Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017
|
|
|
- Lisa Chapman
- 6 years ago
- Views:
Transcription

1 Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017
2
3

4 I will not be discussing this
5 Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of primary hypothyroidism in adults
6
7 Laboratory assessment Thyroxine (T4) and triiodothyronine (T3) secretion regulated by Thyroid Stimulating Hormone (TSH) secretion from pituitary gland TSH secretion regulated by Thyrotropin Releasing Hormone (TRH) from hypothalamus More importantly, TSH secretion regulated by negative feedback by T4 and T3 on both pituitary and hypothalamus
8 Figure 11-8, Williams Textbook of Endocrinology, 13th ed
9 TSH and T4 There is a negative log-linear relationship between serum free T4 and TSH concentrations What does this mean? Very small changes in serum free T4 concentrations cause large changes in TSH values

10 Figure Williams Textbook of Endocrinology, 13th ed
11 TSH assay TSH is the single best test for assessing thyroid function, assuming there are no confounding factors These factors may include Hospitalization Medications that affect thyroid function Medications that affect thyroid function tests Disorders of the pituitary or hypothalamus
12 Current TSH assay Current TSH assay is the third generation assay Detection limit of 0.01 mu/l With that level of detection, patients who are hyperthyroid are readily apparent and differentiated from euthyroid patients Upper limit of normal is subject of some controversy
13 Differences in TSH Age related TSH values are important as are TSH distributions based on race
14 From: Age- and Race-Based Serum Thyrotropin Reference Limits J Clin Endocrinol Metab. 2010;95(2): doi: /jc J Clin Endocrinol Metab Copyright 2010 by The Endocrine Society
15 From: Age- and Race-Based Serum Thyrotropin Reference Limits J Clin Endocrinol Metab. 2010;95(2): doi: /jc J Clin Endocrinol Metab Copyright 2010 by The Endocrine Society
16 Total T4 and Total T3 Total T4 Almost all of T4 is bound to thyroid binding globulin (TBG), transthyretin (TBPA), and albumin Serum total T4 assays measure bound T4 and free T4 Total T3 T3 is less tightly bound to TBG and TBPA T3 is more tightly bound to albumin
17 Free T4 and Free T3 Free refers to that portion of hormone that is readily available for each individual cell to use compare to bound hormone None of the free T4 tests available can measure free T4 directly
18 Free T4 and Free T3 Direct free T4 measurements Assumption is that binding protein abnormalities are taken into account No assessment of free T4 can account for all binding protein abnormalities that can occur Free T4 by equilibrium dialysis is considered the best T4 measurement Most expensive Result takes a long time to come back
19 I want all of my levels checked My practice is to check and to follow TSH only in known primary hypothyroidism
20 Checking T4 and T3 Follow free T4 in secondary (central) hypothyroidism Hyperthyroidism Check free T4 and total T3 because some assessment of these levels is needed, imprecise as they may be T3 dominance T4 levels normal or at upper limit of normal T3 levels are elevated But the above is also based on TSH low or suppressed Clinical picture (symptoms of hyperthyroidism)
21 Thyroid antibodies Almost all patients with Hashimoto s thyroiditis (chronic autoimmune thyroiditis) have positive antibodies to thyroglobulin and thyroid peroxidase Thyroglobulin: protein made by thyroid follicular cells Thyroid peroxidase: enzyme that catalyzes iodination of tyrosine residues of thyroglobulin to form monoiodotyrosine and diiodotyrosine TSH receptor antibodies are frequently elevated when hyperthyroidism is secondary to Graves disease

22 Table Williams Textbook of Endocrinology, 13th ed
23 Hospitalized and seriously ill patients Euthyroid sick syndrome Low serum T4 Low serum T3 Low serum TSH Administering thyroid hormone can actually be harmful Changes in thyroid function during illness can be protective Prevent excessive tissue catabolism Thyroid function should NOT be checked in seriously ill patients unless thyroid dysfunction is high on differential diagnosis In a hospitalized patient, do NOT check TSH alone
24 Figure 1. Thyroid function in nonthyroidal illness. UpToDate Online. July 2017.
25 Hospitalized and seriously ill patients Peripheral 5 monodeiodinases produce T3 from T4 in end organ tissue (muscle, fat, etc) This enzymatic reaction decreases whenever Caloric intake is low There is a nonthyroidal illness
