Delirium in Cancer: Psychopharmacologic Management
|
|
|
- Bruce Bryant
- 6 years ago
- Views:
Transcription
1 Delirium in Cancer: Psychopharmacologic Management William Breitbart, MD Professor and Chief, Psychiatry Service Memorial Sloan-Kettering Cancer Center New York, New York
2 Delirium in Patients with Cancer Prevalence ranges from 15% - 30% in hospitalized cancer patients Highly prevalent in the last weeks of life (40% - 85%) Associated with increased morbidity/distress in patients, family, staff Interferes with symptom assessment and control
3 Delirium in Patients with Cancer Delirium is under-recognized and under-treated. One of the barriers to adequate clinical intervention in delirium is the lack of appreciation for the distress experienced by patients with delirium, as well as the impact of delirium on spouses/caregivers and staff. We suspect that patients with hypoactive delirium are perceived to be in less distress than agitated patients with hyperactive delirium.
4 DSM-IV Criteria for Delirium A. Disturbance of consciousness (i.e., disturbance of awareness of the environment) with reduced ability to focus, sustain or shift attention B. Change in cognition (such as memory deficit, disorientation, language disturbance, perceptual disturbance) that is not better accounted for by a preexisting, established or evolving dementia
5 DSM-IV Criteria for Delirium (Con t) C. The disturbance evolves over a short period of time (usually hours to days) and tends to fluctuate during the course of the day D. There is evidence from the history, physical examination,or laboratory findings of a general medical condition judged to be etiologically related to the disturbance
6 Subtypes of Delirium Delirium is a disturbance of arousal and cognition. Subtypes of delirium are based on the type of arousal disturbance: Hyperactive Hypoactive Mixed
7 Subtypes of Delirium In 12 studies, the prevalence of each of the subtypes of delirium has varied widely A meta-analysis of these studies suggest the following average prevalence for each subtype: Hypoactive: 48% (ranges: 15-71%) Hyperactive: 24% (ranges: 13-46%) Mixed: 36% (ranges: 11-55%)
8 Hypoactive Delirium: Controversies and Barriers to Treatment Hypoactive Delirium is thought to be very rare, but in fact accounts for an average of 50% of delirium cases Hypoactive Delirium is thought not to cause morbidity and therefore does not require pharmacologic intervention. Hypoactive Delirium, because of its phenomenologic differences with Hyperactive Delirium, is thought not to respond to pharmacologic interventions with neuroleptics
9 The Delirium Experience William Breitbart,M.D. Christopher Gibson, PhD. Annie Tremblay, M.D. Memorial Sloan-Kettering Cancer Center Breitbart et al, Psychosomatics, 2002
10 Objectives To describe the experience of delirium in hospitalized cancer patients. To examine the level of distress related to the delirium experience in cancer patients, their spouses/caregivers, and nurses. To examine the relationships among delirium-related distress, delirium phenomenology, etiology, demographic and medical variables.
11 Delirium Experience Questionnaire Do you remember being confused? Yes No If no, are you distressed that you can t remember? Yes_ No_ How distressed? 0-4 numerical rating scale (NRS) If yes, was the experience distressing? Yes No How distressing? 0-4 NRS Can you describe the experience? Spouse /Caregiver: How distressed were you during the patient s delirium? 0-4 NRS Nurse: Your patient was confused. Did you find it distressing? 0-4 NRS 0-4NRS: 0: not at all, 4: extremely
12 Sample Characteristics (n= 101) Mean Age: years (SD= 16.6) Gender: Males= 52; Females= 49 Race: White= 67%; Black= 21%; Hispanic= 9%; Other=3% Cancer Diagnoses: Lung-21%, GI-14%,Lymphoma-13% Breast-11%, Head and Neck-6%, Ovarian-4%, Brain-3%, Other cancers- 28% Stage: Localized=16%, Metastatic=79%, Terminal=5% Brain Metastases: 24%; History of Dementia: 18% Karnofsky: Mean= 35.5 (SD=7.7)
13 Sample Characteristics (n= 101) Memorial Delirium Assessment Scale (MDAS): Mean MDAS = 19 (SD 3.2), range Delirium Subtypes: Hypoactive= 53%; Hyperactive=47% Delirium Etiologies: Multiple causes= 74%; Single cause= 26% Delirium Etiologies encountered: Opioids-65%, infection-39% steroids-30%, hypoxia-26%, dehydration-12%, CNS-12%, Other-13%
14 Results 53.5% of patients (N=54) who recovered from delirium remember being delirious. 93% of patients who remember being delirious report the experience as being distressing. Mean level of patient distress (0-4 NRS)= 3.22 (SD=.86) Mean level of Spouse/Caregiver distress= 3.75 (SD=.47) Mean level of Nurse distress= 3.09 (SD=.77)
15 Logistic Regression Analysis of Predictors of Delirium Recall in Patients Variable P OR Short-term Memory Impairment MDAS Total Score Perceptual Disturbance OR = Odds Ratio
16 Percentage of Patients with Delirium Recall Based Upon Delirium Severity Severe Moderate Mild % of Patients with Delirium Recall
17 Logistic Regression Analysis of Predictors of Patient, Spouse/Caregiver, and Nurse Distress Variable P OR Patient Distress Delusions Spouse/Caregiver Distress Karnofsky (KPS) Nurse Distress MDAS Total Score Perceptual disturbances OR = Odds Ratio
18 Distress in Hyperactive vs Hypoactive Delirium There were no significant differences in the report of distress for patients, or nurses based on subtype of delirium. Spouses/caregivers were more distressed by hypoactive delirium. Hypoactive delirium was equally as distressing as Hyperactive delirium for patients, nurses.
19 Summary: Delirium Experience Delirium is a highly distressing experience for patients, spouses/ caregivers and nurses Delirium is especially distressing when delirium is more severe and is characterized by the presence of delusions and hallucinations Hypoactive delirium is as distressing as hyperactive delirium Delirium is important to treat because it is associated with significant suffering not only in patients, but also in spouses/caregivers and staff
20 Delirium Assessment Methods Diagnostic classification systems DSM-III, DSM-III-R, DSM-IV ICD-9, ICD-10 Diagnostic interview instruments Delirium symptom interview (DS) Confusion Assessment Method (CAM) Delirium rating scales Delirium Rating Scale (DRS) Confusion Rating Scale (CRS) Memorial Delirium Assessment Scale (MDAS) Cognitive impairment screening scales Mini-Mental State Exam (MMSE) Short Portable Mental Status Questionnaire (SPMSQ) Cognitive Capacity Screening Examination Test (BOMC)
21 Memorial Delirium Assessment Scale (MDAS) REDUCED LEVEL OF CONSCIOUSNESS (AWARENESS) DISORIENTATION SHORT-TERM MEMORY IMPAIRMENT IMPAIRED DIGIT SPAN REDUCED ABILITY TO MAINTAIN AND SHIFT ATTENTION DISORGANIZED THINKING PERCEPTUAL DISTURBANCE DELUSIONS DECREASED OR INCREASED PSYCHOMOTOR SLEEP-WAKE CYCLE DISTURBANCE (DISORDER OF AROUSAL Breitbart, et al, JPSM, 1996
22 Validation of the Memorial Delirium Assessment Scale in the Terminally Ill The MDAS is a 10 item delirium severity and diagnostic instrument designed for repeated assessment and treatment evaluation Two validation studies have been conducted to date using large samples of hospitalized cancer and AIDS patients as well as cancer patients admitted to a palliative care unit The MDAS is highly correlated with other diagnostic measures of delirium (e.g. the DRS) and cognition (e.g. the MMSE) Diagnostic cut-off scores of 13/30 in hospitalized cancer patients, and 7/30 in PCU patients have been suggested Prorating item scores is necessary in up to 20% of patients Breitbart,W, et al 1996; Lawlor, P, et al 2000
23 Overview of Delirium Management DELIRIUM TREATMENT OUTCOME Pre Terminal Delirium Terminal Delirium Aimed at reversing etiology Aimed at controlling symptomatology Delirium is reversible Delirium is irreversible
24 Assessment of Etiologies of Delirium in Advanced Cancer Patients Unclear or never discovered in over 50% of patients Three or more etiologies usually present Irreversible 30-40% of the time, especially in the terminally ill Etiology found in 40% - 50% of cases 30% - 70% improve with treatment of etiology
25 Assessment of Etiologies of Delirium in the Advanced Cancer Patient (cont d) Diagnostic work-up must be consistent with the goals of care minimally invasive in the terminally ill treatments are effective and/or minimally burdensome or distressing
26 Causes of Delirium in Advanced Cancer Direct Primary brain tumor Metastatic spread Indirect Hypoxia Metabolic encephalopathy due to organ failure Electrolyte imbalance Withdrawal states
27 Causes of Delirium in Cancer Patients (cont d) Indirect (cont d) Treatment side effects from Chemotherapeutic agents, steroids, biological response modifiers Radiation Opioids Anticholinergics Antiemetics Infection Hematologic abnormalities Nutritional deficiencies Paraneoplastic syndromes
28 Non-Pharmacological Interventions for Delirium in the Advanced Cancer Patient 1. Provide safe and supportive environment for patient, staff, and family 2. Reassure family of the medical nature of delirium Their family member is not having a nervous breakdown 3. Depending on stage of disease, either reassure family of transient nature of delirium or describe as a hallmark of approaching death
29 Non-Pharmacological Interventions for Delirium in Advanced Cancer (cont d) 4. Provide proper sensory environment for patient quiet, well-lit room visible clock, calendar familiar people, objects 5. Communicate with patient and family goals of care and desirable outcomes, i.e., sedation vs. awake but agitated regarding hallucinations and their management or meaning
30 Pharmacological Management of Delirium Approximate daily Generic Name dosage range (mg) Route Neuroleptics Haloperidol q2-12h PO, IV, SC, IM Thioridazine q4-8h PO Chlorpromazine q4-12h PO, IV, IM Methotrimeprazine q4-8h IV, SC, PO Droperidol q12h IM, IV Molindone q8-12h PO
31 Pharmacological Management of Delirium Approximate daily Generic Name dosage range (mg) Route Atypical Antipsychotics Risperidone 1-3 q12h PO Olanzapine q12h PO/IM Quetiapine q12h PO Ziprasidone q12h PO/IM Aripiprazolee qd PO
32 Side Effects of Neuroleptics/Antipsychotics Anticholinergic Dry Mouth Constipation Cardiovascular (BP, QT interval) Antihistaminic Sedation, Weight Gain Dopamine Blocade Extrapyramidal Side Effects Hyperprolctinemia Neuroleptic Malignant Syndrome
33 Side Effects of Atypical Antipsychotics Metabolic Syndrome Hyperglycemia Hyperlipidemia Weight Gain Olanzapine and Clozapine have highest incidence QT Interval Prolongation Torsade des Pointes QTc prolongation beyond 500msec ECG should be monitored daily during delirium RX Consider interactions with other agents that prolong QT
34 Side Effects of Haloperidol vs. Risperidone vs. Olanzapine Side Effect Haloperidol Risperidone Olanzapine EPS >30% >10% >2% ACHE >2% >2% >10% Sedation >2% >10% >30% Hypotension >2% >30% >2% Seizure >2% >2% >2% Bezchlibnyk-Butler & Jeffries, 1999
35 Neurotransmitter/Receptor Effects of Antipsychotics α1 5HT2A α1 α2 5HT2A M1 H1 α1 haloperidol risperidone 5HT2C 5HT3 olanzapine D1 D2 5HT7 D2 5HT6 D4 D3 D2
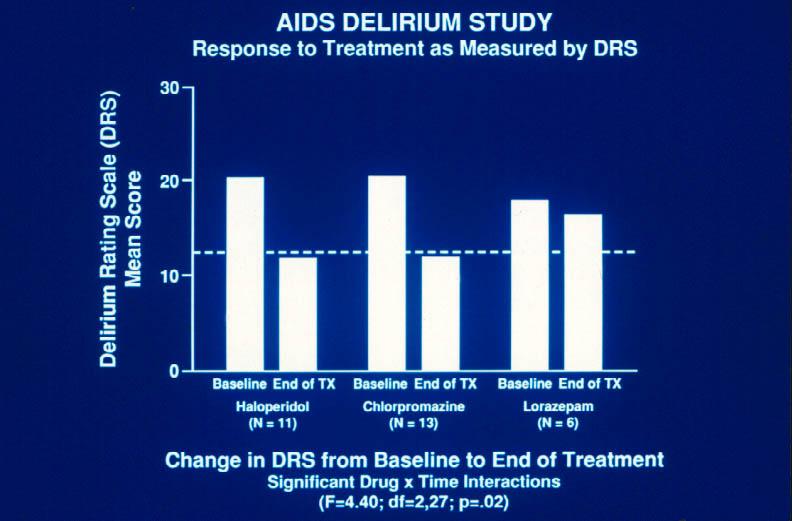
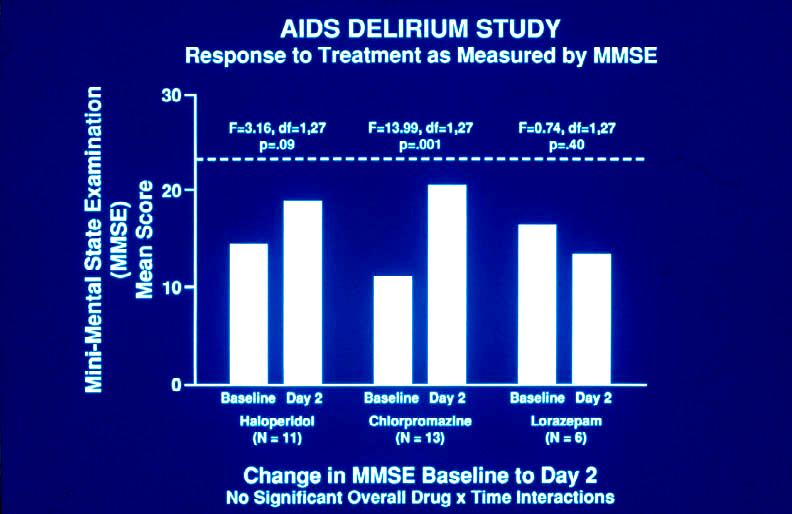
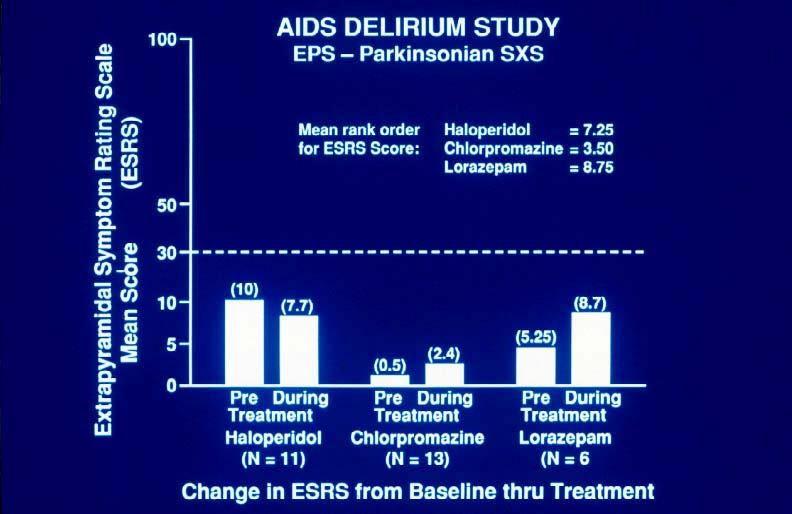
36 Clinical Trials of Delirium Management A double-blind, randomized trial of Haloperidol vs. Chlorpromazine vs. Lorazepam in the treatment of delirium in medically hospitalized AIDS patients with AIDS-related cancers (N=244 screened, 30 on trial.) Results: Both Haloperidol and Chlorpromazine were effective in rapidly resolving the symptoms of delirium utilizing low dosage regimens Lorazepam alone was ineffective No clinically significant side effects Both hypoactive and hyperactive delirium responded to neuroleptics Breitbart et al Am J Psy 1996
37 AIDS Delirium Study Dose Haloperidol Chlorpromazine Lorazepam mg 10 mg 0.5 mg mg 20 mg 1.0 mg mg 40 mg 1.5 mg mg 80 mg 2.0 mg mg 100 mg 2.5 mg mg 100 mg 2.5 mg mg 100 mg 2.5 mg mg 200 mg 4.0 mg mg 200 mg 4.0 mg Max mg 850 mg 20.5 mg All doses PO; Dose IM = 1/2 PO
38
39
40
41
42 AIDS Delirium Study Drug Dosages 1st 24 hours Haloperidol Chlorpromazine Lorazepam mean dose 2.6 mg median dose 1.75 mg range mg mean dose 100 mg median dose 70 mg range mg mean dose 6.9 mg median dose 3.0 mg range mg
43 AIDS Delirium Study Drug Dosages Maintenance Dose Days 2-7 Haloperidol mean dose 1.6 mg median dose 1.0 mg range mg Chlorpromazine Lorazepam mean dose 40 mg median dose 35 mg range mg mean dose 1.5 mg median dose 1.25 mg range mg
44 Neuroleptics for Hypoactive Delirium Both Haloperidol and Chlorpromazine were effective in improving the symptoms of delirium (as measured by the DRS) for both hyperactive (N=9), F=19.06, df=1.18, p<0.001, as well as hypoactive delirium(n=11), F=21.15, df=1.18, p<0.001
45 An Open Trial of Olanzapine for the Treatment of Delirium in Hospitalized Cancer Patients William Breitbart,M.D. Annie Tremblay, M.D. Christopher Gibson, Ph.D. Memorial Sloan-Kettering Cancer Center
46 Efficacy of Olanzapine in the Treatment of Delirium MDAS Score Baseline Time 1 Time 2 t (baseline-time3) = 10.1, p <.001
47 Results- Olanzapine Efficacy Two MDAS cut-off scores were utilized to define delirium resolution: MDAS below 13 at T3: 78.7% improved on olanzapine MDAS below 10 at T3: 73.3% improved on olanzapine
48 Logistic Regression Analysis of Predictors to Olanzapine Treatment Variable P OR Age: CNS Spread Subtype of Delirium Hypoxia History of Dementia Delirium Severity OR = Odds Ratio
49 Effect of Age on Olanzapine Response Percent of Patients w/ MDAS < % 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Under Over 70 X 2 = 22.8 p <.001
50 Efficacy of Olanzapine in Hypoactive and Hyperactive Delirium MDAS Score Baseline Time 1 Time 2 Hypoactive Hyperactive F= 9.51 p <.003
51 Olanzapine Dosage Mean olanzapine dosage: Baseline : T2 (day2-3): T3 (day4-7): 3.0 mgs (SD=0.14) range = 2.5 to 10 mgs 4.6 mgs (SD=0.27) range = 2.5 to 15 mgs 6.3 mgs (SD=0.52) range = 2.5 to 20 mgs
52 Olanzapine Side Effects Olanzapine side effects were common but rarely interfered with treatment or worsened delirium: Side Effect T2% T3% Sedation 29% 29% EPS 0% 0% Delirium 1.2% 1.2% Other 3.7% ----
53 Clinical Trial of Risperidone for Delirium A double-blind, randomized trial of Risperidone vs. Haloperidal in the treatment of delirium in 24 medically hospitalized cancer patients: Results: Both Risperidone and Haloperidol were equally effective in resolving the symptoms of delirium utilizing low dosage regimens No significant difference in side effects Analysis and reporting of response rates, dosage regimens and side effects is insufficient, thus limiting the value of this trial Han and Kim, Psychosomatics, 2004
54 Pharmacological Management of Delirium Approximate daily Generic Name dosage range (mg) Route Neuroleptics Haloperidol q2-12h PO, IV, SC, IM Thioridazine q4-8h PO Chlorpromazine q4-12h PO, IV, IM Methotrimeprazine q4-8h IV, SC, PO Droperidol q12h IM, IV Molindone q8-12h PO Novel Antipsychotics Risperidone 1-3 q12h PO Olanzapine q12h PO/IM
55 Pharmacological Management of Delirium (cont d) Approximate daily Generic Name dosage range (mg) Route Benzodiazepines Lorazepam q1-4h PO, IV, IM Midazolam per 24h IV, SC Anesthetics Propofol q1h IV
56 Pharmacological Management of Delirium Symptoms Delirium Diagnosed Identify and Treat Etiology Assess safety and assure safe environment Hyperactive agitated delirium Add lorazepam 0.5-2mg IV q4h for increased sedation Haloperidol IV/PO 2-10mg q4-12h & prn for agitation Add benztropine 0.5-1mg IV (po tid) for EPS Switch to chlorpromazine 25-50mg IV q4-12h for increased sedation Adjust dosage for optimal control of symptoms Continue indefinitely or until etiology is reversed and taper off slowly Switch to olanzapine if regimen not tolerated or if EPS is an issue
57 Pharmacological Management of Delirium Symptoms Delirium Diagnosed Identify and Treat Etiology Hypoactive Delirium Haloperidol PO/IV mg q4-12h & prn for hallucinations/agitation Add benztropine 0.5-1mg IV (po tid) for EPS Assess safety and assure safe environment Reduce dose if sedated Continue indefinitely or until etiology is reversed and taper off slowly Use olanzapine 2.5-5mg PO bid if EPS is an increasing concern
58 Conclusions Delirium is a common neuropsychiatric complication in terminal cancer Psychiatrists must be familiar with the proper assessment, diagnosis, and management of delirium Appropriate management of delirium is important to minimize morbidity and improve quality of care


59 The HANDBOOK OF PSYCHIATRY IN PALLIATIVE MEDICINE Edited by Harvey M. Chochinov and William Breitbart To order: The Handbook of Psychiatry in Palliative Medicine Please contact: Order Department, Oxford University Press 2001 Evans Road Cary, NC Tel: ; Fax: Website: $75.00, ISBN:
60 New Journal Palliative & Supportive Care William Breitbart, M.D. Editor-in-Chief Memorial Sloan-Kettering Cancer Center New York, NY For Information:
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium. Dr. Lesley Wiesenfeld. Deputy Psychiatrist in Chief, Mount Sinai Hospital. Dr. Carole Cohen
 Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium Dr. Lesley Wiesenfeld Deputy Psychiatrist in Chief, Mount Sinai Hospital Dr. Carole Cohen Department of Psychiatry, University of Toronto and Sunnybrook Health Sciences Centre Case Study Mrs B
Delirium. Approach. Symptom Update Masterclass:
 Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Symptom Update Masterclass: Delirium Jason Boland Senior Clinical Lecturer and Honorary Consultant in Palliative Medicine Wolfson Centre for Palliative Care Research Hull York Medical School University
Interprofessional Webinar Series
 Interprofessional Webinar Series Assessment and Management of Delirium Pauline Lesage, MD, LLM Physician Educator MJHS Institute for Innovation in Palliative Care Disclosure Slide Pauline Lesage, MD, LLM,
Interprofessional Webinar Series Assessment and Management of Delirium Pauline Lesage, MD, LLM Physician Educator MJHS Institute for Innovation in Palliative Care Disclosure Slide Pauline Lesage, MD, LLM,
BRAIN. Tumor byproducts. Autonomic nerves. Somatic nerves. Host immune cells. Cytokines
 Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Patient s Problems Pain (80%) Fatigue (90%) Weight Loss (80%) Lack of Appetite (80%) Nausea, Vomiting (90%) Anxiety (25%) Shortness of Breath (50%) Confusion-Agitation (80%) Tumor Mass Tumor Function Somatic
Delirium. A Plan to Reduce Use of Restraints. David Wensel DO, FAAHPM Medical Director Midland Care
 Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Delirium A Plan to Reduce Use of Restraints David Wensel DO, FAAHPM Medical Director Midland Care Objectives Define delirium Describe pathophysiology of delirium Understand most common etiologies Define
Learning Objectives. Delirium. Delirium. Delirium. Terminal Restlessness 3/28/2016
 Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Terminal Restlessness Dr. Christopher Churchill St. Cloud VA Health Care System EC&R Service Line Director & Medical Director Hospice & Palliative Care March 31, 2016 Learning Objectives Different Terminology
Home Care and Hospice Association of New Jersey Annual Conference 2017
 Home Care and Hospice Association of New Jersey Annual Conference 2017 I D E N T I F I C A T I O N A N D M A N A G E M E N T O F D E L I R I U M E L I Z A B E T H M A G E R - O C O N N O R A C H P N DR
Home Care and Hospice Association of New Jersey Annual Conference 2017 I D E N T I F I C A T I O N A N D M A N A G E M E N T O F D E L I R I U M E L I Z A B E T H M A G E R - O C O N N O R A C H P N DR
Management of Delirium in Hospice Patients
 Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Presentation Objectives Management of Delirium in Hospice Patients Lynn Williams, BSPharm Clinical Pharmacist Hospice Pharmacy Solutions Identify the clinical features of delirium Understand the underlying
Symptom Management Pocket Guides: DELIRIUM
 Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
Symptom Management Pocket Guides: DELIRIUM August 2010 DELIRIUM Page Considerations. 1 Assessment 2 Diagnosis. 3 Non-Pharmacological treatment 3 Pharmacological treatment. 5 Mild Delirium... 6 Moderate
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya
 DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
DIAH MUSTIKA HW SpS,KIC Intensive Care Unit of Emergency Department Naval Hospital dr RAMELAN, Surabaya Encephalopathy is a common complication of systemic illness or direct brain injury. Acute confusional
g Prevention, Diagnosis, and Management in Palliative Care
 8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
8/3/2012 Improving p g Prevention, Diagnosis, g and Management in Palliative Care MN Rural Palliative Care Networking Group Quarterly Education Session June 27,2012 Sandra W. Gordon-Kolb, MD, MMM, CPE
Delirium in Hospital Care
 Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
Delirium in Hospital Care Dr John Puxty 1 Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors,
( delirium ) 15%- ( extrapyramidal syndrome ) risperidone olanzapine ( extrapyramidal side effect ) olanzapine ( Delirium Rating Scale, DRS )
 15%- ( extrapyramidal syndrome ) risperidone olanzapine ( extrapyramidal side effect ) olanzapine ( Delirium Rating Scale, DRS )") 2005 6 48-52 Olanzapine 30% ( delirium 5%- Haloperidol ( extrapyramidal syndrome risperidone ( extrapyramidal side effect ( Delirium Rating Scale, DRS ( Delirium ( Olanzapine ( Delirium Rating Scale, DRS
2005 6 48-52 Olanzapine 30% ( delirium 5%- Haloperidol ( extrapyramidal syndrome risperidone ( extrapyramidal side effect ( Delirium Rating Scale, DRS ( Delirium ( Olanzapine ( Delirium Rating Scale, DRS
Delirium. Delirium. Delirium Etiology and Pathophysiology. Fall 2018
 Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Three most common cognitive problems in adults 1. (acute confusion) 2. Dementia 3. Depression These problems often occur together Can you think of common stimuli for each? 1 1 State of temporary but acute
Delirium. Dr. John Puxty
 Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium Dr. John Puxty Learning Objectives By the end of the workshop participants will be able to: Appreciate the main diagnostic criteria for delirium. Describe common risk factors, causes and main
Delirium in the ICU: Prevention and Treatment. Delirium Defined Officially. Delirium: Really Defined. S. Andrew Josephson, MD
 Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Delirium in the ICU: Prevention and Treatment S. Andrew Josephson, MD Director, Neurohospitalist Service Medical Director, Inpatient Neurology June 2, 2011 Delirium Defined Officially (DSM-IV-TR) criteria
Evidence-Based Treatment of Delirium in Patients With Cancer William Breitbart and Yesne Alici
 Published Ahead of Print on March 12, 2012 as 10.1200/JCO.2011.39.8784 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2011.39.8784 JOURNAL OF CLINICAL ONCOLOGY R E V I E W A R T I
Published Ahead of Print on March 12, 2012 as 10.1200/JCO.2011.39.8784 The latest version is at http://jco.ascopubs.org/cgi/doi/10.1200/jco.2011.39.8784 JOURNAL OF CLINICAL ONCOLOGY R E V I E W A R T I
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
DELIRIUM. Approach and Management
 DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
DELIRIUM Approach and Management By Dr. K.S. Jacob, Professor of Psychiatry and Dr. Anju Kuruvilla, Professor of Psychiatry, Christian Medical College, Vellore. Based on a chapter in the book Psychiatric
Delirium in the Elderly
 Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
Delirium in the Elderly ELITE 2017 Liza Genao, MD Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity Very much under-recognized
ICU Delirium in Infants & Children: Cause for Concern or False Alarm. Objectives
 ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
ICU Delirium in Infants & Children: Cause for Concern or False Alarm Peter (Pete) N. Johnson, Pharm.D., BCPS, BCPPS, FPPAG Associate Professor of Pharmacy Practice University of Oklahoma College of Pharmacy
Delirium in the Elderly
 Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Delirium in the Elderly Jeffrey M. Burock, MD Division Director/ Psychiatry / Miriam Hospital Clinical Assistant Professor Warren Alpert School Of Medicine Learning Objectives Identify the symptoms of
Palliative Care and Delirium. Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care
 Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Palliative Care and Delirium Ambereen K. Mehta, MD MPH Assistant Professor Division of General Medicine, Geriatrics, and Palliative Care Disclosures I have no personal or professional financial relationships
Delirium in the Elderly
 Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium in the Elderly ELITE 2015 Mamata Yanamadala M.B.B.S, MS Division of Geriatrics Why should we care about delirium? It is: common associated with high mortality associated with increased morbidity
Delirium and Dementia. Summary
 Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Delirium and Dementia Paul Kettl, M.D., M.H.A. Summary DELIRIUM Acute brain failure Identify cause (meds, infection) Treat sx Poor prognostic sign DEMENTIA Chronic brain failure AD most common cause Often
Drug induced delirium
 Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Drug induced delirium Knut Erik Hovda, MD, PhD, FACMT, FEAPCCT The Norwegian CBRNe Centre of Medicine Department of Acute Medicine Oslo University hospital Content 1. Introduction 2. Risk factors 3. Prevalence
Delirium in Older Persons
 Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives Delirium in Older Persons ELITE 2018 Liza Isabel Genao, MD Division of Geriatrics Describe rate, cost, complications of delirium Effectively diagnose the syndrome Describe multicomponent model
Objectives. Delirium in the Elderly Patient. Disclosure. Arizona Geriatrics Society Fall Symposium 2010
 Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium in the Elderly Patient Sandra Jacobson, MD Banner Sun Health Research Institute Arizona Geriatrics Society Fall Symposium 2010 Disclosure Dr. Jacobson has disclosed that she does not have any
Delirium: A Condition of All Ages. Delirium, also known as acute confusional state, Definition. Epidemiology
 Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Focus on CME at the University of Calgary : A Condition of All Ages While delirium can strike at any age, physicians need to be particularly watchful for it in elderly patients, so that a search for the
Confusion in the acute setting Dr Susan Shenkin
 Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Confusion in the acute setting Dr Susan Shenkin Susan.Shenkin@ed.ac.uk 4 th International Conference, Society for Acute Medicine, Edinburgh 7-8 October 2010 Summary Confusion is not a diagnosis Main differentials
Delirium Monograph - Update, Spring 2014
 Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
3/27/2013. Objectives. Psychopharmacology at the End of Life Nicole Thurston, MD
 Psychopharmacology at the End of Life Nicole Thurston, MD Psychiatrist Mountain States Tumor Institute Objectives Describe 2 common psychiatric symptoms that can present at or near end of life. Review
Psychopharmacology at the End of Life Nicole Thurston, MD Psychiatrist Mountain States Tumor Institute Objectives Describe 2 common psychiatric symptoms that can present at or near end of life. Review
Delirium. Quick reference guide. Issue date: July Diagnosis, prevention and management
 Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Issue date: July 2010 Delirium Diagnosis, prevention and management Developed by the National Clinical Guideline Centre for Acute and Chronic Conditions About this booklet This is a quick reference guide
Chapter 161 Antipsychotics
 Chapter 161 Antipsychotics Episode Overview Extrapyramidal syndromes are a common complication of antipsychotic medications. First line treatment is benztropine or diphenhydramine. Lorazepam is used in
Chapter 161 Antipsychotics Episode Overview Extrapyramidal syndromes are a common complication of antipsychotic medications. First line treatment is benztropine or diphenhydramine. Lorazepam is used in
譫妄症 (Delirium) Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28
 Objectives. Epidemiology. Delirium. DSM-5 Diagnostic Criteria. Prognosis 台大醫院老年醫學部陳人豪 2016/8/28") 譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
譫妄症 (Delirium) 台大醫院老年醫學部陳人豪 2016/8/28 Objectives Delirium Epidemiology Etiology Diagnosis Evaluation and Management Postoperative delirium Delirium (and acute problematic behavior) in the longterm care
Acute vs. Maintenance
 Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Delirium. Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta
 Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Delirium Geriatric Giants Lecture Series Divisions of Geriatric Medicine and Care of the Elderly University of Alberta Overview A. Delirium - the nature of the beast B. Significance of delirium C. An approach
Cambridge University Press Effective Treatments in Psychiatry Peter Tyrer and Kenneth R. Silk Excerpt More information
 Organic disorders 1 Delirium Based on Delirium by Laura Gage and David K. Conn in Effective Treatments in Psychiatry, Cambridge University Press, 2008 Introduction Delirium needs treatment for both its
Organic disorders 1 Delirium Based on Delirium by Laura Gage and David K. Conn in Effective Treatments in Psychiatry, Cambridge University Press, 2008 Introduction Delirium needs treatment for both its
5 older patients become delirious every minute
 Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Management of Delirium: Nonpharmacologic and Pharmacologic Approaches Sharon K. Inouye, M.D., M.P.H. Professor of Medicine Beth Israel Deaconess Medical Center Harvard Medical School Milton and Shirley
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR
 Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Delirium Screening Tools: Just- In- Time Education and Evaluation Using the EMR Implementation of an EMR based protocol for detection of delirium in elderly Medical and palliative care patients Parul Goyal,
Behavior Management in Children with Cancer
 Behavior Management in Children with Cancer Anna (Nina) Muriel, MD, MPH Chief, Division of Pediatric Psychosocial Oncology Department of Psychosocial Oncology and Palliative Care Behavior matters Behavior
Behavior Management in Children with Cancer Anna (Nina) Muriel, MD, MPH Chief, Division of Pediatric Psychosocial Oncology Department of Psychosocial Oncology and Palliative Care Behavior matters Behavior
Delirium and Nausea. Delirium - definition. Delirium Incidence. Predisposing Risk Factors for Delirium. Impact. Delirium Types 10/14/2016
 Delirium - definition Delirium and Nausea Etiologically non-specific global cerebral dysfunction associated with changes in LOC, attention, thinking, perception, memory, psychomotor behavior, emotion and
Delirium - definition Delirium and Nausea Etiologically non-specific global cerebral dysfunction associated with changes in LOC, attention, thinking, perception, memory, psychomotor behavior, emotion and
GUIDELINES FOR THE MANAGEMENT OF DELIRIUM IN ADVANCED CANCER
 GUIDELINES FOR THE MANAGEMENT OF DELIRIUM IN ADVANCED CANCER 14.1 GENERAL PRINCIPLES Delirium can be defined as: A transient organic brain syndrome characterised by the acute onset of disordered arousal
GUIDELINES FOR THE MANAGEMENT OF DELIRIUM IN ADVANCED CANCER 14.1 GENERAL PRINCIPLES Delirium can be defined as: A transient organic brain syndrome characterised by the acute onset of disordered arousal
Acute cognitive failure and delirium: screening
 Acute cognitive failure and delirium: screening instruments for research and clinical practice Augusto Caraceni Director Palliative Care, Pain therapy and rehabilitation Fondazione IRCCS National Cancer
Acute cognitive failure and delirium: screening instruments for research and clinical practice Augusto Caraceni Director Palliative Care, Pain therapy and rehabilitation Fondazione IRCCS National Cancer
For more information about how to cite these materials visit
 Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Rachel Glick, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Noncommercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
NIH Public Access Author Manuscript Cancer. Author manuscript; available in PMC 2009 September 28.
 NIH Public Access Author Manuscript Published in final edited form as: Cancer. 2009 May 1; 115(9): 2004 2012. doi:10.1002/cncr.24215. The impact of delirium and recall on the level of distress in patients
NIH Public Access Author Manuscript Published in final edited form as: Cancer. 2009 May 1; 115(9): 2004 2012. doi:10.1002/cncr.24215. The impact of delirium and recall on the level of distress in patients
The Agitated. Older Patient: old. What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003
 Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Focus on CME at Queen s University Focus on CME at Queen s University The Agitated The Older Patient: What To Do? Michelle Gibson, MD, CCFP Presented at Brockville General Hospital Rounds, May 2003 Both
Delirium in the Emergency Department. Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte
 Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium in the Emergency Department Emergency Medicine Rounds April 14, 2015 Paul R. Vanhoutte Goals of Rounds: Review Definition Management An Understanding What is important is to spread confusion,
Delirium in the hospitalized patient
 Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
Delirium in the hospitalized patient Jennifer A. Tarin, M.D. Department of Hospital Medicine Geriatric Health Safety Chair Colorado Permanente Medical Group UCLA Reynolds Scholar Delirium Preventing delirium
TREATING DELIRIUM A QUICK REFERENCE GUIDE FOR PSYCHIATRISTS
 TREATING DELIRIUM A QUICK REFERENCE GUIDE FOR PSYCHIATRISTS T he Quick Reference Guide for the treatment of delirium is a summary and synopsis of the American Psychiatric Association s Practice Guideline
TREATING DELIRIUM A QUICK REFERENCE GUIDE FOR PSYCHIATRISTS T he Quick Reference Guide for the treatment of delirium is a summary and synopsis of the American Psychiatric Association s Practice Guideline
Chapter 01 Introduction
 Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Chapter 01 Introduction Defining the Elderly There is no universally accepted age cut-off defining elderly. This reflects the fact that chronological age itself is less important than biological events
Care of the Acutely Agitated Patient. Objectives. Agitation Defined
 Care of the Acutely Agitated Patient James C. Hardy, MD Assistant Professor of Emergency Medicine Department of Emergency Medicine, UCSF Dealing with combative patients is one of the most difficult challenges
Care of the Acutely Agitated Patient James C. Hardy, MD Assistant Professor of Emergency Medicine Department of Emergency Medicine, UCSF Dealing with combative patients is one of the most difficult challenges
Improving Delirium Management: Mapping Out One Unit s Journey. Geriatrics Institute June 27, 2013
 Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Improving Delirium Management: Mapping Out One Unit s Journey Geriatrics Institute June 27, 2013 Rebecca Ramsden, NP Mary Ann Hamelin, CNS Susanne Loay, RN Objectives Background RNAO Best Practice Guideline
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Delirium in Palliative Care. Case Studies 2015
 Delirium in Palliative Care Case Studies 2015 Case 1 - Alex 35 yo M with metastatic melanoma Decreased LOC, unilateral hearing loss and bilateral vision loss, back pain, lower extremity weakness,? confusion/hallucinations
Delirium in Palliative Care Case Studies 2015 Case 1 - Alex 35 yo M with metastatic melanoma Decreased LOC, unilateral hearing loss and bilateral vision loss, back pain, lower extremity weakness,? confusion/hallucinations
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative
 Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Summary of Delirium Clinical Practice Guideline Recommendations Post Operative Intensive Care Unit Clinical Practice Guideline for Postoperative Clinical Practice Guidelines for the Delirium in Older Adults;
Antipsychotic Medications
 TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
TRAIL: Team Review of EVIDENCE REVIEW & RECOMMENDATIONS FOR LTC Behavioural and psychological symptoms of dementia (BPSD) refer to the non-cognitive symptoms of disturbed perception, thought content, mood
Cognitive disorders. Dr S. Mashaphu Department of Psychiatry
 Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Cognitive disorders Dr S. Mashaphu Department of Psychiatry Delirium Syndrome characterised by: Disturbance of consciousness Impaired attention Change in cognition Develops over hours-days Fluctuates during
Delirium. A Geriatric Syndrome. Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine
 Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
Delirium A Geriatric Syndrome Jonathan McCaleb, MD, CMD, HMDC UNSOM, Assistant Professor of Medicine Geriatrics / Hospice & Palliative Medicine Introduction Common Serious Unrecognized: a medical emergency
HHS Public Access Author manuscript Curr Opin Support Palliat Care. Author manuscript; available in PMC 2017 December 01.
 Neuroleptics in the Management of Delirium in Patients with Advanced Cancer David Hui, MD, MSc, Rony Dev, MD and Eduardo Bruera, MD Department of Palliative Care and Rehabilitation Medicine, MD Anderson
Neuroleptics in the Management of Delirium in Patients with Advanced Cancer David Hui, MD, MSc, Rony Dev, MD and Eduardo Bruera, MD Department of Palliative Care and Rehabilitation Medicine, MD Anderson
POST STROKE DELIRIUM. Dr Janet Ballantyne
 POST STROKE DELIRIUM Dr Janet Ballantyne Delirium de: away from/off lira: ridge between ploughed farrows/tracks off the tracks Acute confusional state Acute brain syndrome Acute brain failure Metabolic
POST STROKE DELIRIUM Dr Janet Ballantyne Delirium de: away from/off lira: ridge between ploughed farrows/tracks off the tracks Acute confusional state Acute brain syndrome Acute brain failure Metabolic
Objectives. Epidemiology. Diagnosis 3/27/2013. Identify positive and negative symptoms used for diagnosis of schizophrenia
 Objectives Identify positive and negative symptoms used for diagnosis of schizophrenia Mohamed Sallout, Pharm D. Pharmacist Resident St. Luke s Magic Valley Regional Medical Center List medications used
Objectives Identify positive and negative symptoms used for diagnosis of schizophrenia Mohamed Sallout, Pharm D. Pharmacist Resident St. Luke s Magic Valley Regional Medical Center List medications used
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist. HMS Training Webinar January 27, 2017
 Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Debra Brown, PharmD, FASCP Pharmaceutical Consultant II Specialist HMS Training Webinar January 27, 2017 1 Describe nationwide prevalence and types of elderly dementia + define BPSD Define psychotropic
Haloperidol and risperidone in the treatment of delirium and its subtypes
 Eur. J. Psychiat. Vol. 25, N. 2, (59-67) 2011 Keywords: Delirium; Treatment; Haloperidol; Risperidone; Antipsychotics. Haloperidol and risperidone in the treatment of delirium and its subtypes Soenke Boettger*
Eur. J. Psychiat. Vol. 25, N. 2, (59-67) 2011 Keywords: Delirium; Treatment; Haloperidol; Risperidone; Antipsychotics. Haloperidol and risperidone in the treatment of delirium and its subtypes Soenke Boettger*
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach
 Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
Decreasing Delirium Resolution Times for the Elderly: An Interprofessional Approach Featuring: Felice Rogers Evans BSN RN BC Ty Breiter MSN RN CNL Tampa General Hospital NICHE exemplar hospital Three time
OPIOID- INDUCED NEUROTOXICITY*
 OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
OPIOID- INDUCED NEUROTOXICITY* Sriram Yennu MD, MS, FAAHPM Palliative Care, Rehabilitation and Integrative Medicine U.T. M.D. Anderson Cancer Center *Slide Deck courtesy Dept PRIM MDACC PATIENT #1: MRS
Medication Audit Checklist- Antipsychotics - Atypical
 Medication Audit checklist Page 1 of 7 10-2018 Audit number: Client number: Ordering Provider: INDICATIONS 1) Disorders with psychotic symptoms (schizophrenia, schizoaffective disorder, manic disorders,
Medication Audit checklist Page 1 of 7 10-2018 Audit number: Client number: Ordering Provider: INDICATIONS 1) Disorders with psychotic symptoms (schizophrenia, schizoaffective disorder, manic disorders,
Delirium. Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning.
 and fluctuating course of deterioration in mental functioning.") Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
Delirium Delirium is characterized by an acute onset (hours or days) and fluctuating course of deterioration in mental functioning. DELIRIUM IS A MEDICAL EMERGENCY! Delirium: Hallmark Features Inattention-
A Neurologist s Approach to Altered Mental Status
 A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 23, 2008 The speaker has no disclosures Case 1 A 71 year-old
A Neurologist s Approach to Altered Mental Status S. Andrew Josephson, MD Department of Neurology University of California San Francisco October 23, 2008 The speaker has no disclosures Case 1 A 71 year-old
Antipsychotic Medication
 Antipsychotic Medication Mary Knutson, RN 3-7-12 Mosby items and derived items 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 1 Clinical Uses of Antipsychotics Short-term: in severe depression and
Antipsychotic Medication Mary Knutson, RN 3-7-12 Mosby items and derived items 2009 by Mosby, Inc., an affiliate of Elsevier Inc. 1 Clinical Uses of Antipsychotics Short-term: in severe depression and
Psychopharmacology in the Emergency Room. Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan
 Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan Pretest 1. Which of the following conditions is LEAST likely to benefit from emergency
Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan Pretest 1. Which of the following conditions is LEAST likely to benefit from emergency
What Is Delirium? Causes of Delirium
 1 What Is Delirium? Delirium is a condition that develops quickly (usually over hours or days) and involves changes in consciousness, attention, cognition (thinking and reasoning), and perception. An individual
1 What Is Delirium? Delirium is a condition that develops quickly (usually over hours or days) and involves changes in consciousness, attention, cognition (thinking and reasoning), and perception. An individual
Behavioral Issues in Dementia. March 27, 2014 Dylan Wint, M.D.
 Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Behavioral Issues in Dementia March 27, 2014 Dylan Wint, M.D. OVERVIEW Key points Depression Definitions and detection Treatment Psychosis Definitions and detection Treatment Agitation SOME KEY POINTS
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Psychopharmacology in the Emergency Room. Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan
 Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan Pretest 1. Appropriate target symptoms for emergency room medication treatment
Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Associate Professor of Psychiatry University of Michigan Pretest 1. Appropriate target symptoms for emergency room medication treatment
Acute vs. Maintenance
 Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Acute vs. Maintenance
 Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Acute vs. Maintenance The objective of rapid and effective management of acute agitation, confusion and decompensation is to minimize the morbidities of the post acute or chronic course, and thus reduce
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh. Professor of Critical Care, Edinburgh University
 Tim Walsh. Professor of Critical Care, Edinburgh University") Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Managing Delirium: The best way to achieve clarity (of mind) Tim Walsh Professor of Critical Care, Edinburgh University Lecture Plan: a route to clarity What is delirium? Why is delirium important? Step
Delirium in Palliative care. Presentation to Volunteers 2016 David Falk
 Delirium in Palliative care Presentation to Volunteers 2016 David Falk Delirium What is delirium? Case Study - Delirium 60+ year old PQ presents to hospice very somnolent. She was admitted with her adult
Delirium in Palliative care Presentation to Volunteers 2016 David Falk Delirium What is delirium? Case Study - Delirium 60+ year old PQ presents to hospice very somnolent. She was admitted with her adult
Do you know. Assessment of Delirium. What is Delirium? Which syndrome occurs more commonly in elderly populations? a. Delirium b.
 Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Assessment of Delirium Marianne McCarthy, PhD, GNP, PMHNP Arizona State University College of Nursing and Health Innovation What is Delirium? Delirium is a common clinical syndrome characterized by: Inattention
Critical Care Pharmacological Management of Delirium
 Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Critical Care Pharmacological Management of Delirium Policy Title: in the Critical Care Unit Executive Summary: This policy provides guidance Pharmacological Management of delirium in the Critical Care
Test your Knowledge: Recognizing Delirium
 The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
The Ottawa Hospital Name: Unit: Profession: RN RPN PT OT SW Other Note: Each question has only one correct answer. 1. If a patient is identified as being at high risk for developing delirium, his/her mental
AGED SPECIFIC ASSESSMENT TOOLS. Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services
 AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
AGED SPECIFIC ASSESSMENT TOOLS Anna Ciotta Senior Clinical Neuropsychologist Peninsula Mental Health Services Issues in assessing the Elderly Association between biological, psychological, social and cultural
PSYCHOSOCIAL SYMPTOMS (DELIRIUM)
") PSYCHOSOCIAL SYMPTOMS (DELIRIUM) Rut Kiman MD, MSc Head Pediatric Palliative Care Team Hospital Nacional Prof. A. Posadas Buenos Aires -Argentina Senior Lecturer. Pediatric Department School of Medicine.
PSYCHOSOCIAL SYMPTOMS (DELIRIUM) Rut Kiman MD, MSc Head Pediatric Palliative Care Team Hospital Nacional Prof. A. Posadas Buenos Aires -Argentina Senior Lecturer. Pediatric Department School of Medicine.
Addressing Difficult Behaviors in Dementia
 Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Addressing Difficult Behaviors in Dementia GEORGE SCHOEPHOERSTER, MD GERIATRICIAN GENEVIVE/CENTRACARE CLINIC Objectives By the end of the session, you will be able to: 1) Explain the role of pain management
Drugs used in schizophrenia قادة فریق علم الا دویة : الشكر موصول لا عضاء الفریق المتمیزین :
 MCQs SAQs Summar y Drugs used in schizophrenia قادة فریق علم الا دویة : لین التمیمي & عبدالرحمن ذكري الشكر موصول لا عضاء الفریق المتمیزین : روان سعد القحطاني فؤاد بھجت عبدالرحمن العریفي حاتم النداح pharma436@outlook.com
MCQs SAQs Summar y Drugs used in schizophrenia قادة فریق علم الا دویة : لین التمیمي & عبدالرحمن ذكري الشكر موصول لا عضاء الفریق المتمیزین : روان سعد القحطاني فؤاد بھجت عبدالرحمن العریفي حاتم النداح pharma436@outlook.com
Objectives. Symptom Management in the Frail Elderly Population. Disclosures. Symptom Management: Pain 12/05/2014
 Objectives Symptom Management in the Frail Elderly Population Dr. Katie Marchington, MD, CCFP Palliative Care Physician Toronto Western Hospital Kensington Hospice To reflect on why we should identify
Objectives Symptom Management in the Frail Elderly Population Dr. Katie Marchington, MD, CCFP Palliative Care Physician Toronto Western Hospital Kensington Hospice To reflect on why we should identify
Schizophrenia Pharmacology UNIVERSITY OF HAWAI I HILO PRE -NURSING PROGRAM
 Schizophrenia Pharmacology UNIVERSITY OF HAWAI I HILO PRE -NURSING PROGRAM NURS 203 GENERAL PHARMACOLOGY DANITA NARCISO PHARM D Learning Objectives Understand the result of dopamine binding to D2 receptors
Schizophrenia Pharmacology UNIVERSITY OF HAWAI I HILO PRE -NURSING PROGRAM NURS 203 GENERAL PHARMACOLOGY DANITA NARCISO PHARM D Learning Objectives Understand the result of dopamine binding to D2 receptors
Delirium in Critical Care. Recognition, Management, Research tasters. Dr Valerie Page Watford General Hospital
 Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Delirium in Critical Care. Recognition, Management, Research tasters Dr Valerie Page Watford General Hospital What does it look like? Diagnosing delirium CAM-ICU CAM-ICU Feature 1: Acute onset of mental
Research Article The Phenomenology of Delirium: Presence, Severity, and Relationship between Symptoms
 Geriatrics, Article ID 427042, 6 pages http://dx.doi.org/10.1155/2014/427042 Research Article The Phenomenology of Delirium: Presence, Severity, and Relatiohip between Symptoms Soenke Boettger, 1 Susanne
Geriatrics, Article ID 427042, 6 pages http://dx.doi.org/10.1155/2014/427042 Research Article The Phenomenology of Delirium: Presence, Severity, and Relatiohip between Symptoms Soenke Boettger, 1 Susanne
11/11/2016. Disclosures. Natural history of BPSD. Objectives. Assessment of BPSD. Behavioral Management of Persons with Alzheimer s Disease
 Disclosures Behavioral Management of Persons with Alzheimer s Disease Wisconsin Association of Medical Directors November 17, 2016 Art Walaszek, M.D. Professor of Psychiatry UW School of Medicine & Public
Disclosures Behavioral Management of Persons with Alzheimer s Disease Wisconsin Association of Medical Directors November 17, 2016 Art Walaszek, M.D. Professor of Psychiatry UW School of Medicine & Public
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017.
 DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DEMENTIA and BPSD in PARKINSON'S DISEASE. DR. T. JOHNSON. NOVEMBER 2017. Introduction. Parkinson's disease (PD) has been considered largely as a motor disorder. It has been increasingly recognized that
DELIRIUM IN ICU: Prevention and Management. Milind Baldi
 DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
DELIRIUM IN ICU: Prevention and Management Milind Baldi Contents Introduction Risk factors Assessment Prevention Management Introduction Delirium is a syndrome characterized by acute cerebral dysfunction
AGITATION THE SCOPE AND IMPACT OF DELIRIUM AGITATION, RESTLESSNESS, CONFUSION AND DELIRIUM
 ADVANCE CARE PLANNING AND END OF LIFE CARE UNIT NO. 6 AGITATION Dr Tan Yew Seng ABSTRACT Agitation and delirium are commonly encountered symptoms in palliative care. Based on the clinical features, delirium
ADVANCE CARE PLANNING AND END OF LIFE CARE UNIT NO. 6 AGITATION Dr Tan Yew Seng ABSTRACT Agitation and delirium are commonly encountered symptoms in palliative care. Based on the clinical features, delirium
Psychosis and Agitation in Dementia
 Psychosis and Agitation in Dementia Dilip V. Jeste, MD Estelle & Edgar Levi Chair in Aging, Director, Stein Institute for Research on Aging, Distinguished Professor of Psychiatry & Neurosciences, University
Psychosis and Agitation in Dementia Dilip V. Jeste, MD Estelle & Edgar Levi Chair in Aging, Director, Stein Institute for Research on Aging, Distinguished Professor of Psychiatry & Neurosciences, University
Transitioning to Adult-Gerontology APRN Education: Slide Library
 Transitioning to Adult-Gerontology APRN Education: Slide Library APRN Assessment and Management of Older Adults with Delirium Authors: Lois Evans, PhD, RN, FAAN Pamela Z. Cacchione, PhD, APRN, GNP, BC
Transitioning to Adult-Gerontology APRN Education: Slide Library APRN Assessment and Management of Older Adults with Delirium Authors: Lois Evans, PhD, RN, FAAN Pamela Z. Cacchione, PhD, APRN, GNP, BC
Delirium. Preconference SHPCA Clinical Day Saskatoon, SK May 13, 2014
 Preconference SHPCA Clinical Day 2014 Saskatoon, SK May 13, 2014 Carmen L. Johnson MD, CCFP, ABFP, AAHPM, AAPM, ABAM, ABRPM (Pain Medicine) Medical Director Palliative Care Services, Regina Qu Appelle
Preconference SHPCA Clinical Day 2014 Saskatoon, SK May 13, 2014 Carmen L. Johnson MD, CCFP, ABFP, AAHPM, AAPM, ABAM, ABRPM (Pain Medicine) Medical Director Palliative Care Services, Regina Qu Appelle
Treatment of Schizophrenia
 Treatment of Schizophrenia Conduct comprehensive assessment and use measurement-based care as found in the Principles of Practice (review pages 4-7). Most importantly assess social support system (housing,
Treatment of Schizophrenia Conduct comprehensive assessment and use measurement-based care as found in the Principles of Practice (review pages 4-7). Most importantly assess social support system (housing,
Palliative Care. Barry Lunny Registrar in Palliative Medicine
 Symptom Management in Palliative Care Delirium and Pain Barry Lunny Registrar in Palliative Medicine Delirium outline What delirium is and why it is important How to recognise it What to do about it Delirium
Symptom Management in Palliative Care Delirium and Pain Barry Lunny Registrar in Palliative Medicine Delirium outline What delirium is and why it is important How to recognise it What to do about it Delirium