OUTLINE OF SHORT COURSE WHO CLASSIFICATION DEFINITION OF A LYMPHOMA. FOLLICULAR LYMPHOMA: Outline of Talk. FOLLICULAR LYMPHOMA: Outline of Talk
|
|
|
- Nathaniel James
- 6 years ago
- Views:
Transcription
1 OUTLINE OF SHORT COURSE WHO CLASSIFICATION B-CELL LYMPHOMAS: A PRACTICAL & COST-EFFECTIVE APPROACH TO DIAGNOSIS 1. WHO classification: Integrated approach to diagnosis 2. Practical & cost- effective approach to diagnosis 3. Presentation of 14 cases submitted to participants 4. Follicular lymphoma and 3 cases minutes 5. Mantle cell lymphoma and 1 case minutes 6. Marginal zone B- B cell lymphoma and 3 cases min. 7. Small lymphocytic lymphoma /CLL and Lymphoplasmacytic lymphoma and 4 cases mins 8. Diffuse large B- B cell lymphoma and 3 cases min. WHO CLASSIFICATION DEFINITION OF A LYMPHOMA To Define a Distinct Disease Entity Requires an Integrated Approach to Diagnosis SUMMARY: GOLD STANDARD FOR DIAGNOSIS No Fixed Gold Standard. It Depends on an Individual Case - Morphology sometimes - Immunohistochemistry sometimes - Molecular sometimes - Clinical sometimes Dealing with Discordance Integrated Diagnosis Requires Knowledge and Experience with Lymphoid Diseases Morphology is always important FOLLICULAR LYMPHOMA: Outline of Talk Definition Morphology: Patterns and cytologic features In-situ Follicular Lymphoma Progression and Transformation Value and Limitations of Immunohistochemistry Correlation of cytogenetics and molecular biology with pathology, survival, and prognosis Significance of presence or absence of t(14;18) and correlation with bcl-2 2 protein expression Correlating bcl-6 gene rearrangement with t(14;18) FOLLICULAR LYMPHOMA: Outline of Talk Definition Morphology: Patterns and cytologic features In-situ Follicular Lymphoma Progression and Transformation Value and Limitations of Immunohistochemistry Correlation of cytogenetics and molecular biology with pathology, survival, and prognosis
.")
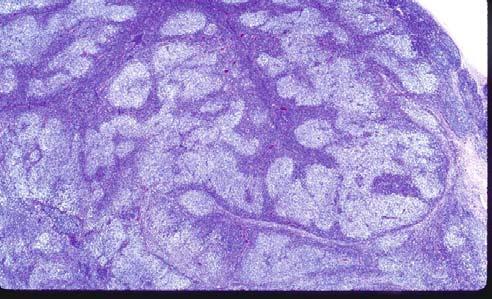
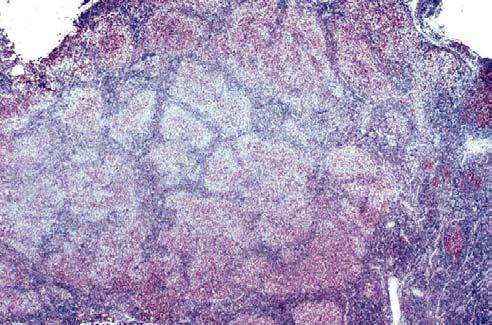
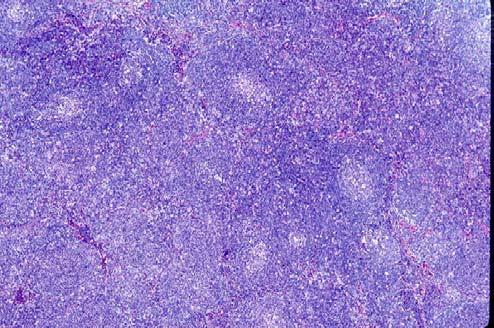
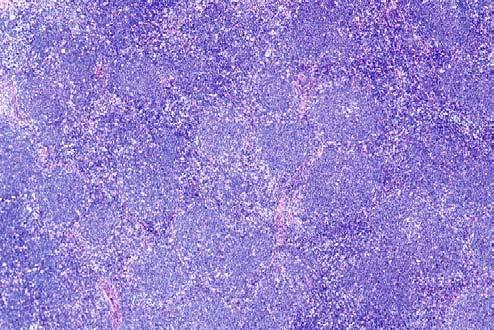
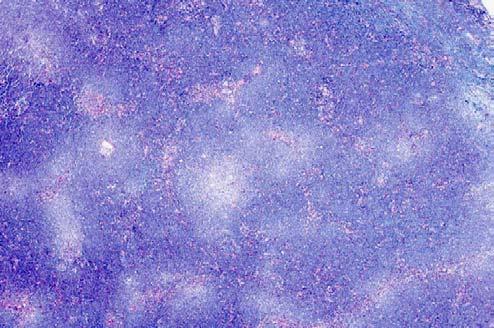
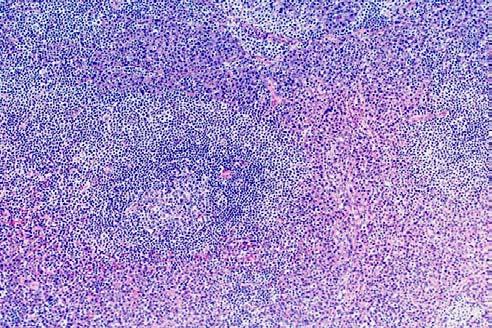
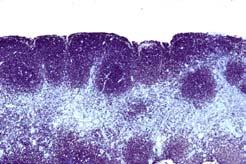
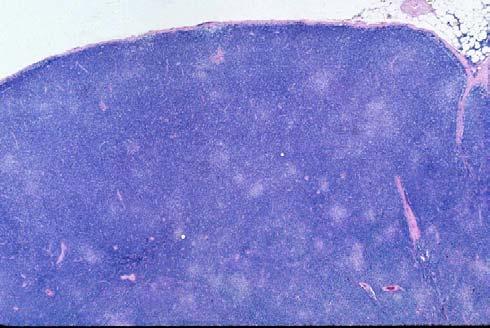
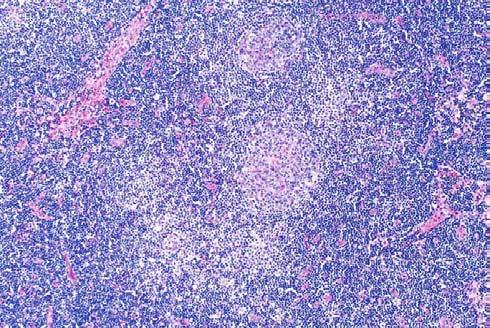
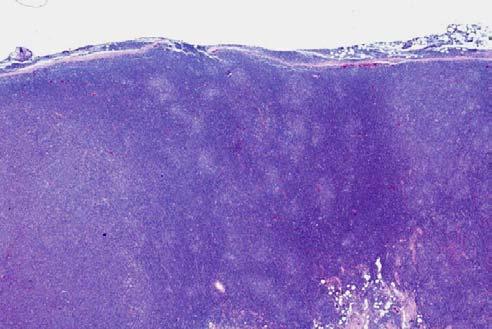
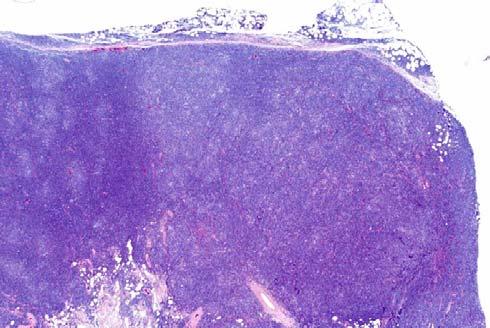
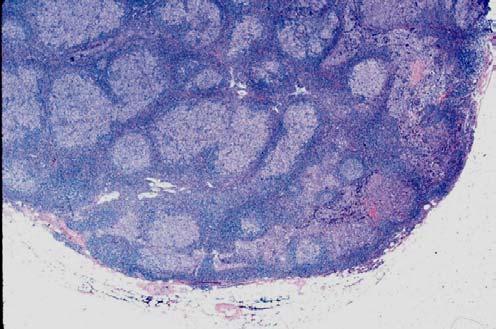
2 FOLLICULAR LYMPHOMA: Definition Lymphoma arising from B cells located within follicular centers, which consist of centrocytes and centroblast (cleaved & non-cleaved cells). This lymphoma has a follicular pattern (not follicular colonization). FOLLICULAR COLONIZATION Colonization of benign follicles by: - Benign mantle cells: CD20+, IgD+, bcl-2+, CD5-, cyclin D1- - Benign normal T- T cells within follicles: CD3+ - Malignant marginal zone B cells: CD20+, bcl-6-, CD10- - Malignant mantle cells: CD20+, CD43+, CD5+, cyclin D1+ - AIL- Tcell lymphoma: CD3+, CD4+, CD10+, bcl-6+ - KSHV+, EBV+, HIV- Germinotropic Lymphoproliferative Disorder Colonization of malignant follicles by: - Benign Mantle Cells - Benign T cells - Malignant Marginal Zone B cells MORPHOLOGY: Outline CRITERIA: Patterns, Cytology PATTERNS: Typical; Unusual; Other CYTOLOGY: Criteria, Unusual, Grading, 3a vs. 3b IN-SITU FOLLICULAR LYMPHOMA PROGRESSION AND TRANSFORMATION VALUE & LIMITATIONS OF IMMUNOSTAINS DIFFERENTIAL DIAGNOSIS VARIANTS CRITERIA: Pattern and Cytology FOLLICULAR LYMPHOMA: Morphologic Criteria Follicular density: Back-to to-back or closely packed Follicular definition: Poorly defined Mantle zones: Absent Polarity: Absent Starry-sky: Absent Cytology within and outside follicles: Similar Follicular Lymphoma

 Typical FL without mantle zones FL with inverse follicular pattern produced by Centroblasts")
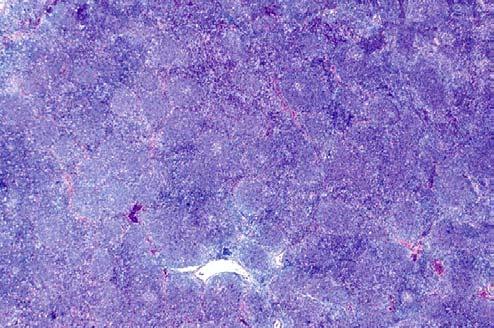
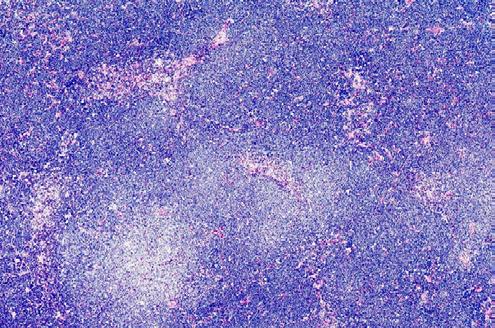
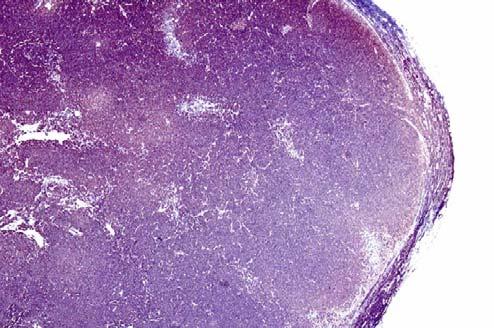
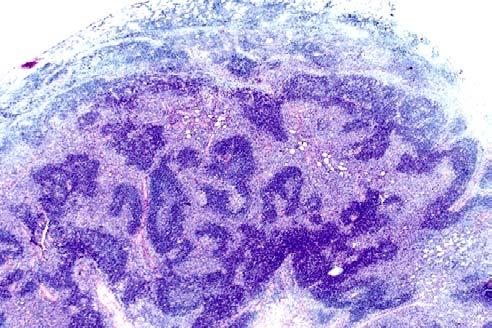
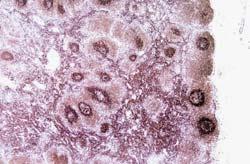
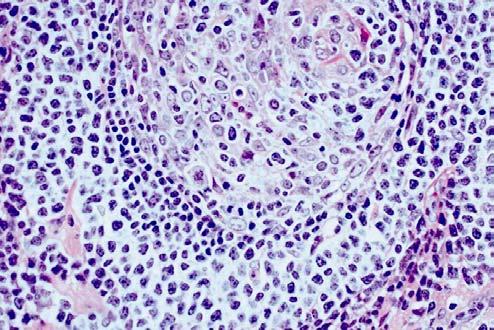
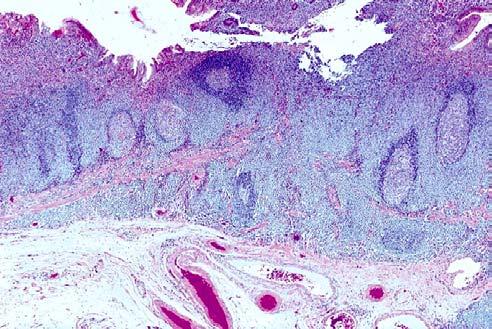
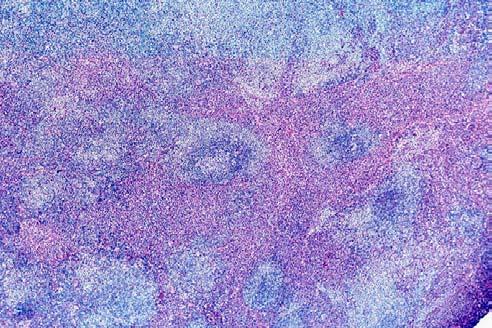
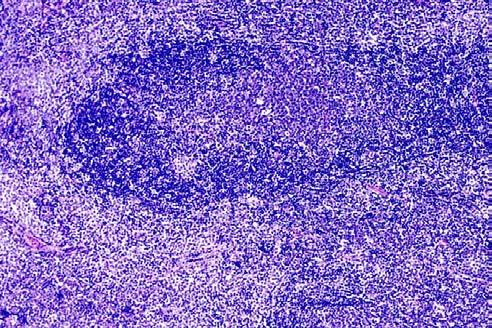
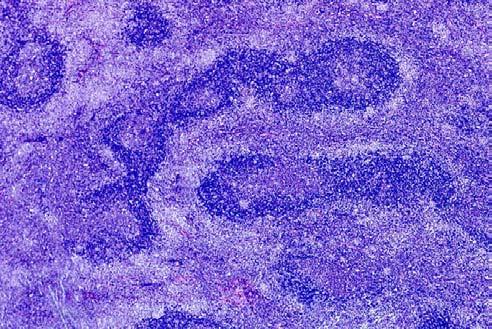
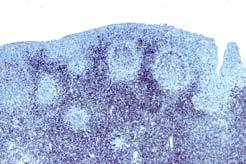
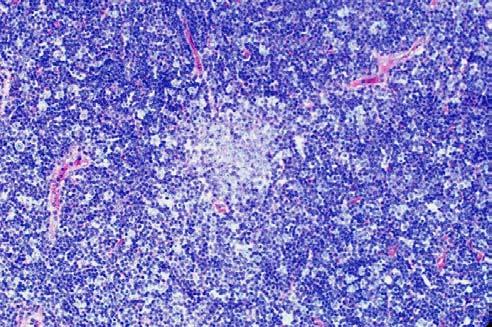
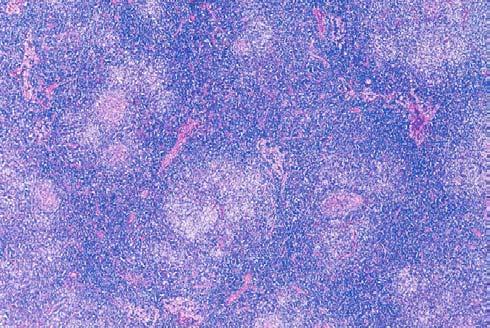
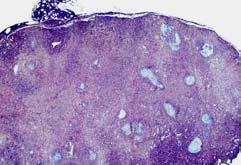
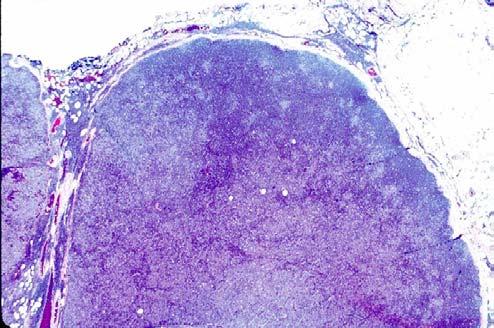
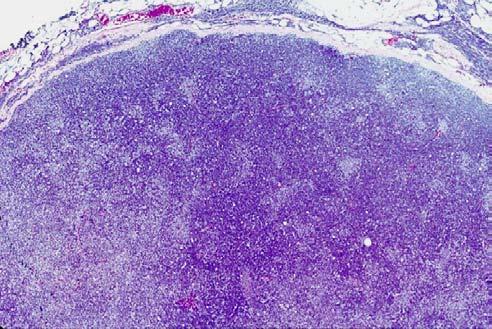
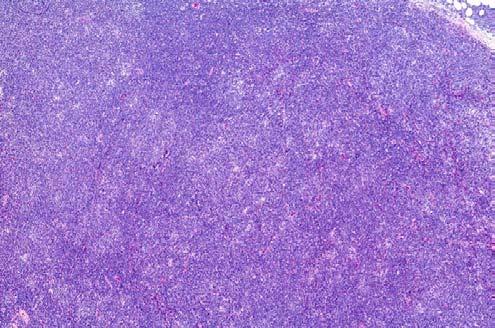
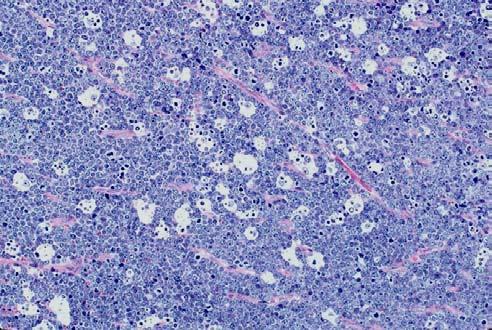
3 SIGNIFICANCE OF BACK-TO-BACK PATTERN OF FOLLICLES 1. In 98% of the cases, such a pattern indicates that the follicles are malignant. 2. In 2% of the cases, this pattern is associated with benign follicles, especially in early HIV. However, these follicles: A. are usually large & well-defined B. exhibit prominent phagocytic & high mitotic activity C. exhibit prominent polarity Marked Follicular Hyperplasia In HIV PATTERNS IN FOLLICULAR LYMPHOMA (FL) Typical FL without mantle zones FL with inverse follicular pattern produced by Centroblasts Marginal Zone B-cells B (MZBCL differentiation) FL with Marginal Zone pattern (MZBCL diff..tion) FL with Diffuse Large B-Cell B Lymphoma Quantifying follicularity: : >75%, 75-25%, <25% Follicular & Interfollicular pattern FL with memory B-cells B in interfollicular area FL- other patterns PATTERNS: TYPICAL, INVERSE, & MARGINAL ZONE One layer (typical): Only FCC proliferation with no mantle zones (73%) Two layers: Normal arrangement -FCC surrounded by benign mantle cells (15%) Inverse arrangement (inverse follicular) -Malignant centrocytes surrounded by malignant centroblasts (2%) -Malignant centrocytes surrounded by malignant marginal zone B-cells B (5%) Three layers: Malignant FCC surrounded by benign mantle cells which are surrounded by an outer third layer of marginal zone B-cellsB (5%) One-Layered Follicles TYPICAL FOLLICULAR PATTERN One-layered follicles Only follicular center cell proliferation with no mantle zones



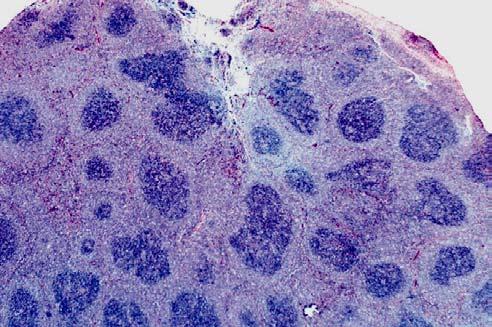
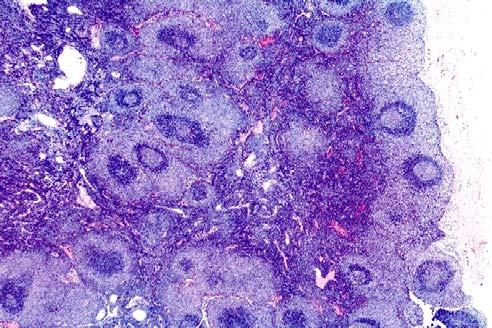
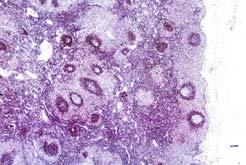
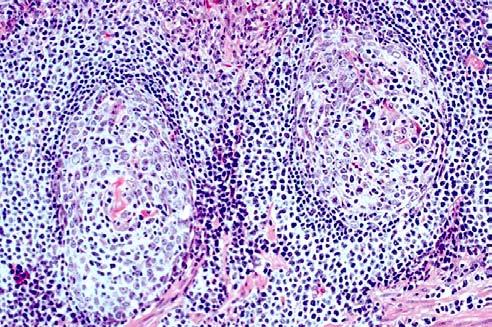
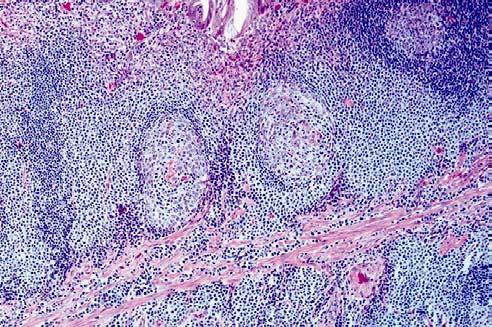
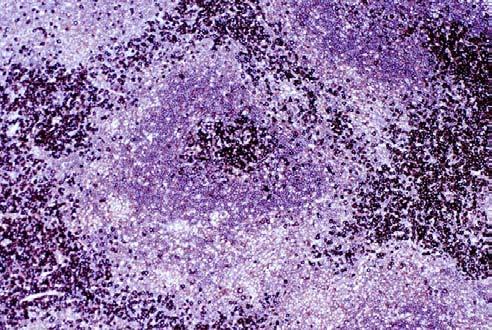
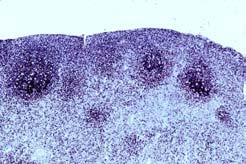
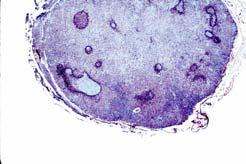
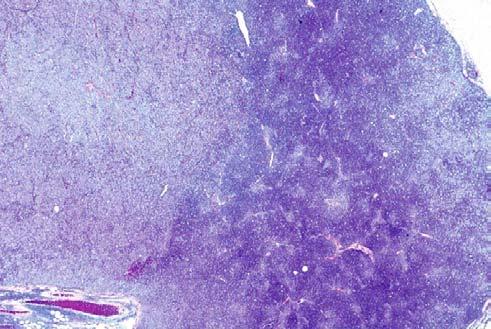
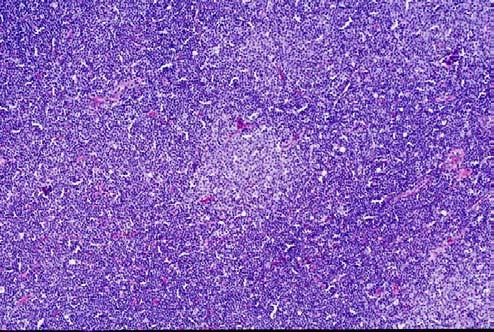
4 FOLLICULAR LYMPHOMA WITH BENIGN MANTLE ZONES Two-Layered Follicles: : (1) Malignant FCCs surrounded by benign mantle zones in a normal arrangement At low magnification, two-layered follicles with normal arrangement of colors Inner layer of lightly staining malignant follicular center cells surrounded by an outer layer of darkly staining benign mantle zones FOLLICULAR LYMPHOMA WITH INVERSE FOLLICULAR PATTERN At low magnification, two-layered follicles with an inverse arrangement of colors Inner layer of darkly staining malignant centrocytes surrounded by an outer layer of lightly staining malignant centroblasts IAP CASE 1 S DIAGNOSIS FOLLICULAR LYMPHOMA GRADE 3/3 WITH AN INVERSE FOLLICULAR PATTERN PRODUCED BY CENTROBLASTS











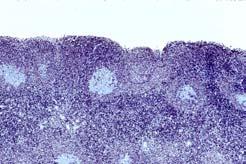
5 CD10 CD20 CD20 bcl-6 CD23 CD23 bcl-6 bcl-6 CD10 bcl-2 FOLLICULAR LYMPHOMA WITH INVERSE FOLLICULAR PATTERN Follicular Lymphoma with Marginal Zone B-cell Differentiation At low magnification, two-layered follicles with an inverse arrangement of colors Inner layer of darkly staining malignant follicular center cells surrounded by an outer layer of lightly staining malignant marginal zone B-cells (marginal zone B-cell differentiation)

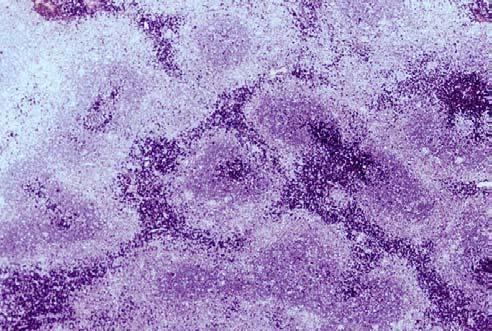
6 CD20 bcl-2 CD10 bcl-6 FOLLICULAR LYMPHOMA WITH MARGINAL ZONE PATTERN Three-layered follicles (marginal zone pattern) Inner layer of malignant fcc, middle layer of benign mantle zone, third outer layer of marginal zone B-cells (marginal zone B-cell differentiation)
 Found in 12% of pure follicular lymphomas Found in > 60% of de novo marginal zone B- B cell lymphomas Found in both follicular center cells & marginal zone B")

7 Significance of Marginal Zone B-Cell Differentiation in Follicular Lymphoma CORRELATION OF MORPHOLOGIC FINDINGS WITH TRISOMY 3 AND 3q TRANSLOCATION ABNORMALITIES INVOLVING CHROMOSOME 3 (TRISOMY 3 OR 3q27-29 TRANSLOCATION) Found in 12% of pure follicular lymphomas Found in > 60% of de novo marginal zone B- B cell lymphomas Found in both follicular center cells & marginal zone B cells in all 3 cases (100%) of follicular lymphomas with marginal zone B- B cell differentiation CONCLUSION: These abnormalities may be responsible for the development of the marginal zone B- B cell component in follicular lymphoma Goodlad, et al., Histopathology 42: , PATTERNS IN FOLLICULAR LYMPHOMA One layer: Only FCC proliferation with no mantle zones (73%) Two layers: Normal arrangement -FCC surrounded by benign mantle cells (15%) Inverse arrangement -Malignant centrocytes surrounded by malignant centroblasts (2%) -Malignant centrocytes surrounded by malignant marginal zone B-cells B (5%) Three layers: Malignant FCC surrounded by benign mantle cells which are surrounded by an outer third layer of marginal zone B-cells B (5%)
 FL with Marginal Zone pattern (MZBCL diff.")

 IAP CASE 11")
8 PATTERNS IN FOLLICULAR LYMPHOMA (FL) Typical FL without mantle zones FL with inverse follicular pattern produced by Centroblasts Marginal Zone B-cells B (MZBCL differentiation) FL with Marginal Zone pattern (MZBCL diff..tion) FL with memory B-cells B in interfollicular area FL with Diffuse Large B-Cell B Lymphoma Quantifying follicularity: : >75%, 75-25%, <25% Follicular & Interfollicular pattern FL- other patterns MALIGNANT B-CELLS IN THE INTERFOLLICULAR AREAS MALIGNANT B-CELLS IN THE INTERFOLLICULAR AREAS Migration of typical follicular center cells; CD20+, CD10+, bcl-6+ Migration of centrocytes which appear smaller and less irregular; CD20+, CD10+, bcl-6+ Malignant memory B-cells B which have slight nuclear irregularities; CD20+, CD10-,, bcl-6- Marginal Zone B-cells; B CD20+, CD10-,, bcl-6- Plasma cells (monoclonal) IAP CASE 11 BNN-9943 DIAGNOSIS g FOLLICULAR LYMPHOMA GRADE 3/3 WITH SMALL MALIGNANT B-CELLS IN INTERFOLLICULAR AREAS
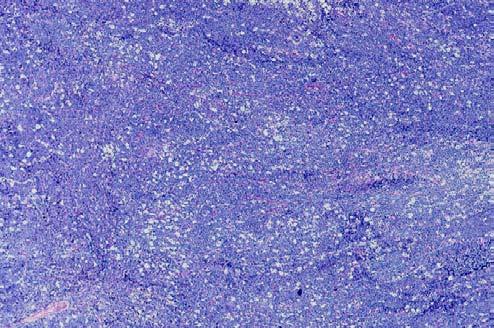
9 PATTERNS IN FOLLICULAR LYMPHOMA (FL) Typical FL without mantle zones FL with inverse follicular pattern produced by Centroblasts Marginal Zone B-cells B (MZBCL differentiation) FL with Marginal Zone pattern (MZBCL diff..tion) FL with memory B-cells B in interfollicular area FL with Diffuse Large B-Cell B Lymphoma Quantifying follicularity: : >75%, 75-25%, <25% Follicular & Interfollicular pattern FL- other patterns DIFFUSE LARGE B-CELL LYMPHOMA IN FOLLICULAR LYMPHOMA Presence of Diffuse Large B-Cell Lymphoma in a Follicular Lymphoma - DLBCL should be explicitly stated in the bottom line diagnosis - The surface area (%) occupied by the DLBCL should also be clearly stated in the bottom line PATTERNS IN FOLLICULAR LYMPHOMA (FL) Typical FL without mantle zones FL with inverse follicular pattern produced by Centroblasts Marginal Zone B-cells B (MZBCL differentiation) FL with Marginal Zone pattern (MZBCL diff..tion) FL with memory B-cells B in interfollicular area FL with Diffuse Large B-Cell B Lymphoma Quantifying follicularity: : >75%, 75-25%, <25% Follicular & Interfollicular pattern FL- other patterns PATTERNS IN FOLLICULAR LYMPHOMA (FL) Typical FL without mantle zones FL with inverse follicular pattern produced by Centroblasts Marginal Zone B-cells B (MZBCL differentiation) FL with Marginal Zone pattern (MZBCL diff..tion) FL with Diffuse Large B-Cell B Lymphoma Quantifying follicularity: : >75%, 75-25%, <25% Follicular & Interfollicular pattern FL with memory B-cells B in interfollicular area FL- other patterns Other Patterns In Follicular Lymphoma Rarely Seen -Floral Variant -Mild Polarity-Like -Castlemanoid -Prominent Starry-Sky Sky Pattern -Marked Sclerosis

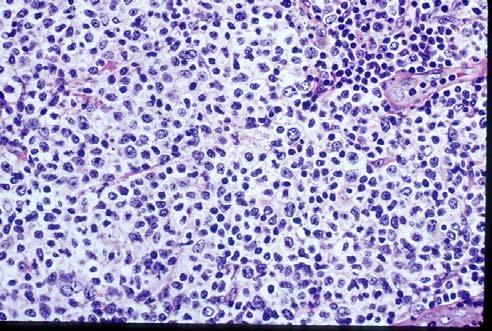
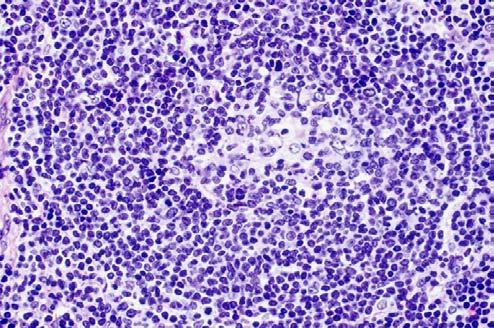
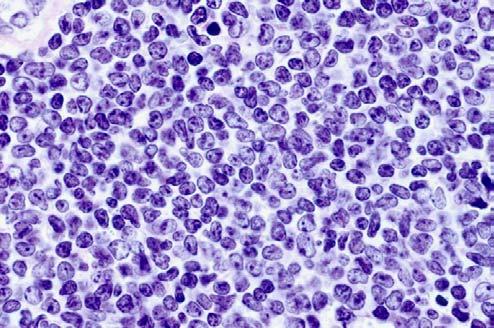
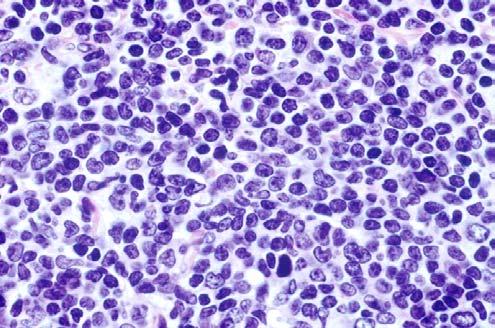
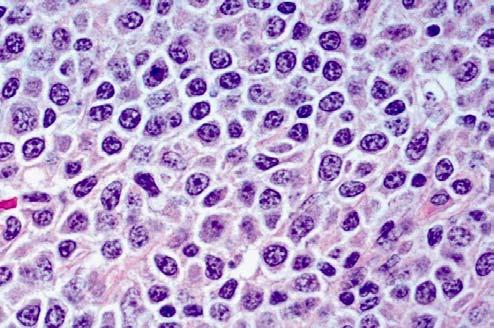
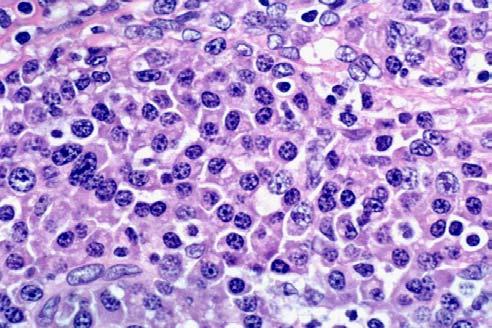
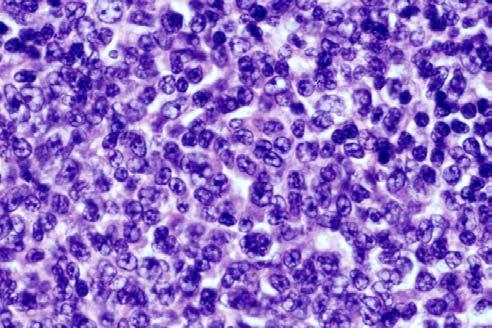
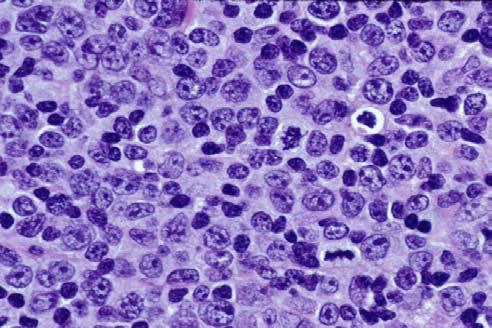
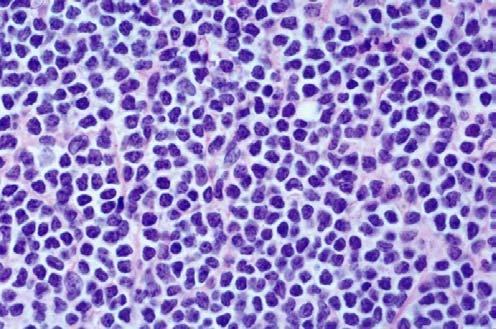
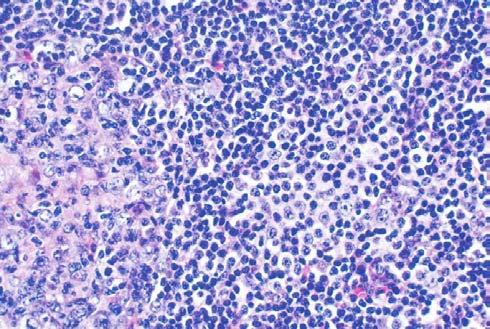
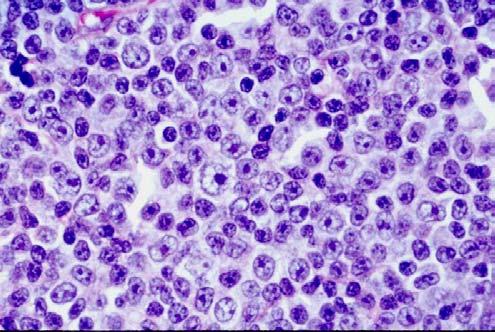
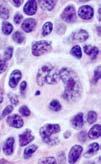
10 CYTOLOGIC FEATURES Cytologic criteria FCC: Unusual cytologic features Grading of Follicular Lymphoma Differences between grade 3A and grade 3B MEASURING CELL SIZE 1. By comparing size with: - red blood cells - small mature lymphocytes - nucleus of a benign histiocyte 2. By using a built-in in micrometer in the eye piece lens. CELL SIZE DEFINITIONS Small cells (up to 2 times the surface area of RBC or small lymphocyte) Medium size cells (2 to 3 times the surface area of RBC or small lymphocyte) Large size cells (>3 times the surface area of RBC or small lymphocyte) MORPHOLOGY OF FOLLICULAR CENTER CELLS (FCC) FCCs are divided into two groups based on the presence or absence of distinct nucleoli 1. Non-nucleolated nucleolated cells are called centrocytes ( cleaved cells), and on the basis of size, are subdivided into two types: A. Small centrocytes B. Large centrocytes Centrocytes MORPHOLOGY OF FCC (cont.) 2. Nucleolated cells are called centroblasts noncleaved cells, and on the basis of size, are subdivided into two types: A. Small centroblast (small noncleaved) B. Large centroblast (large noncleaved)
 Distribution - Single, pair (kissing), other Immunology - CD21+, CD23+, CD35+ Follicular Dendritic Reticulum Cells FOLLICULAR LYMPHOMA:")
. FOLLICULAR LYMPHOMA (cont.) 4.")

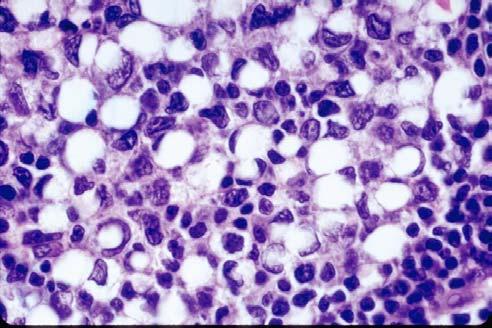
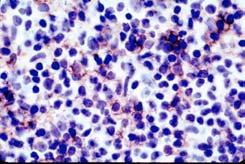
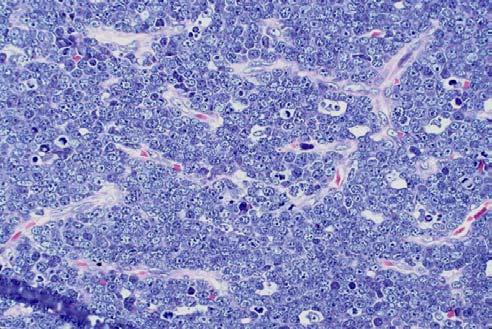
11 Small Centroblasts Large Centroblasts FOLLICULAR DENDRITIC RETICULUM CELLS Morphology Size - Medium to large Shape - Round to oval to spindle Chromatin - Bland Nucleoli - One small Cytoplasm - Scanty (processes not seen in H&E) Distribution - Single, pair (kissing), other Immunology - CD21+, CD23+, CD35+ Follicular Dendritic Reticulum Cells FOLLICULAR LYMPHOMA: Cytologic Criteria 1. >95% of FCC are of the small size (monomorphism with respect to size). 2. >95% of FCC have the same shape (monomorphism with respect to shape). 3. >95% of FCC have the same chromatin structure (monomorphism( with respect to chromatin structure). FOLLICULAR LYMPHOMA (cont.) 4. The small cells ( cleaved ) show pronounced variation in nuclear shape. 5. Numerous spindle shaped cells in non sclerotic areas. 6. The small and medium sized nuclei show nuclear convolutions. 7. Cytology of cells within and outside follicles is identical. Unusual Cytology In Follicular Lymphoma - Clear Cells: (follicular center cells vs. marginal zone B-cells) B ( 5%) - Signet ring cells( 0.1%) - Small Centroblastic:(small (small noncleaved) (1%)

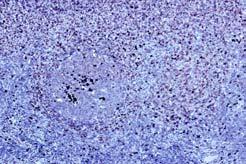
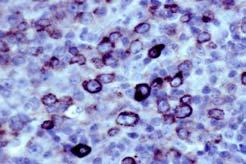
12 Clear Cells bcl-6

 B - Signet ring - Small")

")
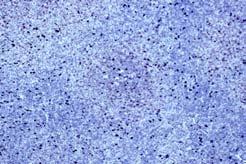
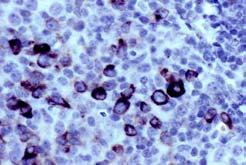
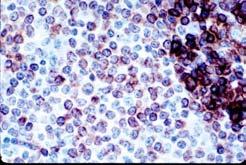
13 Signet-Ring Cells, IgG Kappa Type Unusual Cytologic Features In Follicular Lymphoma - Clear Cells: (follicular center cells vs. marginal zone B-cells) B - Signet ring - Small Centroblastic: (small (small noncleaved) Small Centroblastic Unusual Cytologic Features In Follicular Lymphoma - Clear Cells: (follicular center cells vs. marginal zone B cells) - Signet ring - Small Centroblastic: (small (small noncleaved)




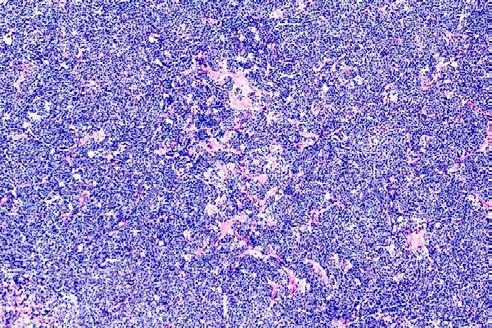
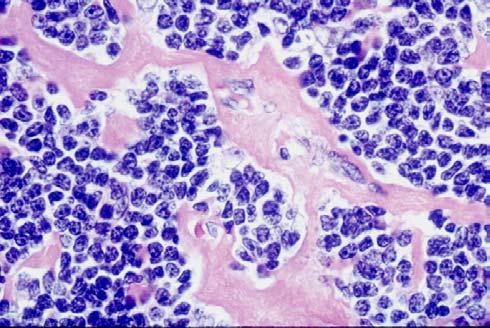
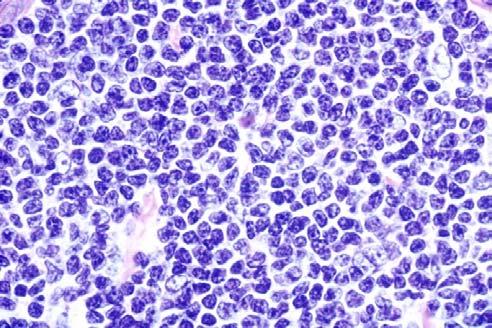
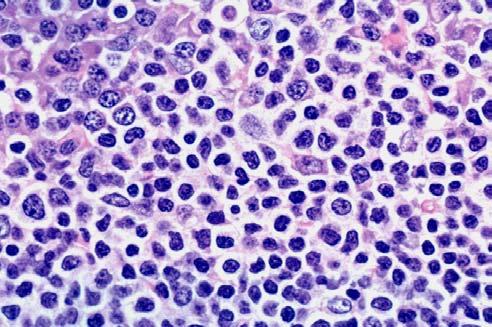
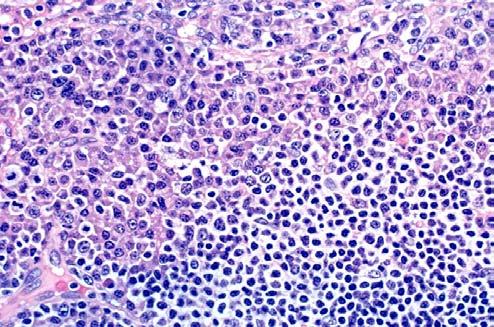
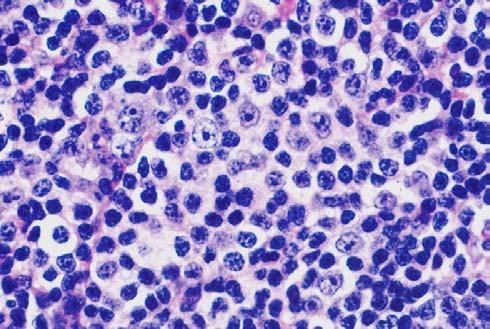
14 FOLLICULAR LYMPHOMA: Grading GRADING OF FOLLICULAR LYMPHOMA Grading Criteria Grade centroblasts per hpf* Grade centroblasts per hpf* Grade 3 >15 centroblasts per hpf* 3a centrocytes admixed 3b solid sheets of centro- blasts without centrocytes FL Grade 1/3 FL Grade 2/3 FL Grade 3a FL Grade 3b
 ----- 100% 50% p<0.01 0 44% p<0.01 73% 13% p<0.")

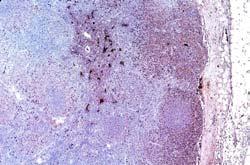
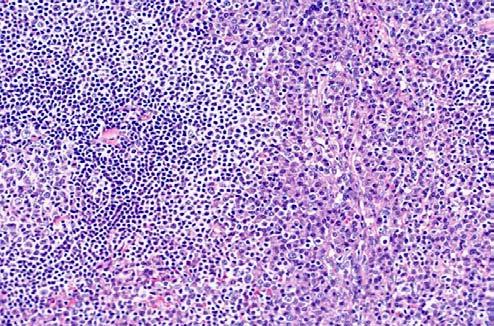
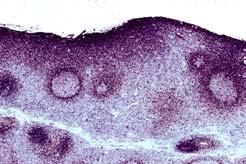
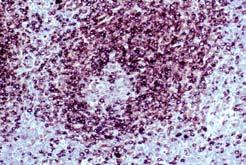
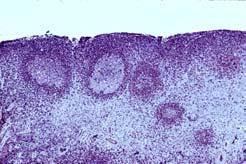
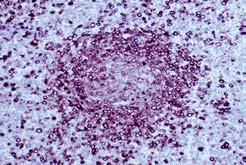
15 DIFFERENCES BETWEEN FOLLICULAR LYMPHOMA GRADE 3A AND 3B PARAMETERS No. of cases 1. CD Cytoplasmic immunoglobulin 3. t(14;18) Ott et. al., Blood 99: , 3812, 2002 Grade 3a Grade 3b p Value (4 w/ DLBC) % 50% p< % p< % 13% p<0.01 MORPHOLOGY: Outline CRITERIA: Patterns, Cytologic PATTERNS: Typical; Unusual; Other CYTOLOGY: Criteria, Unusual, Grading, 3a vs. 3b IN-SITU FOLLICULAR LYMPHOMA PROGRESSION AND TRANSFORMATION VALUE & LIMITATIONS OF IMMUNOSTAINS DIFFERENTIAL DIAGNOSIS VARIANTS IN-SITU FOLLICULAR LYMPHOMA IN-SITU FOLLICULAR LYMPHOMA 23 Nodes: Normal Architecture and Scattered bcl-2 2 Negative Benign Follicles g Few follicles cytologically atypical and suspicious for lymphoma and were bcl-2+ g 56% of cases, bcl follicles >50% g Follow-up: - 28% had FL in other nodes - 17% developed FL, 3 to 72 months later - 55% do not develop FL with median follow-up time of 15.5 months Cong et al, Blood 99: 3376, 2002 In-Situ Follicular Lymphoma




16 bcl-2 bcl-2 bcl-2 PROGRESSION & TRANSFORMATION PROGRESSION AND TRANSFORMATION Progression Grade 1 to 2 Grade 2 to 3 Any grade to diffuse large B-cell B lymphoma Transformation B-Anaplastic: : CD30+, CD20+, ALK-1+ B-Lymphoblastic: Tdt+, CD10+,CD20+ Hodgkin-like: CD15+, CD30+




17 B-Anaplastic Transformation GENETIC CHANGES ASSOCIATED WITH PROGRESSION Initial FL grade At progression/ transformation Genetic change Grade 1 Grade 1 Grade 1 Grade 3a 6q-, +7, +12, +18 Grade 3b, DLBCL p53, p16 Burkitt-like c-myc SECONDARY CYTOGENETIC & MOLECULAR ABNORMALITIES IN TRANSFORMED FL 1. Non-random chromosomal changes 2. Genetic instability 3. c-myc gene rearrangement 4. Changes in expression profiles of c-myc & genes regulated by c-myc 5. Somatic mutations of p53 & (translocated( translocated) ) bcl-2 6. Inactivation of p16 & p15 by deletions, mutations or hypermethylation CONCLUSION: Heterogeneous genetic lesions & different molecular mechanisms underlie the transformation process. VALUES AND LIMITATIONS OF IMMUNHISTOCHEMISTRY
18 LIMITATIONS OF IMMUNOHISTOCHEMISTRY Lack of specificity and sensitivity Lack of counter-staining prevents appreciation of cytologic details of positive and negative cells Antigen retrieval process can cause bubbly nuclear artifacts Interpretation of built-in in controls Background and non-specific staining Summary Of Limitations CD20+ (post Rituxan CD20 maybe negative) CD % bcl- 6+ ~80% bcl- 2+ (overall in adults 85%; in children protein +30%) and bcl- 2 gene in only 12% ) Kappa and lambda are negative in follicular center cells in 60% of cases CD43+ in 6% of G- G 3, 1% of G- G 2, 2% of G- G 1 CD23+ sometimes in malignant FCCs DIFFERENTIAL DIAGNOSIS DIFFERENTIAL DIAGNOSIS A. Daily - Follicular Hyperplasia (HIV and non- HIV) B. Frequently - Marginal Zone B- B Cell Lymphoma with - Exuberant Follicular Hyperplasia C. Infrequently Because of Follicular Colonization - Marginal Zone B- B Cell Lymphoma - Mantle Cell Lymphoma D. Rarely Because of Thick Mantle Zones - Floral Variant of FL - PTGC - Nodular Lymphocyte Predominant Hodgkin Lymphoma and Classical Hodgkin Lymphoma - Mantle Zone Hyperplasia FOLLICULAR LYMPHOMA: Variants FOLLICULAR LYMPHOMA VARIANTS - Cutaneous follicular center lymphoma - Cutaneous diffuse large B-cell B lymphoma of leg - Diffuse follicular center lymphoma Grade 1: 0-50 centroblasts Grade 2: centroblasts


 & Presence of bcl-6")
19 IAP CASE 3 BNN DIAGNOSIS IAP CASE # 3 COMPOSITE LYMPHOMA: FOLLICULAR LYMPHOMA GRADE 3/3 WITH 20% FOLLICULARITY AND DIFFUSE LARGE B-CELL B LYMPHOMA IN 70% PLUS HODGKIN LYMPHOMA, NODULAR SCLEROSIS IN 10% In-situ Follicular Lymphoma Progression & Transformation Values & Limitations Of Immunostains Differential Diagnosis Variants Of Follicular Lymphoma Genetics Absence of t(14;18) & Presence of bcl-6 gene rearrangement
20 RECENT STUDIES IN FL HAVE CORRELATED PRESENCE & ABSENCE OF 1a) t(14;18)(q32;q21) & 1b) bcl- 2protein expression & 2a) bcl-6 gene rearrangement & 2b) bcl- 6protein expression WITH A) Pathologic findings B) Immunohistochemical findings C) Karyotypic features: duplications, deletions & breakpoints D) Clinical features, survival & progression FOLLICULAR LYMPHOMA: Molecular Variants t (14;18) present in 40 to 85%. Sole finding in 10% t(14;18) & bcl- 2protein absent in 15% t(14;18) absent, but bcl- 2protein seen in 8% t(14;18), bcl-6 gene & bcl- 6 protein present t(14;18) present, bcl-6 gene rearrangement present, but bcl- 6protein absent GENE EXPRESSION SIGNATURES PROVIDE PROGNOSTIC INFORMATION INDEPENDENT OF OTHER PARAMETERS MANTLE CELL LYMPHOMA (MCL): OUTLINE DEFINITION POSTULATED CELL OF ORIGIN MORPHOLOGY IMMUNOPHENOTYPE GENETICS CLINICAL GENE EXPRESSION PROFILES DEFINITION A B-cell B neoplasm of monomorphic small to medium- sized cells with irregular nuclei, absent to inconspicuous nucleoli and scanty cytoplasm. Neoplastic transformed cells (centroblasts and paraimmunoblasts) ) are absent. POSTULATED CELL OF ORIGIN Probably originating from primary follicles or mantle zone of secondary follicles. From peripheral B-cell B of inner mantle zone.
21 MORPHOLOGY: Outline PATTERNS: MANTLE CELL LYMPHOMA PATTERNS CYTOLOGY VARIANTS ONE LAYER: Mantle Cell Nodular Follicular Colonization TWO LAYER: Mantle Zone TWO LAYER: Inverse Follicular * THREE LAYER: Marginal Zone * Pattern Incidence(%) 1.Mantle zone 20 2.Fusion of mantle zones 40 3.Mantle cell nodular 20 4.Partial follicular colonization 30 5.Complete follicular colonization 30 6.Mild starry-sky sky pattern 20 7.Hyalinized vascular pattern of 20 small vessels * Multiple patterns usually coexist PATTERNS * IN MCL PATTERNS * IN MCL (cont.) Pattern Incidence(%) 8.Marginal zone pattern 1 9.Diffuse pattern a) Predominantly 10 b) Completely Inverse follicular pattern a) Mantle cells with clear cytoplasm 2 b) Marginal zone B-cell B differentiation 1 c) Blastoid transformation 2 * Multiple patterns usually coexist CYTOLOGIC SPECTRUM OF MCL 1. Round nuclei 2. Slightly to moderately irregular nuclei and scanty cytoplasm 3. Markedly irregular nuclei 4. Convoluted nuclei 5. Blastic/ Blastoid 6. Anaplastic/ Transformed 7. Mantle cells with clear cytoplasm 8. Mantle cell with marginal zone B-cell differentiation VARIANTS OF MANTLE CELL LYMPHOMA 1. Classical Blastoid Resembles Lymphoblastic 2. Pleomorphic Pleomorphic Blastoid Variant Large Cleaved; Rarely, Mixed Large Cleaved and Noncleaved 3. Small round cell - Resembles Small Lymphocytic Lymphoma (SLL)
.")


22 VARIANTS OF MANTLE CELL LYMPHOMA 4. Mantle cells clear cytoplasm a.mantle cell lymphoma with clear cytoplasm (CD5+ BCL-1+). b.mantle cell lymphoma with clear cytoplasm form small monomorphic nodules and may resemble proliferation centers of SLL or marginal zone B-cell B nodules. c.mantle cell lymphoma with marginal zone B-cell B differentiation (clear cells CD5-,, Bcl-1-). DIFFERENT EXAMPLES OF MCL 1. Well-Defined Mantle Zones & Round Cytology 2. Fusion Of Mantle Zones & Slightly Irregular Cells 3. Subtle, Multifocal Mantle Zone Pattern With Irregular Blastic Cytology 4. Completely Colonized Follicles & Round To Slightly Irregular Nuclei 5. Mild Starry-Sky Sky Pattern By Epithelioid Cells 6. Resembling Proliferation Centers & Hyalinized Vascular Pattern 7. Diffuse Pattern With Large Cleaved Cytology 8. Inverse Follicular, Marginal Zone, & Interfollicular Pattern With Blastoid Transformation 9. Multiple Lymphomatous Polyposis EXAMPLE OF MCL WITH Well-Defined Mantle Zones And Round Cytology




23 EXAMPLE OF MCL WITH Fusion Of Mantle Zones And Slightly Irregular Cells EXAMPLE OF MCL WITH Subtle, ubtle, Multifocal Mantle Zone Pattern With Blastic Cytology 2005
24





25 EXAMPLE OF MCL WITH Completely Colonized Follicles And Round Nuclei Variant: Resembling SLL CD21 CD21 Bcl-1




26 Bcl-1 EXAMPLE OF MCL WITH Mild Starry-Sky Sky Pattern By Epithelioid Cells EXAMPLE OF MCL WITH Resemblance to Proliferation Centers Seen in CLL/SLL And Hyalinized Vascular Pattern 2005
27 CD20





28 CD5 Bcl-1 Bcl-1 EXAMPLE OF MCL WITH Diffuse Pattern With Large Cleaved Cytology Variant: Pleomorphic Pleomorphic blastoid



29 CyclinD1 EXAMPLE OF MCL WITH Inverse Follicular, Marginal Zone, And Interfollicular Pattern With Blastoid Transformation IAP CASE 7 BNN CLINICAL HISTORY g A-65-year old male. g Right cervical lymphadenopathy. IAP CASE 7 BNN DIAGNOSIS g MANTLE CELL LYMPHOMA, BLASTOID VARIANT WITH MULTIPLE DISTINCTIVE PATTERNS
 CD43 + (95%) Cyclin D1 (bcl-1, PRAD1) + (70-90%) CD23")

 (q13;q32) translocation between")


..). 2.")

30 CD-20 CD-5 CD-21 Bcl-1 IMMUNOHISTOCHEMICAL STUDIES CD20 + (100%) CD5 + (90%) CD43 + (95%) Cyclin D1 (bcl-1, PRAD1) + (70-90%) CD23 + (2%) MOLECULAR BIOLOGY 1.Most cases show unmutated variable region genes indicative of pre-germinal cell B-cell origin. Few cases show somatic mutations. 2.By FISH all cases show t(11;14) (q13;q32) translocation between immunoglobulin heavy chain and the cyclin D1, genes and overexpression of cyclin D1 mrna. 3.Abnormalities in negative cell cycle proteins. 4.Blastoid shows different cytogenetic abnormalities: deletions, mutations, tetraploidy. PROGNOSTIC FACTORS 1. High mitotic activity (>2.5 per h.p.f.)..). 2. Blastoid cytology associated with aggressive behavior. 3. Poor prognosis associated with multiple cytogenetic abnormalities, complex karyotypes,overexpression or mutation of p Peripheral blood involvement but not bone marrow involvement associated with poor prognosis.
31 GENE EXPRESSION SIGNATURES GENE EXPRESSION PROFILES Diagnostic Tool Specific for Mantle Cell Lymphoma a) Cyclin D1 positive MCL b) Cyclin D1 negative MCL c) Both groups had same survival Prognostic Tool a) Survival inversely correlates with proliferation b) A model of only 4 proliferation signature genes (CDC2, ASPM, tubulin α,, CENP-F) highly predicted length of survival which could be grouped into 4 quartiles- 6.7, 3.3, 2.3, 0.8 yrs c) These 4 quartiles provide a continuous quantitative relationship between proliferation and survival, and, is a more superior method than morphology (blastic)) in predicting survival MARGINAL ZONE B CELL LYMPHOMA Extranodal, Nodal & Splenic Bharat Nathwani,, M.D. Professor of Pathology Chief, Hematopathology University of Southern California Keck School of Medicine Tel: (323) , FAX: (323) nathwani@usc.edu MARGINAL ZONE B CELL LYMPHOMA Extranodal, Nodal & Splenic OUTLINE gmarginal zone B-cell B lymphomas (MZBCL) gmalt MALT lymphoma - Morphology and imunophenotype - Differential Diagnosis gmolecular Pathogenesis gdifferences among MALT, Nodal, & Splenic Marginal Zone Lymphomas gmzbcl MZBCL in Children and Young Adults gatypical Marginal Zone B-cell B Hyperplasia of MALT gconclusions
32 CLASSIFICATION OF MARGINAL ZONE B CELL LYMPHOMA Extranodal Marginal Zone B Cell Lymphoma of MALT type (8%) Primary Nodal (2%) Primary Primary Splenic (<1%) EXTRANODAL MARGINAL ZONE B-CELL B LYMPHOMA OF MUCOSA-ASSOCIATED ASSOCIATED LYMPHOID TISSUE (MALT) TYPE MALT LYMPHOMA INCIDENCE 8% of NHL, & third most common NHL Up to 50% of primary gastric lymphomas In USA, between 1:30,000 and 1:80,000 of H.pylori- infected population have gastric MALT lymphoma Higher incidence of gastric MALT in North- East Italy (13 times higher than in UK) Middle East Cape region of South Africa PRECURSOR LESIONS/ CONDITIONS Chronic inflammatory / autoimmune disorders In MALT lymphoma, the prevalence of H.pylori infection is 90% Sjögren syndrome 44 fold risk increase Hashimoto thyroiditis 70 fold risk increase PRECURSOR LESIONS/CONDITIONS (cont.) Hepatitis C? increased risk of nodal, splenic,, salivary gland Follicular bronchiolitis Borrelia burgdorferi (Lyme disease agent) higher risk of MALT lymphoma of skin in Europe Campylobacter jejuni associated with IPSID MARGINAL ZONE B-CELLS OF MALT TYPE LYMPHOMA ARE DIFFERENT THAN BENIGN MONOCYTOID B-CELLS
33 IMMUNOPHENOTYPE OF MALT LYMPHOMA q CD20 +ve+ ve,, monotypic plasma cells (35%) q CD5 or CD10 positive (rarely), q IgD +ve in 20% of children & young adults q CD43 positive in benign B-cells, B children naïve marginal zone B-cells, B salivary gland MESA (42%) Summary: Compared to other low-grade B-cell B NHL (follicular, small lymphocytic,, mantle cell), there is no specific immunophenotype for marginal zone B cell lymphoma DEFINITION OF MALT LYMPHOMA Morphologically heterogeneous: - Marginal zone B cells with scanty cytoplasm - Marginal zone B cells with moderate to abundant cytoplasm resembling monocytoid B cells - Scattered transformed cells - Monoclonal plasma cells in 35% Infiltrate: - In the marginal zone of reactive follicles and extends into the interfollicular region - Lymphoepithelial lesions MORPHOLOGY OF MALT LYMPHOMA Non-neoplasticneoplastic component Neoplastic component Patterns Cytology Transformation Differential Diagnosis NON-NEOPLASTIC COMPONENT IN MALT LYMPHOMA Non-neoplasticneoplastic component may be multifocal or predominant: Reactive follicles seen in >90% of cases Few to predominating Atrophic or hyperplastic With or without mantle zones Neutrophils Polyclonal plasma cells PATTERNS OF MALT LYMPHOMA: Complete marginal zone pattern Other patterns: Inverse follicular, follicular colonization, interfollicular, & sinus in lymph node Large confluent areas Lymphoepithelial lesions (LEL)

34 CD20 bcl-2 Kap Kap
35 FOLLICULAR COLONIZATION PLASMACYTIC DIFFERENTIATION IN INTERFOLLICULAR AREAS
36
37 PLASMACYTIC DIFFERENTIATION WITHIN FOLLICLES AND INTERFOLLICULAR AREAS Kap Kap




38 Kap CYTOLOGIC FEATURES of MALT LYMPHOMA Cytologic Spectrum: Size: small to medium Nucleus slightly irregular, nucleoli not prominent Cytoplasm: scanty to abundant, pale to lightly eosinophilic Monoclonal plasma cells and plasmacytoid forms in 35% Scattered malignant transformed cells TRANSFORMATION Histologic Criteria: - Monomorphic clusters &/or islands of large cells - >20% large cells that are not in clusters and/or islands



39 DIFFERENTIAL DIAGNOSIS The Marginal Zone is the Margin (interface) between the B-cell and the T-cell zones. And it contains different types of B-cells, T-cells and other cell types. Therefore, these cell types can sometimes produce a marginal zone pattern. DIFFERENTIAL Dxs OF MARGINAL ZONE &/OR INVERSE FOLICULAR PATTERN Diseases/ cells producing marginal zone &/or inverse follicular pattern Probability present Marginal zone lymphoma (MZL) Follicular lymphoma with marginal zone B- cell differentiation Small lymphocytic lymphoma Mantle cells that look like MZBC Mastocytosis All others* * (Plasmacytoma,, benign monocytoid B-cells, LP lymphoma, peripheral T-cell T lymphoma, benign small T-cells, T benign plasma cells, metastatic carcinoma, FL surrounded by benign T-cells) T 75% 10% 5% 5% 5% 1% each FOLLICULAR LYMPHOMA WITH INVERSE FOLLICULAR PATTERN




40 Follicular Lymphoma with Marginal Zone B-cell Differentiation CD20 bcl-2 CD10 bcl-6 FOLLICULAR LYMPHOMA WITH MARGINAL ZONE PATTERN

41 Role of Immunoglobulin Gene Rearrangement in the Diagnosis of MALT Lymphoma DIAGNOSIS OF GASTRIC MALT LYMPHOMA BY IMMUNOGLOBULIN GENE REARRANGEMENT - PCR Ig gene rearrangement can detect 70 to 80% of abnormal clones - 30% cases of overt lymphoma can be negative - False positivity reported in cases with only chronic gastritis or with no histologic evidence of lymphoma after antibiotic- induced regression of lymphoma - SUMMARY: Diagnosis of MALT lymphoma should be made only on histological evidence of or strong suspicion for MALT lymphoma, NOT on the basis of clonality alone
42 GENETIC ALTERATIONS: TYPES MOLECULAR BIOLOGY of MALT LYMPHOMA 1. NUMERICAL ABNORMALITIES (ANEUPLOIDY) 2. RECURRENT BALANCED TRANSLOCATIONS 3. OTHER GENETIC ALTERATIONS: Types & Frequencies 1. NUMERICAL ABNORMALITIES Trisomy 3 found in 12-85% Trisomy 7 found in 3-15% 3 Trisomy 12 found in 3-38% 3 38% Trisomy 18 found in 7-36% 7 GENETIC ALTERATIONS: Types & Frequencies 2. RECURRENT BALANCED TRANSLOCATIONS: - t(11;18)(q21;q21) found in 16% - t(14;18) found in 18% - t(1;14)(p22;q32) found in < 5% - t(3;14)(p14.1;q32) found in 9% NF- κb Activation GENETIC ALTERATIONS: Types & Frequencies 3. OTHER MUTATIONS (associated with transformation &/or progression) c-myc somatic mutation (16%); p53 allele loss (7%) and mutation (19%) (In MALT + DLBCL p53 allele loss in 29% & p53 mutation in 33%) p15/16 inactivation (rare) FAS (APO1 or CD95) mutation (frequently) Microsatellite instability (rare) Involvement of MALT1 Gene in Translocations that Activate the NF- κb 1. NF- κb Pathway Activated - t(11;18)(q21;q21) found in 16% - t(14;18) found in 18% - t(1;14)(p22;q32) found in < 5% 2. NF- κb Pathway Not Activated - t(3;14)(p14.1;q32) found in 9%
43 MALT1 Gene Product is Involved in 3 of 4 Translocations t(1;14) t(14;18) t(11;18) IgH-BCL10 IgH-MALT1 API2-MALT1 Upregulation of Bcl-10 Binds to normal partner, MALT1 Upregulation of MALT1 Binds to normal partner, Bcl-10 Constitutive activation of IKK Novel fusion protein (API2-MALT1) Constitutively active protein Constitutive activation of NF-κB Pathway Sites of Involvement for the 3 Types of Translocations that Activate the NF-κB Pathway 1. t(11;18) is detected overall in 16% (67 of 417) (Ye H. et al, Blood 2003: 102: ): -- Most frequent in lung (38%) & stomach (24%) (usually sole abnormality) -- Moderately frequent in conjunctiva (19%) & orbit (14%) -- Absent in liver, skin, thyroid, IPSID & other sites 2. t(14;18)(q32;q21) detected overall in 18%: -- Only in liver, skin, ocular, & salivary gland (additional abnormalities not uncommon). 3. t(1;14) in < 5% of gastric & pulmonary MALT lymphomas. t(3;14) (p14.1;q32) Translocation Involving IgH & FOXP1 in 8 of 90 (9%) of MALT Lymphoma* Ocular Ocular adnexa 4 of 20 (20%) ThyroidThyroid 2 of 5 (40%) SkinSkin 2 of 20 (10%) Not Not seen at any other extranodal sites or in nodal or splenic Not Not found in association with any other translocations t(11;18), t(14;18), t(1;14) *7 of 8 harbored additional genetic abnormalities such as +3. RT-PCR showed up-regulation of FOXP1 in those with t(3;14) or trisomy 3. Clinical Significance of the t(11;18) Translocation Streubel B et al., ASH. Abstract 550 Clinical Significance of t(11;18)(q21;q21) in MALT Lymphoma Overall found in 16%, but found in 24% of gastric MALT lymphomas Found exclusively in extranodal MALT Not found in any other benign or malignant process Gastric MALT with t(11;18) fail to respond to H. pylori treatment Transformation to a diffuse large B-cell B lymphoma is rare Stage of Gastric MALT Lymphoma with t(11;18) Correlates with Nuclear Expression of Bcl- 10 Extent of disease Confined to stomach Local lymph node involvement Disseminated # of cases with nuclear Bcl-10 expression 38% 78% 93% Liu H, et al. Blood 98: , 2001

44 Role of H. pylori in Pathogenesis of MALT and MALT lymphoma CLINICAL SIGNIFICANCE OF H. PYLORI IN GASTRIC MALT LYMPHOMA Most Most patients with H. pylori infection do not develop lymphoma H. H. pylori present in almost all cases of chronic gastritis which lead to MALT H. H. pylori decreases as lymphoma progresses Eradication of H. pylori with antibiotics results in regression of lymphoma in 75% of cases CLINICAL SIGNIFICANCE OF H. PYLORI IN GASTRIC MALT LYMPHOMA (cont d) Re-infection with H. pylori may be associated with relapse of lymphoma About About 25% of patients with MALT lymphoma do not respond to treatment used for eradicating H. pylori, especially those whose lymphoma extends beyond submucosa H. H. pylori eradication fails in patients with t(11;18), Bcl-10 positivity or advanced MALT lymphoma OTHER PREDICTORS OF POOR RESPONSE TO ANTIBIOTIC THERAPY Proximal location Infiltration beyond the mucosa layers Presence of high-grade lymphoma component Perigastric node enlargement (by endoscopy with ultrasound or computed tomography) MARGINAL ZONE B CELL LYMPHOMA Extranodal Marginal Zone B Cell Lymphoma of MALT type (8%) Primary Nodal (2%) Primary Primary Splenic (<1%) Steinbach 1999, Ruskone-Fourmestraux 2001, Sackmann 1997, Neubauer 1997, Du 2000
45 Comparison of MALT, Nodal & Splenic Marginal Zone B-Cell Lymphomas Molecular & Cytogenetic Immunohistochemical Clinical COMPARISON OF CYTOGENETIC FINDINGS Comparison of Cytogenetic Abnormalities Genetic Abnormality t(11;18)(q21;q21) t(14;18)(q32;q21) t(1;14)(p22;q32) Trisomy 3 Deletion 7q p53 anomalies Other abnormalities MALT 35% 18% <5% 15-70% No Yes del17p, +7, +12, +18, +11q, etc. Nodal No No No Up to 60% Rare Not reported der1p/q, +7, +12, +18 Splenic No No No 15-55% 55% Up to 42% Yes t(11;14), +18, t(9;14), t(6;14) COMPARISON OF IMMUNOHISTOCHEMICAL FINDINGS Comparison of Immunohistochemical Results Comparison of Immunohistochemical Results Immunostain CD5 CD43 CD38 BCL2 BCL-6 Bcl-10 p27 p16 MALT Neg. Var. Pos. Neg. Pos/Neg Neg. Nodal Neg. 46% Pos. 42% Pos. Pos. Neg. Neg. 92% Pos. Pos. Splenic Neg. Neg. Pos. Neg. Neg. Var. Immunostain MALT Nodal IgD 20 % Pos* 35% Pos. IgG Few Pos. 33% Pos. Cyclin D3 48% Pos. Cyclin E** 41% Pos. Caspase 3a 75% Pos. Survivin 88% Pos. * In 20% of children & young adults Splenic Pos. Few Pos. Neg. Neg.
46 COMPARISON OF CLINICAL FINDINGS Clinical Characteristics: Comparing MZBCLs Parameter Frequency B symptoms Advanced Stage Bone marrow Central Nodes Peripheral Nodes Blood - positive IPI = yr Overall Survival 5 yr Failure Free Surv MALT 7-8% of NHL 14% 34% 15-20% 24% 8% Rare 10% 81-86% 86% 65% Nodal 1.8% of NHL 17% 71% 28-43% >56% 100% Rare 9-17% 55-79% 22-29% 29% Splenic <1% of NHL Rare Up to 95% 95% 28% 17% 65% 15% 65-78% Marginal Zone Lymphoma (MZL) in Children & Young Adults MARGINAL ZONE B-CELL LYMPHOMA IN CHILDREN & YOUNG ADULTS L Taddesse-Heath, et al., Am J Surg Pathol 2003; 27: Parameter Incidence Median age Cases 18 years Overall M:F M:F 18 years Common site Autoimmune disease Monoclonality Nodal MZL 32 patients 67% 16 (2-27) 27) 66% 5.4:1 20:1 Cervical None 94% * Only one patient had involvement of the stomach. Extranodal MZL 16 patients* 33% 25 (9-29) 25% 1.2:1 1:1 Ocular adnexa 19% 94% Parameter Stage I Excision only Local radiation Chemotherapy Median follow-up Marginal Zone Lymphoma (MZL) in Children & Young Adults Nodal MZL 32 patients 90% 68% 18% 11% 6 months (1-60) Extranodal MZL 16 patients 73% 22% 56% 22% 3 months (1-24) ATYPICAL MARGINAL ZONE B-CELL HYPERPLASIA OF MALT: A REACTIVE CONDITION OF CHILDHOOD SHOWING IMMUNOGLOBULIN LAMBDA LIGHT CHAIN RESTRICTION Attygale AD et. al., Blood ; 104 :

, but control tonsils positive Genotypes of Marginal Zone B-cells Somatic Mutations: - Unmutated (naïve B-cells); control tonsils mutated")
47 OCCURENCE & SITE OF ORIGIN OF THIS ENTITY Occurs in sites where there is Native MALT Tissue (Tonsils and Peyer s Patches) Origin is likely to be from the Marginal zone B-cell that is: - Unmutated - CD27 negative - CD43 positive Histologic Features Follicles: - Hyperplastic germinal centers Marginal Zones: - Expanded & produce marginal zone pattern: Marginal zone B cells Transformed cells Follicular colonization Lymphoepithelial lesions Immunophenotype of Marginal Zone B-Cells - Positive: CD20, bcl-2, IgM, IgD(weak), CD43, ITRA-1, Ki67, CD21, (like in normal control tonsils) - Light chain restriction: Lambda - Negative: CD27(naïve B-cells), but control tonsils positive Genotypes of Marginal Zone B-cells Somatic Mutations: - Unmutated (naïve B-cells); control tonsils mutated Usage of VH Family: - No biased usage Immunoglobulin Heavy and Light Chain Gene Rearrangements: - Absent, like in control tonsils


48 CD20 Ki67 CD3 Bcl-2 IgD IgM Kap Lam IgD IgM Kap Lam



49 CONCLUSIONS 1. Extranodal MALT lymphomas have at the bare minimum three molecular pathways of development & probably several more 2. The data presented here show that extranodal,, nodal, & splenic marginal zone B-cell lymphomas are - morphologically similar, but different clinically & genetically 3. In addition, primary nodal marginal zone B-cell lymphoma in children & young adults is probably a distinct entity 4. Atypical marginal zone B-cell B hyperplasia of MALT can be mistaken for MALT lymphoma IAP CASE 9 BNN DIAGNOSIS g EXTRANODAL MARGINAL ZONE LYMPHOMA OF MALT TYPE (in the left salivary gland) CASE 9 SHOWN TO ILLUSTRATE Current criteria of MALT lymphoma in the salivary gland require: Confluence of marginal zone cells and/or Light chain restriction in paraffin sections, not by immunoglobulin gene rearrangement studies. Both criteria are fulfilled in this case.

 with moderate cytoplasm (b)")

50 IAP CASE 12 BNN DIAGNOSIS NODAL MARGINAL ZONE B-CELLB LYMPHOMA IAP CASE 12 BNN MORPHOLOGIC FEATURES Marginal zone B cells produce inverse follicular, marginal zone, interfollicular and sinus patterns. Marginal zone B cells are of two types: (a) with moderate cytoplasm (b) with scanty cytoplasm IAP CASE 12 BNN IMMUNOSTAINS RESULTS Both types of marginal zone B cells positive for CD20, bcl-2, lambda. Negative for CD3, CD43, kappa.


, IgM,, kappa,")
51 CD20 bcl-2 IAP CASE 10 BNN DIAGNOSIS MARGINAL ZONE B CELL LYMPHOMA WITH FOLLICULAR COLONIZATION AND PLASMACYTIC DIFFERENTIATION CASE 10 SHOWN TO ILLUSTRATE Granulomatous component can be massive in a lymphoma. It is found in lymphoplasmacytic and marginal zone B-cell lymphoma. Lymphomatous component may be very small and readily overlooked Importence of careful review of all components. Value of flow and immunostains. IAP CASE 10 BNN IMMUNOSTAIN RESULTS gpositive for CD20, bcl-2, bcl-6 6 (some), IgM,, kappa, and CD23 (FDRCs( FDRCs) gnegative for CD5, CD23, CD10, CD43, CD3, lambda.





52 CD21 CD21 CD21 MORPHOLOGY: Outline CHRONIC LYMPHOCYTIC LEUKEMIA/SMALL LYMPHOCYTIC LYMPHOMA (CLL/SLL) CRITERIA PATTERNS CYTOLOGY TRANSFORMATION DIFFERENTIAL DIAGNOSIS

53 PATTERNS OF CLL/SLL Pseudofollicular (Pseudofollicular proliferation growth centers) (Proliferation centers) Seen in 99% of SLL, 30% of lymphoplasmacytoid,, but not lymphoplasmacytic lymphomas Not seen normally, and not seen in any other lymphoma. PSEUDOFOLLICULAR PATTERN (PSEUDOFOLLICULAR GROWTH CENTERS) Low magnification Spherical (ball-like) like) structures Pale staining Always poorly defined Never surrounded by a mantle cell (mantle zone) layer High Magnification Cells loosely packed together with clear spaces often separating cells All cells round Prolymphocytes (cells with one centrally placed prominent nucleolus) present in variable numbers SMALL LYMPHOCYTIC LYMPHOMA PATTERNS Pseudofollicular (throughout or focal) Reactive follicles & pseudofollicular Pseudofollicles Completely surround naked benign germinal centers and form an inverse follicular pattern Completely surround benign follicles as a third layer and form the marginal zone pattern Reactive follicles, pseudofollicles,, inverse follicular, and marginal zone coexist Diffuse very rare DIFFERENT EXAMPLES OF SLL/ CLL 1) Mostly Vague Pseudofollicles And Round Cytology 2) Vague And Well-Defined Pseudofollicles And Round Cytology 3) Vague Pseudofollicles And Moderate Nuclear Irregularities 4) Vague Pseudofollicles And Many Prolymphocytes 5) Pseudofollicles And Reactive Follicles With Follicular Colonization 6) Pseudofollicles Producing A Marginal Zone Pattern (case 5) EXAMPLE OF SLL/ CLL WITH Mostly Vague Pseudofollicles And Round Cytology




54 EXAMPLE OF SLL/ CLL WITH Vague And Well-Defined Pseudofollicles And Round Cytology EXAMPLE OF SLL/ CLL WITH Vague Pseudofollicles And Moderate Nuclear Irregularities


55 EXAMPLE OF SLL/ CLL WITH Vague Pseudofollicles And Many Prolymphocytes

56 EXAMPLE OF SLL/ CLL WITH Pseudofollicles And Reactive Follicles With Follicular Colonization

 IAP CASE 5 BNN- 14113")


57 EXAMPLE OF SLL/ CLL WITH Pseudofollicles Producing A Marginal Zone Pattern (case 5) IAP CASE 5 BNN DIAGNOSIS SMALL LYMPHOCYTIC LYMPHOMA WITH INVERSE FOLLICULAR AND MARGINAL ZONE PATTERNS PRODUCED BY PSEUDOFOLLICLES



58 CD20 CD3 CD23 IgD CD5 CD43 CD23 IgD SLL/CLL with Transformation to Diffuse Large B-Cell B Lymphoma (DLBCL)




59 SLL/CLL Progressing To Hodgkin Lymphoma IAP CASE 8 BNN DIAGNOSIS SMALL LYMPHOCYTIC LYMPHOMA WITH TRANSFORMATION TO HODGKIN LYMPHOMA
60
 1.")


 IMPORTANCE OF ACCURATE IDENTIFICATION OF PSEUDOFOLLICULAR")




61 CD20 CD3 CD15 CD30 CD3 CD3 CD15 CD30 CYTOLOGY Predominance of cells Small (> normal lymphocytes) 1. Clumped chromatin, round nucleus, rare small nucleoli 2. Very rare mitoses Pseudofollicles cellular composition 1. Small 2. Prolymphocytes small, medium and large cells with single centrally located prominent nucleolus 3. Paraimmunoblasts medium, large sized cells with multiple nucleoli (transformed cells) IMPORTANCE OF ACCURATE IDENTIFICATION OF PSEUDOFOLLICULAR PATTERN 1. Failure to identify pseudofollicular pattern A. Diffuse mixed cell lymphoma 2. Misidentification of pseudofollicular pattern as follicular pattern A. Follicular small lymphocytic B. Follicular mixed C. Follicular large cell 3. Clinicopathologic correlations A. Low grade B. Similarities to CLL PLASMACYTOID DIFFERENTIATION IN SLL Monoclonal plasma cells 1. Intracytoplasmic monoclonal immunoglobulin in small cells or small cells with plasmacytoid features. Such cases have proliferation centers and are called lymphoplasmacytoid lymphoma. TRANSFORMATION of CLL/SLL > 30% Large cells > 30% B-immunoblastsB > 30% Prolymphocytes (in tissue sections) > 55% Prolymphocytes (in blood) Blastic Hodgkin's like (scattered cells) Hodgkin (discrete areas with phenotype)
 CD43 + (95%) CD11c + (weak) IgM + IgM & IgD + cig+ + (5%) PROGNOSTIC CATEGORIES IN CLL")


62 IMMUNOSTAINS POSITIVE NEGATIVE CD20 + CD3 CD79a + CD10 - CD5 + (85%) Cyclin D1 (90%) CD23 + (85%) CD43 + (95%) CD11c + (weak) IgM + IgM & IgD + cig+ + (5%) PROGNOSTIC CATEGORIES IN CLL MEDIAN SURVIVAL MEDIAN SURVIVAL 25 yrs 8-10 yrs Mutational Status of IgVH gene Mutated Unmutated CD38 Expression Not Increased Increased 13q Deletion Yes No 17p Deletion No Yes 11q Deletion No Yes ZAP-70 Increased No Yes p53 Defects Present Absent IAP CASE 4 BNN DIAGNOSIS gcomposite LYMPHOMA: FOLLICULAR LYMPHOMA GRADE 2/3 WITH 100% FOLLICULARITY PLUS SMALL LYMPHOCYTIC LYMPHOMA

63 LYMPHOPLASMACYTIC LYMPHOMA (LPL)/ WALDENSTROM MACROGLOBULINEMIA (WM) LYMPHOPLASMACYTIC LYMPHOMA(LPL)/ WALDENSTROM MACROGLOBULINEMIA(WM) Definition A neoplasm of small B lymphocytes, plasmacytoid lymphocytes and plasma cells, usually involving bone marrow, lymph nodes and spleen, usually CD5- Has a monoclonal protein with hyperviscosity due to heavy chain IgM or cryoglobulinemia. CELLS OF ORIGIN A typical WM Derived from a B cell that has undergone somatic mutation prior to transformation, at a point where isotype switch events have not been initiated. LPL AND WM MORPHOLOGY Many B-cells B lymphomas show maturation to plasmacytoid or plasma cells containing cytoplasmic immunoglobulin (B-cell CLL, MZBCL, and FL). LPL is restricted to tumors that lack features of other lymphomas. WM consists of small lymphocytes with a variable degree of plasma cell maturation. IAP CASE 6 BNN DIAGNOSIS LYMPHOPLASMACYTIC LYMPHOMA



64 DIFFUSE LARGE B CELL LYMPHOMA (DLBCL) DLBCL: VARIANTS AND SUBTYPES Diffuse large B-cell B lymphoma Variants: - Centroblastic - Immunoblastic - Plasmablastic - T-Cell or Histiocyte Rich Large B-CellB - Anaplastic Large B-CellB - With Expression of Full-length length ALK Mediastinal Intravascular Primary Effusion Lymphoma Lymphomatoid Granulomatosis MORPHOLOGIC VARIANTS OF DLBCL Centroblastic Immunoblastic Plasmablastic T-Cell or Histiocyte Rich Large B-CellB Anaplastic Large B-CellB With Expression of Full-length length ALK
 - Secondary (progression or transformation")


65 MORPHOLOGIC VARIANTS OF DLBCL CENTROBLASTIC - Primary (de novo) - Secondary (progression or transformation from other lymphomas such as SLL/CLL, Lymphoplasmacytic, Follicular, Marginal Zone, NLP Hodgkin) DIFFUSE LARGE B-CELL LYMPHOMA MORPHOLOGIC VARIANT: IMMUNOBLASTIC DIFFUSE LARGE B-CELL LYMPHOMA MORPHOLOGIC VARIANT: PLASMABLASTIC

66 PLASMABLASTIC A rare subtype with distinctive features Oral lesions in HIV+ individuals Large cells with abundant basophilic cytoplasm and paranuclear hof. EBV+ 50%, HHV8- Progression of multicentric Castleman s disease HIV+, HHV8+, EBV- CD20-,, CD45-,, CD79-/+, VS38+, CD138+, MUM-/+, cytoplasmic IgG in some cases High proliferative rate, absence of mature monoclonal plasma cells PLASMABLASTIC MORPHOLOGY Plasmablastic Myeloma and Plasmacytoma ALK+ Large B-Cell B Lymphoma Primary Effusion Lymphoma Immunoblastic Lymphoma arising in immunosuppressed patients DIFFUSE LARGE B-CELL LYMPHOMA MORPHOLOGIC VARIANT: T-CELL & HISTIOCYTE RICH LARGE B-CELL B LYMPHOMA (TC&HRLCL) MORPHOLOGY OF TC&HRLCL B large neoplastic lymphoid cells in minority (<10%) Non-neoplastic neoplastic small T lymphocytes predominate. Pattern diffuse and no residual nodularity. Sinuses often completely obliterated. Epitheloid cells and/or histiocytes often present. MORPHOLOGY OF TC&HRLCL The neoplastic large cells may appear like centroblasts, immunoblasts,, or they may be multi-lobated lobated or polypoidal and resemble L and H variants or other variants of Sternberg-Reed cells. Small B-cells B are rare.

67 T-CELL & HISTIOCYTE RICH LARGE B-CELL LYMPHOMA: MORPHOLOGIC VARIANTS 1. Lymphocytic & Histiocytic-like: 14 cases 2. Centroblasts or Immunoblasts: : 10 cases 3. Reed-Sternberg cell-like: like: 6 cases Megan LS et al. Am J Surg Pathol 26: , 1466, 2002 COMPARISON OF THREE MORPHOLOGIC VARIANTS OF T-CELL & HRLCL Antibody CD20 CD30 CD15 EMA Bcl-2 Bcl-6 CD10 EBER Bcl-2 2 PCR VJ PCR Median Age/ % Males Centroblastic 100% 20% 0% 1% 6% weak, few cells 90% (1 to 2+) 20% 33% 10% 40% clonal 73; 50% Lympho & Histio 100% 28% 0% 7% 57% 10%, few cells 100% (1 to 2+) 50% 0% 14% 46.5; 71% Reed-Sternberg 100% 50% 0%; CD % 33%; EBER+ 33% but Bcl-6-0% 50% (1+) 16% 80% 0% 50% 56.5; 83% COMPARISON OF THREE MORPHOLOGIC VARIANTS OF T-CELL & HRLCL Antibody CD20 CD30 CD15 EMA Bcl-2 Centroblastic 100% 20% 0% 1% 6% weak, few cells Lympho & Histio 100% 28% 7% 57% 10%, few cells Reed-Sternberg 100% 50% 0%; CD % 33%; EBER+ 33% but Bcl-6-0% COMPARISON OF THREE MORPHOLOGIC VARIANTS OF T-CELL & HRLCL (cont.) Antibody Bcl-6 CD10 EBER Bcl-2 2 PCR VJ PCR Median Age/ % Males Centroblastic 90% (1 to 2+) 20% 33% 10% 40% clonal 73; 50% Lympho & Histio 100% (1 to 2+) 0% 50% 0% 14% 46.5; 71% Reed-Sternberg 50% (1+) 16% 80% 0% 50% 56.5; 83% DIFFUSE LARGE B-CELL LYMPHOMA MORPHOLOGIC VARIANT: ANAPLASTIC LARGE CELL LYMPHOMA (ALCL)




 GROUP AND NON-GCB")

 3.")
68 CD20 CD20 CD30 CD30 IMMUNOSTAINING IN DLBCL WITH EXPRESSION OF FULL-LENGTH ALK CD30-,, CD45+ (weakly), CD20-,, CD79a+/-, VS38- ALK-1+ (granular cytoplasmic and dot-like in the Golgi) Most show t(2;17)(p23;q23) with fusion of ALK and Clathrin Heavy Chain gene Rare cases show t(2;5) with NPM/ALK ciga with light chain restriction CD57+*, CD4+* *Lack other B or T associated antigens GERMINAL CENTER B-CELL-LIKE (GCB) GROUP AND NON-GCB GROUP HAVE SIGNIFICANTLY DIFFERENT: 1. Gene expression profiles 2. Immunohistochemical profile (CD10, Bcl-6, MUM-1, Bcl-2, CyclinD2) 3. Overall and Failure free survival CP Hans et al. Blood 103: ,

69 Parameter 5 yr OS% p value 5 yr EFS% p value CD10 - Negative Positive Bcl-6 - Negative 30 < Positive MUM-1 - Negative Positive Cyclin D2- Negative < Positive 4 7 <0.001 TMA- GCB < Non GCB IPI Score < <0.001 TMA= Tissue microarray; IPI= International Prognostic Index; OS= Overall Survival EFS= Event Free Survivall CP Hans et al. Blood 103: , CONCLUSIONS 1. Expression of Bcl-6 6 or CD10 was associated with better OS 2. Expression of MUM-1 1 or Cyclin D2 was associated with worse OS 3. GCB group (42%) was CD10 +, Bcl-6 6 +, MUM-1 4. Non GCB group (58%) was CD10 -,, Bcl-6 -,, MUM In the Non GCB group, Bcl-2 2 and Cyclin D2 were associated with poor survival 6. In multivariate analysis, high IPI (3-5) and Non GCB phenotype indicated poor prognosis (p < ) 7. Immunostains and cdna microarray predict similar survival information OS= Overall Survival p <0.001 CP Hans et al. Blood 103: , DLBCL IMMUNOPHENOTYPE CD45+, CD20+, CD79a+ (may lack any of them) Surface or cytoplasmic Ig+ + in 50-75% (IgM>IgG>IgA) CD43+ in 30% and CD5+ in < 10% CD5+ may arise de novo (bcl-1-) Bcl-6+ in 37%, many with extranodal involvement and more favorable prognosis. CD10+ in 25-50% 50% BCL-2 2 in 30-50% Ki67 > 40% POOR PROGNOSTIC FACTORS OF DLBL 4 or 5 adverse risk factors in IPI Ki67 > 80% Cytotoxic CD8+ T-cells T < 6% Loss of HLA class I or II antigens Loss of LFA-1 1 and/or ICAM-1 Loss of CD22 Bcl-2 2 protein + p53 gene mutation DIFFUSE LARGE B-CELL LYMPHOMA PRIMARY MEDIASTINAL (THYMIC) LARGE B-CELL B LYMPHOMA (PMLCL)


70 CD20 MORPHOLOGY OF PRIMARY MEDIASTINAL (THYMIC) LARGE B-CELL LYMPHOMA 1. Pattern and Architectural Features Sclerosis is often prominent, and it is often finely trabecular producing compartmentalization. Diffuse pattern. Sinuses are usually completely obliterated. MORPHOLOGY OF PRIMARY MEDIASTINAL (THYMIC) LARGE B-CELL LYMPHOMA 2. Cytologic Features The large neoplastic cells may be cleaved, non-cleaved or multi-lobated lobated. The neoplastic cells often have abundant clear to pale staining cytoplasm. IMMUNOSTAINING OF PRIMARY MEDIASTINAL (THYMIC) LARGE B-CELL LYMPHOMA CD20+ CD23+ 70% MAL+ (Myelin( and lymphocyte protein) CD30+ (weak), may be focal or extensive staining in 70% CD45+ CAM +/- CD21- Immunoglobulin (Ig( Ig) -/+ PRIMARY MEDIASTINAL (THYMIC) LARGE B-CELL LYMPHOMA MAL protein * An integral membrane protein, a component of enriched membrane microdomains,, called lipid rafts Normally expressed in lymphoid cells derived from T-cell T lineage: Thymus, PB T-cells, T CD4 + helper, CD8 + cytotoxic mature T cell clones, leukemic T- cell lines Not expressed in B-cell B lineage * Mod Pathol 2002; 15:



71 MAL IN PRIMARY MEDIASTINAL (THYMIC) LARGE B-CELL LYMPHOMA HISTOLOGY PMLCL Non-mediastinal DLBCL Burkitt s lymphoma Plasmacytoma/Myeloma T lymphoblastic chodgkin Lymphoma MAL EXPRESSION * 70% 3% 0% 60% 83% 10% DEFINITION OF INTRAVASCULAR LARGE B-CELL LYMPHOMA A rare subtype of extranodal DLBCL characterized by the presence of lymphoma cells only in the lumina of small vessels, particularly capillaries CD20 IAP CASE 14 S DIAGNOSIS DIFFUSE LARGE B-CELL B LYMPHOMA, IMMUNOBLASTIC VARIANT





72 IAP CASE 2 BNN DIAGNOSIS DLBCL, anaplastic variant with sinus involvement and follicular colonization thus resembling follicular lymphoma

73 BURKITT S LYMPHOMA (BL)

74 BURKITT S LYMPHOMA (BL): DEFINITION A highly aggressive lymphoma often presenting in extranodal sites or as an acute leukemia. Composed of monomorphic medium-sized B-cells with basophilic cytoplasm and numerous mitoses. Translocation involving MYC is a constant genetic feature Epstein-Barr (EBV) is found in a variable proportion of cases BURKITT S LYMPHOMA Clinical variants Endemic Non-Endemic Non-Endemic with immunodeficiency BL VARIANTS With plasmacytoid differentiation More common in immunodeficient state, may be in children Certain degree of pleomorphism in nuclear size and shape Cytoplasm is eccentric and basophilic with central single nuclei Atypical Burkitt/Burkitt-like Mib-1 1 nearly 100% Greater pleomorphism in nuclear size and shape Nucleoli are prominent and fewer in number Proven or with a strong presumptive evidence of MYC translocation BURKITT S LYMPHOMA Immunostains CD20+ CD10+ Bcl-6+ Ki-67 > 99% of cells+ Bcl-2- CD43+ BURKITT S LYMPHOMA Cytogenetics t(8;14) (75-85%), t(2;8) (5%), or t(8;22) (10%) translocation found. In endemic cases,, the translocation t(8;14) occurs in pre B-cell. B In nonendemic cases,, the translocation occurs at a later stage of B-cell B development. p53 mutation in up to 30% of sporadic and endemic cases Molecular Biology C-myc rearranged. EBV Latency I: expression of EBNA1 only, but not EBNA2-4 4 or LMP-1


