Opioid Initiative Wave I Treating Opioid-Use Disorder in the ED Part 2
|
|
|
- Angela Butler
- 5 years ago
- Views:
Transcription



1 Opioid Initiative Wave I Treating Opioid-Use Disorder in the ED Part 2


2 Presenter Eric Ketcham, MD, MBA Reuben J. Strayer, MD

3 BUPRENORPHINE IN THE E.D.: Initiating Medication Assisted Treatment for Opioid Addiction Expanding the scope of emergency care during an addiction epidemic Eric Ketcham, MD, MBA, FACEP, FASAM, FACHE Medical Director, New Mexico Treatment Services (Opioid Addiction Treatment Clinicc): Farmington, NM & Espanola, NM Staff Emergency Physician: San Juan Regional Medical Center, Farmington, NM Los Alamos Medical Center, Los Alamos, NM Past-President, New Mexico ACEP Reuben J. Strayer, MD, FRCP(EM) Associate Medical Director Department of Emergency Medicine Maimonides Medical Center Brooklyn, NY emupdates.com
4 O.D. is now the #1 cause of death for Americans under age : more than 600,000 overdose deaths Life expectancy for Americans is falling -- two years in a row
5 MAT: Medication Assisted Treatment is the MOST EFFECTIVE Treatment for Opioid Addiction Opioid addiction does not respond to the same treatments as alcoholism. Abstinence based therapies generally DO NOT WORK: ~ 95% relapse rate. Twelve Step programs have a <5% rate of sobriety at one year, when treating Opioid Use Disorder. MAT: Naltrexone Methadone Buprenorphine ( bupe )
. Increasing use in correctional facilities and residential programs.")
6 MAT: Medication Assisted Therapy Depot Naltrexone: Vivitrol Monthly Injection for Assisted Abstinence Therapy Intended to prevent any reward from opioid use, and thus gradually reduce cravings. Patient must have already completed withdrawal, or completely weaned off mu agonist therapy (or will precipitate withdrawal). Increasing use in correctional facilities and residential programs. Some patients opt for Vivitrol after detoxing or after completion of an abstinence program. Overall outpatient numbers are still low. NOT a medication to be initiated in the E.D.
 use liquid methadone (to deter diversion).")
7 MAT: Methadone Very Effective Medication for Opioid Use Disorder: The gold standard by which other treatments are measured. Long half-life (~ 24 hrs), full mu agonist. The dosing is very patient specific. Nearly all methadone clinics (addiction treatment) use liquid methadone (to deter diversion). Many regard methadone as 2 nd line medication for patients who fail office-based buprenorphine treatment.

8 MAT: Methadone HOWEVER: Requires daily travel to the clinic. May not be available in suburban & rural areas. Inconvenient for many occupations -- daily dosing at a clinic. Dosing at the methadone clinic means congregating with other patients with OUD: Pros & Cons. The E.D is NOT the place to begin methadone treatment.

9 PRESCRIBING Methadone DON T PRESCRIPTION FORM very RISKY! High risk drug for treating chronic pain by prescription. 24 hr ½ life for dependency, but only ~ 8 hr ½ life for pain relief. Slow onset ~ 3-4 hours to peak. 24 hr ½ life for potential effects of respiratory depression. Vast majority of Methadone deaths are from treatment for pain by Rx, or diverted use, rather than in an addiction clinic. Vast majority of diverted methadone is in the tablet form (the prescription form).
10 BUPRENORPHINE ( BUPE ) NUTS & BOLTS: Key properties of bupe: Partial agonist Long half-life: ~ 36 hours (treating dependency) Rapidly effective Binds tightly to the Mu receptor (blocking other opioids) Induces less euphoria (particularly after the first dose) Many patients get no euphoria from bupe ever. Very effective analgesic.
11 Partial agonist : NUTS & BOLTS OF BUPE TX Has a ceiling effect on respiratory depression No more respiratory depression at 32mg than at 16mg However, may potentiate respiratory depression effects of alcohol, and other sedating medications (e.g. benzos). Important consideration if prescribing bupe. Any Doc can use bupe in the ED to treat opioid withdrawal. Any Doc can prescribe bupe for pain. Must have an DEA license X-waiver to PRESCRIBE for ADDICTION

12 Long half-life: ~ 36 hours: NUTS & BOLTS OF BUPE TX When dosed daily, at a therapeutic dose, maintains the patient at a therapeutic level a steady state Thus eliminating withdrawal symptoms and cravings Concept Similar to methadone, which has a half-life of ~ 24 hours. However, bupe is: Easier to dose. Safe for office based treatment. Beginning MAT with bupe in the E.D. does not preclude or complicate transitioning the patient to methadone in an addiction clinic (if that is a better option for that patient).
, and peak effects at ~ 1 hour.")
 ~ 15% High rate of first pass")
13 NUTS & BOLTS OF BUPE TX CORRECT placement -- SL Effective within 15 minutes (sublingual), and peak effects at ~ 1 hour. SL bioavailability ~ 50% Be sure it goes under the tongue. Buccal ~ 28% Oral (swallowed) ~ 15% High rate of first pass metabolism Incorrect placement
. Included to prevent the dissolution and IV injection of buprenorphine. In my E.D.")
14 NUTS & BOLTS OF BUPE TX Suboxone (others: Zubsolv and Bunavail ) Combinations of buprenorphine and naloxone (tablets or strips) Suboxone, is a 4:1 ratio of bupe/naloxone. Naloxone has a very poor sublingual and oral bioavailability (~ <2%). Included to prevent the dissolution and IV injection of buprenorphine. In my E.D. we only use the generic mono-product bupe: -- administered by a nurse less expensive.
15 BUPRENORPHINE ( BUPE ) NUTS & BOLTS: Addiction CLINIC Dosing initiation: Therapeutic dosing can begin on the first day of treatment Older protocols suggested starting at low doses, and observing the patient in clinic for an hour. However, most patients with OUD have had experience with buprenorphine. Effective dosing is related to the volume/dose of the patient s habit or tolerance. Eric Ketcham s rule of thumb for INITIAL effective bupe dosing in clinic: <50mg/day of oxycodone or ~<1/2 G/day (or less) of heroin -- ~2-4mg/day ~ mg/day of oxy or ~2 G/day of heroin or more -- ~ 16mg/day Adjust dosing on follow up visits.
 90% reduction in heroin overdoses!! ~50,000 pts down to ~5,000 pts! Auriacombe, et al, Am J Addict. 2004;13 Suppl 1:S17-28.")
16 IN 1996, FRANCE RESPONDED TO ITS HEROIN OVERDOSE EPIDEMIC BY TRAINING/LICENSING GP S TO PRESCRIBE BUPRENORPHINE Over 8 years: 3x increase methadone treated patients (up to ~15,000 pts) 4.5x increase in bupe tx pts (up to ~90,000 pts) 90% reduction in heroin overdoses!! ~50,000 pts down to ~5,000 pts! Auriacombe, et al, Am J Addict. 2004;13 Suppl 1:S Auiracombe20
17 Heroin overdose deaths and opioid agonist treatment: Baltimore, MD, Rapid expansion of access to buprenorphine treatment Rate of heroin overdose deaths drops in half. Despite a substantial increase in local heroin purity. Schwartz et al, Am J Public Health May;103(5):917-22
18 Opioid Agonist Therapy is Much More Valuable than Drug Abuse Counseling!! Swedish Study: 40 patients randomized Daily supervised med administration for the first 6 months 1-year retention in treatment was 75% in the buprenorphine group 0% in the placebo group bupe taper, then placebo (+ counseling) DAILYBUPRENORPHINE (+ COUNSELING) Kakko, et al, Lancet Feb 22;361(9358):662-8.
:CD004147 Review")


19 Cochrane Database Syst Rev Oct 5;(10):CD Review specifically studied value added of routine, mandatory counseling sessions in MAT programs adding any psychosocial support to standard maintenance treatments does not add additional benefits.
20 EVERYONE NEEDS A THERAPIST, BUT AN OPIOIDADDICTNEEDS AN OPIOIDAGONIST
21 Beginning MAT in the ED: the warm hand-off Yale: D'Onofrio: Emergency department-initiated buprenorphine/naloxone treatment for opioid dependence: a randomized clinical trial. 329 ED patients with OUD, screened, and randomized: ~1/3 to the referral group (patient is handed a pamphlet) ~1/3 to the brief intervention group (meets with a social worker or pt advocate) ~1/3 to the buprenorphine treatment group (and above) MAIN OUTCOMES AND MEASURES: Enrollment in, and receiving, addiction treatment 30 days after randomization was the primary outcome. D'Onofrio G, O'Connor PG, Pantalon MV, et al, JAMA Apr 28;313(16):
")
22 YALE (D ONOFRIO) ED-IBPROTOCOL
")
23 YALE (D'Onofrio) ED-IB continued
24 YALE (D'ONOFRIO) ED-IB continued Needed inpatient addiction treatment services? Bupe group: 11% (95% CI, 6%-19%, P <0.001) Referral Group: 37% (95% CI, 27%-48%, P <0.001) Brief Intervention Group: 35% (95% CI, 25%-37%, P <0.001)
 narcotic drugs to a patient for the purpose of relieving acute withdrawal symptoms while arranging for the patient s referral for treatment, under")
25 In the outpatient setting: THREE-DAY RULE According to DEA the three-day rule allows a practitioner who is not separately registered as a narcotic treatment program or certified as a waivered DATA 2000 physician, to administer (but not prescribe) narcotic drugs to a patient for the purpose of relieving acute withdrawal symptoms while arranging for the patient s referral for treatment, under the following conditions: Not more than one day s medication may be administered or given to a patient at one time. Treatment may not be carried out for more than 72 hours The 72-hour period cannot be renewed or extended
26 THREE DAY RULE Is it necessary to be able to refer a patient to an opioid addiction treatment clinic, to administer bupe in the ED for withdrawal or MAT? Officially, it is required In practicality The DEA cares about DIVERSION of prescribed, or dispensed, bupe. The DEA is far, far less concerned about medications ordered and administered in hospitals.
27 NUTS & BOLTS OF BUPE TX Binds tightly to the Mu receptor (blocking other opioids): Displaces full agonist opioids (heroin, morphine, methadone, etc.) Requires high doses of naloxone to displace bupe. Patients must be in withdrawal (or craving post w/d) -- to benefit from bupe! PRECIPITATED WITHDRAWAL CAN BE HORRIBLE.
 Can be in mild withdrawal for short acting")
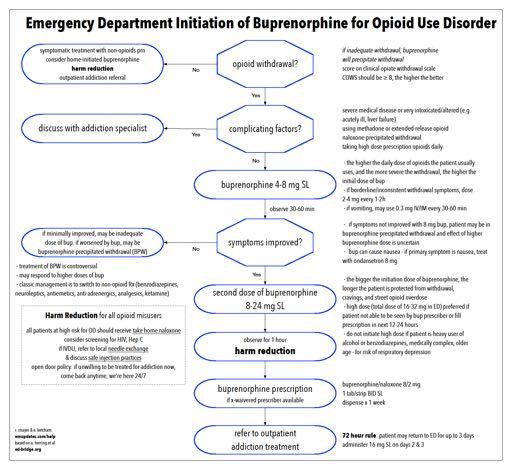
28 Avoiding Precipitating Withdrawal with Bupe Find out what the patient uses (if possible): Type of opioids used Low dose user, high dose user Last use (how many hours ago). Ensure the patient is in adequate withdrawal (or withdrawal completed) Can be in mild withdrawal for short acting opioids, At least moderate for long acting opioids (e.g. methadone) Perform a COWS score: A quick 11 element scale, which includes elements such as heart rate, pupil size, rhinorrhea, tremor, and restlessness. COWS 8 mild, 13 moderate, 36 severe. Takes <1 minute to score
29 Bupe After Naloxone for O.D? To Avoid Precipitating withdrawal: This has not been well studied. Shared decision-making with pt. If pt only uses short acting opioids (e.g. heroin, oxycodone), may consider initiating bupe: Be prepared to monitor pt until the naloxone would have worn off. Offer non-opioid w/d tx as well. After NALOXONE, caution with giving bupe to pts on long half-life opioids, such as methadone, MS Contin, Opana, etc.


30 Treating Buprenorphine Precipitated Withdrawal Treating Precipitated Withdrawal: Also not well studied. Somewhat controversial. Can offer non-opioid Tx. Alternatively.. More bupe. Titrate additional doses, while the patient is monitored, until withdrawal symptoms have subsided. CAUTION: Nausea is a common adverse effect of buprenorphine. Do not assume that all nausea induced by buprenorphine is due to precipitated withdrawal.
31 PATIENT SELECTION PITFALLS FOR E.D. BUPE INITIATION: 1. The very mild withdrawal patient who states, I feel like the withdrawals are just starting is an ideal candidate for counseling and referral (not ED bupe). Check a COWS score! Must be at least 8 -- if no other contraindication. No need to precipitate withdrawal. 2. METHADONE in the last 48 hours (not an absolute contraindication): Unpredictable precipitated withdrawal can occur Unless pt in severe withdrawal, consult an expert first. 3. Intoxicated --alcohol, benzodiazepines, stimulants, etc... Unpredictable immediate results. At risk for polypharmacy synergistic respiratory depression, with polydrug use after discharge. Do your best to engage and encourage them to consider the ED an open door to return when sober.
32 PATIENT SELECTION PITFALLS FOR E.D. BUPE INITIATION: 4. Chronic pain patients taking medically prescribed opioids: Many chronic pain patients truly painful conditions, but also have developed opioid dependence, and experience opioid induced hypersensitivity, tachyphylaxis, and withdrawal reported as pain flares. Although may be excellent candidates for tx with bupe for pain (and OUD) -- very effective analgesic. However, the dosing is different for chronic pain. Better handled in Clinic. 5. Patients with severe medical illnesses: renal failure, advanced liver disease, heart failure, severe COPD: Not an absolute contraindication, may be a good option. HOWEVER, this treatment must be COORDINATED. Requires a team approach.
33 BASIC E.D. DOSING CONCEPTS: Screen out high risk patients (previous slide). Base the first dose based on: Patient s use history (average daily opioid use) high vs. low Severity of withdrawal Example: ~ lower dose user, mild to moderate withdrawal: consider 4mg of bupe. ~ high dose user, in at least mild withdrawal: start at 8mg of bupe. Repeat dosing every 30 minutes as necessary to get the patient comfortable: Then the pt can have a meaningful conversation with a social worker/advocate for clinic referral. If no contraindications: Consider bupe loading (up to 24-32mg) Or, if you have an X-Waiver: write the patient a short-term bupe RX. Prolongs the return of withdrawal symptoms, Gives the patient more time to get to a clinic, without having to return to the ED. Avoid bupe loading in the polypharmacy patient.

34 BUT IF WE START ADMINISTERING BUPE IN THE E.D The E.D. will be awash with drug seekers, trying to get bupe! BUPRENORPHINE EDs which have started bupe programs have not seen significant visits increase, opioid- seeking patient visits may decrease. If more patients did come to the ED hoping to start MAT, would that be a bad thing? These patients are coming to the ED anyway. Might not more patients suffering from opioid addiction get into treatment?
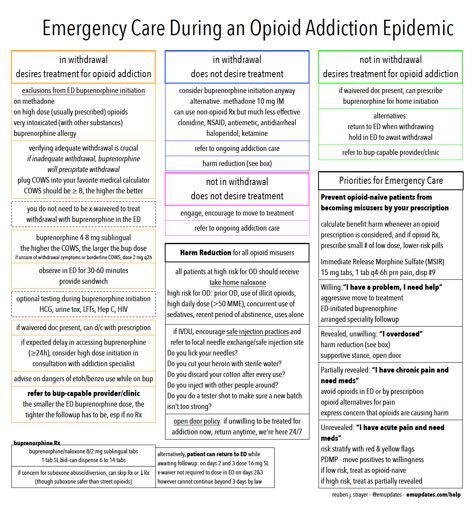
35 ED Management of Pain and Opioid Misuse During an 1.prevent opioid naive patients frombecoming misusers by your prescription calculate benefit:harm whenever opioid Rxconsidered if opioid Rx, small number of low dose, lower-riskpills 2.for existing opioid users 2a. revealed,willing I m an addict, I need help aggressive move to treatment ED-initiated buprenorphine arranged specialityfollowup 2b. revealed,unwilling I overdosed harm reduction e.g. homenaloxone supportive stance, opendoor Addiction Epidemic 2c. partially revealed I havechronic pain and need meds avoid opioids in ED or by prescription opioidalternativesforpain express concern that opioids are causing harm 2d. unrevealed I have acute pain and need meds risk stratify with red & yellow flags PMDP - move positives towillingness
36

37 High dose ED bupe MAT induction: No longer just for the addiction specialist. Coming to an ED near you!
38

39 MAT is a long term program High rate of failure with short term detox approach. Most opioid addicted patients will need many months, if not years of treatment, for some many years or even lifelong Tx. This neuroadaptation to opioids is unique to opioid addiction, as opposed to alcohol dependency. We must think of opioid dependency/addiction as we think of DM, HTN, and other chronic illnesses. Successfully weaning off opioids for the long term (not just Detox ) is a slow, gradual process. Opioid Addiction Treatment is a journey, and a marathon -- not a Sprint

40 scheduled opioid consumption freedom from addiction harms normal life possible
41 THANK YOU! Eric Ketcham, MD Reuben Strayer, MD

 ntarrant@acep.")
42 For More Information E-QUAL Website Contacts: Nalani Tarrant: (Senior Project Manager) Dhruv Sharma: (Project Manager)
43 The guidelines, measures, education and quality improvement activities and related data specifications developed by the American College of Emergency Physicians (ACEP) Emergency Quality Network are intended to facilitate quality improvement activities by physicians. The materials are intended to provide information and assist physicians in enhancing quality of care. The materials do not establish a standard of medical care, and have not been tested for all potential applications and therefore should not be used as a substitute for clinical or medical judgment. Materials are subject to review and may be revised or rescinded at any time by ACEP. The materials may not be altered without prior written approval from ACEP. The materials, while copyrighted, can be reproduced and distributed, without modification, for noncommercial purposes (e.g., use by health care providers in connection with their practices). The E-QUAL Opioid Initiative is funded by the Addiction Policy Forum. The sponsor had no role in the development of this content or quality improvement offering, and the views expressed are of the speaker.
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Opioid Initiative Wave I Treating Opioid-Use Disorder in the ED Part 1
 Opioid Initiative Wave I Treating Opioid-Use Disorder in the ED Part 1 Presenter Eric Ketcham, MD, MBA Reuben J. Strayer, MD emergency department management of the patient with opioid withdrawal OD is
Opioid Initiative Wave I Treating Opioid-Use Disorder in the ED Part 1 Presenter Eric Ketcham, MD, MBA Reuben J. Strayer, MD emergency department management of the patient with opioid withdrawal OD is
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Buprenorphine as a Treatment Option for Opioid Use Disorder
 Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Medications for Opioid Use Disorder. Charles Brackett, MD, MPH General Internal Medicine, DHMC
 Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Medication-Assisted Treatment (MAT) Overview
 Overview") Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Opioid Initiative Wave I Starting an ALTO Program
 Opioid Initiative Wave I Starting an ALTO Program Presenter Alexis LaPietra, DO What is an Alternatives to Opioids Program Comprehensive program focusing on a multi-modal approach to acute pain management
Opioid Initiative Wave I Starting an ALTO Program Presenter Alexis LaPietra, DO What is an Alternatives to Opioids Program Comprehensive program focusing on a multi-modal approach to acute pain management
2018 Opioid Initiative Wave I - Benchmarking Guide
 2018 Opioid Initiative Wave I - Benchmarking Guide Disclosures & Disclaimer Presenter Centers for Medicare and Medicaid Innovation: ACEP TCPI Contracted with Centers for Medicare and Medicaid Services
2018 Opioid Initiative Wave I - Benchmarking Guide Disclosures & Disclaimer Presenter Centers for Medicare and Medicaid Innovation: ACEP TCPI Contracted with Centers for Medicare and Medicaid Services
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates
 and Medication Assisted Treatment (MAT) for Opiates") Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
THA Medication Safety Summit. Wesley Geminn, PharmD, BCPP
 THA Medication Safety Summit Wesley Geminn, PharmD, BCPP Current Trends: Overdose Deaths in 2017 72,000 Or 197 per day 8 per hour National Opioid Overdose Statistics https://www.drugabuse.gov/related-topics/trendsstatistics/overdose-death-rates
THA Medication Safety Summit Wesley Geminn, PharmD, BCPP Current Trends: Overdose Deaths in 2017 72,000 Or 197 per day 8 per hour National Opioid Overdose Statistics https://www.drugabuse.gov/related-topics/trendsstatistics/overdose-death-rates
Management Options for Opioid Dependence:
 Management Options for Opioid Dependence: Policy Implications and Recommendations Dan Ollendorf, PhD Sarah Jane Reed, MSc New England CEPAC Goal: To improve the application of evidence to guide practice
Management Options for Opioid Dependence: Policy Implications and Recommendations Dan Ollendorf, PhD Sarah Jane Reed, MSc New England CEPAC Goal: To improve the application of evidence to guide practice
Buprenorphine: An Introduction. Sharon Stancliff, MD Harm Reduction Coalition September 2008
 Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc.
 Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc. Elements Behavioral Health Diplomate, American Board of Addiction
Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc. Elements Behavioral Health Diplomate, American Board of Addiction
Addiction to Opioids. Marvin D. Seppala, MD Chief Medical Officer
 Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets. Risk Evaluation and Mitigation Strategy (REMS) Program
 Program") SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Identification and Treatment of Opioid Use Disorders in Primary Care Settings
 Identification and Treatment of Opioid Use Disorders in Primary Care Settings 17th Annual Primary Care Symposium February 24, 2018 Kelly S. Barth, DO Associate Professor, Psychiatry & Internal Medicine
Identification and Treatment of Opioid Use Disorders in Primary Care Settings 17th Annual Primary Care Symposium February 24, 2018 Kelly S. Barth, DO Associate Professor, Psychiatry & Internal Medicine
Buprenorphine Prescribing as a Patient- Centered Medical Home Enhancement
 Buprenorphine Prescribing as a Patient- Centered Medical Home Enhancement TANNER NISSLY DO, BOB LEVY MD FASAM, MICHELE MANDRICH MSW, CMPE AS YOU ENTER, PLEASE SET UP TO PARTICIPATE IN OUR POLL EVERYWHERE
Buprenorphine Prescribing as a Patient- Centered Medical Home Enhancement TANNER NISSLY DO, BOB LEVY MD FASAM, MICHELE MANDRICH MSW, CMPE AS YOU ENTER, PLEASE SET UP TO PARTICIPATE IN OUR POLL EVERYWHERE
Opioid Use Disorder Treatment Initiation in Diverse Settings
 Opioid Use Disorder Treatment Initiation in Diverse Settings Sarah Wakeman, MD, FASAM Medical Director, Mass General Substance Use Disorder Initiative Assistant Professor, Harvard Medical School Disclosures
Opioid Use Disorder Treatment Initiation in Diverse Settings Sarah Wakeman, MD, FASAM Medical Director, Mass General Substance Use Disorder Initiative Assistant Professor, Harvard Medical School Disclosures
Opioids Research to Practice
 Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Opioid Use Disorders &Medication Treatment
 Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
The CARA & Buprenorphine Prescribing for APNs & PAs
 The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone
 Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone Alexander Y. Walley, MD, MSc Associate Professor of Medicine Director, Addiction Medicine Fellowship Boston University
Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone Alexander Y. Walley, MD, MSc Associate Professor of Medicine Director, Addiction Medicine Fellowship Boston University
Hospitals Role in Addressing the Opioid Crisis
 Hospitals Role in Addressing the Opioid Crisis Webinar 5: Buprenorphine in the Emergency Department November 14, 2017 Agenda Hospital Based Buprenorphine Initiatives Yngvild Olsen, M.D., Medical Consultant,
Hospitals Role in Addressing the Opioid Crisis Webinar 5: Buprenorphine in the Emergency Department November 14, 2017 Agenda Hospital Based Buprenorphine Initiatives Yngvild Olsen, M.D., Medical Consultant,
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations
 Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Medication Assisted Treatment for Opioid Use Disorders and Veteran Populations Kamala Greene Genece, Ph.D. VP, Clinical Director Phoenix Houses of New York Benjamin R. Nordstrom, M.D., Ph.D. President
Virginia Opioid Addiction ECHO*
 Virginia Opioid Addiction ECHO* Project ECHO: July 27th *ECHO: Extension of Community Healthcare Outcomes Agenda Agenda Agenda Introductions Clinical Director Administrative Medical Director ECHO Hubs
Virginia Opioid Addiction ECHO* Project ECHO: July 27th *ECHO: Extension of Community Healthcare Outcomes Agenda Agenda Agenda Introductions Clinical Director Administrative Medical Director ECHO Hubs
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Vivitrol Vs. Suboxone
 Vivitrol Vs. Suboxone Vivitrol - Naltrexone Indicated for opiate dependence and alcohol withdrawal pure antagonist 380mg once every 4 weeks IM Peak plasma concentration in 2 hrs, followed by a second peak
Vivitrol Vs. Suboxone Vivitrol - Naltrexone Indicated for opiate dependence and alcohol withdrawal pure antagonist 380mg once every 4 weeks IM Peak plasma concentration in 2 hrs, followed by a second peak
Building capacity for a CHC response to Ontario's Opioid Crisis
 Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE
 Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Medication Assisted Treatment
 Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Opioid Agonists. Natural derivatives of opium poppy - Opium - Morphine - Codeine
 Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Agenda. 1 Opioid Addiction in the United States. Evidence-based treatments for OUD. OUD Treatment: Best Practices. 4 Groups: Our Model
 Agenda 1 Opioid Addiction in the United States 2 Evidence-based treatments for OUD OUD Treatment: Best Practices 4 Groups: Our Model 2 Groups is a national network of clinics providing affordable, evidencebased
Agenda 1 Opioid Addiction in the United States 2 Evidence-based treatments for OUD OUD Treatment: Best Practices 4 Groups: Our Model 2 Groups is a national network of clinics providing affordable, evidencebased
Disclosures. Topics of today s training 4/24/2017. Evolving Treads in Medication Assisted Treatment. Christopher J Davis D.O.
 Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Medication Assisted Treatment. Nicole Gastala, MD
 Medication Assisted Treatment Nicole Gastala, MD Objectives Training Goals: To enhance the understanding of the participants in use of medication assisted therapy To increase the knowledge of participants
Medication Assisted Treatment Nicole Gastala, MD Objectives Training Goals: To enhance the understanding of the participants in use of medication assisted therapy To increase the knowledge of participants
Opioid Dependence and Buprenorphine Management
 Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
NALTREXONE DAVID CRABTREE, MD, MPH UNIVERSITY OF UTAH HEALTH, 2018
 NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
1) To understand the scope of the opioid epidemic with relation to Emergency Departments 2) To gain insight into some emerging Emergency Medicine
 To understand the scope of the opioid epidemic with relation to Emergency Departments 2) To gain insight into some emerging Emergency Medicine") 1) To understand the scope of the opioid epidemic with relation to Emergency Departments 2) To gain insight into some emerging Emergency Medicine solutions to the Opioid Epidemic 3) To learn about the
1) To understand the scope of the opioid epidemic with relation to Emergency Departments 2) To gain insight into some emerging Emergency Medicine solutions to the Opioid Epidemic 3) To learn about the
Medication-Assisted Treatment (MAT) for Opioid Use Disorders
 for Opioid Use Disorders") Medication-Assisted Treatment (MAT) for Opioid Use Disorders Sybil Marsh MA MD FASAM Department of Family Medicine and Community Health Case Western Reserve University/UHCMC Learning Objective 1 Following
Medication-Assisted Treatment (MAT) for Opioid Use Disorders Sybil Marsh MA MD FASAM Department of Family Medicine and Community Health Case Western Reserve University/UHCMC Learning Objective 1 Following
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT)
") Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) What has changed? Effective January 16, 2018, Coordinated Care will change the requirement for form HCA 13-333 Medication
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) What has changed? Effective January 16, 2018, Coordinated Care will change the requirement for form HCA 13-333 Medication
What Is Heroin? Examples of Opioids. What Science Says about Opioid Use Disorder and Its Treatment 6/27/2016
 What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI)
") OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI) Case 105- Prep Materials University of Massachusetts Medical School Opioid Conscious Curriculum Learner Prep Objectives The purpose of this prep material
OPIOID SAFE- PRESCRIBING TRAINING IMMERSION (OSTI) Case 105- Prep Materials University of Massachusetts Medical School Opioid Conscious Curriculum Learner Prep Objectives The purpose of this prep material
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT)
") Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) For Apple Health clients served Fee-for-Service and through contracted Medicaid Managed Care Organizations Updated January
Clinical Guidelines and Coverage Limitations for Medication Assisted Treatment (MAT) For Apple Health clients served Fee-for-Service and through contracted Medicaid Managed Care Organizations Updated January
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Opioids Research to Practice
 Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
Suboxone, Zubsolv, Bunavail (buprenorphine with naloxone sublingual tablets and film), Buprenorphine sublingual tablets
, Buprenorphine sublingual tablets") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.32 Subject: Suboxone Drug Class Page: 1 of 7 Last Review Date: June 24, 2016 Suboxone Drug Class Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.70.32 Subject: Suboxone Drug Class Page: 1 of 7 Last Review Date: June 24, 2016 Suboxone Drug Class Description
Methadone Maintenance 101
 Methadone Maintenance 101 OTP/DAILY DOSING CLINICS - ANDREW PUTNEY MD Conflicts of Interest - Employed by Acadia HealthCare 1 Why Methadone? At adequate doses methadone decreases opioid withdrawal symptoms
Methadone Maintenance 101 OTP/DAILY DOSING CLINICS - ANDREW PUTNEY MD Conflicts of Interest - Employed by Acadia HealthCare 1 Why Methadone? At adequate doses methadone decreases opioid withdrawal symptoms
Earl Hightower's Remarks 2014 National Rx Drug Abuse Summit Medication Assisted Treatment for Opiate Addiction
 Earl Hightower's Remarks 2014 National Rx Drug Abuse Summit Medication Assisted Treatment for Opiate Addiction Thank you, Chairman Rogers, for holding this important Summit and helping to bring attention
Earl Hightower's Remarks 2014 National Rx Drug Abuse Summit Medication Assisted Treatment for Opiate Addiction Thank you, Chairman Rogers, for holding this important Summit and helping to bring attention
The Social Worker s Role in Medication Assisted Treatment
 The Social Worker s Role in Medication Assisted Treatment Rocky Ephraim Lucas, LICSW Behavioral Health Consultant, Kanawha City Health Center (Cabin Creek Health Systems) What is Medication-Assisted Treatment
The Social Worker s Role in Medication Assisted Treatment Rocky Ephraim Lucas, LICSW Behavioral Health Consultant, Kanawha City Health Center (Cabin Creek Health Systems) What is Medication-Assisted Treatment
HARM REDUCTION & TREATMENT. Devin Reaves MSW
 HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
OPIOID USE DISORDER AND THE PSYCHIATRIC EMERGENCY ROOM THE VA CT MODEL
 OPIOID USE DISORDER AND THE PSYCHIATRIC EMERGENCY ROOM THE VA CT MODEL Brian Fuehrlein, MD PhD VA Connecticut Healthcare System and Yale University I have no conflicts of interest or relevant financial
OPIOID USE DISORDER AND THE PSYCHIATRIC EMERGENCY ROOM THE VA CT MODEL Brian Fuehrlein, MD PhD VA Connecticut Healthcare System and Yale University I have no conflicts of interest or relevant financial
9/13/2017. Buprenorphine Treatment (Suboxone) Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare
 Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare") Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Opioid Replacement Therapy
 Opioid Replacement Therapy Matthew A. Felgus, MD mafelgus@wisc.edu 6333 Odana Rd, Suite 3, Madison, WI 53719 (608) 257-1581 Board Certified in Addiction Medicine Board Certified in Psychiatry matthewfelgusmd.com
Opioid Replacement Therapy Matthew A. Felgus, MD mafelgus@wisc.edu 6333 Odana Rd, Suite 3, Madison, WI 53719 (608) 257-1581 Board Certified in Addiction Medicine Board Certified in Psychiatry matthewfelgusmd.com
2/21/2018. What are Opioids?
 Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention
 The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
Opioid Initiative Wave I PDMPs and Screening
 Opioid Initiative Wave I PDMPs and Screening Presenter Jason Hoppe, DO PDMPs and Screening Jason Hoppe, DO Department of Emergency Medicine University of Colorado School of Medicine Take away points Embrace
Opioid Initiative Wave I PDMPs and Screening Presenter Jason Hoppe, DO PDMPs and Screening Jason Hoppe, DO Department of Emergency Medicine University of Colorado School of Medicine Take away points Embrace
Arwen Podesta, MD. ABIHM, ABAM, Forensic Psychiatry
 The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
Treating Opioid Use Disorders: An Update for Counselors and Other Providers
 Treating Opioid Use Disorders: An Update for Counselors and Other Providers Brad Shapiro, MD Medical Director Opiate Treatment Outpatient Program Zuckerberg San Francisco General THE DOSING WINDOW HISTORICAL
Treating Opioid Use Disorders: An Update for Counselors and Other Providers Brad Shapiro, MD Medical Director Opiate Treatment Outpatient Program Zuckerberg San Francisco General THE DOSING WINDOW HISTORICAL
Understanding Medication in Addiction Treatment for Drug Court Participants
 Understanding Medication in Addiction Treatment for Drug Court Participants Introduction This pocket guide is for drug court participants who may be prescribed or considering medication as a part of addiction
Understanding Medication in Addiction Treatment for Drug Court Participants Introduction This pocket guide is for drug court participants who may be prescribed or considering medication as a part of addiction
Now available. A maintenance dose of SUBOXONE mg once daily is clinically effective for most patients*1. Once-daily dosing in a single tablet
 Now available SUBOXONE Once-daily dosing1 12 mg and 16 mg tablets A maintenance dose of SUBOXONE 12-16 mg once daily is clinically effective for most patients*1 Effective maintenance dosing with SUBOXONE
Now available SUBOXONE Once-daily dosing1 12 mg and 16 mg tablets A maintenance dose of SUBOXONE 12-16 mg once daily is clinically effective for most patients*1 Effective maintenance dosing with SUBOXONE
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Medication Assisted Treatment of an Opioid Use Disorder. J. Craig Allen, MD. Medical Director, Rushford
 Medication Assisted Treatment of an Opioid Use Disorder J. Craig Allen, MD. Medical Director, Rushford Learning objectives At the conclusion of this activity, participants will be able to: Understand
Medication Assisted Treatment of an Opioid Use Disorder J. Craig Allen, MD. Medical Director, Rushford Learning objectives At the conclusion of this activity, participants will be able to: Understand
Opioids. October 29, Addiction Medicine Review Course CSAM, Newport Beach, CA
 Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
MAT 101: TREATMENT OF OPIOID USE DISORDER
 MAT 101: TREATMENT OF OPIOID USE DISORDER WITH SPECIAL EMPHASIS ON BUPRENORPHINE/NALOXONE ICADD May 22, 2018 Alicia Carrasco, MD Debby Woodall, LCSW, ACADC Magni Hamso, MD, MPH Terry Reilly Health Services
MAT 101: TREATMENT OF OPIOID USE DISORDER WITH SPECIAL EMPHASIS ON BUPRENORPHINE/NALOXONE ICADD May 22, 2018 Alicia Carrasco, MD Debby Woodall, LCSW, ACADC Magni Hamso, MD, MPH Terry Reilly Health Services
Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine
 [Patient-focused, evidence-based addiction treatment] Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine BrightView Health All Rights Reserved www.brightviewhealth.com
[Patient-focused, evidence-based addiction treatment] Shawn A. Ryan MD, MBA President & Chief Medical Officer Board Certified, Addiction Medicine BrightView Health All Rights Reserved www.brightviewhealth.com
Building Community Coalitions to Address the Opioid Crisis
 Building Community Coalitions to Address the Opioid Crisis Understanding the Overdose Epidemic, Addiction, and Treatment Barry Zevin MD Medical Director Street Medicine and Shelter Health San Francisco
Building Community Coalitions to Address the Opioid Crisis Understanding the Overdose Epidemic, Addiction, and Treatment Barry Zevin MD Medical Director Street Medicine and Shelter Health San Francisco
Opioid Step Policy. Description. Section: Prescription Drugs Effective Date: April 1, 2018
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Opioid Step Policy Page: 1 of 6 Last Review Date: March 16, 2018 Opioid Step Policy Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 Subject: Opioid Step Policy Page: 1 of 6 Last Review Date: March 16, 2018 Opioid Step Policy Description
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings
 Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Buprenorphine pharmacology
 Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Buprenorphine pharmacology Victorian Opioid Management ECHO Department of Addiction Medicine St Vincent s Hospital Melbourne 2018 Page 1 Opioids full, partial, antagonist Full Agonists - bind completely
Acute General Medical and Surgical Admission:
 Acute General Medical and Surgical Admission: Managing Substance Use Disorders in Patients Who are Severely Ill Scott Grantham, MD Executive Director, Behavioral Health Saint Francis Health System By the
Acute General Medical and Surgical Admission: Managing Substance Use Disorders in Patients Who are Severely Ill Scott Grantham, MD Executive Director, Behavioral Health Saint Francis Health System By the
Management of Opioid Use Disorder in Primary Care
 1 Northwest ATTC presents Management of Opioid Use Disorder in Primary Care Joseph O. Merrill, MD, MPH University of Washington Associate Professor of Medicine 4/26/2018 Today s Presenter 2 Joseph Merrill,
1 Northwest ATTC presents Management of Opioid Use Disorder in Primary Care Joseph O. Merrill, MD, MPH University of Washington Associate Professor of Medicine 4/26/2018 Today s Presenter 2 Joseph Merrill,
Arizona s Opioid Epidemic
 Arizona s Opioid Epidemic Rise in Heroin Addiction and the Dangers of Fentanyl Sara Salek, MD Chief Medical Officer Shana Malone, MS Clinical Initiatives Project Manager 1 Disclosures None The National
Arizona s Opioid Epidemic Rise in Heroin Addiction and the Dangers of Fentanyl Sara Salek, MD Chief Medical Officer Shana Malone, MS Clinical Initiatives Project Manager 1 Disclosures None The National
Methadone and Naltrexone ER
 Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Medication Assisted Treatment:
 Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
It s Not Just One More Thing! Overcoming Obstacles for Buprenorphine Treatment by Residents, Faculty and Programs
 It s Not Just One More Thing! Overcoming Obstacles for Buprenorphine Treatment by Residents, Faculty and Programs Ken Saffier, MD Maureen Strohm, MD May 7, 2017 Disclosures Ken Saffier, MD, has nothing
It s Not Just One More Thing! Overcoming Obstacles for Buprenorphine Treatment by Residents, Faculty and Programs Ken Saffier, MD Maureen Strohm, MD May 7, 2017 Disclosures Ken Saffier, MD, has nothing
6/6/2018. Objectives. Outline. Rethinking Medication Treatment for Opioid Use Disorder
 Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
Practical Tools to Successfully Taper Prescription Opioids. Melissa Weimer, DO, MCR
 Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Practical Tools to Successfully Taper Prescription Opioids Melissa Weimer, DO, MCR Objectives Understand how to calculate morphine equivalents per day Understand the steps necessary to plan a successful
Expanding Access To Medication Assisted Treatment for Opioid Use Disorders to Patients in the Hospital
 Expanding Access To Medication Assisted Treatment for Opioid Use Disorders to Patients in the Hospital August 28, 2018 Hosted by John A. Renner, Jr., MD, DLFAPA Professor of Psychiatry Boston University
Expanding Access To Medication Assisted Treatment for Opioid Use Disorders to Patients in the Hospital August 28, 2018 Hosted by John A. Renner, Jr., MD, DLFAPA Professor of Psychiatry Boston University
Serious Mental Illness and Opioid Use Disorder
 Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
MEDICATION ASSISTED TREATMENT
 MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
CDC Guideline for Prescribing Opioids for Chronic Pain. Centers for Disease Control and Prevention National Center for Injury Prevention and Control
 CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
CDC Guideline for Prescribing Opioids for Chronic Pain Centers for Disease Control and Prevention National Center for Injury Prevention and Control THE EPIDEMIC Chronic Pain and Prescription Opioids 11%
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT
 and acute pain management on MAT") An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
National Opioid Treatment Guideline Dr. Ronald Lim
 National Opioid Treatment Guideline Dr. Ronald Lim (MD, CCFP, DFASAM, ABAM(D), FISAM, CCSAM, MRO) Clinical Assistant Professor, Department of Psychiatry and Family Practice Cumming School of Medicine University
National Opioid Treatment Guideline Dr. Ronald Lim (MD, CCFP, DFASAM, ABAM(D), FISAM, CCSAM, MRO) Clinical Assistant Professor, Department of Psychiatry and Family Practice Cumming School of Medicine University
FY17 SCOPE OF WORK TEMPLATE. Name of Program/Services: Medication-Assisted Treatment: Buprenorphine
 FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
Revised 9/30/2016. Primary Care Provider Pain Management Toolkit
 Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Revised 9/30/2016 Primary Care Provider Pain Management Toolkit TABLE OF CONTENTS 1. INTRODUCTION Page 1 2. NON-OPIOID SERVICES &TREATMENTS FOR CHRONIC PAIN Page 2 2.1 Medical Services Page 2 2.2 Behavioral
Opioid Use Disorder Treatment: Buprenorphine Treatment Basics
 Opioid Use Disorder Treatment: Buprenorphine Treatment Basics Daniel Warren, MD Eastern Oregon Coordinated Care Organization Provider Forum on Chronic Noncancer Pain Management Pendleton, OR February 24,
Opioid Use Disorder Treatment: Buprenorphine Treatment Basics Daniel Warren, MD Eastern Oregon Coordinated Care Organization Provider Forum on Chronic Noncancer Pain Management Pendleton, OR February 24,
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE
 LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
Changing Course: statewide efforts to combat the opioid epidemic in California
 Changing Course: statewide efforts to combat the opioid epidemic in California Kelly Pfeifer, MD kpfeifer@chcf.org April 26, 2018 State of Reform conference STAT Special Report: 52 weeks, 52 faces Obituaries
Changing Course: statewide efforts to combat the opioid epidemic in California Kelly Pfeifer, MD kpfeifer@chcf.org April 26, 2018 State of Reform conference STAT Special Report: 52 weeks, 52 faces Obituaries
Academic Medical School: Implementing Curriculum in Chronic Pain and Opioid Misuse. Jill M Williams, MD
 Academic Medical School: Implementing Curriculum in Chronic Pain and Opioid Misuse Pain, Pain Management and the Opioid Epidemic Symposium Jill M Williams, MD Professor Psychiatry Director, Division Addiction
Academic Medical School: Implementing Curriculum in Chronic Pain and Opioid Misuse Pain, Pain Management and the Opioid Epidemic Symposium Jill M Williams, MD Professor Psychiatry Director, Division Addiction
OUD & MAR: Caring for Our Communities
 OUD & MAR: Caring for Our Communities Speaker: Elisabeth Fowlie Mock, MD, MPH Video Resources Diversion Alert/recoveryinme video https://www.youtube.com/watch?v=q1lsmwwwm40 CDC Videos RX Awareness Campaign
OUD & MAR: Caring for Our Communities Speaker: Elisabeth Fowlie Mock, MD, MPH Video Resources Diversion Alert/recoveryinme video https://www.youtube.com/watch?v=q1lsmwwwm40 CDC Videos RX Awareness Campaign
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine. March 10, 2016
 The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine March 10, 2016 Objectives Review current state of opioid crisis in Maine Briefly review physiology of
The Role of Primary Care Teams and the Medical Neighborhood in Addressing the Opioid Crisis in Maine March 10, 2016 Objectives Review current state of opioid crisis in Maine Briefly review physiology of
Medication Assisted Treatment. Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs
 Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
2004-L SEPTEMBER
 BULLETIN INTELLIGENCE Buprenorphine: Potential for Abuse Product No. 2004-L0424-013 SEPTEMBER 2004 U. S. D E P A R T M E N T O F J U S T I C E NDIC Within the past 2 years buprenorphine a Schedule III
BULLETIN INTELLIGENCE Buprenorphine: Potential for Abuse Product No. 2004-L0424-013 SEPTEMBER 2004 U. S. D E P A R T M E N T O F J U S T I C E NDIC Within the past 2 years buprenorphine a Schedule III
Pharmacotherapy for opioid addiction. Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco
 Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid