Palliative Care and the Critical Role of the Pharmacist. Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre
|
|
|
- Roderick York
- 5 years ago
- Views:
Transcription
1 Palliative Care and the Critical Role of the Pharmacist Arti Thakerar Education/ Palliative Care Peter MacCallum Cancer Centre
2 Overview What is palliative care Role of a pharmacist in palliative care Issues in palliative care Syringe drivers Ketamine infusion Methadone for pain Resources available in palliative care
3 What is palliative care? Term palliative care has been used since mid-1970s No consensus on the definition used To complicate matters further - hospice, end-of-life care and terminal palliative care are used interchangeably Terminology review (Pastrana 2008) noted that palliative care definitions may include and/or differ based on: the theoretical principles underpinning care provision the goals of care the target group the structure of care provision the tasks to be undertaken the expertise of the care providers
4 WHO definition of Palliative Care Palliative care is an approach that improves the quality of life of patients and their families facing the problem associated with life-threatening illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual
5 WHO definition of Palliative Care provides relief from pain and other distressing symptoms; affirms life and regards dying as a normal process; intends neither to hasten or postpone death; integrates the psychological and spiritual aspects of patient care; offers a support system to help patients live as actively as possible until death; offers a support system to help the family cope during the patients illness and in their own bereavement; uses a team approach to address the needs of patients and their families, including bereavement counselling, if indicated; will enhance quality of life, and may also positively influence the course of illness; is applicable early in the course of illness, in conjunction with other therapies that are intended to prolong life, such as chemotherapy or radiation therapy, and includes those investigations needed to better understand and manage distressing clinical complications.
6 Statistics
7 Why is it important? In developed countries there is a high probability that death will occur with warning as a result of chronic disease or malignancy Depending on a person s position on the disease and overarching goals of care, medications are prescribed to: actively treat disease reduce or eliminate symptoms stop or slow a disease process prevent a disease or symptom
8 Impact on patients 4 components of work relating to burden of treatment rather than the illness itself Learning about the treatment and their consequences Engaging with others to organise care Adhering to treatments and lifestyle changes Monitoring treatments 8 medications on referral to a palliative care unit
9 Why a pharmacist? Symptom management Medications, interactions, side effects Advice on medications that may no longer be needed Informing the family on the use of medications Maintaining a reasonable stock of medication for patients Following up patients after discharge to carers were able to manage medications at home Supporting patients and families Providing extra information about medications to GPs
10 Palliative care pharmacist Palliative care emphasises a multidisciplinary approach to improve quality of life and relieve symptoms Work closely with other healthcare professionals to detect, prevent and resolve medication-related problems Assessments, medication reviews, patient counselling, follow-up, home visits and participate in outpatient clinics Expertise in therapeutic use of medication Complex medication regimens Involved with off-label or off license prescribing
11 Palliative care pharmacist Symptoms Pain, anxiety, constipation delirium, depression dyspnoea, insomnia, nausea and vomiting Pharmacological approach is specific Right choice of drug, dosage, detection of sideeffects, interactions, over or under-utlisation Pharmacist recommendations Change dose, change medication, change route, change time of administration, initiate new medication and stop existing medication

12 Early Palliative Care
13 Palliative Care and Chemotherapy More and more available each year New trials Consider interactions Cytochrome P450 Potential for prolong QT Electrolyte abnormalities
14 The Grey Area The palliative care population are often excluded from clinical trials Best available evidence may therefore be principles based application of pharmacology, physiology and understanding the experience of the patient in front of you Develop the skills to interpret the grey evidence
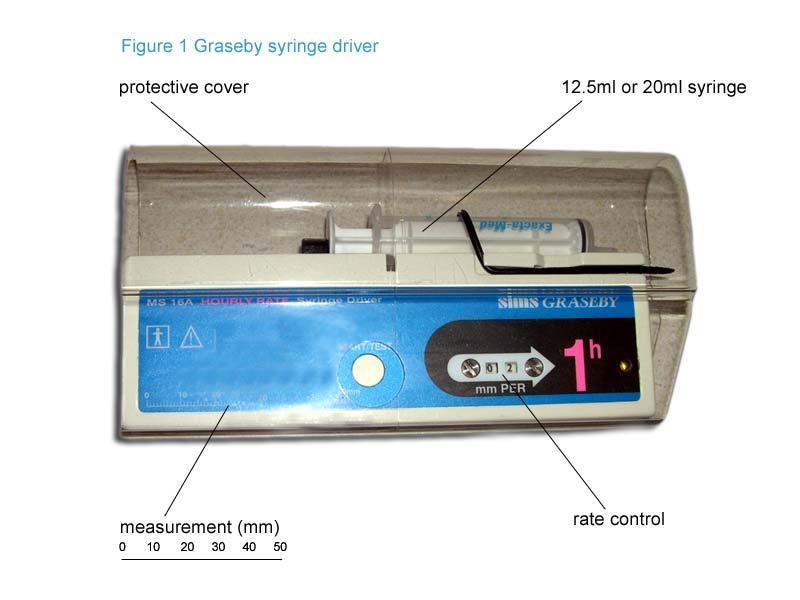


15 1: Continuous subcutaneous infusion (CSCI)
16 CSCI: Considerations Why has it been started? Will these volumes fit in the syringe? Medications and compatibility (consider diluents) What references are available? Does the advice change depending on the patient?
