The Difficult Patient: Risk Mitigation Strategies
|
|
|
- Alice Lamb
- 6 years ago
- Views:
Transcription
1 The Difficult Patient: Risk Mitigation Strategies C. Scott Anthony, D.O. Pain Management of Tulsa 1
2 Opioid Backlash National emergency Opioids not indicated for chronic pain Forces pushing for reduction of opioid use CDC guidelines and the fallout Recent FDA actions White House and congressional actions 2
3 The Perfect Storm Press to manage pain better Federal changes to better address pain Linking pain to outcome scores The fifth vital sign Introduction of extended release opioids Proliferation of pain management Internet reviews 3
4 CDC Guidelines Released March 2016 Opioid overdoses and deaths Emphasis on high dose opioids First governmental guidelines Voluntary Reducing opioid consumption Access to treatment 4
5 Fallout From CDC Guidelines National press response Doctor driven Physician fear of prescribing Patient fears of decreased access Will it become mandatory How will payors respond May mirror the ODG effect on workers compensation 5
6 Contributing Factors to Inadequate Treatment and Prescribing Physician lack of knowledge in best clinical practice Inadequate research Poor understanding of risk mitigation Poor utilization of PMP and UDS Conflicting clinical guidelines Physician misunderstanding of dependence/addiction Complete relief may not be an attainable goal 6
7 National Center on Addiction and Substance Abuse 15.2 million abuse prescription drugs (2.5 X increase in 10 years) 20% of patients obtaining opioids for chronic pain abuse the medication 10-20% of these patients abuse illicit drugs Increased prescribing of opioids linked to misuse, abuse and deaths Absolute link between increased prescribing and availability for abuse 7
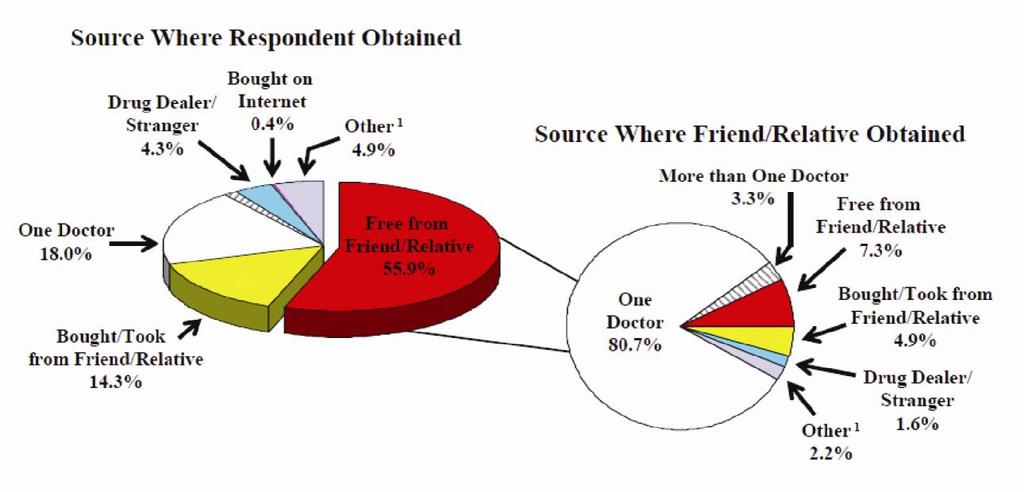
8 Epidemic of Medical Prescription Drug Abuse Supply Explosion in the use of prescription opioids in response to the under treatment of pain Retail grams of opioids sold show significant increase Number of prescriptions for controlled substances nearly doubled in last 10 years Since 2004 risk has escalated without increased evidence of benefit Sources of opioids Number one source is from family and friends The medicine cabinet is our greatest threat 8
9 Opioid Deaths Major reason for CDC involvement Significant escalation Diversion: most deaths are from non-prescribed opioids Lethal combinations especially with benzodiazepines Good data to support dose linked relationship Without question the number one reason for governmental intrusion 9
10 CDC Emphasis Directed at primary care physicians Opioids not recommended for routine use Does not include end of life, cancer pain and palliative pain care Management of pain is a multidisciplinary problem requiring numerous modalities to address physical and psychosocial aspects 10
11 Opioid Prescribing Chronic pain is complex Opioids alone are typically inadequate 25-50% improvement in pain scales Opioids are beneficial in small subset of patients Many patients would do well with discontinuation or reduction of opioids and pursue adjunctive therapies with psychological support No universal efficacy with opioids 11
12 CDC Emphasis: First Line Approach Non-pharmacological approach Non-opioid approach Emphasis on Behavioral therapies Functional therapies Adjunctive medications Patient and provider expectation Opioids are a last resort option 12
13 Are Opioids Efficacious for Chronic Pain? Evidence is scant CDC insights Opioid use may be the most important factor impeding recovery of function Opioids do not consistently and reliably relieve pain and can decrease quality of life The routine use of opioids cannot be recommended Appropriate only for selected patients with moderate-severe pain that significantly affects quality of life 13
14 Patient Selection and Risk Stratification History, physical examination and diagnostic testing Psychosocial risk assessment Expectations: physician and patient Risk assessment is an underdeveloped skill for most clinicians COT should be viewed as a treatment of last resort Consider all other modalities prior to initiation Use opioids in addition to a multidisciplinary approach to pain 14
15 Chronic Opioid Therapy (COT) Consensus agreement that it is may be useful in carefully selected patients with severe pain Demands Compliant patient Documentation Close monitoring through follow up Vigilant monitoring for abuse and diversion Assessment of opioid related side effects Understanding of opioid use in chronic pain 15
16 Chronic Opioid Therapy Informed consent and discussion of risk vs. benefit Therapeutic trial of 4-6 weeks Exhaustion of other modalities Insufficient data on starting dose Start low go slow Conversion tables Ongoing monitoring and assessment of benefit vs. risk, expectations and alternative modalities Consider a taper or wean even in functional patients 16
17 Success Compliant patient who understands the concept of the therapy and importance of close observation Rare dose increases Often dose decreases Honest and straightforward when problems arise ADL s improve Understands the goal of therapy Realistic expectations 17
18 Drug Seeking? Even a skilled physician can be duped Common scenarios patient request for opioids or opioid increase Progression of disease New painful diagnosis Psychological issues Poor understanding of pain Failure to use adjunctives or other therapies Abuse or diversion 18
19 Difficulties: Why? Patient selection Pain syndrome Expectations High dose opioid therapy Opioid Use Disorder Opioid induced hyperalgesia Reliance only on opioids Abuse and diversion 19
20 Expectations Patient and physician usually have a different view Perhaps the best way to avoid problems Explain: Your expectations Listen to the patients expectations Come to a middle ground of understanding Develop a trust Explain the rationale for your decision Have available a print out of the CDC guidelines 20
21 Common Difficulties Benzodiazepine and other sedatives Previous non-fatal overdose Oxygen dependency Sleep apnea Renal or hepatic disease Age >65 Be sure and document the rationale for opioid use 21
22 Patients at Risk Psychosocial issues History of addiction Risk of relapse, harm and treatment failure Adverse Childhood Experience (ACE) Abuse, neglect, household dysfunction and traumatic stressors Poor motivation and lack of insight Disability, Medicaid and even prior criminal activity Unrealistic expectations 22
23 Opioid Use Disorder Significant impairment or distress Inability to reduce opioids Inability to control use Decreased function Social function reduced Failure to fulfill work, home or school obligations Commonly referred to as abuse in the literature 23
24 Risk Factors for OUD Younger age Previous substance abuse Back pain, headache and non-specific pain Co-existing depression and anxiety Greater than 90 MED s a day 24
25 CDC Emphasis: IR vs. ER/LA opioid therapies Little mention of abuse deterrent medications Benzodiazepine use with opioids Significant increase in deaths and ER visits Acute pain leading to chronic therapy Methadone Offering naloxone to patients at risk High dose opioids 25
26 Morphine Equivalent Doses MED s are the major topic of most consensus statements and a focus of research Generally 120mg but growing support for less Very good data supports risks with MED of greater than mg Increased rates of side effects, poor function and death Must be a point of pause for physicians and requires EXTREME caution 26
27 High Dose Opioid Therapy Data is proving more reliable Defined as mg morphine or equivalent a day Continues to decline Opioid rotation vs. weaning? Opioid rotation linked to increased death Strong evidence linked with poor outcome 9x increase in deaths with 100mg or higher MED Remember, existence of persisting pain does NOT constitute evidence of undertreatment 27
28 CDC Emphasis: High Dose Opioids Providers should prescribe lowest possible dose Additional precautions at > 50 MED s Should avoid > 90 MED s Risks of overdose still double at 50 MED s Demands documented increase in function and no adverse side effects Recommend consultation over 90 MED s Closer follow-up Consideration of other risk factors 28
29 Opioid Induced Hyperalgesia Increased sensitivity to noxious or non-noxious stimuli Sensitization of pro-nociceptive mechanisms Hypersensitivity and allodynia Confused with tolerance Caused with rapid escalation and high dose therapy Activity at the NMDA receptor in dorsal horn 29
30 Prescription Drug Monitoring The 4 A s is a useful tool Ongoing dialogue with patients Regular monitoring is critical as risks and benefits do not remain static Changes in the pain condition Presence of co-existing disease Changes in psychological or social factors 30
31 Physician Protect Thyself Pay attention to a pattern of activity that suggests abuse and address Monitor closely through follow up and documentation Use available tools: PMP website UDS and pill counts Pharmacies Obligated to protect yourself, your patient and society from opioid abuse and diversion 31
32 Prescription Monitoring Program Powerful tool Mandated in Oklahoma first visit and every 180 days Physician and staff friendly Helps with determining MED s Helpful to determine other scheduled drugs like benzodiazepines Good teaching moment with the patient 32
33 33
34 Urine Drug Screening All new patients and then random unless triggers seen Becoming standard of care An excellent education tool for the physician Insurance driven limitations Triggers for UDS Need for confirmatory testing Is the prescribed drug in the system Are there illicit drugs or non-prescribed opioids in the urine 34
35 Pill Counts Appropriate disposal of unused meds Where is the medication if not in the urine? On-site or at a local pharmacy Ideally within 24 hours When switching opioids In circumstances of signs of diversion Lockbox or safe 35
36 Don t Forget Documentation A patient problem requires a documented response and action Something occurred so it requires a note UDS result PMP result Non-fatal overdose Lost or stolen prescription Phone calls 36
37 Difficult Situations Pain is subjective Physicians are care givers not law enforcement officers A lost or stolen prescription? Abnormal UDS Illicit drugs Pattern of abuse demands a response Counseling of patient Some better off opioids Poor insight, unrealistic expectations Discussion of alternative treatment modalities 37
38 Common Mistakes Continued escalation of opioids despite no evidence of improvement Why? Think of the differential diagnosis Opioids used in pain syndromes know to be poorly responsive Failure to document Not addressing psychosocial issues Lenient with abuse behaviors Failure to use monitoring systems 38
39 Common Difficulties Overuse of a prescription Illegal drug in the system Nonprescribed drug in the system Abuse or honest mistake? Manipulative and argumentative Bargaining and anger Is there a pattern here? 39
40 Difficult Conversations I think you might have OIH You don t seem to be better on opioids You seem sedated Maybe we need to decrease your dose to <90 MEDS Your urine shows an illegal drug I wonder if you might have an opioid use disorder We received a phone call 40
41 My Personal Views Try not to kick the can down the road Rarely fire a patient with opioid or illicit drug problems Often push for counseling or treatment Continue to provide care with adjunctives unless behavior cannot be tolerated I do not tolerate threats to staff or myself Most chronic pain patients fire themselves Close contact with referring doctor 41
42 Addressing Obvious Abuse and Diversion Don t play the game Contact law enforcement agencies? Refer the patient for appropriate help Treat withdrawal if indicated Contact other physicians and pharmacies 30 day supply of opioids? Consider referral for treatment Under no circumstances may a physician dispense with the knowledge the drug will be abused or diverted (DEA 2006) 42
43 A Final Caution: What the Boards View as Inappropriate Inadequate attention Inadequate monitoring Inadequate patient education and consent Unjustified dose escalations Excessive opioid dosing Not using tools for risk mitigation 43
44 Conclusion: Key Points Thoroughly evaluate the pain complaint Consider psychological issues Consider opioids as a treatment of last resort Use a contract and informed consent Patients should demonstrate a high level of responsibility An accountability system must be in place 44
Opioids: What You Should Know About Opioid Prescribing. Denis G. Patterson, DO Nevada State Medical Association October 19, 2016
 Opioids: What You Should Know About Opioid Prescribing Denis G. Patterson, DO Nevada State Medical Association October 19, 2016 Contact Information Denis G. Patterson, DO Nevada Advanced Pain Specialists
Opioids: What You Should Know About Opioid Prescribing Denis G. Patterson, DO Nevada State Medical Association October 19, 2016 Contact Information Denis G. Patterson, DO Nevada Advanced Pain Specialists
Opioid Review and MAT Clinic CDC Guidelines
 1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
1 Opioid Review and MAT Clinic CDC Guidelines January 10, 2018 Housekeeping Use chat feature to inform everyone who s at your clinic Click chat on Zoom option bar Chat Everyone the names of those who are
Rule Governing the Prescribing of Opioids for Pain
 Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
CDC Guideline for Prescribing Opioids for Chronic Pain. Centers for Disease Control and Prevention National Center for Injury Prevention and Control
 CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine
 D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine Financial Disclosure I have no relevant financial relationships
D. Janene Holladay, M.D. Board Certifications: American Board of Anesthesiology American Board of Pain Medicine American Board of Addiction Medicine Financial Disclosure I have no relevant financial relationships
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Safe Prescribing of Drugs with Potential for Misuse/Diversion
 College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
College of Physicians and Surgeons of British Columbia Safe Prescribing of Drugs with Potential for Misuse/Diversion Preamble This document establishes both professional standards as well as guidelines
Opioid Management of Chronic (Non- Cancer) Pain
 Pain") Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care)
") Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
Standard of Practice for Prescribing Opioids (Excluding Cancer, Palliative, and End-of-Life Care) Preamble This Standard establishes the standards of practice and ethical requirements of all physicians
3. Has the patient had a sustained improvement in Pain or Function (e.g. PEG scale with a 30 percent response from baseline)?
?") Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH KETUCK Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Prescription Monitoring Program (PMP)
") 06/15/2018 FACT SHEET Implementation of Enacted Prescribing Limits and Requirements and Relevant Opioid Prescribing Laws and Rules Background: The 2016 law (Chapter 488) makes five major changes to opioid
06/15/2018 FACT SHEET Implementation of Enacted Prescribing Limits and Requirements and Relevant Opioid Prescribing Laws and Rules Background: The 2016 law (Chapter 488) makes five major changes to opioid
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Readopt with amendment Med 502, effective (Document #11090), to read as follows:
, to read as follows:") Adopted Rules 11-2-16 1 Readopt with amendment Med 502, effective 5-3-16 (Document #11090), to read as follows: PART Med 502 OPIOID PRESCRIBING Med 502.01 Applicability. This part shall apply to the prescribing
Adopted Rules 11-2-16 1 Readopt with amendment Med 502, effective 5-3-16 (Document #11090), to read as follows: PART Med 502 OPIOID PRESCRIBING Med 502.01 Applicability. This part shall apply to the prescribing
OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES
 TITLE 16 CHAPTER 10 PART 14 OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES 16.10.14.1 ISSUING AGENCY: New
TITLE 16 CHAPTER 10 PART 14 OCCUPATIONAL AND PROFESSIONAL LICENSING MEDICINE AND SURGERY PRACTITIONERS MANAGEMENT OF PAIN AND OTHER CONDITIONS WITH CONTROLLED SUBSTANCES 16.10.14.1 ISSUING AGENCY: New
2. Is this request for a preferred medication? Y N
 Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Pharmacy Prior Authorization AETA BETTER HEALTH EW JERSE (MEDICAID) Opioids Long-Acting and Short-Acting (Medicaid) This fax machine is located in a secure location as required by HIPAA regulations. Complete/review
Vermont. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Vermont Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
Prescribing and Dispensing Profile Vermont Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of
Ahsan U. Rashid, M.D., F.A.C.P.
 Ahsan U. Rashid, M.D., F.A.C.P. OPIOID MAINTENANCE AND CONSENT Instructions: Review this document before signing. This document will help both the patient and caregivers in establishing a medical program
Ahsan U. Rashid, M.D., F.A.C.P. OPIOID MAINTENANCE AND CONSENT Instructions: Review this document before signing. This document will help both the patient and caregivers in establishing a medical program
New Guidelines for Opioid Prescribing
 New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
New Guidelines for Opioid Prescribing What They Mean for Elders with Chronic Pain Manu Thakral, PhD, ARNP Kaiser Permanente Washington Health Research Institute Kaiser Permanente Washington Health Research
CDC Guideline for Prescribing Opioids for Chronic Pain
 National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
National Center for Injury Prevention and Control CDC Guideline for Prescribing Opioids for Chronic Pain John Halpin, MD, MPH Medical Officer Division of Unintentional Injury Prevention Prescription Drug
INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine
 INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine The purpose of this agreement is to give you information about the medications you will be taking for
INFORMED CONSENT FOR OPIOID TREATMENT FOR NON-CANCER/CANCER PAIN Texas Pain and Regenerative Medicine The purpose of this agreement is to give you information about the medications you will be taking for
Opioid Abuse in Iowa Rx to Heroin. Iowa Governor s Office of Drug Control Policy January 2016
 1 Opioid Abuse in Iowa Rx to Heroin Iowa Governor s Office of Drug Control Policy January 2016 Why Is This Important? 2 3 National Rx Painkiller Trends CDC, 2013 4 National Rx-Heroin Trends NIH, 2015 5
1 Opioid Abuse in Iowa Rx to Heroin Iowa Governor s Office of Drug Control Policy January 2016 Why Is This Important? 2 3 National Rx Painkiller Trends CDC, 2013 4 National Rx-Heroin Trends NIH, 2015 5
Prescribing Opioids in the Opioid Epidemic. Scott Woffinden, PA-C Jason Chapman, JD
 Prescribing Opioids in the Opioid Epidemic Scott Woffinden, PA-C Jason Chapman, JD What's the Problem? http://www.zdoggmd.com/blank-script-taylor-swift-parody/ What's the Problem? CDC 115 Americans die
Prescribing Opioids in the Opioid Epidemic Scott Woffinden, PA-C Jason Chapman, JD What's the Problem? http://www.zdoggmd.com/blank-script-taylor-swift-parody/ What's the Problem? CDC 115 Americans die
Opioid Prescribing Guidelines for Patients in the Emergency Department
 Opioid Prescribing Guidelines for Patients in the Emergency Department and Immediate Care Centers These guidelines are meant to assist clinicians in treating patients with acute and chronic pain in the
Opioid Prescribing Guidelines for Patients in the Emergency Department and Immediate Care Centers These guidelines are meant to assist clinicians in treating patients with acute and chronic pain in the
Opioids drive continued increase in drug overdose deaths
 CDC: Drug overdose deaths increase for 11th consecutive year Opioids drive continued increase in drug overdose deaths Atlanta, GA, USA (February 20, 2013) - Drug overdose deaths increased for the 11th
CDC: Drug overdose deaths increase for 11th consecutive year Opioids drive continued increase in drug overdose deaths Atlanta, GA, USA (February 20, 2013) - Drug overdose deaths increased for the 11th
Drug Overdoses A Public Health Problem. Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013. Objectives
 Drug Overdoses A Public Health Problem Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013 Objectives O Provide an overview of the trends in opioid prescriptions and impact O Consider implications for the
Drug Overdoses A Public Health Problem Marianne Cloeren, MD, MPH, FACOEM, FACP 10/2/2013 Objectives O Provide an overview of the trends in opioid prescriptions and impact O Consider implications for the
The Prescription Review Program and College Expectations. Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM
 The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM April 28, 2017 Disclosure Relationship with commercial interests: None Professional roles: Addictions
California. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile California Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING
 THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
THE PROS & CONS OF THE CDC GUIDELINES FOR SAFE OPIOID PRESCRIBING Ernest J Dole, PharmD, PhC, FASHP, BCPS Clinical Pharmacist University of New Mexico Hospitals And Clinical Associate Professor University
Proposed Revision to Med (i)
") Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Proposed Revision to Med 501.02 (i) I. Purpose This rule has been adopted to enable the Board to best protect public health and safety while providing a framework for licensees to effectively treat and
Chronic Pain Pharmacist role in the clinic
 Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
Chronic Pain Pharmacist role in the clinic WSPA Annual Meeting 2015 Alvin Goo, PharmD Clinical Associate Professor University of Washington Schools of Pharmacy and Family Medicine Speakers Declaration
The Regulatory Agency Will See You Now Kevin L. Zacharoff, MD Disclosures Nothing to Disclose
 The Regulatory Agency Will See You Now Kevin L. Zacharoff, MD Disclosures Nothing to Disclose 1 Learning Objectives Identify pain treatment related regulatory agencies Discuss the changing role of regulatory
The Regulatory Agency Will See You Now Kevin L. Zacharoff, MD Disclosures Nothing to Disclose 1 Learning Objectives Identify pain treatment related regulatory agencies Discuss the changing role of regulatory
Utah. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Pain and Addiction. Edward Jouney, DO Department of Psychiatry
 Pain and Addiction Edward Jouney, DO Department of Psychiatry Case 43 year-old female with a history chronic lower back pain presents to your clinic ongoing care. She has experienced pain difficulties
Pain and Addiction Edward Jouney, DO Department of Psychiatry Case 43 year-old female with a history chronic lower back pain presents to your clinic ongoing care. She has experienced pain difficulties
Section I. Short-acting opioid Prior Authorization Criteria
 Request for Prior Authorization for Opioid analgesics Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 Requests for opioid analgesics may be subject to prior authorization
Request for Prior Authorization for Opioid analgesics Website Form www.highmarkhealthoptions.com Submit request via: Fax - 1-855-476-4158 Requests for opioid analgesics may be subject to prior authorization
Opioid Prescribing Improvement Program
 Opioid Prescribing Improvement Program Jeff Schiff, MD, MBA, Medical Director of Minnesota Health Care Programs Sarah Rinn, MPH, Opioid Prescribing Improvement Program Coordinator Agenda Opioid Prescribing
Opioid Prescribing Improvement Program Jeff Schiff, MD, MBA, Medical Director of Minnesota Health Care Programs Sarah Rinn, MPH, Opioid Prescribing Improvement Program Coordinator Agenda Opioid Prescribing
Oklahoma. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Oklahoma Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Oklahoma Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
WHAT YOU NEED TO KNOW TO ABOUT AB 474
 WHAT YOU NEED TO KNOW TO ABOUT AB 474 PRESENTED BY: NEVADA STATE BOARD OF OSTEOPATHIC MEDICINE 2275 Corporate Circle, Suite 210 Henderson, NV 89074 702-732-2147 Fax 702-732-2079 Web Site: www.bom.nv.gov
WHAT YOU NEED TO KNOW TO ABOUT AB 474 PRESENTED BY: NEVADA STATE BOARD OF OSTEOPATHIC MEDICINE 2275 Corporate Circle, Suite 210 Henderson, NV 89074 702-732-2147 Fax 702-732-2079 Web Site: www.bom.nv.gov
Who is Behind the Opioid Epidemic?
 Safe and Effective Management of Pain and Addiction CARL CHRISTENSEN, MD PHD MEDICAL DIRECTOR, DAWN FARM CLINICAL ASSOCIATE PROFESSOR, WSU SCHOOL OF MEDICINE WWW.CHRISTENSENRECOVERY.COM Tonight s Talk:
Safe and Effective Management of Pain and Addiction CARL CHRISTENSEN, MD PHD MEDICAL DIRECTOR, DAWN FARM CLINICAL ASSOCIATE PROFESSOR, WSU SCHOOL OF MEDICINE WWW.CHRISTENSENRECOVERY.COM Tonight s Talk:
PRESCRIBING GUIDELINES
 Ohio Department of Health RESPONSE TO OHIO S PRESCRIPTION DRUG OVERDOSE EPIDEMIC: PRESCRIBING GUIDELINES MIPA CONFERENCE PREVENTING INJURY: FROM RESEARCH TO PRACTICE TO PEOPLE SEPTEMBER 30, 2013 Christy
Ohio Department of Health RESPONSE TO OHIO S PRESCRIPTION DRUG OVERDOSE EPIDEMIC: PRESCRIBING GUIDELINES MIPA CONFERENCE PREVENTING INJURY: FROM RESEARCH TO PRACTICE TO PEOPLE SEPTEMBER 30, 2013 Christy
Summary of Recommendations...3. PEG: A Three-Item Scale Assessing Pain (Appendix A) Chronic Pain Flow Sheet Acute Pain Flow Sheet...
 Chronic Pain Flow Sheet Acute Pain Flow Sheet...") Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
Table of Contents Summary of Recommendations....3 PEG: A Three-Item Scale Assessing Pain (Appendix A)...12 Chronic Pain Flow Sheet...13 Acute Pain Flow Sheet...14 Pocket Guide: Tapering Opioids for Chronic
MOA: Practice Managers Program. Presented by: Kimber Debelak, CMC, CMOM, CMIS. May 17, zpain Management. & New Opioid Laws
 MOA: Practice Managers Program Presented by: Kimber Debelak, CMC, CMOM, CMIS May 17, 2018 Pain Management & New Opioid Laws Objectives and Educational Statement Objectives To understand the need for new
MOA: Practice Managers Program Presented by: Kimber Debelak, CMC, CMOM, CMIS May 17, 2018 Pain Management & New Opioid Laws Objectives and Educational Statement Objectives To understand the need for new
SAFE PRESCRIBING: RULES AND REGULATIONS. Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017
 SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017 DISCLOSURES I have no financial disclosures. OBJECTIVES Discuss the significance of the opiate
SAFE PRESCRIBING: RULES AND REGULATIONS Michelle Y. Owens, MD MS State Board of Medical Licensure June 30, 2017 DISCLOSURES I have no financial disclosures. OBJECTIVES Discuss the significance of the opiate
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets. Risk Evaluation and Mitigation Strategy (REMS) Program
 Program") SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
The Role of Dentists in Preventing Opioid Abuse Tufts Health Care Institute Program on Opioid Risk Management 12 th Summit Meeting March 11-12, 2010
 The Role of Dentists in Preventing Opioid Abuse Tufts Health Care Institute Program on Opioid Risk Management 12 th Summit Meeting March 11-12, 2010 EXECUTIVE SUMMARY It is well documented in multiple
The Role of Dentists in Preventing Opioid Abuse Tufts Health Care Institute Program on Opioid Risk Management 12 th Summit Meeting March 11-12, 2010 EXECUTIVE SUMMARY It is well documented in multiple
PRESCRIPTION DRUG ABUSE: THE NATIONAL PERSPECTIVE
 PRESCRIPTION DRUG ABUSE: THE NATIONAL PERSPECTIVE September 20, 2013 Association of State and Territorial Health Officials Annual Meeting R. Gil Kerlikowske Director of National Drug Control Policy National
PRESCRIPTION DRUG ABUSE: THE NATIONAL PERSPECTIVE September 20, 2013 Association of State and Territorial Health Officials Annual Meeting R. Gil Kerlikowske Director of National Drug Control Policy National
As part of the Opioid Analgesic REMS, all opioid analgesic companies must provide the following:
 Introduction FDA s Opioid Analgesic REMS Education Blueprint for Health Care Providers Involved in the Treatment and Monitoring of Patients with Pain (January 2018) Background In July 2012, FDA approved
Introduction FDA s Opioid Analgesic REMS Education Blueprint for Health Care Providers Involved in the Treatment and Monitoring of Patients with Pain (January 2018) Background In July 2012, FDA approved
NBPDP Drug Utilization Review Process Update
 Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Bulletin # 802 December 1, 2010 NBPDP Drug Utilization Review Process Update The New Brunswick Prescription Drug Program (NBPDP) employs a Drug Utilization Review (DUR) process which identifies, investigates
Chronic Pain Management in the Primary Care Setting
 Chronic Pain Management in the Primary Care Setting Keeping you and your patients safe. Joel Porter, MD October 1, 2015 Chronic Pain Management Chronic pain is a major public health problem Existing chronic
Chronic Pain Management in the Primary Care Setting Keeping you and your patients safe. Joel Porter, MD October 1, 2015 Chronic Pain Management Chronic pain is a major public health problem Existing chronic
Practical Tools to Successfully Taper Prescription Opioids. Melissa Weimer, DO, MCR
 Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Anyone Can Become Addicted. Anyone.
 Anyone Can Become Addicted. Anyone. PAStop.org Family Toolkit Seeking Drug Abuse Treatment: Know What to Ask Trying to identify the right treatment programs for a loved one can be a difficult process.
Anyone Can Become Addicted. Anyone. PAStop.org Family Toolkit Seeking Drug Abuse Treatment: Know What to Ask Trying to identify the right treatment programs for a loved one can be a difficult process.
Revised 9/30/2016. Primary Care Provider Pain Management Toolkit
 Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018
 Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Opioid Prescribing Tips & Tricks CANDY STOCKTON, MD MAY 2018 Disclosures None Educational Objectives Understand CA state medical board guidelines for prescribing opioids for chronic pain Understand the
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
Missouri Guidelines for the Use of Controlled Substances for the Treatment of Pain
 Substances for the Treatment of Pain Effective January 2007, the Board of Healing Arts appointed a Task Force to review the current statutes, rules and guidelines regarding the treatment of pain. This
Substances for the Treatment of Pain Effective January 2007, the Board of Healing Arts appointed a Task Force to review the current statutes, rules and guidelines regarding the treatment of pain. This
FY17 SCOPE OF WORK TEMPLATE. Name of Program/Services: Medication-Assisted Treatment: Buprenorphine
 FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
Patient and Family Agreement on Opioids
 Patient and Family Agreement on Opioids We care about our patients and are committed to their recovery and wellness. We offer our patients medications and options for various services to keep them from
Patient and Family Agreement on Opioids We care about our patients and are committed to their recovery and wellness. We offer our patients medications and options for various services to keep them from
KANSAS Kansas State Board of Healing Arts. Source: Kansas State Board of Healing Arts. Approved: October 17, 1998
 KANSAS Kansas State Board of Healing Arts Source: Kansas State Board of Healing Arts Approved: October 17, 1998 GUIDELINES FOR THE USE OF CONTROLLED SUBSTANCES FOR THE TREATMENT OF PAIN Section 1: Preamble
KANSAS Kansas State Board of Healing Arts Source: Kansas State Board of Healing Arts Approved: October 17, 1998 GUIDELINES FOR THE USE OF CONTROLLED SUBSTANCES FOR THE TREATMENT OF PAIN Section 1: Preamble
Canadian Guideline for Opioids for Chronic Non-Cancer Pain. Speaker Disclosure. Objectives. Canadian Guideline for Opioids for Chronic Non-Cancer Pain
 Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
Canadian Guideline for Opioids for Chronic Non-Cancer Pain John Fraser Community Hospital Program New Glasgow November 1, 2017 This speaker has been asked to disclose to the audience any involvement with
The Role of the PDMP: Foundational Knowledge and Best Practices
 The Role of the PDMP: Foundational Knowledge and Best Practices Brent I. Fox, PharmD, PhD Health Outcomes Research and Policy Harrison School of Pharmacy Auburn University DISCLOSURE I, Brent Fox, have
The Role of the PDMP: Foundational Knowledge and Best Practices Brent I. Fox, PharmD, PhD Health Outcomes Research and Policy Harrison School of Pharmacy Auburn University DISCLOSURE I, Brent Fox, have
Strategies for Federal Agencies
 Confronting Pain Management and the Opioid Epidemic Strategies for Federal Agencies Over the past 25 years, the United States has experienced a dramatic increase in deaths from opioid overdose, opioid
Confronting Pain Management and the Opioid Epidemic Strategies for Federal Agencies Over the past 25 years, the United States has experienced a dramatic increase in deaths from opioid overdose, opioid
Virginia. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Prescribing and Dispensing Profile Virginia Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points
Use of Opioids for Chronic Non Malignant Pain (CNMP)
") I. PURPOSE Use of Opioids for Chronic Non Malignant Pain (CNMP) We the Safe Opioid Prescribing and Review Committee (SOPARC) are inspired to support a shift in opioid prescribing that improves clinical
I. PURPOSE Use of Opioids for Chronic Non Malignant Pain (CNMP) We the Safe Opioid Prescribing and Review Committee (SOPARC) are inspired to support a shift in opioid prescribing that improves clinical
Reference for Physicians on the Use of Opioid Analgesics in the Treatment of Chronic Pain, in the Office Setting
 Reference for Physicians on the Use of Opioid Analgesics in the Treatment of Chronic Pain, in the Office Setting The Arizona Medical Board intends this document to be a useful reference tool for physicians
Reference for Physicians on the Use of Opioid Analgesics in the Treatment of Chronic Pain, in the Office Setting The Arizona Medical Board intends this document to be a useful reference tool for physicians
Principles and language suggestions for talking with patients
 SAFER MANAGEMENT OF OPIOIDS FOR CHRONIC PAIN: Principles and language suggestions for talking with patients Use these principles and language suggestions when discussing opioid risks and safety monitoring
SAFER MANAGEMENT OF OPIOIDS FOR CHRONIC PAIN: Principles and language suggestions for talking with patients Use these principles and language suggestions when discussing opioid risks and safety monitoring
The Challenging Patient with Chronic Opioid Usage MD ACP Meeting
 The Challenging Patient with Chronic Opioid Usage. 2018 MD ACP Meeting Darius A. Rastegar, MD March 12, 2018 1 Prescribing Opioids: A question of balance Opioids are an effective treatment for acute pain.
The Challenging Patient with Chronic Opioid Usage. 2018 MD ACP Meeting Darius A. Rastegar, MD March 12, 2018 1 Prescribing Opioids: A question of balance Opioids are an effective treatment for acute pain.
What is drug diversion?
 Learning Objectives Identify the impact of drug diversion on patients and healthcare organizations Explain the common points of risks and methods of drug diversion in healthcare s controlled substance
Learning Objectives Identify the impact of drug diversion on patients and healthcare organizations Explain the common points of risks and methods of drug diversion in healthcare s controlled substance
OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI)
") OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI) Case 1- Prep Materials University of Massachusetts Medical School Opioid Conscious Curriculum March 2018 Learner Prep Objectives The purpose of this prep
OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI) Case 1- Prep Materials University of Massachusetts Medical School Opioid Conscious Curriculum March 2018 Learner Prep Objectives The purpose of this prep
A Response to Opioid Addiction
 A Response to Opioid Addiction Nancy Bradley, BSN, RN-BC The more I learn, the more I find I do not know I have over 20 years experience in Oncology, hospital based I have worked the last 14 years in out
A Response to Opioid Addiction Nancy Bradley, BSN, RN-BC The more I learn, the more I find I do not know I have over 20 years experience in Oncology, hospital based I have worked the last 14 years in out
A LOOK AT ABUSE-DETERRENT OPIOIDS
 JULY 2017 Drugs Under Review ICER s report reviewed evidence on ten abuse-deterrent formulations (ADF) of opioids. Nine of the drugs were extended release (ER) opioids, and one was immediate release (IR).
JULY 2017 Drugs Under Review ICER s report reviewed evidence on ten abuse-deterrent formulations (ADF) of opioids. Nine of the drugs were extended release (ER) opioids, and one was immediate release (IR).
MEDICATION MANAGEMENT AGREEMENT
 MEDICATION MANAGEMENT AGREEMENT The goal of this agreement is to ensure that you and your physician comply with all state and federal regulations concerning the prescribing of controlled substances. The
MEDICATION MANAGEMENT AGREEMENT The goal of this agreement is to ensure that you and your physician comply with all state and federal regulations concerning the prescribing of controlled substances. The
Docket No. FDA-2009-N-0143; Risk Evaluation and Mitigation Strategies for Certain Opioid Drugs
 June 30, 2009 Margaret Hamburg, MD Commissioner Food and Drug Administration U.S. Department of Health & Human Services 5630 Fishers Lane Rockville, MD 20852 Re: Docket No. FDA-2009-N-0143; Risk Evaluation
June 30, 2009 Margaret Hamburg, MD Commissioner Food and Drug Administration U.S. Department of Health & Human Services 5630 Fishers Lane Rockville, MD 20852 Re: Docket No. FDA-2009-N-0143; Risk Evaluation
EMERGENCY DEPARTMENT MODEL PRACTICES DEALING WITH THE PRESCRIPTION OPIOID EPIDEMIC
 EMERGENCY DEPARTMENT MODEL PRACTICES DEALING WITH THE PRESCRIPTION OPIOID EPIDEMIC RAMI R KHOURY, MD, FACEP ASSISTANT MEDICAL DIRECTOR EMERGENCY CARE ALLEGIANCE HEALTH ADVERTISING AT ITS BEST! OVERDOSE
EMERGENCY DEPARTMENT MODEL PRACTICES DEALING WITH THE PRESCRIPTION OPIOID EPIDEMIC RAMI R KHOURY, MD, FACEP ASSISTANT MEDICAL DIRECTOR EMERGENCY CARE ALLEGIANCE HEALTH ADVERTISING AT ITS BEST! OVERDOSE
Legal Issues in Opioid Prescribing
 Legal Issues in Opioid Prescribing Joanne L. Martin, J.D. Legal Counsel Mayo Clinic Rochester, Mn 2015 MFMER slide-1 Conflict of Interest I have no relevant financial relationships to disclose I will not
Legal Issues in Opioid Prescribing Joanne L. Martin, J.D. Legal Counsel Mayo Clinic Rochester, Mn 2015 MFMER slide-1 Conflict of Interest I have no relevant financial relationships to disclose I will not
The Challenge of Treating Pain
 FDA Charge to the Committee: FDA Opioid Action Plan and Incorporating the Broader Public Health Impact into the Formal Risk-Benefit Assessment for Opioids Robert M. Califf, MD Commissioner of Food and
FDA Charge to the Committee: FDA Opioid Action Plan and Incorporating the Broader Public Health Impact into the Formal Risk-Benefit Assessment for Opioids Robert M. Califf, MD Commissioner of Food and
Blueprint for Prescriber Continuing Education Program
 CDER Final 10/25/11 Blueprint for Prescriber Continuing Education Program I. Introduction: Why Prescriber Education is Important Health care professionals who prescribe extended-release (ER) and long-acting
CDER Final 10/25/11 Blueprint for Prescriber Continuing Education Program I. Introduction: Why Prescriber Education is Important Health care professionals who prescribe extended-release (ER) and long-acting
Potential Solutions to Epidemic Substance Abuse in US and Europe
 Potential Solutions to Epidemic Substance Abuse in US and Europe Richard C. Dart, MD, PhD Director, Rocky Mountain Poison and Drug Center, Denver Health 1 Professor, University of Colorado School of Medicine
Potential Solutions to Epidemic Substance Abuse in US and Europe Richard C. Dart, MD, PhD Director, Rocky Mountain Poison and Drug Center, Denver Health 1 Professor, University of Colorado School of Medicine
Pocahontas County. West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators County Report
 West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators Report The West Virginia Violence and Injury Prevention Program ( VIPP), in collaboration with the West Virginia Board
West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators Report The West Virginia Violence and Injury Prevention Program ( VIPP), in collaboration with the West Virginia Board
Department of Veterans Affairs Network Policy No.: VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA
 Date: September 23, 2014 Long Beach, CA") Department of Veterans Affairs Network Policy No.: 2014-01 VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA CHRONIC OPIOID USE FOR NON-MALIGNANT PAIN 1. PURPOSE: To
Department of Veterans Affairs Network Policy No.: 2014-01 VA Desert Pacific Healthcare Network (VISN 22) Date: September 23, 2014 Long Beach, CA CHRONIC OPIOID USE FOR NON-MALIGNANT PAIN 1. PURPOSE: To
WHY GOOD PAIN MANAGEMENT IS GOOD DRUG ABUSE PREVENTION
 WHY GOOD PAIN MANAGEMENT IS GOOD DRUG ABUSE PREVENTION Bob Twillman, Ph.D., FAPM Executive Director Academy of Integrative Pain Management Walking the Tightrope of Pain Management Adverse Events Misuse
WHY GOOD PAIN MANAGEMENT IS GOOD DRUG ABUSE PREVENTION Bob Twillman, Ph.D., FAPM Executive Director Academy of Integrative Pain Management Walking the Tightrope of Pain Management Adverse Events Misuse
Management of Pain - A Comparison of Current Guidelines
 Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Management of Pain - A Comparison of Current Guidelines The Centers for Disease Control and Prevention (CDC) released a guideline in 2016 regarding the prescribing of opioids for chronic non-cancer pain
Managed Care Pushes for Safer Opioid Oversight
 Page 1 of 6 Clinical AUGUST 11, 2017 Managed Care Pushes for Safer Opioid Oversight High-risk pain Rx eyed Denver Health systems haven t escaped the nation s ongoing opioid crisis, as evidenced by surging
Page 1 of 6 Clinical AUGUST 11, 2017 Managed Care Pushes for Safer Opioid Oversight High-risk pain Rx eyed Denver Health systems haven t escaped the nation s ongoing opioid crisis, as evidenced by surging
The Prescription Review Program and College Expectations. Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM
 The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM October 13, 2017 Disclosure Relationship with commercial interests: None Professional roles:
The Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP Dip. ABAM October 13, 2017 Disclosure Relationship with commercial interests: None Professional roles:
Pennsylvania Prescription Drug Monitoring Program Trends,
 DEA Intelligence Report Brief DEA-PHL-DIR-006-17 Pennsylvania Prescription Drug Monitoring Program Trends, 2014-2015 December 2016 1 Executive Summary The abuse and diversion of pharmaceutical drugs, particularly
DEA Intelligence Report Brief DEA-PHL-DIR-006-17 Pennsylvania Prescription Drug Monitoring Program Trends, 2014-2015 December 2016 1 Executive Summary The abuse and diversion of pharmaceutical drugs, particularly
Barbour County. West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators County Report Barbour County
 County West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators County Report County The West Virginia Violence and Injury Prevention Program ( VIPP), in collaboration with
County West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators County Report County The West Virginia Violence and Injury Prevention Program ( VIPP), in collaboration with
NORTHWEST AIDS EDUCATION AND TRAINING CENTER. Opioid Use Disorders. Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Opioid Use Disorders Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014 Opioid Use Disorders Importance of opioid use disorders Screening and
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Opioid Use Disorders Joseph Merrill M.D., M.P.H. University of Washington April 10, 2014 Opioid Use Disorders Importance of opioid use disorders Screening and
FDA s Response to the Opioid Crisis and the FDA Safe Use Initiative
 FDA s Response to the Opioid Crisis and the FDA Safe Use Initiative Scott K. Winiecki, MD Professional Affairs and Stakeholder Engagement Staff (PASES) Center For Drug Evaluation and Research (CDER) U.S.
FDA s Response to the Opioid Crisis and the FDA Safe Use Initiative Scott K. Winiecki, MD Professional Affairs and Stakeholder Engagement Staff (PASES) Center For Drug Evaluation and Research (CDER) U.S.
Controlled Substance and Wellness Agreement
 Controlled Substance and Wellness Agreement You and your provider have agreed on the use of controlled substance medications to treat your: We want to make sure you know how to manage your new prescription(s)
Controlled Substance and Wellness Agreement You and your provider have agreed on the use of controlled substance medications to treat your: We want to make sure you know how to manage your new prescription(s)
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Serious Mental Illness and Opioid Use Disorder
 Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Scope of the Opiate Problem 6/5/18. Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond. Overview.
 Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
Chronic Pain Management and the Use of Opioid Medications: The CDC Guideline and Beyond David Anisman, MD Medical Director, Farmington Health Center (Primary Care) Associate Medical Director, Community
MQAC Rules for the Management of Chronic Non-Cancer Pain For Allopathic Physicians Effective January 2, 2012
 MQAC Rules for the Management of Chronic Non-Cancer Pain For Allopathic Physicians Effective January 2, 2012 WAC 246-919-850 Pain management Intent. These rules govern the use of opioids in the treatment
MQAC Rules for the Management of Chronic Non-Cancer Pain For Allopathic Physicians Effective January 2, 2012 WAC 246-919-850 Pain management Intent. These rules govern the use of opioids in the treatment
There are no financial or other pertinent conflicts of interest to disclose. Learning Objectives: Key Questions To Ask 10/4/2014
 Maintaining Patient Safety When Chronic Opioid Therapy Is Prescribed P. David Pacheco, Ph.C, PA-C, CAAAPM Pain Medication Management Specialist Southwest Interventional Pain Specialists, PC 4700 Jefferson
Maintaining Patient Safety When Chronic Opioid Therapy Is Prescribed P. David Pacheco, Ph.C, PA-C, CAAAPM Pain Medication Management Specialist Southwest Interventional Pain Specialists, PC 4700 Jefferson
OPIOID CRISIS: A PERSPECTIVE. Karl J. Haake, MD
 OPIOID CRISIS: A PERSPECTIVE Karl J. Haake, MD LEARNING OBJECTIVES Summarize the history behind the opioid epidemic in America Identify the issues surrounding the the treatment of chronic pain Demonstrate
OPIOID CRISIS: A PERSPECTIVE Karl J. Haake, MD LEARNING OBJECTIVES Summarize the history behind the opioid epidemic in America Identify the issues surrounding the the treatment of chronic pain Demonstrate
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain
 Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
Best Practices in Prescribing Opioids for Chronic Non-cancer Pain Disclosures S C O T T S T E I G E R, M D, F A C P, D A B A M A S S I S T A N T C L I N I C A L P R O F E S S O R D I V I S I O N O F G
Tapering Opioids Best Practices*
 Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
Tapering Opioids Best Practices* Chuck Hofmann, MD, MACP 5 th Annual EOCCO Office Staff and Provider Summit September 28, 2017 Disclosure No Conflicts of Interest to report Learning Objectives Understand
Mingo County. West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators County Report
 West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators Report The West Virginia Violence and Injury Prevention Program ( VIPP), in collaboration with the West Virginia Board
West Virginia Board of Pharmacy Prescription Opioid Problematic Prescribing Indicators Report The West Virginia Violence and Injury Prevention Program ( VIPP), in collaboration with the West Virginia Board
Prescription Review Program and College Expectations
 Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP ABAM Consultant, Prescription Review Program Prescribers Course May 13, 2016 Disclosure Never had any commercial
Prescription Review Program and College Expectations Dr. Rashmi Chadha MBChB MScCH CCFP MRCGP ABAM Consultant, Prescription Review Program Prescribers Course May 13, 2016 Disclosure Never had any commercial