FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
|
|
|
- Oswald Preston
- 6 years ago
- Views:
Transcription

1 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D.
2
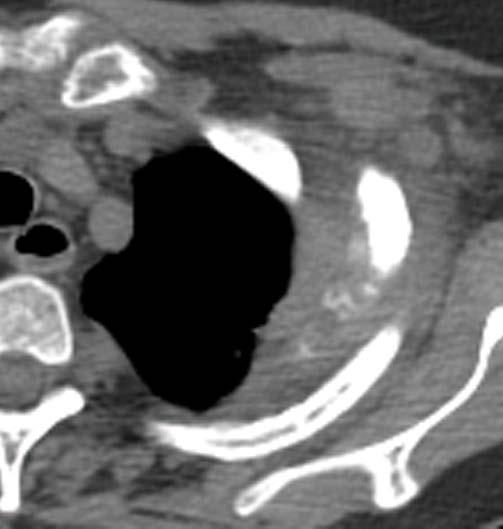
3 Patient with suspected lung cancer presents with left sided chest pain
4 T3
5 What is the T stage of this patient? A) T2a B) T2b C) T3 D) T4
6 What is the T stage of this patient? A) T2a B) T2b C) T3 * D) T4
 for lung cancer If a tumor invades beyond the elastic")


7 Modified Hammar Classification of Visceral Pleural Invasion (VPI) for lung cancer If a tumor invades beyond the elastic layer it is PL1. Tumors that invade to the pleural surface are PL2 and those that invade into any component of the parietal pleura are PL3. PL1 or PL2 indicate VPI and are a T2 descriptor. PL3 indicates invasion of the parietal pleura and is a T3 descriptor.

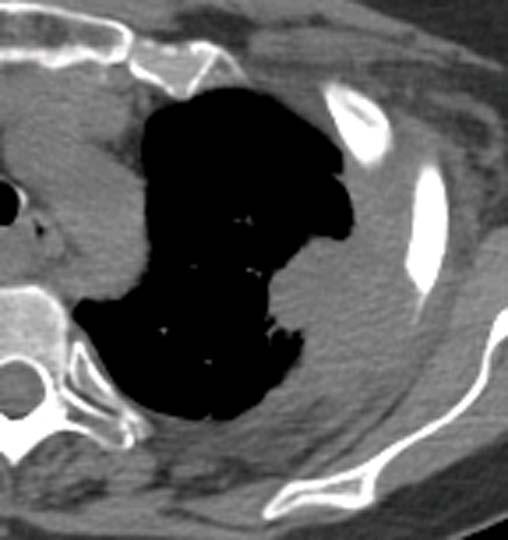
8 If tumor is identified only in the left chest and no nodal or extra-thoracic disease is identified.
9 What is the stage of this patient? A) IIB B) IIIA C) IIIB D) IV
10 What is the stage of this patient? A) IIB* B) IIIA C) IIIB D) IV
11 Staging: Primary Tumor T3 Tumor > 7cm, Direct invasion: chest wall diaphragm, phrenic nerve mediastinal pleura, parietal pericardium main bronchus < 2cm to carina Atelectasis/pneumonitis of entire lung Separate tumor nodule/s in same lobe
12 It ain t braggin if its true.

13 Superior sulcus tumor in a 56-year-old man with sensory loss in the region of the left ulnar nerve distribution and with hoarseness

