Drug Metabolism. Assoc. Prof. Bilgen Basgut 2015
|
|
|
- Frank Simmons
- 5 years ago
- Views:
Transcription
1 Drug Metabolism Assoc. Prof. Bilgen Basgut
2 Introduction Biotransformation: Chemical alteration of the drug in body that converts nonpolar or lipid soluble compounds to polar or lipid insoluble compounds Consequences of biotransformation Active drug Inactive metabolite : Pentobarbitone, Morphine, Chloramphenicol Active drug Active metabolite: Phenacetin Inactive drug active metabolite: Levodopa 2
3 Prodrugs Inactive drug is converted to active metabolite Coined by Albert in 1958 Advantages: Increased absorption Elimination of an unpleasant taste Decreased toxicity Decreased metabolic inactivation Increased chemical stability Prolonged or shortened action 3
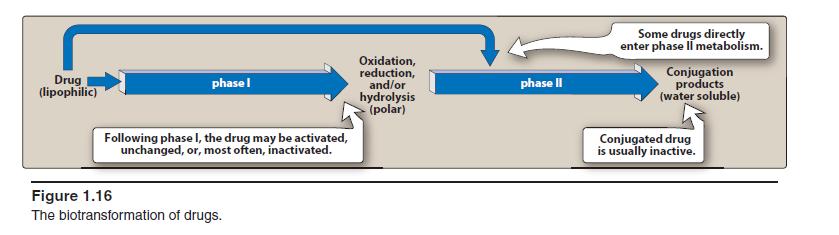
4 Phases of Metabolism Phase I Functionalization reactions Converts the parent drug to a more polar metabolite by introducing or unmasking a functional group (-OH, -NH2, -SH). Phase II Conjugation reactions Subsequent reaction in which a covalent linkage is formed between a functional group on the parent compound or Phase I metabolite and an endogenous substrate such as glucuronic acid, sulfate, acetate, or an amino acid 4
5 Phases of Metabolism Hydrolytic Reactions Phase II - Conjugation Phase I - Functionalization Oxidation Drug Metabolism Conjugation Glucuronic acid Sulfate, Glycine and other AA Glutathione or mercapturic acid Acetylation, Methylation Reduction 5
 Dr Swaroop HS")
6 Sites of Drug Metabolism Extrahepatic microsomal enzymes (oxidation, conjugation) Hepatic microsomal enzymes (oxidation, conjugation) Hepatic non-microsomal enzymes (acetylation, sulfation,gsh, alcohol/aldehyde dehydrogenase, hydrolysis, ox/red) Dr Swaroop HS copyighted 6
7 7
8 Phase I / Non Synthetic Reactions Oxidation Addition of oxygen/ negatively charged radical or removal of hydrogen/ positively charged radical. Reactions are carried out by group of monooxygenases in the liver. Final step: Involves cytochrome P-450 haemoprotein, NADPH, cytochrome P-450 reductase and O2 Dr Swaroop HS copyighted 8
9 Cytochrome P450 enzymes Monooxygenase enzyme family Major catalyst: Drug and endogenous compound oxidations in liver, kidney, G.I. tract, skin and lungs Oxidative reactions require: CYP heme protein, the reductase, NADPH, phosphatidylcholine and molecular oxygen Location: smooth endoplasmic reticulum in close association with NADPH-CYP reductase in 10/1 ratio The reductase serves as the electron source for the oxidative reaction cycle 9
10 Cytochrome P family Multiple CYP gene families have been identified in humans, and the categorized based on protein sequence homology Most of the drug metabolizing enzymes are in CYP 1, 2, & 3 families. Frequently, two or more enzymes can catalyze the same type of oxidation, indicating redundant and broad substrate specificity. CYP3A4 is very common to the metabolism of many drugs; its presence in the GI tract is responsible for poor oral bioavailability of many drugs 10
11 Cytochromes: Metabolism of Drugs CYP Enzyme Examples of substrates 1A1 1A2 2A6 2B6 Caffeine, Testosterone, R-Warfarin Acetaminophen, Caffeine, Phenacetin, R-Warfarin 17 -Estradiol, Testosterone Cyclophosphamide, Erythromycin, Testosterone 2C-family Acetaminophen, Tolbutamide (2C9); Hexobarbital, S- Warfarin (2C9,19); Phenytoin, Testosterone, R- Warfarin, Zidovudine (2C8,9,19); 2E1 2D6 3A4 Acetaminophen, Caffeine, Chlorzoxazone, Halothane Acetaminophen, Codeine, Debrisoquine Acetaminophen, Caffeine, Carbamazepine, Codeine, Cortisol, Erythromycin, Cyclophosphamide, S- and R- Warfarin, Phenytoin, Testosterone, Halothane, Zidovudine Adapted from: S. Rendic Drug Metab Rev 34: ,
12 Non-CYP Drug Oxidations Monoamine Oxidase (MAO), Diamine Oxidase (DAO) MAO (mitochondrial) oxidatively deaminates endogenous substrates including neurotransmitters Dopamine, serotonin, norepinephrine, epinephrine Alcohol & Aldehyde Dehydrogenase Non-specific enzymes found in soluble fraction of liver Ethanol metabolism Flavin Monooxygenases Require molecular oxygen, NADPH, flavin adenosine dinucleotide (FAD) 12
13 Reduction Converse of oxidation Drugs primarily reduced are chloralhydrate, chloramphenicol, halothane. 13
14 Hydrolysis Cleavage of drug molecule by taking up a molecule of water. Sites: Liver, intestines, plasma and other tissues Examples: Choline esters, Procaine, Isoniazid, pethidine, oxytocin. 14
15 Cyclization and Decyclization Cyclization Formation of ring structure from a straight chain compound E.g. Proguanil Decyclization Opening up of ring structure of the cyclic drug molecule E.g. Barbiturates, Phenytoin. 15
16 Phase II reactions Conjugation of the drug or its phase I metabolite with an endogenous substrate to form a polar highly ionized organic acid Types of phase II reactions Glucuronide conjugation Acetylation, Methylation Sulfate conjugation, Glycine conjugation Glutathione conjugation Ribonucleoside/ nucleotide synthesis 16
17 Glucuronide Conjugation Conjugation to α-d-glucuronic acid Quantitatively the most important phase II pathway for drugs and endogenous compounds Products are often excreted in the bile Requires enzyme UDP-glucuronosyltransferase (UGT) Compounds with a hydroxyl or carboxylic acid group are easily conjugated with glucuronic acid which is derived from glucose 17
18 Glucuronide Conjugation Continued.. Enterohepatic recycling may occur due to gut glucuronidases Drug glucuronides excreted in bile can be hydrolysed by bacteria in gut and reabsorbed and undergoes same fate. This recycling of the drug prolongs its action e.g.phenolphtalein, Oral contraceptives Examples: Chloramphenicol, aspirin, phenacetin, morphine, metronidazole 18
19 Acetylation Common reaction for aromatic amines and sulfonamides Requires co-factor acetyl-coa Responsible enzyme is N-acetyltransferase E.g. Sulfonamides, isoniazid, Hydralazine. 19
20 Sulfate Conjugation Major pathway for phenols but also occurs for alcohols, amines and thiols Sulfate conjugates can be hydrolyzed back to the parent compound by various sulfatases Examples include: a-methyldopa, albuterol, terbutaline, acetaminophen, phenacetin 20
21 Amino Acid Conjugation: ATP-dependent acid: CoA ligase forms active CoAamino acid conjugates which then react with drugs by N-Acetylation: Usual amino acids involved are: Glycine. Glutamine, Ornithine, Arginine Glutathione Conjugation: Glutathione is a protective factor for removal of potentially toxic compounds Conjugated compounds can subsequently be attacked by g-glutamyltranspeptidase and a peptidase to yield the cysteine conjugate => product can be further acetylated to N-acetylcysteine conjugate E.g. Paracetamol 21
22 Hofmann elimination Inactivation of the drug in the body fluids by spontaneous molecular re arrangement without the agency of any enzyme e.g. Atracurium. 22
23 First pass Metabolism Metabolism of a drug during its passage from the site of absorption into the systemic circulation. Extent of first pass metabolism differs in different drugs Extent of first pass metabolism of important drugs Low Intermediate High not given orally High oral dose Phenobarbitone Aspirin Isoprenaline propranolol Phenylbutazone Quinidine Lidocaine Alprenolol Tolbutamide Desipramine Hydrocortisone Verapamil Pindolol Nortriptyline Testosterone Salbutamol Dr Swaroop HS copyighted 23
24 Attributes of drugs with high first pass metabolism Oral dose is considerably higher then sublingual or parenteral dose Marked individual variation in the oral dose due to differences in the extent of first pass metabolism Oral bioavailability is apparently increased in patients with severe liver disease Oral bioavailability of a drug is increased if another drug competing with it. E.G. Chloropromazine and Propranolol 24
25 Inhibition of Microsomal enzymes Competitively inhibit the metabolism of another drug if it utilizes the same enzyme or co factors. A drug may inhibit one isoenzyme while being itself a substrate of another isoenzyme e.g. quinidine is metabolized by CYP3A4 but inhibits CYP2D6 Inhibition of drug metabolism occurs in a dose related manner and can precipitate toxicity of the object drug. Blood flow limited metabolism e.g. Propranolol reduces rate of lidocaine metabolism by decreasing hepatic blood flow. 25
26 Microsomal Enzyme Induction ocertain drugs, insecticides and carcinogens increase the synthesis of microsomal enzyme protein. odifferent inducers are relatively selective for certain cytochrome P-450 enzyme families e.g. Phenobarbitone, rifampin, glucorticoids induce CYP3A isoenzymes Isoniazid and chronic alochol consumption induce CYP2E1 oinduction takes 4-14 days to reach its peak and is maintained till the inducing agent is present. 26
27 Consequences of Induction Decreased intensity or Increased Intensity of action of drug Tolerance- autoinduction Interfere with adjustment of dose of another drug Interference with chronic toxicity 27
28 Some foods, other drugs, herbs, environmental agents, inhibit/induce CYP s change in metabolism drugs change drug activity Grapefruit juice, St. John s wort inhibit drug metab by inhib n CYP enz s Brusssels sprouts, cigarettes induce P450 enz s
29 Role of Metabolism in pediatric and elderly New born has low GFR and tubular transport is immature, so the t1/2 of the drug like streptomycin and penicillin is prolonged Hepatic drug metabolising system is inadequate in new borns e.g. chloramphenicol can produce gray baby syndrome In elderly the renal function progressively declines Reduction of hepatic microsomal activity and liver blood flow Incidence of adverse drug reactions is much higher in elderly 29
30 EXCRETION or ELIMINATION OF DRUGS




31 Excretion is a process whereby drugs are transferred from the internal to the external environment Despite the reduction in activity that occurs as a drug leaves its site of action, it may remain in the body for a considerable period, especially if it is strongly bound to tissue components. Excretion, along with metabolism and tissue redistribution, is important in determining both the duration of drug action and the rate of drug elimination. Principal organs involved Kidneys, Lungs, Biliary system Intestines Saliva Milk.
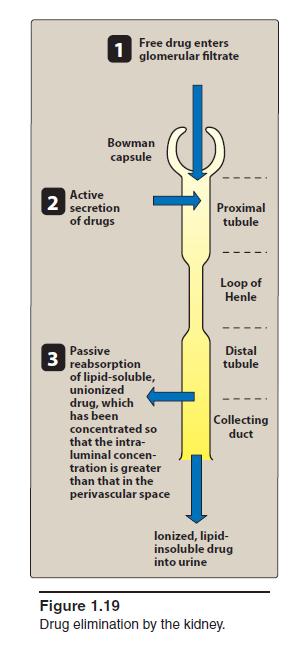
32 RENAL EXCRETION Kidney is the primary organ of removal for most drugs especially for those that are water soluble and not volatile. The three principal processes that determine the urinary excretion of a drug 1. glomerular filtration, 2. tubular secretion, and 3. tubular reabsorption (mostly passive back-diffusion)
33 33
34 Passive Diffusion Urinary excretion of drugs (i.e., weak electrolytes) is the extent to which substances diffuse back across the tubular membranes and reenter the circulation. The concentration gradient thus established will facilitate movement of the drug out of the tubular lumen, given that the lipid solubility and ionization of the drug are appropriate. The ph of the urine (usually between 4.5 and 8) can markedly affect the rate of passive back-diffusion. The back-diffusion occurs primarily in the distal tubules and collecting ducts, (most of the urine acidification takes place) Acidification increases reabsorption (or decreases elimination) of weak acids, such as salicylates, and decreases reabsorption (or promotes elimination) of weak bases, such as amphetamines.
35 Effects of ph on urinary drug elimination may have important applications, especially in cases of overdose. Eg: enhance the elimination of a barbiturate (a weak acid) by administiring bicarbonate to the patient. This procedure alkalinizes the urine and thus promotes the excretion of more completely ionized drug. Excretion of bases can be increased by making the urine more acidic through the use of an acidifying salt, such as ammonium chloride.
36 Active Tubular Secretion A number of drugs can serve as substrates for the two active secretory systems in the PCT Actively transfer drugs from blood to luminal fluid, are independent of each other; one secretes organic anions, and the other secretes organic cations. The secretory capacity of both the organic anion and organic cation secretory systems can be saturated at high drug concentrations. Each drug will have its own characteristic maximum rate of secretion (transport maximum,tm). Some drugs that are not candidates for active tubular secretion. Eg: Metabolites that are formed as a result of conjugative reactions.
37 Any drug known to be largely excreted by the kidney that has a body half-life of less than 2 hours is probably eliminated, at least in part, by tubular secretion. Some drugs can be secreted and have long half-lives, however, because of extensive passive reabsorption in distal segments of the nephron. These tubular transport mechanisms are not as well developed in the neonate as in the adult. Functional capacity may be diminished in the elderly. Compounds that undergo active tubular secretion also are filtered at the glomerulus (assuming protein binding is minimal).
38 Organic Anion Transport Acetazolamide Bile salts Hydrochlorothiazide Furosemide Indomethacin Penicillin G Prostaglandins Organic Cation Transport Acetylcholine Atropine Cimetidine Dopamine Epinephrine Morphine Neostigmine Salicylate Quinine
39 Active Tubular Reabsorption Some substances filtered at the glomerulus are reabsorbed by active transport systems found primarily in the proximal tubules. Active reabsorption is particularly important for endogenous substances, such as ions, glucose, and amino acids, although a small number of drugs also may be actively reabsorbed. The probable location of the active transport system is on the luminal side of the proximal cell membrane.
40 Clinical Implications of Renal Excretion The rate of urinary drug excretion will depend on the drug s volume of distribution, its degree of protein binding, and the following renal factors: 1. Glomerular filtration rate 2. Tubular fluid ph 3. Extent of back-diffusion of the unionized form 4. Extent of active tubular secretion of the compound 5. Possibly, extent of active tubular reabsorption
41 Changes in any of these factors may result in clinically important alterations in drug action. In the final analysis, the amount of drug that finally appears in the urine will represent a balance of filtered, reabsorbed (passively and actively), and secreted drug. For many drugs, the duration and intensity of pharmacological effect will be influenced by the status of renal function, because of the major role played by the kidneys in drug and metabolite elimination.
42 Biliary Excretion Only small amounts of most drugs reach the bile by diffusion. However- Biliary excretion plays a major role (5 95% of the administered dose) in drug removal for some anions, cations, and certain un-ionized molecules, such as cardiac glycosides. Important for the excretion of some heavy metals. The ability of certain compounds to be actively secreted into bile accounts for the large quantity of these drugs removed from the body by way of the feces.
43 On the other hand, most drugs that are secreted by the liver into the bile and then into the small intestine are not eliminated through the feces. ENTEROHEPATIC CIRCULATION The physicochemical properties of most drugs are sufficiently favorable for passive intestinal absorption that the compound will reenter the blood that perfuses the intestine and again be carried to the liver. Such recycling may continue (enterohepatic cycle or circulation) until the drug either undergoes metabolic changes in the liver, is excreted by the kidneys, or both. This process permits the conservation of such important endogenous substances as the bile acids, vitamins D3 and B12, folic acid, and estrogens

44
45 Drugs that Undergo Enterohepatic Circulation Adriamycin Amphetamine Chlordecone 1,25-Dihydroxyvitamin D3 Estradiol Indomethacin Mestranol Methadone Metronidazole Morphine Phenytoin Polar Glucuronic Acid Conjugates Polar Sulfate Conjugates Sulindac
46 Extensive enterohepatic cycling may be partly responsible for a drug s long persistence in the body. Orally administered activated charcoal and/or anion exchange resins have been used clinically to interrupt enterohepatic cycling and trap drugs in the gastrointestinal tract.
47 Frequently, when a compound is secreted into the intestine through the bile, it is in the form of a conjugate. Conjugated drugs will not be reabsorbed readily from the gastrointestinal tract unless the conjugate is hydrolyzed by gut enzymes such as -glucuronidase. Such a continuous recirculation may lead to the appearance of drug-induced toxicity.
48 Liver disease or injury may impair bile secretion and thereby lead to accumulation of certain drugs Example probenecid, digoxin, and diethylstilbestrol. Impairment of liver function can lead to decreased rates of both drug metabolism and secretion of drugs into bile.
49 These effects may be brought about through an alteration in one or more of the following factors: hepatic blood flow uptake into hepatocytes rate of biotransformation transport into bile rate of bile formation. In addition, antibiotics may alter the intestinal flora in such a manner as to diminish the presence of sulfatase and glucuronidase-containing bacteria. This would result in a persistence of the conjugated form of the drug and hence a decrease in its enterohepatic recirculation.
50 PULMONARY EXCRETION Any volatile material, irrespective of its route of administration, has the potential for pulmonary excretion. Certainly, gases and other volatile substances that enter the body primarily through the respiratory tract can be expected to be excreted by this route. No specialized transport systems are involved in the loss of substances in expired air; simple diffusion across cell membranes is predominant. The rate of loss of gases is not constant; it depends on the rate of respiration and pulmonary blood flow. The degree of solubility of a gas in blood also will affect the rate of gas loss. Gases such as nitrous oxide, which are not very soluble in blood, will be excreted rapidly, that is, almost at the rate at which the blood delivers the drug to the lungs.
51 Increasing cardiac output has the greatest effect on the removal of poorly soluble gases; for example, doubling the cardiac output nearly doubles the rates of loss. Agents with high blood and tissue solubility, on the other hand, are only slowly transferred from pulmonary capillary blood to the alveoli.
52 EXCRETION IN OTHER BODY FLUIDS Sweat and Saliva Minor importance for most drugs. Mainly depends on the diffusion of the un-ionized lipidsoluble form of the drug across the epithelial cells of the glands.
53 Milk The ultimate concentration of the individual compound in milk will depend on many factors, including the amount of drug in the maternal blood, its lipid solubility, its degree of ionization, and the extent of its active excretion. The physicochemical properties that govern the excretion of drugs into saliva and sweat also apply to the passage of drugs into milk. Since milk is more acidic (ph 6.5) than plasma, basic compounds (e.g., alkaloids, such as morphine and codeine) may be somewhat more concentrated in this fluid. In general, a high maternal plasma protein binding of drug will be associated with a low milk concentration. A highly lipid-soluble drug should accumulate in milk fat.
54 First-order kinetics the rate of drug metabolism and elimination is directly proportional to the concentration of free drug, and first-order kinetics is observed. This means that a constant fraction of drug is metabolized per unit of time (that is, with each half-life, the concentration decreases by 50%). First-order kinetics is also referred to as linear kinetics. 54
55 Zero-order kinetics The rate of elimination is constant and does not depend on the drug concentration. The enzyme is saturated by a high free drug concentration, and the rate of metabolism remains constant over time. This is called zero-order kinetics (also called nonlinear kinetics). A constant amount of drug is metabolized per unit of time. 55
56 Total body clearance and drug half-life are important measures of drug clearance that are used to optimize drug therapy and minimize toxicity Total body clearance The total body (systemic) clearance, CLtotal, is the sum of all clearances from the drug-metabolizing and drug-eliminating organs. The kidney is often the major organ of elimination. The liver also contributes to drug clearance through metabolism and/or excretion into the bile. Total clearance is calculated using the following equation: Cltotal= CLhepatic + Clrenal +Clpulmonary+CLother where are CLhepatic + Clrenal typically the most important. 56
57 Clinical situations resulting in changes in drug half-life When a patient has an abnormality that alters the half-life of a drug, adjustment in dosage is required. Patients who may have an increase in drug half-life include those with 1) diminished renal or hepatic blood flow, for example, in cardiogenic shock, heart failure, or hemorrhage; 2) decreased ability to extract drug from plasma, for example, in renal disease; and 3) decreased metabolism, for example, when a concomitant drug inhibits metabolism or in hepatic insufficiency, as with cirrhosis. These patients may require a decrease in dosage or less frequent dosing intervals. In contrast, the half-life of a drug may be decreased by increased hepatic blood flow, decreased protein binding, or increased metabolism. This may necessitate higher doses or more frequent dosing intervals. Dr Swaroop HS copyighted 57
58 Optimization of dose Drug regimens are administered as a maintenance dose and may require a loading dose if rapid effects are warranted. Maintenance dose: Drugs are generally administered to maintain a Css within the therapeutic window. It takes four to five half-lives for a drug to achieve Css. To achieve a given concentration, the rate of administration and the rate of elimination of the drug are important. 58
59 Loading dose Sometimes rapid obtainment of desired plasma levels is needed (for example, in serious infections or arrhythmias). Therefore, a loading dose of drug is administered to achieve the desired plasma level rapidly, followed by a maintenance dose to maintain the steady state. In general, the loading dose can be calculated as Loading dose = (Vd) (desired steady-state plasma concentration)/f For IV infusion, the bioavailability is 100%, and the equation becomes Loading dose = (Vd) (desired steady-state plasma concentration) Loading doses can be given as a single dose or a series of doses. Disadvantages of loading doses include increased risk of drug toxicity a longer time for the plasma concentration to fall if excess levels occur. A loading dose is most useful for drugs that have a relatively long half-life. Without an initial loading dose, these drugs would take a long time to reach a therapeutic value that corresponds to the steady-state level 59
60 Which of the following phase II metabolic reactions makes phase I metabolites readily excretable in urine? A. Oxidation. B. Reduction. C. Glucuronidation. D. Hydrolysis. E. Alcohol dehydrogenation. 60
61 Alkalization of urine by giving bicarbonate is used to treat patients presenting with phenobarbital (weak acid) overdose. Which of the following best describes the rationale for alkalization of urine in this setting? A. To reduce tubular reabsorption of phenobarbital. B. To decrease ionization of phenobarbital. C. To increase glomerular filtration of phenobarbital. D. To decrease proximal tubular secretion. E. To increase tubular reabsorption of phenobarbital. Dr Swaroop HS copyighted 61
62 References Dr Swaroop HS, lecture notes, 2014 Goodman and Gilman, Pharmacological basis of Therapeutics, 12 th edition, Laurence L Bruton Essential of Medical Pharmacology, K D Tripathi, 5 th Edition, JP publishers, New Delhi. Wilson and Gisvold s Textbook of Organic Medicinal and Pharmaceutical Chemistry 11 th ed. Lippincott, Williams & Wilkins ed Drug metabolism by S.P. Markey, NIH, accessed on internet on from Drug metabolism and pharmacokinetics in drug discovery: a primer for bioanalytic study: chandrani gunaratna, current separations, 19:1,
Unit 2b: EXCRETION OF DRUGS. Ms.M.Gayathri Mpharm (PhD) Department of Pharmaceutics Krishna Teja Pharmacy college Subject code: 15R00603 (BPPK)
 Department of Pharmaceutics Krishna Teja Pharmacy college Subject code: 15R00603 (BPPK)") Unit 2b: EXCRETION OF DRUGS By Ms.M.Gayathri Mpharm (PhD) Department of Pharmaceutics Krishna Teja Pharmacy college Subject code: 15R00603 (BPPK) Excretion, along with metabolism and tissue redistribution,
Unit 2b: EXCRETION OF DRUGS By Ms.M.Gayathri Mpharm (PhD) Department of Pharmaceutics Krishna Teja Pharmacy college Subject code: 15R00603 (BPPK) Excretion, along with metabolism and tissue redistribution,
Excretion of Drugs. Prof. Hanan Hagar Pharmacology Unit Medical College
 Excretion of Drugs Prof. Hanan Hagar Pharmacology Unit Medical College Excretion of Drugs By the end of this lecture, students should be able to! Identify main and minor routes of excretion including renal
Excretion of Drugs Prof. Hanan Hagar Pharmacology Unit Medical College Excretion of Drugs By the end of this lecture, students should be able to! Identify main and minor routes of excretion including renal
Chapter 4. Drug Biotransformation
 Chapter 4 Drug Biotransformation Drug Biotransformation 1 Why is drug biotransformation necessary 2 The role of biotransformation in drug disposition 3 Where do drug biotransformation occur 4 The enzymes
Chapter 4 Drug Biotransformation Drug Biotransformation 1 Why is drug biotransformation necessary 2 The role of biotransformation in drug disposition 3 Where do drug biotransformation occur 4 The enzymes
Pharmacokinetics Metabolism
 Pharmacokinetics Metabolism Learning object Know the processes involved in ADME of drugs Know how these processes may affect the action of xenobiotics Appreciate how these processes can affect the outcome
Pharmacokinetics Metabolism Learning object Know the processes involved in ADME of drugs Know how these processes may affect the action of xenobiotics Appreciate how these processes can affect the outcome
Renal Excretion of Drugs
 Renal Excretion of Drugs 3 1 Objectives : 1 Identify main and minor routes of Excretion including renal elimination and biliary excretion 2 Describe its consequences on duration of drugs. For better understanding:
Renal Excretion of Drugs 3 1 Objectives : 1 Identify main and minor routes of Excretion including renal elimination and biliary excretion 2 Describe its consequences on duration of drugs. For better understanding:
Pharmacokinetics of Drugs. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Pharmacokinetics of Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Absorption Is the transfer of a drug from its site of administration to the bloodstream.
Pharmacokinetics of Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Absorption Is the transfer of a drug from its site of administration to the bloodstream.
It the process by which a drug reversibly leaves blood and enter interstitium (extracellular fluid) and/ or cells of tissues.
 and/ or cells of tissues.") It the process by which a drug reversibly leaves blood and enter interstitium (extracellular fluid) and/ or cells of tissues. Primarily depends on: 1.Regional blood flow. 2.Capillary permeability. 3.Protein
It the process by which a drug reversibly leaves blood and enter interstitium (extracellular fluid) and/ or cells of tissues. Primarily depends on: 1.Regional blood flow. 2.Capillary permeability. 3.Protein
METABOLISM. Ali Alhoshani, B.Pharm, Ph.D. Office: 2B 84
 METABOLISM Ali Alhoshani, B.Pharm, Ph.D. ahoshani@ksu.edu.sa Office: 2B 84 Metabolism By the end of this lecture, you should: Recognize the importance of biotransformation Know the different sites for
METABOLISM Ali Alhoshani, B.Pharm, Ph.D. ahoshani@ksu.edu.sa Office: 2B 84 Metabolism By the end of this lecture, you should: Recognize the importance of biotransformation Know the different sites for
Industrial Toxicology
 Industrial Toxicology Learning Objectives Know the assumptions of the doseresponse and time-course curves Be able to define and label key points of a curve Know the difference between potency and efficacy
Industrial Toxicology Learning Objectives Know the assumptions of the doseresponse and time-course curves Be able to define and label key points of a curve Know the difference between potency and efficacy
INTRODUCTION TO PHARMACOKINETICS
 INTRODUCTION TO PHARMACOKINETICS 1 http://www.biology.iupui.edu/biocourses/biol540/4pipeline2css.html 2 PHARMACOKINETICS 1. ABSORPTION 2. DISTRIBUTION 3. METABOLISM 4. EXCRETION ALL THESE PROCESSES ARE
INTRODUCTION TO PHARMACOKINETICS 1 http://www.biology.iupui.edu/biocourses/biol540/4pipeline2css.html 2 PHARMACOKINETICS 1. ABSORPTION 2. DISTRIBUTION 3. METABOLISM 4. EXCRETION ALL THESE PROCESSES ARE
Metabolism. Objectives. Metabolism. 26 July Chapter 28 1
 Metabolism bjectives Describe various processes by which drugs are metabolized Describe induction and inhibition of metabolism Use the venous equilibration model to describe hepatic clearance and the effect
Metabolism bjectives Describe various processes by which drugs are metabolized Describe induction and inhibition of metabolism Use the venous equilibration model to describe hepatic clearance and the effect
Introduction to. Pharmacokinetics. University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
Introduction to 1 Pharmacokinetics University of Hawai i Hilo Pre-Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 2 Learning objectives Understand compartment models and how they effects
ADME Review. Dr. Joe Ritter Associate Professor of Pharmacology
 ADME Review Dr. Joe Ritter Associate Professor of Pharmacology 828-1022 jkritter@vcu.edu What percent of a weak base (pka = 7.5) and weak acid (pka = 3.5) will be respectively ionized in urine of ph 5.5?
ADME Review Dr. Joe Ritter Associate Professor of Pharmacology 828-1022 jkritter@vcu.edu What percent of a weak base (pka = 7.5) and weak acid (pka = 3.5) will be respectively ionized in urine of ph 5.5?
Basic Concepts in Pharmacokinetics. Leon Aarons Manchester Pharmacy School University of Manchester
 Basic Concepts in Pharmacokinetics Leon Aarons Manchester Pharmacy School University of Manchester Objectives 1. Define pharmacokinetics 2. Describe absorption 3. Describe distribution 4. Describe elimination
Basic Concepts in Pharmacokinetics Leon Aarons Manchester Pharmacy School University of Manchester Objectives 1. Define pharmacokinetics 2. Describe absorption 3. Describe distribution 4. Describe elimination
DEPARTMENT OF PHARMACOLOGY AND THERAPEUTIC UNIVERSITAS SUMATERA UTARA
 METABOLISME dr. Yunita Sari Pane DEPARTMENT OF PHARMACOLOGY AND THERAPEUTIC UNIVERSITAS SUMATERA UTARA Pharmacokinetic absorption distribution BIOTRANSFORMATION elimination Intravenous Administration Oral
METABOLISME dr. Yunita Sari Pane DEPARTMENT OF PHARMACOLOGY AND THERAPEUTIC UNIVERSITAS SUMATERA UTARA Pharmacokinetic absorption distribution BIOTRANSFORMATION elimination Intravenous Administration Oral
DRUG ELIMINATION II BILIARY EXCRETION MAMMARY, SALIVARY AND PULMONARY EXCRETION
 DRUG ELIMINATION II BILIARY EXCRETION MAMMARY, SALIVARY AND PULMONARY EXCRETION ROUTE OF DRUG ADMINISTRATION AND EXTRAHEPATIC DRUG METABOLISM The decline in plasma concentration after drug administration
DRUG ELIMINATION II BILIARY EXCRETION MAMMARY, SALIVARY AND PULMONARY EXCRETION ROUTE OF DRUG ADMINISTRATION AND EXTRAHEPATIC DRUG METABOLISM The decline in plasma concentration after drug administration
Metabolic Changes of Drugs and Related Organic Compounds. Oxidative Reactions. Shokhan J. Hamid. 3 rd stage/ 1 st course Lecture 6
 Metabolic Changes of Drugs and Related Organic Compounds Oxidative Reactions 3 rd stage/ 1 st course Lecture 6 Shokhan J. Hamid B. OXIDATION INVOLVING CARBON OXYGEN SYSTEMS: Oxidative O-dealkylation of
Metabolic Changes of Drugs and Related Organic Compounds Oxidative Reactions 3 rd stage/ 1 st course Lecture 6 Shokhan J. Hamid B. OXIDATION INVOLVING CARBON OXYGEN SYSTEMS: Oxidative O-dealkylation of
Drug Metabolism Phase 2 conjugation reactions. Medicinal chemistry 3 rd stage
 Drug Metabolism Phase 2 conjugation reactions Medicinal chemistry 3 rd stage 1 Phase II or Conjugation reactions 1. Glucuronic acid conjugation 2. Sulfate conjugation 3. Glycine and Glutamine conjugation
Drug Metabolism Phase 2 conjugation reactions Medicinal chemistry 3 rd stage 1 Phase II or Conjugation reactions 1. Glucuronic acid conjugation 2. Sulfate conjugation 3. Glycine and Glutamine conjugation
Metabolic Changes of Drugs and Related Organic Compounds
 Metabolic Changes of Drugs and Related Organic Compounds 3 rd stage/ 1 st course Lecture 7 Shokhan J. Hamid 1 Phase II or Conjugation Reactions Phase I or functionalization reactions do not always produce
Metabolic Changes of Drugs and Related Organic Compounds 3 rd stage/ 1 st course Lecture 7 Shokhan J. Hamid 1 Phase II or Conjugation Reactions Phase I or functionalization reactions do not always produce
B. Incorrect! Compounds are made more polar, to increase their excretion.
 Pharmacology - Problem Drill 04: Biotransformation Question No. 1 of 10 Instructions: (1) Read the problem and answer choices carefully, (2) Work the problems on paper as 1. What is biotransformation?
Pharmacology - Problem Drill 04: Biotransformation Question No. 1 of 10 Instructions: (1) Read the problem and answer choices carefully, (2) Work the problems on paper as 1. What is biotransformation?
Metabolic Changes of Drugs and Related Organic Compounds
 Metabolic Changes of Drugs and Related Organic Compounds 3 rd stage/ 1 st course Lecture 3 Shokhan J. Hamid 2 Metabolism plays a central role in the elimination of drugs and other foreign compounds from
Metabolic Changes of Drugs and Related Organic Compounds 3 rd stage/ 1 st course Lecture 3 Shokhan J. Hamid 2 Metabolism plays a central role in the elimination of drugs and other foreign compounds from
Pharmacokinetics. Karim Rafaat
 Pharmacokinetics Karim Rafaat Pharmacokinetics The therapeutic effect of a drug is determined by the concentration of drug at the receptor site of action. Even though the concentration of drug that reaches
Pharmacokinetics Karim Rafaat Pharmacokinetics The therapeutic effect of a drug is determined by the concentration of drug at the receptor site of action. Even though the concentration of drug that reaches
Mechanism of Detoxification
 Mechanism of Detoxification Prof.Dr. Hedef Dhafir El-Yassin 1 Objectives: 1. To list the detoxification pathways 2. To describe detoxification pathways and phases in the liver, 2 3 4 o Xenobiotics are
Mechanism of Detoxification Prof.Dr. Hedef Dhafir El-Yassin 1 Objectives: 1. To list the detoxification pathways 2. To describe detoxification pathways and phases in the liver, 2 3 4 o Xenobiotics are
General pharmacology Lecture(3)
") General pharmacology Lecture(3) 2. Specialized transport: It may be: i. Carrier-mediated transport ii. Pinocytosis. i. Carrier-mediated transport: The drug combines with a carrier (a specialized protein
General pharmacology Lecture(3) 2. Specialized transport: It may be: i. Carrier-mediated transport ii. Pinocytosis. i. Carrier-mediated transport: The drug combines with a carrier (a specialized protein
MODULE No.26: Drug Metabolism
 SUBJECT Paper No. and Title Module No. and Title Module Tag PAPER No. 9: Drugs of Abuse MODULE No. 26: Drug Metabolism FSC_P9_M26 TABLE OF CONTENTS 1. Learning Outcomes 2. Introduction 3. Sites of Drug
SUBJECT Paper No. and Title Module No. and Title Module Tag PAPER No. 9: Drugs of Abuse MODULE No. 26: Drug Metabolism FSC_P9_M26 TABLE OF CONTENTS 1. Learning Outcomes 2. Introduction 3. Sites of Drug
Importance of drug antagonism (i) Correcting adverse effects of drugs (ii) Treating drug poisoning. e.g. Morphine with naloxone, organophosphate
 Correcting adverse effects of drugs (ii) Treating drug poisoning. e.g. Morphine with naloxone, organophosphate") Importance of drug antagonism (i) Correcting adverse effects of drugs (ii) Treating drug poisoning. e.g. Morphine with naloxone, organophosphate compounds with atropine. (iii) Predicting drug combinations
Importance of drug antagonism (i) Correcting adverse effects of drugs (ii) Treating drug poisoning. e.g. Morphine with naloxone, organophosphate compounds with atropine. (iii) Predicting drug combinations
Renal Function. 1. Glomerular filtration 2. Active tubular secretion 3. Passive tubular reabsorption 4. Excretion
 59-291 Section 1, Lecture 5 Drug Excretion -most drugs are excreted in urine either as unchanged or drug metabolites Renal Function 1. Glomerular filtration 2. Active tubular secretion 3. Passive tubular
59-291 Section 1, Lecture 5 Drug Excretion -most drugs are excreted in urine either as unchanged or drug metabolites Renal Function 1. Glomerular filtration 2. Active tubular secretion 3. Passive tubular
Lecture 8: Phase 1 Metabolism
 Lecture 8: Phase 1 Metabolism The purpose of metabolism is to detoxify a drug, eliminate a drug or activate a drug. In metabolism there are two phases, Phase I and Phase II. Phase I is the introduction
Lecture 8: Phase 1 Metabolism The purpose of metabolism is to detoxify a drug, eliminate a drug or activate a drug. In metabolism there are two phases, Phase I and Phase II. Phase I is the introduction
PRESCRIBING IN LIVER AND RENAL DISEASE
 THERAPEUTICS FOR INDEPENDENT PRESCRIBERS PRESCRIBING IN LIVER AND RENAL DISEASE Number 6 in a series of 15 articles on Therapeutics Aims and Objectives To outline the pathophysiological changes that occur
THERAPEUTICS FOR INDEPENDENT PRESCRIBERS PRESCRIBING IN LIVER AND RENAL DISEASE Number 6 in a series of 15 articles on Therapeutics Aims and Objectives To outline the pathophysiological changes that occur
Toxicant Disposition and Metabolism. Jan Chambers Center for Environmental Health Sciences College of Veterinary Medicine
 Toxicant Disposition and Metabolism Jan Chambers Center for Environmental Health Sciences College of Veterinary Medicine chambers@cvm.msstate.edu Definitions Disposition Absorption passage across membrane.
Toxicant Disposition and Metabolism Jan Chambers Center for Environmental Health Sciences College of Veterinary Medicine chambers@cvm.msstate.edu Definitions Disposition Absorption passage across membrane.
General Pharmacology
 General Pharmacology (Pharmacokinetic III) Principles of Pharmacology (PP VII) Dr. Ahmad Al-Zohyri Dept. of Pharmacology Baghdad College of Medicine References: Basic & clinical pharmacology by Katzung
General Pharmacology (Pharmacokinetic III) Principles of Pharmacology (PP VII) Dr. Ahmad Al-Zohyri Dept. of Pharmacology Baghdad College of Medicine References: Basic & clinical pharmacology by Katzung
Principles of Drug Action. Intro to Pharmacology: Principles of Courework Drug Action Intro to Pharmacology
 Principles of Drug Action Intro to Pharmacology: Principles of Courework 102.3 Drug Action Intro to Pharmacology Directions Read the PPT and complete R.E.A.D. Assignment. There are videos embedded within
Principles of Drug Action Intro to Pharmacology: Principles of Courework 102.3 Drug Action Intro to Pharmacology Directions Read the PPT and complete R.E.A.D. Assignment. There are videos embedded within
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D.
 RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
RENAL SYSTEM 2 TRANSPORT PROPERTIES OF NEPHRON SEGMENTS Emma Jakoi, Ph.D. Learning Objectives 1. Identify the region of the renal tubule in which reabsorption and secretion occur. 2. Describe the cellular
Non-protein nitrogenous substances (NPN)
") Non-protein nitrogenous substances (NPN) A simple, inexpensive screening test a routine urinalysis is often the first test conducted if kidney problems are suspected. A small, randomly collected urine
Non-protein nitrogenous substances (NPN) A simple, inexpensive screening test a routine urinalysis is often the first test conducted if kidney problems are suspected. A small, randomly collected urine
Chapter 9. Biotransformation
 Chapter 9 Biotransformation Biotransformation The term biotransformation is the sum of all chemical processes of the body that modify endogenous or exogenous chemicals. Focus areas of toxicokinetics: Biotransformation
Chapter 9 Biotransformation Biotransformation The term biotransformation is the sum of all chemical processes of the body that modify endogenous or exogenous chemicals. Focus areas of toxicokinetics: Biotransformation
Tamer Barakat. Abdul Aziz ALShamali. Abdul Aziz ALShamali
 10 Tamer Barakat Abdul Aziz ALShamali Abdul Aziz ALShamali Dr. Alia Elimination: Refampin is used to treat TB not malaria (Quinacrine is used for malaria) It s the opposite process of absorption. It's
10 Tamer Barakat Abdul Aziz ALShamali Abdul Aziz ALShamali Dr. Alia Elimination: Refampin is used to treat TB not malaria (Quinacrine is used for malaria) It s the opposite process of absorption. It's
Drug elimination and Hepatic clearance Chapter 6
 Drug elimination and Hepatic clearance Chapter 6 DRUG ELIMINATION Drugs are removed from the body by various elimination processes. Drug elimination refers to the irreversible removal of drug from the
Drug elimination and Hepatic clearance Chapter 6 DRUG ELIMINATION Drugs are removed from the body by various elimination processes. Drug elimination refers to the irreversible removal of drug from the
Pharmacokinetics for Physicians. Assoc Prof. Noel E. Cranswick Clinical Pharmacologist Royal Children s Hospital Melbourne
 Pharmacokinetics for Physicians Assoc Prof. Noel E. Cranswick Clinical Pharmacologist Royal Children s Hospital Melbourne The Important Therapeutic Questions What drug? What dose? How long? Drug Dosage
Pharmacokinetics for Physicians Assoc Prof. Noel E. Cranswick Clinical Pharmacologist Royal Children s Hospital Melbourne The Important Therapeutic Questions What drug? What dose? How long? Drug Dosage
Pharmacokinetics I. Dr. M.Mothilal Assistant professor
 Pharmacokinetics I Dr. M.Mothilal Assistant professor DRUG TRANSPORT For a drug to produce a therapeutic effect, it must reach to its target and it must accumulate at that site to reach to the minimum
Pharmacokinetics I Dr. M.Mothilal Assistant professor DRUG TRANSPORT For a drug to produce a therapeutic effect, it must reach to its target and it must accumulate at that site to reach to the minimum
Pharmacokinetics in Drug Development. Edward P. Acosta, PharmD Professor & Director Division of Clinical Pharmacology Director, CCC PK/PD Core
 Pharmacokinetics in Drug Development Edward P. Acosta, PharmD Professor & Director Division of Clinical Pharmacology Director, CCC PK/PD Core Finding new drugs: A crap shoot Clinical Development Phase
Pharmacokinetics in Drug Development Edward P. Acosta, PharmD Professor & Director Division of Clinical Pharmacology Director, CCC PK/PD Core Finding new drugs: A crap shoot Clinical Development Phase
JOHN HARGRAVE. Date of Birth : 31-Oct-1973 Sex : M Collected : 24-Aug BENTONS ROAD MOUNT MARTHA VIC Lab id: UR#:
 INTEGRATIVE MEDICINE URINE, SPOT Result Range Units DETOXIFICATION CAPACITY PROFILE PHASE I (OXIDATION) Caffeine Clearance 0.7 0.5-1.6 ml/min/kg PHASE II (CONJUGATION) Glutathionation 5.2 *L 5.6-11.4 %
INTEGRATIVE MEDICINE URINE, SPOT Result Range Units DETOXIFICATION CAPACITY PROFILE PHASE I (OXIDATION) Caffeine Clearance 0.7 0.5-1.6 ml/min/kg PHASE II (CONJUGATION) Glutathionation 5.2 *L 5.6-11.4 %
Chapter Questions. Modern Pharmacology With Clinical Applications. Sixth Edition
 Chapter Questions Modern Pharmacology With Clinical Applications Sixth Edition Mechanism of Drug Action Questions 1. Receptors are macromolecules that a. Are designed to attract drugs b. Are resistant
Chapter Questions Modern Pharmacology With Clinical Applications Sixth Edition Mechanism of Drug Action Questions 1. Receptors are macromolecules that a. Are designed to attract drugs b. Are resistant
Drug Dosing in Renal Insufficiency. Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila
 Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila Declaration of Conflict of Interest For today s lecture on Drug Dosing in Renal
Drug Dosing in Renal Insufficiency Coralie Therese D. Dimacali, MD College of Medicine University of the Philippines Manila Declaration of Conflict of Interest For today s lecture on Drug Dosing in Renal
Pharmacokinetics Dr. Iman Lec. 3
 Pharmacokinetics r. Iman Lec. 3 Pharmacokinetics A dequate drug doses must be delivered to the target organ to get therapeutic but not toxic levels. So, pharmacokinetic examines the movement of drug over
Pharmacokinetics r. Iman Lec. 3 Pharmacokinetics A dequate drug doses must be delivered to the target organ to get therapeutic but not toxic levels. So, pharmacokinetic examines the movement of drug over
Polar bodies are either introduced or unmasked, which results in more polar metabolites Phase I reactions can lead either to activation or
 Polar bodies are either introduced or unmasked, which results in more polar metabolites Phase I reactions can lead either to activation or inactivation of the drug (i.e. therapeutic effects or toxicity)
Polar bodies are either introduced or unmasked, which results in more polar metabolites Phase I reactions can lead either to activation or inactivation of the drug (i.e. therapeutic effects or toxicity)
C.9. Drug. excretion. Prof. Dr. Romeo T. Cristina. See:
 C.9 Drug excretion See: www.veterinarypharmacon.com Prof. Dr. Romeo T. Cristina By drug elimination (excretion) we mean all processes that lead to drug inactivation and their removal through: - kidney,
C.9 Drug excretion See: www.veterinarypharmacon.com Prof. Dr. Romeo T. Cristina By drug elimination (excretion) we mean all processes that lead to drug inactivation and their removal through: - kidney,
Basic Biopharmaceutics, Pharmacokinetics, and Pharmacodynamics
 Basic Biopharmaceutics, Pharmacokinetics, and Pharmacodynamics Learning Outcomes Define biopharmaceutics Describe 4 processes of pharmacokinetics Describe factors that affect medication absorption Describe
Basic Biopharmaceutics, Pharmacokinetics, and Pharmacodynamics Learning Outcomes Define biopharmaceutics Describe 4 processes of pharmacokinetics Describe factors that affect medication absorption Describe
ENVIRONMENTAL TOXICOLOGY
 ENVIRONMENTAL TOXICOLOGY Chapter 4 Toxicokinetics Mohd Amir Bin Arshad Toxicokinetics study on how a substance gets into the body and what happens to it in the body" The kinetics (movement) of substances
ENVIRONMENTAL TOXICOLOGY Chapter 4 Toxicokinetics Mohd Amir Bin Arshad Toxicokinetics study on how a substance gets into the body and what happens to it in the body" The kinetics (movement) of substances
Definition of bilirubin Bilirubin metabolism
 Definition of bilirubin Bilirubin metabolism obilirubin formation otransport of bilirubin in plasma ohepatic bilirubin transport oexcretion through intestine Other substances conjugated by glucuronyl transferase.
Definition of bilirubin Bilirubin metabolism obilirubin formation otransport of bilirubin in plasma ohepatic bilirubin transport oexcretion through intestine Other substances conjugated by glucuronyl transferase.
Slide 1. Slide 2. Slide 3. Drug Action and Handling. Lesson 2.1. Lesson 2.1. Drug Action and Handling. Drug Action and Handling.
 Slide 1 Drug Action and Handling Chapter 2 1 Slide 2 Lesson 2.1 Drug Action and Handling 1. Differentiate dose, potency, and efficacy in the context of the actions of drugs. 2. Explain the pharmacologic
Slide 1 Drug Action and Handling Chapter 2 1 Slide 2 Lesson 2.1 Drug Action and Handling 1. Differentiate dose, potency, and efficacy in the context of the actions of drugs. 2. Explain the pharmacologic
Biopharmaceutics. Tips Worth Tweeting. Contributor: Sandra Earle
 Biopharmaceutics C H A P T E R 2 Contributor: Sandra Earle The physiochemical properties of drugs determine how they will move and interact with the body. By understanding a few principles, predictions
Biopharmaceutics C H A P T E R 2 Contributor: Sandra Earle The physiochemical properties of drugs determine how they will move and interact with the body. By understanding a few principles, predictions
Basic Concepts of TDM
 TDM Lecture 1 5 th stage What is TDM? Basic Concepts of TDM Therapeutic drug monitoring (TDM) is a branch of clinical pharmacology that specializes in the measurement of medication concentrations in blood.
TDM Lecture 1 5 th stage What is TDM? Basic Concepts of TDM Therapeutic drug monitoring (TDM) is a branch of clinical pharmacology that specializes in the measurement of medication concentrations in blood.
Drug Distribution. Joseph K. Ritter, Ph.D., Assoc. Prof. Medical Sciences Building, Room
 Drug Distribution Joseph K. Ritter, Ph.D., Assoc. Prof. Medical Sciences Building, Room 531 jkritter@vcu.edu 828-1022 Department of Pharmacology and Toxicology Medical College of Virginia Campus Virginia
Drug Distribution Joseph K. Ritter, Ph.D., Assoc. Prof. Medical Sciences Building, Room 531 jkritter@vcu.edu 828-1022 Department of Pharmacology and Toxicology Medical College of Virginia Campus Virginia
Introduction to Pharmacokinetics (PK) Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017
 Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017") Introduction to Pharmacokinetics (PK) Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017 1 Outline Definition & Relevance of Pharmacokinetics
Introduction to Pharmacokinetics (PK) Anson K. Abraham, Ph.D. Associate Principal Scientist, PPDM- QP2 Merck & Co. Inc., West Point, PA 5- June- 2017 1 Outline Definition & Relevance of Pharmacokinetics
The ADME properties of most drugs strongly depends on the ability of the drug to pass through membranes via simple diffusion.
 1 MEDCHEM 562 Kent Kunze Lecture 1 Physicochemical Properties and Drug Disposition The ADME properties of most drugs strongly depends on the ability of the drug to pass through membranes via simple diffusion.
1 MEDCHEM 562 Kent Kunze Lecture 1 Physicochemical Properties and Drug Disposition The ADME properties of most drugs strongly depends on the ability of the drug to pass through membranes via simple diffusion.
INTEGRATIVE MEDICINE URINE, SPOT Result Range Units
 P: 1300 688 522 E: info@nutripath.com.au A: PO Box 442 Ashburton VIC 3142 TEST PATIENT TEST PHYSICIAN DR JOHN DOE Sex : 111 CLINIC ST D Collected : 00-00-0000 111 ROADTEST SUBURB AB : 00000000 UR#:0000000
P: 1300 688 522 E: info@nutripath.com.au A: PO Box 442 Ashburton VIC 3142 TEST PATIENT TEST PHYSICIAN DR JOHN DOE Sex : 111 CLINIC ST D Collected : 00-00-0000 111 ROADTEST SUBURB AB : 00000000 UR#:0000000
PHAR 7632 Chapter 16
 PHAR 7632 Chapter 16 Routes of Excretion Routes of Excretion Student Objectives for this Chapter After completing the material in this chapter each student should:- be able to describe the various routes
PHAR 7632 Chapter 16 Routes of Excretion Routes of Excretion Student Objectives for this Chapter After completing the material in this chapter each student should:- be able to describe the various routes
PHARMACOLOGY-1 PHL-313. Ali Alhoshani Office: 2B 84
 PHARMACOLOGY-1 PHL-313 Ali Alhoshani ahoshani@ksu.edu.sa http://fac.ksu.edu.sa/ahoshani Office: 2B 84 General rules Reference: General rules Email [PHL313-1 st Semester 38-39] Student ID- Question Example
PHARMACOLOGY-1 PHL-313 Ali Alhoshani ahoshani@ksu.edu.sa http://fac.ksu.edu.sa/ahoshani Office: 2B 84 General rules Reference: General rules Email [PHL313-1 st Semester 38-39] Student ID- Question Example
BIOMARKERS AND TOXICITY MECHANISMS 07 Mechanisms Metabolism & Detoxification. Luděk Bláha, PřF MU, RECETOX
 BIOMARKERS AND TOXICITY MECHANISMS 07 Mechanisms Metabolism & Detoxification Luděk Bláha, PřF MU, RECETOX www.recetox.cz Metabolism and detoxification Chemicals enter body... mostly via food Pass directly
BIOMARKERS AND TOXICITY MECHANISMS 07 Mechanisms Metabolism & Detoxification Luděk Bláha, PřF MU, RECETOX www.recetox.cz Metabolism and detoxification Chemicals enter body... mostly via food Pass directly
ANTIHYPERLIPIDEMIA. Darmawan,dr.,M.Kes,Sp.PD
 ANTIHYPERLIPIDEMIA Darmawan,dr.,M.Kes,Sp.PD Plasma lipids consist mostly of lipoproteins Spherical complexes of lipids and specific proteins (apolipoproteins). The clinically important lipoproteins, listed
ANTIHYPERLIPIDEMIA Darmawan,dr.,M.Kes,Sp.PD Plasma lipids consist mostly of lipoproteins Spherical complexes of lipids and specific proteins (apolipoproteins). The clinically important lipoproteins, listed
Name: Class: "Pharmacology NSAIDS (1) Lecture
 Lecture") I Name: Class: "Pharmacology NSAIDS (1) Lecture د. احمد الزهيري Inflammation is triggered by the release of chemical mediators from injured tissues and migrating cells. The specific mediators vary with
I Name: Class: "Pharmacology NSAIDS (1) Lecture د. احمد الزهيري Inflammation is triggered by the release of chemical mediators from injured tissues and migrating cells. The specific mediators vary with
Lippincott Questions Pharmacology
 Lippincott Questions Pharmacology Edition Two: Chapter One: 1.Which one of the following statements is CORRECT? A. Weak bases are absorbed efficiently across the epithelial cells of the stomach. B. Coadministration
Lippincott Questions Pharmacology Edition Two: Chapter One: 1.Which one of the following statements is CORRECT? A. Weak bases are absorbed efficiently across the epithelial cells of the stomach. B. Coadministration
Acid-Base Balance 11/18/2011. Regulation of Potassium Balance. Regulation of Potassium Balance. Regulatory Site: Cortical Collecting Ducts.
 Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
Influence of Other Hormones on Sodium Balance Acid-Base Balance Estrogens: Enhance NaCl reabsorption by renal tubules May cause water retention during menstrual cycles Are responsible for edema during
The principal functions of the kidneys
 Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Renal physiology The principal functions of the kidneys Formation and excretion of urine Excretion of waste products, drugs, and toxins Regulation of body water and mineral content of the body Maintenance
Role of metabolism in Drug-Induced Liver Injury (DILI) Drug Metab Rev. 2007;39(1):
 Drug Metab Rev. 2007;39(1):") Role of metabolism in Drug-Induced Liver Injury (DILI) Drug Metab Rev. 2007;39(1):159-234 Drug Metab Rev. 2007;39(1):159-234 Drug Metab Rev. 2007;39(1):159-234 A schematic representation of the most relevant
Role of metabolism in Drug-Induced Liver Injury (DILI) Drug Metab Rev. 2007;39(1):159-234 Drug Metab Rev. 2007;39(1):159-234 Drug Metab Rev. 2007;39(1):159-234 A schematic representation of the most relevant
Biologic Oxidation BIOMEDICAL IMPORTAN
 Biologic Oxidation BIOMEDICAL IMPORTAN Chemically, oxidation is defined as the removal of electrons and reduction as the gain of electrons. Thus, oxidation is always accompanied by reduction of an electron
Biologic Oxidation BIOMEDICAL IMPORTAN Chemically, oxidation is defined as the removal of electrons and reduction as the gain of electrons. Thus, oxidation is always accompanied by reduction of an electron
Nonlinear Pharmacokinetics
 Nonlinear Pharmacokinetics Non linear pharmacokinetics: In some cases, the kinetics of a pharmacokinetic process change from predominantly first order to predominantly zero order with increasing dose or
Nonlinear Pharmacokinetics Non linear pharmacokinetics: In some cases, the kinetics of a pharmacokinetic process change from predominantly first order to predominantly zero order with increasing dose or
Pharmacokinetics in the critically ill. Intensive Care Training Program Radboud University Medical Centre Nijmegen
 Pharmacokinetics in the critically ill Intensive Care Training Program Radboud University Medical Centre Nijmegen In general... Critically ill patients are at higher risk for ADE s and more severe ADE
Pharmacokinetics in the critically ill Intensive Care Training Program Radboud University Medical Centre Nijmegen In general... Critically ill patients are at higher risk for ADE s and more severe ADE
Tala Saleh. Abdul Aziz ALShamali. Abdul Aziz ALShamali
 9 Tala Saleh Abdul Aziz ALShamali Abdul Aziz ALShamali Alia Shatanawi Volume of Distribution (Vd) Understand the concept Imagine having a container with an unknown volume of water in it. Then 1000mg of
9 Tala Saleh Abdul Aziz ALShamali Abdul Aziz ALShamali Alia Shatanawi Volume of Distribution (Vd) Understand the concept Imagine having a container with an unknown volume of water in it. Then 1000mg of
Diuretic Agents Part-2. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Diuretic Agents Part-2 Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Potassium-sparing diuretics The Ion transport pathways across the luminal and basolateral
Renal Reabsorption & Secretion
 Renal Reabsorption & Secretion Topics for today: Nephron processing of filtrate Control of glomerular filtration Reabsorption and secretion Examples of solute clearance rates Hormones affecting kidney
Renal Reabsorption & Secretion Topics for today: Nephron processing of filtrate Control of glomerular filtration Reabsorption and secretion Examples of solute clearance rates Hormones affecting kidney
TOXICOKINETICS; DISPOSITION OF XENOBIOTICS (Absorption, Distribution and Excretion of xenobiotics)
") TOXICOKINETICS; DISPOSITION OF XENOBIOTICS (Absorption, Distribution and Excretion of xenobiotics) Benay Can Eke, Ph.D., ERT Professor of Toxicology Department of Toxicology Faculty of Pharmacy Ankara
TOXICOKINETICS; DISPOSITION OF XENOBIOTICS (Absorption, Distribution and Excretion of xenobiotics) Benay Can Eke, Ph.D., ERT Professor of Toxicology Department of Toxicology Faculty of Pharmacy Ankara
Distribution. Definition. Distribution is the the API s movement to the tissues fromthesytemic circulation.
 Distribution Definition Distribution is the the API s movement to the tissues fromthesytemic circulation. Distribution Distribution is influencedby Permeability of capillaries Perfusionof tissues, speed
Distribution Definition Distribution is the the API s movement to the tissues fromthesytemic circulation. Distribution Distribution is influencedby Permeability of capillaries Perfusionof tissues, speed
UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology
 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology 1 PBL SEMINAR ACUTE & CHRONIC ETHANOL EFFECTS An Overview Sites
UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology 1 PBL SEMINAR ACUTE & CHRONIC ETHANOL EFFECTS An Overview Sites
Bile acid metabolism. doc. Ing. Zenóbia Chavková, CSc.
 Bile acid metabolism doc. Ing. Zenóbia Chavková, CSc. Bile acid metabolism Importance: Availability for fat & cholesterol absorption Regulates total body pool of cholesterol Factors that synthesis promote
Bile acid metabolism doc. Ing. Zenóbia Chavková, CSc. Bile acid metabolism Importance: Availability for fat & cholesterol absorption Regulates total body pool of cholesterol Factors that synthesis promote
Pharmacokinetic Phase
 RSPT 2317 Principles of Drug Action Part 2: The Pharmacokinetic Phase Pharmacokinetic Phase This phase describes the time course and disposition of a drug in the body, based on its absorption, distribution,
RSPT 2317 Principles of Drug Action Part 2: The Pharmacokinetic Phase Pharmacokinetic Phase This phase describes the time course and disposition of a drug in the body, based on its absorption, distribution,
Excretion of drugs. Objectives:
 Objectives: Excretion of drugs Identify major and minor routes of excretion including renal elimination and biliary excretion Describe enterohepatic circulation and its consequences on duration of drugs.
Objectives: Excretion of drugs Identify major and minor routes of excretion including renal elimination and biliary excretion Describe enterohepatic circulation and its consequences on duration of drugs.
UNIVERSITY OF THE WEST INDIES, ST AUGUSTINE
 UNIVERSITY OF THE WEST INDIES, ST AUGUSTINE FACULTY OF MEDICAL SCIENCES SCHOOL OF PHARMACY BACHELOR OF SCIENCE IN PHARMACY DEGREE COURSE SYLLABUS COURSE TITLE: COURSE CODE: BIOPHARMACEUTICS, NEW DRUG DELIVERY
UNIVERSITY OF THE WEST INDIES, ST AUGUSTINE FACULTY OF MEDICAL SCIENCES SCHOOL OF PHARMACY BACHELOR OF SCIENCE IN PHARMACY DEGREE COURSE SYLLABUS COURSE TITLE: COURSE CODE: BIOPHARMACEUTICS, NEW DRUG DELIVERY
Renal Disease and PK/PD. Anjay Rastogi MD PhD Division of Nephrology
 Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
Renal Disease and PK/PD Anjay Rastogi MD PhD Division of Nephrology Drugs and Kidneys Kidney is one of the major organ of drug elimination from the human body Renal disease and dialysis alters the pharmacokinetics
Drug Interactions Year 2 Clinical Pharmacology
 1 Drug Interactions Year 2 Clinical Pharmacology Prof Mark McKeage Department of Pharmacology & Clinical Pharmacology 2 Objectives Explain the potential for interacting drugs to cause beneficial and harmful
1 Drug Interactions Year 2 Clinical Pharmacology Prof Mark McKeage Department of Pharmacology & Clinical Pharmacology 2 Objectives Explain the potential for interacting drugs to cause beneficial and harmful
Title of Lecture: Pharmacokinetics II Metabolism and Excretion (Problem 17, Lecture 2, 2009)
") Author of Lecture: Hilmer, Sarah (Dr.) Title of Lecture: Pharmacokinetics II Metabolism and Excretion (Problem 17, Lecture 2, 2009) COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING This material
Author of Lecture: Hilmer, Sarah (Dr.) Title of Lecture: Pharmacokinetics II Metabolism and Excretion (Problem 17, Lecture 2, 2009) COMMONWEALTH OF AUSTRALIA Copyright Regulations 1969 WARNING This material
1 Introduction COPYRIGHTED MATERIAL. 1.1 Therapeutic w indow Introduction
 1 Introduction 1.1 Therapeutic w indow 1.1.1 Introduction It has been said that if a drug has no side effects, then it is unlikely to work. Drug therapy labours under the fundamental problem that usually
1 Introduction 1.1 Therapeutic w indow 1.1.1 Introduction It has been said that if a drug has no side effects, then it is unlikely to work. Drug therapy labours under the fundamental problem that usually
2- Minimum toxic concentration (MTC): The drug concentration needed to just produce a toxic effect.
: The drug concentration needed to just produce a toxic effect.") BIOPHARMACEUTICS Drug Product Performance Parameters: 1- Minimum effective concentration (MEC): The minimum concentration of drug needed at the receptors to produce the desired pharmacologic effect. 2-
BIOPHARMACEUTICS Drug Product Performance Parameters: 1- Minimum effective concentration (MEC): The minimum concentration of drug needed at the receptors to produce the desired pharmacologic effect. 2-
BASIC PHARMACOKINETICS
 BASIC PHARMACOKINETICS MOHSEN A. HEDAYA CRC Press Taylor & Francis Croup Boca Raton London New York CRC Press is an imprint of the Taylor & Francis Group, an informa business Table of Contents Chapter
BASIC PHARMACOKINETICS MOHSEN A. HEDAYA CRC Press Taylor & Francis Croup Boca Raton London New York CRC Press is an imprint of the Taylor & Francis Group, an informa business Table of Contents Chapter
RENAL FUNCTION An Overview
 RENAL FUNCTION An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS II SEMINAR VJ. Temple 1 Kidneys
RENAL FUNCTION An Overview UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL MBBS II SEMINAR VJ. Temple 1 Kidneys
Pharmacokinetics of strong opioids. Susan Addie Specialist palliative care pharmacist
 Pharmacokinetics of strong opioids Susan Addie Specialist palliative care pharmacist What is the difference between pharmacokinetics and pharmacodynamics? Definitions Pharmacokinetics = what the body does
Pharmacokinetics of strong opioids Susan Addie Specialist palliative care pharmacist What is the difference between pharmacokinetics and pharmacodynamics? Definitions Pharmacokinetics = what the body does
Click to edit Master title style
 A Short Course in Pharmacokinetics Chris Town Research Pharmacokinetics Outline Pharmacokinetics - Definition Ideal Pharmacokinetic Parameters of a New Drug How do we optimize PK for new compounds Why
A Short Course in Pharmacokinetics Chris Town Research Pharmacokinetics Outline Pharmacokinetics - Definition Ideal Pharmacokinetic Parameters of a New Drug How do we optimize PK for new compounds Why
Fundamentals of Pharmacology for Veterinary Technicians Chapter 4
 (A) (B) Figure 4-1 A, B (C) FIGURE 4-1C The active transport process moves particles against the concentration gradient from a region of low concentration to a region of high concentration. Active transport
(A) (B) Figure 4-1 A, B (C) FIGURE 4-1C The active transport process moves particles against the concentration gradient from a region of low concentration to a region of high concentration. Active transport
MEDCHEM 570. First Midterm. January 30, 2015
 Name MEDCHEM 570 First Midterm January 30, 2015 Instructions: Exam packet totals 7 pages. The last page has a 5 points extra credit question. If you need additional space for a question go to the back
Name MEDCHEM 570 First Midterm January 30, 2015 Instructions: Exam packet totals 7 pages. The last page has a 5 points extra credit question. If you need additional space for a question go to the back
WHY... 8/21/2013 LEARNING OUTCOMES PHARMACOKINETICS I. A Absorption. D Distribution DEFINITION ADME AND THERAPEUIC ACTION
 PHARMACOKINETICS I Absorption & Distribution LEARNING OUTCOMES By the end of the lecture students will be able to.. Dr Ruwan Parakramawansha MBBS, MD, MRCP(UK),MRCPE, DMT(UK) (2013/08/21) Define pharmacokinetics,
PHARMACOKINETICS I Absorption & Distribution LEARNING OUTCOMES By the end of the lecture students will be able to.. Dr Ruwan Parakramawansha MBBS, MD, MRCP(UK),MRCPE, DMT(UK) (2013/08/21) Define pharmacokinetics,
Principles of Pharmacology. Pharmacokinetics & Pharmacodynamics. Mr. D.Raju, M.pharm, Lecturer PHL-358-PHARMACOLOGY AND THERAPEUTICS-I
 Principles of Pharmacology Pharmacokinetics & Pharmacodynamics PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr. D.Raju, M.pharm, Lecturer Pharmacokinetics Movement of drugs in the body Four Processes Absorption
Principles of Pharmacology Pharmacokinetics & Pharmacodynamics PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr. D.Raju, M.pharm, Lecturer Pharmacokinetics Movement of drugs in the body Four Processes Absorption
Outline Urinary System
 Urinary System and Excretion Bio105 Lecture Packet 20 Chapter 16 Outline Urinary System I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure B. Urine formation 1. Hormonal regulation
Urinary System and Excretion Bio105 Lecture Packet 20 Chapter 16 Outline Urinary System I. Function II. Organs of the urinary system A. Kidneys 1. Function 2. Structure B. Urine formation 1. Hormonal regulation
Biology 137 Introduction to Toxicology Name Midterm Exam 1 Fall Semester 2001
 Biology 137 Introduction to Toxicology Name Midterm Exam 1 Fall Semester 2001 Part I. Multiple choice. Two points each. 1. Toxicology is the study of A. prevalence of disease and death in a population
Biology 137 Introduction to Toxicology Name Midterm Exam 1 Fall Semester 2001 Part I. Multiple choice. Two points each. 1. Toxicology is the study of A. prevalence of disease and death in a population
ACUTE & CHRONIC ETHANOL EFFECTS An Overview
 ACUTE & CHRONIC ETHANOL EFFECTS An Overview University of Papua New Guinea School of Medicine & Health Sciences, Division of Basic Medical Sciences Clinical Biochemistry: PBL Seminar MBBS Yr 4 VJ Temple
ACUTE & CHRONIC ETHANOL EFFECTS An Overview University of Papua New Guinea School of Medicine & Health Sciences, Division of Basic Medical Sciences Clinical Biochemistry: PBL Seminar MBBS Yr 4 VJ Temple
Helping the liver to detoxify mycotoxins
 Helping the liver to detoxify mycotoxins Mycotoxin strategies have so far focused on binding compounds or detoxifying the compounds by feed additives. Animals however, can also detoxify mycotoxins themselves
Helping the liver to detoxify mycotoxins Mycotoxin strategies have so far focused on binding compounds or detoxifying the compounds by feed additives. Animals however, can also detoxify mycotoxins themselves
PHARMACOKINETICS: DRUG ABSORPTION, DISTRIBUTION, AND ELIMINATION
 CHAPTER 3 PHARMACOKINETICS: DRUG ABSORPTION, DISTRIBUTION, AND ELIMINATION AMANDA J. JENKINS, PH.D. AND EDWARD J. CONE, PH.D. INTRAMURAL RESEARCH PROGRAM, NATIONAL INSTITUTE ON DRUG ABUSE, NATIONAL INSTITUTES
CHAPTER 3 PHARMACOKINETICS: DRUG ABSORPTION, DISTRIBUTION, AND ELIMINATION AMANDA J. JENKINS, PH.D. AND EDWARD J. CONE, PH.D. INTRAMURAL RESEARCH PROGRAM, NATIONAL INSTITUTE ON DRUG ABUSE, NATIONAL INSTITUTES
A&P 2 CANALE T H E U R I N A R Y S Y S T E M
 A&P 2 CANALE T H E U R I N A R Y S Y S T E M URINARY SYSTEM CONTRIBUTION TO HOMEOSTASIS Regulates body water levels Excess water taken in is excreted Output varies from 2-1/2 liter/day to 1 liter/hour
A&P 2 CANALE T H E U R I N A R Y S Y S T E M URINARY SYSTEM CONTRIBUTION TO HOMEOSTASIS Regulates body water levels Excess water taken in is excreted Output varies from 2-1/2 liter/day to 1 liter/hour
Chapter 19 The Urinary System Fluid and Electrolyte Balance
 Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Chapter 19 The Urinary System Fluid and Electrolyte Balance Chapter Outline The Concept of Balance Water Balance Sodium Balance Potassium Balance Calcium Balance Interactions between Fluid and Electrolyte
Homeostatic Regulation
 Homeostatic Regulation A hormone is :a Water-soluble hormones: Composed of amino acids and bind a receptor protein on the of the target cell. This starts a signal cascade inside the cell and the signal
Homeostatic Regulation A hormone is :a Water-soluble hormones: Composed of amino acids and bind a receptor protein on the of the target cell. This starts a signal cascade inside the cell and the signal
2. List routes of exposure in the order of most rapid response.
 Practice Test questions: 1. What are the two areas of toxicology that a regulatory toxicologist must integrate in order to determine the "safety" of any chemical? 2. List routes of exposure in the order
Practice Test questions: 1. What are the two areas of toxicology that a regulatory toxicologist must integrate in order to determine the "safety" of any chemical? 2. List routes of exposure in the order