75 IAP CASE 13 BNN CLINICAL HISTORY A 31-year-old HIV + male. IAP CASE 13 BNN DIAGNOSIS BURKITT LYMPHOMA. Testicular mass. CASE 13 SHOWN TO ILLUSTRATE The typical pattern and cytologic features of Burkitt lymphoma. A typical Burkitt lymphoma can be sometimes bcl-2+. HIV+ Burkitt lymphoma has a cytologic spectrum. Conclusions Morphology is even more important now than ever before, especially in this era of proteomics and genomics. Morphologic differential diagnosis dictates further diagnostics workup. The integretive approach of the WHO classification is very useful in establishing correct diagnosis, reducing errors and is necessary in reducing health care cost.
FOLLICULARITY in LYMPHOMA
 FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
Small B-cell (Histologically Low Grade) Lymphoma
 Lymphoma") Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
11/8/2018 DISCLOSURES. I have NO Conflicts of Interest to Disclose. UTILTY OF DETECTING PATTERNS
 Bharat N. Nathwani, M.D. City of Hope Medical Center Professor, Director of Pathology Consultation Services, 1500 East Duarte Road, Duarte, California, 91010 DISCLOSURES -------------------------------------------------------
Bharat N. Nathwani, M.D. City of Hope Medical Center Professor, Director of Pathology Consultation Services, 1500 East Duarte Road, Duarte, California, 91010 DISCLOSURES -------------------------------------------------------
LYMPHOMAS an overview of some subtypes of NHLs
 One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Many of the hematolymphoid disorders are derived
 REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
Contents. vii. Preface... Acknowledgments... v xiii
 Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Pathology of the indolent B-cell lymphomas Elias Campo
 Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
GENETIC MARKERS IN LYMPHOMA a practical overview. P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute
 GENETIC MARKERS IN LYMPHOMA a practical overview P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute B and T cell monoclonalities Rearrangement of immunoglobin and TCR genes may help
GENETIC MARKERS IN LYMPHOMA a practical overview P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute B and T cell monoclonalities Rearrangement of immunoglobin and TCR genes may help
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Aggressive B-Cell Lymphomas
 Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Anaplastic Large Cell Lymphoma (of T cell lineage)
") Anaplastic Large Cell Lymphoma (of T cell lineage) Definition T-cell lymphoma comprised of large cells with abundant cytoplasm and pleomorphic, often horseshoe-shaped nuclei CD30+ Most express cytotoxic
Anaplastic Large Cell Lymphoma (of T cell lineage) Definition T-cell lymphoma comprised of large cells with abundant cytoplasm and pleomorphic, often horseshoe-shaped nuclei CD30+ Most express cytotoxic
Diagnosis of lymphoid neoplasms has been
 Iranian Journal of Pathology (2007)2 (1), 1-61 Review Article Mehdi Nassiri Dep. of Pathology, University of Miami Miller School of Medicine, Miami, USA Abstract Correct diagnosis and classification of
Iranian Journal of Pathology (2007)2 (1), 1-61 Review Article Mehdi Nassiri Dep. of Pathology, University of Miami Miller School of Medicine, Miami, USA Abstract Correct diagnosis and classification of
DETERMINATION OF A LYMPHOID PROCESS
 Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Aggressive B-cell Lymphomas
 Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Case 3. Ann T. Moriarty,MD
 Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
3/23/2017. Disclosure of Relevant Financial Relationships. Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?!
 Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs. Nancy P. Caraway, M.D.
 A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
Classifications of lymphomas
 Classifications of lymphomas Lukes and Collins Kiel classification Working formulation REAL classification (1994) WHO classification (2000) WHO CLASSIFICATIONF OF NEOPLASMS HAEMATOPETIC AND LYMPHOID TISSUES
Classifications of lymphomas Lukes and Collins Kiel classification Working formulation REAL classification (1994) WHO classification (2000) WHO CLASSIFICATIONF OF NEOPLASMS HAEMATOPETIC AND LYMPHOID TISSUES
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Aggressive B-cell Lymphoma 2013
 Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Lymph node cytopathology : A practical approach to lymphoproliferative disorders
 Lymph node cytopathology : A practical approach to lymphoproliferative disorders Koray Ceyhan, M.D Department of Pathology Faculty of Medicine Ankara University Ankara, Turkey Diagnostic use of FNA in
Lymph node cytopathology : A practical approach to lymphoproliferative disorders Koray Ceyhan, M.D Department of Pathology Faculty of Medicine Ankara University Ankara, Turkey Diagnostic use of FNA in
Defined lymphoma entities in the current WHO classification
 Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Parts 2 and 3
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Parts 2 and 3 NEOPLASTIC LYMPHOID DISEASES Introduction o The bone marrow is the source of all cells in the
The next lymphoma classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno
 Evolution of classification The next classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno The Lymphoma Forum of Excellence, Bellinzona, January 2011 Rappaport Lukes and Collins (immunophenotype)
Evolution of classification The next classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno The Lymphoma Forum of Excellence, Bellinzona, January 2011 Rappaport Lukes and Collins (immunophenotype)
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
2010 Hematopoietic and Lymphoid ICD-O Codes - Alphabetical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
2012 Hematopoietic and Lymphoid ICD-O Codes - Numerical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
, , 2011 HODGKIN LYMPHOMA
 European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent
 Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Incidence. Bimodal age incidence 15-40, >55 years Childhood form (0-14) more common in developing countries M:F=1.5:1; in all subtypes except NS
 more common in developing countries M:F=1.5:1; in all subtypes except NS") Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Combinations of morphology codes of haematological malignancies (HM) referring to the same tumour or to a potential transformation
 referring to the same tumour or to a potential transformation") Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Pathology #07. Hussein Al-Sa di. Dr. Sohaib Al-Khatib. Mature B-Cell Neoplasm. 0 P a g e
 Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
9/28/2017. Follicular Lymphoma and Nodal Marginal Zone Lymphoma. Follicular Lymphoma Definition. Low-Grade B-Cell Lymphomas in WHO Classification
 and L. Jeffrey Medeiros, MD DISCLOSURES I do not have anything to disclose Low-Grade B-Cell Lymphomas in WHO Classification Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6
and L. Jeffrey Medeiros, MD DISCLOSURES I do not have anything to disclose Low-Grade B-Cell Lymphomas in WHO Classification Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6
Immunohistochemical classification of haematolymphoid tumours. Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital
 Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Diagnostic Molecular Pathology of Lymphoid Neoplasms
 Diagnostic Molecular Pathology of Lymphoid Neoplasms (Part II) Rational use of molecular testing in lymphomas Beirut, Lebanon Friday December 2, 2011: Hematopathology Session Adam Bagg University of Pennsylvania
Diagnostic Molecular Pathology of Lymphoid Neoplasms (Part II) Rational use of molecular testing in lymphomas Beirut, Lebanon Friday December 2, 2011: Hematopathology Session Adam Bagg University of Pennsylvania
Osteosclerotic Myeloma (POEMS Syndrome)
") Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas Raju K. Pillai City of Hope National Medical Center I have no disclosures Outline What is new in the WHO 2016 classification Insights from genomic studies Double Hit Lymphoma
Aggressive B cell Lymphomas Raju K. Pillai City of Hope National Medical Center I have no disclosures Outline What is new in the WHO 2016 classification Insights from genomic studies Double Hit Lymphoma
NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA. Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine
 NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine Historical background of Lymphoma classification Rappaport classification
NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine Historical background of Lymphoma classification Rappaport classification
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Lách
 Lách Lách Lách Lách Splenogonadal fusion. Splenic tissue is attached to testicular tissue. Pseudocyst (false or secondary cyst). A, Outer aspect. Pseudocyst (false or secondary cyst). B, Inner surface.
Lách Lách Lách Lách Splenogonadal fusion. Splenic tissue is attached to testicular tissue. Pseudocyst (false or secondary cyst). A, Outer aspect. Pseudocyst (false or secondary cyst). B, Inner surface.
3/24/2017 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS. Disclosure of Relevant Financial Relationships
 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
The patient had a mild splenomegaly but no obvious lymph node enlargement. The consensus phenotype obtained from part one of the exercise was:
 Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Case History An 86 year old male was admitted to hospital with chest infection. Haematological examination subsequently revealed the following: Hb- 11.0 g/dl; WBC- 67.1 x 10^9/l; PLT- 99 x10^9/l; RBC-
Pathology of the Lymphoid System
 Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo
 Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas NAIVE -B LYMPHOCYTE MEMORY CELL CLL MCL FL MZL Small cell size Low proliferation
Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas NAIVE -B LYMPHOCYTE MEMORY CELL CLL MCL FL MZL Small cell size Low proliferation
Patterns of Lymphoid Neoplasia in Peripheral Blood. Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure
 Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Patterns of Lymphoid Neoplasia in Peripheral Blood Leon F. Baltrucki, M.D. Leon F. Baltrucki, M.D. Disclosure Dr Baltrucki has received an honorarium for his participation as a faculty presenter in this
Hematopathology Lab. Third year medical students
 Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Hematopathology Lab Third year medical students Objectives Identify the lesion Know the specific name of the lesion Know associated disease Know relevant pathologic background Spherocytes: appear small,
Thomas Hodgkin and Hodgkin lymphoma
 J Hematopathol (2014) 7:123 138 DOI 10.1007/s12308-014-0214-3 REVIEW ARTICLE Thomas Hodgkin and Hodgkin lymphoma Judith A. Ferry Received: 26 June 2014 /Accepted: 31 July 2014 /Published online: 12 August
J Hematopathol (2014) 7:123 138 DOI 10.1007/s12308-014-0214-3 REVIEW ARTICLE Thomas Hodgkin and Hodgkin lymphoma Judith A. Ferry Received: 26 June 2014 /Accepted: 31 July 2014 /Published online: 12 August
Lymphoid Neoplasms. Sylvie Freeman Department of Clinical Immunology, University of Birmingham
 Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Pulmonary biopsy specimens demonstrate
 A PRACTICAL APPROACH TO THE EVALUATION OF LYMPHOID AND PLASMA CELL INFILTRATES IN THE LUNG Fiona E. Craig, MD KEYWORDS Lymphoma Pulmonary Immunophenotyping Genotyping ABSTRACT Pulmonary biopsy specimens
A PRACTICAL APPROACH TO THE EVALUATION OF LYMPHOID AND PLASMA CELL INFILTRATES IN THE LUNG Fiona E. Craig, MD KEYWORDS Lymphoma Pulmonary Immunophenotyping Genotyping ABSTRACT Pulmonary biopsy specimens
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH
 EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
Lymphoma Update: Lymphoma Update: What s Likely to be New in the New WHO. Patrick Treseler, MD, PhD University of California San Francisco
 Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
Low-grade B-cell lymphoma
 Low-grade B-cell lymphoma Patho-Basic 11. September 2018 Stephan Dirnhofer Pathology Outline Definition LPL, MBL/CLL/SLL, MCL FL Subtypes & variants Diagnosis including Grading Transformation Summary Be
Low-grade B-cell lymphoma Patho-Basic 11. September 2018 Stephan Dirnhofer Pathology Outline Definition LPL, MBL/CLL/SLL, MCL FL Subtypes & variants Diagnosis including Grading Transformation Summary Be
Low-Grade B-Cell Lymphomas in WHO Classification. Follicular Lymphoma Definition. Follicular Lymphoma Clinical Features 11/7/2017 DISCLOSURES
 Low-Grade B-Cell Lymphomas in WHO Classification DISCLOSURES I do not have anything to disclose Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6 % Small lymphocytic lymphoma/cll
Low-Grade B-Cell Lymphomas in WHO Classification DISCLOSURES I do not have anything to disclose Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6 % Small lymphocytic lymphoma/cll
Methods used to diagnose lymphomas
 Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Hyperplasia of Mantle/Marginal Zone B Cells With Clear Cytoplasm in Peripheral Lymph Nodes A Clinicopathologic Study of 35 Cases
 Hematopathology / HYPERPLASIA OF MANTLE/MARGINAL ZONE B CELLS WITH CLEAR CYTOPLASM Hyperplasia of Mantle/Marginal Zone B Cells With Clear Cytoplasm in Peripheral Lymph Nodes A Clinicopathologic Study of
Hematopathology / HYPERPLASIA OF MANTLE/MARGINAL ZONE B CELLS WITH CLEAR CYTOPLASM Hyperplasia of Mantle/Marginal Zone B Cells With Clear Cytoplasm in Peripheral Lymph Nodes A Clinicopathologic Study of
Chapter 12 The Role of Fine Needle Aspiration Biopsy in the Diagnosis and Management of Hematopoietic Neoplasms
 Chapter 12 The Role of Fine Needle Aspiration Biopsy in the Diagnosis and Management of Hematopoietic Neoplasms Rana S. Hoda FINE NEEDLE ASPIRATION Introduction Fine needle aspiration (FNA) is a well-established
Chapter 12 The Role of Fine Needle Aspiration Biopsy in the Diagnosis and Management of Hematopoietic Neoplasms Rana S. Hoda FINE NEEDLE ASPIRATION Introduction Fine needle aspiration (FNA) is a well-established
WHO Classification. B-cell chronic lymphocytic leukemia/small T-cell granular lymphocytic leukemia
 Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Tres
 Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Treseler, MD, PhD University of California San Francisco
Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Treseler, MD, PhD University of California San Francisco
Clinical Policy: Bendamustine (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307
 Reference Number: PA.CP.PHAR.307") Clinical Policy: (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that
Clinical Policy: (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
VENTANA hematopathology solutions. Deliver diagnostic confidence
 VENTANA hematopathology solutions Deliver diagnostic confidence 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping hematological cancers 4 The importance
VENTANA hematopathology solutions Deliver diagnostic confidence 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping hematological cancers 4 The importance
Low grade High grade , immune suppression chronic persistent inflammation viruses B-symptoms
 We've one category for lymphoid neoplasm which is the lymphoma in contrast to that of myeloid which has three categories; acute myeloid leukemias, myeloproliferative & myelodysplastic disorders. Lymphoma
We've one category for lymphoid neoplasm which is the lymphoma in contrast to that of myeloid which has three categories; acute myeloid leukemias, myeloproliferative & myelodysplastic disorders. Lymphoma
Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy?
 Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy? Andreas Rosenwald Institute of Pathology, University of Würzburg, Germany Barcelona, June 18, 2010 NEW WHO CLASSIFICATION
Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy? Andreas Rosenwald Institute of Pathology, University of Würzburg, Germany Barcelona, June 18, 2010 NEW WHO CLASSIFICATION
HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD
 HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD") HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD OUTLINE High grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements Patient presentation 2008/2016
HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD OUTLINE High grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements Patient presentation 2008/2016
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,
: Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,") High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
PRECURSOR LYMHPOID NEOPLASMS. B lymphoblastic leukaemia/lymphoma T lymphoblastic leukaemia/lymphoma
 PRECURSOR LYMHPOID NEOPLASMS B lymphoblastic leukaemia/lymphoma T lymphoblastic leukaemia/lymphoma B lymphoblastic leukaemia/lymphoma Definition: B lymphoblastic leukaemia/lymphoma is a neoplasm of precursor
PRECURSOR LYMHPOID NEOPLASMS B lymphoblastic leukaemia/lymphoma T lymphoblastic leukaemia/lymphoma B lymphoblastic leukaemia/lymphoma Definition: B lymphoblastic leukaemia/lymphoma is a neoplasm of precursor
Clinicopathologic features of 112 cases with mantle cell lymphoma
 Cancer Biol Med 2015;12:46-52. doi: 10.7497/j.issn.2095-3941.2015.0007 ORIGINAL ARTICLE Clinicopathologic features of 112 cases with mantle cell lymphoma Dong-Mei Zhou, Gang Chen, Xiong-Wei Zheng, Wei-Feng
Cancer Biol Med 2015;12:46-52. doi: 10.7497/j.issn.2095-3941.2015.0007 ORIGINAL ARTICLE Clinicopathologic features of 112 cases with mantle cell lymphoma Dong-Mei Zhou, Gang Chen, Xiong-Wei Zheng, Wei-Feng
Bone Marrow. Procedures Blood Film Aspirate, Cell Block Trephine Biopsy, Touch Imprint
 Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
VENTANA hematopathology solutions Comprehensive aids for detecting and subtyping
 VENTANA hematopathology solutions Comprehensive aids for detecting and subtyping 1 12/4/2015 9:47:24 AM 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping
VENTANA hematopathology solutions Comprehensive aids for detecting and subtyping 1 12/4/2015 9:47:24 AM 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas
 ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas Philippe Gaulard, Dept of Pathology, INSERM U955, Hôpital Henri Mondor, 94010 -
ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas Philippe Gaulard, Dept of Pathology, INSERM U955, Hôpital Henri Mondor, 94010 -
Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma
 Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma Nancy Lee Harris, M. D. Massachusetts General Hospital Harvard Medical School Aggressive B-cell Lymphomas WHO 4 th Edition
Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma Nancy Lee Harris, M. D. Massachusetts General Hospital Harvard Medical School Aggressive B-cell Lymphomas WHO 4 th Edition
The development of clonality testing for lymphomas in the Bristol Genetics Laboratory. Dr Paula Waits Bristol Genetics Laboratory
 The development of clonality testing for lymphomas in the Bristol Genetics Laboratory Dr Paula Waits Bristol Genetics Laboratory Introduction The majority of lymphoid malignancies belong to the B cell
The development of clonality testing for lymphomas in the Bristol Genetics Laboratory Dr Paula Waits Bristol Genetics Laboratory Introduction The majority of lymphoid malignancies belong to the B cell
Pathology of the Lymphoid System
 Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Case: The patient is a 73 year old woman with vague complaints of dyspepsia and abdominal pain. Upper endoscopy showed features of gastritis and a
 Case: The patient is a 73 year old woman with vague complaints of dyspepsia and abdominal pain. Upper endoscopy showed features of gastritis and a nodular lesion in the body of the stomach. The patient
Case: The patient is a 73 year old woman with vague complaints of dyspepsia and abdominal pain. Upper endoscopy showed features of gastritis and a nodular lesion in the body of the stomach. The patient
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
Common Problem Areas. WHO Classification. Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS LOW GRADE / HIGH GRADE
 with their CLINICAL AGGRESSIVENESS LOW GRADE / HIGH GRADE") WHO Classification Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS REVIEW OF MOST COMMON LYMPHOMA ENTITIES Dr Stefan Dojcinov LOW GRADE / HIGH GRADE (June 2014) The Non-Hodgkin
WHO Classification Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS REVIEW OF MOST COMMON LYMPHOMA ENTITIES Dr Stefan Dojcinov LOW GRADE / HIGH GRADE (June 2014) The Non-Hodgkin
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo
 Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO
 HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
Lymphoma classification: a still ongoing journey
 Lymphoma classification: a still ongoing journey Stefano A. Pileri Professor of Pathology, Bologna University Medical School Director of Haematopathology, St. Orsola Policlinic (at present) Director of
Lymphoma classification: a still ongoing journey Stefano A. Pileri Professor of Pathology, Bologna University Medical School Director of Haematopathology, St. Orsola Policlinic (at present) Director of
ISIMM Tata Conference on Immunohistochemistry. Kolkata, India, January Immunohistochemistry. A cost effective approach to lymphoma diagnosis
 ISIMM Tata Conference on Immunohistochemistry. Kolkata, India, January 2018 Immunohistochemistry A cost effective approach to lymphoma diagnosis Clive R. Taylor, M.D., Ph.D., Department of Pathology, Keck
ISIMM Tata Conference on Immunohistochemistry. Kolkata, India, January 2018 Immunohistochemistry A cost effective approach to lymphoma diagnosis Clive R. Taylor, M.D., Ph.D., Department of Pathology, Keck
Corrigenda. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run
: corrections made in second print run") Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
Test Utilization: Chronic Lymphocytic Leukemia
 Test Utilization: Chronic Lymphocytic Leukemia Initial Evaluation Diagnostic Criteria Selection of Tests for Prognosis Response to Therapy Challenges Assessment for persistent disease Paul J. Kurtin, M.D.
Test Utilization: Chronic Lymphocytic Leukemia Initial Evaluation Diagnostic Criteria Selection of Tests for Prognosis Response to Therapy Challenges Assessment for persistent disease Paul J. Kurtin, M.D.
Lymphoma and Pseudolymphoma
 Lymphoma and Pseudolymphoma Laura B. Pincus, MD Co-Director, Cutaneous Lymphoma Clinic Associate Professor Dermatology and Pathology University of California, San Francisco I HAVE NO RELEVANT RELATIONSHIPS
Lymphoma and Pseudolymphoma Laura B. Pincus, MD Co-Director, Cutaneous Lymphoma Clinic Associate Professor Dermatology and Pathology University of California, San Francisco I HAVE NO RELEVANT RELATIONSHIPS
PhenoPath. Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA
 PhenoPath Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA C urrent diagnosis of B cell non-hodgkin lymphoma (B-NHL) is based on the 2008 WHO Classification of Tumours of Haematopoietic and Lymphoid
PhenoPath Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA C urrent diagnosis of B cell non-hodgkin lymphoma (B-NHL) is based on the 2008 WHO Classification of Tumours of Haematopoietic and Lymphoid
Lymphoid Neoplasms Associated With IgM Paraprotein A Study of 382 Patients
 Hematopathology / LYMPHOMAS WITH IGM PARAPROTEIN Lymphoid Neoplasms Associated With IgM Paraprotein A Study of 382 Patients Pei Lin, MD, 1 Suyang Hao, MD, 1* Beverly C. Handy, MD, 2 Carlos E. Bueso-Ramos,
Hematopathology / LYMPHOMAS WITH IGM PARAPROTEIN Lymphoid Neoplasms Associated With IgM Paraprotein A Study of 382 Patients Pei Lin, MD, 1 Suyang Hao, MD, 1* Beverly C. Handy, MD, 2 Carlos E. Bueso-Ramos,