Meeting Agenda July 18, 2018 SHTF
|
|
|
- Christian Butler
- 5 years ago
- Views:
Transcription
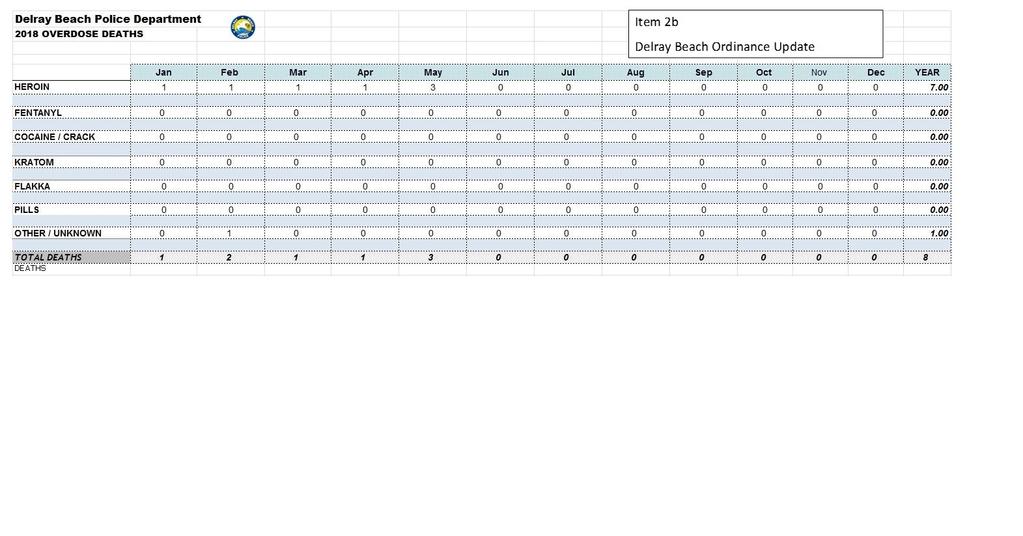
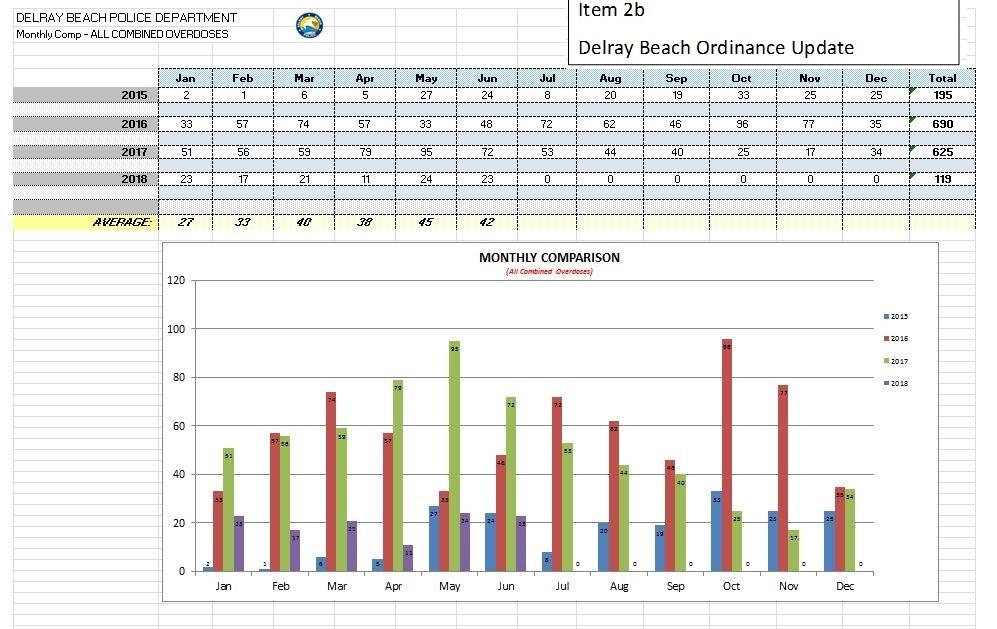
1 1. Introductions: Meeting Agenda July 18, 2018 SHTF 2. Updates a. 100 day challenge b. Delray Beach ordinance update Legislation 4. FARR a. HB 1069 i. Peer Navigators ii. Level II Background Revisions iii. Clarification of Referrals 1. Day Night/ Res Pecuniary Benefit iv. Fire Marshall Standards b. Housing i. Housing and Treatment Supports Communities (HATS) ii. SB 874 (Sen. Passidomo) Segregation of Trust Funds iii. HB 955 Insurance Parity for Substance Use Disorder c. Expansion of University of Miami Syringe Exchange Program F.S a. Current trends/program expansion b. Day/Night-Res. 5- Amethyst Petition/FARR Response c. One Step: Presentation 5. Public comments. 6. Closing remarks.
2
3
4 Florida Senate Bill No. CS/CS/CS/HB 1069, 1st Eng. SENATOR AMENDMENT Ì Î Senate Floor: 2/AD/2R 03/08/ :15 PM LEGISLATIVE ACTION House Senator Garcia moved the following: Senate Amendment (with title amendment) Delete line 110 and insert: 60 days after receipt of a complete application. The department shall provide technical assistance to the personnel requesting an exemption from disqualification regarding the process, including, but not limited to: 1. Providing, in plain language, a description of the process for requesting an exemption, instructions for completing the application to request an exemption, timeframes for Page 1 of 2 3/8/2018 9:01:38 AM
5 Florida Senate Bill No. CS/CS/CS/HB 1069, 1st Eng. SENATOR AMENDMENT Ì Î responses from the department, guidance on addressing problems commonly encountered in completing the application, and contact information for individuals available to provide technical assistance. 2. Within 10 days after a service provider personnel s initial submission of an application for an exemption, conducting a preliminary review and notifying such personnel of likely deficiencies in the application. 3. Advising the service provider personnel requesting an exemption that, if records from a jurisdiction are no longer available, alternative methods that such personnel may use to provide necessary information to the department. 4. Contacting service provider personnel whose applications for an exemption remain incomplete 30 days after the last communication by the department to determine if the personnel need additional technical assistance or wish to withdraw their applications. ================= T I T L E A M E N D M E N T ================ And the title is amended as follows: Delete line 14 and insert: timeframe; requiring the department to provide certain technical assistance to personnel requesting an exemption; authorizing an applicant for an exemption Page 2 of 2 3/8/2018 9:01:38 AM
6 Florida Senate Bill No. CS/CS/CS/HB 1069, 1st Eng. SENATOR AMENDMENT Ì Î Senate Floor: 1/AE/2R 03/08/ :09 PM LEGISLATIVE ACTION House Senator Rouson moved the following: Senate Amendment (with title amendment) Delete lines and insert: mental health or substance use disorders or co-occurring disorders under the supervision of persons who meet all personnel requirements of this chapter for up to 90 days after being notified of the disqualification or until the department a qualified professional licensed under chapter 490 or chapter 491 or a master s-level-certified addictions professional until the agency makes a final determination regarding the request for an Page 1 of 6 3/8/2018 4:58:42 PM seg1
7 Florida Senate Bill No. CS/CS/CS/HB 1069, 1st Eng. SENATOR AMENDMENT Ì Î exemption from disqualification, whichever is earlier. (h)(g) The department may not issue a regular license to any service provider that fails to provide proof that background screening information has been submitted in accordance with chapter 435. (4) EXEMPTIONS FROM DISQUALIFICATION. (a) The department may grant to any service provider personnel an exemption from disqualification as provided in s (b) Since rehabilitated substance abuse impaired persons are effective in the successful treatment and rehabilitation of individuals with substance use disorders, for service providers which treat adolescents 13 years of age and older, service provider personnel whose background checks indicate crimes under s (2)(e), s (4), s (2)(c), s , s , s , s , or s , and any related criminal attempt, solicitation, or conspiracy under s , may be exempted from disqualification from employment pursuant to this paragraph. (c) The department may grant exemptions from disqualification for service provider personnel to work solely in substance abuse treatment programs or facilities or in programs or facilities that treat co-occurring substance use and mental health disorders. The department may further limit such grant exemptions from disqualification which would limit service provider personnel to working with adults in substance abuse treatment facilities. (d) When evaluating a peer specialist s application for exemption from disqualification, the department shall consider: Page 2 of 6 3/8/2018 4:58:42 PM seg1
8 Florida Senate Bill No. CS/CS/CS/HB 1069, 1st Eng. SENATOR AMENDMENT Ì Î The need for peer specialists to provide support services and the shortage of professionals and paraprofessionals to provide behavioral health services. 2. That peer specialists may have criminal histories resulting from substance use disorders or mental illnesses that prevent them from meeting background screening requirements. 3. That peer specialists provide effective mental health and substance abuse treatment support services because they share common life experiences with the persons they assist and promote a sense of community among those in recovery. 4. That research has shown that peer support facilitates recovery and reduces health care costs. Section 4. Section , Florida Statutes, is created to read: Behavioral health peer specialists. (1) An individual is eligible for certification as a peer specialist if he or she has been in recovery from a substance use disorder or mental illness for at least 2 years or if he or she has experience as a family member or caregiver of a person with a substance use disorder or mental illness. (2) The department shall develop and implement a training program for individuals seeking certification as peer specialists. The department may designate one or more credentialing entities that have met nationally recognized standards for developing and administering professional certification programs to certify peer specialists. (3) An individual providing department-funded recovery support services as a peer specialist shall be certified pursuant to subsection (2). However, an individual who is not Page 3 of 6 3/8/2018 4:58:42 PM seg1
9 Florida Senate Bill No. CS/CS/CS/HB 1069, 1st Eng. SENATOR AMENDMENT Ì Î certified may provide recovery support services as a peer specialist for up to 1 year if he or she is working toward certification and is supervised by a qualified professional or by a certified peer specialist with supervisory training who has at least 3 years of full-time experience as a peer specialist at a licensed behavioral health organization. Section 5. Subsection (1) and subsection (6) of section , Florida Statutes, are amended to read: Voluntary certification of recovery residences. (1) The Legislature finds that a person suffering from addiction has a higher success rate of achieving long-lasting sobriety when given the opportunity to build a stronger foundation by living in a recovery residence while receiving treatment or after completing treatment. The Legislature further finds that this state and its subdivisions have a legitimate state interest in protecting these persons, who represent a vulnerable consumer population in need of adequate housing. It is the intent of the Legislature to protect persons who reside in a recovery residence. (6) All owners, directors, and chief financial officers of an applicant recovery residence are subject to level 2 background screening as provided under chapter 435 and s A recovery residence is ineligible for certification, and a credentialing entity shall deny a recovery residence s application, if any owner, director, or chief financial officer has been found guilty of, or has entered a plea of guilty or nolo contendere to, regardless of adjudication, any offense listed in s (4) or s (2) unless the department has issued an exemption under s or s In Page 4 of 6 3/8/2018 4:58:42 PM seg1
10 Florida Senate Bill No. CS/CS/CS/HB 1069, 1st Eng. SENATOR AMENDMENT Ì Î accordance with s , the department shall notify the credentialing agency of an owner s, director s, or chief financial officer s eligibility based on the results of his or her background screening. Section 6. Section , Florida Statutes, is amended to read: Referrals to or from recovery residences; prohibitions; penalties. (1) A service provider licensed under this part may not make a referral of a prospective, current, or discharged patient to, or accept a referral of such a patient from, a recovery residence unless the recovery residence holds a valid certificate of compliance as provided in s and is actively managed by a certified recovery residence administrator as provided in s (2) Subsection (1) does not apply to: (a) A licensed service provider under contract with a managing entity as defined in s (b) Referrals by a recovery residence to a licensed service provider when a resident has experienced a recurrence of substance use and, in the best judgment of the recovery residence administrator, it appears that the resident may benefit from clinical treatment services the recovery residence or its owners, directors, operators, or employees do not benefit, directly or indirectly, from the referral. (c) Referrals made before January 1, 2019 July 1, 2018, by a licensed service provider to that licensed service provider s wholly owned subsidiary, provided that applications and associated fees are submitted by July 1, Page 5 of 6 3/8/2018 4:58:42 PM seg1
11 Florida Senate Bill No. CS/CS/CS/HB 1069, 1st Eng. SENATOR AMENDMENT Ì Î (3) A recovery residence or its owners, directors, operators, employees, or volunteers may not receive a pecuniary benefit, directly or indirectly, from a licensed service provider in exchange for a referral made pursuant to subsection (1) or ================= T I T L E A M E N D M E N T ================ And the title is amended as follows: Delete lines and insert: certain treatment programs and facilities; requiring the department to consider certain factors when evaluating an application for an exemption; creating s , F.S.; providing qualifications for certification as a peer specialist; requiring the department to develop and implement a training program for individuals seeking certification as peer specialists; authorizing the department to designate certain credentialing entities to certify peer specialists; providing requirements for individuals providing certain recovery support services as peer specialists; amending s , F.S.; revising legislative findings relating to voluntary certification of recovery residences; revising background Page 6 of 6 3/8/2018 4:58:42 PM seg1
12 Florida Senate SB 1468 By Senator Rouson A bill to be entitled An act relating to alcohol and substance abuse prevention; creating s , F.S.; creating the Office of Alcohol and Drug Control Policy within the Executive Office of the Governor; providing for appointment of the director of the office; specifying duties of the office; requiring the office to adopt rules; requiring the office to submit an annual report to the Governor and the Legislature; amending s , F.S.; requiring the Agency for Health Care Administration, in consultation with the Department of Children and Families, to seek federal approval for waivers to increase federal Medicaid funding for a specified purpose; providing an effective date. Be It Enacted by the Legislature of the State of Florida: Section 1. Section 14.35, Florida Statutes, is created to read: Office of Alcohol and Drug Control Policy. (1) The Office of Alcohol and Drug Control Policy is created within the Executive Office of the Governor. The director, who shall be appointed by and serve at the pleasure of the Governor, shall oversee the office. (2) The office is responsible for all matters relating to the research of, coordination of, and execution of programs related to alcohol and drug control. (3) The office shall: (a) Develop a strategic plan to reduce the prevalence of Page 1 of 6 CODING: Words stricken are deletions; words underlined are additions.
13 Florida Senate SB alcohol and substance abuse in the state. (b) Monitor data and issues related to state policies concerning youth alcohol use prevention and state substance abuse policies, the impact of such policies on state and local programs, and the flexibility of such policies to adapt to the needs of local communities and service providers. (c) Collect data related to drug crimes and overdoses to generate statistical and analytical reports containing recommendations for this state s criminal justice system. (d) Issue policy recommendations to executive branch agencies for alcohol and substance abuse prevention and treatment to ensure efficiency in efforts undertaken by the administration. (e) Work with behavioral health managing entities to identify existing resources and programs in each community which provide alcohol and substance abuse prevention education or treatment. (f) Facilitate coordination of alcohol and substance abuse prevention education and treatment between the courts, local and state agencies, organizations, service providers, and related public or private programs concerning alcohol and substance abuse. (g) Assist behavioral health managing entities in coordinating activities to ensure the availability of training, technical assistance, and consultation to local service providers for programs funded by the state which provide services related to alcohol or substance abuse. (h) Act as a referral source of information, using existing information clearinghouse resources. Page 2 of 6 CODING: Words stricken are deletions; words underlined are additions.
14 Florida Senate SB (i) Search for grant opportunities to fund the office and its initiatives. (j) Be knowledgeable on alcohol and substance abuse prevention and treatment programs and initiatives in this state and in other states. (k) Review existing research on programs related to substance abuse prevention and treatment. (l) Coordinate with the Department of Education to link schools with community-based agencies and county health departments to implement early intervention programs for the prevention of alcohol and substance abuse. (m) Coordinate media campaigns to demonstrate the negative impact of substance abuse disorders and to prevent the development of such disorders in children, young people, and adults. (n) Prepare and submit legislative budget requests. (o) Adopt rules necessary to administer this section. (p) Submit a report annually to the Governor, the President of the Senate, and the Speaker of the House of Representatives on the effectiveness of state policies and coordinated state efforts related to substance abuse. Section 2. Subsection (14) is added to section , Florida Statutes, to read: Cost-effective purchasing of health care. The agency shall purchase goods and services for Medicaid recipients in the most cost-effective manner consistent with the delivery of quality medical care. To ensure that medical services are effectively utilized, the agency may, in any case, require a confirmation or second physician s opinion of the correct Page 3 of 6 CODING: Words stricken are deletions; words underlined are additions.
15 Florida Senate SB diagnosis for purposes of authorizing future services under the Medicaid program. This section does not restrict access to emergency services or poststabilization care services as defined in 42 C.F.R. s Such confirmation or second opinion shall be rendered in a manner approved by the agency. The agency shall maximize the use of prepaid per capita and prepaid aggregate fixed-sum basis services when appropriate and other alternative service delivery and reimbursement methodologies, including competitive bidding pursuant to s , designed to facilitate the cost-effective purchase of a case-managed continuum of care. The agency shall also require providers to minimize the exposure of recipients to the need for acute inpatient, custodial, and other institutional care and the inappropriate or unnecessary use of high-cost services. The agency shall contract with a vendor to monitor and evaluate the clinical practice patterns of providers in order to identify trends that are outside the normal practice patterns of a provider s professional peers or the national guidelines of a provider s professional association. The vendor must be able to provide information and counseling to a provider whose practice patterns are outside the norms, in consultation with the agency, to improve patient care and reduce inappropriate utilization. The agency may mandate prior authorization, drug therapy management, or disease management participation for certain populations of Medicaid beneficiaries, certain drug classes, or particular drugs to prevent fraud, abuse, overuse, and possible dangerous drug interactions. The Pharmaceutical and Therapeutics Committee shall make recommendations to the agency on drugs for which prior authorization is required. The agency shall inform Page 4 of 6 CODING: Words stricken are deletions; words underlined are additions.
16 Florida Senate SB the Pharmaceutical and Therapeutics Committee of its decisions regarding drugs subject to prior authorization. The agency is authorized to limit the entities it contracts with or enrolls as Medicaid providers by developing a provider network through provider credentialing. The agency may competitively bid singlesource-provider contracts if procurement of goods or services results in demonstrated cost savings to the state without limiting access to care. The agency may limit its network based on the assessment of beneficiary access to care, provider availability, provider quality standards, time and distance standards for access to care, the cultural competence of the provider network, demographic characteristics of Medicaid beneficiaries, practice and provider-to-beneficiary standards, appointment wait times, beneficiary use of services, provider turnover, provider profiling, provider licensure history, previous program integrity investigations and findings, peer review, provider Medicaid policy and billing compliance records, clinical and medical record audits, and other factors. Providers are not entitled to enrollment in the Medicaid provider network. The agency shall determine instances in which allowing Medicaid beneficiaries to purchase durable medical equipment and other goods is less expensive to the Medicaid program than long-term rental of the equipment or goods. The agency may establish rules to facilitate purchases in lieu of long-term rentals in order to protect against fraud and abuse in the Medicaid program as defined in s The agency may seek federal waivers necessary to administer these policies. (14) The agency, in consultation with the department, shall seek federal approval for a waiver to increase the availability Page 5 of 6 CODING: Words stricken are deletions; words underlined are additions.
17 Florida Senate SB of federal Medicaid funding to provide programs that improve the quality of and access to treatment for individuals with substance abuse disorders served by the Medicaid program and to provide a more comprehensive continuum of care for individuals with substance abuse disorders, including detoxification services, residential services, medication-assisted treatment, targeted case management, and recovery support that Medicaid is unable to cover without a waiver. Section 3. This act shall take effect July 1, Page 6 of 6 CODING: Words stricken are deletions; words underlined are additions.
18 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S A bill to be entitled An act relating to substance abuse services; amending s , F.S.; authorizing the Department of Health and the Agency for Health Care Administration to grant exemptions from disqualification for service provider personnel to work solely in certain treatment programs and facilities; amending s , F.S.; defining the term "peer specialist"; amending s , F.S.; revising provisions relating to background checks and exemptions from disqualification for certain service provider personnel; requiring the Department of Children and Families to grant or deny an exemption from disqualification within a certain timeframe; authorizing an applicant for an exemption to work under the supervision of certain persons for a specified period of time while his or her application is pending; authorizing certain persons to be exempted from disqualification from employment; authorizing the department to grant exemptions from disqualification for service provider personnel to work solely in certain treatment programs and facilities; creating s , F.S.; providing qualifications for certification as a peer specialist; requiring the department to develop and implement a training program for individuals seeking certification as peer Page 1 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
19 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S specialists; authorizing the department to designate certain credentialing entities to certify peer specialists; providing requirements for individuals providing certain recovery support services as peer specialists; amending s , F.S.; revising legislative findings relating to voluntary certification of recovery residences; requiring recovery residences to comply with specified Florida Fire Prevention Code provisions; revising background screening requirements for owners, directors, and chief financial officers of recovery residences; amending s , F.S.; providing exceptions to limitations on referrals by recovery residences to licensed service providers; providing additional conditions for an exception to limitations on referrals by licensed service providers to their wholly owned subsidiaries; prohibiting recovery residences and specified affiliated individuals from receiving pecuniary benefits from licensed service providers for certain referrals; providing penalties; amending s , F.S.; authorizing certain persons to be exempted from disqualification from employment; amending ss , , and , F.S.; conforming cross-references; providing an effective date. Page 2 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
20 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S Be It Enacted by the Legislature of the State of Florida: Section 1. Subsection (2) of section , Florida Statutes, is amended to read: Screening of mental health personnel. (2)(a) The department or the Agency for Health Care Administration may grant exemptions from disqualification as provided in chapter 435. (b) The department or the Agency for Health Care Administration, as applicable, may grant exemptions from disqualification for service provider personnel to work solely in mental health treatment programs or facilities or in programs or facilities that treat co-occurring substance use and mental health disorders. Section 2. Subsections (30) through (49) of section , Florida Statutes, are renumbered as subsections (31) through (50), respectively, and a new subsection (30) is added to that section to read: Definitions. As used in this chapter, except part VIII, the term: (30) "Peer specialist" means a person who has been in recovery from a substance use disorder or mental illness for at least 2 years who uses his or her personal experience to deliver services in behavioral health settings to support others in Page 3 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
21 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S their recovery, or a person who has experience as a family member or a caregiver of a person with a substance use disorder or mental illness. The term does not include a person who is a qualified professional or otherwise certified under chapter 394 or 397. Section 3. Paragraphs (a), (f), and (g) of subsection (1) and subsection (4) of section , Florida Statutes, are amended to read: Background checks of service provider personnel. (1) PERSONNEL BACKGROUND CHECKS; REQUIREMENTS AND EXCEPTIONS. (a) For all individuals screened on or after July 1, 2018, background checks shall apply as follows: 1. All owners, directors, chief financial officers, and clinical supervisors of service providers are subject to level 2 background screening as provided under chapter 435. Such screening shall also include background screening as provided in s Inmate substance abuse programs operated directly or under contract with the Department of Corrections are exempt from this requirement. 2. All service provider personnel who have direct contact with children receiving services or with adults who are developmentally disabled receiving services are subject to level 2 background screening as provided under chapter 435. Such screening shall also include background screening as provided in Page 4 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
22 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S s All peer specialists who have direct contact with individuals receiving services are subject to level 2 background screening as provided under chapter 435. Such screening shall also include background screening as provided in s (f) Service provider personnel who request an exemption from disqualification must submit the request within 30 days after being notified of the disqualification. The department shall grant or deny the exemption from disqualification within 60 days after receipt of a complete application. (g) If 5 years or more have elapsed since the applicant for the exemption completed or was lawfully released from confinement, supervision, or nonmonetary condition imposed by the court for the most recent disqualifying offense, such applicant service provider personnel may work with adults with substance use disorders under the supervision of persons who meet all personnel requirements of this chapter for up to 90 days after being notified of the disqualification or until the department a qualified professional licensed under chapter 490 or chapter 491 or a master's-level-certified addictions professional until the agency makes a final determination regarding the request for an exemption from disqualification, whichever is earlier. (h)(g) The department may not issue a regular license to any service provider that fails to provide proof that background Page 5 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
23 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S screening information has been submitted in accordance with chapter 435. (4) EXEMPTIONS FROM DISQUALIFICATION. (a) The department may grant to any service provider personnel an exemption from disqualification as provided in s (b) Since rehabilitated substance abuse impaired persons are effective in the successful treatment and rehabilitation of individuals with substance use disorders, for service providers which treat adolescents 13 years of age and older, service provider personnel whose background checks indicate crimes under s (2)(e), s (4), s (2)(c), s , s , s , s , or s , and any related criminal attempt, solicitation, or conspiracy under s , may be exempted from disqualification from employment pursuant to this paragraph. (c) The department may grant exemptions from disqualification for service provider personnel to work solely in substance abuse treatment programs or facilities or in programs or facilities that treat co-occurring substance use and mental health disorders. The department may further limit such grant exemptions from disqualification which would limit service provider personnel to working with adults in substance abuse treatment facilities. Section 4. Section , Florida Statutes, is created Page 6 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
24 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S to read: Behavioral health peer specialists. (1) An individual is eligible for certification as a peer specialist if he or she has been in recovery from a substance use disorder or mental illness for at least 2 years or if he or she has experience as a family member or caregiver of a person with a substance use disorder or mental illness. (2) The department shall develop and implement a training program for individuals seeking certification as peer specialists. The department may designate one or more credentialing entities that have met nationally recognized standards for developing and administering professional certification programs to certify peer specialists. (3) An individual providing department-funded recovery support services as a peer specialist shall be certified pursuant to subsection (2). However, an individual who is not certified may provide recovery support services as a peer specialist for up to 1 year if he or she is working toward certification and is supervised by a qualified professional or by a certified peer specialist with supervisory training who has at least 3 years of full-time experience as a peer specialist at a licensed behavioral health organization. Section 5. Subsection (1), paragraph (m) of subsection (3), and subsection (6) of section , Florida Statutes, are amended to read: Page 7 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
25 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S Voluntary certification of recovery residences. (1) The Legislature finds that a person suffering from addiction has a higher success rate of achieving long-lasting sobriety when given the opportunity to build a stronger foundation by living in a recovery residence while receiving treatment or after completing treatment. The Legislature further finds that this state and its subdivisions have a legitimate state interest in protecting these persons, who represent a vulnerable consumer population in need of adequate housing. It is the intent of the Legislature to protect persons who reside in a recovery residence. (3) A credentialing entity shall require the recovery residence to submit the following documents with the completed application and fee: (m) Proof of satisfactory fire, safety, and health inspections. A recovery residence must comply with the provisions of the Florida Fire Prevention Code which apply to one-family and two-family dwellings, public lodging establishments, or rooming houses, or other housing facilities, as applicable. (6) All owners, directors, and chief financial officers of an applicant recovery residence are subject to level 2 background screening as provided under chapter 435 and s A recovery residence is ineligible for certification, and a credentialing entity shall deny a recovery residence's Page 8 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
26 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S application, if any owner, director, or chief financial officer has been found guilty of, or has entered a plea of guilty or nolo contendere to, regardless of adjudication, any offense listed in s (4) or s (2) unless the department has issued an exemption under s or s In accordance with s , the department shall notify the credentialing agency of an owner's, director's, or chief financial officer's eligibility based on the results of his or her background screening. Section 6. Section , Florida Statutes, is amended to read: Referrals to or from recovery residences; prohibitions; penalties. (1) A service provider licensed under this part may not make a referral of a prospective, current, or discharged patient to, or accept a referral of such a patient from, a recovery residence unless the recovery residence holds a valid certificate of compliance as provided in s and is actively managed by a certified recovery residence administrator as provided in s (2) Subsection (1) does not apply to: (a) A licensed service provider under contract with a managing entity as defined in s (b) Referrals by a recovery residence to a licensed service provider when a resident has experienced a recurrence of Page 9 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
27 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S substance use and, in the best judgment of the recovery residence administrator, it appears that the resident may benefit from clinical treatment services the recovery residence or its owners, directors, operators, or employees do not benefit, directly or indirectly, from the referral. (c) Referrals made before January 1, 2019 July 1, 2018, by a licensed service provider to that licensed service provider's wholly owned subsidiary, provided that applications and associated fees are submitted by July 1, (3) A recovery residence or its owners, directors, operators, employees, or volunteers may not receive a pecuniary benefit, directly or indirectly, from a licensed service provider for a referral made pursuant to subsection (1) or subsection (2). (4)(3) For purposes of this section, a licensed service provider or recovery residence shall be considered to have made a referral if the provider or recovery residence has informed a patient by any means about the name, address, or other details of a recovery residence or licensed service provider, or informed a licensed service provider or a recovery residence of any identifying details about a patient. (5)(4) A licensed service provider shall maintain records of referrals to or from recovery residences as may be prescribed by the department in rule. (6)(5) After June 30, 2019, a licensed service provider Page 10 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
