RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5
|
|
|
- Della Jasmine Terry
- 6 years ago
- Views:
Transcription
1 RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5
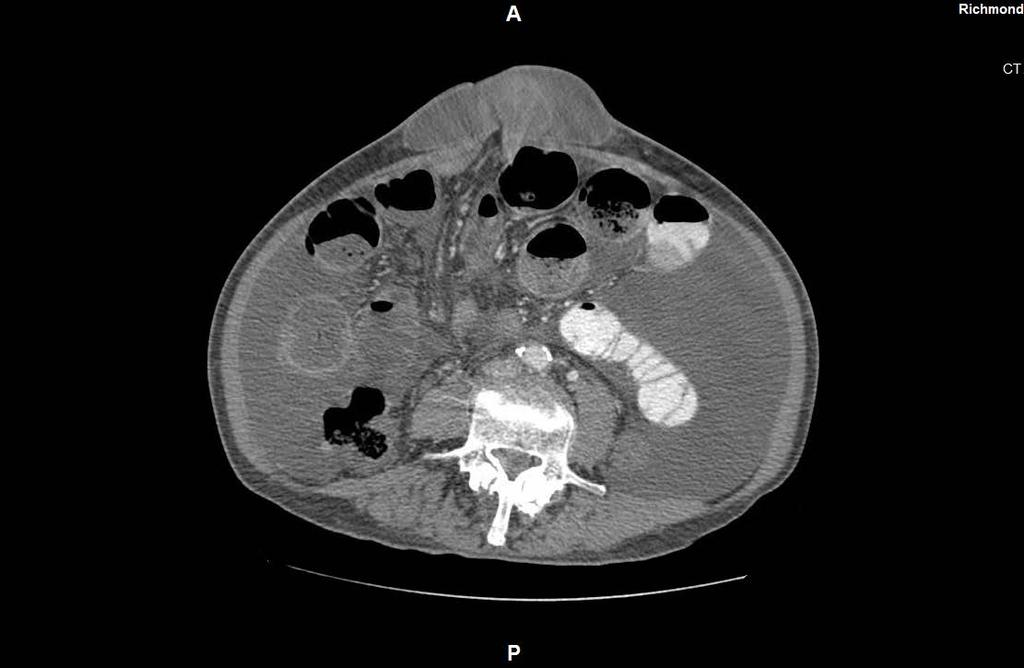
2 PATIENT PRESENTATION 73M w/ Hep B Cirrhosis, HTN, DM II Liver disease followed at OSH x2 years (when moved from China), on tenofivir, lasix Known umbilical hernia, acute onset of pain at hernia site x1d Constipation, obstipation, nausea & vomiting x1d
3 PATIENT PRESENTATION / %RA NAD, AAOx3 Abdomen distended with fluid wave Umbilical hernia with erythematous appearing skin and 2x3 scab at apex. Hernia fluid filled with palpable indurated mass within. Nonreducible. Non-tender. Bilateral inguinal hernias, fluid filled
4 PATIENT PRESENTATION CBC: 5.1/12.2/37.1/53 BMP: 136/4.4/103/27/34/1.3/ /2.2/4.0 LFTs: 8.6/2.5/51/50/88/2.7 Coags: 16.3/27.8/1.8

5
6
7
8
9
10
11
12
13
14 PATIENT PRESENTATION Discussion with patient and son at bedside including significant risks of surgery DNR/DNI status Refusal of surgery Admitted NGT/NPO Serial abdominal exams

15 PATIENT PRESENTATION HD 1-3 pt did not improve and hernia became increasingly discolored, tense, and painful Patient expressed desire for surgery at night, added on for following day /78 99% Creatinine Bilirubin INR Pt became encephalopathic Ammonia 160 Son elected to consent to surgery the following morning, taken to surgery emergently
16 OPERATIVE COURSE Opened hernia sac immediate release of large ascites and obvious necrotic small bowel Hernia defect 1cm, opened to deliver dilated and collapsed small bowel, viable in both directions from defect (opened to approx 6 cm) Removed ascites (total 8L by end of case) Resected 25cm small bowel side-to-side stapled anastomosis Closed defect w/ running #1 prolene Skin left open and packed Operative time: 2h Given 4u FFP, 1000 crystaloid EBL 100, UOP 300 Taken to SICU intubated
17 POSTOPERATIVE COURSE - OVERVIEW POD 0-2: critical POD 3-11: progression to multi-organ failure POD 12: family elected against escalation of care and made DNR status, to maintain abx and ETT, institute comfort care POD 15: expired in PM
18 POSTOPERATIVE COURSE - SYSTEMS N: non-responsive off sedation lactulose POD 4 responsive with agitation POD 10 increasingly obtunded off sedation until expiration C: initially NT/NTC POD 4 hypertensive with new onset afib w/ RVR amiodarone gtt + metoprolol POD 10 switched to metoprolol, rate maintained in afib P/ID: initially kept intubated POD 3 failed SBT CXR after fever demonstrates bilateral infiltrates resp cx w/ MSSA and enterobacter abx initiated and maintained until expiration multiple self-extubations with successful reintubations
19 POSTOPERATIVE COURSE - SYSTEMS Heme Initially on HSQ for DVT ppx Vitamin K POD 8 pt had coffee-ground NGT aspirate and dropped Hct INR 3.1, platelets 38 (ranged throughout admission 20-50) Transfused PRBC, platelets, FFP, HSQ d/c d Intermittent coffee-ground emesis, no additional drop in Hct or PRBC transfusions
20 POSTOPERATIVE COURSE - SYSTEMS Renal/Fluids 8L ascites drained intraop 1u albumin in PACU Normotensive over POD 0-3, became hypertensive controlled with metoprolol until expiration BUN/Crt 40/1.2 BUN increased over 10 days to 120s, Crt stable until POD 7, increased to 2, 3, 5 Na peaked at 154 on POD 4, NS initially to ½ maintenance rate Lasix IV and spironolactone NG for ascites, albumin given daily with lasix, no return of ascitic distension
21 POSTOPERATIVE COURSE - SYSTEMS GI Trickle feeds from POD1 advanced to goal feeds with hepatic formula Bilirubin post-op stable at 4-5 until POD 8 increased to 10 then 20
22
23 OVERVIEW Pathophysiology of Cirrhosis Pre-operative and Post-operative considerations Risk stratification Patient specific factors Contraindications to surgery Scoring systems CTP, MELD, is there a right score to use? Surgery specific factors Umbilical hernia as special case?

24 PATHWAY Pt in need of non-hepatic surgery H&P Suspicious for liver disease Characterize LFTs Serology Imaging Risk Stratification Risk Score Other Patient Factors Surgery Type No evidence of liver disease or cirrhosis Continue preoperative assessment GET SURGERY Unacceptable Risk Pursue alternative therapy Acceptable Risk Optimize SURGERY Manage postoperative care


25 PATHWAY Pt in need of non-hepatic surgery H&P Suspicious for liver disease Characterize LFTs Serology Imaging Risk Stratification Risk Score Other Patient Factors Surgery Type No evidence of liver disease or cirrhosis Continue preoperative assessment GET SURGERY Unacceptable Risk Pursue alternative therapy Acceptable Risk Optimize SURGERY Manage postoperative care
26 PATHOPHYSIOLOGY OF CIRRHOSIS Portal Hypertension Hemodynamics circulating volume and pressure Cardiac function hyperdynamism Renal function Ascites Liver Function Synthetic Coagulation Metabolic Toxins, pharmacology Nutrition Infectious disease
27 Normal System
28 Cirrhosis 1. Intrahepatic NO decreased, TXA increased (+ Scarification) NO TXA
29 NO TXA NO TXA Cirrhosis 1. Intrahepatic NO decreased, TXA increased (+ Scarification) 2. Collateral flow 3. Splanchnic circulation becomes vasodilatory to compensate (with decrease in systemic)
30 NO TXA Principal effects: Hyperdynamic cardiac function with little reserve Maximized hepatic circulation with little reserve Decreased renal blood flow NO TXA
31 Effects on Kidney? Decreased blood flow Activation of Renin- Angiotensin- Aldosterone Non-osmotic release of vasopressin
32 Effects on Kidney? Decreased blood flow Activation of Renin- Angiotensin-Aldosterone Non-osmotic release of vasopressin renal hypoperfusion sodium retention (fluid overload) free-water retention in excess of sodium retention (hyponatremia)
33 Compensation vs Decompensation NO TXA NO TXA
34 PATHOPHYSIOLOGY OF CIRRHOSIS Ascites 10% in cirrhosis 60% 3 year survival after onset Hemodynamic consequences Increased splanchnic flow + increased portal pressure Capillary permeability increases Hypoalbuminemia
35 OPTIMIZATION BY SYSTEMS Cardiac Hyper-dynamism Pre-operative Cardiac assessment Awareness of lack of reserve Post-operative Avoid inotropic agents
36 OPTIMIZATION BY SYSTEMS Renal Pre-operative Renal function studies Assessment for hepatorenal syndrome Judicious use of diuretics for ascites and lactulose for encephalopathy (volume) Albumin vs crystaloid Post-operative Monitoring for HRS Albumin vs crystaloid

37 OPTIMIZATION BY SYSTEMS Hepatorenal Syndrome Overwhelming activation of renin-angiotensinaldosterone system Difficult to reverse High mortality
38 OPTIMIZATION BY SYSTEMS Hepatorenal Syndrome Treatment Terlipressin splanchnic vasoconstriction Albumin+octreotide+midodrine RRT - failure
39 OPTIMIZATION BY SYSTEMS Ascites Pre-operative Diuretic therapy- spironolactone and furosemide Large Volume Paracentesis (LVP) Albumin administration with LVP Screening for SBP Post-operative Same Paracentesis Induced Circulatory Dysfunction Fluid shift vs vasodilation Hypovolemia and R-A-A activation Volume expansion >5L w/ albumin
40 OPTIMIZATION BY SYSTEMS Neurologic Pre-operative Consider diagnosis of hepatic encephalopathy Lactulose, rifaximin, serial ammonia measurements unhelpful Avoidance of sedation Post-operative Same
41 OPTIMIZATION BY SYSTEMS Coagulation Synthetic (factors) + consumptive (platelets) Pre-operative Vitamin K FFP and platelets No benefit of rfvii Post-operative Same
42 OPTIMIZATION BY SYSTEMS Nutrition Pre-operative, Post-operative Maximize nutrition, no good evidence for hepatic formulas (including low-nitrogen) Infectious Disease SBP Sepsis No difference in GDT in cirrhotic - harder Inotropes less effective Lactate metabolism
