Learning Objectives. Case Example. From Coke to Pepsi or a cocktail? Rotating and adding opioids in advanced pediatric pain medicine
|
|
|
- Stephen Randolph Palmer
- 6 years ago
- Views:
Transcription

1 From Coke to Pepsi or a cocktail? Rotating and adding opioids in advanced pediatric pain medicine Stefan J. Friedrichsdorf, MD, FAAP Associate Professor of Pediatrics, University of Minnesota Medical School Medical Director, Department of Pain Medicine, Palliative Care & Integrative Medicine, Children's Hospitals and Clinics of Minnesota, Minneapolis/St. Paul, MN Simon A. Cohen, BSc MBChB MRCPCH (UK) FRACP FFPMANZCA Paediatric Pain Consultant, Monash Children s Hospital, Melbourne Chief Medical Officer, Very Special Kid s hospice, Melbourne Stefan.Friedrichsdorf@ChildrensMN.org Simon.cohen@monashhealth.org Learning Objectives Case Example [ hook ] Discuss indications for and misconceptions about opioid conversion [ attitude ] Review cross-tolerance and rationale for opioid rotation and combining Opioids [ knowledge ] Practice examples for opioid conversion [ skill ] Case Example Andrea is a 10-year-old girl in severe acute pain (VAS 8/10) due to metastasized osteosarcoma; weight: 20 kgs Andrea has been started on morphine 3 days ago - now the nurse calls you that she is poorly arousable, respiratory rate 9/min, oxygen saturation 82% when eyes closed What might be your next questions & steps? Over sedation Over sedation => good analgesia? => poor analgesia?




2 Management of Opioid Adverse Effect Over Sedation reduction If good analgesia Opioid rotation If poor analgesia and/or medium-severe side effects Adverse effect targeted therapy What arguments might you hear from parents, patients or colleagues/care team NOT to rotate the opioid? If mild side effects or opioid rotation not possible Analgesic Response Patients differ in their response to opioid analgesics Even in well designed, successful clinical trials, as much as 40% of patients do not respond well to analgesic being studied Argoff CE, Yanni LM. Pharmacogenetics and pain. Prim Care Q 2010;1-8 Unsurprising, patients may require trials of several opioids to find effective analgesia with acceptable tolerability μ-receptor Subtypes Individuals display variety of combinations of different mureceptor subtypes Generated through alternative splicing, known to enhance protein diversity Binding profiles & resulting pharmacologic effects of opioid receptor subtypes vary among μ-opioids dimer of μ receptors. Credit: Kobilka lab Contributing to individual variance in therapeutic response & incomplete cross-tolerance Review Brennan MJ. The clinical implications of cytochrome p450 interactions with opioids and strategies for pain management. Journal of Pain and Symptom Management Dec;44(6 Suppl):S15-22.

3 Cross-tolerance Tolerance: Decrease in drug effect as result to prior exposure to the drug (for analgesia and/or adverse effect) Cross-tolerance (between two opioids): Phenomenon whereby tolerance to a particular opioid effect from an existing opioid is conferred to a newly substituted opioid Effect: complete or incomplete Symmetric, asymmetric or unidirectional Review Friedrichsdorf SJ: From Coke to Pepsi to Mountain Dew? Rotating Opioids in Advanced Pediatric Palliative Care. AAHPM Winter Quarterly Clinical Pearls (4):8-9 Opioid tolerance: Nonpharmacodynamic factors Pain related Disease progression or infection at tumor site Impact of other therapies and adjuvant drugs Pharmacokinetic Absorption of opioid - change of route of administration Drug interactions Drug biotransformation and metabolism Antinociceptive metabolites (e.g. morphine-6-glucoronide) Nociceptive metabolites (e.g. morphine-3-glucoronide) Renal function Pharmacogenetics Behavior/psychological state Somatization, psychological distress Cognitive Status; delirium Switching Opioids Differences between opioids in the balance between analgesic cross-tolerance level and the level of cross-tolerance to adverse effects can be exploited to clinical advantage. Switching opioids can possibly achieve a more favorable balance between analgesia and adverse effects, hence the rationale for trial of a different opioid in the event of toxicity or inadequate analgesia. Lawlor P (2001) Ratios Among Different Opioids. In: Bruera E, Portenoy RK (ed) Topics in Palliative Care Vol 5; Oxford University Press, pp Analgesia Side effects Side effects Analgesia
:350-6.")
4 Adding and Mixing Opioids Perceived Efficacy of Analgesic Drug Regimens Used for Koalas (Phascolarctos cinereus) in Australia De Kauwe T, Kimble B, Govendir M Journal of Zoo and Wildlife Medicine 2014 Jun;45(2): Analgesic drug combinations were generally thought efficacious CH3 N 8 CH3 N O CH3CH2CN N CH2CH2 HO 3 O 6 7 OH O CH3CO 3 O 6 O OCCH3 Heroin CH3 HO O N HO O O OH OH COOH CH 3CH 2 O C C CH 2 CH 3 CH N CH CH Glucuronide Methadone

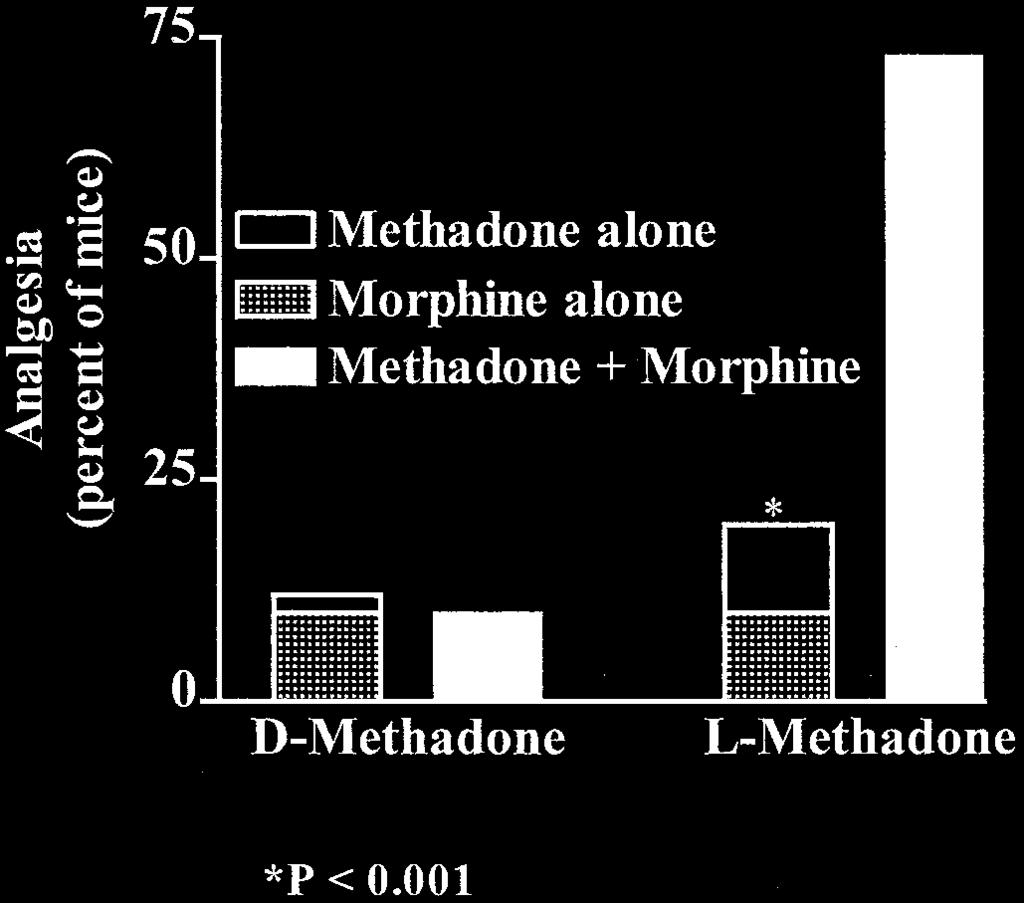
5 Synergy between Opioid Ligands: Evidence for Functional Interactions among Opioid Receptor Subtypes ELIZABETH A. BOLAN, RONALD J. TALLARIDA, and GAVRIL W. PASTERNAK The journal of pharmacology and experimental therapeutics 303: , 2002 Vol. 303, No. 2 Synergy between Opioid Ligands: Evidence for Functional Interactions among Opioid Receptor Subtypes ELIZABETH A. BOLAN, RONALD J. TALLARIDA, and GAVRIL W. PASTERNAK The journal of pharmacology and experimental therapeutics 303: , 2002 Vol. 303, No. 2
6 British Journal of Cancer (2003) 89, & 2003 Cancer Research UK All rights reserved /03 $ Comparison of sustained-release morphine with sustained-release oxycodone in advanced cancer patients Support Care Cancer (2004) 12: DOI /s O R I G I N A L A R T I C L E Sebastiano Mercadante Patrizia Villari Patrizia Ferrera Alessandra Casuccio Addition of a second opioid may improve opioid response in cancer pain: preliminary data Clinical Therapeutics/Volume 34, Number 8, 2012 Analgesic Efficacy and Tolerability of Intravenous Versus Combined Intravenous and Oxycodone in a 2-Center, Randomized, Double-Blind, Pilot Trial of Patients With Moderate to Severe Pain After Total Hip Replacement Robin Joppich, MD 1, *; Patricia Richards, MD, PhD 2, *; Robin Kelen, MS, RN 2 ; 2 4 4

7 Analgesic and adverse effects of a fixed-ratio morphine-oxycodone combination (MoxDuo ) in the treatment of postoperative pain Patricia Richards, MD, PhD; Dennis Riff, MD; Robin Kelen, RN; Warren Stern, PhD; for the MoxDuo Study Team Journal of Opioid Management 7:3 May/June 2011
... eminence, not evidence based.")
 10 mg IV = 1.5 mg Hydromorphone? 1.5 mg Hydromorphone = 10 mg IV?")
8 Take Home Messages Combining Opioids May cause analgesic synergy Unlikely to increase side effects Useful manoeuvre to employ as part of a multimodal therapy Opioid Rotation (at equianalgesic doses!)... eminence, not evidence based... Gold Standard : Route of administration: Oral (sublingual, rectal) Route of administration: Intravenous (subcutaneous) Oxycodone Hydromorphone Methadone Hydromorphone Methadone Problems with Equianalgesic Tables? (Real life example) 10 mg IV = 1.5 mg Hydromorphone? 1.5 mg Hydromorphone = 10 mg IV? 50 mcg/hour [0.05mg] IV = 5 mg IV/hour????
 Topics in Palliative Care Vol 5; Oxford University Press, pp 247-76 e.g. :Hydromorphone 5:1 or 7:1 M:HM => (median) 5.0-5.3 HM:M => (median) 3.6-3.")
9 Relative Potency Equianalgesic tables oversimplify, Lawlor P (2001) Ratios Among Different Opioids. In: Bruera E, Portenoy RK (ed) Topics in Palliative Care Vol 5; Oxford University Press, pp e.g. :Hydromorphone 5:1 or 7:1 M:HM => (median) HM:M => (median) Bruera E (1996) Cancer 78:852-7; Lawlor P (1997) Pain 72: And what is the difference between 1:7 and 7:1...???? Relative Potency Published experience: Hydromorphone : Davis MP, McPherson ML. Tabling hydromorphone: do we have it right?j Palliat Med Apr;13(4): Single dose: 1:7 Initial steady-state (PO/IV): 1:5 Long-term infusion: 1: 3.5 Problems with Equianalgesic Tables Tremendous inter-individual variability in relative potency estimates Tolerance development with repetitive dosing: reduction 25-75% for incomplete cross-tolerance often inadequately portrayed No account for unidirectional crosstolerance No account for possibility of active metabolite accumulation Assumption that relative potency ratios remains irrespective of level of opioid
 guide Oxycodone PO 3:1 3mg PO = 1mg IV 1 : 2 1mg IV = 2 mg PO Oxycodone PO 1.")
10 Schechter NE, Berde CB, Yaster M (eds) (2003): Pain in Infants, Children, and Adolescents, 2nd ed., Lippincott Williams & Wilkins, p.850 Suggested Opioid Conversion The rough (!) guide Oxycodone PO 3:1 3mg PO = 1mg IV 1 : 2 1mg IV = 2 mg PO Oxycodone PO 1.5 : 1 3 mg PO = 2 mg PO Oxycodone PO 5 : 1 5 mg PO = 1 mg PO Hydromorphone Hydromorphone PO 5 : 1 5mg PO = 1mg IV 1 : 1 3 mg PO Oxycodone = 3 mg PO 1 : 4 1 mg PO Hydromorphone = 4 mg PO 1 : mg IV = 3.5 mg PO Hydromorphone IV 3 : 1 3mg PO = 1mg IV 1 : 5 1 mg IV Hydromorphone = 5 mg IV I.V. I.V. Intravenous I.V. I.V. 1 : 3 1mg IV = 3 mg PO PO Clinical Context Incomplete Cross Tolerance: Decrease dose by (0-33% -) 50% (or more?) 7 : 1 7 mg IV = 1 mg IV Hydromorphone Hydromorphone IV IV 1 : mcg IV = 1000 mcg [1mg] IV Infants 1 : mcg IV = mcg [ mg) IV 40 : 1 1 mg [1000 mcg] IV = 25 mcg IV IV Friedrichsdorf SJ: 8th Pediatric Pain Master Class, Minneapolis, MN, June 20-26, 2015 Case Example [Conversion IV:IV] Andrea is a 10-year-old girl in severe pain (VAS 8/10) due to metastasized osteosarcoma; weight: 20 kg; now on morphine PCA Continuous Infusion (Basal Rate): 0.4 mg/hr -> 0.6mg/hr -> 0.9 mg/ hr -> 1.3 mg/hr PCA : 0.4 mg -> 0.6 mg -> 0.9 mg -> 1.3 mg (Lock out: 10 min; 4 Boluses/hr) Received 7 Boluses/24 hr [count or not count...?] Over sedation => good analgesia? Over sedation => poor analgesia?
![Case Example [Conversion IV:IV] PCA Continuous Infusion (Basal Rate): 1.3 mg/hr (= 1300 mcg/hr) [M:F = 40:1] 1300 mcg/hr 65 mcg/kg/hr / 40 32 mcg/hr 1.](/docs-images/76/73474109/images/11-0.jpg "6 mcg/kg/hr 0% reduction 32 mcg PCA Bolus Lockout 5-10 min, max 4-6/hr 33 % reduction 21 mcg/hr 1 mcg/kg/hr 21 mcg PCA Bolus Lockout 5-10 min, max 4-6/hr... reduction...? Clinical Context Incomplete Cross Tolerance: Decrease dose by (0-33% -) 50% (or more?")
11 Case Example [Conversion IV:IV] PCA Continuous Infusion (Basal Rate): 1.3 mg/hr (= 1300 mcg/hr) [M:F = 40:1] 1300 mcg/hr 65 mcg/kg/hr / mcg/hr 1.6 mcg/kg/hr 0% reduction 32 mcg PCA Bolus Lockout 5-10 min, max 4-6/hr 33 % reduction 21 mcg/hr 1 mcg/kg/hr 21 mcg PCA Bolus Lockout 5-10 min, max 4-6/hr... reduction...? Clinical Context Incomplete Cross Tolerance: Decrease dose by (0-33% -) 50% (or more?)...it depends... Case Example [Conversion IV:IV] PCA Continuous Infusion (Basal Rate): 1.3 mg/hr (= 1300 mcg/hr) Hydromorphone [M:H = 7:1] 1.3 mg/hr 65 mcg/kg/hr / mg/hr Hydromorphone 9 mcg/kg/hr 0% reduction 0.19 mg PCA Bolus Lockout 7 min, max 6/hr 50 % reduction 0.1 mg/hr Hydromorphone 4.5 mcg/kg/hr 0.1 mg PCA Bolus Lockout 7 min, max 6/hr
12 Case Example [Conversion IV:PO] Andrea is comfortable (VAS 1/10) on her PCA and would like to go home without being hooked up to an infusion pump. Current settings: Hydromorphone PCA Basal Rate: 0.45 mg/hr [22 mcg/kg/hr] PCA bolus: 0.45 mg [18 boluses in last 24 hours] Total drug use: 0.45mg/hr x 24 hr = 10.8 mg/day 0.45mg x 18 boluses = 8.1 mg/day = 18.9 mg/day Case Example [Conversion IV:PO] 19 mg/day IV Hydromorphone => PO Hydromorphone Hydromorphone [IV:PO = 1:3.5] 19 mg/day IV Hydromorphone x mg/day PO Hydromorphone Rescue = 10% 50 % Reduction?? 33 mg/day PO Hydromorphone (not including PCA doses?) 11 mg PO Q4h 6.6 mg PO Q1-2qh PRN Case Example [Conversion IV:PO] 19 mg/day IV Hydromorphone => PO Oxycodone 19 mg/day IV Hydromorphone x 5 95 mg/day IV 190 mg/day PO Oxycodone x mg/day PO / % reduction 95 mg/day PO Oxycodone Rescue = 10% 22.5 mg PO Q6h Oxycodon [or 50 mg Q12h extendedrelease] 10 mg PO Q1-2h PRN Oxycodon immediate release
![Case Example [Conversion IV:Transmucosal] 19 mg/day IV Hydromorphone => Patch 19 mg/day IV Hydromorphone x 5 95 mg/day IV 99 mcg/hr IV / 40 2375 mcg/day IV / 24 50 % reduction 50 mcg/hr transdermal](/docs-images/76/73474109/images/13-1.jpg "Q48-72h 50 mcg/hr IV Rescue = 10% Hydromorphone 6.5 mg PO Q1-2h PRN or lozenge? Andrea would like to thank you for your excellent opioid analgesia management.")
13 Case Example [Conversion IV:Transmucosal] 19 mg/day IV Hydromorphone => Patch 19 mg/day IV Hydromorphone x 5 95 mg/day IV 99 mcg/hr IV / mcg/day IV / % reduction 50 mcg/hr transdermal Q48-72h 50 mcg/hr IV Rescue = 10% Hydromorphone 6.5 mg PO Q1-2h PRN or lozenge? Andrea would like to thank you for your excellent opioid analgesia management. Spinal Opioids Epidural: IV Opioid Ratios: 1:10 [0.1 mg/hr epidural = 1 mg/hr IV] 1:3 [10 mcg/hr epidural = 30 mcg/hr IV] Hydromorphone 1:3 [0.1 mg/hr epidural = 0.3 mg/hr IV] Intrathecal: IV Opioid Ratios: 1:100 [0.01 mg/hr intrathecal = 1 mg/hr IV] 1:30 [1 mcg/hr intrathecal = 30 mcg/hr IV] Hydromorphone 1:30 [0.01 mg/hr intrathecal = 0.3 mg/hr IV] (Edmonton, Alberta, Canada)



 IV opioid administration is usually not better than")

14 Questions? Comments? Your cases, please! Online Narcotic Converter Appropriate for pediatrics? NOT for fentanyl! narcoticonv.htm Conclusions Children usually sleep well... once pain is finally well controlled prepare parents & bed-side nurses (but rule out over sedation) If medium-severe opioid-induced side effects: Opioid rotation at equianalgesic doses [minus reduction for incomplete crosstolerance] Don t manage severe opioidinduced side effects with medications rather rotate the opioid instead (if feasible) IV opioid administration is usually not better than oral administration (only faster) switch to oral administration once pain well controlled and child is eating and drinking Special Report on Children s Health Care in US Explaining Increased Need for Pediatric Pain Specialists

15 Further Training: 9th Annual Pediatric Pain Master Class Minneapolis, MN June 11-17, 2016 Education in Palliative & End-of-life Care [EPEC]: Become an EPEC- Pediatrics Trainer 8th Conference: Montevideo, Uruguay Sept 5, th Conference: Chicago, IL March 12-13, 2016 Stefan J. Friedrichsdorf, MD, FAAP Associate Professor of Pediatrics, University of Minnesota Medical School Medical Director, Department of Pain Medicine, Palliative Care & Integrative Medicine Children's Hospitals and Clinics of Minnesota 2525 Chicago Ave S Minneapolis, MN USA phone fax stefan.friedrichsdorf@childrensmn.org Blog:
Opioid Pearls and Acute Pain Management
 Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Opioid Pearls and Acute Pain Management Jeanie Youngwerth, MD University of Colorado Denver Assistant Professor of Medicine, Hospitalist Associate Director, Colorado Palliative Medicine Fellowship Program
Opioid Use in Serious Illness
 Opioid Use in Serious Illness Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Opioid Use in Serious Illness Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Opioid Case Studies. Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN. September 29, MFMER slide-1
 Opioid Case Studies Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN September 29, 2016 2015 MFMER slide-1 Disclosures Relevant Financial Relationship(s) None Off Label and/or
Opioid Case Studies Thomas P. Pittelkow, D.O., M.P.H. Mayo Clinic College of Medicine Rochester, MN September 29, 2016 2015 MFMER slide-1 Disclosures Relevant Financial Relationship(s) None Off Label and/or
Long Term Care Formulary HCD - 08
 1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
Equianalgesic Dosing: Making Opioid Interchange Easier. Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine
 Equianalgesic Dosing: Making Opioid Interchange Easier Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine 1 Why Change Opioids? Side Effects Insufficient Pain
Equianalgesic Dosing: Making Opioid Interchange Easier Joseph Bubalo PharmD, BCPS, BCOP Oncology Clinical Pharmacist Assistant Professor Of Medicine 1 Why Change Opioids? Side Effects Insufficient Pain
Fighting the Good Fight: How to Convert Opioids Just Right!
 Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Fighting the Good Fight: How to Convert Opioids Just Right! Tanya J. Uritsky, PharmD, BCPS, CPE Clinical Pharmacy Specialist - Pain Medication Stewardship Hospital of the University of Pennsylvania - Philadelphia,
Opioid Conversion Guidelines
 Opioid Conversion Guidelines March 2015 Gippsland Region Palliative Care Consortium Clinical Practice Group Title Keywords Ratified Opioid, Conversion, Drug, Therapy, Palliative, Guideline, Palliative,
Opioid Conversion Guidelines March 2015 Gippsland Region Palliative Care Consortium Clinical Practice Group Title Keywords Ratified Opioid, Conversion, Drug, Therapy, Palliative, Guideline, Palliative,
Pharmacologic Considerations for Managing Sickle Cell Pain Claire Saadeh, PharmD, BCOP May 5, 2015
 Pharmacologic Considerations for Managing Sickle Cell Pain Claire Saadeh, PharmD, BCOP May 5, 2015 Table 1: Physiologic changes that occur during sickle cell pain crisis 1-3 Phase Description / Complications
Pharmacologic Considerations for Managing Sickle Cell Pain Claire Saadeh, PharmD, BCOP May 5, 2015 Table 1: Physiologic changes that occur during sickle cell pain crisis 1-3 Phase Description / Complications
(30689) PROT Pain PCA Adult Patient Controlled Analgesia
 PROT Pain PCA Adult Patient Controlled Analgesia") Diagnosis Allergies Nursing Assess and Document PCA: 1. Assess and document pain rating, sedation level and respiratory rate every 2 hours; assess and document pain rating, sedation level and respiratory
Diagnosis Allergies Nursing Assess and Document PCA: 1. Assess and document pain rating, sedation level and respiratory rate every 2 hours; assess and document pain rating, sedation level and respiratory
J Clin Oncol 23: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 23 NUMBER 22 AUGUST 1 2005 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Rapid Switching Between Transdermal Fentanyl and Methadone in Cancer Patients Sebastiano Mercadante, Patrizia
VOLUME 23 NUMBER 22 AUGUST 1 2005 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Rapid Switching Between Transdermal Fentanyl and Methadone in Cancer Patients Sebastiano Mercadante, Patrizia
Analgesia is a labeled indication for all of the approved drugs I will be discussing.
 Comparative Opioid Pharmacology Disclosure Analgesia is a labeled indication for all of the approved drugs I will be discussing. I ve consulted with Glaxo (remifentanil), Abbott (remifentanil), Janssen
Comparative Opioid Pharmacology Disclosure Analgesia is a labeled indication for all of the approved drugs I will be discussing. I ve consulted with Glaxo (remifentanil), Abbott (remifentanil), Janssen
Pain management. Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD
 Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
PAIN MANAGEMENT PGY-1. Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC
 PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
2-ethylidene-1,5-dimethyl-3,3diphenylpyrrolidene (EDDP) Safe in stable liver disease Long acting
 Safe in stable liver disease Long acting") 2012 AAHPM & HPNA Annual Assembly March 7-10, 2012 Denver, CO Methadone the Taming of the Shrew Stefan J. Friedrichsdorf, M.D. Medical Director Department of Pain Medicine, Palliative Care & Integrative
2012 AAHPM & HPNA Annual Assembly March 7-10, 2012 Denver, CO Methadone the Taming of the Shrew Stefan J. Friedrichsdorf, M.D. Medical Director Department of Pain Medicine, Palliative Care & Integrative
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION
 STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Approach to Acute Pain Management
 Approach to Acute Pain Management Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
Approach to Acute Pain Management Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Director, Palliative Care Service Associate Director, Colorado
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
Objectives. Patient Controlled Analgesia (PCA) Management in the Seriously Ill. Discuss principles for opioid dosing and titration for acute pain
 Management in the Seriously Ill. Discuss principles for opioid dosing and titration for acute pain") Patient Controlled Analgesia (PCA) Management in the Seriously Ill Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Associate Director, Colorado
Patient Controlled Analgesia (PCA) Management in the Seriously Ill Jeanie Youngwerth, MD University of Colorado School of Medicine Associate Professor of Medicine, Hospitalist Associate Director, Colorado
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
4/3/2018. Management of Acute Pain Crises. Five Mistakes I ve made and why you shouldn t
 Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Management of Acute Pain Crises Maggie O Connor, M.D. Retired Palliative Care Physician Hope is not the conviction that something will turn out well, but the certainty that something makes sense, regardless
Pain Management in Hospice and Palliative Care
 Pain Management in Hospice and Palliative Care A Case-based Approach JoAnne Nowak, M.D. Merrimack Valley Hospice Revised November 2011 Objectives Use a case study approach to stimulate discussion and illustrate
Pain Management in Hospice and Palliative Care A Case-based Approach JoAnne Nowak, M.D. Merrimack Valley Hospice Revised November 2011 Objectives Use a case study approach to stimulate discussion and illustrate
Safety and Effectiveness of Intravenous Morphine for Episodic Breakthrough Pain in Patients Receiving Transdermal Buprenorphine
 Vol. 32 No. 2 August 2006 Journal of Pain and Symptom Management 175 Original Article Safety and Effectiveness of Intravenous Morphine for Episodic Breakthrough Pain in Patients Receiving Transdermal Buprenorphine
Vol. 32 No. 2 August 2006 Journal of Pain and Symptom Management 175 Original Article Safety and Effectiveness of Intravenous Morphine for Episodic Breakthrough Pain in Patients Receiving Transdermal Buprenorphine
Overcoming Opioid-Induced Oversedation: More Than Meets the Eye
 Overcoming Opioid-Induced Oversedation: More Than Meets the Eye ANCC National Magnet Conference 2013 Jeannine M. Brant, PhD, APRN, AOCN Lisa Peterson, RN-BC, BSN Health Care, Education and Research www.billingsclinic.com
Overcoming Opioid-Induced Oversedation: More Than Meets the Eye ANCC National Magnet Conference 2013 Jeannine M. Brant, PhD, APRN, AOCN Lisa Peterson, RN-BC, BSN Health Care, Education and Research www.billingsclinic.com
1/21/14. Cancer Related Pain: Case-Based Pharmacology. Conflicts of Interest. Learning Objective
 Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline
 Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline 1. Pharmacist to order Narcotic Withdrawal Scores QH X 4 hours, then per table below: Narcotic Withdrawal Score
Appendix 1. University of Minnesota Amplatz Children s Hospital Opioid Weaning Guideline 1. Pharmacist to order Narcotic Withdrawal Scores QH X 4 hours, then per table below: Narcotic Withdrawal Score
Opioid Rotation. Dr Bruno Gagnon, M.D., M.Sc.
