Pituitary Tumors and Incidentalomas. Bijan Ahrari, MD, FACE, ECNU Palm Medical Group
|
|
|
- Shavonne Nicholson
- 5 years ago
- Views:
Transcription


1 Pituitary Tumors and Incidentalomas Bijan Ahrari, MD, FACE, ECNU Palm Medical Group
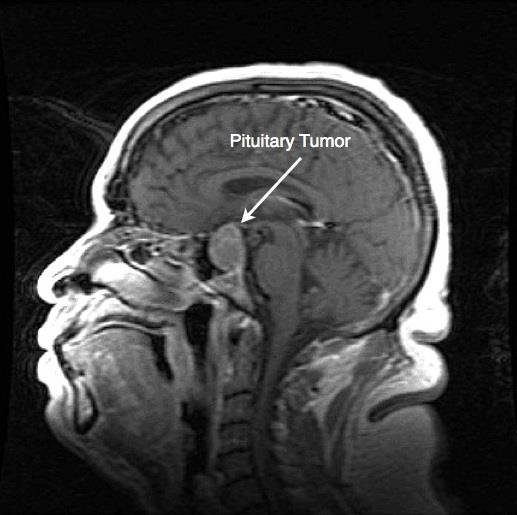
2 Background Pituitary incidentaloma: a previously unsuspected pituitary lesion that is discovered on an imaging study performed for an unrelated reason Microadenoma <1cm Macroadenoma > or equal to 1cm Sellar/Parasellar Mass Pituitary Adenoma
3
4 Prevalence of Pituitary Adenomas Adenomas 77.6 per 100,000 population Lactotroph adenomas 44.4 Nonfunctioning adenomas 22.2 Somatotroph adenomas 8.6 Corticotroph adenomas 1.2 In combined autopsy data, the average frequency of a pituitary adenoma was 10.6% Imaging: microincidentalomas were seen on MRI in 10 38% of patients.
5 Etiology of Incidentalomas 91% are pituitary adenomas 48% functional 43% non-functional 9% are non-pituitary Rathke s cleft cyst Craniopharyngioma Chrodoma Mets Endocrinol Metab Clin N Am 1999;28:81
6 Endocrinol Metab Clin N Am 2008;37:151
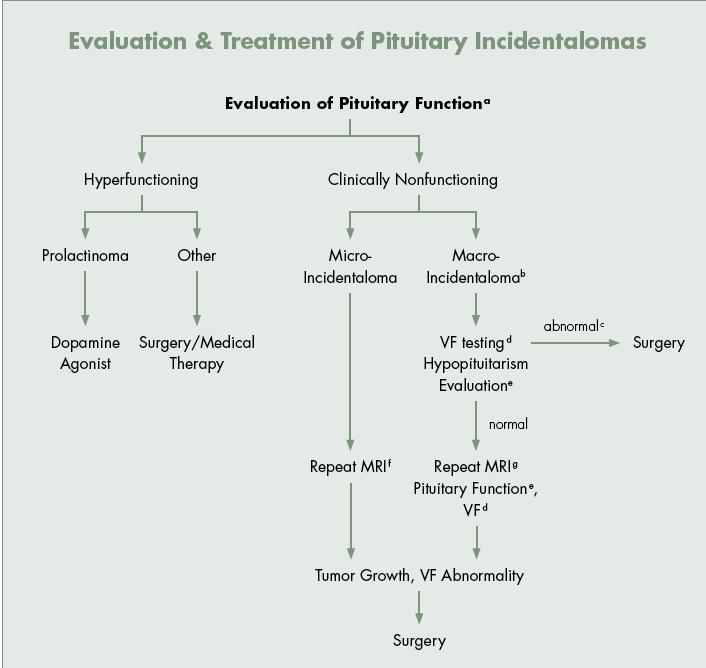
7 Evaluation of a Pituitary Incidentaloma
8 Initial Evaluation We recommend that patients presenting with a pituitary incidentaloma undergo a complete history and physical examination that includes evaluations for evidence of hypopituitarism and a hormone hypersecretion syndrome. Patients with evidence of either of these conditions should undergo an appropriately directed biochemical evaluation
9 Should We Evaluate for Hypersecretion? We recommend that all patients with a pituitary incidentaloma, including those without symptoms, undergo clinical and laboratory evaluations for hormone hypersecretion Level of evidence: moderate quality Rationale: likelihood of finding a hormonally active incidentaloma is low, however, early detection and therapy is likely to reduce morbidity
10 Evaluation for Hypersecretion Data on the prevalence of hormone hypersecretion in incidentalomas is limited Small retrospective observational studies Estimated from autopsy data Data is weak in regards to the pros/cons of pursuing a limited vs. detailed screening strategy Guideline task force was divided on this issue Assessment should include evaluation of prolactin, IGF-1, and an assessment of ACTH hypersecretion
11 Prolactin Hypersecretion Data is strongest for the importance of screening for hyperprolactinemia Pooled data shows overall prevalence of prolactin hypersecretion in incidental pituitary adenomas to be 13.4% 1,2,3 11.9% in microadenomas alone % in macroadenomas alone % in combined micro/macro adenomas 3 During prospective follow up no patients developed hyperprolactinemia after having an initial negative screen 3 1 Clin Endocrinol (Oxf) 1999;51:109 2 Pituitary 2004;7:145 3 Arch Intern Med 1995;155:181
12 Diagnosis of Hyperprolactinemia To establish the diagnosis of hyperprolactinemia, we recommend a single measurement of serum prolactin; a level above the upper limit of normal confirms the diagnosis as long as the serum sample was obtained without excessive venipuncture stress. We recommend against dynamic testing of prolactin secretion for the diagnosis of hyperprolactinemia. A prolactin level greater than 500 mcg/liter is diagnostic of a macroprolactinoma. Although a prolactin level greater than 250 mcg/liter usually indicates the presence of a prolactinoma, selected drugs, including risperidone and metoclopramide, may cause prolactin elevations above Even minimal prolactin elevations may be consistent with the presence of a prolactinoma, but a non-prolactin-secreting mass should first be considered
13 Diagnosis of Hyperprolactinemia In patients with asymptomatic hyperprolactinemia, we suggest assessing for macroprolactin. The term macroprolactinemia denotes the situation in which a preponderance of the circulating prolactin consists of larger molecules: dimeric and polymeric prolactin. Macroprolactin is less bioactive and less likely to cause symptoms, however clinical disease does occur. Galactorrhea is present in 20%, oligo/amenorrhea in 45%, and pituitary adenomas in 20%.
14 Diagnosis of Hyperprolactinemia When there is a discrepancy between a very large pituitary tumor and a mildly elevated prolactin level, we recommend serial dilution of serum samples to eliminate an artifact that can occur with some immunoradiometric assays leading to a falsely low prolactin value ( hook effect ) Expert Consult online
15 Causes of hyperprolactinemia We recommend excluding medication use, renal failure, hypothyroidism, and parasellar tumors in patients with symptomatic nonphysiological hyperprolactinemia. A number of physiological states including pregnancy, breast-feeding, stress, exercise, and sleep can cause prolactin elevation, as can medications. Because prolactin secretion is tonically inhibited by hypothalamic dopamine, disruption or compression of the pituitary stalk by a non-prolactin-secreting pituitary tumor or other parasellar mass will lead to hyperprolactinemia.
16

17 Stalk Effect vs. Prolactinoma Expert Consult Online
18 GH Hypersecretion Silent GH-secreting tumors are rare and data is limited on the prevalence of subclinical GH hypersecretion in incidentalomas Prospective observation study of 18 pituitary incidentalomas 1 1/18 (5.6%) was GH secreting (macroadenoma) 1 JAMA 1990;263:2772
19 ACTH Hypersecretion Prevalence in pituitary incidentalomas is not known No study has systematically screened incidentalomas for subclinical glucorticoid excess Recommendation for screening is based on data in patients with adrenal incidentalomas and subclinical Cushing s who benefit from detection and treatment in terms of co-morbid diabetes, HTN, obesity, and osteoporosis Appropriate screening tests: 1mg DST, 24hr urine free cortisol, MN salivary cortisol Many only screening if clinical symptoms are present

20 Immunohistochemical Data Autopsy series of 3,048 consecutive cases identified 334 pituitary adenomas in 316 pituitary glands 39.5% stained for prolactin 13.8% for ACTH 1.8% for GH Staining characteristics do not necessarily equate to clinically relevant elevations of circulating hormones Eur J Endocrinol Metab 2006;91:4769
21 Immunohistochemical Data Eur J Endocrinol Metab 2006;91:4769
22 Should We Evaluate for Hypopituitarism? We recommend that patients with a pituitary incidentaloma with or without symptoms also undergo clinical and laboratory evaluations for hypopituitarism Level of evidence: moderate Data from small observational studies of combined micro/macroadenomas shows a modest prevalence of hypopituitarism in pituitary incidentalomas 7/66 patients (10.6%) 1 19/46 patients (41.3%) 2 1 J Neurosurg 2006;104:884 2 Pituitary 2004;7:145
23 Does Size Matter? Observational studies show low rates of hypopituitarism in microadenomas 0/31 patients 1 0/15 patients 2 0/7 patients 3 19/38 patients with micoradenomas and nml IGF-1 shown to fail GHRH/Arginine stim test (industry funded) 4 Task force more strongly favored screening for hypopituitarism in macroadenomas and larger microadenomas (6-9mm) but not necessarily in smaller microincidentalomas Evaluation of larger microadenomas is based on expert opinion/experience and no specific data in evaluating hypotiuitarism in small (<6mm) vs. large (6-9mm) incidentalomas exists 1 Clin Endocrinol (Oxf) 1999;51:109 2 Arch Intern Med 1995;155:181 3 JAMA 1990;263: Clin Endocrinol (Oxf) 2008;69:292
24 What Deficits Should We Test For? Pooled hormonal deficiencies across studies (micro/macroadenomas) Gonadotropin deficiency up to 30% Thyroid axis deficiency up to 28% ACTH-cortisol axis deficiency up to 18% GH-IGF-1 axis deficiency up to 8% The recommended screening for all incidentalomas is debated Minimal: FT4, AM cortisol, testosterone (men) More complete: IGF-1, LH/FSH/Testosterone, TSH/FT4, AM cortisol Confirmatory stimulatory testing of the pituitary- adrenal or GH- IGF-1 axis should be performed if baseline testing suggests hypopituitarism
25 Should We Screen for Other Mass Effects? We recommend that all patients presenting with a pituitary incidentaloma abutting the optic nerves or chiasm on magnetic resonance imaging (MRI) undergo a formal visual field (VF) examination Level of evidence: high quality When an incidentaloma abuts the nerves or chiasm baseline visual field assessment should be obtained regardless of mass size or the presence or absence of visual symptoms
26 Occult Visual Field Deficits Prospective observational study of 67 incidentally discovered pituitary adenomas 1 3/67 (4.5%) of patients had unrecognized visual field deficits on formal testing in All were macroadenomas Other studies show undetected rates of visual field defects as high as 15% 2 1 Clin Endocrinol (Oxf) 1999;51:109 2 J Clin Endocrinol Metab 2002;87:4869 -?
27 How Best to Image Pituitary Incidentalomas All patients should have a MRI scan, if possible, to evaluate the pituitary incidentaloma (if the incidentaloma was initially only diagnosed by CT scan) to better delineate the nature and extent of the incidentaloma Level of evidence: high quality MRI should use a pituitary protocol with fine cuts through the sella with and without gadolinium contrast
28 Follow up of Pituitary Incidentalomas
29 Should We Repeat Imaging? MRI scan of the pituitary 6 months after the initial scan if the incidentaloma is a macroincidentaloma and 1 yr after the initial scan if it is a microincidentaloma Level of evidence: low quality In patients whose incidentaloma does not change in size, we suggest repeating the MRI every year for macroincidentalomas and every 1 2 yr in microincidentalomas for the following 3 yrs and gradually less frequently thereafter Level of evidence: low quality
30 Data on Incidentaloma Growth Meta-analysis of prospective studies evaluating the natural history of non-functional pituitary incidentalomas 1 8.2% enlarged over 472 person-years of follow up For microincidentalomas pooled data from 8 prospective observational studies showed 17/160 patients (10.6%) enlarged over 2-7 years of follow-up Meta-analysis data shows enlargement rate of 1.7%/year 1 For macroadenomas pooled data of data from 10 prospective observational studies showed 85/353 patients (24%) enlarged 28/353 patients (8%) developed visual field abnormality 7/353 patients (2%) developed apoplexy 1 J Clin Endocrinol Metab 2011; 96:905
31 Imaging Follow Up Rationale for repeat MRI during the first year of follow up in all pituitary incidentalomas Some tumors enlarge and the true proliferative nature of incidentalomas is unknown Guideline for MRI follow up of pituitary incidentalomas Based on expert opinion Derived from various algorithms proposed in prior studies varied and none have been validated Subsequent imaging is obtained gradually less frequently During first 3 years (q12months for macroadenomas, q12-24 months for microadenomas) Then every other year of the next 6 years, or every five years (debated)
32 When Are Repeat VFs Appropriate? VF testing in patients with a pituitary incidentaloma that enlarges to abut or compress the optic nerves or chiasm on a follow-up imaging study Level of evidence: high quality We suggest that clinicians do not need to test VF in patients whose incidentalomas are not close to the chiasm and who have no new symptoms and are being followed closely by MRI Level of evidence: very low quality Guidelines are unclear as to the specific data leading to these recommendations
33 Should We Repeat Hormonal Evaluation? Clinical and biochemical evaluations for hypopituitarism 6 months after the initial testing and yearly thereafter in patients with a pituitary macro-incidentaloma, although typically hypopituitarism develops with the finding of an increase in size of the incidentaloma Level of evidence: low quality Rationale for recommendation: high risk of untreated hypopituitarism outweighs the paucity of data
34 Data for New Pituitary Dysfunction Meta-analysis of prospective studies evaluating non-functional pituitary incidentalomas 1 New endocrine dysfunction in 2.4%/year For macroadenomas pooled data from 4 prospective observational studies showed new hypofunction in 1/7 patients (14.3%) and 3/28 patients (10.7%) all occurred in the setting of tumor enlargement 4/37 patients (10.8%) and 3/28 patients (10.7%) due to pituitary apoplexy Unclear how often new dysfunction develops in the absence of tumor growth or apoplexy Rapid growth may increase the risk of new hypopituitarism 1 J Clin Endocrinol Metab 2011; 96:905
35 What About Hormonal Evaluation in Microindentalomas? We suggest that clinicians do not need to test for hypopituitarism in patients with pituitary microincidentalomas whose clinical picture, history, and MRI do not change over time Level of evidence: low quality Pooled data from 6 observational studies showed no changes in pituitary function in microincidentalomas during follow-up
36 Follow-up Patients who develop any signs or symptoms potentially related to the incidentaloma or who show an increase in size of the incidentaloma on MRI should undergo more frequent or detailed evaluations as indicated clinically Level of evidence: low quality No studies cited in the guidelines to substantiate this recommendation

37 Indications for Surgical Therapy
38 What are the Indications for Surgery? We recommend that patients with a pituitary incidentaloma be referred for surgery if they have the following: A VF deficit due to the lesion Other visual abnormalities, such as opthalmoplegia or neurological compromise due to compression by the lesion Lesion abutting or compromising the optic nerve or chiasm on MRI Pituitary apoplexy with visual disturbance Hypersecreting tumors other than prolactinomas as recommended by other guidelines of The Endocrine Society and the Pituitary Society Level of evidence: high quality Rationale for recommendation: Task force emphasis on alleviating or preventing visual or neurologic compromise rather than potential surgical morbidities (DI, post-op hypopituitarism, cost)
39 Summary of Evidence Substantial evidence supports the recommendation for surgery in pituitary incidentalomas causing visual or neurologic compromise The risks/benefits of performing surgery in pituitary incidentalomas abutting or in close proximity to the optic chiasm but not causing VF deficits has not been quantified Expert option suggests surgery in these situations given the risk of potential future vision disturbances Benefits of surgery on preventing future VF abnormalities is not known Other guidelines for the management of hypersecretory pituitary adenomas (other than prolactinomas) support surgery for functional tumors
40 Evidence in Apoplexy Surgery is indicated when apoplexy is accompanied by visual disturbances In the absence of visual symptoms, a retrospective review of 30 cases of pituitary apoplexy showed similar rates of long term hypopituitarism in patients managed conservatively (imaging and hormonal testing follow up) vs. those who were treated surgically 1 1 Br J Neurosurg 2006; 20:379
41 Additional Considerations When Recommending Surgery Patient age Young patients have a higher lifetime probability of tumor enlargement Older patients have a higher risk of surgical complications Patient s desire for future fertility The success of the surgery is highly dependent on the availability of skilled neurosurgeons
42 Are There Other Situations in which to Consider Surgery? We suggest that surgery be considered for patients with a pituitary incidentaloma if they have the following Clinically significant growth of the pituitary incidentaloma Loss of endocrinological function A lesion close to the optic chiasm and a plan to become pregnant Unremitting headache Level of evidence: low quality
43 Regarding Tumor Growth There are no size cut-offs for growth that necessitate surgery Clinically significant growth is growth that could pose a health risk to the patient (such as to their vision) Location and growth characteristics are the most important i.e. rapid (within 1-2 years), or toward the chiasm Incidentalomas that have shown the propensity for growth tend to continue to grow Surgery is most effective when lesions are small
44 Surgery to Improve Hypopituitarism Some data from surgical series of symptomatic patients show that pituitary function can improve with surgery 1,2 One series of 26 large non-functional adenomas showed recovery in a significant number of patients by 2-3 months post-op 2 4/26 GH deficient patients (15% recovery) 8/25 hypogonadal patients (32% recovery) 12/21 hypothyroid patients (57% recovery) 6/16 adrenal insufficient patients (38% recovery) It is not clear whether the benefits seen in these symptomatic patients with macroadenomas can be extrapolated to asymptomatic incidentalomas with hormonal deficiencies 1 J Clin Endocrinol Metab 1994;79:348 2 J Clin EndocrinolMetab 1986;62: 1173
45 Other Relative Indications for Surgery Patients planning pregnancy who have tumors close to the optic chiasm Due to the small risk of lactotroph hyerplasia in pregnancy leading to tumor compression of the optic chiasm Headache may or may not improve with transphenoidal removal of the tumor
46
47
Pituitary Adenomas: Evaluation and Management. Fawn M. Wolf, MD 10/27/17
 Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
Pituitary Adenomas: Evaluation and Management Fawn M. Wolf, MD 10/27/17 Over 18,000 pituitaries examined at autopsy: -10.6% contained adenomas (1.5-27%) -Frequency similar for men and women and across
PITUITARY: JUST THE BASICS PART 2 THE PATIENT
 PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
PITUITARY: JUST THE BASICS PART 2 THE PATIENT DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none Steps taken to review and
Hyperprolactinemia: N hidshi i MD. Nahid Shirazian MD. Internist, Endocrinologist
 Diagnosis and Treatment of Hyperprolactinemia: p N hidshi i MD Nahid Shirazian MD. Internist, Endocrinologist An Endocrine Society Clinical Practice Guideline (J Clin Endocrinol Metab 96: 273 288, 2011)
Diagnosis and Treatment of Hyperprolactinemia: p N hidshi i MD Nahid Shirazian MD. Internist, Endocrinologist An Endocrine Society Clinical Practice Guideline (J Clin Endocrinol Metab 96: 273 288, 2011)
Imaging pituitary gland tumors
 November 2005 Imaging pituitary gland tumors Neel Varshney,, Harvard Medical School Year IV Two categories of presenting signs of a pituitary mass Functional tumors present with symptoms due to excess
November 2005 Imaging pituitary gland tumors Neel Varshney,, Harvard Medical School Year IV Two categories of presenting signs of a pituitary mass Functional tumors present with symptoms due to excess
Diseases of pituitary gland
 Diseases of pituitary gland A brief introduction Anterior lobe = adenohypophysis Posterior lobe = neurohypophysis The production of most pituitary hormones is controlled in large part by positively and
Diseases of pituitary gland A brief introduction Anterior lobe = adenohypophysis Posterior lobe = neurohypophysis The production of most pituitary hormones is controlled in large part by positively and
Pituitary Disease Resident Tutorial 2017
 Pituitary Disease Resident Tutorial 2017 Sarat Sunthornyothin MD Division of Endocrinology and Metabolism King Chulalongkorn Memorial Hospital Pituitary Anatomy hypophyseal portal system direct arterial
Pituitary Disease Resident Tutorial 2017 Sarat Sunthornyothin MD Division of Endocrinology and Metabolism King Chulalongkorn Memorial Hospital Pituitary Anatomy hypophyseal portal system direct arterial
Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234)
 The Diagnostic Pathway (11-2K-234)") Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland.
Prolactin-Secreting Pituitary Adenomas (Prolactinomas) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland.
Functional Pituitary Adenomas. Fawn M. Wolf, MD 2/2/2018
 Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
Functional Pituitary Adenomas Fawn M. Wolf, MD 2/2/2018 Outline Prolactinoma Acromegaly Cushing s disease Thyrotroph adenomas Gonadotroph adenomas Hyperprolactinemia Clinically apparent prolactinomas:
in Primary Care (Part 2) Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University
 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University") Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Common Endocrine Problems Seen in Primary Care (Part 2) Lecture #34 Jonathan R. Anolik, MD, FACP, FACE Lewis Katz School of Medicine at Temple University None Conflict of Interest Topics to be Covered
Mechanism of hyperprolactinemia
 Hyperprolactinemia Mechanism of hyperprolactinemia Causes of hyperprolactinemia Hormone-producing pituitary tumors Prolactinoma Acromegaly Hypothalamic/pituitary stalk lesion Tumors, cysts (craniopharyngeoma,
Hyperprolactinemia Mechanism of hyperprolactinemia Causes of hyperprolactinemia Hormone-producing pituitary tumors Prolactinoma Acromegaly Hypothalamic/pituitary stalk lesion Tumors, cysts (craniopharyngeoma,
Introduction to Endocrinology. Hypothalamic and Pituitary diseases Prolactinoma + Acromegaly
 Introduction to Endocrinology. Hypothalamic and Pituitary diseases Prolactinoma + Acromegaly Dr. Peter Igaz MD PhD DSc 2nd Department of Medicine Semmelweis University Fields of Endocrinology Diseases
Introduction to Endocrinology. Hypothalamic and Pituitary diseases Prolactinoma + Acromegaly Dr. Peter Igaz MD PhD DSc 2nd Department of Medicine Semmelweis University Fields of Endocrinology Diseases
panhypopituitarism Pattawan Wongwijitsook Maharat Nakhon Ratchasima hospital 17 Nov 2013
 panhypopituitarism Pattawan Wongwijitsook Maharat Nakhon Ratchasima hospital 17 Nov 2013 PITUITARY GLAND (HYPOPHYSIS CEREBRI) The master of endocrine glands master of endocrine glands It is a small oval
panhypopituitarism Pattawan Wongwijitsook Maharat Nakhon Ratchasima hospital 17 Nov 2013 PITUITARY GLAND (HYPOPHYSIS CEREBRI) The master of endocrine glands master of endocrine glands It is a small oval
HYPOTHALAMO PITUITARY GONADAL AXIS
 HYPOTHALAMO PITUITARY GONADAL AXIS Physiology of the HPG axis Endogenous opioids and the HPG axis (exerciseinduced menstrual disturbances) Effects of the immune system on the HPG axis (cytokines: interleukins
HYPOTHALAMO PITUITARY GONADAL AXIS Physiology of the HPG axis Endogenous opioids and the HPG axis (exerciseinduced menstrual disturbances) Effects of the immune system on the HPG axis (cytokines: interleukins
Imaging The Turkish Saddle. Russell Goodman, HMS III Dr. Gillian Lieberman
 Imaging The Turkish Saddle Russell Goodman, HMS III Dr. Gillian Lieberman Learning Objectives Review the anatomy of the sellar region Discuss the differential diagnosis of sellar masses Discuss typical
Imaging The Turkish Saddle Russell Goodman, HMS III Dr. Gillian Lieberman Learning Objectives Review the anatomy of the sellar region Discuss the differential diagnosis of sellar masses Discuss typical
A survey of pituitary incidentaloma in Japan
 European Journal of Endocrinology (2003) 149 123 127 ISSN 0804-4643 CLINICAL STUDY A survey of pituitary incidentaloma in Japan Naoko Sanno, Ken ichi Oyama, Shigeyuki Tahara, Akira Teramoto and Yuzuru
European Journal of Endocrinology (2003) 149 123 127 ISSN 0804-4643 CLINICAL STUDY A survey of pituitary incidentaloma in Japan Naoko Sanno, Ken ichi Oyama, Shigeyuki Tahara, Akira Teramoto and Yuzuru
Metoclopramide Domperidone. HYPER- PROLACTINAEMIA: the true and the false problems
 Modern management of Hyperprolactinaemia Didier DEWAILLY, M.D. Department of Endocrine Gynaecology and Reproductive Medicine, Hôpital Jeanne de Flandre, C.H.R.U., 59037 Lille, France 1 Metoclopramide Domperidone
Modern management of Hyperprolactinaemia Didier DEWAILLY, M.D. Department of Endocrine Gynaecology and Reproductive Medicine, Hôpital Jeanne de Flandre, C.H.R.U., 59037 Lille, France 1 Metoclopramide Domperidone
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY
 JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
JACK L. SNITZER, DO INTERNAL MEDICINE BOARD REVIEW COURSE 2018 PITUITARY JACK L. SNITZER, D.O. Peninsula Regional Endocrinology 1415 S. Division Street Salisbury, MD 21804 Phone:410-572-8848 Fax:410-572-6890
GLMS CME- Cell Group 5 10 April Greenlane Medical Specialists Pui-Ling Chan Endocrinologist
 GLMS CME- Cell Group 5 10 April 2018 Greenlane Medical Specialists Pui-Ling Chan Endocrinologist Pituitary case one Mrs Z; 64F Seen ORL for tinnitus wax impaction MRI Head Pituitary microadenoma (3mm)
GLMS CME- Cell Group 5 10 April 2018 Greenlane Medical Specialists Pui-Ling Chan Endocrinologist Pituitary case one Mrs Z; 64F Seen ORL for tinnitus wax impaction MRI Head Pituitary microadenoma (3mm)
Pituitary for the General Practitioner. Marilyn Lee Consultant physician and endocrinologist
 Pituitary for the General Practitioner Marilyn Lee Consultant physician and endocrinologist Pituitary tumours Anterior/posterior pituitary Extension of adenoma upwards/downwards/sideways Producing too
Pituitary for the General Practitioner Marilyn Lee Consultant physician and endocrinologist Pituitary tumours Anterior/posterior pituitary Extension of adenoma upwards/downwards/sideways Producing too
Urgent and Emergent Pituitary Conditions
 Urgent and Emergent Pituitary Conditions PANKAJ A. GORE, MD DIRECTOR, BRAIN AND SKULL BASE T UMOR SURGERY PROVIDENCE B R AIN AND S PINE I NSTITUTE Urgent and Emergent Pituitary Conditions Neurosurgical
Urgent and Emergent Pituitary Conditions PANKAJ A. GORE, MD DIRECTOR, BRAIN AND SKULL BASE T UMOR SURGERY PROVIDENCE B R AIN AND S PINE I NSTITUTE Urgent and Emergent Pituitary Conditions Neurosurgical
Pituitary apoplexy 台北榮總內分泌新陳代謝科主治醫師林怡君
 Pituitary apoplexy 台北榮總內分泌新陳代謝科主治醫師林怡君 Williams text book of endocrinology 11 th e Anterior pituitary hormone 10-20% of pituitary cells, increase to 40% during AP PRL releasing factors: TRH, oxytocin,
Pituitary apoplexy 台北榮總內分泌新陳代謝科主治醫師林怡君 Williams text book of endocrinology 11 th e Anterior pituitary hormone 10-20% of pituitary cells, increase to 40% during AP PRL releasing factors: TRH, oxytocin,
What we will cover. Evaluation of the Child with Suspected Pituitary Disease. ituitary
 Evaluation of the Child with Suspected Pituitary Disease Craig Alter, MD University of Pennsylvania Children s Hospital of Philadelphia What we will cover * What laboratory tests to order * MRI: common
Evaluation of the Child with Suspected Pituitary Disease Craig Alter, MD University of Pennsylvania Children s Hospital of Philadelphia What we will cover * What laboratory tests to order * MRI: common
Endocrine Testing. Alice Y.Y. Cheng, MD, FRCP October 14, 2015
 Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Endocrine Testing Alice Y.Y. Cheng, MD, FRCP October 14, 2015 Disclosure No disclosures relevant to the content of this workshop Learning Objectives By the end of this workshop, you will be able to: 1.
Pituitary Incidentaloma: An Endocrine Society Clinical Practice Guideline
 Pituitary Incidentaloma: An Endocrine Society Clinical Practice Guideline Pamela U. Freda, Albert M. Beckers, Laurence Katznelson, Mark E. Molitch, Victor M. Montori, Kalmon D. Post and Mary Lee Vance
Pituitary Incidentaloma: An Endocrine Society Clinical Practice Guideline Pamela U. Freda, Albert M. Beckers, Laurence Katznelson, Mark E. Molitch, Victor M. Montori, Kalmon D. Post and Mary Lee Vance
Diagnosis and Treatment of Hyperprolactinemia: An Endocrine Society Clinical Practice Guideline
 Diagnosis and Treatment of Hyperprolactinemia: An Endocrine Society Clinical Practice Guideline Shlomo Melmed, Felipe F. Casanueva, Andrew R. Hoffman, David L. Kleinberg, Victor M. Montori, Janet A. Schlechte
Diagnosis and Treatment of Hyperprolactinemia: An Endocrine Society Clinical Practice Guideline Shlomo Melmed, Felipe F. Casanueva, Andrew R. Hoffman, David L. Kleinberg, Victor M. Montori, Janet A. Schlechte
Neuroendocrine Disorders in Women
 Neuroendocrine Disorders in Women Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes and Hypertension Brigham and Women s Hospital Professor of Medicine, Harvard Medical School Case Presentation
Neuroendocrine Disorders in Women Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes and Hypertension Brigham and Women s Hospital Professor of Medicine, Harvard Medical School Case Presentation
Where Has My Vision Gone? Evaluation of Sellar Lesions. Caleb Stowell,, HMS III Gillian Lieberman, MD November 2008
 Where Has My Vision Gone? Evaluation of Sellar Lesions Caleb Stowell,, HMS III Gillian Lieberman, MD November 2008 Objectives Present a case highlighting the clinical presentation and evaluation of a sellar
Where Has My Vision Gone? Evaluation of Sellar Lesions Caleb Stowell,, HMS III Gillian Lieberman, MD November 2008 Objectives Present a case highlighting the clinical presentation and evaluation of a sellar
Sharon maslovitz Lis Maternity Hospital
 Sharon maslovitz Lis Maternity Hospital Case report Chief complaint 27 yo, with PMC @ 31+3w, BCBA twins Complaints of severe rt parietal and retrobulbar headaches Medical background Healthy until 24yo
Sharon maslovitz Lis Maternity Hospital Case report Chief complaint 27 yo, with PMC @ 31+3w, BCBA twins Complaints of severe rt parietal and retrobulbar headaches Medical background Healthy until 24yo
Pathology of pituitary gland. By: Shifaa Qa qa
 Pathology of pituitary gland By: Shifaa Qa qa Sella turcica Adenohypophysis (80%): - epithelial cells - acidophil, basophil, chromophobe - Somatotrophs, Mammosomatotrophs, Corticotrophs, Thyrotrophs, Gonadotrophs
Pathology of pituitary gland By: Shifaa Qa qa Sella turcica Adenohypophysis (80%): - epithelial cells - acidophil, basophil, chromophobe - Somatotrophs, Mammosomatotrophs, Corticotrophs, Thyrotrophs, Gonadotrophs
Clinical presentations of endocrine diseases
 Section I Chapter 1 Clinical approaches Clinical presentations of endocrine diseases Karen Gomez-Hernandez and Shereen Ezzat Endocrinology is a fascinating field that covers a wide range of diseases with
Section I Chapter 1 Clinical approaches Clinical presentations of endocrine diseases Karen Gomez-Hernandez and Shereen Ezzat Endocrinology is a fascinating field that covers a wide range of diseases with
Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234)
 The Diagnostic Pathway (11-2K-234)") Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland. In patients
Somatotroph Pituitary Adenomas (Acromegaly) The Diagnostic Pathway (11-2K-234) Common presenting symptoms/clinical assessment: Pituitary adenomas are benign neoplasms of the pituitary gland. In patients
Endocrinological Outcome Among Treated Craniopharyngioma Patients
 Endocrinological Outcome Among Treated Craniopharyngioma Patients Afaf Al Sagheir, MD Head & Consultant, Section of Endocrinology/Diabetes Department of Pediatrics KFSH&RC Introduction Craniopharyngiomas
Endocrinological Outcome Among Treated Craniopharyngioma Patients Afaf Al Sagheir, MD Head & Consultant, Section of Endocrinology/Diabetes Department of Pediatrics KFSH&RC Introduction Craniopharyngiomas
Original Article. Abstract. Introduction. Thinesh Kumran 1,2, Saffari Haspani 1,2, Jafri Malin Abdullah 1,4, Azmi Alias 1,2, Fan Rui Ven 3
 Original Article Factors Influencing Disconnection Hyperprolactinemia and Reversal of Serum Prolactin after Pituitary Surgery in a Non-Functioning Pituitary Macroadenoma Thinesh Kumran 1,2, Saffari Haspani
Original Article Factors Influencing Disconnection Hyperprolactinemia and Reversal of Serum Prolactin after Pituitary Surgery in a Non-Functioning Pituitary Macroadenoma Thinesh Kumran 1,2, Saffari Haspani
See the latest estimates for new cases of pituitary tumors in the US and what research is currently being done.
 About Pituitary Tumors Overview and Types If you have been diagnosed with a pituitary tumor or worried about it, you likely have a lot of questions. Learning some basics is a good place to start. What
About Pituitary Tumors Overview and Types If you have been diagnosed with a pituitary tumor or worried about it, you likely have a lot of questions. Learning some basics is a good place to start. What
Pituitary Disorders Suranut Charoensri, MD
 Pituitary Disorders Suranut Charoensri, MD Division of Endocrinology and Metabolism Department of Medicine Faculty of Medicine, Khon Kaen University Anatomical Landmarks Nat Rev Endocrinol 2014;10:423-435
Pituitary Disorders Suranut Charoensri, MD Division of Endocrinology and Metabolism Department of Medicine Faculty of Medicine, Khon Kaen University Anatomical Landmarks Nat Rev Endocrinol 2014;10:423-435
Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution?
 Case Reports in Radiology Volume 2015, Article ID 268974, 5 pages http://dx.doi.org/10.1155/2015/268974 Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution? Devon
Case Reports in Radiology Volume 2015, Article ID 268974, 5 pages http://dx.doi.org/10.1155/2015/268974 Case Report Rapid Pituitary Apoplexy Regression: What Is the Time Course of Clot Resolution? Devon
(3) Pituitary tumours
 Pituitary tumours") Hypopituitarism Diabetes Insipidus Pituitary tumours (2) Dr T Kemp - Endocrinology and Metabolism Unit - Steve Biko Academic Hospital (3) Pituitary tumours Pituitary microadenoma - intrasellar adenoma
Hypopituitarism Diabetes Insipidus Pituitary tumours (2) Dr T Kemp - Endocrinology and Metabolism Unit - Steve Biko Academic Hospital (3) Pituitary tumours Pituitary microadenoma - intrasellar adenoma
Take Home Messages in Endocrinology
 Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Professor Ian Holdaway. Endocrinologist Auckland District Health Board
 Professor Ian Holdaway Endocrinologist Auckland District Health Board A land of milk and giants hormonesecreting pituitary tumours I M Holdaway, Endocrinologist, Auckland Acromegaly Prolactinomas Cushing
Professor Ian Holdaway Endocrinologist Auckland District Health Board A land of milk and giants hormonesecreting pituitary tumours I M Holdaway, Endocrinologist, Auckland Acromegaly Prolactinomas Cushing
CYSTIC PROLACTINOMA: A SURGICAL DISEASE?
 AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited,
Hypothalamus & Pituitary Gland
 Hypothalamus & Pituitary Gland Hypothalamus and Pituitary Gland The hypothalamus and pituitary gland form a unit that exerts control over the function of several endocrine glands (thyroid, adrenals, and
Hypothalamus & Pituitary Gland Hypothalamus and Pituitary Gland The hypothalamus and pituitary gland form a unit that exerts control over the function of several endocrine glands (thyroid, adrenals, and
Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury
 Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury BACKGROUND Trauma related acquired brain injury (ABI) is known to
Medical and Rehabilitation Innovations Neuroendocrine Screening and Hormone Replacement Therapy in Trauma Related Acquired Brain Injury BACKGROUND Trauma related acquired brain injury (ABI) is known to
15 month-old female with a cystic brain lesion. Magdalena Dumin, MD Pediatric Endocrinology Fellow University of Chicago December 4, 2014
 + 15 month-old female with a cystic brain lesion Magdalena Dumin, MD Pediatric Endocrinology Fellow University of Chicago December 4, 2014 + Chief Complaint 15 month-old female admitted to PICU for concern
+ 15 month-old female with a cystic brain lesion Magdalena Dumin, MD Pediatric Endocrinology Fellow University of Chicago December 4, 2014 + Chief Complaint 15 month-old female admitted to PICU for concern
Hyperprolactinemia in A 15-Year-Old Girl with Primary Amenorrhea
 Clin Pediatr Endocrinol 1996; 5(2), 61-66 Copyright (C) 1996 by The Japanese Society for Pediatric Endocrinology Hyperprolactinemia in A 15-Year-Old Girl with Primary Amenorrhea Toshihisa Okada, Soroku
Clin Pediatr Endocrinol 1996; 5(2), 61-66 Copyright (C) 1996 by The Japanese Society for Pediatric Endocrinology Hyperprolactinemia in A 15-Year-Old Girl with Primary Amenorrhea Toshihisa Okada, Soroku
A Combined Case of Macroprolactinoma, Growth Hormone Excess and Graves' Disease
 A Combined Case of Macroprolactinoma, Growth Hormone Excess and Graves' Disease Z Hussein, MRCP*, B Tress**, P G Cohnan, FRACP***... 'Department of Medicine, Hospital Putrajaya, Putrajaya, Presint 7, 62250
A Combined Case of Macroprolactinoma, Growth Hormone Excess and Graves' Disease Z Hussein, MRCP*, B Tress**, P G Cohnan, FRACP***... 'Department of Medicine, Hospital Putrajaya, Putrajaya, Presint 7, 62250
Disclosures. BMS, Ferring research grant funding NovoNordisk scientific advisory board Chiasma clinical trial investigator
 Pituitary Disorders Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes, and Hypertension Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures BMS, Ferring
Pituitary Disorders Ursula B. Kaiser, M.D. Chief, Division of Endocrinology, Diabetes, and Hypertension Brigham and Women s Hospital Professor of Medicine Harvard Medical School Disclosures BMS, Ferring
Endocrine Topic Review. Sethanant Sethakarun, MD
 Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Case Report. Michael H. Goldman, MD; Alison T. Gruber; Marc A. Herman, MD ABSTRACT
 Case Report CONCURRENT PANHYPOPITUITARISM AND HYPERPROLACTINEMIA DUE TO A GIANT INTERNAL CAROTID ANEURYSM REVEALED BY THYROID HORMONE WITHDRAWAL DURING FOLLOW-UP MANAGEMENT OF THYROID CANCER Michael H.
Case Report CONCURRENT PANHYPOPITUITARISM AND HYPERPROLACTINEMIA DUE TO A GIANT INTERNAL CAROTID ANEURYSM REVEALED BY THYROID HORMONE WITHDRAWAL DURING FOLLOW-UP MANAGEMENT OF THYROID CANCER Michael H.
Pituitary Apoplexy. Updated: April 22, 2018 CLINICAL RECOGNITION
 Pituitary Apoplexy Zeina C Hannoush, MD. Assistant Professor of Clinical Medicine. Division of Endocrinology, Diabetes and Metabolism. University of Miami, Miller School of Medicine. Roy E Weiss, MD, PhD,
Pituitary Apoplexy Zeina C Hannoush, MD. Assistant Professor of Clinical Medicine. Division of Endocrinology, Diabetes and Metabolism. University of Miami, Miller School of Medicine. Roy E Weiss, MD, PhD,
DIAGNOSTIC AND THERAPEUTIC APPROACH TO PITUITARY INCIDENTALOMAS. Anastasios N. Mavrakis, MD, 1 and Nicholas A. Tritos, MD, DSc, MMSc, FACE, FACP 2
 Review Article DIAGNOSTIC AND THERAPEUTIC APPROACH TO PITUITARY INCIDENTALOMAS Anastasios N. Mavrakis, MD, 1 and Nicholas A. Tritos, MD, DSc, MMSc, FACE, FACP 2 ABSTRACT Objective: To review data on epidemiology,
Review Article DIAGNOSTIC AND THERAPEUTIC APPROACH TO PITUITARY INCIDENTALOMAS Anastasios N. Mavrakis, MD, 1 and Nicholas A. Tritos, MD, DSc, MMSc, FACE, FACP 2 ABSTRACT Objective: To review data on epidemiology,
THE ANTERIOR PITUITARY. Embryology cont. Embryology of the pituitary BY MISPA ZUH HS09A179. Embryology cont. THE PITUIYARY GLAND Anatomy:
 THE ANTERIOR PITUITARY BY MISPA ZUH HS09A179 Embryology of the pituitary The pituitary is formed early in embryonic life from the fusion of the Rathke s pouch (anterior) and the diencephalon ( posterior)
THE ANTERIOR PITUITARY BY MISPA ZUH HS09A179 Embryology of the pituitary The pituitary is formed early in embryonic life from the fusion of the Rathke s pouch (anterior) and the diencephalon ( posterior)
Endocrine part two. Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy
 Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
In clinical series, pituitary tumors are the third most. Incidental pituitary adenomas
 Neurosurg Focus 31 (6):E18, 2011 Incidental pituitary adenomas Walavan Sivakumar, M.D., 1 Roukoz Chamoun, M.D., 1 Vinh Nguyen, M.D., 2 and William T. Couldwell, M.D., Ph.D. 1 Departments of 1 Neurosurgery
Neurosurg Focus 31 (6):E18, 2011 Incidental pituitary adenomas Walavan Sivakumar, M.D., 1 Roukoz Chamoun, M.D., 1 Vinh Nguyen, M.D., 2 and William T. Couldwell, M.D., Ph.D. 1 Departments of 1 Neurosurgery
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs
 Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC
 10 th Annual Canadian Endocrine Update 3 rd Canadian Endocrine Review Course Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC 10 th Annual Canadian Endocrine Update Dr.
10 th Annual Canadian Endocrine Update 3 rd Canadian Endocrine Review Course Peri-op Pituitary / Diabetes Insipidus/ Apoplexy Dr. Stan Van Uum, MD, PhD, FRCPC 10 th Annual Canadian Endocrine Update Dr.
Management of incidental pituitary microadenomas: a cost-effectiveness analysis King J T, Justice A C, Aron D C
 Management of incidental pituitary microadenomas: a cost-effectiveness analysis King J T, Justice A C, Aron D C Record Status This is a critical abstract of an economic evaluation that meets the criteria
Management of incidental pituitary microadenomas: a cost-effectiveness analysis King J T, Justice A C, Aron D C Record Status This is a critical abstract of an economic evaluation that meets the criteria
ABNORMAL PITUITARY FUNCTION
 Overview ABNORMAL PITUITARY FUNCTION Specialist Portfolio Seminar Katie Jones Sandwell and West Birmingham Hospitals NHS Trust Anterior pituitary overview Posterior pituitary overview Pituitary dysfunction
Overview ABNORMAL PITUITARY FUNCTION Specialist Portfolio Seminar Katie Jones Sandwell and West Birmingham Hospitals NHS Trust Anterior pituitary overview Posterior pituitary overview Pituitary dysfunction
Hyperprolactinemia. Justin Moore, MD
 Hyperprolactinemia Justin Moore, MD Biography.com The Miraculous Lactation of St. Bernard Bernard prayed before a statue of the Madonna, asking her, "Show yourself a mother" ("Monstra te esse Matrem").
Hyperprolactinemia Justin Moore, MD Biography.com The Miraculous Lactation of St. Bernard Bernard prayed before a statue of the Madonna, asking her, "Show yourself a mother" ("Monstra te esse Matrem").
No Financial Interest
 Pituitary Apoplexy Michael Vaphiades, D.O. Professor Department of Ophthalmology, Neurology, Neurosurgery University of Alabama at Birmingham, Birmingham, AL No Financial Interest N E U R O L O G I C
Pituitary Apoplexy Michael Vaphiades, D.O. Professor Department of Ophthalmology, Neurology, Neurosurgery University of Alabama at Birmingham, Birmingham, AL No Financial Interest N E U R O L O G I C
33-Year-Old Female With Amenorrhea DISHA KUMAR NARANG, MD PITUITARY ENDORAMA DECEMBER 11, 2014
 33-Year-Old Female With Amenorrhea DISHA KUMAR NARANG, MD PITUITARY ENDORAMA DECEMBER 11, 2014 Our Patient 33-year-old female presents to endocrinology clinic after amenorrhea for 4 years History of Present
33-Year-Old Female With Amenorrhea DISHA KUMAR NARANG, MD PITUITARY ENDORAMA DECEMBER 11, 2014 Our Patient 33-year-old female presents to endocrinology clinic after amenorrhea for 4 years History of Present
Pituitary Tumors: adenoma, craniopharyngioma, rathke cyst
 Pituitary Tumors: adenoma, craniopharyngioma, rathke cyst Overview Tumors that grow from the pituitary gland can affect the whole body by interfering with normal hormone levels. They can also cause headaches
Pituitary Tumors: adenoma, craniopharyngioma, rathke cyst Overview Tumors that grow from the pituitary gland can affect the whole body by interfering with normal hormone levels. They can also cause headaches
Reproductive Health and Pituitary Disease
 Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Reproductive Health and Pituitary Disease Janet F. McLaren, MD Assistant Professor Division of Reproductive Endocrinology and Infertility Department of Obstetrics and Gynecology jmclaren@uabmc.edu Objectives
Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary Tumor Apoplexy
 Case Reports in Obstetrics and Gynecology Volume 2013, Article ID 817603, 4 pages http://dx.doi.org/10.1155/2013/817603 Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary
Case Reports in Obstetrics and Gynecology Volume 2013, Article ID 817603, 4 pages http://dx.doi.org/10.1155/2013/817603 Case Report Successful Pregnancy in a Female with a Large Prolactinoma after Pituitary
David Henley. Sir Charles Gairdner Hospital, Nedlands WA University of Western Australia. ESA Seminar Weekend, Melbourne Vic 27 th May 2017
 David Henley Sir Charles Gairdner Hospital, Nedlands WA University of Western Australia ESA Seminar Weekend, Melbourne Vic 27 th May 2017 Disclosures Received honoraria from Ipsen, Novartis, Servier, Bristol-Myers
David Henley Sir Charles Gairdner Hospital, Nedlands WA University of Western Australia ESA Seminar Weekend, Melbourne Vic 27 th May 2017 Disclosures Received honoraria from Ipsen, Novartis, Servier, Bristol-Myers
X/00/$03.00/0 Vol. 85, No. 5 The Journal of Clinical Endocrinology & Metabolism Copyright 2000 by The Endocrine Society
 0021-972X/00/$03.00/0 Vol. 85, No. 5 The Journal of Clinical Endocrinology & Metabolism Printed in U.S.A. Copyright 2000 by The Endocrine Society The Dominant Role of Increased Intrasellar Pressure in
0021-972X/00/$03.00/0 Vol. 85, No. 5 The Journal of Clinical Endocrinology & Metabolism Printed in U.S.A. Copyright 2000 by The Endocrine Society The Dominant Role of Increased Intrasellar Pressure in
Pituitary gland diseases
 Pituitary gland diseases Pituitary Gland Weight 600 mg Is located within the sella turcica Anatomically and functionally distinct anterior and posterior lobes Pituitary Development The pituitary originate
Pituitary gland diseases Pituitary Gland Weight 600 mg Is located within the sella turcica Anatomically and functionally distinct anterior and posterior lobes Pituitary Development The pituitary originate
Pituitary gland Pituitary fossa Mass: 5 gms DIMENSIONS 7mm (Ht) 9mm (AP) 11m(transverse) originates from Rathke s pouch and infundibulum
 9mm (AP) 11m(transverse) originates from Rathke s pouch and infundibulum") Pituitary gland Pituitary fossa Mass: 5 gms DIMENSIONS 7mm (Ht) 9mm (AP) 11m(transverse) originates from Rathke s pouch and infundibulum Cell type hormone Clinical syndrome Tumor type Somatotroph Growth
Pituitary gland Pituitary fossa Mass: 5 gms DIMENSIONS 7mm (Ht) 9mm (AP) 11m(transverse) originates from Rathke s pouch and infundibulum Cell type hormone Clinical syndrome Tumor type Somatotroph Growth
Evaluation and management of pituitary incidentalomas
 REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: To outline an approach to the workup and management of patients with incidentally discovered pituitary masses DINA SERHAL, MD Department of Endocrinology, Diabetes,
REVIEW CME CREDIT EDUCATIONAL OBJECTIVE: To outline an approach to the workup and management of patients with incidentally discovered pituitary masses DINA SERHAL, MD Department of Endocrinology, Diabetes,
Laurie A. Loevner, MD
 Laurie A. Loevner, MD Chief, Division of Neuroradiology UPHS Professor of Radiology, Otorhinolaryngology: Head & Neck Surgery, Neurosurgery, and Ophthalmology University of Pennsylvania Health System Disclosures
Laurie A. Loevner, MD Chief, Division of Neuroradiology UPHS Professor of Radiology, Otorhinolaryngology: Head & Neck Surgery, Neurosurgery, and Ophthalmology University of Pennsylvania Health System Disclosures
Initials:.. Number of patient in the registry:... Date of visit:.. Gender (genetic): female / male
: female / male") 1. Patient personal details Institute code: Physician code: Initials:.. Number of patient in the registry:... Date of visit:.. Gender (genetic): female / male 2. Changes in acromegaly-specific medical
1. Patient personal details Institute code: Physician code: Initials:.. Number of patient in the registry:... Date of visit:.. Gender (genetic): female / male 2. Changes in acromegaly-specific medical
Pituitary Gland Disorders
 Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Pituitary Gland Disorders 1 2 (GH-RH) (CRH) (TRH) (TRH) (GTRH) (GTRH) 3 Classification of pituitary disorders: 1. Hypersecretory diseases: a. Acromegaly and gigantism: Usually caused by (GH)-secreting
Department of Neurosurgery and The California Center for Pituitary Disorders, University of California, San Francisco, California
 clinical article J Neurosurg 124:589 595, 2016 Improved versus worsened endocrine function after transsphenoidal surgery for nonfunctional pituitary adenomas: rate, time course, and radiological analysis
clinical article J Neurosurg 124:589 595, 2016 Improved versus worsened endocrine function after transsphenoidal surgery for nonfunctional pituitary adenomas: rate, time course, and radiological analysis
Non-Functioning Tumours and Pituitary Hormone Testing. Miguel Debono Consultant in Endocrinology
 Non-Functioning Tumours and Pituitary Hormone Testing Miguel Debono Consultant in Endocrinology Agenda Pituitary masses Non functioning pituitary adenomas Testing pituitary function Pituitary Hormone Replacement
Non-Functioning Tumours and Pituitary Hormone Testing Miguel Debono Consultant in Endocrinology Agenda Pituitary masses Non functioning pituitary adenomas Testing pituitary function Pituitary Hormone Replacement
Metastasis. 57 year old with progressive Headache and Right Sided Visual Loss
 Metastasis 1% of sellar/parasellar masses Usually occurs with known primary Can involve third ventricle, hypothalamus, infundibular stalk May be both supra-, intrasellar 57 year old with progressive Headache
Metastasis 1% of sellar/parasellar masses Usually occurs with known primary Can involve third ventricle, hypothalamus, infundibular stalk May be both supra-, intrasellar 57 year old with progressive Headache
Spontaneous remission of acromegaly and Cushing s disease following pituitary apoplexy: Two case reports
 CASE REPORT Spontaneous remission of acromegaly and Cushing s disease following pituitary apoplexy: Two case reports S.H.P.P. Roerink 1 *, E.J. van Lindert 2, A.C. van de Ven 1 Departments of 1 Internal
CASE REPORT Spontaneous remission of acromegaly and Cushing s disease following pituitary apoplexy: Two case reports S.H.P.P. Roerink 1 *, E.J. van Lindert 2, A.C. van de Ven 1 Departments of 1 Internal
Pituitary Stalk Interruption Syndrome. Leena Shahla, MD, PGY5 Endocrinology, Diabetes and Metabolism Fellowship University of Massachusetts
 Pituitary Stalk Interruption Syndrome Leena Shahla, MD, PGY5 Endocrinology, Diabetes and Metabolism Fellowship University of Massachusetts 11/12/2016 Case: NP, 42 year old female, from Dominican Republic.
Pituitary Stalk Interruption Syndrome Leena Shahla, MD, PGY5 Endocrinology, Diabetes and Metabolism Fellowship University of Massachusetts 11/12/2016 Case: NP, 42 year old female, from Dominican Republic.
Radiotherapy approaches to pituitary tumors
 Disclosures No relevant disclosures Radiotherapy approaches to pituitary tumors Pituitary Disorders: Advances in Diagnosis and Management Steve Braunstein, MD, PhD UCSF Department of Radiation Oncology
Disclosures No relevant disclosures Radiotherapy approaches to pituitary tumors Pituitary Disorders: Advances in Diagnosis and Management Steve Braunstein, MD, PhD UCSF Department of Radiation Oncology
Endocrine system overview
 Endocrine system overview Nature of the hormonal system -Major integrator of body function Classification of hormones Endocrine vs paracrine Nature of hormone-receptor systems Role of the hypothalamuspituitary
Endocrine system overview Nature of the hormonal system -Major integrator of body function Classification of hormones Endocrine vs paracrine Nature of hormone-receptor systems Role of the hypothalamuspituitary
Process / Evidence Class. Clinical Assessment / III
 Table 2: Endocrine Author Cozzi et al (2009) 1 Study Design: Prospectively followed case series. Fourteen patients had pre-op hypocortisolism. Patient Population: Seventy-two adult patients who underwent
Table 2: Endocrine Author Cozzi et al (2009) 1 Study Design: Prospectively followed case series. Fourteen patients had pre-op hypocortisolism. Patient Population: Seventy-two adult patients who underwent
Archives of Endocrinology and Metabolism
 Archives of Endocrinology and Metabolism This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction
Archives of Endocrinology and Metabolism This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction
The Management of adrenal incidentaloma
 The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
Silent ACTHoma: A subclinical presentation of Cushing s disease in a 79 year old male
 575 Silent ACTHoma: A subclinical presentation of Cushing s disease in a 79 year old male Meenal Malviya 1, Navneet Kumar 1*, Naseer Ahmad 2 1 MD; Department of Internal Medicine, Providence Hospital &
575 Silent ACTHoma: A subclinical presentation of Cushing s disease in a 79 year old male Meenal Malviya 1, Navneet Kumar 1*, Naseer Ahmad 2 1 MD; Department of Internal Medicine, Providence Hospital &
TREATMENT OF CUSHING S DISEASE
 TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
TREATMENT OF CUSHING S DISEASE Surgery, Radiation, Medication Peter J Snyder, MD Professor of Medicine Disclosures Novartis Research grant Pfizer Consultant Ipsen Research grant Cortendo Research grant
47 Year-Old Female with Headache. Olesya Krivospitskaya, MD Second year endocrinology fellow
 47 Year-Old Female with Headache Olesya Krivospitskaya, MD Second year endocrinology fellow HPI: 47 y.o. female presented to ER with c/o acute onset of headache at the vertex of her head and retro-orbital
47 Year-Old Female with Headache Olesya Krivospitskaya, MD Second year endocrinology fellow HPI: 47 y.o. female presented to ER with c/o acute onset of headache at the vertex of her head and retro-orbital
Visual pathways in the chiasm
 Visual pathways in the chiasm Intracranial relationships of the optic nerve Fixation of the chiasm Chiasmatic pathologies The function of the optic chiasm may be altered by the presence of : 4) Artero
Visual pathways in the chiasm Intracranial relationships of the optic nerve Fixation of the chiasm Chiasmatic pathologies The function of the optic chiasm may be altered by the presence of : 4) Artero
Treating Cystic Prolactinomas with Dopamine Agonists: Partial Cabergoline Resistance and Considering Dose Reduction
 Treating Cystic Prolactinomas with Dopamine Agonists: Partial Cabergoline Resistance and Considering Dose Reduction Mohammad Talha Rauf, MD Internal Medicine Resident PGY3 Dania AbuShanab, MD Julie Samantray,
Treating Cystic Prolactinomas with Dopamine Agonists: Partial Cabergoline Resistance and Considering Dose Reduction Mohammad Talha Rauf, MD Internal Medicine Resident PGY3 Dania AbuShanab, MD Julie Samantray,
DIMENSIONS 1 cm in diameter 0.5 to 1 gm in weight. LOCATION Sella turcica A bony cavity. DIVISIONS Anterior lobe Posterior lobe Pars intermedia
 DIMENSIONS 1 cm in diameter 0.5 to 1 gm in weight LOCATION Sella turcica A bony cavity DIVISIONS Anterior lobe Posterior lobe Pars intermedia body temperature autonomic nervous system emotional and food
DIMENSIONS 1 cm in diameter 0.5 to 1 gm in weight LOCATION Sella turcica A bony cavity DIVISIONS Anterior lobe Posterior lobe Pars intermedia body temperature autonomic nervous system emotional and food
NANOS Patient Brochure
 NANOS Patient Brochure Pituitary Tumor Copyright 2015. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for informational
NANOS Patient Brochure Pituitary Tumor Copyright 2015. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for informational
Pituitary Disorders Pearls
 Disclosures Pituitary Disorders Pearls Whitney Woodmansee M.D. Director, Clinical Neuroendocrine Program Brigham and Women s Hospital / Harvard Medical School Boston, MA July 21, 2012 Eli Lilly and Company-
Disclosures Pituitary Disorders Pearls Whitney Woodmansee M.D. Director, Clinical Neuroendocrine Program Brigham and Women s Hospital / Harvard Medical School Boston, MA July 21, 2012 Eli Lilly and Company-
A Boy with Optic Glioma
 Clin Pediatr Endocrinol 1994;3(Suppl 4): 169-173 Copyright(C)1994 by The Japanese Society for Pediatric Endocrinology Taisuke Okada, Sumitaka Dohno, Yousei Shimasaki, Takashi Tomoda, Makiko Koga, Kumiko
Clin Pediatr Endocrinol 1994;3(Suppl 4): 169-173 Copyright(C)1994 by The Japanese Society for Pediatric Endocrinology Taisuke Okada, Sumitaka Dohno, Yousei Shimasaki, Takashi Tomoda, Makiko Koga, Kumiko
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Secondary amenorrhoea Dr.ASMAA AL SANJARY
 Secondary amenorrhoea Dr.ASMAA AL SANJARY The student at the end of this lecture should be able to: Define secondary amenorrhoea. Classify the causes of secondary amenorrhoea. Describe the commonest three
Secondary amenorrhoea Dr.ASMAA AL SANJARY The student at the end of this lecture should be able to: Define secondary amenorrhoea. Classify the causes of secondary amenorrhoea. Describe the commonest three
Sharon maslovitz Lis Maternity Hospital
 Sharon maslovitz Lis Maternity Hospital Case report Chief complaint 27 yo, with PMC @ 31+3w, BCBA twins Complaints of severe rt parietal and retrobulbar headaches Conditions that may cause episodic headaches:
Sharon maslovitz Lis Maternity Hospital Case report Chief complaint 27 yo, with PMC @ 31+3w, BCBA twins Complaints of severe rt parietal and retrobulbar headaches Conditions that may cause episodic headaches:
High and Low GH: an update of diagnosis and management of GH disorders
 High and Low GH: an update of diagnosis and management of GH disorders Georgia Chapter-AACE 2017 Laurence Katznelson, MD Professor of Medicine and Neurosurgery Associate Dean of Graduate Medical Education
High and Low GH: an update of diagnosis and management of GH disorders Georgia Chapter-AACE 2017 Laurence Katznelson, MD Professor of Medicine and Neurosurgery Associate Dean of Graduate Medical Education
Case report. Open Access. Abstract
 Open Access Case report Hyperthyroidism unmasked several years after the medical and radiosurgical treatment of an invasive macroprolactinoma inducing hypopituitarism: a case report Luca Foppiani 1 *,
Open Access Case report Hyperthyroidism unmasked several years after the medical and radiosurgical treatment of an invasive macroprolactinoma inducing hypopituitarism: a case report Luca Foppiani 1 *,
Pituitary Incidentaloma: An Endocrine Society Clinical Practice Guideline
 SPECIAL FEATURE Clinical Practice Guideline Pituitary Incidentaloma: An Endocrine Society Clinical Practice Guideline Pamela U. Freda, Albert M. Beckers, Laurence Katznelson, Mark E. Molitch, Victor M.
SPECIAL FEATURE Clinical Practice Guideline Pituitary Incidentaloma: An Endocrine Society Clinical Practice Guideline Pamela U. Freda, Albert M. Beckers, Laurence Katznelson, Mark E. Molitch, Victor M.
Subject Index. hypothalamic-pituitary-adrenal axis 158. Atherosclerosis, ghrelin role AVP, see Arginine vasopressin.
 Subject Index Acromegaly, somatostatin analog therapy dopamine agonist combination therapy 132 efficacy 132, 133 overview 130, 131 receptor subtype response 131, 132 SOM30 studies 131, 132 ACTH, see Adrenocorticotropic
Subject Index Acromegaly, somatostatin analog therapy dopamine agonist combination therapy 132 efficacy 132, 133 overview 130, 131 receptor subtype response 131, 132 SOM30 studies 131, 132 ACTH, see Adrenocorticotropic
Pituitary tumour apoplexy within prolactinomas in children: a more aggressive condition?
 https://doi.org/10.1007/s11102-018-0900-8 Pituitary tumour apoplexy within prolactinomas in children: a more aggressive condition? Elizabeth Culpin 1 Matthew Crank 1 Mark Igra 2 Daniel J. A. Connolly 2
https://doi.org/10.1007/s11102-018-0900-8 Pituitary tumour apoplexy within prolactinomas in children: a more aggressive condition? Elizabeth Culpin 1 Matthew Crank 1 Mark Igra 2 Daniel J. A. Connolly 2
By: Mohammad Jomaa & Amer Al-Salamat. Lec:Pathology of pituitary gland. **Sheet contain the slide in Bold. **some book information in Red.
 By: Mohammad Jomaa & Amer Al-Salamat Lec:Pathology of pituitary gland **Sheet contain the slide in Bold. **some book information in Red. Pathology of pituitary gland Before we start :( from book) The endocrine
By: Mohammad Jomaa & Amer Al-Salamat Lec:Pathology of pituitary gland **Sheet contain the slide in Bold. **some book information in Red. Pathology of pituitary gland Before we start :( from book) The endocrine