Most common type of thyroid malignancy-85% of thyroid cancers Most common endocrine malignancy
|
|
|
- Andrea Rogers
- 6 years ago
- Views:
Transcription
1 THE DIAGNOSIS OF PAPILLARY THYROID : How much (or how little) is enough? Virginia A. LiVolsi, MD University of Pennsylvania
2 Most common type of thyroid malignancy-85% of thyroid cancers Most common endocrine malignancy
3 Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis 95% at 25 years
4 Gross Any size Confined or extrathyroidal May show capsule (especially follicular variant) May be cystic May note gross calcification or even bone
5
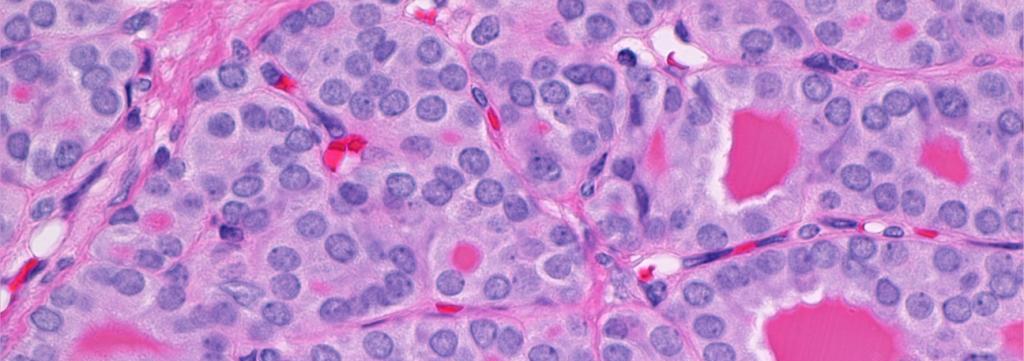
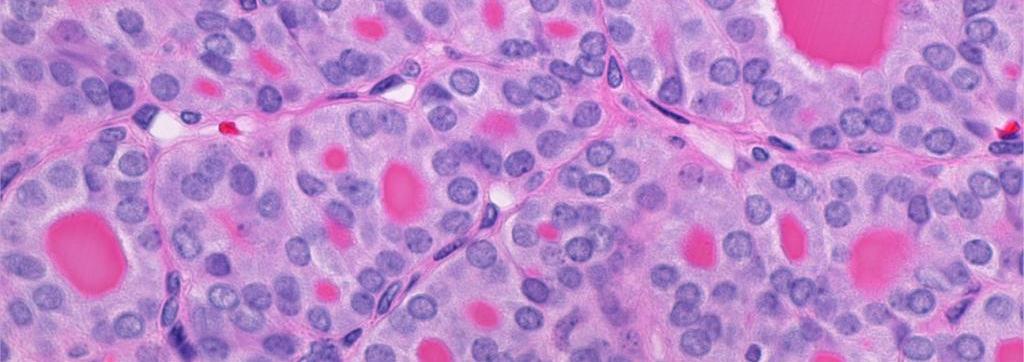
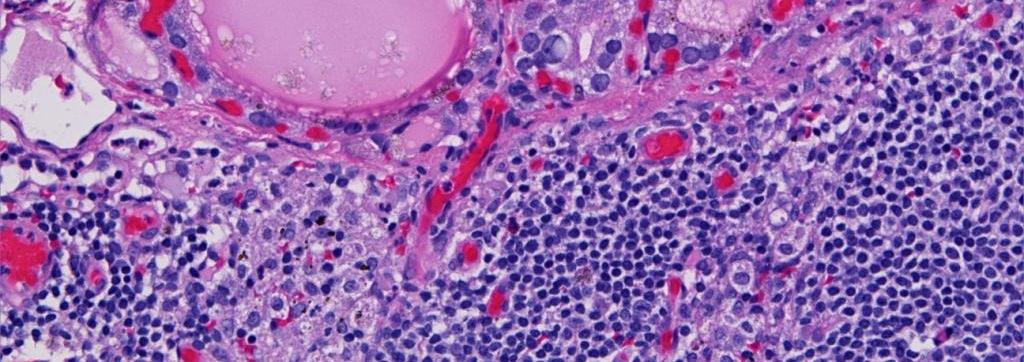
6 Pathology Papillae and/or follicles Can be totally follicular Sclerosis Calcification (psammoma bodies) NUCLEI
7
8
9 Psammoma bodies GHOSTS of dead Papillae In stroma or lymphatics Importance in lymph nodes
10 PATHOLOGY Lymphatic invasion early on May show vascular invasion also Lymph nodes positive over 50% at diagnosis May present as nodal metastasis in neck especially cystic (confused with branchial cleft cyst)
11
12 The characteristic morphologic feature was historically : PAPILLAE In older literature, if greater than 50% of a tumor was follicular in pattern, it was classified as either: MIXED PAPILLARY-FOLLICULAR CA OR FOLLICULAR CA
13
14 In 1960s, some authors (notably Stuart Lindsay) began to pay attention to the nuclear features. Hence over time, the nuclear morphology became the most overriding diagnostic consideration. It no longer mattered how much of the tumor was papillary or even if all of it was follicular in pattern.
15
16
17 In 1977, Chen and Rosai described the FOLLICULAR VARIANT OF PAPILLARY Over 30 years we have witnessed debate and dispute about this tumor; panels of experts have been shown to have wide diagnostic variations ranging from adenoma to carcinoma.
18
19 WHAT ARE THE QUESTIONS TODAY? MORE IMPORTANTLY WHAT ARE THE ANSWERS?
20 If we rely solely on nuclear criteria, then many lesions would be considered FVPTC SUCH AS: Chronic sialadenitis, chronic endometritis, etc.
21 THE NUCLEI Elongated Enlarged Cleared out center Thick nuclear membrane Grooves Inclusions Tiny nucleoli




22
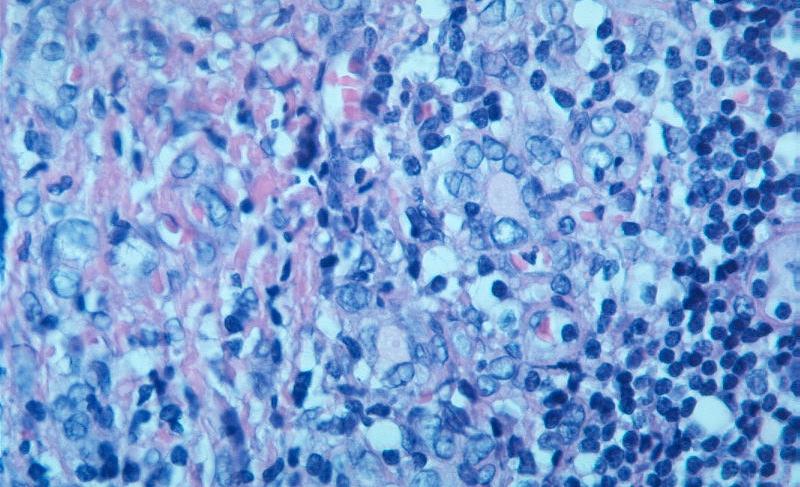
23 In the thyroid the nuclei that are excellent mimics of the PTC nuclei include those in: Hashimoto thyroiditis Graves disease Some nodular goiters

24
25 So perhaps the nuclei alone are not enough. I personally require the nuclei be present in a mass lesion. This is especially true in Hashimoto disease.
26 I do not believe that one can have a diffuse papillary cancer of the thyroid. In some Hashimoto or Graves glands, every follicular epithelial cell had a nucleus with features of PTC. THIS IS NOT CANCER.
27 From molecular analysis it has been shown that in Hashimoto disease 1. Areas of epithelium with abnormal nuclei show LOH and 2. Low levels of ret/ptc translocation 3. But almost no cases of Braf mutations.
28 So the question raised is Is the epithelium in Hashimoto disease DYSPLASTIC, PRENEOPLASTIC?
29 From an epidemiologic and clinical viewpoint, the incidence of clinical papillary carcinoma in Hashimoto disease appears slightly increased over background BUT The frequency of microptc is really elevated.
