: FINAL REPORT EXECUTIVE SUMMARY 3rd Floor Fourways House 57 Hilton Street Manchester M1 2EJ +44 (0) 161 244 5418 www.substance.net 1 Sport England: Evaluation
Sport England Evaluation of Satellite Clubs: FINAL REPORT EXECUTIVE SUMMARY 3rd Floor Fourways House 57 Hilton Street Manchester M1 2EJ +44 (0) 161 244 5418 www.substance.net 1 Sport England: Evaluation
Ayrshire Employability Project
 Integration Joint Board 18 th January 2018 Agenda Item 8 Subject: Transforming Care After Treatment (TCAT) Ayrshire Employability Project Purpose: Recommendation: To update the Integration Joint Board
Integration Joint Board 18 th January 2018 Agenda Item 8 Subject: Transforming Care After Treatment (TCAT) Ayrshire Employability Project Purpose: Recommendation: To update the Integration Joint Board
Children and Young People s Trust
 THREE FOUR ONE TWO Children and Young People s Trust Annual Event, 10 th November 2017 Update Newsletter, January 2018 More than 45 leaders and practitioners from across a range of partnership organisations
THREE FOUR ONE TWO Children and Young People s Trust Annual Event, 10 th November 2017 Update Newsletter, January 2018 More than 45 leaders and practitioners from across a range of partnership organisations
Our passion for recovery. The difference we made in 2016
 Our passion for recovery The difference we made in 2016 welcome from karen At Phoenix we have always known that people can and do recover from the most entrenched of addictions. We also know that whilst
Our passion for recovery The difference we made in 2016 welcome from karen At Phoenix we have always known that people can and do recover from the most entrenched of addictions. We also know that whilst
Healthwatch Cheshire CIC Board Recruitment Information Pack
 Healthwatch Cheshire CIC Board Recruitment Information Pack ` Healthwatch Cheshire CIC is looking to recruit 7 lay people from all communities across both Cheshire East and Cheshire West to become members
Healthwatch Cheshire CIC Board Recruitment Information Pack ` Healthwatch Cheshire CIC is looking to recruit 7 lay people from all communities across both Cheshire East and Cheshire West to become members
Alcohol as a public health issue in croatia. Croatian Institute of Public Health Prof. Danijela Štimac Grbić, MD.,PhD.,MPH.
 Alcohol as a public health issue in croatia Croatian Institute of Public Health Prof. Danijela Štimac Grbić, MD.,PhD.,MPH. Alcohol consumption in Croatia 01 02 03 the total APC (in litres of pure alcohol)
Alcohol as a public health issue in croatia Croatian Institute of Public Health Prof. Danijela Štimac Grbić, MD.,PhD.,MPH. Alcohol consumption in Croatia 01 02 03 the total APC (in litres of pure alcohol)
AND THE COMMUNITY HEALTH PARTNERSHIP INCLUDING THE HEALTH IMPROVEMENT STANDING GROUP. DATE Paper 3.7
 DRAFT PARTNERSHIP AGREEMENT BETWEEN THE EDINBURGH PARTNERSHIP AND THE COMMUNITY HEALTH PARTNERSHIP INCLUDING THE HEALTH IMPROVEMENT STANDING GROUP INTRODUCTION DATE.. 2011 Paper 3.7 1. The Edinburgh Partnership
DRAFT PARTNERSHIP AGREEMENT BETWEEN THE EDINBURGH PARTNERSHIP AND THE COMMUNITY HEALTH PARTNERSHIP INCLUDING THE HEALTH IMPROVEMENT STANDING GROUP INTRODUCTION DATE.. 2011 Paper 3.7 1. The Edinburgh Partnership
Family Violence Integration Project. Eastern Community Legal Centre
 Family Violence Integration Project Eastern Community Legal Centre Mid Term Report February 2012 Prepared by Clare Keating, Effective Change Pty Ltd Introduction Commencing in February 2011, the Family
Family Violence Integration Project Eastern Community Legal Centre Mid Term Report February 2012 Prepared by Clare Keating, Effective Change Pty Ltd Introduction Commencing in February 2011, the Family