B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
|
|
|
- Dwayne Randall
- 5 years ago
- Views:
Transcription
1 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a higher frequency of follicular carcinomas.
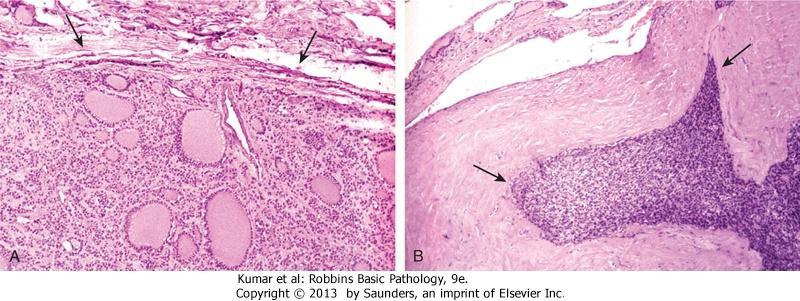
2 1. Papillary Carcinoma : - Is most the most common form - accounts for the majority of thyroid carcinomas associated with previous exposure to ionizing radiation. - The most common thyroid cancer in children - May occur at any age, Gross: Either solitary or multifocal lesions Microscopically 1. The nuclei of papillary carcinoma cells a.are optically clear nuclei, or "Orphan Annie eye" nuclei. b. Have pseudoinclusions)
3 2. A papillary architecture is common 3. Concentrically calcified structures(psammoma bodies) 4. Foci of lymphatic permeation by tumor cells are present, with metastases to cervical lymph nodes in half of cases. 5. but invasion of blood vessels is uncommon Variants: The most common is follicular variant associated with a lower incidence of lymph node metastases and extrathyroidal extension than that for conventional type

4 Papillary carcinoma
5 Clinical Features of papillary carcinomas a. Are nonfunctional tumors manifest as painless mass in the neck, either within the thyroid or as metastasis in a cervical lymph node b. Are indolent lesions, with 10-year survival rates of 95%. c. The presence of isolated cervical nodal metastases. does not have a influence on good prognosis of these lesions.
6 d. In a minority of patients, hematogenous metastases are present at the time of diagnosis, most commonly to lung - The bad prognostic factors are: a. Tumors arising in patients older than 60 b. The presence of extrathyroidal extension c. Presence of distant metastases (stage)
7 2. Follicular Carcinoma : -- More common in women and in areas with dietary iodine deficiency (accounting for 25% to 40% of thyroid cancers in these regions). - The peak incidence between the ages of 40 and 60 years Pathologically It may be a. Widely invasive, infiltrating the thyroid parenchymaand extrathyroidal soft tissues, or b. Minimally invasive that may be impossible to distinguish from follicular adenomas on gross examination and.
8 and/or vascular invasion to differentiate it from follicular adenoma Clinical Features - Manifest frequently as solitary cold thyroid nodule. - Tend to metastasize through hematogenous routes to lungs, bone, and liver but uncommon regional nodal metastases are uncommon. - Half of patients with widely invasive carcinomas succumb to their disease within 10 years, -less than 10% of patients with minimally invasive follicular carcinomas die within the same time span.
9 Follicular carcinoma
10 - Are treated with surgical excision. - Because better-differentiated lesions may be stimulated by TSH, patients usually are placed on a thyroid hormone regimen after surgery to suppress endogenous TSH..
11 3. Anaplastic Carcinoma - Are undifferentiated tumors of the thyroid epithelium, with mean age of 65 years. - They are aggressive, with a mortality rate of 100%. - Approximately 1/4 th of patients have a past history a well-differentiated carcinoma, and harbor a welldifferentiated tumor in the resected specimen Metastases to distant sites are common, but death occurs in less than 1 year as a result of aggressive local growth which compromise of vital structures in the neck.
12 4. Medullary Carcinoma - Are neuroendocrine neoplasms. - Secrete calcitonin, the measurement of which plays an important role in the diagnosis and postoperative follow-up evaluation of patients. - In some cases, the tumor cells elaborate, serotonin, and vasoactive intestinal peptide (VIP) - Are sporadic in about 70% of cases - 30% are familial cases
13 a. Occurring in the setting of MEN syndrome 2A or 2B, have been reported in younger patients, including children b. or familial medullary thyroid carcinoma without an associated MEN syndrome Note: Both familial and sporadic forms demonstrate activating RET mutations. - Sporadic medullary carcinomas, as well as familial cases without an associated MEN syndrome, occur in adults, with a peak incidence in the fifth and sixth decades.
14 . MORPHOLOGY - Multicentricity is particularly common in familial cases. On microscopic examination, - The tumor cells may form nests, trabeculae, and even follicles. - Amyloid deposits, derived from calcitonin molecules, are present in the adjacent stroma in many cases - Calcitonin is readily demonstrable both within the cytoplasm of the tumor cells or amyloid
15 - Familial cases are characterized by the presence of multicentric C cell hyperplasia in the surrounding thyroid parenchyma, a feature usually absent in sporadic lesions. - And these foci are believed to represent the precursor lesions from which medullary carcinomas arise Clinical Features - The sporadic cases manifests most often as a mass in the neck, sometimes associated with dysphagia or hoarseness.

16 Medullary carcinoma
17 - In some instances, the initial manifestations are caused by the secretion of a peptide hormone (e.g., diarrhea caused by the secretion of VIP). - Screening of the patient's relatives for elevated calcitonin levels or RET mutations permits early detection of tumors in familial cases - All members of MEN-2 kindreds carrying RET mutations are offered prophylactic thyroidectomies to prevent the development of medullary carcinomas
18 - Often, the only finding in the resected thyroid of these asymptomatic carriers is the presence of C cell hyperplasia or small (<1 cm) micromedullary carcinomas.
19 II. Parathyroid gland
20 I. HYPERPARATHYROIDISM : 3 categories a. Primary Hyperparathyroidism - Is a common disorder and important cause of hypercalcemia - There has been an increase in the detection of cases as a result of the routine inclusion of serum calcium assays in testing for a variety of clinical conditions Causes of primary hyperparathyrpoidism 1. Parathyroid adenoma (85% to 95%) 2. Primary parathyroid hyperplasia-5% to 10%. 3. Parathyroid carcinoma-(1%)
21 Genetic changes in parathyroid adenoma 1. Cyclin D1 is overexpressed in 40% of adenomas, 2. MEN1 mutations: About 20% to 30% of parathyroid tumors not associated with the MEN-1 syndrome have mutations in both copies of the MEN1 gene
22 Primary hyperparathyroidism - is a disease of adults and is much more common in women than in men. - The most common manifestation is an increase in serum calcium and is the most common cause of clinically silent hypercalcemia. - The most common cause of clinically apparent hypercalcemia in adults is a. paraneoplastic syndromes associated with malignancy
23 b. and bone metastases Lab findings a- In persons with hypercalcemia caused by parathyroid hyperfunction, serum PTH is inappropriately elevated b. in hypercalcemia due to non parathyroid diseases, serum PTH is low to undetectable c. Hypophosphatemia d. Increased urinary excretion of calcium and phosphate
24 Clinical Manifestations : - Traditionally has been associated with a constellation of symptoms "painful bones, renal stones, abdominal groans, psychic moans. 1. Pain was at one time a prominent manifestation of primary hyperparathyroidism and is secondary to a. Fractures of bones b. and resulting from renal stones c. Pancreatitis and gall stones d. Peptic ulcer
25 Note; - Because serum calcium is now routinely assessed in the most patients who need blood tests for other conditions, clinically silent hyperparathyroidism is detected early. - Hence, many of the classic clinical manifestations,, are seen much less frequently. 2. Gastrointestinal disturbances, including constipation, nausea, peptic ulcers, pancreatitis, and gallstones
26 3. CNS alterations, - depression, lethargy, and seizures 4. Neuromuscular abnormalities,- weakness and hypotonia 5. Polyuria and secondary polydipsia
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS. BY: Shifaa Qa qa
 NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Lec : NEOPLASMS OF THE THYROID,PATHOLOGY OF PARATHYROID GLAND
 By: Saef B Al-Abbadi Lec : NEOPLASMS OF THE THYROID,PATHOLOGY OF PARATHYROID GLAND Note: I brought a lot of information from the book to make this lecture easier to understand let s go ;) thyroid nodules>>
By: Saef B Al-Abbadi Lec : NEOPLASMS OF THE THYROID,PATHOLOGY OF PARATHYROID GLAND Note: I brought a lot of information from the book to make this lecture easier to understand let s go ;) thyroid nodules>>
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
Goiter, Nodules and Tumors
 Goiter, Nodules and Tumors Howard J. Sachs, MD www.12daysinmarch.com Thyroid Cancer Anaplastic Medullary Thyroid Cancer Anaplastic Medullary Thyroid Cancer Anaplastic Medullary Anaplastic Medullary MEN
Goiter, Nodules and Tumors Howard J. Sachs, MD www.12daysinmarch.com Thyroid Cancer Anaplastic Medullary Thyroid Cancer Anaplastic Medullary Thyroid Cancer Anaplastic Medullary Anaplastic Medullary MEN
Calcitonin. 1
 Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Disclosures. Parathyroid Pathology. Objectives. The normal parathyroid 11/10/2012
 Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Endocrine system pathology
 Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
Thyroid and Parathyroid Disease. RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010
 Thyroid and Parathyroid Disease RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010 Case Presentation # 1 CC: Neck Mass HPI: 51f found to have a neck mass on routine PE.
