Management of Alcoholic Liver Disease. Hafez Fakheri Professor of medicine, Sari, Iran
|
|
|
- Aubrie Ryan
- 6 years ago
- Views:
Transcription
1 Management of Alcoholic Liver Disease Hafez Fakheri Professor of medicine, Sari, Iran

2 Alcoholic Hepatitis
3 Scores DF = (4.6 x [ PT- control PT]) + (bili ) MELD = 10 * ((0.957 * ln(cr)) + (0.378 * ln(bil)) + (1.12 * ln(inr))) GAHS: Age, WBC, Urea, Bili, INR
4 28 days mortality 7% 25-45% (32%) 13% 54% 4% 55%
5 Causes of death for AH First 84 days: Liver Failure HRS Infection Dan Med J, 2013, 1951 AH death,
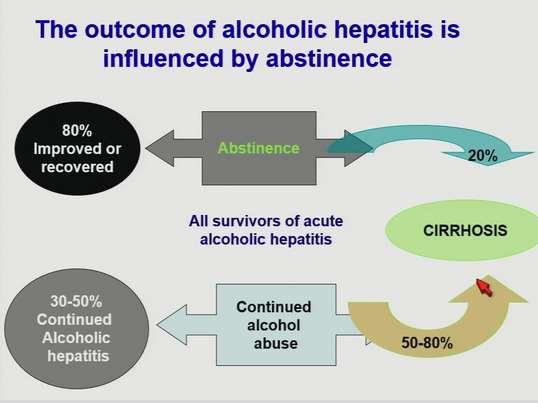
6 General management in AH Alcohol abstinence Prevention and treatment of alcohol withdrawal Fluid management Nutritional support Infection surveillance Prophylaxis against gastric mucosal bleeding Discontinuing nonselective beta blockers in patients with severe AH
7 Alcohol abstinence All patients ( mild - moderate / sever AH) Baclofen may aid Risk for alcohol withdrawal Combined approaches (cognitive behavioral therapy, motivational enhancement therapy, medical care) reduce recidivism
8
9 Hydration All patients ( mild - moderate / sever AH) Poor oral intake prior to presentation Volume expansion, to prevent renal failure Overhydration should be avoided, particularly in stigmata of cirrhosis, since it increase ascites, lower the Na, precipitate GIB from varices
10 Patients with AH often develop ARF which negatively impacts survival Most frequent causes of ARF are Type 1 HRS and tubular necrosis Severe AH is a risk factor of radiocontrastinduced nephropathy
11 Nutritional Support All patients ( mild - moderate / sever AH) Most are malnourished Signs of tissue wasting and severe protein-calorie malnutrition (low albumin, edema) in almost Indices of malnutrition correlated with the severity of liver disease Improvement in liver function and histology,but not consistently found reductions in mortality
12 Patients eat almost no calories unless spoon-fed by relatives. If the patient is not taking enough calori, a duodenal feeding tube can improve intake Enteral feeding is preferred over IV nutrition Protein feeding is well tolerated Protein should not be routinely restricted In encephalopathy associated with protein feeding, use of branched-chain amino acids may be helpful
13 Adequate calories and protein, vitamin ( B1, folate, B6) and mineral ( p, mg) Consider risk of Wernicke s encephalopathy, supplement with B-complex Daily protein( 1.5 g/kg ) independent from encephalopathy Compensate liposoluble vitamins deficiency
14 Infection surveillance Infection screening ; ¼ in admited patients Impossible to distinguish between the fever of hepatitis and infection Blood and urine cultures in evidence of infection Sputum cultures in productive cough CSF examined and cultured in fever and neurologic signs of CNS infection rather than encephalopathy Ascitic fluid culture, cell count, protein, albumin Clinical or biological deterioration disclose a higher risk of infection and should be screened repeatedly
15 Acid suppression Prophylaxis against gastric mucosal bleeding with a PPI, H2-blocker, or Sucralfate particularly if the patient is in an ICU, GC, OB+
16 Discontinue nonselective beta blockers If indicated, should not be started until after AH have recovered Due to the 90 % acute kidney injury with beta blocker in this setting, NOT perform screen endoscopy for varices until the patient has recovered (outpatient) If large varices are detected, beta blockers are started by physicians who are not familiar with the intolerance to these agents

17 Specific therapy in severe AH 1-Corticosteroids %85 %65 28
18 Severe AH (DF 32) *****GC is not recommended in Non sever AH General supportive care Prednisolone has traditionally been used Prednisolone is preferred over prednisone Start with 40 mg
19 Treatment is continued for 28 days For those who receive 28 days of prednisolone, finish therapy with a 16-day taper (decrease the dose by 10 mg/day every 4 days until a dose of 10 mg/day is reached, at which point decrease it by 5 mg/day every 3 days)
20 Exclusion criteria for GC 1. Concomitant pancreatitis 2. GIB 3. Renal failure( HRS) 4. Active infection *GC may not be precluded in patients with infection after appropriate antibiotic therapy
21 Infection developed in 24% of patients who received GC More likely to develop in null responder to GC (43% vs 11 %)
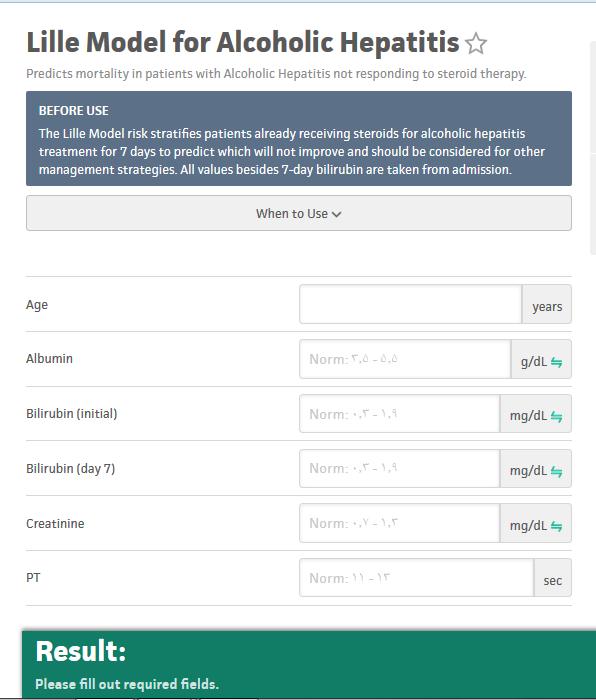
22 After 7 days on GC, Lille score >0.45 predicts poor response 40 % of patients had a Lille score >0.45 High 6 mns mortality in lille score >0.45 (75% vs 15%) Interrupt GC In poor responders Lille score = [ * (age in yrs) * (albumin day 0 in g/l) * (evolution in bili in mm) * (renal insufficiency) * (bili day 0 in mm) * (PT in seconds)].
x 28 days")
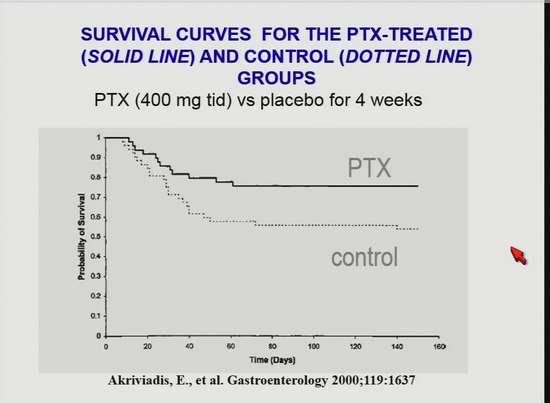
23 Specific therapy in severe AH 2-PTX and antioxidant 400 mg tds (400 mg/day in cr clearance <30 ml/min)x 28 days
24
25 Several studies failed to show a benefit with regard to mortality, while other studies suggested that PTX may prevent HRS and/or decrease mortality The largest meta-analysis supports that PTX decreases the risk of acute kidney injury and suggests that PTX improves mortality compared with placebo, but is not superior to glucocorticoids
26 Role of PTX in AH remains uncertain Alternative in: *patients at risk for sepsis *becoming lost to follow-up after discharge (not be tapered off,serious SE) Do not treat with PTX (lack of efficacy data ) However, AASLDand the EASL, do recommend PTX in who cannot receive GC
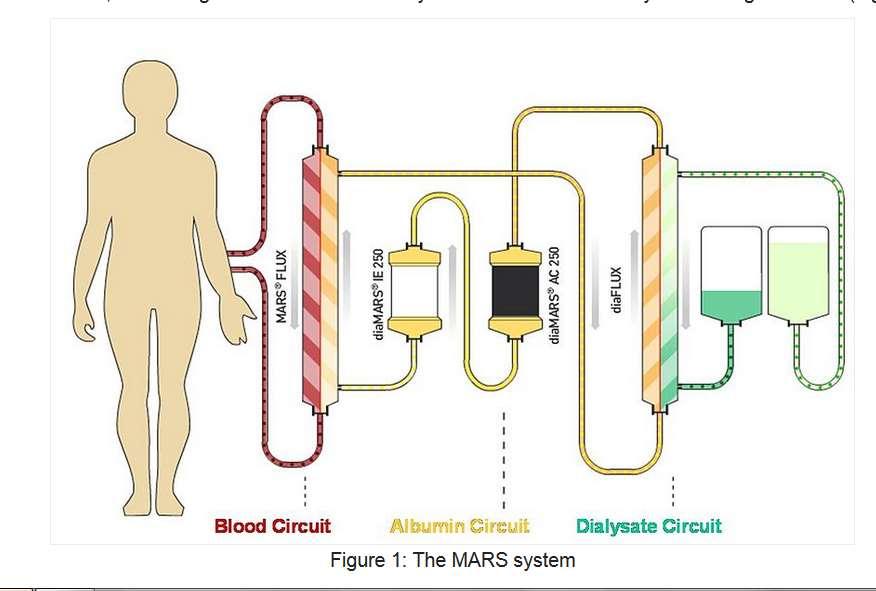
27 In poor responders to GC PTX does not effective Switch to PTX or MARS (molecular adsorbent recirculating system) appears not to modify the outcome
28 Possibly effective treatments Entral feeding: deserves to be tested in combination with corticosteroids PN + N-AC( antioxidant) have synergistic effects & recommend by EASL Granulocyte colony-stimulating factor: Mobilize bone marrow-derived stem cells and promote hepatic regeneration
29 Ineffective treatments Anti-TNF agents PTU Colchicine
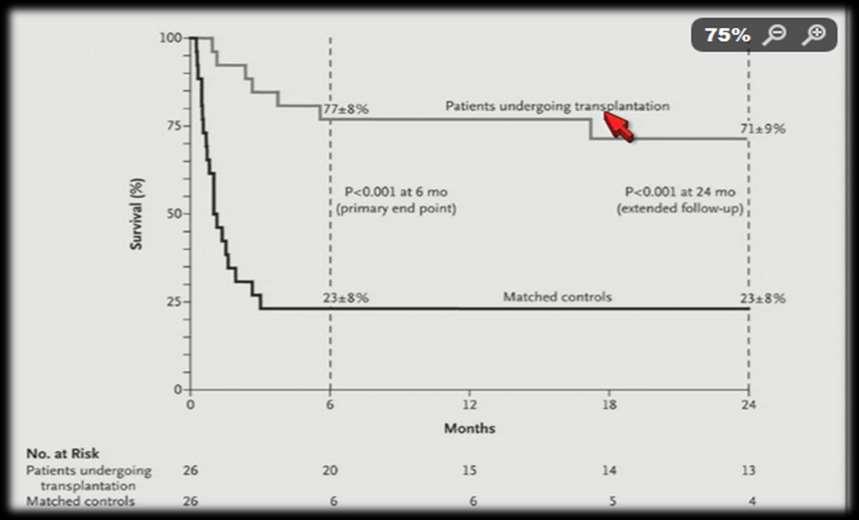
30 Liver transplantation in AH
31 6-mo rule : 85% of transplant programs require Patients who do not respond to steroids have a the 3-mo mortality about 70% and in (HRS) >90% Substance abuse training before & after transplant(alcohol Addiction Unit (Alcohology unit) within transplant center : relapse rate 24-29% good family support and living donor
32 Long-term management of ALD
33 Abstinence from Alcohol Alcoholic fatty liver: steatosis resolution(6wks) Fibrosis/Cirrhosis: improve fibrosis, ascites portal pressure in some Low decompensation Higher survival rates at 1, 5, 10 yrs (95% vs 63%, 61 vs 36%, and 31 vs 11 %)
34 Medications to treat alcohol dependence Only 10% maintain safe drinking after 1 year and 75% relapse Referred for treatment for alcohol abuse or dependence Disulfirum is the oldest, but has poor tolerability and there is little evidence that it increases abstinence Short-term treatment with opioid antagonists such as naltrexone (available in injectable extended release form) is useful in lowering the risk of relapse The GABA B receptor agonist improve abstinence and decrease relapse. Baclofen is a relatively safe and effective agent (devoid of hepatotoxicity) in advanced cirrhosis, and is the most preferred mode of treatment
35 N-methyl-D-aspartate receptor blockers are being investigated as a new pharmacological treatment Alcohol abstinence support groups may also be helpful for alcohol cessation Majority of patients classed as alcoholics also smoke. Smoking cessation decreases progression of hepatic fibrosis, risk of sepsis related deaths, risk of HCC, and post-transplant complication
36 Nutritional therapy Severe malnutrition in CP Class A: 45%, C:95% Malnutrition associate high 1-year mortality (20% vs 0%) and complication(65% vs 13%) Alcoholism is associated with nutritional deficiencies; protein calorie malnutrition, deficiencies of vitamins and trace minerals Protein calorie malnutrition increases the risk of complications; infection, encephalopathy, ascites
37 Nutritional therapy is indicated for alcoholic fatty liver who are malnourished Nutritional therapy is indicated for Alcoholic cirrhosis (protein, carbohydrate, lipid metabolism all affected) Eat multiple times per day, including breakfast and a nighttime snack. The diet should consist of higher amounts of protein (1.2 to 1.5 g/kg) and total calories (35 to 40 kcal/kg) in a standard healthy diet Treat any vitamin or mineral deficiencies
38 Nutritional therapy has not been shown to improve mortality but improves nitrogen balance and albumin levels, decreases hospitalization rates, and decreases the frequency of complications related to cirrhosis (encephalopathy, GIB, ascites)
39 Depletion of hepatic glycogen stores in cirrhotic patients leads to early starvation at 12 hrs (leads to peripheral muscle proteolysis), compared with 48 hrs in normal individuals Therefore, protein restriction should be limited to an initial hrs in hepatic encephalopathy Branched-chain amino acids may be substituted for standard enteral formula if the latter causes hepatic encephalopathy
40 Experimental Therapies None of the existing therapies (silymarin, SAMe, vitamin E, and PTX, colchicine) improved survival in alcoholic cirrhosis other than abstinence Metadoxine,antioxidant,approved for the treatment of ALD in Europe that may be effective
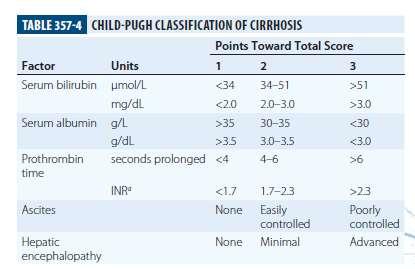
41 Complications of cirrhosis Patients with decompensated cirrhosis are managed the same as patients with other forms of end-stage liver disease and require treatment for complications such as ascites, variceal bleeding, and encephalopathy. In some cases, liver transplantation may be required
42 Liver Transplantation 1 yr mortality: 30% in alcoholic cirrhosis with ascites, 50% in ascites + variceal bleeding, 65% in encephalopathy CP score >11 in spite of at least 6 mns of abstinence have improved survival with liver transplantation In CH- B cirrhosis mortality increases with transplant (different malignancies)
43 HCC In alcoholic liver disease, the chance of HCC is 2 to 3-times higher and co-existent (HCV) doubles the risk Higher in males and the elderly

44 AASLD 2010
45
46
47
48
49 Five-year survival in alcoholic cirrhosis can be best predicted by Child Pugh (CP) score patients with cirrhosis can be stratified into groups A: 5 6; B: 7 8; or C: 9) One-year mortality in CP score A, B, and C are 15%, 25 30%, and 70 80%
50 A recent, large randomized controlled trial of 270 patients with Bx documented severe AH testing the combination of(pn + PTX) failed to show any benefit over GC alone
51
52
53 Steroids or PTX for Alcoholic Hepatitis (STOPHA) 1,103 patients with a clinical diagnosis of severe AH studied into 4 arms: A. Placebo/Placebo; B. PN/ Placebo C. PTX/Placebo; D. PTX/PN At 28 days, death were 17%, 14%, 19%, and 13%. PN reduced the risk of 28-day mortality, but was not sustained at 3 mns and 1 yr Concluded PTX has no impact on disease progression and should no longer be used for treatment of severe AH
54
Paul Martin, MD, FACG. University of Miami. 30,000 deaths from cirrhosis per annum, alcohol implicated in 48%
 Paul Martin, MD, FACG University of Miami 30,000 deaths from cirrhosis per annum, alcohol implicated in 48% Second commonest indication for liver transplant NIAA 2007 Page 1 of 26 Risk Factors Medical
Paul Martin, MD, FACG University of Miami 30,000 deaths from cirrhosis per annum, alcohol implicated in 48% Second commonest indication for liver transplant NIAA 2007 Page 1 of 26 Risk Factors Medical
Alcoholic Hepatitis: Routine Screening for Early Recognition and Management. Juan Guerrero, MD
 Alcoholic Hepatitis: Routine Screening for Early Recognition and Management Juan Guerrero, MD Global Problem 1% of GNP of medium/high income countries Additional societal costs Disproportionately affects
Alcoholic Hepatitis: Routine Screening for Early Recognition and Management Juan Guerrero, MD Global Problem 1% of GNP of medium/high income countries Additional societal costs Disproportionately affects
NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS
 NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS ACHIEVING NUTRITIONAL ADEQUACY Dr N MURUGAN Consultant Hepatologist Apollo Hospitals Chennai NUTRITION IN LIVER FAILURE extent of problem and consequences
NUTRITIONAL OPTIMIZATION IN PRE LIVER TRANSPLANT PATIENTS ACHIEVING NUTRITIONAL ADEQUACY Dr N MURUGAN Consultant Hepatologist Apollo Hospitals Chennai NUTRITION IN LIVER FAILURE extent of problem and consequences
ALCOHOLIC LIVER DISEASE (ALD) Nayan Patel, DO Transplant Hepatology/GI Banner Advanced Liver Disease and Transplant Center
 Nayan Patel, DO Transplant Hepatology/GI Banner Advanced Liver Disease and Transplant Center") ALCOHOLIC LIVER DISEASE (ALD) Nayan Patel, DO Transplant Hepatology/GI Banner Advanced Liver Disease and Transplant Center Objectives Spectrum of alcoholic liver disease Focus on Alcoholic Hepatitis (AH)
ALCOHOLIC LIVER DISEASE (ALD) Nayan Patel, DO Transplant Hepatology/GI Banner Advanced Liver Disease and Transplant Center Objectives Spectrum of alcoholic liver disease Focus on Alcoholic Hepatitis (AH)
Alcoholic Hepatitis: Management Options
 Alcoholic Hepatitis: Management Options Paul J. Thuluvath, MD. FRCP Institute of Digestive Health & Liver Diseases, Mercy Medical Center, Baltimore Professor of Surgery & Medicine, Georgetown University,
Alcoholic Hepatitis: Management Options Paul J. Thuluvath, MD. FRCP Institute of Digestive Health & Liver Diseases, Mercy Medical Center, Baltimore Professor of Surgery & Medicine, Georgetown University,
4/3/2014. Elizabeth Thompson, PharmD April Understand the importance of the liver and basic physiology.
 Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
Hepatology for the Nonhepatologist
 Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL
 Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Management of alcoholic hepatitis: Implications for options beyond the STOPAH study
 Management of alcoholic hepatitis: Implications for options beyond the STOPAH study Gyongyi Szabo, MD, PhD Professor University of Massachusetts Medical School Worcester, MA Cape Town, South Africa 2015
Management of alcoholic hepatitis: Implications for options beyond the STOPAH study Gyongyi Szabo, MD, PhD Professor University of Massachusetts Medical School Worcester, MA Cape Town, South Africa 2015
PACT module Acute hepatic failure. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
HCV care after cure. This program is supported by educational grants from
 HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
HCV care after cure This program is supported by educational grants from Raffaele Bruno,MD Department of Infectious Diseases, Hepatology Outpatients Unit University of Pavia Fondazione IRCCS Policlinico
ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries
 ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries Ashwani K. Singal, MD, MS, FACG 1, Ramon Bataller, MD, PhD, FACG 2, Joseph Ahn, MD, MS, FACG (GRADE Methodologist) 3, Patrick S. Kamath,
ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries Ashwani K. Singal, MD, MS, FACG 1, Ramon Bataller, MD, PhD, FACG 2, Joseph Ahn, MD, MS, FACG (GRADE Methodologist) 3, Patrick S. Kamath,
Alcoholic Liver Disease Strategies for Seamless Care or An Clinical Approach to the Jaundiced Alcoholic Patient
 Alcoholic Liver Disease Strategies for Seamless Care or An Clinical Approach to the Jaundiced Alcoholic Patient Liver Disease for the General Physician Royal College of Physicians July 2017 Dr Ewan Forrest
Alcoholic Liver Disease Strategies for Seamless Care or An Clinical Approach to the Jaundiced Alcoholic Patient Liver Disease for the General Physician Royal College of Physicians July 2017 Dr Ewan Forrest
Alcoholic Hepatitis. Christian Doppler Research Laboratory for Gut Inflammation Medical University Innsbruck. Herbert Tilg
 Alcoholic Hepatitis Christian Doppler Research Laboratory for Gut Inflammation Medical University Innsbruck Herbert Tilg Overview Background I: Alcoholic steatohepatitis (ASH) is a severe and often life-threatening
Alcoholic Hepatitis Christian Doppler Research Laboratory for Gut Inflammation Medical University Innsbruck Herbert Tilg Overview Background I: Alcoholic steatohepatitis (ASH) is a severe and often life-threatening
CHAPTER 1. Alcoholic Liver Disease
 CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Alcoholism and Alcohol Liver Disease from a Transplant Hepatology Perspective
 Alcoholism and Alcohol Liver Disease from a Transplant Hepatology Perspective Clark Kulig, MD Director, Porter Center for Liver Care Denver, CO February 2015 Does quantity of alcohol correlate with liver
Alcoholism and Alcohol Liver Disease from a Transplant Hepatology Perspective Clark Kulig, MD Director, Porter Center for Liver Care Denver, CO February 2015 Does quantity of alcohol correlate with liver
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist. K V Speeg, MD, PhD UT Health San Antonio
 The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
DIFFERENTIAL BENEFITS OF DAAs IN DIFFERENT PATIENT POPULATIONS. IN PATIENTS ON A WAITING LIST FOR TRANSPLANTATION. THE CLINIC.
 DIFFERENTIAL BENEFITS OF DAAs IN DIFFERENT PATIENT POPULATIONS. IN PATIENTS ON A WAITING LIST FOR TRANSPLANTATION. THE CLINIC. Robert J. de Knegt, Erasmus MC, Rotterdam r.deknegt@erasmusmc.nl Disclosures
DIFFERENTIAL BENEFITS OF DAAs IN DIFFERENT PATIENT POPULATIONS. IN PATIENTS ON A WAITING LIST FOR TRANSPLANTATION. THE CLINIC. Robert J. de Knegt, Erasmus MC, Rotterdam r.deknegt@erasmusmc.nl Disclosures
Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR
 Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR This program is supported by educational grants from AbbVie, Gilead Sciences, and Merck About These Slides Please feel free to use,
Hepatitis Alert: Management of Patients With HCV Who Have Achieved SVR This program is supported by educational grants from AbbVie, Gilead Sciences, and Merck About These Slides Please feel free to use,
Denver Shunts vs TIPS for Ascites
 Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
OVERVIEW OF ALD ALCOHOLIC LIVER DISEASE DISCLOSURE
 ALCOHOLIC LIVER DISEASE KEVIN D MULLEN MD West Virginia University Morgantown WV DISCLOSURE I have nothing to disclose. AMOUNT OF ALCOHOL PER STANDARD DRINK > (30 ) GRAM OF ALCOHOL PER DAY USA Canada UK
ALCOHOLIC LIVER DISEASE KEVIN D MULLEN MD West Virginia University Morgantown WV DISCLOSURE I have nothing to disclose. AMOUNT OF ALCOHOL PER STANDARD DRINK > (30 ) GRAM OF ALCOHOL PER DAY USA Canada UK
Evaluating HIV Patient for Liver Transplantation. Marion G. Peters, MD Professor of Medicine University of California San Francisco USA
 Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
Faculty Disclosure. Objectives. Cirrhosis Management for the Family Physician 18/11/2014
 Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Alcohol-Related Liver Disease
 Alcohol-Related Liver Disease Nonalcoholic Fatty Liver Disease (NAFLD) 1 Why is the liver important? Your liver is a vital organ that performs many essential functions. It filters out harmful substances
Alcohol-Related Liver Disease Nonalcoholic Fatty Liver Disease (NAFLD) 1 Why is the liver important? Your liver is a vital organ that performs many essential functions. It filters out harmful substances
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate
 Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Learning Objectives. After attending this presentation, participants will be able to:
 Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Chronic Hepatic Disease
 Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Conflicts of Interest in the last 12 months
 STEATOHEPATITIS Richard K. Sterling, MD, MSc, FACP, FACG VCU Hepatology Professor of Medicine Chief, Section of Hepatology Virginia Commonwealth University Richmond, VA Conflicts of Interest in the last
STEATOHEPATITIS Richard K. Sterling, MD, MSc, FACP, FACG VCU Hepatology Professor of Medicine Chief, Section of Hepatology Virginia Commonwealth University Richmond, VA Conflicts of Interest in the last
Stress Ulcer Prophylaxis In The ICU. Scott W. Wolf Anesthesiology Critical Care Medicine
 Stress Ulcer Prophylaxis In The ICU Scott W. Wolf Anesthesiology Critical Care Medicine Some history Stress Ulceration described in ICU patients as long as 45 years ago Patients had a constellation of
Stress Ulcer Prophylaxis In The ICU Scott W. Wolf Anesthesiology Critical Care Medicine Some history Stress Ulceration described in ICU patients as long as 45 years ago Patients had a constellation of
Acute Liver Failure. Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018
 Acute Liver Failure Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018 Disclosures None Outline Overview of ALF Management of ALF Diagnosis of ALF Treatments and Support
Acute Liver Failure Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018 Disclosures None Outline Overview of ALF Management of ALF Diagnosis of ALF Treatments and Support
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis
 ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
Stick or twist management options in hepatitis C
 Stick or twist management options in hepatitis C Dr. Chris Durojaiye & Dr. Matthijs Backx SpR Microbiology and Infectious Diseases University Hospital of Wales, Cardiff Patient history 63 year old female
Stick or twist management options in hepatitis C Dr. Chris Durojaiye & Dr. Matthijs Backx SpR Microbiology and Infectious Diseases University Hospital of Wales, Cardiff Patient history 63 year old female
Life After SVR for Cirrhotic HCV
 Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Louisville and Louisville VAMC 2015
 Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Louisville and Louisville VAMC 2015 Protein-calorie malnutrition (PCM) is extremely common
Luis S. Marsano, MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Louisville and Louisville VAMC 2015 Protein-calorie malnutrition (PCM) is extremely common
GI bleeding in chronic liver disease
 GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of
 Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology www.livermd.org HCV in advanced disease In principle
Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology www.livermd.org HCV in advanced disease In principle
Therapeutic Strategy in Severe Alcoholic Hepatitis: Present to future development of New
 Therapeutic Strategy in Severe Alcoholic Hepatitis: Present to future development of New Philippe Mathurin Service Maladies de l Appareil Digestif Inserm U995 Hôpital Claude Huriez Lille France molecules
Therapeutic Strategy in Severe Alcoholic Hepatitis: Present to future development of New Philippe Mathurin Service Maladies de l Appareil Digestif Inserm U995 Hôpital Claude Huriez Lille France molecules
PACT module Acute hepatic failure. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
NUTRITION PLANNING FOR PRE AND POST LIVER TRANSPLANT DAPHNEE.D.K HEAD DEPARTMENT OF DIETETICS APOLLO HOSPITALS (MAIN) CHENNAI
 CHENNAI") NUTRITION PLANNING FOR PRE AND POST LIVER TRANSPLANT DAPHNEE.D.K HEAD DEPARTMENT OF DIETETICS APOLLO HOSPITALS (MAIN) CHENNAI PRE - OPERATIVE Case Presentation Name: Mr. XXX Age: 51yrs Sex: Male No. of
NUTRITION PLANNING FOR PRE AND POST LIVER TRANSPLANT DAPHNEE.D.K HEAD DEPARTMENT OF DIETETICS APOLLO HOSPITALS (MAIN) CHENNAI PRE - OPERATIVE Case Presentation Name: Mr. XXX Age: 51yrs Sex: Male No. of
Posthepatectomy Liver Failure. C. Jeske
 Posthepatectomy Liver Failure C. Jeske Introduction Major source of morbidity and mortality after liver resection Devastating complication Little treatment Incidence: 4-19% Recently < 10% Mortality following
Posthepatectomy Liver Failure C. Jeske Introduction Major source of morbidity and mortality after liver resection Devastating complication Little treatment Incidence: 4-19% Recently < 10% Mortality following
What s new in Hepatology AASLD 2016
 What s new in Hepatology AASLD 2016 CWN Spearman C Kassianides What s new in Hepatology? AASLD 2016 CWN SPEARMAN Hepatitis C Alcoholic liver disease Cholestatic Liver Disease Primary biliary Cholangitis
What s new in Hepatology AASLD 2016 CWN Spearman C Kassianides What s new in Hepatology? AASLD 2016 CWN SPEARMAN Hepatitis C Alcoholic liver disease Cholestatic Liver Disease Primary biliary Cholangitis
Nutrition in Liver Disease An overview of the EASL Clinical Practice Guidelines
 Nutrition in Liver Disease An overview of the EASL Clinical Practice Guidelines Marike Bauermeister Registered Dietitian Wits Donald Gordon Medical Centre Malnutrition Malnutrition is a complication in
Nutrition in Liver Disease An overview of the EASL Clinical Practice Guidelines Marike Bauermeister Registered Dietitian Wits Donald Gordon Medical Centre Malnutrition Malnutrition is a complication in
Case Report: Refractory variceal bleeding Christophe Hézode, Henri Mondor Hospital, Paris-Est University, Créteil, France
 Case Report: Refractory variceal bleeding Christophe Hézode, Henri Mondor Hospital, Paris-Est University, Créteil, France Thank you to Marika Rudler, Dominique Thabut, Adrian Gadano, and Jaime Bosch for
Case Report: Refractory variceal bleeding Christophe Hézode, Henri Mondor Hospital, Paris-Est University, Créteil, France Thank you to Marika Rudler, Dominique Thabut, Adrian Gadano, and Jaime Bosch for
DISCLOSURES. This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea
 DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Cardea Services is approved as a provider of continuing nursing education by Montana Nurses Association,
DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Cardea Services is approved as a provider of continuing nursing education by Montana Nurses Association,
Causes of Liver Disease in US
 Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES
 SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES YEON SEOK SEO, 1 SOO YOUNG PARK, 2 MOON YOUNG KIM, 3 SANG GYUNE KIM, 4 JUN YONG PARK, 5 HYUNG JOON YIM,
SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES YEON SEOK SEO, 1 SOO YOUNG PARK, 2 MOON YOUNG KIM, 3 SANG GYUNE KIM, 4 JUN YONG PARK, 5 HYUNG JOON YIM,
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Enterprise Interest Nothing to declare
 Enterprise Interest Nothing to declare 29 th European Congress of Pathology, Amsterdam, Sept 2 nd -6 th, 2017 What s new in alcohol-mediated liver injury? Carolin Lackner Institute of Pathology Medical
Enterprise Interest Nothing to declare 29 th European Congress of Pathology, Amsterdam, Sept 2 nd -6 th, 2017 What s new in alcohol-mediated liver injury? Carolin Lackner Institute of Pathology Medical
Approved regimens for cirrhotic patients
 5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
5th Workshop on HCV THERAPY ADVANCES New antivirals in clinical practice Approved regimens for cirrhotic patients Amsterdam, 4-5 december 2015 Disease burden in Spain 400000 350000 300000 F0 Peak cirrhosis
Key Aspects of Diagnosing Alcoholic Hepatitis. Mark Sonderup University of Cape Town & Groote Schuur Hospital
 Key Aspects of Diagnosing Alcoholic Hepatitis Mark Sonderup University of Cape Town & Groote Schuur Hospital 42 year old woman, married with 3 children No significant co-morbidities or illnesses Habits
Key Aspects of Diagnosing Alcoholic Hepatitis Mark Sonderup University of Cape Town & Groote Schuur Hospital 42 year old woman, married with 3 children No significant co-morbidities or illnesses Habits
CIRROSI E IPERTENSIONE PORTALE NELLA DONNA
 Cagliari, 16 settembre 2017 CIRROSI E IPERTENSIONE PORTALE NELLA DONNA Vincenza Calvaruso, MD, PhD Ricercatore di Gastroenterologia Gastroenterologia & Epatologia, Di.Bi.M.I.S. Università degli Studi di
Cagliari, 16 settembre 2017 CIRROSI E IPERTENSIONE PORTALE NELLA DONNA Vincenza Calvaruso, MD, PhD Ricercatore di Gastroenterologia Gastroenterologia & Epatologia, Di.Bi.M.I.S. Università degli Studi di
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
Steps in Assessing Fibrosis 4/30/2015. Overview of Liver Disease Associated With HCV
 Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Intradialytic Parenteral Nutrition in Hemodialysis Patients. Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia
 Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia Disclosure Information Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy
Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy Amin, Pharm.D., MBA, BCNSP Riyadh, Saudi Arabia Disclosure Information Intradialytic Parenteral Nutrition in Hemodialysis Patients Hamdy
Treating now vs. post transplant
 Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Metabolic diseases of the liver
 Metabolic diseases of the liver Central role in metabolism Causes and mechanisms of dysfunction Clinical patterns of metabolic disease Clinical approach to problem-solving Specific disorders Liver s central
Metabolic diseases of the liver Central role in metabolism Causes and mechanisms of dysfunction Clinical patterns of metabolic disease Clinical approach to problem-solving Specific disorders Liver s central
Bariatric Surgery For Patients With End-Organ Failure
 Bariatric Surgery For Patients With End-Organ Failure Arnold D. Salzberg, M.D. Andrew M. Posselt, M.D., PhD Divisions of Transplant and Minimally Invasive Surgery University of California, San Francisco
Bariatric Surgery For Patients With End-Organ Failure Arnold D. Salzberg, M.D. Andrew M. Posselt, M.D., PhD Divisions of Transplant and Minimally Invasive Surgery University of California, San Francisco
Liver disease in 2017: challenges and opportunities
 Liver disease in 2017: challenges and opportunities Dr Matthew Cowan Consultant Gastroenterologist and Hepatologist Surrey and Sussex Healthcare NHS Trust Faculty of Physician Associates 2 nd National
Liver disease in 2017: challenges and opportunities Dr Matthew Cowan Consultant Gastroenterologist and Hepatologist Surrey and Sussex Healthcare NHS Trust Faculty of Physician Associates 2 nd National
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives
 Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives Margo N. Woods, D.Sc. 1. Define protein-calorie, or protein-energy malnutrition (PEM) and
Nutrition and Medicine, 2006 Tufts University School of Medicine Nutrition and Acute Illness: Learning Objectives Margo N. Woods, D.Sc. 1. Define protein-calorie, or protein-energy malnutrition (PEM) and
HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management
 HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management Stephen G. M. Wong BSc, BSc(Med), MD, MHSc, FRCPC Associate Professor of Medicine Director, Hepatology Education Section of Hepatology
HEPATOrenal Syndrome Type I: Correct Diagnosis = Correct Management Stephen G. M. Wong BSc, BSc(Med), MD, MHSc, FRCPC Associate Professor of Medicine Director, Hepatology Education Section of Hepatology
HCV Management in Decompensated Cirrhosis: Current Therapies
 Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Hepatology cases for the generalist. Will Gelson Consultant Hepatologist Addenbrooke s Hospital
 Hepatology cases for the generalist Will Gelson Consultant Hepatologist Addenbrooke s Hospital 30 y o man with upper GI haemorrhage Background heavy alcohol use Hxof 3 pint haematemesis P 100, BP 90/40,
Hepatology cases for the generalist Will Gelson Consultant Hepatologist Addenbrooke s Hospital 30 y o man with upper GI haemorrhage Background heavy alcohol use Hxof 3 pint haematemesis P 100, BP 90/40,
ESPEN LLL Programme in Clinical Nutrition and Metabolism. List of Topics and Modules 2014
 ESPEN LLL Programme in Clinical Nutrition and Metabolism List of Topics and Modules 204 Code Title Credits for Live course Credits for on-line course Credits for Grading Quiz Topic 0 Introduction in Nutrition
ESPEN LLL Programme in Clinical Nutrition and Metabolism List of Topics and Modules 204 Code Title Credits for Live course Credits for on-line course Credits for Grading Quiz Topic 0 Introduction in Nutrition
Ammonia level at admission predicts in-hospital mortality for patients with alcoholic hepatitis
 Gastroenterology Report, 5(3), 2017, 232 236 doi: 10.1093/gastro/gow010 Advance Access Publication Date: 1 May 2016 Original article ORIGINAL ARTICLE Ammonia level at admission predicts in-hospital mortality
Gastroenterology Report, 5(3), 2017, 232 236 doi: 10.1093/gastro/gow010 Advance Access Publication Date: 1 May 2016 Original article ORIGINAL ARTICLE Ammonia level at admission predicts in-hospital mortality
Complications of Cirrhosis
 Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
List of Topics and Modules (2012)
") List of Topics and Modules (202) Code Title Credits for Live course Topic 0 Introduction to Clinical Nutrition EDU T0 M 0. Introduction to clinical nutrition support Topic Metabolism of Metabolism of Macronutrients,
List of Topics and Modules (202) Code Title Credits for Live course Topic 0 Introduction to Clinical Nutrition EDU T0 M 0. Introduction to clinical nutrition support Topic Metabolism of Metabolism of Macronutrients,
Case 1 AND. Treatment of HCV: Pre- vs Post- Transplant. 58 yo male, ESRD/diabetic nephropathy, HD for 3 weeks
 Treatment of HCV: Pre- vs Post- Transplant Roy D. Bloom MD Professor of Medicine University of Pennsylvania Roy D. Bloom MD Professor of Medicine Medical Director, Kidney Transplant Program University
Treatment of HCV: Pre- vs Post- Transplant Roy D. Bloom MD Professor of Medicine University of Pennsylvania Roy D. Bloom MD Professor of Medicine Medical Director, Kidney Transplant Program University
Etiology based definitions for adult malnutrition: Role of inflammation A systematic approach to nutrition assessment
 Etiology based definitions for adult malnutrition: Role of inflammation A systematic approach to nutrition assessment Gordon L Jensen, MD, PhD Penn State University University Park, PA Objectives Review
Etiology based definitions for adult malnutrition: Role of inflammation A systematic approach to nutrition assessment Gordon L Jensen, MD, PhD Penn State University University Park, PA Objectives Review
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Liver Transplant: Alcoholic liver disease as first indication
 Monotematica AISF The future of liver disease: beyond HCV there is a role for hepatologist? Milano, 13-15 Ottobre 2016 Liver Transplant: Alcoholic liver disease as first indication Giacomo Germani Multivisceral
Monotematica AISF The future of liver disease: beyond HCV there is a role for hepatologist? Milano, 13-15 Ottobre 2016 Liver Transplant: Alcoholic liver disease as first indication Giacomo Germani Multivisceral
The Liver for the Nonhepatologist
 The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Hepatology Director and Medical Director of Liver Transplantation Intermountain Medical Center Salt Lake City, Utah FORMATTED: 05-14-15
The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Hepatology Director and Medical Director of Liver Transplantation Intermountain Medical Center Salt Lake City, Utah FORMATTED: 05-14-15
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
Nutritional Issues In Advanced Liver Disease. Corrie Clark, RDN, LD
 Nutritional Issues In Advanced Liver Disease Corrie Clark, RDN, LD Objectives List specific points to keep in mind when assessing the nutritional status of patients with advanced liver disease. Describe
Nutritional Issues In Advanced Liver Disease Corrie Clark, RDN, LD Objectives List specific points to keep in mind when assessing the nutritional status of patients with advanced liver disease. Describe
Management of acute alcoholic hepatitis
 Management of acute alcoholic hepatitis Yesim ALAHDAB Marmara University Hospital, Istanbul/TURKEY 5 th European Young Hepatologists Workshop August, 27-29, 2015 Moulin de Vernègues, France 1.4L ALCOHOL
Management of acute alcoholic hepatitis Yesim ALAHDAB Marmara University Hospital, Istanbul/TURKEY 5 th European Young Hepatologists Workshop August, 27-29, 2015 Moulin de Vernègues, France 1.4L ALCOHOL
Protocol for daclatasvir (Daklinza ) Approved October 2015 (updated February 2018)
 Approved October 2015 (updated February 2018)") PREFERRED AGENTS: (See drug specific NOTES for exceptions.) Protocol for daclatasvir (Daklinza ) Approved October 2015 (updated February 2018) https://providers.amerigroup.com For genotype 1, Mavyret and
PREFERRED AGENTS: (See drug specific NOTES for exceptions.) Protocol for daclatasvir (Daklinza ) Approved October 2015 (updated February 2018) https://providers.amerigroup.com For genotype 1, Mavyret and
The Liver for the Nonhepatologist
 The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Professor of Medicine University of Chicago Chicago, Illinois Overview Initial assessment of liver disease How do you diagnose cirrhosis?
The Liver for the Nonhepatologist Michael R. Charlton, MBBS, FRCP Professor of Medicine University of Chicago Chicago, Illinois Overview Initial assessment of liver disease How do you diagnose cirrhosis?
Nutritional Issues in Cholestatic Disease
 THE HOSPITAL FOR SICK CHILDREN Nutritional Issues in Cholestatic Disease NASPGHAN-CPNP Joint Session Binita M. Kamath, MBBChir MRCP MTR Associate Professor Division of Gastroenterology, Hepatology and
THE HOSPITAL FOR SICK CHILDREN Nutritional Issues in Cholestatic Disease NASPGHAN-CPNP Joint Session Binita M. Kamath, MBBChir MRCP MTR Associate Professor Division of Gastroenterology, Hepatology and
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Metabolic Disorders. Chapter Thomson - Wadsworth
 Metabolic Disorders Chapter 28 1 Metabolic Disorders Inborn errors of metabolism group of diseases that affect a wide variety of metabolic processes; defective processing or transport of amino acids, fatty
Metabolic Disorders Chapter 28 1 Metabolic Disorders Inborn errors of metabolism group of diseases that affect a wide variety of metabolic processes; defective processing or transport of amino acids, fatty
Investigations before OLT, Immunosuppression and rejection, Follow up after OLT.
 Investigations before OLT, Immunosuppression and rejection, Follow up after OLT andrea.degottardi@insel.ch When is liver transplantation indicated? When is liver transplantation indicated? Frequent: CIRRHOSIS
Investigations before OLT, Immunosuppression and rejection, Follow up after OLT andrea.degottardi@insel.ch When is liver transplantation indicated? When is liver transplantation indicated? Frequent: CIRRHOSIS
The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
Nutrition. ICU Fellowship Training Radboudumc
 Nutrition ICU Fellowship Training Radboudumc Critical Care MCQ s Nasogastric (NG) and nasojejunal (NJ) feeding tubes: A. Enteral nutrition is associated with a reduced risk of bacterial and toxin translocation.
Nutrition ICU Fellowship Training Radboudumc Critical Care MCQ s Nasogastric (NG) and nasojejunal (NJ) feeding tubes: A. Enteral nutrition is associated with a reduced risk of bacterial and toxin translocation.
ESLD a Guide for HIV Physicians. Marion Peters University of California San Francisco June 2015
 ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
PROGRAMME AT A GLANCE
 PROGRAMME AT A GLANCE Hotel Hyatt Andaz Hotel Pullman Date Hall-H1 Hall-H2 Hall-P1 Hall-P2 Hall-P3 Hall-P4 Hall-P5 Hall-P6 Basic science workshop 1 Basic Science Workshop 2 Postgraduate Course - Liver
PROGRAMME AT A GLANCE Hotel Hyatt Andaz Hotel Pullman Date Hall-H1 Hall-H2 Hall-P1 Hall-P2 Hall-P3 Hall-P4 Hall-P5 Hall-P6 Basic science workshop 1 Basic Science Workshop 2 Postgraduate Course - Liver
End-Stage Liver Disease (ESLD): A Guide for HIV Physicians
: A Guide for HIV Physicians") Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Evidence-Base Management of Esophageal and Gastric Varices
 Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
Evidence-Base Management of Esophageal and Gastric Varices Rino Alvani Gani Hepatobiliary Division Department of Internal Medicine Faculty of Medicine Universitas Indonesia Cipto Mangunkusumo National
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents
 Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
Management of the Cirrhotic Patient in the ICU
 Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
MALIGNANT CACHEXIA (CACHEXIA ANOREXIA SYNDROME): Overview
: Overview") MALIGNANT CACHEXIA (CACHEXIA ANOREXIA SYNDROME): Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS II SEMINAR VJ Temple 1 Cachexia:
MALIGNANT CACHEXIA (CACHEXIA ANOREXIA SYNDROME): Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS II SEMINAR VJ Temple 1 Cachexia:
King s College Hospital NHS Foundation Trust. Acute on Chronic Liver Failure: Practical management outside the tertiary centre.
 King s College Hospital NHS Foundation Trust NHS Acute on Chronic Liver Failure: Practical management outside the tertiary centre. William Bernal Professor of Liver Critical Care Liver Intensive Therapy
King s College Hospital NHS Foundation Trust NHS Acute on Chronic Liver Failure: Practical management outside the tertiary centre. William Bernal Professor of Liver Critical Care Liver Intensive Therapy
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Primary Sclerosing Cholangitis Medical Management
 Primary Sclerosing Cholangitis Medical Management Kapil Chopra M.D. Assistant Professor of Medicine Division of Transplant Medicine Mayo Clinic Arizona PSC Primary sclerosing cholangitis is a progressive
Primary Sclerosing Cholangitis Medical Management Kapil Chopra M.D. Assistant Professor of Medicine Division of Transplant Medicine Mayo Clinic Arizona PSC Primary sclerosing cholangitis is a progressive
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Assessment of Liver Function: Implications for HCC Treatment
 Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
Clinical Trials & Endpoints in NASH Cirrhosis
 Clinical Trials & Endpoints in NASH Cirrhosis April 25, 2018 Peter G. Traber, MD CEO & CMO, Galectin Therapeutics 2018 Galectin Therapeutics NASDAQ: GALT For more information, see galectintherapeutics.com
Clinical Trials & Endpoints in NASH Cirrhosis April 25, 2018 Peter G. Traber, MD CEO & CMO, Galectin Therapeutics 2018 Galectin Therapeutics NASDAQ: GALT For more information, see galectintherapeutics.com