Michael W. Fried, M.D., FAASLD Professor of Medicine Director, UNC Liver Center University of North Carolina at Chapel Hill
|
|
|
- Martina Parker
- 6 years ago
- Views:
Transcription

1 Michael W. Fried, M.D., FAASLD Professor of Medicine Director, UNC Liver Center University of North Carolina at Chapel Hill

2 Disclosures Michael W. Fried, M.D. Grants/Research Support AbbVie, BMS, Gilead, Janssen, Merck Consultant: AbbVie, BMS, Gilead, Janssen, Merck Stock/Shareholder: TARGET PharmaSolutions Speakers Bureau: None Other Financial Support: NIH Grants Some slides courtesy of Paul Kwo, MD
3 Hepatitis C is No Longer a Medical Science... It s Now a Social Science! Attributed to Ira Jacobson, 2017
4 High Rates of HCV Cure Across All Regimens: GT1, Non-Cirrhotic, Tx-Naïve Regimen Weeks Study SVR12 Sofosbuvir + ledipasvir (HCV RNA <6 M IU) (HCV RNA >6 M IU) Elbasvir/grazoprevir (1b) (-) -NS5A RAVs (1a) C-EDGE ION-3 119/123 (97%) 206/216 (95%) 133/135 (99%) 129/131 (99%) Sofosbuvir + velpatasvir 12 ASTRAL-1 323/328 (98%) Glecaprevir + Pibrentasvir 8 ENDURANCE-1 348/351 (99%) Not Head-to-Head Trials
5 High Rates of HCV Cure Across All Regimens: GT1, Non-Cirrhotic, Tx-Experienced* Regimen Weeks Study SVR12 Sofosbuvir/ Ledipasvir (Prior Peg/RBV or PI + Peg/RBV) Elbasvir /Grazoprevir 1B and 1A (RAV-) Sofosbuvir /Velpatasvir (Prior Peg/RBV or PI + Peg/RBV) Glecaprevir/ Pibrentasvir * Previous Treatment with PEG/RBV 12 ION-2 83/87 (95%) 12 C-EDGE 190/192 (99%) 12 ASTRAL-1 109/110 (99%) 8 ENDURANCE-1 131/132 (99%) Not Head-to-Head Trials
6 Treatment-Naïve, Compensated Cirrhotic (GT1a) Regimen Weeks Study SVR12 Sofosbuvir/ledipasvir 12 ION-1 32/33 (97%) Elbasvir/grazoprevir 1a (-) NS5A RAV 12 C-EDGE 135/138 (98%) Sofosbuvir/Velpatasvir 12 ASTRAL-1 48/48 (100%) Glecaprevir /Pibrentasvir 12 EXPEDITION-1 47/48 (99%) AASLD/IDSA Recommendations for testing, managing, and treating hepatitis C. Accessed 2/26/2016. Afdhal et al. NEJM 2014; 370: Poordad et al. NEJM 2014; 370: Zeuzem et al. Ann. Int. Med. 2015; 163:1-13. Feld et al. NEJM 2015; 373:
7 Recommended Treatment Regimens (alphabetically) for Treatment-Naïve Genotype 1a Patients without Cirrhosis Recommended Daily fixed-dose combination of elbasvir/grazoprevir); for patients in whom no baseline NS5A RASs for elbasvir are detected Daily fixed-dose combination of glecaprevir/pibrentasvir Daily fixed-dose combination of ledipasvir/sofosbuvir Daily fixed-dose combination of ledipasvir/sofosbuvir; for patients who are non-black, HIV-uninfected, and whose HCV RNA level is <6 million IU/mL Daily fixed-dose combination of sofosbuvir/velpatasvir Duration 12 weeks 8 weeks 12 weeks 8 weeks 12 weeks Antiviral Treatment for HCV Infection - 7
8 Recommended Treatment Regimens (alphabetically) for Treatment-Experienced Genotype 1a Patients without Cirrhosis Recommended Daily fixed-dose combination of elbasvir/grazoprevir; for patients in whom no baseline NS5A RASs for elbasvir are detected Daily fixed-dose combination of glecaprevir/pibrentasvir Daily fixed-dose combination of ledipasvir/sofosbuvir Daily fixed-dose combination of sofosbuvir/velpatasvir Duration 12 weeks 8 weeks 12 weeks 12 weeks Antiviral Treatment for HCV Infection - 8
9 Recommended Treatment Regimens (alphabetically) for Treatment-Naïve Genotype 1a Patients with Compensated Cirrhosis Recommended Daily fixed-dose combination of elbasvir /grazoprevir; for patients in whom no baseline NS5A RASs for elbasvir are detected Daily fixed-dose combination of glecaprevir /pibrentasvir Daily fixed-dose combination of ledipasvir/sofosbuvir Daily fixed-dose combination of sofosbuvir/velpatasvir Duration 12 weeks 12 weeks 12 weeks 12 weeks Antiviral Treatment for HCV Infection - 9


10 The Therapeutic Landscape Will Not Change In The Foreseeable Future Current regimens leave no unmet needs Two promising regimens recently terminated NS5a + NUC NS5a + NUC Lawitz E, et al. AASLD 2017,#61 Zeuzem S, et al. AASLD #65



11 Pooled Analysis of Treatment Naïve GT3 Patients Treated for 8 or 12 weeks with Glecaprevir/Pibrebtasvir Similar results for 8 vs 12 weeks across all sub populations Flamm SL, et al. AASLD 2017, #62

12 Real-World Experience with Black Patients Treated for 8 Weeks VA retrospective analysis suggested that African American patients treated for 8 weeks had a ~3% lower SVR compared to Caucasian patients AASLD/IDSA Guideline suggests GT1, treatment-naïve, non-cirrhotic African American patients should be treated for 12 weeks, rather than 8-weeks for other racial groups Wilson E, et al. AASLD 2017,. #1131


13 Sofosbuvir/Velpatasvir for 12 Weeks in GT 1 4 HCV Liver Transplant Recipients No change to immunosuppression regimen Agarwal et al, AASLD 2017 #1069
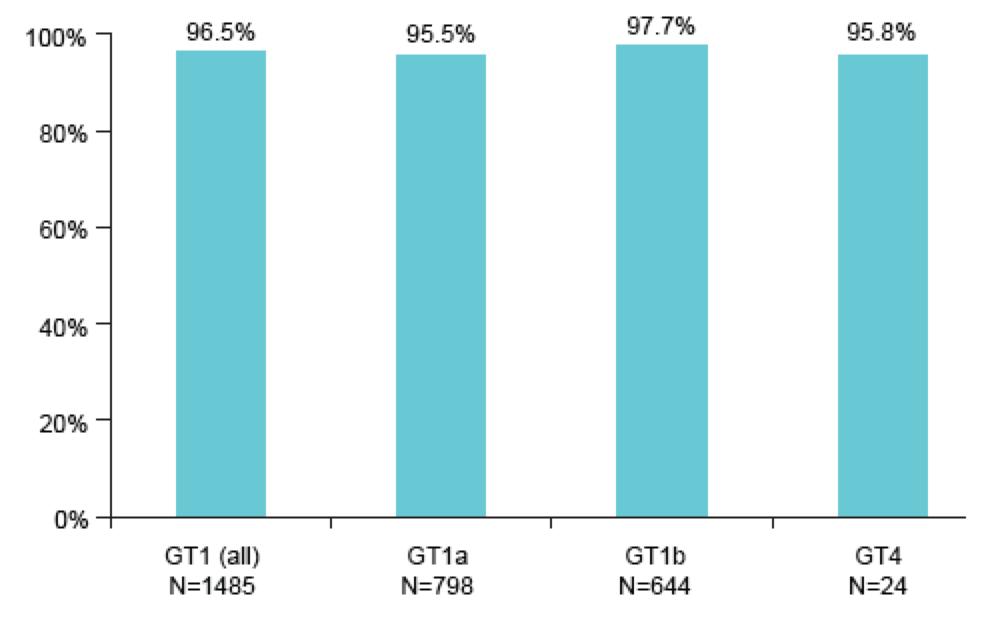
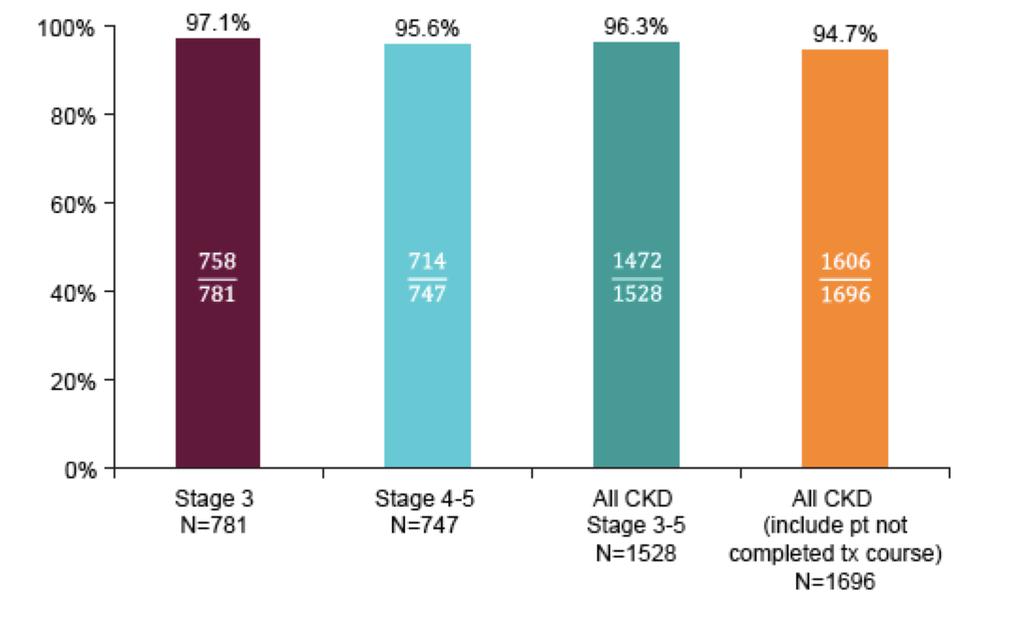
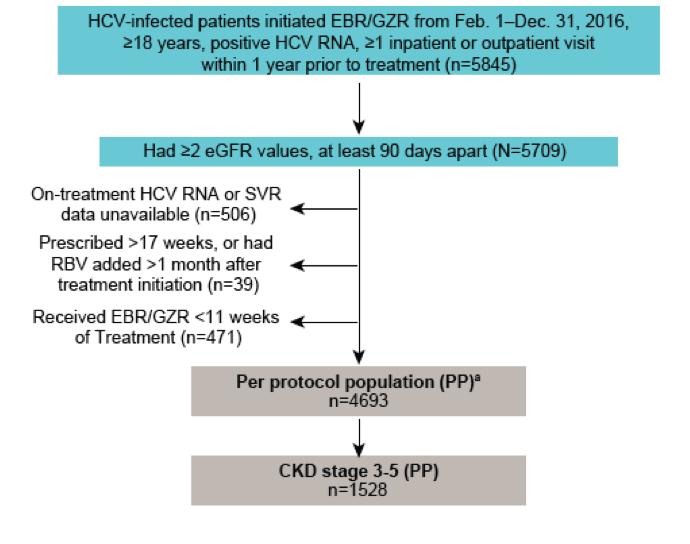
14 Elbasvir/Grazoprevir in Patients With HCV and Chronic Kidney Disease: Results From the VA Kramer et al AASLD 2017; #1113


15 SOF/VEL/VOX 12 Weeks in NS5A Experienced Patients
16 Hepatitis C is No Longer a Medical Science... It s Now a Social Science! Attributed to Ira Jacobson, 2017



17 17 Substances Contributing to Medication or Drug Overdose Deaths North Carolina Residents, * Prescription Opioid Cocaine Heroin 350% increase in deaths since 1999 Fentanyl 738 Number of deaths ,000+ Deaths per year 20,000+ Emergency Dept. visits per year 884% increase in Heroin deaths since Source: N.C. State Center for Health Statistics, Vital Statistics-Deaths, *2015 Provisional Data (August 2016) Analysis by Injury Epidemiology and Surveillance Unit
18 Acute HBV and HCV Cases in North Carolina Number of Case Reports HCV cases HBV cases
19 HCV Vulnerability Assessment of North Carolina Counties Northampton Camden Alleghany Gates Rockingham Currituck Ashe Surry Warren Stokes Caswell Person Vance Hertford Pasquotank Halifax Watauga Wilkes Granville Perquimans Yadkin Mitchell Forsyth Orange Avery Guilford Franklin Bertie Chowa Yancey Caldwell Nash n Alexander Alamance Durham Madison Davie Edgecombe Washington Burke Iredell Martin Dare Davidson Wake Tyrrell Buncombe Haywood McDowell Catawba Randolph Chatham Wilson Rowan Pitt Swain Beaufort Graham Rutherford Lincoln Johnston Hyde Jackson Henderson Lee Greene Cabarrus Cherokee Polk Stanly Cleveland Gaston Montgomery Harnett Wayne Lenoir Macon Transylvania Craven Moore Clay Pamlico Mecklenburg Cumberland Union Anson Richmond Sampson Jones Hoke Duplin Scotland Carteret Onslow Robeson Bladen Pender RED = highest injection drug use and acute HCV incidence Columbus Brunswick New Hanover Courtesy of NC DHHS
20 Meeting HCV Elimination Goals Requires Attention to Different Populations To reduce transmission: actively injecting drug users Younger, often imprisoned or homeless Low extent of liver disease SVR benefit: prevent progression to advanced fibrosis and related complications To prevent progression of disease: all patients with HCV Fibrosis progression is unpredictable Response rates remain best for those without cirrhosis who can be treated with shorter duration of therapy To reduce mortality/morbidity: cirrhotic patients Older, less likely to transmit virus Advanced fibrosis or at risk of cirrhosis/hcc SVR benefit: longer life expectancy, improved QOL, restored liver function, avoid liver transplant QOL = quality of life. NASEM. Eliminating the Public Health Problem of Hepatitis B and C in the US: Phase One Report. Washington, DC: The National Academies Press; 2016.
 Wk 12 Wk 16 Wk 28 EBR/GZR 100/50 mg QD (n = 100) Overall reinfection rate 8 patients = 4.0 reinfections/100 yrs (95% CI: 1.7 8.0) Persistent reinfection rate 5 patients = 2.")
21 Treatment of Persons Who Inject Drugs with Elbasvir/Grazoprevir: COSTAR Tx-naive pts with GT1, 4, or 6 HCV cirrhosis on opiate agonist therapy 3 mos (N = 301) SVR EBR/GZR 100/50 mg QD (n = 201) Placebo (n = 100) Wk 12 Wk 16 Wk 28 EBR/GZR 100/50 mg QD (n = 100) Overall reinfection rate 8 patients = 4.0 reinfections/100 yrs (95% CI: ) Persistent reinfection rate 5 patients = 2.5 reinfections/100 yrs (95% CI: All pts followed 24 wks post treatment Randomized, doubleblind, placebocontrolled phase III trial of PWID on Opiate Substitution Therapy Most patients tested positive for drugs during 12 weeks of therapy High rate of adherence Treating PWID is increasingly important in light of heroin epidemic and IOM report on controlling viral hepatitis by 2030 Dore et al, 2016

22 Low Risk of HCV Reinfection After Treatment with Elbasvir/Grazoprevir in Patients on OAT Open to all participants who received 1 dose of EBR/GZR in COSTAR Assessments every 6 months HCV RNA Comparison of viral sequences at baseline and virologic recurrence to determine reinfection Urine drug screen Participant-reported behaviors Behavioral questionnaire: selfreported drug use Reinfection rate was 2.3/100 person-years, with a persistent reinfection rate of 1.6/100 personyears Dore et al HEPATOLOGY (1). 195
23 HCV reinfection and injecting risk behavior following EBR/GZR treatment in participants on opiate agonist therapy (OAT): CO-STAR Part B Incidence of reinfection Part B: Part A: Part A: Through Through FW12Through FW2424 months of f/u 5 reinfections 1 reinfection 74 participants (37%) reported injection drug use Rate of reinfection: 4.2 reinfections/100 PY 95% CI: reinfections 10 reinfections 2.3 reinfections per 100 PY Increased risk of reinfection based on reported injection drug use during f/u 199 participants enrolled in Part B from the EOT through all available follow up 125 participants (63%) reported NO injection drug use Rate of reinfection: 0.4 reinfections/100 PY 95% CI: All reinfections: From EOT through 24 months of f/u 10 reinfections 426 person-years 2.3 reinfections per 100 PY (95% CI: 1.1, 4.3) Persistent reinfections: From EOT through 24 months of f/u (includes only those participants with persistent HCV RNA) 7 reinfections 429 PY 1.6 reinfections per 100 PY (95% CI: 0.7, 3.4) Clearance of reinfection was observed in 3/10 (30%) reinfection cases After SVR, IDU was stable in PWID receiving OAT (25%) Reinfection rates were low and consistent with prior estimates Dore GJ, et al. AASLD 2017, #195
24 Hepatitis C: Going the Last Mile Drug development for HCV is no longer a priority Current generation of medications fulfill all previously unmet needs Major issue now is delivering treatment to those in need Underserved populations remain a reservoir for new HCV infections Opiate epidemic fueling increasing HCV incidence among young people Injecting drug users can be successfully treated with a relatively low risk of reinfection Innovative care models are needed now to minimize future disease burden
County-Level Estimates of Non-Elderly Uninsured
 County-Level Estimates of Non-Elderly Uninsured 2006-2007 Prepared by the North Carolina Institute of Medicine & the Cecil G. Sheps Center for Health Services Research, University of North Carolina at
County-Level Estimates of Non-Elderly Uninsured 2006-2007 Prepared by the North Carolina Institute of Medicine & the Cecil G. Sheps Center for Health Services Research, University of North Carolina at
North Carolina Childhood Blood Lead Surveillance Data. 10 micrograms per deciliter ( g/dl). Confirmation is g/dl within a six-
. Confirmation is g/dl within a six-") North Carolina Childhood Blood Lead Surveillance Data 10 micrograms per deciliter ( g/dl). Confirmation is g/dl within a six- 2011 NORTH CAROLINA CHILDHOOD BLOOD LEAD SURVEILLANCE DATA, BY COUNTY Ages
North Carolina Childhood Blood Lead Surveillance Data 10 micrograms per deciliter ( g/dl). Confirmation is g/dl within a six- 2011 NORTH CAROLINA CHILDHOOD BLOOD LEAD SURVEILLANCE DATA, BY COUNTY Ages
Table A: Leading Causes of Death* by Age Group North Carolina Residents, 2016
 Table A: Leading Causes of Death* by Age Group All Ages 1 Cancer 19,526 2 Diseases of the heart 18,276 3 Chronic lower respiratory diseases 5,317 4 Cerebrovascular disease 4,941 5 Alzheimer's disease 4,152
Table A: Leading Causes of Death* by Age Group All Ages 1 Cancer 19,526 2 Diseases of the heart 18,276 3 Chronic lower respiratory diseases 5,317 4 Cerebrovascular disease 4,941 5 Alzheimer's disease 4,152
North Carolina HIV/STD Quarterly Surveillance Report: Vol. 2015, No. 1 HIV/STD Surveillance Unit
 North Carolina HIV/STD Quarterly Surveillance Report: Vol. 2015, No. 1 HIV/STD Surveillance Unit Communicable Disease Branch 1902 Mail Service Center Epidemiology Section, Division of Public Health Raleigh,
North Carolina HIV/STD Quarterly Surveillance Report: Vol. 2015, No. 1 HIV/STD Surveillance Unit Communicable Disease Branch 1902 Mail Service Center Epidemiology Section, Division of Public Health Raleigh,
North Carolina s Pilot Teleaudiology Project
 North Carolina s Pilot Teleaudiology Project Kathleen Watts, Program Manager Early Hearing Detection and Intervention North Carolina Division of Public Health Our Goals Provide infant diagnostic evaluations
North Carolina s Pilot Teleaudiology Project Kathleen Watts, Program Manager Early Hearing Detection and Intervention North Carolina Division of Public Health Our Goals Provide infant diagnostic evaluations
Managing Ammonia Emissions. ARE WE THERE YET? Past Roads, Future Paths Gary Saunders NC DENR, DAQ
 Managing Ammonia Emissions ARE WE THERE YET? Past Roads, Future Paths Gary Saunders NC DENR, DAQ Where the Farms Are If you build it, they will come The Voice, Field of Dreams NC As An Agricultural State
Managing Ammonia Emissions ARE WE THERE YET? Past Roads, Future Paths Gary Saunders NC DENR, DAQ Where the Farms Are If you build it, they will come The Voice, Field of Dreams NC As An Agricultural State
ARE WE THERE YET? Past Roads, Future Paths An Update Gary Saunders NC DENR, DAQ
 ARE WE THERE YET? Past Roads, Future Paths An Update Gary Saunders NC DENR, DAQ If you build it, they will come The Voice, Field of Dreams NC As An Agricultural State Long, established farm history Crops
ARE WE THERE YET? Past Roads, Future Paths An Update Gary Saunders NC DENR, DAQ If you build it, they will come The Voice, Field of Dreams NC As An Agricultural State Long, established farm history Crops
CAFOs/AFOs and Permitting. ARE WE THERE YET? One State s Experience with Past Roads, Future Paths Gary Saunders NC DENR, DAQ
 CAFOs/AFOs and Permitting ARE WE THERE YET? One State s Experience with Past Roads, Future Paths Gary Saunders NC DENR, DAQ Where the Farms Are If you build it, they will come The Voice, Field of Dreams
CAFOs/AFOs and Permitting ARE WE THERE YET? One State s Experience with Past Roads, Future Paths Gary Saunders NC DENR, DAQ Where the Farms Are If you build it, they will come The Voice, Field of Dreams
for Truth regional brief City and County Budget Crises When in a hole, first stop digging Joseph Coletti and Dr. Michael Sanera March 2009 Quick Facts
 regional brief No. 73 City and County Budget Crises When in a hole, first stop digging for Truth Quick Facts 200 W. Morgan, #200 Raleigh, NC 27601 phone: 919-828-3876 fax: 919-821-5117 www.johnlocke.org
regional brief No. 73 City and County Budget Crises When in a hole, first stop digging for Truth Quick Facts 200 W. Morgan, #200 Raleigh, NC 27601 phone: 919-828-3876 fax: 919-821-5117 www.johnlocke.org
Tuberculosis Statistics for North Carolina
 27 Tuberculosis Statistics for North Carolina State of North Carolina Department of Health and Human Services Division of Public Health Communicable Disease Branch Tuberculosis Control Program April 28
27 Tuberculosis Statistics for North Carolina State of North Carolina Department of Health and Human Services Division of Public Health Communicable Disease Branch Tuberculosis Control Program April 28
How many times have you participated in the Holiday Challenge?
 Eat Smart, Move More, Maintain, don t gain! Holiday Challenge Holiday Challenge Registration: 13,632 2015 Final Report Pre Challenge Survey: 5,967 (43.8% response rate) Post Challenge Survey: 2,503 (18.4%
Eat Smart, Move More, Maintain, don t gain! Holiday Challenge Holiday Challenge Registration: 13,632 2015 Final Report Pre Challenge Survey: 5,967 (43.8% response rate) Post Challenge Survey: 2,503 (18.4%
Tobacco Use Prevention Among Youth and Young Adults
 Tobacco Use Prevention Among Youth and Young Adults North Carolina Child Fatality Task Force Jim D. Martin, MS, Director of Policy and Programs N.C. Tobacco Prevention and Control Division of Public Health
Tobacco Use Prevention Among Youth and Young Adults North Carolina Child Fatality Task Force Jim D. Martin, MS, Director of Policy and Programs N.C. Tobacco Prevention and Control Division of Public Health
July Following is a guide to charts and graphs for this report:
 July 29 Strategic tourism marketing and policy decisions depend on accurate, consistent tracking of business indicators such as lodging statistics, attraction and welcome center visitation, transportation
July 29 Strategic tourism marketing and policy decisions depend on accurate, consistent tracking of business indicators such as lodging statistics, attraction and welcome center visitation, transportation
How many times have you participated in the Holiday Challenge?
 Eat Smart, Move More, Maintain, don t gain! Holiday Challenge Holiday Challenge Registration: 15,605 2016 Final Report Pre Challenge Survey: 7,732 (49.5% response rate) Post Challenge Survey: 2,428 (15.6%
Eat Smart, Move More, Maintain, don t gain! Holiday Challenge Holiday Challenge Registration: 15,605 2016 Final Report Pre Challenge Survey: 7,732 (49.5% response rate) Post Challenge Survey: 2,428 (15.6%
Tobacco Use Cessation and Prevention
 Tobacco Use Cessation and Prevention Presentation to the Justus-Warren Heart Disease and Stroke Prevention Task Force Sally Herndon, MPH N.C. Tobacco Prevention and Control Branch Division of Public Health
Tobacco Use Cessation and Prevention Presentation to the Justus-Warren Heart Disease and Stroke Prevention Task Force Sally Herndon, MPH N.C. Tobacco Prevention and Control Branch Division of Public Health
Diversion of People with Behavioral Health Disorders from the Criminal Justice System
 Diversion of People with Behavioral Health Disorders from the Criminal Justice System Robert Kurtz, Ph.D. Program Manager March 6 th 2018 Without change, large numbers of people with mental illnesses will
Diversion of People with Behavioral Health Disorders from the Criminal Justice System Robert Kurtz, Ph.D. Program Manager March 6 th 2018 Without change, large numbers of people with mental illnesses will
North Carolina Department of Health and Human Services Division of Mental Health, Developmental Disabilities and Substance Abuse Services
 North Carolina Department of Health and Human Services Division of Mental Health, Developmental Disabilities and Substance Abuse Services 3001 Mail Service Center Raleigh, North Carolina 27699-3001 Tel
North Carolina Department of Health and Human Services Division of Mental Health, Developmental Disabilities and Substance Abuse Services 3001 Mail Service Center Raleigh, North Carolina 27699-3001 Tel
ECU, Center for Health Services Research and Development, 2000
 Map 12.1 Progress Towards Pneumonia and Influenza Mortality Objective Northampton Gates Currituck Camden Pasquotank Halifax Hertford Perquimans Nash Bertie Chowan Edgecombe Martin Washington Tyrrell Dare
Map 12.1 Progress Towards Pneumonia and Influenza Mortality Objective Northampton Gates Currituck Camden Pasquotank Halifax Hertford Perquimans Nash Bertie Chowan Edgecombe Martin Washington Tyrrell Dare
A Report on Violent Injuries Treated in North Carolina Emergency Departments,
 A Report on Violent Injuries Treated in North Carolina Emergency Departments, 2012-2015 Report Prepared By: K. Harmon, A. Waller, L. Harduar Morano, and A. Ising Carolina Center for Health Informatics,
A Report on Violent Injuries Treated in North Carolina Emergency Departments, 2012-2015 Report Prepared By: K. Harmon, A. Waller, L. Harduar Morano, and A. Ising Carolina Center for Health Informatics,
EMERGENCY DEPARTMENTS
 CAROLINAS POISON CENTER BIENNIAL REPORT 2010 2011 POISONINGS LEAD TO MORE THAN 35,000 DEATHS EACH YEAR. DRUG-RELATED POISONINGS RESULT IN NEARLY 700,000 VISITS TO HOSPITAL EMERGENCY DEPARTMENTS EACH YEAR.
CAROLINAS POISON CENTER BIENNIAL REPORT 2010 2011 POISONINGS LEAD TO MORE THAN 35,000 DEATHS EACH YEAR. DRUG-RELATED POISONINGS RESULT IN NEARLY 700,000 VISITS TO HOSPITAL EMERGENCY DEPARTMENTS EACH YEAR.
ECU, Center for Health Services Research and Development, 2001
 Map 13.1 Progress Towards Diabetes Mortality Objective Northampton Gates Currituck Camden Pasquotank Halifax Hertford Perquimans Nash Bertie Chowan Edgecombe Martin Washington Tyrrell Dare Wilson Johnston
Map 13.1 Progress Towards Diabetes Mortality Objective Northampton Gates Currituck Camden Pasquotank Halifax Hertford Perquimans Nash Bertie Chowan Edgecombe Martin Washington Tyrrell Dare Wilson Johnston
Preventive Medicine 54 (2012) Contents lists available at SciVerse ScienceDirect. Preventive Medicine
 Contents lists available at SciVerse ScienceDirect. Preventive Medicine") Preventive Medicine 54 (2012) 270 276 Contents lists available at SciVerse ScienceDirect Preventive Medicine journal homepage: www.elsevier.com/locate/ypmed Burden of invasive cervical cancer in North
Preventive Medicine 54 (2012) 270 276 Contents lists available at SciVerse ScienceDirect Preventive Medicine journal homepage: www.elsevier.com/locate/ypmed Burden of invasive cervical cancer in North
North Carolina Arthritis Report 2002
 North Carolina Arthritis Report 2002 Division of Public Health March 2002 North Carolina Arthritis Report 2002 A report from Thurston Arthritis Research Center University of North Carolina at Chapel Hill
North Carolina Arthritis Report 2002 Division of Public Health March 2002 North Carolina Arthritis Report 2002 A report from Thurston Arthritis Research Center University of North Carolina at Chapel Hill
Soybean Insect Pest Management Update Ames Herbert, Virginia Tech
 Soybean Insect Pest Management Update 2012 Ames Herbert, Virginia Tech Stink bugs in soybean M. Spellman L. Schimming M. Spellman Green adult Green nymph Spined soldier bug M. Spellman Russ O=ens, UGA
Soybean Insect Pest Management Update 2012 Ames Herbert, Virginia Tech Stink bugs in soybean M. Spellman L. Schimming M. Spellman Green adult Green nymph Spined soldier bug M. Spellman Russ O=ens, UGA
Grade Growth/Gain Performance Spec. System and School(s) Span Expected Exemplary Composite Cond. Status
 Span Expected Exemplary Composite Cond. Status") 010 ALAMANCE-BURLINGTON 378 SELLARS-GUNN ALT 6 12 No No 16.4 3 040 ANSON COUNTY 305 ANSON CHALLENGE ACAD 7 12 No No 4.6 3, 6 050 ASHE COUNTY 306 ASHE COUNTY CAREER CTR UN 3 070 BEAUFORT COUNTY 310 B C
010 ALAMANCE-BURLINGTON 378 SELLARS-GUNN ALT 6 12 No No 16.4 3 040 ANSON COUNTY 305 ANSON CHALLENGE ACAD 7 12 No No 4.6 3, 6 050 ASHE COUNTY 306 ASHE COUNTY CAREER CTR UN 3 070 BEAUFORT COUNTY 310 B C
North Carolina s Injury & Violence Prevention Program
 North Carolina s Injury & Violence Prevention Program NEHA AEC 2012 San Diego, CA NC Injury & Violence Prevention Branch Home NC Division of Public Health, Chronic Disease and Injury Section Organization
North Carolina s Injury & Violence Prevention Program NEHA AEC 2012 San Diego, CA NC Injury & Violence Prevention Branch Home NC Division of Public Health, Chronic Disease and Injury Section Organization
2014 Cancer Incidence and Mortality in North Carolina
 State Center for Health Statistics February 2017 Contributing Editor Gary Leung, Ph.D. STATE OF NORTH CAROLINA Roy Cooper, Governor DEPARTMENT OF HEALTH AND HUMAN SERVICES Mandy Cohen, M.D., MPH, Secretary
State Center for Health Statistics February 2017 Contributing Editor Gary Leung, Ph.D. STATE OF NORTH CAROLINA Roy Cooper, Governor DEPARTMENT OF HEALTH AND HUMAN SERVICES Mandy Cohen, M.D., MPH, Secretary
ECU, Center for Health Services Research and Development, 2001
 Map 1.1 Progress Towards Heart Disease Mortality Objective Northampton Gates Currituck Camden Pasquotank Halifax Hertford Perquimans Nash Bertie Chowan Edgecombe Martin Washington Tyrrell Dare Wilson Johnston
Map 1.1 Progress Towards Heart Disease Mortality Objective Northampton Gates Currituck Camden Pasquotank Halifax Hertford Perquimans Nash Bertie Chowan Edgecombe Martin Washington Tyrrell Dare Wilson Johnston
NORTH CAROLINA WEEKLY INFLUENZA SURVEILLANCE SUMMARY # INFLUENZA SEASON WEEK 20: ENDING MAY 21, 2011
 Statewide Updates NORTH CAROLINA WEEKLY INFLUENZA SURVEILLANCE SUMMARY #33 2010 11 INFLUENZA SEASON WEEK 20: ENDING MAY 21, 2011 Geographic spread of influenza in the state was NO ACTIVITY. ILI activity
Statewide Updates NORTH CAROLINA WEEKLY INFLUENZA SURVEILLANCE SUMMARY #33 2010 11 INFLUENZA SEASON WEEK 20: ENDING MAY 21, 2011 Geographic spread of influenza in the state was NO ACTIVITY. ILI activity
ECU, Center for Health Services Research and Development, Communicable Diseases
 Communicable Diseases COMMUNICABLE DISEASES The second edition of the Atlas includes a new section that brings together the AIDS and Pneumonia and Influenza discussions from the previous Atlas with discussions
Communicable Diseases COMMUNICABLE DISEASES The second edition of the Atlas includes a new section that brings together the AIDS and Pneumonia and Influenza discussions from the previous Atlas with discussions
Physical Activity in the Workplace for People with Arthritis
 Physical Activity in the Workplace for People with Arthritis March 19, 2015 Leigh F. Callahan, PhD Mary Link Briggs Distinguished Professor of Medicine, Professor of Social Medicine Director, Osteoarthritis
Physical Activity in the Workplace for People with Arthritis March 19, 2015 Leigh F. Callahan, PhD Mary Link Briggs Distinguished Professor of Medicine, Professor of Social Medicine Director, Osteoarthritis
Current trends in CHC 1st genotype treatment
 Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
NORTH CAROLINA WEEKLY INFLUENZA SURVEILLANCE SUMMARY # INFLUENZA SEASON WEEK 5: ENDING FEBRUARY 7, 2015
 NORTH CAROLINA WEEKLY INFLUENZA SURVEILLANCE SUMMARY #19 2014 15 INFLUENZA SEASON WEEK 5: ENDING FEBRUARY 7, 2015 Statewide Updates Influenza-like illness decreased during week 5. The geographic spread
NORTH CAROLINA WEEKLY INFLUENZA SURVEILLANCE SUMMARY #19 2014 15 INFLUENZA SEASON WEEK 5: ENDING FEBRUARY 7, 2015 Statewide Updates Influenza-like illness decreased during week 5. The geographic spread
10/21/2016. Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina. Learning Objectives
 A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
School Calendar Information
 2016-2017 School Calendar Information State County First Day Spring Break Last Day Georgia Kentucky New York Georgia Atlanta 8/3/2016 April 3-7 5/25/2017 Augusta 8/4/2016 April 3-7 5/23/2017 Marietta 8/3/2016
2016-2017 School Calendar Information State County First Day Spring Break Last Day Georgia Kentucky New York Georgia Atlanta 8/3/2016 April 3-7 5/25/2017 Augusta 8/4/2016 April 3-7 5/23/2017 Marietta 8/3/2016
Treatment of Unique Populations Raymond T. Chung, MD
 Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Treatment of Unique Populations Raymond T. Chung, MD Director of Hepatology and Liver Center Vice Chief, Gastroenterology Kevin and Polly Maroni Research Scholar Mass General Hospital Disclosures Research
Flu Information and Guidance
 NORTH CAROLINA WEEKLY INFLUENZA SURVEILLANCE SUMMARY #21 2015 16 INFLUENZA SEASON WEEK 8: ENDING FEBRUARY 27, 2016 Statewide Updates Influenza-like illness (ILI) increased this week. The geographic spread
NORTH CAROLINA WEEKLY INFLUENZA SURVEILLANCE SUMMARY #21 2015 16 INFLUENZA SEASON WEEK 8: ENDING FEBRUARY 27, 2016 Statewide Updates Influenza-like illness (ILI) increased this week. The geographic spread
Community Cancer Needs Assessment
 Community Cancer Needs Assessment Standard 3.1 JEAN B. SELLERS, RN, MSN ADMINISTRATIVE CLINICAL DIRECTOR LINEBERGER COMPREHENSIVE CANCER CENTER MEGAN L. CARLSON, MPH LAY NAVIGATION PROGRAM MANAGER LINEBERGER
Community Cancer Needs Assessment Standard 3.1 JEAN B. SELLERS, RN, MSN ADMINISTRATIVE CLINICAL DIRECTOR LINEBERGER COMPREHENSIVE CANCER CENTER MEGAN L. CARLSON, MPH LAY NAVIGATION PROGRAM MANAGER LINEBERGER
RECOMMENDATION FOR THE MANAGEMENT OF HEPATITIS C VIRUS INFECTION AMONG PEOPLE WHO INJECT DRUGS
 RECOMMENDATION FOR THE MANAGEMENT OF HEPATITIS C VIRUS INFECTION AMONG PEOPLE WHO INJECT DRUGS The International Network on Hepatitis in Substance users (INHSU) Olav Dalgard Oslo Grebely J et al Int J
RECOMMENDATION FOR THE MANAGEMENT OF HEPATITIS C VIRUS INFECTION AMONG PEOPLE WHO INJECT DRUGS The International Network on Hepatitis in Substance users (INHSU) Olav Dalgard Oslo Grebely J et al Int J
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
REQUESTS FOR NO-REVIEW DETERMINATIONS
 REQUESTS FOR NO-REVIEW DETERMINATIONS 10.22.2008 Please Note: The no-review and declaratory ruling information in the reports was obtained from the N.C. Department of Health and Human Services. Williams
REQUESTS FOR NO-REVIEW DETERMINATIONS 10.22.2008 Please Note: The no-review and declaratory ruling information in the reports was obtained from the N.C. Department of Health and Human Services. Williams
HARVARD PILGRIM HEALTH CARE RECOMMENDED MEDICATION REQUEST GUIDELINES
 HARVARD PILGRIM HEALTH CARE Generic Brand HICL GCN Exception/Other DACLATASVIR DAKLINZA 41377 ELBASVIR/GRAZOPREVIR ZEPATIER 43030 GLECAPREVIR/PIBRENTASVIR MAVYRET 44453 OMBITASVIR/PARITAPREVIR/ RITONAVIR
HARVARD PILGRIM HEALTH CARE Generic Brand HICL GCN Exception/Other DACLATASVIR DAKLINZA 41377 ELBASVIR/GRAZOPREVIR ZEPATIER 43030 GLECAPREVIR/PIBRENTASVIR MAVYRET 44453 OMBITASVIR/PARITAPREVIR/ RITONAVIR
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Management of HCV in Prior Treatment Failure
 Management of HCV in Prior Treatment Failure Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending this presentation, learners
Management of HCV in Prior Treatment Failure Arthur Y. Kim, MD Associate Professor of Medicine Harvard Medical School Boston, Massachusetts Learning Objectives After attending this presentation, learners
NC Council for Women & Youth Involvement (NCCFW/YI) N.C Council for Women & Youth Involvement s Mission
 N.C Council for Women & Youth Involvement s Mission") N.C Council for Women & Youth Involvement s Mission The NC Council for Women & Youth Involvement s (NCCFW/YI) mission is to advise the Governor, the North Carolina legislature & state agencies on the issues
N.C Council for Women & Youth Involvement s Mission The NC Council for Women & Youth Involvement s (NCCFW/YI) mission is to advise the Governor, the North Carolina legislature & state agencies on the issues
NASW-NC Local Program Unit Manual Page 1 of 17. Local Program Unit Manual
 Page 1 of 17 Local Program Unit Manual Revised October 2014 Page 2 of 17 TABLE OF CONTENTS NASW-NC LPU Chairperson Guidelines and Quick Facts....3 The Purpose of Local Program Units (LPUs). 4 The Structure
Page 1 of 17 Local Program Unit Manual Revised October 2014 Page 2 of 17 TABLE OF CONTENTS NASW-NC LPU Chairperson Guidelines and Quick Facts....3 The Purpose of Local Program Units (LPUs). 4 The Structure
What is the Optimized Treatment Duration? To Overtreat versus Undertreat. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
Drug Class Prior Authorization Criteria Hepatitis C
 Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim (pending P&T approval) Effective Date: July 1, 2018 This policy has been developed through review
Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim (pending P&T approval) Effective Date: July 1, 2018 This policy has been developed through review
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
Drug Class Prior Authorization Criteria Hepatitis C
 Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim Criteria Pending P&T Approval Effective Date: August 16, 2018 This drug class prior authorization
Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: Interim Criteria Pending P&T Approval Effective Date: August 16, 2018 This drug class prior authorization
Update on Hepatitis C. Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017
 Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
Update on Hepatitis C Francesco Negro Hôpitaux Universitaires de Genève Berne, November 15, 2017 The global prevalence of HCV was 1 0% (95% uncertainty interval 0 8 1 1) in 2015: 71 1 million (62 5 79
Hepatitis C in Disclosures
 Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Hepatitis C in 2018 Sandeep Mukherjee, MD CHI Health and Creighton University Medical Center Division of Gastroenterology Grant support: Abbvie Disclosures Speaker: Abbvie, Gilead, Merck Section editor
Hepatitis C Introduction and Overview
 Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Hepatitis C Introduction and Overview Michael S. Saag, MD Professor of Medicine Associate Dean of Global Health Director, Center for AIDS Research University of Alabama at Birmingham Birmingham, Alabama
Glecaprevir-Pibrentasvir in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2)
") Phase 3 Treatment-Experienced in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2) in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2): Study Features MAGELLAN-1 (Part 2) Trial Design: Randomized,
Phase 3 Treatment-Experienced in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2) in HCV GT 1 or 4 & Prior DAA Treatment MAGELLAN-1 (Part 2): Study Features MAGELLAN-1 (Part 2) Trial Design: Randomized,
Management of Chronic HCV 2017 and Beyond
 Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
Management of Chronic HCV 2017 and Beyond Blaire E Burman, MD Virginia Mason Gastroenterology & Hepatology Relevant Disclosures No financial disclosures to report Leaning Objectives Burden of HCV Prevalence
Individual Optmizaton of therapy. Graham R Foster Professor of Hepatology QMUL
 Individual Optmizaton of therapy Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novarts, Springbank,
Individual Optmizaton of therapy Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novarts, Springbank,
HEPATITIS C: UPDATE AND MANAGEMENT
 HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
HEPATITIS C: UPDATE AND MANAGEMENT José Franco, MD Professor of Medicine Associate Dean for Educational Improvement Associate Director, Kern Institute STAR Center Director José Franco, MD Disclosures I
Drug Class Prior Authorization Criteria Hepatitis C
 Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: November 14, 2018 Effective Date: January 1, 2019 This drug class prior authorization criteria have been
Drug Class Prior Authorization Criteria Hepatitis C Line of Business: Medicaid P & T Approval Date: November 14, 2018 Effective Date: January 1, 2019 This drug class prior authorization criteria have been
Hepatitis C Prior Authorization Policy
 Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Hepatitis C Prior Authorization Policy Line of Business: Medi-Cal P&T Approval Date: November 15, 2017 Effective Date: January 1, 2018 This policy has been developed through review of medical literature,
Eliminating Hepatitis C from New Zealand
 Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
Eliminating Hepatitis C from New Zealand Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures I have the following
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline
 PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir ) Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir)
CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015
 CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015 CCO Official Conference Coverage of the 2015 Annual Meeting of the American Association for the Study of Liver Diseases, November
CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015 CCO Official Conference Coverage of the 2015 Annual Meeting of the American Association for the Study of Liver Diseases, November
Disclosures. Advanced HCV management. Overview. Renal failure 1/10/2018. Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH
 Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
Disclosures Advanced HCV management Annie Luetkemeyer, MD Division of HIV, ID and Global Medicine ZSFG, UCSF Research Grant support to UCSF from AbbVie Gilead Merck Proteus NIH Overview Renal failure Acute
Hepatitis C Update: Screening, Diagnosis, and Treatment
 Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
Mountain West AIDS Education and Training Center Hepatitis C Update: Screening, Diagnosis, and Treatment Brian R. Wood, MD (bwood2@uw.edu) Assistant Professor of Medicine, University of Washington Medical
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
Hepatitis C Difficult to Treat. Population. Disclosures
 Hepatitis C Difficult to Treat Populations Paul Y Kwo MD Professor of Medicine Director of Hepatology Stanford University School of Medicine 75 Welch Road #21 Palo Alto, CA 9434 Disclosures Advisory Board
Hepatitis C Difficult to Treat Populations Paul Y Kwo MD Professor of Medicine Director of Hepatology Stanford University School of Medicine 75 Welch Road #21 Palo Alto, CA 9434 Disclosures Advisory Board
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret
 New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
New Antivirals for Hep C in Context of HIV: Vosevi and Mavyret John Scott, MD, MSc, FIDSA November 16, 2017 This presentation is intended for educational use only and does not in any way constitute medical
Viva La Revolución: Options to Combat Hepatitis C
 Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Hepatitis C Elimination: Screening, Linkage and Treatment. Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas
 Hepatitis C Elimination: Screening, Linkage and Treatment Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas Hepatitis C: Worldwide Presence Worldwide prevalence: 130-150 million Viral hepatitis
Hepatitis C Elimination: Screening, Linkage and Treatment Eric Lawitz, MD The Texas Liver Institute San Antonio, Texas Hepatitis C: Worldwide Presence Worldwide prevalence: 130-150 million Viral hepatitis
Hepatitis C in Special Populations
 Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
PHARMACY PRIOR AUTHORIZATION Hepatitis C Clinical Guideline
 Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir) PHARMACY PRI AUTHIZATION Hepatitis C Clinical Guideline Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir) Harvoni
Preferred Regimen Based on Diagnosis: Mavyret (glecaprevir/pibrentasvir) PHARMACY PRI AUTHIZATION Hepatitis C Clinical Guideline Non-Preferred: Daklinza (daclatasvir) Epclusa (sofosbuvir/velpatasvir) Harvoni
Treating Hepatitis C Virus (HCV) Infection
 Infection") Slide 1 of 42 Treating Hepatitis C Virus (HCV) Infection Susanna Naggie, MD, MHS Associate Professor of Medicine Duke Clinical Research Institute Durham, North Carolina Slide 3 of 42 Learning Objectives
Slide 1 of 42 Treating Hepatitis C Virus (HCV) Infection Susanna Naggie, MD, MHS Associate Professor of Medicine Duke Clinical Research Institute Durham, North Carolina Slide 3 of 42 Learning Objectives
STATE OF THE ART Update: Treatment Options 2016 Mark Sulkowski, MD
 Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany
 Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
Hepatitis C: Difficult-to-treat Patients 11th Paris Hepatology Conference 16th January 2018 Stefan Zeuzem, MD University Hospital, Frankfurt, Germany PHC 2018 - www.aphc.info Disclosures Advisory boards:
North Carolina Triangle to the Coast Affiliate of Susan G. Komen Quantitative Data Report
 North Carolina Triangle to the Coast Affiliate of Susan G. Komen Quantitative Data Report 2015-2019 Contents 1. Purpose, Intended Use, and Summary of Findings... 4 2. Quantitative Data... 6 2.1 Data Types...
North Carolina Triangle to the Coast Affiliate of Susan G. Komen Quantitative Data Report 2015-2019 Contents 1. Purpose, Intended Use, and Summary of Findings... 4 2. Quantitative Data... 6 2.1 Data Types...
Special developments in the management of Hepatitis C. Disclosures
 Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
Special developments in the management of Hepatitis C Sandeep Mukherjee,MD Division of Gastroenterology CHI Health and Creighton University Medical Center Omaha, NE 68154 Sandeep.Mukherjee@alegent.org
HCV in 2017: New Therapies and New Opportunities. Presentation prepared by: Date prepared: OBJECTIVES
 Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Project ECHO HCV Collaborative HCV in 217: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College of Pharmacy University
Cases: Initial Treatment of Hepatitis C
 Cases: Initial Treatment of Hepatitis C Kristen Marks, MD Assistant Professor of Medicine Weill Cornell Medical College New York, New York Off-Label Warning I will discuss the following off-label use in
Cases: Initial Treatment of Hepatitis C Kristen Marks, MD Assistant Professor of Medicine Weill Cornell Medical College New York, New York Off-Label Warning I will discuss the following off-label use in
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD
 Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD") Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Not good for children and other living things Blue Ridge Environmental Defense League June 2012
 Weakening North Carolina s Air Toxics Regulations: Not good for children and other living things Blue Ridge Environmental Defense League June 2012 What s Going On? Industry-backed legislation currently
Weakening North Carolina s Air Toxics Regulations: Not good for children and other living things Blue Ridge Environmental Defense League June 2012 What s Going On? Industry-backed legislation currently
Australasian Professional Society on Alcohol and other Drugs, Annual Conference 2016 Sydney Australia
 Efficacy and safety of ledipasvir/sofosbuvir with and without ribavirin in patients with chronic HCV genotype 1 infection receiving opioid substitution therapy: Analysis of Phase 3 ION trials J Grebely
Efficacy and safety of ledipasvir/sofosbuvir with and without ribavirin in patients with chronic HCV genotype 1 infection receiving opioid substitution therapy: Analysis of Phase 3 ION trials J Grebely
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
The Changing World of Hepatitis C
 The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
The Changing World of Hepatitis C Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia St. Paul s Hospital Site Disclosures
Genotype 1 HCV in 2016: Clinical Decision Making in a Time of Plenty
 Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Hepatitis C Genotypes
 9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
9/2/21 OBJECTIVES Project ECHO HCV Collaborative HCV in 21: New Therapies and New Opportunities Paulina Deming, PharmD Assistant Director Hepatitis C Programs, ECHO Institute Associate Professor College
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy
 Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
Monitoring Patients Who Are Starting HCV Treatment, Are On Treatment, Or Have Completed Therapy WV ECHO August 10, 2017 Selection of patients for HCV treatment Despite current guidance to treat everyone,
Minimizing treatment duration and doses
 Minimizing treatment duration and doses Jordan J. Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto Disclosures Research: Abbvie, Gilead, Janssen,
Minimizing treatment duration and doses Jordan J. Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto Disclosures Research: Abbvie, Gilead, Janssen,
Treatment of Hepatitis C in People Who Inject Drugs (PWIDs) Andrew Seaman, MD OHA P&T Meeting January, 2017
 Andrew Seaman, MD OHA P&T Meeting January, 2017") Treatment of Hepatitis C in People Who Inject Drugs (PWIDs) Andrew Seaman, MD OHA P&T Meeting January, 2017 Conflicts of interest Receive
Treatment of Hepatitis C in People Who Inject Drugs (PWIDs) Andrew Seaman, MD OHA P&T Meeting January, 2017 Conflicts of interest Receive
Universal HCV treatment: Strategies for simplification
 Universal HCV treatment: Strategies for simplification PARIS HEPATOLOGY CONFERENCE 3 January 217 Tarik Asselah (MD, PhD) Hepatology & Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures
Universal HCV treatment: Strategies for simplification PARIS HEPATOLOGY CONFERENCE 3 January 217 Tarik Asselah (MD, PhD) Hepatology & Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures
IFN-free therapy in naïve HCV GT1 patients
 IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
Shorter Durations and Pan-genotypic Regimens The Final Frontier. Professor Greg Dore
 Shorter Durations and Pan-genotypic Regimens The Final Frontier Professor Greg Dore Disclosures Funding and speaker fees from AbbVie, Bristol-Myers Squibb, Gilead Sciences and Merck Efficacy Evolution
Shorter Durations and Pan-genotypic Regimens The Final Frontier Professor Greg Dore Disclosures Funding and speaker fees from AbbVie, Bristol-Myers Squibb, Gilead Sciences and Merck Efficacy Evolution
HCV Treatment Options in 2017/2018: What s Here and What s Coming Soon
 HCV Treatment Options in 2017/2018: What s Here and What s Coming Soon Supported by educational grants from AbbVie; Bristol-Myers Squibb; Gilead Sciences; Janssen Therapeutics; Merck & Co., Inc; and ViiV
HCV Treatment Options in 2017/2018: What s Here and What s Coming Soon Supported by educational grants from AbbVie; Bristol-Myers Squibb; Gilead Sciences; Janssen Therapeutics; Merck & Co., Inc; and ViiV
HCV Resistance Clinical Aspects. Sanjay Bhagani Royal Free Hospital/UCL London
 HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
Hepatitis C Resistance Associated Variants (RAVs)
") Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Hepatitis C Resistance Associated Variants (RAVs) Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Nothing to disclose Disclosure
Impatto della clearance virale e rischio di carcinoma epatocellulare
 EPATITE CRONICA DA HCV: Impatto della clearance virale e rischio di carcinoma epatocellulare Rodolfo Sacco, M.D., PhD Direttore U.O.C. Gastroenterologia ed Endoscopia Digestiva A.O.U. Ospedali Riuniti"
EPATITE CRONICA DA HCV: Impatto della clearance virale e rischio di carcinoma epatocellulare Rodolfo Sacco, M.D., PhD Direttore U.O.C. Gastroenterologia ed Endoscopia Digestiva A.O.U. Ospedali Riuniti"
What Should We Do With Difficult to Treat HCV Populations?
 What Should We Do With Difficult to Treat HCV Populations? Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah
What Should We Do With Difficult to Treat HCV Populations? Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah
A treatment revolution: current management for chronic HCV
 A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
Treatment of HCV : 100 % cure?
 Treatment of HCV : % cure? PHC 8 PARIS January 5th, 8 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief ISERM UMR 49, Hôpital Beaujon, Clichy, France. PHC 8 - www.aphc.info Disclosures Employee
Treatment of HCV : % cure? PHC 8 PARIS January 5th, 8 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief ISERM UMR 49, Hôpital Beaujon, Clichy, France. PHC 8 - www.aphc.info Disclosures Employee