Treatment of Substance Use Disorders in the Real World. Jessica M. Peirce, Ph.D. Johns Hopkins University School of Medicine
|
|
|
- Georgina Gordon
- 5 years ago
- Views:
Transcription
1 Treatment of Substance Use Disorders in the Real World Jessica M. Peirce, Ph.D. Johns Hopkins University School of Medicine
2 Objectives identify the core components of the most common substance use disorder treatment modalities compare substance use disorder treatment options to make realistic and informed recommendations for patients/clients describe common addiction-related behaviors that patients/clients display and how to address them
3 Take home points 1. You are already treating people with substance use disorders 2. You know more than you think you do
4 Definitions Drug = all licit and illicit drugs, alcohol; NOT tobacco Patients vs. clients
5
6

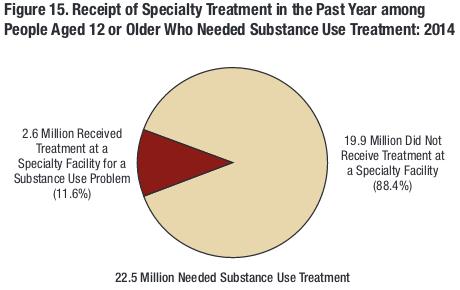
7 NSDUH, 2014
8 History of SUD treatment Developed parallel to other psychiatric treatment Group-based and paraprofessionals Standards for training vary widely Evidence-based treatment is not uniformly offered Conceptualization and treatment for SUD may not reflect the highest current standards
9 Treatment modalities Adjunctive Care: NOT treatment Inpatient treatment Short-term; Long-term Psychosocial outpatient & intensive outpatient Medication-assisted treatment Buprenorphine; methadone Disulfiram (Antabuse); naltrexone (Vivitrol)
10 Adjunctive care Detoxification ~3 days in hospital Purpose is to medically manage withdrawal Benzodiazepines and alcohol most common
11 Adjunctive care 12-step (and other) fellowships: AA, NA, Smart Recovery Typically regular meeting times Format varies, but no leader and no expectation of specific training for helpers Purpose is to offer social support for recovery Sponsor, home group
12 Adjunctive care Recovery housing Typically a group home for people with SUD Most are privately managed, but some are affiliated with SUD treatment Minimal training or regulations Purpose is to offer a drug-free living environment
13

14 Short-term inpatient treatment Length Indication Purpose Advantages Disadvantages Best for 7-30 days Any SUD Controlled environment Establish motivation Removes triggers and daily stressors Can be expensive Difficult to accommodate Doesn t allow skills practice Beginning of extended treatment
15 Long-term inpatient treatment Length Indication Purpose Advantages Disadvantages Best for 3-6 months Any SUD Controlled environment Establish new habits and skills Removes triggers and daily stressors Very few available Expensive Difficult to accommodate Doesn t allow skills practice Beginning of extended treatment

16 Psychosocial outpatient/ Intensive outpatient Length Indication Purpose Advantages Disadvantages Best for Varies (1-3 months typical) Any SUD Learn and practice skills Allows skills practice High dropout Quality varies widely Medication not usually offered Drug screens not universal Extended treatment
17 N Engl J Med 2015; 373:
18



19 Medication-assisted treatment Length Indication Purpose Advantages Disadvantages Best for Long-term ( > 1 year) Opioid use disorder (+- other SUD) Reduce/eliminate opioid use Drug screens common Highly effective May not address related problems Very long term Requires more frequent visits Extended treatment




20 Medication-assisted treatment Buprenorphine Methadone (Suboxone, Zubsolv) Setting Office or clinic Clinic Visits Weekly to quarterly Daily to 2x/mo Counseling Minimal Varies Subjective effect Overdose potential Less acute effect Less withdrawal Less risk More acute effect* Greater withdrawal More risk
: careful monitoring acamprosate (Campral)")
21 Other pharmacotherapy Opioids naltrexone (Vivitrol, Revia) Alcohol disulfiram (Antabuse): careful monitoring acamprosate (Campral) naltrexone
22 Evidence-based treatment: Strong Cognitive behavioral therapy Relapse Prevention: Marlatt; Witkiewitz Coping with Craving: Carroll Contingency Management: Higgins; Stitzer; Petry Community Reinforcement (CRA/CRAFT): Meyers; Azrin Behavioral Couples Therapy: O Farrell
23 Evidence-based treatment: Moderate 12-step Facilitation Therapy: Baker Dialectical Behavior Therapy: Linehan Acceptance and Commitment Therapy: Hayes

24 Evidence-based treatment components Skills training and practice Objective and subjective monitoring of symptoms (e.g., drug use) Strengthen support for recovery Monitor treatment adherence, including medication

25 Elements of evidence-based treatment Joseph video #14
26 Treatment elements not recommended Confrontation and punishment Focus on graduation Reliance on self-report alone Discharge from treatment for drug use
27 But what should I do?
28 What you can do Be aware of your own assumptions Conceptualize the problem accurately SBIRT Encourage harm reduction Use CBT principles/skills Consider and monitor medication Encourage recovery-oriented social support Recognize and address problems
29 Stigma the shame or disgrace attached to something regarded as socially unacceptable a mark of disgrace associated with a particular circumstance, quality, or person a set of negative and often unfair beliefs that a society or group of people have about something Remember: WE are members of society!






30
31 Life with addiction Joseph video #13




32 Stigma MORAL FAILING TREATMENT Drug users are weak, lazy, sinful, immoral Drug users are inherently flawed or broken Drug users should be ashamed Drug users have an addictive personality Only the right treatment is appropriate
33 Stigma COMPLEX DISORDER Drug users have a psychiatric disorder Some people have a chronic disorder Drug users may do bad things, but are not bad people Treatment should be targeted to the patient and patient needs TREATMENT Psychosocial and medical intervention Need for repeated/longer treatments and continued monitoring Take responsibility for actions, not disorder Different or combined treatments may be necessary
34 Conceptualization Mood disorder Substance use disorder



35 Conceptualization Mood disorder Hiding evidence of selfharm Refusal to participate in treatment/take medications Belief that manic symptoms are helpful and should not be stopped Substance use disorder Lying about/hiding drug use and consequences Refusal to participate in treatment/take medications Belief that drug use is harmless or beneficial
36 Conceptualization As severity increases, treatment intensity increases Relapse is possible and more likely as severity increases Relapse is not failure of patient or treatment More severe and chronic disorders may need very long-term monitoring and treatment Medication is a tool to be used neither the sum total of treatment nor to be discarded without consideration
37 SBIRT Screening: include a screening measure in your assessment for everyone Brief Intervention: review your assessment, commenting on drug use Place drug use in context, like any other behavior Could end here if problem is mild
38 Referral to treatment Things to consider: Type, frequency, amount of drugs used Need for medical withdrawal Motivation Social support for recovery Barriers to participation Comorbid problems
39 Sue, a 43 year old African-American woman, seeks help with anxious and depressive symptoms she relates to her troubled relationship. She and her husband argue several times a week; sometimes the argument gets physical. The arguments center on Sue s husband s complaints about finances and her behavior, including her drinking. Sue believes she is a social drinker, because everyone drinks like she does. They both drink several days a week, but more on Friday and Saturday nights when they go out with friends. Those nights, Sue has 4-5 mixed drinks. Weeknights, she will have as much as a bottle of wine.
