BILATERAL ABDUCTOR VOCAL CORD PALSY. Dr NITYA G Final year PG KIMS
|
|
|
- Maximilian Carr
- 5 years ago
- Views:
Transcription
1 BILATERAL ABDUCTOR VOCAL CORD PALSY Dr NITYA G Final year PG KIMS
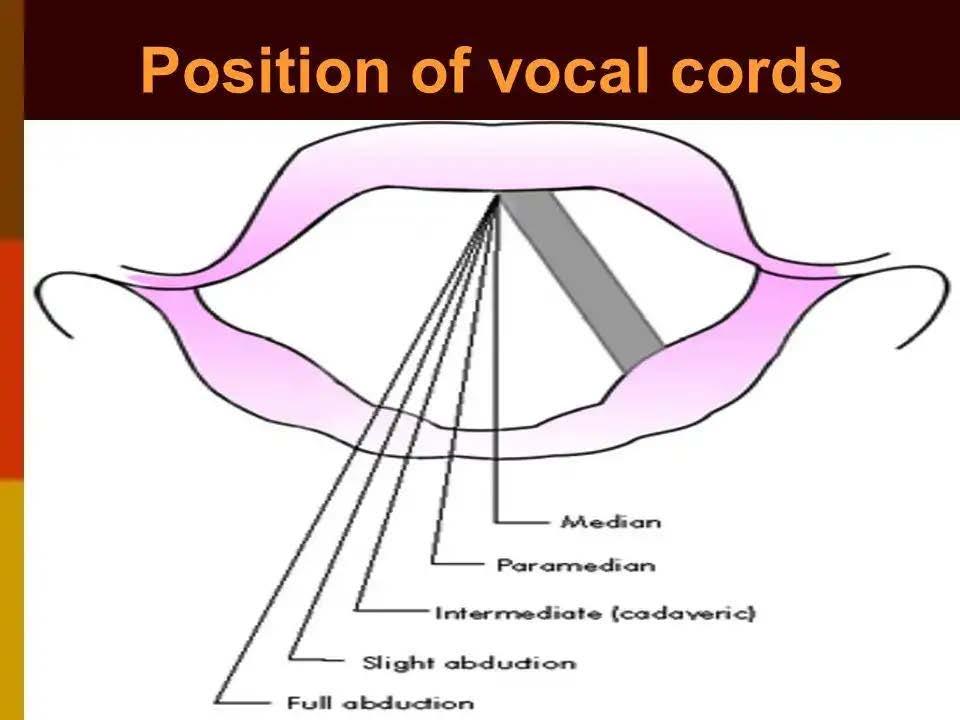
2 INTRODUCTION Vocal cord paralysis is a sign of a disease It results from dysfunction of Recurrent laryngeal nerves on both sides Paralysis of abductors of both the cords causes vocal cords to lie in the midline/ paramedian position This compromises airway and causes respiratory distress (aggravated by Bernoulli s effect) - STRIDOR Patients usually have a good voice and cough Aspiration and dysphagia not seen until unless SLN is involved The severity of stridor depends on the exertion
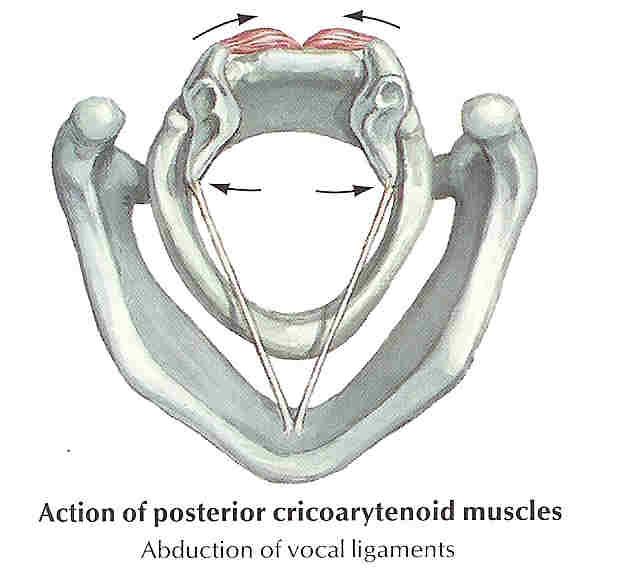
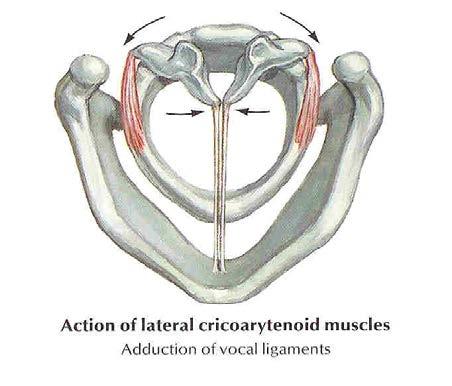
3 ANATOMY 1. Muscles acting on vocal cords Abductor - Posterior cricoarytenoid Adductors - Lateral cricoarytenoid Transverse arytenoids Thyroarytenoids Cricothyroid (weak) Tensors -Thyroarytenoids (vocalis) Cricothyroid


4
5
6
7 ETIOLOGY Iatrogenic (82.8%) Thyroidectomy Cervical oesophageal surgeries Tracheal surgeries Intubation injuries Radiation Malignancy (8.6%) Oesophageal cancer Thyroid cancer Cervical nodal metastasis Lung cancer Neurological (3.8%) Brainstem ischemia Arnold chiari malformation Head injuries PCF tumors Mechanical (2.7%) NG tube syndrome Stent placement in proximal oesophagus Idiopathic (2.2%) Viral infections
8
9 WAGNER GROSSMAN THEORY In complete paralysis of recurrent laryngeal nerve, the cord lies in paramedian position due to intact cricothyroid muscle which is a weak adductor of the cord
10 SEMON S LAW In course of a gradually progressing organic lesion involving Recurrent laryngeal nerve, the fibres supplying the abductors of the vocal cords are involved much earlier than the adductors - 1 st stage abductors damaged with weak adduction - 2 nd stage cords midline and immobile - 3 rd stage cords in cadaveric position
11 CLINICAL PRESENTATION Chief presenting complaint is typically shortness of breath or stridor Degree of airway compromise is variable and can range from mild stridor on exertion to life threatening airway obstruction No hoarseness of voice due to close proximity of immobile cords Voice monotone Speech short hurried phrases interrupted by stridorous inspiration
12 CLINICAL HISTORY Symptoms of etiology like H/O Trauma Fever with evening rise Weight loss Reduced appetite Swelling in neck Symptoms of hypo/hyperthyroidism Limb weakness / numbness Previous surgeries Prolonged intubation Radiation exposure Smoking

13 CLINICAL EXAMINATION Examination of cranial nerves Indirect laryngoscopy Direct laryngoscopy to rule out local causes and to assess the CA joint fixity Vocal cords are in paramedian position
14 INVESTIGATIONS For diagnosis and morbidity assessment Rigid endoscopy ( 30 o / 70 o ) Fibre optic laryngoscopy (FOL) Laryngeal electromyography (LEMG) - Differentiate between VCP, synkinetic activity, CA joint fixation - Determining the prognosis for recovery - Differentiate muscular and neurological causes
15 LEMG
16 Routine blood investigations CBP ESR RBS Rheumatoid factor Parathormone levels VDRL Thyroid profile
17 Radiological CECT skull base to aortic arch Gadolinium enhanced MRI Brain Barium swallow CT chest Targeted FNAC/biopsy (if any lesion detected)
18 SURGICAL MANAGEMENT AIRWAY MANAGEMENT 1. Tracheostomy CORD PROCEDURES STATIC PROCEDURES 1. Posterior cordectomy 2. Arytenoidectomy 3. Arytenoidopexy DYNAMIC PROCEDURES 1. Nerve pedicle transfer 2. Pacing of vocal cords 3. Botox injection
19 FRAMEWORK SURGERIES 1. Type II thyroplasty 2. Posterior cricoid lamina split OTHERS 1. Gene therapy 2. Stem cell therapy
20 TRACHEOSTOMY Warranted in acute respiratory embarrassment Temporary management Immediate relief of airway obstruction Indicated Expecting spontaneous recovery If surgical expertise/facilities not available If dynamic/framework procedures are planned that do not provide immediate relief from airway obstruction Complications infections, granulations, aphonia (can be overcome with a speaking valve)
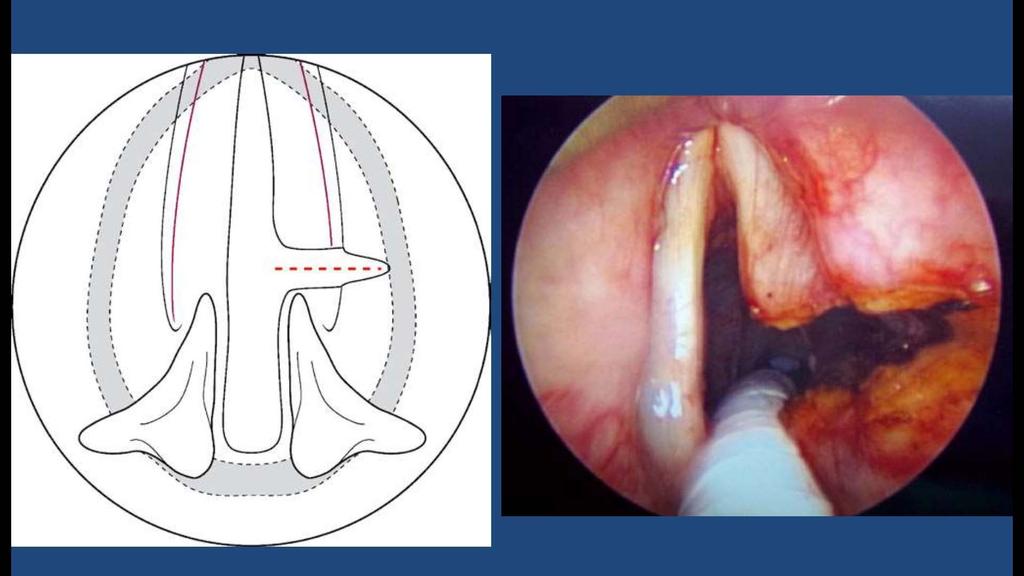
21 POSTERIOR CORDECTOMY Irreversible procedure 2 approaches 1. Laryngofissure 2. Microlaryngoscopy and CO 2 LASER cordectomy (KASHIMA procedure) Dissection focussed on submucosa, preserving mucosa to avoid scarring and voice disturbance C shaped wedge of posterior vocal fold excised Susceptible to granulation formation, rough (when LASER not used) and breathy voice
22
23

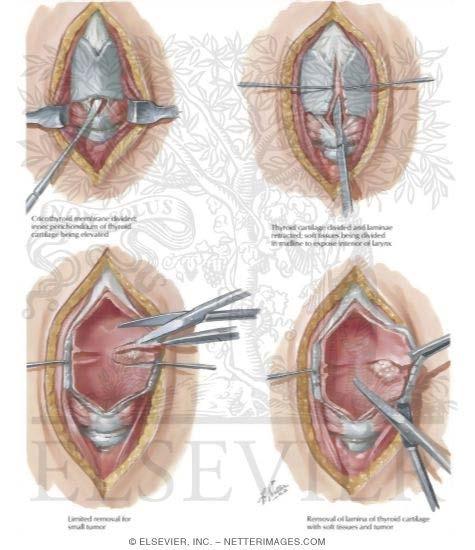
24 ARYTENOIDECTOMY Permanent and irreversible Glottis expanded in transverse axis - Woodman s approach (Lateral neck approach) - Anterior laryngofissure procedure Expose arytenoids resect except vocal process sutures through remaining arytenoid to thyroid lamina
25 Endoscopic ( Thornell s, Ossoff s technique, Crumley s ELMA) CO 2 LASER excision of arytenoid body and vocal process Used alone or in combination with partial vocal fold resection
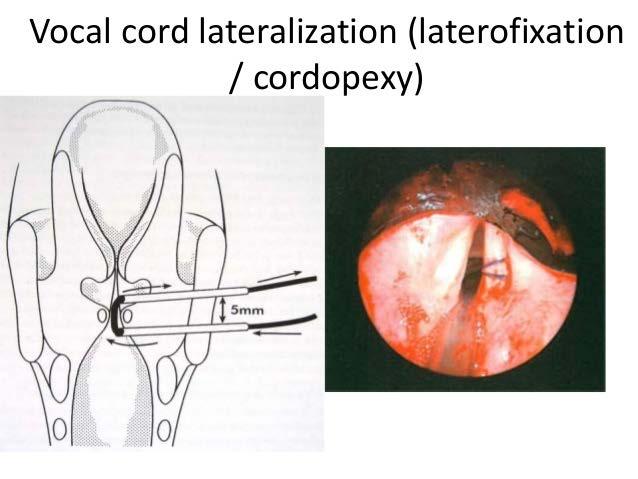
26 ARYTENOIDOPEXY Vocal cord abduction by suture lateralization Combined endoscopic and open approach Reversible used as temporary management when spontaneous recovery is expected DLscopy CA joint assessed TA muscle released Sutures passed around vocal process and posterior third of vocal fold fixed to thyroid ala / strap muscles Greater glottal opening, better phonatory closure, low risk of aspiration
27
28 LARYNGEAL PACING Functional electrical stimulation (FES) of paralysed muscle Potential therapy If spontaneous recovery does not occur within a year Electrical pacing is delivered to Posterior cricoarytenoid muscle with EMG feedback signals from ipsilateral cricothyroid muscle through needle electrodes Trigger signals are produced as a product of feedback from Diaphragmatic EMG/ Intercostal EMG / temperature difference in respiratory cycle
 Device has to be replaced every")
29 Greater ventilatory improvement than any other approach, no voice compromise Still experimental Very expensive (not available in India) Device has to be replaced every 5-10 years
30 REINNERVATION Prerequisites CA joint not fixed Nerve for graft functioning EMG should reveal functioning muscle 2 types 1. Nerve muscle transfer ( Ansa cervicalis Anterior belly of omohyoid) 2. Nerve pedicle transfer ( Ansa cervicalis/ Phrenic nerve RLN anastamosis)
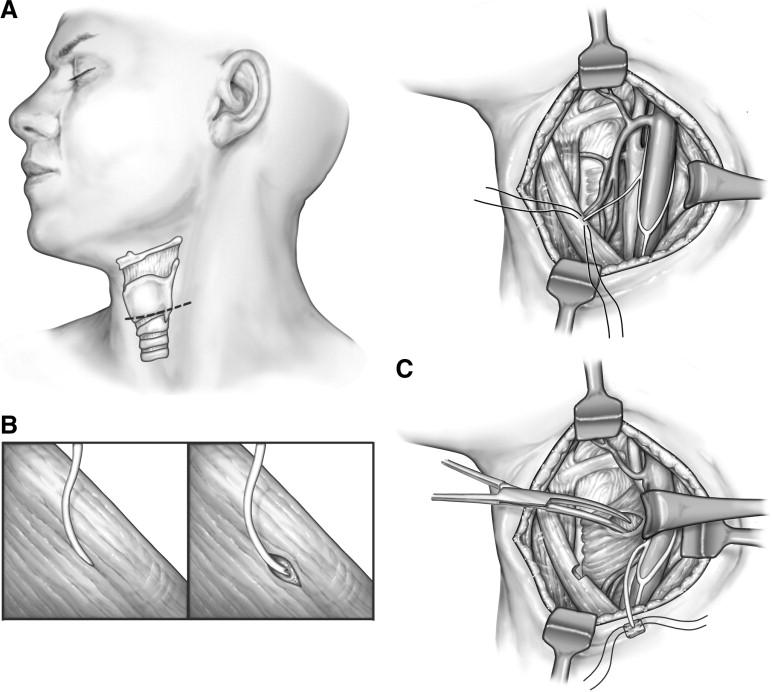
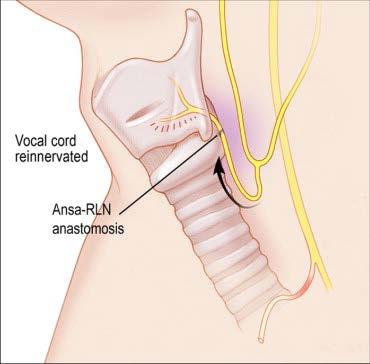
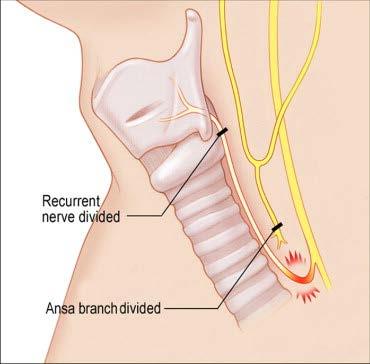
31


32 TYPE II THYROPLASTY II a lateral approach II b medial/midline approach Complication breathy voice voice
33 POSTERIOR CRICOID SPLIT Posterior cricoid split + costal cartilage graft 2 approaches - Endoscopic - Partial laryngofissure (external)
34 BOTULINUM TOXIN Neurotoxin produced by Clostridium botulinum There are 7 types ( A G), type A and B most frequently used clinically Prevents release of acetylecholine from nerve terminals flaccid paralysis Botox injection into bilateral adductor muscles found to improve ventilation Results found acceptable but temporary ( 3 months) therefore requires multiple injections
35 GENE THERAPY Genes encoding neurotrophic growth factors injected into damaged RLN and PCA muscle Stimulates cellular proliferation and differentiation Absorbed by the muscle cells / neurons by retrograde axonal transport transduced into nucleus produce peptides Animal studies using IGF 1 gene ( PCA muscle), GDNF ( RLN) have shown improvement Major drawback is it does not prevent synkinesis Only animal studies performed so far
36 STEM CELL THERAPY Autologous muscle derived stem cells isolated, cultured to critical mass and re-implanted into PCA This attenuated overall muscle atrophy Drawback cannot prevent synkinesis No human trials so far
37 CONCLUSION Bilateral abductor vocal cord palsy can range from exertional stridor to potentially fatal condition Therefore requires prompt and accurate diagnosis followed by adequate treatment Iatrogenic causes which are the leading need to be avoided Almost all the treatment modalities may produce a poorer voice quality as increasing the airway will always create a phonatory gap
38 THANK YOU
Vocal Cord Paresis:Background and Case Reports The Greater Baltimore Medical Center, The Johns Hopkins Voice Center at GBMC Stroboscopy Grand Rounds
 Presented by: David F Smith, MD, PhD March 2, 2012 Vocal Cord Paresis:Background and Case Reports The Greater Baltimore Medical Center, The Johns Hopkins Voice Center at GBMC Stroboscopy Grand Rounds 1
Presented by: David F Smith, MD, PhD March 2, 2012 Vocal Cord Paresis:Background and Case Reports The Greater Baltimore Medical Center, The Johns Hopkins Voice Center at GBMC Stroboscopy Grand Rounds 1
VOCAL CORD PALSY. Department of ENT, Head and Neck Surgery DR OSEGHALE DR AKPALABA
 VOCAL CORD PALSY Department of ENT, Head and Neck Surgery DR OSEGHALE DR AKPALABA Case Presentation M /70 years Pensioner Christain Bini Resides in Benin Had total thyroidectomy. Follicular Ca of thyroid
VOCAL CORD PALSY Department of ENT, Head and Neck Surgery DR OSEGHALE DR AKPALABA Case Presentation M /70 years Pensioner Christain Bini Resides in Benin Had total thyroidectomy. Follicular Ca of thyroid
Vocal Cord Medialization Medialization Laryngoplasty
 Vocal Cord Medialization Medialization Laryngoplasty Carolyn Waddington RN MSN FNP CORLN The Methodist Hospital Houston, TX SOHN, Boston, 2010 Objectives Describe the history of the first treatments for
Vocal Cord Medialization Medialization Laryngoplasty Carolyn Waddington RN MSN FNP CORLN The Methodist Hospital Houston, TX SOHN, Boston, 2010 Objectives Describe the history of the first treatments for
Superior Laryngeal Nerve Injury: Diagnosis and Management. Presented by: Nyall London October 10, 2014
 Superior Laryngeal Nerve Injury: Diagnosis and Management Presented by: Nyall London October 10, 2014 1 Case Presentation 49 year old male s/p right side approach anterior cervical discectomy and fusion
Superior Laryngeal Nerve Injury: Diagnosis and Management Presented by: Nyall London October 10, 2014 1 Case Presentation 49 year old male s/p right side approach anterior cervical discectomy and fusion
Carcinoma of the larynx L 4. Carcinoma of the larynx is the most common head & neck cancer, this has a high cure rate which may reach 90%.
 L 4 Carcinoma of the larynx Carcinoma of the larynx is the most common head & neck cancer, this has a high cure rate which may reach 90%. Incidence: It is more common in males than females in ratio 5:1.
L 4 Carcinoma of the larynx Carcinoma of the larynx is the most common head & neck cancer, this has a high cure rate which may reach 90%. Incidence: It is more common in males than females in ratio 5:1.
Hoarseness. Common referral Hoarseness reflects any abnormality of normal phonation
 Hoarseness Kevin Katzenmeyer, MD Faculty Advisor: Byron J Bailey, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation October 24, 2001 Hoarseness Common referral
Hoarseness Kevin Katzenmeyer, MD Faculty Advisor: Byron J Bailey, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation October 24, 2001 Hoarseness Common referral
Vocal Fold Motion Impairment. Surgical options 10/17/2008. Voice Changes after Treatment for Bilateral Vocal Fold Motion Impairment
 Voice Changes after Treatment for Bilateral Vocal Fold Motion Impairment Betty S. Tsai, MD Mark S. Courey, MD Sarah L. Schneider, MS, CCC-SLP Soha Al-Jurf, MS, CCC-SLP UCSF Department of Otolaryngology
Voice Changes after Treatment for Bilateral Vocal Fold Motion Impairment Betty S. Tsai, MD Mark S. Courey, MD Sarah L. Schneider, MS, CCC-SLP Soha Al-Jurf, MS, CCC-SLP UCSF Department of Otolaryngology
Anatomy of the Airway
 Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
Anatomy of the Airway Nagelhout, 5 th edition, Chapter 26 Morgan & Mikhail, 5 th edition, Chapter 23 Mary Karlet, CRNA, PhD Airway Anatomy The airway consists of the nose, pharynx, larynx, trachea, and
The Immobile Vocal Fold: Paralysis vs. Fixation
 The Immobile Vocal Fold: Paralysis vs. Fixation DISCLOSURE Ted Mau, MD PhD Director UT Southwestern Voice Center I have nothing to disclose www.utsouthwestern.org/voice DALLAS, TEXAS OUTLINE Terminology
The Immobile Vocal Fold: Paralysis vs. Fixation DISCLOSURE Ted Mau, MD PhD Director UT Southwestern Voice Center I have nothing to disclose www.utsouthwestern.org/voice DALLAS, TEXAS OUTLINE Terminology
A Ten-Year Kuala Lumpur Review on Laser Posterior Cordectomy for Bilateral Vocal Fold Immobility
 Original Article Submitted: 3 Aug 2015 Accepted: 6 Mar 2016 A Ten-Year Kuala Lumpur Review on Laser Posterior Cordectomy for Bilateral Vocal Fold Immobility Azman MAWADDAH 1, Mat Baki MARINA 1, Sawali
Original Article Submitted: 3 Aug 2015 Accepted: 6 Mar 2016 A Ten-Year Kuala Lumpur Review on Laser Posterior Cordectomy for Bilateral Vocal Fold Immobility Azman MAWADDAH 1, Mat Baki MARINA 1, Sawali
A Ten-Year Kuala Lumpur Review on Laser Posterior Cordectomy for Bilateral Vocal Fold Immobility
 Original Original Article Submitted: 3 Aug 2015 Accepted: 6 Mar 2016 Online: 30 June 2016 A Ten-Year Kuala Lumpur Review on Laser Posterior Cordectomy for Bilateral Vocal Fold Immobility Azman Mawaddah
Original Original Article Submitted: 3 Aug 2015 Accepted: 6 Mar 2016 Online: 30 June 2016 A Ten-Year Kuala Lumpur Review on Laser Posterior Cordectomy for Bilateral Vocal Fold Immobility Azman Mawaddah
CHAPTER 7 Procedures on Respiratory System
 CHAPTER 7 Propunere noua clasificare proceduri folosind codificarea ICD-10-AM versiunea 3, 30 martie 2004 Procedures on Respiratory System BLOCK 520 Examination procedures on larynx 41764-03 Fibreoptic
CHAPTER 7 Propunere noua clasificare proceduri folosind codificarea ICD-10-AM versiunea 3, 30 martie 2004 Procedures on Respiratory System BLOCK 520 Examination procedures on larynx 41764-03 Fibreoptic
Pourquoi je fais moins d EMG laryngées. Philippe H. Dejonckere
 Pourquoi je fais moins d EMG laryngées Philippe H. Dejonckere EMG Technique électrophysiologique qui renseigne sur l activité électrique musculaire (tonus & mouvement) Phonation = mouvement Indication
Pourquoi je fais moins d EMG laryngées Philippe H. Dejonckere EMG Technique électrophysiologique qui renseigne sur l activité électrique musculaire (tonus & mouvement) Phonation = mouvement Indication
Aetiology. Poor tube management. Small cricoid (acquired on congenital) Reflux Poor general status. Size of tube (leak) Duration of intubation
 Reflux Poor general status. Size of tube (leak) Duration of intubation") Aetiology Poor tube management Size of tube (leak) Duration of intubation Small cricoid (acquired on congenital) Reflux Poor general status Prevention Laryngeal Rest Medical Tubes Cricoid split Developing
Aetiology Poor tube management Size of tube (leak) Duration of intubation Small cricoid (acquired on congenital) Reflux Poor general status Prevention Laryngeal Rest Medical Tubes Cricoid split Developing
Disclosures. Primary Methods for Treating UVP. Key Factors Influencing Treatment Planning. Guiding principle with Treatment Planning 2/4/2018
 Zen and art of vocal mechanics: Key Factors That Influence Unilateral Vocal Fold Paralysis (UVP) Treatment Decisions Julie Barkmeier Kraemer, Ph.D. Professor, Division of Otolaryngology Clinic Director,
Zen and art of vocal mechanics: Key Factors That Influence Unilateral Vocal Fold Paralysis (UVP) Treatment Decisions Julie Barkmeier Kraemer, Ph.D. Professor, Division of Otolaryngology Clinic Director,
Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation
 Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation G. Kurland, MD Children s Hospital of Pittsburgh Geoffrey.kurland@chp.edu 11/2014 Objectives Discuss
Laryngotracheal/Pulmonary Problems and the Mechanically Ventilated Patient: Pediatric Lung Transplantation G. Kurland, MD Children s Hospital of Pittsburgh Geoffrey.kurland@chp.edu 11/2014 Objectives Discuss
Sunshine Act Disclosure
 A Laryngologist s Approach to Voice Presentation at the Nebraska Speech- Language-Hearing Association Fall Convention Thursday, September 27, 2018 15:45-16:45 Christopher M. Bingcang, MD Assistant Professor
A Laryngologist s Approach to Voice Presentation at the Nebraska Speech- Language-Hearing Association Fall Convention Thursday, September 27, 2018 15:45-16:45 Christopher M. Bingcang, MD Assistant Professor
MSA. Sleep disorders MULTIPLE SYSTEM ATROPHY AND NOCTURNAL STRIDOR 1/26/2015. Alex Iranzo Neurology Service Hospital Clinic de Barcelona Spain
 MULTIPLE SYSTEM ATROPHY AND NOCTURNAL STRIDOR Alex Iranzo Neurology Service Hospital Clinic de Barcelona Spain MSA Neurodegenerative disease Parkinsonism, cerebellar, dysautonomia Mean survival is less
MULTIPLE SYSTEM ATROPHY AND NOCTURNAL STRIDOR Alex Iranzo Neurology Service Hospital Clinic de Barcelona Spain MSA Neurodegenerative disease Parkinsonism, cerebellar, dysautonomia Mean survival is less
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September ISSN
 International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 1196 Pneumomediastinum and subcutaneous emphysema secondary to blunt laryngeal traumafavourable outcome with
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 1196 Pneumomediastinum and subcutaneous emphysema secondary to blunt laryngeal traumafavourable outcome with
Contents. Part A Clinical Evaluation of Laryngeal Disorders. 3 Videostroboscopy and Dynamic Voice Evaluation with Flexible Laryngoscopy...
 Contents Part A Clinical Evaluation of Laryngeal Disorders 1 Anatomy and Physiology of the Larynx....... 3 1.1 Anatomy.................................. 3 1.1.1 Laryngeal Cartilages........................
Contents Part A Clinical Evaluation of Laryngeal Disorders 1 Anatomy and Physiology of the Larynx....... 3 1.1 Anatomy.................................. 3 1.1.1 Laryngeal Cartilages........................
Case Presentation JC: 65 y/o retired plumber CC: Hoarseness HPI: Admitted to a local hospital on May 30 for severe pneumonia. Intubated in ICU for 10
 GBMC Stroboscopy Rounds October 12, 2007 Case Presentation JC: 65 y/o retired plumber CC: Hoarseness HPI: Admitted to a local hospital on May 30 for severe pneumonia. Intubated in ICU for 10 days, total
GBMC Stroboscopy Rounds October 12, 2007 Case Presentation JC: 65 y/o retired plumber CC: Hoarseness HPI: Admitted to a local hospital on May 30 for severe pneumonia. Intubated in ICU for 10 days, total
Complex Airway problems - Paediatric Perspective
 Complex Airway problems - Paediatric Perspective Dave Albert BACO Liverpool 2009 www.albert.uk.com Complex Ξ not simple, multiple parts Multiple problems with airway Combined Web/stenosis/multiple levels
Complex Airway problems - Paediatric Perspective Dave Albert BACO Liverpool 2009 www.albert.uk.com Complex Ξ not simple, multiple parts Multiple problems with airway Combined Web/stenosis/multiple levels
Chapter 112: Phonosurgical Procedures. Paul W. Flint, Charles W. Cummings
 Chapter 112: Phonosurgical Procedures Paul W. Flint, Charles W. Cummings While still in its infancy, laryngeal phonosurgery has grown to encompass a variety of procedures designed to effect alterations
Chapter 112: Phonosurgical Procedures Paul W. Flint, Charles W. Cummings While still in its infancy, laryngeal phonosurgery has grown to encompass a variety of procedures designed to effect alterations
Botulinum Therapy in the Laryngopharynx October 2004
 TITLE: Botulinum Therapy in the Laryngopharynx SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: October 27, 2004 RESIDENT PHYSICIAN: Sam J. Cunningham, MD, PhD FACULTY ADVISOR: David
TITLE: Botulinum Therapy in the Laryngopharynx SOURCE: Grand Rounds Presentation, UTMB, Dept. of Otolaryngology DATE: October 27, 2004 RESIDENT PHYSICIAN: Sam J. Cunningham, MD, PhD FACULTY ADVISOR: David
Supplementary Online Content
 Supplementary Online Content Wang C-C, Chang M-H, Jiang R-S, et al. Laryngeal electromyography-guided hyaluronic acid vocal fold injection for unilateral vocal fold paralysis: a prospective long-term follow-up
Supplementary Online Content Wang C-C, Chang M-H, Jiang R-S, et al. Laryngeal electromyography-guided hyaluronic acid vocal fold injection for unilateral vocal fold paralysis: a prospective long-term follow-up
Specialist Referral Service Willows Information Sheets. Laryngeal paralysis
 Specialist Referral Service Willows Information Sheets Laryngeal paralysis Laryngeal paralysis tends to affect middle aged and older animals, especially large breed dogs such as Labrador Retrievers, Golden
Specialist Referral Service Willows Information Sheets Laryngeal paralysis Laryngeal paralysis tends to affect middle aged and older animals, especially large breed dogs such as Labrador Retrievers, Golden
Electrophysiological studies. Dr Carmen Górriz Gil Otorhinolaryngologist Voice Unit
 Electrophysiological studies Dr Carmen Górriz Gil Otorhinolaryngologist Voice Unit Who does LEMG? ENT + Neurophysiologist, neurologist Dr Martínez Dr Álvarez Dr Gª Berrocal Dr Vicente EMG Technique Sitting
Electrophysiological studies Dr Carmen Górriz Gil Otorhinolaryngologist Voice Unit Who does LEMG? ENT + Neurophysiologist, neurologist Dr Martínez Dr Álvarez Dr Gª Berrocal Dr Vicente EMG Technique Sitting
Neonatal Airway Disorders, Treatments, and Outcomes. Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center
 Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
Neonatal Airway Disorders, Treatments, and Outcomes Steven Goudy, MD Pediatric Otolaryngology Emory University Medical Center Disclosure I have nothing to disclose Neonatal and Pediatric Tracheostomy Tracheostomy
External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other
 Internal trauma (Endotracheal intubation, tracheostomy) Other") Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Etiology External trauma (MVA, surf board, assault, etc.) Internal trauma (Endotracheal intubation, tracheostomy) Other Systemic diseases (vasculitis, etc.) Chemo/XRT Idiopathic Trans nasal Esophagoscope
Larynx. Rudimentary. Behind the posterior surface : -stylopharyngeus - salpingopharyngeus -platopharyngeus
 Larynx The larynx is an organ that provides a protective sphincter at the inlet of the air passages and is responsible for voice production. It extends from C3-C6: *Posterior: the pharynx *Lateral: the
Larynx The larynx is an organ that provides a protective sphincter at the inlet of the air passages and is responsible for voice production. It extends from C3-C6: *Posterior: the pharynx *Lateral: the
Treatment of Adductor Spasmodic Dysphonia with Selective Laryngeal Adductor Denervation and Reinnervation Surgery
 Otolaryngol Clin N Am 39 (2006) 101 109 Treatment of Adductor Spasmodic Dysphonia with Selective Laryngeal Adductor Denervation and Reinnervation Surgery Dinesh K. Chhetri, MD*, Gerald S. Berke, MD Division
Otolaryngol Clin N Am 39 (2006) 101 109 Treatment of Adductor Spasmodic Dysphonia with Selective Laryngeal Adductor Denervation and Reinnervation Surgery Dinesh K. Chhetri, MD*, Gerald S. Berke, MD Division
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Complications with laryngoplasty
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Complications with laryngoplasty Author : Robin Fearon Categories : Vets Date : December 5, 2011 Safia Barakzai discusses
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Complications with laryngoplasty Author : Robin Fearon Categories : Vets Date : December 5, 2011 Safia Barakzai discusses
Laryngeal electromyography findings of vocal fold immobility in patients after radiotherapy for nasopharyngeal carcinoma
 ORIGINAL ARTICLE Laryngeal electromyography findings of vocal fold immobility in patients after radiotherapy for nasopharyngeal carcinoma Yi-Ling Hsieh, MD, 1 Ming-Hong Chang, MD, 2 Chen-Chi Wang, MD 1,3,4*
ORIGINAL ARTICLE Laryngeal electromyography findings of vocal fold immobility in patients after radiotherapy for nasopharyngeal carcinoma Yi-Ling Hsieh, MD, 1 Ming-Hong Chang, MD, 2 Chen-Chi Wang, MD 1,3,4*
Treatment of Bilateral Vocal Fold Immobility
 Curr Otorhinolaryngol Rep (2014) 2:114 118 DOI 10.1007/s40136-014-0042-0 MANAGEMENT OF VOCAL CORD IMMOBILITY (J BLUMIN, SECTION EDITOR) Treatment of Bilateral Vocal Fold Immobility Joseph P. Bradley Adam
Curr Otorhinolaryngol Rep (2014) 2:114 118 DOI 10.1007/s40136-014-0042-0 MANAGEMENT OF VOCAL CORD IMMOBILITY (J BLUMIN, SECTION EDITOR) Treatment of Bilateral Vocal Fold Immobility Joseph P. Bradley Adam
Bilateral vocal fold immobility: a 13 year review of etiologies, management and the utility of the empey index
 Brake and Anderson Journal of Otolaryngology - Head and Neck Surgery (2015) 44:27 DOI 10.1186/s40463-015-0080-8 ORIGINAL RESEARCH ARTICLE Open Access Bilateral vocal fold immobility: a 13 year review of
Brake and Anderson Journal of Otolaryngology - Head and Neck Surgery (2015) 44:27 DOI 10.1186/s40463-015-0080-8 ORIGINAL RESEARCH ARTICLE Open Access Bilateral vocal fold immobility: a 13 year review of
Larynx - cartilaginous structure holding the vocal folds which protrude into airstream
 1! Larynx - cartilaginous structure holding the vocal folds which protrude into airstream 2! Flow increase - like thumb over garden hose Pressure drop - narrower space forces pressure drop due to speed
1! Larynx - cartilaginous structure holding the vocal folds which protrude into airstream 2! Flow increase - like thumb over garden hose Pressure drop - narrower space forces pressure drop due to speed
Alexander C Vlantis. Total Laryngectomy 57
 07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
Respiratory System. Clinical notes. Published on Second Faculty of Medicine, Charles University ( https://www.lf2.cuni.cz)
") Published on Second Faculty of Medicine, Charles University ( https://www.lf2.cuni.cz) Respiratory System The test of the respiratory system follows the general rules for written tests (see Continuous
Published on Second Faculty of Medicine, Charles University ( https://www.lf2.cuni.cz) Respiratory System The test of the respiratory system follows the general rules for written tests (see Continuous
POST-OPERATIVE LARYNGEAL COMPLICATIONS AFTER ENDOCRINE SURGERY
 POST-OPERATIVE LARYNGEAL COMPLICATIONS AFTER ENDOCRINE SURGERY Amy L. Rutt, D.O. Mayo Clinic Jacksonville, FL AOCOO-HNS Foundation 2015 MFMER slide-1 Etiology 1985-1995 (n=280) 1995-2005 (n=363) Overall
POST-OPERATIVE LARYNGEAL COMPLICATIONS AFTER ENDOCRINE SURGERY Amy L. Rutt, D.O. Mayo Clinic Jacksonville, FL AOCOO-HNS Foundation 2015 MFMER slide-1 Etiology 1985-1995 (n=280) 1995-2005 (n=363) Overall
Organ preservation in laryngeal cancer
 Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
Organ preservation in laryngeal cancer Wojciech Golusiński Department of Head and Neck Surgery The Great Poland Cancer Centre, Poznan, Poland Poznan University of Medical Sciences, Poznan, Poland Silver
Normal Voice. Evaluation of a Patient with Hoarseness. No disclosures. Hoarseness. Assessment. Assessment
 Evaluation of a Patient with Hoarseness No disclosures Mari Hagiwara, MD NYU Langone Medical Center ASHNR 2017 Hoarseness Symptom: any deviation from normal voice quality as perceived by self or others;
Evaluation of a Patient with Hoarseness No disclosures Mari Hagiwara, MD NYU Langone Medical Center ASHNR 2017 Hoarseness Symptom: any deviation from normal voice quality as perceived by self or others;
Evaluating the timing of injection laryngoplasty for vocal fold paralysis in an attempt to avoid future type 1 thyroplasty
 Alghonaim et al. Journal of Otolaryngology - Head and Neck Surgery 2013, 42:24 ORIGINAL RESEARCH ARTICLE Open Access Evaluating the timing of injection laryngoplasty for vocal fold paralysis in an attempt
Alghonaim et al. Journal of Otolaryngology - Head and Neck Surgery 2013, 42:24 ORIGINAL RESEARCH ARTICLE Open Access Evaluating the timing of injection laryngoplasty for vocal fold paralysis in an attempt
Prior Authorization Review Panel MCO Policy Submission
 Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Basic Science Review Wound Healing
 Subglottic Stenosis Deborah P. Wilson, M.D. Faculty Advisor: Norman Friedman, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation April 14, 1999 Basic Science
Subglottic Stenosis Deborah P. Wilson, M.D. Faculty Advisor: Norman Friedman, M.D. The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation April 14, 1999 Basic Science
International Journal of Medical Science and Education pissn eissn
 Original research article International Journal of Medical Science and Education pissn- 2348 4438 eissn-2349-3208 INCIDENCE AND ETIO-PATHOGENESIS OF VOCAL CORD PARALYSIS IN A TERTIARY CARE HOSPITAL Natwar
Original research article International Journal of Medical Science and Education pissn- 2348 4438 eissn-2349-3208 INCIDENCE AND ETIO-PATHOGENESIS OF VOCAL CORD PARALYSIS IN A TERTIARY CARE HOSPITAL Natwar
Pathophysiology and Surgical Treatment of Unilateral Vocal Fold Paralysis
 Pathophysiology and Surgical Treatment of Unilateral Vocal Fold Paralysis Denervation and Reinnervation Eiji Yumoto 123 Pathophysiology and Surgical Treatment of Unilateral Vocal Fold Paralysis Eiji Yumoto
Pathophysiology and Surgical Treatment of Unilateral Vocal Fold Paralysis Denervation and Reinnervation Eiji Yumoto 123 Pathophysiology and Surgical Treatment of Unilateral Vocal Fold Paralysis Eiji Yumoto
The Larynx. Prof. Dr.Mohammed Hisham Al-Muhtaseb
 The Larynx Prof. Dr.Mohammed Hisham Al-Muhtaseb The Larynx Extends from the middle of C3 vertebra till the level of the lower border of C6 Continue as Trachea Above it opens into the laryngo-pharynx Suspended
The Larynx Prof. Dr.Mohammed Hisham Al-Muhtaseb The Larynx Extends from the middle of C3 vertebra till the level of the lower border of C6 Continue as Trachea Above it opens into the laryngo-pharynx Suspended
Difficulties with: vision, hemosthasia, suture and flaps transposition
 Universidade Federal de São Paulo UNIFESP-EPM EPM New surgical technique for the larynx Transventricular Chondroplastic Laryngotomy - TCL Marcos Sarvat, Nédio Steffen, Henrique Olival-Costa, and Paulo
Universidade Federal de São Paulo UNIFESP-EPM EPM New surgical technique for the larynx Transventricular Chondroplastic Laryngotomy - TCL Marcos Sarvat, Nédio Steffen, Henrique Olival-Costa, and Paulo
Structure and Nerve Supply of The Larynx
 Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical sciences Structure and Nerve Supply of The Larynx This presentation was originally prepared by: Dr. Kumar Notes were added by:
Kingdom of Bahrain Arabian Gulf University College of Medicine and Medical sciences Structure and Nerve Supply of The Larynx This presentation was originally prepared by: Dr. Kumar Notes were added by:
Case Presentation Topic: Difficult to Ventilate Difficult to Intubate
 Case Presentation Topic: Difficult to Ventilate Difficult to Intubate Dr. K. Shruthi Jeevan 1 st Year Post Graduate Department of Anaesthesiology CASE SCENARIO : 1 A 65 years old female patient, resident
Case Presentation Topic: Difficult to Ventilate Difficult to Intubate Dr. K. Shruthi Jeevan 1 st Year Post Graduate Department of Anaesthesiology CASE SCENARIO : 1 A 65 years old female patient, resident
Adenoid Cystic Carcinoma Minor Salivary Gland Origin
 Adenoid Cystic Carcinoma Minor Salivary Gland Origin Educational Session Presenter: Smith JA Supervisors: Palme CE, Gupta R Content Case report Imaging Primary Therapy Surgery Adjuvant Therapy Radiotherapy
Adenoid Cystic Carcinoma Minor Salivary Gland Origin Educational Session Presenter: Smith JA Supervisors: Palme CE, Gupta R Content Case report Imaging Primary Therapy Surgery Adjuvant Therapy Radiotherapy
TRACHEOSTOMY. Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion
 TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
TRACHEOSTOMY Definition Tracheostomy means creation an artificial opening in the trachea with tracheostomy tube insertion Indications for tracheostomy 1-upper airway obstruction with stridor, air hunger,
Hoarseness. Evidence-based Key points for Approach
 Hoarseness Evidence-based Key points for Approach Sasan Dabiri, Assistant Professor Department of otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medial Sciences Definition:
Hoarseness Evidence-based Key points for Approach Sasan Dabiri, Assistant Professor Department of otorhinolaryngology Head & Neck Surgery Amir A lam hospital Tehran University of Medial Sciences Definition:
Innervation of the cricothyroid muscle by the recurrent laryngeal nerve
 ORIGINAL ARTICLE Innervation of the cricothyroid muscle by the recurrent laryngeal nerve Hiroo Masuoka, MD, PhD,* Akira Miyauchi, MD, PhD, Tomonori Yabuta, MD, PhD, Mitsuhiro Fukushima, MD, PhD, Akihiro
ORIGINAL ARTICLE Innervation of the cricothyroid muscle by the recurrent laryngeal nerve Hiroo Masuoka, MD, PhD,* Akira Miyauchi, MD, PhD, Tomonori Yabuta, MD, PhD, Mitsuhiro Fukushima, MD, PhD, Akihiro
Recurrent Laryngeal Nerve Recovery Patterns Assessed by Serial Electromyography
 The Laryngoscope VC 2015 The American Laryngological, Rhinological and Otological Society, Inc. Recurrent Laryngeal Nerve Recovery Patterns Assessed by Serial Electromyography Randal C. Paniello, MD, PhD;
The Laryngoscope VC 2015 The American Laryngological, Rhinological and Otological Society, Inc. Recurrent Laryngeal Nerve Recovery Patterns Assessed by Serial Electromyography Randal C. Paniello, MD, PhD;
Endoscopic carbon dioxide laser cricopharyngeal myotomy for relief of oropharyngeal dysphagia
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Endoscopic carbon dioxide laser cricopharyngeal myotomy for relief of oropharyngeal dysphagia Difficulty
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Endoscopic carbon dioxide laser cricopharyngeal myotomy for relief of oropharyngeal dysphagia Difficulty
Dysarthria and Dysphagia: a Neurology Perspective William Meador, MD Assistant Professor of Neurology, UAB
 Dysarthria and Dysphagia: a Neurology Perspective William Meador, MD Assistant Professor of Neurology, UAB 2.11.16 Disclosures I have no relevant conflicts or potential conflicts to disclose regarding
Dysarthria and Dysphagia: a Neurology Perspective William Meador, MD Assistant Professor of Neurology, UAB 2.11.16 Disclosures I have no relevant conflicts or potential conflicts to disclose regarding
The Role of the Speech Language Pathologist & Spinal Cord Injury
 The Role of the Speech Language Pathologist & Spinal Cord Injury Facts According to the National Spinal Cord Injury Statistical Center (NSCISC) there are approxiamtely 12,000 new spinal cord injuries (SCI)
The Role of the Speech Language Pathologist & Spinal Cord Injury Facts According to the National Spinal Cord Injury Statistical Center (NSCISC) there are approxiamtely 12,000 new spinal cord injuries (SCI)
ISPUB.COM. Medialization Thyroplasty Using Silatic Implant. S Singh Yadav, J Singh Gulia, K Singh, S Singh INTRODUCTION MATERIAL AND METHODS
 ISPUB.COM The Internet Journal of Head and Neck Surgery Volume 1 Number 1 Medialization Thyroplasty Using Silatic Implant S Singh Yadav, J Singh Gulia, K Singh, S Singh Citation S Singh Yadav, J Singh
ISPUB.COM The Internet Journal of Head and Neck Surgery Volume 1 Number 1 Medialization Thyroplasty Using Silatic Implant S Singh Yadav, J Singh Gulia, K Singh, S Singh Citation S Singh Yadav, J Singh
Laser Cordectomy. Glottic Carcinoma
 Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Laser Cordectomy in Glottic Carcinoma Department of Otolaryngology gy Head & Neck Surgery Alexandria University Historical Review Endolaryngeal extirpation of vocal cord cancers is a controversial o issue
Evaluation of the Hoarse Patient
 Evaluation of the Hoarse Patient Herve J. LeBoeuf, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation May 17, 2000 Anatomy- Vagus N. ambiguus: Motor - skeletal
Evaluation of the Hoarse Patient Herve J. LeBoeuf, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation May 17, 2000 Anatomy- Vagus N. ambiguus: Motor - skeletal
Management of Hoarseness in Primary Care
 Management of Hoarseness in Primary Care Dr Jeeve Kanagalingam MA (Cantab), BM BCh (Oxon), DLO, DOHNS, FRCS Eng (ORL-HNS), FAMS (ORL) Consultant Department of Otorhinolaryngology TTSH Apr 1, 2010 Straits
Management of Hoarseness in Primary Care Dr Jeeve Kanagalingam MA (Cantab), BM BCh (Oxon), DLO, DOHNS, FRCS Eng (ORL-HNS), FAMS (ORL) Consultant Department of Otorhinolaryngology TTSH Apr 1, 2010 Straits
LA DISFONIA SPASMODICA: LA DIAGNOSI E LE TECNICHE DI TRATTAMENTO CON TOSSINA BOTULINICA Enrico Alfonsi Dipartimento di Neurofisiopatologia Istituto
 LA DISFONIA SPASMODICA: LA DIAGNOSI E LE TECNICHE DI TRATTAMENTO CON TOSSINA BOTULINICA Enrico Alfonsi Dipartimento di Neurofisiopatologia Istituto Neurologico Nazionale Casimiro Mondino Pavia (Italy)
LA DISFONIA SPASMODICA: LA DIAGNOSI E LE TECNICHE DI TRATTAMENTO CON TOSSINA BOTULINICA Enrico Alfonsi Dipartimento di Neurofisiopatologia Istituto Neurologico Nazionale Casimiro Mondino Pavia (Italy)
Continuing Education Independent Study Series
 Continuing Education Independent Study Series Association of Surgical Technologists Publication made possible by an educational grant provided by Kim berly-clark Corporation OF SURGICAL Association of
Continuing Education Independent Study Series Association of Surgical Technologists Publication made possible by an educational grant provided by Kim berly-clark Corporation OF SURGICAL Association of
Idiopathic laryngotracheal stenosis
 Surgical Technique Idiopathic laryngotracheal stenosis Christina L. Costantino, Douglas J. Mathisen Massachusetts General Hospital, Boston, MA 02114, USA Correspondence to: Douglas J. Mathisen, MD. Massachusetts
Surgical Technique Idiopathic laryngotracheal stenosis Christina L. Costantino, Douglas J. Mathisen Massachusetts General Hospital, Boston, MA 02114, USA Correspondence to: Douglas J. Mathisen, MD. Massachusetts
Faculty of Clinical Forensic Medicine Committee 1/2018
 Guideline Subject: Clinical Forensic Assessment and Management of Non-Fatal Strangulation Approval Date: January 2018 Review Date: January 2021 Review By: Number: Faculty of Clinical Forensic Medicine
Guideline Subject: Clinical Forensic Assessment and Management of Non-Fatal Strangulation Approval Date: January 2018 Review Date: January 2021 Review By: Number: Faculty of Clinical Forensic Medicine
Respiratory System. Ling Shucai
 Respiratory System Ling Shucai General Description Ⅰ. Constituents: Respiratory tract Lungs Pleura and plural cavity Ⅱ. Function: exchange O 2 and CO 2 mainly Mediastinum Respiratory tract Upper respiratory
Respiratory System Ling Shucai General Description Ⅰ. Constituents: Respiratory tract Lungs Pleura and plural cavity Ⅱ. Function: exchange O 2 and CO 2 mainly Mediastinum Respiratory tract Upper respiratory
Please refer back to the slides as these are extra notes only. Slide 2 -The Larynx is a Box of cartilage.
 [ANATOMY #3] 1 بسم رلاهللا Please refer back to the slides as these are extra notes only. Slide 2 -The Larynx is a Box of cartilage. -The lower border of c6 is the lower border of cricoid cartilage. -The
[ANATOMY #3] 1 بسم رلاهللا Please refer back to the slides as these are extra notes only. Slide 2 -The Larynx is a Box of cartilage. -The lower border of c6 is the lower border of cricoid cartilage. -The
Penetrating Neck Injuries. Jason Levine MD Lutheran Medical Center July 22, 2010
 Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Penetrating Neck Injuries Jason Levine MD Lutheran Medical Center July 22, 2010 CASE PRESENTATION 19 YO M 3 Stab Wounds Right zone I neck SW 2 SW anterior abdomen Left epigastrium anterior axillary line
Validation of ultrasound as a diagnostic tool to assess vocal cord motion in an animal feasibility study
 Original Article Validation of ultrasound as a diagnostic tool to assess vocal cord motion in an animal feasibility study Karuna Dewan 1, Merry E. Sebelik 2, John D. Boughter 3, Courtney B. Shires 4 1
Original Article Validation of ultrasound as a diagnostic tool to assess vocal cord motion in an animal feasibility study Karuna Dewan 1, Merry E. Sebelik 2, John D. Boughter 3, Courtney B. Shires 4 1
Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience
 1 Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience John P. Dahl, MD, PhD, MBA 1,2, *, Patricia L. Purcell, MD 1, MPH, Sanjay R. Parikh, MD, FACS 1, and Andrew F.
1 Endoscopic Posterior Cricoid Split with Costal Cartilage Graft: A Fifteen Year Experience John P. Dahl, MD, PhD, MBA 1,2, *, Patricia L. Purcell, MD 1, MPH, Sanjay R. Parikh, MD, FACS 1, and Andrew F.
Surgical Treatment of Benign Subglottic Stenosis. JLKasperbauer MD Mayo Clinic Rochester, MN USA
 Surgical Treatment of Benign Subglottic Stenosis JLKasperbauer MD Mayo Clinic Rochester, MN USA Goals Review Subglottic Stenosis Anatomy, Airway Dynamics, Etiology Idiopathic Subglottic Stenosis Definition,
Surgical Treatment of Benign Subglottic Stenosis JLKasperbauer MD Mayo Clinic Rochester, MN USA Goals Review Subglottic Stenosis Anatomy, Airway Dynamics, Etiology Idiopathic Subglottic Stenosis Definition,
Hemilaryngeal Transplantation in the Canine Model: Technique and Implications
 Hemilaryngeal Transplantation in the Canine Model: Technique and Implications Robert J. Andrews, MD,* Gera]d S. Berke, MD,* Keith E. BIackwe]], MD,* MichaeI Jakobsen, MD, * Marilene B. Wang, MD, * and
Hemilaryngeal Transplantation in the Canine Model: Technique and Implications Robert J. Andrews, MD,* Gera]d S. Berke, MD,* Keith E. BIackwe]], MD,* MichaeI Jakobsen, MD, * Marilene B. Wang, MD, * and
DYSPHAGIA MANAGEMENT IN ACUTE CARE AMANDA HEREFORD, MA, CCC- SLP
 DYSPHAGIA MANAGEMENT IN ACUTE CARE AMANDA HEREFORD, MA, CCC- SLP OVERVIEW Decision making re: swallowing in the medically compromised patient Swallow evaluation vs. Nursing Swallow Screening Instrumental
DYSPHAGIA MANAGEMENT IN ACUTE CARE AMANDA HEREFORD, MA, CCC- SLP OVERVIEW Decision making re: swallowing in the medically compromised patient Swallow evaluation vs. Nursing Swallow Screening Instrumental
Esophageal Perforation
 Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Esophageal Perforation Dr. Carmine Simone Thoracic Surgeon, Division of General Surgery Head, Division of Critical Care May 15, 2006 Overview Case presentation Radiology Pre-operative management Operative
Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital
 AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
AIRWAY MANAGEMENT Angkana Lurngnateetape,, MD. Department of Anesthesiology Siriraj Hospital Perhaps the most important responsibility of the anesthesiologist is management of the patient s airway Miller
Causes of recurrent laryngeal nerve paralysis
 Auris Nasus Larynx 29 (2002) 41 45 www.elsevier.com/locate/anl Causes of recurrent laryngeal nerve paralysis Eiji Yumoto a, *, Ryosei Minoda a, Masamitsu Hyodo b, Takahiko Yamagata b a Department of Otolaryngology-Head
Auris Nasus Larynx 29 (2002) 41 45 www.elsevier.com/locate/anl Causes of recurrent laryngeal nerve paralysis Eiji Yumoto a, *, Ryosei Minoda a, Masamitsu Hyodo b, Takahiko Yamagata b a Department of Otolaryngology-Head
Evaluation of Neck Mass. Disclosure. Learning Objectives 3/24/2014. Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ. Nothing to disclose
 Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
A Comparison of Outcomes in Interventions for Unilateral Vocal Fold Paralysis: A Systematic Review
 The Laryngoscope VC 2015 The American Laryngological, Rhinological and Otological Society, Inc. Systematic Review A Comparison of Outcomes in Interventions for Unilateral Vocal Fold Paralysis: A Systematic
The Laryngoscope VC 2015 The American Laryngological, Rhinological and Otological Society, Inc. Systematic Review A Comparison of Outcomes in Interventions for Unilateral Vocal Fold Paralysis: A Systematic
Treatment for Supraglottic Ca History: : Total Laryngectomy y was routine until early 50 s, when XRT was developed Ogura and Som developed the one-sta
 Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Role of Laser Therapy in Laryngeal Cancer Khalid Hussain AL-Qahtani MD,MSc,FRCS(c) MSc Assistant Professor Consultant of Otolaryngology Advance Head & Neck Oncology, Thyroid & Parathyroid,Microvascular
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Phonosurgery. The poor lymphatic drainage of the lamina propria predisposes it to collect tissue fluid (Reinke's oedema)
") Phonosurgery Phonosurgery is defined as 'any surgery designed primarily for the improvement or restoration of the voice'. Complete assessment of a patient with a voice disorder should now include video
Phonosurgery Phonosurgery is defined as 'any surgery designed primarily for the improvement or restoration of the voice'. Complete assessment of a patient with a voice disorder should now include video
Cricothyroid Muscle Dysfunction Impairs Vocal Fold Vibration in Unilateral Vocal Fold Paralysis
 The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. Cricothyroid Muscle Dysfunction Impairs Vocal Fold Vibration in Unilateral Vocal Fold Paralysis Yu-Cheng
The Laryngoscope VC 2013 The American Laryngological, Rhinological and Otological Society, Inc. Cricothyroid Muscle Dysfunction Impairs Vocal Fold Vibration in Unilateral Vocal Fold Paralysis Yu-Cheng
Airway Emergencies: Pearls for the Anesthesiologist
 Airway Emergencies: Pearls for the Anesthesiologist Pavan S. Mallur, MD, FACS Division of Otolaryngology, Department of Surgery Beth Israel Deaconess Medical Center Department of Otology and Laryngology
Airway Emergencies: Pearls for the Anesthesiologist Pavan S. Mallur, MD, FACS Division of Otolaryngology, Department of Surgery Beth Israel Deaconess Medical Center Department of Otology and Laryngology
Karoline Nowillo, MD. February 1, 2008
 Case Presentation Karoline Nowillo, MD SUNY Downstate t February 1, 2008 Case Presentation Chief complaint enlarging goiter x 8 months History of present illness shortness of breath, heaviness in chest
Case Presentation Karoline Nowillo, MD SUNY Downstate t February 1, 2008 Case Presentation Chief complaint enlarging goiter x 8 months History of present illness shortness of breath, heaviness in chest
Anita Gheller-Rigoni, DO, FACAAI Allergist-Immunologist. Exercise-Induced Vocal Cord Dysfunction
 Anita Gheller-Rigoni, DO, FACAAI Allergist-Immunologist Exercise-Induced Vocal Cord Dysfunction Objectives 1. Understand the concept of vocal cord dysfunction 2. Recognize the difference between exercised
Anita Gheller-Rigoni, DO, FACAAI Allergist-Immunologist Exercise-Induced Vocal Cord Dysfunction Objectives 1. Understand the concept of vocal cord dysfunction 2. Recognize the difference between exercised
1/3/2008. Karen Burke Priscilla LeMone Elaine Mohn-Brown. Medical-Surgical Nursing Care, 2e Karen Burke, Priscilla LeMone, and Elaine Mohn-Brown
 Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 23 Caring for Clients with Upper Respiratory Disorders Rhinitis Inflammation of Nasal Cavities Types
Medical-Surgical Nursing Care Second Edition Karen Burke Priscilla LeMone Elaine Mohn-Brown Chapter 23 Caring for Clients with Upper Respiratory Disorders Rhinitis Inflammation of Nasal Cavities Types
Subject Index. Bacterial infection, see Suppurative lung disease, Tuberculosis
 Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
Subject Index Abscess, virtual 107 Adenoidal hypertrophy, features 123 Airway bleeding, technique 49, 50 Airway stenosis, see Stenosis, airway Anaesthesia biopsy 47 complications 27, 28 flexible 23 26
Biomechanics of Voice
 Biomechanics of Voice Stephen F. Austin, M.M., Ph.D. Chair, Division of Vocal Studies College of Music University of North Texas Goals: To offer medical professionals a review of the function of the vocal
Biomechanics of Voice Stephen F. Austin, M.M., Ph.D. Chair, Division of Vocal Studies College of Music University of North Texas Goals: To offer medical professionals a review of the function of the vocal
COMD #6305 The Phonatory system Chapters 4, 5
 COMD #6305 The Phonatory system Chapters 4, 5 Laryngeal function Theory of phonation Jitter, shimmer Vocal registers Normal vs. abnormal voice qualities Measurements of voice quality Clinical applications
COMD #6305 The Phonatory system Chapters 4, 5 Laryngeal function Theory of phonation Jitter, shimmer Vocal registers Normal vs. abnormal voice qualities Measurements of voice quality Clinical applications
How to use the Control-Cric to perform a surgical cricothyrotomy
 TRAININGGROUNDS How to use the Control-Cric to perform a surgical cricothyrotomy Product Description The Control-Cric is a System which verifies tracheal location during a surgical airway procedure, without
TRAININGGROUNDS How to use the Control-Cric to perform a surgical cricothyrotomy Product Description The Control-Cric is a System which verifies tracheal location during a surgical airway procedure, without
Current Treatment Options for Bilateral Vocal Fold Paralysis: A State-of-the-Art Review
 Review Clinical and Experimental Otorhinolaryngology Vol. 10, No. 3: 203-212, September 2017 https://doi.org/10.21053/ceo.2017.00199 pissn 1976-8710 eissn 2005-0720 Current Treatment Options for Bilateral
Review Clinical and Experimental Otorhinolaryngology Vol. 10, No. 3: 203-212, September 2017 https://doi.org/10.21053/ceo.2017.00199 pissn 1976-8710 eissn 2005-0720 Current Treatment Options for Bilateral
AIRWAY MANAGEMENT AND VENTILATION
 AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
AIRWAY MANAGEMENT AND VENTILATION D1 AIRWAY MANAGEMENT AND VENTILATION Basic airway management and ventilation The laryngeal mask airway and Combitube Advanced techniques of airway management D2 Basic
Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy
 Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy Disclaimer This material is intended for use by trained family members and caregivers of children with tracheostomies who are
Tracheostomy and Ventilator Education Program Module 2: Respiratory Anatomy Disclaimer This material is intended for use by trained family members and caregivers of children with tracheostomies who are
Vocal Fold Paralysis: Improved Adductor Recovery by Vincristine Blockade of Posterior Cricoarytenoid
 The Laryngoscope VC 2014 The American Laryngological, Rhinological and Otological Society, Inc. Vocal Fold Paralysis: Improved Adductor Recovery by Vincristine Blockade of Posterior Cricoarytenoid Randal
The Laryngoscope VC 2014 The American Laryngological, Rhinological and Otological Society, Inc. Vocal Fold Paralysis: Improved Adductor Recovery by Vincristine Blockade of Posterior Cricoarytenoid Randal
Lisa T. Fry, PhD Marshall University. Joseph C. Stemple, PhD University of Kentucky
 Lisa T. Fry, PhD Marshall University Joseph C. Stemple, PhD University of Kentucky Muscular Components of Voice Disorders Resonance Requires balance among the 3 Phonation Disruption in 1 may perturb the
Lisa T. Fry, PhD Marshall University Joseph C. Stemple, PhD University of Kentucky Muscular Components of Voice Disorders Resonance Requires balance among the 3 Phonation Disruption in 1 may perturb the
Diffusion of aniline blue injected into the thyroarytenoid muscle as a proxy for botulinum toxin injection: an experimental study in cadaver larynges
 Original Article Int. Arch. Otorhinolaryngol. 2013;17(3):315-320. DOI: 10.7162/S1809-977720130003000012 Diffusion of aniline blue injected into the thyroarytenoid muscle as a proxy for botulinum toxin
Original Article Int. Arch. Otorhinolaryngol. 2013;17(3):315-320. DOI: 10.7162/S1809-977720130003000012 Diffusion of aniline blue injected into the thyroarytenoid muscle as a proxy for botulinum toxin
If you suspect airway problems, get a second opinion before you anaesthetise, not after!
 Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Assessing the airway It is more important to be aware of the various methods of dealing with difficult laryngoscopy than to expect to be able to accurately identify the rare difficult patients without
Rehabilitation of the Paralyzed Face
 Rehabilitation of the Paralyzed Face Elizabeth J. Rosen, MD Faculty Advisor: Karen H. Calhoun, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation October 30,
Rehabilitation of the Paralyzed Face Elizabeth J. Rosen, MD Faculty Advisor: Karen H. Calhoun, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation October 30,