17 CSCI: Indications Persistent nausea and vomiting Dysphagia Intestinal obstruction Coma Poor absorption of oral medications Avoid intermittent bolus injections
18 CSCI: Volumes Dependent on the device used Total volume of the medications Rate of the delivery Greater dilutions reduce: Risk of incompatibility Impact of priming Injection site reactions May need shorter infusion times if volumes exceed the maximum 24hr volume (high doses of high volume medications: metoclopramide, morphine and midazolam)
19 CSCI: Diluent (WFI v 0.9% saline) 0.9% saline Adv: isotonic, less infusion site pain/reactions Disadv: incompatible with drugs (cyclizine), less data available WFI Adv: more data for common drugs (hydromorphone, ketamine, octreotide) Disadv: large volumes is hypotonic therefore possible site reaction
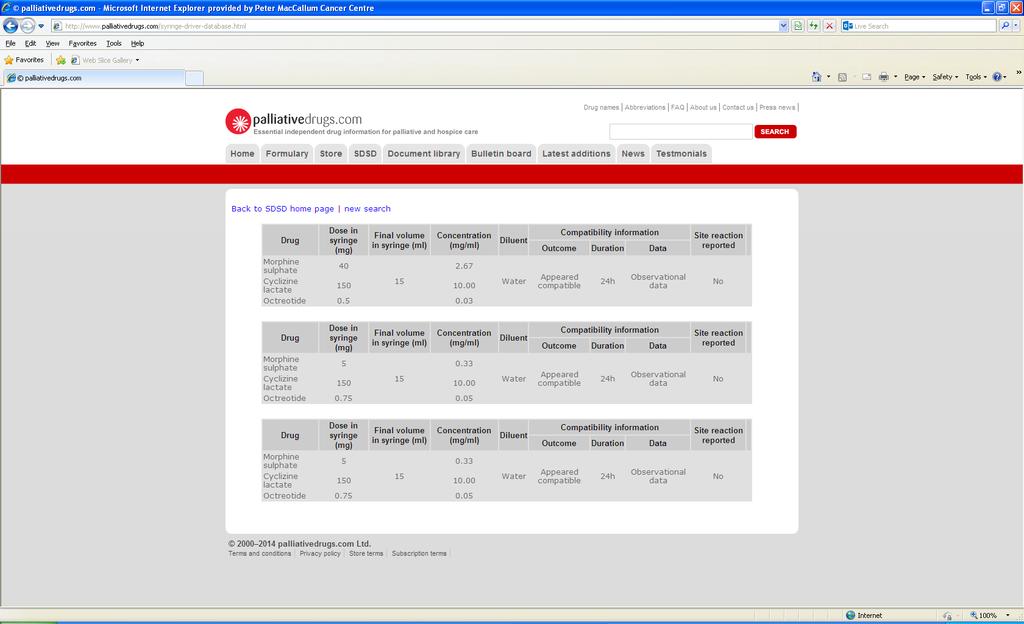
20 CSCI: Compatibility Concentrations, brand, diluent, duration of infusion, temperature, light exposure, order of mixing and device Compatibility information might be presented as: physical, observational, laboratory or chemical No data? - ph of medications should be considered. Similar ph drugs are more likely to be compatible than differing ones (most drugs are acidic) But dexamethasone, frusemide, ketoralac and phenobarbital are alkaline Adding dexamethasone last reduces the precipitation risk
21 CSCI: References Eastern Metropolitan Region Palliative Care Consortium Palliative Drugs The Syringe Drive: Continuous Subcutaneous Infusions in Palliative Care (Dickman) Handbook on Injectable Drugs (Trissel)

22
23
24 CSCI: The patient Disease trajectory Discharging home
25 2: Ketamine infusion Mechanisms include: Interrupts N-methyl-d-aspartate (NMDA) receptor blockade Interrupts cholinergic transmission Inhibits the reuptake of noradrenaline and 5-hydroxytryptamine Suggested benefits: Decrease of central sensitisation Reduction of hyperalgesia Reverse of opioid tolerance Evidence to support the use of ketamine in chronic cancer pain has been extrapolated from other settings and uncontrolled studies All studies reported adverse-effects
26 Controversial Pulse Ketamine Infusion Jackson, K., et al "Burst" ketamine for refractory cancer pain: an open-label audit of 39 patients. J Pain Symptom Manage 22(4): Day 1: 100mg ketamine CSCI Day 2: 300mg ketamine CSCI Day 3-7: 500mg ketamine CSCI Hardy, J., et al Randomized, double-blind, placebo-controlled study to assess the efficacy and toxicity of subcutaneous ketamine in the management of cancer pain. J Clin Oncol 30(29): Same as protocol as above Multi site, double blinded, randomized control, placebo control study

27 Would you recommend it?
28 3: Methadone for pain Wide interindividual variation / variable plasma half-life Mixed opioid properties: mu, NMDA, pre-synaptic block of serotonin re-uptake QT prolongation / fatal cardiac arrhythmias Social stigma associated with methadone Metabolised by several cytochrome P450 iso-enzymes (CYP3A4, CYP 2B6, CYP2D6, CYP2C9, CYP2C19 & CYP 1A2) Rotation to methadone is reserved for patients who fail to respond to other opioids Several methods exists but none are superior
29 Why is there a concern?
30 Switching to methadone Option 1 Stop and Go approach PO morphine to PO methadone Give methadone loading dose which is 1/10 of the 24hr PO morphine dose (max 30mg methadone) Give methadone 3hrly prn which is 1/30 of the 24hr PO morphine dose (max 30mg methadone) Examples: Morphine 300mg/24hr PO = loading dose of methadone 30mg PO and 10mg 3hrly prn Morphine 1200mg/24hr PO = loading dose of methadone 120mg PO and 40mg 3hrly prn. These are both capped at 30mg
31 Option 1 On day 6: amount of methadone used over the last two days is noted and divided by 4 to give a 12hrly daily dose with 1/6-1/10 of the 24hr dose available as prn Example: Methadone 80mg used in previous 48hrs = 20mg twice a day with 5mg 3hrly prn If needing prn more frequently than 3hrly then an alternative opioid should be available
32 Switching to methadone Option 2 Edmonton model for switching from (slow transition) Day 1: Decrease morphine dose by 30% and replace with methadone PO 8hrly using 10:1 ratio Day 2: If pain controlled, decrease the original dose of morphine by another 30%. Only increase methadone if pain not controlled Day 3: Discontinue the last 40% of morphine and continue 8hrly methadone plus 10% of daily methadone dose as a prn Treat transient pain with rescue doses of short acting opioids.
33 Adjuvant methadone Option 3
34 To conclude The principle and practice of palliative care has changed and therefore the role of the palliative care pharmacist is evolving Symptoms are becoming more complex but the evidence / information is still limited We have the PK/PD knowledge and therefore ideally located to help review (or extrapolate) data regarding medications We should be adding to the evidence
35 Useful Palliative Care Resources Caresearch Palliative Drugs WA Cancer and Palliative Care Network hp_palliative.cfm#resources Eastern Metropolitan Region Palliative Care Consortium Therapeutic Guidelines Palliative Care The pharmacy Guild of Australia initiated steps to enhance the role of community pharmacist in palliative care
36 References O'Connor M, et al. The palliative care interdisciplinary team: where is the community pharmacist? J Palliat Med Jan;14(1):7-11 Wilson S, et al. Impact of pharmacist intervention on clinical outcomes in the palliative care setting. Am J Hosp Palliat Care Aug;28(5): Prommer, E. E Methadone for Cancer Pain. Palliative Care: Research and Treatment 4(2181-PCRT- Methadone-for-Cancer-Pain.pdf): Walker, P. W., et al. (2008). Switching from Methadone to a Different Opioid: What Is the Equianalgesic Dose Ratio? J Palliat Med 11(8):
Syringe driver in Palliative Care
 Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
Syringe driver in Palliative Care Introduction: Syringe drivers are portable, battery operated devices widely used in palliative care to deliver medication as a continuous subcutaneous infusion over 24
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT
 PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
PRESCRIBING GUIDELINES FOR SYMPTOM MANAGEMENT IN THE DYING PATIENT A collaboration between: St. Rocco s Hospice, Bridgewater Community Healthcare NHS Trust, NHS Warrington Clinical Commissioning Group,
What is palliative care? What is palliative care? Dr Claire L Hookey
 What is palliative care? What is palliative care? Dr Claire L Hookey Palliative Care an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening
What is palliative care? What is palliative care? Dr Claire L Hookey Palliative Care an approach that improves the quality of life of patients and their families facing the problems associated with life-threatening
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
PAIN MANAGEMENT Patient established on oral morphine or opioid naive.
 PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Patient established on oral morphine or opioid naive. Important; It is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Isle of Wight Syringe Driver Compatibility Guidelines
 Isle of Wight Syringe Driver Compatibility Guidelines Produced by The Earl Mountbatten Hospice, Isle of Wight Written January 2015, revision due January 2018 This guideline is available as a paper pocketbook
Isle of Wight Syringe Driver Compatibility Guidelines Produced by The Earl Mountbatten Hospice, Isle of Wight Written January 2015, revision due January 2018 This guideline is available as a paper pocketbook
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
New Zealand Palliative Care: A Working Definition.
 New Zealand Palliative Care: A Working Definition. 1. Preamble The NZ Palliative Care Strategy (2001) aims to set in place a systematic and informed approach to the provision and funding of palliative
New Zealand Palliative Care: A Working Definition. 1. Preamble The NZ Palliative Care Strategy (2001) aims to set in place a systematic and informed approach to the provision and funding of palliative
Transitioning to palliative care: How early is early palliative care?
 Transitioning to palliative care: How early is early palliative care? Cancer: a growing problem Cancer is an increasing health care problem It is estimated that by 2020, there will be 20 million new cases
Transitioning to palliative care: How early is early palliative care? Cancer: a growing problem Cancer is an increasing health care problem It is estimated that by 2020, there will be 20 million new cases
PAIN MANAGEMENT Person established taking oral morphine or opioid naive.
 PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
PAIN MANAGEMENT Person established taking oral morphine or opioid naive. Important; it is the responsibility of the prescriber to ensure that guidelines are followed when prescribing opioids. Every member
Case studies: palliative care in Vital Signs 2014: The State of Safety and Quality in Australian Health Care
 University of Wollongong Research Online Australian Health Services Research Institute Faculty of Business 2014 Case studies: palliative care in Vital Signs 2014: The State of Safety and Quality in Australian
University of Wollongong Research Online Australian Health Services Research Institute Faculty of Business 2014 Case studies: palliative care in Vital Signs 2014: The State of Safety and Quality in Australian
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE
 PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
PAIN AND SYMPTOM MANAGEMENT GUIDANCE IN THE LAST DAYS OF LIFE Reference: DCM029 Version: 1.1 This version issued: 07/06/18 Result of last review: Minor changes Date approved by owner (if applicable): N/A
Renal Prescribing at End of Life Guidance for Anticipatory prescribing for patients in renal failure (egfr<30) at the end of life
 at the end of life") Guidance for Anticipatory prescribing for patients in renal failure (egfr
Guidance for Anticipatory prescribing for patients in renal failure (egfr
Anticipatory Medications for End of Life Patients. Doses must be proportional to the current analgesic medication YES NO YES NO
 Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
Anticipatory Medications for End of Life Patients oses must be proportional to the current analgesic medication Please refer ALL patients on Methadone or Ketamine to palliative care team for advice. Patients
PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS
 PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS The benefits of prefilled syringes for palliative care from the hospital pharmacy service In
PHARMACY SERVICE ARRANGEMENTS FOR THE SUPPLY OF PALLIATIVE CARE SYRINGES AND MEDICINES FOR COMMUNITY PATIENTS The benefits of prefilled syringes for palliative care from the hospital pharmacy service In
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL
 SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
SYMPTOM MANAGEMENT GUIDANCE FOR PATIENTS RECEIVING PALLIATIVE CARE AT ROYAL DERBY HOSPITAL If a patient is believed to be approaching the end of their life, medication should be prescribed in anticipation
ALLERGIES/ SENSITIVITIES This section must be completed before prescribing/administering any drug
 COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
COMMUNITY PRESCRIPTION CHART All entries should be in CAPITAL letters and in indelible black ink. If medications/ doses are stopped, cross through the relevant line clearly to avoid error. GP: PRESCRIBER
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER
 1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
1. GUIDELINES FOR THE MANAGEMENT OF AGITATION IN ADVANCED CANCER 1.1 GENERAL PRINCIPLES There are many causes of agitation in palliative care patients, which makes recommendations for treatment difficult.
WPCA Policy statement on defining palliative care
 The Worldwide Palliative Care Alliance Hospice House 34-44 Britannia Street London WC1X 9JG info@thewpca.org WPCA Policy statement on defining palliative care Purpose To provide clarification on palliative
The Worldwide Palliative Care Alliance Hospice House 34-44 Britannia Street London WC1X 9JG info@thewpca.org WPCA Policy statement on defining palliative care Purpose To provide clarification on palliative
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL IMPAIRMENT
 ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
ANTICIPATORY PRESCRIBING FOR PATIENTS AT END OF LIFE WITH RENAL Doses of opiates must be proptional to current analgesic medication Please refer ALL patients on Methadone Ketamine to SPCT f advice. Patients
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life
 MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
MMG035 Symptom Management Guidelines for a Person thought to be in the Last Few Days and Hours of Life The following pages are guidelines for the management of common symptoms for a person thought to be
GUIDELINES FOR CONVERSION FROM A STRONG OPIOID TO METHADONE
 GUIDELINES FOR CONVERSION FROM A STRONG OPIOID TO METHADONE GENERAL PRINCIPLES Methadone may be used as a strong opioid alternative when severe cancer-related pain responds poorly to other opioids, or
GUIDELINES FOR CONVERSION FROM A STRONG OPIOID TO METHADONE GENERAL PRINCIPLES Methadone may be used as a strong opioid alternative when severe cancer-related pain responds poorly to other opioids, or
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
Ketamine and Methadone Supra- Regional Audit Presentation
 Ketamine and Methadone Supra- Regional Audit Presentation Audit Group: Alison Coackley, Anthony Thompson, Graham Whyte, Helen Bonwick, Ruth Clark, Agnes Noble, Aileen Scott, Andrew Dickman, Sarah Fradsham
Ketamine and Methadone Supra- Regional Audit Presentation Audit Group: Alison Coackley, Anthony Thompson, Graham Whyte, Helen Bonwick, Ruth Clark, Agnes Noble, Aileen Scott, Andrew Dickman, Sarah Fradsham
Symptom Management Guidelines for End of Life Care
 Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Symptom Management Guidelines for End of Life Care The following pages are guidelines for the management of common symptoms in the last few days of life. General principles: 1. Consider how symptoms can
Ketamine and Methadone Supra- Regional Audit Presentation
 Ketamine and Methadone Supra- Regional Audit Presentation Audit Group: Alison Coackley, Anthony Thompson, Graham Whyte, Helen Bonwick, Ruth Clark, Agnes Noble, Aileen Scott, Andrew Dickman, Sarah Fradsham
Ketamine and Methadone Supra- Regional Audit Presentation Audit Group: Alison Coackley, Anthony Thompson, Graham Whyte, Helen Bonwick, Ruth Clark, Agnes Noble, Aileen Scott, Andrew Dickman, Sarah Fradsham
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
Palliative care for heart failure patients. Susan Addie
 Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
Palliative care for heart failure patients Susan Addie Treatments The most common limiting and distressing complaint is of fatigue and breathlessness. Optimal treatment strategies relieve symptoms, improves
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]
![[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]](/thumbs/92/110296570.jpg "[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text]") [Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
[Type text] Anticipatory Medication STAT dose and Syringe Driver Guidance [Type text] Patients with egfr greater than 30mL/min Patients with egfr less than 30mL/min Symptom Drug Dose Symptom Drug Dose
Specialist Palliative Care Audit and Guidelines Group (SPAGG)
") Specialist Palliative Care Audit and Guidelines Group (SPAGG) Clinical Guideline for the Prescribing and Administration of Furosemide via continuous subcutaneous infusion (CSCI) for Heart Failure Patients
Specialist Palliative Care Audit and Guidelines Group (SPAGG) Clinical Guideline for the Prescribing and Administration of Furosemide via continuous subcutaneous infusion (CSCI) for Heart Failure Patients
PART one. The Palliative Care Spectrum: Providing Care Across Settings
 PART one The Palliative Care Spectrum: Providing Care Across Settings Chapter 1 An Introduction to Palliative Pharmacy Care Jennifer M. Strickland To palliate means to alleviate. Palliative care, as the
PART one The Palliative Care Spectrum: Providing Care Across Settings Chapter 1 An Introduction to Palliative Pharmacy Care Jennifer M. Strickland To palliate means to alleviate. Palliative care, as the
What is Palliative Care? DEFINITIONS PALLIATIVE CARE. Palliative & End of Life Care Services N E Lincs 28/09/2017 1
 What is Palliative Care? 1 DEFINITIONS Palliative Care: is the active holistic care of patients with advanced progressive illness. The goal of palliative care is achievement of the best quality of life
What is Palliative Care? 1 DEFINITIONS Palliative Care: is the active holistic care of patients with advanced progressive illness. The goal of palliative care is achievement of the best quality of life
Hospice and Palliative Medicine
 Hospice and Palliative Medicine Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
Hospice and Palliative Medicine Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the
SYRINGE DRIVER MEDICATIONS
 SYRINGE DRIVER MEDICATIONS Christine Hull & Anita Webb Staff Nurses, Hospice in the Home 2015 Analgesics:- Groups of Medication used in Syringe Drivers Morphine sulphate Diamorphine Oxycodone Alfentanil
SYRINGE DRIVER MEDICATIONS Christine Hull & Anita Webb Staff Nurses, Hospice in the Home 2015 Analgesics:- Groups of Medication used in Syringe Drivers Morphine sulphate Diamorphine Oxycodone Alfentanil
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients.
 We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients. The closing date for responses is 19th December The results
We would like to thank you for completing this audit questionnaire which looks at how you manage nausea and vomiting in palliative care patients. The closing date for responses is 19th December The results
Palliative care competencies: is it for all? Khon Kaen International Conference in Palliative Care 2018
 Palliative care competencies: is it for all? Khon Kaen International Conference in Palliative Care 2018 Definition Competence The ability to do something successfully or efficiently For us it means reaching
Palliative care competencies: is it for all? Khon Kaen International Conference in Palliative Care 2018 Definition Competence The ability to do something successfully or efficiently For us it means reaching
Ageing & Palliation. Dr. Thiru Thirukkumaran Palliative Care Services Northwest Tasmania
 Ageing & Palliation Dr. Thiru Thirukkumaran Palliative Care Services Northwest Tasmania How this Session is planned? What is palliative Care? What changes take place when a young adult becomes elderly?
Ageing & Palliation Dr. Thiru Thirukkumaran Palliative Care Services Northwest Tasmania How this Session is planned? What is palliative Care? What changes take place when a young adult becomes elderly?
Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings
 Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings NHS Highland Authorised by: Planning For Fairness: Yes/No (Formerly EQIA) Distribution Consultant
Guidance for the Use of Subcutaneous Furosemide by Continuous Infusion for Heart Failure in Community Settings NHS Highland Authorised by: Planning For Fairness: Yes/No (Formerly EQIA) Distribution Consultant
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Algorithms for Symptom Management. In End of Life Care
 Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Algorithms for Symptom Management In End of Life Care The Use of Drugs Beyond Licence (off label) -The Medicines and Healthcare Products Regulatory Agency (MHRA) in the UK regulates the activity of the
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Interprofessional Webinar Series
 Interprofessional Webinar Series Opioids in the Medically Ill: Principles of Administration Russell K. Portenoy, MD Chief Medical Officer MJHS Hospice and Palliative Care Director MJHS Institute for Innovation
Interprofessional Webinar Series Opioids in the Medically Ill: Principles of Administration Russell K. Portenoy, MD Chief Medical Officer MJHS Hospice and Palliative Care Director MJHS Institute for Innovation
The last days of life in hospital and at home
 The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
The last days of life in hospital and at home Beaumont Multi-disciplinary Palliative Care Study Day 28/9/2017 Dr Sarah McLean Consultant in Palliative Medicine St Francis Hospice Beaumont Hospital Overview
SUPPLEMENTAL NOTE ON HOUSE BILL NO. 2031
 SESSION OF 2018 SUPPLEMENTAL NOTE ON HOUSE BILL NO. 2031 As Amended by Senate Committee on Public Health and Welfare Brief* HB 2031, as amended, would create the Palliative Care and Quality of Life Interdisciplinary
SESSION OF 2018 SUPPLEMENTAL NOTE ON HOUSE BILL NO. 2031 As Amended by Senate Committee on Public Health and Welfare Brief* HB 2031, as amended, would create the Palliative Care and Quality of Life Interdisciplinary
Criteria and Guidance for Referral to Specialist Palliative Care Services
 Criteria and Guidance for Referral to Specialist Palliative Care Services March 2014 Introduction This guidance is for health professionals caring for patients who may need referral to specialist palliative
Criteria and Guidance for Referral to Specialist Palliative Care Services March 2014 Introduction This guidance is for health professionals caring for patients who may need referral to specialist palliative
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015
 Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Palliative Care for Primary Care Providers QUYNH BUI, MD MPH DECEMBER 2015 Objectives Define palliative care and primary palliative care Describe the rationale for providing primary palliative care in
Palliative Care in Patients with Brain Tumors: How to maintain hope and quality of life, even when treatments fail
 Tobias Walbert MD PhD MPH Assistant Professor Neurology Wayne State University Henry Ford Hospital Detroit twalber1@hfhs.org Palliative Care in Patients with Brain Tumors: How to maintain hope and quality
Tobias Walbert MD PhD MPH Assistant Professor Neurology Wayne State University Henry Ford Hospital Detroit twalber1@hfhs.org Palliative Care in Patients with Brain Tumors: How to maintain hope and quality
For patients and their carers this means smoother symptom control, better support in a crisis, and avoidance of admission if that is their choice.
 Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
Bedfordshire Palliative Care Palliative Care Medicines Guidance This folder has been produced to support professionals providing palliative care in any setting. Its aim is to make best practice in palliative
EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
EAST LANCASHIRE SPECIALIST PALLIATIVE CARE TEAM EAST LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Reviewed and updated August 2009 Next review date August 2011 Approved
Care of the Dying. For dosing in severe renal impairment see separate guidance for care of the dying in severe renal failure.
 Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Care of the Dying Early diagnosis of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance covers the prescribing and management of patients
Palliative care for patients with brain cancer
 Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Palliative care for patients with brain cancer Lyn Cave Clinical Nurse Specialist Palliative Care Hospital2Home (H2H) Dr Jayne Wood Clinical Lead Palliative Care The Royal Marsden and Royal Brompton Palliative
Palliative Care Out-of-hours. A resource pack for West Dorset. Contents:
 Palliative Care Out-of-hours. A resource pack for West Dorset Contents: Section 1 Supply of drugs DCH Pharmacy hours and arrangements How to contact a community pharmacist out of hours Palliative care
Palliative Care Out-of-hours. A resource pack for West Dorset Contents: Section 1 Supply of drugs DCH Pharmacy hours and arrangements How to contact a community pharmacist out of hours Palliative care
Dr. Andrea Johnson Saskatoon Health Region/Saskatoon Cancer Centre September 30, 2016
 Dr. Andrea Johnson Saskatoon Health Region/Saskatoon Cancer Centre September 30, 2016 Conflicts of Interest None... Our drugs are old and cheap (for the most part) so big pharma isn t really interested
Dr. Andrea Johnson Saskatoon Health Region/Saskatoon Cancer Centre September 30, 2016 Conflicts of Interest None... Our drugs are old and cheap (for the most part) so big pharma isn t really interested
PAIN MANAGEMENT PGY-1. Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC
 PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
PAIN MANAGEMENT PGY-1 Aaron D. Storms, MD Carin van Zyl, MD Adult and Pediatric Palliative Care, LAC+USC Keck School of Medicine of USC Perception Matters A builder aged 29 came to the accident and emergency
Long Term Care Formulary HCD - 08
 1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
1 of 5 PREAMBLE Opioids are an important component of the pharmaceutical armamentarium for management of chronic pain. The superiority of analgesic effect of one narcotic over another is not generally
Palliative & End of Life Care Plan
 Palliative & End of Life Care Plan 2018-2023 Contents 1. Palliative Care Definition Page 1 2. Our Vision Page 2 3. Key Aims Page 2 4. Planned Actions Page 3-5 5. Priorities Page 6-7 6. Appendix 1 HSCP
Palliative & End of Life Care Plan 2018-2023 Contents 1. Palliative Care Definition Page 1 2. Our Vision Page 2 3. Key Aims Page 2 4. Planned Actions Page 3-5 5. Priorities Page 6-7 6. Appendix 1 HSCP
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT (estimated glomerular filtration rate<30)
") GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
GUIDELINES FOR PRESCRIBING AT THE END OF LIFE FOR PATIENTS WITH RENAL IMPAIRMENT These guidelines have been produced in collaboration with Dr Lucy Smyth, Consultant in Renal Medicine, Royal Devon and Exeter
Palliative Care Management Diploma
 Palliative Care Management Diploma Introduction Palliative care (WHO, 2002) is an approach that improves the quality of life of patients and their families facing the problems associated with lifethreatening
Palliative Care Management Diploma Introduction Palliative care (WHO, 2002) is an approach that improves the quality of life of patients and their families facing the problems associated with lifethreatening
Using syringe pumps in palliative care
 Using syringe pumps in palliative care Facilitator: Barbara Stone RN Ground rules Medication matching game Learning outcomes To identify the indications for using a syringe pump To discuss the general
Using syringe pumps in palliative care Facilitator: Barbara Stone RN Ground rules Medication matching game Learning outcomes To identify the indications for using a syringe pump To discuss the general
Syringe Drivers. Back to top
 Page 1 of 8 Syringe Drivers Introduction Indications for use Advantages Method Siting syringe driver Boost facility Transfer to hospital/hospice syringe driver drugs Drug compatibility P.r.n medication
Page 1 of 8 Syringe Drivers Introduction Indications for use Advantages Method Siting syringe driver Boost facility Transfer to hospital/hospice syringe driver drugs Drug compatibility P.r.n medication
Diamorphine 4 hour. alfentanil (500microgram/mL) Calculated by dividing 24 hour oral morphine dose by 30
 Calculated by dividing 24 hour oral morphine dose by 30") If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
If more information is required please seek help from specialist palliative care pioid dose conversion chart, syringe driver doses, rescue/prn doses and opioid patches Use the conversion chart to work
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE
 PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
PENNINE LANCASHIRE GUIDELINES FOR THE MANAGEMENT OF SYMPTOMS IN THE LAST DAYS OF LIFE Originally produced: July 2006 First Review: August 2009 Second Review: November 2011 For review November 2013 Approved
Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat.
 Difficult Pain Syndrome/Intractable/Refractory Pain Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat. Reasonable efforts Differs for specialties/regions/countries
Difficult Pain Syndrome/Intractable/Refractory Pain Intractable pain syndrome is defined as persistent pain despite all the reasonable efforts to treat. Reasonable efforts Differs for specialties/regions/countries
How importance of palliative care in lung cancer patient? Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University
 How importance of palliative care in lung cancer patient? Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Outline 1. What is palliative care? 2. Palliative care and Lung cancer : A PERFECT
How importance of palliative care in lung cancer patient? Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Outline 1. What is palliative care? 2. Palliative care and Lung cancer : A PERFECT
Palliative care in long-term conditions Scottish Palliative Care Pharmacists Association
 Palliative care in long-term conditions 2011 2012 Scottish Palliative Care Pharmacists Association Aims & Objectives To explore symptoms, general management principles and appropriate palliative treatment
Palliative care in long-term conditions 2011 2012 Scottish Palliative Care Pharmacists Association Aims & Objectives To explore symptoms, general management principles and appropriate palliative treatment
Supporting Last Days of Life Symptom Control Medication Guidance: Algorithm. Agitation & Anxiety
 Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Agitation & Anxiety (Exclude or treat REVERSIBLE causes*) Patient is anxious / frightened, but lucid Patient is confused, agitated and / or hallucinating MIDAZOLAM 2.5-5mg s/c (Max total 24 hour dose of
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
End of life prescribing guidance
 End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
End of life prescribing guidance Introduction This guidance has been prepared to ASSIST IN DECISION MAKING for the prescribing and monitoring of medicines useful in the management of symptoms commonly
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
PALLIATIVE CARE PRESCRIBING FOR PATIENTS WHO ARE SUBSTANCE MISUSERS
 PALLIATIVE CARE PRESCRIBING FOR PATIENTS WHO ARE SUBSTANCE MISUSERS Background information Substance misusers who develop palliative care needs are likely to have psychological, social and existential
PALLIATIVE CARE PRESCRIBING FOR PATIENTS WHO ARE SUBSTANCE MISUSERS Background information Substance misusers who develop palliative care needs are likely to have psychological, social and existential
The pain of it all. Rod MacLeod MNZM. Hibiscus Hospice, Auckland and University of Auckland
 The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
What You Need To Know About Palliative Care. Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director
 What You Need To Know About Palliative Care Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director None of the faculty, planners, speakers, providers, nor CME committee members
What You Need To Know About Palliative Care Natalie Wu Moy, LCSW, MSPA RUHS Medical Center Hospital Social Services Director None of the faculty, planners, speakers, providers, nor CME committee members
Use of Subcutaneous Levetiracetam at the end of life:
 Use of Subcutaneous Levetiracetam at the end of life: a literature review and audit Dr Anna Sutherland ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network
Use of Subcutaneous Levetiracetam at the end of life: a literature review and audit Dr Anna Sutherland ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network
Use of Subcutaneous Levetiracetam at the end of life:
 Use of Subcutaneous Levetiracetam at the end of life: a literature review and audit Dr Victoria Bradley ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network
Use of Subcutaneous Levetiracetam at the end of life: a literature review and audit Dr Victoria Bradley ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network
What s New 2003? What new treatments? What have you discontinued? More information please!
 What s New 2003? What new treatments? What have you discontinued? More information please! 1 What s New 2003? Submissions = 137 UK = 52 (38%) Doctors = 60% Nurses = 25% Pharmacists = 15% 2 What s New?
What s New 2003? What new treatments? What have you discontinued? More information please! 1 What s New 2003? Submissions = 137 UK = 52 (38%) Doctors = 60% Nurses = 25% Pharmacists = 15% 2 What s New?
Palliative care: Pharmacist challenges and Opportunities
 Palliative care: Pharmacist challenges and Opportunities Palliative care medicine was officially recognized as a specialty in Lebanon 28 June 2013 Ministry of Public Health issued decree number 1/1048
Palliative care: Pharmacist challenges and Opportunities Palliative care medicine was officially recognized as a specialty in Lebanon 28 June 2013 Ministry of Public Health issued decree number 1/1048
Care of the Dying Management in Severe Renal Failure
 Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Care of the Dying Management in Severe Renal Failure Clinical Guideline Early recognition of the dying process allows for adequate preparation of the patient, the family and the carers. This clinical guidance
Use of Subcutaneous Levetiracetam at the end of life:
 Use of Subcutaneous Levetiracetam at the end of life: a literature review and audit Dr Victoria Bradley ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network
Use of Subcutaneous Levetiracetam at the end of life: a literature review and audit Dr Victoria Bradley ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital.
 Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
Managing Respiratory Symptoms - Breathlessness, Cough and Secretions. Dr Laura Healy. Palliative Medicine Registrar, Beaumont Hospital. Things to consider: 1. Very common symptoms. 2. Can occur in any
 The last days of life Linda Magann CNC Palliative Care St George Hospital I m not afraid of dying, I just don t want to be there when it happens Woody Allen Palliative Care is an approach that improves
The last days of life Linda Magann CNC Palliative Care St George Hospital I m not afraid of dying, I just don t want to be there when it happens Woody Allen Palliative Care is an approach that improves
Hospice Basics and Benefits
 Hospice Basics and Benefits Goal To educate health care professionals about hospice basics and the benefits for the patient and family. 2 Objectives Describe the history and philosophy of the hospice movement
Hospice Basics and Benefits Goal To educate health care professionals about hospice basics and the benefits for the patient and family. 2 Objectives Describe the history and philosophy of the hospice movement
1/21/14. Cancer Related Pain: Case-Based Pharmacology. Conflicts of Interest. Learning Objective
 Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth)
") Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Guidelines: EOLC Symptom Control for Patients with Normal Renal Function (in Wandsworth) Policy Number : DC020 Issue Date: October 2014 Review date: October 2016 Policy Owner: Head Community Services Monitor:
Opioid Conversion Guidelines
 Opioid Conversion Guidelines March 2015 Gippsland Region Palliative Care Consortium Clinical Practice Group Title Keywords Ratified Opioid, Conversion, Drug, Therapy, Palliative, Guideline, Palliative,
Opioid Conversion Guidelines March 2015 Gippsland Region Palliative Care Consortium Clinical Practice Group Title Keywords Ratified Opioid, Conversion, Drug, Therapy, Palliative, Guideline, Palliative,
20/11/2013. Dr. Sinead Maguire Neurology Registrar 22 nd November 2013
 Dr. Sinead Maguire Neurology Registrar 22 nd November 2013 The active total care of patients whose disease is not responsive to curative treatment. Control of pain, of other symptoms, and psychological,
Dr. Sinead Maguire Neurology Registrar 22 nd November 2013 The active total care of patients whose disease is not responsive to curative treatment. Control of pain, of other symptoms, and psychological,
Palliative Emergencies. Ken Stakiw
 Palliative Emergencies Ken Stakiw Disclosure None to disclose for this lecture Have received honoraria from a number of agencies and companies previously Intend to discuss some off label use of medications
Palliative Emergencies Ken Stakiw Disclosure None to disclose for this lecture Have received honoraria from a number of agencies and companies previously Intend to discuss some off label use of medications
Hospice Care vs Palliative Care
 Hospice Care vs Palliative Care Easing the burden of illness, Improving quality of life Seasons Hospice and Palliative Care Cheryl Ledesma, FNP-BC Jacklyn Griffin, ACNP-BC Objectives After completing this
Hospice Care vs Palliative Care Easing the burden of illness, Improving quality of life Seasons Hospice and Palliative Care Cheryl Ledesma, FNP-BC Jacklyn Griffin, ACNP-BC Objectives After completing this
SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRESCRIPTION & ADMINISTRATION RECORD (SPAR) Name: Address: Postcode: Date of Birth: NHS Number:
 Name: Address: Postcode: Date of Birth: NHS Number:") FILE IN PATIENT S COMMUNITY HEALTH RECORD FOLDER : SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRERIPTION & ADMINISTRATION RECORD (SPAR) Abbreviations used in this document to be listed here with the full
FILE IN PATIENT S COMMUNITY HEALTH RECORD FOLDER : SUBCUTANEOUS AS REQUIRED & SYRINGE PUMP PRERIPTION & ADMINISTRATION RECORD (SPAR) Abbreviations used in this document to be listed here with the full
Doncaster & Bassetlaw Cancer Locality. Palliative Care Core Formulary
 Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
Doncaster & Bassetlaw Cancer Locality Palliative Core Formulary Approved by Doncaster & Bassetlaw Hospitals NHS Foundation Trust Drugs and Therapeutics Committee. DJ14/2155 Oct 2014 Review date: Oct 2017
Palliative Care. Anticipatory Prescribing Guidelines & June Gippsland Region Palliative Care Consortium Clinical Practice Group
 Palliative Care Anticipatory Prescribing Guidelines June 2016 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy No. Title Keywords Ratified GRPCC-CPG008_1.1_2016 Anticipatory Prescribing
Palliative Care Anticipatory Prescribing Guidelines June 2016 Gippsland Region Palliative Care Consortium Clinical Practice Group Policy No. Title Keywords Ratified GRPCC-CPG008_1.1_2016 Anticipatory Prescribing
Management of Seizures at the End of Life A new way forward?
 Management of Seizures at the End of Life A new way forward? Dr Victoria Bradley ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network Dr Anna Sutherland,
Management of Seizures at the End of Life A new way forward? Dr Victoria Bradley ST4 Palliative Medicine On behalf of the Health Education Thames Valley Registrars Research Network Dr Anna Sutherland,
In our patients the cause of seizures can be broadly divided into structural and systemic causes.
 Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
PAEDIATRIC DOSAGE GUIDELINES For management of post-operative acute pain
 Index No: MMG43 PAEDIATRIC DOSAGE GUIDELINES For management of post-operative acute pain Version: 3.1 (Includes anti-emetics and naloxone) Date ratified: July 2013 Ratified by: (Name of Committee) Name
Index No: MMG43 PAEDIATRIC DOSAGE GUIDELINES For management of post-operative acute pain Version: 3.1 (Includes anti-emetics and naloxone) Date ratified: July 2013 Ratified by: (Name of Committee) Name
Palliative care for children with Rare Diseases
 Palliative care for children with Rare Diseases Busi Nkosi International Children s Palliative Care Network Need for children s palliative care More than 21 million children need palliative care worldwide
Palliative care for children with Rare Diseases Busi Nkosi International Children s Palliative Care Network Need for children s palliative care More than 21 million children need palliative care worldwide
Dudley End of Life and Palliative Care Strategy Implementation Plan 2017
 Dudley End of Life and Palliative Care Strategy Implementation Plan 2017 End of Life and Palliative Care Strategy 2017 1 Contents Page What is a strategy plan? 3 Terminology 3 Demographics 3 Definitions
Dudley End of Life and Palliative Care Strategy Implementation Plan 2017 End of Life and Palliative Care Strategy 2017 1 Contents Page What is a strategy plan? 3 Terminology 3 Demographics 3 Definitions
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)
 Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC)") Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
Waterloo Wellington (WW) Symptom Management Guideline for the End of Life (EOL) Medication Order Set for Long Term Care (LTC) May 2018 THE WATERLOO WELLINGTON SYMPTOM MANAGEMENT GUIDELINE FOR THE END OF
BREATHLESSNESS MANAGEMENT
 Guideline Name: Breathlessness BACKGROUND Breathlessness is a common symptom in patients with cancer, end-stage heart failure and end-stage chronic obstructive pulmonary disease (COPD). There are many
Guideline Name: Breathlessness BACKGROUND Breathlessness is a common symptom in patients with cancer, end-stage heart failure and end-stage chronic obstructive pulmonary disease (COPD). There are many
EVALUATION OF THE CARESEARCH GP WEBPAGES. Christine Sanderson Associate Professor Geoff Mitchell Jennifer Tieman
 EVALUATION OF THE CARESEARCH GP WEBPAGES Christine Sanderson Associate Professor Geoff Mitchell Jennifer Tieman Background Development of the CareSearch website www.caresearch.com.au The policy context
EVALUATION OF THE CARESEARCH GP WEBPAGES Christine Sanderson Associate Professor Geoff Mitchell Jennifer Tieman Background Development of the CareSearch website www.caresearch.com.au The policy context