14 Superior sulcus tumor in a 56-year-old man with sensory loss in the region of the left ulnar nerve distribution and with hoarseness
 and middle (M) trunks of the brachial plexus are clearly separate from the mass, but the lower trunk has been encased and is no")
15 SST invading the fat above the apical pleura and encasing the subclavian artery (*). The upper (U) and middle (M) trunks of the brachial plexus are clearly separate from the mass, but the lower trunk has been encased and is no longer visible, which means that the tumor is not resectable.
16 What is the T stage of this patient? A) T2a B) T2b C) T3 D) T4
17 What is the T stage of this patient? A) T2a B) T2b C) T3 D) T4*
18 Staging: Primary Tumor T4 Tumor of any size that invades: mediastinum, heart, great vessels trachea, esophagus, vertebral body, carina malignant pericardial or pleural effusion Separate tumor nodule/s in a different ipsilateral lobe
19
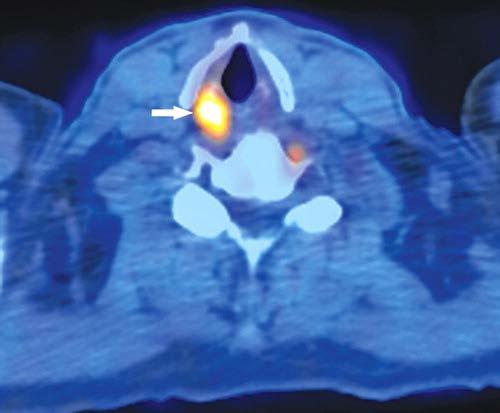
20 FDG uptake by the arytenoid insertion of the right vocal cord A) Metastatic B) Vocal cord paralysis right side C) Can t tell need to biopsy D) Vocal cord paralysis left side
21 FDG uptake by the arytenoid insertion of the right vocal cord A) Metastatic B) Vocal cord paralysis right side C) Can t tell need to biopsy D) Vocal cord paralysis left side*
22
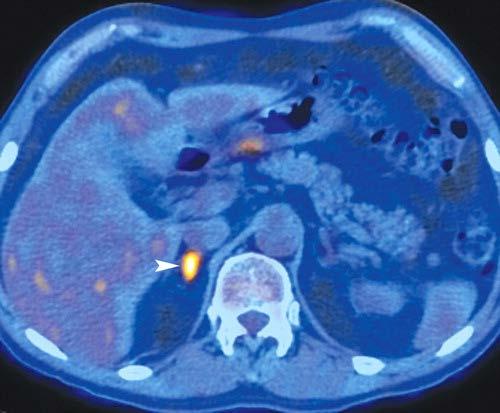
23 FDG uptake by the right adrenal gland A) Likely metastatic B) Likely physiologic C) Can t tell if malignant or benign D) Related to vocal cord paralysis
24 FDG uptake by the right adrenal gland A) Likely metastatic* B) Likely physiologic C) Can t tell if malignant or benign D) Related to vocal cord paralysis
25 Utility of PET/CT in differentiating benign from malignant adrenal nodules. 112 adrenal nodules in 96 patients. Adrenal nodules (+) if average SUV > the liver. 25 / 30 malignant nodules had (+) PET 12 / 82 benign nodules were (+) PET Sensitivity of 83.3% and Specificity of 85.4%. 4/5 malignant nodules with (+) PET had previous therapy. PPV was 67%, and the NPV was 93%. Adrenal masses that are not FDG avid are likely benign. Significant false-negative rate in patients being treated. A considerable # of benign nodules have FDG activity. Vikram, R. et al. Am. J. Roentgenol. 2008;191:
 8 months later shows new focal FDG uptake in the right")
26 58-y/o NSCLC, CT showed 2.5-cm right adrenal low-attenuation lesion -19 HU (C) 8 months later shows new focal FDG uptake in the right adrenal (SUV, 7.3) consistent with interval development of metastatic disease (arrow).
27 What is the stage of this patient? A) IIB B) IIIA C) IIIB D) IV
28 What is the stage of this patient? A) IIB B) IIIA C) IIIB D) IV*
 contains the subclavian artery and its branches, as well as the trunks of the brachial plexus;")
29 Three-dimensional drawing shows the surgical anatomy of the superior sulcus Anatomy of the superior sulcus divided into anterior, middle, and posterior compartments by the scalene muscles. The anterior compartment contains the subclavian vein; the middle compartment (interscalene triangle) contains the subclavian artery and its branches, as well as the trunks of the brachial plexus; and the posterior compartment contains the costovertebral groove, the roots of the brachial plexus, and the stellate ganglion.

30 Sagittal T1-weighted MR image of the superior sulcus shows the courses of the C5 through T1 nerve roots laterally and inferiorly from the neurovertebral foramina. The T1 nerve root is located inferior to the neck of the first rib (R)

31
32 Clinical Summary Patient presented with a middle lobe opacity suspicious for lung cancer. FDG PET CT requested for staging.


33 Low grade FDG uptake in right middle lobe consolidation.
34 What is your impression of the right middle lobe consolidation? a) RML malignancy b) RML pneumonia c) Cannot distinguish RML pneumonia from malignancy d) Pulmonary metastasis from thyroid cancer
35 What is your impression of the right middle lobe consolidation? a) RML malignancy* b) RML pneumonia c) Cannot distinguish RML pneumonia from malignancy d) Pulmonary metastasis from thyroid cancer



36 The tumor formerly known as BAC Adenocarcinoma in situ (<3 cm, solitary, pure lepidic growth; formerly BAC), minimally invasive adenocarcinoma (<3 cm with predominant lepidic growth and 5-mm invasion), invasive adenocarcinoma, and variants of invasive adenocarcinoma. Semin Nucl Med Jul;42(4):
37 Pathology after surgery Right middle lobectomy: Multifocal well differentiated adenoca with papillary features and bronchoalveolar pattern. 0/8 nodes negative


38 FDG avid low density nodule in the right lobe of the thyroid gland. A lymph node with FDG uptake noted below left lobe of the thyroid.
39 What is your impression of the uptake in the right neck? A) Metastases from lung primary to the thyroid gland and right cervical node. B) Consideration of Thyroid primary with nodal metastasis can be evaluated with sonography C) Benign thyroid adenoma and right cervical inflammatory adenopathy. D) de Quervain (subacute) thyroiditis with right cervical inflammatory adenopathy.
40 What is your impression of the uptake in the right neck? A) Metastases from lung primary to the thyroid gland and right cervical node. B) Consideration of Thyroid primary with nodal metastasis can be evaluated with sonography* C) Benign thyroid adenoma and right cervical inflammatory adenopathy. D) de Quervain (subacute) thyroiditis with right cervical inflammatory adenopathy.
41 Pathology after surgery Total thyroidectomy: 2.2 cm papillary thyroid ca extending to soft tissue. Right Neck Dissection 4/64 lymph nodes (+)
42 Discussion Incidental FDG avid focal nodules in the thyroid gland could represent a malignancy in about a third of these findings. Ultrasound evaluation with biopsy may be necessary to verify either a benign thyroid nodule or cancer.
43 Prevalence of malignant incidental thyroid nodules on FDG PET 55,160 patients with 571 patients (1%) having an unexpected focal abnormality Confirmed Dx: 200 (62.1%) benign, 107 (33.2%) malignant, 15 (4.7%) indeterminate Papillary thyroid ca 82.2% most prevalent. mean max SUV for 73 benign lesions was 4.6+/-2.1, and for the 52 malignant lesions was 6.8+/-4.6 (P<0.001). Shie, P, et.al. Nucl Med Commun Sep;30(9):742-8.

44 I'm from Texas, and one of the reasons I like Texas is because there's no one in control. Willie Nelson
45 A 61-year-old man with a 4-month history of cough. CT scan shows a left upper lobe mass and right paratracheal adenopathy
46 What is your impression of the contralateral paratracheal adenopathy? A) Possibility of malignant adenopathy should be considered. B) Chronic inflammatory adenopathy. C) Sarcoidosis D) Negative FDG in lymph node indicates absence of malignancy in this site.
47 What is your impression of the contralateral paratracheal adenopathy? A) Possibility of malignant adenopathy should be considered.* B) Chronic inflammatory adenopathy. C) Sarcoidosis D) Negative FDG in lymph node indicates absence of malignancy in this site.
 disease from the primary lung cancer and the")
48 A 61-year-old man with a 4-month history of cough. CT scan shows a left upper lobe mass and right paratracheal adenopathy Mediastinoscopy confirmed N3 (contralateral nodal) disease from the primary lung cancer and the patient was treated palliatively. A negative PET scan does not preclude biopsy of enlarged mediastinal lymph nodes.

49 NASA
50 Clinical Summary Newly diagnosed Left upper lobe lung cancer with left upper lobe bronchus obstruction. FDG PET/CT performed for radiotherapy planning.

51 Left upper lobe lung primary and right upper lobe FDG avid lesion
52 Tree in bud appearance in right upper lobe
53 What is your diagnosis of the FDG avid RUL nodules? A) Findings typical for atypical mycobacterial infection. B) Findings typical for lymphangitic carcinomatosis. C) Findings typical for multifocal well differentiated adenocarcinoma of the lung. D) Findings typical for pulmonary sarcoidosis.
54 What is your diagnosis of the FDG avid RUL nodules? A) Findings typical for atypical mycobacterial infection.* B) Findings typical for lymphangitic carcinomatosis. C) Findings typical for multifocal well differentiated adenocarcinoma of the lung. D) Findings typical for pulmonary sarcoidosis.