43 OPTIMIZATION Cardiac Avoidance of inotropes Neuro Encephalopathy - lactulose Renal Hyponatremia fluid restriction HRS albumin, terlipressin, octreotide+midodrine Ascites Diuretics, LVP w/ albumin Coagulopathy Vitamin K, platelets and FFP Awareness of the precariousness of cirrhotic physiology, readiness to act
44 PATHWAY Pt in need of non-hepatic surgery H&P Suspicious for liver disease Characterize LFTs Serology Imaging Risk Stratification Other Patient Factors Risk Score Surgery Type No evidence of liver disease or cirrhosis Continue preoperative assessment GET SURGERY Unacceptable Risk Pursue alternative therapy Acceptable Risk Optimize SURGERY Manage postoperative care

45 WHY RISK STRATIFY? Patients with cirrhosis need surgery Umbilical hernia Gallbladder Colon Cardiac Emergency surgical conditions Liver surgery and transplantation Patients with cirrhosis do worse The effects of surgery (and other stressors) are complicated and unpredictable 7
46 OTHER PATIENT FACTORS

47 OTHER PATIENT FACTORS Hepatopulmonary Syndrome Up to 50% of cirrhotic patients Significant increase in mortality Median survival 11 months No studies on effect on post-op mortality Irreversible cause of hypoxia
48 OTHER PATIENT FACTORS Hepatopulmonary Syndrome Algorithm
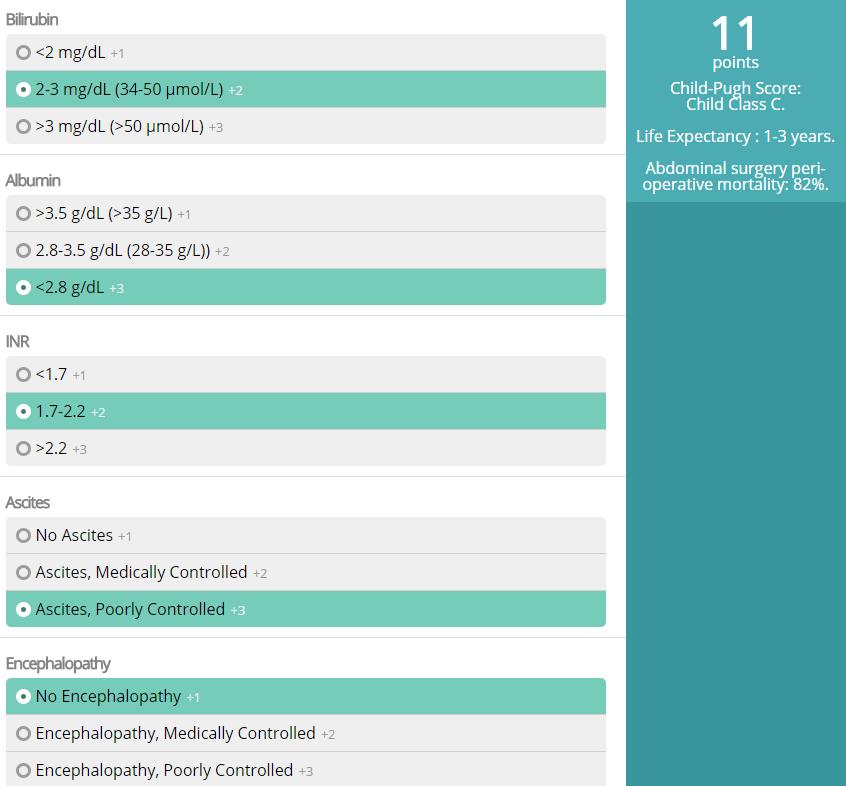
49 RISK SCORES: CHILD-TURCOTTE-PUGH Child & Turcotte Mortality after shunting surgery for portal htn Variables, original: Albumin Bilirubin Encephalopathy Ascites Nutritional status
50 RISK SCORES: CHILD-TURCOTTE-PUGH Pugh et al Transection of the oesophagus for bleeding oesophageal varices (BJS) Mortality after surgery for bleeding varices Variables, updated: Albumin Bilirubin Encephalopathy Ascites Nutritional status Prothrombin time
51 RISK SCORES: CHILD-TURCOTTE-PUGH Ease of use, simplicity 40 years and 100s of papers Ruptured esophageal varices Subclinical encephalopathy Hepatocellular carcinoma Alcoholic cirrhosis Decompensated HCV-related cirrhosis Primary sclerosing cholangitis Primary biliary cirrhosis Budd Chiari syndrome Liver surgery and transplant Mortality after non-hepatic surgery

52 patients with cirrhosis undergoing emergent or elective surgery 54 variables evaluated retrospectively CTP score most predictive of mortality The study thought of as the validation study as the mortality figures mirror those from original paper
53 RISK SCORES: CHILD-TURCOTTE-PUGH MDCalc
54 RISK SCORES: CHILD-TURCOTTE-PUGH Disadvantages: Ascites and encephalopathy are SUBJECTIVE Validation has been mainly in RETROSPECTIVE studies with SMALL study populations Variables NOT WEIGHTED CAUSE of cirrhosis not included SURGERY type not included
 3 weighted variables: bilirubin, INR,")
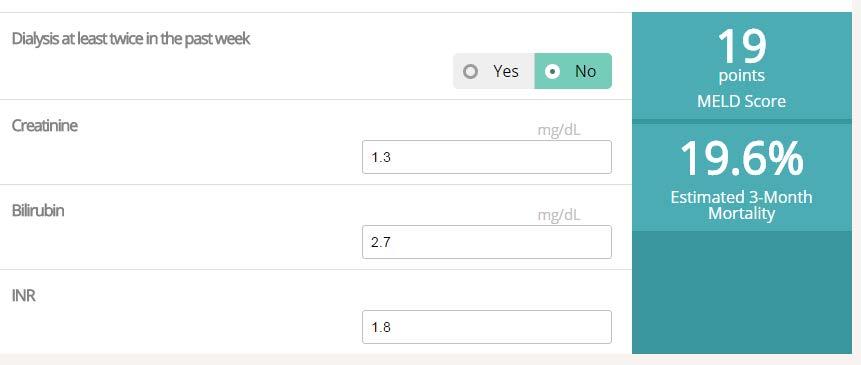
55 RISK SCORES: MELD MELD: Model for End-stage Liver Disease 2000 retrospective 231 patients who underwent TIPS Cox-proportio (statistics) 3 weighted variables: bilirubin, INR, creatinine
56 RISK SCORES: MELD Validation with 4 larger data sets (n=282 to n=1179) Mortality overall, unrelated to undergoing a procedure Allogenic transplant allocation

57 RISK SCORES: MELD MDCalc
58 RISK SCORES: MELD
59 RISK SCORES: MELD prospective 40 patients undergoing elective (n=24) or emergent (n=16) surgical procedures CTP and MELD
60 RISK SCORES: MELD Advantages: All variables are OBJECTIVE Validation for overall mortality risk has utilized LARGE study populations Variables WEIGHTED MELD = 3.78 ln[serum bilirubin (mg/dl)] ln[inr] ln[serum creatinine (mg/dl)] Disadvantages Assessment of mortality in cirrhotic patients after surgery continued to rely on SMALL data sets CAUSE of cirrhosis not included SURGERY type not included
61 RISK SCORES - WHAT TO USE?
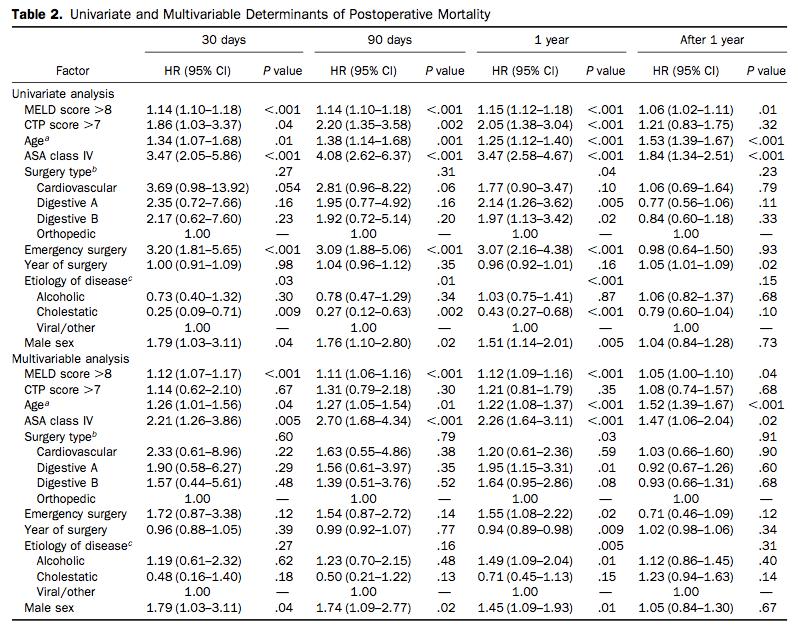
62 RISK SCORES - WHAT TO USE? retrospective 772 cirrhotic patients undergoing digestive(n=586), orthopedic (n=107) or cardiac surgery (n=79) Multivariable analysis (w/ statistics)
63
64
65
66 IS THAT IT? Pt in need of non-hepatic surgery H&P Suspicious for liver disease Characterize LFTs Serology Imaging Risk Stratification Risk Score Other Patient Factors Surgery Type No evidence of liver disease or cirrhosis Continue preoperative assessment GET SURGERY Unacceptable Risk Pursue alternative therapy Acceptable Risk Optimize SURGERY Manage postoperative care
67 SURGERY SPECIFIC FACTORS Type of surgery has significant impact

68
69 UMBILICAL HERNIA Significant problem in cirrhotics 20% prevalence, 40-50% in setting of ascites Enlarge over time Skin breakdown and necrosis SBP What role do risk scores play? Surgery for UH an exception to these scores?

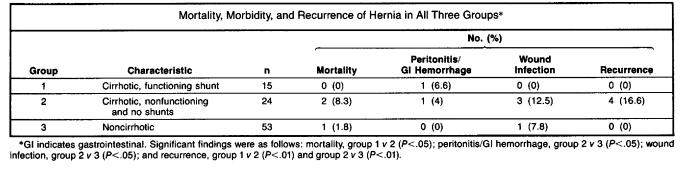
70 UMBILICAL HERNIA
71 UMBILICAL HERNIA
72 UMBILICAL HERNIA 32,033 patients who underwent abdominal wall hernias between 1999 and 2004 (excluding inguinal) 1197 cirrhotic patients Emergency surgery performed in 60% of cirrhotics (vs 30% non-cirrhotics) Does not include table comparison between study groups
73 UMBILICAL HERNIA
74 UMBILICAL HERNIA
75 UMBILICAL HERNIA
76 UMBILICAL HERNIA
77 SUMMARY 1 Pre- and Post-operative issues in cirrhotics 1. There are dysfunctions related to cirrhosis that deserve special attention 2. Awareness of the precariousness of cirrhotic physiology, readiness to act
78 SUMMARY 2 Risk stratification for cirrhotic patients undergoing non-hepatic surgery includes 1. Review and consider contraindications to elective surgery, including HPS 2. Calculation of a risk score, of which the Mayo Clinic augmented MELD appears the most robust 3. Consideration of surgery specific data on morbidity and mortality
79 SUMMARY 3 Umbilical hernia repair in cirrhotic patients Is safe, with acceptable morbidity and mortality When performed under elective conditions, has comparable morbidity and mortality to non-cirrhotics Should be performed when found to avoid the increase in mortality under emergent conditions Can probably be performed using synthetic mesh

80
81

82
Definition: fibrosis and nodular regeneration resulting from hepatocellular injury
 Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Cirrhosis Understanding the liver: Patterns of LFT Abnormalities - Hepatocellular/Transaminitis: o Ratio of AST: ALT >2:1 ETOH (keep in mind AST is also produced by red cells, heart muscle) o If Aminotransferases
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Etiology of liver cirrhosis
 Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
Liver cirrhosis 1 Liver cirrhosis Liver cirrhosis is the progressive replacement of normal hepatic cells by fibrous scar tissue, This scarring is accompanied by the loss of viable hepatocytes, which are
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT
 MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
MANAGEMENT OF LIVER CIRRHOSIS: PRACTICE ESSENTIALS AND PATIENT SELF-MANAGEMENT Sherona Bau, ACNP The Pfleger Liver Institute 200 UCLA Medical Plaza, Suite 214 Los Angeles, CA 90095 September 30, 2017 I
Chronic Hepatic Disease
 Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Complications of Cirrhosis
 Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
Complications of Cirrhosis Causes of Cirrhosis Alcohol Chronic Viral Hepatitis (B/C) Haemochromatosis Autoimmune Hepatitis NAFLD/NASH Primary Biliary Cirrhosis Primary Sclerosing Cholangitis 1-AT deficiency
The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals. By: Dr. Kevin Dolehide
 Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
Management of Chronic Liver Failure/Cirrhosis Complications in Hospitals By: Dr. Kevin Dolehide Overview DX Cirrhosis and Prognosis Compensated Decompensated Complications Of Cirrhosis Management Of Complications
End-Stage Liver Disease (ESLD): A Guide for HIV Physicians
: A Guide for HIV Physicians") Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications
 PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
PORTAL HYPERTENSION An Introduction to the Culprit of Many Liver Failure Complications Edy G. Trujillo, RN, MSN, ACNP-BC Liver Transplant RRUCLA Medical Center July 31, 2018 What Do We All Look Forward
Update in abdominal Surgery in cirrhotic patients
 Update in abdominal Surgery in cirrhotic patients Safi Dokmak HBP department and liver transplantation Beaujon Hospital, Clichy, France Cairo, 5 April 2016 Cirrhosis Prevalence in France (1%)* Patients
Update in abdominal Surgery in cirrhotic patients Safi Dokmak HBP department and liver transplantation Beaujon Hospital, Clichy, France Cairo, 5 April 2016 Cirrhosis Prevalence in France (1%)* Patients
ESLD a Guide for HIV Physicians. Marion Peters University of California San Francisco June 2015
 ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
Initial approach to ascites
 Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Ascites: Filling and Draining the Water Balloon Common Pathogenesis in Refractory Ascites, Hyponatremia, and Cirrhosis intrahepatic resistance sinusoidal portal hypertension Splanchnic vasodilation (effective
Management of the Cirrhotic Patient in the ICU
 Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Steps in Assessing Fibrosis 4/30/2015. Overview of Liver Disease Associated With HCV
 Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome
 Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Norepinephrine versus Terlipressin for the Treatment of Hepatorenal Syndrome Disclosure I have no conflicts of interest to disclose Name: Margarita Taburyanskaya Title: PharmD, PGY1 Pharmacy Practice Resident
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Index Note: Page numbers of article titles are in boldface type. A Accelerated intravascular coagulation and fibrinolysis (AICF) in liver disease, 390 391 Acid suppression in liver disease, 403 404 ACLF.
Conflict of interest disclosures. Complications of end stage liver disease. None. The many complications of Cirrhosis. Portal Hypertension.
 Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
Complications of end stage liver disease Conflict of interest disclosures None Amir Qamar, MD Instructor of Medicine Brigham and Women s s Hospital Harvard Medical School Boston, MA 02115 The many complications
JOURNAL PRESENTATION. Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013
 JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
JOURNAL PRESENTATION Dr Tina Fan Tseung Kwan O Hospital 17 th Jan 2013 THE COMBINATION OF OCTREOTIDE AND MIDODRINE IS NOT SUPERIOR TO ALBUMIN IN PREVENTING RECURRENCE OF ASCITES AFTER LARGE-VOLUME PARACENTESIS
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist. K V Speeg, MD, PhD UT Health San Antonio
 The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
Contraindications. Indications. Complications. Currently TIPS is considered second or third line therapy for:
 Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Management of Cirrhotic Patients Undergoing Non-Transplant Surgery
 Management of Cirrhotic Patients Undergoing Non-Transplant Surgery Jason S. Wakakuwa, M.D. Assistant Professor of Anesthesia Director, Transplant Anesthesia Beth Israel Deaconess Medical Center I have
Management of Cirrhotic Patients Undergoing Non-Transplant Surgery Jason S. Wakakuwa, M.D. Assistant Professor of Anesthesia Director, Transplant Anesthesia Beth Israel Deaconess Medical Center I have
CHAPTER 7. End Stage Liver Disease in the ICU: Walking a Tightrope. Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing
 CHAPTER 7 End Stage Liver Disease in the ICU: Walking a Tightrope Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing Besey Oren, Assistant Professor Istanbul University Health
CHAPTER 7 End Stage Liver Disease in the ICU: Walking a Tightrope Lynn A. Kelso, MSN, APRN, FCCM, FAANP University of Kentucky College of Nursing Besey Oren, Assistant Professor Istanbul University Health
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC
 Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Decompensated chronic liver disease
 Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
Decompensated chronic liver disease Definition of decompensated chronic liver disease Patients with chronic liver disease can present with acute decompensation due to various causes. The decompensation
following the last documented transfusion; thereafter, evaluate the residual impairment(s).
.") Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
Adult Listings 5.01 Category of Impairments, Digestive System 5.02 Gastrointestinal hemorrhaging from any cause, requiring blood transfusion (with or without hospitalization) of at least 2 units of blood
Dialyzing challenging patients: Patients with hepato-renal conditions
 Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Dialyzing challenging patients: Patients with hepato-renal conditions Nidyanandh Vadivel MD Medical Director for Living kidney Donor and Pancreas Transplant Programs Swedish Organ Transplant, Seattle Acute
Acute Liver Failure. Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018
 Acute Liver Failure Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018 Disclosures None Outline Overview of ALF Management of ALF Diagnosis of ALF Treatments and Support
Acute Liver Failure Neil Shah, MD UNC School of Medicine High-Impact Hepatology Saturday, Dec 8 th, 2018 Disclosures None Outline Overview of ALF Management of ALF Diagnosis of ALF Treatments and Support
58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia. Jess Hwang 11/8/12
 58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia Jess Hwang 11/8/12 HPI Fluid leaking from umbilical hernia secondary to his ascites Went to OR for drain placement which was complicated
58 Year-old Male with Alcoholic Cirrhosis Presents with Hyponatremia Jess Hwang 11/8/12 HPI Fluid leaking from umbilical hernia secondary to his ascites Went to OR for drain placement which was complicated
Life After SVR for Cirrhotic HCV
 Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Life After SVR for Cirrhotic HCV KIM NEWNHAM MN, NP CIRRHOSIS CARE CLINIC UNIVERSITY OF ALBERTA Objectives To review the benefits of HCV clearance in cirrhotic patients To review some of the emerging data
Denver Shunts vs TIPS for Ascites
 Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
WEEK. MPharm Programme. Liver Biochemistry. Slide 1 of 49 MPHM14 Liver Biochemistry
 MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
Sign up to receive ATOTW weekly -
 HEPATORENAL SYNDROME ANAESTHESIA TUTORIAL OF THE WEEK 240 10 TH SEPTEMBER 2011 Gerry Lynch Rotherham General Hospital Correspondence to gerry.lynch@rothgen.nhs.uk QUESTIONS Before continuing, try to answer
HEPATORENAL SYNDROME ANAESTHESIA TUTORIAL OF THE WEEK 240 10 TH SEPTEMBER 2011 Gerry Lynch Rotherham General Hospital Correspondence to gerry.lynch@rothgen.nhs.uk QUESTIONS Before continuing, try to answer
Nursing Care & Management of the Pre-Liver Transplant Population. Christine Kiamzon, RN, MSN, PCCN 8 North Educator
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population
 Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Nursing Care & Management of the Pre-Liver Transplant Population Christine Kiamzon, RN, MSN, PCCN 8 North Educator Objectives 1. Identify key nursing interventions in caring for pre-transplant ESLD patients.
Anaesthetic considerations and peri-operative risks in patients with liver disease
 Anaesthetic considerations and peri-operative risks in patients with liver disease Dr. C. K. Pandey Professor & Head Department of Anaesthesiology & Critical Care Medicine Institute of Liver and Biliary
Anaesthetic considerations and peri-operative risks in patients with liver disease Dr. C. K. Pandey Professor & Head Department of Anaesthesiology & Critical Care Medicine Institute of Liver and Biliary
VARICEAL BLEEDING. Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta.
 VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
VARICEAL BLEEDING Ram Subramanian MD Hepatology & Critical Care Medical Director of Liver Transplant Emory University, Atlanta Disclosures: None OUTLINE Pathophysiology of portal hypertension Splanchnic
Chronic liver failure Assessment for liver transplantation
 Chronic liver failure Assessment for liver transplantation Liver Transplantation Dealing with the organ shortage Timing of listing must reflect length on waiting list Ethical issues Justice, equity, utility
Chronic liver failure Assessment for liver transplantation Liver Transplantation Dealing with the organ shortage Timing of listing must reflect length on waiting list Ethical issues Justice, equity, utility
Clinical Controversies in Perioperative Medicine
 Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
4/3/2014. Elizabeth Thompson, PharmD April Understand the importance of the liver and basic physiology.
 Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
Liver Disease Elizabeth Thompson, PharmD thompse@sarmc.org April 2014 Objectives Understand the importance of the liver and basic physiology. Review hepatic disorders Recognize liver function scoring systems
GI bleeding in chronic liver disease
 GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
Causes of Liver Disease in US
 Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
CrackCast Episode 28 Jaundice
 CrackCast Episode 28 Jaundice Episode overview: 1) Describe heme metabolism 2) List common pre-hepatic/hepatic/post-hepatic causes of jaundice Wisecracks: 1) What are clinical signs of liver disease? 2)
CrackCast Episode 28 Jaundice Episode overview: 1) Describe heme metabolism 2) List common pre-hepatic/hepatic/post-hepatic causes of jaundice Wisecracks: 1) What are clinical signs of liver disease? 2)
Beta-blockers in cirrhosis: Cons
 Beta-blockers in cirrhosis: Cons Eric Trépo MD, PhD Dept. of Gastroenterology. Hepatopancreatology and Digestive Oncology. C.U.B. Hôpital Erasme. Université Libre de Bruxelles. Bruxelles. Belgium Laboratory
Beta-blockers in cirrhosis: Cons Eric Trépo MD, PhD Dept. of Gastroenterology. Hepatopancreatology and Digestive Oncology. C.U.B. Hôpital Erasme. Université Libre de Bruxelles. Bruxelles. Belgium Laboratory
Clinical Controversies in Perioperative Medicine!
 Clinical Controversies in Perioperative Medicine! Hugo Quinny Cheng, MD! Division of Hospital Medicine! University of California, San Francisco! Disclosures! Perioperative beta-blockade & statin therapy
Clinical Controversies in Perioperative Medicine! Hugo Quinny Cheng, MD! Division of Hospital Medicine! University of California, San Francisco! Disclosures! Perioperative beta-blockade & statin therapy
Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association
 CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
Hepatorenal Syndrome
 Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
Necker Seminars in Nephrology Institut Pasteur Paris, April 22, 2013 Hepatorenal Syndrome Dr. Richard Moreau 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Paris Diderot
LIVER CIRRHOSIS. The liver extracts nutrients from the blood and processes them for later use.
 LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
LIVER CIRRHOSIS William Sanchez, M.D. & Jayant A. Talwalkar, M.D., M.P.H. Advanced Liver Disease Study Group Miles and Shirley Fiterman Center for Digestive Diseases Mayo College of Medicine Rochester,
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL
 Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Assessment of Liver Function: Implications for HCC Treatment
 Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Liver Transplantation Evaluation: Objectives
 Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
Esophageal Varices Beta-Blockers or Band Ligation. Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph
 Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Esophageal Varices Beta-Blockers or Band Ligation Cesar Yaghi MD Hotel-Dieu de France University Hospital Universite Saint Joseph Esophageal Varices Beta-Blockers or Band Ligation? Risk of esophageal variceal
Portogram shows opacification of gastroesophageal varices.