26 Figure 2. Thyroid function in nonthyroidal illness. UpToDate Online. July 2017.
27 Hospitalized and seriously ill patients Why does the decrease in T3 production occur? High endogenous serum cortisol concentrations Exogenous steroid therapy Inhibitors of deiodinase activity increase in illness Cytokines Drugs that affect 5 monodeiodinase activity Amiodarone Propanolol
28 Hospitalized and seriously ill patients Measure T3 in patients with low TSH Differential diagnosis: hyperthyroidism v. nonthyroidal illness T3 elevated in hyperthyroidism T3 low in euthyroid sick syndrome Speaks to the importance of checking all thyroid function tests in hospitalized patients
29 Hospitalized and seriously ill patients Low T4 Fifteen to twenty percent of hospitalized patients have low total T4 levels Total T4 is usually low because of reductions of one of the three thyroid hormone binding proteins Free T4 is usually normal in patients with illness that is not severe Can be low due to Inability to account for all binding protein abnormalities Decreased production of normal TBG Production of TBG that binds T4 poorly
30 Hospitalized and seriously ill patients T4 to T3 conversion Low serum T3 levels may be beneficial in critically ill patients Inactivation of T4 to T3 conversion during illness may be beneficial In a study of patients in an ICU, lower T3 and higher T4 levels were associated with higher likelihood of earlier discharge Very low T4 levels in critically ill patients is a poor prognostic sign
31 Hospitalized and seriously ill patients TSH Low but detectable Almost always, TSH will be within normal limits after recovery from illness Undetectable Seventy five percent will have true hyperthyroidism from some etiology Elevated Transient elevations even up to 20 mu/l common during recovery from nonthyroidal illness Greater than 20: usually are hypothyroid
32 Medications that decrease TSH secretion Glucocorticoids Usually an acute effect Those on chronic steroid treatment usually not affected because TSH secretion increases in response >20 mg/day of prednisone or equivalent doses of other steroids Dopamine Dobutamine Octreotide
33 Medications that cause hyperthyroidism High doses of iodide or drugs that contain iodide may cause hyperthyroidism Can occur with patients with goiter who are iodine deficient Can occur in patients who are not iodine deficient if they have autonomous nodules but only when they are exposed to large amount of iodide Amiodarone can cause hyperthyroidism either because of Causing a thyroiditis The high iodine load of amiodarone in patients with autonomous nodules
34 Medications that can cause hypothyroidism Iodine Wolff-Chaikoff effect In iodine sufficient patients Lithium Should not be discontinued if hypothyroidism occurs Treat hypothyroidism Tyrosine kinase inhibitors Chemotherapeutic agents used for treatment of gastrointestinal stromal tumors, hepatocellular carcinoma, chronic myeloid leukemia
35 Euthyroid hyperthyroxinemia and hypothyroxinemia Medications that interfere with thyroid hormone (T4 and T3) binding in serum Results in a change in serum total T4 and total T3 concentrations, not in the free levels of those hormones Most clinically relevant situations: OCPS, estrogens, selective estrogen receptor modulators Increase TBG Androgens, anabolic steroids, glucocorticoids Lower TBG
36
37 Gastrointestinal absorption of thyroid hormone Bile acid binding resins bind thyroid hormones and decrease absorption E.g., cholestyramine, colestipol, colesevelam No effect in euthyroid patients without thyroid disease Levothyroxine should be administered at least 4 hours after administration of bile acid binding resins
38 Gastrointestinal absorption of thyroid hormone Proton pump inhibitors may affect absorption of thyroid hormone since gastric acid is required for absorption Calcium and iron are notorious for binding with levothyroxine, decreasing absorption Separate calcium and/or iron containing supplements by several hours
39 Biotin Because of the lab assays, high dose biotin supplements may cause lab values consistent with hyperthyroidism, specifically consistent with Graves disease Falsely low TSH values High levels of T4, T3, and TSH receptor antibodies Have patients hold biotin for about two days prior to checking thyroid function tests
40
41 Diagnosis of hypothyroidism Nonspecific symptoms, some or all of which we all experience at one time or another Thus, diagnosis of hypothyroidism must also rely on lab testing
42 Diagnosis of hypothyroidism Primary hypothyroidism High TSH, low serum free T4 Subclinical hypothyroidism High TSH, normal serum free T4 Secondary (central) hypothyroidism Low serum free T4, inappropriate TSH (not elevated)
43 Diagnosis of hypothyroidism More common in women (5-8 times more common) Some familial predisposition
44 Diagnosis of hypothyroidism Physical exam findings Goiter Bradycardia Hypertension Delayed relaxation of deep tendon reflexes Other lab abnormalities Hyperlipidemia Macrocytic anemia Elevated creatine kinase Hyponatremia
45 Primary hypothyroidism Primary hypothyroidism Intrinsic to thyroid Not secondary to pituitary or hypothalamus Ninety-five percent of cases
46 Diagnosis of hypothyroidism TSH should be initial test Elevated repeat TSH along with free T4 If repeat TSH is elevated and free T4 is low, start levothyroxine If repeat TSH is still elevated but free T4 is normal, this is subclinical hypothyroidism Decision to make about whether to treat with levothyroxine Depends on Individual patient factors Degree of TSH elevation Normal but patient has symptoms of hypothyroidism Check free T4 to assess for secondary hypothyroidism
47 Secondary hypothyroidism Caused by problem with hypothalamus and/or pituitary Specifically a problem with the thyrotroph cells in the pituitary that produce TSH (thyrotropin) TSH does not appropriately increase as T4 levels decrease Suspect when patient has Known hypothalamic or pituitary disease Pituitary adenoma History of surgery for pituitary adenoma Known other hormonal deficiencies such as adrenal insufficiency or growth hormone deficiency
48 Thyroid antibodies in hypothyroidism Hashimoto s thyroiditis Most common etiology for primary hypothyroidism in the world in patients who are iodine sufficient Both thyroglobulin (Tg) antibodies and thyroid peroxidase (TPO) antibodies can be elevated TPO antibodies are elevated in > 90% of patients with Hashimoto s thyroiditis
49 Thyroid antibodies in hypothyroidism In most instances, it is not necessary or recommended to check thyroid antibodies Elevated levels of thyroid antibodies may indicate that a patient with normal TSH and normal free T4 is more predisposed to develop hypothyroidism Elevated levels of thyroid antibodies do not indicate When a patient may develop hypothyroidism What the starting dose of levothyroxine should be How often or how much to change the dose of levothyroxine
50 Thyroid antibodies in hypothyroidism Recommend checking TSH annually in patients with elevated thyroid antibodies Definitely no utility in checking thyroid antibodies in patients who already have a diagnosis of primary hypothyroidism and who are on treatment Check thyroglobulin antibodies as part of a thyroglobulin panel in patients who have had thyroid cancer treated by total thyroidectomy and radioactive iodine remnant ablation
51
52 Treatment of hypothyroidism T4 levothyroxine is treatment of choice T4 is a prohormone Peripheral enzymatic deiodination of T4 forms T3 T3 is the actual thyroid hormone used in peripheral cells
53 Treatment of hypothyroidism Half life of T4 is seven days Half life of T3 is < one day Once daily dosing of T4 results in steady state of both T4 and T3
54 Treatment of Primary Hypothyroidism in Adults. UpToDate Online. July 2017.
55 Dosing of levothyroxine Rule of thumb Dose 1.6 mcg/kg/day of lean body weight E.g., for 70 kg person dose would be levothyroxine 112 mcg daily Again, this is an approximation Can use this in young, otherwise healthy patients In this population, I find levothyroxine dose of 25 mcg daily to be useless In older patients and/or those with heart disease, start with levothyroxine 25 mcg 50 mcg daily Titrate slowly, based on checking TSH every 6-8 weeks
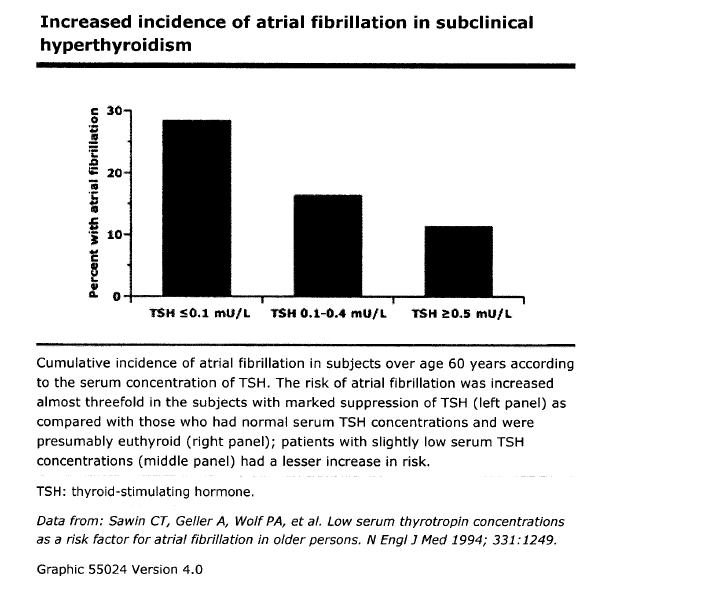
56 Dosing of levothyroxine Excessive levothyroxine replacement Patients who are hyperthyroid generally feel better Obviously this is not the correct treatment approach Risks the lower the TSH, the greater the risks Cardiovascular atrial fibrillation Bone loss
57
58 T3 and combined T4-T3 therapy I almost never advise combination T4-T3 therapy Remember that T4 is deiodinated to T3 in peripheral tissues In most studies, serum T3 concentrations were normal in hypothyroid patients treated with levothyroxine Almost all studies have concluded that combination T4-T3 therapy is not superior to T4 alone for resolution of hypothyroid symptoms
59 T3 and combined T4-T3 therapy Normal ratio of T4 to T3 in the body is 13:1 to 16:1 The few studies in which patients stated that they felt better on combination therapy, they were receiving very high doses of T3 One study from Lithuania in 1999 indicated improvement in mood and psychological function with combination therapy Only 33 patients were studied
60 T3 and combined T4-T3 therapy Due to short half life of T3, any combination therapy of T4 and T3 is not ideal Creates pulses of T3 Correct dosing may require taking very small doses of T3 several times per day (doses that are not available) or a slow release formulation of T3 (which is not available either) Some patients may have a polymorphism in type 2 deiodinase which results in impaired conversion of T4 T3
61 T4 and combined T4-T3 therapy Possible treatment strategy Try to mimic normal physiologic ratio of T4:T3 of 13:1 to 16:1 Example: Patient who is taking levothyroxine 175 mcg daily and persistently has hypothyroid symptoms with normal TSH Decrease levothyroxine to 150 mcg daily Start T3 at dose of 5 mcg bid (10 mcg total per day) Check TSH only 6-8 weeks later If TSH is normal, and patient feels better continue the T3 If TSH is normal, but patient does not feel better discontinue the T3
62
63 T3 and combined T4-T3 therapy Pig thyroid gland extracts ( natural ) are not appropriate treatment T4:T3 ratio in these preparations is excessive
64 T3 and combined T4-T3 therapy American Thyroid Association Levothyroxine should remain the standard of care No consistently strong evidence for superiority of alternative preparations over levothyroxine only European Thyroid Association Combination therapy should be considered solely as an experimental treatment overseen by accredited internists / endocrinologists, and discontinued if no improvement is experienced after three months. Italian Thyroid Association Combination therapy generally not recommended Trial can be considered to improve adherence to treatment or patient well-being.
65 T3 and combined T4-T3 therapy ABSOLUTELY avoid in pregnancy Fetus uses maternal T4, not T3 Fetuses of women taking dessicated thyroid hormone or combination T4-T3 therapy may not have appropriate neurologic development ABSOLUTELY avoid in elderly More susceptible to adverse effects of thyroid hormone excess Atrial fibrillation Osteoporotic fractures
66 Hypothyroidism and pregnancy Dose of levothyroxine in patients with preexisting hypothyroidism can increase by as much as 50% during pregnancy Treatment strategy Check TSH every 4 weeks during pregnancy Maintain mother s TSH in population and trimester specific range; or TSH < 2.5 if those are not available
67 Summary In the outpatient setting, in almost all instances, TSH is the single best test for diagnosing hypothyroidism Moreover, TSH is the best test to follow when a patient is already being treated for hypothyroidism Lab testing for thyroid disorders can be affected by any number of factors, such as hospitalization and medications Treatment of choice in hypothyroidism is levothyroxine
68
Chapter I.A.1: Thyroid Evaluation Laboratory Testing
 Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
Hypothyroidism. Definition:
 Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Thyroid and Antithyroid Drugs. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014
 Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS
 LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
THYROID HORMONES: An Overview
 1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY PBL SEMINAR MBBS III; BMLS & BDS Year 3 What are the Thyroid Hormones? THYROID
1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY PBL SEMINAR MBBS III; BMLS & BDS Year 3 What are the Thyroid Hormones? THYROID
None. Thyroid Potpourri for the Primary Care Physician. Evaluating Thyroid Function. Disclosures. Learning Objectives
 Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Decoding Your Thyroid Tests and Results
 Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Thyroid Function TSH Analyte Information
 Thyroid Function TSH Analyte Information 1 2013-05-01 Thyroid-stimulating hormone (TSH) Introduction Thyroid-stimulating hormone (thyrotropin, TSH) is a glycoprotein with molecular weight of approximately
Thyroid Function TSH Analyte Information 1 2013-05-01 Thyroid-stimulating hormone (TSH) Introduction Thyroid-stimulating hormone (thyrotropin, TSH) is a glycoprotein with molecular weight of approximately
Approach to thyroid dysfunction
 Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
THYROID HORMONES & THYROID FUNCTION TESTS
 THYROID HORMONES & THYROID FUNCTION TESTS SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY LECTURE BMLS III
THYROID HORMONES & THYROID FUNCTION TESTS SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY CLINICAL BIOCHEMISTRY LECTURE BMLS III
Thyroid and Antithyroid Drugs. Dr. Alia Shatanawi Feb,
 Thyroid and Antithyroid Drugs Dr. Alia Shatanawi Feb, 24 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed of epithelial cells which
Thyroid and Antithyroid Drugs Dr. Alia Shatanawi Feb, 24 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed of epithelial cells which
Hypothalamo-Pituitary-Thyroid Axis
 SMGr up Hypothalamo-Pituitary-Thyroid Axis Orluwene Chituru Godwill 1 * and Ohiri John U 1 1 Chemical Pathology Department, University of Port Harcourt Teaching Hospital, Nigeria *Corresponding author:
SMGr up Hypothalamo-Pituitary-Thyroid Axis Orluwene Chituru Godwill 1 * and Ohiri John U 1 1 Chemical Pathology Department, University of Port Harcourt Teaching Hospital, Nigeria *Corresponding author:
Thyroid Disease. I have no disclosures. Overview TSH. Matthew Kim, M.D. July, 2012
 Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Back to the Basics: Thyroid Gland Structure, Function and Pathology
 Back to the Basics: Thyroid Gland Structure, Function and Pathology JANELLE M. CHIASERA LEARNING OBJECTIVES 1. Explain the HPT feedback system involving the thyroid gland. Include the hormone produced
Back to the Basics: Thyroid Gland Structure, Function and Pathology JANELLE M. CHIASERA LEARNING OBJECTIVES 1. Explain the HPT feedback system involving the thyroid gland. Include the hormone produced
HORMONES OF THE POSTERIOR PITUITARY
 HORMONES OF THE POSTERIOR PITUITARY HORMONES OF THE POSTERIOR PITUITARY In contrast to the hormones of the anterior lobe of the pituitary, those of the posterior lobe, vasopressin and oxytocin, are not
HORMONES OF THE POSTERIOR PITUITARY HORMONES OF THE POSTERIOR PITUITARY In contrast to the hormones of the anterior lobe of the pituitary, those of the posterior lobe, vasopressin and oxytocin, are not
Index. Graves disease, 111 thyroid autoantigens, 110 Autoimmune thyroiditis, 11, 58, 180, 181. B Bamforth Lazarus syndrome, 27
 Index A Adrenergic activation, 77 Allan Herndon Dudley syndrome, 31 Ambulatory practice choice of test, 156, 157 screening general population, thyroid dysfunction, 163, 164 targeted population, 164 167
Index A Adrenergic activation, 77 Allan Herndon Dudley syndrome, 31 Ambulatory practice choice of test, 156, 157 screening general population, thyroid dysfunction, 163, 164 targeted population, 164 167
B-Resistance to the action of hormones, Hormone resistance characterized by receptor mediated, postreceptor.
 Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Understanding Thyroid Labs
 Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Thyroid hormone. Functional anatomy of thyroid gland
 Thyroid hormone ส ว ฒณ ค ปต ว ฒ ต กจ ฑาธ ช ห อง 101 Aims Functional anatomy of thyroid gland Synthesis, secretion and metabolism of the thyroid hormones The mechanism of thyroid hormone action Role of
Thyroid hormone ส ว ฒณ ค ปต ว ฒ ต กจ ฑาธ ช ห อง 101 Aims Functional anatomy of thyroid gland Synthesis, secretion and metabolism of the thyroid hormones The mechanism of thyroid hormone action Role of
Common Issues in Management of Hypothyroidism
 Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Thyroid Gland 甲状腺. Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel:
, PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel:") Thyroid Gland 甲状腺 Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel: 88208292 Outline Thyroid Hormones Types Biosynthesis Storage and Release
Thyroid Gland 甲状腺 Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel: 88208292 Outline Thyroid Hormones Types Biosynthesis Storage and Release
Pitfalls of TFTs Interpretation
 Mohammad Reza Bakhtiari DCLS, PhD Pitfalls of TFTs Interpretation CME July 2006 Vol.24 No.7, http://keck.usc.edu HPT axis physiology Log-linear relationship between TSH and FT4 Patient Specific Set Point
Mohammad Reza Bakhtiari DCLS, PhD Pitfalls of TFTs Interpretation CME July 2006 Vol.24 No.7, http://keck.usc.edu HPT axis physiology Log-linear relationship between TSH and FT4 Patient Specific Set Point
Endocrine part two. Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy
 Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Understanding thyroid function tests. Dr. Colette George
 Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
Thyroid Plus. Central Thyroid Regulation & Activity. Peripheral Thyroid Function. Thyroid Auto Immunity. Key Guide. Patient: DOB: Sex: F MRN:
 Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
HYPERTHYROIDISM. Hypothalamus. Thyrotropin-releasing hormone (TRH) Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3
 Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3") HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY
 ENDOCRINE DISORDERS IN THE ELDERLY (part 2) TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY Pituitary axis Target organs of the pituitary gland Negative feedback Hypothalamus-Pituitary-Thyroid axis Thyroid
ENDOCRINE DISORDERS IN THE ELDERLY (part 2) TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY Pituitary axis Target organs of the pituitary gland Negative feedback Hypothalamus-Pituitary-Thyroid axis Thyroid
Requesting and Management of abnormal TFTs.
 Requesting and Management of abnormal TFTs. At the request of a number of GPs I have produced summary guidelines surrounding thyroid testing. These have been agreed with our Endocrinology leads Dr Bell
Requesting and Management of abnormal TFTs. At the request of a number of GPs I have produced summary guidelines surrounding thyroid testing. These have been agreed with our Endocrinology leads Dr Bell
Thyroid Function. Thyroglobulin Analyte Information
 Thyroid Function Thyroglobulin Analyte Information - 1-2011-01-11 Thyroglobulin Introduction Thyroglobulin (Tg) is a big dimeric protein consisting of two identical subunits. It has 2,748 amino acids in
Thyroid Function Thyroglobulin Analyte Information - 1-2011-01-11 Thyroglobulin Introduction Thyroglobulin (Tg) is a big dimeric protein consisting of two identical subunits. It has 2,748 amino acids in
Table 1: Thyroid panel. Result (reference interval) TSH 89.5 miu/l ( ) Total T4 5.2 µg/dl ( ) T3 uptake 39% (22-35)
 TSH 89.5 miu/l ( ) Total T4 5.2 µg/dl ( ) T3 uptake 39% (22-35)") Introduction Thyroid disease is the second most common endocrine disorder (behind diabetes), and its prevalence increases with increasing age. The incidence of newly diagnosed thyroid cancer is increasing
Introduction Thyroid disease is the second most common endocrine disorder (behind diabetes), and its prevalence increases with increasing age. The incidence of newly diagnosed thyroid cancer is increasing
DRUGS. 4- Two molecules of DIT combine within the thyroglobulinto form L-thyroxine (T4)' One molecule of MIT & one molecule of DIT combine to form T3
' One molecule of MIT & one molecule of DIT combine to form T3") THYROID HORMONEs & ANTITHYROID The thyroid secretes 2 types of hormones: DRUGS 1- Iodine containing amino acids (are important for growth, development and metabolism) and these are: triodothyronine, tetraiodothyronine,(
THYROID HORMONEs & ANTITHYROID The thyroid secretes 2 types of hormones: DRUGS 1- Iodine containing amino acids (are important for growth, development and metabolism) and these are: triodothyronine, tetraiodothyronine,(
Sample Type - Serum Result Reference Range Units. Central Thyroid Regulation Surrey & Activity KT3 4Q. Peripheral Thyroid D Function mark
 Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
Thyrotoxicosis in Pregnancy: Diagnose and Management
 Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Lecture title. Name Family name Country
 Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Thyroid Hormones (T 4 & T 3 )
") 1 Thyroid Hormones (T 4 & T 3 ) Normalize growth and development, body temperature, and energy levels. Used as thyroid replacement therapy in hypothyroidism. Thyroxine (T 4 ) is peripherally metabolized
1 Thyroid Hormones (T 4 & T 3 ) Normalize growth and development, body temperature, and energy levels. Used as thyroid replacement therapy in hypothyroidism. Thyroxine (T 4 ) is peripherally metabolized
DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT ENDOCRINE SYSTEM AT A GLANCE OBJECTIVES ANATOMY OF THE THYROID
 OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
Thyroid Screen (Serum)
") Thyroid Screen (Serum) Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4)
Thyroid Screen (Serum) Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4)
The interpretation and management of thyroid disorders
 Journal of Endocrinology, Metabolism and Diabetes of South Africa 2015 ; 20(2) http://dx.doi.org/10.1080/16089677.2015.1056468 Open Access article distributed under the terms of the Creative Commons License
Journal of Endocrinology, Metabolism and Diabetes of South Africa 2015 ; 20(2) http://dx.doi.org/10.1080/16089677.2015.1056468 Open Access article distributed under the terms of the Creative Commons License
Thyroid disorders. Dr Enas Abusalim
 Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Disorders of Thyroid Function
 Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Underactive Thyroid. Diagnosis, Treatment & Controversies
 Underactive Thyroid Diagnosis, Treatment & Controversies Dr. Asif Malik Humayun Consultant Endocrinologist Milton Keynes University Hospital NHS Foundation Trust Thyroid Hormone Control of metabolism
Underactive Thyroid Diagnosis, Treatment & Controversies Dr. Asif Malik Humayun Consultant Endocrinologist Milton Keynes University Hospital NHS Foundation Trust Thyroid Hormone Control of metabolism
Pearls and Pitfalls of Thyroid Diagnosis. Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS
 Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Mastering Thyroid Disorders. Douglas C. Bauer, MD UCSF Division of General Internal Medicine
 Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
Alvin C. Powers, M.D. 1/27/06
 Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid Gland 甲状腺. Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel:
, PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel:") Thyroid Gland 甲状腺 Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel: 88208292 Outline Thyroid Hormones Types Biosynthesis Storage and Release
Thyroid Gland 甲状腺 Huiping Wang ( 王会平 ), PhD Department of Physiology Rm C541, Block C, Research Building, School of Medicine Tel: 88208292 Outline Thyroid Hormones Types Biosynthesis Storage and Release
Hypothyroidism part two diagnosis, treatment and nursing
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk Hypothyroidism part two diagnosis, treatment and nursing Author : Gemma Reid Categories : RVNs Date : July 1, 2008 Gemma Reid
Vet Times The website for the veterinary profession https://www.vettimes.co.uk Hypothyroidism part two diagnosis, treatment and nursing Author : Gemma Reid Categories : RVNs Date : July 1, 2008 Gemma Reid
Hypothyroidism in Women
 Illustration istock Collection / thinkstockphotos.com T Hypothyroidism in Women Donna Dunn Thyroid disease is a major health issue in the United States. Approximately 20 million Americans have been diagnosed
Illustration istock Collection / thinkstockphotos.com T Hypothyroidism in Women Donna Dunn Thyroid disease is a major health issue in the United States. Approximately 20 million Americans have been diagnosed
Understanding Your Blood Tests by Larry Levin, MD
 Bulletin #42 GRAVES DISEASE & THYROID FOUNDATION Educate * Encourage * Empower P.O. Box 2793 Rancho Santa Fe, CA 92067 (877) 643-3123 www.gdatf.org info@gdatf.org Understanding Your Blood Tests by Larry
Bulletin #42 GRAVES DISEASE & THYROID FOUNDATION Educate * Encourage * Empower P.O. Box 2793 Rancho Santa Fe, CA 92067 (877) 643-3123 www.gdatf.org info@gdatf.org Understanding Your Blood Tests by Larry
Virginia ACP Clinical Update Thyroid Clinical Pearls. University of Virginia. Richard J. Santen MD
 Virginia ACP Clinical Update Thyroid Clinical Pearls University of Virginia Richard J. Santen MD Goal Provide a guide to frequently encountered problems in thyroid disease Follow my approach to recently
Virginia ACP Clinical Update Thyroid Clinical Pearls University of Virginia Richard J. Santen MD Goal Provide a guide to frequently encountered problems in thyroid disease Follow my approach to recently
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital
 The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
Timothy Bilash MD MS OBG Northern Inyo Hospital, Bishop, CA October 20, :30 PM
 Thyroxine Deficiency in Pregnancy Timothy Bilash MD MS OBG Northern Inyo Hospital, Bishop, CA October 20, 2006 1:30 PM WHI Estrogen recap In http://courses.washington.edu/bonephys/opestrogen.html. from:
Thyroxine Deficiency in Pregnancy Timothy Bilash MD MS OBG Northern Inyo Hospital, Bishop, CA October 20, 2006 1:30 PM WHI Estrogen recap In http://courses.washington.edu/bonephys/opestrogen.html. from:
Thyroid Management. Evolving Controversy - Science, Dogma, Opinion. The Ogden Surgical Medical Society May 2016
 Thyroid Management Evolving Controversy - Science, Dogma, Opinion The Ogden Surgical Medical Society May 2016 Published Guidelines AACE and ATA - Clinical Practice Guidelines in 2012 Guidelines are neither
Thyroid Management Evolving Controversy - Science, Dogma, Opinion The Ogden Surgical Medical Society May 2016 Published Guidelines AACE and ATA - Clinical Practice Guidelines in 2012 Guidelines are neither
Hypothyroidism in pregnancy. Nor Shaffinaz Yusoff Azmi Jabatan Perubatan Hospital Sultanah Bahiyah Kedah
 Hypothyroidism in pregnancy Nor Shaffinaz Yusoff Azmi Jabatan Perubatan Hospital Sultanah Bahiyah Kedah Agenda 1. Epidemiology and clinical characteristics of maternal hypothyroidism 2. Prevention and
Hypothyroidism in pregnancy Nor Shaffinaz Yusoff Azmi Jabatan Perubatan Hospital Sultanah Bahiyah Kedah Agenda 1. Epidemiology and clinical characteristics of maternal hypothyroidism 2. Prevention and
Pathophysiology of Thyroid Disorders. PHCL 415 Hadeel Alkofide April 2010
 Pathophysiology of Thyroid Disorders PHCL 415 Hadeel Alkofide April 2010 1 Learning Objectives Understand the pathophysiology of hyperthyroidism & hypothyroidism Describe the signs & symptoms of hyperthyroidism
Pathophysiology of Thyroid Disorders PHCL 415 Hadeel Alkofide April 2010 1 Learning Objectives Understand the pathophysiology of hyperthyroidism & hypothyroidism Describe the signs & symptoms of hyperthyroidism
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
THYROID DISEASE AND TESTING. Jack L. Snitzer, D.O., FACOI, FACE, CCD
 THYROID DISEASE AND TESTING Jack L. Snitzer, D.O., FACOI, FACE, CCD MAPA MEETING 2018 JACK L. SNITZER, D.O. 410-572-8848 JACK.SNITZER@PENINSULA.ORG NO CONFLICTS OF INTEREST THYROID THYROID Goiter Hyperthyroidism
THYROID DISEASE AND TESTING Jack L. Snitzer, D.O., FACOI, FACE, CCD MAPA MEETING 2018 JACK L. SNITZER, D.O. 410-572-8848 JACK.SNITZER@PENINSULA.ORG NO CONFLICTS OF INTEREST THYROID THYROID Goiter Hyperthyroidism
Hyperthyroidism. Objectives. Clinical Manifestations. Slide 1. Slide 2. Slide 3. Implications for Primary Care. hyperthyroidism
 1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
19th Century Thyroidology
 1 19th Century Thyroidology Dr. Kinnicutt s patient (1893) A cold, tired, constipated middle aged woman Slow pulse rate Low body temperature From physiology it was likely patient needed thyroid replacement
1 19th Century Thyroidology Dr. Kinnicutt s patient (1893) A cold, tired, constipated middle aged woman Slow pulse rate Low body temperature From physiology it was likely patient needed thyroid replacement
Laboratory assessment of thyroid function. Nahid Shirazian MD. Internist, Endocrinologist
 Laboratory assessment of thyroid function Nahid Shirazian MD. Internist, Endocrinologist Physiology Thyroid gland produces Thyroxine Converted to active form T3 in tissue Scattered dc cells within ihi
Laboratory assessment of thyroid function Nahid Shirazian MD. Internist, Endocrinologist Physiology Thyroid gland produces Thyroxine Converted to active form T3 in tissue Scattered dc cells within ihi
Management of Common Thyroid Disorders
 Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Hypothyroidism. Causes. Diagnosis. Christopher Theberge
 Hypothyroidism Pronunciations: (Hypothyroidism) Hypothyroidism (under active thyroid) is a condition where the thyroid gland fails to secrete enough of the thyroid hormones thyroxine (T4) and triiodothyronine
Hypothyroidism Pronunciations: (Hypothyroidism) Hypothyroidism (under active thyroid) is a condition where the thyroid gland fails to secrete enough of the thyroid hormones thyroxine (T4) and triiodothyronine
4) Thyroid Gland Defects - Dr. Tara
 Thyroid Gland Defects - Dr. Tara") 4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
PRESCRIBING INFORMATION THYROID. Desiccated Thyroid 30, 60, 125 mg Tablets. Hypothyroidism Therapy
 PRESCRIBING INFORMATION THYROID Desiccated Thyroid 30, 60, 125 mg Tablets Hypothyroidism Therapy 8250 Décarie Blvd, suite 110 Montréal, QC Canada, H4P 2P5 Date of preparation: 17-May-2000 Date of Revision:
PRESCRIBING INFORMATION THYROID Desiccated Thyroid 30, 60, 125 mg Tablets Hypothyroidism Therapy 8250 Décarie Blvd, suite 110 Montréal, QC Canada, H4P 2P5 Date of preparation: 17-May-2000 Date of Revision:
What to do when the furnace breaks? Addressing hypothyroidism in children
 What to do when the furnace breaks? Addressing hypothyroidism in children M. Tracy Bekx, MD Associate Professor of Pediatrics University of Wisconsin-Madison American Family Children s Hospital Disclosure
What to do when the furnace breaks? Addressing hypothyroidism in children M. Tracy Bekx, MD Associate Professor of Pediatrics University of Wisconsin-Madison American Family Children s Hospital Disclosure
THYROID DISEASE IN PREGNANCY
 THYROID DISEASE IN PREGNANCY https://www.wddty.com/magazine/2016/june/depression-its-not-your-brain-its-your-thyroid.html Grand Rounds December 5, 2018 Maria Kolojeski, DO (PGY3) REVIEW OF THYROID HORMONES
THYROID DISEASE IN PREGNANCY https://www.wddty.com/magazine/2016/june/depression-its-not-your-brain-its-your-thyroid.html Grand Rounds December 5, 2018 Maria Kolojeski, DO (PGY3) REVIEW OF THYROID HORMONES
The Thyroid and Pregnancy OUTLINE OF DISCUSSION 3/19/10. Francis S. Greenspan March 19, Normal Physiology. 2.
 The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
Thyroid hormones derived from two iodinated tyrosine molecules
 Thyroid Hormones OBJECTIVES Chemical nature of the thyroid hormones How different enzymes play a role in thyroid hormone formation? And what drugs affect them? Describe Function & Metabolism of thyroid
Thyroid Hormones OBJECTIVES Chemical nature of the thyroid hormones How different enzymes play a role in thyroid hormone formation? And what drugs affect them? Describe Function & Metabolism of thyroid
Thyroid gland defects. Dr. Tara Husain
 Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
Thyroid Disorders Towards a Healthy Endocrine System
 Thyroid Disorders Towards a Healthy Endocrine System What are Thyroid Disorders? The thyroid is a butterfly-shaped gland in the middle of the lower neck. Through the release of hormones, the thyroid regulates
Thyroid Disorders Towards a Healthy Endocrine System What are Thyroid Disorders? The thyroid is a butterfly-shaped gland in the middle of the lower neck. Through the release of hormones, the thyroid regulates
Critical illness and endocrinology. ICU Fellowship Training Radboudumc
 Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
Critical illness and endocrinology ICU Fellowship Training Radboudumc Critical illness Ultimate form of severe physical stress Generates an orchestrated endocrine response to provide the energy for fight
BELIEVE MIDWIFERY SERVICES
 TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
The Effects of Anesthesia and Surgery on Thyroid Function Tests in Dogs. Melinda A. Wood ABSTRACT
 The Effects of Anesthesia and Surgery on Thyroid Function Tests in Dogs Melinda A. Wood ABSTRACT Background: Many non-thyroidal factors affect thyroid function tests. Anesthesia and surgery have been documented
The Effects of Anesthesia and Surgery on Thyroid Function Tests in Dogs Melinda A. Wood ABSTRACT Background: Many non-thyroidal factors affect thyroid function tests. Anesthesia and surgery have been documented
Grave s disease (1 0 )
") THYROID DYSFUNCTION Grave s disease (1 0 ) Autoimmune - activating AB s to TSH receptor High concentrations of circulating thyroid hormones Weight loss, tachycardia, tiredness Diffuse goitre - TSH stimulating
THYROID DYSFUNCTION Grave s disease (1 0 ) Autoimmune - activating AB s to TSH receptor High concentrations of circulating thyroid hormones Weight loss, tachycardia, tiredness Diffuse goitre - TSH stimulating
Southern Derbyshire Shared Care Pathology Guidelines. Hypothyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Hypothyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hypothyroidism in adults. Background Hypothyroidism
Southern Derbyshire Shared Care Pathology Guidelines Hypothyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hypothyroidism in adults. Background Hypothyroidism
Update on Gestational Thyroid Disease. Aidan McElduff The Discipline of Medicine, The University of Sydney
 IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
Effect of thyroid hormones of metabolism Thyroid Diseases
 Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
THYROID AWARENESS. By: Karen Carbone. January is thyroid awareness month. At least 30 million Americans
 THYROID AWARENESS By: Karen Carbone January is thyroid awareness month. At least 30 million Americans have a thyroid disorder and half-15 million-are silent sufferers who are undiagnosed, according to
THYROID AWARENESS By: Karen Carbone January is thyroid awareness month. At least 30 million Americans have a thyroid disorder and half-15 million-are silent sufferers who are undiagnosed, according to
university sciences of Isfahan university Com
 Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
OUTLINE. Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis
 THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
Subclinical Hypothyroidism
 Subclinical Hypothyroidism Key Clinical Points Subclinical hypothyroidism is defined as an elevated thyrotropin level with a normal free thyroxine (T 4 ) level. To confirm the diagnosis, a transient increase
Subclinical Hypothyroidism Key Clinical Points Subclinical hypothyroidism is defined as an elevated thyrotropin level with a normal free thyroxine (T 4 ) level. To confirm the diagnosis, a transient increase
Guidance for Thyroid Function Testing in Primary Care in Lothian
 Guidance for Thyroid Function Testing in Primary Care in Lothian In July 2006 following a lengthy consultation process, a joint working group comprising representatives from the Association of Clinical
Guidance for Thyroid Function Testing in Primary Care in Lothian In July 2006 following a lengthy consultation process, a joint working group comprising representatives from the Association of Clinical
Jim Paoletti BS Pharmacy, FAARM, FIACP, Director of Education, P2P
 presents A Pioneering Functional Technologies Approach For to Hypothyroidism Lifestyle Based Medicine Part 3 of 3 with Jim Paoletti BS Pharmacy, FAARM, FIACP, Director of Education, P2P Clinical Consultant
presents A Pioneering Functional Technologies Approach For to Hypothyroidism Lifestyle Based Medicine Part 3 of 3 with Jim Paoletti BS Pharmacy, FAARM, FIACP, Director of Education, P2P Clinical Consultant
Some Issues in the Management of Hypothyroidism
 Some Issues in the Management of Hypothyroidism Family Medicine Refresher Course April 6, 2016 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Some Issues in the Management of Hypothyroidism Family Medicine Refresher Course April 6, 2016 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Pregnancy & Thyroid. Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University. Imam Reza weeky Conferance
 Pregnancy & Thyroid Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University Imam Reza weeky Conferance Objectives Thyroid Disorders & Pregnancy Normal thyroid phsyiology
Pregnancy & Thyroid Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University Imam Reza weeky Conferance Objectives Thyroid Disorders & Pregnancy Normal thyroid phsyiology
Structural Formulas. Levothyroxine (T4) I
 I") Armour Thyroid (thyroid tablets, USP) Rx only Content Updated: June 2018 DESCRPTON Armour Thyroid (thyroid tablets, USP)* for oral use is a natural preparation derived from porcine thyroid glands and has
Armour Thyroid (thyroid tablets, USP) Rx only Content Updated: June 2018 DESCRPTON Armour Thyroid (thyroid tablets, USP)* for oral use is a natural preparation derived from porcine thyroid glands and has
THYROID FUNCTION TESTING
 THYROID FUNCTION TESTING ENDOCRINE UPDATES Shlomo Melmed, M.D., Series Editor For further volumes: http://www.springer.com/series/5917 THYROID FUNCTION TESTING Edited by Gregory A. Brent Professor of Medicine
THYROID FUNCTION TESTING ENDOCRINE UPDATES Shlomo Melmed, M.D., Series Editor For further volumes: http://www.springer.com/series/5917 THYROID FUNCTION TESTING Edited by Gregory A. Brent Professor of Medicine
Management of Common Thyroid Disorders
 Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures Cases 68 yr old woman with new atrial fibrillation and no other findings except TSH=0.04,
Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures Cases 68 yr old woman with new atrial fibrillation and no other findings except TSH=0.04,
THYROID DISEASE IN CHILDREN
 THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
Update In Hyperthyroidism
 Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Thyroid Function. Thyroid Antibodies. Analyte Information
 Thyroid Function Thyroid Antibodies Analyte Information - 1-2013-04-30 Thyroid Antibodies Determination of thyroid autoantibodies are, besides TSH and FT4, one of the most important diagnostic parameters.
Thyroid Function Thyroid Antibodies Analyte Information - 1-2013-04-30 Thyroid Antibodies Determination of thyroid autoantibodies are, besides TSH and FT4, one of the most important diagnostic parameters.
Common Causes of Hypothyroidism
 Common Causes of Hypothyroidism Autoimmune thyroidi4s Surgical removal of thyroid gland Medica4on Therapy Iodine and iodine containing medica4ons Neck radia4on Post Partum thyroidi4s Prevalence of Hypothyroidism
Common Causes of Hypothyroidism Autoimmune thyroidi4s Surgical removal of thyroid gland Medica4on Therapy Iodine and iodine containing medica4ons Neck radia4on Post Partum thyroidi4s Prevalence of Hypothyroidism
Limits of Liability/Disclaimer of Warranty
 Page 0 of 8 Limits of Liability/Disclaimer of Warranty The author, Brad Shook has made their best effort to produce a high quality and informative reference. The author makes no representation or warranties
Page 0 of 8 Limits of Liability/Disclaimer of Warranty The author, Brad Shook has made their best effort to produce a high quality and informative reference. The author makes no representation or warranties
An Approach to: Thyroid Function Tests. Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital
 An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
 Thyroid Hormones Exophthalmos GOITRE / GOITER Hyperthyroidism GOITRE / GOITER Endemic Goiter, a Hypertrophy of the Thyroid Gland Resulting from Iodine Deficiency ENDEMIC GOITRES: were common in Central
Thyroid Hormones Exophthalmos GOITRE / GOITER Hyperthyroidism GOITRE / GOITER Endemic Goiter, a Hypertrophy of the Thyroid Gland Resulting from Iodine Deficiency ENDEMIC GOITRES: were common in Central
Hypothalamic Control of Posterior Pituitary
 Hypothalamic Control of Posterior Pituitary Hypothalamus neuron cell bodies produce ADH: supraoptic nuclei Oxytocin: paraventricular nuclei Transported along the hypothalamohypophyseal tract Stored in
Hypothalamic Control of Posterior Pituitary Hypothalamus neuron cell bodies produce ADH: supraoptic nuclei Oxytocin: paraventricular nuclei Transported along the hypothalamohypophyseal tract Stored in
Psychiatric illness or thyroid disease? Richard A. Bermudes, MD
 Primary care update Psychiatric illness or thyroid disease? D on t be misled by false lab tests Richard A. Bermudes, MD Departments of family medicine and psychiatry University of Cincinnati College of
Primary care update Psychiatric illness or thyroid disease? D on t be misled by false lab tests Richard A. Bermudes, MD Departments of family medicine and psychiatry University of Cincinnati College of
Icd 10 low tsh level. Icd 10 low tsh level. Search
 Search Icd 10 low tsh level Icd 10 low tsh level 1-10-2012 The 2012 updates to the Current Procedural Terminology 4th Edition (CPT-4) and Healthcare Common Procedure Coding System (HCPCS) National Level
Search Icd 10 low tsh level Icd 10 low tsh level 1-10-2012 The 2012 updates to the Current Procedural Terminology 4th Edition (CPT-4) and Healthcare Common Procedure Coding System (HCPCS) National Level
NEWBORN FEMALE WITH GOITER PAYAL PATEL, M.D. PEDIATRIC ENDOCRINOLOGY FELLOW FEBRUARY 12, 2015
 NEWBORN FEMALE WITH GOITER PAYAL PATEL, M.D. PEDIATRIC ENDOCRINOLOGY FELLOW FEBRUARY 12, 2015 CHIEF COMPLAINT 35 6/7 week F with goiter, born to a mother with Graves disease (GD) HPI 35 6/7 week F born
NEWBORN FEMALE WITH GOITER PAYAL PATEL, M.D. PEDIATRIC ENDOCRINOLOGY FELLOW FEBRUARY 12, 2015 CHIEF COMPLAINT 35 6/7 week F with goiter, born to a mother with Graves disease (GD) HPI 35 6/7 week F born
Euthyroid sick syndrome
 Euthyroid sick syndrome Background Euthyroid sick syndrome can be described as abnormal findings on thyroid function tests that occur in the setting of a nonthyroidal illness (NTI) without preexisting
Euthyroid sick syndrome Background Euthyroid sick syndrome can be described as abnormal findings on thyroid function tests that occur in the setting of a nonthyroidal illness (NTI) without preexisting
Thyroid Disease. Scott D. Isaacs, MD, FACP, FACE HRT Symposium Savannah GA July 14 16, All Rights Reserved. 1
 Thyroid Disease Scott D. Isaacs, MD, FACP, FACE HRT Symposium Savannah GA July 14 16, 2016 2016. All Rights Reserved. 1 Disclosure Scott D. Isaacs, MD, FACP, FACE, is the Medical Director at Atlanta Center
Thyroid Disease Scott D. Isaacs, MD, FACP, FACE HRT Symposium Savannah GA July 14 16, 2016 2016. All Rights Reserved. 1 Disclosure Scott D. Isaacs, MD, FACP, FACE, is the Medical Director at Atlanta Center