55 Tree in bud appearance in right upper lobe typical for atypical mycobacterial infection

56 DIAGNOSIS No evidence of malignancy Granulation tissue and chronic inflammation consistent with organizing pneumonia SUPPLEMENTAL REPORT A GMS stain, performed over a Pap-stained smear, is negative for Pneumocystis and fungal forms. There is no change in the diagnosis. BAL grew MAI- therapy with azithromycin, ciprofloxacin, and ethambutol.

57 Patient with NSCLC with hematogenously disseminated lung metastases. RUL primary (M) and multiple discrete sharply marginated nodules.

58 Patient with NSCLC and lymphangitic carcinomatosis. CT shows thickening of interlobular septa and peribronchovascular interstitium and visualization of the polygonal shape of the secondary pulmonary lobules.
59 Patterns of Tumor Spread Lung Cancer Incidence of hematogenously disseminated metastases is related to cell type. Hematogenous dissemination occurs late with SCC. Hematogenous dissemination is high with invasive adenoca, large cell ca, and small cell ca and low with localized/indolent adenoca. Lymphatic dissemination of metastasis occurs late with SCC and early and frequently in patients with invasive adenocarcinoma, large cell carcinoma, and SCLC. Lymphatic pathways explaining the likely pattern of spread of mediastinal nodal metastases based on the lobar location of the primary tumor are unreliable.
60 Clinical Summary Physician with suspected lung cancer He had lung biopsy the day before Had complaints of shortness of breath after the PET/CT scan
61 FDG avid right lung mass
62 Pneumothorax

63 Clinical Summary 52 year old patient with CNS high grade B- cell lymphoma, previously treated with chemotherapy referred for restaging.

64
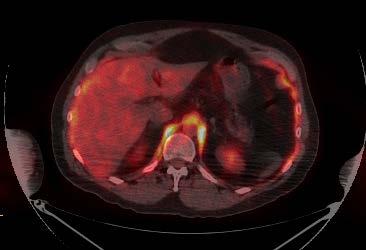
65 What is your impression of the uptake in crico-arytenoid muscles and the diaphragm? A) Lymphoma B) Inflammation or lymphoma C) Inflammation D) Variant uptake
66 What is your impression of the uptake in crico-arytenoid muscles and the diaphragm? A) Lymphoma B) Inflammation or lymphoma C) Inflammation D) Variant uptake*
67 Answer: Variant uptake caused by singultus Patient had chronic hiccups, for 2 weeks. Continued to have hiccups during the uptake phase following FDG injection and PET/CT scanning.
68 Teaching points FDG uptake is increased in muscles contracting during the uptake phase. History is important, including the patient conditions during the period following FDG injection and during image acquisition.

