VOLUME C. Pharmacological Treatment for Drug Use Disorders Drug Treatment for Special Populations
|
|
|
- Buck Dalton
- 6 years ago
- Views:
Transcription



1 VOLUME C Pharmacological Treatment for Drug Use Disorders Drug Treatment for Special Populations




2 Module 2 Basics of opioid dependence Pharmacotherapy options Opioids: Definition, effects and treatment implications Opioid dependence treatment with Methadone Opioid dependence treatment with Buprenorphine Opioid antagonist treatment


3 Workshop 4 Opioid antagonist treatment

4 Training objectives At the end of this workshop you will be able to: Understand the neurobiology conditioning, underpinning opioid relapse Identify the rationale for the use of Naloxone for opioid overdose Understand the rationale for the use of Naltrexone for relapse prevention Explain the challenges and limitations of Naltrexone treatment

5 Naloxone for opioid overdose

6 Let s reflect! Have you ever witnessed an oipoid overdose and what did you do? Share your experience! 6
7 Naloxone for opioid overdose Naloxone is a medication used to counter the effects of opioid overdose, for example heroin and morphine overdose Specifically, Naloxone is used in opioid overdoses for countering life-threatening depression of the central nervous system and respiratory system It is marketed under trade names including Narcan, Nalone and Narcanti 7
8 Naloxone pharmacology The drug is derived from Thebaine and has an extremely high affinity for μ-opioid receptors in the central nervous system Naloxone is a μ-opioid receptor competitive antagonist, and its rapid blockade of those receptors often produces rapid onset of withdrawal symptoms 8
 Naloxone spray has become commercially available in North America")
9 Naloxone pharmacology Naloxone, administered intravenously (IV), intramuscularly (IM), or subcutaneously (SC) has been used in opioid overdose management for over 40 years, with minimal adverse effects beyond the induction of opioid withdrawal symptoms It also carries no potential for abuse Recently, a first intranasal (IN) Naloxone spray has become commercially available in North America The drug acts after about two minutes, and its effects may last about 45 minutes 9

10 Opioid overdose

11 Signs of opioid overdose Opioid overdose is identified by a combination of three signs and symptoms referred to as the opioid overdose triad. The symptoms of the triad are: Pinpoint pupils Unconsciousness Respiratory depression Treatment of overdose should be initiated if the person is not rousable and the respiratory rate is visibly slowed (i.e., less than 10 breaths per minute). 11
12 Naloxone for opioid overdose World Drug Report 2014 A number of countries have implemented communitybased programmes that make Naloxone more readily available to appropriately trained opioid users, their peers and family members In the USA, there were 188 local opioid overdose prevention programmes distributing Naloxone in 2010 Between 1996 and 2010, those programmes reported 10,171 opioid overdose reversals through use of Naloxone 12

13 Naloxone for opioid overdose: WHO recommendation Deaths from opioid overdose are preventable by reducing opioid dependency, restricting supply & by reversing the effects of opioids after an overdose has occurred Naloxone is recommended by the WHO to immediately reverse the effects of an opioid overdose It is highly effective and safe and has no significant side effects and no potential for misuse 13

14 Management of opioid overdose
15 Management of opioid overdose Treatment should be initiated if the person is not rousable & respiratory rate < 10 bpm Primary focus should be to address respiration and oxygenation For the treatment (reversal) of opioid overdose, WHO recommends using Naloxone In the case of suspected opioid overdose, any respiratory arrest should be managed with assisted breathing and / or oxygen while waiting for Naloxone to be administered and take effect. Naloxone is fast-acting, and adequate respiration will typically resume within 3-7 minutes of intramuscular administration of Naloxone 15
16 Dose of Naloxone to treat known or suspected opioid overdose An initial dose of 1 2 mg should be given to patients with Apnoea or in cardiovascular arrest. Signs of improvement - increase in respiratory rate and pupillary dilation should occur within 2-3 minutes following IV administration If no response is seen during this time, a higher (1-2 mg repeated doses should be given 2-3 minute intervals while ventilation and oxygenation is maintained Higher doses of Naloxone may be required for Buprenorphine, methadone or fentanyl overdose 16
17 Dose of Naloxone to treat known or suspected opioid overdose The primary goal of Naloxone is to restore adequate ventilation (above 12 respirations/minute) and oxygenation (above 92%) rather than full alertness Administering higher doses of Naloxone can precipitate opioid withdrawal and cause difficult to control agitation An acute lung injury (with hypoxia, rales and mouth frothing) can be seen in rapid overdose reversals in patients with marked hypoventilation. If intravenous administration is impracticable, Naloxone may be administered by the intramuscular or subcutaneous route 17
18 Opioid overdose: Steps to take The ideal dose of Naloxone improves respiration without inducing opioid withdrawal If in doubt, error on the side of too large a dose If there is access to injecting equipment and adequate patient ventilation, smaller amounts can be given in repeated dose, until breathing rate > 10 bpm Naloxone s effect last for min, which is usually sufficient to prevent death Naloxone may be administered as IV, IM, s/c or as a spray into the nose using an atomizer 18
19 Opioid overdose: Steps to take If Naloxone not available, overdose can be treated with respiratory support Ideally, patient should then be transported to the hospital for observation for at least 1 hr. If patient refuses observation for an hr. & is able to walk and speak coherently, the risk of reverting to potentially fatal sedation when the Naloxone wears off is relatively small l (1 in 600) A medical professional/caregiver stay with patient for several hours, counsel them not to use more opioids and keep the individual active 19
20 Opioid overdose: Steps to take In Overdoses of long-acting opioids, the duration of the sedation may outlast the effects of Naloxone The safest method of treating the overdose of a long-acting opioid is ventilation Patients can also be managed with repeated boluses of Naloxone or Naloxone infusions However, death can occur if there is an unnoticed interruption to the Naloxone infusion or if the patient wakes up and prematurely discharges him/herself from medical care. This is rare event 20
21 Opioid overdose: Steps to take The aftermath of an OD should include discussion of ongoing drug or pain treatment after the effects of the Naloxone have worn off All people using opioids, should receive education on the factors the risk of overdose and on recognition of overdose symptoms, as well as on the need for respiratory support and medical assistance in cases of overdose In addition, negative health outcomes associated with nonfatal overdose, such as respiratory infections, may develop later Individuals should thus be advised to seek a basic health screening in the days following an overdose 21

22 Where are we so far? What are the signs of opioid overdose? What is Naloxone and what are its properties? What are the key steps to take in case of opioid overdose? What is the most effective strategy to reduce the frequency of overdose? 22

23 Naltrexone for relapse prevention

24 Naltrexone in relapse prevention Naltrexone is an opioid Antagonist used in Relapse management of Opioid dependence Alcohol dependence It is available as Oral preparation Implants Long acting injections 24
25 Naltrexone for opioid relapse prevention Naltrexone is an opioid antagonist which, when taken regularly, blocks a former opiate user from experiencing the effects of opiates. It can be helpful following detoxification in enabling a patient to maintain abstinence. 25
26 Naltrexone What it does Naltrexone, and its active metabolite 6-β-Naltrexol, are competitive antagonists at μ- and κ-opioid receptors, and also at δ-opioid receptors. This blockade of opioid receptors is the basis of its action in the management of opioid dependence it reversibly blocks or attenuates the effects of opioids. Commence Treatment time Side effects Contraindications Cautions After at least 7-10 opioid free days. May be initiated 2-3days post buprenorphine detoxification in specialist inpatient setting. Patients are to have urine screen negative for opioid prior to commencing. Initially, for period of 3 months. Extended treatment may be necessary as time to full recovery in opioid dependence is variable. Nausea, vomiting, abdominal pain, diarrhea, constipation, reduced appetite, increased thirst, chest pain, anxiety, sleep disorders, headache etc. Currently dependent on opioid, severe hepatic impairment, acute hepatitis, hepatic failure, severe renal impairment, lactation LFTS before and during treatment. Pregnancy (use only if benefit outweighs risk). Avoid concomitant use of Opioid but increased dose of opioid analgesic may be required for pain. Warn patients of risk of acute opioid intoxication if they over-dose in attempt to overcome opioid receptor blockade. 26

27 Naltrexone: Mechanism of action 27
28 Naltrexone: Mechanism of action Naltrexone, and its active metabolite 6-βnaltrexol, are competitive antagonists at μ- and κ-opioid receptors, and to a lesser extent at δ- opioid receptors This blockade of opioid receptors is the basis behind its action in the management of opioid dependence it reversibly blocks or attenuates the effects of opioids 28
29 Naltrexone for opioid relapse prevention Side effects Acute opioid withdrawal precipitated (e.g., lethargy, aches, cramps, low energy) Depression, irritability Anxiety, nervousness Sleeping difficulties Skin rash Poor appetite Dizziness Precautions If Naltrexone ceased and opioid use reinstated, reduced tolerance to opioids increases risk of overdose and death Precipitates withdrawals in opioid-dependent patients 29

30 Naltrexone: Clinical properties
31 Naltrexone for opioid relapse prevention Naltrexone will cause withdrawal symptoms in people who are physically dependent on narcotics Naltrexone treatment is started after an individual is no longer dependent on narcotics It is important for an individual to be fully withdrawn from opioids If Naltrexone is taken by individuals who are incompletely detoxified from opioids, it can precipitate a rapid and unpleasant withdrawal syndrome 31
32 Naltrexone precipitated withdrawal Ingestion of Naltrexone in opioid dependent people will result in an acute block of opioid receptors and may precipitate a severe opioid withdrawal reaction if opioids are present Withdrawal can appear after minutes after ingestion and may last up to 48 hrs Symptoms include confusion, agitation, hallucinations, sweating, tachycardia, abdominal pain and episodes of profuse vomiting and/or diarrhoea, which may result in significant fluid losses 32

33 Starting Naltrexone Before starting Naltrexone or during the course of treatment it is important to conduct blood test and monitor liver enzymes. Naltrexone can be given unless liver enzymes are elevated > 5 times upper limit of normal If uncertain whether the patient has used opioids, it may be necessary to conduct a Naloxone dose challenge before administering Naltrexone. If opioids have been used then severe and prolonged withdrawal symptoms will result if Naltrexone is administered 33
34 Starting Naltrexone: Naloxone / Naltrexone challenge Following a negative urine test for opioids, the patient is given: First Naltrexone dose of 6-12 mg orally or Naloxone 0.8 mg or higher If the patient does not experience any withdrawal symptoms after a few hours, a 50 mg tablet of Naltrexone can be given Patients can be commenced on Naltrexone within a few days of finishing a buprenorphine detoxification The usual maintenance dose is then 50 mg a day 34
35 Starting Naltrexone after withdrawal from Methadone Patient must be methadone free for at least 7-10 days prior to commencing Naltrexone treatment, due to the long half-life of methadone Once a satisfactory Naloxone challenge is achieved, Naltrexone treatment can be commenced Patient may experience opioid withdrawal symptoms for several days after commencing Naltrexone treatment 35
36 Starting Naltrexone Change font size after withdrawal from Buprenorphine in neighbouring slides A negative Naloxone challenge does not preclude the onset of withdrawal symptoms when a patient treated with buprenorphine is initiated on Naltrexone This is why Naloxone dose should be higher, usually 1.2 mg is sufficient to assure negative challenge This could be due the higher affinity of buprenorphine to the opioid receptor Therefore a drug screen to test for the presence of opioids should also be carried out Reduce buprenorphine dose to 400 micrograms per day Wait at least for 4-5 days after the last dose of buprenorphine before commencing Naltrexone therapy 36
37 Maintenance dose of Naltrexone for opioid relapse prevention After Day 1 of starting treatment with Naltrexone, the maintenance dose is 50 mg/day The usual weekly dose is 350 mg/week The weekly dose may be divided up according to one of the following schedules: 50 mg every day 100 mg every other day 50 mg/day during the week and 100 mg on Saturday 100 mg on Monday, Wednesday &150 mg on Friday 150 mg every three days 37
38 Naltrexone for relapse management outcome The outcome of Naltrexone treatment is improved by a programme of supervision, which can involve carers to ensure compliance with the regimen Naltrexone should only be administered under adequate supervision to people who have been fully informed of the potential adverse effects of treatment. It should be given as part of a programme of supportive care 38
39 Naltrexone with psychosocial intervention Positive results when Naltrexone is combined with cognitive behavioural therapy and treatment with the Matrix Model Contingency management produces large increases in retention on Naltrexone Family therapy promotes successful treatment with Naltrexone Using legal pressure (individuals sentenced to treatment by courts) to mandate people to take Naltrexone can greatly increase retention on Naltrexone and outcome success 39
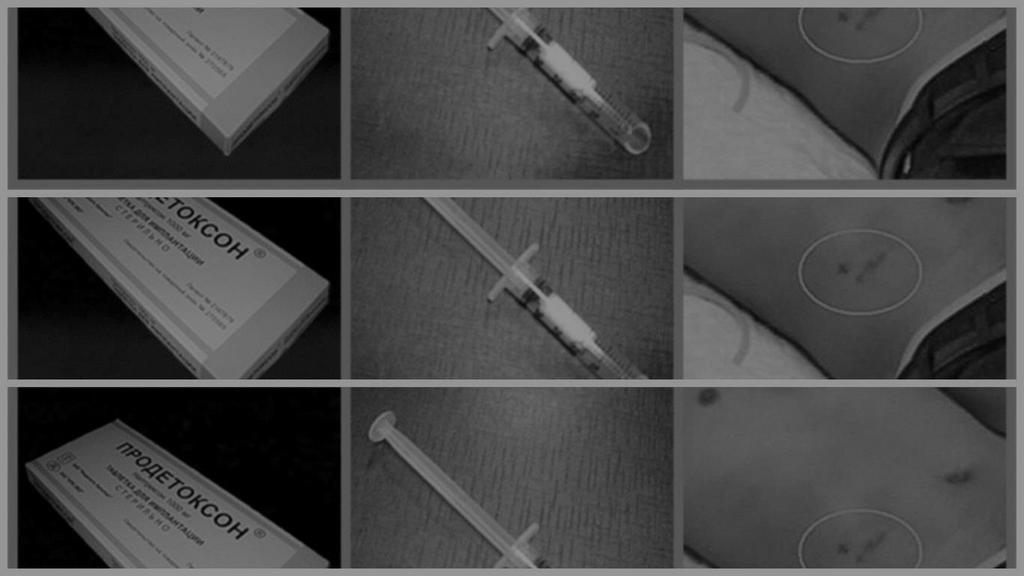
40 Naltrexone implant
41 Naltrexone implant A Bulwark Against Ambivalence To succeed with Naltrexone therapy, patients must consistently choose to take the next dose of medication rather than satisfy urges to reexperience effects of drugs However, Naltrexone does not reliably suppress drug craving, and many patients waver in their resolve to remain abstinent The rationale for extended-release Naltrexone formulations is to provide sustained, long-lasting protection against such ambivalence 41
42 Naltrexone implant for opioid relapse prevention Naltrexone can be administered as a low-dose implant. These implants can remain effective for days. They dissolve slowly and are usually put in under a local anaesthetic in the left iliac fossa This implant procedure has not been shown scientifically to be successful in "curing" the patient of their addiction, although it does provide a better solution than oral Naltrexone for medication compliance reasons 42

43 Conclusion: Naltrexone for opioid dependence Naltrexone, nonselective opioid antagonist Induction issues Retention Depot preparation Better outcomes with specific therapies or legal interventions 43

44 Naltrexone for alcohol relapse prevention
45 Naltrexone for alcohol dependence: Pharmacology Alcohol produces some of its reinforcing properties by releasing the body s own opiate-like substance (endorphin) Naltrexone can block endorphin effects A person with alcohol dependence, who is maintained on Naltrexone will not experience endorphin-mediated alcohol-induced euphoria Maintenance on Naltrexone will reduce alcohol use 45
46 Naltrexone in alcohol dependence: Pharmacology The μ-opioid receptor modulates dopaminergic cell firing in the ventral tegmental area and therefore blocking the μ-opioid receptor with Naltrexone prevents any increase in dopaminergic activity Consequently, Naltrexone reduces alcohol s rewarding effects and also motivation to drink or craving 46


47 Naltrexone for alcoholism evidence Two landmark studies documented that Naltrexone can be an effective treatment for treating alcoholics: Naltrexone in the Treatment of Alcohol Dependence by Volpicelli, W., Alterman, A., Hayashida, M., O Brien, C. Naltrexone and Coping Skills Therapy for Alcohol Dependence by O Malley, S., Jaffe, A., Chang, G., Schottenfeld, R., Meyer, R., Rounsaville, B. O Malley et al. demonstrated that if Naltrexone is used with coping skills therapy, relapses are reduced and the severity of the relapse is reduced. 47
48 Naltrexone in alcohol dependence: Evidence There have been several meta-analyses and systematic reviews which broadly have the same conclusion that oral Naltrexone significantly reduces return to heavy drinking, probably by reducing lapse to relapse, but does not necessarily improve cumulative or continuous abstinence rates. Lingford-Hughes AR,
49 Naltrexone for relapse prevention: Summary Opioid antagonist, Naltrexone can be beneficial in relapse management of both opioid and alcohol dependence The compliance with Naltrexone treatment is improved by a programme of supervision, which can involve carers It is most effective when delivered as part of a programme of psychosocial intervention and supportive care 49

50 Let s think! Discuss with your colleagues: Who are the best candidates for treatment with Naltrexone for relapse prevetion? 50
51 Questions

52 Wrap-up Why and how use Naloxone for opioid overdose? How to use of Naltrexone for relapse prevention? What are the challenges and limitations of Naltrexone treatment?


53 Post-assessment

54 Thank you for your time! End of module 2
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE
 SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE INDICATION Naltrexone is a pure opiate antagonist licensed as an adjunctive prophylactic therapy in the maintenance
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE INDICATION Naltrexone is a pure opiate antagonist licensed as an adjunctive prophylactic therapy in the maintenance
Prescribing Framework for Naltrexone in Relapse Prevention (Opioid Dependence)
") Hull & East Riding Prescribing Committee Prescribing Framework for Naltrexone in Relapse Prevention (Opioid Dependence) Patients Name: Unit Number: Patients Address:.. G.P s Name:.. Communication We agree
Hull & East Riding Prescribing Committee Prescribing Framework for Naltrexone in Relapse Prevention (Opioid Dependence) Patients Name: Unit Number: Patients Address:.. G.P s Name:.. Communication We agree
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION
 SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION Naltrexone is used as part of a comprehensive programme of treatment against alcoholism to reduce the
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION Naltrexone is used as part of a comprehensive programme of treatment against alcoholism to reduce the
Guidance for naltrexone prescribing
 Document level: Drug Alcohol (Trustwide) Code: DA7 Issue number: 2 Guidance for naltrexone prescribing Lead executive Authors details Type of document Target audience Document purpose Lead Clinical Director
Document level: Drug Alcohol (Trustwide) Code: DA7 Issue number: 2 Guidance for naltrexone prescribing Lead executive Authors details Type of document Target audience Document purpose Lead Clinical Director
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents
 Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
Long term treatment for opioid dependence Antagonist therapy
 Long term treatment for opioid dependence Antagonist therapy Treatment of Opioid Dependence Antagonist treatment Naltrexone Naltrexone (NTX) synthesized in 1965 Eliminate drug carving and prevent relapse
Long term treatment for opioid dependence Antagonist therapy Treatment of Opioid Dependence Antagonist treatment Naltrexone Naltrexone (NTX) synthesized in 1965 Eliminate drug carving and prevent relapse
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE
 LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of Opioid Dependence Abbreviated Version
 Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of Opioid Dependence Abbreviated Version Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of
Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of Opioid Dependence Abbreviated Version Clinical Guidelines and Procedures for the Use of Naltrexone in the Management of
MEDICATION ASSISTED TREATMENT
 MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
Guidance For The Use Of Naltrexone In The Maintenance Of Abstinence in Formerly Opioid Dependent Adults By Clinicians Working Within NHS Grampian
 Title: Identifier: Guidance For The Use Of Naltrexone In The Maintenance Of Abstinence in Formerly Opioid Dependent Adults By Clinicians Working Within NHS Grampian NHSG/Guide/NHSG_NaltexMA_885 Replaces:
Title: Identifier: Guidance For The Use Of Naltrexone In The Maintenance Of Abstinence in Formerly Opioid Dependent Adults By Clinicians Working Within NHS Grampian NHSG/Guide/NHSG_NaltexMA_885 Replaces:
NALTREXONE DAVID CRABTREE, MD, MPH UNIVERSITY OF UTAH HEALTH, 2018
 NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
Opioid Agonists. Natural derivatives of opium poppy - Opium - Morphine - Codeine
 Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Buprenorphine pharmacology
 Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They?
 Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Medication-Assisted Treatment (MAT) Overview
 Overview") Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Talking with your doctor
 SUBOXONE (buprenorphine and naloxone) Sublingual Film (CIII) Talking with your doctor Opioid dependence can be treated. Talking with your healthcare team keeps them aware of your situation so they may
SUBOXONE (buprenorphine and naloxone) Sublingual Film (CIII) Talking with your doctor Opioid dependence can be treated. Talking with your healthcare team keeps them aware of your situation so they may
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Analgesia for Patients with Substance Abuse Disorders. Lisa Jennings CN November 2015
 Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
Buprenorphine as a Treatment Option for Opioid Use Disorder
 Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Prescribing Framework for Naltrexone in Alcohol Relapse Prevention
 Prescribing Framework for Naltrexone in Alcohol Relapse Prevention Patients Name:.. NHS Number: Patients Address:... (Use addressograph sticker) GP s Name:... Communication We agree to treat this patient
Prescribing Framework for Naltrexone in Alcohol Relapse Prevention Patients Name:.. NHS Number: Patients Address:... (Use addressograph sticker) GP s Name:... Communication We agree to treat this patient
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE SHARED CARE AGREEMENT
 DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE SHARED CARE AGREEMENT NALTREXONE 50mg TABLETS For Opioid Relapse Prevention (in formerly opioid dependent patients) This shared care agreement is aimed at all
DERBYSHIRE JOINT AREA PRESCRIBING COMMITTEE SHARED CARE AGREEMENT NALTREXONE 50mg TABLETS For Opioid Relapse Prevention (in formerly opioid dependent patients) This shared care agreement is aimed at all
OST. Pharmacology & Therapeutics. Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO
 OST Pharmacology & Therapeutics Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO Disclaimer In the past two years I have received no payment for services from any agency other than government or academic.
OST Pharmacology & Therapeutics Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO Disclaimer In the past two years I have received no payment for services from any agency other than government or academic.
Controlled Substance and Wellness Agreement
 Controlled Substance and Wellness Agreement You and your provider have agreed on the use of controlled substance medications to treat your: We want to make sure you know how to manage your new prescription(s)
Controlled Substance and Wellness Agreement You and your provider have agreed on the use of controlled substance medications to treat your: We want to make sure you know how to manage your new prescription(s)
Naloxone. Medical Uses. Opiate overdose. From Wikipedia, the free encyclopedia. Naloxone
 Naloxone From Wikipedia, the free encyclopedia Naloxone Naloxone, sold under the brandname Narcan among others, is a medication used to reverse the effects of opioids, especially in overdose. [2] Naloxone
Naloxone From Wikipedia, the free encyclopedia Naloxone Naloxone, sold under the brandname Narcan among others, is a medication used to reverse the effects of opioids, especially in overdose. [2] Naloxone
Module II Opioids 101 Opiate Opioid
 BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module II Opioids 101 Module II Goals of the Module This module reviews the following:! Opioid addiction and the brain!
BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module II Opioids 101 Module II Goals of the Module This module reviews the following:! Opioid addiction and the brain!
SW OREGON OPIOID SUMMIT. Medication Assisted Recovery for Opioid Use Disorder. Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass
 SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
ROSC & MAT II: Opioid Treatment Services
 ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Take Home Naloxone elearning Module Script
 elearning Module Script Slide 1-3 Review the outline and the plan for the presentation. Slide 4 We do accept the cynicism of this poster. Slide 5 Read from the slide the definition of Harm Reduction Slide
elearning Module Script Slide 1-3 Review the outline and the plan for the presentation. Slide 4 We do accept the cynicism of this poster. Slide 5 Read from the slide the definition of Harm Reduction Slide
Medication for the Treatment of Alcohol Use Disorder. Pocket Guide
 Medication for the Treatment of Alcohol Use Disorder Pocket Guide Medications are underused in the treatment of alcohol use disorder. According to the National Survey on Drug Use and Health, of the estimated
Medication for the Treatment of Alcohol Use Disorder Pocket Guide Medications are underused in the treatment of alcohol use disorder. According to the National Survey on Drug Use and Health, of the estimated
VIVITROL (naltrexone for extended-release injectable suspension) A µ-opioid Receptor Antagonist
 A µ-opioid Receptor Antagonist") MECHANISM OF ACTION VIVITROL (naltrexone for extended-release injectable suspension) A µ-opioid Receptor Antagonist VIVITROL is indicated for prevention of relapse to opioid dependence, following opioid
MECHANISM OF ACTION VIVITROL (naltrexone for extended-release injectable suspension) A µ-opioid Receptor Antagonist VIVITROL is indicated for prevention of relapse to opioid dependence, following opioid
Prescription Opioid Addiction
 CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
Brief History of Methadone Maintenance Treatment
 METHADONE Brief History of Methadone Maintenance Treatment Methadone maintenance treatment was on the cusp of the social revolution in the sixties. Doctors and public health workers had concluded what
METHADONE Brief History of Methadone Maintenance Treatment Methadone maintenance treatment was on the cusp of the social revolution in the sixties. Doctors and public health workers had concluded what
Opioid dependence: Detoxification
 Opioid dependence: Detoxification What is detoxification? A. Process of removal of toxins from the body? B. Admitting a drug dependent person in a hospital and giving him nutrition? C. Stopping drug use
Opioid dependence: Detoxification What is detoxification? A. Process of removal of toxins from the body? B. Admitting a drug dependent person in a hospital and giving him nutrition? C. Stopping drug use
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines
 The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
GOALS AND OBJECTIVES
 SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
Opioid Use Disorders &Medication Treatment
 Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
People inject, sniff, snort, or smoke heroin. Some people mix heroin with crack cocaine, a practice called speedballing.
 What is heroin? Heroin is an opioid drug made from morphine, a natural substance taken from the seed pod of the various opium poppy plants grown in Southeast and Southwest Asia, Mexico, and Colombia. Heroin
What is heroin? Heroin is an opioid drug made from morphine, a natural substance taken from the seed pod of the various opium poppy plants grown in Southeast and Southwest Asia, Mexico, and Colombia. Heroin
Module Two: Pharmacotherapies for Opioid Substitution Treatment
 Module Two: Pharmacotherapies for Opioid Substitution Treatment Neurobiology of Addiction Pharmacology of Opioids Methadone Buprenorphine Pharmacokinetics of Methadone & Buprenorphine Opioid effects Intoxication
Module Two: Pharmacotherapies for Opioid Substitution Treatment Neurobiology of Addiction Pharmacology of Opioids Methadone Buprenorphine Pharmacokinetics of Methadone & Buprenorphine Opioid effects Intoxication
Medication Assisted Treatment. MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment
 Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Essential Shared Care Agreement Naltrexone
 In partnership with as part of Please complete the following details: Patient s name, address, date of birth Consultant s contact details (p.3) And send One copy to: 1. The patient s GP 2. Put one copy
In partnership with as part of Please complete the following details: Patient s name, address, date of birth Consultant s contact details (p.3) And send One copy to: 1. The patient s GP 2. Put one copy
Slide 1. Slide 2. Slide 3. Opioid (Narcotic) Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists
 Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists") Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
BASIC VOLUME. Elements of Drug Dependence Treatment
 BASIC VOLUME Elements of Drug Dependence Treatment Module 3 Principles of CBT and relapse prevention strategies Introduction to Cognitive Behavioural Therapy Basics of pharmacological treatment Workshop
BASIC VOLUME Elements of Drug Dependence Treatment Module 3 Principles of CBT and relapse prevention strategies Introduction to Cognitive Behavioural Therapy Basics of pharmacological treatment Workshop
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04
 Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04 Date issued Issue 1 Nov 2018 Planned review Nov 2021 PPT-PGN 18 part of NTW(C)38 Pharmaceutical
Policy on Pharmacological Therapies Practice Guidance Note Reducing Dosing Errors with Opioid Medicines V04 Date issued Issue 1 Nov 2018 Planned review Nov 2021 PPT-PGN 18 part of NTW(C)38 Pharmaceutical
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Naloxone HCI 4 mg/0.1. nostril. Repeat after 3 minutes if minimal or no
 THE SOUTH CAROLINA BOARD OF MEDICAL EXAMINERS AND THE SOUTH CAROLINA BOARD OF PHARMACY S JOINT PROTOCOL TO INITIATE DISPENSING OF NALOXONE HCI WITHOUT A PRESCRIPTION This joint protocol authorizes any
THE SOUTH CAROLINA BOARD OF MEDICAL EXAMINERS AND THE SOUTH CAROLINA BOARD OF PHARMACY S JOINT PROTOCOL TO INITIATE DISPENSING OF NALOXONE HCI WITHOUT A PRESCRIPTION This joint protocol authorizes any
Methadone Maintenance
 Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
3/26/14. Opiates PSY B396 ALCOHOL, ALCOHOLISM, & DRUG ABUSE. Early History Cont d. Early History. Opiate Use in the 19th century. Technology Advances
 Opiates PSY B396 ALCOHOL, ALCOHOLISM, & DRUG ABUSE Chapter 10 Opiates The most dramatic example of the doubleedged sword character of drugs Most potent painkillers Prototype addictive drug: Heroin Early
Opiates PSY B396 ALCOHOL, ALCOHOLISM, & DRUG ABUSE Chapter 10 Opiates The most dramatic example of the doubleedged sword character of drugs Most potent painkillers Prototype addictive drug: Heroin Early
SAN JOAQUIN COUNTY EMERGENCY MEDICAL SERVICES AGENCY. Administration of Naloxone for Opiate Overdose
 SAN JOAQUIN COUNTY EMERGENCY MEDICAL SERVICES AGENCY Administration of Naloxone for Opiate Overdose Disclaimer: Authorization - EMT Optional Skills Only authorized Emergency Medical Technicians (EMT) who
SAN JOAQUIN COUNTY EMERGENCY MEDICAL SERVICES AGENCY Administration of Naloxone for Opiate Overdose Disclaimer: Authorization - EMT Optional Skills Only authorized Emergency Medical Technicians (EMT) who
WR Fentanyl Symposium. Opioids, Overdose, and Fentanyls
 Opioids, Overdose, and Fentanyls Outline: What are opioids? Why are we experiencing and opioid crisis? Potency, purity, and product How do opioids cause overdose and overdose deaths? What is naloxone and
Opioids, Overdose, and Fentanyls Outline: What are opioids? Why are we experiencing and opioid crisis? Potency, purity, and product How do opioids cause overdose and overdose deaths? What is naloxone and
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets. Risk Evaluation and Mitigation Strategy (REMS) Program
 Program") SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
Treatment Approaches for Drug Addiction
 Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Now available. A maintenance dose of SUBOXONE mg once daily is clinically effective for most patients*1. Once-daily dosing in a single tablet
 Now available SUBOXONE Once-daily dosing1 12 mg and 16 mg tablets A maintenance dose of SUBOXONE 12-16 mg once daily is clinically effective for most patients*1 Effective maintenance dosing with SUBOXONE
Now available SUBOXONE Once-daily dosing1 12 mg and 16 mg tablets A maintenance dose of SUBOXONE 12-16 mg once daily is clinically effective for most patients*1 Effective maintenance dosing with SUBOXONE
Buprenorphine: An Introduction. Sharon Stancliff, MD Harm Reduction Coalition September 2008
 Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Pharmacotherapy for Substance Use Disorders
 Pharmacotherapy for Substance Use Disorders Vanessa de la Cruz, MD Chief of Psychiatry Mental Health and Substance Abuse Services Santa Cruz County Health Services Agency 1400 Emeline Avenue Santa Cruz,
Pharmacotherapy for Substance Use Disorders Vanessa de la Cruz, MD Chief of Psychiatry Mental Health and Substance Abuse Services Santa Cruz County Health Services Agency 1400 Emeline Avenue Santa Cruz,
The doctor/nmp who prescribes the medication legally assumes clinical responsibility for the drug and the consequences of its use.
 The 3T s Formulary NHS Swindon, NHS Wiltshire Great Western Hospitals NHS Foundation Trust (In collaboration with Avon and Wiltshire Mental Health Partnership and Oxford Health NHS Foundation Trust) Shared
The 3T s Formulary NHS Swindon, NHS Wiltshire Great Western Hospitals NHS Foundation Trust (In collaboration with Avon and Wiltshire Mental Health Partnership and Oxford Health NHS Foundation Trust) Shared
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
SUBOXONE (buprenorphine and naloxone) sublingual film (CIII) IMPORTANT SAFETY INFORMATION
 sublingual film (CIII) IMPORTANT SAFETY INFORMATION") SUBOXONE (buprenorphine and naloxone) sublingual film (CIII) IMPORTANT SAFETY INFORMATION What is the most important information I should know about SUBOXONE Film? Keep SUBOXONE Film in a secure place
SUBOXONE (buprenorphine and naloxone) sublingual film (CIII) IMPORTANT SAFETY INFORMATION What is the most important information I should know about SUBOXONE Film? Keep SUBOXONE Film in a secure place
Dr Alistair Dunn. General Practitioner Whangarei
 Dr Alistair Dunn General Practitioner Whangarei 1982 Temgesic = Buprenorphine Sublingual opiate analgesic 0.2 mg Popular drug of abuse 1991 Temgesic NX = Bup & Nalxone Nalxone added to deter abuse 1999
Dr Alistair Dunn General Practitioner Whangarei 1982 Temgesic = Buprenorphine Sublingual opiate analgesic 0.2 mg Popular drug of abuse 1991 Temgesic NX = Bup & Nalxone Nalxone added to deter abuse 1999
Biological Addictions Treatment. Psychology 470. Many Types of Approaches
 Many Types of Approaches Biological Addictions Treatment Psychology 470 Introduction to Chemical Additions Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Detoxification approaches
Many Types of Approaches Biological Addictions Treatment Psychology 470 Introduction to Chemical Additions Steven E. Meier, Ph.D. Listen to the audio lecture while viewing these slides Detoxification approaches
Medication Assisted Treatment. Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs
 Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Opioids Research to Practice
 Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
HARM REDUCTION & TREATMENT. Devin Reaves MSW
 HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
Opioids. October 29, Addiction Medicine Review Course CSAM, Newport Beach, CA
 Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
Opioids Research to Practice
 Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
TRAPADOL INJECTION FOR I.V./I.M. USE ONLY
 TRAPADOL INJECTION FOR I.V./I.M. USE ONLY Composition : Each 2ml. contains : Tramadol Hydrochloride I.P. Water for injection I.P. 100mg. q.s. CLINICAL PHARMACOLOGY : Pharmacodynamics Tramadol is a centrally
TRAPADOL INJECTION FOR I.V./I.M. USE ONLY Composition : Each 2ml. contains : Tramadol Hydrochloride I.P. Water for injection I.P. 100mg. q.s. CLINICAL PHARMACOLOGY : Pharmacodynamics Tramadol is a centrally
Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services
 Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services www.randallwebber.com MAT clients are still addicted Truth: MAT clients will experience withdrawal symptoms if they stop
Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services www.randallwebber.com MAT clients are still addicted Truth: MAT clients will experience withdrawal symptoms if they stop
Slow Release Opioids. Morphine (Zomorph/MST) Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For the Treatment of Pain
 Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For the Treatment of Pain") NHS Greater Glasgow And Clyde Pain Management Service Information for Adult Patients who are Prescribed Slow Release Opioids Morphine (Zomorph/MST) Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For
NHS Greater Glasgow And Clyde Pain Management Service Information for Adult Patients who are Prescribed Slow Release Opioids Morphine (Zomorph/MST) Oxycodone (Longtec, Oxycontin) Tapentadol (Palexia) For
Doctor Discussion Guide
 Doctor Discussion Guide Getting the pain relief you need to stay active is important. Keeping track of your symptoms can help you and your healthcare provider determine if there is a need to adjust your
Doctor Discussion Guide Getting the pain relief you need to stay active is important. Keeping track of your symptoms can help you and your healthcare provider determine if there is a need to adjust your
Opioid Overdose Epidemic A Crises and Opportunity
 Opioid Overdose Epidemic A Crises and Opportunity Samuel M. Silverman MD, FAPA, DFASAM Assistant Clinical Professor, UConn Medical School Director, Medical Education Rushford, A Hartford HealthCare Partner
Opioid Overdose Epidemic A Crises and Opportunity Samuel M. Silverman MD, FAPA, DFASAM Assistant Clinical Professor, UConn Medical School Director, Medical Education Rushford, A Hartford HealthCare Partner
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off.
 1 2 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. 3 4 5 6 Course Outline Introduction
1 2 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. 3 4 5 6 Course Outline Introduction
OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI)
") OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI) Case 105- Prep Materials University of Massachusetts Medical School Opioid Conscious Curriculum Learner Prep Objectives The purpose of this prep material
OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI) Case 105- Prep Materials University of Massachusetts Medical School Opioid Conscious Curriculum Learner Prep Objectives The purpose of this prep material
What Is Heroin? Examples of Opioids. What Science Says about Opioid Use Disorder and Its Treatment 6/27/2016
 What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
Implementing Buprenorphine Treatment in Opioid Treatment Programs Webinar 2, October 3, 2018
 Implementing Buprenorphine Treatment in Opioid Treatment Programs Webinar 2, October 3, 2018 Judith Martin, MD, Medical Director of Substance Use Services, San Francisco Department of Public Health Webinar
Implementing Buprenorphine Treatment in Opioid Treatment Programs Webinar 2, October 3, 2018 Judith Martin, MD, Medical Director of Substance Use Services, San Francisco Department of Public Health Webinar
POLICY DOCUMENT. CG/pain management in opioid dependency/03/15. Associate Director of Pharmacy
 POLICY DOCUMENT Document Title Reference Number PRESCRIBING FOR PAIN MANAGEMENT IN OPIOID DEPENDENT CLIENTS CG/pain management in opioid dependency/03/15 Policy Type Clinical Guideline Electronic File/Location
POLICY DOCUMENT Document Title Reference Number PRESCRIBING FOR PAIN MANAGEMENT IN OPIOID DEPENDENT CLIENTS CG/pain management in opioid dependency/03/15 Policy Type Clinical Guideline Electronic File/Location
Opioid rotation or switching may be considered if a patient obtains pain relief with one opioid and is suffering severe adverse effects.
 Dose equivalence and switching between opioids Key Messages Switching from one opioid to another should only be recommended or supervised by a healthcare practitioner with adequate competence and sufficient
Dose equivalence and switching between opioids Key Messages Switching from one opioid to another should only be recommended or supervised by a healthcare practitioner with adequate competence and sufficient
Opioids. Sergio Hernandez, MD
 Opioids Sergio Hernandez, MD Required Slide Disclosures 1. SIGNIFICANT FINANCIAL INTERESTS NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT 2. GENERAL AND OBLIGATION INTERESTS All general
Opioids Sergio Hernandez, MD Required Slide Disclosures 1. SIGNIFICANT FINANCIAL INTERESTS NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT 2. GENERAL AND OBLIGATION INTERESTS All general
Tuscarawas County Health Department. Vivitrol Treatment Consent
 Tuscarawas County Health Department Vivitrol Treatment Consent I. Vivitrol Medication Guide: a. VIVITROL (viv-i-trol) (naltrexone for extended-release injectable suspension) b. Read this Medication Guide
Tuscarawas County Health Department Vivitrol Treatment Consent I. Vivitrol Medication Guide: a. VIVITROL (viv-i-trol) (naltrexone for extended-release injectable suspension) b. Read this Medication Guide
Naloxone Intranasal EMT OPTIONAL SKILL. Cell Phones and Pagers. Course Outline 09/2017
 EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and Overview
EMT OPTIONAL SKILL Naloxone Intranasal Cell Phones and Pagers Be courteous to your classmates! Please set your cell phones and/or pagers to silent or turn them off. Course Outline Introduction and Overview
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT
 and acute pain management on MAT") An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
PAIN & ANALGESIA. often accompanied by clinical depression. fibromyalgia, chronic fatigue, etc. COX 1, COX 2, and COX 3 (a variant of COX 1)
") Pain - subjective experience associated with detection of tissue damage ( nociception ) acute - serves as a warning chronic - nociception gone bad often accompanied by clinical depression fibromyalgia,
Pain - subjective experience associated with detection of tissue damage ( nociception ) acute - serves as a warning chronic - nociception gone bad often accompanied by clinical depression fibromyalgia,
Clinical Guidelines for the Pharmacologic Treatment of Opioid Use Disorder
 Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Treatment of drug dependence What you need to know
 Treatment of drug dependence What you need to know Opioid Replacement Therapy for heroin and opioid dependence Information for family members and significant others Contents What help is there for family
Treatment of drug dependence What you need to know Opioid Replacement Therapy for heroin and opioid dependence Information for family members and significant others Contents What help is there for family
Naltrexone Overview. Todd Korthuis, MD, MPH ECHO-MAT Conference February 14, 2017
 Naltrexone Overview Todd Korthuis, MD, MPH ECHO-MAT Conference February 14, 2017 Pharmacotherapy for Opioid Use Disorder % Mu Receptor Intrinsic Activity 100 90 80 Full Agonist: Methadone ( How High )
Naltrexone Overview Todd Korthuis, MD, MPH ECHO-MAT Conference February 14, 2017 Pharmacotherapy for Opioid Use Disorder % Mu Receptor Intrinsic Activity 100 90 80 Full Agonist: Methadone ( How High )
Unit II Problem 7 Pharmacology: Substance Abuse, Dependence and Addiction
 Unit II Problem 7 Pharmacology: Substance Abuse, Dependence and Addiction Drugs are classified as being Used (medically approved) abused (medically NOT approved) - What is the difference between dependence
Unit II Problem 7 Pharmacology: Substance Abuse, Dependence and Addiction Drugs are classified as being Used (medically approved) abused (medically NOT approved) - What is the difference between dependence
Fentanyls and Naloxone. Opioids, Overdose, and Naloxone
 Opioids, Overdose, and Naloxone Presenter Disclosure Presenter s Name: Michael Beazely I have no current or past relationships with commercial entities Speaking Fees for current program: I have received
Opioids, Overdose, and Naloxone Presenter Disclosure Presenter s Name: Michael Beazely I have no current or past relationships with commercial entities Speaking Fees for current program: I have received
Medication Assisted Treatment:
 Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Otterbein Police Department. Opioid Addition Awareness
 Otterbein Police Department Opioid Addition Awareness What are Opiates? Opioids are substances that act on opioid receptors to produce morphinelike effects. Medically they are primarily used for pain relief,
Otterbein Police Department Opioid Addition Awareness What are Opiates? Opioids are substances that act on opioid receptors to produce morphinelike effects. Medically they are primarily used for pain relief,
C AT E G O R Y I I I COMMUNICATION, TREATMENT & PREVENTION INTERVENTIONS PHARMACOLOGY OF ADDICTIONS
 C AT E G O R Y I I I COMMUNICATION, TREATMENT & PREVENTION INTERVENTIONS PHARMACOLOGY OF ADDICTIONS 1.0 Introduction Medications are used in the treatment of drug, alcohol and nicotine dependence to manage
C AT E G O R Y I I I COMMUNICATION, TREATMENT & PREVENTION INTERVENTIONS PHARMACOLOGY OF ADDICTIONS 1.0 Introduction Medications are used in the treatment of drug, alcohol and nicotine dependence to manage
Pain Management for Adult sickle cell disease patients: Information for patients, relatives and carers
 Pain Management for Adult sickle cell disease patients: Information for patients, relatives and carers Why you should read this leaflet This leaflet will give you the information necessary to manage your
Pain Management for Adult sickle cell disease patients: Information for patients, relatives and carers Why you should read this leaflet This leaflet will give you the information necessary to manage your
Buprenorphine for Family Medicine. Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17
 + Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
+ Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
Guideline for the use of Naloxone in Adults
 Guideline for the use of Naloxone in Adults Controlled document This document is uncontrolled when downloaded or printed Reference number Version 1 Authors WHHT: MM098 Date ratified February 2016 Committee:
Guideline for the use of Naloxone in Adults Controlled document This document is uncontrolled when downloaded or printed Reference number Version 1 Authors WHHT: MM098 Date ratified February 2016 Committee: