Abnormal LFTs GP CME 2014 Workshop Fri 55 mins. Dr Alasdair Patrick Macmurray Center GP CME 2014
|
|
|
- Shannon Knight
- 6 years ago
- Views:
Transcription

1 Abnormal LFTs GP CME 2014 Workshop Fri 55 mins Dr Alasdair Patrick Macmurray Center GP CME 2014
2 Dr Alasdair Patrick Gastroenterologist
3 Overview Liver Function Tests Cholestasis Hepatocellular / Hepatitic Tests of Liver Synthetic Function Bilirubin, Albumin & INR Clinical aspects Cases Cirrhosis Middlemore Cirrhosis Audit


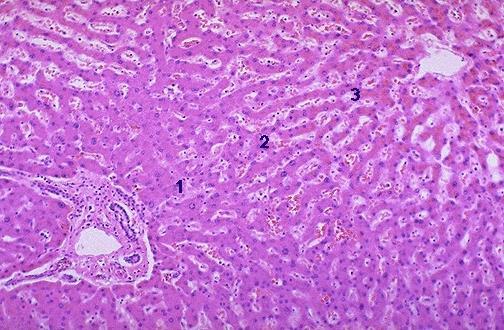
4 Normal Liver Anatomy Hepatic Artery Bile Duct Portal Vein Central Vein
5 Liver Function Tests (ULN) Nature of liver disease Synthetic Function Cholestasis ALP (110) GGT (60) Bilirubin (<24) Albumin (35-47) Prothrombin ratio (<1.2) Hepatitis ALT (45) AST (45)
6 Patterns of raised LFT s A purely cholestatic or purely hepatitic picture is uncommon Cholestatic ALT / ALP < 2 Mixed ALT / ALP 2-5 Hepatitic ALT / ALP > 5 [ Ratio = ALT (x ULN) / ALP (x ULN)]
7 Cholestatic Enzymes Alkaline phosphatase (ALP) Produced in many tissues Raised levels usually come from the biliary epithelium, bones, or placenta If GGT normal unlikely hepatic source Cholestasis causes increased synthesis of ALP and leakage of ALP in to the circulation
8 Cholestatic Enzymes Gammaglutamyl transpeptidase (GGT) Found in cell membranes throughout the body including hepatocytes and biliary epithelium Levels are not raised in bone disease or pregnancy Raised serum levels almost always have a liver origin (usually relating to cholestasis or fatty liver) Serum levels can be elevated in the absence of liver disease due to enzyme induction by anticonvulsants (phenytoin) or EtOH
9 Causes of Cholestasis Bile duct obstruction Stones, tumour, surgery, parasites Drugs Clavulanic acid, Flucloxacillin, Erythromycin Liver congestion / heart failure Sepsis / systemic inflammatory disorders Hormonal Pregnancy, OCP Chronic biliary disorders Primary Biliary Cirrhosis, Primary Sclerosing Cholangitis Inherited conditions Biliary atresia, Cystic fibrosis

10 Cholestasis Normal Stones & dilated CBD
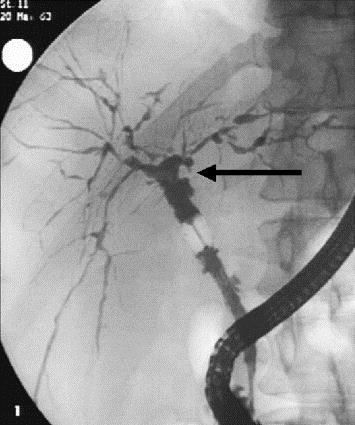
11 Cholestasis Normal PSC
12 Hepatocellular Alanine Aminotransferase (ALT) Catalyses the formation of pyruvate in the cytosol Found in many tissues but by far the highest levels are in the liver Elevated levels are relatively specific for liver disease More sensitive marker of liver disease in chronic viral hepatitis than the AST
13 Hepatocellular Aspartate Aminotransferase (AST) Catalyses the formation of oxaloacetate in the cell cytosol and mitochondria Found in many tissues but high levels in liver and muscle (cardiac & skeletal) Elevated levels are not as specific for liver disease as an elevated ALT Less sensitive marker of hepatic inflammation than ALT
14 Hepatocellular Damage Acute Viral hepatitis EBV, HAV, HBV Drugs & herbal remedies Paracetamol OD Ischaemic / hypoxic Rare: Autoimmune (AIH) Wilson s disease, Budd Chiari Syndrome, AFLP Chronic (> 6 months) Viral hepatitis HBV, HCV Fatty liver (NALFD) EtOH (AFLD) Drugs Haemochromatosis Autoimmune Wilson s
15 Transaminases Rules of thumb Chronic liver disease - ALT & AST are usually only mildly elevated ( typically x ULN) - May be normal Ratio AST / ALT ratio is < 1 in most liver disease Alcohol related hepatitis is the exception where the ratio is usually > 2 The degree of elevation of the does not correlate well with the degree of histological damage in the liver Levels may go in to the many thousands acutely and the liver recover completely Falling levels usually denote recovery but are an ominous sign if the liver synthetic function is worsening Levels < 10x ULN are non-specific
16 Causes: Transaminases > 1000 IU / L Ischaemic hepatitis (shock) Acute viral hepatitis HAV, HBV Drugs Paracetamol OD, halothane, Carbemazepine [Alcoholic hepatitis ALT & AST < 300 IU/L]
17 Two primary sources Bilirubin Indirect (unconjugated): old red cells, removed by the spleen, sent to the liver Liver adds glucuronic acid, making these cells water soluble for excretion; now called direct (or conjugated)
; if conjugated - hepatobiliary diseases Only conjugated (direct) bilirubin can be excreted in the urine Unconjugated hyperbilirubinaemia may occur due to over production of bilirubin")
18 Synthetic Function Bilirubin 80% comes from breakdown of haemoglobin Taken up by hepatocytes and conjugated with glucuronic acid and excreted in bile Normally > 95% of serum bilirubin is unconjugated (indirect); if conjugated - hepatobiliary diseases Only conjugated (direct) bilirubin can be excreted in the urine Unconjugated hyperbilirubinaemia may occur due to over production of bilirubin (haemolysis) or inherited disorders of bilirubin conjugation (Gilbert s syndrome)
19 Bilirubin and Prognosis Poor sensitivity for detecting liver dysfunction Large reserve capacity of the liver to remove bilirubin without the development of hyperbilirubinaemia In acute cholestatic disease (stone disease) hepatocyte synthetic function is normal and the degree of hyperbilirubinaemia does not influence prognosis In viral hepatitis, alcoholic hepatitis and PBC the serum bilirubin does correlate with the degree of injury on biopsy and the prognosis

20 Synthetic Function Albumin Made in the liver (30g/day) Quantitatively the most important protein in the blood (500g in body fluids), important role in maintaining colloid osmotic pressure Serum albumin level is determined by the rate of synthesis, rate of loss / degradation and the volume of distribution
21 Albumin A low serum albumin is a good indicator of liver synthetic failure in the presence of chronic liver disease, however other causes of hypoalbuminaemia need to be considered: Renal loss (Nephrotic syndrome) Protein-calorie malnutrition Haemodilution (raised)plasma volume
22 Synthetic Function PR/INR Most clotting factors are synthesised in the liver Liver transplantation is a surgical cure for haemophilia! In the setting of both acute and chronic liver failure the INR is a very useful indicator of liver synthetic function and prognosis, however other causes of a raised INR need to be excluded: Vitamin K deficiency (prolonged cholestasis) Increased clotting factor consumption (DIC) Warfarin therapy
23 PR/INR In chronic liver failure INR rarely rises above 2.0 In acute or fulminant liver failure the INR may rise rapidly to very high levels (>10), this is associated with a very poor prognosis and liver transplanation should be considered Even an INR of 1.3 in the setting of an acute severe hepatitis is of concern and should be repeated after 6-8 hrs
24 LFT s & Liver Failure Acute (FHF) ALT & AST usually > 1,000 INR & Bilirubin rise rapidly Alb falls rapidly Patient unwell for hours or days Death within days of cerebral oedema, sepsis or multi-organ failure Chronic (Cirrhosis) ALT & AST usually < 200 INR & Bilirubin rise slowly Alb falls slowly Patient unwell for months or years Death from variceal haemorrrhage, sepsis, encephalopathy or other complications
25 Clinical aspects Please call out what these signs are!!

26 Examination Findings Dupytrons Contracture

27 Examination Findings Palmar Erythema

28 Examination Findings Gynaecomastia


29 Examination Findings Spider Naevi


30
31 Patient with abnormal LFTs History Alcohol: try to quantify Blood products or IVDU Past history Diabetes, hyperlipidaemia Medications Including OTC Paracetamol, Amoxicillin-clavulanic acid, erythromycin, HMGCoA reductase inhibitors, NSAIDS Family history Travel history
32 Questions to ask yourself Is the illness a primary liver disorder or is it secondary to another condition? Clue can be in the LFTs Is the source of the liver test extra-hepatic? An abnormality of a single test may be due to a non hepatic cause Is this an acute illness or chronic? If chronic, is it compensated or decompensated? Do the tests signify a serious illness? What is the diagnosis and prognosis?
33 Suggested work up Screen Fasting lipids and glucose Viruses HBV HCV (EBV CMV) Auto immune markers ANA, AMA, SMA Immunoglobulins Coeliac serology, Iron studies, Thyroid function tests USS focal lesions, fatty liver, portal hypertension Second run Alpha one anti-trypsin, Copper and ceruloplasmin in pt <40, Anti LKM, SLA
34 Case 1: AS23 Unwell 2 days Abdominal pain and lethargy Depressed but otherwise well OE: Jaundiced, No signs of CLD LFTs Bil 250 ALP 160 GGT 200 ALT 2380 AST 1960 Thoughts?
35 Case 1: AS23 Other Bloods: INR 2.3, Cr 85, ph 7.40, Paracetamol 120 Liver Screen Negative (HAV and HBcoreIgM Negative) Imaging USS: Normal Pattern of LFT Disturbance Hyperbilirubinaemia, Hepatitic Picture ALT>1000 Diagnosis Paracetamol Overdose

36 Case 1: AS23 Paracetamol Treatment Nomogram x
37 Paracetomol overdose Liver Transplant Criteria (Kings College) Paracetamol Arterial ph < 7.3; or All three: INR>6.5, Cr>300, G3-4 Encephalopathy Non Paracetamol INR >6.5; or Three of the following five criteria Patient age <11 or >40; Bilirubin >300; Time from onset of jaundice to enceph. greater than 7 days; INR >3.5; or, Drug toxicity
38 Paracetomol overdose Follow up Gradual improvement of LFT s and synthetic function Treatment Close Observation Frequent Blood test repeat Rx n-acetyl cysteine (NAC) Psychiatry
39 Case 2: GH66 Gradual Itch Previous autoimmuine thyroid disease OE: Normal apart from scratch marks LFT s Bil 15 ALP 502 GGT 438 ALT 65 AST 48 Thoughts?
40 Case 2: GH66 Other Bloods: INR 1.0, Alb 40 Liver Screen AMA Positive, ANA 1:80 Imaging USS: Normal Pattern of LFT Disturbance Choleststatic picture with preserved synthetic function Diagnosis Primary Biliary Cirrhosis

41 Primary biliary cirrhosis Auto-immune disease of the liver Slow progressive destruction of small bile ducts Female to male ratio 9:1 Prevalence 1:4000
42 Primary biliary cirrhosis Treatment Ursodeoxycholic acid Reduce the cholestasis - improves LFT s results Minimal effect on symptoms Whether it improves prognosis is controversial Cholestyramine (bile acid sequestrant) Absorb bile acids in the gut Alternative agents: Naltrexone & Rifampicin Ongoing follow up
43 Case 3: GF 56 Heavy alcohol consumption Many years Stopped 4 weeks ago Gradual jaundice, confusion and lethargy OE: Jaundiced, Spider Naevi, Small liver LFTs Bil 406 GGT 198 ALP 137 AST 126 ALT 52 Thoughts?
44 Case 3: GF 56 Other Bloods: INR 1.8, Albumin 30 Pattern of LFT Disturbance Mixed, significant hyperbilirubinaemia, AST>ALT Liver Screen Negative Imaging USS: Coarse Liver Echotexture Diagnosis Alcoholic Hepatitis

45 Alcoholic hepatitis
46 Alcoholic hepatitis Treatment Abstinence from Alcohol Monitor for withdrawal Vitamin K In Hospital 3 weeks Good improvement Prednisone 30mg Daily for 4 weeks Cirrhosis follow up
47 Case 4: 22 Chinese lady who says she has Hep B ALT normal sag +ve, eag +ve, anti HBE ve HBV DNA 10*9 What would you do? Watch 6/12ly and get flare and seroconverts
48 Case 5 47 year old Indian man Ex boozer ALT 55 What else would you check? HBsAg positive HBe Ag-ve, anti HBe +ve What would you do now? Rpt 6/12 ALT 127 What would you do now? Fibroscan- cirrhosis
49 Viral Hepatitis
50 Viral Hepatitis : Hepatitis A Food, water borne; heat labile Faecal - oral contamination; contagious Usually self limited, lasting days to weeks 99% spontaneous recovery, no treatment Tests: HAV IgM antibody = acute infection HAV total antibody (IgM & IgG) = exposure only, could be post infection or vaccination

51 Viral Hepatitis : Hepatitis B Blood, semen, saliva, vaginal secretions Highly contagious; sexually transmitted 90-95% self limited over 6 months Chronic infection: >6 months DNA virus: incorporates into host with chronic infection
52 Viral Hepatitis : Hepatitis B HBV at risk groups (who to test) Maori, Pacificans, Asians, contacts of those with HBsAg patients, IVDU, MSM Abnormal liver function tests

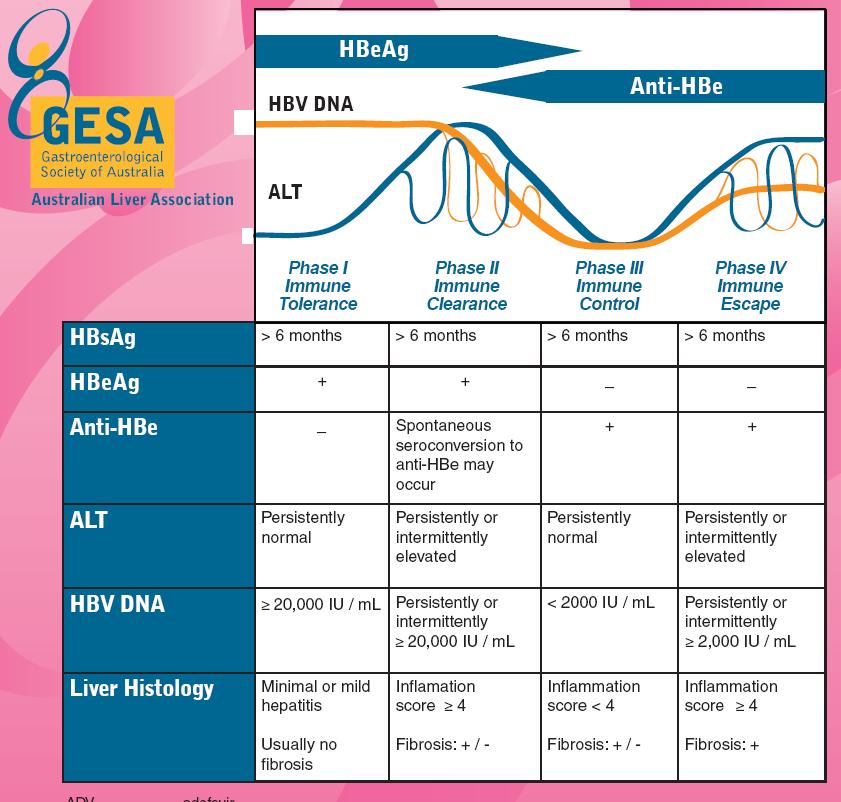
53 HBV Serology HBV s Ag: surface antigen; + infection HBV s Ab: surface antibody; - infection HBV c Ab: core antibody IgM, IgG; only + with infection, not vaccination HBV e Ag: envelope antigen; if + actively replicating virus HBV DNA: actual viral load in blood
54
 DNA (PCR if")
55 Serologic markers of infection and their significance Acute hepatitis B Recovery from acute hepatitis B Chronic HBeAg + disease Chronic HBeAg disease Successful vaccination HBsAg Anti-HBs Anti-HBc IgM Anti-HBc IgG HBeAg Anti-HBe (in some cases) DNA (PCR if required)
56 HBV Treatment Decision E- Antigen Status Likelihood of progression ie significant fibrosis now Likelihood of adhering to treatment Lamivudine (not first line) Entecavir Adefovir (Lam Resistant) Tenofovir Pegylated interferon
57 Why treat Hepatitis B? To prevent complications of cirrhosis ie decompensated cirrhosis and its complications eg HCC Ultimate Goal cure, permanent suppression, roadmap concept Once decision made, more or less life long

58 Viral Hepatitis : Hepatitis C Blood borne, not in food or water; not highly sexually transmitted* Not highly contagious 20% self clearing; 80% chronicity RNA virus: does not incorporate into host
59 Viral Hepatitis: Hepatitis C HCV Ab: + means past exposure; can take 3-6 months to form; not found if acute ELISA: used to confirm Ab; + rules out false positives HCV PCR RNA: confirms actual viral presence in blood; can be +/- or a viral count (qualitative vs. quantitative) HCV Genotype: there are at least six (6) different (geno)types of HCV virus
60 Viral Hepatitis : Hepatitis C HCV Genotypes: different mutations of same virus (different branches, same tree) Can vary by global geography Not predicative of damage or symptoms Can predict response to treatment Can be used to determine who is the best treatment candidate G1 & 4: most stubborn; G2 & 3: most responsive; G5 & 6: most rare
61 HCV: When to refer to a HCV Ab + RNA + specialist Suitability for treatment alcohol use, ongoing drug use, motivation, mental state eg depression (consider SSRI at the time of referral) Treatment improving all the time Expect 70-90% cure with new drugs
62 Case 5 Asymptomatic 40 year old man Screening LFTs Bili 38 ALT 15 IU/ml ALP 85 GGT 30 Alb 36 What other information would be helpful?
63 Case 5 Otherwise well No alcohol No family history What bloods would you check? Diagnosis: Gilberts syndrome How could you confirm this? unconjugated hyperbilirubinaemia Often increases in infections but also on starving

64 Case 6 46 year old European man Feeling tired Gaining weight Wt 120kg, BMI 32 Occasional alcohol LFTs T bili 20 GGT 198 ALP 88 AST 40 ALT 65 Thoughts?
65 Non-alcoholic fatty liver disease (NAFLD) Spectrum of severity Mild fatty infiltration Non-alcoholic steatohepatitis Fibrosis, cirrhosis Most common cause of abnormal LFT s in primary care Hepatic manifestation of metabolic syndrome
66 Associated with NAFLD Obesity - central Type-2 diabetes Hypertension Hypertriglyceridaemia FHx of type-2 DM common in absence
67 NAFLD Thought to affect up to 24% population 70% of obese 50% of type-2 DM Mostly benign. Cirrhosis and hepatocellular carcinoma? Cirrhosis risks - age, obesity, DM
68 Symptoms NAFLD - Clinical Usually none Fatigue, RUQ discomfort Laboratory Elev GGT and ALT If AST > ALT suspect ETOH, or cirrhosis if denied Elev TG/Chol, glucose USS (CT also)
69 Hepatomegaly Altered echogenicity Ultrasound Can t distinguish mild form from steatohapatitis/cirrhosis
70 Differential Should exclude other causes Viral hepatitis Drugs - esp alcohol Autoimmune (ANA, SMA) Metabolic (iron, copper) High ferritin with normal transferrin saturation common in NAFLD If saturation >45% ---> HH studies in Caucasians Investigate for metabolic syndrome if not known Almost always assoc with insulin resistance High risk of type 2 diabetes
71 Role of liver biopsy Not clearly elucidated Consider in Pts at risk severe disease Concerning lab studies AST>ALT, low platelets
72 Not really known Management Evidence accumulating that reducing BMI and improving insulin resistance with diet/exercise can reverse Some evidence that there are promising drugs coming Bariatric surgery?

73 Aim 0.5-1kg/wk Weight loss Faster can precipitate steatohepatitis or gallstones Decrease refined sugars Increase fibre Cholesterol improving and DM diet
74 Exercise Increases oxidative capacity of myocytes Increases insulin sensitivity Check LFTs monthly Should see improvements in 2-3/12
75 Metformin Insulin resistance Improves insulin sens of all tissues Improves transaminases in NASH Reverses fatty liver in mice Glitazones Other classes under investigation
76 Statins Lipids Reduce LDL and TG Improves LFTs in NASH Fibrates Gemfibrozil Increases HDL, decreases TG Modest effect only on NASH
77 Helpful points Fatty liver can lead to cirrhosis Females and elderly do worse Often asymptomatic USS usually sufficient for diagnosis No established treatment Steady weight loss first line if obese Rapid weight loss may be dangerous




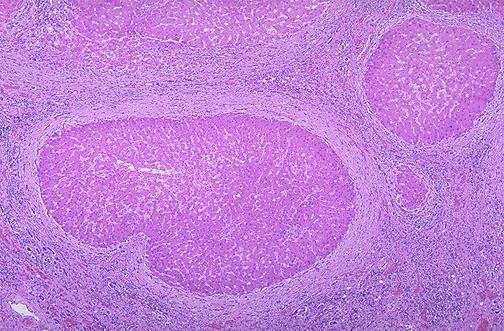
78 Cirrhosis Normal Cirrhosis

79 Liver Cirrhosis May be the end result of chronic cholestatic or hepatitic disease Liver synthetic function may be impaired or normal The enzymes may be of any pattern or may be normal if the underlying aetiology is inactive or no longer present
80 Cirrhosis - Importance Why Important? Hepatoma 1-2% per annum Variceal Bleeding Decompensation Risk of Liver Failure Suggested By Bloods Platelets, Albumin, INR, Bilirubin Clinical Examination Liver Specific / Other Organ injury Imaging: USS / CT Irregular contour, PV size, Splenomegaly, Varices Endoscopy Varices, Portal Hypertensive Gastropathy (PHG)
81 Survival according to Child- Pugh Score POINTS Encephalopathy None Grade 1, 2 Grade 3, 4 Ascites None Mild Moderate Bilirubin < > 50 Albumin > < 28 INR < > 1.5 Grade Score 1 year 5 year 10 year A % 44% 27% B % 20% 10% C % 21% 0% Pugh et al. Br J Surg, 1973
82 Middlemore Hospital Audit - Cirrhosis New patients presenting each year Before 2001 Number Linear (Number) Gerred et al. 2012
83 Y e a r Cirrhosis: Patients removed from the database p r e T ra n s p la n te d L o s t o r m o v e d D e c e a s e d C a s e s w ith d ra w n fro m F o llo w -u p Gerred et al. 2012
84 Cirrhosis: Number of patients under Follow-up Number Linear (Number) Gerred et al. 2012
85 Y e a r o f p re s e n ta tio n Cirrhosis New Case Aetiology O th e r N A F L D H C V H B V A L D N u m b e r o f N e w C a s e s Gerred et al. 2012
86 Cirrhosis: Primary Aetiology and Gender Number of patients Male Female M ale F emale 0 HBV HCV ALD NAFLD Other Primary Aetiology of Cirrhosis 35% 20% 18% 14% 12% Gerred et al. 2012
87 A g e Cirrhosis: Age of presentation & 8 0 Aetiology P < A L D H B V H C V N A F L D A e tio lo g y Gerred et al. 2012
88 A g e Cirrhosis: Race y rs 5 9 y rs 5 7 y rs 5 2 y rs 5 6 y rs 2 0 A s ia n E u r o p e a n In d ia n M a o r i P I E th n ic ity Gerred et al. 2012
89 E th n ic ity Aetiology of Cirrhosis and Ethnicity P I M a o r i In d ia n O th e r N A F L D H C V H B V A L D E u r o p e a n As ia n N u m b e r o f c a s e s Gerred et al. 2012
90 P e rc e n t s u rv iv a l Cirrhosis: Survival & Aetiology C h a r t-5 : S u r v iv a l & A e tio lo g y A L D H B V 4 0 H C V N A F L D 2 0 P< Y e a rs o f F o llo w -u p Gerred et al. 2012
91 P e rc e n t s u rv iv a l Cirrhosis: Survival & Ethnicity C h a r t-4 : S u r v iv a l & E th n ic itie s In d ia n M a o ri P a c ific A s ia n E u ro p e a n 2 0 P= Y e a rs o f F o llo w -u p Gerred et al. 2012



92 Cirrhosis: Complications - 4yr FU Variceal bleed ALD HBV HCV NAFLD 24% 6% 10% 18% SBP 12% 6% 7% 6% Ascites 57% 24% 21% 34% Encephalop athy 35% 11% 13% 14% HCC 11% 25% 13% 13%
93 Transplant and death - 4yr FU ALD NAFLD HBV HCV OLT 2% 3% 7% 6% Liver Death Other Death Total Death 22% 17% 20% 12% 26% 18% 7% 7% 48% 35% 27% 19%
94 HCC Surveillance Period (-1:1 st 6 months, -2:2 nd 6 months)
95 Cirrhosis Middlemore - Conclusions Number of Cirrhotic patients under follow-up has quadrupled in the last 10 years HCV and NAFLD are driving rising numbers of new cases in recent years Generally patients with cirrhosis are living longer but death and complications remain common Poor prognosis in Maori despite predominantly HBV and young Poor prognosis in ALD and NAFLD - older and sicker at presentation
96 Take home messages: Patient care Jaundice and evidence of liver failure Immediate discussion and consider admission Jaundice, no liver failure Immediate discussion?admission Urgent USS, (haemolysis screen) Major elevation ALT/ AST (10 X ULN) Immediate discussion?admission Repeat and review within 24 hours with synthetic function
97 Take home messages: Patient care Moderate elevation LFTs (5 X ULN) INR, Bilirubin, early Repeat with 48 hours with liver screen Early referral Evidence of cirrhosis, no liver failure Abnormal LFTs, abnormal USS, low platelets Early referral with liver screen
98 Take home messages: Patient care Mild Elevation of LFTs (2-3x ULN) Repeat Liver screen USS Referral A methodical approach will usually yield the diagnosis!
99 Dr Alasdair Patrick Gastroenterologist
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
IN THE NAME OF GOD. D r. MANIJE DEZFULI AZAD UNIVERCITY OF TEHRAN BOOALI HOSPITAL INFECTIOUS DISEASES SPECIALIST
 IN THE NAME OF GOD AZAD UNIVERCITY OF TEHRAN BOOALI HOSPITAL D r. MANIJE DEZFULI INFECTIOUS DISEASES SPECIALIST Acute Viral Hepatitis The Anatomy of the Liver Hepatic Physiology Liver: Largest solid organ
IN THE NAME OF GOD AZAD UNIVERCITY OF TEHRAN BOOALI HOSPITAL D r. MANIJE DEZFULI INFECTIOUS DISEASES SPECIALIST Acute Viral Hepatitis The Anatomy of the Liver Hepatic Physiology Liver: Largest solid organ
Hepatocytes produce. Proteins Clotting factors Hormones. Bile Flow
 R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
A Review of Liver Function Tests. James Gray Gastroenterology Vancouver
 A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
A Review of Liver Function Tests James Gray Gastroenterology Vancouver Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
EVALUATION OF ABNORMAL LIVER TESTS
 EVALUATION OF ABNORMAL LIVER TESTS MIA MANABAT DO PGY6 MOA 119 TH ANNUAL SPRING SCIENTIFIC CONVENTION MAY 19, 2018 EVALUATION OF ABNORMAL LIVER TESTS Review of liver enzymes vs liver function tests Clinical
EVALUATION OF ABNORMAL LIVER TESTS MIA MANABAT DO PGY6 MOA 119 TH ANNUAL SPRING SCIENTIFIC CONVENTION MAY 19, 2018 EVALUATION OF ABNORMAL LIVER TESTS Review of liver enzymes vs liver function tests Clinical
LFTs: an update A MacGilchrist PLIG meeting 31st January 2019
 LFTs: an update A MacGilchrist PLIG meeting 31 st January 2019 LFTs: what are we trying to achieve? (1) The case against investigation abnormal LFTs in up to 21% of the population only 1-2% develop significant
LFTs: an update A MacGilchrist PLIG meeting 31 st January 2019 LFTs: what are we trying to achieve? (1) The case against investigation abnormal LFTs in up to 21% of the population only 1-2% develop significant
ABNORMAL LIVER FUNCTION TESTS. Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust
 ABNORMAL LIVER FUNCTION TESTS Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust INTRODUCTION Liver function tests Cases Non invasive fibrosis measurement Questions UK MORTALITY RATE
ABNORMAL LIVER FUNCTION TESTS Dr Uthayanan Chelvaratnam Hepatology Consultant North Bristol NHS Trust INTRODUCTION Liver function tests Cases Non invasive fibrosis measurement Questions UK MORTALITY RATE
What to do with abnormal LFTs? Andrew M Smith Hepatobiliary Surgeon
 What to do with abnormal LFTs? Andrew M Smith Hepatobiliary Surgeon "it looks like there's something wrong.with your television set. Matt Groenig, creator of The Simpsons Probability of an abnormal screening
What to do with abnormal LFTs? Andrew M Smith Hepatobiliary Surgeon "it looks like there's something wrong.with your television set. Matt Groenig, creator of The Simpsons Probability of an abnormal screening
2. Liver blood tests and what they mean p2 Acute and chronic liver screen
 Hepatology referral pathways for GP 1 Scope For use within hepatology Contents 2. Liver blood tests and what they mean p2 Acute and chronic liver screen p2 Common reasons for hepatology referral 3. Raised
Hepatology referral pathways for GP 1 Scope For use within hepatology Contents 2. Liver blood tests and what they mean p2 Acute and chronic liver screen p2 Common reasons for hepatology referral 3. Raised
2. Liver blood tests and what they mean p2 Acute and chronic liver screen
 1 Scope For use within hepatology Contents 2. Liver blood tests and what they mean p2 Acute and chronic liver screen p2 Common reasons for referral 3. Raised ALT +/- GGT p3 4. Non alcoholic fatty liver
1 Scope For use within hepatology Contents 2. Liver blood tests and what they mean p2 Acute and chronic liver screen p2 Common reasons for referral 3. Raised ALT +/- GGT p3 4. Non alcoholic fatty liver
CITY AND HACKNEY CCG ABNORMAL LIVER FUNCTION TESTS (LFTs) in ADULTS
 in ADULTS") CITY AND HACKNEY CCG ABNORMAL LIVER FUNCTION TESTS (LFTs) in ADULTS Interpreting abnormal liver function tests (LFTs) and trying to diagnose any underlying liver disease is a common scenario in Primary
CITY AND HACKNEY CCG ABNORMAL LIVER FUNCTION TESTS (LFTs) in ADULTS Interpreting abnormal liver function tests (LFTs) and trying to diagnose any underlying liver disease is a common scenario in Primary
Hepatitis. Dr. Mohamed. A. Mahdi 5/2/2019. Mob:
 Hepatitis Dr. Mohamed. A. Mahdi Mob: 0123002800 5/2/2019 Hepatitis Hepatitis means the inflammation of the liver. May cause by viruses or bacteria, parasites, radiation, drugs, chemical and toxins (alcohol).
Hepatitis Dr. Mohamed. A. Mahdi Mob: 0123002800 5/2/2019 Hepatitis Hepatitis means the inflammation of the liver. May cause by viruses or bacteria, parasites, radiation, drugs, chemical and toxins (alcohol).
Approach to the Patient with Liver Disease
 Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Interpreting Liver Function Tests
 PSH Clinical Guidelines Statement 2017 Interpreting Liver Function Tests Dr. Asad A Chaudhry Consultant Hepatologist, Chaudhry Hospital, Gujranwala, Pakistan. Liver function tests (LFTs) generally refer
PSH Clinical Guidelines Statement 2017 Interpreting Liver Function Tests Dr. Asad A Chaudhry Consultant Hepatologist, Chaudhry Hospital, Gujranwala, Pakistan. Liver function tests (LFTs) generally refer
WEEK. MPharm Programme. Liver Biochemistry. Slide 1 of 49 MPHM14 Liver Biochemistry
 MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
MPharm Programme Liver Biochemistry Slide 1 of 49 MPHM Liver Biochemistry Learning Outcomes Assess and evaluate the signs and symptoms of illness Assess and critically appraise a patients medication regimen,
Biochemical Investigations in Liver Disease. Dr Roshitha de Silva Department of Pathology Faculty of Medicine University of Kelaniya
 Biochemical Investigations in Liver Disease Dr Roshitha de Silva Department of Pathology Faculty of Medicine University of Kelaniya Biochemical markers Albumin ALP ALT, AST Gamma-glutamyl transpeptidase
Biochemical Investigations in Liver Disease Dr Roshitha de Silva Department of Pathology Faculty of Medicine University of Kelaniya Biochemical markers Albumin ALP ALT, AST Gamma-glutamyl transpeptidase
Abnormal Liver Chemistries. Lauren Myers, MMsc. PA-C Oregon Health and Science University
 Abnormal Liver Chemistries Lauren Myers, MMsc. PA-C Oregon Health and Science University Disclosure 1. The speaker/planner Lauren Myers, MMSc, PA-C have no relevant financial relationships to disclose
Abnormal Liver Chemistries Lauren Myers, MMsc. PA-C Oregon Health and Science University Disclosure 1. The speaker/planner Lauren Myers, MMSc, PA-C have no relevant financial relationships to disclose
Viral Hepatitis. Dr Melissa Haines Gastroenterologist Waikato Hospital
 Viral Hepatitis Dr Melissa Haines Gastroenterologist Waikato Hospital Viral Hepatitis HAV HBV HCV HDV HEV Other viral: CMV, EBV, HSV Unknown Hepatitis A Hepatitis A Transmitted via the faecal-oral route
Viral Hepatitis Dr Melissa Haines Gastroenterologist Waikato Hospital Viral Hepatitis HAV HBV HCV HDV HEV Other viral: CMV, EBV, HSV Unknown Hepatitis A Hepatitis A Transmitted via the faecal-oral route
Investigating and Referring Incidental Findings of Abnormal Liver Tests
 Investigating and Referring Incidental Findings of Abnormal Liver Tests Note on Referral Guidelines: these revised guidelines are presented as a tool to aid appropriate referral and management of common
Investigating and Referring Incidental Findings of Abnormal Liver Tests Note on Referral Guidelines: these revised guidelines are presented as a tool to aid appropriate referral and management of common
King s College Hospital NHS Foundation Trust. Acute Liver Disease: what you really need to know.
 King s College Hospital NHS Foundation Trust Acute Liver Disease: what you really need to know. William Bernal Professor of Liver Critical Care Liver Intensive Therapy Unit Institute of Liver Studies Kings
King s College Hospital NHS Foundation Trust Acute Liver Disease: what you really need to know. William Bernal Professor of Liver Critical Care Liver Intensive Therapy Unit Institute of Liver Studies Kings
Viral hepatitis Blood Born hepatitis. Dr. MONA BADR Assistant Professor College of Medicine & KKUH
 Viral hepatitis Blood Born hepatitis Dr. MONA BADR Assistant Professor College of Medicine & KKUH Outline Introduction to hepatitis Characteristics of viral hepatitis Mode of transmission Markers of hepatitis
Viral hepatitis Blood Born hepatitis Dr. MONA BADR Assistant Professor College of Medicine & KKUH Outline Introduction to hepatitis Characteristics of viral hepatitis Mode of transmission Markers of hepatitis
A Rational Evidence-based Approach to Abnormal Liver Tests
 A Rational Evidence-based Approach to Abnormal Liver Tests Jane D. Ricaforte-Campos, MD FPCP, FPSG, FPSDE 2013 HSP Post-graduate Course Radisson Blu Hotel, Cebu City misnomer Liver Function Tests Does
A Rational Evidence-based Approach to Abnormal Liver Tests Jane D. Ricaforte-Campos, MD FPCP, FPSG, FPSDE 2013 HSP Post-graduate Course Radisson Blu Hotel, Cebu City misnomer Liver Function Tests Does
Viral hepatitis. Supervised by: Dr.Gaith. presented by: Shaima a & Anas & Ala a
 Viral hepatitis Supervised by: Dr.Gaith presented by: Shaima a & Anas & Ala a Etiology Common: Hepatitis A Hepatitis B Hepatitis C Hepatitis D Hepatitis E Less common: Cytomegalovirus EBV Rare: Herpes
Viral hepatitis Supervised by: Dr.Gaith presented by: Shaima a & Anas & Ala a Etiology Common: Hepatitis A Hepatitis B Hepatitis C Hepatitis D Hepatitis E Less common: Cytomegalovirus EBV Rare: Herpes
What to do about the high ALT picked up at the annual review. Dr Michael Yee Consultant in Diabetes and Endocrinology
 What to do about the high ALT picked up at the annual review Dr Michael Yee Consultant in Diabetes and Endocrinology Mrs DC HPC PMH Type 2 Diabetes (decades) Regular retinal screening No foot complications/neuropathy
What to do about the high ALT picked up at the annual review Dr Michael Yee Consultant in Diabetes and Endocrinology Mrs DC HPC PMH Type 2 Diabetes (decades) Regular retinal screening No foot complications/neuropathy
Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP
 Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP Autoimmune hepatobiliary diseases The liver is an important target for immunemediated injury. Three disease phenotypes are recognized:
Autoimmune Hepatobiliary Diseases PROF. DR. SABEHA ALBAYATI CABM,FRCP Autoimmune hepatobiliary diseases The liver is an important target for immunemediated injury. Three disease phenotypes are recognized:
HEPETIC SYSTEMS BIOCHEMICAL HEPATOCYTIC SYSTEM HEPATOBILIARY SYSTEM RETICULOENDOTHELIAL SYSTEM
 EVALUATION OF LIVER FUNCTION R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty HEPETIC SYSTEMS BIOCHEMICAL HEPATOCYTIC SYSTEM HEPATOBILIARY SYSTEM RETICULOENDOTHELIAL SYSTEM METABOLIC FUNCTION
EVALUATION OF LIVER FUNCTION R. Mohammadi Biochemist (Ph.D.) Faculty member of Medical Faculty HEPETIC SYSTEMS BIOCHEMICAL HEPATOCYTIC SYSTEM HEPATOBILIARY SYSTEM RETICULOENDOTHELIAL SYSTEM METABOLIC FUNCTION
Acute Hepatitis: An Approach to Infectious and Other Causes. Mary Anne Cooper MSc, MD, MEd, FRCPC
 : An Approach to Infectious and Other Causes Mary Anne Cooper MSc, MD, MEd, FRCPC Faculty: Dr. Mary Anne Cooper Relationships with commercial interests: Consulting Fees: Lupin Pharmaceuticals, Canada Objectives
: An Approach to Infectious and Other Causes Mary Anne Cooper MSc, MD, MEd, FRCPC Faculty: Dr. Mary Anne Cooper Relationships with commercial interests: Consulting Fees: Lupin Pharmaceuticals, Canada Objectives
End Stage Liver Disease & Disease Specific Indications for Liver Transplant. Susan Kang, RN, MSN, ANP-BC
 End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP-BC Introduction (https://www.srtr.org) What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP-BC Introduction (https://www.srtr.org) What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC
 End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC Introduction (https://www.srtr.org) 1 What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
End Stage Liver Disease & Disease Specific Indications for Liver Transplant Susan Kang, RN, MSN, ANP BC Introduction (https://www.srtr.org) 1 What does the liver do? STORAGE METABOLIC DETOXIFICATION SYNTHETIC
Hepatitis B Virus. Taylor Page PharmD Candidate 2019 February 1, 2019
 Hepatitis B Virus Taylor Page PharmD Candidate 2019 February 1, 2019 Epidemiology 3218 cases of acute HBV reported in 2016 847,000 non-institutionalized persons living with chronic HBV in 2011-2012 Viral
Hepatitis B Virus Taylor Page PharmD Candidate 2019 February 1, 2019 Epidemiology 3218 cases of acute HBV reported in 2016 847,000 non-institutionalized persons living with chronic HBV in 2011-2012 Viral
Abnormal LFTs in migrant populations. Dr Doug Macdonald Consultant Hepatologist Royal Free Hospital
 Abnormal LFTs in migrant populations Dr Doug Macdonald Consultant Hepatologist Royal Free Hospital www.migrationobservatory.ox.ac.uk Migrants in London Migrants in London Migrants in London Common liver
Abnormal LFTs in migrant populations Dr Doug Macdonald Consultant Hepatologist Royal Free Hospital www.migrationobservatory.ox.ac.uk Migrants in London Migrants in London Migrants in London Common liver
Anaemia Pathway. Anaemia. Type of Anaemia Check Haematinics (Iron stores,b12,folate) Fit for endoscopies. endoscopies yes no. Non Iron Deficient
 Fit for endoscopies. endoscopies yes no. Non Iron Deficient") Cognitive if unable to consent, must attend clinic with next of kin to act as advocate. Rockwood Frailty Score 6 consider appropriate referral to elderly care. See attachment Anaemia Pathway Anaemia Type
Cognitive if unable to consent, must attend clinic with next of kin to act as advocate. Rockwood Frailty Score 6 consider appropriate referral to elderly care. See attachment Anaemia Pathway Anaemia Type
Initial Evaluation for HCV Therapy. Hope McGratty PA-C, MPH
 Initial Evaluation for HCV Therapy Hope McGratty PA-C, MPH Conflict of Interest Disclosure Statement None Who are we talking about today? Treatment naïve Chronic infection This patient seems complicated
Initial Evaluation for HCV Therapy Hope McGratty PA-C, MPH Conflict of Interest Disclosure Statement None Who are we talking about today? Treatment naïve Chronic infection This patient seems complicated
I have no disclosures relevant to this presentation LIVER TESTS: WHAT IS INCLUDED? LIVER TESTS: HOW TO UTILIZE THEM OBJECTIVES
 LIVER TESTS: HOW TO UTILIZE THEM I have no disclosures relevant to this presentation José Franco, MD Professor of Medicine, Surgery and Pediatrics Medical College of Wisconsin OBJECTIVES Differentiate
LIVER TESTS: HOW TO UTILIZE THEM I have no disclosures relevant to this presentation José Franco, MD Professor of Medicine, Surgery and Pediatrics Medical College of Wisconsin OBJECTIVES Differentiate
Approach to Abnormal Liver Tests
 Approach to Abnormal Liver Tests Scott W. Biggins, MD, MAS Assistant Professor Division of Gastroenterology UCSF Scott.Biggins@ucsf.edu (Thanks to Hal Yee, MD) This Morning s Presentation Clinical vignettes
Approach to Abnormal Liver Tests Scott W. Biggins, MD, MAS Assistant Professor Division of Gastroenterology UCSF Scott.Biggins@ucsf.edu (Thanks to Hal Yee, MD) This Morning s Presentation Clinical vignettes
Jaundice Chris Wells Regional CMT teaching 6 th June 2017
 Jaundice Chris Wells Regional CMT teaching 6 th June 2017 By the end you will Have a systematic approach to the patient with jaundice Be able to diagnose the cause of jaundice Have a framework for managing
Jaundice Chris Wells Regional CMT teaching 6 th June 2017 By the end you will Have a systematic approach to the patient with jaundice Be able to diagnose the cause of jaundice Have a framework for managing
4/27/2018. Disclosures LIVER FUNCTION TESTS LIVER FUNCTION TESTS LIVER FUNCTION TESTS APPROACH TO THE PATIENT WITH ABNORMAL LIVER TESTS
 APPROACH TO THE PATIENT WITH ABNORMAL TESTS Kimberly A. Brown, M.D, FAST, FAASLD, AGAF Chief, Division of Gastroenterology and Hepatology Henry Ford Hospital Henry Ford Health System Detroit, Michigan
APPROACH TO THE PATIENT WITH ABNORMAL TESTS Kimberly A. Brown, M.D, FAST, FAASLD, AGAF Chief, Division of Gastroenterology and Hepatology Henry Ford Hospital Henry Ford Health System Detroit, Michigan
Hepatitis B screening and surveillance in primary care
 Hepatitis B screening and surveillance in primary care Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures
Hepatitis B screening and surveillance in primary care Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital Disclosures
CHAPTER 1. Alcoholic Liver Disease
 CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
CHAPTER 1 Alcoholic Liver Disease Major Lesions of Alcoholic Liver Disease Alcoholic fatty liver - >90% of binge and chronic drinkers Alcoholic hepatitis precursor of cirrhosis Alcoholic cirrhosis end
Viral Hepatitis. Dr. Abdulwahhab S. Abdullah CABM, FICMS-G&H PROF. DR. SABEHA ALBAYATI CABM,FRCP
 Viral Hepatitis Dr. Abdulwahhab S. Abdullah CABM, FICMS-G&H PROF. DR. SABEHA ALBAYATI CABM,FRCP Viral hepatitis Viral hepatitis must be considered in any patient presenting with hepatitis on LFTs (high
Viral Hepatitis Dr. Abdulwahhab S. Abdullah CABM, FICMS-G&H PROF. DR. SABEHA ALBAYATI CABM,FRCP Viral hepatitis Viral hepatitis must be considered in any patient presenting with hepatitis on LFTs (high
Diseases of liver. Dr. Mohamed. A. Mahdi 4/2/2019. Mob:
 Diseases of liver Dr. Mohamed. A. Mahdi Mob: 0123002800 4/2/2019 Cirrhosis Cirrhosis is a complication of many liver disease. Permanent scarring of the liver. A late-stage liver disease. The inflammation
Diseases of liver Dr. Mohamed. A. Mahdi Mob: 0123002800 4/2/2019 Cirrhosis Cirrhosis is a complication of many liver disease. Permanent scarring of the liver. A late-stage liver disease. The inflammation
Chronic Hepatitis B Infection
 Chronic Hepatitis B Infection Mohssen Nassiri Toosi, MD Imam Khomeinin Hospital Tehran University of Medical Sciences Chronic Hepatitis B Infection Virus : HBs Ag Positive Host Liver Health Chronic Hepatitis
Chronic Hepatitis B Infection Mohssen Nassiri Toosi, MD Imam Khomeinin Hospital Tehran University of Medical Sciences Chronic Hepatitis B Infection Virus : HBs Ag Positive Host Liver Health Chronic Hepatitis
World Health Organization. Western Pacific Region
 Standard modules for HBV 1 HBV Module 1 Hepatitis B serological markers and virology 2 Acute hepatitis HAV HBV HCV HDV HEV Case fatality Case fatality Uncommon increases with increases with age age Superinfection
Standard modules for HBV 1 HBV Module 1 Hepatitis B serological markers and virology 2 Acute hepatitis HAV HBV HCV HDV HEV Case fatality Case fatality Uncommon increases with increases with age age Superinfection
Primary Biliary Cholangitis
 Primary Biliary Cholangitis PBC Foundation (UK) Ltd 6 Hill Street Edinburgh EH2 3JZ Tel: +44 (0) 131 556 6811 info@pbcfoundation.org.uk www.pbcfoundation.org.uk PBC for Healthcare Practitioners Introduction
Primary Biliary Cholangitis PBC Foundation (UK) Ltd 6 Hill Street Edinburgh EH2 3JZ Tel: +44 (0) 131 556 6811 info@pbcfoundation.org.uk www.pbcfoundation.org.uk PBC for Healthcare Practitioners Introduction
LIVER FUNCTION TESTS. G M Kellerman. Hunter Area Pathology Service
 LIVER FUNCTION TESTS G M Kellerman Hunter Area Pathology Service FUNCTIONS OF LIVER Carbohydrate metabolism storage (glycogen), release, synthesis (gluconeogenesis), interconversion (galactose, fructose),
LIVER FUNCTION TESTS G M Kellerman Hunter Area Pathology Service FUNCTIONS OF LIVER Carbohydrate metabolism storage (glycogen), release, synthesis (gluconeogenesis), interconversion (galactose, fructose),
Management of Hepatitis B - Information for primary care providers
 Management of Hepatitis B - Information for primary care providers July 2018 Chronic hepatitis B (CHB) is often a lifelong condition. Not everyone infected needs anti-viral therapy. This document outlines
Management of Hepatitis B - Information for primary care providers July 2018 Chronic hepatitis B (CHB) is often a lifelong condition. Not everyone infected needs anti-viral therapy. This document outlines
ABIM Review Hepatobiliary
 ABIM Review Hepatobiliary Danielle Brandman, MD, MAS Assistant Professor of Medicine University of California San Francisco ABIM Certification Exam ABIM Certification Exam Hepatobiliary Review Diagnostic
ABIM Review Hepatobiliary Danielle Brandman, MD, MAS Assistant Professor of Medicine University of California San Francisco ABIM Certification Exam ABIM Certification Exam Hepatobiliary Review Diagnostic
ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries
 ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries Paul Y. Kwo, MD, FACG, FAASLD 1, Stanley M. Cohen, MD, FACG, FAASLD 2, and Joseph K. Lim, MD, FACG, FAASLD 3 1 Division of Gastroenterology/Hepatology,
ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries Paul Y. Kwo, MD, FACG, FAASLD 1, Stanley M. Cohen, MD, FACG, FAASLD 2, and Joseph K. Lim, MD, FACG, FAASLD 3 1 Division of Gastroenterology/Hepatology,
World Health Organization. Western Pacific Region
 Basic modules for hepatitis 1 Basic Module 1 Liver anatomy and physiology 2 Position of liver Midline Located in right upper abdomen Protected by the right rib cage Right upper Measures: 12 15 cm in vertical
Basic modules for hepatitis 1 Basic Module 1 Liver anatomy and physiology 2 Position of liver Midline Located in right upper abdomen Protected by the right rib cage Right upper Measures: 12 15 cm in vertical
Pathophysiology I Liver and Biliary Disease
 Pathophysiology I Liver and Biliary Disease The Liver The liver is located in the right upper portion of the abdominal cavity just beneath the right side of the rib cage. The liver has many functions that
Pathophysiology I Liver and Biliary Disease The Liver The liver is located in the right upper portion of the abdominal cavity just beneath the right side of the rib cage. The liver has many functions that
Liver Disease. By: Michael Martins
 Liver Disease By: Michael Martins Recently I have been getting a flurry of patients that have some serious liver complications. This week s literature review will be the dental management of the patients
Liver Disease By: Michael Martins Recently I have been getting a flurry of patients that have some serious liver complications. This week s literature review will be the dental management of the patients
Liver Network. Guidelines for the Management of Adults with Asymptomatic Liver Function Abnormalities
 Liver Network Guidelines for the Management of Adults with Asymptomatic Liver Function Abnormalities Dr Mark Hudson Dr Stuart McPherson On behalf of the North East & North Cumbria Hepatology Network 1
Liver Network Guidelines for the Management of Adults with Asymptomatic Liver Function Abnormalities Dr Mark Hudson Dr Stuart McPherson On behalf of the North East & North Cumbria Hepatology Network 1
Laboratory Tests and Diagnostic Procedures in Liver Disease: Adventures in Liverland
 Laboratory Tests and Diagnostic Procedures in Liver Disease: Adventures in Liverland Sanjiv Chopra, MD, MACP Professor of Medicine Harvard Medical School Editor In Chief Hepatology Section Up To Date Serum
Laboratory Tests and Diagnostic Procedures in Liver Disease: Adventures in Liverland Sanjiv Chopra, MD, MACP Professor of Medicine Harvard Medical School Editor In Chief Hepatology Section Up To Date Serum
Mrs Janet Catt. Pre-Conference Nurse s Course. Royal Free London NHS Foundation Trust. Janet Catt MSc RN Lead Nurse Specialist Practic 12/12/2014
 Pre-Conference Nurse s Course in partnership with Mrs Janet Catt Royal Free London NHS Foundation Trust Janet Catt MSc RN Lead Nurse Specialist Practic 1 Liver blood tests monitoring cirrhosis HIV/HCV
Pre-Conference Nurse s Course in partnership with Mrs Janet Catt Royal Free London NHS Foundation Trust Janet Catt MSc RN Lead Nurse Specialist Practic 1 Liver blood tests monitoring cirrhosis HIV/HCV
Module 1 Introduction of hepatitis
 Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
Primary Biliary Cholangitis
 Primary Biliary Cholangitis What is primary biliary cholangitis? Primary biliary cholangitis (PBC), formerly known as primary biliary cirrhosis, is a chronic liver disease. When a person has PBC, the immune
Primary Biliary Cholangitis What is primary biliary cholangitis? Primary biliary cholangitis (PBC), formerly known as primary biliary cirrhosis, is a chronic liver disease. When a person has PBC, the immune
EAST LONDON INTEGRATED CARE
 CITY & HACKNEY ELIC EAST LONDON INTEGRATED CARE MANAGEMENT OF CHRONIC HEPATITIS B IN PRIMARY CARE Chronic Hepatitis B virus (HBV) is an important public health problem globally and a leading cause of liver
CITY & HACKNEY ELIC EAST LONDON INTEGRATED CARE MANAGEMENT OF CHRONIC HEPATITIS B IN PRIMARY CARE Chronic Hepatitis B virus (HBV) is an important public health problem globally and a leading cause of liver
Mr Ricky Gellissen Imperial College Healthcare NHS Trust, London, UK
 Mr Ricky Gellissen Imperial College Healthcare NHS Trust, London, UK Ms Sally Bufton University Hospital Birmingham NHS Foundation Trust, Queen Elizabeth Hospital, Birmingham Mrs Janet Catt Royal Free
Mr Ricky Gellissen Imperial College Healthcare NHS Trust, London, UK Ms Sally Bufton University Hospital Birmingham NHS Foundation Trust, Queen Elizabeth Hospital, Birmingham Mrs Janet Catt Royal Free
Chronic Hepatitis. Andrew Bathgate Chris Bellamy Royal Infirmary of Edinburgh
 Chronic Hepatitis Andrew Bathgate Chris Bellamy Royal Infirmary of Edinburgh Autoimmune Hepatitis Annual incidence 1.9/100 000 in N Europe Prevalence 16.9/100 000 ~5% all liver transplants Female preponderance
Chronic Hepatitis Andrew Bathgate Chris Bellamy Royal Infirmary of Edinburgh Autoimmune Hepatitis Annual incidence 1.9/100 000 in N Europe Prevalence 16.9/100 000 ~5% all liver transplants Female preponderance
Dr David Rowbotham NHS. The Leeds Teaching Hospitals. NHS Trust
 Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust NHS Nurses Update June 2010 Chronic Hepatitis HBV / HCV David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology
Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust NHS Nurses Update June 2010 Chronic Hepatitis HBV / HCV David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology
Liver Network Guidelines for the Management of Adults with Asymptomatic Liver Function Abnormalities
 Liver Network Guidelines for the Management of Adults with Asymptomatic Liver Function Abnormalities Dr Mark Hudson Dr Stuart McPherson On behalf of the North East & North Cumbria Hepatology Network 1
Liver Network Guidelines for the Management of Adults with Asymptomatic Liver Function Abnormalities Dr Mark Hudson Dr Stuart McPherson On behalf of the North East & North Cumbria Hepatology Network 1
Liver Function Testing. in primary care. Quiz Feedback
 Liver Function Testing in primary care Quiz Feedback Contents Expert Summary, Associate Professor Ed Gane 3 Liver Function Testing in Primary Care Quiz 4 Quiz Feedback: Responses from Colleagues, and Specialist
Liver Function Testing in primary care Quiz Feedback Contents Expert Summary, Associate Professor Ed Gane 3 Liver Function Testing in Primary Care Quiz 4 Quiz Feedback: Responses from Colleagues, and Specialist
What are LFTs? What are LFTs? 3/20/2017. Evaluation of Abnormal Liver Chemistry Tests. Transaminases. Alkaline phosphatase.
 Evaluation of Abnormal Liver Chemistry Tests James Panetta, DO What are LFTs? Transaminases Alkaline phosphatase Bilirubin Gamma-glutamyl transpeptidase What are LFTs? 5 nucleosidase Lactate Dehydrogenase
Evaluation of Abnormal Liver Chemistry Tests James Panetta, DO What are LFTs? Transaminases Alkaline phosphatase Bilirubin Gamma-glutamyl transpeptidase What are LFTs? 5 nucleosidase Lactate Dehydrogenase
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Outline. Updates in the Clinical Management of Hepatitis B and C. Who should be screened for HBV? Chronic Hepatitis B 10/7/2018
 Outline Updates in the Clinical Management of Hepatitis B and C Jennifer C. Lai, MD, MBA Transplant Hepatologist Associate Professor of Medicine In Residence University of California, San Francisco Initial
Outline Updates in the Clinical Management of Hepatitis B and C Jennifer C. Lai, MD, MBA Transplant Hepatologist Associate Professor of Medicine In Residence University of California, San Francisco Initial
GI Workshop Case Studies
 GI Workshop Case Studies Cliff Titcomb MD Hannover Re AAIM Annual Meeting San Diego, October, 2012 5 Tests Commonly Known as Liver Function Tests Alanine Aminotransferase (ALT, SGPT) Aspartate Aminotransferase
GI Workshop Case Studies Cliff Titcomb MD Hannover Re AAIM Annual Meeting San Diego, October, 2012 5 Tests Commonly Known as Liver Function Tests Alanine Aminotransferase (ALT, SGPT) Aspartate Aminotransferase
Western Health Specialist Clinics Access & Referral Guidelines
 Gastroenterology Specialist Clinics at Western Health: Western Health provides the following Specialist Clinics for patients who require assessment and management of Gastroenterology / Hepatology conditions.
Gastroenterology Specialist Clinics at Western Health: Western Health provides the following Specialist Clinics for patients who require assessment and management of Gastroenterology / Hepatology conditions.
Pediatric PSC A children s tale
 Pediatric PSC A children s tale September 8 th PSC Partners seeking a cure Tamir Miloh Assistant Professor Pediatric Hepatology Mount Sinai Hospital, NY Incidence Primary Sclerosing Cholangitis (PSC) ;
Pediatric PSC A children s tale September 8 th PSC Partners seeking a cure Tamir Miloh Assistant Professor Pediatric Hepatology Mount Sinai Hospital, NY Incidence Primary Sclerosing Cholangitis (PSC) ;
HBV in HIV Forgotten but not Gone
 Activity Code FA376 HBV in HIV Forgotten but not Gone Richard K. Sterling, MD, MSc VCU Hepatology Professor of Medicine Chief, Section of Hepatology Virginia Commonwealth University Learning Objectives
Activity Code FA376 HBV in HIV Forgotten but not Gone Richard K. Sterling, MD, MSc VCU Hepatology Professor of Medicine Chief, Section of Hepatology Virginia Commonwealth University Learning Objectives
Drug therapy in patient with hepatic impairment
 Drug therapy in patient with hepatic impairment Arzneimitteltherapie bei Leberinsuffizienz Dominik Wilke 03/04 Mai 2018 43. ADKA-Kongress, Stuttgart Functions of the Liver I Metabolism (Carbohydrates,
Drug therapy in patient with hepatic impairment Arzneimitteltherapie bei Leberinsuffizienz Dominik Wilke 03/04 Mai 2018 43. ADKA-Kongress, Stuttgart Functions of the Liver I Metabolism (Carbohydrates,
CrackCast Episode 28 Jaundice
 CrackCast Episode 28 Jaundice Episode overview: 1) Describe heme metabolism 2) List common pre-hepatic/hepatic/post-hepatic causes of jaundice Wisecracks: 1) What are clinical signs of liver disease? 2)
CrackCast Episode 28 Jaundice Episode overview: 1) Describe heme metabolism 2) List common pre-hepatic/hepatic/post-hepatic causes of jaundice Wisecracks: 1) What are clinical signs of liver disease? 2)
Chronic Hepatitis B. What every GP should know. Prof Ed Gane NZ Liver Unit
 Chronic Hepatitis B What every GP should know Prof Ed Gane Z Liver Unit Case 1 55 Yr old Tonga male»well but dad died of liver cancer»lfts: ALT 85, GGT 60; ALP 75; bilirubin 12 What next? Case 1 55 Yr
Chronic Hepatitis B What every GP should know Prof Ed Gane Z Liver Unit Case 1 55 Yr old Tonga male»well but dad died of liver cancer»lfts: ALT 85, GGT 60; ALP 75; bilirubin 12 What next? Case 1 55 Yr
Management of Hepatitis C in Primary Care BABAFEMI ONABANJO, MD & BEN ALFRED, FNP UMASS FAMILY HEALTH CENTER WORCESTER
 Management of Hepatitis C in Primary Care BABAFEMI ONABANJO, MD & BEN ALFRED, FNP UMASS FAMILY HEALTH CENTER WORCESTER Objective Epidemiology Screening criteria Appropriate work up Treatment Guidelines
Management of Hepatitis C in Primary Care BABAFEMI ONABANJO, MD & BEN ALFRED, FNP UMASS FAMILY HEALTH CENTER WORCESTER Objective Epidemiology Screening criteria Appropriate work up Treatment Guidelines
Dr Alasdair Patrick Gastroenterologist
 Dr Alasdair Patrick Gastroenterologist Evaluation of Abnormal Liver Function Tests Dr Alasdair Patrick Gastroenterologist MacMurray Gastroenterology Overview Components of LFTs Abnormalities Hepatitis
Dr Alasdair Patrick Gastroenterologist Evaluation of Abnormal Liver Function Tests Dr Alasdair Patrick Gastroenterologist MacMurray Gastroenterology Overview Components of LFTs Abnormalities Hepatitis
9/28/2016. Elevated Liver Function Tests: A Case Based Approach. Objectives. Identify patterns of abnormal liver function tests
 Elevated Liver Function Tests: A Case Based Approach Terrance M. James, NP C The Oregon Clinic Hepatology 503 963 2707 tejames@orclinic.com Objectives Identify patterns of abnormal liver function tests
Elevated Liver Function Tests: A Case Based Approach Terrance M. James, NP C The Oregon Clinic Hepatology 503 963 2707 tejames@orclinic.com Objectives Identify patterns of abnormal liver function tests
Interpreting Liver Tests What Do They Mean? Roman E. Perri, MD
 Interpreting Liver Tests What Do They Mean? Roman E. Perri, MD The assessment of patients with abnormal liver tests is common in both primary care and gastroenterology clinics. However, among patients
Interpreting Liver Tests What Do They Mean? Roman E. Perri, MD The assessment of patients with abnormal liver tests is common in both primary care and gastroenterology clinics. However, among patients
ABIM Review Hepatobiliary
 Hepatobiliary Review ABIM Review Hepatobiliary Oren Fix, MD, MSc Assistant Professor of Medicine University of California San Francisco Diagnostic algorithms for cholestatic versus hepatitic pattern of
Hepatobiliary Review ABIM Review Hepatobiliary Oren Fix, MD, MSc Assistant Professor of Medicine University of California San Francisco Diagnostic algorithms for cholestatic versus hepatitic pattern of
AAIM: GI Workshop Follow Up to Case Studies. Non-alcoholic Fatty Liver Disease Ulcerative Colitis Crohn s Disease
 AAIM: GI Workshop Follow Up to Case Studies Non-alcoholic Fatty Liver Disease Ulcerative Colitis Crohn s Disease Daniel Zimmerman, MD VP and Medical Director, RGA Global October 2015 Non-alcoholic Fatty
AAIM: GI Workshop Follow Up to Case Studies Non-alcoholic Fatty Liver Disease Ulcerative Colitis Crohn s Disease Daniel Zimmerman, MD VP and Medical Director, RGA Global October 2015 Non-alcoholic Fatty
PBC/AIH variant/ overlap syndrome vs PBC with hepatitic features?
 22 November 2018 BD-IAP UK-LPG Liver Update PBC/AIH variant/ overlap syndrome vs PBC with hepatitic features? in a UDCA non-responder Dina G. Tiniakos Institute of Cellular Medicine, Faculty of Medical
22 November 2018 BD-IAP UK-LPG Liver Update PBC/AIH variant/ overlap syndrome vs PBC with hepatitic features? in a UDCA non-responder Dina G. Tiniakos Institute of Cellular Medicine, Faculty of Medical
Disclosure. Evaluation of Abnormal Hepatic Enzymes
 Evaluation of Abnormal Hepatic Enzymes Bruce D. Askey, MS, ANP-BC Associate Lecturer North Andover, MA Adult Nurse Practitioner Dept. of Hepatology/Gastroenterology Guthrie Clinic Sayre, Pa Disclosure
Evaluation of Abnormal Hepatic Enzymes Bruce D. Askey, MS, ANP-BC Associate Lecturer North Andover, MA Adult Nurse Practitioner Dept. of Hepatology/Gastroenterology Guthrie Clinic Sayre, Pa Disclosure
ABIM Review Hepatology
 ABIM Review Hepatology Norah Terrault, MD, MPH Associate Professor University of California San Francisco July 15, 2009 Liver Review Diagnostic algorithms for cholestatic versus hepatitic pattern of liver
ABIM Review Hepatology Norah Terrault, MD, MPH Associate Professor University of California San Francisco July 15, 2009 Liver Review Diagnostic algorithms for cholestatic versus hepatitic pattern of liver
CASES FOR DISCUSSION. Yohannes B
 CASES FOR DISCUSSION Yohannes B HCV CASE-1 A 34 years old apparently healthy lady who came to us after being told to have HCV infection on medical checkup done as part of a visa approval process to travel
CASES FOR DISCUSSION Yohannes B HCV CASE-1 A 34 years old apparently healthy lady who came to us after being told to have HCV infection on medical checkup done as part of a visa approval process to travel
Key Points: Autoimmune Liver Disease: Update for Pathologists from the Hepatologist s Perspective. Jenny Heathcote, MD. University of Toronto
 Autoimmune Liver Disease: Update for Pathologists from the Hepatologist s Perspective Jenny Heathcote, MD University of Toronto Key Points: AILD comprise autoimmune hepatitis, primary biliary cirrhosis
Autoimmune Liver Disease: Update for Pathologists from the Hepatologist s Perspective Jenny Heathcote, MD University of Toronto Key Points: AILD comprise autoimmune hepatitis, primary biliary cirrhosis
Managing abnormal LFTs in Primary care
 Managing abnormal LFTs in Primary care Summary guideline, April 2015 Sally Hull, Lucy Carter Managing abnormal LFTs in Primary care Draft guideline written by Dr Sally Hull and Dr Lucy Carter at CEG, with
Managing abnormal LFTs in Primary care Summary guideline, April 2015 Sally Hull, Lucy Carter Managing abnormal LFTs in Primary care Draft guideline written by Dr Sally Hull and Dr Lucy Carter at CEG, with
Viral Hepatitis Diagnosis and Management
 Viral Hepatitis Diagnosis and Management CLINICAL BACKGROUND Viral hepatitis is a relatively common disease (25 per 100,000 individuals in the United States) caused by a diverse group of hepatotropic agents
Viral Hepatitis Diagnosis and Management CLINICAL BACKGROUND Viral hepatitis is a relatively common disease (25 per 100,000 individuals in the United States) caused by a diverse group of hepatotropic agents
Not All Patients With Liver Disease Have HCV Diagnosis and Management of Some Common Non HCV Liver Diseases
 Not All Patients With Liver Disease Have HCV Diagnosis and Management of Some Common Non HCV Liver Diseases Prevalence of Chronic Liver Disorders in the United States Nonalcoholic Fatty Liver Disorder
Not All Patients With Liver Disease Have HCV Diagnosis and Management of Some Common Non HCV Liver Diseases Prevalence of Chronic Liver Disorders in the United States Nonalcoholic Fatty Liver Disorder
Monitoring Hepatitis C
 Monitoring Hepatitis C Section Six Monitoring Hepatitis C Screening for hepatitis C is not routinely done, so you may have to request a test from your medical provider. This usually involves an antibody
Monitoring Hepatitis C Section Six Monitoring Hepatitis C Screening for hepatitis C is not routinely done, so you may have to request a test from your medical provider. This usually involves an antibody
Dr Mere Kende. MBBS,Mmed(Path), MAACB, MACTM, MACRRM Lecturer -SMHS
, MAACB, MACTM, MACRRM Lecturer -SMHS") Dr Mere Kende MBBS,Mmed(Path), MAACB, MACTM, MACRRM Lecturer -SMHS Reasons for LFT Classification of Liver Diseases Signs and Symptoms of Liver Disease Routine Liver Tests Jaundice Examples of Liver Diseases
Dr Mere Kende MBBS,Mmed(Path), MAACB, MACTM, MACRRM Lecturer -SMHS Reasons for LFT Classification of Liver Diseases Signs and Symptoms of Liver Disease Routine Liver Tests Jaundice Examples of Liver Diseases
Alpha-1 Antitrypsin Deficiency: Liver Disease
 Alpha-1 Antitrypsin Deficiency: Liver Disease Who is at risk to develop Alpha-1 liver disease? Alpha-1 liver disease may affect children and adults who have abnormal Alpha-1 antitrypsin genes. Keys to
Alpha-1 Antitrypsin Deficiency: Liver Disease Who is at risk to develop Alpha-1 liver disease? Alpha-1 liver disease may affect children and adults who have abnormal Alpha-1 antitrypsin genes. Keys to
Liver Pathology Symposium - medical livers
 Liver Pathology Symposium - medical livers London, April 13 th 2018 Dr Susan E Davies, Addenbrooke s Hospital, Case 1 SED 65/F Diabetic. Raised ALT, USS fatty. Fibroscan? cirrhosis Reticulin (untoned),
Liver Pathology Symposium - medical livers London, April 13 th 2018 Dr Susan E Davies, Addenbrooke s Hospital, Case 1 SED 65/F Diabetic. Raised ALT, USS fatty. Fibroscan? cirrhosis Reticulin (untoned),
LIVER DISORDERS (PRACTICAL MANAGEMENT) Dr Pok Kern (PK) TAN Gastroenterologist Calvary hospital, ACT 1 st April 2017
 Dr Pok Kern (PK) TAN Gastroenterologist Calvary hospital, ACT 1 st April 2017") LIVER DISORDERS (PRACTICAL MANAGEMENT) Dr Pok Kern (PK) TAN Gastroenterologist Calvary hospital, ACT 1 st April 2017 TOPICS TO COVER Acute liver failure Chronic liver failure Portal hypertension : Ascites
LIVER DISORDERS (PRACTICAL MANAGEMENT) Dr Pok Kern (PK) TAN Gastroenterologist Calvary hospital, ACT 1 st April 2017 TOPICS TO COVER Acute liver failure Chronic liver failure Portal hypertension : Ascites
Drug-induced liver injury
 Drug-induced liver injury Vincent Wong MBChB(Hons), MD, FRCP, FHKCP, FHKAM Professor, Department of Medicine and Therapeutics Director, Cheng Suen Man Shook Foundation Centre for Hepatitis Studies Deputy
Drug-induced liver injury Vincent Wong MBChB(Hons), MD, FRCP, FHKCP, FHKAM Professor, Department of Medicine and Therapeutics Director, Cheng Suen Man Shook Foundation Centre for Hepatitis Studies Deputy
JAUNDICE. Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc
 JAUNDICE Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Definition of Jaundice Icterus A yellowish staining of the skin, sclerae and deeper
JAUNDICE Zdeněk Fryšák 3rd Clinic of Internal Medicine Nephrology-Rheumatology-Endocrinology Faculty Hospital Olomouc Definition of Jaundice Icterus A yellowish staining of the skin, sclerae and deeper
Diagnosis and Management of PBC
 Diagnosis and Management of PBC Cynthia Levy, MD, FAASLD University of Miami Miller School of Medicine Miami, Florida 1 Primary Biliary Cholangitis (PBC) Chronic cholestatic liver disease Autoimmune in
Diagnosis and Management of PBC Cynthia Levy, MD, FAASLD University of Miami Miller School of Medicine Miami, Florida 1 Primary Biliary Cholangitis (PBC) Chronic cholestatic liver disease Autoimmune in
NATIONAL LABORATORY HANDBOOK
 NATIONAL LABORATORY HANDBOOK The Abnormal Liver Chemistry Profile Document reference number Document developed by National Clinical Programme for Pathology Revision number Version 1. Document approved
NATIONAL LABORATORY HANDBOOK The Abnormal Liver Chemistry Profile Document reference number Document developed by National Clinical Programme for Pathology Revision number Version 1. Document approved
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Fat, ballooning, plasma cells and a +ANA. Yikes! USCAP 2016 Evening Specialty Conference Cynthia Guy
 Fat, ballooning, plasma cells and a +ANA. Yikes! USCAP 2016 Evening Specialty Conference Cynthia Guy Goals Share an interesting case Important because it highlights a common problem that we re likely to
Fat, ballooning, plasma cells and a +ANA. Yikes! USCAP 2016 Evening Specialty Conference Cynthia Guy Goals Share an interesting case Important because it highlights a common problem that we re likely to
Management of Chronic Hepatitis B in Asian Americans
 Management of Chronic Hepatitis B in Asian Americans Myron J Tong; UCLA, CA Calvin Q. Pan; Mount Sinai, NY Hie-Won Hann; Thomas Jefferson, PA Kris V. Kowdley; Virginia Mason, WA Steven Huy B Han; UCLA,
Management of Chronic Hepatitis B in Asian Americans Myron J Tong; UCLA, CA Calvin Q. Pan; Mount Sinai, NY Hie-Won Hann; Thomas Jefferson, PA Kris V. Kowdley; Virginia Mason, WA Steven Huy B Han; UCLA,
GI DISEASE WORKSHOP CASE STUDIES
 GI DISEASE WORKSHOP CASE STUDIES American Academy of Insurance Medicine Triennial Course in Insurance Medicine 2012 Clifton Titcomb Jr., MD (Hannover Re) James Topic, MD (Protective Life) 1 CASE #1 Application
GI DISEASE WORKSHOP CASE STUDIES American Academy of Insurance Medicine Triennial Course in Insurance Medicine 2012 Clifton Titcomb Jr., MD (Hannover Re) James Topic, MD (Protective Life) 1 CASE #1 Application