40 Sue, a 43 year old African-American woman, seeks help with anxious and depressive symptoms she relates to her troubled relationship. She and her husband argue several times a week; sometimes the argument gets physical. The arguments center on Sue s husband s complaints about finances and her behavior, including her drinking. Sue believes she is a social drinker, because everyone drinks like she does. They both drink several days a week, but more on Friday and Saturday nights when they go out with friends. Those nights, Sue has 4-5 mixed drinks. Weeknights, she will have as much as a bottle of wine.
41 Referral to treatment: Sue Things to consider: Type, frequency, amount of drugs used Need for medical withdrawal Motivation Social support for recovery Barriers to participation Comorbid problems
42 John, a 29 year old Caucasian man, seeks help for depressive symptoms related to losing his job. He had a work-related back injury ~9 months ago and hasn t been able to work since then. John has increased his daily Oxycontin dose, but he s running out before the end of the month and the doctor is threatening to discharge him. He spends his days watching TV, smoking pot, and sleeping. John thinks he might be taking too many pills, but he also reports excruciating pain that no one cares about. His girlfriend is fed up with his complaining and not helping around the house.
43 John, a 29 year old Caucasian man, seeks help for depressive symptoms related to losing his job. He had a work-related back injury ~9 months ago and hasn t been able to work since then. John has increased his daily Oxycontin dose, but he s running out before the end of the month and the doctor is threatening to discharge him. He spends his days watching TV, smoking pot, and sleeping. John thinks he might be taking too many pills, but he also reports excruciating pain that no one cares about. His girlfriend is fed up with his complaining and not helping around the house.
44 Referral to treatment: John Things to consider: Type, frequency, amount of drugs used Need for medical withdrawal Motivation Social support for recovery Barriers to participation Comorbid problems
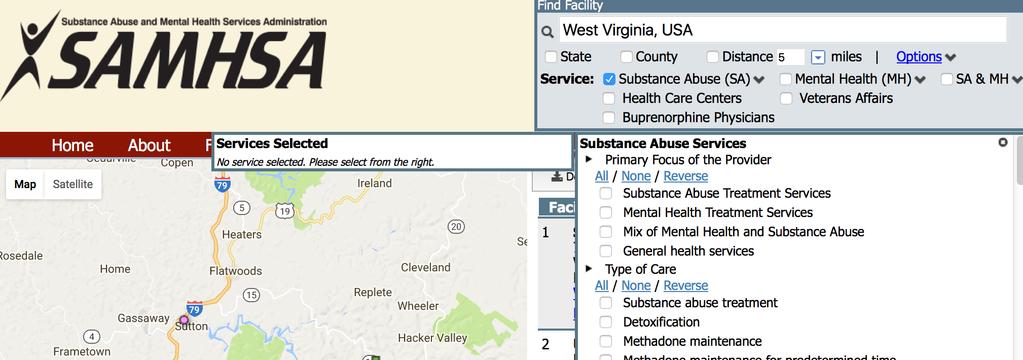
45 Referral to treatment Check SAMHSA treatment locator Look into your local treatment centers Ask to visit Talk to providers Ask about referral requirements/availability Ask patients about their experiences*

46

47




48 Availability Methadone providers Buprenorphine providers* West Virginia New Hampshire Kentucky * 2/3 or more of physicians with a buprenorphine waiver do not write any prescriptions
49 Within your treatment Harm reduction Reducing use Safety measures: Narcan, informing others of use CBT principles/skills training Motivational approaches (MI/MET) Triggers: people, places, and things Coping strategies
50 Within your treatment Medications Addiction medications Consider SUD when thinking about other medications State PDMP Social support for recovery Establish contact with family/other treatment providers Social skills and practice
51 The role of supports in recovery Joseph video #19
52 But what if they?
53 Problem situations Active drug use interfering with recovery goals Denial of drug use Acute drug use Ongoing drug use Nonadherence to treatment goals Refusal to attend treatment Inadequate treatment Concern about relapse
54 Active drug use Acute vs. chronic drug use Consider alcohol, prescription and illicit drugs Use non-stigmatizing language Drug-affected instead of high Describe concerning objective behaviors Your eyes are closing while I m talking, and I m worried you re not able to fully focus on this meeting. You haven t attended the medical appointments that you said you would.
55 Active drug use Ask! What do you think the problem is? The benzodiazepines you re taking could be affecting your memory. How many have you taken? Have you taken anything that could be affecting you in that way? Join together to solve the problem If taking those medications makes you so tired, what do you think you could do differently?
56 Active drug use Don t engage with severely drug-affected people Be very directive; focus on safety Postpone discussion about concerns until they are alert and aware Potential for overdose if Not arousable Acute medical problem: vomiting, seizures Get immediate help Acute drug use is similar to acute suicidality!
57 Nonadherence to treatment Motivational approach to explore ideas Encourage SUD treatment if needed Support SUD treatment goals Attendance for counseling, medication Self-help groups Offer to coordinate care Special release of information
58 Concern about relapse Lapses and relapses are common and don t indicate failure Ask! Cravings, triggers, any lapses Provide support Engagement/reengagement with treatment Shorter is better help to shorten relapses!
