DELIRIUM IN ICU: Prevention and Management. Milind Baldi
|
|
|
- Maximillian Brett Boyd
- 6 years ago
- Views:
Transcription
1 DELIRIUM IN ICU: Prevention and Management Milind Baldi
2 Contents Introduction Risk factors Assessment Prevention Management
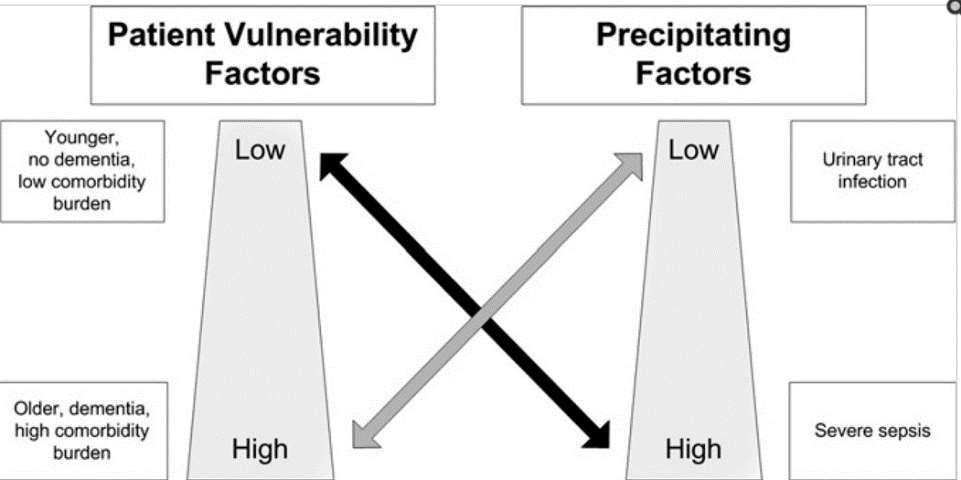
3 Introduction Delirium is a syndrome characterized by acute cerebral dysfunction with a change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Crit Care Med 2013;41(1):
4 Introduction The prevalence of delirium in ICU cohort studies has been reported as low as 20 30% and as high as 70 80% or more. Incidence and prevalence rate of delirium were 24.4% and 53.6% respectively Best Pract Res Clin Anaesthesiol Sep; 26(3): Gen Hosp Psych 2012 Nov-Dec;34(6):639-46
5
6 Diagnosis a standard clinical evaluation does not have an adequate accuracy for the diagnosis Intensive Care Med. 2009, 35:
7 Clinical manifestations o Cognitive Symptoms disorientation, inability to sustain attention, impaired short-term memory, reduced level of consciousness o Behavioral Symptoms sleep-wake cycle disturbance, irritability, hallucinations delusions

8 Delerium Scales
9
10 Critical Care 2012, 16:R115
11 Critical Care 2012, 16:R115
12 The present meta-analysis demonstrates that the CAM ICU is an excellent tool for the detection of delirium in critically ill ICU patients regardless of the subgroup of patients evaluated Critical Care 2012, 16:R115
13
14 the CAM-ICU has a fast application (2-5 min) and does not depend exclusively on the verbal response, thus being relevant for patients on mechanical ventilation
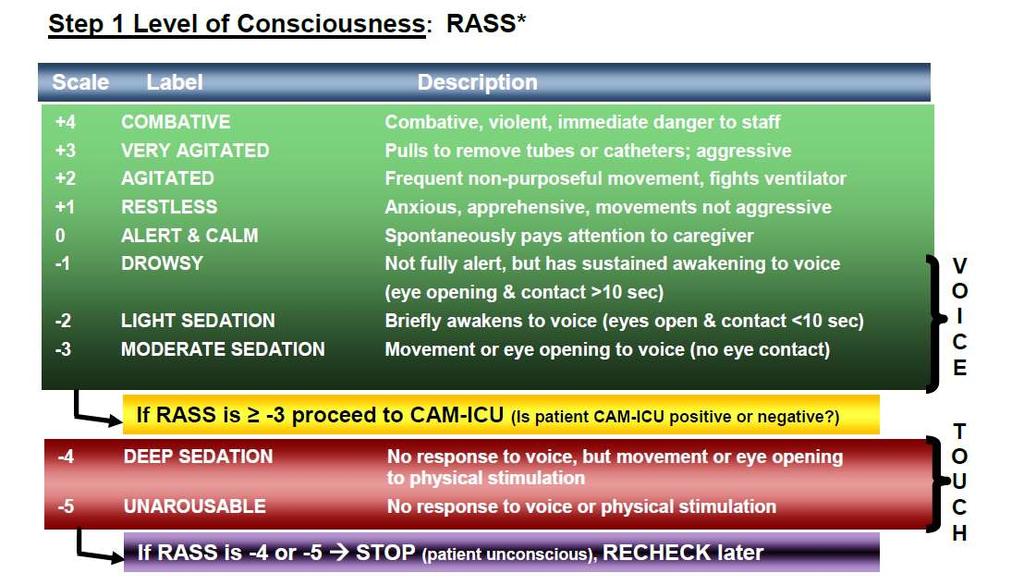
15 Assessing Delirium Step 1: Level of Consciousness
16
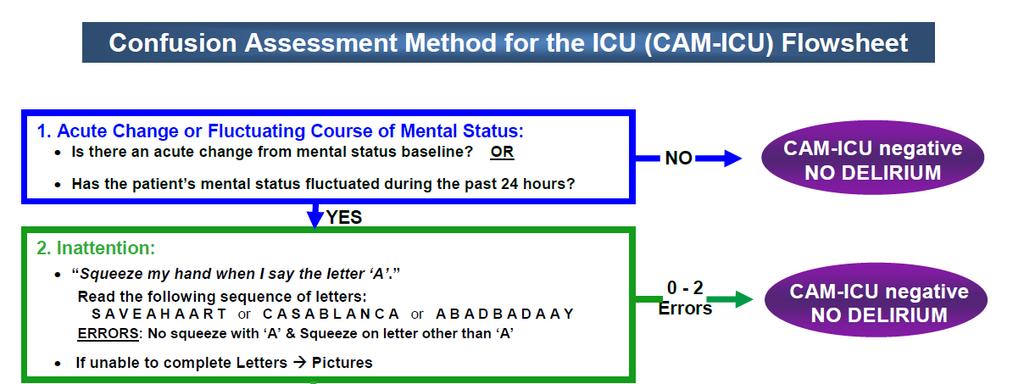
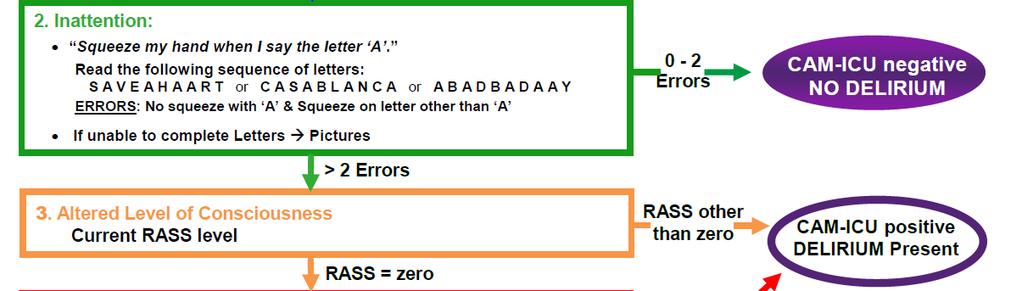
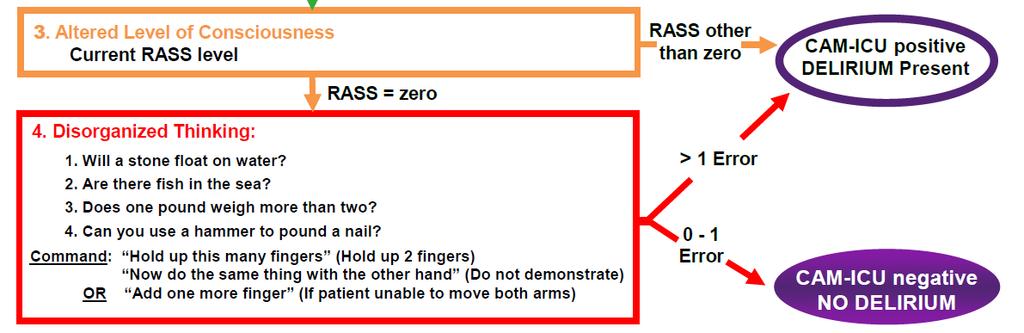
17 Step 2: Content of consciousness
18 Delirium is a syndrome characterized by acute cerebral dysfunction with a change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness.
19 Delirium is a syndrome characterized by acute cerebral dysfunction with a change in baseline mental status,
20 Delirium is a syndrome characterized by acute cerebral dysfunction with a change in baseline mental status, inattention
21 Delirium is a syndrome characterized by acute cerebral dysfunction with a change in baseline mental status, inattention, and either disorganized thinking
22 Delirium is a syndrome characterized by acute cerebral dysfunction with a change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness.
23
24
25
26
27 Versions available in Hindi and other regional languages too
28 DSM V No major changes from DSM-IV were made to the core elements of DSM-5 criteria for delirium, there are some differences in content and wording of the criteria.
29 BMC Medicine 2014, 12:164
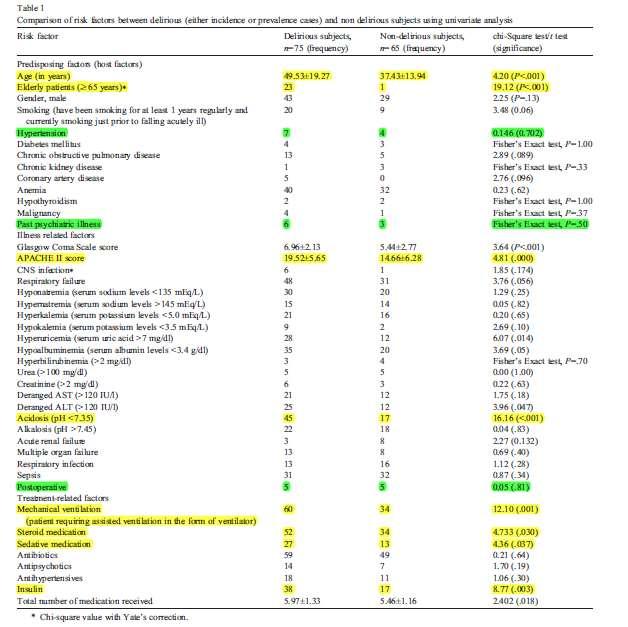
30 PREDECTING Delirium Development and validation of PRE-DELIRIC (PREdiction of DELIRium in ICu patients) delirium prediction model for intensive care patients: observational multicentre study 10 risk factors age, APACHE-II score, admission group, coma, infection, metabolic acidosis, use of sedatives and morphine, urea concentration, and urgent admission BMJ 2012;344:e420
31 Intensive Care Med (2014) 40:
32 RISK FACTORS Strong o Age o Dementia o Hypertension o Coma o APACHE II o Delirium previous day o Emergency surgery o Mechanical ventilation o Polytrauma o Metabolic acidosis Inconclusive o Alcohol use o Nicotine use o Acute respiratory disease o Kidney failure o Fever o benzodiazepines Crit Care Med 2015; 43:40 47
33 Delirium risk factors Four baseline risk factors are positively and significantly associated with the development of delirium in the ICU: preexisting dementia, history of hypertension and/or alcoholism, and a high severity of illness at admission. Benzodiazepine use may be a risk factor for the development of delirium in adult ICU patients. In mechanically ventilated adult ICU patients at risk of developing delirium, dexmedetomidine infusions administered for sedation may be associated with a lower prevalence of delirium compared to benzodiazepine infusions Crit Care Med 2013; 41:
34
35 In this article, we advocate for the adoption and implementation of a standard bundle of ICU measures with great potential to reduce the burden of ICU-acquired delirium and weakness CHEST 2010; 138(5):
36 Prevention Individual components of this bundle are evidence based and can help standardize communication, improve interdisciplinary care, reduce mortality, and improve cognitive and functional outcomes. ABCDE bundle, for awakening and breathing coordination, delirium monitoring, and exercise/early mobility CHEST 2010; 138(5):
37 Building blocks of managing Pain, Agitation and Delirium A B C D E
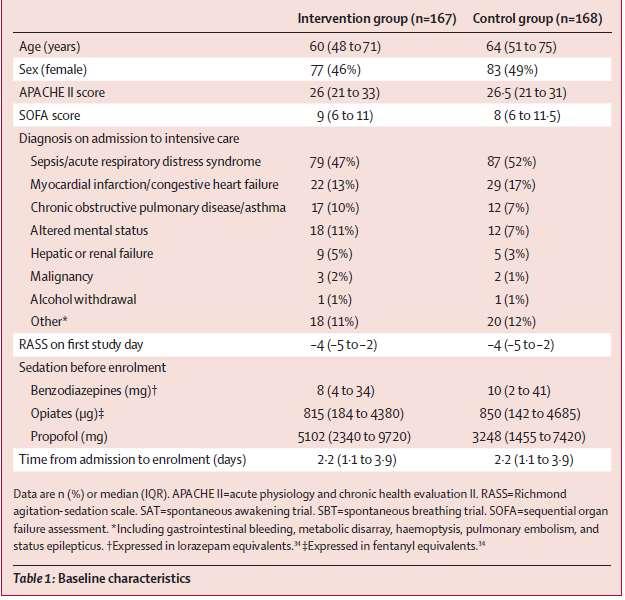
38 Birth of ABCDE A Kress JP, et al. N Engl J Med 2000;342: B Ely EW, et al. N Engl J Med 1996;335: C Riker R. et al, JAMA. 2009;301: D Preventing and Managing Delirium E Schweickert et al, Lancet 2009;373:
39 Birth of ABCDE A Kress JP, et al. N Engl J Med 2000;342: B Ely EW, et al. N Engl J Med 1996;335: C Riker R. et al, JAMA. 2009;301: D Preventing and Managing Delirium E Schweickert et al, Lancet 2009;373:
40 Ely EW, et al. N Engl J Med 1996;335: Birth of ABCDE
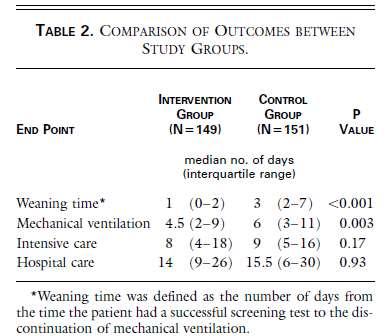
41 Spontaneous Breathing Trial Daily screening of the respiratory function of adults receiving mechanical ventilation, followed by trials of spontaneous breathing Ely EW, et al. N Engl J Med 1996;335:1864-9
42
43 Your patient has successfully completed a 2- hour trial of spontaneous breathing and has an 85 percent chance of successfully staying off mechanical ventilation for 48 hours
44
45 A Kress JP, et al. N Engl J Med 2000;342: B Ely EW, et al. N Engl J Med 1996;335: C Riker R. et al, JAMA. 2009;301: D Preventing and Managing Delirium E Schweickert et al, Lancet 2009;373:
46 N Engl J Med 2000;342: Birth of ABCDE
47

48 Spontaneous Awakening Trial

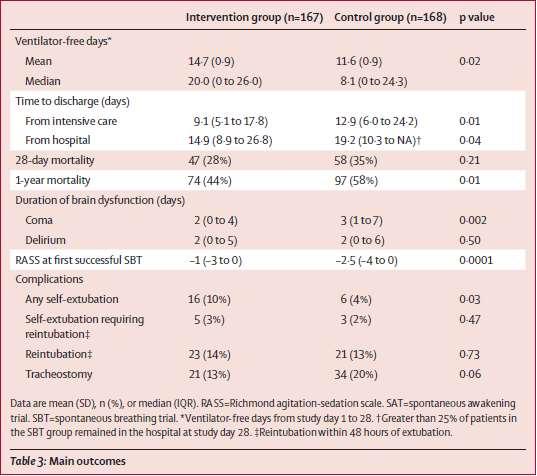
49 Lancet 2008; 371: C (A+B)
50 administration of sedatives by continuous infusion has been identified as an independent predictor of a longer duration of mechanical ventilation as well as a longer stay in the intensive care unit and in the hospital. Extended sedation may limit clinicians ability to interpret physical examinations. It may be difficult to distinguish changes in mental status that are due to the action of a sedative from those that are due to neurologic injury.
51
52
53
54 Birth of ABCDE A Kress JP, et al. N Engl J Med 2000;342: B Ely EW, et al. N Engl J Med 1996;335: C Riker R. et al, JAMA. 2009;301: D Preventing and Managing Delirium E Schweickert et al, Lancet 2009;373:

55 Birth of ABCDE
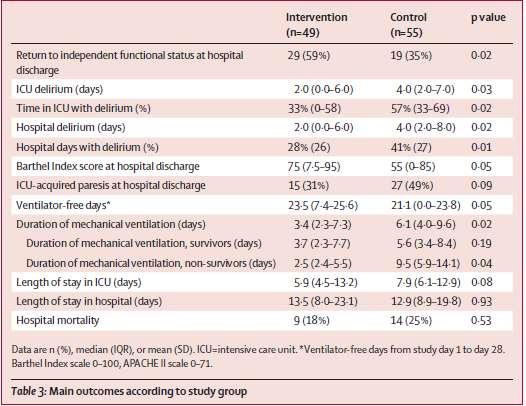
56 Birth of ABCDE randomization to early exercise and mobilization (physical and occupational therapy) during periods of daily interruption of sedation (intervention; n=49) or to daily interruption of sedation with therapy as ordered by the primary care team

57 Early Mobilty and Exercise
58
59 Birth of ABCDE A Kress JP, et al. N Engl J Med 2000;342: B Ely EW, et al. N Engl J Med 1996;335: C Riker R. et al, JAMA. 2009;301: D Preventing and Managing Delirium E Schweickert et al, Lancet 2009;373:
60 Preventing delirium through improving sleep in the ICU Very little sleep in the ICU is restorative, REM sleep Reasons for poor sleep in the ICU include the continuous cycle of alarms, lights, beepers, carerelated interruptions, pain, anxiety and ventilator dyssynchrony. medications that disrupt REM sleep including sedatives (particularly benzodiazepines), analgesics, vasopressors, beta-agonists, and corticosteroids Crit Care Clin January ; 29(1): 51 65
61 Preventing delirium through improving sleep in the ICU Peak noise is not the main determinant disturbing the patient in the ICU. Phones ringing and people talking are reported as more annoying Patients sleeping with earplugs showed 15% mild confusion, whereas the control patients scored 40% in this category. Taking both categories, delirium and mild confusion, into account, 60% of the control group showed cognitive disturbances against only 35% in the study group. Critical Care 2012, 16:R73
62 Preventing delirium through pharmacologic interventions no medication is FDA approved for the prevention or treatment of delirium
63 Haloperidol prophylaxis in critically ill patients with a high risk for delirium Results of prophylactic treatment were compared with a historical control group and a contemporary group (n = ) The predicted chance of developing delirium in the intervention and control group was 75 ± 19% and 73 ± 22%, respectively (P = 0.50) intravenous haloperidol 1 mg/8 h Critical Care 2013, 17:R9
64 The actual delirium incidence was 65% in the intervention group, compared with 75% in the control group (P = 0.01) Prophylactic treatment with haloperidol resulted in a relative 28-day mortality reduction of 20% (hazard rate 0.80; 95% CI 0.66 to 0.98). Haloperidol was stopped in 12 patients because of QTc-time prolongation (n = 9), renal failure (n = 1) or suspected neurological side-effects (n = 2).
65 Effect of intravenous haloperidol on the duration of delirium and coma in critically ill patients (Hope-ICU): a randomised, doubleblind, placebo-controlled trial to receive haloperidol 2 5 mg or 0 9% saline placebo intravenously every 8 h Lancet Respir Med 2013;1:
66 Patients in the haloperidol group spent about the same number of days alive, without delirium, and without coma as did patients in the placebo group These results do not support the hypothesis that haloperidol modifies duration of delirium in critically ill patients
67 The HARPOON study Efficacy and safety of haloperidol prophylaxis for delirium prevention in older medical and surgical at-risk patients acutely admitted to hospital through the emergency department
:489-499")
68 Preventing delirium through management of sedatives JAMA. 2009;301(5):
:489-499")
69 JAMA. 2009;301(5): Choice of Sedation
70 Preventing delirium through management of sedatives Benzodiazepine Versus Nonbenzodiazepine- Based Sedation for Mechanically Ventilated, Critically Ill Adults: A Systematic Review and Meta-Analysis of Randomized Trials Critical care medicine, 2013 Sep;41(9 Suppl 1):S30-8
71 Critical care medicine, 2013 Sep;41(9 Suppl 1):S30-8
72 Benzodiazepine Versus Nonbenzodiazepine-Based Sedation Compared to a benzodiazepine sedative strategy, a nonbenzodiazepine sedative strategy was associated with a shorter ICU length of stay (n = 6 studies; difference = 1.62 d; 95% CI, ; p = ) duration of mechanical ventilation (n = 4 studies; difference = 1.9 d; 95% CI, ; p < ) But a similar prevalence of delirium (n = 2; risk ratio = 0.83; 95% CI, ; p = 0.19) Critical care medicine, 2013 Sep;41(9 Suppl 1):S30-8
73 Alpha-2 agonists for long-term sedation during mechanical ventilation in critically ill patients Seven studies, covering 1624 participants, compared dexmedetomidine with traditional sedatives reduced the mean duration of mechanical ventilation by 22% (95% CI 10% to 33%; four studies, 1120 participants, low quality evidence) the length of stay in the intensive care unit (ICU) by 14% (95% CI 1% to 24%; five studies, 1223 participants, very low quality evidence). no evidence that dexmedetomidine decreased the risk of delirium (RR 0.85; 95% CI 0.63 to 1.14; seven studies, 1624 participants, very low quality evidence) Cochrane Database of Systematic Reviews,2015 Jan 6;1:CD010269
74 Preventing delirium through pain management ICU patients who were assessed for pain were less likely to receive sedatives, particularly deliriogenic benzodiazepines, and more likely to receive analgesic medications (non-opioids or opioids) than those who never had a pain assessment Anesthesiology 2009 Dec;111(6):
75 Crit Care Med 2013; 41: Delirium prevention Early mobilization of adult ICU patients whenever feasible to reduce the incidence and duration of delirium. no recommendation for using a pharmacologic delirium prevention protocol in adult ICU patients, as no compelling data demonstrate that this reduces the incidence or duration of delirium in these patients. Haloperidol or atypical antipsychotics administration is not recommended to prevent delirium in adult ICU patients. We provide no recommendation for the use of dexmedetomidine to prevent delirium in adult ICU patients, as there is no compelling evidence regarding its effectiveness in these patients.
76 Treatment Nonpharmacological and pharmacological therapy. the therapy of potential underlying cause, that is, medical conditions that promote delirium should be evaluated and treated. The nonpharmacological treatment strategy is in large part similar to the prevention strategies. Current Opinion in Critical Care 2011, 17:
77 The question how to treat delirium correctly is not easily answered, because there has been no conclusive evidence from a multitude of surveys Current Opinion in Critical Care 2011, 17:
78 In the previous version of these guidelines, the recommended use of haloperidol for the treatment of delirium was a Level C recommendation based only on a case series. These data did not meet the evidence standard for this version of the guidelines. No recent prospective trials have verified the safety and efficacy of haloperidol for the treatment of delirium in adult ICU patients. Data on the use of other antipsychotics in this patient population are similarly sparse. Robust data on haloperidol in non-icu patients that could potentially be applied to the ICU patient population are lacking Crit Care Med 2013; 41:
79 Haloperidol, risperidone, olanzapine and aripiprazole in the management of delirium: A comparison of efficacy, safety, and side effects were equally effective in the management of delirium; however, they differed in terms of their side-effect Palliat Support Care Sep 5:1-7
80 The atypical antipsychotics are attractive alternatives to haloperidol with improved safety profiles but are flawed by limited data to support dosing and efficacy Future studies that provide large, prospective, double-blinded, placebo-controlled data to support the implementation of these agents as standard therapy over haloperidol are needed Journal of Intensive Care Medicine 2012 Nov Dec 27(6)
81 Rapidity of onset Haloperidol has an onset of action 15 to 20 minutes after intravenous infusion. Duration of effect it's duration of effect varies and depends upon the cumulative dose. Dosage regimens The administration of haloperidol intravenously is common, but it has not been approved by the United States' Food and Drug Administration (FDA). 2 to 10 mg intravenous bolus doses administered every 20 to 30 minutes until calm is achieved
82 Take home message Identifying patients with high risk factors Frequent formal assessment for delirium Assess for pain at frequent intervals Sticking to a bundled approach for delirium prevention Haloperidol prophylaxis in patients with high risk Non pharmacological treatment of delirium
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
ICU Liberation for the Pharmacist. A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center
 ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
ICU Liberation for the Pharmacist A. Kendall Gross, PharmD, BCPS, BCCCP Critical Care Pharmacist UCSF Medical Center Disclosure No conflicts of interest to disclose Objectives o Outline the elements of
+ Change in baseline mental status, inattention, and either disorganized thinking or altered level of consciousness. Delirium. Disclosure.
 47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
47 th Annual Meeting August 2-4, 2013 Orlando, FL Identification, Prevention and Treatment of Delirium: The Role of the Health System Pharmacist Jennifer Cortes, PharmD, BCPS Medical ICU Clinical Pharmacy
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting
 Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
Sarah V. Cogle, PharmD, BCCCP Assistant Clinical Professor Auburn University Harrison School of Pharmacy Auburn, AL ALSHP Annual Clinical Meeting 2018 I have no actual or potential conflict of interest
KEY REFERENCES Laying the foundation for D of ABCDEF bundle
 KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
KEY REFERENCES Laying the foundation for D of ABCDEF bundle Ely E. JAMA. 2001;286:2703-2710 (CAM-ICU) Bergeron N. Intensive Care Med. 2001;27:859-864 (ICDSC) Dubois M. Intensive Care Med. 2001;27:1297-1304
Conducting Delirium Research
 Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Optimizing Clinical Trials When Conducting Research Research funding: Disclosure NHLBI, NIA, AstraZeneca John W. Devlin, PharmD, FCCP, FCCM, Professor of Pharmacy, Northeastern University Scientific Staff,
Ventilator-Associated Event Prevention: Innovations
 Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Ventilator-Associated Event Prevention: Innovations Michael J. Apostolakos, MD Professor of Medicine Director, Adult Critical Care University of Rochester Mobility/Sedation in the ICU Old teaching: Keep
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018
 ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
ABCs of ICU Delirium Marian Maxwell, Pharm.D., BCCCP January 6, 2018 Disclosures I do not have any financial/non-financial relationships to disclose. Learning Objectives Define delirium and discuss the
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium Monograph - Update, Spring 2014
 Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Sedation of the Critically Ill Patient
 Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
Buffalo theory of sedation It s a well known fact that a herd of buffalo can only move as fast as the slowest buffalo. And when the herd is hunted, it s the slowest and weakest ones at the back that are
ICU Delirium and sedation: understanding their role in long-term patient outcomes. Yoanna Skrobik MD FRCP(c)
") ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
ICU Delirium and sedation: understanding their role in long-term patient outcomes Yoanna Skrobik MD FRCP(c) Conflicts of interest Member, SCCM Pain, Agitation and Delirium guidelines writing committee
Overview of Presentation. Delirium Definition. Assessing & Managing ICU Delirium: What is the Evidence?
 Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Assessing & Managing ICU Delirium: What is the Evidence? Dale Needham, MD, PhD Professor Pulmonary & Critical Care Medicine, and Physical Medicine & Rehabilitation Medical Director, Critical Care Physical
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Canadian Practices for the Treatment of Delirium. Lisa Burry, BScPharm, PharmD
 Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Canadian Practices for the Treatment of Delirium Lisa Burry, BScPharm, PharmD Disclosures & Acknowledgements Conflicts of interest: None Acknowledgements: our patients and the clinical staff that supported
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
DELIRIUM. J. Sukanya 28.Jun.12
 DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
DELIRIUM J. Sukanya 28.Jun.12 Outline Why? What? How? What s next? Delirium Introduction Delirium An acute decline in attention and cognition The most frequent neuropsychiatric syndrome A common, life-threatening,
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University
 Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico
 Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Interaction between Sedation and Weaning: How to Balance Them? Guillermo Castorena MD Fundacion Clinica Medica Sur Mexico Balance is not that easy! Weaning Weaning is the liberation of a patient from
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients
 Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit January 2013 Volume 41 Number 1 Society of Critical Care Medicine 本檔僅供內部教學使用檔案內所使用之照片之版權仍屬於原期刊公開使用時,
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
Delirium Screening and Prevention Faculty Disclosures
 Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Faculty Disclosures I have nothing to disclose Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Objectives Discuss prevalence, risk factors
Management of delirium in mechanically ventilated patients. Advances in Critical Care Medicine King Hussein Cancer Center
 Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Management of delirium in mechanically ventilated patients Advances in Critical Care Medicine King Hussein Cancer Center Introduction Outline: Prevalence of delirium in ICU Why it is important to screen
Conflict of Interest. Patient Case. Objectives. The Balancing Act. Why We Need Sedation
 Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Agitation in the ICU Have we swung the pendulum too far from benzodiazepines? Conflict of Interest The author of this presentation has no conflicts of interest to disclose Nina Vadiei, PharmD PGY1 Pharmacy
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Screening and Prevention. Faculty Disclosures. Objectives 5/13/2014. I have nothing to disclose
 Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
Delirium Screening and Prevention Kathleen Puntillo RN, PhD, FAAN, FCCM Professor Emeritus School of Nursing, UCSF Faculty Disclosures I have nothing to disclose Objectives Discuss prevalence, risk factors
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Centre for Clinical Practice Surveillance Programme
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Centre for Clinical Practice Surveillance Programme Recommendation for Guidance Executive (post-consultation) Clinical guideline CG103: Delirium: diagnosis,
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Centre for Clinical Practice Surveillance Programme Recommendation for Guidance Executive (post-consultation) Clinical guideline CG103: Delirium: diagnosis,
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice
 in the Intensive Care Unit: Translating Evidence Into Practice") Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Improving the Management of Pain, Agitation, and Delirium (PAD) in the Intensive Care Unit: Translating Evidence Into Practice Christine M. Groth, Pharm.D., BCCCP NYS Partnership for Patients September
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba
 Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Kendiss Olafson MD FRCPC MPH Section of Critical Care University of Manitoba Outline Sedation in ICU Purpose/Goals Common Drugs Sedation delivery strategies Mobility in the ICU Weakness with critical illness
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Page VJ, Casarin A, Ely EW, et al. Evaluation
Can Goal Directed Sedation Improve Outcomes?
 Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Can Goal Directed Sedation Improve Outcomes? Yahya SHEHABI, FANZCA, FCICM, EMBA Professor and Program Director Critical care Monash Health and Monash University - Melbourne School of Medicine, University
Antipsychotic Medications
 TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS
 ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
ICU LIBERATION: IMPLEMENTING THE ABCDEF BUNDLE AND IMPROVING THE LIVES OF ICU PATIENTS J. MATTHEW ALDRICH, MD ASSOCIATE CLINICAL PROFESSOR OF ANESTHESIA AND PERIOPERATIVE CARE UNIVERSITY OF CALIFORNIA
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University
 Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University Crit Care Med. 2004;32(4):955 62. BMJ. 2015;350:h2538. Background Delirium, defined as acute brain
Jie Chen Department of Critical Care Medicine, Zhongda Hospital, School of Medicine, Southeast University Crit Care Med. 2004;32(4):955 62. BMJ. 2015;350:h2538. Background Delirium, defined as acute brain
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network
 Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
Doug Paul, D.O. FACOS Medical Director, Trauma Services Kettering Health Network A paradigm shift (or revolutionary science) is, a change in the basic assumptions, or paradigms, within the ruling theory
VENTILATOR ACQUIRED DELIRIUM CREATED BY JOSHUA VRONA COHP 450
 VENTILATOR ACQUIRED DELIRIUM CREATED BY JOSHUA VRONA COHP 450 INTRODUCTION: Delirium is defined as An acute change in mental status or a fluctuating course, impaired attention, and disorganized thinking.
VENTILATOR ACQUIRED DELIRIUM CREATED BY JOSHUA VRONA COHP 450 INTRODUCTION: Delirium is defined as An acute change in mental status or a fluctuating course, impaired attention, and disorganized thinking.
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Preventing Delirium in the IntensiveCareUnit
 Preventing Delirium in the IntensiveCareUnit Nathan E. Brummel, MD a,b,c, *, Timothy D. Girard, MD, MSCI a,b,c,d KEYWORDS Delirium Intensive care unit Prevention Sedation KEY POINTS Delirium in the intensive
Preventing Delirium in the IntensiveCareUnit Nathan E. Brummel, MD a,b,c, *, Timothy D. Girard, MD, MSCI a,b,c,d KEYWORDS Delirium Intensive care unit Prevention Sedation KEY POINTS Delirium in the intensive
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Collaborative Regional Benchmarking Group (North of England, North Yorkshire & Humber and West Yorkshire)
") Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Best Practice Guidance Sedation These recommendations are bound by the current evidence and best practice at the time of writing and so will be subject to change as further developments are made in this
Disclosure. Hospira Pharmaceuticals. Unrestricted research funding Honoraria for CME education administered via France Foundation
 Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Disclosure Hospira Pharmaceuticals Unrestricted research funding Honoraria for CME education administered via France Foundation Economics in Sedation: Responsible Use of the ICU Budget John W. Devlin,
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Dexmedetomidine: the various roles and utilization strategies. Julie Belfer, PharmD September 2014
 Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR
 Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry
 Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
Do benzos, opioids, or strong anticholinergics cause delirium? Lisa Burry Delirium in the ICU Occurs in up to 85% of MICU/SICU MV patients 20-50% of lower severity ICU patients develop delirium Hypoactive
9/28/2016. Sedation Strategies in the ICU. Outline. ICU sedation. Recent clinical practice guidelines Top 10 myths A practical approach
 Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Update - Delirium in Elders
 Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
Update - Delirium in Elders Impact Recognition Prevention, and Management Michael J. Lichtenstein, MD F. Carter Pannill, Jr. Professor of Medicine Chief, Division of Geriatrics, Gerontology and Palliative
North Wales Critical Care Network
 North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State
 Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
Delirium Prevention: The State-of-the-Art & Implications to Improve Care in our State Jonny Macias, MD & Michael Malone, MD Aurora Health Care/ University of Wisconsin School of Medicine & Public Health
BRAIN. Tumor byproducts. Autonomic nerves. Somatic nerves. Host immune cells. Cytokines
 Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Liberation from Mechanical Ventilation in Critically Ill Adults
 Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
Liberation from Mechanical Ventilation in Critically Ill Adults 2017 ACCP/ATS Clinical Practice Guidelines Timothy D. Girard, MD, MSCI Clinical Research, Investigation, and Systems Modeling of Acute Illness
ABCDEF Bundle Breakout
 ABCDEF Bundle Breakout Andrew Masica, MD, MSCI VP, Chief Clinical Effectiveness Officer Baylor Scott & White Health andrew.masica@bswhealth.org Disclosures/Funding Support Grant R18-HS021459 from the Agency
ABCDEF Bundle Breakout Andrew Masica, MD, MSCI VP, Chief Clinical Effectiveness Officer Baylor Scott & White Health andrew.masica@bswhealth.org Disclosures/Funding Support Grant R18-HS021459 from the Agency
Supplementary Online Content
 Supplementary Online Content van den Boogaard M, Slooter AJC, Brüggemann RJM. Effect of haloperidol on survival among critically ill adults with a high risk of delirium: the REDUCE randomized clinical
Supplementary Online Content van den Boogaard M, Slooter AJC, Brüggemann RJM. Effect of haloperidol on survival among critically ill adults with a high risk of delirium: the REDUCE randomized clinical
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Geriatrics and Cancer Care
 Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
Geriatrics and Cancer Care Roger Wong, BMSc, MD, FRCPC, FACP Postgraduate Dean of Medical Education Clinical Professor, Division of Geriatric Medicine UBC Faculty of Medicine Disclosure No competing interests
ICU Updates: Delirium in Hospitalized Patients
 ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
ICU Updates: Delirium in Hospitalized Patients James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC Recognizing and preventing delirium
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018
 Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018") Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Pain, Agitation & Delirium (2013) Immobility & Sleep (2018) Catherine Jones Practice Educator GICU October 2018 1 Plan for session Why Pain Agitation & Delirium are important considerations in critical
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics
 Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Jacinta Lucke Resident Emergency Medicine PHD Gerontology & Geriatrics TAKE HOME MESSAGE When managing confusion in older patients: Routinely screen for impaired cognition Patients with impaired cognition
Delirium is a frequent complication in the ICU setting.
 Clinical Investigations Dexmedetomidine for the Treatment of Hyperactive Delirium Refractory to Haloperidol in Nonintubated ICU Patients: A Nonrandomized Controlled Trial* Genís Carrasco, PhD, MD; Nacho
Clinical Investigations Dexmedetomidine for the Treatment of Hyperactive Delirium Refractory to Haloperidol in Nonintubated ICU Patients: A Nonrandomized Controlled Trial* Genís Carrasco, PhD, MD; Nacho
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
DELIRIUM IN THE PICU ALLISON M. CHUNG, PHARM.D., BCPPS, BCPS, FCCP
 DELIRIUM IN THE PICU ALLISON M. CHUNG, PHARM.D., BCPPS, BCPS, FCCP Associate Professor Auburn University Harrison School of Pharmacy Adjunct Professor University of South Alabama, Children and Women s
DELIRIUM IN THE PICU ALLISON M. CHUNG, PHARM.D., BCPPS, BCPS, FCCP Associate Professor Auburn University Harrison School of Pharmacy Adjunct Professor University of South Alabama, Children and Women s
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
Early Goal Directed Sedation In Critically Ill Patients
 Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
Early Goal Directed Sedation In Critically Ill Patients Yahya Shehabi, FCICM, FANZCA, EMBA Professor, Intensive Care Medicine Clinical School of Medicine, University New South Wales School of Epidemiology
ICU Updates: Delirium in Hospitalized Patients
 Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Outline James A. Frank, MD Associate Professor Pulmonary and Critical Care UCSF Dept. of Medicine Director, MICU San Francisco VAMC ICU Updates: in Hospitalized Patients Recognizing and preventing delirium
Strategies to minimize delirium for hip fracture patients
 Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Strategies to minimize delirium for hip fracture patients Stephen L Kates, M.D. Professor and Chairman Department Date of Orthopaedic Surgery Delirium incidence Up to 61% of hip fracture patients get delirium
Nicotine replacement therapy for agitation and delirium management in the intensive care unit: a systematic review of the literature
 Kowalski et al. Journal of Intensive Care (2016) 4:69 DOI 10.1186/s40560-016-0184-x RESEARCH Nicotine replacement therapy for agitation and delirium management in the intensive care unit: a systematic
Kowalski et al. Journal of Intensive Care (2016) 4:69 DOI 10.1186/s40560-016-0184-x RESEARCH Nicotine replacement therapy for agitation and delirium management in the intensive care unit: a systematic
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome (ACS), burden of condition, 83 diagnosis of, 82 83 evaluation of, 83, 87 major complications of, 86 risk for,
Index Note: Page numbers of article titles are in boldface type. A Acute coronary syndrome (ACS), burden of condition, 83 diagnosis of, 82 83 evaluation of, 83, 87 major complications of, 86 risk for,
Risks of Antipsychotics use In Dementia
 AHCA/NCAL Quality Initiative for Assisted Living Webinar Series: Safely Reducing the Off-Label Use of Antipsychotics Risks of Antipsychotics use In Dementia Sanjay P. Singh, MD Chairman & Professor, Department
AHCA/NCAL Quality Initiative for Assisted Living Webinar Series: Safely Reducing the Off-Label Use of Antipsychotics Risks of Antipsychotics use In Dementia Sanjay P. Singh, MD Chairman & Professor, Department
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know
 Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, MS, CPNP-AC/PC, CNS, CCRN Pediatric Intensive Care Nurse Practitioner Lucile Packard
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, MS, CPNP-AC/PC, CNS, CCRN Pediatric Intensive Care Nurse Practitioner Lucile Packard
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know
 Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, PhD, CPNP-AC/PC, CNS; Cincinnati Children s Hospital Medical Center Mary Rummell,
Comfort Management in the Adult with Congenital Heart Disease What the ICU Bedside Nurse Needs to Know Sandy Staveski RN, PhD, CPNP-AC/PC, CNS; Cincinnati Children s Hospital Medical Center Mary Rummell,
Cambridge University Press Effective Treatments in Psychiatry Peter Tyrer and Kenneth R. Silk Excerpt More information
 Organic disorders 1 Delirium Based on Delirium by Laura Gage and David K. Conn in Effective Treatments in Psychiatry, Cambridge University Press, 2008 Introduction Delirium needs treatment for both its
Organic disorders 1 Delirium Based on Delirium by Laura Gage and David K. Conn in Effective Treatments in Psychiatry, Cambridge University Press, 2008 Introduction Delirium needs treatment for both its
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
POST-INTUBATION ANALGESIA AND SEDATION. August 2012 J Pelletier
 POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
New approaches of sedation in critically ill patients.
 New approaches of sedation in critically ill patients. Jean Mantz, MD, PhD Professor and Chair, Department of Anesthesia and Critical Care F- Paris Val de Seine University Hospitals Univ Paris Diderot,
New approaches of sedation in critically ill patients. Jean Mantz, MD, PhD Professor and Chair, Department of Anesthesia and Critical Care F- Paris Val de Seine University Hospitals Univ Paris Diderot,
A Healthy Brain. An Injured Brain
 A Healthy Brain Before we can understand what happens when a brain is injured, we must realize what a healthy brain is made of and what it does. The brain is enclosed inside the skull. The skull acts as
A Healthy Brain Before we can understand what happens when a brain is injured, we must realize what a healthy brain is made of and what it does. The brain is enclosed inside the skull. The skull acts as
Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium
 Online Data Supplement Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium Monitoring/Management, and Early Exercise/Mobility (ABCDE) Bundle Authors-Michele C. Balas, Eduard
Online Data Supplement Effectiveness and Safety of the Awakening and Breathing Coordination, Delirium Monitoring/Management, and Early Exercise/Mobility (ABCDE) Bundle Authors-Michele C. Balas, Eduard
Disclosures. Post operative Delirium. Set up audience participation. Delirium Definitions. Incidence of Delirium
 Post operative Delirium Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set up audience
Post operative Delirium Disclosures IP for monitoring technology licensed to Medtronic Ken Brady, MD Pediatrics, Anesthesia, Critical Care Texas Children s Hospital Baylor College of Medicine Set up audience
Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes
 The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
The Intensive Care Society 2008 Delirium in the intensive care unit: a narrative review of published assessment tools and the relationship between ICU delirium and clinical outcomes C Waters Delirium is
譫妄症 (Delirium) Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28
 Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28") 譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
Critical Care Strategic Clinical Network Provincial ICU Delirium Framework
 Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting
Pain assessed and documentation using validated tool (CPOT and NRS) Assess and document q4h and prn 100% of patients assessed for pain and documented q4h A: Assess, Prevent & Manage Pain Self Reporting