Thyroid and Parathyroid Disease RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010 Case Presentation # 1 CC: Neck Mass HPI: 51f found to have a neck mass on routine PE.
Chapter 14: Thyroid Cancer
 The American Academy of Otolaryngology Head and Neck Surgery Foundation (AAO-HNSF) Presents... Chapter 14: Thyroid Cancer Daiichi Pharmaceutical Corporation, marketers and distributors of FLOXIN Otic (ofloxacin
The American Academy of Otolaryngology Head and Neck Surgery Foundation (AAO-HNSF) Presents... Chapter 14: Thyroid Cancer Daiichi Pharmaceutical Corporation, marketers and distributors of FLOXIN Otic (ofloxacin
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
PEDIATRIC THYROID MALIGNACY
 PEDIATRIC THYROID MALIGNACY Anthony Sheyn MD Assistant Professor of Otolaryngology Head and Neck Surgery University of Tennessee Health Science Center Thyroid nodules 20 per 1000 children nodules in children
PEDIATRIC THYROID MALIGNACY Anthony Sheyn MD Assistant Professor of Otolaryngology Head and Neck Surgery University of Tennessee Health Science Center Thyroid nodules 20 per 1000 children nodules in children
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Thyroid and Parathyroid Surgery
 Med 5 Surgery Refresher Course 2013 2014 Thyroid and Parathyroid Surgery Dr Shirley Liu Resident Specialist Honorary Clinical Assistant Professor Team 2 Surgery Prince of Wales Hospital Case scenario:
Med 5 Surgery Refresher Course 2013 2014 Thyroid and Parathyroid Surgery Dr Shirley Liu Resident Specialist Honorary Clinical Assistant Professor Team 2 Surgery Prince of Wales Hospital Case scenario:
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Nodules. Family Medicine Refresher Course Geeta Lal MD, FACS April 2, No financial disclosures
 Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
An Alphabet Soup of Thyroid Neoplasms
 Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
10/24/2008. Surgery for Well-differentiated Thyroid Carcinoma- The Primary
 Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Surgery for Well-differentiated Thyroid Carcinoma- The Primary Head and Neck Endocrine Surgery Department of Otolaryngology-Head and Neck Surgery, UCSF October 24-25, 2008 Robert A. Sofferman, MD Professor
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Neoplasia literally means "new growth.
 NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
NEOPLASIA Neoplasia literally means "new growth. A neoplasm, defined as "an abnormal mass of tissue the growth of which exceeds and is uncoordinated with that of the normal tissues and persists in the
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE
 HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
Thyroid and Adrenal Gland
 Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
encapsulated thyroid nodule with a follicular architecture and some form of atypia. The problem is when to diagnose
 Histological Spectrum of Papillary Carcinoma of Thyroid A Two Years Study Gomathi Srinivasan 1, M. Vennila 2 1 Associate Professor Pathology, Government Medical College, Omandurar Estate, Chennai 600 002
Histological Spectrum of Papillary Carcinoma of Thyroid A Two Years Study Gomathi Srinivasan 1, M. Vennila 2 1 Associate Professor Pathology, Government Medical College, Omandurar Estate, Chennai 600 002
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
The parathyroid glands participate in the regulation
 41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
hypercalcemia of malignancy hyperparathyroidism PHPT the most common cause of hypercalcemia in the outpatient setting the second most common cause
 hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
BREAST PATHOLOGY. Fibrocystic Changes
 BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
BREAST PATHOLOGY Lesions of the breast are very common, and they present as palpable, sometimes painful, nodules or masses. Most of these lesions are benign. Breast cancer is the 2 nd most common cause
OUTLINE. Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis
 THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
MEDULLARY THYROID CANCER and RELATED MEN SYNDROMES. Irina Kovatch, MD SUNY Downstate Medical Center Grand Rounds January 26 th, 2012
 MEDULLARY THYROID CANCER and RELATED MEN SYNDROMES Irina Kovatch, MD SUNY Downstate Medical Center Grand Rounds January 26 th, 2012 Thyroid Cancer Comprises 95% of all endocrine malignancies and 1.5% of
MEDULLARY THYROID CANCER and RELATED MEN SYNDROMES Irina Kovatch, MD SUNY Downstate Medical Center Grand Rounds January 26 th, 2012 Thyroid Cancer Comprises 95% of all endocrine malignancies and 1.5% of
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Note: The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
- In the 15- to 34-year-old age group, they are the most common tumors of men. - Tumors of the testis are a heterogeneous group of neoplasms that include: I. Germ cell tumors : 95%; all are malignant.
HYPERCALCEMIA. Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences
 HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
HYPERCALCEMIA Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra hospital, Isfahan university of medical sciences ESSENTIALS OF DIAGNOSIS Serum calcium level > 10.5 mg/dl Serum ionized
WTC 2013 Panel Discussion: Minimal disease
 WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
WTC 2013 Panel Discussion: Minimal disease Susan J. Mandel MD MPH Panelists Ken Ain Yasuhiro Ito Stephanie Lee Erich Sturgis Mark Urken Faculty/Presenter Disclosure Relationships with commercial interests
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Index. Surg Oncol Clin N Am 15 (2006) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
3/29/2012. Thyroid cancer- what s new. Thyroid Cancer. Thyroid cancer is now the most rapidly increasing cancer in women
 Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid cancer- what s new Thyroid Cancer Changing epidemiology Molecular markers Lymph node dissection Technical advances rhtsh Genetic testing and prophylactic surgery Vandetanib What s new? Jessica
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
1. Protocol Summary Summary of Trial Design. IoN
 1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
1. Protocol Summary 1.1. Summary of Trial Design Title: Short Title/acronym: IoN Is ablative radioiodine Necessary for low risk differentiated thyroid cancer patients IoN EUDRACT no: 2011-000144-21 Sponsor
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine
 Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Maram Abdaljaleel, MD Dermatopathologist and Neuropathologist University of Jordan, School of Medicine The most common non-skin malignancy of women 2 nd most common cause of cancer deaths in women, following
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid pathology Practical part
 Thyroid pathology Practical part My Algorithm After a good macroscopy and a microscopic overview of the lesion, I especially look at the capsule and the thyroid just above and just beneath the capsule.
Thyroid pathology Practical part My Algorithm After a good macroscopy and a microscopic overview of the lesion, I especially look at the capsule and the thyroid just above and just beneath the capsule.
Thyroid Cancer. With 51 Figures and 30 Tables. Springer
 H.-J. Biersack F. Griinwald (Eds.) Thyroid Cancer With 51 Figures and 30 Tables Springer PART 1 Basics 1 The Changing Epidemiology of Thyroid Cancer 3 R. GORGES 1.1 Basic Epidemiological Problems in Thyroid
H.-J. Biersack F. Griinwald (Eds.) Thyroid Cancer With 51 Figures and 30 Tables Springer PART 1 Basics 1 The Changing Epidemiology of Thyroid Cancer 3 R. GORGES 1.1 Basic Epidemiological Problems in Thyroid
Basement membrane in lobule.
 Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Bahram Memar, MD Basement membrane in lobule. Normal lobule-luteal phase Normal lobule-follicular phase Lactating breast Greater than 95% are adenocarcinomas in situ carcinomas and invasive carcinomas.
Calcium metabolism and the Parathyroid Glands. Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands
 Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
Calcium metabolism and the Parathyroid Glands Calcium, osteoclasts and osteoblasts-essential to understand the function of parathyroid glands Calcium is an essential element for contraction of voluntary/smooth
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Carcinoma of thyroid - clinical presentation and outcome
 Med. J. Malaysia Vol. 46 No. 3 September 1991 Carcinoma of thyroid - clinical presentation and outcome K. Sothy, MBBS M. Mafauzy, MBBS, MRCP, M.Med. Sci. W.B. Wan Mohamad, MD, MRCP B.E. Mustaffa, MBBS,
Med. J. Malaysia Vol. 46 No. 3 September 1991 Carcinoma of thyroid - clinical presentation and outcome K. Sothy, MBBS M. Mafauzy, MBBS, MRCP, M.Med. Sci. W.B. Wan Mohamad, MD, MRCP B.E. Mustaffa, MBBS,
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
A rare case of solitary toxic nodule in a 3yr old female child a case report
 Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms
 Hindawi Publishing Corporation Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Hindawi Publishing Corporation Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
ظظظ/ -Dana Alrafaiah. -Amani Nofal. - MousaAlabbadi. 1 P a g e
 ظظظ/ -2 -Dana Alrafaiah -Amani Nofal - MousaAlabbadi 1 P a g e You don t need to go back to slide from 34-77 to any info. Only check the clinical picture. From the last lecture, adenomas can be functional
ظظظ/ -2 -Dana Alrafaiah -Amani Nofal - MousaAlabbadi 1 P a g e You don t need to go back to slide from 34-77 to any info. Only check the clinical picture. From the last lecture, adenomas can be functional
Epithelial tumors. Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev
 Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Epithelial tumors Dr. F.F. Khuzin, PhD Dr. M.O. Mavlikeev Epithelial tumors Tumors from the epithelium are the most frequent among tumors. There are 2 group features of these tumors: The presence in most
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate (start to develop symptoms) 3.0 3.4
Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
 yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
THE FOLLICULAR VARIANT OF PAPILLARY THYROID CARCINOMA AND NIFTP
 THE FOLLICULAR VARIANT OF PAPILLARY THYROID CARCINOMA AND NIFTP FOLLICULAR VARIANT OF PAPILLARY CARCINOMA HISTORICAL PERSPECTIVE FOLLICULAR VARIANT OF PAPILLARY CARCINOMA 1960 described by Dr. Stuart Lindsay
THE FOLLICULAR VARIANT OF PAPILLARY THYROID CARCINOMA AND NIFTP FOLLICULAR VARIANT OF PAPILLARY CARCINOMA HISTORICAL PERSPECTIVE FOLLICULAR VARIANT OF PAPILLARY CARCINOMA 1960 described by Dr. Stuart Lindsay
CARCINOMA OF THYROID Muhammad Shuja Tahir, FRCS
 Indep Rev Oct-Dec 2017;19(10-12) CARCINOMA OF THYROID Muhammad Shuja Tahir, FRCS IR-465 Abstract: Carcinoma of thyroid is a malignant tumour of thyroid commonly occurring in both young and old age patients.
Indep Rev Oct-Dec 2017;19(10-12) CARCINOMA OF THYROID Muhammad Shuja Tahir, FRCS IR-465 Abstract: Carcinoma of thyroid is a malignant tumour of thyroid commonly occurring in both young and old age patients.
Diffuse Follicular Variant of Papillary Thyroid Carcinoma in a 69-Year-old Man with Extensive Extrathyroidal Extension: A Case Report
 SE REPORT Oncology & Hematology http://dx.doi.org/10.3346/jkms.2013.28.3.480 J Korean Med Sci 2013; 28: 480-484 Diffuse Follicular Variant of Papillary Thyroid arcinoma in a 69-Year-old Man with Extensive
SE REPORT Oncology & Hematology http://dx.doi.org/10.3346/jkms.2013.28.3.480 J Korean Med Sci 2013; 28: 480-484 Diffuse Follicular Variant of Papillary Thyroid arcinoma in a 69-Year-old Man with Extensive
Thyroid Diseases. Dr Rodney Itaki Lecturer Anatomical Pathology Discipline
 Thyroid Diseases Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology This is the normal appearance of thethyroid
Thyroid Diseases Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology This is the normal appearance of thethyroid
Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff.
, taken without using a cuff.") Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
Authoriser: Fiona Davidson Page 1 of 5 Hypercalcaemia Definition Elevated Adjusted Calcium > 2.6 mmol/l (adjusted for albumin), taken without using a cuff. Mild (usually no symptoms) 2.6 3.0 mmol/l Moderate
ABSITE Review. RTC Conference Christina Bailey January 15, 2009
 ABSITE Review RTC Conference Christina Bailey January 15, 2009 How It s Broken Down? 220 questions Junior level (PGY 1 and 2) Exam 60% Basic Science 40% Clinical Management Senior Level (PGY 3-5) exam
ABSITE Review RTC Conference Christina Bailey January 15, 2009 How It s Broken Down? 220 questions Junior level (PGY 1 and 2) Exam 60% Basic Science 40% Clinical Management Senior Level (PGY 3-5) exam
Disclosure. Relevant Financial Relationship(s) None. Off Label Usage None MFMER slide-1
 None. Off Label Usage None MFMER slide-1") Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Disclosure Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-1 Case Presentation A 43 year old male, with partial nephrectomy for a right kidney mass 2013 MFMER slide-2 2013
Persistent & Recurrent Differentiated Thyroid Cancer
 Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Persistent & Recurrent Differentiated Thyroid Cancer Electron Kebebew University of California, San Francisco Department of Surgery Objectives Risk factors for persistent & recurrent disease Causes of
Diseases of the breast (2 of 2) Breast cancer
 Breast cancer") Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
Diseases of the breast (2 of 2) Breast cancer Epidemiology & etiology The most common type of cancer & the 2 nd most common cause of cancer death in women 1 of 8 women in USA Affects 7% of women Peak at
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Objectives. 1)To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy
To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy") Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
An Unexpected Cause of Hypoglycemia
 An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
INDEX. Note: Page numbers of issue and article titles are in boldface type. cell carcinoma. ENDOCRINE SURGERY
 ENDOCRINE SURGERY INDEX Note: Page numbers of issue and article titles are in boldface type. Adenylate cyclase, in signal transduction 425-426 Adrenal incidentalomas, 499-509 imaging of, 502-504 in patients
ENDOCRINE SURGERY INDEX Note: Page numbers of issue and article titles are in boldface type. Adenylate cyclase, in signal transduction 425-426 Adrenal incidentalomas, 499-509 imaging of, 502-504 in patients
Neuroendocrine Tumors
 Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
-The cause of testicular neoplasms remains unknown
 - In the 15- to 34-year-old age group, they are the most common tumors of men. - include: I. Germ cell tumors : (95%); all are malignant. II. Sex cord-stromal tumors: from Sertoli or Leydig cells; usually
- In the 15- to 34-year-old age group, they are the most common tumors of men. - include: I. Germ cell tumors : (95%); all are malignant. II. Sex cord-stromal tumors: from Sertoli or Leydig cells; usually
PRIMARY HYPERPARATHYROIDISM PRIMARY HYPERPARATHYROIDISM. Hyperparathyroidism Etiology. Common Complex Insidious Chronic Global Only cure is surgery
 ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms
 Case Reports in Pathology Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Case Reports in Pathology Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy
 "Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
Pediatric Thyroid Cancer Lung Metastases. Liora Lazar MD
 Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Pediatric Thyroid Cancer Lung Metastases Liora Lazar MD Differentiated thyroid cancer (DTC) The 3rd most common solid tumor in childhood and adolescence Accounting for 1.5%-3% of all childhood cancers
Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination
 Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Histogenesis of medullary carcinoma of the thyroid
 J. clin. Path., (1966), 19, 114 E. D. WILLIAMS1 From the Institute ofpathology, The London Hospital SYNOPSIS Thirty-one dog thyroid tumours and 28 spontaneous rat thyroid tumours were studied histologically
J. clin. Path., (1966), 19, 114 E. D. WILLIAMS1 From the Institute ofpathology, The London Hospital SYNOPSIS Thirty-one dog thyroid tumours and 28 spontaneous rat thyroid tumours were studied histologically
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Gerard M. Doherty, MD
 Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Reoperative central neck surgery
 Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Reoperative central neck surgery R. Pandev, I. Tersiev, M. Belitova, A. Kouizi, D. Damyanov University Clinic of Surgery, Section Endocrine Surgery University Hospital Queen Johanna ISUL Medical University
Oncogenes/Growth Factors & Environment
 Oncogenes/Growth Factors & Environment 8 th Postgraduate Course in Endocrine Surgery Crete, Greece September, 2006 Orlo H. Clark M.D. Thyroid Cancer Thyroid cancer is the 8 th most common and most rapidly
Oncogenes/Growth Factors & Environment 8 th Postgraduate Course in Endocrine Surgery Crete, Greece September, 2006 Orlo H. Clark M.D. Thyroid Cancer Thyroid cancer is the 8 th most common and most rapidly
Lung tumors & pleural lesions
 Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration
 AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
Thyroid Ultrasonography: clinical and radiological correlations
 Thyroid Ultrasonography: clinical and radiological correlations Dr.M.Thijs Radiology Anatomy Inflammatory Thyroid Disease Benign lesions Thyroid tumors Thyroglossal duct cyst Anatomy Transverse Longitudinal
Thyroid Ultrasonography: clinical and radiological correlations Dr.M.Thijs Radiology Anatomy Inflammatory Thyroid Disease Benign lesions Thyroid tumors Thyroglossal duct cyst Anatomy Transverse Longitudinal