Dr sadeghi, MD Assistant professor of gastroenterology and hepatology
|
|
|
- Marsha Adams
- 5 years ago
- Views:
Transcription
1 Dr sadeghi, MD Assistant professor of gastroenterology and hepatology
2 Acute intermittent porphyria is estimated to affect about one in people in European countries, apart from in northern Sweden, where, because of a founder effect, it is more frequent (one in 1000). Acute attacks are very rare before puberty and after menopause, with a peak occurrence within the third decade. They are more common in women than in men. Most patients have one or a few attacks and then recover fully for the rest of their lives. Less than 10% develop recurrent acute attacks.
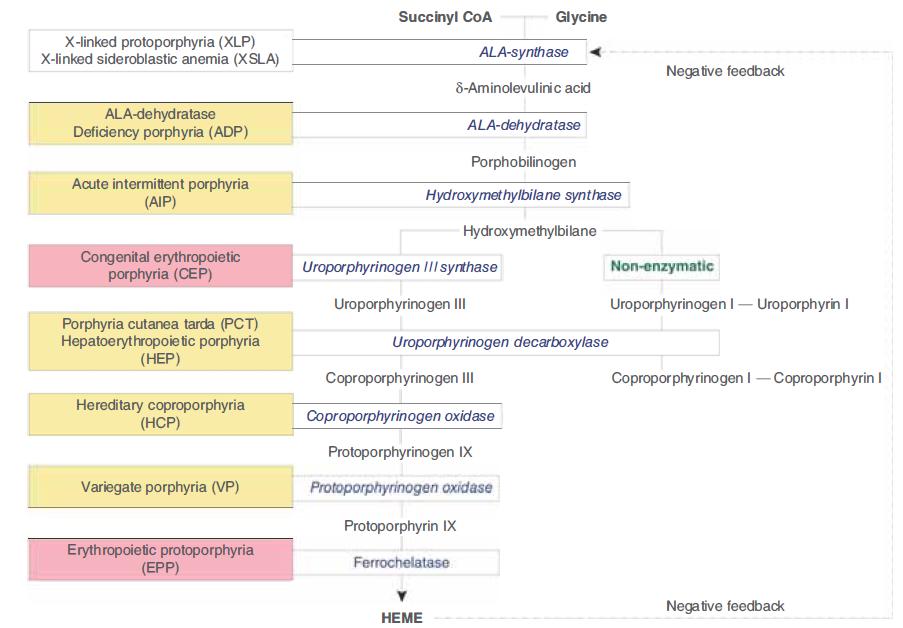
3 Pathophysiology The alteration in enzyme activity is usually due to an inherited mutation in the gene for that enzyme. However, in porphyria cutanea tarda (PCT), the most common of the porphyrias, acquired inhibition of the fifth enzyme in the pathway, uroporphyrin decarboxylase (UROD), develops during life, specifically in the liver.

4 By way of general introduction, the acute porphyrias are rare metabolic disorders caused by 1 of 4 inherited enzymatic defects in normal heme biosynthesis. The 4 diseases have rather daunting names: acute intermittent porphyria, hereditary coproporphyria, variegate porphyria, and ALA dehydratase-deficiency porphyria. Those defects may result in an overproduction of heme precursors, especially delta aminolevulinic acid, which we will generally refer to as ALA, and porphobilinogen, or PBG.

5
6
7 Overproduction fortunately doesn't occur in most patients most of the time; only a minority of people suffer these problems. But when there is marked, uncontrolled overproduction of ALA and PBG due to a marked induction of hepatic ALA synthase, which is the first rate-controlling enzyme in heme synthesis, then there may be accumulation, first in the liver and then in the blood. These are then overexcreted in the urine and the stool.
8 Heme is made in all tissues, but the bone marrow and liver are the most active organs involved in overall heme synthesis. The bone marrow accounts for >80 percent of daily heme synthesis ( all of the synthesized heme is utilized as the prosthetic group for hemoglobin). The liver accounts for most of the rest of overall heme synthesis. In the liver, heme is utilized primarily for the production of the various cytochrome P450 enzymes (CYPs)

9
10 People with autosomal-dominant acute porphyrias acute intermittent porphyria, variegate porphyria, and hereditary coproporphyria can present with a sudden lifethreatening crisis. Skin lesions (similar to PCT) never develop in acute intermittent porphyria but are the only clinical manifestation in some patients with variegate porphyria (60% of patients), and rarely (5%) develop in patients with hereditary coprophorphyria.

11

12
13 ACUTE INTERMITTENT PORPHYRIA

14

15

16
17 Porphyric attacks begin with a prodromic phase including minor behavioural changes such as anxiety, restlessness, and insomnia. The cardinal manifestation is abdominal pain, although the pain can be in the chest, back, or extremities. Most people with acute attacks present with severe abdominal pain. Most acute attacks last for no longer than 1 or 2 weeks.
18
19 Abdominal pain is the most common symptom in AIP, occurring in 85 to 95 % of patients with acute attacks. Often it can be pelvic. It is less often upper abdominal, but it can also involve the upper abdomen. Because the pain and other symptoms are neuropathic rather than inflammatory, abdominal tenderness, rebound, fever, and leukocytosis are usually minimal or absent during an acute attack.
20 It is usually severe, steady, and poorly localized but is sometimes cramping, and is often accompanied by constipation and signs of ileus such as nausea, vomiting, abdominal distension, and decreased bowel sounds. However, diarrhea and increased bowel sounds are sometimes seen. In most series, severe constipation, often to the point of obstipation, is present in around 90%-95% of patients, although a small percentage report diarrhea.
21 Electerolyte disturbnce : During acute attacks, patients frequently become dehydrated and electrolyte imbalanced. Hyponatraemia attributable to inappropriate anti diuretic hormone secretion syndrome develops in 40% of cases, and when severe can lead to convulsion and hallucination. Hypomanasemia and hypercalcemia may be seen.
22 Autonomic nervous system involvement : The autonomic nervous system is affected in AIP and circulating catecholamine levels are increased. Tachycardia is the most common physical sign, occurring in approximately 80 percent of attacks, and is often accompanied by hypertension, sweating, restlessness, and tremor.
23 CNS manifestations: Seizures in acute attacks can develop because of hyponatraemia or hypomagnesaemia or as a manifestation of porphyria. Acute attacks can also be life threatening because of severe neurological complications.
24 Especially with prolonged attacks, it may also involve cranial nerves and lead to bulbar paralysis, respiratory impairment, and death. Pyramidal signs, cerebellar syndrome, transitory blindness, or consciousness abnormalities (from somnolence to coma) can arise.
25 Peripheral neuropathy : Sensory neuropathy is common and presents with pain in the back, chest, and extremities, and may precede the abdominal pain. Patchy numbness, paresthesias, and dysesthesias may occur.
26 Sometimes in an acute setting, peripheral motor neuropathy like Guillain-Barré syndrome (an ascending motor paralysis) may be seen. Onset of a motor neuropathy is often characterised by severe pain and stiffness in the thighs and back, and then loss of tendon reflexes and motor paralysis.
27 A peripheral motor neuropathy develops early in some attacks, but is more often a later manifestation of a prolonged attack. Motor weakness usually begins in the proximal muscles, more frequently in the arms than in the legs. Limb paresis, when it occurs, can be very local. Muscle weakness can progress and lead to tetraplegia, with respiratory and bulbar paralysis and death.
28 Cerebrospinal fluid is normal in most cases. Although advanced motor neuropathy with quadriplegia and respiratory paralysis is potentially reversible with appropriate treatment (eg, intravenous hemin), some permanent paralysis may remain

29
30 Neuropsychiatric manifestations: Insomnia is often an early symptom of an attack. Other neuropsychiatric manifestations (In 20 30% of patients) include anxiety, restlessness, agitation, hallucinations, hysteria, disorientation, delirium, apathy, depression, phobias and altered consciousness, ranging from somnolence to coma.
31 Occasionally, excretion of red or dark-coloured urine helps physicians with their investigations. ALA and PBG are colorless But PBG degrades to form porphobilin, a brownish product dark urine Also urinary porphyrine are increased in AIP reddish brown urine

32

33
34 The key point is that there are women who, unfortunately, suffer acute attacks of porphyria almost every month, and it is in the mid-cycle, right after ovulation and the formation of the corpus luteum. It is not at the time of menstruation, unlike so many other symptoms that are cyclical in these women.
35 The progestins can cause or precipitate porphyrias, so females, during the luteal phase of their menstrual cycle, often will have a precipitation of their symptoms. Progestrone and testosterone are induce ALAS1 and CYPs. Estrogen have less effect and could be harmful mostly in association with progestrone
36 If a patient comes in recurrently and we do an initial gastrointestinal workup, specifically endoscopies and some sort of imaging study, and, perhaps, even do some empiric treatment for irritable bowel syndrome without any margin of success, then at that point I need to start considering a porphyria, especially if the symptoms are more intermittent and less chronic in nature.

37

38
39 Examination of urine for excess porphobilinogen is the essential first-line test for patients with a suspected attack of acute porphyria. The best test is a urine PBG screening test at the time of symptoms. Testing for increased urinary PBG is also highly specific, since a substantial increase in urinary PBG does not occur in medical conditions other than AIP, HCP and VP
40 Testing for increased urinary PBG is rapid and sensitive, since marked increases are expected in acute porphyrias, especially at the time of an acute attack. It is is sensitive enough that, were it to be negative, it would completely exclude the diagnosis of acute intermittent porphyria. Porphobilinogen is not a porphyrin. It is a monopyrrole, not a tetrapyrrole.
41 However, PBG may not be elevated when the patient with AIP, HCP, or VP is asymptomatic, and is normal in ALA dehydratase porphyria. Increases in PBG and ALA can persist for prolonged periods between attacks of AIP but fall more rapidly after acute attacks of HCP and VP. Urinary ALA and PBG excretion often remains elevated between frequent exacerbations, and is sometimes elevated in those who have never had symptoms.
42 A commercially-available semiquantitative kit rapidly and reliably detects increased urinary PBG on a spot urine specimen During an acute attack of AIP, urinary PBG excretion is generally 20 to 200 mg/day (markedly higher than the normal rate of approximately 0 to 4 mg/day or per gram of creatinine), with ALA excretion being approximately one-half that amount (normal range 0 to 7 mg/day).
43 In patients with end-stage renal disease, the diagnosis of acute porphyria can be established by the presence of a marked elevation in plasma PBG. Measurement of 5-aminolaevulinic acid is not essential to establish the diagnosis but can be helpful for differentiation of the disorder from the rare 5- aminolaevulinic acid dehydratase porphyria.
44 I should just mention that there is this one very, very rare form of porphyria caused by severe deficiency of the enzyme ALA dehydratase. There have only been 7 or so reported cases in the entire medical literature. That is the one form of acute porphyria in which there is not an increase in porphobilinogen. The reason is that the site of the block is proximal to the formation of porphobilinogen, so the defect is in the inability to make porphobilinogen.
45 Urinary PBG and ALA are increased in all three acute hepatic porphyrias (acute intermittent porphyria, hereditary coproporphyria, and variegate porphyria) alththe concentrations are higher and longer lasting in acute intermittent porphyriaough than in the other two types (hereditary coporphyria and variegate porphyria).
46 If a screening test for increased urinary PBG is negative on a spot urine specimen but the index of suspicion is high for an acute porphyria, a 24-hour urine collection should be obtained for quantitative assessment of PBG.
47 Measurement of urinary porphyrins is unhelpful and might be misleading because of frequent and nonspecific coproporphyrinuria in many common disorders (such as chronic liver disease). There are lots of disorders or conditions that are not porphyria that have mild increases in urinary porphyrins, particularly in coproporphyrin. There is a long list of drugs and other conditions that can do that, so it is very important not to jump to the diagnosis just because there is a slight abnormality in urinary porphyrins.
48 Urinary coproporphyrin is usually more elevated in HCP and VP than in AIP. However, coproporphyrin is the predominant porphyrin in normal urine and is also increased in many medical conditions other than porphyria. Its urinary excretion increases in liver disease because it is normally partially excreted in bile
49 Differentiating AIP from other acute porphyrias Attacks of all four of the acute porphyrias (ie, acute intermittent porphyria, ALA dehydratase porphyria, hereditary coproporphyria, variegate porphyria) are treated in the same manner. As a result, treatment can be initiated once there is definite laboratory documentation of a substantial increase in urinary or plasma PBG, while further testing, including measurement of porphyrins in plasma, urine, and feces, and erythrocyte PBG deaminase (PBGD) activity is in progress.
50 Measurements of total plasma and fecal porphyrins, which are normal or only slightly increased in AIP, are recommended to definitively exclude HCP and VP. Plasma porphyrins are increased in VP with a characteristic fluorescence peak at neutral ph.
51 For diagnosis of the type of acute porphyria in the proband, plasma fluorescence emission spectroscopy is a first-line test because a peak at nm establishes the diagnosis of variegate porphyria. However, it does not distinguish acute intermittent porphyria from hereditary coproporhyria, for which the emission peak at 620 nm is usually present for both types.
52 Fecal porphyrins are normal or minimally increased in AIP but substantially increased in HCP (with a marked predominance of coproporphyrin III) and in VP (with approximately equal increases in coproporphyrin III and protoporphyrin). Total faecal porphyrin concentration is raised in hereditary coproporphyria, with coproporphyrin as the main component and a ratio of isomer III to isomer I greater than 2.
53 When present, a 50% decrease of PBG deaminase (PBGD) activity can positively identify acute intermittent porphyria patients. Although erythrocyte PBGD activity is approximately halfnormal in most patients with AIP, this measurement is not definitive for confirming or excluding a diagnosis. Erythrocyte PBGD measurement is not useful for the initial diagnosis of acute porphyria in ill patients. Its use as a second line test to confirm a diagnosis of AIP and for screening asymptomatic family members is now largely replaced by DNA testing.

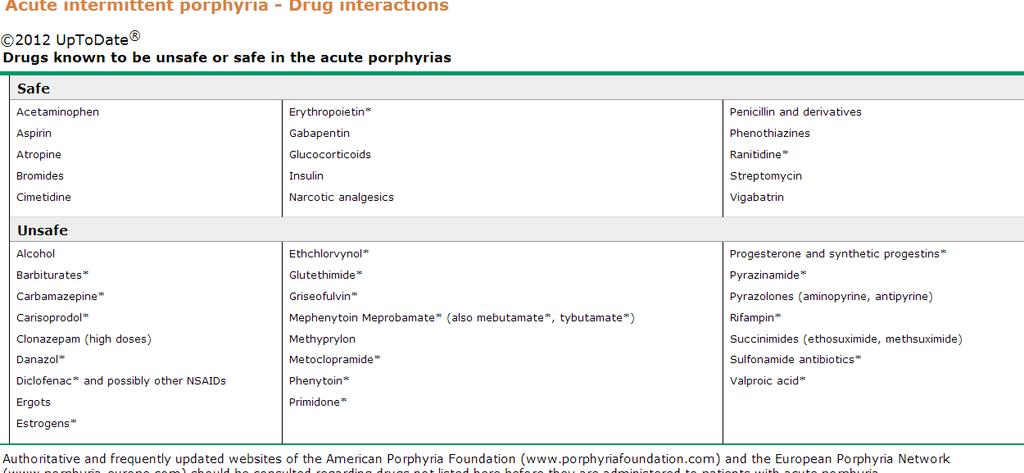
54
55 Family screening is essential to prevent acute attacks in those with latent disease. DNA analysis to identify the mutation is the gold standard. For DNA analysis, previous identification of the mutation in an unequivocally affected family member is needed. Enzyme measurements are reserved for families in which a mutation cannot be identified.
56 DNA testing The underlying PBGD mutation should be identified by DNA testing after the diagnosis of AIP is established by biochemical methods. This not only further confirms the diagnosis, but most importantly enables accurate identification of other gene carriers in a family. The great majority of heterozygous carriers of PBGD mutations have a good prognosis and remain asymptomatic during their lifetime. Attacks of acute porphyria are rare in children, thus reducing the urgency of making a diagnosis.
57

58
59 Acute attacks are precipitated by events that either directly induce ALAS1 or increase the demand for haem synthesis. These events include hormonal fluctuations during the menstrual cycle, fasting, smoking, infections, and exposure to porphyrinogenic drugs. Less than 10% of patients have recurrent acute attacks without clearly identified precipitating factors.
60 Most drugs that exacerbate porphyria are closely associated with induction of cytochrome P450 enzymes, which increase hepatic haem turnover. Inflammatory and infectious diseases induce hepatic expression of the acute-phase protein haem oxygenase, which catabolises haem.
61 We review their medical history and medications, looking for clues that would point to the porphyrias. These include medications that are unsafe for use in the porphyrias, such as the barbiturates and sulfonamides. Barbiturates or seizure-control medicines affect porphyrias, especially if patients have had new ones added or a dosage changed.
62 UNSAFE ( INDUCE HEPATIC ALAS1 AND CYPs) Alcohol Barbiturate Carbamazepine rifampin Clonazepam Danazol Diclofenac and other NSAIDS Metoclorpramide Phenytoin Pirimidone Na Valproate Progesterone Rifampin Pyrainamide Sulfanamide AB SAFE Acetaminophen Aspirin Atropine Bromides Cimetidine Epo Gabapentin Gc Insuline narcotic
63
64 Treatment should be started promptly and any precipitating factors especially drugs (including oestrogens and progestagens) avoided, underlying infection should be treated and hypocaloric diets corrected.
65 Nutritional factors ALAS1 is upregulated by starvation or other conditions where glucose level is low. Exacerbation of AIP by reduced intake of calories which may occur during illness, surgery or other stress They want to maintain a good, regular diet, not one that is low in carbohydrates or low in calories, because those things might precipitate an attack. They also would want to avoid alcohol and stressful situations that could bring on an attack.
66 Pain, nausea, and vomiting are generally severe and require narcotic analgesics, chlorpromazine, or another phenothiazine or ondansetron, agents which are safe to use in the acute porphyrias. Short-acting benzodiazepines in low doses are probably safe for anxiety and insomnia.
67 Beta-adrenergic blocking agents may be useful to control tachycardia and hypertension. Careful management of fluid balance, with avoidance of large volumes of hypotonic dextrose, is necessary to limit the risk of severe hyponatraemia, which could provoke convulsions.
68 Cardiovascular complications such as hypertension and tachycardia are rarely severe, therapy with β blockers is needed in some cases. Very occasionally, acute attacks are accompanied by a severe adrenergic crisis with dangerous hypertension, encephalopathy and seizures. Intravenous infusion of magnesium sulphate can be effective for control of adrenergic symptoms.
69 Seizures are treated by carefully correcting hyponatremia, if present. Almost all anticonvulsant drugs have at least some potential for exacerbating acute porphyrias. Clonazepam may be less harmful than phenytoin, barbiturates or valproic acid. Bromides, gabapentin, and vigabatrin are safe.
70 Attacks should be treated with either carbohydrate loading or hemin, both of which repress hepatic delta aminolevulinic acid synthase (ALAS1) and are considered specific therapies. Glucose and other carbohydrates reduce porphyrin precursor excretion, but the effects are weak compared with those of hemin. Therefore, only attacks with mild pain and without severe manifestations (eg, no paresis or hyponatremia present) should be treated with carbohydrate loading
71 An adequate intake of calories should be ensured, given orally as carbohydrate-rich food supplements (more than half of energy intake), or infused as normal saline with 5-10% dextrose when the patient has severe vomiting. Intravenous treatment with 300 to 500 grams of intravenous glucose is recommended. You are really driving mild hyperglycemia in that patient to help reverse the process.
72 Intravenous haemin administration, which inhibits upregulated ALAS1 and curtails urinary excretion of 5- aminolaevulinic acid and porphobilinogen, is the specific (or aetiopathogenic) treatment of choice. Most patients with uncomplicated attacks improve within 5 days. Measurement of urinary porphobilinogen excretion is useful to document the metabolic response to human haemin.
73 When infused intravenously, these heme preparations become bound mostly to circulating albumin as heme albumin. These are taken up primarily by hepatocytes, where the heme component reconstitutes the regulatory heme pool. This leads to repression of the synthesis of hepatic ALAS1, followed by dramatic reductions in ALA and PBG in plasma and urine.
74 However, human haemin will not reverse an established neuropathy, but might prevent neuropathy onset and halt further progression if given sufficiently early. A stable preparation of human haemin solution stabilised with arginine (Normosang) is widely available, whereas in the USA a form of lyophilised haemin (Panhaematin) is available.
75 Coagulopathies reported with other haem preparations do not develop with stabilised haemin with arginine. Administration after 1:1 dilution in 4 20% human serum albumin increases haem solubility and stability and lowers the risk of vein injury.
76 The standard regimen for the acute attack is 3 to 4 mg/kg of hemin daily for four days. Treatment may be extended if a response is not observed within this time. Hemin prophylactically administered once or twice weekly can prevent frequent, non-cyclic attacks of porphyria in some patients Hemin has been administered safely during pregnancy Subacute or chronic symptoms are unlikely to respond to this agent.
77 Attacks during pregnancy have been treated without any apparent adverse effects to either mother or child. Management of repeated attacks that are severe enough to need admission is difficult, and long-term treatment with human haemin is needed. Regular treatment with a once-per-week single dose can help to control the disease.
78 The most frequently reported event after several courses of haem therapy is the disappearence of the superficial venous system. Most of these patients will probably need permanent indwelling venous catheters, which have many attendant complications.
79 A single dose of human haemin contains 22.7 mg of iron. Therefore, iron overload is possible in patients who are given regular doses. The patient may require a liver biopsy down the road, depending on what their total iron exposure is.
80 Side effects of hemin: Infusion site phlebitis other side effect are uncommon and have included fever, aching, malaise, hemolysis, anaphylaxis, and circulatory collapse Excessive dosing caused reversible acute renal tubular damage in one case Some patients treated repeatedly with hemin have developed iron overload. Therefore, serum ferritin should be monitored and small-volume phlebotomies considered during remission, with a goal to normalize serum ferritin levels into the range of 100 to 200 ng/ml. Phlebotomyinduced iron deficiency should be avoided.
81 5-aminolaevulinic acid or other metabolites that are overproduced by the liver are neurotoxic, and this notion is consistent with the substantial benefit of liver transplantation in patients with severe acute intermittent porphyria.
82 A few patients with severe acute intermittent porphyria have received liver transplants. This intervention returns 5-aminolaevulinic acid and porphobilinogen excretion to normal, abolishes acute attacks, and improves quality of life. Thus, liver transplantation should be considered for selected patients with the most severe form of acute intermittent porphyria.

83

84
85 Other therapies : Uncontrolled observations in small numbers of patients suggest that cimetidine is a cost-effective alternative to hemin for treating acute attacks. Cimetidine inhibits hepatic CYPs, and can prevent experimental forms of porphyria induced by chemicals that are activated by CYPs However, chemicals activated by CYPs are rarely, if ever, implicated in human AIP. Therefore, cimetidine cannot be recommended as an alternative to hemin.
86 If present, iron deficiency, which at least theoretically might further impair heme synthesis, should be corrected. Frequently recurring attacks confined to the luteal phase of the menstrual cycle can be prevented with a GnRH analogue. If treatment is effective after several months, low-dose estradiol, preferably by the transdermal route, or a bisphosphonate may be added to prevent bone loss and other side effects, or treatment changed to a low-dose oral contraceptive.
87 In patients with acute porphyrias who have episodes that are worsened during the luteal phase of their menstrual period, a GnRH analog for a period of 2-3 months is often helpful in decreasing the number of episodes that a patient may have. GnRH analogs have been helpful in reducing attacks in patients with cyclical attacks.
88
89 Carriers of the gene defect, symptomatic or not, should be counselled about maintenance of a healthy diet with regular meals, avoidance of alcohol and smoking, and use of the list of potentially safe and unsafe drugs.
90 Finally, patients with both symptomatic and latent disease have increased risks of hypertension and chronic renal failure. I would just add to that that for not very wellunderstood reasons, usually not due to secondary iron overload, these people are at increased risk of developing chronic liver disease, cirrhosis, and hepatocellular carcinoma.
91 Cutaneous porphyrias Cutaneous porphyrias are associated with : photosensitivity due to activation of porphyrins in the skin by visible and long wave ultraviolet light (also known as UV-A). Most cutaneous porphyrias are manifested by chronic blistering skin lesions on sun-exposed areas of the skin, particularly the backs of the hands. If severe, these may become infected and mutilating.

92

93
Clinical diagnosis? AIP (Acute Intermittent Porphyria)
") Case 1 18 yo woman came to ER with a 5-day history of severe abdominal pain Localized, intermittent, sharp, epigastric and periumbilical pain associated with mild nausea but no vomiting for the past 6
Case 1 18 yo woman came to ER with a 5-day history of severe abdominal pain Localized, intermittent, sharp, epigastric and periumbilical pain associated with mild nausea but no vomiting for the past 6
ACUTE PORPHYRIAS: EMERGENCY ROOM RECOMMENDATIONS
 ACUTE PORPHYRIAS: EMERGENCY ROOM RECOMMENDATIONS Neville R Pimstone MD, PhD Gastroenterology/Hepatology, Head Liver Diseases Greater West Los Angeles Veterans Affairs, and Professor Emeritus UC Davis Karl
ACUTE PORPHYRIAS: EMERGENCY ROOM RECOMMENDATIONS Neville R Pimstone MD, PhD Gastroenterology/Hepatology, Head Liver Diseases Greater West Los Angeles Veterans Affairs, and Professor Emeritus UC Davis Karl
Acute Porphyria. Penelope Stein Haematological Medicine, King s College Hospital, London
 Acute Porphyria Penelope Stein Haematological Medicine, King s College Hospital, London Why is acute porphyria important? Easy to miss - rare, non-specific presentation Severe attacks may be life-threatening
Acute Porphyria Penelope Stein Haematological Medicine, King s College Hospital, London Why is acute porphyria important? Easy to miss - rare, non-specific presentation Severe attacks may be life-threatening
PORPHYRINS AND PORPHYRIN DISORDERS
 1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY ` CLINICAL BIOCHEMISTRY FOR BMLT 3 & BDS 4 PORPHYRINS AND PORPHYRIN DISORDERS
1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY ` CLINICAL BIOCHEMISTRY FOR BMLT 3 & BDS 4 PORPHYRINS AND PORPHYRIN DISORDERS
Iron deficiency anemia and porphyrias
 Iron deficiency anemia and porphyrias Fleur Wolff¹, Frédéric Cotton¹, Axelle Gilles² ¹Department of clinical chemistry, Hôpital Erasme, ULB ²Department of hematology, Hôpital Erasme, ULB BHS, November
Iron deficiency anemia and porphyrias Fleur Wolff¹, Frédéric Cotton¹, Axelle Gilles² ¹Department of clinical chemistry, Hôpital Erasme, ULB ²Department of hematology, Hôpital Erasme, ULB BHS, November
Directorate of Laboratory Medicine Blood Sciences Page 1 of 7 BS-CTG-Biochem-25 Revision Version: 1
 Blood Sciences Page 1 of 7 BS-CTG-Biochem-25 Revision Version: 1 SELECTING TESTS FOR THE INVESTIGATION OF THE PORPHYRIAS 1. INTRODUCTION The s are a group of disorders of haem synthesis that can present
Blood Sciences Page 1 of 7 BS-CTG-Biochem-25 Revision Version: 1 SELECTING TESTS FOR THE INVESTIGATION OF THE PORPHYRIAS 1. INTRODUCTION The s are a group of disorders of haem synthesis that can present
Presentations associated with porphyrias in intensive care units
 ICU ROUNDS Presentations associated with porphyrias in intensive care units Doungporn Ruthirago MD, Parunyou Julayanont MD, Supannee Rassameehiran MD ABSTRACT Porphyrias are a group of uncommon congenital
ICU ROUNDS Presentations associated with porphyrias in intensive care units Doungporn Ruthirago MD, Parunyou Julayanont MD, Supannee Rassameehiran MD ABSTRACT Porphyrias are a group of uncommon congenital
There are four types of acute porphyrias:
 www.thinkporphyria.com.au Acute porphyrias manifest as intermittent clinical presentations known as the acute porphyria attack. Failure to recognise an acute attack may lead to complications, and in some
www.thinkporphyria.com.au Acute porphyrias manifest as intermittent clinical presentations known as the acute porphyria attack. Failure to recognise an acute attack may lead to complications, and in some
Concise Review for Primary-Care Physicians
 Concise Review for Primary-Care Physicians Acute Porphyrias: Diagnosis and Management AYALEW TEFFERI, M.D., JOSEPH P. COLGAN, M.D., AND LAWRENCE A. SOLBERG, JR., M.D. To summarize recent information about
Concise Review for Primary-Care Physicians Acute Porphyrias: Diagnosis and Management AYALEW TEFFERI, M.D., JOSEPH P. COLGAN, M.D., AND LAWRENCE A. SOLBERG, JR., M.D. To summarize recent information about
The acute porphyrias are well-defined genetic disorders
 Review Recommendations for the Diagnosis and Treatment of the Acute Porphyrias Karl E. Anderson, MD; Joseph R. Bloomer, MD; Herbert L. Bonkovsky, MD; James P. Kushner, MD; Claus A. Pierach, MD; Neville
Review Recommendations for the Diagnosis and Treatment of the Acute Porphyrias Karl E. Anderson, MD; Joseph R. Bloomer, MD; Herbert L. Bonkovsky, MD; James P. Kushner, MD; Claus A. Pierach, MD; Neville
2013 OTS Annual Meeting Pre-clinical Development of ALN-AS1 RNAi Therapeutic for the Treatment of Acute Intermittent Porphyria.
 2013 OTS Annual Meeting Pre-clinical Development of ALN-AS1 RNAi Therapeutic for the Treatment of Acute Intermittent Porphyria October 8, 2013 Acute Intermittent Porphyria (AIP) Program Unmet Need and
2013 OTS Annual Meeting Pre-clinical Development of ALN-AS1 RNAi Therapeutic for the Treatment of Acute Intermittent Porphyria October 8, 2013 Acute Intermittent Porphyria (AIP) Program Unmet Need and
Porphyrias. Thomas A. Kruzel, N D
 Porphyrias Thomas A. Kruzel, N D Until recently, cases of porphyrias have been considered rare. It has only been within the past decade or so that an increasing number of patients have been diagnosed with
Porphyrias Thomas A. Kruzel, N D Until recently, cases of porphyrias have been considered rare. It has only been within the past decade or so that an increasing number of patients have been diagnosed with
Fatal Neurological Manifestations of Acute Intermittent Porphyria
 Bahrain Medical Bulletin, Vol.26, No. 2, June 2004 Fatal Neurological Manifestations of Acute Intermittent Porphyria Adel A Al Jishi, FRCPI* Sreekantaswamy, MD, DM(Neurology)** Three patients of acute
Bahrain Medical Bulletin, Vol.26, No. 2, June 2004 Fatal Neurological Manifestations of Acute Intermittent Porphyria Adel A Al Jishi, FRCPI* Sreekantaswamy, MD, DM(Neurology)** Three patients of acute
Research Article Clinical and Laboratory Features of Acute Porphyria: A Study of 36 Subjects in a Chinese Tertiary Referral Center
 BioMed Research International Volume 2016, Article ID 3927635, 5 pages http://dx.doi.org/10.1155/2016/3927635 Research Article Clinical and Laboratory Features of Acute Porphyria: A Study of 36 Subjects
BioMed Research International Volume 2016, Article ID 3927635, 5 pages http://dx.doi.org/10.1155/2016/3927635 Research Article Clinical and Laboratory Features of Acute Porphyria: A Study of 36 Subjects
الفريق االكاديمي الطبي HLS/ Biochemistry Sheet Porphyrin and Heme metabolism By: Shatha Khtoum
 الفريق االكاديمي الطبي HLS/ Biochemistry Sheet Porphyrin and Heme metabolism By: Shatha Khtoum اا Today we will take about heme metabolism: -Heme is iron (Fe +2 ) with 4 pyrrole rings. -Its function it
الفريق االكاديمي الطبي HLS/ Biochemistry Sheet Porphyrin and Heme metabolism By: Shatha Khtoum اا Today we will take about heme metabolism: -Heme is iron (Fe +2 ) with 4 pyrrole rings. -Its function it
Acute porphyrias : Diagnosis, complications and treatment options
 Porphyrins & Porphyrias / Patients Day Lucerne, May 18 th, 2013 Acute porphyrias : Diagnosis, complications and treatment options Pr Jean-Charles Deybach, MD, PhD Centre National Maladies Rares Porphyries
Porphyrins & Porphyrias / Patients Day Lucerne, May 18 th, 2013 Acute porphyrias : Diagnosis, complications and treatment options Pr Jean-Charles Deybach, MD, PhD Centre National Maladies Rares Porphyries
PORPHYRIAS (Vampires and Crazy Kings)
") PORPHYRIAS (Vampires and Crazy Kings) Urs A. Meyer Biozentrum of the University of Basel CH-4056 Basel, Switzerland www.biozentrum.unibas.ch/meyer.html Falk Symposium No.156, Genetics in Liver Diseases
PORPHYRIAS (Vampires and Crazy Kings) Urs A. Meyer Biozentrum of the University of Basel CH-4056 Basel, Switzerland www.biozentrum.unibas.ch/meyer.html Falk Symposium No.156, Genetics in Liver Diseases
Variegate porphyria: an unusual cause of skin blistering
 H.K. Dermatol. Venereol. Bull. (2003) 11, 20-24 Case Report Variegate porphyria: an unusual cause of skin blistering Variegate porphyria (VP) is an autosomal dominant disorder caused by a partial deficiency
H.K. Dermatol. Venereol. Bull. (2003) 11, 20-24 Case Report Variegate porphyria: an unusual cause of skin blistering Variegate porphyria (VP) is an autosomal dominant disorder caused by a partial deficiency
Clinical Issues in AIP: When to Suspect and How to Proceed CME/CE
 Clinical Issues in AIP: When to Suspect and How to Proceed CME/CE Supported by an independent educational grant from Recordati Rare Diseases. Clinical Issues in AIP: When to Suspect and How to Proceed
Clinical Issues in AIP: When to Suspect and How to Proceed CME/CE Supported by an independent educational grant from Recordati Rare Diseases. Clinical Issues in AIP: When to Suspect and How to Proceed
therapy and with normal erythrocyte porphobilinogen
 Br. J. clin. Pharmac. (1989), 27, 491-497 Acute intermittent porphyria in two patients on anticonvulsant therapy and with normal erythrocyte porphobilinogen deaminase activity A. L. HERRICK, K. E. L. McCOLL,
Br. J. clin. Pharmac. (1989), 27, 491-497 Acute intermittent porphyria in two patients on anticonvulsant therapy and with normal erythrocyte porphobilinogen deaminase activity A. L. HERRICK, K. E. L. McCOLL,
Citation Acta Medica Nagasakiensia. 1992, 37
 NAOSITE: Nagasaki University's Ac Title Author(s) An Autopsy Case of Acute Intermitte Murase, Kunihiko; Makiyama, Kazuya; Nonaka, Shigeru Citation Acta Medica Nagasakiensia. 1992, 37 Issue Date 1992-12-25
NAOSITE: Nagasaki University's Ac Title Author(s) An Autopsy Case of Acute Intermitte Murase, Kunihiko; Makiyama, Kazuya; Nonaka, Shigeru Citation Acta Medica Nagasakiensia. 1992, 37 Issue Date 1992-12-25
Clinical indications for the investigation of porphyria: case examples and evolving laboratory approaches to its diagnosis in New Zealand
 Vol 118 No 1222 ISSN 1175 8716 Clinical indications for the investigation of porphyria: case examples and evolving laboratory approaches to its diagnosis in New Zealand Christiaan Sies, Christopher Florkowski,
Vol 118 No 1222 ISSN 1175 8716 Clinical indications for the investigation of porphyria: case examples and evolving laboratory approaches to its diagnosis in New Zealand Christiaan Sies, Christopher Florkowski,
Case Report Feigning Acute Intermittent Porphyria
 Case Reports in Psychiatry, Article ID 152821, 4 pages http://dx.doi.org/10.1155/2014/152821 Case Report Feigning Acute Intermittent Porphyria Rania Elkhatib, 1 Modupe Idowu, 2 Gregory S. Brown, 3 Yasmeen
Case Reports in Psychiatry, Article ID 152821, 4 pages http://dx.doi.org/10.1155/2014/152821 Case Report Feigning Acute Intermittent Porphyria Rania Elkhatib, 1 Modupe Idowu, 2 Gregory S. Brown, 3 Yasmeen
When mixed as directed with Sterile Water for Injection, USP, each 48 ml provides the equivalent of approximately 336 mg hematin (7 mg/ml).
.") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use PANHEMATIN safely and effectively. See full prescribing information for PANHEMATIN. PANHEMATIN (hemin
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use PANHEMATIN safely and effectively. See full prescribing information for PANHEMATIN. PANHEMATIN (hemin
Porphyrias in Japan. Epidemiological Statistics of Porphyrias
 Porphyrias in Japan Masao Kondo,a Yuzo Yanob "Department of Nutrition and Biochemistry, The Institute of Public Health, Tokyo, Japan; btokyo Metropolitan Toshima General Hospital, Tokyo, Japan Key Words.
Porphyrias in Japan Masao Kondo,a Yuzo Yanob "Department of Nutrition and Biochemistry, The Institute of Public Health, Tokyo, Japan; btokyo Metropolitan Toshima General Hospital, Tokyo, Japan Key Words.
BIOCHEMISTRY LECTURE BY OJEMEKELE O. BLOOD CHEMISTRY; BLOOD AS A TISSUE AND PORPHYRINS
 BIOCHEMISTRY LECTURE BY OJEMEKELE O. BLOOD CHEMISTRY; BLOOD AS A TISSUE AND PORPHYRINS BLOOD AS A TISSUE Blood is a liquid connective tissue The total blood volume makes up about 6-8 percent of the body
BIOCHEMISTRY LECTURE BY OJEMEKELE O. BLOOD CHEMISTRY; BLOOD AS A TISSUE AND PORPHYRINS BLOOD AS A TISSUE Blood is a liquid connective tissue The total blood volume makes up about 6-8 percent of the body
Research Institute, NC, USA. Journal of Exploratory Research in Pharmacology 2017 vol
 Review Article Pathophysiology, Pharmacology and Treatment of Acute Intermittent Porphyria: A Patient Case Description and Recommendations from the Current Literature Teminioluwa Ajayi 1, Rachael Ward
Review Article Pathophysiology, Pharmacology and Treatment of Acute Intermittent Porphyria: A Patient Case Description and Recommendations from the Current Literature Teminioluwa Ajayi 1, Rachael Ward
LATE ACUTE INTERMITTENT PORPHYRIA ATTACK IN A PATIENT WITH TYPE 2 DIABETES
 2015 ILEX PUBLISHING HOUSE, Bucharest, Roumania http://www.jrdiabet.ro Rom J Diabetes Nutr Metab Dis. 22(2):125-131 doi: 10.1515/rjdnmd-2015-0016 LATE ACUTE INTERMITTENT PORPHYRIA ATTACK IN A PATIENT WITH
2015 ILEX PUBLISHING HOUSE, Bucharest, Roumania http://www.jrdiabet.ro Rom J Diabetes Nutr Metab Dis. 22(2):125-131 doi: 10.1515/rjdnmd-2015-0016 LATE ACUTE INTERMITTENT PORPHYRIA ATTACK IN A PATIENT WITH
The Atkins Diet as a Possible Trigger for an ICU Admission: A Case Report
 The Atkins Diet as a Possible Trigger for an ICU Admission: A Case Report J. F. FRASER, P. LONGDEN Intensive Care Unit, St Andrew s Hospital, Toowoomba, QUEENSLAND ABSTRACT A case of initial presentation
The Atkins Diet as a Possible Trigger for an ICU Admission: A Case Report J. F. FRASER, P. LONGDEN Intensive Care Unit, St Andrew s Hospital, Toowoomba, QUEENSLAND ABSTRACT A case of initial presentation
M0BCore Safety Profile
 M0BCore Safety Profile Active substance: Aciclovir Pharmaceutical form(s)/strength: Tablets 200, 400 or 800 mg Dispersible tablets 200, 400 or 800 mg Oral suspensions 200 mg or 400 mg per 5 ml. Freeze
M0BCore Safety Profile Active substance: Aciclovir Pharmaceutical form(s)/strength: Tablets 200, 400 or 800 mg Dispersible tablets 200, 400 or 800 mg Oral suspensions 200 mg or 400 mg per 5 ml. Freeze
SUMMARY OF PRODUCT CHARACTERISTICS. Human hemin mg/ml. One ampoule of 10 ml contains 250 mg human hemin.
 SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Normosang 25 mg/ml, concentrate for solution for infusion. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Human hemin... 25 mg/ml. One ampoule
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Normosang 25 mg/ml, concentrate for solution for infusion. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Human hemin... 25 mg/ml. One ampoule
Doaa Kotkot. Somaya Alkiswani. Nayef
 6 Doaa Kotkot Somaya Alkiswani Nayef Heme Synthesis In the previous lecture we talked about heme synthesis and we said that the rate limiting step is the condensation of Glycine + Succinyl CoA to produce
6 Doaa Kotkot Somaya Alkiswani Nayef Heme Synthesis In the previous lecture we talked about heme synthesis and we said that the rate limiting step is the condensation of Glycine + Succinyl CoA to produce
Family evaluations in acute intermittent porphyria using red cell uroporphyrinogen I synthetasel
 Journal of Medical Genetics, 1979, 16, 134-139 Family evaluations in acute intermittent porphyria using red cell uroporphyrinogen I synthetasel JOEL M. LAMON, BRUCE C. FRYKHOLM, AND DONALD P. TCHUDY From
Journal of Medical Genetics, 1979, 16, 134-139 Family evaluations in acute intermittent porphyria using red cell uroporphyrinogen I synthetasel JOEL M. LAMON, BRUCE C. FRYKHOLM, AND DONALD P. TCHUDY From
Communiqué. The Challenges of Testing For and Diagnosing Porphyrias
 Communiqué November 2002 AVolume 27 Number 11 Features The Challenges of Testing For and Diagnosing Porphyrias Inside Ask Us Abstracts of Interest Calendar Test Updates: Cobalt Serum Specimen Correction
Communiqué November 2002 AVolume 27 Number 11 Features The Challenges of Testing For and Diagnosing Porphyrias Inside Ask Us Abstracts of Interest Calendar Test Updates: Cobalt Serum Specimen Correction
Nursing Process Focus: Patients Receiving Dextran 40 (Gentran 40)
") Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
Assess for presence/history of hypovolemia, shock, venous thrombosis. Assess vital signs: Hypovolemic shock secondary to surgery, burns, hemorrhage, other serious condition PT and PTT abnormalities Venous
DOWNLOAD PDF DIAGNOSIS AND THERAPY OF PORPHYRIAS AND LEAD INTOXICATION
 Chapter 1 : Porphyria - Wikipedia Diagnosis and Therapy of Porphyrias and Lead Intoxication and millions of other books are available for Amazon Kindle. Learn more Enter your mobile number or email address
Chapter 1 : Porphyria - Wikipedia Diagnosis and Therapy of Porphyrias and Lead Intoxication and millions of other books are available for Amazon Kindle. Learn more Enter your mobile number or email address
number Done by Corrected by Doctor Diala
 number 36 Done by Baraa Ayed Corrected by Moath Darweesh Doctor Diala 1 P a g e Today we are going to cover these concepts: Porphyrin structure Biosynthesis of Heme Regulation of heme synthesis A clinical
number 36 Done by Baraa Ayed Corrected by Moath Darweesh Doctor Diala 1 P a g e Today we are going to cover these concepts: Porphyrin structure Biosynthesis of Heme Regulation of heme synthesis A clinical
SAFE USE OF PERAMPANEL IN A CARRIER OF VARIEGATE PORPHYRIA: A CASE REPORT
 SAFE USE OF PERAMPANEL IN A CARRIER OF VARIEGATE PORPHYRIA: A CASE REPORT S Balestrini 1-2, Y Hart 3, S Thunell 4, SM Sisodiya 1 1 NIHR University College London Hospitals Biomedical Research Centre, Department
SAFE USE OF PERAMPANEL IN A CARRIER OF VARIEGATE PORPHYRIA: A CASE REPORT S Balestrini 1-2, Y Hart 3, S Thunell 4, SM Sisodiya 1 1 NIHR University College London Hospitals Biomedical Research Centre, Department
Hematopoiesis, The hematopoietic machinery requires a constant supply iron, vitamin B 12, and folic acid.
 Hematopoiesis, 200 billion new blood cells per day The hematopoietic machinery requires a constant supply iron, vitamin B 12, and folic acid. hematopoietic growth factors, proteins that regulate the proliferation
Hematopoiesis, 200 billion new blood cells per day The hematopoietic machinery requires a constant supply iron, vitamin B 12, and folic acid. hematopoietic growth factors, proteins that regulate the proliferation
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING
 AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
AUTOIMMUNE DISORDERS IN THE ACUTE SETTING Diagnosis and Treatment Goals Aimee Borazanci, MD BNI Neuroimmunology Objectives Give an update on the causes for admission, clinical features, and outcomes of
Open-Label Study of Hemin for Acute Porphyria: Clinical Practice Implications
 The American Journal of Medicine (2006) 119, 801.e19-801.e24 CLINICAL RESEARCH STUDY AJM Theme Issue: GI and Nutrition Open-Label Study of Hemin for Acute Porphyria: Clinical Practice Implications Karl
The American Journal of Medicine (2006) 119, 801.e19-801.e24 CLINICAL RESEARCH STUDY AJM Theme Issue: GI and Nutrition Open-Label Study of Hemin for Acute Porphyria: Clinical Practice Implications Karl
How could I be having migraine when I don't have a headache?
 Migraine Your doctor thinks you may have migraine. Classic migraine attacks start with visual symptoms (often zig-zag colored lights or flashes of light expanding to one side over 10-30 minutes) followed
Migraine Your doctor thinks you may have migraine. Classic migraine attacks start with visual symptoms (often zig-zag colored lights or flashes of light expanding to one side over 10-30 minutes) followed
Dr. M. Fathima Riswana IIyrMD MII & Hematology Dept, ICH & HC Prof.Dr.S.Sundari Prof.Dr.V.Thilagavathy
 Dr. M. Fathima Riswana IIyrMD MII & Hematology Dept, ICH & HC Prof.Dr.S.Sundari Prof.Dr.V.Thilagavathy History 1yr old male child, 1st born of 3rd degree consanguineous marriage with c/o abdominal distension
Dr. M. Fathima Riswana IIyrMD MII & Hematology Dept, ICH & HC Prof.Dr.S.Sundari Prof.Dr.V.Thilagavathy History 1yr old male child, 1st born of 3rd degree consanguineous marriage with c/o abdominal distension
COMPOSITION. A film coated tablet contains. Active ingredient: irbesartan 75 mg, 150 mg or 300 mg. Rotazar (Film coated tablets) Irbesartan
 Irbesartan") Rotazar (Film coated tablets) Irbesartan Rotazar 75 mg, 150 mg, 300 mg COMPOSITION A film coated tablet contains Active ingredient: irbesartan 75 mg, 150 mg or 300 mg. Rotazar 75 mg, 150 mg, 300 mg PHARMACOLOGICAL
Rotazar (Film coated tablets) Irbesartan Rotazar 75 mg, 150 mg, 300 mg COMPOSITION A film coated tablet contains Active ingredient: irbesartan 75 mg, 150 mg or 300 mg. Rotazar 75 mg, 150 mg, 300 mg PHARMACOLOGICAL
Each tablet contains:
 Composition: Each tablet contains: Tolvaptan 15/30mg Pharmacokinetic properties: In healthy subjects the pharmacokinetics of tolvaptan after single doses of up to 480 mg and multiple doses up to 300 mg
Composition: Each tablet contains: Tolvaptan 15/30mg Pharmacokinetic properties: In healthy subjects the pharmacokinetics of tolvaptan after single doses of up to 480 mg and multiple doses up to 300 mg
Drug Interactions Lisa Armitige, MD, PhD November 17, 2010
 Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Substance Abuse and Tuberculosis Oklahoma City, Oklahoma November 17, 2010 Drug Interactions Lisa Armitige, MD, PhD November 17, 2010 Drug Interactions Lisa Y. Armitige, M.D., Ph.D. Medical Consultant
Dosing, preparation, and infusion instructions
 Dosing, preparation, and infusion instructions About PANHEMATIN PANHEMATIN is supplied as a sterile, lyophilized, black powder in single-dose dispensing vials containing 350 mg hemin, 240 mg sodium carbonate,
Dosing, preparation, and infusion instructions About PANHEMATIN PANHEMATIN is supplied as a sterile, lyophilized, black powder in single-dose dispensing vials containing 350 mg hemin, 240 mg sodium carbonate,
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY
 1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL SEMINAR: SEX HORMONES PART 1 An Overview What are steroid hormones? Steroid
1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY & MOLECULAR BIOLOGY PBL SEMINAR: SEX HORMONES PART 1 An Overview What are steroid hormones? Steroid
Case Challenges in Acute Intermittent Porphyria CME
 Case Challenges in Acute Intermittent Porphyria CME Supported by an independent educational grant from Recordati Rare Diseases 1 This article is a CME activity. To earn credit for this activity visit:
Case Challenges in Acute Intermittent Porphyria CME Supported by an independent educational grant from Recordati Rare Diseases 1 This article is a CME activity. To earn credit for this activity visit:
Basic Biopharmaceutics, Pharmacokinetics, and Pharmacodynamics
 Basic Biopharmaceutics, Pharmacokinetics, and Pharmacodynamics Learning Outcomes Define biopharmaceutics Describe 4 processes of pharmacokinetics Describe factors that affect medication absorption Describe
Basic Biopharmaceutics, Pharmacokinetics, and Pharmacodynamics Learning Outcomes Define biopharmaceutics Describe 4 processes of pharmacokinetics Describe factors that affect medication absorption Describe
BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel
 BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel Protocol Code Tumour Group Contact Physician UGOOVBEVP Gynecologic Oncology Dr. Anna Tinker
BC Cancer Protocol for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and PACLitaxel Protocol Code Tumour Group Contact Physician UGOOVBEVP Gynecologic Oncology Dr. Anna Tinker
IV Fluids. I.V. Fluid Osmolarity Composition 0.9% NaCL (Normal Saline Solution, NSS) Uses/Clinical Considerations
 Uses/Clinical Considerations") IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
IV Fluids When administering IV fluids, the type and amount of fluid may influence patient outcomes. Make sure to understand the differences between fluid products and their effects. Crystalloids Crystalloid
YEAR III Pharm.D Dr. V. Chitra
 YEAR III Pharm.D Dr. V. Chitra Anemia can be defined as a reduction in the hemoglobin,hematocrit or red cell number. In physiologic terms an anemia is any disorder in which the patient suffers from tissue
YEAR III Pharm.D Dr. V. Chitra Anemia can be defined as a reduction in the hemoglobin,hematocrit or red cell number. In physiologic terms an anemia is any disorder in which the patient suffers from tissue
GLUCOSE TESTING-BLOOD
 648.83 ABNORMAL GLUCOSE TOLERANCE COMPLICATING PREGNANCY, CHILDBIRTH OR THE PUERPERIUM, ANTEPARTUM CONDITION OR 648.84 ABNORMAL GLUCOSE TOLERANCE COMPLICATING PREGNANCY, CHILDBIRTH OR THE PUERPERIUM, POSTPARTUM
648.83 ABNORMAL GLUCOSE TOLERANCE COMPLICATING PREGNANCY, CHILDBIRTH OR THE PUERPERIUM, ANTEPARTUM CONDITION OR 648.84 ABNORMAL GLUCOSE TOLERANCE COMPLICATING PREGNANCY, CHILDBIRTH OR THE PUERPERIUM, POSTPARTUM
BC Cancer Protocol Summary for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and Vinorelbine
 BC Cancer Protocol Summary for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and Vinorelbine Protocol Code Tumour Group Contact Physician UGOOVBEVV Gynecologic Oncology Dr.
BC Cancer Protocol Summary for Treatment of Platinum Resistant Epithelial Ovarian Cancer with Bevacizumab and Vinorelbine Protocol Code Tumour Group Contact Physician UGOOVBEVV Gynecologic Oncology Dr.
Neither activated charcoal nor whole bowel irrigation (WBI) is indicated in the routine management of acute or chronic lithium toxicity.
 is indicated in the routine management of acute or chronic lithium toxicity.") CRACKCast E160 Lithium Key concepts; The clinical pattern of acute and chronic toxicity is different. Gastrointestinal symptoms occur early and neurological toxicity manifest late in acute toxicity. Neurological
CRACKCast E160 Lithium Key concepts; The clinical pattern of acute and chronic toxicity is different. Gastrointestinal symptoms occur early and neurological toxicity manifest late in acute toxicity. Neurological
Immodium / loprarmide
 Immodium / loprarmide IMODIUM (loperamide hydrochloride) is indicated for the control and symptomatic relief of acute nonspecific diarrhea and of chronic diarrhea associated with inflammatory bowel disease.
Immodium / loprarmide IMODIUM (loperamide hydrochloride) is indicated for the control and symptomatic relief of acute nonspecific diarrhea and of chronic diarrhea associated with inflammatory bowel disease.
PHENTOLAMINE MESYLATE INJECTION SANDOZ STANDARD 5 mg/ ml THERAPEUTIC CLASSIFICATION Alpha-adrenoreceptor Blocker
 PACKAGE INSERT Pr PHENTOLAMINE MESYLATE INJECTION SANDOZ STANDARD 5 mg/ ml THERAPEUTIC CLASSIFICATION Alpha-adrenoreceptor Blocker ACTIONS AND CLINICAL PHARMACOLOGY Phentolamine produces an alpha-adrenergic
PACKAGE INSERT Pr PHENTOLAMINE MESYLATE INJECTION SANDOZ STANDARD 5 mg/ ml THERAPEUTIC CLASSIFICATION Alpha-adrenoreceptor Blocker ACTIONS AND CLINICAL PHARMACOLOGY Phentolamine produces an alpha-adrenergic
DBL MAGNESIUM SULFATE CONCENTRATED INJECTION
 DBL MAGNESIUM SULFATE CONCENTRATED INJECTION NAME OF MEDICINE Magnesium Sulfate BP DESCRIPTION DBL Magnesium Sulfate Concentrated Injection is a clear, colourless, sterile solution. Each ampoule contains
DBL MAGNESIUM SULFATE CONCENTRATED INJECTION NAME OF MEDICINE Magnesium Sulfate BP DESCRIPTION DBL Magnesium Sulfate Concentrated Injection is a clear, colourless, sterile solution. Each ampoule contains
Woman in Acute Abdominal Pain: What s the Diagnosis? CME / ABIM MOC / CE
 http://medscape.org/case/porphyria Woman in Acute Abdominal Pain: What s the Diagnosis? CME / ABIM MOC / CE Supported by an independent educational grant from Recordati Rare Diseases http://medscape.org/case/porphyria
http://medscape.org/case/porphyria Woman in Acute Abdominal Pain: What s the Diagnosis? CME / ABIM MOC / CE Supported by an independent educational grant from Recordati Rare Diseases http://medscape.org/case/porphyria
Acute Intermittent Porphyria: Psychosis as the Only Clinical Manifestation
 Isr J Psychiatry Relat Sci Vol 43 No. 1 (2006) 52 56 Acute Intermittent Porphyria: Psychosis as the Only Clinical Manifestation Natalie Ellencweig, MD, 1 Nili Schoenfeld, PhD, 2,3 and Zvi Zemishlany, MD
Isr J Psychiatry Relat Sci Vol 43 No. 1 (2006) 52 56 Acute Intermittent Porphyria: Psychosis as the Only Clinical Manifestation Natalie Ellencweig, MD, 1 Nili Schoenfeld, PhD, 2,3 and Zvi Zemishlany, MD
TNF Receptor Associated Periodic Syndrome (TRAPS)
") https://www.printo.it/pediatric-rheumatology/gb/intro TNF Receptor Associated Periodic Syndrome (TRAPS) Version of 2016 1. WHAT IS TRAPS 1.1 What is it? TRAPS is an inflammatory disease characterised by
https://www.printo.it/pediatric-rheumatology/gb/intro TNF Receptor Associated Periodic Syndrome (TRAPS) Version of 2016 1. WHAT IS TRAPS 1.1 What is it? TRAPS is an inflammatory disease characterised by
MIGRAINE A MYSTERY HEADACHE
 MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
MIGRAINE A MYSTERY HEADACHE The migraine is a chronic neurological disease that is characterized by moderate to severe episodes of headache that is mostly associated with other central nervous system (CNS)
New Zealand Datasheet
 New Zealand Datasheet Name of Medicine ONREX Tablets Ondansetron hydrochloride dihydrate tablets 4mg and 8mg. Presentation ONREX tablets 4 mg: White, circular, biconvex, film coated tablet debossed with
New Zealand Datasheet Name of Medicine ONREX Tablets Ondansetron hydrochloride dihydrate tablets 4mg and 8mg. Presentation ONREX tablets 4 mg: White, circular, biconvex, film coated tablet debossed with
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE. Jules B. Puschett, M.D.
 DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
DIAGNOSIS AND MANAGEMENT OF DIURETIC RESISTANCE Jules B. Puschett, M.D. Diuretic Resistance A clinical circumstance in which patients do not respond to a combination of salt restriction and even large
Laboratory tests in emergency medicine. Dr O Kiabilua Block SA 13 Department of Chemical Pathology University of Pretoria
 Laboratory tests in emergency medicine Dr O Kiabilua Block SA 13 Department of Chemical Pathology University of Pretoria Acute abdomen The diagnosis depends : The clinical examination, Experience of the
Laboratory tests in emergency medicine Dr O Kiabilua Block SA 13 Department of Chemical Pathology University of Pretoria Acute abdomen The diagnosis depends : The clinical examination, Experience of the
TIP Paclitaxel, Ifosfamide and Cisplatin
 Systemic Anti Cancer Treatment Protocol TIP Paclitaxel, Ifosfamide and Cisplatin PROTOCOL REF: MPHATIPGC (Version No: 1.0) Approved for use in: Second line treatment of germ cell tumours Dosage: Drug Dosage
Systemic Anti Cancer Treatment Protocol TIP Paclitaxel, Ifosfamide and Cisplatin PROTOCOL REF: MPHATIPGC (Version No: 1.0) Approved for use in: Second line treatment of germ cell tumours Dosage: Drug Dosage
INTERMEDIARY METABOLISM
 INTERMEDIARY METABOLISM Porphyrin Metabolism Dr Puneet Kumar Nigam M-117, Greater Kailash Part II New Delhi 110048 31 Mar 2007 (Revised 15 Oct 2007) CONTENTS Porphyrins Porphyrias Erythropoietic Porphyrias
INTERMEDIARY METABOLISM Porphyrin Metabolism Dr Puneet Kumar Nigam M-117, Greater Kailash Part II New Delhi 110048 31 Mar 2007 (Revised 15 Oct 2007) CONTENTS Porphyrins Porphyrias Erythropoietic Porphyrias
Nivolumab. Other Names: Opdivo. About this Drug. Possible Side Effects (More Common) Warnings and Precautions
 Warnings and Precautions") Nivolumab Other Names: Opdivo About this Drug Nivolumab is used to treat cancer. It is given in the vein (IV). Possible Side Effects (More Common) Bone marrow depression. This is a decrease in the number
Nivolumab Other Names: Opdivo About this Drug Nivolumab is used to treat cancer. It is given in the vein (IV). Possible Side Effects (More Common) Bone marrow depression. This is a decrease in the number
UNIT VI: ACID BASE IMBALANCE
 UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
UNIT VI: ACID BASE IMBALANCE 1 Objectives: Review the physiological mechanism responsible to regulate acid base balance in the body i.e.: Buffers (phosphate, hemoglobin, carbonate) Renal mechanism Respiratory
Chapter 13. Learning Objectives. Learning Objectives 9/11/2012. Poisonings, Overdoses, and Intoxications
 Chapter 13 Poisonings, Overdoses, and Intoxications Learning Objectives Discuss use of activated charcoal in treatment of poisonings List treatment options for acetaminophen overdose List clinical manifestations
Chapter 13 Poisonings, Overdoses, and Intoxications Learning Objectives Discuss use of activated charcoal in treatment of poisonings List treatment options for acetaminophen overdose List clinical manifestations
NURSING PROCESS FOCUS: Patients Receiving Amphotericin B (Fungizone, Abelcet)
") NURSING PROCESS FOCUS: Patients Receiving Amphotericin B (Fungizone, Abelcet) ASSESSMENT Prior to administration: Obtain complete health history including allergies, drug history, and possible drug interactions.
NURSING PROCESS FOCUS: Patients Receiving Amphotericin B (Fungizone, Abelcet) ASSESSMENT Prior to administration: Obtain complete health history including allergies, drug history, and possible drug interactions.
Methotrexate. About This Drug. Possible Side Effects. Warnings and Precautions
 Methotrexate About This Drug Methotrexate is used to treat cancer. This drug is given in the vein (IV). Possible Side Effects Soreness of the mouth and throat. You may have red areas, white patches, or
Methotrexate About This Drug Methotrexate is used to treat cancer. This drug is given in the vein (IV). Possible Side Effects Soreness of the mouth and throat. You may have red areas, white patches, or
Patient Guide Levonorgestrel and Ethinyl Estradiol Tablets USP (0.1 mg/0.02 mg) and Ethinyl Estradiol Tablets USP (0.
 and Ethinyl Estradiol Tablets USP (0.") Patient Guide Levonorgestrel and Ethinyl Estradiol Tablets USP (0.1 mg/0.02 mg) and Ethinyl Estradiol Tablets USP (0.01 mg) Rx Only This product (like all oral contraceptives) is intended to prevent pregnancy.
Patient Guide Levonorgestrel and Ethinyl Estradiol Tablets USP (0.1 mg/0.02 mg) and Ethinyl Estradiol Tablets USP (0.01 mg) Rx Only This product (like all oral contraceptives) is intended to prevent pregnancy.
Clodronate BE/H/PSUR/001/001 October 2011 Agreed CSP
 Clodronate BE/H/PSUR/001/001 October 2011 Agreed CSP 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Intravenous use Treatment of hypercalcemia due to malignancy. Oral use Treatment of hypercalcemia
Clodronate BE/H/PSUR/001/001 October 2011 Agreed CSP 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Intravenous use Treatment of hypercalcemia due to malignancy. Oral use Treatment of hypercalcemia
1/31/2009. Paroxysmal, uncontrolled electrical discharge of neurons in brain interrupting normal function
 Paroxysmal, uncontrolled electrical discharge of neurons in brain interrupting normal function In epilepsy abnormal neurons undergo spontaneous firing Cause of abnormal firing is unclear Firing spreads
Paroxysmal, uncontrolled electrical discharge of neurons in brain interrupting normal function In epilepsy abnormal neurons undergo spontaneous firing Cause of abnormal firing is unclear Firing spreads
SUMMARY OF PRODUCT CHARACTERISTICS FOR BENZODIAZEPINES AS ANXIOLYTICS OR HYPNOTICS
 SUMMARY OF PRODUCT CHARACTERISTICS FOR BENZODIAZEPINES AS ANXIOLYTICS OR HYPNOTICS Guideline Title Summary of Product Characteristics for Benzodiazepines as Anxiolytics or Hypnotics Legislative basis Directive
SUMMARY OF PRODUCT CHARACTERISTICS FOR BENZODIAZEPINES AS ANXIOLYTICS OR HYPNOTICS Guideline Title Summary of Product Characteristics for Benzodiazepines as Anxiolytics or Hypnotics Legislative basis Directive
Package leaflet: Information for the user. Morfin Abcur 10 mg/ml, solution for injection. morphine hydrochloride
 Package leaflet: Information for the user Morfin Abcur 10 mg/ml, solution for injection morphine hydrochloride Read all of this leaflet carefully before you start using this medicine because it contains
Package leaflet: Information for the user Morfin Abcur 10 mg/ml, solution for injection morphine hydrochloride Read all of this leaflet carefully before you start using this medicine because it contains
New Patient Specialty Intake Form Department of Surgery
 This form contains questions specific to the Department of Surgery. If you are new to Baylor College of Medicine and have not been seen in any of our offices, please be sure to complete our New Patient
This form contains questions specific to the Department of Surgery. If you are new to Baylor College of Medicine and have not been seen in any of our offices, please be sure to complete our New Patient
Lorazepam Tablets, USP
 Lorazepam Tablets, USP DESCRIPTION: Lorazepam, an antianxiety agent, has the chemical formula, 7-chloro-5-(o-chlorophenyl)-1,3-dihydro-3-hydroxy-2H -1,4-benzodiazepin-2-one: Cl H N N O Cl OH It is a white
Lorazepam Tablets, USP DESCRIPTION: Lorazepam, an antianxiety agent, has the chemical formula, 7-chloro-5-(o-chlorophenyl)-1,3-dihydro-3-hydroxy-2H -1,4-benzodiazepin-2-one: Cl H N N O Cl OH It is a white
New antiepileptic drugs
 Chapter 29 New antiepileptic drugs J.W. SANDER UCL Institute of Neurology, University College London, National Hospital for Neurology and Neurosurgery, Queen Square, London, and Epilepsy Society, Chalfont
Chapter 29 New antiepileptic drugs J.W. SANDER UCL Institute of Neurology, University College London, National Hospital for Neurology and Neurosurgery, Queen Square, London, and Epilepsy Society, Chalfont
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept
 Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Systemic Hypertension Dr ahmed almutairi Assistant professor Internal medicine dept Continents 1- introduction 2- classification/definition 3- classification/etiology 4-etiology in both categories 5- complications
Metabolism of porphyrins and bile pigments. Mária Sasvári 2017
 Metabolism of porphyrins and bile pigments Mária Sasvári 2017 1 The biological role of porphyrins rotoporphyrin IX + Fe 2+ heme the prosthetic group of several proteins, such as: hemoglobin, myoglobin
Metabolism of porphyrins and bile pigments Mária Sasvári 2017 1 The biological role of porphyrins rotoporphyrin IX + Fe 2+ heme the prosthetic group of several proteins, such as: hemoglobin, myoglobin
Goodridge - Heme Synthesis
 Goodridge - Heme Synthesis Study online at quizlet.com/_8r779 1. Acquired Porphyrias (lead poisoning) -inactivates ALA DHD -ALA appears in urine -inhibits protoporphyrinogen oxidase -free protoporphyrinogen
Goodridge - Heme Synthesis Study online at quizlet.com/_8r779 1. Acquired Porphyrias (lead poisoning) -inactivates ALA DHD -ALA appears in urine -inhibits protoporphyrinogen oxidase -free protoporphyrinogen
Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005
 Close this window to return to IVIS Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005 Hosted by: Reprinted in the IVIS website with the permission of the WSAVA anticonvulsant
Close this window to return to IVIS Proceedings of the World Small Animal Veterinary Association Mexico City, Mexico 2005 Hosted by: Reprinted in the IVIS website with the permission of the WSAVA anticonvulsant
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Women s Issues in Epilepsy. Esther Bui, Epilepsy Fellow MD, FRCPC
 Women s Issues in Epilepsy Esther Bui, Epilepsy Fellow MD, FRCPC How are women different? Different habitus Different metabolism Different co-morbidities Different psychosocial stigma Different hormonal
Women s Issues in Epilepsy Esther Bui, Epilepsy Fellow MD, FRCPC How are women different? Different habitus Different metabolism Different co-morbidities Different psychosocial stigma Different hormonal
European PSUR Work Sharing Project CORE SAFETY PROFILE. Lendormin, 0.25mg, tablets Brotizolam
 European PSUR Work Sharing Project CORE SAFETY PROFILE Lendormin, 0.25mg, tablets Brotizolam 4.2 Posology and method of administration Unless otherwise prescribed by the physician, the following dosages
European PSUR Work Sharing Project CORE SAFETY PROFILE Lendormin, 0.25mg, tablets Brotizolam 4.2 Posology and method of administration Unless otherwise prescribed by the physician, the following dosages
Autonomic Nervous System Testing Creating Central Balance
 Autonomic Nervous System Testing Creating Central Balance Overview of the Autonomic Nervous System Our nervous system is comprised of many different components. Some portions help us think, others give
Autonomic Nervous System Testing Creating Central Balance Overview of the Autonomic Nervous System Our nervous system is comprised of many different components. Some portions help us think, others give
Clinical Information on West Nile Virus (WNV) Infection
 Infection") Clinical Information on West Nile Virus (WNV) Infection Introduction In 1999, West Nile Virus (WNV), an Old World flavivirus, producing a spectrum of disease including severe meningoencephalitis, appeared
Clinical Information on West Nile Virus (WNV) Infection Introduction In 1999, West Nile Virus (WNV), an Old World flavivirus, producing a spectrum of disease including severe meningoencephalitis, appeared
Tranquilizers & Sedative-Hypnotics
 Tranquilizers & Sedative-Hypnotics 1 Tranquilizer or anxiolytic: Drugs used therapeutically to treat agitation or anxiety Sedative-Hypnotic: drugs used to sedate and aid in sleep Original sedatives (before
Tranquilizers & Sedative-Hypnotics 1 Tranquilizer or anxiolytic: Drugs used therapeutically to treat agitation or anxiety Sedative-Hypnotic: drugs used to sedate and aid in sleep Original sedatives (before
Like us on Facebook (JU Nursing Leaders) & check our website
 & check our website") Like us on Facebook (JU Nursing Leaders) & check our website www.junursingleaders.wordpress.com nurseslabs.com/nclex- Questions Substance and eating disorders test bank The nurse is assessing a 19 year-old
Like us on Facebook (JU Nursing Leaders) & check our website www.junursingleaders.wordpress.com nurseslabs.com/nclex- Questions Substance and eating disorders test bank The nurse is assessing a 19 year-old
BCM 317 LECTURE OJEMEKELE O.
 BCM 317 LECTURE BY OJEMEKELE O. JAUNDICE Jaundice is yellowish discoloration of the skin, sclera and mucous membrane, resulting from an increased bilirubin concentration in the body fluid. It is usually
BCM 317 LECTURE BY OJEMEKELE O. JAUNDICE Jaundice is yellowish discoloration of the skin, sclera and mucous membrane, resulting from an increased bilirubin concentration in the body fluid. It is usually
Package leaflet: Information for the patient. Morphine Unimedic 1 mg/ml solution for injection morphine hydrochloride trihydrate
 Package leaflet: Information for the patient Morphine Unimedic 1 mg/ml solution for injection morphine hydrochloride trihydrate Read all of this leaflet carefully before you start using this medicine because
Package leaflet: Information for the patient Morphine Unimedic 1 mg/ml solution for injection morphine hydrochloride trihydrate Read all of this leaflet carefully before you start using this medicine because
Chronic Hepatitis C. Risk Factors
 Chronic Hepatitis C The hepatitis C virus is one of the most important causes of chronic liver disease in the United States. Almost 4 million Americans or 1.8 percent of the U.S. population have an antibody
Chronic Hepatitis C The hepatitis C virus is one of the most important causes of chronic liver disease in the United States. Almost 4 million Americans or 1.8 percent of the U.S. population have an antibody
Metformin Hydrochloride
 Metformin Hydrochloride 500 mg, 850 mg, 500 mg LA and 750 mg LA Tablet Description Informet is a preparation of metformin hydrochloride that belongs to a biguanide class of oral antidiabetic drugs. Metformin
Metformin Hydrochloride 500 mg, 850 mg, 500 mg LA and 750 mg LA Tablet Description Informet is a preparation of metformin hydrochloride that belongs to a biguanide class of oral antidiabetic drugs. Metformin
MINOR TRANQUILIZERS CHAPTER TWO : MINOR TRANQUILIZERS
 MINOR TRANQUILIZERS 76. The term 'minor tranquilizers' was introduced into the scientific literature in the 1950s to distinguish the medicines prescribed to reduce anxiety and tension from the major tranquillizers,
MINOR TRANQUILIZERS 76. The term 'minor tranquilizers' was introduced into the scientific literature in the 1950s to distinguish the medicines prescribed to reduce anxiety and tension from the major tranquillizers,
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy
 Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided
Example Clinician Educational Material for Providers of Immune Effector Cellular Therapy Disclaimer: This example is just one of many potential examples of clinician education material that can be provided