28 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S violating this section shall be subject to an administrative fine of $1,000 per occurrence. Repeat violations of this section may subject a provider to license suspension or revocation pursuant to s (7)(6) Nothing in this section requires a licensed service provider to refer a patient to or to accept a referral of a patient from a recovery residence. Section 7. Subsection (2) of section , Florida Statutes, is amended to read: Exemptions from disqualification. Unless otherwise provided by law, the provisions of this section apply to exemptions from disqualification for disqualifying offenses revealed pursuant to background screenings required under this chapter, regardless of whether those disqualifying offenses are listed in this chapter or other laws. (2) Persons employed, or applicants for employment, by treatment providers who treat adolescents 13 years of age and older who are disqualified from employment solely because of crimes under s (2)(e), s (4), s (2)(c), s , s , s , s , or s , and any related criminal attempt, solicitation, or conspiracy under s , may be exempted from disqualification from employment pursuant to this chapter without application of the waiting period in subparagraph (1)(a)1. Section 8. Paragraph (e) of subsection (5) of section Page 11 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
29 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S , Florida Statutes, is amended to read: Discretionary sales surtaxes; legislative intent; authorization and use of proceeds. It is the legislative intent that any authorization for imposition of a discretionary sales surtax shall be published in the Florida Statutes as a subsection of this section, irrespective of the duration of the levy. Each enactment shall specify the types of counties authorized to levy; the rate or rates which may be imposed; the maximum length of time the surtax may be imposed, if any; the procedure which must be followed to secure voter approval, if required; the purpose for which the proceeds may be expended; and such other requirements as the Legislature may provide. Taxable transactions and administrative procedures shall be as provided in s (5) COUNTY PUBLIC HOSPITAL SURTAX. Any county as defined in s (1) may levy the surtax authorized in this subsection pursuant to an ordinance either approved by extraordinary vote of the county commission or conditioned to take effect only upon approval by a majority vote of the electors of the county voting in a referendum. In a county as defined in s (1), for the purposes of this subsection, "county public general hospital" means a general hospital as defined in s which is owned, operated, maintained, or governed by the county or its agency, authority, or public health trust. Page 12 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
30 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S (e) A governing board, agency, or authority shall be chartered by the county commission upon this act becoming law. The governing board, agency, or authority shall adopt and implement a health care plan for indigent health care services. The governing board, agency, or authority shall consist of no more than seven and no fewer than five members appointed by the county commission. The members of the governing board, agency, or authority shall be at least 18 years of age and residents of the county. No member may be employed by or affiliated with a health care provider or the public health trust, agency, or authority responsible for the county public general hospital. The following community organizations shall each appoint a representative to a nominating committee: the South Florida Hospital and Healthcare Association, the Miami-Dade County Public Health Trust, the Dade County Medical Association, the Miami-Dade County Homeless Trust, and the Mayor of Miami-Dade County. This committee shall nominate between 10 and 14 county citizens for the governing board, agency, or authority. The slate shall be presented to the county commission and the county commission shall confirm the top five to seven nominees, depending on the size of the governing board. Until such time as the governing board, agency, or authority is created, the funds provided for in subparagraph (d)2. shall be placed in a restricted account set aside from other county funds and not disbursed by the county for any other purpose. Page 13 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
31 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S The plan shall divide the county into a minimum of four and maximum of six service areas, with no more than one participant hospital per service area. The county public general hospital shall be designated as the provider for one of the service areas. Services shall be provided through participants' primary acute care facilities. 2. The plan and subsequent amendments to it shall fund a defined range of health care services for both indigent persons and the medically poor, including primary care, preventive care, hospital emergency room care, and hospital care necessary to stabilize the patient. For the purposes of this section, "stabilization" means stabilization as defined in s (46) s (45). Where consistent with these objectives, the plan may include services rendered by physicians, clinics, community hospitals, and alternative delivery sites, as well as at least one regional referral hospital per service area. The plan shall provide that agreements negotiated between the governing board, agency, or authority and providers shall recognize hospitals that render a disproportionate share of indigent care, provide other incentives to promote the delivery of charity care to draw down federal funds where appropriate, and require cost containment, including, but not limited to, case management. From the funds specified in subparagraphs (d)1. and 2. for indigent health care services, service providers shall receive reimbursement at a Medicaid rate to be determined by the Page 14 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
32 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S governing board, agency, or authority created pursuant to this paragraph for the initial emergency room visit, and a per-member per-month fee or capitation for those members enrolled in their service area, as compensation for the services rendered following the initial emergency visit. Except for provisions of emergency services, upon determination of eligibility, enrollment shall be deemed to have occurred at the time services were rendered. The provisions for specific reimbursement of emergency services shall be repealed on July 1, 2001, unless otherwise reenacted by the Legislature. The capitation amount or rate shall be determined before program implementation by an independent actuarial consultant. In no event shall such reimbursement rates exceed the Medicaid rate. The plan must also provide that any hospitals owned and operated by government entities on or after the effective date of this act must, as a condition of receiving funds under this subsection, afford public access equal to that provided under s as to any meeting of the governing board, agency, or authority the subject of which is budgeting resources for the retention of charity care, as that term is defined in the rules of the Agency for Health Care Administration. The plan shall also include innovative health care programs that provide cost-effective alternatives to traditional methods of service and delivery funding. 3. The plan's benefits shall be made available to all Page 15 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
33 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S county residents currently eligible to receive health care services as indigents or medically poor as defined in paragraph (4)(d). 4. Eligible residents who participate in the health care plan shall receive coverage for a period of 12 months or the period extending from the time of enrollment to the end of the current fiscal year, per enrollment period, whichever is less. 5. At the end of each fiscal year, the governing board, agency, or authority shall prepare an audit that reviews the budget of the plan, delivery of services, and quality of services, and makes recommendations to increase the plan's efficiency. The audit shall take into account participant hospital satisfaction with the plan and assess the amount of poststabilization patient transfers requested, and accepted or denied, by the county public general hospital. Section 9. Section , Florida Statutes, is amended to read: Substance abuse treatment services; qualified professional. Notwithstanding any other provision of law, a person who was certified through a certification process recognized by the former Department of Health and Rehabilitative Services before January 1, 1995, may perform the duties of a qualified professional with respect to substance abuse treatment services as defined in this chapter, and need not meet the certification requirements contained in s (35) s. Page 16 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
34 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S (34). Section 10. Paragraphs (d) and (g) of subsection (1) of section , Florida Statutes, are amended to read: Drug-free workplace program requirements. The following provisions apply to a drug-free workplace program implemented pursuant to law or to rules adopted by the Agency for Health Care Administration: (1) DEFINITIONS. Except where the context otherwise requires, as used in this act: (d) "Drug rehabilitation program" means a service provider, established pursuant to s (44) s (43), that provides confidential, timely, and expert identification, assessment, and resolution of employee drug abuse. (g) "Employee assistance program" means an established program capable of providing expert assessment of employee personal concerns; confidential and timely identification services with regard to employee drug abuse; referrals of employees for appropriate diagnosis, treatment, and assistance; and followup services for employees who participate in the program or require monitoring after returning to work. If, in addition to the above activities, an employee assistance program provides diagnostic and treatment services, these services shall in all cases be provided by service providers pursuant to s (44) s (43). Section 11. This act shall take effect July 1, Page 17 of 17 CODING: Words stricken are deletions; words underlined are additions. hb e1
35 Voluntary certification of recovery residences. (3) A credentialing entity shall require the recovery residence to submit the following documents with the completed application and fee: (m) Proof of satisfactory fire, safety, and health inspections. A recovery residence must comply with the provisions of the Florida Fire Prevention Code which apply to one-family and two-family dwellings, public lodging establishments, or rooming houses, or other housing facilities, as applicable. (m) Proof of satisfactory fire, safety, and health inspections. A recovery residence must comply with the provisions of the Florida Fire Prevention Code which apply to one-family and two-family dwellings, multi-family dwellings, public lodging establishments, or rooming houses, or other housing facilities, as applicable. The use of a structure as a recovery residence, standing alone, shall not be deemed a conversion of use requiring heightened life safety standards including but not limited to fire sprinkler protection Page 1 of 1 CODING: Words stricken are deletions; words underlined are additions. Draft Legislation 2018 part 1

36

37
38


39
40
41 HOUSING AND TREATMENT SUPPORTS (HATS) COMMUNITIES A Proposal to Integrate Permanent Supportive Housing with Targeted Support Services to Individuals/Families Who Are Chronically Homeless or at Risk of Being Homeless and Who Have One or More Behavioral Health Conditions $4.444 million to Serve 180 Single Individual/Family Units This proposal promotes funding of three HATS community pilots in conjunction with funding awarded through the Florida Housing Finance Corporation in targeted communities across the state. The plan is to create Housing First opportunities to for targeted individuals who frequent acute care services as a result of their recurring mental health or substance use order condition. This initiative requires coordination at the local level between the managing entity, local housing authorities, behavioral health providers, and community housing resources. Workforce training and linkages to primary care will also be a focus. Homelessness in Florida The Department of Children and Families (DCF) and the Florida Housing Finance Corporation (FHFC) utilize several funding mechanisms to address homeless and special needs housing. Florida s per capita average is 21.2 per 10,000 individuals vs. national per capita average of 18.3 per 10,000 individuals. There are 5,185 homeless individuals (33.2%) with a substance use disorder. There are 5,352 homeless individuals (34.2%) with a mental illness. This is a high percentage for both than data collected in There is a GAP that connects homeless individuals who have substance use disorders or mental illness to housing and treatment supports critically needed to promote greater selfdetermination, and achieve long-term housing stability and economic self-sufficiency. Using the existing Housing First EBP combined with other evidence-informed interventions to address behavioral health conditions, multi-disciplinary teams are proposed within a community to place individuals/families who are chronically homeless or at risk of being homeless and have one or more cooccurring mental health or substance use disorder into permanent or supportive housing and linking them with behavioral health, primary care and environmental supports. Target population The target populations in this proposal are: Individuals and families who are chronically homeless or at risk of being homeless Have multiple and complex health and behavioral health conditions Have frequent stays in jails, state hospitals, or prisons Are high utilizers of acute care services Case management and ancillary services Case management, in various forms, is critical to ensuring the success of a HATS community. Some of the services that may be provided in case management include, but are not limited to life skills development, community linkages, parenting and intensive supports Managing Entities Managing Entities will coordinate efforts with DCF, the Agency for Health Care Administration, Florida Department of Veterans Affairs, Florida Department of Elderly Affairs, the Florida Housing Finance Corporation, community-based providers, county jails, hospitals, Federally Qualified Health Centers, property developers and managers, local government, county school systems, and charitable organizations. 1
42 HATS Service Team At a minimum, a HATS community should utilize peer support specialists and tenant services coordinators who work in concert with each other. Additionally, a HATS community should have a flexible behavioral health component built into the program to provide treatment for mental health, substance abuse or cooccurring behavioral health disorders. Some of these will include: Treatment for Behavioral health conditions Tenant Supportive Care Manager Tenant Services Coordinator Peer Support Specialists Financing a HATS Community Each HATS community will serve an approximate 60 individual/family units and is expected to cost $1.482 million per HATS Community for the first year ($4.444 million total for three communities). The front-end expenses for new tenants, such as start-up costs will not carry forward into the second year of occupancy. There is also a greater chance that treatment supports will decrease over time. Therefore, second year funding for a HATS Community will not require as much funding as the first year. Based on case load ratio for other targeting programs such as Family Intensive Treatment, Community Action Teams, and FACT, it is recommended the following: HATS Staffing Team ($318,000 total per community x 3 communities = $952,000) Tenant Care Manager: 1:60 housing units (1.0 FTE = $60,000) Tenant Services Coordinator: 1:20 housing units (3.0 FTE x $48,000 = $144,000) Peer Support Specialists: 1:205 individuals (3.0 FTE x $38,000 = $114,000) HATS Services and Supports ($1.092 million/community x 3 communities = $3.276 million) Behavioral Health treatment capacity (30 tenants x 3 hrs/week x $150/hr x 36/weeks =$486,000): While the target population has an identified substance abuse, behavioral health or co-occurring disorder, the likelihood of each of them receiving treatment is not realistic. The target goal for individuals to receive treatment for their mental health or substance use disorders is 50%. While funding for treatment services should be flexible, it is assumed an individual who seeks treatment will receive a minimum of 3 hours of outpatient treatment per week for a period of nine months. Supportive Housing Rental subsidies: ($400 per unit/mo x 60 units x 12 mo. = $288,000) Rental supports consistent with funds provided to Assisted Living Facilities Start-up funding: ($3000 per unit x 60 units + plus ($30,000 turnover) = $210,000): Once a unit is available for a tenant, initial funding will equip the unit with furniture and other supports necessary for occupancy. Discretionary funds: ($250 per unit/mo x 60 units x 12 mo = $180,000): Resources to assist success in housing such as child care, transportation, workforce training, and costs associated with housing. 2
43 HOUSING AND TREATMENT SUPPORTS (HATS) COMMUNITIES A Proposal to Integrate Permanent Supportive Housing with Targeted Support Services to Individuals/Families Who Are Chronically Homeless or at Risk of Being Homeless and Who Have One or More Behavioral Health Conditions $4.344 million to Serve 180 Single Individual/Family Units This proposal is intended to use existing evidence-based practices to develop a multi-disciplinary approach to place individuals/families with a substance use or mental health disorder who are chronically homeless or at risk of being homeless or for individuals who struggle to maintain safe affordable housing into permanent or supportive housing and linking them with behavioral health, primary care and environmental supports to promote greater self-determination, economic selfsufficiency, and long-term housing stability. This proposal maximizes federal, state local and community resources to achieve the greatest return on investment. Background Supportive Housing, Defined The Substance Abuse Mental Health Services Administration (SAMHSA) defines Supportive Housing as an evidence-based practice that combines permanent, affordable housing with flexible, voluntary and client-centered support services designed to help tenants stay housed and build necessary skills to live independently. There are four permanent supportive housing (PSH) models commonly used today (Burt, 2008; Locke, Khadduri, and O Hara, 2007): Single-site, all-psh building: Project operates in only one building, with tenants wholly occupying the building; typically with more than eight units in the building Single-site, mixed-used building: Project operated in one building, but project tenants represent only a minority or portion of whole tenant population Scattered-site: Projects place tenants in apartments scattered throughout a community Clustered-scattered: Project operates two or more small buildings, wholly occupied by project tenants in close proximity to each other Literature Review Research has long validated the success of Supportive Housing (Caton, Wilkens, and Anderson, 2007; Rog, Holupka and Brito, 1996; Rog, 2004) for three primary reasons. First, it supports the theory that housing linked with supports greatly improves long-term stability. Second, there is a public cost avoidance from acute care, as well as other public outlay areas such as the criminal 1
44 justice system (Gulcer, et al., 2003; Culhane et al., 2002; Larimer et al., 2009). Finally, there is an overall improvement in health, and other aspects of an individual s life. For purposes of this proposal, the literature review will primarily focus on cost avoidance and offsets and overall improvement in behavioral and physical health conditions, which greatly contribute to cost savings. Local Government Cost Studies: The volume of research drawing same or similar conclusions has prompted state and local governments to develop and analyze their own initiatives, many of which placed an emphasis on individuals with one or more behavioral health conditions. Nearly every analysis showed a costsavings to state and local governments. In particular: A study of 1811 Eastlake, run by Seattle s Downtown Emergency Services Center (Larimer et al., 2009), that targeted the most frequent users of alcohol-related hospital emergency room care, the sobering center, and the county jail, and showed substantial cost savings. A study of Central City Concern s (CCC s) Community Empowerment Program, in Portland, Oregon (Moore, 2006), that also showed cost savings. Two studies in Maine, one in the greater Portland area (Mondello et al., 2007) and one, the first in the country to focus on an entirely rural population (Mondello et al., 2009), that showed cost savings while developing study techniques to cover a very broad array of services offered by 102 organizations and the ability to conduct a cost analysis statewide in a very rural state. Cost avoidance information was collected for one year before and one year after the first 49 individuals were housed in Skid Row Los Angeles: Project 50. Participants averaged 9.8 years homeless; 55 percent were tri-morbid (mental health, substance use, and chronic illness conditions). Results showed that more money was spent on hospital and jail visits during the year prior to housing than the net operating cost of Project 50. Inpatient days were reduced by about 75 percent, emergency department visits by about 70 percent, and days in jail by about 83 percent (Los Angeles County Department of Mental Health). An extensive and complex study in Los Angeles (Flaming et al., 2009) examined service use across nine public agencies for over 10,000 recipients of General Relief, many of them homeless. The study found cost offsets for housing placement while considering several levels of service need and use of services. It showed that public costs go down when individuals are no longer homeless. In the book Where We Sleep (Flaming et al., 2009), data examining common characteristics on over 10,000 single adults showed that individuals who are older, have a long history of unemployment, disabled, and have a substance use or mental health disorder were among the costliest. 2
45 A 2014 Central Florida regional study showed that the aggregate costs of emergency shelter, incarcerations, emergency room visits, and inpatient hospitalizations for individuals who are chronically homeless cost is $31,065 per person annually; whereas the annual cost of permanent supportive housing is $10,051 a 68% cost savings. Value of Supportive Housing for Individuals with Substance Use Disorders Numerous studies validate theories that PSH with treatment supports will increase housing stability and reduce substance abuse (Rog et al., 2014; Clark & Rich, 2003). Most notably: National Center on Family Homelessness (2009), for the Minnesota Supportive Housing and Managed Care Pilot Project, for 343 adults (both single and in families) in Ramsey and Blue Earth Counties. Outcomes for pilot project participants showed self-reported reductions in use of alcohol and drugs. VA patients in the early 1990s (n=460) were randomly assigned to one of the three groups: (1) HUD-VASH, which offered both Section 8 vouchers and intensive case management; (2) case management only; and (3) standard VA care. Using multiple imputation statistical methods to account for the missing observations (which were usually missed appointments), significant benefits in reduced abuse of drugs and alcohol were found for those assigned to HUD-VASH compared to the other two groups (Cheng et al., 2007). Residents of 1811 Eastlake in Seattle, who were offered PSH because they were frequent users of alcohol-related emergency room care, detoxification/sobering facilities, and jail reported reduced alcohol consumption and fewer days of drinking to intoxication after they were housed (Larimer et al., 2009, n=75). Value of Supportive Housing for Individuals with Mental Health Disorders: Research suggests that there is improved functioning and reduced anti-social behaviors (Sacks, et al, 2003). Conversely, Greenwood et al. (2005) found that the lack of personal choice and control was associated with experience in mental health symptoms. Additionally, the following studies reported: National Center on Family Homelessness found that during follow-up interviews, adult participants self-reported an average reduction of one symptom from intake to the end of the follow-up period. While this result may appear small, that symptom was often a big one such as going from hearing voices frequently to never. Assessment of the impacts on participants of receiving PSH through the first 11 projects funded by the HUD/HHS/VA Chronic Homelessness Initiative (Rosenheck and Mares, 2009) found reduced psychiatric symptomatology during the study s four years of follow-up. Data were collected through formal interviews with participants as part of a national evaluation of the 11 projects run through VA. Schwarcz et al. (2009), examining outcomes after housing for 106 people with AIDS and comparing them to 39 similar people on the waiting list for housing through the Department 3
46 of Public Health s (DPH s) Direct Access to Housing (DAH) program in San Francisco, found better adherence to antipsychotic medications as documented by clinic records. Perlman and Parvensky (2006) report that 43 percent of the sample they followed, of participants in Denver s Housing First Collaborative, had improvements in their mental health status documented by clinic records. Value of Supportive Housing for Individuals with Physical Health Conditions/Frequent Hospital Stays: There is robust evidence from both randomized trials and quasi-experimental studies that supported housing interventions of various types can significantly improve residential status among individuals who are psychiatrically disabled (Tsemberis et al., 2004; Gulcur et al., 2003; Shern et al., 1997; Rosenheck et al., 2003; Goldfinger et al., 1999). Overall hospitalizations due to physical or co-morbid conditions decreases in both emergency room visits and inpatient stays as well as a decrease in acute care services (Georing et al, 1997; Wong et al., 2008; Martinez & Burt, 2006; Newman et al., 1994; Hanrahan et al., 2001 Middleboe, 1997). Mondello et al. (2009) found that PSH residents in rural Maine (n=163) self-reported improved physical health following their move into housing, compared to their own selfreported health status while homeless. The same was true for the 99 PSH tenants in the companion study done in Portland (Mondello et al., 2007). Srebnick (2008), in the report cited above, found that PSH tenants agreed with statements that their physical health had improved since move-in. Schwarcz et al. (2009), in the article cited above, found greater glucose control among diabetics, and better adherence to antiretroviral medications, both documented in clinic records. Markedly better control of diabetes and other chronic conditions was also an outcome for the integrated service team serving street-homeless single adults at the Center for Community Health in downtown Los Angeles (County of Los Angeles, 2010, Attachment B, p. 15). Perlman and Parvensky (2006) report that 50 percent of the sample they followed, of participants in Denver s Housing First Collaborative, had improvements in their physical health status that were documented in clinic records. Value of Evidence Based Practices: Assertive Community Treatment Assertive Community Treatment (ACT) is a model of intensive, team-based, flexible, client centered services that provide support for community living for persons with SMI--and often cooccurring substance abuse problems--who might otherwise have frequent or extended stays in hospitals. In many states, ACT is a covered rehabilitation. The ACT model or hybrid form of the ACT model is used in myriad communities and has shown to reduce psychiatric symptoms and reported decreased use of illicit substances. While the ACT 4
47 typically increases utilization of community-based services such as outpatient treatments, it has decreases the use of costlier inpatient stays and emergency room visits (Morse et al., 2006). Florida Data Homeless, defined (Excerpts taken from the Council on Homelessness, 2016 Annual Report) Florida statutes define homeless in chapter (5) and FL Department of Education as: Sharing the housing of others due to loss of housing, economic hardship, or similar reason; Living in motels, hotels, trailer parks, and camping grounds, due to lack of adequate alternative housing; Living in emergency or transitional shelters; Abandoned in hospitals or awaiting foster care placement; Living in a public or private place not designed for or used as a regular sleeping accommodation for human beings to live; Living in cars, parks, abandoned buildings, bus or train stations, substandard housing, or similar setting; and Migratory children living in any of the above circumstances. Moving frequently from one place to another due to a variety of circumstances such as cost, safety, etc. The term does not refer to an individual imprisoned pursuant to state or federal law or to individuals or families who are sharing housing due to cultural preferences, voluntary arrangements, or traditional networks of support. The terms include an individual who has been released from jail, prison, the juvenile justice system, the child welfare system, a mental health and developmental disability facility, a residential addiction treatment program, or a hospital, for whom no subsequent residence has been identified, and who lacks the resources and support network to obtain housing. The Extent of Homelessness in Florida Coupled with national strategies within the American Recovery Act of 2009 such as the Homelessness Prevention and the Rapid Rehousing Program (HPRP), as well as the Homeless Emergency Assistance and Rapid Transition to Housing (HEARTH) Act (2009), and through Opening Doors, the 2010 national roadmap to prevent and end homelessness by the U.S. Interagency Council on Homelessness addressing specific subpopulations of veterans, children, families, and youth, there has been a slow but steady national decline of homelessness. Florida has also experienced a decline, but is still higher per capita than the national average. According to the 2015 Central Florida Commission on Homelessness report, Florida s per capita average is 21.2 per 10,000 individuals versus the national per capita average of 18.3 per 10,000 individuals. The Central Florida Commission report also states that while the state has made significant progress within the family homelessness subpopulation, showing a 15% decline since 2007, other subpopulations have seen sharp increases. One example is the rate of chronic homelessness which has shown a 7% increase since Another example is the 150% spike in the number of homeless youth, compared to the national average increase of 80%. Finally, there is a disproportionate share of unsheltered veterans in Florida (15.3%), versus the national average of 9.9%. 5
48 Point in Time Counts Florida communities participated in the HUD Point in Time (PIT) counts in January For one day and one night, there were 33,502 persons who were living on the street or in temporary shelters, including 2,888 homeless veterans and 6,079 who have a disability and are chronically homeless (i.e., homeless for more than a year or for repeated episodes). This data covers all 27 Continuum of Care (CoCs) across the state, representing nearly every county. Further, for school year , Florida s public schools identified 73,417 students as homeless, including those families that have lost their housing and are staying with family and friends or in motels. (Excerpts taken from the Council on Homelessness, 2016 Annual Report) Disabling Conditions The Council on Homelessness 2016 Annual Report contained a chart displaying disabling conditions by type of disability. Substance use disorder and mental illness are the strongest indicators of disabling condition and the frequency of both have increased from 2015 to In the survey point in time survey, respondents may report more than one disabling condition. Disabling Condition Condition 2016 Number 2016 Percentage 2015 Percentage Physical 4,060 26% 28% Substance Abuse 5, % 32.6% Mental Illness 5, % 33.6% HIV/AIDS % 2.6% Developmental % 3.1% Total 15,640 Florida s Response to Homelessness Three entities have responsibility to address homelessness in the state: the Council on Homelessness, to develop and implement policy recommendations; the Florida Department of Children & Families (DCF) through the Office on Homelessness, which administers state and federal assistance and coordinate with other state and local government agencies and programs to serve individuals and families who are homeless; and the Florida Housing Finance Corporation (FHFC) which administers state and federal assistance programs to provide a range of affordable housing in Florida. Financing Models DCF and FHFC utilize several funding mechanisms to address homeless and special needs housing. These include: DCF Administered: Emergency Solutions Grant (federal pass through) Challenge Grants: to 28 CoC agencies to implement written plans for addressing the needs of homeless individuals Continuum of Care Staff Grants Homelessness Prevention Grants: provide emergency financial assistance to families with children facing the loss of their housing due to financial or other crisis 6
