DSM-5 AND ASAM CRITERIA. Presented by Jaime Goffin, LCSW
|
|
|
- Debra Gregory
- 6 years ago
- Views:
Transcription
1 DSM-5 AND ASAM CRITERIA Presented by Jaime Goffin, LCSW
2 MODULE 1: GOALS & OBJECTIVES What is your experience with using ASAM and DSM 5 criteria? What are your learning expectations for today?
3 GOAL FOR TRAINING To develop and/or enhance the knowledge and skills to make more informed and accurate clinical decisions and write concise clinical justifications for those decisions using the DSM-5 and ASAM Criteria 3 rd Edition.
4 OBJECTIVES Identify and explain rationale and benefits of using the ASAM Criteria to make patient placements Identify characteristics and differentiate between various levels of care Identify and differentiate between ASAM s six dimensions of assessment Identify information to formulate a dimension risk rating Learn how dimension risk rating and clinical justification directly drive treatment planning
5 CRITICAL THINKING Practitioners who are willing to call into question the assumptions underlining their customary, habitual ways of thinking and acting, and are ready to think and act differently on the basis of critical questioning...
6 TRAINING IS NOT Designed to answer all of your questions regarding the assessment, placement and treatment of persons with addictive disorders Sufficient to make you competent in the use of ASAM criteria, but rather an introduction to it. Further practice, training and supervision is required to learn how to use the criteria successfully.
7 MODULE 2: CHALLENGES FACING THE FIELD 1. Standardization in the collection of client information 2. Consistency of the interpretation of data collected for patient placement and treatment planning purposes 3. Matching of appropriate evidence based, proven and effective treatment interventions to the client s identified problems 4. Correct implementation of evidenced based interventions 5. Development and implementation of policies and procedures to monitor the above.
8 MODULE 3: RATIONALE & BENEFITS OF STANDARDIZED ASSESSMENT CRITERIA
9 WHAT DOES THE RESEARCH SAY? Clients that are mismatched to treatment have lower retention rates and poorer outcomes. Less treatment is NOT Good. More treatment is NOT Good.
10 WHAT S HAPPENING IN SOME PROGRAMS Client s are being referred to wrong levels of care. Client s assessed are referred to, and treated in the agency conducting the assessment Assessments don t justify the recommendations being made. Clinical justifications are provided
11 WHAT IF.. We asked 200 Counselors to make a patient placement decision and provide a clinical justification for that decision? All given the same case.

12 WHAT DO YOU THINK HAPPENED?


13 BENEFITS OF USING EVIDENCE BASED CRITERIA Improve Performance and Treatment Outcomes Increase Motivation, Engagement and Retention Rates More Efficient and Effective Utilization Reviews Use of a common language
14 IMPORTANT! Tools and Criteria s are NOT substitutes for GOOD Clinical Judgment. Tools and Criteria s support, guide and enhance GOOD Clinical Judgment.
15 MODULE 4: ASAM CRITERIA The ASAM Criteria describes in detail an IDEAL continuum of care with the various services and interventions provide at each levels.
16 HISTORY: UNDERLYING PRINCIPLES CLINICAL CARE Complications-driven Treatment No diagnosis of Substance Use Disorder Treatment of Complications of the addiction with no continuing care Relapse Triggers treatment of complications only. Companies.net
17 DIAGNOSIS, PROGRAM-DRIVEN TREATMENT Diagnosis determines treatment Treatment is the primary program and aftercare Relapse- triggers a repeat of the program Companies.net
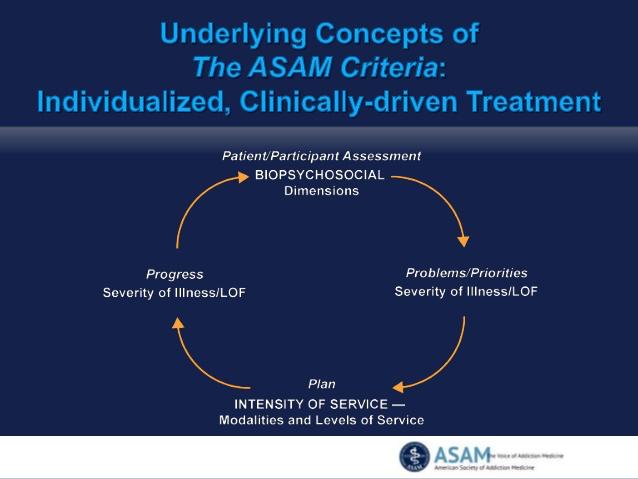
18 INDIVIDUALIZED, CLINICALLY-DRIVEN
19 CLIENT-DIRECTED, OUTCOME INFORMED
20 GUIDING PRINCIPLES OF THE ASAM CRITERIA 2013 Moving from one-dimensional to multidimensional assessment
21 PRINCIPLE #2 Moving from program-driven to clinically driven and outcomes-driven treatment
22 PRINCIPLE #3 Moving from fixed length of service to variable length of service
23 PRINCIPLE #4 Identifying adolescent-specific needs
24 PRINCIPLE #5 Clarifying the goals of treatment
25 PRINCIPLE #6 Moving away from using treatment failure as an admission prerequisite
26 PRINCIPLE #7 Moving toward an interdisciplinary, team approach to care
27 PRINCIPLE #8 Clarifying the role of the physician
28 PRINCIPLE #9 Focusing on treatment outcomes
29 PRINCIPLE #10 Engaging with Informed Consent
30 PRINCIPLE #11 Clarifying Medical Necessity
31 PRINCIPLE #12 Harnessing ASAM s Definition of Addiction
32 MODULE 5:WHATS NEW IN DSM-5 11 Criteria for Substance-Related and Addictive Disorders DSM 5 Severity How to code using new manual
33 CRITERIA 1-4: IMPULSE CONTROL 1.Use in larger amounts or longer than intended 2.Desire or unsuccessful effort to cut down 3.Great deal of time using or recovering 4.Craving or strong urge to use
34 CRITERIA 5-7: SOCIAL IMPAIRMENT 5. Role obligation failure 6. Continued use despite social/interpersonal problems 7. Sacrificing activities to use or because of use
35 CRITERIA 8-9: RISKY USE 8. Use in situations where it is hazardous 9. Continued use despite knowledge of having physical or psychological problem caused or exacerbated by use
36 CRITERIA 10-11: PHARMACOLOGICAL 10. Tolerance 11. Withdrawal
37 SUD CRITERIA PRIMARILY IN SEVERE DESIGNATION ONLY The Big Five: Wanting to cut down/unable to do so Craving with compulsion to use Sacrifice activities to use Failure at role fulfillment due to use Withdrawal symptoms
38 CRITERIA PREVALENT IN MILD & MODERATE GROUPS Unplanned use Time spent using Medical/psych. consequences of use Use where impairment is dangerous Interpersonal conflicts Legal problems and use to relieve emotional distress similar in distribution to these
39 CLINICAL IMPLICATIONS Most of those in the mild designation can probably benefit from moderation and harm reduction strategies Those in the severe designation will require more intensive and extended services where abstinence is essential to recovery The moderate group may have characteristics that fit the mild or severe characteristics.
40 SEVERITY SCALE DSM-5 The severity of each Substance Use Disorder is based on: 0 criteria or 1 criteria: No diagnosis 2-3 criteria: Mild Substance Use Disorder 4-5 criteria: Moderate Substance Use Disorder 6 or more criteria: Severe Substance Use Disorder
41 EXAMPLE IN DSM Alcohol Use Disorder, severe 303 Alcohol Intoxication with use disorder, severe Alcohol Withdrawal, with perceptual disturbances Other Alcohol-Induced Disorder Unspecified Alcohol-Related Disorder
42 SEVERITY AN COURSE SPECIFIERS In early remission: Full criteria for SUD was previously met None of the criteria for SUD have been met for at least 3 months, but for less than 12 months Except for Criteria 4 (Craving or a strong desire to use)
43 IN A SUSTAINED REMISSION: Full criteria for SUD were previously met None of the criteria for SUD have been met at any time during a period of 12 months or longer, Except for Criteria 4 (Craving or a strong desire to use)
44 IN A CONTROLLED ENVIRONMENT This additional specifier is used if the individual is in an environment where access to alcohol or controlled substances is restricted. Examples of these environments are closely supervised and substance-free jails, therapeutic communities and locked hospital units.
45 HOW TO CODE Diagnosis code for specific substance such as Alcohol Use, followed by any medical conditions, psychosocial stressors, followed by a severity rating of mild, moderate or severe based on criterion met. Other specifiers would include in early remission, sustained remission, on maintenance therapy and in controlled environment.
46 DIAGNOSTIC STRATEGIES Assessing for substance use disorder: In assessing for substance use disorder, one initially attempts to determine whether the patient s substance use is causing negative consequences. If such consequences are significant and recurrent in a 12 month-period, then diagnosis of substance use disorder is warranted.
47 DIAGNOSTIC STRATEGIES CONT. Even if client does not meet criteria for substance use disorder, there may be substance-induced withdrawal or intoxication; or variety of substance-induced disorders including anxiety, depression, psychosis, sleep disorder or sexual dysfunction.
48 MODULE 6: WHAT S NOT NEW IN ASAM The six assessment dimensions The overall levels of care (though not Roman numerals) for addiction management The decision rules, which link Intensity of Service back to the Severity of Illness maintained except for some updates in Withdrawal Management ( Detox )
49 WHAT S NEW IN ASAM New Title: The ASAM Criteria Treatment Criteria for Addictive, Substance- Related, and Co-Occurring Conditions Shift away from placement criteria to treatment criteria: it s more than just placement
50 WHAT S NEW IN ASAM Diagnostic Admission Criteria terminology changed to be compatible with DSM-5 Section on working with managed care Table of contents Re-ordered to be more user-friendly Follows the flow from Historical Foundations to Guiding Principles to Assessment, Service Planning, and Placement decisions
51 WHAT S NEW IN ASAM Adolescent Criteria Still separate criteria for adolescents Consolidated Adult & Adolescent content on principles to minimize redundancy, while preserving adolescent-specific content
52 WHAT S NEW IN ASAM Appendices Withdrawal Management instruments Dimension 5 constructs Glossary
53 WHAT S NEW IN ASAM Withdrawal Management The wording in the Levels of Care Former section Detoxification becomes Withdrawal Management Levels are now called WM-1, WM-2, WM-3, and WM-4 New approaches described to support increased use of less intensive levels of care for safe/effective management of withdrawal
54 WHAT S NEW IN ASAM Withdrawal Management New approaches described to support increased use of less intensive levels of care for safe/effective management of withdrawal A broader range of severity of withdrawal syndromes is discussed in The Criteria as being able to be safely and appropriately managed on an outpatient basis
55 WHAT S NEW IN ASAM Updated/revised terminology Contemporary, strength-based, recovery oriented: dual diagnosis becomes co-occurring disorders inappropriate use of substances becomes high risk use of substances
56 WHAT S NEW IN ASAM Opioid use disorder specialized services Opioid Maintenance Therapy (OMT) becomes Opioid Treatment Services (OTS) Opioid antagonist medication (naltrexone) Opioid agonist medications (methadone, buprenorphine) Their use in OTPs (regulated Opioid Treatment Programs for methadone) or in office-based opioid treatment (OBOT for buprenorphine)
57 NEW CONTENT AND SECTIONS Additional text to improve application to address addiction treatment for Special Populations: Older Adults Persons in Safety Sensitive Occupations Parents with Children and Pregnant Women Persons in the Criminal Justice System (CJS)
58 NEW CONTENT AND SECTIONS Additional text to address treatment of conditions not traditionally included in specialty addiction treatment services: Tobacco Use Disorder Gambling Disorder
59 NEW CONTENT AND SECTIONS Revision of the text to address emerging issues: Healthcare Reform and the integration of addiction treatment into general medical care The role of physicians on the care team, addiction specialist physicians in particular (addiction medicine physicians, addiction psychiatrists)
60 NEW CONTENT AND SECTIONS Inclusion of Recovery Oriented System of Care to facilitate understanding of addiction treatment with a recovery oriented chronic disease management continuum, rather than as a repeated, disconnected acute episodes of treatment for acute complications of addiction and/or repeated and disconnected admissions to programs that employ rigid lengths of stay in which patients are placed.
61 NEW CONTENT AND SECTIONS A new section on Gambling Disorder that is consistent with ASAM s definition of addiction Pathological pursuit of reward or relief can involve not just the use of psychoactive substances but other certain behaviors.. Tobacco Disorder chapter to reflect on the treatment field s inconsistencies in, and even ambivalence about, viewing this addiction as similar to alcohol and substances.
62 MODULE 7: ASAM LOC Level 0.5 Early Intervention Level 1 Outpatient Services Level 2.1 Intensive Outpatient Services Level 2.5 Partial Hospitalization Services Level 3.1 Clinically Managed Low-Intensity Residential Level 3.3 Clinically Managed Population-Specific High-Intensity Residential (Adult Only) Level 3.5 Clinical Managed High-Intensity Residential Services (Adult Criteria) Level 3.5 Clinical Managed Medium-Intensity Residential Services (Adolescent Criteria)
63 LEVELS CONT. Level 3.7 Medically Monitored Intensive Inpatient Services (Adult Criteria) Level 3.7 Medically Monitored High-Intensity Inpatient Services (Adolescent Criteria) Level 4 Medically-Managed Intensive Inpatient Services Opioid Treatment Services (OTS) Withdrawal Management
64 WITHDRAWAL MANAGEMENT Level 1-Withdrawal Management (Outpatient), ambulatory withdrawal management without extended on-site monitoring Level 2-Withdrawal Management (Intensive Outpatient and Partial Hospitalization), ambulatory withdrawal management with extended on-site monitoring Level 3.2-Withdrawal Management (clinically-managed) residential withdrawal management Level 3.7-Withdrawal Management (medically-monitored) residential withdrawal management. Inpatient detox is ASAM Level 4-Withdrawal Management and is medically managed. Inpatient detox is a service provided in an inpatient hospital setting. Level 4-Withdrawal Management Intensive Inpatient Withdrawal Management
65 INFORMED CONSENT Proposed modalities The risks and benefits Appropriate alternative treatment Risks of treatment versus no treatment
66 EXCEPTIONS TO THE PLACEMENT Lack of availability of services Failure of a patient to progress at a given level of care State laws that differ from ASAM criteria
67 RISK RATING SYSTEM High, Medium, Low pgs Point Scale, Page 57 0: Low Risk 1: mild 2: moderate 3: serious 4: utmost severity
68 MATCHING DIMENSIONAL SEVERITY Step 1: Risk of Imminent danger Step 2: Determine risk rating in each dimension Step 3: Identify appropriate types of services Step 4: Development of initial treatment plan Step 5: Ongoing Utilization Management throughout continuum of care
69 DIMENSION 1: ACUTE INTOXICATION AND/OR WITHDRAWAL POTENTIAL What risk is associated with the patient s current level of acute intoxication? Are intoxication management services needed? Is there significant risk of severe withdrawal symptoms, seizures or medical complications? Are there current signs of withdrawal? Standardized withdrawal scale score? Vital signs? Does the patient have supports to assist in ambulatory withdrawal management?
70 DIMENSION 2: BIOMEDICAL CONDITIONS AND COMPLICATIONS Are there current physical illnesses, other withdrawal that need to be addressed? Are there chronic conditions that need stabilization or ongoing disease management? Is there a communicable disease present? Is the patient pregnant, what is her pregnancy history?