59 What you can do Be aware of your own assumptions Conceptualize the problem accurately SBIRT Encourage harm reduction Use CBT principles/skills Consider and monitor medication Encourage recovery-oriented social support Recognize and address problems
60 Take home points 1. You are already treating people with substance use disorders 2. You know more than you think you do

61 Thank you Jessica M. Peirce, Ph.D.
7/7/2016 Journal of the American Medical Association,
 1 2 Journal of the American Medical Association, 2008 3 The Clinical Trial 152 Adolescents and Young Adults (Age 15 to 21) randomly assigned to either; 1. 2 weeks of Buprenorphine detox 2. 12 weeks of
1 2 Journal of the American Medical Association, 2008 3 The Clinical Trial 152 Adolescents and Young Adults (Age 15 to 21) randomly assigned to either; 1. 2 weeks of Buprenorphine detox 2. 12 weeks of
Minneapolis VA s Intensive Outpatient Program (IOP): Screening, Treating, and Tracking Veterans
: Screening, Treating, and Tracking Veterans") Minneapolis VA s Intensive Outpatient Program (IOP): Screening, Treating, and Tracking Veterans Stephanie Bertucci, LICSW, IOP Coordinator Marcus Moore, Certified Peer Specialist Daniel Silversmith, PsyD,
Minneapolis VA s Intensive Outpatient Program (IOP): Screening, Treating, and Tracking Veterans Stephanie Bertucci, LICSW, IOP Coordinator Marcus Moore, Certified Peer Specialist Daniel Silversmith, PsyD,
A MULTI-LAYERED APPROACH TO RECOVERY: VETERAN AND MILITARY FAMILY CASE EXAMPLES
 A MULTI-LAYERED APPROACH TO RECOVERY: VETERAN AND MILITARY FAMILY CASE EXAMPLES Heather Kapson, PhD Ann Stewart, LICSW September 18, 2017 DISCLOSURES None HOME BASE PROGRAM Red Sox Foundation and Massachusetts
A MULTI-LAYERED APPROACH TO RECOVERY: VETERAN AND MILITARY FAMILY CASE EXAMPLES Heather Kapson, PhD Ann Stewart, LICSW September 18, 2017 DISCLOSURES None HOME BASE PROGRAM Red Sox Foundation and Massachusetts
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Substance Use Disorders in Primary Care
 Substance Use Disorders in Primary Care Jin Hee Yoon-Hudman, MD Assistant Vice President, Medical Director, Behavioral Health Healthfirst Fall Symposium Prevention as a Priority in Value-Based Healthcare,
Substance Use Disorders in Primary Care Jin Hee Yoon-Hudman, MD Assistant Vice President, Medical Director, Behavioral Health Healthfirst Fall Symposium Prevention as a Priority in Value-Based Healthcare,
RECOMMENDATIONS FOR HEALTH CARE PROVIDERS
 Ending Addiction Changes Everything RECOMMENDATIONS FOR HEALTH CARE PROVIDERS CRITICAL ADDICTION PREVENTION, TREATMENT AND MANAGEMENT SERVICES TO INCLUDE IN ROUTINE HEALTH CARE PRACTICE JULY 2013 In the
Ending Addiction Changes Everything RECOMMENDATIONS FOR HEALTH CARE PROVIDERS CRITICAL ADDICTION PREVENTION, TREATMENT AND MANAGEMENT SERVICES TO INCLUDE IN ROUTINE HEALTH CARE PRACTICE JULY 2013 In the
WHAT CAN I EXPECT?: DUAL SUBSTANCE USE AND MENTAL HEALTH TREATMENT FOR MILITARY POPULATIONS
 WHAT CAN I EXPECT?: DUAL SUBSTANCE USE AND MENTAL HEALTH TREATMENT FOR MILITARY POPULATIONS René Lento, PhD Lauren Brenner, PhD September 25, 2018 DISCLOSURES None HOME BASE PROGRAM 3 LEARNING OBJECTIVES
WHAT CAN I EXPECT?: DUAL SUBSTANCE USE AND MENTAL HEALTH TREATMENT FOR MILITARY POPULATIONS René Lento, PhD Lauren Brenner, PhD September 25, 2018 DISCLOSURES None HOME BASE PROGRAM 3 LEARNING OBJECTIVES
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates
 and Medication Assisted Treatment (MAT) for Opiates") Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Treatment Team Approaches in Substance Abuse Treatment
 Treatment Team Approaches in Substance Abuse Treatment PLANT A SEED AND WATCH IT GROW 2 Substance use disorders span a wide variety of problems arising from substance use, and cover 11 different criteria:
Treatment Team Approaches in Substance Abuse Treatment PLANT A SEED AND WATCH IT GROW 2 Substance use disorders span a wide variety of problems arising from substance use, and cover 11 different criteria:
Treatment Approaches for Drug Addiction
 Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
BASIC VOLUME. Elements of Drug Dependence Treatment
 BASIC VOLUME Elements of Drug Dependence Treatment Module 2 Motivating clients for treatment and addressing resistance Basic counselling skills for drug dependence treatment Special considerations when
BASIC VOLUME Elements of Drug Dependence Treatment Module 2 Motivating clients for treatment and addressing resistance Basic counselling skills for drug dependence treatment Special considerations when
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
AODA RECOVERY. How to support those in recovery, and those not yet ready to commit
 AODA RECOVERY How to support those in recovery, and those not yet ready to commit YOUR PRESENTER TODAY Robin Lickel is a psychotherapist and addictions specialist at Journey Mental Health Center in Madison,
AODA RECOVERY How to support those in recovery, and those not yet ready to commit YOUR PRESENTER TODAY Robin Lickel is a psychotherapist and addictions specialist at Journey Mental Health Center in Madison,
Making Referrals. Welcome to the Recovery U module on making referrals.
 Making Referrals Welcome to the Recovery U module on making referrals. By the end of this learning module, you ll be able to describe referral resource options for patients with substance use disorders,
Making Referrals Welcome to the Recovery U module on making referrals. By the end of this learning module, you ll be able to describe referral resource options for patients with substance use disorders,
Screening, Identification, Counseling, and Treatment of Opioid Use Disorder
 Screening, Identification, Counseling, and Treatment of Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry, Harvard Medical School Director, Division of Addiction Psychiatry, Brigham
Screening, Identification, Counseling, and Treatment of Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry, Harvard Medical School Director, Division of Addiction Psychiatry, Brigham
The science of the mind: investigating mental health Treating addiction
 The science of the mind: investigating mental health Treating addiction : is a Consultant Addiction Psychiatrist. She works in a drug and alcohol clinic which treats clients from an area of London with
The science of the mind: investigating mental health Treating addiction : is a Consultant Addiction Psychiatrist. She works in a drug and alcohol clinic which treats clients from an area of London with
Medication for Addiction Treatment (MAT)
") SBIRT Training Screening, Brief Intervention & Referral to Treatment Medication for Addiction Treatment (MAT) The Faith & Spirituality Integrated SBIRT Network Navigating the Training Welcome! These health
SBIRT Training Screening, Brief Intervention & Referral to Treatment Medication for Addiction Treatment (MAT) The Faith & Spirituality Integrated SBIRT Network Navigating the Training Welcome! These health
NURSING FOLLOW-UP: BUPRENORPHINE/NALOXONE BUPRENORPHINE/NALOXONE CLINIC VISITS
 Provider Name: NURSING FOLLOW-UP: BUPRENORPHINE/NALOXONE Provider Signature: Date: BUPRENORPHINE/NALOXONE CLINIC VISITS Once stable, schedule clinic visits every 2 to 4 weeks, with refills that coincide
Provider Name: NURSING FOLLOW-UP: BUPRENORPHINE/NALOXONE Provider Signature: Date: BUPRENORPHINE/NALOXONE CLINIC VISITS Once stable, schedule clinic visits every 2 to 4 weeks, with refills that coincide
Addiction Medicine: What s new for primary care
 Addiction Medicine: What s new for primary care Dan Vinson, MD Family and Community Medicine How to talk so our patients listen, and listen so our patients talk. 1 2 Comfortably engaging your patient in
Addiction Medicine: What s new for primary care Dan Vinson, MD Family and Community Medicine How to talk so our patients listen, and listen so our patients talk. 1 2 Comfortably engaging your patient in
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
What is Measurement Based Care?
 ur agenda Background & Development of the BAM What is the BAM? Contents, Administration, Scoring Who gets the BAM and when do they get it? Treatment Planning Integrating the BAM into your practice and
ur agenda Background & Development of the BAM What is the BAM? Contents, Administration, Scoring Who gets the BAM and when do they get it? Treatment Planning Integrating the BAM into your practice and
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc.
 Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc. Elements Behavioral Health Diplomate, American Board of Addiction
Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc. Elements Behavioral Health Diplomate, American Board of Addiction
Trigger. Myths About the Use of Medication in Recovery BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS
 BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module VI Counseling Buprenorphine Patients Myths About the Use of Medication in Recovery! Patients are still addicted!
BUPRENORPHINE TREATMENT: A TRAINING FOR MULTIDISCIPLINARY ADDICTION PROFESSIONALS Module VI Counseling Buprenorphine Patients Myths About the Use of Medication in Recovery! Patients are still addicted!
POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE MARK DUNCAN, MD November 8, 2018 SPEAKER
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE MARK DUNCAN, MD November 8, 2018 SPEAKER
Alcoholism has been demonstrated to have a genetic component, especially among men.
 Causes and Treatment of Substance-Related Disorders (Chapter 10) Familial and Genetic Influences Alcoholism has been demonstrated to have a genetic component, especially among men. Seems to be a common
Causes and Treatment of Substance-Related Disorders (Chapter 10) Familial and Genetic Influences Alcoholism has been demonstrated to have a genetic component, especially among men. Seems to be a common
Screening and Addressing Alcohol Use In Primary Care
 Screening and Addressing Alcohol Use In Primary Care Mark R. Loush, LMSW, CAADC August 15, 20167 Objectives Identify the primary reasons why screening for alcohol in primary care is important Understand
Screening and Addressing Alcohol Use In Primary Care Mark R. Loush, LMSW, CAADC August 15, 20167 Objectives Identify the primary reasons why screening for alcohol in primary care is important Understand
VOLUME B. Elements of Psychological Treatment
 VOLUME B Elements of Psychological Treatment VOLUME B MODULE 1 Drug dependence and basic counselling skills Biology of drug dependence Principles of drug dependence treatment Basic counselling skills for
VOLUME B Elements of Psychological Treatment VOLUME B MODULE 1 Drug dependence and basic counselling skills Biology of drug dependence Principles of drug dependence treatment Basic counselling skills for
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment
 an informational booklet for opioid pain treatment") ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI)
") OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI) Case 105- Prep Materials University of Massachusetts Medical School Opioid Conscious Curriculum Learner Prep Objectives The purpose of this prep material
OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI) Case 105- Prep Materials University of Massachusetts Medical School Opioid Conscious Curriculum Learner Prep Objectives The purpose of this prep material
BASIC VOLUME. Elements of Drug Dependence Treatment
 BASIC VOLUME Elements of Drug Dependence Treatment BASIC VOLUME MODULE 1 Drug dependence concept and principles of drug treatment MODULE 2 Motivating clients for treatment and addressing resistance MODULE
BASIC VOLUME Elements of Drug Dependence Treatment BASIC VOLUME MODULE 1 Drug dependence concept and principles of drug treatment MODULE 2 Motivating clients for treatment and addressing resistance MODULE
Associate Medical Director of Addiction Medicine, Summa Physicians Inc., Akron, OH Medical Director Esper Treatment Center, Erie, PA Chief Medical
 Associate Medical Director of Addiction Medicine, Summa Physicians Inc., Akron, OH Medical Director Esper Treatment Center, Erie, PA Chief Medical Officer, Interval Brotherhood Home, Akron, OH Director
Associate Medical Director of Addiction Medicine, Summa Physicians Inc., Akron, OH Medical Director Esper Treatment Center, Erie, PA Chief Medical Officer, Interval Brotherhood Home, Akron, OH Director
Can 12 Step and Medications for Substance Use Disorders Co-Exist?
 Can 12 Step and Medications for Substance Use Disorders Co-Exist? Laura G. Kehoe, MD, MPH Medical Director, Substance Use Disorders Unit Bridge Clinic Massachusetts General Hospital Overview Brief overview
Can 12 Step and Medications for Substance Use Disorders Co-Exist? Laura G. Kehoe, MD, MPH Medical Director, Substance Use Disorders Unit Bridge Clinic Massachusetts General Hospital Overview Brief overview
Here are a few ideas to help you cope and get through this learning period:
 Coping with Diabetes When you have diabetes you may feel unwell and have to deal with the fact that you have a life long disease. You also have to learn about taking care of yourself. You play an active
Coping with Diabetes When you have diabetes you may feel unwell and have to deal with the fact that you have a life long disease. You also have to learn about taking care of yourself. You play an active
What Is Heroin? Examples of Opioids. What Science Says about Opioid Use Disorder and Its Treatment 6/27/2016
 What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
Psychosocial Treatments for Opioid Use Disorder Overview
 Psychosocial Treatments for Opioid Use Disorder Overview Nalan Ward, MD Director Outpatient Addiction Services Department of Psychiatry Massachusetts General Hospital *Images used for educational purposes
Psychosocial Treatments for Opioid Use Disorder Overview Nalan Ward, MD Director Outpatient Addiction Services Department of Psychiatry Massachusetts General Hospital *Images used for educational purposes
William H. Swiggart, MS
 William H. Swiggart, MS Co-Director, Center for Professional Health Vanderbilt University Medical Center 2015 All rights reserved. I have no financial relationships to disclose. The purpose of this session
William H. Swiggart, MS Co-Director, Center for Professional Health Vanderbilt University Medical Center 2015 All rights reserved. I have no financial relationships to disclose. The purpose of this session
WHAT ARE SOME BEHAVIORAL STRATEGIES TO HELP MY PATIENT STAY SOBER?
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHAT ARE SOME BEHAVIORAL STRATEGIES TO HELP MY PATIENT STAY SOBER? MARK DUNCAN MD ADD RELAPSE PREVENTION PLAN SPEAKER
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHAT ARE SOME BEHAVIORAL STRATEGIES TO HELP MY PATIENT STAY SOBER? MARK DUNCAN MD ADD RELAPSE PREVENTION PLAN SPEAKER
Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry
 Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry In broad terms, substance use disorders occur when a substance is used in a compulsive manner with a lack of control over
Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry In broad terms, substance use disorders occur when a substance is used in a compulsive manner with a lack of control over
Practitioner Guidelines for Enhanced IMR for COD Handout #2: Practical Facts About Mental Illness
 Chapter II Practitioner Guidelines for Enhanced IMR for COD Handout #2: Practical Facts About Mental Illness There are four handouts to choose from, depending on the client and his or her diagnosis: 2A:
Chapter II Practitioner Guidelines for Enhanced IMR for COD Handout #2: Practical Facts About Mental Illness There are four handouts to choose from, depending on the client and his or her diagnosis: 2A:
The Impaired Professional. Peter Cohen, D.O.
 The Impaired Professional Peter Cohen, D.O. Definition The American Medical Association (AMA) defines impairment as the inability to practice medicine with reasonable skill and safety to patients by reason
The Impaired Professional Peter Cohen, D.O. Definition The American Medical Association (AMA) defines impairment as the inability to practice medicine with reasonable skill and safety to patients by reason
Choosing Life: Empowerment, Action, Results! CLEAR Menu Sessions. Substance Use Risk 2: What Are My External Drug and Alcohol Triggers?
 Choosing Life: Empowerment, Action, Results! CLEAR Menu Sessions Substance Use Risk 2: What Are My External Drug and Alcohol Triggers? This page intentionally left blank. What Are My External Drug and
Choosing Life: Empowerment, Action, Results! CLEAR Menu Sessions Substance Use Risk 2: What Are My External Drug and Alcohol Triggers? This page intentionally left blank. What Are My External Drug and
PHARMACOTHERAPY: INTEGRATING NEW TOOLS INTO PRACTICE
 NAADAC S 2007 LIFE-LONG LEARNING SERIES PHARMACOTHERAPY: INTEGRATING NEW TOOLS INTO PRACTICE Participant s Reference Guide and Workbook presented by: NAADAC, the Association for Addiction Professionals
NAADAC S 2007 LIFE-LONG LEARNING SERIES PHARMACOTHERAPY: INTEGRATING NEW TOOLS INTO PRACTICE Participant s Reference Guide and Workbook presented by: NAADAC, the Association for Addiction Professionals
ROSC & MAT II: Opioid Treatment Services
 ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
ROSC & MAT II: Opioid Treatment Services September 23, 2015 Stan DeKemper Executive Director Indiana Credentialing Association on Addiction and Drug Abuse 1 GOALS Review medication assisted recovery Identify
Improving Outcomes in Methadone Treatment
 Improving Outcomes in Methadone Treatment Cognitive/Behavioral Treatment Contingency Management Michael J. McCann, MA Matrix Institute on Addictions COMP Symposium September 11, 2007 Overview of Presentation
Improving Outcomes in Methadone Treatment Cognitive/Behavioral Treatment Contingency Management Michael J. McCann, MA Matrix Institute on Addictions COMP Symposium September 11, 2007 Overview of Presentation
Insight Addictionary
 Insight Addictionary This resource contains a range of definitions of common clinical terms in the alcohol and drug sector and suggested ways that they can be explained to clients. It has been developed
Insight Addictionary This resource contains a range of definitions of common clinical terms in the alcohol and drug sector and suggested ways that they can be explained to clients. It has been developed
Your Child s Treatment Roadmap
 Your Child s Treatment Roadmap The road to recovery isn t the same for everyone. There are many options to consider for your son, daughter, or loved one. Our guide outlines key steps to help you make the
Your Child s Treatment Roadmap The road to recovery isn t the same for everyone. There are many options to consider for your son, daughter, or loved one. Our guide outlines key steps to help you make the
Opioid Use Disorder Treatment Initiation in Diverse Settings
 Opioid Use Disorder Treatment Initiation in Diverse Settings Sarah Wakeman, MD, FASAM Medical Director, Mass General Substance Use Disorder Initiative Assistant Professor, Harvard Medical School Disclosures
Opioid Use Disorder Treatment Initiation in Diverse Settings Sarah Wakeman, MD, FASAM Medical Director, Mass General Substance Use Disorder Initiative Assistant Professor, Harvard Medical School Disclosures
Stigma, Myths, Realities Limit Access to Care
 Stigma, Myths, Realities Limit Access to Care MARGARET RUKSTALIS, MD Director ACGME Addiction Medicine Fellowship @ Wake Forest School of Medicine No personal or family conflicts of interest or history
Stigma, Myths, Realities Limit Access to Care MARGARET RUKSTALIS, MD Director ACGME Addiction Medicine Fellowship @ Wake Forest School of Medicine No personal or family conflicts of interest or history
IDDT Fidelity Action Planning Guidelines
 1a. Multidisciplinary Team IDDT Fidelity Action Planning Guidelines Definition: All clients targeted for IDDT receive care from a multidisciplinary team. A multi-disciplinary team consists of, in addition
1a. Multidisciplinary Team IDDT Fidelity Action Planning Guidelines Definition: All clients targeted for IDDT receive care from a multidisciplinary team. A multi-disciplinary team consists of, in addition
9/17/2018 MISSION IMPOSSIBLE: IF YOU CHOOSE TO ACCEPT MISSION JOIN JUSTICE LEAGUE I M POSSIBLE HEPBURN
 MISSION IMPOSSIBLE: IF YOU CHOOSE TO ACCEPT MISSION JOIN JUSTICE LEAGUE I M POSSIBLE HEPBURN 1 ADDICTION PREVENTION & TREATMENT SAVES LIVES According to the Food and Drug Administration s standards for
MISSION IMPOSSIBLE: IF YOU CHOOSE TO ACCEPT MISSION JOIN JUSTICE LEAGUE I M POSSIBLE HEPBURN 1 ADDICTION PREVENTION & TREATMENT SAVES LIVES According to the Food and Drug Administration s standards for
BASIC VOLUME. Elements of Drug Dependence Treatment
 BASIC VOLUME Elements of Drug Dependence Treatment Module 3 Principles of CBT and relapse prevention strategies Introduction to Cognitive Behavioural Therapy Basics of pharmacological treatment Workshop
BASIC VOLUME Elements of Drug Dependence Treatment Module 3 Principles of CBT and relapse prevention strategies Introduction to Cognitive Behavioural Therapy Basics of pharmacological treatment Workshop
Welcome to the Opioid Overdose Prevention Project
 Welcome to the Opioid Overdose Prevention Project Narcan Training TODAY S OBJECTIVES Define drug addiction Identify symptoms of addiction Treatment options including support for family members How to recognize
Welcome to the Opioid Overdose Prevention Project Narcan Training TODAY S OBJECTIVES Define drug addiction Identify symptoms of addiction Treatment options including support for family members How to recognize
Note: The trainings below represent a foundational list, and may be adapted based on audience and need.
 MOTIVATIONAL INTERVIEWING Introduction to Motivational Interviewing (offered in English and Spanish) 2-day Course (12-14 credit hours) This course is designed to introduce clinicians and staff members
MOTIVATIONAL INTERVIEWING Introduction to Motivational Interviewing (offered in English and Spanish) 2-day Course (12-14 credit hours) This course is designed to introduce clinicians and staff members
Medication Assisted Treatment
 Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
8/5/2013. MOSBIRT Annual Training The Big change in addiction medicine? Before we dive into pharmacotherapy
 Medication Assisted Treatment for Substance Abuse in Primary Care Dan Vinson August 1, 2013 1 The Big change in addiction medicine? These diseases are rapidly becoming medical diseases. Done are the days
Medication Assisted Treatment for Substance Abuse in Primary Care Dan Vinson August 1, 2013 1 The Big change in addiction medicine? These diseases are rapidly becoming medical diseases. Done are the days
Borderline Personality Disorder and Substance Use. Australian BPD Foundation 6th Annual National Conference Achieving Recovery Together Sydney, 2016
 Borderline Personality Disorder and Substance Use Chris Willcox Head of Psychology Hunter New England Mental Health Conjoint Associate Professor School of Psychology, University of Newcastle Australian
Borderline Personality Disorder and Substance Use Chris Willcox Head of Psychology Hunter New England Mental Health Conjoint Associate Professor School of Psychology, University of Newcastle Australian
Buprenorphine & Controlled Substance Treatment Agreement
 Buprenorphine & Controlled Substance Treatment Agreement I agree to accept the following treatment contract for buprenorphine office-based opioid addiction treatment: 1. I will keep my medication in a
Buprenorphine & Controlled Substance Treatment Agreement I agree to accept the following treatment contract for buprenorphine office-based opioid addiction treatment: 1. I will keep my medication in a
Dr. Oslin receives grant support from the NIH, VA, and the Pennsylvania Department of Aging.
 David W. Oslin, MD University of Pennsylvania Philadelphia VAMC Dr. Oslin receives grant support from the NIH, VA, and the Pennsylvania Department of Aging. Dr. Oslin is a consultant to the Hazelden Betty
David W. Oslin, MD University of Pennsylvania Philadelphia VAMC Dr. Oslin receives grant support from the NIH, VA, and the Pennsylvania Department of Aging. Dr. Oslin is a consultant to the Hazelden Betty
Effective Treatment: Doing the Right Thing, In the Right Way. Terrence D Walton, MSW, ICADC
 Effective Treatment: Doing the Right Thing, In the Right Way Terrence D Walton, MSW, ICADC Monitor Manage Impact 1. Understand the Treatment Field, including Evidenced Based Practices 2. Understand Your
Effective Treatment: Doing the Right Thing, In the Right Way Terrence D Walton, MSW, ICADC Monitor Manage Impact 1. Understand the Treatment Field, including Evidenced Based Practices 2. Understand Your
Medicated Assisted Treatment
 Medicated Assisted Treatment Enhancing the Potential for Recovery Part I Diana Padilla Program Manager NeC-ATTC 2 Diana Padilla, RCR, CASAC-T padilla@ndri.org Diana Padilla is a program manager at NDRI-USA,
Medicated Assisted Treatment Enhancing the Potential for Recovery Part I Diana Padilla Program Manager NeC-ATTC 2 Diana Padilla, RCR, CASAC-T padilla@ndri.org Diana Padilla is a program manager at NDRI-USA,
Vivitrol/Suboxone. Comparison Study Summary
 Vivitrol/Suboxone Comparison Study Summary Lee, J. D., Nunes, E. V., Novo, P., Bachrach, K., Bailey, G. L., Bhatt, S., & King, J. (2017). Comparative effectiveness of extended-release naltrexone versus
Vivitrol/Suboxone Comparison Study Summary Lee, J. D., Nunes, E. V., Novo, P., Bachrach, K., Bailey, G. L., Bhatt, S., & King, J. (2017). Comparative effectiveness of extended-release naltrexone versus
Main Questions. Why study addiction? Substance Use Disorders, Part 1 Alecia Schweinsburg, MA Abnromal Psychology, Fall Substance Use Disorders
 Substance Use Disorders Main Questions Why study addiction? What is addiction? Why do people become addicted? What do alcohol and drugs do? How do we treat substance use disorders? Why study addiction?
Substance Use Disorders Main Questions Why study addiction? What is addiction? Why do people become addicted? What do alcohol and drugs do? How do we treat substance use disorders? Why study addiction?
MEDICATION ASSISTED ADDICTION TREATMENT: Appropriate Use
 MEDICATION ASSISTED ADDICTION TREATMENT: Appropriate Use Louis E. Baxter, Sr., M.D., DFASAM Executive Medical Director-PAPNJ Assistant Clinical Professor Medicine Rutgers New Jersey Medical School DMHAS-Addiction
MEDICATION ASSISTED ADDICTION TREATMENT: Appropriate Use Louis E. Baxter, Sr., M.D., DFASAM Executive Medical Director-PAPNJ Assistant Clinical Professor Medicine Rutgers New Jersey Medical School DMHAS-Addiction
What I Want From Treatment User Information
 What I Want From Treatment User Information The tailoring to treatment to individual needs has long been lauded, but often it is designing treatment to what the counselor thinks the client needs. This
What I Want From Treatment User Information The tailoring to treatment to individual needs has long been lauded, but often it is designing treatment to what the counselor thinks the client needs. This
NALTREXONE DAVID CRABTREE, MD, MPH UNIVERSITY OF UTAH HEALTH, 2018
 NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
Arwen Podesta, MD. ABIHM, ABAM, Forensic Psychiatry
 The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
Treating Opioid Addiction
 Treating Opioid Addiction Some people who start taking opioid pain medications eventually have serious problems with them and become addicted. Every day, 68 people die in the US from opioid overdose. More
Treating Opioid Addiction Some people who start taking opioid pain medications eventually have serious problems with them and become addicted. Every day, 68 people die in the US from opioid overdose. More
Referral to Treatment: Utilizing the ASAM Criteria
 Referral to Treatment: Utilizing the ASAM Criteria AOAAM Essentials in Addiction Medicine October 22, 2016 East Lansing, MI Stephen A. Wyatt, DO Medical Director, Addiction Medicine Behavioral Health Service
Referral to Treatment: Utilizing the ASAM Criteria AOAAM Essentials in Addiction Medicine October 22, 2016 East Lansing, MI Stephen A. Wyatt, DO Medical Director, Addiction Medicine Behavioral Health Service
Session outline. Introduction to depression Assessment of depression Management of depression Follow-up Review
 Depression 1 Session outline Introduction to depression Assessment of depression Management of depression Follow-up Review 2 Activity 1: Person s story followed by group discussion Present the first person
Depression 1 Session outline Introduction to depression Assessment of depression Management of depression Follow-up Review 2 Activity 1: Person s story followed by group discussion Present the first person
Welcome to the second module of the Screening, Brief Intervention, and Referral to Treatment Core Curriculum. In this module, we ll address screening
 Welcome to the second module of the Screening, Brief Intervention, and Referral to Treatment Core Curriculum. In this module, we ll address screening patients for substance use in a clinical setting. 1
Welcome to the second module of the Screening, Brief Intervention, and Referral to Treatment Core Curriculum. In this module, we ll address screening patients for substance use in a clinical setting. 1
Intermountain Healthcare
 Intermountain Healthcare Suicide Assessment/ Prevention Substance Use Disorder Managment 2015 Updates Carolyn Tometich PMHNP-BC BHCP Operations Director Why Focus On Substance Use Disorder? Addiction often
Intermountain Healthcare Suicide Assessment/ Prevention Substance Use Disorder Managment 2015 Updates Carolyn Tometich PMHNP-BC BHCP Operations Director Why Focus On Substance Use Disorder? Addiction often
Management of high risk MMT patients. Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013
 Management of high risk MMT patients Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013 CFPC CoI Templates: Slide 1 Faculty Disclosure Faculty: Meldon Kahan Relationships with commercial
Management of high risk MMT patients Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013 CFPC CoI Templates: Slide 1 Faculty Disclosure Faculty: Meldon Kahan Relationships with commercial
Anyone Can Become Addicted. Anyone.
 Anyone Can Become Addicted. Anyone. PAStop.org Family Toolkit Seeking Drug Abuse Treatment: Know What to Ask Trying to identify the right treatment programs for a loved one can be a difficult process.
Anyone Can Become Addicted. Anyone. PAStop.org Family Toolkit Seeking Drug Abuse Treatment: Know What to Ask Trying to identify the right treatment programs for a loved one can be a difficult process.
OPIOID USE DISORDER (OUD) TREATMENT IN A PATIENT CENTERED HEALTH CENTER
 TREATMENT IN A PATIENT CENTERED HEALTH CENTER") OPIOID USE DISORDER (OUD) TREATMENT IN A PATIENT CENTERED HEALTH CENTER Ed Johnson M.Ed., MAC, LPC, CCS Associate Director, Training & Technical Assistance Southeast Addiction Technology Transfer Center
OPIOID USE DISORDER (OUD) TREATMENT IN A PATIENT CENTERED HEALTH CENTER Ed Johnson M.Ed., MAC, LPC, CCS Associate Director, Training & Technical Assistance Southeast Addiction Technology Transfer Center
NIDA Principles of Treatment. NIDA Principles of Treatment. Peter Banys, M.D., M.Sc. No single treatment is appropriate for all individuals.
 NIDA Principles of Treatment Peter Banys, M.D., M.Sc. CSAM Addiction Medicine Review Course San Francisco October 5 th, 2006 NIDA Principles of Treatment 1. Treatment Matching 2. Availability 3. Domains
NIDA Principles of Treatment Peter Banys, M.D., M.Sc. CSAM Addiction Medicine Review Course San Francisco October 5 th, 2006 NIDA Principles of Treatment 1. Treatment Matching 2. Availability 3. Domains
V. EVIDENCE-BASED APPROACHES TO TREATING ADOLESCENT SUBSTANCE USE DISORDERS
 V. EVIDENCE-BASED APPROACHES TO TREATING ADOLESCENT SUBSTANCE USE DISORDERS R esearch evidence supports the effectiveness of various substance abuse treatment approaches for adolescents. Examples of specific
V. EVIDENCE-BASED APPROACHES TO TREATING ADOLESCENT SUBSTANCE USE DISORDERS R esearch evidence supports the effectiveness of various substance abuse treatment approaches for adolescents. Examples of specific
THE STATE OF MEDICINE IN ADDICTION RECOVERY
 OVERVIEW: Review addiction stats and trends Define addiction Explain neurobiology of addiction Review treatments of addiction Addiction Definition: A Primary, chronic, relapsing disease of brain reward,
OVERVIEW: Review addiction stats and trends Define addiction Explain neurobiology of addiction Review treatments of addiction Addiction Definition: A Primary, chronic, relapsing disease of brain reward,
HELPING PEOPLE STOP SMOKING
 HELPING PEOPLE STOP SMOKING Using motivational interviewing skills JENNIFER PERCIVAL RGN. RM.RHV. FETC Counselling Dip RCN TOBACCO POLICY ADVISOR TOBACCO IS A SERIOUS PROBLEM In the year 2000 1 in every
HELPING PEOPLE STOP SMOKING Using motivational interviewing skills JENNIFER PERCIVAL RGN. RM.RHV. FETC Counselling Dip RCN TOBACCO POLICY ADVISOR TOBACCO IS A SERIOUS PROBLEM In the year 2000 1 in every
Understanding Medication in Addiction Treatment for Drug Court Participants
 Understanding Medication in Addiction Treatment for Drug Court Participants Introduction This pocket guide is for drug court participants who may be prescribed or considering medication as a part of addiction
Understanding Medication in Addiction Treatment for Drug Court Participants Introduction This pocket guide is for drug court participants who may be prescribed or considering medication as a part of addiction
Substance Abuse and Brain Injury: A Toxic Mix
 Substance Abuse and Brain Injury: A Toxic Mix BIANJ Annual Seminar May 18, 2017 Scott Peters MS, OTR/L speters@remed.com TBI and Substance Abuse (Ohio Valley Center for Brain Injury Prevention and Treatment)
Substance Abuse and Brain Injury: A Toxic Mix BIANJ Annual Seminar May 18, 2017 Scott Peters MS, OTR/L speters@remed.com TBI and Substance Abuse (Ohio Valley Center for Brain Injury Prevention and Treatment)
Substance and Alcohol Related Disorders. Substance use Disorder Alcoholism Gambling Disorder
 Substance and Alcohol Related Disorders Substance use Disorder Alcoholism Gambling Disorder What is a Substance Use Disorder? According to the DSM-5, a substance use disorder describes a problematic pattern
Substance and Alcohol Related Disorders Substance use Disorder Alcoholism Gambling Disorder What is a Substance Use Disorder? According to the DSM-5, a substance use disorder describes a problematic pattern
In 2008, an estimated 282,000 persons
 National Survey of Substance Abuse Treatment Services The N-SSATS Report January 28, 2010 Similarities and Differences in Opioid Treatment Programs that Provide Methadone Maintenance or Buprenorphine Maintenance
National Survey of Substance Abuse Treatment Services The N-SSATS Report January 28, 2010 Similarities and Differences in Opioid Treatment Programs that Provide Methadone Maintenance or Buprenorphine Maintenance
MEDICATION ASSISTED TREATMENTS (MAT) FOR SUBSTANCE USE DISORDERS
 FOR SUBSTANCE USE DISORDERS") MEDICATION ASSISTED TREATMENTS (MAT) FOR SUBSTANCE USE DISORDERS PHYLLIS RAYNOR, PHD, PMHNP-BC, APRN CLINICAL ASSISTANT PROFESSOR, USC COLLEGE OF NURSING LEARNING OBJECTIVES: Define types of SUD and purposes
MEDICATION ASSISTED TREATMENTS (MAT) FOR SUBSTANCE USE DISORDERS PHYLLIS RAYNOR, PHD, PMHNP-BC, APRN CLINICAL ASSISTANT PROFESSOR, USC COLLEGE OF NURSING LEARNING OBJECTIVES: Define types of SUD and purposes
Buprenorphine 2.0: I have my waiver, now what? Dr. Ritu Bhatnagar, M.D., M.P.H. Dr. John Ewing, M.D., FASAM. Disclosures
 Buprenorphine 2.0: I have my waiver, now what? Dr. Ritu Bhatnagar, M.D., M.P.H. Dr. John Ewing, M.D., FASAM Disclosures Dr. Bhatnagar: no disclosures to report Dr. Ewing: no disclosures to report 1 Our
Buprenorphine 2.0: I have my waiver, now what? Dr. Ritu Bhatnagar, M.D., M.P.H. Dr. John Ewing, M.D., FASAM Disclosures Dr. Bhatnagar: no disclosures to report Dr. Ewing: no disclosures to report 1 Our
maintaining gains and relapse prevention
 maintaining gains and relapse prevention Introduction to maintaining gains and relapse prevention 2 Steps to success 2 Keep on doing what works to improve your mood using the skills you have learned and
maintaining gains and relapse prevention Introduction to maintaining gains and relapse prevention 2 Steps to success 2 Keep on doing what works to improve your mood using the skills you have learned and
GOALS AND OBJECTIVES
 SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
Other significant mental health complaints
 Other significant mental health complaints 2 Session outline Introduction to other significant mental health complaints Assessment of other significant mental health complaints Management of other significant
Other significant mental health complaints 2 Session outline Introduction to other significant mental health complaints Assessment of other significant mental health complaints Management of other significant
Principles and language suggestions for talking with patients
 SAFER MANAGEMENT OF OPIOIDS FOR CHRONIC PAIN: Principles and language suggestions for talking with patients Use these principles and language suggestions when discussing opioid risks and safety monitoring
SAFER MANAGEMENT OF OPIOIDS FOR CHRONIC PAIN: Principles and language suggestions for talking with patients Use these principles and language suggestions when discussing opioid risks and safety monitoring
Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention
 The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
Treatment of Youth Opioid Addiction: Approaches to a Modern Epidemic. What should we do with this case? Heroin Addiction History
 Treatment of Youth Opioid Addiction: Approaches to a Modern Epidemic What should we do with this case? 17 M Onset prescription opioids 15, progressing to daily use with withdrawal within 8 months Onset
Treatment of Youth Opioid Addiction: Approaches to a Modern Epidemic What should we do with this case? 17 M Onset prescription opioids 15, progressing to daily use with withdrawal within 8 months Onset
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
The Language of Addiction Counseling
 The Language of Addiction Counseling Geri Miller, Ph.D., LP, LCAS, LPC Appalachian State University (828)262-6048 millerga@appstate.edu The Language of Addiction Counseling The session begins with an overview
The Language of Addiction Counseling Geri Miller, Ph.D., LP, LCAS, LPC Appalachian State University (828)262-6048 millerga@appstate.edu The Language of Addiction Counseling The session begins with an overview
Note: The trainings below represent a foundational list, and may be adapted based on audience and need.
 MOTIVATIONAL INTERVIEWING Introduction to Motivational Interviewing (offered in English and Spanish) 2-day Course (12-14 credit hours) This course is designed to introduce clinicians and staff members
MOTIVATIONAL INTERVIEWING Introduction to Motivational Interviewing (offered in English and Spanish) 2-day Course (12-14 credit hours) This course is designed to introduce clinicians and staff members
Serious Mental Illness and Opioid Use Disorder
 Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
TEN early signs of a Dementia
 TEN early signs of a Dementia 1. Memory loss on a day-to-day basis Memory loss, especially forgetting things that happened only hours or days ago. forgetting important dates or events repeatedly asking
TEN early signs of a Dementia 1. Memory loss on a day-to-day basis Memory loss, especially forgetting things that happened only hours or days ago. forgetting important dates or events repeatedly asking
CMBHS Clinical Management of Behavioral Health Services
 Client: CMBHS Clinical Management of Behavioral Health Services Case Management AST022 Assessment Information Assessment Number Assessment Date Assessment Type Contact Type Assessment Site Referred By
Client: CMBHS Clinical Management of Behavioral Health Services Case Management AST022 Assessment Information Assessment Number Assessment Date Assessment Type Contact Type Assessment Site Referred By
the facts about BUPRENORPHINE for Treatment of Opioid Addiction
 the facts about BUPRENORPHINE for Treatment of Opioid Addiction i I d been shot on the streets, I d been in detox. It was jails, institutions. Death, I knew, was imminent for me so I started my recovery
the facts about BUPRENORPHINE for Treatment of Opioid Addiction i I d been shot on the streets, I d been in detox. It was jails, institutions. Death, I knew, was imminent for me so I started my recovery
TREATING OPIOID ADDICTION IN HOMELESS POPULATIONS
 TREATING OPIOID ADDICTION IN HOMELESS POPULATIONS Challenges and Opportunities Providing Medication Assisted Treatment (Buprenorphine) August 18, 2016 SPEAKERS TODAY Nilesh Kalyanaraman, MD, Chief Health
TREATING OPIOID ADDICTION IN HOMELESS POPULATIONS Challenges and Opportunities Providing Medication Assisted Treatment (Buprenorphine) August 18, 2016 SPEAKERS TODAY Nilesh Kalyanaraman, MD, Chief Health
Medication Assisted Treatment of an Opioid Use Disorder. J. Craig Allen, MD. Medical Director, Rushford
 Medication Assisted Treatment of an Opioid Use Disorder J. Craig Allen, MD. Medical Director, Rushford Learning objectives At the conclusion of this activity, participants will be able to: Understand
Medication Assisted Treatment of an Opioid Use Disorder J. Craig Allen, MD. Medical Director, Rushford Learning objectives At the conclusion of this activity, participants will be able to: Understand