 Portogram shows opacification of gastroesophageal varices. http://clinicalgate.com/radiologic-hepatobiliary-interventions/ courtesyhttp://emedicine.medscape.com/article/372708-overview DR.Thulfiqar Baiae
Portogram shows opacification of gastroesophageal varices. http://clinicalgate.com/radiologic-hepatobiliary-interventions/ courtesyhttp://emedicine.medscape.com/article/372708-overview DR.Thulfiqar Baiae
Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia
 Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia Il sottoscritto dichiara di non aver avuto/di aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Filippo Schepis, MD Università degli Studi di Modena e Reggio Emilia Il sottoscritto dichiara di non aver avuto/di aver avuto negli ultimi 12 mesi conflitto d interesse in relazione a questa presentazione
Organ allocation for liver transplantation: Is MELD the answer? North American experience
 Organ allocation for liver transplantation: Is MELD the answer? North American experience Douglas M. Heuman, MD Virginia Commonwealth University Richmond, VA, USA March 1998: US Department of Health and
Organ allocation for liver transplantation: Is MELD the answer? North American experience Douglas M. Heuman, MD Virginia Commonwealth University Richmond, VA, USA March 1998: US Department of Health and
Preoperative elective transjugular intrahepatic portosystemic shunt for cirrhotic patients undergoing abdominal surgery
 REVIEW ARTICLE Annals of Gastroenterology (2017) 31, 330-337 Preoperative elective transjugular intrahepatic portosystemic shunt for cirrhotic patients undergoing abdominal Deepanshu Jain a, Ejaz Mahmood
REVIEW ARTICLE Annals of Gastroenterology (2017) 31, 330-337 Preoperative elective transjugular intrahepatic portosystemic shunt for cirrhotic patients undergoing abdominal Deepanshu Jain a, Ejaz Mahmood
Liver Failure. The most severe clinical consequence of liver disease is liver failure:
 Liver diseases I The major primary diseases of the liver are: - Viral hepatitis, - Nonalcoholic fatty liver disease (NAFLD), - Alcoholic liver disease, - Hepatocellular carcinoma (HCC) Hepatic damage also
Liver diseases I The major primary diseases of the liver are: - Viral hepatitis, - Nonalcoholic fatty liver disease (NAFLD), - Alcoholic liver disease, - Hepatocellular carcinoma (HCC) Hepatic damage also
CONTROLLED DOCUMENT. Cirrhosis Care Bundle CATEGORY: Clinical Guidelines. CLASSIFICATION: Clinical. Controlled Document CG201 Number:
 Cirrhosis Care Bundle CONTROLLED DOCUMENT CATEGORY: Clinical Guidelines CLASSIFICATION: Clinical Controlled Document CG201 Number: Version Number: 1 Controlled Document Clinical Guidelines Group Sponsor:
Cirrhosis Care Bundle CONTROLLED DOCUMENT CATEGORY: Clinical Guidelines CLASSIFICATION: Clinical Controlled Document CG201 Number: Version Number: 1 Controlled Document Clinical Guidelines Group Sponsor:
Conflicts of Interest
 Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
Anesthesia for Major Abdominal Cancer Resection John E. Ellis MD Adjunct Professor University of Pennsylvania johnellis1700@gmail.com Conflicts of Interest 1 Upper Abdominal Surgery Focus on oncologic
CIRRHOSIS Definition
 Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
Cirrhosis Update Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology Weill Cornell Medical College CIRRHOSIS Definition Irreversible fibrous
ACUTE-ON-CHRONIC LIVER FAILURE: DEFINITION, DIAGNOSIS AND CLINICAL CHARACTERISTICS.
 ACUTE-ON-CHRONIC LIVER FAILURE: DEFINITION, DIAGNOSIS AND CLINICAL CHARACTERISTICS. Vicente Arroyo 1, 2, Rajiv Jalan 2, 3 1 Institut de Investigacions Biomèdiques August Pi I Sunyer. University of Barcelona.
ACUTE-ON-CHRONIC LIVER FAILURE: DEFINITION, DIAGNOSIS AND CLINICAL CHARACTERISTICS. Vicente Arroyo 1, 2, Rajiv Jalan 2, 3 1 Institut de Investigacions Biomèdiques August Pi I Sunyer. University of Barcelona.
RENAL DISEASE IN END STAGE LIVER DISEASE
 RENAL DISEASE IN END STAGE LIVER DISEASE Mitchell L Shiffman, MD Director Health System Richmond and Newport News, VA Medical Group Good Help to Those in Need Mitchell L Shiffman, MD POTENTIAL CONFLICTS
RENAL DISEASE IN END STAGE LIVER DISEASE Mitchell L Shiffman, MD Director Health System Richmond and Newport News, VA Medical Group Good Help to Those in Need Mitchell L Shiffman, MD POTENTIAL CONFLICTS
Prof. Mohammad Umar. MBBS, MCPS, FCPS, FACG (USA), FRCP (London), FRCP (Glasgow), FAGA
, FRCP (London), FRCP (Glasgow), FAGA") Prof. Mohammad Umar MBBS, MCPS, FCPS, FACG (USA), FRCP (London), FRCP (Glasgow), FAGA Chairman and Head Department of Medicine Rawalpindi Medical College, Rawalpindi. Consultant Gastroenterologist / Hepatologist
Prof. Mohammad Umar MBBS, MCPS, FCPS, FACG (USA), FRCP (London), FRCP (Glasgow), FAGA Chairman and Head Department of Medicine Rawalpindi Medical College, Rawalpindi. Consultant Gastroenterologist / Hepatologist
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
Hepatology on the AMU
 Hepatology on the AMU RCP day, 8 th February 2018 Jo Leithead Consultant in Hepatology and Liver Transplantation Addenbrookes Hospital Cambridge Is liver disease relevant to me? Williams R, Lancet 2014
Hepatology on the AMU RCP day, 8 th February 2018 Jo Leithead Consultant in Hepatology and Liver Transplantation Addenbrookes Hospital Cambridge Is liver disease relevant to me? Williams R, Lancet 2014
For patients with cirrhosis, increased operative risk relative
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:451 457 ORIGINAL ARTICLES LIVER, PANCREAS, AND BILIARY TRACT Factors That Predict Outcome of Abdominal Operations in Patients With Advanced Cirrhosis DANA
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:451 457 ORIGINAL ARTICLES LIVER, PANCREAS, AND BILIARY TRACT Factors That Predict Outcome of Abdominal Operations in Patients With Advanced Cirrhosis DANA
PACT module Acute hepatic failure. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility
 Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources/HEN Course Materials & Disclosure Course materials including
Renal Care and Liver Disease: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources/HEN Course Materials & Disclosure Course materials including
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
PORTAL HYPERTENSION. Tianjin Medical University LIU JIAN
 PORTAL HYPERTENSION Tianjin Medical University LIU JIAN DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg (0.7 1.3kPa),
PORTAL HYPERTENSION Tianjin Medical University LIU JIAN DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg (0.7 1.3kPa),
Hepatorenal syndrome. Jan T. Kielstein Departent of Nephrology Medical School Hannover
 Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Hepatorenal syndrome Jan T. Kielstein Departent of Nephrology Medical School Hannover Hepatorenal Syndrome 1) History of HRS 2) Pathophysiology of HRS 3) Definition of HRS 4) Clinical presentation of HRS
Faculty Disclosure. Objectives. Cirrhosis Management for the Family Physician 18/11/2014
 Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Hepatic Encephalopathy
 Hepatic Encephalopathy John Barber UMassMedical Student, Class of 2019 www.12daysinmarch.com Outline Overview Normal Physiology Pathology Symptoms Diagnosis Treatment Overview Ammonia (NH 3 ) is a byproduct
Hepatic Encephalopathy John Barber UMassMedical Student, Class of 2019 www.12daysinmarch.com Outline Overview Normal Physiology Pathology Symptoms Diagnosis Treatment Overview Ammonia (NH 3 ) is a byproduct
Hepatocytes produce. Proteins Clotting factors Hormones. Bile Flow
 R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
CIRRHOTIC MANAGEMENT
 DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
DISCLAIMER: These guidelines were prepared by the Department of Surgical Education, Orlando Regional Medical Center. They are intended to serve as a general statement regarding appropriate patient care
PACT module Acute hepatic failure. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
PACT module Acute hepatic failure Intensive Care Training Program Radboud University Medical Centre Nijmegen Acute Liver Failure Acute on Chronic Liver Failure Acute loss of hepatocellular function in
Ascites. Matthew Johnson M.D.
 Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
Ascites Matthew Johnson M.D. The most common complication of portal hypertension 50% of patients who have compensated cirrhosis develop ascites by 10 years Survival after ascites develops: 1-year: 85%
Learning Objectives. After attending this presentation, participants will be able to:
 Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Evaluating HIV Patient for Liver Transplantation. Marion G. Peters, MD Professor of Medicine University of California San Francisco USA
 Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
Iatrogenic Cardiac Injuries. Kings County Hospital Center Verena Liu, MD 9/1/2011
 Iatrogenic Cardiac Injuries Kings County Hospital Center Verena Liu, MD 9/1/2011 Case Presentation 69 year old male recently diagnosed with a 3.8 cm x 4.3 cm hepatocellular CA in the superior segment of
Iatrogenic Cardiac Injuries Kings County Hospital Center Verena Liu, MD 9/1/2011 Case Presentation 69 year old male recently diagnosed with a 3.8 cm x 4.3 cm hepatocellular CA in the superior segment of
Ascites, a New Cause for Bilateral Hydronephrosis: Case Report
 Case Study TheScientificWorldJOURNAL (2009) 9, 1035 1039 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2009.112 Ascites, a New Cause for Bilateral Hydronephrosis: Case Report D. Jain*, S. Dorairajan, and
Case Study TheScientificWorldJOURNAL (2009) 9, 1035 1039 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2009.112 Ascites, a New Cause for Bilateral Hydronephrosis: Case Report D. Jain*, S. Dorairajan, and
The Kidney in Liver Disease. Jeff Kaufhold MD FACP Jan 2018
 The Kidney in Liver Disease Jeff Kaufhold MD FACP Jan 2018 Objectives 1. Understand new evidence in the pathophysiology of Hepatorenal syndrome 2. Review current treatment guidelines and some over the
The Kidney in Liver Disease Jeff Kaufhold MD FACP Jan 2018 Objectives 1. Understand new evidence in the pathophysiology of Hepatorenal syndrome 2. Review current treatment guidelines and some over the
Entrustable Professional Activity
 Entrustable Professional Activity 1. EPA Title: Care of infants, children and adolescents with acute and chronic s 2. Description of Activity Practicing subspecialists must be trained to care for children
Entrustable Professional Activity 1. EPA Title: Care of infants, children and adolescents with acute and chronic s 2. Description of Activity Practicing subspecialists must be trained to care for children
Anesthesia for Liver Transplantation. Current Practice and Future Directions
 Anesthesia for Liver Transplantation Current Practice and Future Directions U.S. Liver Transplants performed 1988-2002 Transplants 0 1000 2000 3000 4000 5000 Deceased Donor Living Donor 1988 1990 1992
Anesthesia for Liver Transplantation Current Practice and Future Directions U.S. Liver Transplants performed 1988-2002 Transplants 0 1000 2000 3000 4000 5000 Deceased Donor Living Donor 1988 1990 1992
Management of refractory ascites in cirrhosis: Are we out of date?
 Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.4254/wjh.v8.i28.1182 World J Hepatol 2016 October 8; 8(28): 1182-1193 ISSN 1948-5182 (online)
Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.4254/wjh.v8.i28.1182 World J Hepatol 2016 October 8; 8(28): 1182-1193 ISSN 1948-5182 (online)
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL
 Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
Resuscitation Before Emergency Surgeries FEIRAN LOU SUNY DOWNSTATE MEDICAL CENTER KINGS COUNTY HOSPITAL Case 73 yo woman h/o HTN three days abdominal pain and nausea. The pain was diffuse, cramp-like,
From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs. Florence Wong University of Toronto. Falk Symposium October 14, 2007
 From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs Florence Wong University of Toronto Falk Symposium October 14, 2007 Sodium Retention in Cirrhosis Occurs as a result of hemodynamic
From Sodium Retention to Therapy for Refractory Ascites The Role for New Drugs Florence Wong University of Toronto Falk Symposium October 14, 2007 Sodium Retention in Cirrhosis Occurs as a result of hemodynamic
Diagnostic Procedures. Measurement of Hepatic venous pressure in management of cirrhosis. Clinician s opinion
 5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
5 th AISF Post-Meeting Course Diagnostic and Therapeutic Invasive Procedures in Hepatology Rome, February 25 th Diagnostic Procedures Measurement of Hepatic venous pressure in management of cirrhosis Clinician
Posthepatectomy Liver Failure. C. Jeske
 Posthepatectomy Liver Failure C. Jeske Introduction Major source of morbidity and mortality after liver resection Devastating complication Little treatment Incidence: 4-19% Recently < 10% Mortality following
Posthepatectomy Liver Failure C. Jeske Introduction Major source of morbidity and mortality after liver resection Devastating complication Little treatment Incidence: 4-19% Recently < 10% Mortality following
EDUCATION PRACTICE. Cirrhosis With Refractory Ascites: Serial Large Volume Paracentesis, TIPS, or Transplantation?
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:931 935 EDUCATION PRACTICE Cirrhosis With Refractory Ascites: Serial Large Volume Paracentesis, TIPS, or Transplantation? VANDANA KHUNGAR* and SAMMY SAAB*,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2011;9:931 935 EDUCATION PRACTICE Cirrhosis With Refractory Ascites: Serial Large Volume Paracentesis, TIPS, or Transplantation? VANDANA KHUNGAR* and SAMMY SAAB*,