49 Homeless Housing Assistance Grants: for construction of repair of existing rental housing for occupancy by individuals who are homeless FHFC Administered: Florida Housing Trust Fund: appropriates a portion to housing programs that address homelessness Link to Permanent Housing Strategy: addresses persons with special needs the opportunity to live in affordable, permanent supportive housing Tax Credits (Low Income Housing Tax Credits via the Qualified Allocation Plan): pilot project currently underway to target chronically homeless individuals with significant needs who are high utilizers of public resources with community supports State Housing Initiatives Partnership (SHIP): provides funding to local governments as an incentive to create partnerships that produce and preserve affordable homeownership and multifamily housing State Apartment Incentive Loan (SAIL) Program: provides low-interest loans on a competitive basis to affordable housing developers that propose construction or substantial rehabilitation of multifamily units affordable to very low income individuals and families According 2015 data collected from the FHFC, there has been an overall increase in the inventory of available housing units to serve the homeless and persons with special needs from 2013 (3,568 units) to 2015 (5,257 units). Florida Assertive Community Treatment (FACT) FACT teams are based on the evidence-based model of Assertive Community Treatment (ACT) for individuals with a severe and chronic mental illness. The multidisciplinary FACT teams offer a mobile, integrated, around-the-clock, system of care with a full array of treatment, support and rehabilitation services. There are 31 FACT teams across the state. Each team is staffed with a program psychiatrist, peer specialist and a team leader with a total staffing of 12.3 Full Time Equivalents (FTEs). Each team has an independent advisory committee to assist the team develop resources in its community. Currently, it is the only service available that offers a housing, medication, and flexible funding subsidy to enrolled individuals. Each team is mandated to serve 100 individuals. FACT guidelines have recently been revised so that enhancement funds can be used for an expanded variety of services and supports. FACT is not a self-directed program and participants do not receive fixed budget amounts for discretionary use. Clinical services are provided entirely within the FACT Team. One limitation of FACT is the limited opportunity for participants in the program to articulate and achieve individualized recovery goals for participants of the program Legislative Initiatives The Legislature took significant steps in addressing chronic homelessness during the 2016 Legislative Session which include: (Excerpts taken from the Council on Homelessness, 2016 Annual Report) Statutory recognition of Rapid Re-housing was recognized in statute. Challenge Grant funding is allocated to provide statewide technical assistance and training on best practices for local CoCs. SB 1534 requires FHFC to reserve at least 5% of its annual appropriation from the State Housing Trust Fund for housing projects designed and constructed to serve persons who 7
50 have a disabling condition, including those who are homeless. SB 1534 also gave FHFC the ability to forgive indebtedness, in certain circumstances, for SAIL loans provided to nonprofits to create permanent rental housing units for persons who are homeless, or for persons residing in time-limited transitional housing or institutions as a result of a lack of permanent affordable housing. HB 439 and SB 12 will largely redirect persons experiencing homelessness who have serious mental health issues from reentering the criminal justice system by improving the delivery of comprehensive behavioral health systems and allowing for alternatives to incarceration. The Agency for Health Care Administration (AHCA) Medicaid program was appropriated $10 million to implement a program to pay for flexible services for persons with severe mental illness or substance use disorders, including, but not limited to, temporary housing assistance. The legislation directs AHCA to implement this program under the Managed Medical Assistance program. Council members, including AHCA, DCF, FHFC, and FCH are increasing collaboration around housing coordination between Medicaid Managed Care organizations, DCF-funded Managing Entities, and Homeless CoC Lead Agencies. The Legislature encouraged Florida SHIP communities to use SHIP funding for rehousingtype programs. Rapid Re-housing programs are also supported by state Emergency Solutions Grants and Challenge Grants administered out of the Department of Children and Families (DCF) Office on Homelessness. Increase in access to affordable housing, namely: - $200.1 million appropriation within the Sadowski Affordable Housing Act funds for homeownership and rental housing. - $135.5 million appropriation to the Local Government Housing Trust Fund for SHIP - SB 1534 included language that allows a county or an eligible municipality to expend a portion of its local distribution for a rapid re-housing type rental assistance program for households that are homeless or special needs The Florida Gap The strong evidence that approximately one-third of individuals who are homeless or at risk of being homeless have a mental health (33.8%), substance abuse (32.6%) or co-occurring disorder and the rise in the special needs subpopulation of homeless persons, up from 15,640 in 2014 to 19,812 in 2015, infer that a gap exists between federal and state housing resources and existing deep end programs offered in the state. In 2016, the Legislature passed SB 12, which heavily focused on care coordination for high utilizers of the justice system, child welfare system, and state mental health hospitals to produce better health outcomes, reduce recidivism and reduce homelessness. To achieve care coordination, behavioral health Managing Entities are directed to work with key stakeholders in the community include local government, law enforcement, community-based providers, child welfare, criminal justice, and hospitals, to name a few. Managing Entities are also directed to conduct community needs assessments and make recommendations to the Department of Children & Families and the Legislature on how best to address targeted community needs. While this legislation outlined the framework for care coordination, the concept is merely words on paper rather than meaning reform without proper funding in place. 8
51 The solution is to connect behavioral health treatment supports with housing options by coordinating services through tenant supportive care managers with behavioral health managing (through the Department of Children & Families) and the Florida Housing Finance Corporation. Housing and Treatment Supports (HATS) Community Proposal Using the existing evidence-based practice of Housing First combined with evidence-based interventions to address behavioral health conditions, multi-disciplinary teams are proposed within a community to place individuals/families who are chronically homeless or at risk of being homeless and have one or more co-occurring mental health or substance use disorder into permanent or supportive housing and linking them with behavioral health, primary care and environmental supports. This proposal promotes funding of three HATS community pilots in conjunction with funding awarded through the Florida Housing Finance Corporation in targeted communities across the state. The plan is to create Housing First opportunities to for targeted individuals who frequent acute care services as a result of their recurring mental health or substance use order condition. This initiative requires coordination at the local level between the managing entity, local housing authorities, behavioral health providers, and community housing resources. Workforce training and linkages to primary care will also be a focus. A HATS community is broadly conceived and should include support services to tenants in supportive housing that address prevention, intervention, treatment, aftercare and long-term recovery, using the community needs assessment conducted by the Managing Entity. When identifying individuals who will receive the treatment supports, the research has shown that housing choice and preference should have broad, flexible options that meet the diverse needs of the population. This is predicated that individuals are more likely to embrace services tailored to their preference and is recognized as an important factor in recovery as it engages their willingness and motivation to make life changes. The end goal is to promote greater self-determination, economic self-sufficiency, and long-term housing stability by maximizing federal, state, local and community resources to achieve the greatest return on investment. This approach will result in decreased use of emergency rooms, jails, and state hospitals. Target population The target populations in this proposal are: Individuals and families who are chronically homeless or at risk of being homeless Have multiple and complex health and behavioral health conditions Have frequent stays in jails, state hospitals, or prisons Are high utilizers of acute care services Case management and ancillary services Case management, in various forms, is critical to ensuring the success of a HATS community. Most importantly, the primary case manager should act as an advocate for the tenant. Some of the services that may be provided in case management include, but are not limited to: 9
52 Life skills: Personal care/hygiene, money management, nutrition education, independent living skills, goal setting Linkages: Referrals or support groups, educational opportunities, child care, community-based resources, transportation, legal services, primary health care, applying for Medicaid or other public program Parenting: Personal and family safety, child protection, parenting supports Intensive supports: Substance abuse or mental health counseling, grief counseling, harm reduction strategies, service planning, crisis intervention, medication management, relapse prevention, group therapy, HIV counseling Managing Entities The Managing Entity will be charged with the lead on implementing a HATS Community. Managing Entities will coordinate efforts with DCF, the Agency for Health Care Administration, Florida Department of Veterans Affairs, Florida Department of Elderly Affairs, the Florida Housing Finance Corporation, community-based providers, county jails, hospitals, Federally Qualified Health Centers, property developers and managers, local government, county school systems, and charitable organizations. Each Managing Entity currently staffs a Housing Specialist, which will assume the role of managing and directing other staff to coordinate the HATS pilot. HATS Service Team At a minimum, a HATS community should utilize peer support specialists and tenant services coordinators who work in concert with each other. Additionally, a HATS community should have a flexible behavioral health component built into the program to provide treatment for mental health, substance abuse or co-occurring behavioral health disorders. Tenant Supportive Care Manager: Through the Managing Entity, the tenant care manager will be responsible for navigating through multiple state and federal systems such as health care, housing, educational and other federal assistance programs to maximize opportunities available for tenants. The manager should also review data provided by the tenant services coordinator and peer specialists to identify trends in the supportive housing arena; explore opportunities to increase market capacity to serve this population; and make recommendations to enhance the HATS community. Tenant Services Coordinator: Conducts initial orientations; works with site staff; responsible for coordinating on-site leisure activities and support groups; educational activities; and maintains data on participation in activities. Peer Support Specialists: Serves as the tenant advocate. Duties include outreach and engagement, coordination with both case managers and the tenant services coordinator, providing linkages to coordinated services provided by case manager and tenant services coordinator, as well as linkage 10
53 to primary health, transportation and other needs that may arise; must keep data on all linkages and activities with tenants Behavioral health treatment capacity: Provides oversight for peer specialists. Conducts initial assessments; developing and implementing tenant goal plans; problem-solving and linkages to treatment Financing a HATS Community Each HATS community will serve an approximate 60 individual/family units and is expected to cost $1.448 million per HATS Community for the first year ($4.344 million total for three communities). Based on research analyzing similar projects nationwide, it is assumed that not all individuals/families will remain in a HATS community. Some will achieve greater economic selfsufficiency, while other may choose to vacate the support housing model entirely. The front-end expenses for new tenants, such as start-up costs will not carry forward into the second year of occupancy. There is also a greater chance that treatment supports will decrease over time. Therefore, second year funding for a HATS Community will not require as much funding as the first year. Based on case load ratio for other targeting programs such as Family Intensive Treatment, Community Action Teams, and FACT, it is recommended the following: HATS Staffing Team ($356,000 total per community x 3 communities = $1.068 million) Tenant Care Manager: 1:60 housing units (1.0 FTE = $60,000) Ensures housing financing opportunities are maximized and tenant services and case management plans are compliant with the care coordination concept of SB 12 Tenant Services Coordinator: 1:20 housing units (3.0 FTE x $48,000 = $144,000) Conducts initial orientations; works with site staff; responsible for coordinating on-site recreational activities, support groups; educational activities; and maintains statistics on participation in activities. The staffing ratio for a tenant services coordinator could be 1:25 housing units, depending on community needs. Peer Support Specialists: 1:15 individuals (4.0 FTE x $38,000 = $140,000) Serves as the tenant advocate. Duties include outreach and engagement, coordination with both case managers and the tenant services coordinator, providing linkages to coordinated services provided by case manager and tenant services coordinator, as well as linkage to primary health, transportation and other needs that may arise; must keep data on all linkages and activities with tenants. The staffing ratio for a peer support specialist could be 1:20 housing units, depending on community needs. HATS Services and Supports ($1.092 million/community x 3 communities = $3.276 million) Behavioral Health treatment capacity (30 tenants x 3 hrs/week x $150/hr x 36/weeks =$486,000): While the target population has an identified substance abuse, behavioral health or co-occurring disorder, evidence-based practices have shown that removing requirements such as receiving treatment for their disorder will achieve a greater overall outcome and yield a higher cost-savings. 11
54 Meaning, while these individuals should be receiving treatment, the likelihood of each of them receiving treatment is not realistic. The target goal for individuals to receive treatment for their mental health or substance use disorders is 50%. While funding for treatment services should be flexible, it is assumed an individual who seeks treatment will receive a minimum of 3 hours of outpatient treatment per week for a period of nine months. Supportive Housing Rental subsidies: ($400 per unit/mo x 60 units x 12 mo. = $288,000) Rental supports consistent with funds provided to Assisted Living Facilities Start-up funding: ($3000 per unit x 60 units + plus ($30,000 turnover) = $210,000): Once a unit is available for a tenant, initial funding will equip the unit with furniture and other supports necessary for occupancy. Discretionary funds: ($150 per unit/mo x 60 units x 12 mo = $108,000): Resources to assist success in housing such as child care, transportation, workforce training, and costs associated with housing. Outcome Measures The goal of a HATS community is to promote greater self-determination, economic self-sufficiency, and long-term housing stability by maximizing federal, state local and community resources to achieve the greatest return on investment. Outcome objectives shall be used to track the progress on a monthly basis for individuals who were at risk of being homeless. Engagement by support service staff: 100% Stable housing after one year: 80% Gainful Employment within six months of enrollment: 30-50% Outcome objectives shall be used to track the progress on a monthly basis for individuals who were previously homeless. Engagement by support staff: 100% Participation in monthly organized skill-building activity: 30% (with a higher goal of 70% participation over the year) Gainful employment within twelve months: 15% Development of individualized service plan establishing objectives and goals within first ninety days: 70% Reduction of acute care services within first twelve months: 85% Achieve stable and/or permanent housing: 50% Reported reduction in substance use Reported adherence to maintenance medications Reported improvement in chronic physical health conditions References Burt, M.R "Evolution of PSH in Taking Health Care Home, : Tenants, Programs, Policies, and Funding at Project End." Oakland, CA: Corporation for Supportive Housing. 12
55 Caton C., C. Wilkins, and J. Anderson "People Who Experience Long-Term Homelessness: Characteristics and Interventions." In Toward Understanding Homelessness: The 2007 National Symposium on Homelessness Research. Washington, DC: HHS and HUD. Clark C, Rich AR: Outcomes of homeless adults with mental illness in a housing program and in case management only. Psychiatric Services 54:78 83, 2003 Culhane DP, Metraux S, Hadley T: Public service reductions associated with placement of homeless persons with severe mental illness in supportive housing. Housing Policy Debate 13: , 2002 Cheng, An-Lin, Haiqun Lin, Wesley Kasprow, and Robert A. Rosenheck Impact of supported housing on clinical outcomes: Analysis of a randomized trial using multiple imputation technique. Journal of Nervous and Mental Disease, 195, Flaming, Daniel, Patrick Burns, Michael Matsunaga, Gerald Sumner, Manuel H. Moreno, Halil Toros, and Duc Doan Where we sleep: Costs when homeless and housed in Los Angeles. Los Angeles, CA: Economic Roundtable. Goering, P., Wasylenki D., Lindsay, S., Lemire, D., & Rhodes, A. (1997). Process and outcome in hostel outreach program for homeless clients with severe mental illness. American Journal of Orthopsychiatry, 67(4), Goldfinger, S.M., Schutt, R.K., Tolomiczenko, G.S., Seidman, L., Penk, W.E., Turner, W. et al. (1999). Housing placement and subsequent days homeless among formerly homeless adults with mental illness. Psychiatric Services, 50(5), Gulcur, L., Stefancic, A., Shinn, M., Tsemberis, S., & Fischer, S.N. (2003). Housing, hospitalization, and cost outcomes for homeless individuals with psychiatric disabilities participating in continuum of care and Housing First programmes. Journal of Community & Applied Social Psychology, 13(2), Greenwood, R.M., Schaefer-McDaniel, N., Winkel, G., & S. Tsemberis. (2005). Decreasing psychiatric symptoms by increasing choice in services for adults with histories of homelessness. American Journal of Community Psychologhy, 36(3-4), Hanrahan, P., McCoy, M., Cloninger, L., Dincin, J., Zeitz, M., Simpatico, T. et al. (2005). The mothers project for homeless mothers with mental illnesses and their children: A pilot study. Psychiatric Rehabilitation Journal, 28(3), Larimer, Mary E., Daniel K. Malone, Michelle D. Garner, David C. Atkins, Bonnie Burlingham, Heather S. Lonczak, Kenneth Tanzer, Joshua Ginzler, Seema L. Clifasefi, William G. Hobson, and G. Alan Marlatt Health care and public service use and costs before and after provision of housing for chronically homeless persons with severe alcohol problems. Journal of the American Medical Association, 301, 13, Locke, G., Khadduri, J., and A. O Hara Housing Models. In Toward Understanding Homelessness: The 2007 National Symposium on Homelessness Research. Washington, DC: HHS and HUD. Martinez, T.E., & Burt, M.R. (2006). Impact of permanent supportive housing on the use of acute care health services by homeless adults. Psychiatric Services, 57(7), Middelboe, T. (1997). Prospective study of clinical and social outcome of stay in small group homes for people with mental illness. British Journal of Psychiatry, 151(1), Mondello, Melanie, Jon Bradley, Thomas C. McLaughlin, and Nancy Shore Cost analysis of permanent supportive housing in rural Maine. Augusta, ME: Maine Housing. Mondello, Melanie, Ann B. Gass, Thomas Chalmers McLaughlin and Nancy Shore Cost analysis of permanent supportive housing in the Greater Portland area. Augusta, ME: Maine Housing. Moore, Tom L Estimated cost savings following enrollment in the Community Engagement Program: Findings from a pilot study of dually diagnosed adults. Portland, OR: Central City Concern. 13
56 Morse, G.A., Calsyn, R.J., Klinkenberg, W.D., Helminiak, T.W., Wolff, N., Drake, R.E. et al. (2006). Treating homeless clients with severe mental illness and substance use disorders: Costs and outcomes. Community Mental Health Journal, 42(4), Newman, S.J., Reschovsky, J.D., Kaneda, K., & Hendrick, A.M. (1994). The effects of independent living on persons with chronic mental illness: An assessment of the Section 8 certificate program. Milbank Quarterly, 72(1), hh Perlman, J. and Parvensky, J. (2006). Cost Benefit Analysis and Program Outcomes Report, Denver Housing First Collaborative. Available at Poppe, Barbara and Associates (2015). Central Florida Commission on Homelessness. The Path Forward: Rethinking Solutions for Homelessness in Florida. Rog, D. (2004). Building the case: Emerging research on solutions to end homelessness. Paper presented at the National Alliance to End Homelessness Annual Conference, Washington, DC. Rog, D., & Holupka, S. (1999). Reconnecting homeless individuals and families to the community. In L. B. Fosberg & D. L. Dennis (Eds.) Practical lessons: The 1998 National Symposium on Homelessness Research. Washington, DC: U.S. Department of Housing and Urban Development and U.S. Department of Health and Human Services. Rog, D., Marshall, T., Dougherty, R.H., George, P., Daniels, A.S., Ghose, S.S., and M.E. Delphin-Rittmon. (2014). Permanent Supportive Housing: Assessing the Evidence. Published online: March 01, Rosenheck, R., Kasprow, W., Frisman, L., & Liu-Mares, W. (2003). Cost-effectiveness of supported housing for homeless persons with mental illness. Archives of General Psychiatry, 60(9), Rosenheck, Robert A., and Alvin S. Mares Final client outcomes report of the HUD/HHS/VA Collaborative Initiative to Help End Chronic Homelessness, National Performance Outcomes Assessment. West Haven, CT: Northeast Program Evaluation Center. Sacks, S., De Leon, G., Sacks, J.Y., McKendrick, K., and B.S. Brown. (2003). TC-oriented supported housing for homeless MICAs. Journal of Psychoactive Drugs, 35(3), Schwarcz, Sandra K., Ling C. Hsu, Eric Vittinghoff, Annie Vu, Joshua D. Bamburger, and Mithcell H. Katz Impact of housing on the survival of persons with AIDS. BMC Public Health, 9, 220. Shern, D.L., Felton, C.J., Hough, R.L., Lehman, A.F., Goldfinger, S., Valencia, E. et al. (1997). Housing outcomes for homeless adults with mental illness: Results from the Second-Round McKinney Program. Psychiatric Services, 48(2), Strebnick, Debra Housing First: Begin at Home- pilot project for chronically homeless single adults: One year outcomes. Seattle, WA: Department of Community and Human Services, Mental Health and Chemical Abuse and Dependency Services Division. Tsemberis, S., Gulcur, L., & Nakae, M. (2004). Housing First, consumer choice, and harm reduction for homeless individuals with a dual diagnosis. American Journal of Public Health, 94(4), Wong, Y.I., Poulin, S.R., Lee, S., Davis, M.R., & Hadley, T.R. (2008). Tracking residential outcomes of supported independent living programs for persons with serious mental illness. Evaluation and Program Planning, 31(4),
57 HATS Model DCF Proposal Key Differences Concept Provide linkages with housing and supports to 67 high risk individuals with behavioral health conditions. Provide linkages with housing and supports to 67 high risk individuals with behavioral health conditions. Same TOTAL $1.482 million $1.0 million (annualized) HATS builds the staffing team into the pilot whereas DCF makes a second funding request ($1.685m) to build staffing capacity through the managing entity Individuals served Similar Housing $400/mo $719/mo HATS assumes supplemental funding will be obtained through other federal and/or state resources Discretionary $250/mo $380/mo Staffing $318,000 for Tenant Care Manager, 3 tenant services coordinators, and 3 peer specialists $0 HATS assumes supplemental funding will be obtained through other federal and/or state resources DCF allocated $150/mo p/p for case management, which equals to $108,000 annually. They also build capacity for the managing entities for housing. HATS Care Manager is through the ME Case management $1800/mo for all individuals $150/mo for each individual HATS assumes that at least one-half of the tenants will need SUD or MH treatment and funds both treatment through this proposal rather than taking funding through base. It also builds the case management into staffing.
58
59 Florida Senate SB 874 By Senator Passidomo A A bill to be entitled An act relating to state funds; amending s , F.S.; exempting the State Housing Trust Fund and the Local Government Housing Trust Fund from a provision authorizing the Legislature, in the General Appropriations Act, to transfer unappropriated cash balances from specified trust funds to the Budget Stabilization Fund and General Revenue Fund; providing an effective date. Be It Enacted by the Legislature of the State of Florida: Section 1. Upon the expiration and reversion of the amendments made to section , Florida Statutes, pursuant to section 56 of chapter , Laws of Florida, paragraph (b) of subsection (2) of section , Florida Statutes, is amended to read: State funds; segregation. (2) The source and use of each of these funds shall be as follows: (b)1. The trust funds shall consist of moneys received by the state which, under law or under trust agreement, are segregated for a purpose authorized by law. The state agency or branch of state government receiving or collecting such moneys is shall be responsible for their proper expenditure as provided by law. Upon the request of the state agency or branch of state government responsible for the administration of the trust fund, the Chief Financial Officer may establish accounts within the trust fund at a level considered necessary for proper Page 1 of 4 CODING: Words stricken are deletions; words underlined are additions.
60 Florida Senate SB A accountability. Once an account is established within a trust fund, the Chief Financial Officer may authorize payment from that account only upon determining that there is sufficient cash and releases at the level of the account. 2. In addition to other trust funds created by law, each agency, to the extent possible, each agency shall use the following trust funds as described in this subparagraph for dayto-day operations: a. An operations or operating trust fund, for use as a depository for funds to be used for program operations funded by program revenues, with the exception of administrative activities when the operations or operating trust fund is a proprietary fund;. b. An operations and maintenance trust fund, for use as a depository for client services funded by third-party payors;. c. An administrative trust fund, for use as a depository for funds to be used for management activities that are departmental in nature and funded by indirect cost earnings and assessments against trust funds; however,. proprietary funds are not required to use excluded from the requirement of using an administrative trust fund;. d. A grants and donations trust fund, for use as a depository for funds to be used for allowable grant or donor agreement activities funded by restricted contractual revenue from private and public nonfederal sources;. e. An agency working capital trust fund, for use as a depository for funds to be used pursuant to s ;. f. A clearing funds trust fund, for use as a depository for funds to account for collections pending distribution to lawful Page 2 of 4 CODING: Words stricken are deletions; words underlined are additions.
61 Florida Senate SB A recipients; and. g. A federal grant trust fund, for use as a depository for funds to be used for allowable grant activities funded by restricted program revenues from federal sources. To the extent possible, each agency must adjust its internal accounting to use existing trust funds consistent with the requirements of this subparagraph. If an agency does not have a trust fund specified trust funds listed in this subparagraph and cannot make such adjustment, the agency must recommend the creation of the necessary trust funds to the Legislature no later than the next scheduled review of the agency s trust funds pursuant to s All such moneys are hereby appropriated to be expended in accordance with the law or trust agreement under which they were received, subject always to the provisions of chapter 216 relating to the appropriation of funds and to the applicable laws relating to the deposit or expenditure of moneys in the State Treasury. 4.a. Notwithstanding any provision of law restricting the use of trust funds to specific purposes, unappropriated cash balances from selected trust funds may be authorized by the Legislature for transfer to the Budget Stabilization Fund and General Revenue Fund in the General Appropriations Act. b. This subparagraph does not apply to trust funds required by federal programs or mandates; trust funds established for bond covenants, indentures, or resolutions whose revenues are legally pledged by the state or public body to meet debt service or other financial requirements of any debt obligations of the Page 3 of 4 CODING: Words stricken are deletions; words underlined are additions.
62 Florida Senate SB A state or any public body; the Division of Licensing Trust Fund in the Department of Agriculture and Consumer Services; the State Transportation Trust Fund; the trust fund containing the net annual proceeds from the Florida Education Lotteries; the Florida Retirement System Trust Fund; trust funds under the management of the State Board of Education or the Board of Governors of the State University System, when where such trust funds are for auxiliary enterprises, self-insurance, and contracts, grants, and donations, as those terms are defined by general law; trust funds that serve as clearing funds or accounts for the Chief Financial Officer or state agencies; trust funds that account for assets held by the state in a trustee capacity as an agent or fiduciary for individuals, private organizations, or other governmental units; the State Housing Trust Fund; the Local Government Housing Trust Fund; and other trust funds authorized by the State Constitution. Section 2. This act shall take effect July 1, Page 4 of 4 CODING: Words stricken are deletions; words underlined are additions.
63 Senator Passidomo, District 28 Press Release FOR IMMEDIATE RELEASE CONTACT: Jared Willis, November 14, 2017 State Senator Passidomo Files Bipartisan Affordable Housing Legislation Senator Passidomo & Representative Shaw Join to Stop Sweeps of State and Local Housing Trust Tallahassee, Fla. With representatives from the 30 diverse statewide organizations that make up the Sadowski Coalition joining her in front of the Florida Senate Chamber doors in the State Capitol in Tallahassee, State Senator Kathleen Passidomo today announced she has filed bipartisan affordable housing legislation. This legislation, Senate Bill 874, would prohibit the sweep of the State and Local Housing Trust Fund. State Representative Sean Shaw is the sponsor of the House companion bill, House Bill 191. Senator Passidomo was joined by Representative Shaw and Senate and House Cosponsors, as well as Sadowski Coalition Facilitator Jaimie Ross and representatives from the Sadowski Coalition, including Danielle Scoggins, senior public policy representative for the Florida Realtors. I m honored to announce today that I have filed legislation, Senate Bill 874, to stop the sweeps of the State and Local Housing Trust Fund, said Senator Passidomo. With this legislation, this much-needed funding can become a certainty, and we can begin to use all of our available housing resources toward solving our affordable housing problem. Florida s state and local housing trust fund programs are national models they work, but only to the degree that they are funded. Governor Rick Scott s budget proposal, released today, showed a significant reduction in sweeps of Florida s state and local housing trust funds. The Governor s budget proposed a $224M sweep, while the budget proposes a much lower $91.8M sweep, affirming the Governor s commitment to affordable housing in the wake of a disastrous hurricane season. we are on the right track. And hopefully, SB 874 and HB 191 can bring us that much closer to the end goal of using all affordable housing trust fund monies toward their intended purpose affordable housing, said Senator Passidomo. I filed HB 191 in the House before our housing needs were exacerbated by Hurricane Irma and the displacement of our fellow Americans by Hurricane Maria, said
64 Representative Shaw. Florida is proud to open our arms to our fellow Americans from Puerto Rico and the Virgin Islands who need refuge or intend to establish a new residence here. We must have more housing opportunities to make that happen, and it is time we stop the sweeping of affordable housing trust fund monies. This year marks 25 years since the Sadowski Act became law with bipartisan support in Florida, said Jaimie Ross, president and CEO of the Florida Housing Coalition, and facilitator of the Sadowski Coalition. This landmark legislation was intended to create a source of funding for affordable housing that could be relied upon. There were no sweeps of the housing trust funds during the first 10 years. We need to bring back that norm. This legislation is intended to do that. The timing could not be better. Florida Realtors has been a proud supporter of the state and local government housing trust funds from the very beginning because our members understand that every community relies on dependable and accessible housing options to stay vibrant and healthy, said Carrie O Rourke, vice president of public policy for Florida Realtors, which is a member of the Sadowski Coalition. We applaud Senator Passidomo and Representative Shaw for being leaders on this important issue and for calling attention to one of the biggest hurdles facing the continued economic prosperity of our state. Only by working together can we solve Florida s affordable housing problem.
65 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S HB A bill to be entitled An act relating to insurance coverage parity for mental health and substance use disorders; amending s , F.S.; requiring contracts between the Agency for Health Care Administration and certain managed care plans to require the plans to submit a specified annual report to the agency relating to parity between mental health and substance use disorder benefits and medical and surgical benefits; amending s , F.S.; conforming a cross-reference; transferring, renumbering, and amending s , F.S.; deleting certain provisions that require insurers, health maintenance organizations, and nonprofit hospital and medical service plan organizations transacting group health insurance or providing prepaid health care to offer specified optional coverage for mental and nervous disorders; requiring such entities transacting individual or group health insurance or providing prepaid health care to comply with specified provisions prohibiting the imposition of less favorable benefit limitations on mental health and substance use disorder benefits than on medical and surgical benefits; requiring such entities to submit a specified annual report relating to parity between such benefits to the Office of Insurance Regulation; Page 1 of 13 CODING: Words stricken are deletions; words underlined are additions. hb
66 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S HB requiring the office to implement and enforce specified federal provisions, guidance, and regulations; specifying actions the office must take relating to such implementation and enforcement; requiring the office to issue a specified annual report to the Legislature; providing an effective date. Be It Enacted by the Legislature of the State of Florida: Section 1. Paragraph (p) is added to subsection (2) of section , Florida Statutes, to read: Managed care plan accountability. (2) The agency shall establish such contract requirements as are necessary for the operation of the statewide managed care program. In addition to any other provisions the agency may deem necessary, the contract must require: (p) Annual reporting relating to parity in mental health and substance use disorder benefits. Every managed care plan shall submit an annual report to the agency, on or before July 1, which contains all of the following information: 1. A description of the process used to develop or select the medical necessity criteria for: a. Mental or nervous disorder benefits; b. Substance use disorder benefits; and Page 2 of 13 CODING: Words stricken are deletions; words underlined are additions. hb
67 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S HB c. Medical and surgical benefits. 2. Identification of all nonquantitative treatment limitations (NQTLs) applied to both mental or nervous disorder and substance use disorder benefits and medical and surgical benefits. Within any classification of benefits, there may not be separate NQTLs that apply to mental or nervous disorder and substance use disorder benefits but do not apply to medical and surgical benefits. 3. The results of an analysis demonstrating that for the medical necessity criteria described in subparagraph 1. and for each NQTL identified in subparagraph 2., as written and in operation, the processes, strategies, evidentiary standards, or other factors used to apply the criteria and NQTLs to mental or nervous disorder and substance use disorder benefits are comparable to, and are applied no more stringently than, the processes, strategies, evidentiary standards, or other factors used to apply the criteria and NQTLs, as written and in operation, to medical and surgical benefits. At a minimum, the results of the analysis must: a. Identify the factors used to determine that an NQTL will apply to a benefit, including factors that were considered but rejected; b. Identify and define the specific evidentiary standards used to define the factors and any other evidentiary standards relied upon in designing each NQTL; Page 3 of 13 CODING: Words stricken are deletions; words underlined are additions. hb
68 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S HB c. Identify and describe the methods and analyses used, including the results of the analyses, to determine that the processes and strategies used to design each NQTL, as written, for mental or nervous disorder and substance use disorder benefits are comparable to and no more stringently applied than the processes and strategies used to design each NQTL, as written, for medical and surgical benefits; d. Identify and describe the methods and analyses used, including the results of the analyses, to determine that processes and strategies used to apply each NQTL, in operation, for mental or nervous disorder and substance use disorder benefits are comparable to and no more stringently applied than the processes or strategies used to apply each NQTL, in operation, for medical and surgical benefits; and e. Disclose the specific findings and conclusions reached by the managed care plan that the results of the analyses indicate that the insurer, health maintenance organization, or nonprofit hospital and medical service plan corporation is in compliance with this section, the Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act of 2008 (MHPAEA); any regulations relating to MHPAEA, including, but not limited to, 45 C.F.R. s , 45 C.F.R. s , and 45 C.F.R. s (a)(3); and any other relevant current or future regulations. Section 2. Paragraph (b) of subsection (8) of section Page 4 of 13 CODING: Words stricken are deletions; words underlined are additions. hb
69 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S HB , Florida Statutes, is amended to read: Conversion on termination of eligibility. Subject to all of the provisions of this section, a group policy delivered or issued for delivery in this state by an insurer or nonprofit health care services plan that provides, on an expense-incurred basis, hospital, surgical, or major medical expense insurance, or any combination of these coverages, shall provide that an employee or member whose insurance under the group policy has been terminated for any reason, including discontinuance of the group policy in its entirety or with respect to an insured class, and who has been continuously insured under the group policy, and under any group policy providing similar benefits that the terminated group policy replaced, for at least 3 months immediately prior to termination, shall be entitled to have issued to him or her by the insurer a policy or certificate of health insurance, referred to in this section as a "converted policy." A group insurer may meet the requirements of this section by contracting with another insurer, authorized in this state, to issue an individual converted policy, which policy has been approved by the office under s An employee or member shall not be entitled to a converted policy if termination of his or her insurance under the group policy occurred because he or she failed to pay any required contribution, or because any discontinued group coverage was replaced by similar group Page 5 of 13 CODING: Words stricken are deletions; words underlined are additions. hb
70 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S HB coverage within 31 days after discontinuance. (8) BENEFITS OFFERED. (b) An insurer shall offer the benefits specified in s s and the benefits specified in s if those benefits were provided in the group plan. Section 3. Section , Florida Statutes, is transferred, renumbered as section , Florida Statutes, and amended, to read: Requirements for mental health and substance use disorder benefits; reporting requirements Optional coverage for mental and nervous disorders required; exception. (1) Every insurer, health maintenance organization, and nonprofit hospital and medical service plan corporation transacting individual or group health insurance or providing prepaid health care in this state must comply with the Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act of 2008 (MHPAEA) and any regulations relating to MHPAEA, including, but not limited to, 45 C.F.R. s , 45 C.F.R. s , and 45 C.F.R. s (a)(3); and must provide shall make available to the policyholder as part of the application, for an appropriate additional premium under a group hospital and medical expense-incurred insurance policy, under a group prepaid health care contract, and under a group hospital and medical service plan contract, the benefits or level of benefits specified in subsection (2) for the necessary care and Page 6 of 13 CODING: Words stricken are deletions; words underlined are additions. hb
71 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S HB treatment of mental and nervous disorders, including substance use disorders, as defined in the standard nomenclature of the American Psychiatric Association, subject to the right of the applicant for a group policy or contract to select any alternative benefits or level of benefits as may be offered by the insurer, health maintenance organization, or service plan corporation provided that, if alternate inpatient, outpatient, or partial hospitalization benefits are selected, such benefits shall not be less than the level of benefits required under paragraph (2)(a), paragraph (2)(b), or paragraph (2)(c), respectively. (2) Under individual or group policies or contracts, inpatient hospital benefits, partial hospitalization benefits, and outpatient benefits consisting of durational limits, dollar amounts, deductibles, and coinsurance factors may shall not be less favorable than for physical illness, in accordance with 45 C.F.R. s (c)(2) and (3) generally, except that: (a) Inpatient benefits may be limited to not less than 30 days per benefit year as defined in the policy or contract. If inpatient hospital benefits are provided beyond 30 days per benefit year, the durational limits, dollar amounts, and coinsurance factors thereto need not be the same as applicable to physical illness generally. (b) Outpatient benefits may be limited to $1,000 for consultations with a licensed physician, a psychologist licensed Page 7 of 13 CODING: Words stricken are deletions; words underlined are additions. hb
72 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S HB pursuant to chapter 490, a mental health counselor licensed pursuant to chapter 491, a marriage and family therapist licensed pursuant to chapter 491, and a clinical social worker licensed pursuant to chapter 491. If benefits are provided beyond the $1,000 per benefit year, the durational limits, dollar amounts, and coinsurance factors thereof need not be the same as applicable to physical illness generally. (c) Partial hospitalization benefits shall be provided under the direction of a licensed physician. For purposes of this part, the term "partial hospitalization services" is defined as those services offered by a program that is accredited by an accrediting organization whose standards incorporate comparable regulations required by this state. Alcohol rehabilitation programs accredited by an accrediting organization whose standards incorporate comparable regulations required by this state or approved by the state and licensed drug abuse rehabilitation programs shall also be qualified providers under this section. In a given benefit year, if partial hospitalization services or a combination of inpatient and partial hospitalization are used, the total benefits paid for all such services may not exceed the cost of 30 days after inpatient hospitalization for psychiatric services, including physician fees, which prevail in the community in which the partial hospitalization services are rendered. If partial hospitalization services benefits are provided beyond the limits Page 8 of 13 CODING: Words stricken are deletions; words underlined are additions. hb
73 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S HB set forth in this paragraph, the durational limits, dollar amounts, and coinsurance factors thereof need not be the same as those applicable to physical illness generally. (3) Insurers must maintain strict confidentiality regarding psychiatric and psychotherapeutic records submitted to an insurer for the purpose of reviewing a claim for benefits payable under this section. These records submitted to an insurer are subject to the limitations of s , relating to the furnishing of patient records. (4) Every insurer, health maintenance organization, and nonprofit hospital and medical service plan corporation transacting individual or group health insurance or providing prepaid health care in this state shall submit an annual report to the office, on or before July 1, which contains all of the following information: (a) A description of the process used to develop or select the medical necessity criteria for: 1. Mental or nervous disorder benefits; 2. Substance use disorder benefits; and 3. Medical and surgical benefits. (b) Identification of all nonquantitative treatment limitations (NQTLs) applied to both mental or nervous disorder and substance use disorder benefits and medical and surgical benefits. Within any classification of benefits, there may not be separate NQTLs that apply to mental or nervous disorder and Page 9 of 13 CODING: Words stricken are deletions; words underlined are additions. hb
74 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S HB substance use disorder benefits but do not apply to medical and surgical benefits. (c) The results of an analysis demonstrating that for the medical necessity criteria described in paragraph (a) and for each NQTL identified in paragraph (b), as written and in operation, the processes, strategies, evidentiary standards, or other factors used to apply the criteria and NQTLs to mental or nervous disorder and substance use disorder benefits are comparable to, and are applied no more stringently than, the processes, strategies, evidentiary standards, or other factors used to apply the criteria and NQTLs, as written and in operation, to medical and surgical benefits. At a minimum, the results of the analysis must: 1. Identify the factors used to determine that an NQTL will apply to a benefit, including factors that were considered but rejected; 2. Identify and define the specific evidentiary standards used to define the factors and any other evidentiary standards relied upon in designing each NQTL; 3. Identify and describe the methods and analyses used, including the results of the analyses, to determine that the processes and strategies used to design each NQTL, as written, for mental or nervous disorder and substance use disorder benefits are comparable to and no more stringently applied than the processes and strategies used to design each NQTL, as Page 10 of 13 CODING: Words stricken are deletions; words underlined are additions. hb
75 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S HB written, for medical and surgical benefits; 4. Identify and describe the methods and analyses used, including the results of the analyses, to determine that processes and strategies used to apply each NQTL, in operation, for mental or nervous disorder and substance use disorder benefits are comparable to and no more stringently applied than the processes or strategies used to apply each NQTL, in operation, for medical and surgical benefits; and 5. Disclose the specific findings and conclusions reached by the insurer, health maintenance organization, or nonprofit hospital and medical service plan corporation that the results of the analyses indicate that the insurer, health maintenance organization, or nonprofit hospital and medical service plan corporation is in compliance with this section; MHPAEA; any regulations relating to MHPAEA, including, but not limited to, 45 C.F.R. s , 45 C.F.R. s , and 45 C.F.R. s (a)(3); and any other relevant current or future regulations. (5) The office shall implement and enforce applicable provisions of MHPAEA and federal guidance or regulations relating to MHPAEA, including, but not limited to, 45 C.F.R. s , 45 C.F.R. s , and 45 C.F.R. s (a)(3), and this section, which includes: (a) Ensuring compliance by each insurer, health maintenance organization, and nonprofit hospital and medical Page 11 of 13 CODING: Words stricken are deletions; words underlined are additions. hb
76 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S HB service plan corporation transacting individual or group health insurance or providing prepaid health care in this state. (b) Detecting violations by any insurer, health maintenance organization, or nonprofit hospital and medical service plan corporation transacting individual or group health insurance or providing prepaid health care in this state. (c) Accepting, evaluating, and responding to complaints regarding potential violations. (d) Reviewing, from consumer complaints, for possible parity violations regarding mental or nervous disorder and substance use disorder coverage. (e) Performing parity compliance market conduct examinations, which include, but is not limited to, reviews of medical management practices, network adequacy, reimbursement rates, prior authorizations, and geographic restrictions of insurers, health maintenance organizations, and nonprofit hospital and medical service plan corporations transacting individual or group health insurance or providing prepaid health care in this state. (6) No later than December 31 of each year, the office shall issue a report to the Legislature which describes the methodology the office is using to check for compliance with MHPAEA; any regulations relating to MHPAEA, including, but not limited to, 45 C.F.R. s , 45 C.F.R. s , and 45 C.F.R. s (a)(3); and this section. The report must be Page 12 of 13 CODING: Words stricken are deletions; words underlined are additions. hb
77 F L O R I D A H O U S E O F R E P R E S E N T A T I V E S HB written in nontechnical and readily understandable language and must be made available to the public by posting the report on the office's website and by other means the office finds appropriate. Section 4. This act shall take effect July 1, Page 13 of 13 CODING: Words stricken are deletions; words underlined are additions. hb
78 JL : Education; sterile needle and syringe exchange pilot program (4) The University of Miami and its affiliates may establish single sterile needle and syringe exchange pilot programs. The Pilot programs may operate at a fixed location or through a mobile health unit. The pilot programs shall offer the free exchange of clean, unused needles and hypodermic syringes for used needles and hypodermic syringes as a means to prevent the transmission of HIV, AIDS, viral hepatitis, or other blood-borne diseases among intravenous drug users and their sexual partners and offspring. (e) County or municipal funds may be used to operate these pilot programs. The pilot programs may be funded through grants and donations from private resources and funds. (f) The pilot programs shall expire July 1, Page 1 of 1 CODING: Words stricken are deletions; words underlined are additions. Draft Legislation 2018 part 1
79 BEFORE THE FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES IN THE MATTER OF: Notice ID# (June 13, 2018) Amethyst Recovery Center, LLC, Petitioner MOTION TO INTERVENE BY FLORIDA ASSOCIATION OF RECOVERY RESIDENCES The Florida Association of Recovery Residences (FARR) hereby serves its Motion to Intervene, pursuant to Rule , F.A.C. In conjunction with its Motion to Intervene, FARR also submits and incorporates comments on Amethyst Recovery Center, LLC s ( Amethyst ) Petition, as set forth below. Amethyst has submitted a Petition in which it asks the Florida Department of Children and Families ( DCF ) to interpret Florida statutes such that Sections and would not apply to its provision of Day or Night Treatment with Community Housing. For the reasons set forth herein, FARR urges the DCF to reject that interpretation. Basis for Motion to Intervene FARR has a direct interest in the nature and outcome of these proceedings. Fla. Stat provide a statutory scheme of credentialing and regulating recovery residences in Florida. FARR is an affiliate of the National Alliance for Recovery Residences (NARR) and operates as a nonprofit entity administering certification programs according to NARR standards. FARR is a credentialing entity under Fla Stat , and has been approved by the DCF under Fla. Stat (2). Under Fla. Stat , a recovery residence s ability to make or accept referrals depends, in many cases, upon whether it is certified by a credentialing agency. As of the time of this Motion, FARR believes it is the only credentialing entity approved in Florida for the certification of recovery residences. FARR therefore has a substantial interest in this Department s ultimate decision concerning what entities are subject to certification by a credentialing entity. For these reasons, FARR submits that it should be permitted to intervene as party to the Petition filed by Amethyst, pursuant to Fla. Stat (13)(b) and Rule (2)(c), F.A.C. 1
80 Discussion and Comments It is FARR s position that Fla. Stat and are properly interpreted to apply to entities licensed for Day or Night treatment with Community Housing ( D/N with Community Housing ). There is no question that these statutes apply to recovery residences in Florida. Recovery residence is defined as a residential dwelling unit, or other form of group housing, that is offered or advertised through any means, including oral, written, electronic, or printed means, by any person or entity as a residence that provides a peer-supported, alcoholfree, and drug-free living environment. Fla. Stat (37). The Community Housing component of D/N with Community Housing fits squarely within the definition of Recovery Residence : such housing is residential in nature, houses a group of people, is offered and/or advertised to persons seeking substance abuse treatment, and provides a living environment that is peer-supported, alcohol-free, and drug-free. There is no aspect of community housing that distinguishes it from recovery residence. The definition of Day or night treatment with community housing is a program intended for individuals who can benefit from living independently in peer community housing while participating in treatment services for a minimum of 5 hours a day for a minimum of 25 hours per week. Fla. Stat (26)(a)(3). This definition is a sub-definition of Clinical treatment, indicating that D/N with Community Housing is licensable, which indeed it is under DCF rules. There is nothing in the statute to indicate that a provider is free from requirements placed on recovery residences if it operates housing that meets the definition of recovery residence, notwithstanding that it may label itself under another name. To interpret the statute in any other manner, such as the way Amethyst suggests in its Petition, would frustrate the intent and the letter of Florida statutes. As set forth below, (1) the legislative purpose of statutory amendments was to create oversight of group residences for people undergoing substance abuse treatment, (2) the practices of clinical treatment providers have evaded much-needed oversight of group housing, (3) NARR certification criteria are consistent with the requirements of Florida law, and (4) treating community housing as distinct from recovery residence would be inconsistent with the statutory scheme. 2
81 1. The legislative purpose of statutory amendments was to create oversight of group residences for people undergoing substance abuse treatment. In 2015, the Florida Legislature enacted HB 21, which created Fla. Stat , and thus created the system by which recovery residences obtained certificates of compliance from a credentialing entity. HB 21 further amended Sections and The amendment to Section added the definition of recovery residence, in addition to other related definitions. The amendment to Section added subsection (11), a provision that read in full: Effective July 1, 2016, a service provider licensed under this part may not refer a current or discharged patient to a recovery residence unless the recovery residence holds a valid certificate of compliance as provided in s and is actively managed by a certified recovery residence administrator as provided in s or the recovery residence is owned and operated by a licensed service provider or a licensed service provider s wholly owned subsidiary. For purposes of this subsection, the term refer means to inform a patient by any means about the name, address, or other details of the recovery residence. However, this subsection does not require a licensed service provider to refer any patient to a recovery residence. Under this provision, a service provider could place a patient in a residence without obtaining any certification as long as the service provider owned and operated the residence. In 2017, the Legislature passed HB 807, which deleted Section (11) and added Section Under the new statute, all recovery residences must have a certificate of compliance in order to accept referrals, regardless of whether the recovery residence is owned by the licensed service provider, subject to certain other exceptions. A referral occurs any time a provider informs a patient by any means about the name, address, or other details of a recovery residence. Section (3) (this definition of referral is unchanged from the previous version of the statute). The now-superseded statutory text permitted a licensed service provider to house patients in residences owned by that provider without any need for certification. The fact that the statute explicitly contemplated this scenario a licensed service provider owning patient residences shows that the Legislature, at that time, permitted D/N with Community Housing programs to have an exception to the general rule that recovery residences must be certified. The 2017 amendment in HB 807 eliminated that exception. This amendment shows that the legislature intended to end the exception that applied to D/N treatment with Community Housing programs. 3
82 It is therefore incorrect for Amethyst to state in its Petition that For Community Housing, there are no referrals to the Community Housing component of a D/N treatment facility. (Petition, p. 4). The treatment facility must obviously inform a patient of the name and address of the residence, which constitutes a referral under (3). Amethyst s argument presupposes that the statute excludes community housing from the definition of recovery residence, which the statute does not. 2. The practices of clinical treatment providers have evaded much-needed oversight of group housing. Community-based recovery housing, when coupled with outpatient clinical care, has been shown to produce improved outcomes for persons seeking resilient recovery from substance use disorder. However, research has also shown that such improved outcomes depend on patients/residents engagement in meaningful, community-based activities while residing in peersupportive environments that foster a culture of recovery support. The Recovery Support domain of NARR Quality Standards suggests thirteen concrete practices that promote resident engagement in their own recovery plan. D/N with Community Housing licensure criteria pertaining to the housing component focus entirely on property and safety concerns. FARR certification of licensed providers recovery housing ensures that the residential environments, where patients spend 85% of their week, contribute positively to the overall therapeutic experience. Without any requirement for certification by some credentialing entity, the DCF has no means of ensuring that any community housing is conducive to patients well-being. The history of patient housing practices in Florida has demonstrated the need for this oversight. The recent Grand Jury Report, upon which the Legislature based its amendments to Chapter 397, specifically found: evidence of horrendous abuses that occur in recovery residences that operate with no standards. For example, some residents were given drugs so that they could go back into detox, some were sexually abused, and others were forced to work in labor pools. There is currently no oversight on these businesses that house this vulnerable class. Even community housing that is a part of a DCF license has no oversight other than fire code compliance. This has proven to be extremely harmful to patient. p.17 (last visited July 17, 2018). The grand jury report continued: 4
83 Id., pp [T]here is a need for oversight on patient housing during PHP and IOP treatment, which most often takes place immediately after discharge from inpatient treatment. Accordingly, the Grand Jury finds that the Legislature should eliminate the loophole found in Florida Statute section (11) that allows treatment providers to refer patients to uncertified recovery residences that they own. This loophole only benefits treatment providers who can afford to own patient housing in addition to an inpatient treatment center, and allows them to refer patients to non-certified recovery residences which have no DCF or FARR oversight. In other words, it allows providers to send patients to unverified and unregulated recovery residences while those patients are in their most vulnerable state of recovery (during or immediately after inpatient treatment). This is contrary to the purpose of recently enacted section (11), which was designed to protect patients from being referred to unregulated recovery residences. The fact that the provider happens to have an ownership interest in the uncertified recovery residence does nothing to protect this vulnerable class of disabled consumers. Therefore, we recommend that this loophole for provider-owned referrals be closed. Amethyst s position is completely contrary to the Legislative intent behind closing this loophole for providers who own housing. 3. NARR certification criteria are consistent with the requirements of Florida law. NARR Support Level IV Recovery Residences are the housing components of licensed outpatient treatment providers. Community housing components of D/N with Community Housing are thus considered Level IV Recovery Residences. Such Recovery Residences are required to offer clinical services; however, in accordance with state law, these clinical services are not delivered within the residence itself. Support Level IV Recovery Residences blend clinical and social models of recovery to produce enhanced outcomes for the population served. Incidentally, this blended model mirrors the statutory definition of Day or night treatment with community housing in Fla. Stat (26)(a)(1). NARR Support Level IV locations account for 39.22% of FARR current census. All have successfully achieved this blend and comply with NARR Quality Standards for Support Level IV Residences. Amethyst claims that it cannot be considered a Recovery Residence because recovery residences must charge for rent. To the contrary, NARR Quality Standards are silent on the subject of patient responsibility for payment for room and board while living in certified 5
84 recovery housing operated by a licensed outpatient provider. Actually, many certified recovery residences accept payment from third-party entities and/or family members until the resident has achieved gainful employment. FARR does, however; deny certification to any applicant, regardless of NARR Support Level, when evidence demonstrates that free or discounted room and board is offered as a patient inducement to drive enrollment in outpatient services. Such a practice would violate Fla. Stat , which prohibits patient brokering. FARR considers the practice of bundling room and board into D/N with Community Housing services as consistent with Florida Law. Patients who are engaged in twenty-five (25) hours a week of clinical outpatient care cannot reasonably be expected to also maintain full-time employment to support their basic needs for shelter and nutrition. This practice does not, in FARR s opinion, violate Fla. Stat or produce an event of non-compliance with NARR Quality Standards. However; should FARR uncover, as part of its certification process, that these patient benefits are employed by an applicant for marketing purposes as an inducement to drive enrollment in a D/N with Community Housing program, this would result in a recommendation for declination by the FARR Certification Administrator to the FARR Compliance Committee. Amethyst, therefore, is not required to charge rent to its patients in order to obtain FARR certification, as long as it is not otherwise violating generally applicable Florida law prohibiting patient brokering. In addition, Amethyst has listed eight FARR requirements in its petition that it claims are inconsistent with the Community Housing component of licensed service providers (Petition, p. 3). This assertion is incorrect. Taken in turn: NARR Quality Standards (Resident fees and required policies and accounting systems): These standards to do not mandate that the licensed provider charge rent, if the practice of providing residence rent-free is permitted by Florida Law (D/N with Community Housing License or State funded vouchers). NARR Quality Standards state that Recovery Residences must inform residents of all FEES and CHARGES they will, or could potentially be responsible for, have a clear refund policy, and implements an accounting system that documents financial transactions. Fees and charges include more than housing. Licensed service providers are required to provide residents a fee schedule which includes costs associated 6
: Recovery residences must provide current residents with a voice in the acceptance of new members.")
85 with treatment and treatment w/housing, ancillary charges, any fines for community rule violations, drug testing, etc. NARR Quality Standard 8.01 (Residents have a voice in the acceptance of new members): Recovery residences must provide current residents with a voice in the acceptance of new members. This does not mean the provider should allow the residents to conduct screening assessment and/or make final admission determinations. Many NARR Support Level IV Recovery Residences incorporate a senior peer in the new resident orientation process. The senior peer informs management via written evaluation of any potential risks presented by the new member or his/her perceptions regarding the new resident s willingness to comply with community rules/requirements. Other NARR Support Level IV Recovery Residences incorporate a buddy system wherein a senior peer is assigned to accompany new residents during all offsite excursions during the first four weeks. The senior peer communicates to management any concerns observed pertaining to that new resident s engagement in communitybased activities. The peer voice is essential to fostering a culture of recovery support within the residential peer community. Furthermore, this accommodation allows new residents to get acquainted with peers. It further enhances the community by providing senior peers responsibility for nurturing a culture recovery support NARR Quality Standard (Residents share in household expenses) There is no FARR requirement that Residents share in household expenses. Rather, in order to be certified, recovery residences are required to show that 50% of the following six criteria are met. 7

86 This standard ensures that there is a functionally equivalent family in the residence, which is foundational to Fair Housing protections for persons with a substance use disorder. One of the six criteria is do residents share in household expenses? However, the recovery residence must meet only three of the criteria in order to be certified for instance, if residents are involved in food preparation and cleaning, and they have access to the common areas of the home, then they need not necessarily share in household expenses. NARR Quality Standard 8.02 (Policies that promote resident-driven length of stay.) This standard is inapplicable to Amethyst. A D/N with Community Housing provider is considered a Level IV Recovery Residence. Level IV Recovery Residences determine the length of stay based on clinical assessment. As Standard 8 makes clear, policies and procedures that promote resident-driven length of stay does not apply to Level IV Recovery Residences: NARR Quality Standard (Involve peers in governance in meaningful ways) Amethyst has misleadingly re-worded this standard as some rules are made by and enforced by the residents (not the staff). In reality, peer governance is an essential factor in creating a family equivalent and a culture wherein residents hold one another accountable to community rules and engagement in concrete recovery plans. This does not necessarily suggest that residents create and enforce rules, but that they should be provided the opportunity to contribute to creation and enforcement of some rules. For example, ethical operators would never want or permit residents to hold negative contracts, i.e. have knowledge that a fellow housemate is using alcohol and/or illicit drugs and failing to inform management. As another example: as part of developing a healthy lifestyle, most recovery residences, regardless of Support Level, assign household chores to their residents. Often, operators form a peer council that is empowered to determine chore responsibilities and to hold peers accountable 8
87 for completing these assignments. The peer council may decide that TVs should be silenced at 11 pm so as to create/maintain a harmonious living environment for all residents. This standard is intended to implement peer governance in meaningful ways and prepare residents for independent living. NARR Quality Standard (A resident council that has a voice in the governance of the home.) Standard 12 nurtures a peer supportive environment and helps create a functional family dynamic. It does not mean that residents are responsible for managing or governing the home, but rather that residents have a voice in governance of their home. NARR Quality Standard (evidence of documentation that residents participate in the development of their recovery plan including an exit plan and lifelong plan): Typically, NARR Support Level IV Recovery Residences show compliance to this standard via individual Treatment Plans and Treatment Plan reviews. This does not mean that clinical services are actually being provided in the residence. In the certification process, FARR requests evidence that treatment planning also includes community integration and social model integration. Examples include attending mutual aid meetings and/or faith-based organization meetings, participating in educational opportunities, developing a network of sober support contacts, obtaining a 12 step sponsor/recovery mentor and/or recovery coach, engaging in a concrete recovery pathway, community volunteerism or service commitments, community-based life skills programming, attending employment readiness classes, or while enrolled in IOP/OP level of care, obtaining employment while participating in clinical services. This Standard is consistent with the DCF s requirements for D/N with Community Housing services as set forth in 65D (2), F.A.C. NARR Quality Standard (Weekly schedule of recovery-oriented presentations, group exercises, and activities.) There is no requirement that these presentations, exercises and activities be provided onsite at the recovery residence. Recovery Residences may demonstrate that residents are participating in recovery support services in formal settings recognized by NARR such as: evidencing Treatment Modalities, Life Skills Programming, Relapse Prevention, Peer Support Services are delivered at the clinical facility. This Standard is also consistent with the DCF s 9
88 requirements for D/N treatment with Community Housing services as set forth in 65D (2), F.A.C. d. Treating community housing as distinct from recovery residence would be inconsistent with the statutory scheme. Prior to amendments to the relevant statutes, a business operating D/N with Community Housing could refer patients to the community housing it owned as long as it was licensed by the DCF for its clinical services. Under 65D , F.A.C., such a provider faced virtually no scrutiny regarding its community housing beyond demonstrating that it complied with fire, health, and safety codes. Providers could therefore avoid having to satisfy credentialing entities that the community housing did what was contemplated by the statutory definition of Day or night treatment with community housing : a program intended for individuals who can benefit from living independently in peer community housing while participating in treatment services. Without FARR certification, there would be no way for the DCF or any other state agency to be satisfied that patients are likely to benefit at all from their living condition. It is unlikely that the Florida Legislature ever intended for such providers to escape this scrutiny when other recovery residences generally had to seek certification. However, following the 2017 amendments to the statute, there can be no lingering doubt. The statute contains broad definitions of both recovery residence and referral that clearly encompass the business practices that Amethyst describes in its Petition. Under the statutory interpretation that Amethyst proposes, providers that own recovery residences could return to pre-amendment conditions as long as they seek licensure as a day or night treatment with community housing provider. This is precisely the conduct that the amendments sought to eliminate. Conclusion Although Amethyst has attempted to identify FARR requirements that are inconsistent with Florida law, in reality the NARR guidelines that FARR employs are entirely consistent with, and help to further, existing Florida law as it pertains to D/N with Community Housing providers. Furthermore, nowhere in its petition does Amethyst identify any definition or characteristic of its housing component that does not fall squarely within the definition of recovery residence in the relevant statute. Both the text of the statute and the intent of the legislature dictate that businesses licensed to provide day or night treatment with community housing should be governed by Sections and
89 CERTIFICATE OF SERVICE The undersigned hereby certifies that a true and correct copy of the foregoing Motion to intervene has been furnished by to Agency.Clerk@myflfamilies.com; and by to counsel for Amethyst Recovery Center, LLC: Karina P. Gonzales, Esquire, at Karina@floridahealthcarelawfirm.com and Admin.Pleadings@floridahealthcarelawfirm.com on July 3, By: /s/ Susan B. Ramsey Susan B. Ramsey Fla. Bar No Jeffrey V. Mansell Fla. Bar No ROMANO LAW GROUP 1005 Lake Avenue Lake Worth, FL Telephone: (561) Facsimile: (561) Susan@romanolawgroup.com Jeff@romanolawgroup.com Dawn@romanolawgroup.com Copies also furnished to: Ute Gazioch: Ute.Gazioch@myflfamilies.com John Bryant: John.Bryant@myflfamilies.com Suzette Fleischmann: Suzette.Fleischmann@myflfamilies.com Chris Weller: Chris.Weller@myflfamilies.com Al Johnson: Ajohnson@sa15.org Justin Chapman: jchapman@sa15.org Dave Aronberg: dave@sa15.org 11
90 PETITION FOR DECLARATORY STATEMENT BEFORE THE FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES IN THE MATTER OF: Amethyst Recovery Center, LLC, Petitioner / Case No.: PETITION FOR DECLARATORY STATEMENT Petitioner, Amethyst Recovery Center, LLC, (Petitioner) pursuant to Section , Fla. Stat., and Rule , F.A.C., serves this Petition for Declaratory Statement on the Florida Department of Children and Family ( DCF ). The Petitioner believes a controversy exists and/or is in doubt concerning the applicability of statutory provisions under Sections and , Fla. Stat. and as grounds in support of its Petition states as follows: Petitioner is a Substance Abuse treatment facility and is currently licensed by DCF for Day or Night treatment with Community Housing. (D/N with Community Housing) pursuant to Section with standards defined in Rule 65D Petitioner is located at 2000 SE Port St. Lucie Blvd. Suites A, B, C D, Port St. Lucie, Florida All the Petitioner s licensed components, including Community Housing is owned by one company, Amethyst Recovery Center, LLC. The Community Housing is not a wholly owned subsidiary. Amethyst has standing to request a Declaratory Statement from the DCF agency because FARR (Florida Association of Recovery Residences) has threatened provider license suspension or revocation of D/N with Community Housing [including Residential 5] programs that are not certified pursuant to Section Fla. Stat. by July 1, FARR s position substantially affects the Petitioner as the standards for Recovery Residences are inconsistent with DCF s regulations governing D/N with Community Housing. The State Attorneys office has stated that it agrees with FARR s position. Amethyst is not involved with any litigation related to the question presented for a Declaratory Statement. Amethyst has not filed or plans to file a similar question with any other state or local agency. BASIS OF THE REQUEST FOR AN AGENCY DECLARATORY STATEMENT Does the Voluntary Certification of Recovery Residences administered by FARR apply to a Florida treatment facility that is licensed by DCF to provide clinical services under D/N treatment with Community Housing program? The Statutory provisions and agency rules on which the Declaratory Statement is sought relates to Sections and
91 DAY/NIGHT WITH COMMUNITY HOUSING DCF regulates substance abuse treatment through licensing individual treatment components under Chapter 397, Fla. Sta. and Rule 65D-30, F.A.C. Petitioner operates a D/N with Community Housing which is one service component set out in Rule 65D-30. DCF issued one license which is valid for the specific service component listed for the specific location identified on the license. Sec (6). A separate license is required for each service component maintained by the service provider listed in Sec (26). Petitioner Amethyst provides clinical treatment defined as professional directed, deliberate, and planned regime of services and interventions that are designed to reduce or eliminate the misuse of drugs and alcohol and promote a healthy, drug-free lifestyle. Clinical treatment services include D/N with Community Housing as a licensable service component. Section (26(a). D/N treatment with Community Housing means a program intended for individuals who can benefit from living independently in peer community housing while participating in treatment services for a minimum of 5 hours a day for a minimum of 25 hours a week. Section (26(a)(3). (Bolded for emphasis). Clinical treatment services include a range of licensable service components set out in Rule 65D-30. Some of these are Addictions receiving facility, Day or Night treatment, D/N treatment with community housing, Detoxification, Intensive inpatient treatment, and Intensive outpatient treatment, to name a few. Standards for D/N Treatment with Community housing require that clients live in a supportive, community housing location while participating in treatment. Further 65D prohibits D/N Community Housing operators from providing services in the community housing. There are no resident fees for living in community housing, length of stay is determined by clinical team based on the individual s progress in treatment. There are no referrals made or accepted to the Community Housing component; it is a part of the service component licensed by DCF. An individual must be admitted to a clinical treatment program to live in the Community Housing component of the program. Community Housing is used solely for the purpose of assisting clients, who are participating in treament experience needed life skills to transition to independent living. RECOVERY RESIDENCES The Florida legislature found that a person suffering from addiction has a higher success rate of achieving long-lasting sobriety when given the opportunity to build a stronger foundation by living in a Recovery Residence after completing treatment. The Legislature further finds that this state and its subdivisions have a legitimate state interest in protecting these persons, who represent a vulnerable consumer population in need of adequate housing. Section (1) Fla. Stat. Voluntary certification of recovery residences. (Bolded for emphasis). PAGE 2
92 Recovery residences (also known as sober homes or sober living homes) are alcohol and drugfree living environments for individuals in recovery who are trying to maintain abstinence. A recovery residence offers no formal treatment, but some residences strongly encourage voluntary attendance at 12-step groups. An individual living in a recovery residence is required to pay for room and board and any other services they receive in the residence. DCF does not license recovery residences. The legislature enacted law to establish a program for recovery residences and recovery residence administrators. DCF approved two credentialing private entities to design a certification program and issue certificates. FARR certifies the recovery residences and The Florida Certification Board certifies recovery residence administrators. Since July 1, 2016, Florida has prohibited licensed substance abuse service providers from referring patients to a Recovery Residence unless the Residence holds a valid certificate of compliance from FARR and is actively managed by a FARR certified recovery residence administrator. There is no such mandate for the Community Housing component of a licensed D/N treatment facility. This difference between a Community House and a Recovery Residence is the area of conflict and doubt that has arisen. FARR requires applicants to have policies or procedures which licensed service providers cannot comply with. Rule 65D-30, prohibits D/N Community Housing operators from providing services in the housing. FARR requirements below are part of a clinical program and would not apply to D/N Treatment with Community Housing. Evidence of documentation that residents participate in the development of their recovery plan including an exit plan and lifelong plan. Weekly schedule of recovery-oriented presentations, group exercises, and activities. Neither the definition of recovery residence nor Section make mention of providing services to residents. Regardless of whether the services are clinical, life skills or are recovery oriented.. The following FARR requirements are also inconsistent with the Community Housing component of licensed service providers and may also be inconsistent with Recovery Residences as FARR seeks to fit NARR (National Alliance of Recovery Residences) levels onto the Florida models: Resident fees and required policies and accounting systems. Residents have a voice in the acceptance of new members. Residents share in household expenses. Policies that promote resident-driven length of stay. Some rules are made by and enforced by the residents (not the staff). A resident council that has a voice in the governance of the home. Evidence of documentation that residents participate in the development of their recovery plan including an exit plan and lifelong plan. Weekly schedule of recovery-oriented presentations, group exercises, and activities. PAGE 3
93 DISCUSSION/CONCLUSION Licensed facilities are being bombarded with notice, blogs, memos, s from FARR, the State Attorneys Office, and a member of the Sober Home Task Force-Proviso Group with interpretations mandating that voluntary certification from FARR is required for DCF licensed facilities. Further FARR and its supporters are equating licensable components such as Community Housing with Recovery Residences or Sober Homes. For Community Housing, there are no referrals to the Community Housing component of a D/N treatment facility. There are no referrals from a D/N treatment facility to Community Housing. D/N treatment and Community Housing are one and the same in the eyes of the statute. Clients in Community Housing are participating in treatment. Unlike a sober living facility where clients have completed treatment and are now focusing on sober living. DCF mandates that no services are to be provided in Community Housing. Clients are in treatment and are residing in Community Housing and are not charged for rent or food. Section requires that a FARR certified Recovery Residence be actively managed by a certified recovery residence administrator. The only staff coverage for Community Housing that is required is a paid employee on call during the time when clients are at the housing location. Rule 56D Our review of the Statutes and Rules lead to one conclusion which is that FARR s voluntary certification is not required for a DCF licensed facility. However, FARR and its supporters are pushing voluntary certification and advising the community that it is mandatory to avoid suspension of DCF license and avoid sanctions imposed for operating. A review of CS/CS/HB 807 Final Bill Analysis does not provide any historical support for FARR s attempt to push D/N treatment facilities with Community Housing into their certification program. DCF already has the right to enter and inspect a licensed provider at any time to determine statutory and regulatory compliance. Noncompliance licensed facilities are provided with reports of their noncompliance and given corrective action plans with completion deadlines. DCF may deny, suspend or revoke a license, it may impose restrictions and penalties on licensed providers who are not in compliance. DCF also recognizes accreditation by accrediting organizations such as the Commission on Accreditation of Rehabilitation Facilities (CARF), The Joint Commission (TJC), and the Council on Accreditation (COA). Where providers are licensed based in part on a survey report of a DHS recognized accrediting organization, the license includes a statement to that effect. 65D (a)(d). On the other hand, Recovery Residences had no such accrediting organizations. To correct some of the deficiencies found in an unaccredited and unregulated residence, the legislature created the certification process now under FARR s jurisdiction. There would be no need to create a certification process for a housing component of D/N treatment which already had accredited organizations. PAGE 4
94 Because of the FARR certification deadline, Petitioner Amethyst requests an expedited review so that the agency can issue a Declaratory Statement clarifying the applicability of Sections and to Florida licensed facilities under Section , and Rule 65D CERTIFICATE OF SERVICE I CERTIFY that a true and correct copy of the Petition for Declaratory Statement has been furnished by , Agency.Clerk@myfamilies.com; and to Fax No to the Agency Clerk, Department of Children and Families at 1317 Winewood Blvd., Building 2, Room 204, Tallahassee, Florida on June 12, KARINA P. GONZALEZ, ESQUIRE Attorney for Petitioner Amethyst The Florida Healthcare Law Firm The CenterState Bank Building 909 Southeast 5 th Avenue, Suite 200 Delray Beach, FL Phone: Fax: Karina@floridahealthcarelawfirm.com Admin.Pleadings@floridahealthcarelawfirm.com By: _/s/_karina P. Gonzalez KARINA P. GONZALEZ, ESQUIRE Fla. Bar No.: PAGE 5
95 BEFORE THE FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES IN THE MATTER OF: Amethyst Recovery Center, LLC, Case No.: CF Petitioner Notice ID (June 13, 2018) / PETITIONER S RESPONSE IN OPPOSITION TO FARR S MOTION TO INTERVENE Amethyst Recovery Center, LLC ( Petitioner ) pursuant to Rule serves its Response in Opposition to FARR s Motion to Intervene served by Florida Association of Recovery Residences ( FARR ) Petitioner served the Petition for Declaratory Statement to the DCF Agency because it believes a controversy exists and it is in doubt concerning the applicability of Sections and , Fla Stat. to its DCF licensed Day or Night treatment with Community Housing program. (D/N with Community Housing). FARR LACKS STANDING TO INTERVENE FARR moved to intervene claiming that it has a direct interest in the nature and outcome of the Petition for Declaratory Statement because it is the credentialing entity that has been approved by DCF. It claims that as the only credentialing entity it has a substantial interest in DCF s ultimate decision concerning what entities are subject to certification by FARR. FARR has not plead any facts to show how it will be affected by the disposition of the Declaratory Statement. FARR s arguments are centered on its jurisdiction as the credentialing entity approved in Florida for the certification of Recovery Residences. FARR has not plead any details of how its substantial interests will be affected and what is the nature of the injury which would result from a Declaratory Statement from DCF. FARR lacks standing to intervene in the Petition for Declaratory Statement. Rule (1) allows persons, other than the original parties, whose substantial interests will be affected by the Declaratory Statement and who desire to become parties to move for leave to intervene. Page 1
96 Before a party can be considered to have a substantial interest in the outcome of the proceeding, it must show that (1) it will suffer injury in fact which is of sufficient immediacy to entitle the party to a Section hearing, and (2) that the substantial injury is of a type or nature which the proceeding is designed to protect. Agrico Chem. Co. v. Dep t of Envtl. Regulation, 406 So. 2d 478 (Fla. 2d DCA 1981). The Agrico two-prong test is used to determine when a third party meets the substantial interest element of Section (13) (b). What FARR pleads as a substantial interest is its interpretation of the legislative purpose in enacting Sections and The interests identified in the Motion to Intervene are framed as: the practices of clinical treatment providers evading much-needed oversight of group housing; NARR (National Alliances for Recovery Residences) certification criteria as being consistent with Florida law; and considering Community Housing as distinct from Recovery Residence is inconsistent with the statutory scheme. Page 2 of FARR s Motion to Intervene. UNPROMULGATED RULE/STATUTORY ENLARGMENT In its Discussion and Comments section, FARR claims that Sections and are properly interpreted to apply to entities licensed for D/N treatment with Community Housing. FARR goes on to interpret the definition of a Recovery Residence in Section (37) Fla. Stat. as applying to the Community Housing component of D/N treatment. FARR s discussion is fatally flawed because no Rule has been promulgated that interprets Sections and FARR states that the definition of Community Housing fits squarely within the definition of Recovery Residence because the housing is residential in nature, houses a group of people, is offered and/or advertised to persons seeking substance abuse treatment and provides a living environment that is peer-supported, alcohol and drug free. FARR then concludes that there is no aspect of Community Housing that distinguishes it from a Recovery Residence. As FARR pointed out, the legislature enacted HB 21 (1015) which created Section HB 807 (2017). The legislature passed House Bill 807 (2017) which added Section The Bill Analysis for House Bill 21 clearly states that DCF regulates substance abuse treatment through licensure. House Bill 807 Bill Analysis states that Florida does not license recovery residences. Page 2
97 Instead, in 2015 the Legislature enacted sections , F. S., which establish voluntary certification programs for recovery residences and recovery residence administrators, implemented by private credentialing entities. Further, Section (1) is very explicit in its language that Recovery Residences are inhabited by persons who have completed treatment: The Legislature finds that a person suffering from addiction has a higher success rate of achieving long-lasting sobriety when given the opportunity to build a stronger foundation by living in a recovery residence after completing treatment. (Emphasis supplied.) By way of comparison, persons utilizing D/N Treatment with Community Housing must be participating in treatment services for a minimum of 5 hours a day for a minimum of 25 hours per week. Purportedly acting as a representative of DCF, FARR enlarges on the statutory language itself and the intent of the statute as demonstrated through HB 21 (2015) and HB 807 (2017) Bill Analyses. Further, FARR s statement that the Community Housing component of D/N with Community Housing fits squarely within the definition of Recovery Residence... amounts to an agency statement of general applicability, and thus a rule as defined by Section (16), Fla. Stat. Rule means each agency statement of general applicability that implements, interprets, or prescribes law or policy or describes the procedure or practice requirements of an agency and includes any form which imposes any requirement or solicits any information not specifically required by statutes or by an existing rule. The term also includes the amendment or repeal of a rule. Section (1)(a) requires that each agency statement defined as a rule by Section , Fla. Stat. be adopted pursuant to rulemaking procedures under Section Here, no rule has been promulgated which incorporates the Community Housing aspect of D/N with Community Housing into the application of Section or An agency statement that meets the definition of a rule under Section , but which has not been promulgated pursuant to Section , constitutes an invalid exercise of delegated legislative authority and, therefore, is unenforceable. Dep t of Revenue v. Vanjaria Enters, Inc., 675 So. 2d 252 (Fla. 5th DCA 1996) (citing Dep t of Natural Resources v. Wingfield Dev. Co., 581 So. 2d 193, 196 (Fla. 1st DCA Page 3
98 1991)). FARR s statements regarding the applicable statutes amounts to an unpromulgated rule and cannot be enforced. DISCUSSION OF FARR S AGRUMENTS IN ITS MOTION FARR admits that under Section (26) (a)(3) D/N with Community Housing is a licensed service component which includes a comprehensive continuum of accessible and quality substance abuse prevention, intervention, and clinical treatment services under Chapter 397. FARR admits that D/N with Community Housing program are subject to DCF Licensing and Regulatory Standards. But, FARR s concludes that there is nothing in the statute to indicate that a provider is free from requirements placed on recovery residences if it operates housing that meets the definition of recovery residence, notwithstanding that it may label itself under another name. Page 2 of FARR s Motion. FARR s interpretation is flawed and not supported by standards and requirement of Florida law and not supported by logic or facts: it is therefore arbitrary. Further, FARR s interpretation enlarges on Section , Florida Statutes. Section (1) provides that recovery residences are for persons to live in after completing treatment. FARR s interpretation to include Community Housing of D/N within Section , attempts to circumvent the clinical components of care which are part of the D/N treatment program -- admission to the treatment program is mandatory to be eligible for Community Housing. If the person is not in treatment, they would not qualify for D/N with Community Housing. Persons in D/N with Community Housing have not yet reached the recovery phase of addiction where they have completed treatment as indicated in the language of Section FARR s interpretation is irrational and therefore capricious. In addition to its DCF license for the D/N with Community Housing, Petitioner is accredited by The Joint Commission. It follows ASAM (American Society of Addiction Medicine) Admission Criteria for adults in the D/N program which is a national set of criteria for providing outcomeoriented and results-based care in the treatment of additions. FARR s interpretation that D/N with Community Housing must be FARR separately certified using its NARR Level IV standards for recovery residences conflicts with Florida s statutory and rule provisions. Indeed, FARR s interpretation is not logical and is irrational. It is both arbitrary and capricious. Further, FARR s Page 4
99 interpretation imposes additional regulatory costs on Petitioner Amethyst, an already regulated entity, licensed by DCF and accredited by The Joint Commission. FARR states that the Community Housing components of D/N programs are considered NARR Level IV Recovery Residences they are the licensed outpatient treatment providers. Page 5 of the Motion to Intervene. It claims that these NARR Level IV Recovery Residence are required to offer clinical services, however in accordance with state law these clinical services are not delivered within the residence itself. FARR states that these Level IV Recovery Residences blend clinical and socials models to produce advanced outcomes. Page 5. FARR s argument is illogical and irrational and contrary to Section (1) which states that it is unlawful for any person or agency to act as substance abuse provider unless it is licensed or exempt from licensure. Unlike Recovery Residences which the Florida legislature found needed oversight because they were unlicensed and unregulated, offered no formal treatment and are self-funded through resident fees, D/N with Community Housing goes through a licensing process with DCF. (House Bill 807, Bill Analysis). D/N treatment providers pay licensing fees, are inspected, respond to deficiencies and comply with corrective actions, and are governed by rules set forth in Rule 65D Certification of D/N with Community Housing serves no additional state purpose other than for FARR to collect fees and costs to perform the Recovery Residence certification process. FARR argues that The practices of clinical treatment providers have evaded much-needed oversight of group housing. Paragraph 2. Clearly this is not the case. While this statement may have applied to the unlicensed and unregulated Recovery Houses, there is nothing in the statutes or any regulation to substantiated this interpretation. FARR intermingles the standards for Community Housing while a patient is in treatment with Recovery Housing which traditionally had no treatment, no oversight and may have been susceptible to questionable practices. Florida DCF has oversight jurisdiction over standards for D/N with Community Housing. In addition to inspections for fire, safety and health codes, the Petitioner must comply with Facility Standards pursuant to Rule 65D This component allows clients to live in a supportive community housing while participating in treatment. This means that no treatment takes place in Page 5
100 the community housing where the clients live. The housing is used solely to assist the clients in making a transition to independent living while in treatment. There are standards for the appropriateness of the level of care as it applies to the individual client. Rule 65D (1) (a-f). These clients are provided with ancillary services such as transportation, assistance with shopping, or assistance with medical referrals and may attend and participate in social and recovery-oriented activities in addition to other clinical services. Services are provided according to the needs of the client identified in the facility treatment plan; included are individual counseling, group counseling, counseling with families, substance abuse education. Clients receive life skills training in areas such as anger management, communication skills, employability skills, problem solving, relapse prevention, recovery management, decision-making relationship skills, symptom management and food purchase and preparation and non-verbal therapies. Petitioner Amethyst is not a Recovery Residence as the term is defined in Section (37). D/N treatment with Community Housing is explicitly defined in Section (26) (3) and falls under licensed service components which means a discrete operational entity with a service provider which is subject to licensing as defined by rule. Sections (26), (42). Section (37) defines Recovery Residence as a residential dwelling unit or other form of group housing that is offered or advertised through any means, including oral, written, electronic, or printed means, by any person or entity as a residence that provides a peer-supported, alcoholfree and drug free environment. If Petitioner wants to refer an individual who has completed D/N treatment, is ready for discharge and desires to live in a Recovery Residence, it must refer to a Recovery Residence that is FARR certified and managed by a certified Recovery Residence Administrator. Section Likewise, Petitioner cannot accept a referral from a Recovery Residence that is not FARR certified. Section (1). Except, however, referrals may be made by a Recovery Residence to a licensed service provider when the Recovery Residence owners, directors, operators do not benefit from the referral. Section After July 1, 2018, if a licensed service provider has a Page 6
101 Recovery Residence that is its wholly owned subsidiary, then it can only refer or accept a referral if the residence is FARR certified. Under (6) there is nothing in that section requiring Petitioner to refer a patient or accept a referral of a patient from a Recovery Residence. CONCLUSION In its Motion to Intervene, FARR has not plead any details of how its substantial interests will be affected and what is the nature of the injury which would result from a Declaratory Statement from DCF. FARR lacks standing to intervene in the Petition for Declaratory Statement. Rule (1) allows persons, other than the original parties, whose substantial interests will be affected by the Declaratory Statement, to move for leave to intervene and become parties. FARR s interpretation that the statutory language in Sections and applies to D/N treatment with Community Housing licensed programs amounts to an agency statement of general applicability thus a rule under Section (16). No rule has been promulgated which incorporates Community Housing into the application of Sections , or therefore this is an invalid exercise of delegated legislative authority and is unenforceable. Page 7
102 CERTIFICATE OF SERVICE I CERTIFY that a true and correct copy of the Petitioner s Response in Opposition to FARR s Motion to Intervene has been furnished by , to Agency.Clerk@myfamilies.com; and to Fax No to the Agency Clerk, Department of Children and Families at 1317 Winewood Blvd., Building 2, Room 204, Tallahassee, Florida ; and by to Counsel for FARR, Susan B. Ramsey at susan@romanolawgroup.com; Jeff@romanolawgroup.com; Dawn@romanolawgroup.com on July 9, KARINA P. GONZALEZ, ESQUIRE Attorney for Petitioner Amethyst The Florida Healthcare Law Firm The CenterState Bank Building 909 Southeast 5th Avenue, Suite 200 Delray Beach, FL Phone: / Fax: Karina@floridahealthcarelawfirm.com Admin.Pleadings@floridahealthcarelawfirm.com By: /s/ Karina P. Gonzalez KARINA P. GONZALEZ Fla. Bar No.: Page 8

103
104
105
106
107
108
109 Research The Effect of Incomplete Death Certificates on Estimates of Unintentional Opioid-Related Overdose Deaths in the United States, Public Health Reports Vol. XX(X) 1-9 ª 2018, Association of Schools and Programs of Public Health All rights reserved. Reprints and permission: sagepub.com/journalspermissions.nav DOI: / journals.sagepub.com/home/phr Jeanine M. Buchanich, PhD, MEd 1, Lauren C. Balmert, PhD 2, Karl E. Williams, MD, MPH 3, and Donald S. Burke, MD 4 Abstract Objectives: A complete and accurate count of the number of opioid-related overdose deaths is essential to properly allocate resources. We determined the rate of unintentional overdose deaths (non opioid-related, opioid-related, or unspecified) in the United States and by state from 1999 to 2015 and the possible effects of underreporting on national estimates of opioid abuse. Methods: We abstracted unintentional drug overdose deaths (International Classification of Diseases, 10th Revision, codes X40-X44) with contributory drug-specific T codes (T36.0-T50.9) from the Mortality Multiple Cause Micro-Data Files. We assumed that the proportion of unspecified overdose deaths that might be attributed to opioids would be the same as the proportion of opioid-related overdose deaths among all overdose deaths and calculated the number of deaths that could be reallocated as opioid-related for each state and year. We then added these reallocated deaths to the reported deaths to determine their potential effect on total opioid-related deaths. Results: From 1999 to 2015, a total of people died from unintentional drug overdoses. Opioid-related overdose deaths rose 401% (from 5868 to ), non opioid-related overdose deaths rose 150% (from 3005 to 7505), and unspecified overdose deaths rose 220% (from 2255 to ). In 5 states (Alabama, Indiana, Louisiana, Mississippi, and Pennsylvania), more than 35% of unintentional overdose deaths were coded as unspecified. Our reallocation resulted in classifying more than unspecified overdose deaths as potential additional opioid-related overdose deaths. Conclusions: States may be greatly underestimating the effect of opioid-related overdose deaths because of incomplete cause-of-death reporting, indicating that the current opioid overdose epidemic may be worse than it appears. Keywords death, drug overdose, death certificates, epidemics, opioids The recent increase in overdose deaths in the United States is well documented. 1-3 This increase has been attributed to opioids, both prescription opioid pain relievers and heroin. 1 For example, in 2010, opioid pain relievers were reported in 75% of overdose deaths involving a medicinal drug. 4 Although 28 states reported that heroin deaths doubled from 1779in2010to3635in2012,duringthatsameperiod,the same 28 states reported that deaths from opioid pain relievers decreased 6.6%, from to From 2013 to 2014, deaths from opioid pain relievers increased 9%, deaths from heroin increased 26%, and deaths from synthetic opioid pain relievers increased 80%. 6 Data from 2015 suggest that rates continue to rise, 7 with 63% of overdose deaths involving an opioid. 6 1 Department of Biostatistics, Graduate School of Public Health, University of Pittsburgh, Pittsburgh, PA, USA 2 Department of Preventive Medicine, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA 3 Office of the Medical Examiner of Allegheny County, Pittsburgh, PA, USA 4 Graduate School of Public Health, University of Pittsburgh, Pittsburgh, PA, USA Corresponding Author: Jeanine M. Buchanich, PhD, MEd, University of Pittsburgh, Graduate School of Public Health, Department of Biostatistics, 7124 Public Health, 130 DeSoto St, Pittsburgh, PA 15261, USA. jeanine@pitt.edu
110 2 Public Health Reports XX(X) In the United States, cause-of-death codes are assigned by the National Center for Health Statistics in accordance with international rules set forth by the World Health Organization. 8 Since 1999, the International Classification of Diseases, 10th Revision (ICD-10) has been used to classify causes of death. Unintentional drug poisoning or overdose deaths are assigned an underlying ICD-10 code of X40-X44. Drug-specific overdose deaths are identified by the contributory causes of death indicated by T codes. Drug-specific T codes are assigned as contributory causes based on the drugs recorded by the coroner or medical examiner completing the death certificate. The drug-specific contributory causes of death are assigned ICD-10 codes of T36.0-T50.9 ( poisoning by drugs, medicaments and biological substances ). Within these codes, non-opioid drugs (eg, cocaine and benzodiazepines) are coded as T36.0-T39.9, T40.5, or T40.7-T50.8. Opioidrelated deaths are coded as T40.0-T40.4 and T40.6: T40.0: opium T40.1: heroin T40.2: other opioids (ie, opioid pain relievers) T40.3: methadone T40.4: other synthetic narcotics (eg, fentanyl) T40.6: other and unspecified narcotics Code T50.9 ( other and unspecified drugs, medicaments and biological substances ) can be combined with other T codes to indicate drugs that do not have specific codes (eg, bath salts) or used alone to indicate that no drug was reported on the death certificate. When the death is classified only by the drug-related T code T50.9 (meaning a drug is not specified), the missing information on drug types leads to underestimating deaths from specific drugs, such as opioid-related deaths. 9,10 This underreporting problem has been addressed by the Council of State and Territorial Epidemiologists, which has advocated for more accurate drug reporting on death certificates, 11 and by the American College of Medical Toxicology and the National Association of Medical Examiners, which also have recommended listing all responsible and contributing substances on death certificates. 12 We sought to determine the proportion of unintentional overdose deaths coded as unspecified (ie, codes X40-X44: drug overdose deaths containing only ICD-10 code T50.9 as the contributory cause of death) and the extent to which this code likely underreports opioid-related, unintentional overdose deaths nationally and by state from 1999 through Methods We abstracted data on deaths using ICD-10 codes by state and year ( ) from the Mortality Multiple Cause Data Files of the National Vital Statistics System of the National Center for Health Statistics. 13 Each record in the micro-data files is based on information abstracted from death certificates filed in vital statistics offices of each state and the District of Columbia. We abstracted data on overdose deaths (ICD-10 codes X40-X44 for unintentional drug overdose), along with all of the contributory cause-of-death T codes for each death. We did not include drug overdose deaths with other intents, including intentional self-harm (suicide, X60-X64), assault (homicide, X85), and undetermined intent (Y10-Y14). We categorized overdose deaths as opioid-related if they contained 1 or more of codes T40.0-T40.4 or T40.6. Opioidrelated deaths could also include non-opioid drugs if both were reported together. We categorized overdose deaths as non opioid-related if they contained 1 or more of codes T36.0-T39.9, T40.5, or T40.7-T50.8 and none of codes T40.0-T40.4 or T40.6. We categorized overdose deaths as unspecified if they were coded only as T50.9 and had no other drug-specific T code (T36.0-T50.8). Generally, unintentional overdose deaths coded only as T50.9 are from unspecified drugs, although code T50.9 has recently been used for deaths involving drugs with no other appropriate T code, such as bath salts. However, this practice would affect only a tiny proportion of deaths evaluated in this study. We counted overdose deaths by state and year. We calculated the percentages of overdose deaths by state and year coded as opioid-related, non opioid-related, and unspecified. We also calculated the change in the percentage of opioid-related overdose deaths and the percentage of unspecified overdose deaths from for each state. We expressed the number of opioid-related unintentional overdose deaths as a proportion of specified drug overdose deaths (any death coded as T30.6-T50.9) by state and year. We multiplied this proportion by the number of unspecified unintentional overdose deaths by state and year and reallocated this proportion as potential additional opioid-related, unintentional overdose deaths. In other words, we assumed that the proportion of unspecified overdose deaths that might be attributed to opioids would be the same as the proportion of opioid-related overdose deaths among all overdose deaths. We calculated actual and reallocated opioid-related unintentional overdose mortality rates by state for We ranked states from highest to lowest by their actual and reallocated opioid-related unintentional overdose mortality rates. We also calculated the changes from the reallocation in rates and ranks. We analyzed data using SAS version Results From 1999 through 2015, a total of people died from an unintentional drug overdose (Table 1). Most opioidrelated overdose deaths were coded as X42, and most unspecified overdose deaths were coded as X44. Of overdose deaths, (58%) were coded as opioidrelated, (20%) were coded as non opioid-related, and (22%) were coded as unspecified. Opioid pain relievers (41.5%) were the most commonly reported, followed by heroin (25.4%), methadone (20.3%), other and unspecified narcotics (14.4%), synthetic opioids other than methadone (14.2%), and opium (0.01%) (categories are not mutually
111 Buchanich et al 3 Table 1. Unintentional drug overdose deaths in the United States, by underlying (X) codes and all combinations of contributory (T) codes, T Codes Present ICD-10 Codes for Unintentional Drug Overdose Deaths Opioid-Related (T40.0-T40.4; T40.6) Non Opioid-Related (T36.0-T39.9; T40.5; T40.7-T50.8) Unspecified (T50.9) X40 a No. (%) X41 b No. (%) X42 c No. (%) X43 d No. (%) X44 e No. (%) Total f No. (%) Yes No No 3 (<0.1) 37 (<0.1) (99.4) 6 (<0.1) 514 (0.5) (100.0) Yes Yes No 25 (<0.1) 248 (0.4) (33.9) 7 (<0.1) (65.6) (100.0) Yes No Yes 1 (<0.1) 26 (<0.1) (89.5) 1 (<0.1) 4663 (10.4) (100.0) Yes Yes Yes 7 (<0.1) 219 (0.4) 9902 (17.7) 10 (<0.1) (81.8) (100.0) No Yes No 2891 (4.7) (31.1) (44.1) 220 (0.4) (19.8) (100.0) No Yes Yes 850 (3.5) 9847 (40.7) 7264 (30.0) 109 (0.5) 6121 (25.3) (100.0) No No Yes 5 (<0.1) 108 (0.1) 422 (0.4) 2 (<0.1) (99.4) (100.0) No No No 36 (11.5) 13 (4.1) 31 (9.9) 3 (1.0) 230 (73.5) 313 (100.0) Total 3818 (0.9) (6.7) (45.6) 358 (0.1) (46.7) (100.0) Abbreviation: ICD-10, International Classification of Diseases, 10th Revision. 8 a Accidental poisoning by and exposure to non-opioid analgesics, antipyretics, and antirheumatics. b Accidental poisoning by and exposure to antiepileptic, sedative-hypnotic, antiparkinsonism, and psychotropic drugs, not elsewhere classified. c Accidental poisoning by and exposure to psychodysleptics (hallucinogens) not elsewhere classified. d Accidental poisoning by and exposure to other drugs acting on the autonomic nervous system. e Accidental poisoning by and exposure to other and unspecified drugs, medicaments, and biological substances. f The subtotal for opioid-related deaths is (58% of total); the subtotal for non opioid-related deaths is (20% of total); the subtotal for unspecified deaths is (22% of total); and the subtotal for deaths with no code is 313 (<0.1% of total). exclusive and could sum to more than 100%). The most common non opioid-related drug codes were for cocaine, psychostimulants with abuse potential, benzodiazepines, and other and unspecified antidepressants. Non opioid-related overdose deaths rose 150%, from 3005 in 1999 to 7505 in 2015, and unspecified overdose deaths rose 220%, from 2255 in 1999 to 7227 in 2015, with a peak in the number of unspecified deaths in 2011 at 8145 (Figure 1). Opioidrelated overdose deaths rose 401% during that period, from 5868 in 1999 to in In 2015, Hawaii had the lowest percentage of opioidrelated overdose deaths (36.0%), and New Hampshire had the highest (97.0%) (Figure 2). The percentage of non opioid-related overdose deaths ranged from 2.4% in New Hampshire to 56.8% in Hawaii. In 5 states, more than 35% of overdose deaths were coded as unspecified (from highest to lowest: Pennsylvania, Louisiana, Alabama, Indiana, and Mississippi), and 17 states had fewer than 5% of overdose deaths coded as unspecified. The District of Columbia had no unspecified overdose deaths, whereas Pennsylvania had the highest unspecified overdose deaths (50.8%). During the study period, the percentage of opioid-related overdose deaths decreased in 9 states (California, Hawaii, Idaho, Montana, Nevada, New Jersey, New Mexico, Oklahoma, and Washington State) and ranged from 0.1% to 16.9%. The percentage of unspecified overdose deaths decreased in 35 states, ranging from 0.2% in Louisiana to 42.2% in North Dakota, and increased in 16 states, ranging from 0.2% in New Mexico to 12.8% in New Jersey. States with a high percentage of unspecified overdose deaths were most affected by reallocation (Figure 3). In total, reallocation reclassified more than unspecified overdose deaths to opioid-related overdose deaths, ranging from 9 in Vermont to in Pennsylvania. The number of opioid-related overdose deaths more than doubled in Alabama, Indiana, Louisiana, Mississippi, and Pennsylvania with reallocation. California, Florida, and Pennsylvania each added more than 5000 opioid-related overdose deaths through reallocation, bringing their totals to , , and , respectively. The state-specific 2015 actual and reallocated opioidrelated unintentional overdose mortality rates in Connecticut, the District of Columbia, New Hampshire, Maine, and Rhode Island changed by less than 1% (Table 2). The rates in Alabama, Indiana, Mississippi, Louisiana, and Pennsylvania increased by more than 50%. Pennsylvania s rate increased 103%, from 9.9 to 20.1 per population. West Virginia ranked highest both before and after reallocation, with opioid-related overdose mortality rates of 31.2 and 31.6 deaths per population, respectively (Table 2). Eight states had no change in rank. The ranks of 17 states increased using the reallocated opioid-related overdose mortality rates, with 4 states moving up at least 10 places (Indiana, Louisiana, New Jersey, and Pennsylvania). Indiana had the largest change in rank, going from 34th to 15th after reallocation. The ranks of 5 states (Oklahoma, South Carolina, Utah, Virginia, and Washington State) decreased by 7 places. South Dakota had the lowest rank both before and after reallocation. Discussion Several reports on rates of opioid-related overdose deaths have used the opioid-related T codes without accounting for deaths in which a specific drug was not reported. 1,5-7 Drugspecific reporting from the use of contributory T codes reflects the effect of specific drugs on mortality more
112 4 Public Health Reports XX(X) 35,000 30,000 Non opioid-related Opioid-related Unspecified 25,000 No. of Deaths 20,000 15,000 10,000 5, Year Figure 1. Unintentional opioid-related and non opioid-related unintentional drug overdose deaths in the United States, , using International Classification of Diseases, 10th Revision (ICD-10) codes X40-X44. 8 accurately than does the overall overdose mortality rate. However, drug-specific overdose death counts are clearly underestimates because death certificates with no drug specified cannot be attributed to a specific drug. Our analyses indicated that potentially more than unspecified, unintentional overdose deaths in the past 17 years, including more than 5600 in 2015, could be categorized as opioidrelated unintentional overdose deaths. However, complete cause-of-death reporting was disproportionate by state. The 5 states with the highest number of reallocated opioid-related overdose deaths (California, Florida, Ohio, Pennsylvania, and Texas) accounted for nearly half (46.4%, of ) of the reallocated unintentional overdose deaths. Alabama, Indiana, Louisiana, Mississippi, and Pennsylvania had much higher rates when overdose death rates were adjusted for lack of specificity. Our findings for states with a high percentage of unspecified overdose deaths are consistent with the findings of previous evaluations. Ruhm 9 corrected opioid- and heroininvolved drug-poisoning death rates for 2014 and found the largest difference between reported and corrected rates in Pennsylvania. For opioid-involved death rates, the next 4 states affected by reallocation were Indiana, Louisiana, Alabama, and Kentucky. For heroin-involved death rates, the next 4 most affected states were Indiana, Louisiana, New Jersey, and Delaware. In our study, with reallocation based on any mention of an opioid, Delaware was the 11th and Kentucky was the 17th most affected state. The absolute change in rate, not the percentage change, would make Kentucky the 5th most affected state. Although Ruhm used a different methodology from ours to reallocate cases and included all intentions (suicide, homicide, and undetermined), the similarity of those findings with ours supports the conclusion that we correctly identified the states in which opioid-related accidental overdoses were most underestimated. 9 Another evaluation by Ruhm 15 found that the largest difference from correcting rates of opioid-involved mortality occurred in 2011 for any opioid and in 2015 for heroin and synthetic opioids. Ruhm recommended imputing drugs on death certificates on which none are reported. Warner et al 10 indicated that states with centralized state medical examiner systems had a higher percentage (92%) of drugs specified than did those with decentralized county coroner systems (62%). Although we determined the percentage of unspecified overdose deaths without regard to the medicolegal death investigation system in a state, we also found that states with a decentralized or hybrid system had a low percentage of overdose deaths from a specified drug. Of the 5 states with the highest percentage of unspecified overdose deaths in our study, 3 had a hybrid coroner medical examiner death investigation system (Alabama, Mississippi, and Pennsylvania), and 2 had a decentralized county coroner system (Indiana and Louisiana). Coroners are less likely than medical examiners to be physicians and do not necessarily
113 Buchanich et al 5 Pennsylvania Louisiana Alabama Indiana Mississippi New Jersey Montana Arkansas Kansas Florida Wyoming Nebraska Delaware Idaho California Kentucky Colorado Arizona Michigan North Dakota Texas Missouri Minnesota Wisconsin South Dakota Alaska Georgia Tennessee Iowa Hawaii Illinois Ohio North Carolina Maryland Washington Nevada Oregon New Mexico New York Oklahoma South Carolina Virginia Utah West Virginia Vermont Massachuse s Maine Connec cut Rhode Island New Hampshire District of Columbia Unspecified Opioid-related Non opioid-related Percentage Figure 2. Percentage of non opioid-related, opioid-related, and unspecified unintentional drug overdose deaths in the United States in 2015, using International Classification of Diseases, 10th Revision (ICD-10) codes T36.0-T39.9 and T40.5-T50.8 (opioid-related), T40.0-T40.4 (non opioid-related), and T50.9 (unspecified). 8 Sum may not equal 100.0%; a small number of X40-X44 deaths had no T36.0-T50.9 code. have the medical training needed to complete drug information for death certificates based on toxicology reports States with a decentralized system, including those with hybrid coroner medical examiner systems, are likely to have less standardization than those with a centralized system, leading to greater variation in reporting accuracy in states with a decentralized system. 10 We examined the percentage of unintentional overdose deaths from unspecified drugs in 2015 and found that states with centralized medical examiner systems (as classified by Warner et al 10 ) had lower percentages of unspecified drugs than did the other 3 systems (decentralized county or district medical examiner, hybrid, or decentralized county coroner), although the differences were not significant. In 2016, the Council of State and Territorial Epidemiologists issued a lessons-learned report from state-specific efforts to improve drug-specific reporting in overdose deaths. 19 States such as Kansas and Kentucky recognized
114 6 Public Health Reports XX(X) Pennsylvania California Florida Ohio Texas Indiana New Jersey Michigan Kentucky Louisiana Alabama Georgia Arizona Tennessee South Carolina Missouri Illinois Colorado Mississippi North Carolina New York Connec cut New Mexico Kansas Wisconsin Minnesota Arkansas Washington Idaho Delaware Virginia Montana Oregon Alaska Massachuse s Oklahoma Nebrasks Maine Wyoming Utah Nevada Maryland West Virginia Iowa Hawaii Rhode Island New Hampshire North Dakota South Dakota District of Columbia Vermont 0 5,000 10,000 15,000 20,000 25,000 30,000 35,000 Number Reallocated opioid-related deaths Reported opioid-related deaths Figure 3. Reallocated and reported opioid-related unintentional drug overdose deaths in the United States, The numbers of reallocated opioid-related unintentional overdose deaths were estimated by reallocating such deaths from unspecified drugs according to the number of known opioid-related overdose deaths as a percentage of all unintentional drug overdose deaths during the same period.
115 Buchanich et al 7 Table 2. Reported and reallocated mortality rates from opioid-related unintentional drug overdose, by state, 2015 a State No. of Reported Opioid- Related Deaths Opioid-Related Death Rate per Population Rate Rank No. of Reallocated Opioid-Related Deaths Opioid-Related Death Rate per Population Reallocated Rate Rank % Change in Rate Change in Rank Alabama Alaska Arizona Arkansas California Colorado Connecticut Delaware District of Columbia Florida Georgia Hawaii Idaho Illinois Indiana Iowa Kansas Kentucky Louisiana Maine Maryland Massachusetts Michigan Minnesota Mississippi Missouri Montana Nebraska Nevada New Hampshire New Jersey New Mexico New York North Carolina North Dakota Ohio Oklahoma Oregon Pennsylvania Rhode Island South Carolina South Dakota Tennessee Texas Utah Vermont Virginia Washington West Virginia Wisconsin Wyoming a Reallocated rates were calculated assuming the proportion of reported opioid-related unintentional overdose deaths of all unintentional overdose deaths would estimate the proportion of unspecified overdose deaths that could be attributed to opioids.
116 8 Public Health Reports XX(X) that the lack of drug specificity in reporting overdose deaths prevents understanding the extent of the epidemic and may inhibit effective public health interventions. The report described extensive efforts by Kentucky to improve reporting. We found that from 1999 through 2015, the percentage of opioid-related drug codes in Kentucky increased 43%, whereas unspecified drug reporting decreased 28%, suggesting that state-based efforts can improve the accuracy of drugspecific reporting for overdose deaths. When we assessed the differences in the percentage of unspecified drug reporting on overdose mortality statistics for 11 states using 2010 data, we found the most variation and therefore the greatest potential to improve reporting in Kansas, Kentucky, and Michigan. 11 Using 2015 data, Kentucky and Michigan were still in the top 10 states with the most variability, but Kansas was not. However, several other states, including Pennsylvania, had greater differences than Kentucky or Michigan. Our analysis emphasizes the importance of reporting complete drug information on overdose deaths. However, the ICD- 10 has a set number of codes for drug classes. Overdoses are now being attributed to new drugs, such as fentanyl analogs, but the drug class codes have not changed (eg, acryl fentanyl would be coded as T40.4), meaning that even with complete drug reporting, death certificates lose some drug specificity during the coding process. The development of ICD-11 (currently planned for release in 2018) may help, but accurately capturing the effect on overdose mortality of designer drugs may continue to be problematic. In addition, coroners and medical examiners may not be able to accurately test for and identify newly developing synthetic opioids and other designer drugs in toxicological tests, meaning that these drugs will not be recorded on the death certificate. National Association of Medical Examiners expert panel recommend classifying opioid-related overdose deaths without an indication of self-harm as accidental deaths, specifically stating, assigning undetermined as the manner of death as a matter of course for deaths due to intoxication does not serve the public good, nor does this practice support efforts to intervene and prevent future intoxication deaths of a similar sort. 12 However, the proportion of drug-related deaths coded as undetermined varies by state. 20 States with a higher proportion of undetermined deaths would have been less affected by our reallocation calculations. Identifying locations where residents are at high risk for opioid-related overdose death relies on having complete and accurate information about the types of drugs involved. Our findings indicate that incompletely reported unspecified deaths could have a substantial effect on the opioid-related, unintentional overdose mortality rates by state. Proper allocation of resources for the opioid epidemic depends on understanding the magnitude of the problem, and incomplete death certificate reporting prevents lawmakers, treatment specialists, and public health officials from doing so. States differ widely in the completeness of overdose mortality reporting, making it difficult to identify communities most at risk. However, variation within states by county or parish is also likely, especially in states with decentralized or hybrid death investigation systems. Warner et al 10 noted that smaller counties might perceive or experience more barriers to toxicological services to determine the types of drugs involved. Future research needs to identify which factors (eg, decedent age, race, or sex) influence whether an unintentional overdose death is reported as unspecified in various regions. Strengths and Weaknesses We made several assumptions in these analyses, primarily that the proportion of reported opioid-related overdose deaths to all unintentional drug overdose deaths would be the same in all unspecified drug-related overdose deaths by state by year. We know that these data are state-specific and can change over time, but this rather strong assumption should be explored further by comparing characteristics and patterns of the deaths, such as age, race, sex, and geography, with and without specific drugs reported. We also assumed that no bias in death certificate reporting existed (ie, that coroners and medical examiners reported drug information for each death in their jurisdiction in the same way). However, drug reporting could be affected by the extent to which toxicological testing was conducted: by post-mortem distribution, or the shift in detectable drug concentrations after a person dies; by coroner or medical examiner experience; and by the size of their jurisdiction. 10 This assumption could be evaluated more fully by comparing the completeness of reporting within jurisdictions. We examined only unintentional or accidental overdoses. The American College of Medical Toxicology and the Conclusions States may be markedly underestimating the effect of opioidrelated overdose deaths because of incomplete cause-of-death reporting. Potentially opioid-related, unintentional overdose deaths from 1999 through 2015 have been missed because of incomplete reporting, indicating that the opioid overdose epidemic may be worse than it appears. Declaration of Conflicting Interests The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Funding The authors received no financial support for the research, authorship, and/or publication of this article. References 1. Chen LH, Hedegaard H, Warner M. Quickstats: rates of deaths from drug poisoning and drug poisoning involving opioid analgesics United States, MMWR Morb Mortal Wkly Rep. 2015;64(1):32.
117 Buchanich et al 9 2. Warner M, Chen LH, Makuc DM, Anderson RN, Minino AM. Drug poisoning deaths in the United States, NCHS Data Brief. 2011;81: Buchanich JM, Balmert LC, Pringle JL, Williams KE, Burke DS, Marsh GM. Patterns and trends in accidental poisoning death rates in the US, Prev Med. 2016;89: Jones CM, Mack KA, Paulozzi LJ. Pharmaceutical overdose deaths, United States, JAMA. 2013;309(7): Rudd RA, Paulozzi LJ, Bauer MJ, et al. Increases in heroin overdose deaths 28 states, 2010 to MMWR Morb Mortal Wkly Rep. 2014;63(39): Rudd RA, Aleshire N, Zibbell JE, Gladden RM. Increases in drug and opioid overdose deaths United States, MMWR Morb Mortal Wkly Rep. 2016;64(50-51): Hedegaard H, Warner M, Miniño AM. Drug overdose deaths in the United States, NCHS Data Brief. 2017;273: World Health Organization. International Statistical Classification of Diseases and Related Health Problems. Geneva: World Health Organization; Ruhm CJ. Drug poisoning deaths in the United States, : a statistical adjustment analysis. Popul Health Metrics. 2016;14: Warner M, Paulozzi LJ, Nolte KB, Davis GG, Nelson LS. State variation in certifying manner of death and drugs involved in drug intoxication deaths. Acad Forensic Pathol. 2013;2: Slavova S, O Brien DB, Creppage K, et al. Drug overdose deaths: let s get specific. Public Health Rep. 2015;130(4): Davis GG. National Association of Medical Examiners and American College of Medical Toxicology Expert Panel on Evaluating and Reporting Opioid Deaths. Complete republication: National Association of Medical Examiners position paper: recommendations for the investigation, diagnosis, and certification of deaths related to opioid drugs. J Med Toxicol. 2014;10(1): National Center for Health Statistics. Mortality Multiple Cause Data Files. Atlanta, GA: Centers for Disease Control and Prevention, US Department of Health and Human Services; SAS Institute, Inc. SAS/STAT Version 9.4. Cary, NC: SAS Institute, Inc; Ruhm CJ. Corrected US opioid-involved drug poisoning deaths and mortality rates, [published online February 12, 2018]. Addiction. doi: /add Committee for the Workshop on the Medicolegal Death Investigation System. Medicolegal Death Investigation System: Workshop Summary. Washington, DC: National Academies Press; Hanzlick R. Medical examiners, coroners, and public health: a review and update. Arch Pathol Lab Med. 2006;130(9): Committee on Identifying the Needs of the Forensic Sciences Community, National Research Council. Strengthening Forensic Science in the United States: A Path Forward. Washington, DC: National Academies Press; Sabel JC, Poel A, Tuazon E, et al. Recommendations and Lessons Learned for Improved Reporting of Drug Overdose Deaths on Death Certificates. Atlanta, GA: Council of State and Territorial Epidemiologists; sites/ FINAL-Drug_Overdos.pdf. Accessed March 2, Breidling MJ, Wiersema B. Variability of undetermined manner of death classification in the US. Inj Prev. 2006; 12(suppl 2):ii49-ii54.
118
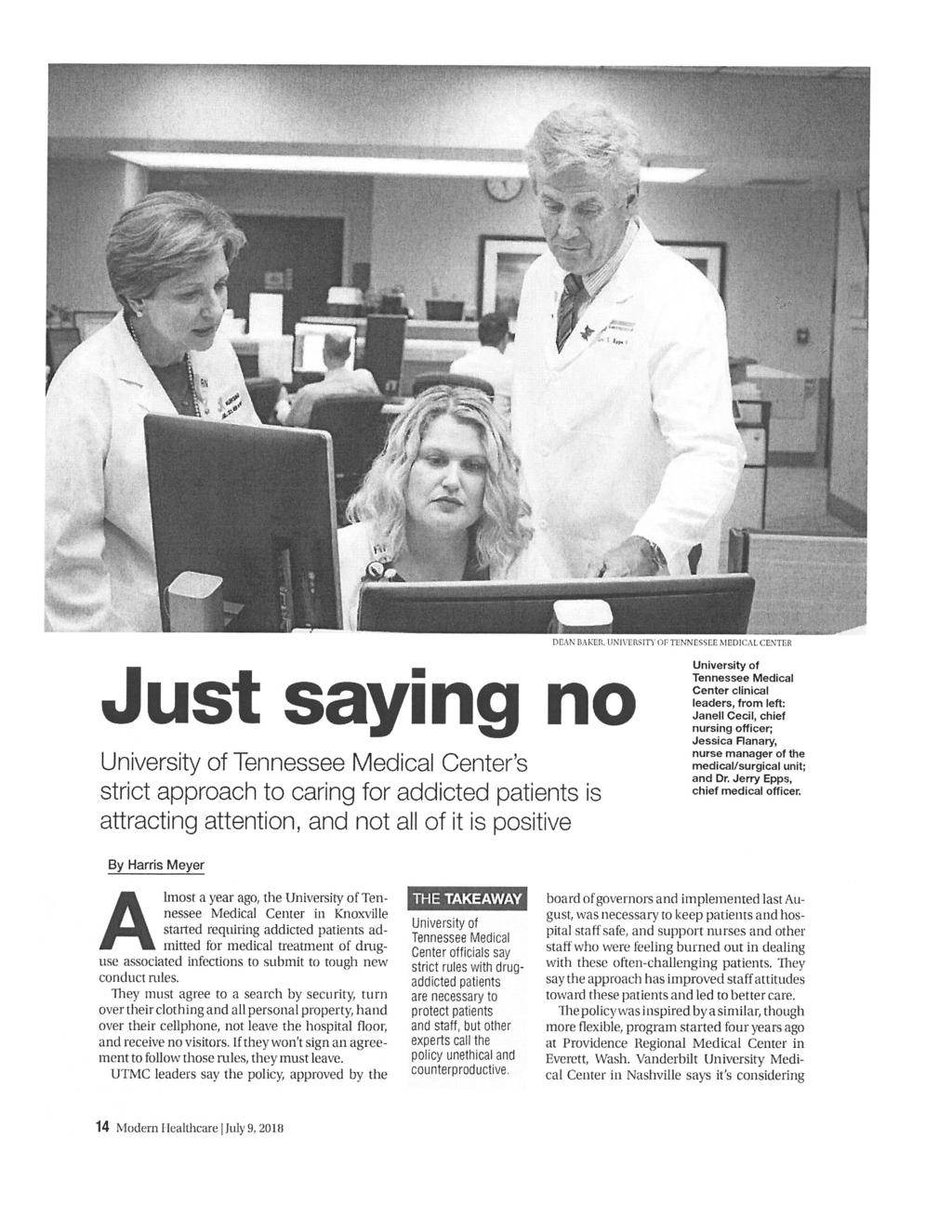
119

120

121

122
CHAPTER Committee Substitute for Committee Substitute for Senate Bill No. 2760
 CHAPTER 2008-64 Committee Substitute for Committee Substitute for Senate Bill No. 2760 An act relating to dentistry; amending s. 466.003, F.S.; providing a definition; amending s. 466.006, F.S.; revising
CHAPTER 2008-64 Committee Substitute for Committee Substitute for Senate Bill No. 2760 An act relating to dentistry; amending s. 466.003, F.S.; providing a definition; amending s. 466.006, F.S.; revising
For An Act To Be Entitled. Subtitle
 0 0 State of Arkansas INTERIM STUDY PROPOSAL 0-0th General Assembly A Bill DRAFT JMB/JMB Second Extraordinary Session, 0 SENATE BILL By: Senator J. Hutchinson Filed with: Arkansas Legislative Council pursuant
0 0 State of Arkansas INTERIM STUDY PROPOSAL 0-0th General Assembly A Bill DRAFT JMB/JMB Second Extraordinary Session, 0 SENATE BILL By: Senator J. Hutchinson Filed with: Arkansas Legislative Council pursuant
A Bill Regular Session, 2017 HOUSE BILL 1250
 Stricken language would be deleted from and underlined language would be added to present law. 0 State of Arkansas st General Assembly As Engrossed: H// S// A Bill Regular Session, HOUSE BILL 0 By: Representative
Stricken language would be deleted from and underlined language would be added to present law. 0 State of Arkansas st General Assembly As Engrossed: H// S// A Bill Regular Session, HOUSE BILL 0 By: Representative
California Comprehensive Addiction Recovery Act; Physical Capacity Expansion for Addiction Treatment
 California Comprehensive Addiction Recovery Act; Physical Capacity Expansion for Addiction Treatment (a) The Legislature finds and declares all of the following: 1. There are only 25 hospitals in California
California Comprehensive Addiction Recovery Act; Physical Capacity Expansion for Addiction Treatment (a) The Legislature finds and declares all of the following: 1. There are only 25 hospitals in California
SENATE, No STATE OF NEW JERSEY. 217th LEGISLATURE INTRODUCED FEBRUARY 8, 2016
 SENATE, No. STATE OF NEW JERSEY th LEGISLATURE INTRODUCED FEBRUARY, 0 Sponsored by: Senator JOSEPH F. VITALE District (Middlesex) SYNOPSIS Makes it a crime of the third degree to practice psychology without
SENATE, No. STATE OF NEW JERSEY th LEGISLATURE INTRODUCED FEBRUARY, 0 Sponsored by: Senator JOSEPH F. VITALE District (Middlesex) SYNOPSIS Makes it a crime of the third degree to practice psychology without
SENATE BILL No. 501 AMENDED IN SENATE MAY 1, 2017 AMENDED IN SENATE APRIL 20, 2017 AMENDED IN SENATE APRIL 17, Introduced by Senator Glazer
 AMENDED IN SENATE MAY 1, 2017 AMENDED IN SENATE APRIL 20, 2017 AMENDED IN SENATE APRIL 17, 2017 SENATE BILL No. 501 Introduced by Senator Glazer February 16, 2017 An act to amend Sections 1601.4, 1646,
AMENDED IN SENATE MAY 1, 2017 AMENDED IN SENATE APRIL 20, 2017 AMENDED IN SENATE APRIL 17, 2017 SENATE BILL No. 501 Introduced by Senator Glazer February 16, 2017 An act to amend Sections 1601.4, 1646,
AS AMENDED A BILL WHEREAS, WHEREAS WHEREAS, WHEREAS, WHEREAS WHEREAS, WHEREAS,
 1 1 0 1 0 1 BY AUTHORITY ORDINANCE NO. COUNCIL BILL NO. CB-01 SERIES OF 0 COMMITTEE OF REFERENCE: AS AMENDED 0-1- Special Issues: Marijuana Moratorium A BILL For an ordinance concerning the licensing of
1 1 0 1 0 1 BY AUTHORITY ORDINANCE NO. COUNCIL BILL NO. CB-01 SERIES OF 0 COMMITTEE OF REFERENCE: AS AMENDED 0-1- Special Issues: Marijuana Moratorium A BILL For an ordinance concerning the licensing of
CHAPTER Committee Substitute for Committee Substitute for Senate Bill No. 1030
 CHAPTER 2014-157 Committee Substitute for Committee Substitute for Senate Bill No. 1030 An act relating to cannabis; providing a short title; creating s. 381.986, F.S.; defining terms; authorizing specified
CHAPTER 2014-157 Committee Substitute for Committee Substitute for Senate Bill No. 1030 An act relating to cannabis; providing a short title; creating s. 381.986, F.S.; defining terms; authorizing specified
DRUG FREE WORKPLACE POLICY
 GENERAL STATEMENT DRUG FREE WORKPLACE POLICY Kitsap County Government is obligated and committed to provide our employees and the citizens of Kitsap County with an alcohol and drug free, healthy, safe,
GENERAL STATEMENT DRUG FREE WORKPLACE POLICY Kitsap County Government is obligated and committed to provide our employees and the citizens of Kitsap County with an alcohol and drug free, healthy, safe,
Legislative Bill Watch As of Thursday March, 13, 2014
 Passed Bills Legislative Bill Watch As of Thursday March, 13, 2014 Bill Number and Title Bill Sponsors Summary Status HB 11 Overdose Reporting HB 23 Suicide Prevention Revisions H.B. 38 Second Substitute
Passed Bills Legislative Bill Watch As of Thursday March, 13, 2014 Bill Number and Title Bill Sponsors Summary Status HB 11 Overdose Reporting HB 23 Suicide Prevention Revisions H.B. 38 Second Substitute
SOUTH DAKOTA BOARD OF REGENTS. Policy Manual
 SUBJECT: Drug Free Environment NUMBER: 4:27 SOUTH DAKOTA BOARD OF REGENTS Policy Manual Drug Free Workplace Policy The South Dakota Board of Regents is committed to providing a drug free workplace. Additional
SUBJECT: Drug Free Environment NUMBER: 4:27 SOUTH DAKOTA BOARD OF REGENTS Policy Manual Drug Free Workplace Policy The South Dakota Board of Regents is committed to providing a drug free workplace. Additional
RESIDENTIAL SERVICE PROTECTION FUND
 RESIDENTIAL SERVICE PROTECTION FUND 759.685 Surcharge assessed on retail telecommunications subscribers; rules. (1)(a) In order to fund the programs provided in sections 2 to 6, chapter 290, Oregon Laws
RESIDENTIAL SERVICE PROTECTION FUND 759.685 Surcharge assessed on retail telecommunications subscribers; rules. (1)(a) In order to fund the programs provided in sections 2 to 6, chapter 290, Oregon Laws
Florida Senate SB 446
 By Senator Hays 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 A bill to be entitled An act relating to dentistry and dental hygiene; amending s. 466.003, F.S.; revising
By Senator Hays 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 A bill to be entitled An act relating to dentistry and dental hygiene; amending s. 466.003, F.S.; revising
Senate Bill No. 481 Committee on Health and Human Services
 Senate Bill No. 481 Committee on Health and Human Services CHAPTER... AN ACT relating to disabilities; transforming the Subcommittee on Communication Services for Persons Who Are Deaf or Hard of Hearing
Senate Bill No. 481 Committee on Health and Human Services CHAPTER... AN ACT relating to disabilities; transforming the Subcommittee on Communication Services for Persons Who Are Deaf or Hard of Hearing
ASSEMBLY COMMITTEE ON HUMAN SERVICES Blanca Rubio, Chair AB 2702 (McCarty) As Amended April 2, 2018
 As Amended April 2, 2018") Page 1 Date of Hearing: April 24, 2018 SUBJECT: Trustline registry. ASSEMBLY COMMITTEE ON HUMAN SERVICES Blanca Rubio, Chair AB 2702 (McCarty) As Amended April 2, 2018 SUMMARY: Requires the Department
Page 1 Date of Hearing: April 24, 2018 SUBJECT: Trustline registry. ASSEMBLY COMMITTEE ON HUMAN SERVICES Blanca Rubio, Chair AB 2702 (McCarty) As Amended April 2, 2018 SUMMARY: Requires the Department
Legislative Counsel s Digest:
 Senate Bill No. 250 Senator Carlton (by request) CHAPTER... AN ACT relating to dentistry and dental hygiene; revising various provisions governing the qualifications, examination and licensure of dentists
Senate Bill No. 250 Senator Carlton (by request) CHAPTER... AN ACT relating to dentistry and dental hygiene; revising various provisions governing the qualifications, examination and licensure of dentists
ENROLLED 2014 Legislature CS for CS for SB 1030, 1st Engrossed
 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 An act relating to cannabis; providing a short title; creating s. 381.986, F.S.; defining terms; authorizing specified physicians
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 An act relating to cannabis; providing a short title; creating s. 381.986, F.S.; defining terms; authorizing specified physicians
Act 443 of 2009 House Bill 1379
 Act 443 of 2009 House Bill 1379 AN ACT TO PROVIDE FOR THE LICENSURE OF ALCOHOLISM AND DRUG ABUSE COUNSELORS; TO PROVIDE FOR THE REGISTRATION OF CLINICAL ALCOHOLISM AND DRUG ABUSE COUNSELOR SUPERVISORS;
Act 443 of 2009 House Bill 1379 AN ACT TO PROVIDE FOR THE LICENSURE OF ALCOHOLISM AND DRUG ABUSE COUNSELORS; TO PROVIDE FOR THE REGISTRATION OF CLINICAL ALCOHOLISM AND DRUG ABUSE COUNSELOR SUPERVISORS;
ASSEMBLY, No STATE OF NEW JERSEY. 216th LEGISLATURE INTRODUCED MAY 15, 2014
 ASSEMBLY, No. STATE OF NEW JERSEY th LEGISLATURE INTRODUCED MAY, 0 Sponsored by: Assemblyman RONALD S. DANCER District (Burlington, Middlesex, Monmouth and Ocean) Assemblyman HERB CONAWAY, JR. District
ASSEMBLY, No. STATE OF NEW JERSEY th LEGISLATURE INTRODUCED MAY, 0 Sponsored by: Assemblyman RONALD S. DANCER District (Burlington, Middlesex, Monmouth and Ocean) Assemblyman HERB CONAWAY, JR. District
The State of Maryland Executive Department
 The State of Maryland Executive Department Executive Order 01.01.1991.16 State of Maryland Substance Abuse Policy WHEREAS, Substance abuse is a serious national crisis which has had a detrimental effect
The State of Maryland Executive Department Executive Order 01.01.1991.16 State of Maryland Substance Abuse Policy WHEREAS, Substance abuse is a serious national crisis which has had a detrimental effect
LAWS OF ALASKA AN ACT
 LAWS OF ALASKA 01 Source HCS SB (RLS) am H Chapter No. AN ACT Requiring insurance coverage for autism spectrum disorders, describing the method for establishing a covered treatment plan for those disorders,
LAWS OF ALASKA 01 Source HCS SB (RLS) am H Chapter No. AN ACT Requiring insurance coverage for autism spectrum disorders, describing the method for establishing a covered treatment plan for those disorders,
Human Resources All Personnel BP 4020 DRUG AND ALCOHOL-FREE WORKPLACE
 BP 4020 DRUG AND ALCOHOL-FREE WORKPLACE The Governing Board believes that the maintenance of drug and alcohol-free workplaces is essential to school and district operations. No employee shall unlawfully
BP 4020 DRUG AND ALCOHOL-FREE WORKPLACE The Governing Board believes that the maintenance of drug and alcohol-free workplaces is essential to school and district operations. No employee shall unlawfully
No An act relating to health insurance coverage for early childhood developmental disorders, including autism spectrum disorders. (S.
 No. 158. An act relating to health insurance coverage for early childhood developmental disorders, including autism spectrum disorders. (S.223) It is hereby enacted by the General Assembly of the State
No. 158. An act relating to health insurance coverage for early childhood developmental disorders, including autism spectrum disorders. (S.223) It is hereby enacted by the General Assembly of the State
NC General Statutes - Chapter 90 Article 16 1
 Article 16. Dental Hygiene Act. 90-221. Definitions. (a) "Dental hygiene" as used in this Article shall mean the performance of the following functions: Complete oral prophylaxis, application of preventive
Article 16. Dental Hygiene Act. 90-221. Definitions. (a) "Dental hygiene" as used in this Article shall mean the performance of the following functions: Complete oral prophylaxis, application of preventive
House Bill 2198 Ordered by the House July 1 Including House Amendments dated June 2 and July 1
 th OREGON LEGISLATIVE ASSEMBLY--0 Regular Session (Including Amendments to Resolve Conflicts) B-Engrossed House Bill Ordered by the House July Including House Amendments dated June and July Introduced
th OREGON LEGISLATIVE ASSEMBLY--0 Regular Session (Including Amendments to Resolve Conflicts) B-Engrossed House Bill Ordered by the House July Including House Amendments dated June and July Introduced
POLICY ON SUBSTANCE ABUSE FOR FACULTY, STAFF, AND STUDENTS
 University Policies and Procedures 07-01.10 POLICY ON SUBSTANCE ABUSE FOR FACULTY, STAFF, AND STUDENTS I. Policy Statement: The use of controlled substances and the abuse of alcohol present a serious threat
University Policies and Procedures 07-01.10 POLICY ON SUBSTANCE ABUSE FOR FACULTY, STAFF, AND STUDENTS I. Policy Statement: The use of controlled substances and the abuse of alcohol present a serious threat
SENATE, No. 359 STATE OF NEW JERSEY. 217th LEGISLATURE PRE-FILED FOR INTRODUCTION IN THE 2016 SESSION
 SENATE, No. STATE OF NEW JERSEY th LEGISLATURE PRE-FILED FOR INTRODUCTION IN THE 0 SESSION Sponsored by: Senator RICHARD J. CODEY District (Essex and Morris) Senator JOSEPH F. VITALE District (Middlesex)
SENATE, No. STATE OF NEW JERSEY th LEGISLATURE PRE-FILED FOR INTRODUCTION IN THE 0 SESSION Sponsored by: Senator RICHARD J. CODEY District (Essex and Morris) Senator JOSEPH F. VITALE District (Middlesex)
Substance Abuse Policy. Substance Abuse Policy for Employees and Students
 College Rules and Regulations 2.2008.1 Substance Abuse Policy Substance Abuse Policy for Employees and Students I. Substance Abuse Policy for Employees and Students A. Purpose The County College of Morris
College Rules and Regulations 2.2008.1 Substance Abuse Policy Substance Abuse Policy for Employees and Students I. Substance Abuse Policy for Employees and Students A. Purpose The County College of Morris
CHAPTER Section 3 of P.L.1983, c.296 (C.45: ) is amended to read as follows:
 is amended to read as follows:") CHAPTER 121 AN ACT concerning the practice of physical therapy, amending P.L.2003, c.18, and amending and supplementing P.L.1983, c.296. BE IT ENACTED by the Senate and General Assembly of the State of
CHAPTER 121 AN ACT concerning the practice of physical therapy, amending P.L.2003, c.18, and amending and supplementing P.L.1983, c.296. BE IT ENACTED by the Senate and General Assembly of the State of
WHEREAS, the Tennessee General Assembly finds that thousands of Tennesseans are
 AN ACT to license sign language interpreters WHEREAS, the Tennessee General Assembly finds that thousands of Tennesseans are individuals who are Deaf, Deaf-Blind, or Hard of Hearing; and WHEREAS, the General
AN ACT to license sign language interpreters WHEREAS, the Tennessee General Assembly finds that thousands of Tennesseans are individuals who are Deaf, Deaf-Blind, or Hard of Hearing; and WHEREAS, the General
[CORRECTED COPY] CHAPTER 115
![[CORRECTED COPY] CHAPTER 115](/thumbs/90/102852289.jpg "[CORRECTED COPY] CHAPTER 115") [CORRECTED COPY] CHAPTER 115 AN ACT concerning the practice of optometry and revising parts of the statutory law. BE IT ENACTED by the Senate and General Assembly of the State of New Jersey: 1. R.S.45:12-1
[CORRECTED COPY] CHAPTER 115 AN ACT concerning the practice of optometry and revising parts of the statutory law. BE IT ENACTED by the Senate and General Assembly of the State of New Jersey: 1. R.S.45:12-1
79th OREGON LEGISLATIVE ASSEMBLY Regular Session. Enrolled. House Bill 2198
 79th OREGON LEGISLATIVE ASSEMBLY--2017 Regular Session Enrolled House Bill 2198 Introduced and printed pursuant to House Rule 12.00. Presession filed (at the request of Joint Interim Committee on Marijuana
79th OREGON LEGISLATIVE ASSEMBLY--2017 Regular Session Enrolled House Bill 2198 Introduced and printed pursuant to House Rule 12.00. Presession filed (at the request of Joint Interim Committee on Marijuana
Report No May 2016
 Report No. 15-08 May 2016 Office of the Inspector General Internal Audit Background Screening Clearinghouse Program EXECUTIVE SUMMARY As part of the Agency for Health Care Administration (Agency) fiscal
Report No. 15-08 May 2016 Office of the Inspector General Internal Audit Background Screening Clearinghouse Program EXECUTIVE SUMMARY As part of the Agency for Health Care Administration (Agency) fiscal
STAFF REPORT City of Lancaster NB 2
 STAFF REPORT City of Lancaster NB 2 12/13/16 MVB Date: December 13, 2016 To: From: Subject: Mayor Parris and City Council Members Mark V. Bozigian, City Manager Allison E. Burns, City Attorney Ordinance
STAFF REPORT City of Lancaster NB 2 12/13/16 MVB Date: December 13, 2016 To: From: Subject: Mayor Parris and City Council Members Mark V. Bozigian, City Manager Allison E. Burns, City Attorney Ordinance
16 SB 319/AP. Senate Bill 319 By: Senators Jackson of the 2nd, Kirk of the 13th, Unterman of the 45th, Henson of the 41st and Orrock of the 36 th
 1 2 3 4 5 6 7 8 9 10 11 12 13 Senate Bill 319 By: Senators Jackson of the 2nd, Kirk of the 13th, Unterman of the 45th, Henson of the 41st and Orrock of the 36 th AS PASSED A BILL TO BE ENTITLED AN ACT
1 2 3 4 5 6 7 8 9 10 11 12 13 Senate Bill 319 By: Senators Jackson of the 2nd, Kirk of the 13th, Unterman of the 45th, Henson of the 41st and Orrock of the 36 th AS PASSED A BILL TO BE ENTITLED AN ACT
TEXAS COMPASSIONATE-USE ACT
 Ch. 301, 1 MEDICAL USE OF LOW-THC CANNABIS AND THE REGULATION OF RELATED ORGANIZATIONS AND INDIVIDUALS; REQUIRING A DISPENSING ORGANIZATION TO OBTAIN A LICENSE TO DISPENSE LOW-THC CANNABIS AND ANY EMPLOYEE
Ch. 301, 1 MEDICAL USE OF LOW-THC CANNABIS AND THE REGULATION OF RELATED ORGANIZATIONS AND INDIVIDUALS; REQUIRING A DISPENSING ORGANIZATION TO OBTAIN A LICENSE TO DISPENSE LOW-THC CANNABIS AND ANY EMPLOYEE
FL AT Act As amended 5/30/06 by Chapter (SB 366) (Amendments not noted; see SB 366 file for changes) PART XIII ATHLETIC TRAINERS
 (Amendments not noted; see SB 366 file for changes) PART XIII ATHLETIC TRAINERS") FL AT Act As amended 5/30/06 by Chapter 2006-39 (SB 366) (Amendments not noted; see SB 366 file for changes) PART XIII ATHLETIC TRAINERS 468.70 Legislative intent.--it is the intent of the Legislature
FL AT Act As amended 5/30/06 by Chapter 2006-39 (SB 366) (Amendments not noted; see SB 366 file for changes) PART XIII ATHLETIC TRAINERS 468.70 Legislative intent.--it is the intent of the Legislature
OREGON MEDICAL MARIJUANA ACT
 OREGON MEDICAL MARIJUANA ACT 475.300 Findings. The people of the state of Oregon hereby find that: (1) Patients and doctors have found marijuana to be an effective treatment for suffering caused by debilitating
OREGON MEDICAL MARIJUANA ACT 475.300 Findings. The people of the state of Oregon hereby find that: (1) Patients and doctors have found marijuana to be an effective treatment for suffering caused by debilitating
Title 32: PROFESSIONS AND OCCUPATIONS
 Title 32: PROFESSIONS AND OCCUPATIONS Chapter 45-A: PHYSICAL THERAPIST PRACTICE ACT Table of Contents Section 3111. DEFINITIONS... 3 Section 3111-A. SCOPE OF PRACTICE... 3 Section 3112. BOARD CREATED;
Title 32: PROFESSIONS AND OCCUPATIONS Chapter 45-A: PHYSICAL THERAPIST PRACTICE ACT Table of Contents Section 3111. DEFINITIONS... 3 Section 3111-A. SCOPE OF PRACTICE... 3 Section 3112. BOARD CREATED;
UNOFFICIAL COPY OF HOUSE BILL 1329 A BILL ENTITLED
 UNOFFICIAL COPY OF HOUSE BILL 1329 J2 6lr1558 CF 6lr1733 By: Delegate Hubbard Introduced and read first time: February 10, 2006 Assigned to: Health and Government Operations 1 AN ACT concerning A BILL
UNOFFICIAL COPY OF HOUSE BILL 1329 J2 6lr1558 CF 6lr1733 By: Delegate Hubbard Introduced and read first time: February 10, 2006 Assigned to: Health and Government Operations 1 AN ACT concerning A BILL
CHAPTER Committee Substitute for Committee Substitute for House Bill No. 321
 CHAPTER 2015-110 Committee Substitute for Committee Substitute for House Bill No. 321 An act relating to HIV testing; amending s. 381.004, F.S.; revising and providing definitions; specifying the notification
CHAPTER 2015-110 Committee Substitute for Committee Substitute for House Bill No. 321 An act relating to HIV testing; amending s. 381.004, F.S.; revising and providing definitions; specifying the notification
Florida Senate SB 224
 By Senator Benacquisto 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 A bill to be entitled An act relating to alternative nicotine products; amending s. 569.002, F.S.; providing
By Senator Benacquisto 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 A bill to be entitled An act relating to alternative nicotine products; amending s. 569.002, F.S.; providing
State of Minnesota HOUSE OF REPRESENTATIVES
 This Document can be made available in alternative formats upon request 02/09/2017 State of Minnesota HOUSE OF REPRESENTATIVES 926 NINETIETH SESSION H. F. No. Authored by Metsa, Applebaum, Schultz, Ecklund,
This Document can be made available in alternative formats upon request 02/09/2017 State of Minnesota HOUSE OF REPRESENTATIVES 926 NINETIETH SESSION H. F. No. Authored by Metsa, Applebaum, Schultz, Ecklund,
2. Discussion of land use concerns and potential updates to City Codes
 RIVERDALE CITY PLANNING COMMISSION AGENDA CIVIC CENTER - 4600 S. WEBER RIVER DR. TUESDAY MARCH 8, 2016 6:00 p.m. Planning Commission Work Session Meeting (City Offices) The purpose of the work session
RIVERDALE CITY PLANNING COMMISSION AGENDA CIVIC CENTER - 4600 S. WEBER RIVER DR. TUESDAY MARCH 8, 2016 6:00 p.m. Planning Commission Work Session Meeting (City Offices) The purpose of the work session
I. POLICY: DEFINITIONS: Applicant: Any individual who applies for employment with the Department of Juvenile Justice.
 GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: {x} All DJJ Staff { } Administration { } Community Services { } Secure Facilities (RYDC s and YDC s) Transmittal # 17-14 Policy # 3.15 Related Standards
GEORGIA DEPARTMENT OF JUVENILE JUSTICE Applicability: {x} All DJJ Staff { } Administration { } Community Services { } Secure Facilities (RYDC s and YDC s) Transmittal # 17-14 Policy # 3.15 Related Standards
Title 32, Chapter 127-A, ATHLETIC TRAINERS (HEADING: PL 1995, c. (new))
)") Chapter 127-A: ATHLETIC TRAINERS 14351. Purpose The Legislature finds that the practice of athletic training affects the public health, safety and welfare and is subject to regulation and control in the
Chapter 127-A: ATHLETIC TRAINERS 14351. Purpose The Legislature finds that the practice of athletic training affects the public health, safety and welfare and is subject to regulation and control in the
Z E N I T H M E D I C A L P R O V I D E R N E T W O R K P O L I C Y Title: Provider Appeal of Network Exclusion Policy
 TheZenith's Z E N I T H M E D I C A L P R O V I D E R N E T W O R K P O L I C Y Title: Provider Appeal of Network Exclusion Policy Application: Zenith Insurance Company and Wholly Owned Subsidiaries Policy
TheZenith's Z E N I T H M E D I C A L P R O V I D E R N E T W O R K P O L I C Y Title: Provider Appeal of Network Exclusion Policy Application: Zenith Insurance Company and Wholly Owned Subsidiaries Policy
CHAPTER Committee Substitute for Committee Substitute for Senate Bill No. 224
 CHAPTER 2014-65 Committee Substitute for Committee Substitute for Senate Bill No. 224 An act relating to tobacco and nicotine product regulation; amending s. 569.14, F.S.; allowing alternate signage requirements
CHAPTER 2014-65 Committee Substitute for Committee Substitute for Senate Bill No. 224 An act relating to tobacco and nicotine product regulation; amending s. 569.14, F.S.; allowing alternate signage requirements
1 HB By Representative Williams (JD) 4 RFD: Health. 5 First Read: 09-JAN-18 6 PFD: 11/28/2017. Page 0
 4 RFD: Health. 5 First Read: 09-JAN-18 6 PFD: 11/28/2017. Page 0") 1 HB37 2 188862-1 3 By Representative Williams (JD) 4 RFD: Health 5 First Read: 09-JAN-18 6 PFD: 11/28/2017 Page 0 1 188862-1:n:11/16/2017:PMG/tj LSA2017-3516 2 3 4 5 6 7 8 SYNOPSIS: This bill would establish
1 HB37 2 188862-1 3 By Representative Williams (JD) 4 RFD: Health 5 First Read: 09-JAN-18 6 PFD: 11/28/2017 Page 0 1 188862-1:n:11/16/2017:PMG/tj LSA2017-3516 2 3 4 5 6 7 8 SYNOPSIS: This bill would establish
416 DRUG AND ALCOHOL TESTING I. PURPOSE
 416 DRUG AND ALCOHOL TESTING I. PURPOSE A. The school board recognizes the significant problems created by drug and alcohol use in society in general, and the public schools in particular. The school board
416 DRUG AND ALCOHOL TESTING I. PURPOSE A. The school board recognizes the significant problems created by drug and alcohol use in society in general, and the public schools in particular. The school board
THE GENERAL ASSEMBLY OF PENNSYLVANIA SENATE BILL AN ACT
 PRINTER'S NO. THE GENERAL ASSEMBLY OF PENNSYLVANIA SENATE BILL No. Session of INTRODUCED BY LEACH AND FARNESE, FEBRUARY, REFERRED TO LAW AND JUSTICE, FEBRUARY, AN ACT 1 1 1 Providing for personal use of
PRINTER'S NO. THE GENERAL ASSEMBLY OF PENNSYLVANIA SENATE BILL No. Session of INTRODUCED BY LEACH AND FARNESE, FEBRUARY, REFERRED TO LAW AND JUSTICE, FEBRUARY, AN ACT 1 1 1 Providing for personal use of
UNOFFICIAL COPY OF SENATE BILL 735 CHAPTER
 UNOFFICIAL COPY OF SENATE BILL 735 E4 5lr1315 By: Senator Grosfeld Introduced and read first time: February 4, 2005 Assigned to: Judicial Proceedings Reassigned to: Education, Health, and Environmental
UNOFFICIAL COPY OF SENATE BILL 735 E4 5lr1315 By: Senator Grosfeld Introduced and read first time: February 4, 2005 Assigned to: Judicial Proceedings Reassigned to: Education, Health, and Environmental
SIXTY-FOURTH LEGISLATURE OF THE STATE OF WYOMING 2017 GENERAL SESSION
 AN ACT relating to public health and safety; creating the advisory council on palliative care; providing definitions; providing for council membership; providing duties for the council; providing duties
AN ACT relating to public health and safety; creating the advisory council on palliative care; providing definitions; providing for council membership; providing duties for the council; providing duties
AN ACT. The General Assembly of the Commonwealth of Pennsylvania hereby enacts as follows:
 Pennsylvania General Assembly http://www.legis.state.pa.us/cfdocs/legis/li/uconscheck.cfm?txttype=htm&yr=2014&sessind=0&smthlwind=0&act=89 07/17/2014 12:54 PM Home / Statutes of Pennsylvania / Unconsolidated
Pennsylvania General Assembly http://www.legis.state.pa.us/cfdocs/legis/li/uconscheck.cfm?txttype=htm&yr=2014&sessind=0&smthlwind=0&act=89 07/17/2014 12:54 PM Home / Statutes of Pennsylvania / Unconsolidated
Current through Chapter 199 and Chapters of the 2015 Legislative Session
 26-21-101. Short title. 26-21-101. Short title This article shall be known and may be cited as the "Colorado Commission for the Deaf and Hard of Hearing Act". Cite as C.R.S. 26-21-101 History. L. 2000:
26-21-101. Short title. 26-21-101. Short title This article shall be known and may be cited as the "Colorado Commission for the Deaf and Hard of Hearing Act". Cite as C.R.S. 26-21-101 History. L. 2000:
DEPARTMENT OF VETERANS AFFAIRS SUMMARY: The Department of Veterans Affairs (VA) proposes to amend its medical
 proposes to amend its medical") This document is scheduled to be published in the Federal Register on 08/05/2016 and available online at http://federalregister.gov/a/2016-18660, and on FDsys.gov DEPARTMENT OF VETERANS AFFAIRS 8320-01
This document is scheduled to be published in the Federal Register on 08/05/2016 and available online at http://federalregister.gov/a/2016-18660, and on FDsys.gov DEPARTMENT OF VETERANS AFFAIRS 8320-01
The proposal affects Texas Occupations Code, Title 3, Subtitle D and Texas Administrative Code, Title 22, Part 5.
 Page 1 of 22 TITLE 22.EXAMINING BOARDS Part 5. STATE BOARD OF DENTAL EXAMINERS Chapter 101. DENTAL LICENSURE 22 TAC 101.1-101.7, 101.9 The State Board of Dental Examiners (Board) proposes amendments to
Page 1 of 22 TITLE 22.EXAMINING BOARDS Part 5. STATE BOARD OF DENTAL EXAMINERS Chapter 101. DENTAL LICENSURE 22 TAC 101.1-101.7, 101.9 The State Board of Dental Examiners (Board) proposes amendments to
A Bill Regular Session, 2019 HOUSE BILL 1471
 Stricken language would be deleted from and underlined language would be added to present law. 0 0 0 State of Arkansas nd General Assembly As Engrossed: H// A Bill Regular Session, 0 HOUSE BILL By: Representative
Stricken language would be deleted from and underlined language would be added to present law. 0 0 0 State of Arkansas nd General Assembly As Engrossed: H// A Bill Regular Session, 0 HOUSE BILL By: Representative
CHAPTER 391. (House Bill 326) Maryland Audiologists, Hearing Aid Dispensers, and Speech Language Pathologists Act Revision
 Maryland Audiologists, Hearing Aid Dispensers, and Speech Language Pathologists Act Revision") CHAPTER 391 (House Bill 326) AN ACT concerning Maryland Audiologists, Hearing Aid Dispensers, and Speech Language Pathologists Act Revision FOR the purpose of specifying that certain provisions of law
CHAPTER 391 (House Bill 326) AN ACT concerning Maryland Audiologists, Hearing Aid Dispensers, and Speech Language Pathologists Act Revision FOR the purpose of specifying that certain provisions of law
GENERAL ASSEMBLY OF NORTH CAROLINA SESSION 2009
 H GENERAL ASSEMBLY OF NORTH CAROLINA SESSION 0 HOUSE BILL Committee Substitute Favorable //0 Committee Substitute # Favorable //0 Fourth Edition Engrossed //0 Corrected Copy //0 Senate Health Care Committee
H GENERAL ASSEMBLY OF NORTH CAROLINA SESSION 0 HOUSE BILL Committee Substitute Favorable //0 Committee Substitute # Favorable //0 Fourth Edition Engrossed //0 Corrected Copy //0 Senate Health Care Committee
ORDINANCE NO. City Attorney s Synopsis
 Eff: ORDINANCE NO. AN ORDINANCE OF THE COUNCIL OF THE CITY OF BURBANK AMENDING TITLE 3 (BUSINESSES AND LICENSES), TITLE 5 (POLICE AND PUBLIC SAFETY) AND TITLE 10 (ZONING REGULATIONS) OF THE BURBANK MUNICIPAL
Eff: ORDINANCE NO. AN ORDINANCE OF THE COUNCIL OF THE CITY OF BURBANK AMENDING TITLE 3 (BUSINESSES AND LICENSES), TITLE 5 (POLICE AND PUBLIC SAFETY) AND TITLE 10 (ZONING REGULATIONS) OF THE BURBANK MUNICIPAL
GILMER COUNTY SCHOOLS Policy No POLICY MANUAL
 GILMER COUNTY SCHOOLS Policy No. 4080 POLICY MANUAL TITLE: DRUG FREE WORKPLACE POLICY 1. General Policy. The Board believes it is imperative to establish, promote and maintain a safe, healthy working and
GILMER COUNTY SCHOOLS Policy No. 4080 POLICY MANUAL TITLE: DRUG FREE WORKPLACE POLICY 1. General Policy. The Board believes it is imperative to establish, promote and maintain a safe, healthy working and
79th OREGON LEGISLATIVE ASSEMBLY Regular Session. Enrolled. House Bill 3440
 79th OREGON LEGISLATIVE ASSEMBLY--2017 Regular Session Enrolled House Bill 3440 Sponsored by Representatives WILLIAMSON, BUEHLER, GREENLICK, HERNANDEZ, KENNEMER, MALSTROM, MEEK, Senator STEINER HAYWARD;
79th OREGON LEGISLATIVE ASSEMBLY--2017 Regular Session Enrolled House Bill 3440 Sponsored by Representatives WILLIAMSON, BUEHLER, GREENLICK, HERNANDEZ, KENNEMER, MALSTROM, MEEK, Senator STEINER HAYWARD;
By: Senators Steele, Altes, Madison, Whitaker By: Representatives Bradford, Mahony, Judy, Wood, Lendall, Martin, Penix. For An Act To Be Entitled
 Stricken language would be deleted from and underlined language would be added to the law as it existed prior to this session of the General Assembly. 0 0 0 State of Arkansas As Engrossed: S//0 S//0 S/0/0
Stricken language would be deleted from and underlined language would be added to the law as it existed prior to this session of the General Assembly. 0 0 0 State of Arkansas As Engrossed: S//0 S//0 S/0/0
Sub. S.B. 119 As Passed by the Senate
 AM3404 Sub. S.B. 119 As Passed by the Senate Topic: Opioid Data and Communication Expansion Act moved to amend as follows: In line 1 of the title, after "4723.52," insert "4729.01, 4729.44, 4729.75, 4729.79,
AM3404 Sub. S.B. 119 As Passed by the Senate Topic: Opioid Data and Communication Expansion Act moved to amend as follows: In line 1 of the title, after "4723.52," insert "4729.01, 4729.44, 4729.75, 4729.79,
REQUEST FOR PROPOSALS FOR CY 2019 FUNDING. Issue Date: Monday, July 30, Submission Deadline: 5:00 p.m., Friday, August 24, 2018
 REQUEST FOR PROPOSALS FOR CY 2019 FUNDING Issue Date: Monday, July 30, 2018 Submission Deadline: 5:00 p.m., Friday, August 24, 2018 NOTE: RFP proposals received after the deadline will not be considered.
REQUEST FOR PROPOSALS FOR CY 2019 FUNDING Issue Date: Monday, July 30, 2018 Submission Deadline: 5:00 p.m., Friday, August 24, 2018 NOTE: RFP proposals received after the deadline will not be considered.
Business Impact Analysis
 ACTION: Original DATE: 05/01/2018 10:55 AM Business Impact Analysis Agency Name: Ohio Department of Health Regulation/Package Title: Chapter 3701-52 Smoke Free Workplace Rule Number(s): 3701-52 Date: November
ACTION: Original DATE: 05/01/2018 10:55 AM Business Impact Analysis Agency Name: Ohio Department of Health Regulation/Package Title: Chapter 3701-52 Smoke Free Workplace Rule Number(s): 3701-52 Date: November
Model Intervention for Students with Substance Abuse Problems Act
 Model Intervention for Students with Substance Abuse Problems Act MODEL INTERVENTION FOR STUDENTS WITH SUBSTANCE ABUSE PROBLEMS ACT Table of Contents G-103 Policy Statement G-105 Highlights Section One
Model Intervention for Students with Substance Abuse Problems Act MODEL INTERVENTION FOR STUDENTS WITH SUBSTANCE ABUSE PROBLEMS ACT Table of Contents G-103 Policy Statement G-105 Highlights Section One
General Terms and Conditions
 General Terms and Conditions Revision history (November 2007) Date issued Replaced pages Effective date 11/07 ii, iii, 2, 4 11/07 11/06 all pages 11/06 01/06 all pages 01/06 02/05 ii, iii, 4, 7 8 02/05
General Terms and Conditions Revision history (November 2007) Date issued Replaced pages Effective date 11/07 ii, iii, 2, 4 11/07 11/06 all pages 11/06 01/06 all pages 01/06 02/05 ii, iii, 4, 7 8 02/05
SUMMARY Provides for the award of certain grants relating to the prevention and treatment
 SUMMARY Provides for the award of certain grants relating to the prevention and treatment of substance abuse. (BDR 40-1023) FISCAL NOTE: Effect on Local Government: No. Effect on the State: Yes. AN ACT
SUMMARY Provides for the award of certain grants relating to the prevention and treatment of substance abuse. (BDR 40-1023) FISCAL NOTE: Effect on Local Government: No. Effect on the State: Yes. AN ACT
42 USC 290aa. NB: This unofficial compilation of the U.S. Code is current as of Jan. 4, 2012 (see
 TITLE 42 - THE PUBLIC HEALTH AND WELFARE CHAPTER 6A - PUBLIC HEALTH SERVICE SUBCHAPTER III-A - SUBSTANCE ABUSE AND MENTAL HEALTH SERVICES ADMINISTRATION Part A - Organization and General Authorities 290aa.
TITLE 42 - THE PUBLIC HEALTH AND WELFARE CHAPTER 6A - PUBLIC HEALTH SERVICE SUBCHAPTER III-A - SUBSTANCE ABUSE AND MENTAL HEALTH SERVICES ADMINISTRATION Part A - Organization and General Authorities 290aa.
XV. DRUG-FREE WORKPLACE PROCEDURES XV-1
 XV. DRUG-FREE WORKPLACE PROCEDURES XV-1 THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK XV-2 DRUG-FREE WORKPLACE GENERAL POLICY STATEMENT 6Gx13-4-1.05 The School Board of Miami-Dade County, Florida recognizes
XV. DRUG-FREE WORKPLACE PROCEDURES XV-1 THIS PAGE HAS BEEN LEFT INTENTIONALLY BLANK XV-2 DRUG-FREE WORKPLACE GENERAL POLICY STATEMENT 6Gx13-4-1.05 The School Board of Miami-Dade County, Florida recognizes
General Terms and Conditions
 General Terms and Conditions Revision history (July 2008) Date issued Replaced pages Effective date 07/08 all pages 07/08 11/07 ii, iii, 2, 4 11/07 11/06 all pages 11/06 01/06 all pages 01/06 02/05 ii,
General Terms and Conditions Revision history (July 2008) Date issued Replaced pages Effective date 07/08 all pages 07/08 11/07 ii, iii, 2, 4 11/07 11/06 all pages 11/06 01/06 all pages 01/06 02/05 ii,
CHAPTER 2 NETWORK PROVIDER/SERVICE DELIVERY REQUIREMENTS
 CHAPTER 2 NETWORK PROVIDER/SERVICE DELIVERY REQUIREMENTS 2.9 SPECIAL POPULATIONS ADHS/DBHS receives Federal grants and State appropriations to deliver behavioral health services to special populations
CHAPTER 2 NETWORK PROVIDER/SERVICE DELIVERY REQUIREMENTS 2.9 SPECIAL POPULATIONS ADHS/DBHS receives Federal grants and State appropriations to deliver behavioral health services to special populations
78th OREGON LEGISLATIVE ASSEMBLY Regular Session. Senate Bill 964 SUMMARY
 Sponsored by Senators BURDICK, KRUSE th OREGON LEGISLATIVE ASSEMBLY-- Regular Session Senate Bill SUMMARY The following summary is not prepared by the sponsors of the measure and is not a part of the body
Sponsored by Senators BURDICK, KRUSE th OREGON LEGISLATIVE ASSEMBLY-- Regular Session Senate Bill SUMMARY The following summary is not prepared by the sponsors of the measure and is not a part of the body
Alcohol & Drug Practice
 Alcohol & Drug Practice Vice-President, Health & Safety June 1, 2011 Purpose Cenovus recognizes that the use of alcohol and drugs can adversely affect job performance, the work environment and the safety
Alcohol & Drug Practice Vice-President, Health & Safety June 1, 2011 Purpose Cenovus recognizes that the use of alcohol and drugs can adversely affect job performance, the work environment and the safety
APPENDIX C: HIV/AIDS TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1
 APPENDIX C: HIV/AIDS TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1 JANUARY 2018 TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1 JANUARY 2018 APPENDIX C: HIV/AIDS Table of Contents C.1 CDC Revised
APPENDIX C: HIV/AIDS TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1 JANUARY 2018 TEXAS MEDICAID PROVIDER PROCEDURES MANUAL: VOL. 1 JANUARY 2018 APPENDIX C: HIV/AIDS Table of Contents C.1 CDC Revised
THE NORTH CAROLINA MASSAGE AND BODYWORK THERAPY PRACTICE ACT NORTH CAROLINA GENERAL STATUTES
 Page 1 THE NORTH CAROLINA MASSAGE AND BODYWORK THERAPY PRACTICE ACT NOTE: This legislation was originally signed into law by Governor James B. Hunt on November 6, 1998, and was amended in 2003 and 2005
Page 1 THE NORTH CAROLINA MASSAGE AND BODYWORK THERAPY PRACTICE ACT NOTE: This legislation was originally signed into law by Governor James B. Hunt on November 6, 1998, and was amended in 2003 and 2005
First Regular Session Seventy-first General Assembly STATE OF COLORADO INTRODUCED SENATE SPONSORSHIP HOUSE SPONSORSHIP
 First Regular Session Seventy-first General Assembly STATE OF COLORADO INTRODUCED LLS NO. 1-0.01 Michael Dohr x SENATE BILL 1-0 Marble, SENATE SPONSORSHIP Melton, HOUSE SPONSORSHIP Senate Committees Business,
First Regular Session Seventy-first General Assembly STATE OF COLORADO INTRODUCED LLS NO. 1-0.01 Michael Dohr x SENATE BILL 1-0 Marble, SENATE SPONSORSHIP Melton, HOUSE SPONSORSHIP Senate Committees Business,
Assembly Amendment to Assembly Bill No. 382 (BDR ) Proposed by: Assembly Committee on Commerce and Labor
 Proposed by: Assembly Committee on Commerce and Labor") 0 Session (th) A AB 0 Amendment No. 0 Assembly Amendment to Assembly Bill No. (BDR -0) Proposed by: Assembly Committee on Commerce and Labor Amends: Summary: No Title: Yes Preamble: No Joint Sponsorship:
0 Session (th) A AB 0 Amendment No. 0 Assembly Amendment to Assembly Bill No. (BDR -0) Proposed by: Assembly Committee on Commerce and Labor Amends: Summary: No Title: Yes Preamble: No Joint Sponsorship:
The Radiation Health and Safety Act, 1985
 1 The Radiation Health and Safety Act, 1985 Repealed by Chapter S-15.1 of the Statutes of Saskatchewan, 2013 (effective April 29, 2014) Formerly Chapter R-1.1 of the Statutes of Saskatchewan, 1984-85-86
1 The Radiation Health and Safety Act, 1985 Repealed by Chapter S-15.1 of the Statutes of Saskatchewan, 2013 (effective April 29, 2014) Formerly Chapter R-1.1 of the Statutes of Saskatchewan, 1984-85-86
CHAPTER Council Substitute for Committee Substitute for House Bill No. 1167
 CHAPTER 2008-129 Council Substitute for Committee Substitute for House Bill No. 1167 An act relating to the Reduced Cigarette Ignition Propensity Standard and Firefighter Protection Act; creating s. 633.042,
CHAPTER 2008-129 Council Substitute for Committee Substitute for House Bill No. 1167 An act relating to the Reduced Cigarette Ignition Propensity Standard and Firefighter Protection Act; creating s. 633.042,
NORTH DAKOTA STATE BOARD OF EXAMINERS AUDIOLOGY AND SPEECH-LANGUAGE PATHOLOGY
 NORTH DAKOTA STATE BOARD OF EXAMINERS AUDIOLOGY AND SPEECH-LANGUAGE PATHOLOGY LAW and RULES CHAPTER 43-37 AUDIOLOGISTS AND SPEECH-LANGUAGE PATHOLOGISTS Section 43-37-01 Policy 43-37-02 Definitions 43-37-03
NORTH DAKOTA STATE BOARD OF EXAMINERS AUDIOLOGY AND SPEECH-LANGUAGE PATHOLOGY LAW and RULES CHAPTER 43-37 AUDIOLOGISTS AND SPEECH-LANGUAGE PATHOLOGISTS Section 43-37-01 Policy 43-37-02 Definitions 43-37-03
Department of Legislative Services Maryland General Assembly 2009 Session
 Senate Bill 261 Judicial Proceedings Department of Legislative Services Maryland General Assembly 2009 Session FISCAL AND POLICY NOTE Revised (The President, et al.) (By Request - Administration) SB 261
Senate Bill 261 Judicial Proceedings Department of Legislative Services Maryland General Assembly 2009 Session FISCAL AND POLICY NOTE Revised (The President, et al.) (By Request - Administration) SB 261
A Bill Regular Session, 2015 SENATE BILL 717
 Stricken language would be deleted from and underlined language would be added to present law. 0 State of Arkansas 0th General Assembly As Engrossed: S// H// A Bill Regular Session, SENATE BILL By: Senator
Stricken language would be deleted from and underlined language would be added to present law. 0 State of Arkansas 0th General Assembly As Engrossed: S// H// A Bill Regular Session, SENATE BILL By: Senator
Oklahoma Statutes on Prevention of Youth Access to Tobacco
 Oklahoma Statutes on Prevention of Youth Access to Tobacco Title 21 21-1241. Furnishing cigarettes or other tobacco or vapor products to minors - Punishment. Any person who shall furnish to any minor by
Oklahoma Statutes on Prevention of Youth Access to Tobacco Title 21 21-1241. Furnishing cigarettes or other tobacco or vapor products to minors - Punishment. Any person who shall furnish to any minor by
One Hundred Ninth Congress of the United States of America
 S. 843 One Hundred Ninth Congress of the United States of America AT THE SECOND SESSION Begun and held at the City of Washington on Tuesday, the third day of January, two thousand and six An Act To amend
S. 843 One Hundred Ninth Congress of the United States of America AT THE SECOND SESSION Begun and held at the City of Washington on Tuesday, the third day of January, two thousand and six An Act To amend
HOUSE BILL No page 2
 HOUSE BILL No. 2744 AN ACT concerning insurance; providing coverage for autism spectrum disorder; requiring licensure of persons providing applied behavior analysis; amending K.S.A. 2013 Supp. 40-2,103
HOUSE BILL No. 2744 AN ACT concerning insurance; providing coverage for autism spectrum disorder; requiring licensure of persons providing applied behavior analysis; amending K.S.A. 2013 Supp. 40-2,103
Secretary of the Senate. Chief Clerk of the Assembly. Private Secretary of the Governor
 Senate Bill No. 132 Passed the Senate October 14, 2009 Secretary of the Senate Passed the Assembly September 8, 2009 Chief Clerk of the Assembly This bill was received by the Governor this day of, 2009,
Senate Bill No. 132 Passed the Senate October 14, 2009 Secretary of the Senate Passed the Assembly September 8, 2009 Chief Clerk of the Assembly This bill was received by the Governor this day of, 2009,
ASSEMBLY, No STATE OF NEW JERSEY. 218th LEGISLATURE INTRODUCED FEBRUARY 1, 2018
 ASSEMBLY, No. STATE OF NEW JERSEY th LEGISLATURE INTRODUCED FEBRUARY, 0 Sponsored by: Assemblywoman PAMELA R. LAMPITT District (Burlington and Camden) SYNOPSIS Provides for Medicaid coverage of comprehensive
ASSEMBLY, No. STATE OF NEW JERSEY th LEGISLATURE INTRODUCED FEBRUARY, 0 Sponsored by: Assemblywoman PAMELA R. LAMPITT District (Burlington and Camden) SYNOPSIS Provides for Medicaid coverage of comprehensive
South Carolina General Assembly 122nd Session,
 South Carolina General Assembly 1nd Session, 01-01 S. STATUS INFORMATION General Bill Sponsors: Senator Shealy Document Path: l:\s-res\ks\0sign.dmr.ks.docx Introduced in the Senate on March 1, 01 Currently
South Carolina General Assembly 1nd Session, 01-01 S. STATUS INFORMATION General Bill Sponsors: Senator Shealy Document Path: l:\s-res\ks\0sign.dmr.ks.docx Introduced in the Senate on March 1, 01 Currently
IC Applicability Sec. 1. The definitions in this chapter apply throughout this article. As added by P.L , SEC.8.
 IC 25-21.8 ARTICLE 21.8. MASSAGE THERAPISTS IC 25-21.8-1 Chapter 1. Definitions IC 25-21.8-1-1 Applicability Sec. 1. The definitions in this chapter apply throughout this article. IC 25-21.8-1-1.5 Approved
IC 25-21.8 ARTICLE 21.8. MASSAGE THERAPISTS IC 25-21.8-1 Chapter 1. Definitions IC 25-21.8-1-1 Applicability Sec. 1. The definitions in this chapter apply throughout this article. IC 25-21.8-1-1.5 Approved
AN ACT. relating to the medical use of low-thc cannabis and the regulation. of related organizations and individuals; requiring a dispensing
 Chapter 0 S.B. No. AN ACT relating to the medical use of low-thc cannabis and the regulation of related organizations and individuals; requiring a dispensing organization to obtain a license to dispense
Chapter 0 S.B. No. AN ACT relating to the medical use of low-thc cannabis and the regulation of related organizations and individuals; requiring a dispensing organization to obtain a license to dispense
IC ARTICLE 13. DENTAL HYGIENISTS. IC Chapter 1. Regulation of Dental Hygienists by State Board of Dentistry
 IC 25-13 ARTICLE 13. DENTAL HYGIENISTS IC 25-13-1 Chapter 1. Regulation of Dental Hygienists by State Board of Dentistry IC 25-13-1-1 Short title Sec. 1. This chapter may be known and cited as The Dental
IC 25-13 ARTICLE 13. DENTAL HYGIENISTS IC 25-13-1 Chapter 1. Regulation of Dental Hygienists by State Board of Dentistry IC 25-13-1-1 Short title Sec. 1. This chapter may be known and cited as The Dental
HILLSBOROUGH COUNTY AVIATION AUTHORITY AIRPORT BOARD OF ADJUSTMENT RULES OF PROCEDURE
 HILLSBOROUGH COUNTY AVIATION AUTHORITY AIRPORT BOARD OF ADJUSTMENT RULES OF PROCEDURE PURPOSE AND AUTHORITY Adopted May 6, 2010 Revised June 2, 2016 The Hillsborough County Aviation Authority Airport Board
HILLSBOROUGH COUNTY AVIATION AUTHORITY AIRPORT BOARD OF ADJUSTMENT RULES OF PROCEDURE PURPOSE AND AUTHORITY Adopted May 6, 2010 Revised June 2, 2016 The Hillsborough County Aviation Authority Airport Board
DEPARTMENT OF VETERANS AFFAIRS SUMMARY: The Department of Veterans Affairs (VA) is amending its medical
 is amending its medical") This document is scheduled to be published in the Federal Register on 03/23/2017 and available online at https://federalregister.gov/d/2017-05799, and on FDsys.gov DEPARTMENT OF VETERANS AFFAIRS 8320-01
This document is scheduled to be published in the Federal Register on 03/23/2017 and available online at https://federalregister.gov/d/2017-05799, and on FDsys.gov DEPARTMENT OF VETERANS AFFAIRS 8320-01
ASSEMBLY, No. 542 STATE OF NEW JERSEY. 218th LEGISLATURE PRE-FILED FOR INTRODUCTION IN THE 2018 SESSION
 ASSEMBLY, No. STATE OF NEW JERSEY th LEGISLATURE PRE-FILED FOR INTRODUCTION IN THE 0 SESSION Sponsored by: Assemblyman VINCENT MAZZEO District (Atlantic) Assemblyman JOSEPH A. LAGANA District (Bergen and
ASSEMBLY, No. STATE OF NEW JERSEY th LEGISLATURE PRE-FILED FOR INTRODUCTION IN THE 0 SESSION Sponsored by: Assemblyman VINCENT MAZZEO District (Atlantic) Assemblyman JOSEPH A. LAGANA District (Bergen and
(4) Be as detailed as necessary to provide history of work performed; and:
 Be as detailed as necessary to provide history of work performed; and:") www.omarfigueroa.com Page 66 of 278 (4) Be as detailed as necessary to provide history of work performed; and: (A) Include information adequate to identify any associated manufacturing facility (e.g.,
www.omarfigueroa.com Page 66 of 278 (4) Be as detailed as necessary to provide history of work performed; and: (A) Include information adequate to identify any associated manufacturing facility (e.g.,
NCADD :fts?new JERSEY
 - :fts?new JERSEY 2013 NEW JERSEY STATE LEGISLATIVE ADDICTION PREVENTION, TREATMENT, and RECOVERY SURVEY I. General Views on Alcohol and Drug Addiction Policies to Address Stigma Addictive illness is recognized
- :fts?new JERSEY 2013 NEW JERSEY STATE LEGISLATIVE ADDICTION PREVENTION, TREATMENT, and RECOVERY SURVEY I. General Views on Alcohol and Drug Addiction Policies to Address Stigma Addictive illness is recognized