69 It ain t braggin if its true.
70
Collaborative Stage. Site-Specific Instructions - LUNG
 Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
Collecting Cancer Data: Lung
 Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Lung /1/16. Please submit all questions concerning webinar content through the Q&A panel. Reminder:
 1 NAACCR 2015-2016 Webinar Series Collecting Cancer Data: Lung NAACCR 2015 2016 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
1 NAACCR 2015-2016 Webinar Series Collecting Cancer Data: Lung NAACCR 2015 2016 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
GUIDELINES FOR CANCER IMAGING Lung Cancer
 GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
AJCC-NCRA Education Needs Assessment Results
 AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
Lung 8/7/14. Collecting Cancer Data: Lung NAACCR Webinar Series. August 7, 2014
 Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Lung Cancer Staging: The Revised TNM Classification
 Norwegian Society of Thoracic Imaging Oslo, October 2011 Lung Cancer Staging: The Revised TNM Classification Sujal R Desai King s College Hospital, London Lung Cancer The Scale of the Problem Leading cause
Norwegian Society of Thoracic Imaging Oslo, October 2011 Lung Cancer Staging: The Revised TNM Classification Sujal R Desai King s College Hospital, London Lung Cancer The Scale of the Problem Leading cause
The 8th Edition Lung Cancer Stage Classification
 The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Role of Surgery in Management of Non Small Cell Lung Cancer. Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City
 Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
PET CT for Staging Lung Cancer
 PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
6 th Reprint Handbook Pages AJCC 7 th Edition
 6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!!
 The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
PET/CT in lung cancer
 PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Lung. 10/24/13 Chest X-ray: 2.9 cm mass like density in the inferior lingular segment worrisome for neoplasm. Malignancy cannot be excluded.
 Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Boot Camp Case Scenarios
 Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
NAACCR Webinar Series 1
 Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Syllabus: 6 pages (Page 6 lists corresponding figures for Grant's Atlas 11 th & 12 th Eds.)
") PLEURAL CAVITY AND LUNGS Dr. Milton M. Sholley SELF STUDY RESOURCES Essential Clinical Anatomy 3 rd ed. (ECA): pp. 70 81 Syllabus: 6 pages (Page 6 lists corresponding figures for Grant's Atlas 11 th &
PLEURAL CAVITY AND LUNGS Dr. Milton M. Sholley SELF STUDY RESOURCES Essential Clinical Anatomy 3 rd ed. (ECA): pp. 70 81 Syllabus: 6 pages (Page 6 lists corresponding figures for Grant's Atlas 11 th &
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013
 Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Sectional Anatomy Quiz - III
 Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
Sectional Anatomy - III Rashid Hashmi * Rural Clinical School, University of New South Wales (UNSW), Wagga Wagga, NSW, Australia A R T I C L E I N F O Article type: Article history: Received: 30 Jun 2018
OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function
 The root of the neck Jeff Dupree, Ph.D. e mail: jldupree@vcu.edu OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function READING ASSIGNMENT: Moore and
The root of the neck Jeff Dupree, Ph.D. e mail: jldupree@vcu.edu OBJECTIVE: To obtain a fundamental knowledge of the root of the neck with respect to structure and function READING ASSIGNMENT: Moore and
Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis
 19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
19 th Congress of APSR PG of Lung Cancer (ESAP): Update of Lung Cancer Thoracic CT pattern in lung cancer: correlation of CT and pathologic diagnosis Kazuma Kishi, M.D. Department of Respiratory Medicine,
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
THE DESCENDING THORACIC AORTA
 Intercostal Arteries and Veins Each intercostal space contains a large single posterior intercostal artery and two small anterior intercostal arteries. The anterior intercostal arteries of the lower spaces
Intercostal Arteries and Veins Each intercostal space contains a large single posterior intercostal artery and two small anterior intercostal arteries. The anterior intercostal arteries of the lower spaces
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Introduction to Chest CT Interpretation. Objectives 8/28/2017
 Introduction to Chest CT Interpretation Deborah Stein ACNP BC, CCRN NP Education Specialist Department of Anesthesia and Critical Care Medicine August 28, 2017 Objectives Basic Principles Thoracic Anatomy
Introduction to Chest CT Interpretation Deborah Stein ACNP BC, CCRN NP Education Specialist Department of Anesthesia and Critical Care Medicine August 28, 2017 Objectives Basic Principles Thoracic Anatomy
Accomplishes fundamental surgical tenets of R0 resection with systematic nodal staging for NSCLC Equivalent survival for Stage 1A disease
 Segmentectomy Made Simple Matthew J. Schuchert and Rodney J. Landreneau Department of Cardiothoracic Surgery University of Pittsburgh Medical Center Financial Disclosures none Why Consider Anatomic Segmentectomy?
Segmentectomy Made Simple Matthew J. Schuchert and Rodney J. Landreneau Department of Cardiothoracic Surgery University of Pittsburgh Medical Center Financial Disclosures none Why Consider Anatomic Segmentectomy?
MEDIASTINAL STAGING surgical pro
 MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
Sectional Anatomy Quiz II
 Sectional Anatomy II Rashid Hashmi Rural Clinical School, University of New South Wales, Wagga Wagga, New South Wales, Australia A R T I C L E I N F O Article type: Article history: Received: 3 Aug 2017
Sectional Anatomy II Rashid Hashmi Rural Clinical School, University of New South Wales, Wagga Wagga, New South Wales, Australia A R T I C L E I N F O Article type: Article history: Received: 3 Aug 2017
Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer. Quick Reference Chart and Diagrams
 CHEST Special Features Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer Quick Reference Chart and Diagrams Omar Lababede, MD ; Moulay Meziane, MD ; and Thomas Rice, MD, FCCP
CHEST Special Features Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer Quick Reference Chart and Diagrams Omar Lababede, MD ; Moulay Meziane, MD ; and Thomas Rice, MD, FCCP
Lung Cancer. Definition of lung cancer Malignancy arising from lung tissue
 Lung Cancer Definition of lung cancer Malignancy arising from lung tissue Epidemiology of lung cancer Commonest malignancy in western world Commonest cause of death in men and women in the UK Approximately
Lung Cancer Definition of lung cancer Malignancy arising from lung tissue Epidemiology of lung cancer Commonest malignancy in western world Commonest cause of death in men and women in the UK Approximately
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
Mediastinal Tumors: Imaging
 Mediastinal Tumors: Imaging References Imaging in Oncology, Husband and Reznek Computed Tomography and Magnetic Resonance of the thorax, Naidich, Zerhouni, Siegelman, Mediastinal compartments Anterior:
Mediastinal Tumors: Imaging References Imaging in Oncology, Husband and Reznek Computed Tomography and Magnetic Resonance of the thorax, Naidich, Zerhouni, Siegelman, Mediastinal compartments Anterior:
Division of Diagnostic Imaging, The University of Texas M.D. Anderson Cancer Center, Houston, Texas, USA
 89 Lymphology 28 (1995) 89-94 Division of Diagnostic Imaging, The University of Texas M.D. Anderson Cancer Center, Houston, Texas, USA ABSTRACT The anatomy of the posterior intercostal lymphatics and lymph
89 Lymphology 28 (1995) 89-94 Division of Diagnostic Imaging, The University of Texas M.D. Anderson Cancer Center, Houston, Texas, USA ABSTRACT The anatomy of the posterior intercostal lymphatics and lymph
North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma [Based on WOSCAN SCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED WHEN PRINTED Document
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma [Based on WOSCAN SCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED WHEN PRINTED Document
Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer
 Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer Poster No.: C-2297 Congress: ECR 2012 Type: Educational Exhibit Authors: Y.
Pictorial essay of unusual radiologic manifestations of pulmonary and airway metastasis at initial presentation of lung cancer Poster No.: C-2297 Congress: ECR 2012 Type: Educational Exhibit Authors: Y.
Lymphoma Read with the experts
 Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Mediastinum It is a thick movable partition between the two pleural sacs & lungs. It contains all the structures which lie
 Dr Jamila EL medany OBJECTIVES At the end of the lecture, students should be able to: Define the Mediastinum. Differentiate between the divisions of the mediastinum. List the boundaries and contents of
Dr Jamila EL medany OBJECTIVES At the end of the lecture, students should be able to: Define the Mediastinum. Differentiate between the divisions of the mediastinum. List the boundaries and contents of
Special Treatment Issues in Non-small Cell Lung Cancer
 CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES Special Treatment Issues in Non-small Cell Lung Cancer Diagnosis and Management of Lung Cancer, 3rd ed: American College
CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES Special Treatment Issues in Non-small Cell Lung Cancer Diagnosis and Management of Lung Cancer, 3rd ed: American College
Pulmonary Nodules & Masses
 Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Pulmonary Nodules & Masses A Diagnostic Approach Heber MacMahon The University of Chicago Department of Radiology Disclosure Information Consultant for Riverain Technology Minor equity in Hologic Royalties
Mediastinal Mysteries: What can be solved with EBUS?
 Mediastinal Mysteries: What can be solved with EBUS? W. Graham Carlos MD Pulmonary & Critical Care Fellow Indiana University School of Medicine Disclosures None Objectives Introduce you to the technique
Mediastinal Mysteries: What can be solved with EBUS? W. Graham Carlos MD Pulmonary & Critical Care Fellow Indiana University School of Medicine Disclosures None Objectives Introduce you to the technique
ANATOMY OF THE PLEURA. Dr Oluwadiya KS
 ANATOMY OF THE PLEURA Dr Oluwadiya KS www.oluwadiya.sitesled.com Introduction The thoracic cavity is divided mainly into: Right pleural cavity Mediastinum Left Pleural cavity Pleural cavity The pleural
ANATOMY OF THE PLEURA Dr Oluwadiya KS www.oluwadiya.sitesled.com Introduction The thoracic cavity is divided mainly into: Right pleural cavity Mediastinum Left Pleural cavity Pleural cavity The pleural
PLEURAE and PLEURAL RECESSES
 PLEURAE and PLEURAL RECESSES By Dr Farooq Aman Ullah Khan PMC 26 th April 2018 Introduction When sectioned transversely, it is apparent that the thoracic cavity is kidney shaped: a transversely ovoid space
PLEURAE and PLEURAL RECESSES By Dr Farooq Aman Ullah Khan PMC 26 th April 2018 Introduction When sectioned transversely, it is apparent that the thoracic cavity is kidney shaped: a transversely ovoid space
Positron Emission Tomography in Lung Cancer
 May 19, 2003 Positron Emission Tomography in Lung Cancer Andrew Wang, HMS III Patient DD 53 y/o gentleman presented with worsening dyspnea on exertion for the past two months 30 pack-year smoking Hx and
May 19, 2003 Positron Emission Tomography in Lung Cancer Andrew Wang, HMS III Patient DD 53 y/o gentleman presented with worsening dyspnea on exertion for the past two months 30 pack-year smoking Hx and
Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer. Doug Rahn 6/1/12
 Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer Doug Rahn 6/1/12 Outline I. Presentation of Case II. Epidemiology III. Staging IV. Review of Literature V. Recommendations VI.
Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer Doug Rahn 6/1/12 Outline I. Presentation of Case II. Epidemiology III. Staging IV. Review of Literature V. Recommendations VI.
Thyroid and Adrenal Gland
 Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Non small cell Lung Cancer
 Non small cell Lung Cancer The 13th refresher course for residents in radiation oncology Jiraporn Setakornnukul, M.D. Radiation oncology division, Radiology department Siriraj Hospital, Mahidol University
Non small cell Lung Cancer The 13th refresher course for residents in radiation oncology Jiraporn Setakornnukul, M.D. Radiation oncology division, Radiology department Siriraj Hospital, Mahidol University
Imaging of Lung Cancer: A Review of the 8 th TNM Staging System
 Imaging of Lung Cancer: A Review of the 8 th TNM Staging System Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco
Imaging of Lung Cancer: A Review of the 8 th TNM Staging System Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco
Comparison of High-resolution CT Findings between Miliary Metastases and Miliary Tuberculosis 1
 Comparison of High-resolution CT Findings between Miliary Metastases and Miliary Tuberculosis 1 Chan Sung Kim, M.D., Ki-Nam Lee, M.D., Jin Hwa Lee, M.D. Purpose: To compare the findings of high-resolution
Comparison of High-resolution CT Findings between Miliary Metastases and Miliary Tuberculosis 1 Chan Sung Kim, M.D., Ki-Nam Lee, M.D., Jin Hwa Lee, M.D. Purpose: To compare the findings of high-resolution
Imaging of the cisterna chyli on PET-CT in patients with known malignancy: Report of two cases
 Imaging of the cisterna chyli on PET-CT in patients with known malignancy: Report of two cases Natalie Burns, B.S., Jason Barksdale, M.D., Linh Ho, M.D., and Patrick M. Colletti, M.D. Citation: Burns N,
Imaging of the cisterna chyli on PET-CT in patients with known malignancy: Report of two cases Natalie Burns, B.S., Jason Barksdale, M.D., Linh Ho, M.D., and Patrick M. Colletti, M.D. Citation: Burns N,
Lung cancer in patients with chronic empyema
 Lung cancer in patients with chronic empyema Poster No.: P-0025 Congress: ESTI 2015 Type: Scientific Poster Authors: Y. Lee, C.-K. Park; Guri/KR Keywords: Neoplasia, Biopsy, PET-CT, CT, Thorax, Lung DOI:
Lung cancer in patients with chronic empyema Poster No.: P-0025 Congress: ESTI 2015 Type: Scientific Poster Authors: Y. Lee, C.-K. Park; Guri/KR Keywords: Neoplasia, Biopsy, PET-CT, CT, Thorax, Lung DOI:
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Dr. Weyrich G07: Superior and Posterior Mediastina. Reading: 1. Gray s Anatomy for Students, chapter 3
 Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Dr. Weyrich G07: Superior and Posterior Mediastina Reading: 1. Gray s Anatomy for Students, chapter 3 Objectives: 1. Subdivisions of mediastinum 2. Structures in Superior mediastinum 3. Structures in Posterior
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010
 Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
10/14/2018 Dr. Shatarat
 2018 Objectives To discuss mediastina and its boundaries To discuss and explain the contents of the superior mediastinum To describe the great veins of the superior mediastinum To describe the Arch of
2018 Objectives To discuss mediastina and its boundaries To discuss and explain the contents of the superior mediastinum To describe the great veins of the superior mediastinum To describe the Arch of
Surgical management of lung cancer
 Surgical management of lung cancer Nick Roubos FRACS Cardiothoracic Surgeon Box Hill Hospital, Epworth Eastern Thoracic Oncology Non Small Cell Lung Cancer (NSCLC) Small Cell Lung Cancer Mesothelioma Pulmonary
Surgical management of lung cancer Nick Roubos FRACS Cardiothoracic Surgeon Box Hill Hospital, Epworth Eastern Thoracic Oncology Non Small Cell Lung Cancer (NSCLC) Small Cell Lung Cancer Mesothelioma Pulmonary
Karoline Nowillo, MD. February 1, 2008
 Case Presentation Karoline Nowillo, MD SUNY Downstate t February 1, 2008 Case Presentation Chief complaint enlarging goiter x 8 months History of present illness shortness of breath, heaviness in chest
Case Presentation Karoline Nowillo, MD SUNY Downstate t February 1, 2008 Case Presentation Chief complaint enlarging goiter x 8 months History of present illness shortness of breath, heaviness in chest
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Tumors. Chapter 3. Primary neurogenic tumors. Tumors 27
 Tumors 27 Chapter 3 Tumors MR imaging of the brachial plexus is frequently requested to rule out a tumor in or near the brachial plexus, or to evaluate the extension of a known tumor in the region of the
Tumors 27 Chapter 3 Tumors MR imaging of the brachial plexus is frequently requested to rule out a tumor in or near the brachial plexus, or to evaluate the extension of a known tumor in the region of the
Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer
 November 2010 Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer Laura Myers, Harvard Medical School, Year III Clinical Presentation 79yo woman with cough productive of green
November 2010 Use of Integrated PET CT in the Clinical Staging of Non Small Cell Lung Cancer Laura Myers, Harvard Medical School, Year III Clinical Presentation 79yo woman with cough productive of green
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
The International Association for the Study of Lung Cancer (IASLC) Lung Cancer Staging Project, Data Elements
 Lung Cancer Staging Project, Data Elements") Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Histopathology of NSCLC, IHC markers and ptnm classification
 ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
Lung /4/18. Please submit all questions concerning the webinar content through the Q&A panel.
 Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Educational Objectives. Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach.
 Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Ashley Pyfferoen, MS, CMD. Gundersen Health Systems La Crosse, WI
 Ashley Pyfferoen, MS, CMD Gundersen Health Systems La Crosse, WI 3 Radiation Oncologists 3 Physicists 2 Dosimetrists 9 Radiation Therapists o o o o o o o o o Brachial Plexus Anatomy Brachial Plexopathy
Ashley Pyfferoen, MS, CMD Gundersen Health Systems La Crosse, WI 3 Radiation Oncologists 3 Physicists 2 Dosimetrists 9 Radiation Therapists o o o o o o o o o Brachial Plexus Anatomy Brachial Plexopathy
Lung Cancer-a primer. Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo
 Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
Thoracic Imaging: A Case of Metastatic Adenocarcinoma of Unknown Primary
 January 28, 2009 Thoracic Imaging: A Case of Metastatic Adenocarcinoma of Unknown Primary Kristina Mirabeau-Beale, Harvard Medical School Year III Gillian Lieberman, MD Agenda Introduce Patient RS Discuss
January 28, 2009 Thoracic Imaging: A Case of Metastatic Adenocarcinoma of Unknown Primary Kristina Mirabeau-Beale, Harvard Medical School Year III Gillian Lieberman, MD Agenda Introduce Patient RS Discuss
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Pulmonary Neoplasms & Chest Disorders Ahmed Mahmoud
 Pulmonary Neoplasms & Chest Disorders Ahmed Mahmoud Lung Ca ;Pathological types Adenocarcinoma More common in females Peripheral location Spread mainly by blood(brain..) Incidence is increasing (the most
Pulmonary Neoplasms & Chest Disorders Ahmed Mahmoud Lung Ca ;Pathological types Adenocarcinoma More common in females Peripheral location Spread mainly by blood(brain..) Incidence is increasing (the most