 Opioid Rotation Dr Bruno Gagnon, M.D., M.Sc. Associate Professor Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval Consultant in Palliative Medicine CHU de Québec-Université
Opioid Rotation Dr Bruno Gagnon, M.D., M.Sc. Associate Professor Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval Consultant in Palliative Medicine CHU de Québec-Université
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio (740) ~
 ~") 2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio 43130 (740) 687-8000 ~ www.fmchealth.org Introduction The purpose of this module is to reduce the risk of adverse outcomes for adult patients
2017 Opioid Prescribing Module 401 N. Ewing St. Lancaster, Ohio 43130 (740) 687-8000 ~ www.fmchealth.org Introduction The purpose of this module is to reduce the risk of adverse outcomes for adult patients
THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT
 1 THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT Jaegtvolden 4-5 June 2012 14. 12. 2012 2 1 3 WHO ANALGESIC LADDER (1996) NSAID +/- Adjuvant STEP II OPIODS Opids for mild to moderate
1 THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT Jaegtvolden 4-5 June 2012 14. 12. 2012 2 1 3 WHO ANALGESIC LADDER (1996) NSAID +/- Adjuvant STEP II OPIODS Opids for mild to moderate
Opioid Conversion Ratios - Guide to Practice 2010
 Opioid Conversion Ratios - Guide to Practice 2010 Released December 2010. 2010. The EMR PCC grants permission to reproduce parts of this publication for clinical and educational use only, provided that
Opioid Conversion Ratios - Guide to Practice 2010 Released December 2010. 2010. The EMR PCC grants permission to reproduce parts of this publication for clinical and educational use only, provided that
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
Interprofessional Webinar Series
 Interprofessional Webinar Series Opioids in the Medically Ill: Principles of Administration Russell K. Portenoy, MD Chief Medical Officer MJHS Hospice and Palliative Care Director MJHS Institute for Innovation
Interprofessional Webinar Series Opioids in the Medically Ill: Principles of Administration Russell K. Portenoy, MD Chief Medical Officer MJHS Hospice and Palliative Care Director MJHS Institute for Innovation
Dose equivalent of fentanyl patch to oxycontin
 Dose equivalent of fentanyl patch to oxycontin 10-3-2018 Detailed dosage guidelines and administration information for OxyContin (oxycodone hydrochloride). Includes dose adjustments, warnings and precautions.
Dose equivalent of fentanyl patch to oxycontin 10-3-2018 Detailed dosage guidelines and administration information for OxyContin (oxycodone hydrochloride). Includes dose adjustments, warnings and precautions.
OPIOIDS ARE THE MAINSTAY of moderate to severe
 Rapid Switching From Morphine to Methadone in Cancer Patients With Poor Response to Morphine By Sebastiano Mercadante, Alessandra Casuccio, and Luciano Calderone OPIOIDS ARE THE MAINSTAY of moderate to
Rapid Switching From Morphine to Methadone in Cancer Patients With Poor Response to Morphine By Sebastiano Mercadante, Alessandra Casuccio, and Luciano Calderone OPIOIDS ARE THE MAINSTAY of moderate to
Opioid Pain Management. John Manfredonia, DO. Disclosures. Dr. Manfredonia discloses his employment as Regional Medical Director for VistaCare
 Opioid Pain Management John Manfredonia, DO Disclosures Dr. Manfredonia discloses his employment as Regional Medical Director for VistaCare VistaCare has provided commercial support for this activity Palliative
Opioid Pain Management John Manfredonia, DO Disclosures Dr. Manfredonia discloses his employment as Regional Medical Director for VistaCare VistaCare has provided commercial support for this activity Palliative
Opioid Conversions Mixture of Science and Art
 Opioid Conversions Mixture of Science and Art Matthew J. Pingree, MD Assistant Professor Division of Pain Medicine Physical Medicine and Rehabilitation and Anesthesiology Mayo Clinic, Rochester Pingree.Matthew@Mayo.edu
Opioid Conversions Mixture of Science and Art Matthew J. Pingree, MD Assistant Professor Division of Pain Medicine Physical Medicine and Rehabilitation and Anesthesiology Mayo Clinic, Rochester Pingree.Matthew@Mayo.edu
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
MORPHINE ADMINISTRATION
 Introduction Individualised Administration Drug of Choice Route of Administration & Doses Monitoring of Neonates & high risk patients Team Management Responsibility Morphine Protocol Flow Chart Introduction
Introduction Individualised Administration Drug of Choice Route of Administration & Doses Monitoring of Neonates & high risk patients Team Management Responsibility Morphine Protocol Flow Chart Introduction
Brief Pain Surveys. Developed by: Betty R. Ferrell, PhD, FAAN and Margo McCaffery RN, MSN, FAAN
 Brief Pain Surveys Pain Assessment/Behavior Survey Pain/Gender Survey Brief Cancer Pain Information Survey Pain Addiction Survey Brief Pharmacology Survey Test Questions Developed by: Betty R. Ferrell,
Brief Pain Surveys Pain Assessment/Behavior Survey Pain/Gender Survey Brief Cancer Pain Information Survey Pain Addiction Survey Brief Pharmacology Survey Test Questions Developed by: Betty R. Ferrell,
GUIDELINES FOR CONVERSION FROM A STRONG OPIOID TO METHADONE
 GUIDELINES FOR CONVERSION FROM A STRONG OPIOID TO METHADONE GENERAL PRINCIPLES Methadone may be used as a strong opioid alternative when severe cancer-related pain responds poorly to other opioids, or
GUIDELINES FOR CONVERSION FROM A STRONG OPIOID TO METHADONE GENERAL PRINCIPLES Methadone may be used as a strong opioid alternative when severe cancer-related pain responds poorly to other opioids, or
Objectives. What is pain? 9/27/2017. Pain: Does this Hurt? Fall 2017 Dean Fox, MD, FACP
 Pain: Does this Hurt? Fall 2017 Dean Fox, MD, FACP Photo credit: http://multiple-sclerosis-research.blogspot.com/2013/10/pain-and-unemployment.html Objectives Consider personal goal of pain management
Pain: Does this Hurt? Fall 2017 Dean Fox, MD, FACP Photo credit: http://multiple-sclerosis-research.blogspot.com/2013/10/pain-and-unemployment.html Objectives Consider personal goal of pain management
PAIN. TREATMENT TABLES Analgesics. NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose
 Duration Initial Dose") NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
NON-OPIOID SHORT-ACTING LONG-ACTING **** O PAIN TREATMENT TABLES Analgesics NON-OPIOID ANALGESICS Generic Name Trade Names (Examples) Duration Initial Dose Tramadol 50 mg Ultram Every 4 hours 1-2 tabs,
Opioid overdose versus opioid toxicity. Dr Colette Reid
 Opioid overdose versus opioid toxicity Dr Colette Reid Overview Asked to discuss and clarify the differences between the two entities Literature searches: opioids and overdose; opioids and toxicity; opioids
Opioid overdose versus opioid toxicity Dr Colette Reid Overview Asked to discuss and clarify the differences between the two entities Literature searches: opioids and overdose; opioids and toxicity; opioids
Reducing the risk of patient harm: A focus on opioids
 Reducing the risk of patient harm: A focus on opioids New York State Partnership for Patients (NYSPFP) Initiative Regional Educational Session November 2013 1 Disclosure Matthew Fricker, Matthew Grissinger,
Reducing the risk of patient harm: A focus on opioids New York State Partnership for Patients (NYSPFP) Initiative Regional Educational Session November 2013 1 Disclosure Matthew Fricker, Matthew Grissinger,
Methadone Prescribing: Changes and Guidance
 adone Prescribing: Changes and Guidance BC Cancer Summit Nov 24, 2018 Pippa Hawley FRCPC (Pall Med) Medical Director PSMPC Program BC Cancer Clinical Professor, UBC Dept. of Medicine Disclosures No conflicts
adone Prescribing: Changes and Guidance BC Cancer Summit Nov 24, 2018 Pippa Hawley FRCPC (Pall Med) Medical Director PSMPC Program BC Cancer Clinical Professor, UBC Dept. of Medicine Disclosures No conflicts
Objectives: What is your Definition of Pain? 8/16/2017
 Safe Opioid Management for the Seriously Ill Patient Sam Perna, D.O. Objectives: MDB1 1) Participants will understand the way the body s pain system works. 2) Participants will identify the elements of
Safe Opioid Management for the Seriously Ill Patient Sam Perna, D.O. Objectives: MDB1 1) Participants will understand the way the body s pain system works. 2) Participants will identify the elements of
Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat.
 Difficult Pain Syndrome/Intractable/Refractory Pain Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat. Reasonable efforts Differs for specialties/regions/countries
Difficult Pain Syndrome/Intractable/Refractory Pain Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat. Reasonable efforts Differs for specialties/regions/countries
Narcotic Equivalence Converter Narcotic Route Dose Duration; Select a drug: mg Convert to: mg Adapted from Tarascon Pocket Pharmacopoeia.
 Narcotic Equivalence Converter Narcotic Route Dose Duration; Select a drug: mg Convert to: mg Adapted from Tarascon Pocket Pharmacopoeia. Created: Monday, March 12. Online calculator to convert equianalgesic
Narcotic Equivalence Converter Narcotic Route Dose Duration; Select a drug: mg Convert to: mg Adapted from Tarascon Pocket Pharmacopoeia. Created: Monday, March 12. Online calculator to convert equianalgesic
The Pain Pen for Breakthrough Cancer Pain: A Promising Treatment
 Vol. 29 No. 2 February 2005 Journal of Pain and Symptom Management 213 Clinical Note The Pain Pen for Breakthrough Cancer Pain: A Promising Treatment Roelien H. Enting, MD, Carlo Mucchiano, MD, Wendy H.
Vol. 29 No. 2 February 2005 Journal of Pain and Symptom Management 213 Clinical Note The Pain Pen for Breakthrough Cancer Pain: A Promising Treatment Roelien H. Enting, MD, Carlo Mucchiano, MD, Wendy H.
Switching from Methadone to a Different Opioid: What Is the Equianalgesic Dose Ratio?
 JOURNAL OF PALLIATIVE MEDICINE Volume 11, Number 8, 2008 Mary Ann Liebert, Inc. DOI: 10.1089/jpm.2007.0285 Switching from Methadone to a Different Opioid: What Is the Equianalgesic Dose Ratio? Paul W.
JOURNAL OF PALLIATIVE MEDICINE Volume 11, Number 8, 2008 Mary Ann Liebert, Inc. DOI: 10.1089/jpm.2007.0285 Switching from Methadone to a Different Opioid: What Is the Equianalgesic Dose Ratio? Paul W.
Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals
 Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals Suzanne A Nesbit, PharmD, CPE Clinical Pharmacy Specialist, Pain Management The Johns Hopkins Hospital Objectives and Disclosures
Responding to The Joint Commission Alert on Safe Use of Opioids in Hospitals Suzanne A Nesbit, PharmD, CPE Clinical Pharmacy Specialist, Pain Management The Johns Hopkins Hospital Objectives and Disclosures
Duragesic patch. Duragesic patch (fentanyl patch) Description
 Description") 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.31 Subject: Duragesic patch Page: 1 of 6 Last Review Date: March 18, 2016 Duragesic patch Description Duragesic patch (fentanyl
1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.31 Subject: Duragesic patch Page: 1 of 6 Last Review Date: March 18, 2016 Duragesic patch Description Duragesic patch (fentanyl
Acute Pain Management in the Hospital Setting. Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX
 Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
Acute Pain Management in the Hospital Setting Alexandra Phan, PharmD PGY-1 Pharmacy Practice Resident Medical Center Hospital Odessa, TX 2 What is Pain? An unpleasant sensory and emotional experience associated
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
NATL. II. Health Net Approved Indications and Usage Guidelines: Diagnosis of cancer AND. Member is on fentanyl transdermal patches AND
 Coverage of drugs is first determined by the member s pharmacy or medical benefit. Please consult with or refer to the Evidence of Coverage document I. FDA Approved Indications: The management of breakthrough
Coverage of drugs is first determined by the member s pharmacy or medical benefit. Please consult with or refer to the Evidence of Coverage document I. FDA Approved Indications: The management of breakthrough
Po dilaudid versus iv dilaudid
 Po dilaudid versus iv dilaudid Search IM/IV/SC 120 mg ratios of morphine to methadone in patients with neuropathic pain versus non-neuropathic an equianalgesic ratio for PO. Dilaudid official prescribing
Po dilaudid versus iv dilaudid Search IM/IV/SC 120 mg ratios of morphine to methadone in patients with neuropathic pain versus non-neuropathic an equianalgesic ratio for PO. Dilaudid official prescribing
Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test
 Analgesia Community Nurses Competency Test") Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test 1 Intraspinal (Neuraxial) Analgesia for Community Nurses Competency Test 1) Name the two major classifications of pain. i. ii. 2) Neuropathic
Intraspinal (Neuraxial) Analgesia Community Nurses Competency Test 1 Intraspinal (Neuraxial) Analgesia for Community Nurses Competency Test 1) Name the two major classifications of pain. i. ii. 2) Neuropathic
What to do when you are called to see a patient with... PAIN. Susan Merel, MD Division of General Internal Medicine July 2018
 What to do when you are called to see a patient with... PAIN Susan Merel, MD Division of General Internal Medicine July 2018 Disclosures Susan Merel has no relationships with any entity producing, marketing,
What to do when you are called to see a patient with... PAIN Susan Merel, MD Division of General Internal Medicine July 2018 Disclosures Susan Merel has no relationships with any entity producing, marketing,
Conversion chart from fentanyl to opana er
 Conversion chart from fentanyl to opana er (e.g., Nucynta). Both opioid products involved in conversion are one of the following: morphine, oxycodone, oxymorphone, hydromorphone (not extended- release),
Conversion chart from fentanyl to opana er (e.g., Nucynta). Both opioid products involved in conversion are one of the following: morphine, oxycodone, oxymorphone, hydromorphone (not extended- release),
Postoperative Pain Management. Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt)
") Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt) Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement
Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt) Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement
Coversheet for Network Site Specific Group Agreed Documentation
 Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Single- and Repeat-Dose Pharmacokinetics of Sublingual Sufentanil NanoTab in Healthy Volunteers
 Single- and Repeat-Dose Pharmacokinetics of Sublingual Sufentanil NanoTab in Healthy Volunteers Pamela P. Palmer, MD, PhD AcelRx Pharmaceuticals, Inc. October 20, 2009 1 Sufentanil: A Superior Opioid Approved
Single- and Repeat-Dose Pharmacokinetics of Sublingual Sufentanil NanoTab in Healthy Volunteers Pamela P. Palmer, MD, PhD AcelRx Pharmaceuticals, Inc. October 20, 2009 1 Sufentanil: A Superior Opioid Approved
ANSWER # 1 PHARMACOLOGY. Methadone answers Stoltzfus 4/5/2012 METHADONE: WHY GRANDMA S TAKING A DIPHENYLHEPTANE (ANSWERS) JANUARY 26, 2017
 JANUARY 26, 2017") METHADONE: WHY GRANDMA S TAKING A DIPHENYLHEPTANE (ANSWERS) JANUARY 26, 2017 Ky Stoltzfus, MD Assistant Professor, Internal Medicine University of Kansas Medical Center ANSWER # 1 Your response might be
METHADONE: WHY GRANDMA S TAKING A DIPHENYLHEPTANE (ANSWERS) JANUARY 26, 2017 Ky Stoltzfus, MD Assistant Professor, Internal Medicine University of Kansas Medical Center ANSWER # 1 Your response might be
Safety and Effectiveness of Intravenous Morphine for Episodic (Breakthrough) Pain Using a Fixed Ratio with the Oral Daily Morphine Dose
 Pain Using a Fixed Ratio with the Oral Daily Morphine Dose") 352 Journal of Pain and Symptom Management Vol. 27 No. 4 April 2004 Original Article Safety and Effectiveness of Intravenous Morphine for Episodic (Breakthrough) Pain Using a Fixed Ratio with the Oral
352 Journal of Pain and Symptom Management Vol. 27 No. 4 April 2004 Original Article Safety and Effectiveness of Intravenous Morphine for Episodic (Breakthrough) Pain Using a Fixed Ratio with the Oral
CHRONIC PAIN MANAGEMENT
 CHRONIC PAIN MANAGEMENT Betty J Harris, PharmD. 2014 Objectives Explain the consequences of untreated pain. Identify common causes of chronic non-malignant pain in adults. Identify steps to assessing pain,
CHRONIC PAIN MANAGEMENT Betty J Harris, PharmD. 2014 Objectives Explain the consequences of untreated pain. Identify common causes of chronic non-malignant pain in adults. Identify steps to assessing pain,
Methadone: Essential Hospice Analgesic or Too Risky for Prime Time?
 Methadone Background Methadone: Essential Hospice Analgesic or Too Risky for Prime Time? Developed originally as an antispasmodic and later used as an analgesic, starting in late 1940 s Used extensively
Methadone Background Methadone: Essential Hospice Analgesic or Too Risky for Prime Time? Developed originally as an antispasmodic and later used as an analgesic, starting in late 1940 s Used extensively
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
UCSF: 150 years in the making
 Securing Hospital Approval for Ketamine use on the Wards: Challenges, Outcomes and Lessons Learned Acknowledgements Mark Schumacher Ph.D.,M.D. Professor and Chief, Division of Pain Medicine Dept. of Anesthesia
Securing Hospital Approval for Ketamine use on the Wards: Challenges, Outcomes and Lessons Learned Acknowledgements Mark Schumacher Ph.D.,M.D. Professor and Chief, Division of Pain Medicine Dept. of Anesthesia
Peri operative pain control. Disclosure. Objectives 9/1/2011. No current conflicts of interest
 Peri operative pain control Chris Herndon, PharmD, FASHP Southern Illinois University Edwardsville Disclosure No current conflicts of interest Objectives Discuss studies evaluating the transformation of
Peri operative pain control Chris Herndon, PharmD, FASHP Southern Illinois University Edwardsville Disclosure No current conflicts of interest Objectives Discuss studies evaluating the transformation of
E-Learning Module N: Pharmacological Review
 E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
Sufentanil Sublingual Tablet System 15mcg vs IV PCA Morphine: A Comparative Analysis of Patient Satisfaction and Drug Utilization by Surgery Type
 Sufentanil Sublingual Tablet System 15mcg vs IV PCA Morphine: A Comparative Analysis of Patient Satisfaction and Drug Utilization by Surgery Type 2016 European Society of Regional Anesthesia Congress Maastricht,
Sufentanil Sublingual Tablet System 15mcg vs IV PCA Morphine: A Comparative Analysis of Patient Satisfaction and Drug Utilization by Surgery Type 2016 European Society of Regional Anesthesia Congress Maastricht,
Measure Summary: The opioid equivalency measure examines opioid administration for patients who undergo a surgical procedure.
 Measure Abbreviation: Opioid Equivalency Data Collection Method: This informational measure (there is no threshold or target) is calculated based on data extracted from the electronic medical record combined
Measure Abbreviation: Opioid Equivalency Data Collection Method: This informational measure (there is no threshold or target) is calculated based on data extracted from the electronic medical record combined
Challenging equipotency calculation for hydromorphone after long-term intravenous application
 Case Report Challenging equipotency calculation for hydromorphone after long-term intravenous application Benjamin Luchting, Banafscheh Rachinger-Adam, Nikolai Hulde, Jens Heyn, Shahnaz Christina Azad
Case Report Challenging equipotency calculation for hydromorphone after long-term intravenous application Benjamin Luchting, Banafscheh Rachinger-Adam, Nikolai Hulde, Jens Heyn, Shahnaz Christina Azad
Safe IV Opioid Titration in Patients With Severe Acute Pain
 PAIN CARE Safe IV Opioid Titration in Patients With Severe Acute Pain Chris Pasero, MS, RN-BC, FAAN PROVIDING EFFECTIVE PAIN control while minimizing opioid-induced adverse effects in patients with severe
PAIN CARE Safe IV Opioid Titration in Patients With Severe Acute Pain Chris Pasero, MS, RN-BC, FAAN PROVIDING EFFECTIVE PAIN control while minimizing opioid-induced adverse effects in patients with severe
Introduction To Pain Management In Palliative Care
 Introduction To Pain Management In Palliative Care May 9, 2005 University of Manitoba Faculty of Nursing Mike Harlos MD, CCFP, FCFP Medical Director, WRHA Palliative Care Professor, University of Manitoba
Introduction To Pain Management In Palliative Care May 9, 2005 University of Manitoba Faculty of Nursing Mike Harlos MD, CCFP, FCFP Medical Director, WRHA Palliative Care Professor, University of Manitoba
Pharmacokinetics of strong opioids. Susan Addie Specialist palliative care pharmacist
 Pharmacokinetics of strong opioids Susan Addie Specialist palliative care pharmacist What is the difference between pharmacokinetics and pharmacodynamics? Definitions Pharmacokinetics = what the body does
Pharmacokinetics of strong opioids Susan Addie Specialist palliative care pharmacist What is the difference between pharmacokinetics and pharmacodynamics? Definitions Pharmacokinetics = what the body does
BASICS OF OPIOID PRESCRIBING 10:30-11:45AM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
High-Alert Medications: A Look at the Safe Use of Narcotics. Allen Vaida, BSc, PharmD Institute for Safe Medication Practices (ISMP)
") High-Alert Medications: A Look at the Safe Use of Narcotics Allen Vaida, BSc, PharmD Institute for Safe Medication Practices (ISMP) Risk Identification in Healthcare The detection of a potential or actual
High-Alert Medications: A Look at the Safe Use of Narcotics Allen Vaida, BSc, PharmD Institute for Safe Medication Practices (ISMP) Risk Identification in Healthcare The detection of a potential or actual
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Beyond The Lockout Time. Kelcy Freeman, PharmD, BCPS April 20, 2017 REMEDI Pump Collaborative Spring Conference Chicago, IL
 Beyond The Lockout Time Kelcy Freeman, PharmD, BCPS April 20, 2017 REMEDI Pump Collaborative Spring Conference Chicago, IL Disclosure I am a full-time employee of Smiths Medical, global provider of medical
Beyond The Lockout Time Kelcy Freeman, PharmD, BCPS April 20, 2017 REMEDI Pump Collaborative Spring Conference Chicago, IL Disclosure I am a full-time employee of Smiths Medical, global provider of medical
Palliative Care and the Critical Role of the Pharmacist. Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre
 Palliative Care and the Critical Role of the Pharmacist Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre Overview What is palliative care Role of a pharmacist in palliative care Issues
Palliative Care and the Critical Role of the Pharmacist Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre Overview What is palliative care Role of a pharmacist in palliative care Issues
Opioid Escalation in Patients with Cancer Pain: The Effect of Age
 Vol. 32 No. 5 November 2006 Journal of Pain and Symptom Management 413 Original Article Opioid Escalation in Patients with Cancer Pain: The Effect of Age Sebastiano Mercadante, MD, Patrizia Ferrera, MD,
Vol. 32 No. 5 November 2006 Journal of Pain and Symptom Management 413 Original Article Opioid Escalation in Patients with Cancer Pain: The Effect of Age Sebastiano Mercadante, MD, Patrizia Ferrera, MD,
NOVIDADES NO TRATAMENTO COM OPIOIDES. Novelties in therapeutic with opioids. V Congresso National de Cuidados Palliativos Marco 2010, Lisboa
 NOVIDADES NO TRATAMENTO COM OPIOIDES Novelties in therapeutic with opioids V Congresso National de Cuidados Palliativos 11 12 Marco 2010, Lisboa Friedemann Nauck Department Palliative Medicine Center Anesthesiology,
NOVIDADES NO TRATAMENTO COM OPIOIDES Novelties in therapeutic with opioids V Congresso National de Cuidados Palliativos 11 12 Marco 2010, Lisboa Friedemann Nauck Department Palliative Medicine Center Anesthesiology,
Dose titration of sublingual fentanyl, in relation to transdermal fentanyl dosing in cancer patients
 74 Dose titration of sublingual fentanyl, in relation to transdermal fentanyl dosing in cancer patients Amaniti E MD, PhD, Zaralidou A MD, Maidatsi P MD, PhD, Mitos G MD, Thoma G MD, Vasilakos D MD, PhD.