71 DIMENSION 3: EMOTIONAL, BEHAVIORAL, COGNITIVE COMPLICATIONS Are there current psychiatric illnesses or psychological, behavioral, emotional or cognitive problems that need to be addressed? Are there chronic conditions that affect treatment such as bipolar or anxiety? Do any emotional, behavioral, or cognitive signs or symptoms appear to be an expected part of the addictive disorder?
72 DIMENSION 3CONT. Are they severe enough to warrant specific mental health treatment, even if symptoms are caused by substance use? Is the patient able to manage the activities of daily living? Can he or she cope with any emotional, behavioral or cognitive problems?
73 DIMENSION 3 RISK DOMAINS Dangerousness/Lethality Interference with Addiction Recovery Efforts Social Functioning Ability for Self-Care Course of Illness
74 DIMENSION 4: READINESS TO CHANGE How aware is the patient of the relationship between his or her alcohol, tobacco, or other drug use or behaviors involved in the pathological pursuit of reward or relief and his or her negative life consequences? How ready, willing, or able does the patient feel to make changes? How much does the patient feel in control of his or her treatment services? Assess each treatment issue for separate stage of change.
75 DIMENSION 5: RELAPSE/CONTINUED USE Historical Pattern of Use Pharmacologic Responsivity External Stimuli Responsivity Cognitive and Behavioral Measures of Strengths and Weaknesses What are your policy and procedures to deal with Dim 5 situations?
76 DIMENSION 5: RELAPSE, CONTINUED USE OR POTENTIAL Is the patient in immediate danger of continued severe mental health distress and/or alcohol, tobacco and/or drug use? Does the patient have any recognition or understanding of, or skills in coping with his or her addictive, co-occurring, or mental disorder? Have addiction and/or psychotropic medications assisted in recovery before? What are the person s skills in coping with protracted withdrawal, cravings, or impulses?
77 DIMENSION 5 CONT. How well can the patient cope with negative effects, peer pressure, and stress without recurrence of addictive thinking and behavior? How severe are the problems and further distress that may continue or reappear if the patient is not successfully engaged in treatment? How aware is the patient of relapse triggers and skills to control addiction impulses or impulses to harm self or others?
78 DIMENSION 6: RECOVERY ENVIRONMENT Do any family members, significant others, living situations, or school work situations pose a threat to the patient s safety or engagement in treatment? Does the individual have supportive friendships, financial resources, or educational or vocational resources that can increase the likelihood of successful recovery? Are there legal, vocational, regulatory (eg professional licensure), social service agency, or criminal justice mandates that may enhance the person s motivation for engagement in treatment if indicated? Are there transportation, childcare, housing, or employment issues that need to be clarified and addressed?
79 DECISION HIERARCHY Dimensions 1, 2, 3, generally help indicate Inpatient or Outpatient Dimensions 4, 5, 6 generally help indicate the intensity of outpatient ( there are often times that Dim 5 and 6 will indicate inpatient treatment. Each dimension receives a Risk Rating
80 CASE PRACTICE Dimension Severity? Services Needed? Level of Care Recommendation?
81 LENGTH OF STAY AND DISCHARGE Clinically Driven NOT Program Driven
82 LOC RECOMMENDATION PROCESS Interpret the Assessment Information Select Risk Rating and Write Clinical Justification for each Dim Asses if the Risk Status on some of Dimensions Influence/Increase the risk of other Dimensions Assess Recovery & Other Support Services Available Level of Care/Service Recommendation Treatment Planning
83 5 M S Motivate - Dimension 4 Manage All Six Dimensions Medication Dimensions 1, 2, 3, 5 Meetings Dimensions 2, 3, 4, 5, 6 Monitor- All Six Dimensions
84 SEVERITY OF ASSESSMENT THE 3 H S HISTORY HERE AND NOW HOW WORRIED NOW
85 CLINICAL JUSTIFICATION Risk Rating Clinical Justification- each dimensional summary includes a statement indicating severity/risk rating. Level of Care Clinical Justification
86 LEVEL OF CARE RECOMMENDATION 1. Clinical justification is a summary of the evidence that supports and justifies a clinical decision. 2. Clinical justifications generally include symptoms that meet established criteria: ASAM, DSM5 other tools Treatment professionals are responsible for documenting clinical decisions and justifying them with evidence.

87 THANK YOU!
88 REFERENCES American Psychiatric Association, Diagnostic and Statistical manual of Mental Disorders, Fifth Edition, American Society of Addiction Medicine, 3 rd edition, Mee-Lee, David (2013): The New edition of the ASAM Criteria: What s New and Why Counselor Vol. 14. No.4 pp August 2013 Mee-Lee, David (2013): How to Really Use the New Edition of The ASAM Criteria: What To Do & What Not to Do. Counselor Vol. 14. No. 6 pp December 2013.
ASAM CRITERIA 3 rd Edition
 ASAM CRITERIA 3 rd Edition Presented by Mark Disselkoen, LCSW, LADC CASAT Based on DSM 5 & The ASAM Criteria Manual The ATTC Network Ten Regional Centers Central Rockies ATTC is now the Mountain Plains
ASAM CRITERIA 3 rd Edition Presented by Mark Disselkoen, LCSW, LADC CASAT Based on DSM 5 & The ASAM Criteria Manual The ATTC Network Ten Regional Centers Central Rockies ATTC is now the Mountain Plains
Understanding and Using Current ASAM Criteria. for Ce-Classes.com
 Understanding and Using Current ASAM Criteria for Ce-Classes.com Learning Objectives After completing this course, participants will: Identify ASAM and the history of its development Describe how ASAM
Understanding and Using Current ASAM Criteria for Ce-Classes.com Learning Objectives After completing this course, participants will: Identify ASAM and the history of its development Describe how ASAM
Referral to Treatment: Utilizing the ASAM Criteria
 Referral to Treatment: Utilizing the ASAM Criteria AOAAM Essentials in Addiction Medicine October 22, 2016 East Lansing, MI Stephen A. Wyatt, DO Medical Director, Addiction Medicine Behavioral Health Service
Referral to Treatment: Utilizing the ASAM Criteria AOAAM Essentials in Addiction Medicine October 22, 2016 East Lansing, MI Stephen A. Wyatt, DO Medical Director, Addiction Medicine Behavioral Health Service
The New ASAM Criteria: Implications for Drug Courts
 The New ASAM Criteria: Implications for Drug Courts NADCP 21 st Annual Training Conference July 29, 2015 Washington, DC David Mee-Lee, M.D. Chief Editor, The ASAM Criteria Senior Vice President The Change
The New ASAM Criteria: Implications for Drug Courts NADCP 21 st Annual Training Conference July 29, 2015 Washington, DC David Mee-Lee, M.D. Chief Editor, The ASAM Criteria Senior Vice President The Change
What Using The ASAM Criteria Really Means: Skill-Building and Systems Change. David Mee-Lee, M.D.
 What Using The ASAM Criteria Really Means: Skill-Building and Systems Change David Mee-Lee, M.D. Chief Editor, The ASAM Criteria Senior Vice President The Change Companies Carson City, NV Davis, CA davidmeelee@gmail.com
What Using The ASAM Criteria Really Means: Skill-Building and Systems Change David Mee-Lee, M.D. Chief Editor, The ASAM Criteria Senior Vice President The Change Companies Carson City, NV Davis, CA davidmeelee@gmail.com
Substance Abuse Level of Care Criteria
 Substance Abuse Level of Care Criteria Table of Contents SUBSTANCE ABUSE OUTPATIENT: Adolescent... 3 SUBSTANCE ABUSE PREVENTION: Adult... 7 OPIOID MAINTENANCE THERAPY: Adult... 8 SUBSTANCE ABUSE INTERVENTION:
Substance Abuse Level of Care Criteria Table of Contents SUBSTANCE ABUSE OUTPATIENT: Adolescent... 3 SUBSTANCE ABUSE PREVENTION: Adult... 7 OPIOID MAINTENANCE THERAPY: Adult... 8 SUBSTANCE ABUSE INTERVENTION:
Evidence based Practices
 Evidence base Practices Adjunct Professor of Psychology, Western Carolina University President, Evince Clinical Assessments Evidence based Treatment Utilize treatment models documented to be effective
Evidence base Practices Adjunct Professor of Psychology, Western Carolina University President, Evince Clinical Assessments Evidence based Treatment Utilize treatment models documented to be effective
ASAM Level.05 DIMENSIONS Circle all items in each dimension that apply to the client. ADMISSION CRITERIA
 Print Client Name: Client Identification Number: Date: Adolescent 65D-30 Intervention ASAM Level.05 ADMISSION CRITERIA Acute Intoxication and /or Withdrawal Biomedical Conditions and of validation for
Print Client Name: Client Identification Number: Date: Adolescent 65D-30 Intervention ASAM Level.05 ADMISSION CRITERIA Acute Intoxication and /or Withdrawal Biomedical Conditions and of validation for
ADVANCED BEHAVIORAL HEALTH, INC. Clinical Level of Care Guidelines
 The Clinical Level of Care Guidelines contained on the following pages have been developed as a guide to assist care managers, physicians and providers in making medical necessity decisions about the least
The Clinical Level of Care Guidelines contained on the following pages have been developed as a guide to assist care managers, physicians and providers in making medical necessity decisions about the least
Adult 65D-30 Intervention ASAM Level.05 DIMENSIONS Circle all items in each dimension that apply to the client. ADMISSION CRITERIA
 Adult 65D-30 Intervention ASAM Level.05 ADMISSION CRITERIA Place a check in the yes or no box that indicates validation or lack ASAM Requirements Withdrawal and of validation for placement into this level
Adult 65D-30 Intervention ASAM Level.05 ADMISSION CRITERIA Place a check in the yes or no box that indicates validation or lack ASAM Requirements Withdrawal and of validation for placement into this level
SUD Requirements. Proprietary
 SUD Requirements Triage screening to determine eligibility and appropriateness (proper member placement) for admission and referral. A comprehensive bio-psychosocial evaluation must be completed prior
SUD Requirements Triage screening to determine eligibility and appropriateness (proper member placement) for admission and referral. A comprehensive bio-psychosocial evaluation must be completed prior
Clinical Evaluation: Assessment Goals
 Clinical Evaluation: Assessment Goals 1. Define Assessment Process 2. Identify Assessment Instruments 3. Define DSM-5 criteria for Substance Abuse and Dependence, specifiers and multi-axial assessment
Clinical Evaluation: Assessment Goals 1. Define Assessment Process 2. Identify Assessment Instruments 3. Define DSM-5 criteria for Substance Abuse and Dependence, specifiers and multi-axial assessment
ASAM Criteria What it is and Why it s Important
 ASAM Criteria What it is and Why it s Important ASAM Criteria: What it is and Why it s Important Webinar Wednesday, June 10, 2015 10:00 AM 11:30 AM Facilitator: Will Rhett-Mariscal, PhD, MS, Associate
ASAM Criteria What it is and Why it s Important ASAM Criteria: What it is and Why it s Important Webinar Wednesday, June 10, 2015 10:00 AM 11:30 AM Facilitator: Will Rhett-Mariscal, PhD, MS, Associate
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) دکتر راد گودرزی
 دکتر راد گودرزی") The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) 1 Expanded to include Gambling Disorder Cannabis Withdrawal and Caffeine Withdrawal are new disorders Caffeine Withdrawal
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) 1 Expanded to include Gambling Disorder Cannabis Withdrawal and Caffeine Withdrawal are new disorders Caffeine Withdrawal
What is Treatment Planning? Clinical Evaluation: Treatment Planning Goals and Objectives
 Clinical Evaluation: Treatment Planning Goals and Objectives 1) Define Treatment Planning 2) Understanding of Correlation Between Assessment and Treatment Planning 3) Overview of Treatment Planning Process
Clinical Evaluation: Treatment Planning Goals and Objectives 1) Define Treatment Planning 2) Understanding of Correlation Between Assessment and Treatment Planning 3) Overview of Treatment Planning Process
Chapter 7. Screening and Assessment
 Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Substance Use Disorders
 Substance Use Disorders Substance Use Disorder This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars monthly to address topics related to risk adjustment documentation and
Substance Use Disorders Substance Use Disorder This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars monthly to address topics related to risk adjustment documentation and
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
ASAM Criteria, Third Edition Matrix for Matching Adult Severity and Level of Function with Type and Intensity of Service
 1: Acute Intoxication and/or Withdrawal Potential Risk Rating: 0 1: Acute Intoxication and/or Withdrawal Potential Risk Rating: 1 1: Acute Intoxication and/or Withdrawal Potential Risk Rating: 2 The patient
1: Acute Intoxication and/or Withdrawal Potential Risk Rating: 0 1: Acute Intoxication and/or Withdrawal Potential Risk Rating: 1 1: Acute Intoxication and/or Withdrawal Potential Risk Rating: 2 The patient
GUIDANCE FOR APPLICATION OF ASAM IN PENNSYLVANIA S SUBSTANCE USE DISORDER (SUD) SYSTEM OF CARE May 2018
 SYSTEM OF CARE May 2018") GUIDANCE FOR APPLICATION OF ASAM IN PENNSYLVANIA S SUBSTANCE USE DISORDER (SUD) SYSTEM OF CARE May 2018 1 Contents GUIDANCE INTRODUCTION... 3 WITHDRAWAL MANAGEMENT SERVICES... 4 1 WM or 2 WM: Ambulatory
GUIDANCE FOR APPLICATION OF ASAM IN PENNSYLVANIA S SUBSTANCE USE DISORDER (SUD) SYSTEM OF CARE May 2018 1 Contents GUIDANCE INTRODUCTION... 3 WITHDRAWAL MANAGEMENT SERVICES... 4 1 WM or 2 WM: Ambulatory
Trigger. Myths About the Use of Medication in Recovery BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS
 BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module VI Counseling Buprenorphine Patients Myths About the Use of Medication in Recovery! Patients are still addicted!
BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module VI Counseling Buprenorphine Patients Myths About the Use of Medication in Recovery! Patients are still addicted!
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
BASIC VOLUME. Elements of Drug Dependence Treatment
 BASIC VOLUME Elements of Drug Dependence Treatment Module 3 Principles of CBT and relapse prevention strategies Introduction to Cognitive Behavioural Therapy Basics of pharmacological treatment Workshop
BASIC VOLUME Elements of Drug Dependence Treatment Module 3 Principles of CBT and relapse prevention strategies Introduction to Cognitive Behavioural Therapy Basics of pharmacological treatment Workshop
Outpatient Treatment, Psychiatric and Substance Use Disorders, Rehabilitation
 Outpatient Treatment, Psychiatric and Substance Use Disorders, Rehabilitation Criteria for Treatment Status Review The specified requirements for severity of need and intensity and quality of service must
Outpatient Treatment, Psychiatric and Substance Use Disorders, Rehabilitation Criteria for Treatment Status Review The specified requirements for severity of need and intensity and quality of service must
ROSC & MAT II: Opioid Treatment Services
 ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
ADULT Addictions Treatment: Medically Monitored Residential Treatment (3B)
") ADULT Addictions Treatment: Medically Monitored Residential Treatment (3B) Program Medically Monitored Short Term Residential treatment provides 24 hour professionally directed evaluation, care, and treatment
ADULT Addictions Treatment: Medically Monitored Residential Treatment (3B) Program Medically Monitored Short Term Residential treatment provides 24 hour professionally directed evaluation, care, and treatment
Opioid Use Issues: All the Players
 Opioid Use Issues: All the Players Objectives After review, the participant will be able to: 1) Identify criteria for opioid use disorders Andrew J. McLean, MD, MPH Medical Director, ND Department of Human
Opioid Use Issues: All the Players Objectives After review, the participant will be able to: 1) Identify criteria for opioid use disorders Andrew J. McLean, MD, MPH Medical Director, ND Department of Human
Addiction Assessment and the ASAM PPC-2R
 Talk Outline Addiction Assessment and the ASAM Patient Placement Criteria George Kolodner,, M.D. Medical Director, Talbott Recovery Chair, Steering Committee of Atlanta, Georgia the Coalition for National
Talk Outline Addiction Assessment and the ASAM Patient Placement Criteria George Kolodner,, M.D. Medical Director, Talbott Recovery Chair, Steering Committee of Atlanta, Georgia the Coalition for National
TOOL 1: QUESTIONS BY ASAM DIMENSIONS
 TOOL 1: QUESTIONS BY ASAM DIMENSIONS The following tool highlights specific questions that should be asked of the patient for each ASAM dimension. Name Date of Birth Date of Interview Address Referred
TOOL 1: QUESTIONS BY ASAM DIMENSIONS The following tool highlights specific questions that should be asked of the patient for each ASAM dimension. Name Date of Birth Date of Interview Address Referred
Clinical UM Guideline
 Clinical UM Guideline Subject: Substance-Related and Addictive Disorder Treatment Guideline #: CG-BEH-04 Publish Date: 03/29/2018 Status: Reviewed Last Review Date: 02/27/2018 Description This document
Clinical UM Guideline Subject: Substance-Related and Addictive Disorder Treatment Guideline #: CG-BEH-04 Publish Date: 03/29/2018 Status: Reviewed Last Review Date: 02/27/2018 Description This document
Addiction. Concept of Addiction R. Corey Waller MD, MS, FACEP, FASAM Director, Center for Integrative Medicine
 Addiction Concept of Addiction R. Corey Waller MD, MS, FACEP, FASAM Director, Center for Integrative Medicine Twitter: @rcwallermd Objectives Understand the Concept of Addiction Survival FOOD WATER DOPAMINE
Addiction Concept of Addiction R. Corey Waller MD, MS, FACEP, FASAM Director, Center for Integrative Medicine Twitter: @rcwallermd Objectives Understand the Concept of Addiction Survival FOOD WATER DOPAMINE
DMHAS ASAM SERVICE DESCRIPTIONS
 (DMHAS) Fee for Service (FFS) ANNEX A1 DMHAS ASAM SERVICE DESCRIPTIONS Please carefully review the Service Descriptions that are included in the DMHAS FFS Initiatives in this Annex A1 contract section.
(DMHAS) Fee for Service (FFS) ANNEX A1 DMHAS ASAM SERVICE DESCRIPTIONS Please carefully review the Service Descriptions that are included in the DMHAS FFS Initiatives in this Annex A1 contract section.
Clinical UM Guideline. This document provides medical necessity criteria for levels of care relating to substance and addictive disorders.
 Clinical UM Guideline Subject: Substance-Related and Addictive Disorder Treatment Guideline #: CG-BEH-04 Current Effective Date: 04/05/2016 Status: Revised Last Review Date: 02/04/2016 Description This
Clinical UM Guideline Subject: Substance-Related and Addictive Disorder Treatment Guideline #: CG-BEH-04 Current Effective Date: 04/05/2016 Status: Revised Last Review Date: 02/04/2016 Description This
Service Review Criteria
 Pre-Review Review for HUM 26: immediate health/safety concerns. If MET, refer to medical staff and outreach phone call to Provider. Please note concerns here and in the Clinical Justification: Review for
Pre-Review Review for HUM 26: immediate health/safety concerns. If MET, refer to medical staff and outreach phone call to Provider. Please note concerns here and in the Clinical Justification: Review for
IDDT Fidelity Action Planning Guidelines
 1a. Multidisciplinary Team IDDT Fidelity Action Planning Guidelines Definition: All clients targeted for IDDT receive care from a multidisciplinary team. A multi-disciplinary team consists of, in addition
1a. Multidisciplinary Team IDDT Fidelity Action Planning Guidelines Definition: All clients targeted for IDDT receive care from a multidisciplinary team. A multi-disciplinary team consists of, in addition
Child Welfare and MOMS: Building Partnerships to Improve Care
 Child Welfare and MOMS: Building Partnerships to Improve Care Goals Develop collaborative partnerships between MOMS pilot sites and child welfare agencies: Facilitate successful outcomes for clients Jointly
Child Welfare and MOMS: Building Partnerships to Improve Care Goals Develop collaborative partnerships between MOMS pilot sites and child welfare agencies: Facilitate successful outcomes for clients Jointly
Adult Mental Health Services applicable to Members in the State of Connecticut subject to state law SB1160
 Adult Mental Health Services Comparison Create and maintain a document in an easily accessible location on such health carrier's Internet web site that (i) (ii) compares each aspect of such clinical review
Adult Mental Health Services Comparison Create and maintain a document in an easily accessible location on such health carrier's Internet web site that (i) (ii) compares each aspect of such clinical review
Doing Time or Doing Treatment: Moving Beyond Program Phases to Real Lasting Change
 Doing Time or Doing Treatment: Moving Beyond Program Phases to Real Lasting Change BJA Drug Court Technical Assistance Project at American University March 14, 2016 David Mee-Lee, M.D. Chief Editor, The
Doing Time or Doing Treatment: Moving Beyond Program Phases to Real Lasting Change BJA Drug Court Technical Assistance Project at American University March 14, 2016 David Mee-Lee, M.D. Chief Editor, The
WHY THE ASI SHOULD BE REPLACED AND WHY MANDATES FOR ITS USE SHOULD BE ELIMINATED
 WHY THE ASI SHOULD BE REPLACED AND WHY MANDATES FOR ITS USE SHOULD BE ELIMINATED The ASI (Addiction Severity Index) was initially designed as a program evaluation tool for VA populations and subsequently
WHY THE ASI SHOULD BE REPLACED AND WHY MANDATES FOR ITS USE SHOULD BE ELIMINATED The ASI (Addiction Severity Index) was initially designed as a program evaluation tool for VA populations and subsequently
Effectively Addressing Co-Occurring Nicotine Dependence and Marijuana Use. Chad Morris, PhD March 7, 2018
 Effectively Addressing Co-Occurring Nicotine Dependence and Marijuana Use Chad Morris, PhD March 7, 2018 2018 BHWP Behavioral Causes of Death in U.S. 2018 BHWP 2018 BHWP Health Disparities Population Behavioral
Effectively Addressing Co-Occurring Nicotine Dependence and Marijuana Use Chad Morris, PhD March 7, 2018 2018 BHWP Behavioral Causes of Death in U.S. 2018 BHWP 2018 BHWP Health Disparities Population Behavioral
4/27/2017. The ATTC Network. Co-Occurring Treatment Adolescents & Adults. Mark Disselkoen, MSW, LCSW, LADC
 Presented by: Mark Disselkoen, MSW, LCSW, LADC Co-Occurring Treatment Adolescents & Adults Mark Disselkoen, MSW, LCSW, LADC Northwest Addiction Technology Transfer Center The ATTC Network Ten Regional
Presented by: Mark Disselkoen, MSW, LCSW, LADC Co-Occurring Treatment Adolescents & Adults Mark Disselkoen, MSW, LCSW, LADC Northwest Addiction Technology Transfer Center The ATTC Network Ten Regional
What Using The ASAM Criteria Really Means: Skill-Building and Systems Change
 Pretest Questions Select the Best Answer: What Using The ASAM Criteria Really Means: Skill-Building and Systems Change Davis, CA (530) 753-4300; Voice Mail (916) 715-5856 davidmeelee@gmail.com www.changecompanies.net
Pretest Questions Select the Best Answer: What Using The ASAM Criteria Really Means: Skill-Building and Systems Change Davis, CA (530) 753-4300; Voice Mail (916) 715-5856 davidmeelee@gmail.com www.changecompanies.net
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE
 Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Addiction and Recovery Treatment Services (ARTS) Service Authorization Review Form Extension Requests ASAM Levels 2.1/2.5/3.1/3.3/3.5/3.7/4.
 Service Authorization Review Form Extension Requests ASAM Levels 2.1/2.5/3.1/3.3/3.5/3.7/4.") Addiction and Recovery Treatment Services (ARTS) Service Authorization Review Form Extension Requests ASAM Levels 2.1/2.5/3.1/3.3/3.5/3.7/4.0 No Service Authorization Needed for ASAM Level 0.5/1.0/OTP/OBOT
Addiction and Recovery Treatment Services (ARTS) Service Authorization Review Form Extension Requests ASAM Levels 2.1/2.5/3.1/3.3/3.5/3.7/4.0 No Service Authorization Needed for ASAM Level 0.5/1.0/OTP/OBOT
Appendix F Federation of State Medical Boards
 Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
IMPLEMENTING RECOVERY ORIENTED CLINICAL SERVICES IN OPIOID TREATMENT PROGRAMS PILOT UPDATE. A Clinical Quality Improvement Program
 IMPLEMENTING RECOVERY ORIENTED CLINICAL SERVICES IN OPIOID TREATMENT PROGRAMS PILOT UPDATE A Clinical Quality Improvement Program Today: National completion rates for OTP s hover between 11 14% Retention
IMPLEMENTING RECOVERY ORIENTED CLINICAL SERVICES IN OPIOID TREATMENT PROGRAMS PILOT UPDATE A Clinical Quality Improvement Program Today: National completion rates for OTP s hover between 11 14% Retention
OUTPATIENT TREATMENT WESTPORT, CONNECTICUT
 OUTPATIENT TREATMENT WESTPORT, CONNECTICUT ABOUT CLEARPOINT At Clearpoint, we focus on healing the whole person: mind, body, and spirit. Our comprehensive care methods set clients up for long-term success
OUTPATIENT TREATMENT WESTPORT, CONNECTICUT ABOUT CLEARPOINT At Clearpoint, we focus on healing the whole person: mind, body, and spirit. Our comprehensive care methods set clients up for long-term success
Inpatient Psychiatric Services for Under Age 21 Manual. Acute Inpatient Mental Health (Child/Adolescent)
") Inpatient Psychiatric Services for Under Age 21 Manual Acute Inpatient Mental Health (Child/Adolescent) Description of Services: Acute inpatient mental health treatment represents the most intensive level
Inpatient Psychiatric Services for Under Age 21 Manual Acute Inpatient Mental Health (Child/Adolescent) Description of Services: Acute inpatient mental health treatment represents the most intensive level
NORTHWEST AIDS EDUCATION AND TRAINING CENTER. Opioid Use Disorders. Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Opioid Use Disorders Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014 Opioid Use Disorders Importance of opioid use disorders Screening and
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Opioid Use Disorders Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014 Opioid Use Disorders Importance of opioid use disorders Screening and
Questions Asked During the Live Webinar Broadcast on 3/14/12
 Questions Asked During the Live Webinar Broadcast on 3/14/12 Q: How much does the 1 11.1 and 11.5 require? A: Level I, Outpatient Services is less than nine hours of clinical service per week in the Adult
Questions Asked During the Live Webinar Broadcast on 3/14/12 Q: How much does the 1 11.1 and 11.5 require? A: Level I, Outpatient Services is less than nine hours of clinical service per week in the Adult
CSAT s Knowledge Application Program. KAP Keys. For Clinicians
 The Role and Current Status of Patient Placement Criteria in the Treatment of Substance Use Disorders CSAT s Knowledge Application Program KAP Keys For Clinicians Based on TIP 13 The Role and Current Status
The Role and Current Status of Patient Placement Criteria in the Treatment of Substance Use Disorders CSAT s Knowledge Application Program KAP Keys For Clinicians Based on TIP 13 The Role and Current Status
Effective Treatment: Doing the Right Thing, In the Right Way. Terrence D Walton, MSW, ICADC
 Effective Treatment: Doing the Right Thing, In the Right Way Terrence D Walton, MSW, ICADC Monitor Manage Impact 1. Understand the Treatment Field, including Evidenced Based Practices 2. Understand Your
Effective Treatment: Doing the Right Thing, In the Right Way Terrence D Walton, MSW, ICADC Monitor Manage Impact 1. Understand the Treatment Field, including Evidenced Based Practices 2. Understand Your
NorthSTAR. Section II Substance Abuse and Chemical Dependency LEVEL OF CARE CRITERIA
 NorthSTAR Section II Substance Abuse and Chemical Dependency LEVEL OF CARE CRITERIA 1 TABLE OF CONTENTS Level of Care Page Inpatient Detoxification Services (Hospital and 24 Hour Residential) 3 Outpatient
NorthSTAR Section II Substance Abuse and Chemical Dependency LEVEL OF CARE CRITERIA 1 TABLE OF CONTENTS Level of Care Page Inpatient Detoxification Services (Hospital and 24 Hour Residential) 3 Outpatient
Commi ee Lecture: Neurocogni ve Disorders TBI : Trauma c Brain Disorders. William L. Bograkos, MA, DO, FACOEP
 Commi ee Lecture: Neurocogni ve Disorders TBI : Trauma c Brain Disorders Toxic Brain Disorders William L. Bograkos, MA, DO, FACOEP TBI: Traumatic Brain Injury / Toxic Brain Injury (Trauma and Substance
Commi ee Lecture: Neurocogni ve Disorders TBI : Trauma c Brain Disorders Toxic Brain Disorders William L. Bograkos, MA, DO, FACOEP TBI: Traumatic Brain Injury / Toxic Brain Injury (Trauma and Substance
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines
 The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
Child and Adolescent Screening and Assessment Tools
 Child and Adolescent Screening and Assessment Tools Randall Stiles, PhD. State of Nevada Division of Child and Family Services The views, opinions, and content expressed in this presentation do not necessarily
Child and Adolescent Screening and Assessment Tools Randall Stiles, PhD. State of Nevada Division of Child and Family Services The views, opinions, and content expressed in this presentation do not necessarily
Alberta Alcohol and Drug Abuse Commission. POSITION ON ADDICTION AND MENTAL HEALTH February 2007
 Alberta Alcohol and Drug Abuse Commission POSITION ON ADDICTION AND MENTAL HEALTH POSITION The Alberta Alcohol and Drug Abuse Commission (AADAC) recognizes that among clients with addiction problems, there
Alberta Alcohol and Drug Abuse Commission POSITION ON ADDICTION AND MENTAL HEALTH POSITION The Alberta Alcohol and Drug Abuse Commission (AADAC) recognizes that among clients with addiction problems, there
Virginia Medicaid Peer Support Services UM Guideline
 Virginia Medicaid Peer Support Services UM Guideline Subject: Virginia Medicaid Peer Support Services Current Effective Date: 08/24/2017 Status: Final Last Review Date: 10/23/2018 Description Peer Supports
Virginia Medicaid Peer Support Services UM Guideline Subject: Virginia Medicaid Peer Support Services Current Effective Date: 08/24/2017 Status: Final Last Review Date: 10/23/2018 Description Peer Supports
Acute General Medical and Surgical Admission:
 Acute General Medical and Surgical Admission: Managing Substance Use Disorders in Patients Who are Severely Ill Scott Grantham, MD Executive Director, Behavioral Health Saint Francis Health System By the
Acute General Medical and Surgical Admission: Managing Substance Use Disorders in Patients Who are Severely Ill Scott Grantham, MD Executive Director, Behavioral Health Saint Francis Health System By the
7/7/2016 Journal of the American Medical Association,
 1 2 Journal of the American Medical Association, 2008 3 The Clinical Trial 152 Adolescents and Young Adults (Age 15 to 21) randomly assigned to either; 1. 2 weeks of Buprenorphine detox 2. 12 weeks of
1 2 Journal of the American Medical Association, 2008 3 The Clinical Trial 152 Adolescents and Young Adults (Age 15 to 21) randomly assigned to either; 1. 2 weeks of Buprenorphine detox 2. 12 weeks of
2/21/2018. What are Opioids?
 Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Substance and Alcohol Related Disorders. Substance use Disorder Alcoholism Gambling Disorder
 Substance and Alcohol Related Disorders Substance use Disorder Alcoholism Gambling Disorder What is a Substance Use Disorder? According to the DSM-5, a substance use disorder describes a problematic pattern
Substance and Alcohol Related Disorders Substance use Disorder Alcoholism Gambling Disorder What is a Substance Use Disorder? According to the DSM-5, a substance use disorder describes a problematic pattern
Advanced ASAM Criteria Training
 2017 New England School of Best Practices in Addiction Treatment ASAM Criteria for Substance Related, Co Occurring and Addictive Disorders in order to Provide Quality, Cost Effective Treatment 8/30/17
2017 New England School of Best Practices in Addiction Treatment ASAM Criteria for Substance Related, Co Occurring and Addictive Disorders in order to Provide Quality, Cost Effective Treatment 8/30/17
Health Share Level of Care Authorization Form Adult Mental Health Services Initial Treatment Registration Form
 Health Share Level of Care Authorization Form Adult Mental Health Services Initial Treatment Registration Form Member Information Member Name: OHP ID: Date of Birth: Provider: Location: Service Period
Health Share Level of Care Authorization Form Adult Mental Health Services Initial Treatment Registration Form Member Information Member Name: OHP ID: Date of Birth: Provider: Location: Service Period
FY17 SCOPE OF WORK TEMPLATE. Name of Program/Services: Medication-Assisted Treatment: Buprenorphine
 FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
The Role of the PDMP: Foundational Knowledge and Best Practices
 The Role of the PDMP: Foundational Knowledge and Best Practices Brent I. Fox, PharmD, PhD Health Outcomes Research and Policy Harrison School of Pharmacy Auburn University DISCLOSURE I, Brent Fox, have
The Role of the PDMP: Foundational Knowledge and Best Practices Brent I. Fox, PharmD, PhD Health Outcomes Research and Policy Harrison School of Pharmacy Auburn University DISCLOSURE I, Brent Fox, have
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Approaches for Drug Addiction
 Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
Feeding and Eating Disorders
 The Time is Here: Differential Diagnosis and Coding Using the DSM 5 and ICD 10 Diane Snow, PhD, RN, PMHNP-BC, FAANP, FIAAN University of Texas at Arlington College of Nursing and Health Innovation IntNSA
The Time is Here: Differential Diagnosis and Coding Using the DSM 5 and ICD 10 Diane Snow, PhD, RN, PMHNP-BC, FAANP, FIAAN University of Texas at Arlington College of Nursing and Health Innovation IntNSA
The ASAM Criteria Introduction. [ June 2017]
![The ASAM Criteria Introduction. [ June 2017]](/thumbs/75/72352964.jpg "The ASAM Criteria Introduction. [ June 2017]") The ASAM Criteria Introduction [ June 2017] The ASAM Criteria The ASAM Criteria: Treatment Criteria for Addictive, Substance- Related, and Co-Occurring Conditions American Society of Addiction Medicine
The ASAM Criteria Introduction [ June 2017] The ASAM Criteria The ASAM Criteria: Treatment Criteria for Addictive, Substance- Related, and Co-Occurring Conditions American Society of Addiction Medicine
General Principles for the Use of Pharmacological Agents for Co- Occurring Disorders
 General Principles for the Use of Pharmacological Agents for Co- Occurring Disorders Individuals with co-occurring mental and substance use disorders (COD) are common in behavioral and primary health settings
General Principles for the Use of Pharmacological Agents for Co- Occurring Disorders Individuals with co-occurring mental and substance use disorders (COD) are common in behavioral and primary health settings
Serious Mental Illness and Opioid Use Disorder
 Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Opioid Use and Justice Involvement: Challenges in Treatment, Engagement, and Continuity
 Opioid Use and Justice Involvement: Challenges in Treatment, Engagement, and Continuity Holly Hills, Ph.D. June 13, 2017 Department of Mental Health Law and Policy Overview: Persons who have not been in
Opioid Use and Justice Involvement: Challenges in Treatment, Engagement, and Continuity Holly Hills, Ph.D. June 13, 2017 Department of Mental Health Law and Policy Overview: Persons who have not been in
WHAT CAN I EXPECT?: DUAL SUBSTANCE USE AND MENTAL HEALTH TREATMENT FOR MILITARY POPULATIONS
 WHAT CAN I EXPECT?: DUAL SUBSTANCE USE AND MENTAL HEALTH TREATMENT FOR MILITARY POPULATIONS René Lento, PhD Lauren Brenner, PhD September 25, 2018 DISCLOSURES None HOME BASE PROGRAM 3 LEARNING OBJECTIVES
WHAT CAN I EXPECT?: DUAL SUBSTANCE USE AND MENTAL HEALTH TREATMENT FOR MILITARY POPULATIONS René Lento, PhD Lauren Brenner, PhD September 25, 2018 DISCLOSURES None HOME BASE PROGRAM 3 LEARNING OBJECTIVES
HARM REDUCTION & TREATMENT. Devin Reaves MSW
 HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
Addiction and Recovery Treatment Services (ARTS) Service Authorization Review Form Initial Requests ASAM Levels 2.1/2.5/3.1/3.3/3.5/3.7/4.
 Service Authorization Review Form Initial Requests ASAM Levels 2.1/2.5/3.1/3.3/3.5/3.7/4.") Addiction and Recovery Treatment Services (ARTS) Service Authorization Review Form Initial Requests ASAM Levels 2.1/2.5/3.1/3.3/3.5/3.7/4.0 No Service Authorization Needed for ASAM Levels 0.5/1.0/OTP/OBOT
Addiction and Recovery Treatment Services (ARTS) Service Authorization Review Form Initial Requests ASAM Levels 2.1/2.5/3.1/3.3/3.5/3.7/4.0 No Service Authorization Needed for ASAM Levels 0.5/1.0/OTP/OBOT
Assessment. Clinical Steps To ensuring the needs Of your clients are Identified
 Assessment Clinical Steps To ensuring the needs Of your clients are Identified Session Objectives Learn what the best strategies are to determine which potential drug court clients are most suitable for
Assessment Clinical Steps To ensuring the needs Of your clients are Identified Session Objectives Learn what the best strategies are to determine which potential drug court clients are most suitable for
Neurobiology of Drug Abuse and Addiction PSYC 450
 Neurobiology of Drug Abuse and Addiction PSYC 450 Healthy Control Drug Abuser Illicit drug use, lifetime and past year, in Canada 50 Canabis only Any drug Any of 5 drugs (without canabis) (CADUMS 2012)
Neurobiology of Drug Abuse and Addiction PSYC 450 Healthy Control Drug Abuser Illicit drug use, lifetime and past year, in Canada 50 Canabis only Any drug Any of 5 drugs (without canabis) (CADUMS 2012)
What Using The ASAM Criteria Really Means: Skill-Building and Systems Change
 Pretest Questions Select the Best Answer: What Using The ASAM Criteria Really Means: Skill-Building and Systems Change Davis, CA (530) 753-4300; Mobile (916) 715-5856 davidmeelee@gmail.com ASAMCriteria.org
Pretest Questions Select the Best Answer: What Using The ASAM Criteria Really Means: Skill-Building and Systems Change Davis, CA (530) 753-4300; Mobile (916) 715-5856 davidmeelee@gmail.com ASAMCriteria.org
Members must meet medical necessity criteria for a particular LOC of care. Medically necessary services are those which are:
 BEACON HEALTH STRATEGIES, LLC. / NEW YORK LEVEL OF CARE CRITERIA LEVEL OF CARE CRITERIA Beacon s Level of Care (LOC) criteria were developed from the comparison of national, scientific and evidence based
BEACON HEALTH STRATEGIES, LLC. / NEW YORK LEVEL OF CARE CRITERIA LEVEL OF CARE CRITERIA Beacon s Level of Care (LOC) criteria were developed from the comparison of national, scientific and evidence based
Rates of Co-Occurring Disorders Among Youth. Working with Adolescents with Substance Use Disorders
 1 Working with Adolescents with Substance Use Disorders Michael S. Levy, Ph.D. CAB Health & Recovery Services, Inc. Health and Education Services 8% of 12-17 year old youth have substance abuse or dependence
1 Working with Adolescents with Substance Use Disorders Michael S. Levy, Ph.D. CAB Health & Recovery Services, Inc. Health and Education Services 8% of 12-17 year old youth have substance abuse or dependence
FAMILY FUNCTIONAL THERAPY (FFT)
") FAMILY FUNCTIONAL THERAPY (FFT) Family Functional Therapy (FFT) - Youth Program Description Family Functional Therapy (FFT) is a family-focused, community-based treatment for youth who are exhibiting severely
FAMILY FUNCTIONAL THERAPY (FFT) Family Functional Therapy (FFT) - Youth Program Description Family Functional Therapy (FFT) is a family-focused, community-based treatment for youth who are exhibiting severely
substance use and mental disorders: one, the other, or both?
 substance use and mental disorders: one, the other, or both? Stephen Strobbe, PhD, RN, PMHCNS-BC, CARN-AP Dawn Farm Education Series St. Joe s Education Center, Ypsilanti, MI Tuesday, January 27, 2015
substance use and mental disorders: one, the other, or both? Stephen Strobbe, PhD, RN, PMHCNS-BC, CARN-AP Dawn Farm Education Series St. Joe s Education Center, Ypsilanti, MI Tuesday, January 27, 2015
Community Services - Eligibility
 Community Services - Eligibility In order for DMH to reimburse care, the individual must meet both financial and clinical eligibility criteria. These criteria are described in detail in the DMH provider
Community Services - Eligibility In order for DMH to reimburse care, the individual must meet both financial and clinical eligibility criteria. These criteria are described in detail in the DMH provider
Addiction Overview. Diane A. Rothon MD. Causes Consequences Treatments. Methadone/Buprenorphine 101 April 1, 2017
 Addiction Overview Causes Consequences Treatments Methadone/Buprenorphine 101 April 1, 2017 Diane A. Rothon MD Why? would you listen to this presentation Review the definition and neurobiology of addiction
Addiction Overview Causes Consequences Treatments Methadone/Buprenorphine 101 April 1, 2017 Diane A. Rothon MD Why? would you listen to this presentation Review the definition and neurobiology of addiction
What Is Heroin? Examples of Opioids. What Science Says about Opioid Use Disorder and Its Treatment 6/27/2016
 What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
Medication Assisted Treatment. Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs
 Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
DSM-5 UPDATE. Supplement to DIAGNOSTIC AND STATISTICAL MANUAL OF MENTAL DISORDERS, FIFTH EDITION
 DSM-5 UPDATE Supplement to DIAGNOSTIC AND STATISTICAL MANUAL OF MENTAL DISORDERS, FIFTH EDITION October 2017 DSM-5 Update October 2017 Supplement to Diagnostic and Statistical Manual of Mental Disorders,
DSM-5 UPDATE Supplement to DIAGNOSTIC AND STATISTICAL MANUAL OF MENTAL DISORDERS, FIFTH EDITION October 2017 DSM-5 Update October 2017 Supplement to Diagnostic and Statistical Manual of Mental Disorders,
Clinical Assessment. Client Name (Last, First, MI) ID # Medicaid # DOB: Age:
 ID # Medicaid # DOB: Age:") Clinical Assessment Client Name (Last, First, MI) ID # Medicaid # DOB: Age: Sex: Ethnic Group: Marital Status: Occupation: Education: Multiaxial Diagnosis Axis I: Clinical Disorders / Other Conditions
Clinical Assessment Client Name (Last, First, MI) ID # Medicaid # DOB: Age: Sex: Ethnic Group: Marital Status: Occupation: Education: Multiaxial Diagnosis Axis I: Clinical Disorders / Other Conditions
SUBSTANCE USE DISORDER IN ADOLESCENT POPULATION
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences SUBSTANCE USE DISORDER IN ADOLESCENT POPULATION ANNABELLE SIMPSON, MD UNIVERSITY OF WASHINGTON GENERAL DISCLOSURES
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences SUBSTANCE USE DISORDER IN ADOLESCENT POPULATION ANNABELLE SIMPSON, MD UNIVERSITY OF WASHINGTON GENERAL DISCLOSURES
Mark Edlund, MD, PhD RTI International. Photo courtesy of The Herb Museum, Vancouver, BC
 Opioid Use Disorders and Their Treatment Mark Edlund, MD, PhD RTI International Photo courtesy of The Herb Museum, Vancouver, BC Acknowledgements Funded by NIDA R01 DA022560-01 NIDA R01 DA034627 NIDA R01
Opioid Use Disorders and Their Treatment Mark Edlund, MD, PhD RTI International Photo courtesy of The Herb Museum, Vancouver, BC Acknowledgements Funded by NIDA R01 DA022560-01 NIDA R01 DA034627 NIDA R01
ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH
 ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV
ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV
Treatment Team Approaches in Substance Abuse Treatment
 Treatment Team Approaches in Substance Abuse Treatment PLANT A SEED AND WATCH IT GROW 2 Substance use disorders span a wide variety of problems arising from substance use, and cover 11 different criteria:
Treatment Team Approaches in Substance Abuse Treatment PLANT A SEED AND WATCH IT GROW 2 Substance use disorders span a wide variety of problems arising from substance use, and cover 11 different criteria:
Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry
 Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry In broad terms, substance use disorders occur when a substance is used in a compulsive manner with a lack of control over
Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry In broad terms, substance use disorders occur when a substance is used in a compulsive manner with a lack of control over
*IN10 BIOPSYCHOSOCIAL ASSESSMENT*
 BIOPSYCHOSOCIAL ASSESSMENT 224-008B page 1 of 5 / 06-14 Please complete this questionnaire and give it to your counselor on your first visit. This information will help your clinician gain an understanding
BIOPSYCHOSOCIAL ASSESSMENT 224-008B page 1 of 5 / 06-14 Please complete this questionnaire and give it to your counselor on your first visit. This information will help your clinician gain an understanding
Members must meet medical necessity criteria for a particular LOC of care. Medically necessary services are those which are:
 BEACON HEALTH OPTIONS / NEW YORK LEVEL OF CARE CRITERIA LEVEL OF CARE CRITERIA Beacon s Level of Care (LOC) criteria were developed from the comparison of national, scientific and evidence based criteria
BEACON HEALTH OPTIONS / NEW YORK LEVEL OF CARE CRITERIA LEVEL OF CARE CRITERIA Beacon s Level of Care (LOC) criteria were developed from the comparison of national, scientific and evidence based criteria
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine
 [Patient-focused, evidence-based addiction treatment] Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine BrightView Health All Rights Reserved www.brightviewhealth.com
[Patient-focused, evidence-based addiction treatment] Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine BrightView Health All Rights Reserved www.brightviewhealth.com
Addiction and Recovery Treatment Services (ARTS) Service Authorization Review Form ASAM Levels 2.1/2.5/3.1/3.5/3.7/4.0
 Service Authorization Review Form ASAM Levels 2.1/2.5/3.1/3.5/3.7/4.0") Member Name: Member ID: Provider Group/Clinic: Street Address: City State Zip: Phone: Addiction and Recovery Treatment Services (ARTS) Service Authorization Review Form ASAM Levels 2.1/2.5/3.1/3.5/3.7/4.0
Member Name: Member ID: Provider Group/Clinic: Street Address: City State Zip: Phone: Addiction and Recovery Treatment Services (ARTS) Service Authorization Review Form ASAM Levels 2.1/2.5/3.1/3.5/3.7/4.0