30 The problems with these data are myriad but a few are: The definition (clinically, serologically and histopathologically) of Hashimoto thyroiditis. The definition of the background population. Most patients with thyroiditis do not have surgery (if there is no nodule) so it impossible to know the true incidence of cancer (microptc).
31 Data for Graves disease are even sparser, since it is unusual to have surgery for this disorder. Clinical cancer in Graves disease is unusual.
32 NOW Let us turn attention to nodules (mass lesions). We consider mass lesions as any size nodule that appears at low power magnification as a lesion and different from whatever is going on in the diffuse background disease.
33 If such a nodule has a papillary architecture and nuclei as previously defined, it is papillary cancer no matter what its size. If such a nodule has a totally follicular architecture and nuclei as previously defined, is it papillary cancer? MY ANSWER IS YES.
34 We need to recognize that there are different patterns of the FOLLICULAR VARIANT OF PAPILLARY
35 FOLLICULAR VARIANT OF PAPILLARY The easiest to recognize is the infiltrative pattern.
36 TYPE PAPILLARY THYROID, FOLLICULAR VARIANT Dx: CANCER Dx: OTHER Infiltrative YES Encapsulated; invasive; nuclei diffuse or multifocal Encapsulated; diffuse nuclei Encapsulated; multifocal nuclei or equivocal nuclei Encapsulated; one focus nuclei YES Most YES Few YES Many microptc in adenoma WHY? Atypical adenoma; UMP Many atypical adenoma; few UMP Many just adenoma
37
38 ENCAPSULATED FVPTC FVPTC FVPTC WITH CAP & VAS INV (Per Baloch ZW) FVPTC PTC MCA IN ADENOMA
39 THE NUCLEI Elongated Enlarged Cleared out center Thick nuclear membrane Grooves Inclusions Tiny nucleoli
40 BACK TO THE NUCLEI My reasoning for considering encapsulated follicular tumors with multifocal nuclei as FVPTC Sometimes in node and/or bone metastases, the nuclei look normal and not like PTC nuclei, yet these are metastases. Thus, if can happen in mets, why not in the primary site?
41
42 , FOLLICULAR VARIANT A little Molecular data. The follicular variant (the encapsulated varieties) tend to fall somewhere in between classic papillary carcinoma and classic follicular carcinoma Thus they have less ret/ptc rearrangements, rarely Braf mutations ( as does classic PTC) and more ras mutations (similar to follicular carcinoma).
43 , FOLLICULAR VARIANT A little Clinicopathologic data. The follicular variant (the encapsulated varieties) tend to show fewer nodal metastases (about 20-25%) 25%) than classical PTC. They show more bony metastases and often have vascular invasion in the primary.
44 BACK TO THE NUCLEI NOW FOR THE CYTOPATHOLOGIST WHY IS IT SO DIFFICULT TO DIAGNOSE FOLLICULAR VARIANT PTC ON FNA?
45 NOW FOR THE CYTOPATHOLOGIST WHY IS IT SO DIFFICULT TO DIAGNOSE FOLLICULAR VARIANT PTC ON FNA? I think it is because although the nuclei are enlarged oval and have grooves, they rarely show intranuclear inclusions and so the FNA diagnosis is often suspicious but not definitive.
46 FOLLICULAR VARIANT Sometimes there are undercalls Best nuclei tend to be under capsule of lesion, not usually sampled by the FNA (tends to sample center where nuclei may not be well developed).
47 NOW BACK TO THE CYTOPATHOLOGIST Sometimes there are overcalls although these are rare. Grooves can be seen in other nuclei in the thyroid. One can get squamous metaplasia (spontaneous) in benign conditions and this can be overdiagnosed.
48 NOW FOR THE CYTOPATHOLOGIST There is a possible marker that may be useful EMERIN As shown by Bussolati s group this marker shows nuclear irregularities in histological and cytological preps of papillary carcinoma but not in nonptc lesions. HISTOPATH April 2009
49 NOW FOR THE CYTOPATHOLOGIST Sometimes there are overcalls although these are rare. Beware of oncocytic cells which can be large and have nuclear grooves, especially in hyperfunctioning glands and nodules. If the nucleus has a nucleolus and/or is round, do not make a diagnosis of PTC.
50 THE DIAGNOSIS OF PAPILLARY THYROID : How much (or how little) is enough? Virginia A. LiVolsi, MD University of Pennsylvania
51 THE DIAGNOSIS OF PAPILLARY THYROID : HOW MUCH OR HOW LITTLE IS ENOUGH? Virginia A. LiVolsi, MD. University of Pennsylvania Department of Pathology and Laboratory Medicine Philadelphia, Pennsylvania Address for Correspondence: Virginia A. LiVolsi, M.D. University of Pennsylvania Department of Pathology and Laboratory Medicine 3400 Spruce Street, Sixth Floor, Founders Pavillion Philadelphia, Pennsylvania Joint ASC-PAP Society Meeting, USCAP, Washington, DC 2010 SALIENT POINTS At the conclusion of this lecture, the members of the audience should: 1. Understand the subtypes of follicular variant of papillary carcinoma (currently a controversial diagnosis). 2. Recognize that certain benign reactive conditions can demonstrate nuclear changes that simulate papillary cancer nuclei. 3. Learn the diagnostic clues that are helpful in dividing these lesions into clinically relevant entities. 4. Appreciate the applications of the diagnostic criteria to the cytological diagnosis of papillary thyroid carcinoma. Keywords: Papillary thyroid carcinoma, follicular variant, nuclear features, diagnostic criteria
52 The entity of follicular variant of papillary thyroid carcinoma (FVPC) which had been recognized in the 1960s by Lindsay 1 was elegantly defined in 1977 by Chen and Rosai.. Until that time, most textbooks and review articles on the pathology of papillary thyroid carcinoma (PTC) classified follicular patterned thyroid tumors as follicular carcinoma without reference to nuclear features or growth pattern. 3 In a short time, the pathology community noticed the importance of nuclear characteristics in the classification of, and biological behavior of well differentiated thyroid carcinoma. The AFIP fascicle and the WHO defined lesions as papillary carcinoma solely on the basis of peculiar nuclear morphology without regard to architectural growth, i.e. whether or not papillary structures were present. Over the past 30 years, many follicular patterned tumors of the thyroid were diagnosed as papillary carcinoma based on these nuclear features (enlargement, elongation (oval rather than rounded shape), nuclear clearing, intranuclear grooves and inclusions, and small nucleoli with thickened nuclear membranes). Lesions which were infiltrative and those which were partially or completely encapsulated were included in this category. Problems arose in the diagnosis of completely en capsulated tumors since even so-called experts in endocrine pathology showed very poor agreement among themselves in defining the nuclei of papillary carcinoma. Lloyd et al evaluated interobserver variability in the diagnosis of FVPC; 87 cases were reviewed 10 experienced endocrine pathologists. The cohort included cases with one or more diagnostic nuclear features of papillary carcinoma and some with capsular (67%) and vascular invasion (5.7%). A concordant diagnosis of FVPCA was made by all 10 reviewers with a cumulative frequency of 39%. In this series, 24.1% of the patients had metastatic disease, in this group a diagnosis of FVPCA was made by all 10 reviewers with a cumulative frequency of 66.7%, and 7 of the reviewers made a diagnosis of FVPCA with a cumulative frequency of 100%. Hirokawa et al submitted 21 encapsulated follicular patterned thyroid lesions to four American and four Japanese pathologists for expert review. There was unanimous agreement among all pathologists in 2 (10%) cases, 7 of 8 pathologists agreed in 29% and 6 of 8 pathologists in 76% of cases. All pathologists, however, agreed on the diagnosis of benign vs. malignant lesion in 13(62%) of 21 cases. Interestingly, the American pathologists frequently made the diagnosis FVPC as compared to Japanese pathologists (25% vs. 4%). 9 Elsheikh et al assessed inter and intra-observer agreement among 6 thyroid experts by using 15 cases in which the original pathologists considered the differential diagnosis of FVPC vs. follicular adenoma (FA). There was complete agreement in the diagnosis of FVPC in 2 (13%), complete agreement on benign and malignant diagnoses in 4 (27%) and majority agreement in 8 (53%) cases. Several authors agree that this variability in the diagnosis of FVPC is due to the lack of agreement on the minimal diagnostic criteria. The diagnosis of papillary cancer is established by examining the nucleus. Most often the cytopathologists will not render the diagnosis of papillary carcinoma in thyroid fine needle aspiration specimens until all
53 major diagnostic features are evident. Any specimens which fell short of this are diagnosed as suspicious for papillary carcinoma. Numerous studies have shown that that rate of malignancy in cases diagnosed as such is 60-75% and interestingly most cases on histologic examination are found to FVPC. Verhulst et al employed a scoring system for the diagnosis of PTC. In this study the 132 thyroid tumors (66 PTC and 66 follicular adenoma) were used as a training set to establish the scoring system which was tested on a validation set of 58 thyroid tumors (29 PTC and 29 FNA) to assess its efficacy in the diagnosis of PTC. Theses authors found that the microscopic criteria for PTC were highly variable among cases and ranged from 0% to 75%, nuclear enlargement was the only feature that was present in 75% of the tumor cells in 94% of cases. Interestingly, in the validation part of the study eight cases of PTC majority of which were follicular patterned were in gray zone i.e. at or below the threshold score for the diagnosis of PTC. The hope for a marker that may help define the nuclei of papillary carcinoma remains to be fulfilled. At least one marker may show some promise but more work needs to be done to confirm it. The group from the University of Turino has studied Emerin a nuclear membrane component and found that immunohistochemical staining shows differences between papillary carcinomas and benign mimics, normal thyroid and nonmalignant lesions. The staining is applicable to both cytologic and histologic preparations. The considerable inter and intra-observer variability in the diagnosis of FVPC which often creates treatment dilemmas among clinicians i.e. whether to treat or not i.e. completion thyroidectomy (in cases where lobectomy is done as the initial procedure) and/or radioiodine ablation. The result of this confusion is that many cases of FVPC (especially encapsulated lesions) are sent to thyroid pathology experts for second opinion Due to this controversy the Chernobyl Pathologist group have proposed the term well-differentiated thyroid tumor of uncertain malignant potential for encapsulated follicular patterned tumor that only shows some or unconvincing features of PTC. We recognize that the follicular variant of papillary carcinoma represents a heterogeneous group of tumors due to its variable growth patterns (architectural) and distribution of nuclear features of papillary carcinoma. The un-encapsulated invasive tumor is a lesion which grows in an infiltrative pattern and is without question therefore a carcinoma. In its growth pattern resembles classical papillary carcinoma. However, the lesion demonstrates no papillae and is composed exclusively of follicles. The nuclei throughout the lesion are the characteristic nuclei of papillary carcinoma. These lesions may show lymphatic invasion, multifocal growth within the thyroid, and on occasion psammoma bodies; lymph node metastases are not unusual and may even demonstrate papillary growth. These cases do not usually produce difficulties in diagnosis The encapsulated tumor represents the group that may cause diagnostic disagreements. In encapsulated tumors which show invasion of the tumor capsule or capsular blood vessels, most pathologists will consider these cancers; the diagnostic issue is whether these should be classified as follicular or papillary carcinoma. We consider these papillary carcinomas if the nuclear features are present, whether these are diffuse throughout the tumor or are present in multiple locations within the neoplasm. The encapsulated FVPC without invasion and showing diffuse nuclear changes of PTC will
54 be classified by many experienced pathologists as FVPTC; however, problems exist in those encapsulated noninvasive lesions with multifocal nuclear change but in which the nuclei do not show all of the characteristic features listed above of papillary cancer i.e. unconvincing.. Most often, there are few if any nuclear inclusions. Finally there are lesions that contain a sub-centimeter area of follicles with papillary nuclei that if present in the normal thyroid would be diagnosed as a papillary microcarcinoma; such rare lesions should be diagnosed as papillary microcarcinoma arising in and confined within a follicular adenoma. These have the biologic characteristics and probably better clinical outlook than identical lesions of intraglandular incidentally found microcarcinoma; i.e., very small to almost nonexistent risk of metastatic potential.
55 REFERENCES 1. Lindsay S. Carcinoma of the thyroid gland: a clinical and pathologic study of 239 patients at the University of California Hospital. Sprigfield, IL; Chen KT, Rosai J. Follicular variant of thyroid papillary carcinoma: a clinicopathologic study of six cases. Am J Surg Pathol. 1977;1: Meissner WA. Follicular carcinoma of the thyroid; frozen section diagnosis. Am J Surg Pathol. 1977;1: DeLellis RA, Lloyd RD, Heitz PU, Eng C, eds. WHO: Pathology and Genetics. Tumours of Endocrine Organs. Lyon, France: IARC Press; Rosai J, Carcangui ML, DeLellis RA. Tumors of The Thyroid Gland. 3rd Series, Fascicle 5 vol. Washington, DC: Armed Forces Institute of Pathology; LiVolsi VA. Surgical Pathology of The Thyroid. Philadelphia, PA: WB. Saunders; LiVolsi VA, Asa SL. The demise of follicular carcinoma of the thyroid gland. Thyroid. 1994;4: Lloyd RV, Erickson LA, Casey MB et al. Observer variation in the diagnosis of follicular variant of papillary thyroid carcinoma. Am J Surg Pathol. 2004;28: Hirokawa M, Carney JA, Goellner JR et al. Observer variation of encapsulated follicular lesions of the thyroid gland. Am J Surg Pathol. 2002;26: Renshaw AA, Gould EW. Why there is tendency to "overdiagnose" the follicular variant of papillary thyroid carcinoma. Am J Clin Pathol. 2002;117: Chan JK. Strict criteria should be applied in the diagnosis of encapsulated follicular variant of papillary thyroid carcinoma. Am J Clin Pathol. 2002;117: Baloch ZW, Livolsi VA. Follicular-patterned lesions of the thyroid: the bane of the pathologist. Am J Clin Pathol. 2002;117: Elsheikh TM, Asa SL, Chan JK et al. Interobserver and intraobserver variation among experts in the diagnosis of thyroid follicular lesions with borderline nuclear features of papillary carcinoma. Am J Clin Pathol. 2008;130: Logani S, Gupta PK, LiVolsi VA, Mandel S, Baloch ZW. Thyroid nodules with FNA cytology suspicious for follicular variant of papillary thyroid carcinoma: follow-up and management. Diagn Cytopathol. 2000;23:380-5.
56 15. Zacks JF, de las Morenas A, Beazley RM, O'Brien MJ. Fine-needle aspiration cytology diagnosis of colloid nodule versus follicular variant of papillary carcinoma of the thyroid. Diagn Cytopathol. 1998;18: Baloch ZW, Livolsi VA, Asa SL et al. Diagnostic terminology and morphologic criteria for cytologic diagnosis of thyroid lesions: A synopsis of the National Cancer Institute Thyroid Fine-Needle Aspiration State of the Science Conference. Diagn Cytopathol. 2008;36: Verhulst P, Devos P, Aubert S et al. A score based on microscopic criteria proposed for analysis of papillary carcinoma of the thyroid. Virchows Arch. 2008;452: Baloch ZW, LiVolsi VA. Our approach to follicular-patterned lesions of the thyroid. J Clin Pathol. 2007;60: Williams ED, Abrosimov A, Bogdanova TI, Roasi J, Sidorov Y, Thomas GA. Two proposals regarding the terminology of thyroid tumors. Guest Editorial. Int J Surg Pathol. 2000;8: Baloch ZW, LiVolsi VA. Pathologic diagnosis of papillary thyroid carcinoma: today and tomorrow. Expert Rev Mol Diagn. 2005;5: Kaur A, Jayaram G. Thyroid tumors: cytomorphology of follicular neoplasms. Diagnostic Cytopathology. 1991;7: Baloch ZW, Fleisher S, LiVolsi VA, Gupta PK. Diagnosis of "follicular neoplasm": A gray zone in thyroid fine-needle aspiration cytology. Diagn Cytopathol. 2002;26: LiVolsi VA, Baloch ZW. Follicular neoplasms of the thyroid: view, biases, and experiences. Adv Anat Pathol. 2004;11: Nayar R, Ivanovic M. The indeterminate thyroid fine-needle aspiration: experience from an academic center using terminology similar to that proposed in the 2007 National Cancer Institute Thyroid Fine Needle Aspiration State of the Science Conference. Cancer Cytopathol. 2009;117: Rivera M, Tuttle RM, Patel S, Shaha A, Shah JP, Ghossein RA. Encapsulated papillary thyroid carcinoma: a clinico-pathologic study of 106 cases with emphasis on its morphologic subtypes (histologic growth pattern). Thyroid. 2009;19: Baloch ZW, LiVolsi VA. Encapsulated follicular variant of papillary thyroid carcinoma with bone metastases. Mod Pathol. 2000;13:
57 27. Mizukami Y, Nonomura A, Hayashi Y, et.al. Late bone metastasis from an encapsulated follicular carcinoma of the thyroid without capsular and vascular invasion. Pathol Internat. 1996;46: Goldstein NS, Czako P, Neill JS. Metastatic minimally invasive (encapsulated) follicular and Hurthle cell thyroid carcinoma: a study of 34 patients. Modern Pathology. 2000;13: Hunt JL, Dacic S, Barnes EL, Bures JC. Encapsulated follicular variant of papillary thyroid carcinoma. Am J Clin Pathol. 2002;118:602-3; author reply Giordano TJ, Kuick R, Thomas DG et al. Molecular classification of papillary thyroid carcinoma: distinct BRAF, RAS, and RET/PTC mutation-specific gene expression profiles discovered by DNA microarray analysis. Oncogene. 2005;24: Nikiforov YE, Nikiforova MN, Gnepp DR, Fagin JA. Prevalence of mutations of ras and p53 in benign and malignant thyroid tumors from children exposed to radiation after the Chernobyl nuclear accident. Oncogene. 1996;13: Zhu Z, Gandhi M, Nikiforova MN, Fischer AH, Nikiforov YE. Molecular profile and clinical-pathologic features of the follicular variant of papillary thyroid carcinoma. An unusually high prevalence of ras mutations. Am J Clin Pathol. 2003;120: Pizzolanti G, Russo L, Richiusa P et al. Fine-needle aspiration molecular analysis for the diagnosis of papillary thyroid carcinoma through BRAF V600E mutation and RET/PTC rearrangement. Thyroid. 2007;17: Nikiforov YE, Steward DL, Robinson-Smith TM et al. Molecular testing for mutations in improving the fine-needle aspiration diagnosis of thyroid nodules. J Clin Endocrinol Metab. 2009;94: Asioli S, Bussolati G. Emerin immunohistochemistry reveals diagnostic features of nuclear membrane arrangement in thyroid lesions.histopathology;54:571-9, LiVolsi VA and Baloch ZW. The many faces of follicular variant of papillary thyroid carcinoma. Path Case Rev 2010 (in press).
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Pathology of the Thyroid
 Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Pathology of the Thyroid Thyroid Carcinoma Arising from Follicular Cells 2015-01-19 Prof. Dr. med. Katharina Glatz Pathologie Carcinomas Arising from Follicular Cells Differentiated Carcinoma Papillary
Follicular Derived Thyroid Tumors
 Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
Follicular Derived Thyroid Tumors Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for Medical Sciences
THE FOLLICULAR VARIANT OF PAPILLARY THYROID CARCINOMA AND NIFTP
 THE FOLLICULAR VARIANT OF PAPILLARY THYROID CARCINOMA AND NIFTP FOLLICULAR VARIANT OF PAPILLARY CARCINOMA HISTORICAL PERSPECTIVE FOLLICULAR VARIANT OF PAPILLARY CARCINOMA 1960 described by Dr. Stuart Lindsay
THE FOLLICULAR VARIANT OF PAPILLARY THYROID CARCINOMA AND NIFTP FOLLICULAR VARIANT OF PAPILLARY CARCINOMA HISTORICAL PERSPECTIVE FOLLICULAR VARIANT OF PAPILLARY CARCINOMA 1960 described by Dr. Stuart Lindsay
DIAGNOSIS AND REPORTING OF FOLLICULAR-PATTERNED THYROID LESIONS BY FINE NEEDLE ASPIRATION
 Follicular-patterned thyroid lesions, WC Faquin 1 DIAGNOSIS AND REPORTING OF FOLLICULAR-PATTERNED THYROID LESIONS BY FINE NEEDLE ASPIRATION William C. Faquin, M.D., Ph.D Department of Pathology, Massachusetts
Follicular-patterned thyroid lesions, WC Faquin 1 DIAGNOSIS AND REPORTING OF FOLLICULAR-PATTERNED THYROID LESIONS BY FINE NEEDLE ASPIRATION William C. Faquin, M.D., Ph.D Department of Pathology, Massachusetts
Accepted 18 December 2009 Published online 25 May 2010 in Wiley Online Library (wileyonlinelibrary.com). DOI: /hed.21373
. DOI: /hed.21373") ORIGINAL ARTICLE DIMINISHING DIAGNOSIS OF FOLLICULAR THYROID CARCINOMA Kristen J. Otto, MD, 1 Jacqueline S. C. Lam, MBBS, 2 Christina MacMillan, MD, 3 Jeremy L. Freeman, MD, FRCSC 2 1 Department of Otolaryngology
ORIGINAL ARTICLE DIMINISHING DIAGNOSIS OF FOLLICULAR THYROID CARCINOMA Kristen J. Otto, MD, 1 Jacqueline S. C. Lam, MBBS, 2 Christina MacMillan, MD, 3 Jeremy L. Freeman, MD, FRCSC 2 1 Department of Otolaryngology
Thyroid Pathology: It starts and ends with the gross. Causes of Thyrophobia. Agenda. Diagnostic ambiguity. Treatment/prognosis disconnect
 Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Pathology: It starts and ends with the gross Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University of Arkansas for
Thyroid Cytopathology: Weighing In The Bethesda System
 Thyroid Cytopathology: Weighing In The Bethesda System V8 Conflicts No financial consideration Bias Work in the Canadian environment where litigation is less Thyroid cytology is often referred in by small
Thyroid Cytopathology: Weighing In The Bethesda System V8 Conflicts No financial consideration Bias Work in the Canadian environment where litigation is less Thyroid cytology is often referred in by small
04/09/2018. Follicular Thyroid Tumors Updates in Classification & Practical Tips. Dissecting Indeterminants. In pursuit of the low grade malignancy
 Follicular Thyroid Tumors Updates in Classification & Practical Tips Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Follicular Thyroid Tumors Updates in Classification & Practical Tips Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
CN 925/15 History. Microscopic Findings
 CN 925/15 History 78 year old female. FNA indeterminate lesion right thyroid lobe. Previous THY1C (UK) Bethesda category 1 cyst fluid. Ultrasound showed part solid/cystic changes, indeterminate in nature
CN 925/15 History 78 year old female. FNA indeterminate lesion right thyroid lobe. Previous THY1C (UK) Bethesda category 1 cyst fluid. Ultrasound showed part solid/cystic changes, indeterminate in nature
NIFTP: Histopathology of a Cytological Monkey Wrench. B. Wehrli
 NIFTP: Histopathology of a Cytological Monkey Wrench B. Wehrli Non-Invasive Encapsulated Follicular Variant of Papillary Thyroid Carcinoma Before 2016 Non-Invasive Follicular Thyroid Neoplasm with Papillary-Like
NIFTP: Histopathology of a Cytological Monkey Wrench B. Wehrli Non-Invasive Encapsulated Follicular Variant of Papillary Thyroid Carcinoma Before 2016 Non-Invasive Follicular Thyroid Neoplasm with Papillary-Like
ACCME/Disclosures. Questions to Myself? 4/11/2016
 The New Diagnostic Paradigms in Thyroid Surgical Pathology and Affects on Reporting of Thyroid Fine-Needle Aspiration Specimens Deliberations, Criticisms & Discussions Zubair W. Baloch, MD, PhD. Professor
The New Diagnostic Paradigms in Thyroid Surgical Pathology and Affects on Reporting of Thyroid Fine-Needle Aspiration Specimens Deliberations, Criticisms & Discussions Zubair W. Baloch, MD, PhD. Professor
An Alphabet Soup of Thyroid Neoplasms
 Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
Overall Objectives An Alphabet Soup of Thyroid Neoplasms Lester D. R. Thompson www.lester-thompson.com What is the current management of papillary carcinoma? What are the trends and what can we do differently?
The Korean Journal of Cytopathology 15(1) : 60-64, 2004
 : 60-64, 2004") 15 1 The Korean Journal of Cytopathology 15(1) : 60-64, 2004 : INTRODUCTION Papillary carcinoma of the thyroid gland has for long been traditionally diagnosed on the basis of the characteristic papillary
15 1 The Korean Journal of Cytopathology 15(1) : 60-64, 2004 : INTRODUCTION Papillary carcinoma of the thyroid gland has for long been traditionally diagnosed on the basis of the characteristic papillary
Let s Make Sense of Present & Predict Future. In Light of Past 1/12/2016
 The New Diagnostic Paradigms in Thyroid Surgical Pathology and Affects on Reporting of Thyroid Fine Needle Aspiration Specimens Deliberations, Criticisms & Discussions Zubair W. Baloch, MD, PhD. Professor
The New Diagnostic Paradigms in Thyroid Surgical Pathology and Affects on Reporting of Thyroid Fine Needle Aspiration Specimens Deliberations, Criticisms & Discussions Zubair W. Baloch, MD, PhD. Professor
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS
 Shamlal Mangray, MB, BS") Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Thyroid Nodules: Understanding FNA Cytology (The Bethesda System for Reporting of Thyroid Cytopathology) Shamlal Mangray, MB, BS Attending Pathologist Rhode Island Hospital, Providence, RI DISCLOSURE:
Dilemmas in Cytopathology and Histopathology
 Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
Dilemmas in Cytopathology and Histopathology Yuri E. Nikiforov, MD, PhD Division of Molecular & Genomic Pathology University of Pittsburgh Medical Center, USA Objectives Discuss new WHO classification
Thyroid pathology Practical part
 Thyroid pathology Practical part My Algorithm After a good macroscopy and a microscopic overview of the lesion, I especially look at the capsule and the thyroid just above and just beneath the capsule.
Thyroid pathology Practical part My Algorithm After a good macroscopy and a microscopic overview of the lesion, I especially look at the capsule and the thyroid just above and just beneath the capsule.
New entities in thyroid pathology: update according to the WHO classification
 New entities in thyroid pathology: update according to the WHO classification R.R. de Krijger, Dept. of Pathology, University Medical Center and Princess Maxima Center, Utrecht, The Netherlands New issues
New entities in thyroid pathology: update according to the WHO classification R.R. de Krijger, Dept. of Pathology, University Medical Center and Princess Maxima Center, Utrecht, The Netherlands New issues
The Frozen Section: Diagnostic Challenges and Pitfalls
 The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
The Frozen Section: Diagnostic Challenges and Pitfalls William C. Faquin, M.D., Ph.D. Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Harvard Medical
Case #1. Ed Stelow, MD University of Virginia
 Case #1 Ed Stelow, MD University of Virginia Imagine, If You Will It s 4:30 on Friday Last cytology case A thyroid FNA from outside that did not have any onsite interpretation It is from a 45-year old
Case #1 Ed Stelow, MD University of Virginia Imagine, If You Will It s 4:30 on Friday Last cytology case A thyroid FNA from outside that did not have any onsite interpretation It is from a 45-year old
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events
 Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
encapsulated thyroid nodule with a follicular architecture and some form of atypia. The problem is when to diagnose
 Histological Spectrum of Papillary Carcinoma of Thyroid A Two Years Study Gomathi Srinivasan 1, M. Vennila 2 1 Associate Professor Pathology, Government Medical College, Omandurar Estate, Chennai 600 002
Histological Spectrum of Papillary Carcinoma of Thyroid A Two Years Study Gomathi Srinivasan 1, M. Vennila 2 1 Associate Professor Pathology, Government Medical College, Omandurar Estate, Chennai 600 002
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
3/22/2017. Disclosure of Relevant Financial Relationships. Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC
 Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Disclosure
Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Disclosure
Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease
 Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease Robert L. Ferris, MD, PhD Department of Otolaryngology/Head and Neck Surgery and Yuri E. Nikiforov, MD, PhD Division of
Clinical and Molecular Approach to Using Thyroid Needle Biopsy for Nodular Disease Robert L. Ferris, MD, PhD Department of Otolaryngology/Head and Neck Surgery and Yuri E. Nikiforov, MD, PhD Division of
TBSRTC 1- Probabilistic approach and Relationship to Clinical Algorithms
 The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
The Benefits of a Uniform Reporting System for Thyroid Cytopathology BETHESDA REPORTING SYSTEM Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular
Background to the Thyroid Nodule
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital THYROID FNA: PART I Background to the
Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC
 Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Case Study
Cytomorphologic Thresholds for Classifying Thyroid FNAs as Suspicious and Positive for PTC Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic Laboratories Case Study
Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases
 Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases Can Potential Clues of Malignancy Be Identified? Mohammad Jaragh, MD 1 ; V. Bessie Carydis, MMedSci (Cytol) 1 ; Christina
Predictors of Malignancy in Thyroid Fine-Needle Aspirates Cyst Fluid Only Cases Can Potential Clues of Malignancy Be Identified? Mohammad Jaragh, MD 1 ; V. Bessie Carydis, MMedSci (Cytol) 1 ; Christina
THYROID CYTOLOGY THYROID CYTOLOGY FINE-NEEDLE-ASPIRATION ANCILLARY TESTS IN THYROID FNA
 ANCILLARY TESTS IN THYROID FNA Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular Pathology Unit, IPATIMUP General-Secretary of the International
ANCILLARY TESTS IN THYROID FNA Prof. Fernando Schmitt Department of Pathology and Oncology, Medical Faculty of Porto University Head of Molecular Pathology Unit, IPATIMUP General-Secretary of the International
NIFTP addendum to the RCPath Dataset for thyroid cancer histopathology reports. June 2016
 NIFTP addendum to the RCPath Dataset for thyroid cancer histopathology reports June 2016 Authors: Dr Sarah J Johnson, Royal Victoria Infirmary, Newcastle upon Tyne Professor TJ Stephenson, Sheffield Teaching
NIFTP addendum to the RCPath Dataset for thyroid cancer histopathology reports June 2016 Authors: Dr Sarah J Johnson, Royal Victoria Infirmary, Newcastle upon Tyne Professor TJ Stephenson, Sheffield Teaching
Thyroid follicular neoplasms in cytology. Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia
 Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Thyroid follicular neoplasms in cytology Ulrika Klopčič Institute of Oncology, Department of Cytopathology, Ljubljana, Slovenia Lecture overview importance of FNAB in assessing thyroid lesions follicular
Thyroid FNA: Diagnosis, Challenges and Solutions. Disclosures
 Thyroid FNA: Diagnosis, Challenges and Solutions Zubair W. Baloch, MD, PhD None Disclosures 1 Questions to Myself? Where We are Now? The Present 2 Reality Check There is More to How Thyroid Nodules are
Thyroid FNA: Diagnosis, Challenges and Solutions Zubair W. Baloch, MD, PhD None Disclosures 1 Questions to Myself? Where We are Now? The Present 2 Reality Check There is More to How Thyroid Nodules are
Normal thyroid tissue
 Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Thyroid Pathology Overview Normal thyroid tissue Normal thyroid tissue with follicles filled with colloid. Thyroid cells form follicles, spheres of epithelial cells (always single layered in health, usually
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case #1 FNA of nodule in left lobe of thyroid in 67 y.o. woman
 Challenging Cases Manon Auger M.D., F.R.C.P. (C) Professor, Department of Pathology McGill University Director, Cytopathology Laboratory McGill University it Health Center Case #1 FNA of nodule in left
Challenging Cases Manon Auger M.D., F.R.C.P. (C) Professor, Department of Pathology McGill University Director, Cytopathology Laboratory McGill University it Health Center Case #1 FNA of nodule in left
Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms
 Hindawi Publishing Corporation Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Hindawi Publishing Corporation Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
The Bethesda System for Reporting Thyroid Cytopathology, Laila Khazai 11/4/17
 The Bethesda System for Reporting Thyroid Cytopathology, 2017 Laila Khazai 11/4/17 In Summary No major changes for cytologists. The clinical team is faced with different risk of malignancies (ROM) associated
The Bethesda System for Reporting Thyroid Cytopathology, 2017 Laila Khazai 11/4/17 In Summary No major changes for cytologists. The clinical team is faced with different risk of malignancies (ROM) associated
Cytological features of well-differentiated tumors of uncertain malignant potential: Indeterminate cytology and WDT-UMP
 Endocrine Journal 2012, 59 (6), 483-487 Or i g i n a l Cytological features of well-differentiated tumors of uncertain malignant potential: Indeterminate cytology and WDT-UMP Keiko Nishigami 1), Zhiyan
Endocrine Journal 2012, 59 (6), 483-487 Or i g i n a l Cytological features of well-differentiated tumors of uncertain malignant potential: Indeterminate cytology and WDT-UMP Keiko Nishigami 1), Zhiyan
NIFTP Cytologic Aspects
 NIFTP Cytologic Aspects William C. Faquin, MD PhD Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Boston, MA USA So, what is the story about FVPTC
NIFTP Cytologic Aspects William C. Faquin, MD PhD Director, Head and Neck Pathology Massachusetts General Hospital & Massachusetts Eye and Ear Infirmary Boston, MA USA So, what is the story about FVPTC
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Section 2 Original Policy Date 2013 Last Review Status/Date September 1, 2014
 Policy Number 2.04.82 Molecular Markers in Fine Needle Aspirates of the Thyroid Medical Policy Section 2 Original Policy Date 2013 Last Review Status/Date September 1, 2014 Disclaimer Our medical policies
Policy Number 2.04.82 Molecular Markers in Fine Needle Aspirates of the Thyroid Medical Policy Section 2 Original Policy Date 2013 Last Review Status/Date September 1, 2014 Disclaimer Our medical policies
Sylvia L. Asa, MD, PhD Pathologist-in-Chief Medical Director Laboratory Medicine Program University Health Network, Toronto
 Minimizing in Thyroid Grey Zones Pathology Sylvia L. Asa, MD, PhD Pathologist-in-Chief Medical Director Laboratory Medicine Program University Health Network, Toronto Controversies Nodules in Thyroiditis
Minimizing in Thyroid Grey Zones Pathology Sylvia L. Asa, MD, PhD Pathologist-in-Chief Medical Director Laboratory Medicine Program University Health Network, Toronto Controversies Nodules in Thyroiditis
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms
 Case Reports in Pathology Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Case Reports in Pathology Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Volume 2 Issue ISSN
 Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Volume 2 Issue 3 2012 ISSN 2250-0359 Correlation of fine needle aspiration and final histopathology in thyroid disease: a series of 702 patients managed in an endocrine surgical unit *Chandrasekaran Maharajan
Hyalinizing Trabecular Neoplasm of the Thyroid: Controversies in Management
 ISPUB.COM The Internet Journal of Endocrinology Volume 2 Number 1 Hyalinizing Trabecular Neoplasm of the Thyroid: Controversies in Management J D'Elia, D Charous, J Miller, J Palazzo, E Pribitkin Citation
ISPUB.COM The Internet Journal of Endocrinology Volume 2 Number 1 Hyalinizing Trabecular Neoplasm of the Thyroid: Controversies in Management J D'Elia, D Charous, J Miller, J Palazzo, E Pribitkin Citation
Enterprise Interest None
 Enterprise Interest None Risk stratification of salivary gland lesions on cytology based on the proposed Milan System for reporting salivary gland cytopathology: A pilot study Kartik Viswanathan, M.D.,
Enterprise Interest None Risk stratification of salivary gland lesions on cytology based on the proposed Milan System for reporting salivary gland cytopathology: A pilot study Kartik Viswanathan, M.D.,
Dr Catherine Woolnough, Hospital Scientist, Chemical Pathology, Royal Prince Alfred Hospital. NSW Health Pathology University of Sydney
 Dr Catherine Woolnough, Hospital Scientist, Chemical Pathology, Royal Prince Alfred Hospital NSW Health Pathology University of Sydney Thyroid Cancer TC incidence rates in NSW Several subtypes - Papillary
Dr Catherine Woolnough, Hospital Scientist, Chemical Pathology, Royal Prince Alfred Hospital NSW Health Pathology University of Sydney Thyroid Cancer TC incidence rates in NSW Several subtypes - Papillary
Building On The Best A Review and Update on Bethesda Thyroid 2017
 Building On The Best A Review and Update on Bethesda Thyroid 2017 Syed Z. Ali, MD, FRCPath, FIAC Professor of Pathology and Radiology The Johns Hopkins Hospital, Baltimore, Maryland USA TBSRTC Diagnostic
Building On The Best A Review and Update on Bethesda Thyroid 2017 Syed Z. Ali, MD, FRCPath, FIAC Professor of Pathology and Radiology The Johns Hopkins Hospital, Baltimore, Maryland USA TBSRTC Diagnostic
Introduction 10/27/2011. Follicular Lesion/Atypia of Undetermined Significance
 Follicular Lesion/Atypia of Undetermined Significance Tarik M. Elsheikh, MD Cleveland Clinic Cleveland, Ohio Diagnostic Categories Proposed by Bethesda System/NCI Thyroid Conference 1. Benign 2. Follicular
Follicular Lesion/Atypia of Undetermined Significance Tarik M. Elsheikh, MD Cleveland Clinic Cleveland, Ohio Diagnostic Categories Proposed by Bethesda System/NCI Thyroid Conference 1. Benign 2. Follicular
Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
 yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
Non-Invasive Follicular Thyroid Neoplasm with Papillary-like Nuclei (NIFTP)
") Papillary Thyroid Carcinoma: Follicular Variant Encapsulated Type Replaced by: Non-Invasive Follicular Thyroid Neoplasm with Papillary-like Nuclei (NIFTP) Lester D. R. Thompson www.lester-thompson.com
Papillary Thyroid Carcinoma: Follicular Variant Encapsulated Type Replaced by: Non-Invasive Follicular Thyroid Neoplasm with Papillary-like Nuclei (NIFTP) Lester D. R. Thompson www.lester-thompson.com
Evaluation and Management of Thyroid Nodules. Overview of Thyroid Nodules and Their Management. Thyroid Nodule detection: U/S versus Exam
 Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Cytology for the Endocrinologist. Nicole Massoll M.D
 Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
Cytology for the Endocrinologist Nicole Massoll M.D Objectives Discuss slide preperation Definitions of adequacy ROSE (Rapid On-Site Evaluation) Thyroid Cytology Adequacy Nicole Massoll M.D. University
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT?
 POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
BE AWARE OF THE PATIENT WITH BENIGN FOLLICULAR THYROID LESION HISTOLOGY AND RISING THYROGLOBULIN LEVEL
 ENDOCRINE PRACTICE Rapid Electronic Article in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited, typeset
ENDOCRINE PRACTICE Rapid Electronic Article in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited, typeset
THYROID TUMOR DIAGNOSIS: MARKER OF THE MONTH CLUB
 THYROID TUMOR DIAGNOSIS: MARKER OF THE MONTH CLUB CHARACTERISTIC OF THE IDEAL TUMOR MARKER Specific Sensitive Easy to perform Easy to interpret Adaptable to FNA Reasonable cost (CHEAP) THYROID TUMOR MARKERS
THYROID TUMOR DIAGNOSIS: MARKER OF THE MONTH CLUB CHARACTERISTIC OF THE IDEAL TUMOR MARKER Specific Sensitive Easy to perform Easy to interpret Adaptable to FNA Reasonable cost (CHEAP) THYROID TUMOR MARKERS
Repeat Thyroid Nodule Fine-Needle Aspiration in Patients With Initial Benign Cytologic Results
 Anatomic Pathology / REPEAT THYROID FINE-NEEDLE ASPIRATION Repeat Thyroid Nodule Fine-Needle Aspiration in Patients With Initial Benign Cytologic Results Melina B. Flanagan, MD, MSPH, 1 N. Paul Ohori,
Anatomic Pathology / REPEAT THYROID FINE-NEEDLE ASPIRATION Repeat Thyroid Nodule Fine-Needle Aspiration in Patients With Initial Benign Cytologic Results Melina B. Flanagan, MD, MSPH, 1 N. Paul Ohori,
Thyroid Nodules. Family Medicine Refresher Course Geeta Lal MD, FACS April 2, No financial disclosures
 Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
"Atypical": Criteria and
 "Atypical": Criteria and Controversies Esther Rossi MD PhD MIAC Division of Anatomic Pathology and Cytology Catholic University of Sacred Heart Rome, Italy CASE HISTORY In 2015, 45 y/o woman underwent
"Atypical": Criteria and Controversies Esther Rossi MD PhD MIAC Division of Anatomic Pathology and Cytology Catholic University of Sacred Heart Rome, Italy CASE HISTORY In 2015, 45 y/o woman underwent
Cytokeratin 19 Immunolocalization in Cell Block Preparation of Thyroid Aspirates
 Cytokeratin 19 Immunolocalization in Cell Block Preparation of Thyroid Aspirates An Adjunct to Fine-Needle Aspiration Diagnosis of Papillary Thyroid Carcinoma Kamal K. Khurana, MD; Luan D. Truong, MD;
Cytokeratin 19 Immunolocalization in Cell Block Preparation of Thyroid Aspirates An Adjunct to Fine-Needle Aspiration Diagnosis of Papillary Thyroid Carcinoma Kamal K. Khurana, MD; Luan D. Truong, MD;
Usefulness of Diagnostic Qualifiers for Thyroid Fine-Needle Aspirations With Atypia of Undetermined Significance
 Anatomic Pathology / AUS Qualifiers in Thyroid FNAs Usefulness of Diagnostic Qualifiers for Thyroid Fine-Needle Aspirations With Atypia of Undetermined Significance Paul A. VanderLaan, MD, PhD, 1 Ellen
Anatomic Pathology / AUS Qualifiers in Thyroid FNAs Usefulness of Diagnostic Qualifiers for Thyroid Fine-Needle Aspirations With Atypia of Undetermined Significance Paul A. VanderLaan, MD, PhD, 1 Ellen
Cytopathological evaluation of various thyroid lesions based on Bethesda system for reporting thyroid lesions
 International Journal of Research in Medical Sciences Khadatkar AS et al. Int J Res Med Sci. 2017 Apr;5(4):1339-1343 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Original Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20170901
International Journal of Research in Medical Sciences Khadatkar AS et al. Int J Res Med Sci. 2017 Apr;5(4):1339-1343 www.msjonline.org pissn 2320-6071 eissn 2320-6012 Original Research Article DOI: http://dx.doi.org/10.18203/2320-6012.ijrms20170901
Molecular Markers in Fine Needle Aspirates of the Thyroid
 Molecular Markers in Fine Needle Aspirates of the Thyroid Policy Number: 2.04.78 Last Review: 3/2014 Origination: 3/2013 Next Review: 3/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will
Molecular Markers in Fine Needle Aspirates of the Thyroid Policy Number: 2.04.78 Last Review: 3/2014 Origination: 3/2013 Next Review: 3/2015 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Potential Pitfalls for False Suspicion of Papillary Thyroid Carcinoma:
 SUPPLEMENT 1 SPECIAL ISSUE: CYTOPATHOLOGY OF THE THYROID GLAND Guest Editor: Zubair Baloch Potential Pitfalls for False Suspicion of Papillary Thyroid Carcinoma: A Cytohistologic Review of 22 Cases Xin
SUPPLEMENT 1 SPECIAL ISSUE: CYTOPATHOLOGY OF THE THYROID GLAND Guest Editor: Zubair Baloch Potential Pitfalls for False Suspicion of Papillary Thyroid Carcinoma: A Cytohistologic Review of 22 Cases Xin
Clinical Significance of Distinguishing Between Follicular Lesion and Follicular Neoplasm in Thyroid Fine-Needle Aspiration Biopsy
 Ann Surg Oncol (2009) 16:3146 3153 DOI 10.1245/s10434-009-0666-3 ORIGINAL ARTICLE ENDOCRINE TUMORS Clinical Significance of Distinguishing Between Follicular Lesion and Follicular Neoplasm in Thyroid Fine-Needle
Ann Surg Oncol (2009) 16:3146 3153 DOI 10.1245/s10434-009-0666-3 ORIGINAL ARTICLE ENDOCRINE TUMORS Clinical Significance of Distinguishing Between Follicular Lesion and Follicular Neoplasm in Thyroid Fine-Needle
Scholars Journal of Medical Case Reports
 Scholars Journal of Medical Case Reports Sch J Med Case Rep 2017; 5(9):521-526 Scholars Academic and Scientific Publishers (SAS Publishers) (An International Publisher for Academic and Scientific Resources)
Scholars Journal of Medical Case Reports Sch J Med Case Rep 2017; 5(9):521-526 Scholars Academic and Scientific Publishers (SAS Publishers) (An International Publisher for Academic and Scientific Resources)
Follicular patterned lesions of the thyroid gland: a practical algorithmic approach
 1 Department of Cellular Pathology, John Radcliffe Hospital/University of Oxford, Oxford, UK 2 Nuffield Department of Clinical Laboratory Sciences, Biomedical Research Centre, John Radcliffe Hospital/University
1 Department of Cellular Pathology, John Radcliffe Hospital/University of Oxford, Oxford, UK 2 Nuffield Department of Clinical Laboratory Sciences, Biomedical Research Centre, John Radcliffe Hospital/University
Differentiated Thyroid Carcinoma
 Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Differentiated Thyroid Carcinoma The GOOD cancer? Jennifer Sipos, MD Associate Professor of Medicine Director, Benign Thyroid Program Division of Endocrinology, Diabetes and Metabolism The Ohio State University
Thyroid master class. Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson
 Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
Thyroid master class Thyroid Fine needle aspiration cytology and liquid-based techniques: Hologic and Becton Dickinson Principle of LBC Collection of cells in liquid medium Immediate fixation Processor-prepared
ASC Companion Meeting at the 2017 USCAP: Ancillary Molecular Testing in "Indeterminate. Thyroid Nodules: How Far Have We Come?
 ASC Companion Meeting at the 2017 USCAP: Ancillary Molecular Testing in "Indeterminate Thyroid Nodules: How Far Have We Come? William C. Faquin, MD, PhD, Massachusetts General Hospital, Boston, MA The
ASC Companion Meeting at the 2017 USCAP: Ancillary Molecular Testing in "Indeterminate Thyroid Nodules: How Far Have We Come? William C. Faquin, MD, PhD, Massachusetts General Hospital, Boston, MA The
Disclosures. Parathyroid Pathology. Objectives. The normal parathyroid 11/10/2012
 Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
Disclosures Parathyroid Pathology I have nothing to disclose Annemieke van Zante MD/PhD Assistant Professor of Clinical Pathology Associate Chief of Cytopathology Objectives 1. Review the pathologic features
CLINICAL MEDICAL POLICY
 Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Molecular Markers for Fine Needle Aspirates of Thyroid Nodules MP-065-MD-DE Medical Management Provider Notice Date: 10/15/2018;
Policy Name: Policy Number: Responsible Department(s): CLINICAL MEDICAL POLICY Molecular Markers for Fine Needle Aspirates of Thyroid Nodules MP-065-MD-DE Medical Management Provider Notice Date: 10/15/2018;
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration
 AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
AACE Thyroid Cancer Tumor board 25 years of the Endocrine and Surgery collaboration Dr. Peter Singer, Endocrinology Dr. Peter Sadow, Pathology Moderator Dr. Greg Randolph, Otolaryngology Relevant Financial
Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: a single-institutional experience in Japan
 2017, 64 (12), 1149-1155 Original Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: a single-institutional experience in Japan Mitsuyoshi Hirokawa 1), Miyoko Higuchi 2), Ayana
2017, 64 (12), 1149-1155 Original Noninvasive follicular thyroid neoplasm with papillary-like nuclear features: a single-institutional experience in Japan Mitsuyoshi Hirokawa 1), Miyoko Higuchi 2), Ayana
Disclosure of Relevant Financial Relationships
 Squamous entities of the thyroid: Reactive to Neoplastic Michelle D. Williams Associate Professor Dept of Pathology, Head & Neck Section University of Texas MD Anderson Cancer Center Disclosure of Relevant
Squamous entities of the thyroid: Reactive to Neoplastic Michelle D. Williams Associate Professor Dept of Pathology, Head & Neck Section University of Texas MD Anderson Cancer Center Disclosure of Relevant
Thyroid Gland. Protocol applies to all malignant tumors of the thyroid gland, except lymphomas.
 Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
Thyroid Gland Protocol applies to all malignant tumors of the thyroid gland, except lymphomas. Procedures Cytology (No Accompanying Checklist) Partial Thyroidectomy Total Thyroidectomy With/Without Lymph
JMSCR Vol 06 Issue 12 Page December 2018
 www.jmscr.igmpublication.org Impact Factor (SJIF): 6.379 Index Copernicus Value: 79.54 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v6i12.26 Histopathological and Cytological
www.jmscr.igmpublication.org Impact Factor (SJIF): 6.379 Index Copernicus Value: 79.54 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v6i12.26 Histopathological and Cytological
Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination
 Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Lester D. R. Thompson 1 & David N. Poller 2 & Kennichi Kakudo 3 & Raoul Burchette 4 & Yuri E. Nikiforov 5 & Raja R. Seethala 5
 Endocrine Pathology https://doi.org/10.1007/s12022-018-9520-0 An International Interobserver Variability Reporting of the Nuclear Scoring Criteria to Diagnose Noninvasive Follicular Thyroid Neoplasm with
Endocrine Pathology https://doi.org/10.1007/s12022-018-9520-0 An International Interobserver Variability Reporting of the Nuclear Scoring Criteria to Diagnose Noninvasive Follicular Thyroid Neoplasm with
Kyle C. Strickland, MD, PhD; Brooke E. Howitt, MD; Justine A. Barletta, MD; Edmund S. Cibas, MD Jeffrey F. Krane, MD, PhD
 Suggesting the Cytologic Diagnosis of Noninvasive Follicular Thyroid Neoplasm With Papillary-Like Nuclear Features (NIFTP): A Retrospective Analysis of Atypical and Suspicious Nodules Kyle C. Strickland,
Suggesting the Cytologic Diagnosis of Noninvasive Follicular Thyroid Neoplasm With Papillary-Like Nuclear Features (NIFTP): A Retrospective Analysis of Atypical and Suspicious Nodules Kyle C. Strickland,
Follicular Variant of Papillary Thyroid Carcinoma on the Basis of Histopathological and Immunohistochemical Diagnosis
 Bangladesh Med Res Counc Bull 2016; 42: 21-27 Follicular Variant of Papillary Thyroid Carcinoma on the Basis of Histopathological and Immunohistochemical Diagnosis Rahman MM 1, Banu SG 2, Barua AR 2, Kamal
Bangladesh Med Res Counc Bull 2016; 42: 21-27 Follicular Variant of Papillary Thyroid Carcinoma on the Basis of Histopathological and Immunohistochemical Diagnosis Rahman MM 1, Banu SG 2, Barua AR 2, Kamal
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
ASCP Competency Assessment
 ASCP Competency Assessment Thyroid Cytopathology Ricardo R. Lastra, MD Michelle R. Pramick, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman
ASCP Competency Assessment Thyroid Cytopathology Ricardo R. Lastra, MD Michelle R. Pramick, MD Zubair W. Baloch, MD, PhD Department of Pathology & Laboratory Medicine University of Pennsylvania, Perelman
Fine Needle Aspiration Cytology of Thyroid Follicular Neoplasm: Cytohistologic Correlation and Accuracy
 The Korean Journal of Pathology 2013; 47: 61-66 ORIGINAL ARTICLE Fine Needle Aspiration Cytology of Thyroid Follicular Neoplasm: Cytohistologic Correlation and Accuracy Changyoung Yoo Hyun Joo Choi Soyoung
The Korean Journal of Pathology 2013; 47: 61-66 ORIGINAL ARTICLE Fine Needle Aspiration Cytology of Thyroid Follicular Neoplasm: Cytohistologic Correlation and Accuracy Changyoung Yoo Hyun Joo Choi Soyoung
Molecular Diagnostics in Thyroid Tumors
 USCAP 2011 Endocrine Pathology Society Companion Meeting Molecular Diagnostics in Thyroid Tumors Yuri E. Nikiforov, M.D., Ph.D. Department of Pathology University of Pittsburgh Medical Center Outline Overview
USCAP 2011 Endocrine Pathology Society Companion Meeting Molecular Diagnostics in Thyroid Tumors Yuri E. Nikiforov, M.D., Ph.D. Department of Pathology University of Pittsburgh Medical Center Outline Overview
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
Columnar Cell Variant of Papillary Thyroid Carcinoma: Ultrasonographic and Clinical Differentiation between the Indolent and Aggressive Types
 Brief Communication Thyroid https://doi.org/10.3348/kjr.2018.19.5.1000 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2018;19(5):1000-1005 Columnar Cell Variant of Papillary Thyroid Carcinoma: Ultrasonographic
Brief Communication Thyroid https://doi.org/10.3348/kjr.2018.19.5.1000 pissn 1229-6929 eissn 2005-8330 Korean J Radiol 2018;19(5):1000-1005 Columnar Cell Variant of Papillary Thyroid Carcinoma: Ultrasonographic
RE-AUDIT OF THYROID FNA USING THE THY GRADING SYSTEM AND HISTOLOGY AT SUNDERLAND ROYAL HOSPITAL, 2011
 Audit: RE-AUDIT OF THYROID FNA USING THE THY GRADING SYSTEM AND HISTOLOGY AT SUNDERLAND ROYAL HOSPITAL, 2011 Auditors: Dr Lena Wilkinson SpR Histopathology Dr. Debra Milne Consultant Histocytopathologist
Audit: RE-AUDIT OF THYROID FNA USING THE THY GRADING SYSTEM AND HISTOLOGY AT SUNDERLAND ROYAL HOSPITAL, 2011 Auditors: Dr Lena Wilkinson SpR Histopathology Dr. Debra Milne Consultant Histocytopathologist
My personal experience at University of Toronto and recent updates of
 My personal experience at University of Toronto and recent updates of Endocrine Pathology Toshitetsu Hayashi M.D. Ph.D. ¹Department of Diagnostic Pathology, Takamatsu Red Cross Hospital, Japan ²Laboratory
My personal experience at University of Toronto and recent updates of Endocrine Pathology Toshitetsu Hayashi M.D. Ph.D. ¹Department of Diagnostic Pathology, Takamatsu Red Cross Hospital, Japan ²Laboratory
Introduction: Ultrasound guided Fine Needle Aspiration: When and how
 International Course of Thyroid Ultrasonography and minimally invasive procedure 7-8 October 2016 University of Pisa, Italy Introduction: Ultrasound guided Fine Needle Aspiration: When and how Teresa Rago
International Course of Thyroid Ultrasonography and minimally invasive procedure 7-8 October 2016 University of Pisa, Italy Introduction: Ultrasound guided Fine Needle Aspiration: When and how Teresa Rago
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release
 CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
CAP Cancer Protocol and ecc Summary of Changes for August 2014 Thyroid Agile Release 2 REVISION HISTORY Date Author / Editor Comments 5/19/2014 Jaleh Mirza Created the document 8/12/2014 Samantha Spencer/Jaleh
Molecular Testing for Indeterminate Thyroid Nodules. October 20, 2018
 Molecular Testing for Indeterminate Thyroid Nodules October 20, 2018 Patient 1: Left 1.0 cm AP x 1.6 cm transverse x 2.1 cm in length Well defined Isoechoic heterogeneous No calcification Grade 3 Vascularity
Molecular Testing for Indeterminate Thyroid Nodules October 20, 2018 Patient 1: Left 1.0 cm AP x 1.6 cm transverse x 2.1 cm in length Well defined Isoechoic heterogeneous No calcification Grade 3 Vascularity
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches
 Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A
Salivary gland tumor cytologic and histologic correlation: Algorithmic and risk stratification based approaches Christopher C. Griffith, MD, PhD Raja R. Seethala, MD 1. Salivary gland tumor cytology: A