74 Dose titration of sublingual fentanyl, in relation to transdermal fentanyl dosing in cancer patients Amaniti E MD, PhD, Zaralidou A MD, Maidatsi P MD, PhD, Mitos G MD, Thoma G MD, Vasilakos D MD, PhD.
HIGH DOSE OPIOID THERAPY: ARE WE STILL TREATING PAIN?
 HIGH DOSE OPIOID THERAPY: ARE WE STILL TREATING PAIN? Sebastiano Mercadante, MD Director of Anesthesia and Intensive Care Unit & Pain Relief and Palliative Care Unit La Maddalena Cancer Center Professor
HIGH DOSE OPIOID THERAPY: ARE WE STILL TREATING PAIN? Sebastiano Mercadante, MD Director of Anesthesia and Intensive Care Unit & Pain Relief and Palliative Care Unit La Maddalena Cancer Center Professor
Complex Symptom Management at the End of Life of Pediatric Patients
 Complex Symptom Management at the End of Life of Pediatric Patients Justin N Baker, MD, FAAP, FAAHPM Chief, Division of Quality of Life and Palliative Care Director, Hematology/Oncology Fellowship Program
Complex Symptom Management at the End of Life of Pediatric Patients Justin N Baker, MD, FAAP, FAAHPM Chief, Division of Quality of Life and Palliative Care Director, Hematology/Oncology Fellowship Program
Session II. Learning Objectives for Session II. Key Principles of Safe Prescribing. Benefits and Limitations of ER/LA Opioids
 Learning Objectives for Session II Session II Best Practices for How to Start Therapy with ER/LA Opioids, How to Stop, and What to Do in Between Upon completion of this module, the participants will be
Learning Objectives for Session II Session II Best Practices for How to Start Therapy with ER/LA Opioids, How to Stop, and What to Do in Between Upon completion of this module, the participants will be
FENTANYL CITRATE TRANSMUCOSAL UTILIZATION MANAGEMENT CRITERIA
 FENTANYL CITRATE TRANSMUCOSAL UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: BRAND (generic) NAMES: HICL = H3AT Fentanyl citrate transmucosal Actiq (fentanyl citrate) lozenge on a handle 200, 400, 600, 800,
FENTANYL CITRATE TRANSMUCOSAL UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: BRAND (generic) NAMES: HICL = H3AT Fentanyl citrate transmucosal Actiq (fentanyl citrate) lozenge on a handle 200, 400, 600, 800,
Renal Prescribing at End of Life Guidance for Anticipatory prescribing for patients in renal failure (egfr<30) at the end of life
 at the end of life") Guidance for Anticipatory prescribing for patients in renal failure (egfr
Guidance for Anticipatory prescribing for patients in renal failure (egfr
Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center
 Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Stefan J. Friedrichsdorf, MD,
 From Denial To Palliactive: Practical Steps for Developing a PPC Program. Part 1:Training Stefan J. Friedrichsdorf, MD, FAAP Medical Director, Department of Pain Medicine, Palliative Care & Integrative
From Denial To Palliactive: Practical Steps for Developing a PPC Program. Part 1:Training Stefan J. Friedrichsdorf, MD, FAAP Medical Director, Department of Pain Medicine, Palliative Care & Integrative
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Stefan J. Friedrichsdorf, MD,
 Pain Treatment in Children with Serious Illness and Intellectual Disability: From Myths, Morphine and Multimodal Analgesia Stefan J. Friedrichsdorf, MD, FAAP Medical Director, Department of Pain Medicine,
Pain Treatment in Children with Serious Illness and Intellectual Disability: From Myths, Morphine and Multimodal Analgesia Stefan J. Friedrichsdorf, MD, FAAP Medical Director, Department of Pain Medicine,
Management of cancer pain
 DOI 10.1007/s11739-010-0448-8 SYMPOSIUM: MANAGING OF COMPLICATIONS IN PATIENTS WITH CANCER Management of cancer pain Sebastiano Mercadante Ó SIMI 2010 Abstract In the last decades, studies validating the
DOI 10.1007/s11739-010-0448-8 SYMPOSIUM: MANAGING OF COMPLICATIONS IN PATIENTS WITH CANCER Management of cancer pain Sebastiano Mercadante Ó SIMI 2010 Abstract In the last decades, studies validating the
RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM ACPE UAN: 107-000-14-016-L05-P Activity Type: Application-Based 0.1 CEU/1.0 hr Learning Objectives for
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA RELIEVING VIRGINIA S PAIN AND SUFFERING 3:45-4:45PM ACPE UAN: 107-000-14-016-L05-P Activity Type: Application-Based 0.1 CEU/1.0 hr Learning Objectives for
Applications for Anaesthesia. arcomed syringe and infusion pumps
 Applications for Anaesthesia arcomed syringe and infusion pumps TIVA TCI PCA PCEA PCS PIEB Anaesthesia programs and applications for arcomed Infusion Devices TIVA TCI PCA PCEA PCS PIEB (Total Intravenous
Applications for Anaesthesia arcomed syringe and infusion pumps TIVA TCI PCA PCEA PCS PIEB Anaesthesia programs and applications for arcomed Infusion Devices TIVA TCI PCA PCEA PCS PIEB (Total Intravenous
Pain in the Pediatric Palliative Care Context
 Pain in the Pediatric Palliative Care Context Erin Shepherd, RN, MN; CNS WRHA Pediatric Symptom Management and Palliative Care Service David Lambert, MD, FRCPC; Director Pediatric Acute Pain Service, Physician
Pain in the Pediatric Palliative Care Context Erin Shepherd, RN, MN; CNS WRHA Pediatric Symptom Management and Palliative Care Service David Lambert, MD, FRCPC; Director Pediatric Acute Pain Service, Physician
The pain of it all. Rod MacLeod MNZM. Hibiscus Hospice, Auckland and University of Auckland
 The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage