Opioid Dependence and Its Treatment. Laura F. McNicholas, M.D., Ph.D. CMJC VAMC, Philadelphia University of Pennsylvania, Dept of Psychiatry
|
|
|
- Rosanna Tyler
- 6 years ago
- Views:
Transcription
1 Opioid Dependence and Its Treatment Laura F. McNicholas, M.D., Ph.D. CMJC VAMC, Philadelphia University of Pennsylvania, Dept of Psychiatry
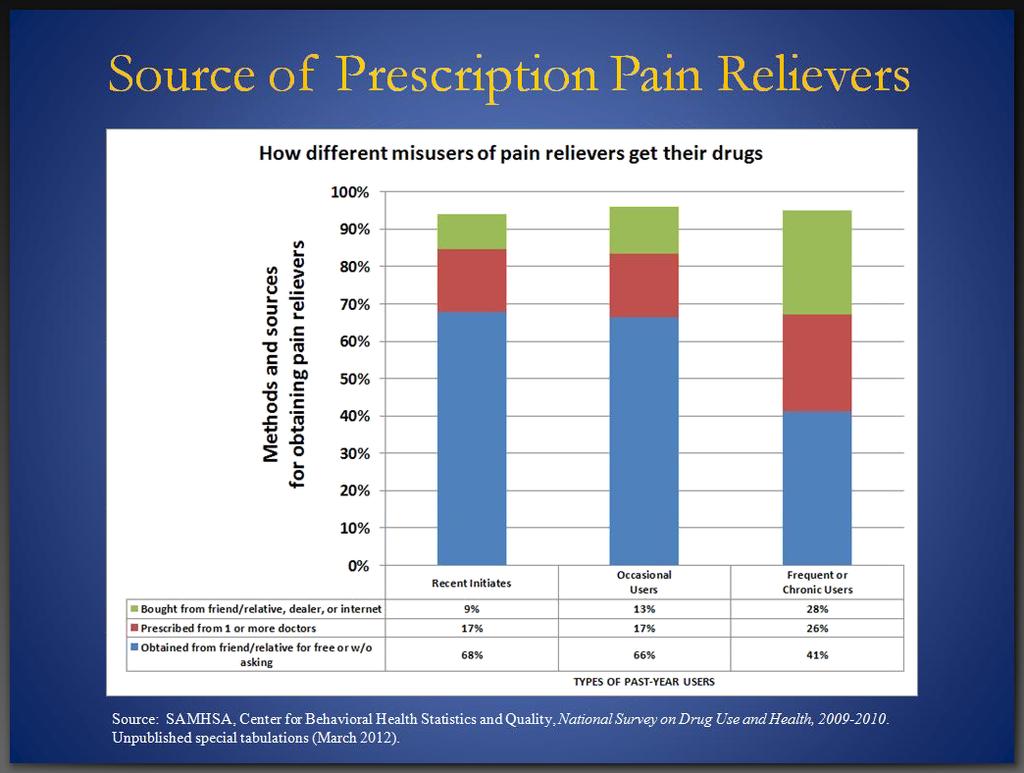
2 NSDUH 2013
3 NSDUH 2013
4 NSDUH 2013

5 NSDUH 2013
6
7 Commonly Abused Opioids Diacetylmorphine (Heroin) Hydromorphone (Dilaudid) Oxycodone (OxyContin, Percodan, Percocet, Tylox) Meperidine (Demerol) Hydrocodone (Lortab, Vicodin) recently moved from C-III to C-II
8 Commonly Abused Opioids (continued) Morphine (MS Contin, Oramorph) Fentanyl (Sublimaze) Propoxyphene (Darvon) Methadone (Dolophine) Codeine Opium
9 Commonly Abused Opioids Opioids are abused by all routes of administration including oral, inhalation, smoking, and injection. Heroin is most commonly used intranasally or intravenously, but can be inhaled, smoked, or injected intramuscularly or subcutaneously. Opium is usually smoked. The pharmaceutical opioids are usually taken orally (but may also be injected).
10 Psychiatric Assessment Features of Disorders Opioid intoxication and withdrawal It is important to recognize and distinguish symptoms of opioid intoxication and withdrawal, since their symptomatic presentations can overlap with the signs and symptoms of other psychiatric disorders.
11 Psychiatric Assessment Features of Disorders Opioid intoxication Signs and symptoms: Feeling of high or euphoria Pupillary constriction Drowsiness or coma Slurred speech Impaired attention or memory
12 Psychiatric Assessment Features of Disorders Opioid withdrawal Occurs after stopping or decreasing use that has been occurring regularly (e.g., daily for weeks) this is spontaneous withdrawal Note it can also occur if person receives a dose of an opioid antagonist or partial agonist this is precipitated withdrawal
13 Psychiatric Assessment Features of Disorders Opioid withdrawal Signs and symptoms: Dysphoric mood Nausea or vomiting Muscle aches/cramps Lacrimation Rhinorrhea
14 Psychiatric Assessment Features of Disorders Opioid withdrawal (continued) Pupillary dilation Sweating, piloerection Diarrhea Yawning Fever Insomnia
15 Endogenous Opioid System Unknown early 70 s, remained unproven - Recognized, opiate receptor binding sites in the brain discovered Three distinct families of opioid peptides - Enkephalins - Endorphins - Dynorphins Reference: Opioid Analgesics, Chapter 21, Goodman and Gilman s The Pharmacological Basis of Therapeutics, 11th edition.
16 Opioid Receptors Mu (MOR) Subtypes: µ 1, µ 2 Kappa (KOR) Subtypes: κ 1, κ 2, κ 3 Delta (DOR) Subtypes: δ 1, δ 2 Reference: Opioid Analgesics, Chapter 21, Goodman and Gilman s The Pharmacological Basis of Therapeutics, 11th edition.
17
18 Opioid Effects upon Physiological Systems Produce analgesia Affect mood Affect rewarding behavior Alter respiratory function Alter cardiac function Alter gastrointesintal function Alter neuroendocrine function References: Opioid Analgesics, Chapter 21, Goodman and Gilman s The Pharmacological Basis of Therapeutics, 11th edition. Tafton JA, Abhinav R, Methadone: A New Old Drug With Promises and Pitfalls, Current Pain and Headache Reports :24-30
19 Respiratory Direct effect on brainstem respiratory centers - Reduction in responsiveness to carbon dioxide Depress all phases of respiratory activity (rate, minute volume, tidal exchange) Rate may fall to 3-4 breaths/min Underlying pulmonary dysfunction
20 Opioid Physiological Effects Cough - Depress cough center in the medulla Anti-Nausea/Emetic - Stimulation of chemoreceptor trigger zone in the medulla Skin - Dilatation of cutaneous blood vessels - Sweating, pruritus Cardiovascular - Peripheral vasodilation - Peripheral resistance Gastrointestinal - Decrease gastric motility, prolongs gastric emptying - Bilary tract, constricts Sphincter of Odi, epigastric distress to typical biliary colic References: Opioid Analgesics, Chapter 21, Goodman and Gilman s The Pharmacological Basis of Therapeutics, 11th edition. Tafton JA, Abhinav R, Methadone: A New Old Drug With Promises and Pitfalls, Current Pain and Headache Reports :24-30
21 Opioid Physiological Effects Ureter / Urinary Bladder - Smooth muscle tone, combined with antidiuretic decrease urine flow Immune System - Complex, acute and chronic - Overall suppression - Different opioid agonist have unique immunomodulatory properties Hypothalamus - Morphine inhibits GnRH, CRH LH, FSH, ACTH and β-endorphins - Pituitary concentrations of testosterone and cortisol decline - Women (Methadone) - Chronic administration, tolerance develops, menstrual cycles normalize after disruption due to heroin - Men (Methadone) - Chronic administration, tolerance to hypothalamic releasing factors develops, circulation concentrations of LH and testosterone are wnl - Antidiuretic effect urinary retention References: Opioid Analgesics, Chapter 21, Goodman and Gilman s The Pharmacological Basis of Therapeutics, 11th edition. Tafton JA, Abhinav R, Methadone: A New Old Drug With Promises and Pitfalls, Current Pain and Headache Reports :24-30
22 Heroin Simulated 24 Hr. Dose/Response With established heroin tolerance/dependence Dose Response Loaded High Normal Range Comfort Zone Subjective w/d Abnormal Normality Sick Objective w/d 0 hrs. Time 24 hrs. 22
23 Methadone Simulated 24 Hr. Dose/Response At steady-state in tolerant patient Dose Response Loaded High Normal Range Comfort Zone Subjective w/d Abnormal Normality Sick Objective w/d 0 hrs. Time 24 hrs. 23
24 Medication Options Agonists: - Methadone - Buprenorphine Antagonists: - Naltrexone, p.o. - Naltrexone depot
25 Rationale for opioid agonist medications Advantages of opioid agonist medication over heroin Non-parenteral administration Known composition Gradual onset and offset Long-acting Mildly reinforcing Medically supervised
26 Rationale for opioid agonist medications Opioid agonist treatment Most effective treatment for opioid dependence Controlled studies have shown significant: Decreases in illicit opioid use Decreases in other drug use Decreases in criminal activity Decreases in needle sharing Improvements in prosocial activities Improvements in mental health
27 Methadone
28 OUTCOMES Effectiveness of Treatment: 28
29 Early Efficacy & Outcome Studies Retention - VS. TC and Drug Free - NYC, DARP, & TOPS (>40K patients) Retention relative to dose/placebo - Newman, Strain, & Caplehorn Reincarceration and heroin use - Dole, Newman & Whitehill ( 69 & 76)

30 Efficacy: Retention Studies Methadone Modality

31 Efficacy: Retention Studies Methadone Modality by Dose
32 Evidence-Based Practices: Elements to Maximize OAT Outcomes Adequate Methadone Dose Availability of counseling Maintenance versus abstinence/detoxification program orientation Contingency management with focus on positive and immediate reinforcement/rewards Source: Opioid Agonist Therapy Monitoring System (OMS) Willenbring et al
33 What Does OMT DO? Impact of Treatment! 33
34 Impact of Maintenance Treatment Ø Reduction death rates (Grondblah, 90) Ø Reduction IVDU (Ball & Ross, 91) Ø Reduction crime days (Ball & Ross) Ø Reduction rate of HIV seroconversion (Bourne, 88; Novick 90,; Metzger 93) Ø Reduction relapse to IVDU (Ball & Ross) Ø Improved employment, health, & social function 34


35 % Annual Death Rates DEATH RATES IN TREATED AND UNTREATED HEROIN ADDICTS Slide data courtesy of Frank Vocci, MD, NIDA - Reference: Grondblah, L. et al. ACTA PSCHIATR SCAND, P ,
36 Impact of MMT on IV Drug Use for 388 Male MMT Patients in 6 Programs 100% 10 0 PERCENT IV USERS 0 LAST ADDICTION PERIOD ADMISSION 81.4% 63.3% Pre- 1st Year 2nd Year 3rd Year 4th Year Admission Adapted from Ball & Ross - The Effectiveness of Methadone Maintenance Treatment, 1991 * 41.7% * 28.9%

37 Crime among 491 patients before and during MMT at 6 programs Crime Days Per Year Adapted from Ball & Ross - The Effectiveness of Methadone Maintenance Treatment,
38 HIV Infection Rates by Treatment Status at Time of Enrollment 60% In Treatment Out of Treatment 51% Percent Testing Positive 50% 40% 30% 21% 39% 18% 21% 20% 13% 10% 0% Treatment Research Institute B Baseline through 36 Months


39 Relapse to IV drug use after MMT 105 male patients who left treatment Percent IV Users Treatment Adapted from Ball & Ross - The Effectiveness of Methadone Maintenance Treatment, 1991 Months Since Stopping Treatment

40 McLellan, et al, 1993
41 Other Pharmacotherapies for Maintenance Treatment of Opioid Dependence: Buprenorphine, Buprenorphine/Naloxone and Naltrexone
42 Buprenorphine and Buprenorphine/Naloxone
43 Intrinsic Activity: Full Agonist (Methadone), Partial Agonist (Buprenorphine), Antagonist (Naloxone) Full Agonist (Methadone) % Efficacy Log Dose of Opioid Partial Agonist (Buprenorphine Antagonist (Naloxone)
44 Affinity and Dissociation Buprenorphine has: high affinity for mu opioid receptor competes with other opioids and blocks their effects slow dissociation from mu opioid receptor prolonged therapeutic effect for opioid dependence treatment

45 Zubieta et al.,
46 Potential for Physical Dependence Repeated administration of buprenorphine produces or maintains physical dependence However, degree of physical dependence is less than that produced by full agonist opioids This means withdrawal syndrome should be less severe for buprenorphine
47 Rationale for Buprenorphine/naloxone When taken sublingually - Buprenorphine will be well absorbed - Naloxone absorption will be minimal If taken intravenously - Naloxone 100% bioavailable - Precipitated withdrawal occurs in opioid maintained patients
48 Buprenorphine/naloxone infusion Study on methadone maintained patients (Mendelson) Looked at 6 patients on stable methadone doses of 45 to 60 mg/ day Challenged IV with - Buprenorphine 0.2 mg - Naloxone 0.1 mg - Buprenorphine 0.2 and Naloxone 0.1 mg - Placebo
49 PEAK EFFECTS MEAN (±SD) Bad Drug Effect (0-100) Bad Drug Sickness Scale (0-100) Sickness 0 A B C D A Buprenorphine placebo, Naloxone placebo B Buprenorphine 0.2 mg, Naloxone placebo D 0 A B C C Buprenorphine placebo, Naloxone 0.1 mg Buprenorphine 0.2 mg, Naloxone 0.1 mg D
50 Intoxication (0-100) Withdrawal (0-100) H H H H 20 H H H 16 H B B B H B H B H B H 12 B B 8 B 4 B B B B 0 J H F J F J F J F J F J F J F F J J F J F J F J F J F J J J J J J 30 B B J B B J 20 B J J J J J B B H F F F F 10 F F F B F B F F F F F B B B B 0 H H H H H H H H H H H H Minutes B Bup/Nal J Naloxone H Buprenorphine F Placebo Mean Peak Amount Would Pay for Drug Bup/Nal $ 1.90 ± 3.70 Naloxone 0.00 ± 0.00 Buprenorphine ± 7.00 Placebo 0.00 ± 0.00
51 Benzodiazepines and Other Sedating Drugs Reports of deaths when buprenorphine injected along with benzodiazepines Reported from France, where tablets available appears patients dissolve and inject tablets Probably possible for this to occur with other sedatives as well
52 Maintenance Treatment Using Buprenorphine Numerous outpatient clinical trials comparing efficacy of daily buprenorphine to placebo, and to methadone.
53 Maintenance Treatment Using Buprenorphine These studies conclude: Buprenorphine more effective than placebo Buprenorphine equally effective as moderate doses of methadone (e.g., 60 mg per day)
54 Different Doses of Buprenorphine: Opiate Use 25 % Ss With 13 Consecutive Opiate Free Urines Buprenorphine dose (mg) (Ling et al., 1998)
55 Buprenorphine, Methadone, LAAM: Treatment Retention % Hi Meth Percent Retained % Bup 53% LAAM 20% Lo Meth Study Week Adapted from Johnson, et al., 2000
56 Buprenorphine, Methadone, LAAM: Opioid Urine Results Mean % Negative All Subjects 49% 39% 19% 40% LAAM Bup Hi Meth Lo Meth Study Week Adapted from Johnson, et al., 2000
57 Buprenorphine methadone: treatment retention Percent Buprenorphine 20 Methadone Week (Strain et al., 1994)
58 Buprenorphine methadone: opioid urine results Buprenorphine Methadone Stabilization (n=47) (n=45) Detoxification (n=22) (n=19) Percent Positive Week (Strain et al., 1994)
59
60 PATIENT SELECTION Issues related to recommending buprenorphine over methadone: Psychiatric co-morbidities Substance abuse co-morbidity BZD s and alcohol Policy regarding take-home doses Finances
61 POLICY ISSUES Other policy issues: Whether to offer buprenorphine at all Patient selection
62 POLICY ISSUES What to do if patient refuses physician recommendation of medication? 1. Engage the patient in motivational therapy 2. Educate the patient on the reasons for the decision 3. Offer higher level of care 4. ensure that patient knows the clinic is available if/ when s/he decides to engage at an appropriate level of care
63 Buprenorphine Maintenance Once patient has achieved stable dose, determine office schedule. Normal daily dose is ~14mg/day; little evidence of need for dose greater than 24mg/day. NO evidence of need for more than once daily dose; patients may prefer more than once daily dose.
64 Withdrawal Using Buprenorphine Studies have primarily looked at buprenorphine maintenance, not withdrawal In general, withdrawal using opioids (e.g., methadone) has had poor outcomes Results with buprenorphine may be better (may have a milder withdrawal syndrome)
65 Buprenorphine Maintenance/Withdrawal" Buprenorphine maintenance vs. withdrawal:" - Double-blind, random assignment to:" - 16 mg/day SL buprenorphine tablets, or " - 6 day buprenorphine withdrawal followed by placebo" - 20 patients per group" - Used tablets of buprenorphine, placebo" " " " " " "Kakko et al. 2003"
66 Buprenorphine Maintenance/Withdrawal" Comparison of buprenorphine maintenance vs. withdrawal:" - First week of study was inpatient; study lasted one year; take home doses allowed after 6 months of treatment " - Outcome measures included " - treatment retention" - urine samples that were collected under supervision and tested three times per week" - ASI scores"
67 Buprenorphine Maintenance/Withdrawal" Comparison of buprenorphine maintenance vs. withdrawal:" - All participants also received a relatively rich set of psychosocial treatments" - group and individual counseling " - assistance with various social service agencies (for example, for housing and employment) "
68 Buprenorphine Maintenance/Withdrawal: Retention Remaining in treatment (nr) Control Buprenorphine Treatment duration (days) (Kakko et al., 2003)
69 Buprenorphine Maintenance/Withdrawal: Mortality Placebo Buprenorphine Cox Regression Dead 4/20 (20%) 0/20 (0% ) X 2 =5.9; p=0.015 (Kakko et al, 2003)
70 Summary Buprenorphine/naloxone and buprenorphine are safe and and highly effective in treating opioid dependence. Buprenorphine can be effectively utilized in OTPs and in office-based practice to assist opioid-dependent patients. Physicians and allied health personnel need to understand the complex pharmacology of buprenorphine in order to use it effectively for their patient s good.
71 Naltrexone
72 Naltrexone Injectable 2 Groups of patients are appropriate for use of naltrexone injectable: - Patients entering treatment in active addiction OR after short-term detoxification/rehabilitation - Patients who have succeeded on methadone or buprenorphine and successfully tapered off agonist medication
73 Naltrexone Injectab;e Use for Opioid Dependence Unintended precipitation of opioid withdrawal To prevent occurrence of an acute abstinence syndrome (withdrawal) in patients dependent on opioids, or exacerbation of a preexisting subclinical abstinence syndrome: Patients must be opioid free for a minimum of 7-10 days before starting VIVITROL treatment Patients must be free of all opioid-containing medications, including medications used to treat opioid dependence (eg, methadone, buprenorphine and buprenorphne/naloxone)
74 Naltrexone Injectable - Use for Opioid Dependence Naloxone Challenge The absence of an opioid drug in the urine is often not sufficient proof that a patient is opioid free: A naloxone challenge test should be given if the prescribing physician feels there is risk of precipitating a withdrawal reaction following administration of VIVITROL
75 Naltrexone Injectable The efficacy of naltrexone injectable in the treatment of opioid dependence was evaluated in a 24 week, placebo-controlled, multi-center, double-blind, randomized trial of opioiddependent (DSM-IV) outpatients, who were completing or had recently completed detoxification. Subjects were treated with an injection every 4 weeks of naltrexone injectble 380 mg or placebo. Oral naltrexone was not administered prior to the initial or subsequent injections of study medication. Standardized, manual-based psychosocial support was provided on a biweekly basis to all subjects in addition to medication.

76 Naltrexone Injectable Efficacy for Opioid Dependence
77 Pharmacokinetics Mean steady-state naltrexone concentration following monthly XR- NTX 380 mg compared to daily oral dosing XR-NTX 380 mg Oral naltrexone 50 mg Dean RL. Front Biosci Jan 1;10: Dunbar JL, et al. Alc Clin Exp Res. 2006;30: Data on File, Alkermes, Inc.
78 Naltrexone Injectable Steady state by 2 nd dose Minimal accumulation 6β-naltrexol Limited 1 st pass metabolism by liver Monthly naltrexone (380 mg vs 1,500 mg)
79 Response Profile Cumulative % of Participants at Each Rate of Weekly Confirmed Abstinence: XR-NTX 380 mg vs. Placebo Total abstinence (100% opioid-free weeks) during Weeks 5-24 was reported in 45 (35.7%) of subjects in the XR-NTX group versus 28 (22.6%) subjects in placebo group (P=0.0224).
80 Mean Change From Baseline in VAS-Opioid Craving Score Baseline craving scores: XR-NTX = 18; Placebo = 22 XR-NTX patients showed a 50% reduction-from-baseline in VAS-craving vs. no change for placebo

81 XR naltrexone is effective for heroin users Extended Release Naltrexone Improves Abstinence Arch Gen Psychiatry 2006; 63:
82 Mean Neonatal Morphine Dose, Length of Neonatal Hospital Stay, and Duration of Treatment for Neonatal Abstinence Syndrome Jones HE et al. N Engl J Med 2010;363:
83 Issues Related to Pregnancy
84 Cicero, et al Archives Psychiatry 2014
85 Cicero, et al Archives Psychiatry 2014
86 Methadone as Gold Standard for Pregnant Opiate Addict NIH Consensus Panel 1998 WHO Guidelines for the Psychosocially Assisted Pharmacological Treatment of Opioid Dependence 2009 CSAT Tip 43 ASAM/ACOG Opinion of the Committee on Health Care for Underserved Women 2012
87 Methadone as Gold Standard for the Pregnant Opiate Addict As evidenced by jails, which do not provide MAT to addicts, do provide methadone for pregnant addicts Steady levels of opiates normalize neuroendocrine functioning and prevent fetal distress Decreases rates of pregnancy complications, e.g. miscarriage, stillbirth, IUGR, abruptio placenta, hemorrhage, infection Improves prenatal care Allows for psychosocial interventions to improve level of functioning
88 Risk-Benefit Comparison of Methadone during Pregnancy Risks Opiate abstinence syndrome in newborn Benefits Protects fetus from repeated withdrawal episodes in utero Decreases risk of obstetric and fetal complications Decreases IUGR Decreases neonatal morbidity and mortality
89 Risk-Benefit Comparison of Methadone during Pregnancy Benefits - Decreases infections which could be vertically transmitted - Decreases opiate and other illicit drug use - Decreases criminal activity - Improves overall health and well-being
90 Tolia, et al NEJM 2015
91 Tolia, et al NEJM 2015

92 Primary and Secondary Outcomes in the Methadone and Buprenorphine Groups Jones HE et al. N Engl J Med 2010;363:
93 Summary Addiction is a common problem, across all sectors of society. It is frequently undiagnosed or, if recognized ignored. Opioid addiction is on the rise. - Appropriate therapies are available, but may be difficult to access. - Agonist therapy is the preferred modality for patients with longstanding opioid addiction.
Pharmacotherapy for opioid addiction. Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco
 Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Treating Opioid Use Disorders: An Update for Counselors and Other Providers
 Treating Opioid Use Disorders: An Update for Counselors and Other Providers Brad Shapiro, MD Medical Director Opiate Treatment Outpatient Program Zuckerberg San Francisco General THE DOSING WINDOW HISTORICAL
Treating Opioid Use Disorders: An Update for Counselors and Other Providers Brad Shapiro, MD Medical Director Opiate Treatment Outpatient Program Zuckerberg San Francisco General THE DOSING WINDOW HISTORICAL
Opioids. Sergio Hernandez, MD
 Opioids Sergio Hernandez, MD Required Slide Disclosures 1. SIGNIFICANT FINANCIAL INTERESTS NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT 2. GENERAL AND OBLIGATION INTERESTS All general
Opioids Sergio Hernandez, MD Required Slide Disclosures 1. SIGNIFICANT FINANCIAL INTERESTS NO SIGNIFICANT FINANCIAL, GENERAL, OR OBLIGATION INTERESTS TO REPORT 2. GENERAL AND OBLIGATION INTERESTS All general
Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services
 Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services www.randallwebber.com MAT clients are still addicted Truth: MAT clients will experience withdrawal symptoms if they stop
Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services www.randallwebber.com MAT clients are still addicted Truth: MAT clients will experience withdrawal symptoms if they stop
Buprenorphine as a Treatment Option for Opioid Use Disorder
 Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Module II Opioids 101 Opiate Opioid
 BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module II Opioids 101 Module II Goals of the Module This module reviews the following:! Opioid addiction and the brain!
BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module II Opioids 101 Module II Goals of the Module This module reviews the following:! Opioid addiction and the brain!
Slide 1. Slide 2. Slide 3. Opioid (Narcotic) Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists
 Analgesics and Antagonists. Lesson 6.1. Lesson 6.1. Opioid (Narcotic) Analgesics and Antagonists") Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
Slide 1 Opioid (Narcotic) Analgesics and Antagonists Chapter 6 1 Slide 2 Lesson 6.1 Opioid (Narcotic) Analgesics and Antagonists 1. Explain the classification, mechanism of action, and pharmacokinetics
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE
 LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
Opioid Agonists. Natural derivatives of opium poppy - Opium - Morphine - Codeine
 Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Opioids Research to Practice
 Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Medication Assisted Treatment. MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment
 Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Medication Assisted Treatment:
 Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Opioids Research to Practice
 Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
Implementing Buprenorphine Treatment in Opioid Treatment Programs Webinar 2, October 3, 2018
 Implementing Buprenorphine Treatment in Opioid Treatment Programs Webinar 2, October 3, 2018 Judith Martin, MD, Medical Director of Substance Use Services, San Francisco Department of Public Health Webinar
Implementing Buprenorphine Treatment in Opioid Treatment Programs Webinar 2, October 3, 2018 Judith Martin, MD, Medical Director of Substance Use Services, San Francisco Department of Public Health Webinar
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
OST. Pharmacology & Therapeutics. Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO
 OST Pharmacology & Therapeutics Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO Disclaimer In the past two years I have received no payment for services from any agency other than government or academic.
OST Pharmacology & Therapeutics Leo O. Lanoie, MD, MPH, FCFP, CCSAM, ABAM, MRO Disclaimer In the past two years I have received no payment for services from any agency other than government or academic.
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Extended-Release Naltrexone for Opioid Relapse Prevention
 Extended-Release Naltrexone for Opioid Relapse Prevention 1.NYU SOM; Bellevue Hospital Center 2.Brown Univ. 3. Friends Research Institute 4. Columbia Univ. 5. Univ. Pennsylvania 6. Univ. Virginia Funding:
Extended-Release Naltrexone for Opioid Relapse Prevention 1.NYU SOM; Bellevue Hospital Center 2.Brown Univ. 3. Friends Research Institute 4. Columbia Univ. 5. Univ. Pennsylvania 6. Univ. Virginia Funding:
Opioids. October 29, Addiction Medicine Review Course CSAM, Newport Beach, CA
 Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
Medication Assisted Treatment. Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs
 Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
BUPRENORPHINE and Office-Based Treatment of Opioid Use Disorder
 BUPRENORPHINE and Office-Based Treatment of Opioid Use Disorder Stephen A. Wyatt, DO Anthony Dekker, DO William Morrone, DO Funding for this initiative was made possible (in part) by Providers Clinical
BUPRENORPHINE and Office-Based Treatment of Opioid Use Disorder Stephen A. Wyatt, DO Anthony Dekker, DO William Morrone, DO Funding for this initiative was made possible (in part) by Providers Clinical
Overdose Treatment. Naloxone is the drug of choice to treat methadone and other opioid overdose including heroin and morphine.
 Part B 2 3 4 Overdose Treatment Naloxone is the drug of choice to treat methadone and other opioid overdose including heroin and morphine. Specifically used to counteract lifethreatening depression of
Part B 2 3 4 Overdose Treatment Naloxone is the drug of choice to treat methadone and other opioid overdose including heroin and morphine. Specifically used to counteract lifethreatening depression of
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I. Mr.D.Raju,M.pharm, Lecturer
 Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
Methadone Maintenance
 Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
Methadone Maintenance A Practical Guide to Pharmacotherapy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Ron Joe, MD, DABAM Objectives I. Pharmacology Of Methadone II. Practical Application of Pharmacology
SW OREGON OPIOID SUMMIT. Medication Assisted Recovery for Opioid Use Disorder. Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass
 SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They?
 Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
The Rising Tide of Prescription Opioid Use Disorders and Current Treatment Options
 The Rising Tide of Prescription Opioid Use Disorders and Current Treatment Options Michelle R. Lofwall, MD UK Dept of Psychiatry November 4, 2008 Outline for Today s Talk Past & current state of affairs
The Rising Tide of Prescription Opioid Use Disorders and Current Treatment Options Michelle R. Lofwall, MD UK Dept of Psychiatry November 4, 2008 Outline for Today s Talk Past & current state of affairs
WR Fentanyl Symposium. Opioids, Overdose, and Fentanyls
 Opioids, Overdose, and Fentanyls Outline: What are opioids? Why are we experiencing and opioid crisis? Potency, purity, and product How do opioids cause overdose and overdose deaths? What is naloxone and
Opioids, Overdose, and Fentanyls Outline: What are opioids? Why are we experiencing and opioid crisis? Potency, purity, and product How do opioids cause overdose and overdose deaths? What is naloxone and
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Charles P. O Brien, MD, PhD University of Pennsylvania No financial conflicts, patents, speakers bureaus
 Pain & Opioid Epidemic 2018 Charles P. O Brien, MD, PhD University of Pennsylvania No financial conflicts, patents, speakers bureaus Opioids 3400 BC Mesopotamia, Joy plant 1843 morphine by syringe 1874
Pain & Opioid Epidemic 2018 Charles P. O Brien, MD, PhD University of Pennsylvania No financial conflicts, patents, speakers bureaus Opioids 3400 BC Mesopotamia, Joy plant 1843 morphine by syringe 1874
Heroin, Fentanyl and Other Opioids. Steve Hanson
 Heroin, Fentanyl and Other Opioids Steve Hanson Heroin/Opiates Neurotransmitter-receptor interactions To transmit instructions to cells, neurotransmitters interact with their receptors. receptor neurotransmitters
Heroin, Fentanyl and Other Opioids Steve Hanson Heroin/Opiates Neurotransmitter-receptor interactions To transmit instructions to cells, neurotransmitters interact with their receptors. receptor neurotransmitters
THE MEDICAL MODEL: ADDICTION IS A BRAIN DISEASE. Judith Martin, MD Medical Director of Substance Use Services San Francisco Dept.
 THE MEDICAL MODEL: ADDICTION IS A BRAIN DISEASE Judith Martin, MD Medical Director of Substance Use Services San Francisco Dept. Public Health disclosures Dr. Martin has no conflict of interest to disclose.
THE MEDICAL MODEL: ADDICTION IS A BRAIN DISEASE Judith Martin, MD Medical Director of Substance Use Services San Francisco Dept. Public Health disclosures Dr. Martin has no conflict of interest to disclose.
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines
 The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
Disclosure Statement. Learning Objectives. American Psychiatric Nurses Association. Christian J. Teter, PharmD, BCPP 1 BUPRENORPHINE UPDATE
 BUPRENORPHINE UPDATE Christian J. Teter, Pharm.D., BCPP Associate Professor, Psychopharmacology College Of Pharmacy, University Of New England Portland, ME E-Mail: cteter@une.edu Image Source: pubchem.ncbi.nlm.nih.gov
BUPRENORPHINE UPDATE Christian J. Teter, Pharm.D., BCPP Associate Professor, Psychopharmacology College Of Pharmacy, University Of New England Portland, ME E-Mail: cteter@une.edu Image Source: pubchem.ncbi.nlm.nih.gov
Medications for Opioid Use Disorder. Charles Brackett, MD, MPH General Internal Medicine, DHMC
 Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Methadone Maintenance: safe and effective opioid pharmacotherapy. Karen Miotto, MD UCLA Department of Psychiatry
 Methadone Maintenance: safe and effective opioid pharmacotherapy Karen Miotto, MD UCLA Department of Psychiatry Opioid abuse and dependence statistics, 2007 Persons who reported abuse or dependence in
Methadone Maintenance: safe and effective opioid pharmacotherapy Karen Miotto, MD UCLA Department of Psychiatry Opioid abuse and dependence statistics, 2007 Persons who reported abuse or dependence in
Buprenorphine: An Introduction. Sharon Stancliff, MD Harm Reduction Coalition September 2008
 Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Dr Alistair Dunn. General Practitioner Whangarei
 Dr Alistair Dunn General Practitioner Whangarei 1982 Temgesic = Buprenorphine Sublingual opiate analgesic 0.2 mg Popular drug of abuse 1991 Temgesic NX = Bup & Nalxone Nalxone added to deter abuse 1999
Dr Alistair Dunn General Practitioner Whangarei 1982 Temgesic = Buprenorphine Sublingual opiate analgesic 0.2 mg Popular drug of abuse 1991 Temgesic NX = Bup & Nalxone Nalxone added to deter abuse 1999
Optimizing Suboxone in Opioid Addicts
 Optimizing Suboxone in Opioid Addicts David Chim, D.O. Integrated Substance Abuse Programs Dept. of Psychiatry, UCLA K30 Translational Research Interest March 24, 2009 dchim@mednet.ucla.edu www.uclaisap.org
Optimizing Suboxone in Opioid Addicts David Chim, D.O. Integrated Substance Abuse Programs Dept. of Psychiatry, UCLA K30 Translational Research Interest March 24, 2009 dchim@mednet.ucla.edu www.uclaisap.org
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations
 Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Medication-Assisted Treatment (MAT) Overview
 Overview") Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
What is an opioid? What do opioids do? Why is there an opioid overdose crisis? What is fentanyl? What about illicit or bootleg fentanyls?
 What is an opioid? What do opioids do? Why is there an opioid overdose crisis? What is fentanyl? What about illicit or bootleg fentanyls? What is an opioid? What do opioids do?: The term opioid can be
What is an opioid? What do opioids do? Why is there an opioid overdose crisis? What is fentanyl? What about illicit or bootleg fentanyls? What is an opioid? What do opioids do?: The term opioid can be
Medication Assisted Treatment. Nicole Gastala, MD
 Medication Assisted Treatment Nicole Gastala, MD Objectives Training Goals: To enhance the understanding of the participants in use of medication assisted therapy To increase the knowledge of participants
Medication Assisted Treatment Nicole Gastala, MD Objectives Training Goals: To enhance the understanding of the participants in use of medication assisted therapy To increase the knowledge of participants
PAIN & ANALGESIA. often accompanied by clinical depression. fibromyalgia, chronic fatigue, etc. COX 1, COX 2, and COX 3 (a variant of COX 1)
") Pain - subjective experience associated with detection of tissue damage ( nociception ) acute - serves as a warning chronic - nociception gone bad often accompanied by clinical depression fibromyalgia,
Pain - subjective experience associated with detection of tissue damage ( nociception ) acute - serves as a warning chronic - nociception gone bad often accompanied by clinical depression fibromyalgia,
5/29/2015. Responding to the Opioid Crisis. Responding to the Opioid Crisis. Objectives
 Responding to the Opioid Crisis Responding to the Opioid Crisis David Cohen Ramsen Kasha Objectives Gain knowledge on Current opioid epidemic Historical perspective of opioids The impact of opioids on
Responding to the Opioid Crisis Responding to the Opioid Crisis David Cohen Ramsen Kasha Objectives Gain knowledge on Current opioid epidemic Historical perspective of opioids The impact of opioids on
Opioid dependence: Detoxification
 Opioid dependence: Detoxification What is detoxification? A. Process of removal of toxins from the body? B. Admitting a drug dependent person in a hospital and giving him nutrition? C. Stopping drug use
Opioid dependence: Detoxification What is detoxification? A. Process of removal of toxins from the body? B. Admitting a drug dependent person in a hospital and giving him nutrition? C. Stopping drug use
OAT Transitions - focus on microdosing. Mark McLean MD MSc FRCPC CISAM DABAM
 OAT Transitions - focus on microdosing Mark McLean MD MSc FRCPC CISAM DABAM Disclosures No pharmaceutical industry or other financial conflicts of interest Study Physician for research funded by Canadian
OAT Transitions - focus on microdosing Mark McLean MD MSc FRCPC CISAM DABAM Disclosures No pharmaceutical industry or other financial conflicts of interest Study Physician for research funded by Canadian
Opioid Use in Youth. Amy Yule M.D. March 2,
 Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
ROSC & MAT II: Opioid Treatment Services
 ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
Pharmacology of Buprenorphine & Other Opioids Table of Contents
 Pharmacology of Buprenorphine & Other Opioids Table of Contents...1 Goal:... 1 After completing this module participants will be able to:...1 Professional Practice Gaps...1 Module Introduction... 2 Case
Pharmacology of Buprenorphine & Other Opioids Table of Contents...1 Goal:... 1 After completing this module participants will be able to:...1 Professional Practice Gaps...1 Module Introduction... 2 Case
6/6/2018. Objectives. Outline. Rethinking Medication Treatment for Opioid Use Disorder
 Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
Medication for the Treatment of Addiction (MAT)
") Medication for the Treatment of Addiction (MAT) Karol Kaltenbach, PhD Emeritus Professor of Pediatrics Sidney Kimmel Medical College at Thomas Jefferson University Terminology: Words Matter Medication
Medication for the Treatment of Addiction (MAT) Karol Kaltenbach, PhD Emeritus Professor of Pediatrics Sidney Kimmel Medical College at Thomas Jefferson University Terminology: Words Matter Medication
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT
 and acute pain management on MAT") An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
Buprenorphine pharmacology
 Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone
 Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone Alexander Y. Walley, MD, MSc Associate Professor of Medicine Director, Addiction Medicine Fellowship Boston University
Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone Alexander Y. Walley, MD, MSc Associate Professor of Medicine Director, Addiction Medicine Fellowship Boston University
MAT - ICAAD 2018 Ron Jackson, MSW, LICSW
 The ATTC Network Ten Regional Centers northwest@attcnetwork.org www.attcnetwork.org/northwest phone. 206-685-4419 1107 NE 45 th St, Ste 120, Seattle, WA 98105 http://attcnetwork.org/northwest U.S. Opioid
The ATTC Network Ten Regional Centers northwest@attcnetwork.org www.attcnetwork.org/northwest phone. 206-685-4419 1107 NE 45 th St, Ste 120, Seattle, WA 98105 http://attcnetwork.org/northwest U.S. Opioid
Opioid Use Disorders as a Brain Disease Why MAT is so important. Ron Jackson, M.S.W., L.I.C.S.W.
 Opioid Use Disorders as a Brain Disease Why MAT is so important Ron Jackson, M.S.W., L.I.C.S.W. Affiliate Professor School of Social Work University of Washington Organization Name: CareOregon Course Title:
Opioid Use Disorders as a Brain Disease Why MAT is so important Ron Jackson, M.S.W., L.I.C.S.W. Affiliate Professor School of Social Work University of Washington Organization Name: CareOregon Course Title:
3/26/14. Opiates PSY B396 ALCOHOL, ALCOHOLISM, & DRUG ABUSE. Early History Cont d. Early History. Opiate Use in the 19th century. Technology Advances
 Opiates PSY B396 ALCOHOL, ALCOHOLISM, & DRUG ABUSE Chapter 10 Opiates The most dramatic example of the doubleedged sword character of drugs Most potent painkillers Prototype addictive drug: Heroin Early
Opiates PSY B396 ALCOHOL, ALCOHOLISM, & DRUG ABUSE Chapter 10 Opiates The most dramatic example of the doubleedged sword character of drugs Most potent painkillers Prototype addictive drug: Heroin Early
Special Populations health complications of Substance Use Anthony Dekker DO, OMED 2018 San Diego
 Special Populations health complications of Substance Use Anthony Dekker DO, OMED 2018 San Diego 1 Disclosure Anthony Dekker DO has presented numerous programs on Chronic Pain Management and Addiction
Special Populations health complications of Substance Use Anthony Dekker DO, OMED 2018 San Diego 1 Disclosure Anthony Dekker DO has presented numerous programs on Chronic Pain Management and Addiction
OPIOIDS. Testing and Interpretation
 OPIOIDS Testing and Interpretation TOPICS OF DISCUSSION Effects of Opioids Opiates vs. Opioids Drug Testing Recent Trends OPIOIDS: Testing and Interpretation 2018 2 EFFECTS OF OPIOIDS 3 Opioid Receptors
OPIOIDS Testing and Interpretation TOPICS OF DISCUSSION Effects of Opioids Opiates vs. Opioids Drug Testing Recent Trends OPIOIDS: Testing and Interpretation 2018 2 EFFECTS OF OPIOIDS 3 Opioid Receptors
Disclosures. Topics of today s training 4/24/2017. Evolving Treads in Medication Assisted Treatment. Christopher J Davis D.O.
 Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Buprenorphine for Family Medicine. Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17
 + Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
+ Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
Opioid dependence and buprenorphine treatment
 Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
Rates of Opioid Overdose Deaths, Sales, and Treatment Admissions: US,
 Rates of Opioid Overdose Deaths, Sales, and Treatment Admissions: US, 1999 21 8 Rates of Prescription Painkiller Sales, Deaths, and Substance Abuse Treatment Admissions (1999 21) 7 Rate 6 5 4 3 Sales per
Rates of Opioid Overdose Deaths, Sales, and Treatment Admissions: US, 1999 21 8 Rates of Prescription Painkiller Sales, Deaths, and Substance Abuse Treatment Admissions (1999 21) 7 Rate 6 5 4 3 Sales per
MARRCH Minnesota Society of Addiction Medicine Presents. Addiction as a Brain Disease
 MARRCH 2008 Minnesota Society of Addiction Medicine Presents Addiction as a Brain Disease Gavin Bart, MD Charles Reznikoff, MD Steven Fu, MD, MSCE David Frenz, MD, MS October 22, 2008 Schedule 10:00-12:00
MARRCH 2008 Minnesota Society of Addiction Medicine Presents Addiction as a Brain Disease Gavin Bart, MD Charles Reznikoff, MD Steven Fu, MD, MSCE David Frenz, MD, MS October 22, 2008 Schedule 10:00-12:00
2/21/2018. What are Opioids?
 Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
NALTREXONE DAVID CRABTREE, MD, MPH UNIVERSITY OF UTAH HEALTH, 2018
 NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
HIV/AIDS Definition: CDC Classification of HIV Infection Stage 1: Stage 2: Stage 3: Risk Factors
 HIV/AIDS Definition: Acquired immune deficiency syndrome (AIDS) is a progressive, incurable disease caused by the human immunodeficiency virus (HIV). Aids destroys the CD4+ T cells, impairing the immune
HIV/AIDS Definition: Acquired immune deficiency syndrome (AIDS) is a progressive, incurable disease caused by the human immunodeficiency virus (HIV). Aids destroys the CD4+ T cells, impairing the immune
Opioid Treatment in North Carolina SEPTEMBER 13, 2016
 Opioid Treatment in North Carolina SEPTEMBER 13, 2016 Source Where Pain Relievers Were Obtained for Most Recent Nonmedical Use among Past Year Users Aged 12 or Older: 2007 Source Where Respondent Obtained
Opioid Treatment in North Carolina SEPTEMBER 13, 2016 Source Where Pain Relievers Were Obtained for Most Recent Nonmedical Use among Past Year Users Aged 12 or Older: 2007 Source Where Respondent Obtained
Opioids: Use, Abuse and Cause of Death. Jennifer Harmon Assistant Director - Forensic Chemistry Orange County Crime Laboratory
 Opioids: Use, Abuse and Cause of Death Jennifer Harmon Assistant Director - Forensic Chemistry Orange County Crime Laboratory jharmon@occl.ocgov.com Opioid: Any psychoactive chemical that resembles morphine
Opioids: Use, Abuse and Cause of Death Jennifer Harmon Assistant Director - Forensic Chemistry Orange County Crime Laboratory jharmon@occl.ocgov.com Opioid: Any psychoactive chemical that resembles morphine
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
9/13/2017. Buprenorphine Treatment (Suboxone) Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare
 Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare") Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
MAT in the Corrections Setting
 MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
Understanding and Combating the Heroin Epidemic
 Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
LESSON ASSIGNMENT. After completing this lesson, you should be able to: Given a group of definitions, select the definition of analgesia.
 LESSON ASSIGNMENT LESSON 11 Narcotic Agents. LESSON ASSIGNMENT Paragraphs 11-1--11-7 LESSON OBJECTIVES After completing this lesson, you should be able to: 11-1. Given a group of definitions, select the
LESSON ASSIGNMENT LESSON 11 Narcotic Agents. LESSON ASSIGNMENT Paragraphs 11-1--11-7 LESSON OBJECTIVES After completing this lesson, you should be able to: 11-1. Given a group of definitions, select the
Medication-Assisted Treatment and HIV/AIDS: Aspects in Treating HIV- Infected Drug Users.
 Slide #1 Medication-Assisted Treatment and HIV/AIDS: Aspects in Treating HIV- Infected Drug Users. R. Douglas Bruce, MD, MA, MSc Assistant Professor Yale AIDS Program Medical Director South Central Rehabilitation
Slide #1 Medication-Assisted Treatment and HIV/AIDS: Aspects in Treating HIV- Infected Drug Users. R. Douglas Bruce, MD, MA, MSc Assistant Professor Yale AIDS Program Medical Director South Central Rehabilitation
Addiction to Opioids. Marvin D. Seppala, MD Chief Medical Officer
 Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
THE OPIUM POPPY OPIOID PHARMACOLOGY 2/18/16. PCTH 300/305 Andrew Horne, PhD MEDC 309. Papaver somniferum. Poppy Seeds Opiates
 OPIOID PHARMACOLOGY PCTH 300/305 Andrew Horne, PhD andrew.horne@ubc.ca MEDC 309 THE OPIUM POPPY Papaver somniferum Sleep-bringing poppy Poppy Seeds Opiates Opium Poppy Straw 1 OPIATES VS. OPIOIDS Opiates:
OPIOID PHARMACOLOGY PCTH 300/305 Andrew Horne, PhD andrew.horne@ubc.ca MEDC 309 THE OPIUM POPPY Papaver somniferum Sleep-bringing poppy Poppy Seeds Opiates Opium Poppy Straw 1 OPIATES VS. OPIOIDS Opiates:
Fentanyls and Naloxone. Opioids, Overdose, and Naloxone
 Opioids, Overdose, and Naloxone Presenter Disclosure Presenter s Name: Michael Beazely I have no current or past relationships with commercial entities Speaking Fees for current program: I have received
Opioids, Overdose, and Naloxone Presenter Disclosure Presenter s Name: Michael Beazely I have no current or past relationships with commercial entities Speaking Fees for current program: I have received
Methadone Maintenance Treatment for the Opioid Dependent Patient
 Methadone Maintenance Treatment for the Opioid Dependent Patient Janice F. Kauffman RN, MPH, CAS, LADC1 Assistant Professor of Psychiatry, Harvard Medical School V. P., Addiction Treatment Services, North
Methadone Maintenance Treatment for the Opioid Dependent Patient Janice F. Kauffman RN, MPH, CAS, LADC1 Assistant Professor of Psychiatry, Harvard Medical School V. P., Addiction Treatment Services, North
Vivitrol Vs. Suboxone
 Vivitrol Vs. Suboxone Vivitrol - Naltrexone Indicated for opiate dependence and alcohol withdrawal pure antagonist 380mg once every 4 weeks IM Peak plasma concentration in 2 hrs, followed by a second peak
Vivitrol Vs. Suboxone Vivitrol - Naltrexone Indicated for opiate dependence and alcohol withdrawal pure antagonist 380mg once every 4 weeks IM Peak plasma concentration in 2 hrs, followed by a second peak
HARM REDUCTION & TREATMENT. Devin Reaves MSW
 HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
Overview of Opioid Use Disorder
 Overview of Opioid Use Disorder Doug Burgess, MD Medical Director of Outpatient Services, Truman Medical Centers Assistant Professor of Psychiatry, University of Missouri- Kansas City Objectives History
Overview of Opioid Use Disorder Doug Burgess, MD Medical Director of Outpatient Services, Truman Medical Centers Assistant Professor of Psychiatry, University of Missouri- Kansas City Objectives History
VIVITROL (naltrexone for extended-release injectable suspension) A µ-opioid Receptor Antagonist
 A µ-opioid Receptor Antagonist") MECHANISM OF ACTION VIVITROL (naltrexone for extended-release injectable suspension) A µ-opioid Receptor Antagonist VIVITROL is indicated for prevention of relapse to opioid dependence, following opioid
MECHANISM OF ACTION VIVITROL (naltrexone for extended-release injectable suspension) A µ-opioid Receptor Antagonist VIVITROL is indicated for prevention of relapse to opioid dependence, following opioid
GOALS AND OBJECTIVES
 SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
Serious Mental Illness and Opioid Use Disorder
 Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
FY17 SCOPE OF WORK TEMPLATE. Name of Program/Services: Medication-Assisted Treatment: Buprenorphine
 FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
Building capacity for a CHC response to Ontario's Opioid Crisis
 Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Methadone and Pregnancy
 Methadone and Pregnancy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Charissa Patricelli, MD, CCFP, ABAM Clinical Associate Professor, Dept. of Family Practice UBC American Board of Addiction Medicine
Methadone and Pregnancy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Charissa Patricelli, MD, CCFP, ABAM Clinical Associate Professor, Dept. of Family Practice UBC American Board of Addiction Medicine
Maternal-fetal Opiate Medical Home (MOMH) Jocelyn Davis DNP,CNM, RN, CEFMM Karen Frantz BSN, RNC
 Jocelyn Davis DNP,CNM, RN, CEFMM Karen Frantz BSN, RNC") Maternal-fetal Opiate Medical Home (MOMH) Jocelyn Davis DNP,CNM, RN, CEFMM Karen Frantz BSN, RNC Objectives 1. Discuss the effects of opiate addiction on mothers and infants. 2. Discuss a Medical Home
Maternal-fetal Opiate Medical Home (MOMH) Jocelyn Davis DNP,CNM, RN, CEFMM Karen Frantz BSN, RNC Objectives 1. Discuss the effects of opiate addiction on mothers and infants. 2. Discuss a Medical Home
Treatment of Opioid Use Disorder
 Treatment of Opioid Use Disorder Casia Horseman, MD Assistant Professor Department of Psychiatry and Behavioral Health The Ohio State University Wexner Medical Center Objectives Discuss the historical
Treatment of Opioid Use Disorder Casia Horseman, MD Assistant Professor Department of Psychiatry and Behavioral Health The Ohio State University Wexner Medical Center Objectives Discuss the historical
Treatment of Opioid Use Disorder
 Treatment of Opioid Use Disorder Casia Horseman, MD Assistant Professor Department of Psychiatry and Behavioral Health The Ohio State University Wexner Medical Center Objectives Discuss the historical
Treatment of Opioid Use Disorder Casia Horseman, MD Assistant Professor Department of Psychiatry and Behavioral Health The Ohio State University Wexner Medical Center Objectives Discuss the historical
Medication Assisted Treatment
 Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Latest Research on Addiction and Treatment
 Latest Research on Addiction and Treatment Joshua D Lee MD MSc joshua.lee@nyumc.org / @DrJoshuaDLee Associate Professor NYU School of Medicine, Department of Population Health Disclosures, LeeJD Grants:
Latest Research on Addiction and Treatment Joshua D Lee MD MSc joshua.lee@nyumc.org / @DrJoshuaDLee Associate Professor NYU School of Medicine, Department of Population Health Disclosures, LeeJD Grants:
Opioid Use in Pregnant Women and Prenatal Care. Murray F Dweck MD, FACOG Medical Director/OBGYN Florida Department of Health -Brevard
 Opioid Use in Pregnant Women and Prenatal Care Murray F Dweck MD, FACOG Medical Director/OBGYN Florida Department of Health -Brevard Objectives Summarize contextual and co-morbid factors observed among
Opioid Use in Pregnant Women and Prenatal Care Murray F Dweck MD, FACOG Medical Director/OBGYN Florida Department of Health -Brevard Objectives Summarize contextual and co-morbid factors observed among
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents
 Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol