Opioids Research to Practice
|
|
|
- Delphia Hamilton
- 6 years ago
- Views:
Transcription



1 Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education (CARE) Unit
2 Case 32 yo female brought in after heroin overdose Brisk response to IV naloxone 0.4 mg Re-sedation after 1 hr requiring repeat naloxone Arm cellulitis at injection drug use site Admitted for drug overdose, persistent altered mental status and arm cellulitis
3 Why is heroin so pleasurable? Heroin is highly lipid soluble Crosses blood brain barrier within 15 seconds= rush After IV administration 68% heroin in brain compared to <5% of morphine Within 30 minutes metabolized to morphine HEROIN is a prodrug of MORPHINE

4 Institute for Defense Analysis and ONDCP
5 Withdrawal Normal Euphoria Natural History of Opioid Use Disorder Acute use Tolerance & Physical Dependence Chronic use

6 Conflicting Priorities...
7 Case continued Substance use history ½ gram of heroin/day Intranasal use for 6 months then IV for 7 years Had been in recovery for 2 years by going to NA but relapsed 3 months ago Denies sharing needles History of 10 detox s, no maintenance treatment No other drug, alcohol or tobacco use HIV and hepatitis C negative Unemployed elementary school teacher Lives with husband (in recovery) and 2 young children Now complaining of opioid withdrawal How will you assess and treat her?
8 Which is NOT a sign of opioid withdrawal? 1. Vomiting 2. Diarrhea 3. Pinpoint pupils 4. Rhinorrhea 5. Lacrimation 6. Piloerection 79% 10% 3% 3% 3% 0%
9 Opioid Withdrawal Assessment Grade Anxiety, Drug Craving Symptoms / Signs Yawning, Sweating, Runny nose, Tearing eyes, Restlessness Insomnia Dilated pupils, Gooseflesh, Muscle twitching & shaking, Muscle & Joint aches, Loss of appetite Nausea, extreme restlessness, elevated blood pressure, Heart rate > 100, Fever Vomiting / dehydration, Diarrhea, Abdominal cramps, Curled-up body position Clinical Opiate Withdrawal Scale (COWS): pulse, sweating, restlessness & anxiety, pupil size, aches, runny nose & tearing, GI sx, tremor, yawning, gooseflesh (score 5-12 mild, mod, mod sev, severe)
10 How is acute opioid withdrawal treated on your inpatient service? 1. Clonidine 2. Methadone 3. Buprenorphine 4. Don t know 5. Other 53% 38% 0% 6% 3%
11 Inpatient Goals Prevent/treat acute opioid withdrawal Inadequate treatment may prevent full treatment of medical/surgical condition Do not expect to cure opioid dependence during this hospital stay Withholding opioids will not cure patient s addiction Giving opioids will not worsen patient s addiction Diagnose and treat medical illness Initiate substance abuse treatment referral
12 Inpatient Goals Methadone or buprenorphine (more expensive) are the best choices! Other Clonidine (hyperadrenergic state) + NSAIDS (muscle cramps and pain) + Benzodiazepines (insomnia) + Dicyclomine (abdominal cramps) + Bismuth subsalicylate (diarrhea)
13 Inpatient Methadone Dosing Guidelines Assess signs and symptoms of acute opioid withdrawal Reassure patient Discuss specific dose and goals openly with patient and nursing staff Don t use heroin : methadone conversions
14 Inpatient Methadone Dosing Guidelines Start with 20 mg of methadone Reassess q 2-3 hours, give additional 5-10 mg until withdrawal signs abate Do not exceed 40 mg in 24 hours Monitor for CNS and respiratory depression
15 Inpatient Methadone Dosing Guidelines On following day, give total dose QD Goal is to alleviate acute withdrawal Patient will continue to crave opioids Discuss taper vs maintained dose w/ pt daily Referral for long-term substance abuse treatment
16 Inpatient Methadone Dosing Guidelines Maintained dose option Give same dose each daily including day of discharge Allows hour withdrawal-free period after d/c Tapered dose option If patient requests a taper, decrease by 5 mg per day and stop taper if patient requests it Don t prolong hospitalization to complete taper Don t give a prescription for methadone
17 Case continued Hospital course Arm Cellulitis treated with IV Vancomycin Opioid withdrawal Day 1 Methadone 20 mg Day 2 Very anxious, demanded increase in methadone dose Was off the floor for 2 hours Repeat urine drug test was positive for opiates
18 All of the following are possible explanations for her opiate positive drug test EXCEPT? 1. Illicit opioid (heroin) use during hospitalization 2. Heroin use prior to admission 3. Hydromorphone (Dilaudid) given for pain last night 4. Methadone given during hospitalization 7% 25% 4% 64%
19
20 Case continued 6 months later She presents to your primary care clinic requesting treatment for her heroin addiction She has been using heroin since the day she left the hospital
21 Case continued Recommended options from primary care Narcotics Anonymous (NA) Clonidine + NSAID + benzodiazepine + Naltrexone (po or injectable) Buprenorphine maintenance (if waivered) Overdose prevention education and naloxone Referral Detoxification program Needle exchange Acupuncture Outpatient counseling Methadone maintenance Buprenorphine maintenance (if not waivered)
22 Opioid Detoxification Outcomes Low rates of retention in treatment High rates of relapse post-treatment < 50% abstinent at 6 months < 15% abstinent at 12 months Increased rates of overdose due to decreased tolerance O Connor PG JAMA 2005 Mattick RP, Hall WD. Lancet 1996 Stimmel B et al. JAMA 1977
23 Reasons for Relapse Protracted abstinence syndrome Secondary to derangement of endogenous opioid receptor system Symptoms Generalized malaise, fatigue, insomnia Poor tolerance to stress and pain Opioid craving Conditioned cues (triggers) Priming with small dose of drug
24 Pharmacotherapy Goals Alleviate physical withdrawal Opioid blockade Alleviate drug craving Normalized deranged brain changes and physiology Some options Naltrexone (opioid antagonist) Methadone (full opioid agonist) Buprenorphine (partial opioid agonist)
25 Withdrawal Normal Euphoria Opioid Agonist Treatment (OAT) Acute use Tolerance & Physical Dependence Chronic use OAT Maintenance
26 Naltrexone Pure opioid antagonist Oral naltrexone Well tolerated, safe Duration of action hours FDA approved 1984 Injectable naltrexone (Vivitrol ) IM injection (w/ customized needle) once/month FDA approved 2010 Patients must be opioid free for a minimum of 7-10 days before treatment
27 Oral Naltrexone 10 RCTs ~700 participants to naltrexone alone or with psychosocial therapy compared with psychosocial therapy alone or placebo No clear benefit in treatment retention or relapse at follow up Benefit in highly motivated patients Impaired physicians > 80% abstinence at 18 months Cochrane Database of Systematic Reviews 2006
28 Injectable Naltrexone (XR-NTX) Multicenter (13 sites in Russia) Funded by Alkermes DB RPCT, 24 wks, n=250 w/ opioid dependence XR-NTX vs placebo, all offered biweekly individual drug counseling Weeks of confirmed abstinence (90% vs 35%) Patients with confirmed abstinence (36% vs 23%) Craving (-10 vs +0.7) Krupitsky E, et al. Lancet, 2011
29 Methadone Hydrochloride Full opioid agonist PO onset of action minutes Duration of action hours to treat opioid addiction 6-8 hours to treat pain Proper dosing for opioid addiction mg for acute withdrawal > 80 mg for craving, opioid blockade


30 Methadone Maintenance Over 45 Years of Experience JAMA 1965 JAMA 2005
31 Methadone Maintenance Dosing
32 Ball JC, Ross A. The effectiveness of methadone maintenance treatment, 1991
33 Effects of Psychosocial Services McLellan, AT et.al, J AMA 1993
34 What is the single best question to assess a patient s success on methadone maintenance treatment? 1. Are you using drugs? 2. Are you on take home doses? 3. Are you compliant with methadone treatment? 4. How long have you been on methadone treatment? 6% 39% 6% 48%
35 Methadone Maintenance Treatment Highly Structured Daily nursing assessment Weekly individual and/or group counseling Random supervised drug testing Psychiatric services Medical services Methadone dosing Observed daily Take homes
36 In a Comprehensive Rehabilitation Program Increases overall survival Increases treatment retention Decreases illicit opioid use Decreases hepatitis and HIV seroconversion Decreases criminal activity Increases employment Improves birth outcomes
37 Methadone Maintenance Limitations Highly regulated - Narcotic Addict Treatment Act 1974 Created methadone clinics (Opioid Treatment Programs) Separate system not involving primary care or pharmacists Limited access Inconvenient and highly punitive Mixes stable and unstable patients Lack of privacy No ability to graduate from program Stigma

38 Methadone Maintenance Still controversial I don t believe in methadone substituting one drug for another liquid handcuffs
39 DATA 2000 and Buprenorphine 2000: Drug Addiction Treatment Act (DATA) 2000 Allows qualified physician to prescribe scheduled III - V, narcotic FDA approved for opioid maintenance or detoxification treatment limit 30 patients per practice 2002: Suboxone and Subutex FDA approved 2005: Limit to 30 patients per physician 2007: Limit to 100 patients per physician after 1 year
40 Physician Qualifications The physician is licensed under State law and qualified based on one of the following: Certified in Addiction Psychiatry or Medicine Completed eight hours of training List of trainings: Online training:
41 Buprenorphine Buprenorphine (Subutex or generic) mono Buprenorphine + naloxone (Suboxone) combo Schedule III Sublingual tablets, film Treatment of opioid dependence High receptor affinity Slow dissociation Ceiling effect for respiratory depression






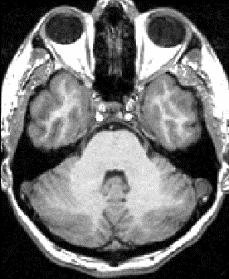

42 Opioid Blockade MRI Bup 00 mg Binding Potential (Bmax/Kd) Bup 02 mg 4 - Bup 16 mg 0 - Bup 32 mg

43 Buprenorphine Maintenance vs Taper Results: Completed 52 wk trial taper 0% maintenance 75% Mean % urine neg maintenance 75% Mortality Taper 20% Kakko J et al. Lancet 2003
44 Buprenorphine Efficacy Studies (RCT) show buprenorphine more effective than placebo and equally effective to moderate doses (80 mg) of methadone on primary outcomes of: Abstinence from illicit opioid use Retention in treatment Decreased opioid craving Johnson et al. NEJM 2000 Fudala PJ et al. NEJM 2003 Kakko J et al. Lancet 2003
45 Methadone vs Buprenorphine 9 OTPs n=1,267 RCT buprenorphine vs methadone 6 month retention Hser Y, et al. Addiction. 2014

46 Patients with OUD Receiving Medications Source: IMS Total Patient Tracker, Sep Buprenorphine data exclude forms indicated for pain. Oral naltrexone factored for opioid dependence use only (40% factor provided by Alkermes). Methadone patients, N-SSATS

47 OUD Treatment Gap: million * Number of individuals receiving buprenorphine or naltrexone from IMS plus number of patients receiving methadone from NSSATS. Source: IMS Total Patient Tracker, Sept 2014 and SAMHSA NSSATS. Buprenorphine data exclude forms indicated for pain. Oral naltrexone factored for opioid dependence use. Methadone patients from SAMHSA, N-SSATS 2012.
48 Opioid Maintenance Treatment and Acute Pain Management Patients on opioid maintenance treatment (i.e. methadone or buprenorphine) have less pain tolerance then matched controls Patients who are physically dependent on opioids (i.e. methadone or buprenorphine) must be maintained on daily equivalence before ANY analgesic effect is realized with opioids used for acute pain management Opioid analgesic requirements are often higher due to increased pain sensitivity and opioid cross tolerance Alford DP, Compton P, Samet JH. Ann Intern Med 2006
Opioids Research to Practice
 Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids. October 29, Addiction Medicine Review Course CSAM, Newport Beach, CA
 Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone
 Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone Alexander Y. Walley, MD, MSc Associate Professor of Medicine Director, Addiction Medicine Fellowship Boston University
Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone Alexander Y. Walley, MD, MSc Associate Professor of Medicine Director, Addiction Medicine Fellowship Boston University
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They?
 Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Buprenorphine as a Treatment Option for Opioid Use Disorder
 Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
SW OREGON OPIOID SUMMIT. Medication Assisted Recovery for Opioid Use Disorder. Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass
 SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Medication Assisted Treatment. MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment
 Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Buprenorphine for Family Medicine. Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17
 + Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
+ Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
Opioid Agonists. Natural derivatives of opium poppy - Opium - Morphine - Codeine
 Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services
 Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services www.randallwebber.com MAT clients are still addicted Truth: MAT clients will experience withdrawal symptoms if they stop
Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services www.randallwebber.com MAT clients are still addicted Truth: MAT clients will experience withdrawal symptoms if they stop
Medications for Opioid Use Disorder. Charles Brackett, MD, MPH General Internal Medicine, DHMC
 Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Opioid dependence and buprenorphine treatment
 Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Medication Treatment and Opioid Use Disorder
 Medication Treatment and Opioid Use Disorder Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBOT-B Boston Medical Center Disclosures I have no disclosures
Medication Treatment and Opioid Use Disorder Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBOT-B Boston Medical Center Disclosures I have no disclosures
Responding to the Opioid Epidemic
 Responding to the Opioid Epidemic Jessica Gray, MD Addiction Medicine Fellow Boston Medical Center ROME New England August 17, 2017 Disclosures for Jessica Gray, MD No conflicts Learning Objectives Describe
Responding to the Opioid Epidemic Jessica Gray, MD Addiction Medicine Fellow Boston Medical Center ROME New England August 17, 2017 Disclosures for Jessica Gray, MD No conflicts Learning Objectives Describe
6/6/2018. Objectives. Outline. Rethinking Medication Treatment for Opioid Use Disorder
 Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
Module II Opioids 101 Opiate Opioid
 BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module II Opioids 101 Module II Goals of the Module This module reviews the following:! Opioid addiction and the brain!
BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module II Opioids 101 Module II Goals of the Module This module reviews the following:! Opioid addiction and the brain!
Opioid Use Disorders as a Brain Disease Why MAT is so important. Ron Jackson, M.S.W., L.I.C.S.W.
 Opioid Use Disorders as a Brain Disease Why MAT is so important Ron Jackson, M.S.W., L.I.C.S.W. Affiliate Professor School of Social Work University of Washington Organization Name: CareOregon Course Title:
Opioid Use Disorders as a Brain Disease Why MAT is so important Ron Jackson, M.S.W., L.I.C.S.W. Affiliate Professor School of Social Work University of Washington Organization Name: CareOregon Course Title:
Opioid Dependence and Buprenorphine Management
 Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
ROSC & MAT II: Opioid Treatment Services
 ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
NALTREXONE DAVID CRABTREE, MD, MPH UNIVERSITY OF UTAH HEALTH, 2018
 NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
Opioid dependence: Detoxification
 Opioid dependence: Detoxification What is detoxification? A. Process of removal of toxins from the body? B. Admitting a drug dependent person in a hospital and giving him nutrition? C. Stopping drug use
Opioid dependence: Detoxification What is detoxification? A. Process of removal of toxins from the body? B. Admitting a drug dependent person in a hospital and giving him nutrition? C. Stopping drug use
Buprenorphine: An Introduction. Sharon Stancliff, MD Harm Reduction Coalition September 2008
 Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Medication-Assisted Treatment (MAT) Overview
 Overview") Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Disclosures. I have no disclosures or commercial interests to report
 Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center Disclosures I have no disclosures or commercial interests to report Medication-Assisted
Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center Disclosures I have no disclosures or commercial interests to report Medication-Assisted
Disclosure Statement. Learning Objectives. American Psychiatric Nurses Association. Christian J. Teter, PharmD, BCPP 1 BUPRENORPHINE UPDATE
 BUPRENORPHINE UPDATE Christian J. Teter, Pharm.D., BCPP Associate Professor, Psychopharmacology College Of Pharmacy, University Of New England Portland, ME E-Mail: cteter@une.edu Image Source: pubchem.ncbi.nlm.nih.gov
BUPRENORPHINE UPDATE Christian J. Teter, Pharm.D., BCPP Associate Professor, Psychopharmacology College Of Pharmacy, University Of New England Portland, ME E-Mail: cteter@une.edu Image Source: pubchem.ncbi.nlm.nih.gov
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines
 The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
Medical Assisted Treatment of Opioid
 Medical Assisted Treatment of Opioid Dependence with XR-NTX(Vivitrol) Michael McNamara DO, FACN Medical Director Mental Health Center of Greater Manchester Manchester NH Outline Overview of Opioid Dependence
Medical Assisted Treatment of Opioid Dependence with XR-NTX(Vivitrol) Michael McNamara DO, FACN Medical Director Mental Health Center of Greater Manchester Manchester NH Outline Overview of Opioid Dependence
Treating Opioid Use Disorders: An Update for Counselors and Other Providers
 Treating Opioid Use Disorders: An Update for Counselors and Other Providers Brad Shapiro, MD Medical Director Opiate Treatment Outpatient Program Zuckerberg San Francisco General THE DOSING WINDOW HISTORICAL
Treating Opioid Use Disorders: An Update for Counselors and Other Providers Brad Shapiro, MD Medical Director Opiate Treatment Outpatient Program Zuckerberg San Francisco General THE DOSING WINDOW HISTORICAL
Medication Assisted Treatment:
 Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Arwen Podesta, MD. ABIHM, ABAM, Forensic Psychiatry
 The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
Initiation of Medication in Treating Opioid Use Disorder.
 Initiation of Medication in Treating Opioid Use Disorder. Colleen T. LaBelle MSN RN-BC CARN Program Director STATE OBAT B Nurse Manager Boston Medical Center OBAT Executive Director MA IntNSA *Images used
Initiation of Medication in Treating Opioid Use Disorder. Colleen T. LaBelle MSN RN-BC CARN Program Director STATE OBAT B Nurse Manager Boston Medical Center OBAT Executive Director MA IntNSA *Images used
Pharmacotherapy for opioid addiction. Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco
 Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Virginia Opioid Addiction ECHO*
 Virginia Opioid Addiction ECHO* Project ECHO: July 27th *ECHO: Extension of Community Healthcare Outcomes Agenda Agenda Agenda Introductions Clinical Director Administrative Medical Director ECHO Hubs
Virginia Opioid Addiction ECHO* Project ECHO: July 27th *ECHO: Extension of Community Healthcare Outcomes Agenda Agenda Agenda Introductions Clinical Director Administrative Medical Director ECHO Hubs
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE
 LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
MAT - ICAAD 2018 Ron Jackson, MSW, LICSW
 The ATTC Network Ten Regional Centers northwest@attcnetwork.org www.attcnetwork.org/northwest phone. 206-685-4419 1107 NE 45 th St, Ste 120, Seattle, WA 98105 http://attcnetwork.org/northwest U.S. Opioid
The ATTC Network Ten Regional Centers northwest@attcnetwork.org www.attcnetwork.org/northwest phone. 206-685-4419 1107 NE 45 th St, Ste 120, Seattle, WA 98105 http://attcnetwork.org/northwest U.S. Opioid
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations
 Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Management of Opioid Use Disorder in Primary Care
 1 Northwest ATTC presents Management of Opioid Use Disorder in Primary Care Joseph O. Merrill, MD, MPH University of Washington Associate Professor of Medicine 4/26/2018 Today s Presenter 2 Joseph Merrill,
1 Northwest ATTC presents Management of Opioid Use Disorder in Primary Care Joseph O. Merrill, MD, MPH University of Washington Associate Professor of Medicine 4/26/2018 Today s Presenter 2 Joseph Merrill,
Serious Mental Illness and Opioid Use Disorder
 Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Medication Assisted Treatment. Nicole Gastala, MD
 Medication Assisted Treatment Nicole Gastala, MD Objectives Training Goals: To enhance the understanding of the participants in use of medication assisted therapy To increase the knowledge of participants
Medication Assisted Treatment Nicole Gastala, MD Objectives Training Goals: To enhance the understanding of the participants in use of medication assisted therapy To increase the knowledge of participants
Understanding and Combating the Heroin Epidemic
 Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
GOALS AND OBJECTIVES
 SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
Managing Pain in the Patient with Opioid Use Disorder: Inpatient Management. Melissa Weimer, DO, MCR Oregon Health & Science University
 Managing Pain in the Patient with Opioid Use Disorder: Inpatient Management Melissa Weimer, DO, MCR Oregon Health & Science University 1 Educational Objectives At the conclusion of this activity participants
Managing Pain in the Patient with Opioid Use Disorder: Inpatient Management Melissa Weimer, DO, MCR Oregon Health & Science University 1 Educational Objectives At the conclusion of this activity participants
Methadone and Naltrexone ER
 Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Building capacity for a CHC response to Ontario's Opioid Crisis
 Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
THE MEDICAL MODEL: ADDICTION IS A BRAIN DISEASE. Judith Martin, MD Medical Director of Substance Use Services San Francisco Dept.
 THE MEDICAL MODEL: ADDICTION IS A BRAIN DISEASE Judith Martin, MD Medical Director of Substance Use Services San Francisco Dept. Public Health disclosures Dr. Martin has no conflict of interest to disclose.
THE MEDICAL MODEL: ADDICTION IS A BRAIN DISEASE Judith Martin, MD Medical Director of Substance Use Services San Francisco Dept. Public Health disclosures Dr. Martin has no conflict of interest to disclose.
Naltrexone Overview. Todd Korthuis, MD, MPH ECHO-MAT Conference November 7, 2017
 Naltrexone Overview Todd Korthuis, MD, MPH ECHO-MAT Conference November 7, 2017 Disclosure Information Speaker/Planner: Todd Korthuis, MD, has nothing to disclose. 2 Pharmacotherapy for Opioid Use Disorder
Naltrexone Overview Todd Korthuis, MD, MPH ECHO-MAT Conference November 7, 2017 Disclosure Information Speaker/Planner: Todd Korthuis, MD, has nothing to disclose. 2 Pharmacotherapy for Opioid Use Disorder
Opioid Replacement Therapy
 Opioid Replacement Therapy Matthew A. Felgus, MD mafelgus@wisc.edu 6333 Odana Rd, Suite 3, Madison, WI 53719 (608) 257-1581 Board Certified in Addiction Medicine Board Certified in Psychiatry matthewfelgusmd.com
Opioid Replacement Therapy Matthew A. Felgus, MD mafelgus@wisc.edu 6333 Odana Rd, Suite 3, Madison, WI 53719 (608) 257-1581 Board Certified in Addiction Medicine Board Certified in Psychiatry matthewfelgusmd.com
Health Systems and Addiction: Provider Issues
 Health Systems and Addiction: Provider Issues The Emerging Roles of Primary Care Patrick G. O Connor MD, MPH Dan and Amanda Adams Professor of General Medicine Chief, General Internal Medicine Yale University
Health Systems and Addiction: Provider Issues The Emerging Roles of Primary Care Patrick G. O Connor MD, MPH Dan and Amanda Adams Professor of General Medicine Chief, General Internal Medicine Yale University
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT
 and acute pain management on MAT") An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
What Is Heroin? Examples of Opioids. What Science Says about Opioid Use Disorder and Its Treatment 6/27/2016
 What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
DISCLOSURES MANAGEMENT OF OPIOID USE DISORDERS LECTURE COVERS. SUDs ARE IMPORTANT. I have nothing to declare
 MANAGEMENT OF OPIOID USE DISORDERS DISCLOSURES Marc A Schuckit Distinguished Professor of Psychiatry, UCSD Medical School I have nothing to declare SUDs ARE IMPORTANT Affect > 20% of your patients Are
MANAGEMENT OF OPIOID USE DISORDERS DISCLOSURES Marc A Schuckit Distinguished Professor of Psychiatry, UCSD Medical School I have nothing to declare SUDs ARE IMPORTANT Affect > 20% of your patients Are
Medication Assisted Treatment. Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs
 Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
MAT 101: TREATMENT OF OPIOID USE DISORDER
 MAT 101: TREATMENT OF OPIOID USE DISORDER WITH SPECIAL EMPHASIS ON BUPRENORPHINE/NALOXONE ICADD May 22, 2018 Alicia Carrasco, MD Debby Woodall, LCSW, ACADC Magni Hamso, MD, MPH Terry Reilly Health Services
MAT 101: TREATMENT OF OPIOID USE DISORDER WITH SPECIAL EMPHASIS ON BUPRENORPHINE/NALOXONE ICADD May 22, 2018 Alicia Carrasco, MD Debby Woodall, LCSW, ACADC Magni Hamso, MD, MPH Terry Reilly Health Services
Naltrexone Overview. Todd Korthuis, MD, MPH ECHO-MAT Conference February 14, 2017
 Naltrexone Overview Todd Korthuis, MD, MPH ECHO-MAT Conference February 14, 2017 Pharmacotherapy for Opioid Use Disorder % Mu Receptor Intrinsic Activity 100 90 80 Full Agonist: Methadone ( How High )
Naltrexone Overview Todd Korthuis, MD, MPH ECHO-MAT Conference February 14, 2017 Pharmacotherapy for Opioid Use Disorder % Mu Receptor Intrinsic Activity 100 90 80 Full Agonist: Methadone ( How High )
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Rates of Opioid Overdose Deaths, Sales, and Treatment Admissions: US,
 Rates of Opioid Overdose Deaths, Sales, and Treatment Admissions: US, 1999 21 8 Rates of Prescription Painkiller Sales, Deaths, and Substance Abuse Treatment Admissions (1999 21) 7 Rate 6 5 4 3 Sales per
Rates of Opioid Overdose Deaths, Sales, and Treatment Admissions: US, 1999 21 8 Rates of Prescription Painkiller Sales, Deaths, and Substance Abuse Treatment Admissions (1999 21) 7 Rate 6 5 4 3 Sales per
MANAGING OPIOID WITHDRAWAL AND OPIOID USE DISORDER (OUD)
") MANAGING OPIOID WITHDRAWAL AND OPIOID USE DISORDER (OUD) Michelle Meyer, PharmD, BCPS, BCNSP Andrea Wetshtein, PharmD, BCPS,CPE OhioHealth Grant Medical Center OBJECTIVES Pharmacist Learning Objectives
MANAGING OPIOID WITHDRAWAL AND OPIOID USE DISORDER (OUD) Michelle Meyer, PharmD, BCPS, BCNSP Andrea Wetshtein, PharmD, BCPS,CPE OhioHealth Grant Medical Center OBJECTIVES Pharmacist Learning Objectives
Latest Research on Addiction and Treatment
 Latest Research on Addiction and Treatment Joshua D Lee MD MSc joshua.lee@nyumc.org / @DrJoshuaDLee Associate Professor NYU School of Medicine, Department of Population Health Disclosures, LeeJD Grants:
Latest Research on Addiction and Treatment Joshua D Lee MD MSc joshua.lee@nyumc.org / @DrJoshuaDLee Associate Professor NYU School of Medicine, Department of Population Health Disclosures, LeeJD Grants:
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets. Risk Evaluation and Mitigation Strategy (REMS) Program
 Program") SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
Opioid Treatment in North Carolina SEPTEMBER 13, 2016
 Opioid Treatment in North Carolina SEPTEMBER 13, 2016 Source Where Pain Relievers Were Obtained for Most Recent Nonmedical Use among Past Year Users Aged 12 or Older: 2007 Source Where Respondent Obtained
Opioid Treatment in North Carolina SEPTEMBER 13, 2016 Source Where Pain Relievers Were Obtained for Most Recent Nonmedical Use among Past Year Users Aged 12 or Older: 2007 Source Where Respondent Obtained
Methadone Maintenance Treatment for the Opioid Dependent Patient
 Methadone Maintenance Treatment for the Opioid Dependent Patient Janice F. Kauffman RN, MPH, CAS, LADC1 Assistant Professor of Psychiatry, Harvard Medical School V. P., Addiction Treatment Services, North
Methadone Maintenance Treatment for the Opioid Dependent Patient Janice F. Kauffman RN, MPH, CAS, LADC1 Assistant Professor of Psychiatry, Harvard Medical School V. P., Addiction Treatment Services, North
Vivitrol Drug Court and Medication Assisted Treatment
 Vivitrol Drug Court and Medication Assisted Treatment Amy Black, CNP and Judge Fred Moses Court program Self-starters Mission Statement To provide court-managed, medically assisted drug intervention treatment
Vivitrol Drug Court and Medication Assisted Treatment Amy Black, CNP and Judge Fred Moses Court program Self-starters Mission Statement To provide court-managed, medically assisted drug intervention treatment
Medication Assisted Treatment. Michael Palladini, RPh MBA CAC
 Medication Assisted Treatment Michael Palladini, RPh MBA CAC palladini.michael@gmail.com History of MAT Addiction as a Disease The concept of addiction as a disease of the brain challenges deeply ingrained
Medication Assisted Treatment Michael Palladini, RPh MBA CAC palladini.michael@gmail.com History of MAT Addiction as a Disease The concept of addiction as a disease of the brain challenges deeply ingrained
9/13/2017. Buprenorphine Treatment (Suboxone) Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare
 Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare") Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Opioid Use Disorders &Medication Treatment
 Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Arizona s Opioid Epidemic
 Arizona s Opioid Epidemic Rise in Heroin Addiction and the Dangers of Fentanyl Sara Salek, MD Chief Medical Officer Shana Malone, MS Clinical Initiatives Project Manager 1 Disclosures None The National
Arizona s Opioid Epidemic Rise in Heroin Addiction and the Dangers of Fentanyl Sara Salek, MD Chief Medical Officer Shana Malone, MS Clinical Initiatives Project Manager 1 Disclosures None The National
Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center
 Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center Disclosures I have no disclosures or commercial interests to report Addiction
Colleen T. LaBelle, MSN, RN-BC,CARN Program Director, Office-Based Addiction Treatment Director, STATE OBAT Boston Medical Center Disclosures I have no disclosures or commercial interests to report Addiction
Opioid Overdose Epidemic A Crises and Opportunity
 Opioid Overdose Epidemic A Crises and Opportunity Samuel M. Silverman MD, FAPA, DFASAM Assistant Clinical Professor, UConn Medical School Director, Medical Education Rushford, A Hartford HealthCare Partner
Opioid Overdose Epidemic A Crises and Opportunity Samuel M. Silverman MD, FAPA, DFASAM Assistant Clinical Professor, UConn Medical School Director, Medical Education Rushford, A Hartford HealthCare Partner
Disclosures. Topics of today s training 4/24/2017. Evolving Treads in Medication Assisted Treatment. Christopher J Davis D.O.
 Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
MEDICATION ASSISTED TREATMENT
 MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
Naltrexone for Opioid Use Disorder. A Project RAMP Resource Adam J. Gordon, MD MPH FACP DFASAM CMRO December 2017
 Naltrexone for Opioid Use Disorder A Project RAMP Resource Adam J. Gordon, MD MPH FACP DFASAM CMRO December 2017 LEARNING OBJECTIVES Be able to inform patients regarding the use and latest literature of
Naltrexone for Opioid Use Disorder A Project RAMP Resource Adam J. Gordon, MD MPH FACP DFASAM CMRO December 2017 LEARNING OBJECTIVES Be able to inform patients regarding the use and latest literature of
OPIOID USE DISORDER AND THE PSYCHIATRIC EMERGENCY ROOM THE VA CT MODEL
 OPIOID USE DISORDER AND THE PSYCHIATRIC EMERGENCY ROOM THE VA CT MODEL Brian Fuehrlein, MD PhD VA Connecticut Healthcare System and Yale University I have no conflicts of interest or relevant financial
OPIOID USE DISORDER AND THE PSYCHIATRIC EMERGENCY ROOM THE VA CT MODEL Brian Fuehrlein, MD PhD VA Connecticut Healthcare System and Yale University I have no conflicts of interest or relevant financial
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
FY17 SCOPE OF WORK TEMPLATE. Name of Program/Services: Medication-Assisted Treatment: Buprenorphine
 FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
Opioid Initiative Wave I Treating Opioid-Use Disorder in the ED Part 1
 Opioid Initiative Wave I Treating Opioid-Use Disorder in the ED Part 1 Presenter Eric Ketcham, MD, MBA Reuben J. Strayer, MD emergency department management of the patient with opioid withdrawal OD is
Opioid Initiative Wave I Treating Opioid-Use Disorder in the ED Part 1 Presenter Eric Ketcham, MD, MBA Reuben J. Strayer, MD emergency department management of the patient with opioid withdrawal OD is
Opioid Use in Youth. Amy Yule M.D. March 2,
 Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
Prescription Opioid Addiction
 CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
Addiction to Opioids. Marvin D. Seppala, MD Chief Medical Officer
 Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
Buprenorphine pharmacology
 Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates
 and Medication Assisted Treatment (MAT) for Opiates") Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
MAT in the Corrections Setting
 MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
Extended-Release Naltrexone for Opioid Relapse Prevention
 Extended-Release Naltrexone for Opioid Relapse Prevention 1.NYU SOM; Bellevue Hospital Center 2.Brown Univ. 3. Friends Research Institute 4. Columbia Univ. 5. Univ. Pennsylvania 6. Univ. Virginia Funding:
Extended-Release Naltrexone for Opioid Relapse Prevention 1.NYU SOM; Bellevue Hospital Center 2.Brown Univ. 3. Friends Research Institute 4. Columbia Univ. 5. Univ. Pennsylvania 6. Univ. Virginia Funding:
8/28/2017. Headlines. How Did We Get Here? Pain is the number one reason patients go the doctors office, urgent care and/or emergency room.
 Ashel Kruetzkamp, MSN, RN, SANE Headlines How Did We Get Here? Pain is the number one reason patients go the doctors office, urgent care and/or emergency room. Opiates are the most effective pain medication
Ashel Kruetzkamp, MSN, RN, SANE Headlines How Did We Get Here? Pain is the number one reason patients go the doctors office, urgent care and/or emergency room. Opiates are the most effective pain medication
THE STATE OF MEDICINE IN ADDICTION RECOVERY
 OVERVIEW: Review addiction stats and trends Define addiction Explain neurobiology of addiction Review treatments of addiction Addiction Definition: A Primary, chronic, relapsing disease of brain reward,
OVERVIEW: Review addiction stats and trends Define addiction Explain neurobiology of addiction Review treatments of addiction Addiction Definition: A Primary, chronic, relapsing disease of brain reward,
Long term treatment for opioid dependence Antagonist therapy
 Long term treatment for opioid dependence Antagonist therapy Treatment of Opioid Dependence Antagonist treatment Naltrexone Naltrexone (NTX) synthesized in 1965 Eliminate drug carving and prevent relapse
Long term treatment for opioid dependence Antagonist therapy Treatment of Opioid Dependence Antagonist treatment Naltrexone Naltrexone (NTX) synthesized in 1965 Eliminate drug carving and prevent relapse
Opioid Step Policy. Description. Section: Prescription Drugs Effective Date: April 1, 2018
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Opioid Step Policy Page: 1 of 6 Last Review Date: March 16, 2018 Opioid Step Policy Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Opioid Step Policy Page: 1 of 6 Last Review Date: March 16, 2018 Opioid Step Policy Description
Medication Assisted Treatment
 Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
In 2008, an estimated 282,000 persons
 National Survey of Substance Abuse Treatment Services The N-SSATS Report January 28, 2010 Similarities and Differences in Opioid Treatment Programs that Provide Methadone Maintenance or Buprenorphine Maintenance
National Survey of Substance Abuse Treatment Services The N-SSATS Report January 28, 2010 Similarities and Differences in Opioid Treatment Programs that Provide Methadone Maintenance or Buprenorphine Maintenance
Rationale & Strategy For Integrating Buprenorphine Treatment Into Community Health Centers
 Rationale & Strategy For Integrating Buprenorphine Treatment Into Community Health Centers Marwan S. Haddad, M.D. Community Health Center, Inc. Connecticut September 16, 2008 Community Health Center, Inc.
Rationale & Strategy For Integrating Buprenorphine Treatment Into Community Health Centers Marwan S. Haddad, M.D. Community Health Center, Inc. Connecticut September 16, 2008 Community Health Center, Inc.
2/21/2018. What are Opioids?
 Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
OPIOID REPLACEMANT THERAPY: AN OVERVIEW
 OPIOID REPLACEMANT THERAPY: AN OVERVIEW Matthew Felgus MD FASAM Matthew A Felgus, MD, FASAM mafelgus@wisc.edu matthewfelgusmd.com 6333 Odana Rd, Ste 3, Madison WI 53719 (608) 257-1581 Board Certified in
OPIOID REPLACEMANT THERAPY: AN OVERVIEW Matthew Felgus MD FASAM Matthew A Felgus, MD, FASAM mafelgus@wisc.edu matthewfelgusmd.com 6333 Odana Rd, Ste 3, Madison WI 53719 (608) 257-1581 Board Certified in