Respiratory Interactive Session. Elaine Borg
|
|
|
- Susan Robertson
- 6 years ago
- Views:
Transcription
1 Respiratory Interactive Session Elaine Borg
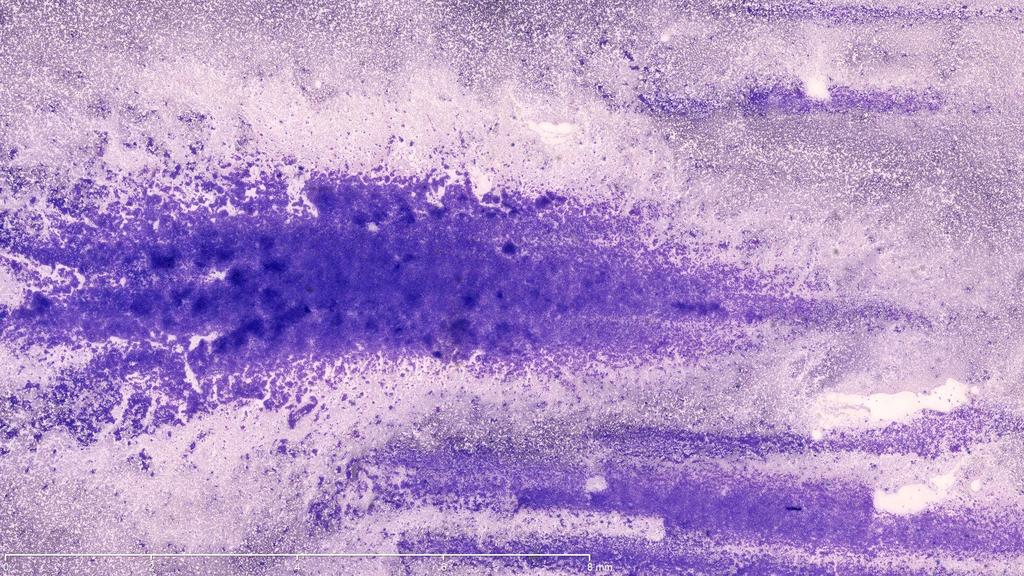
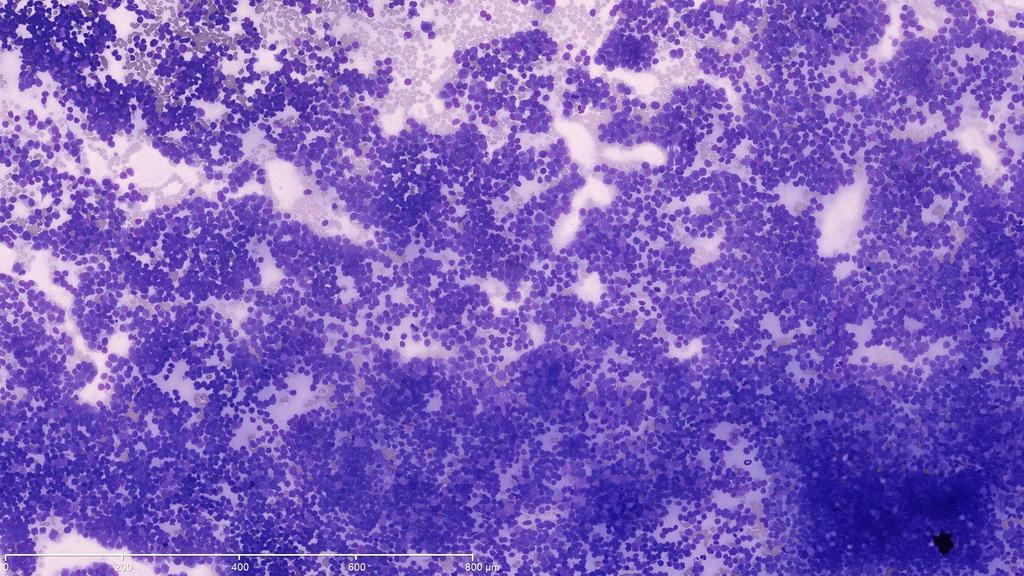
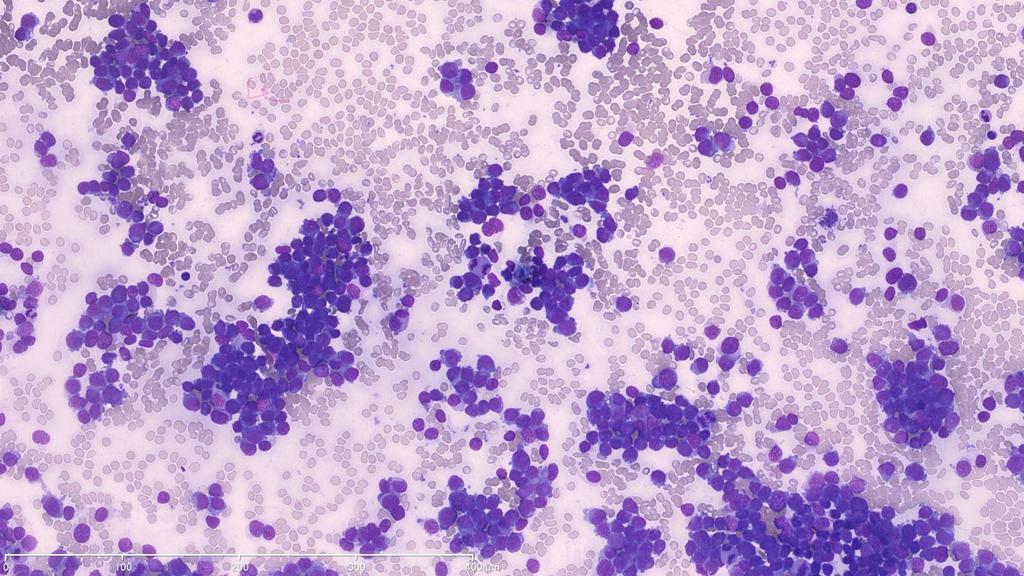
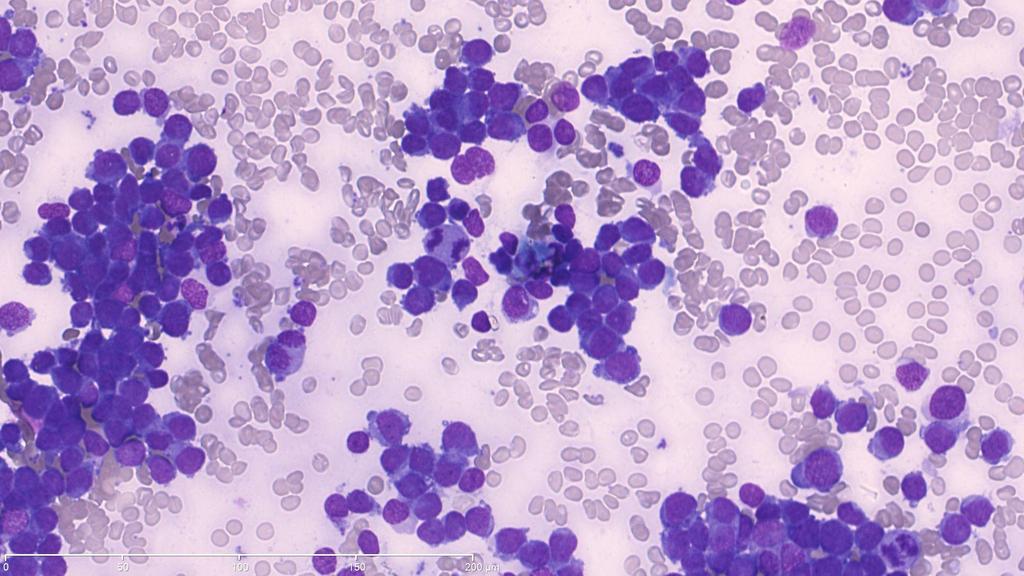
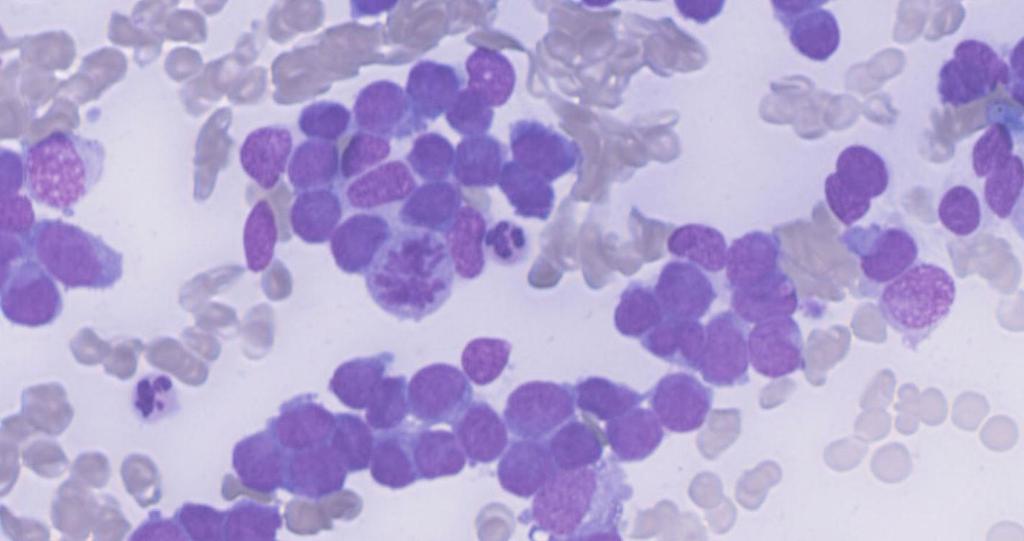
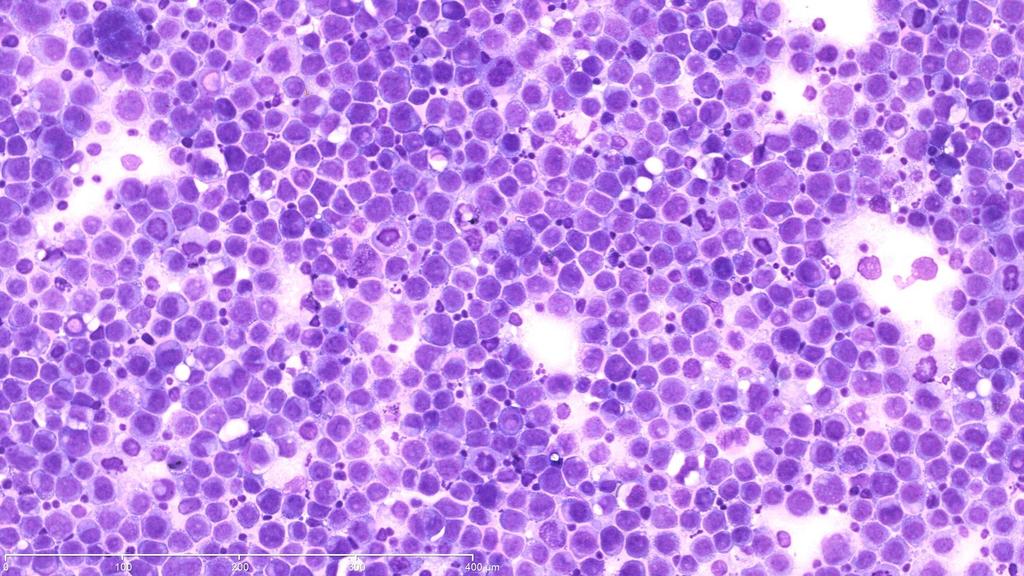
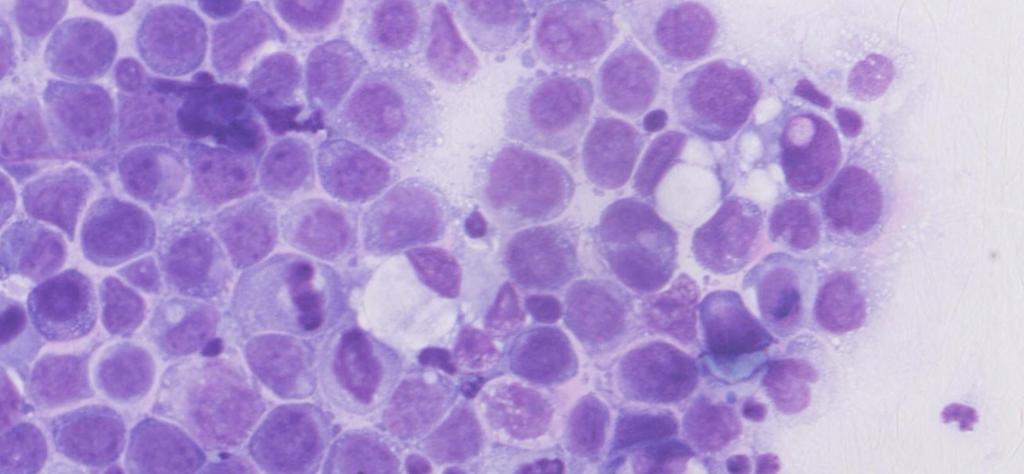
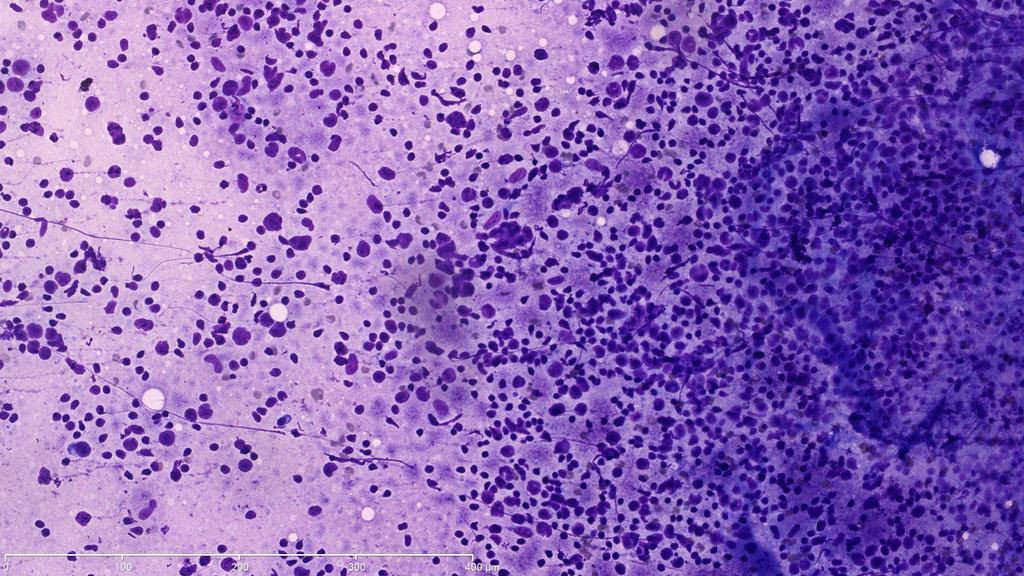
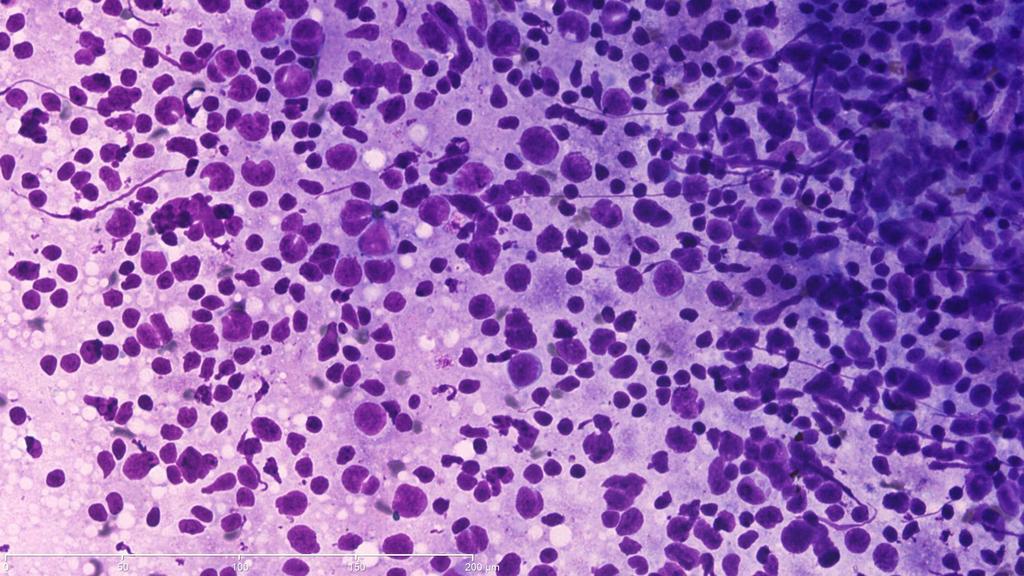
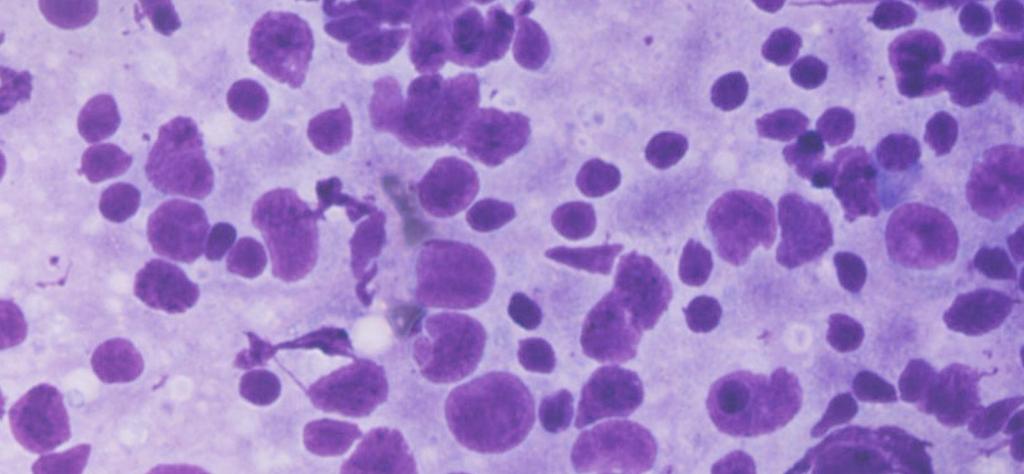
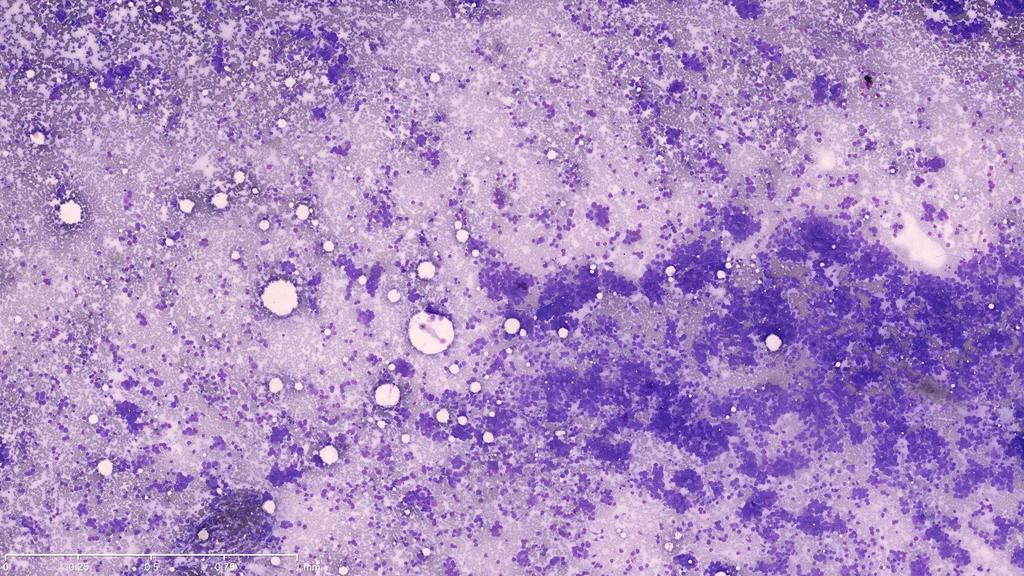
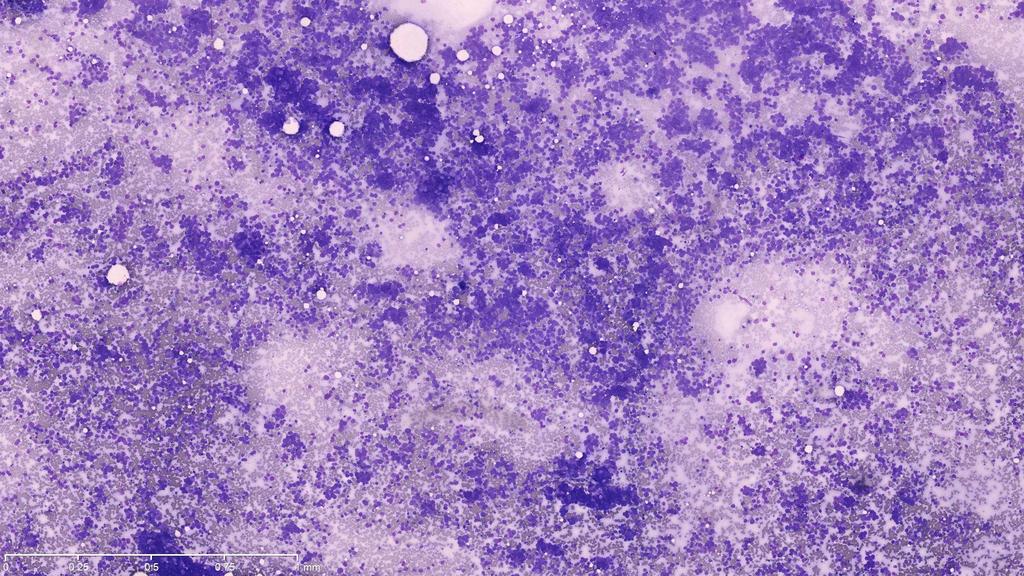
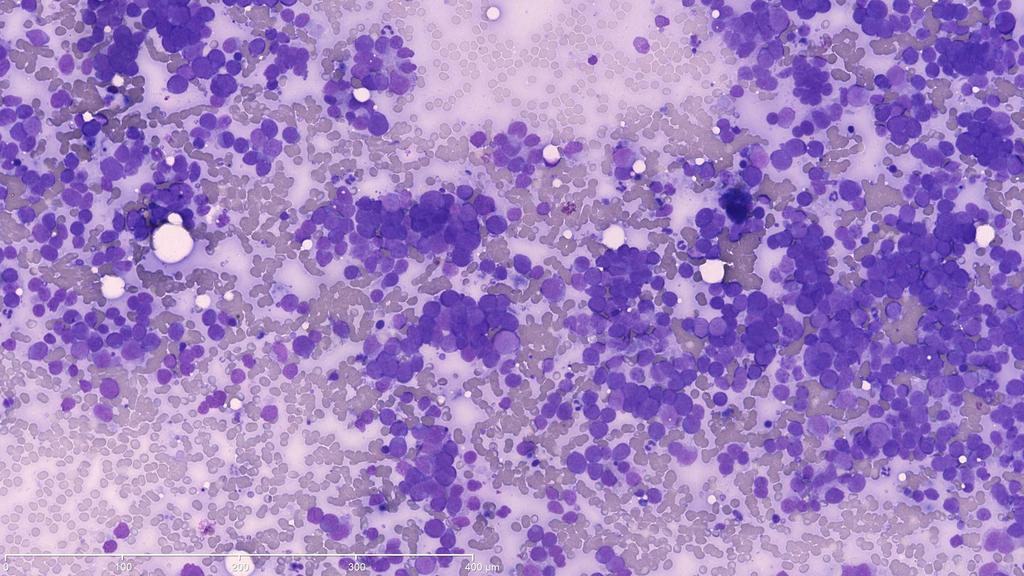
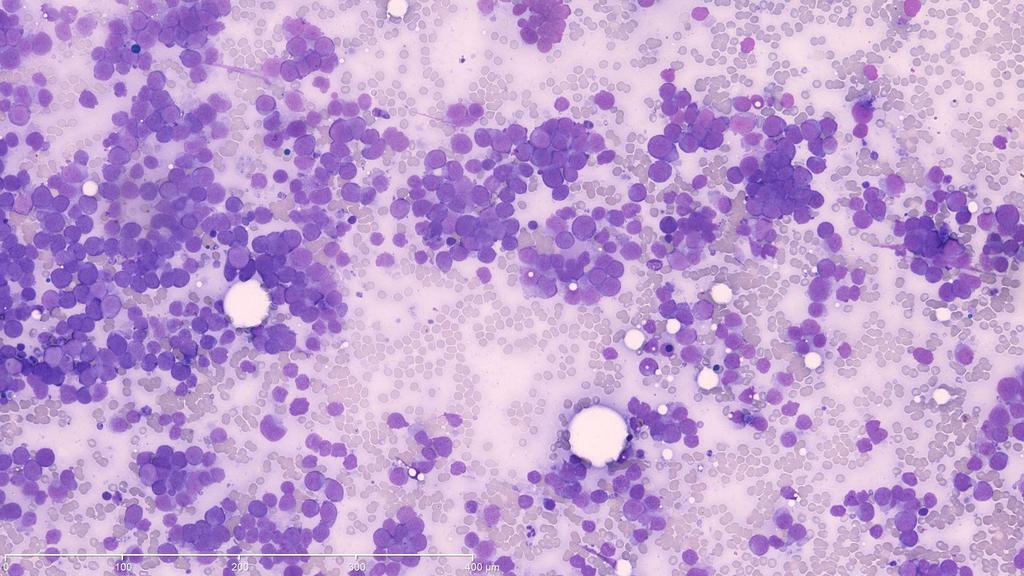
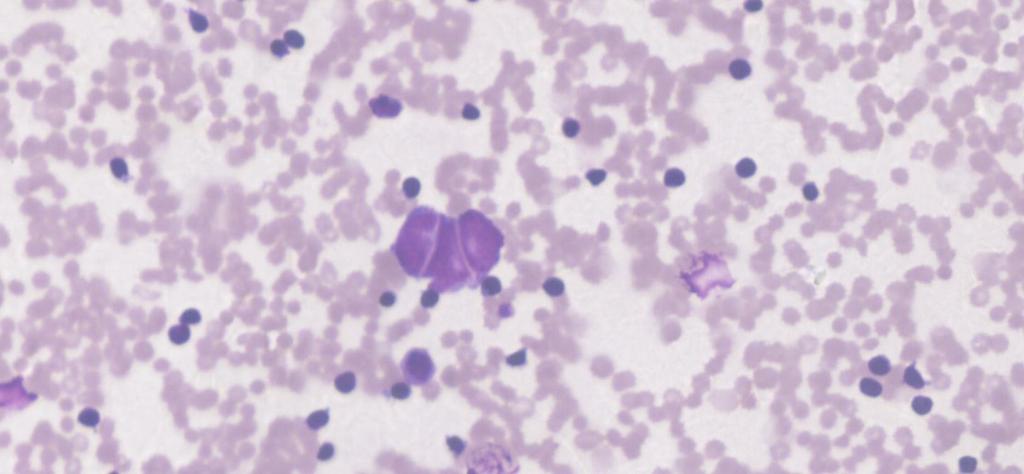
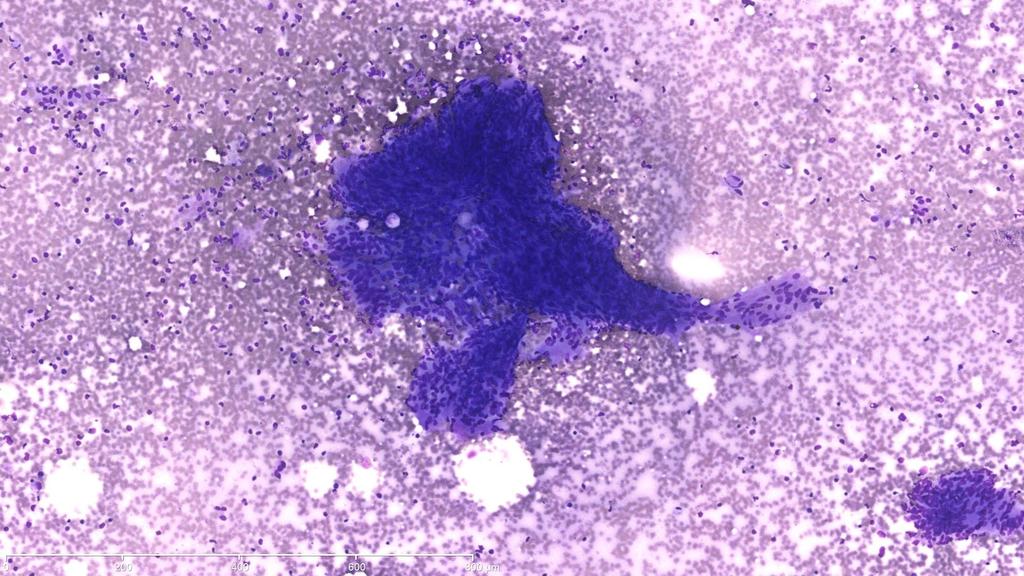
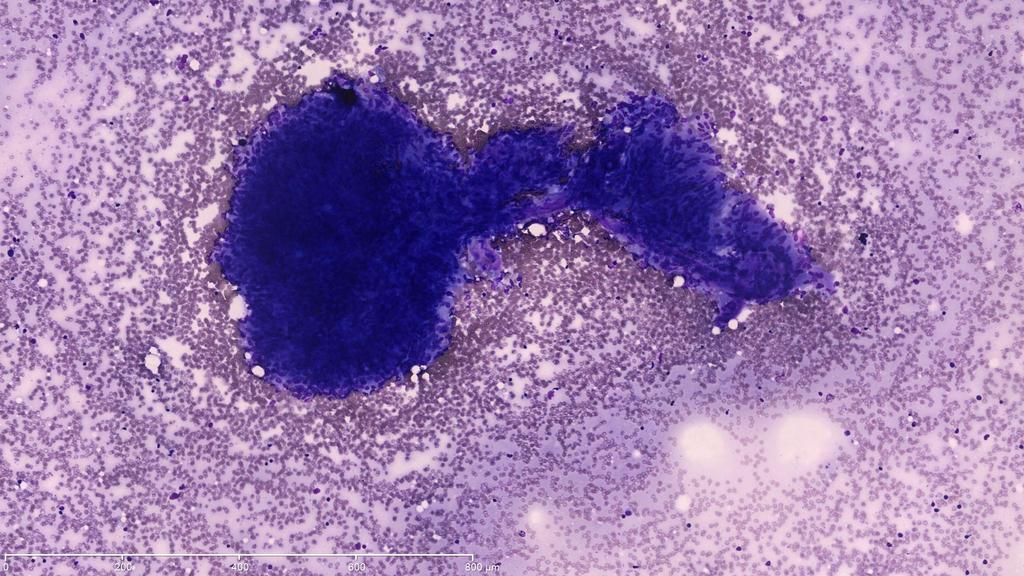
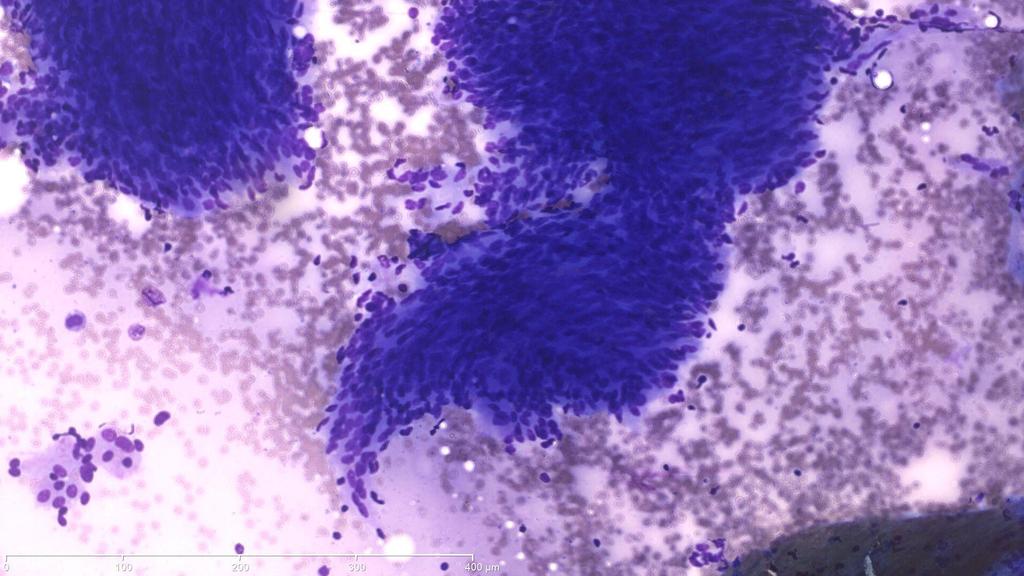
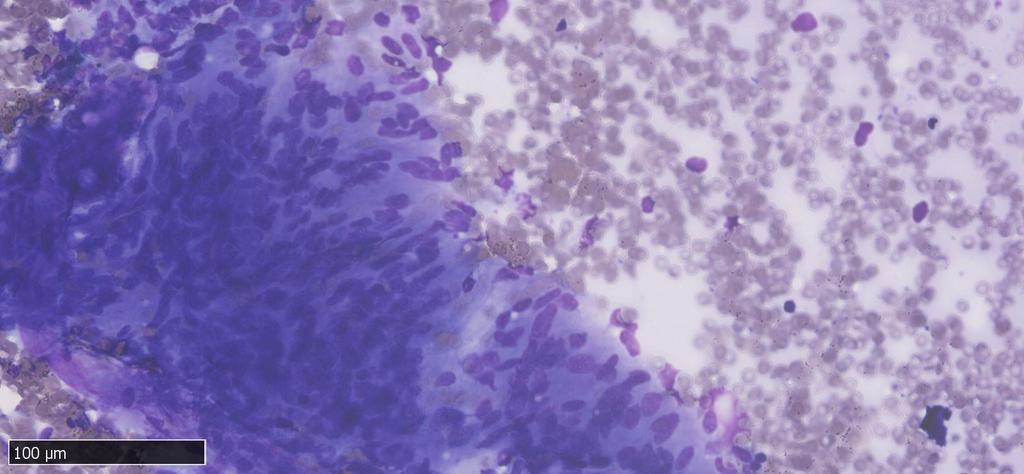
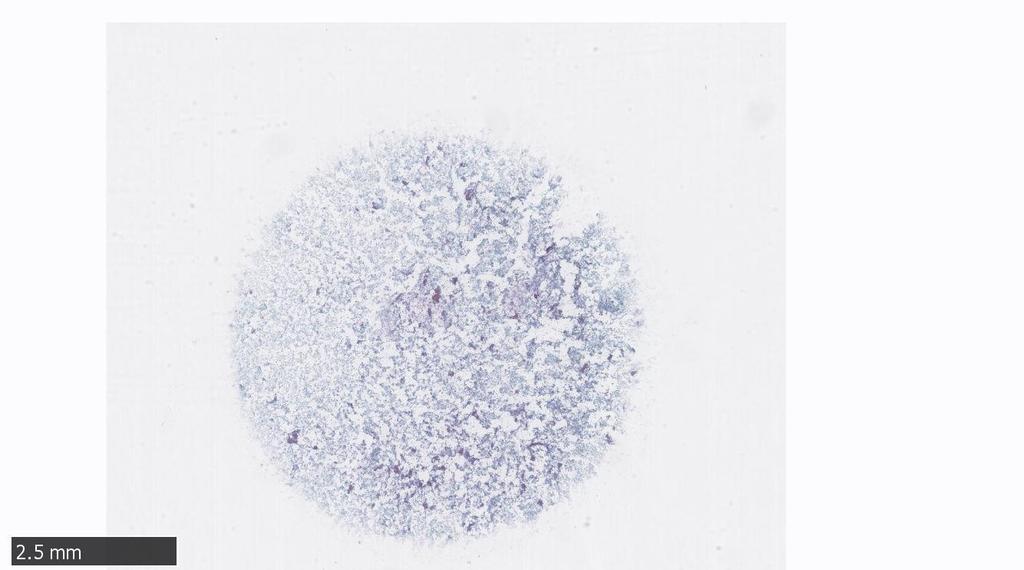
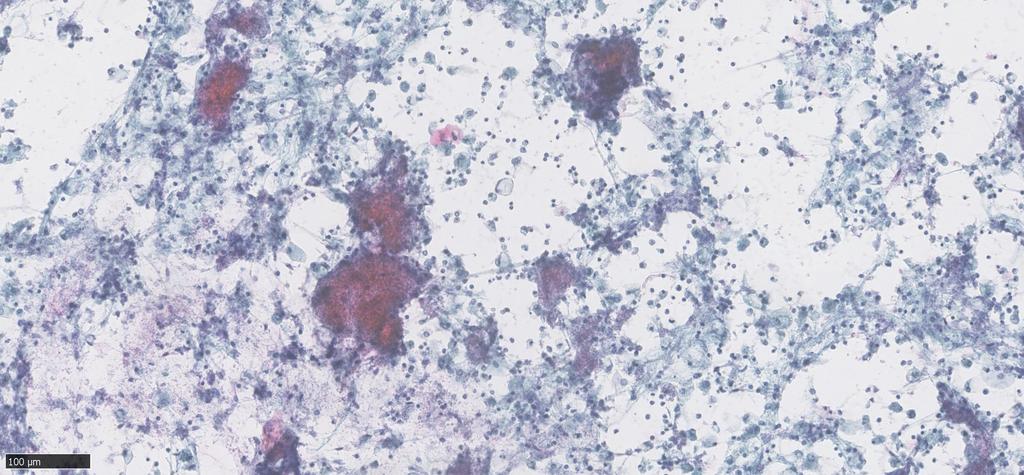
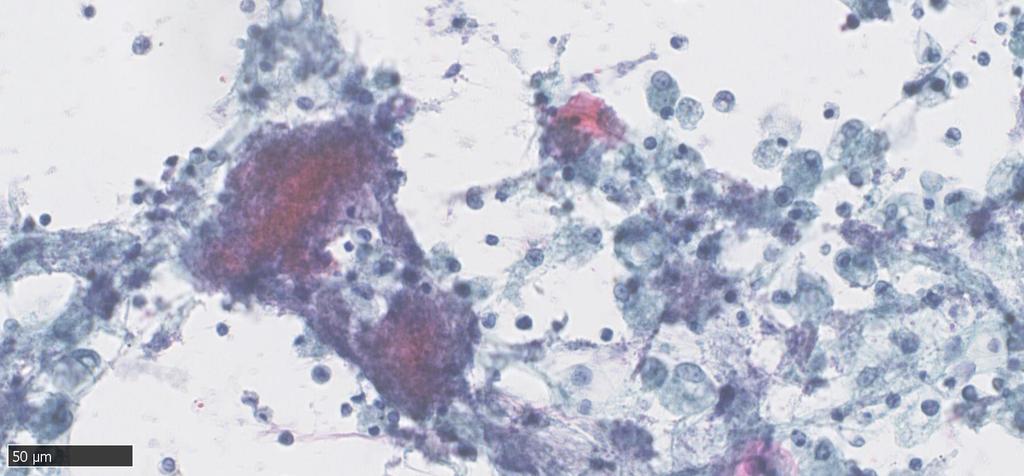
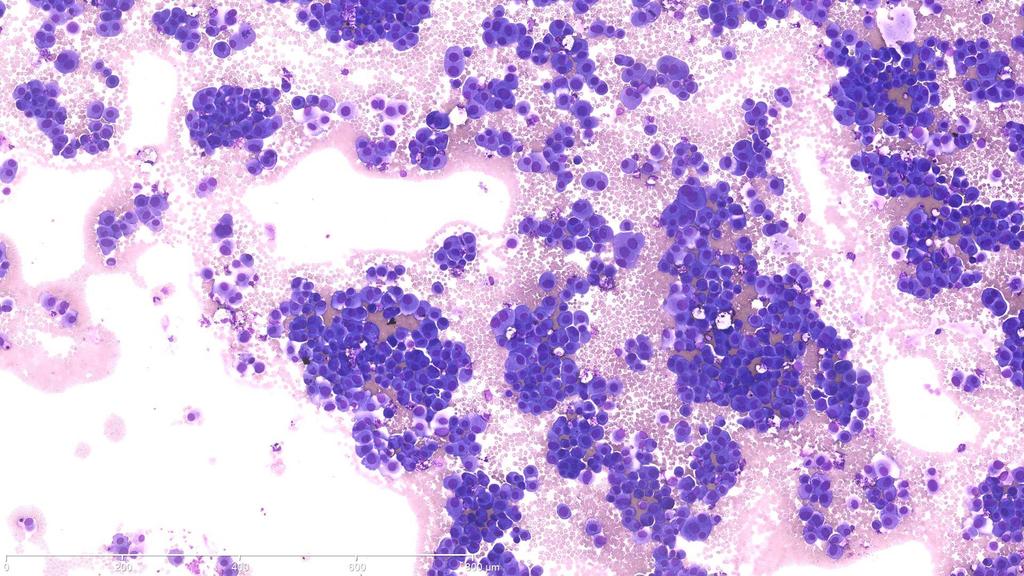
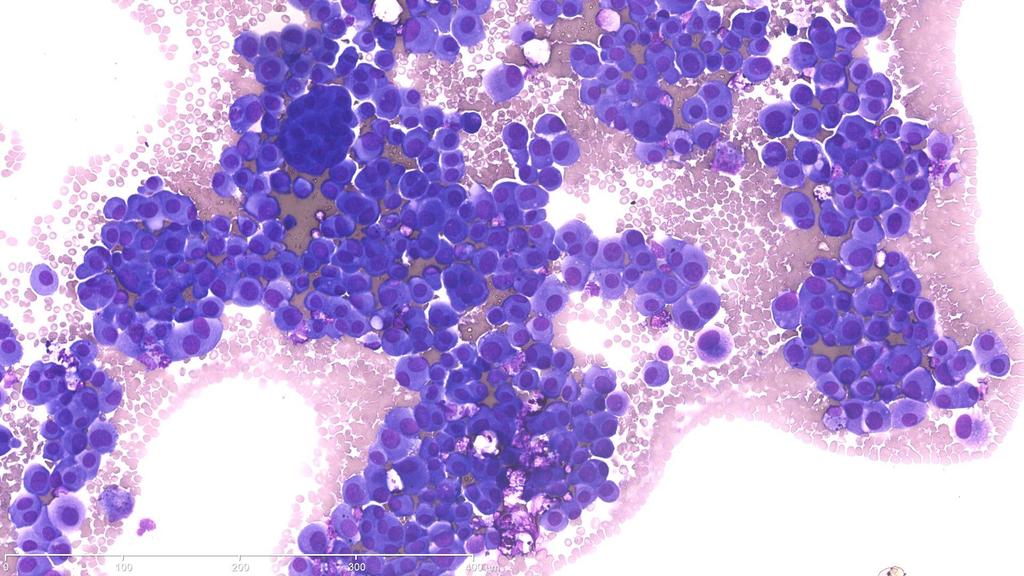
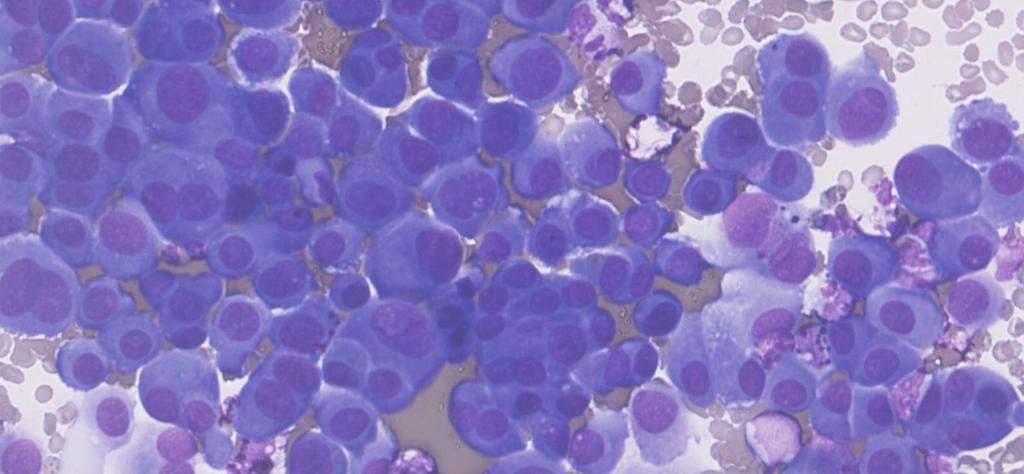
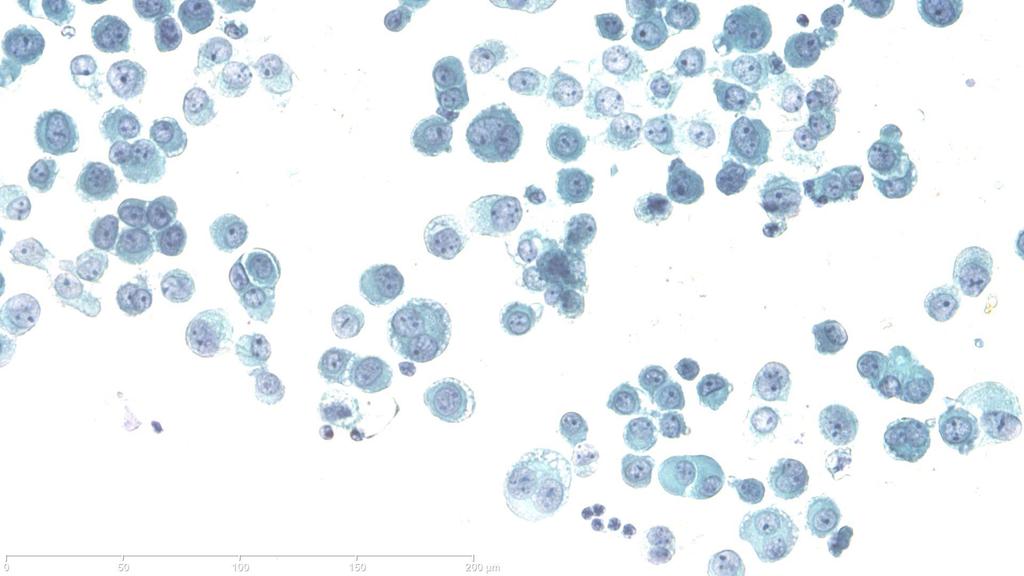
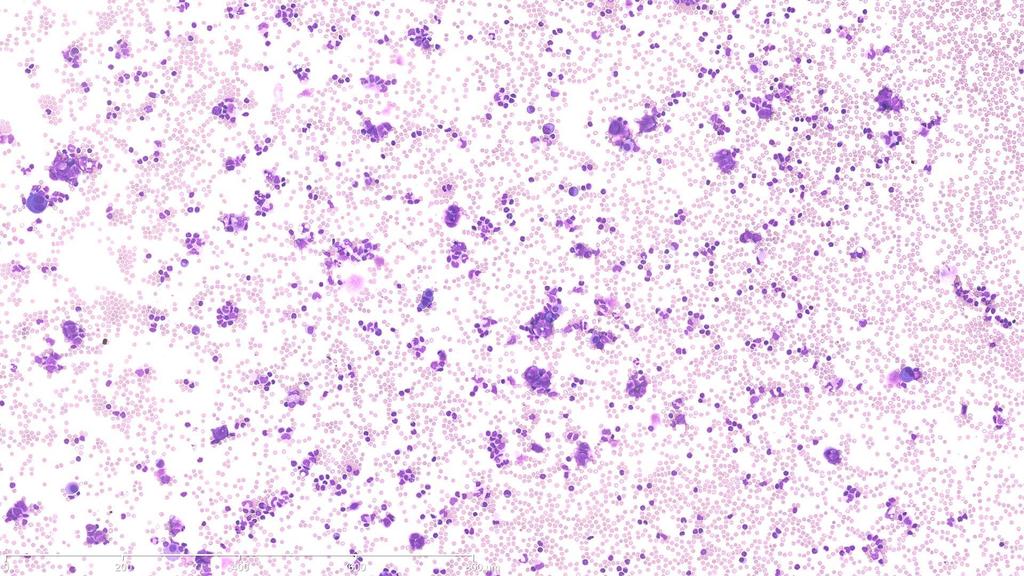
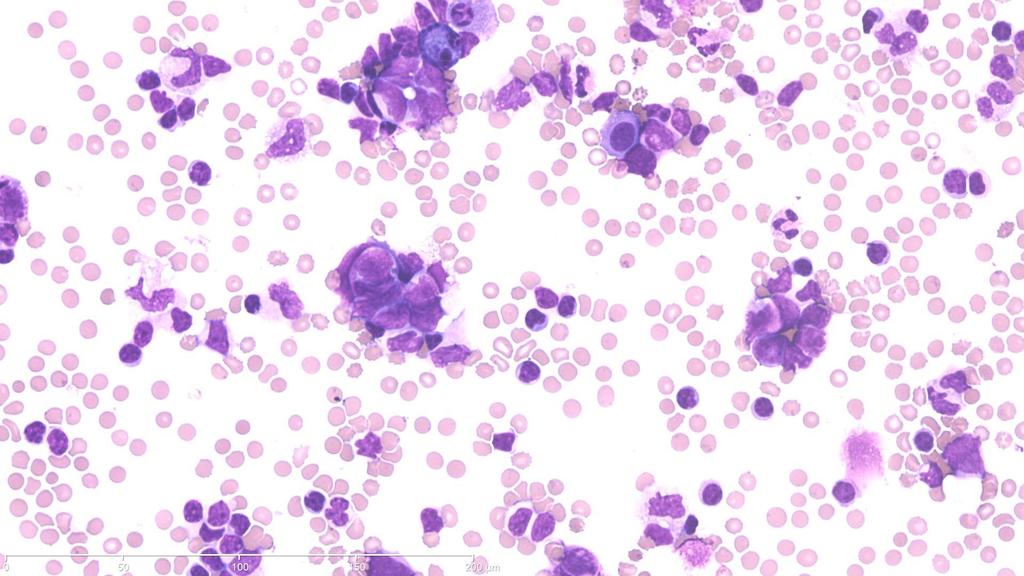
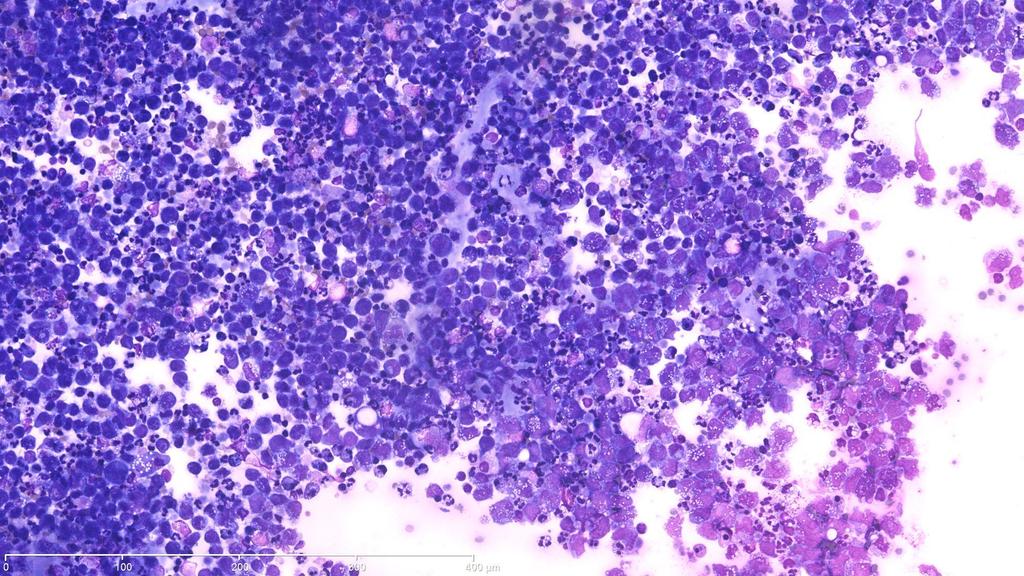
2 Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA
3
4
5
6

7
8
9
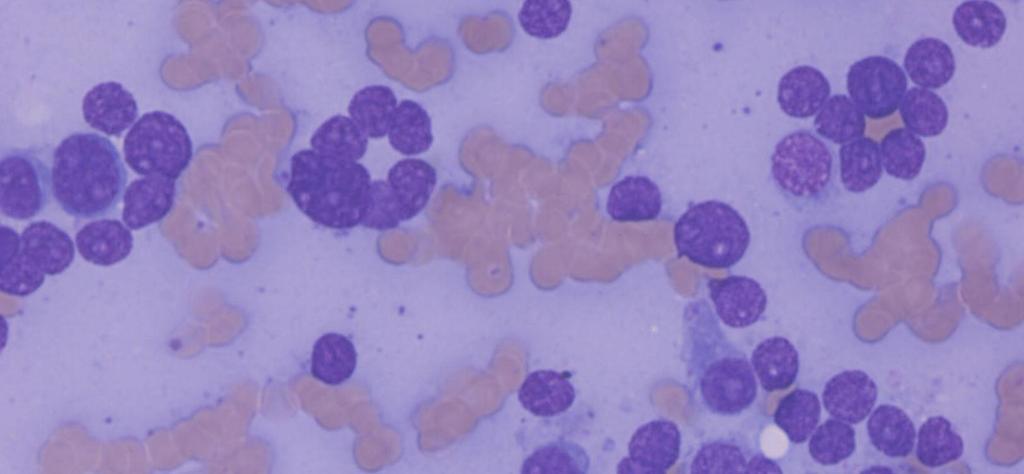
10 Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal mass EBUS FNA Differential Diagnosis A. High Grade Lymphoma B. Small Round Blue Cell Tumour C. Small Cell Carcinoma D. Plasma Cell Neoplasm
11 DIAGNOSIS
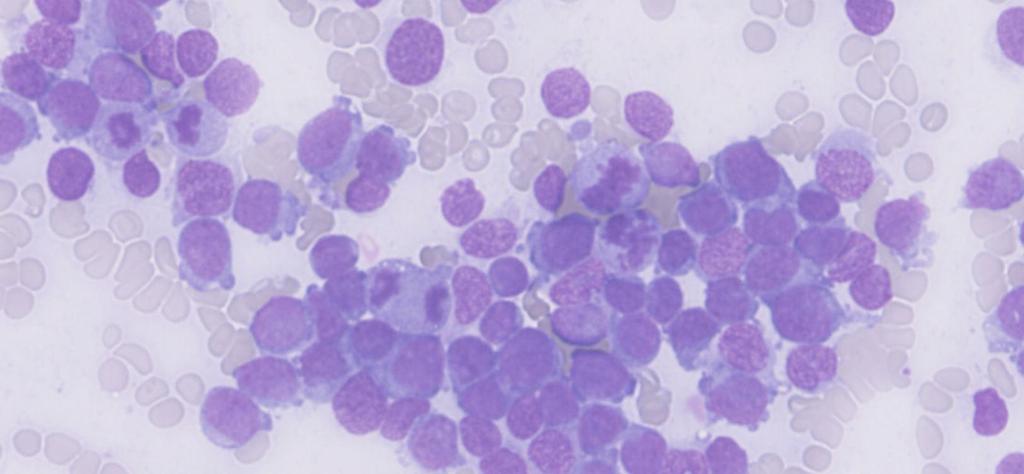
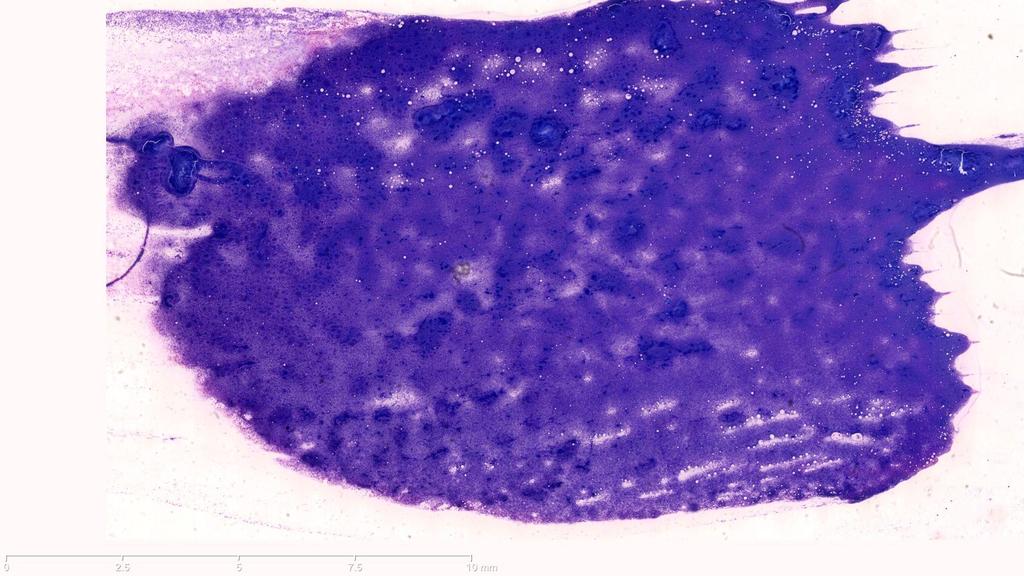
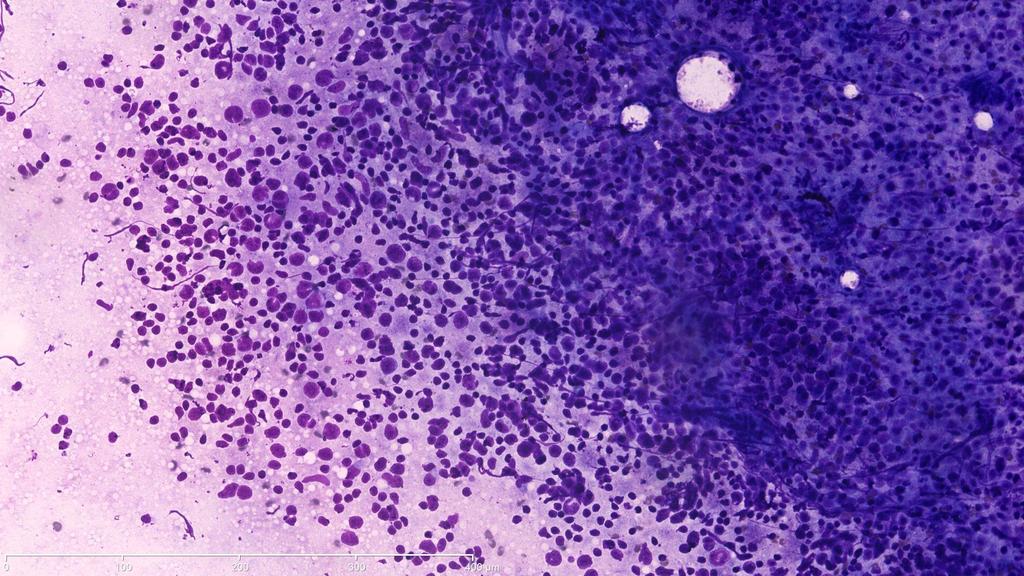
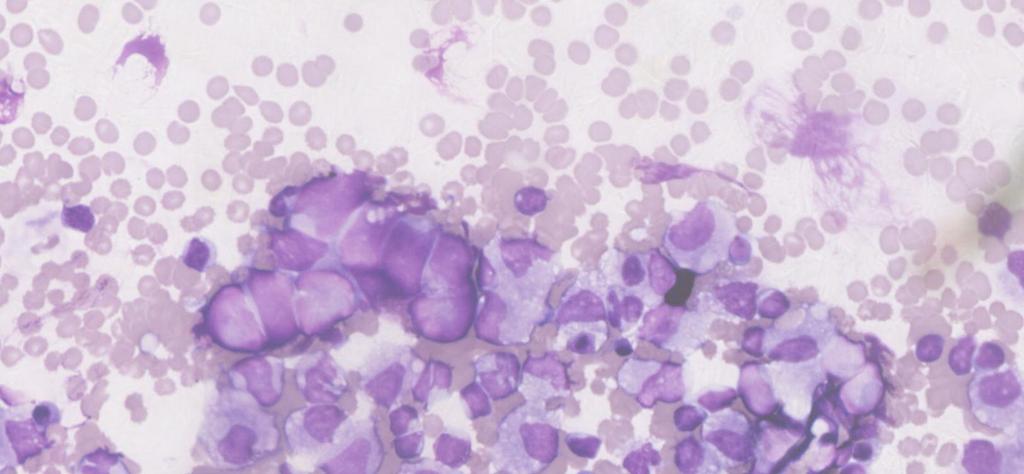
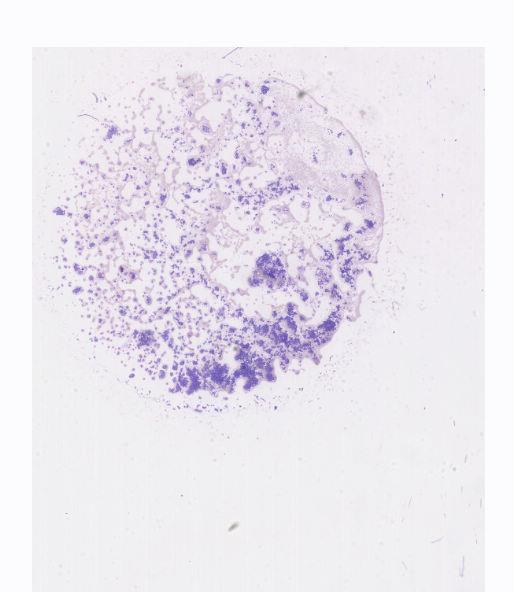
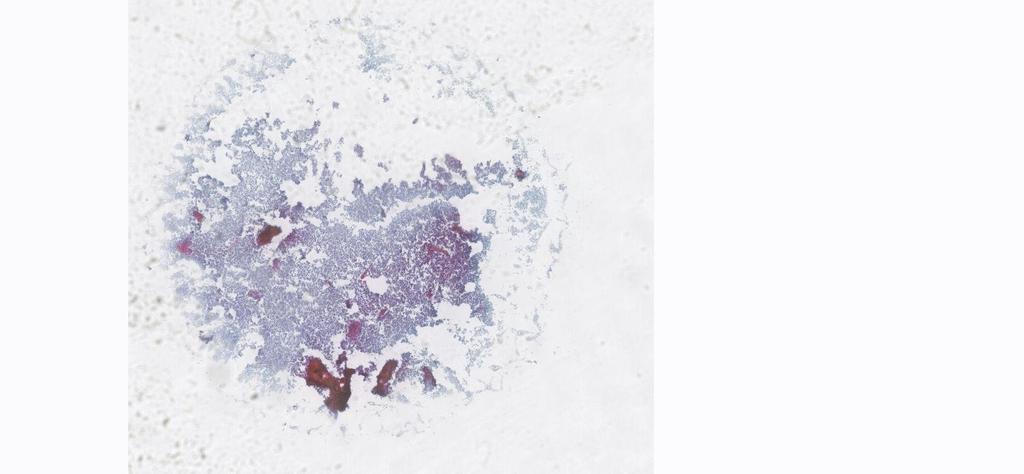
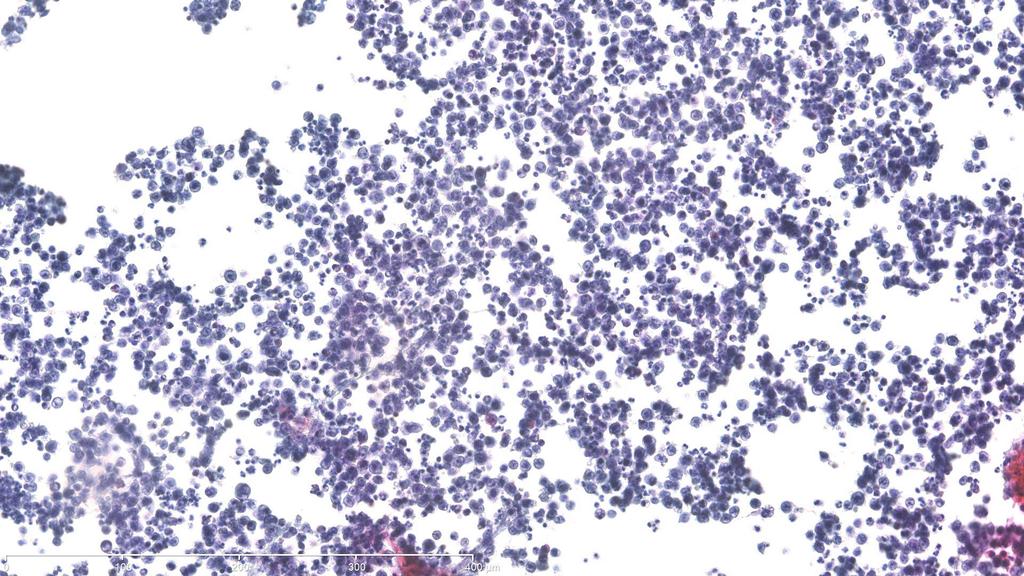
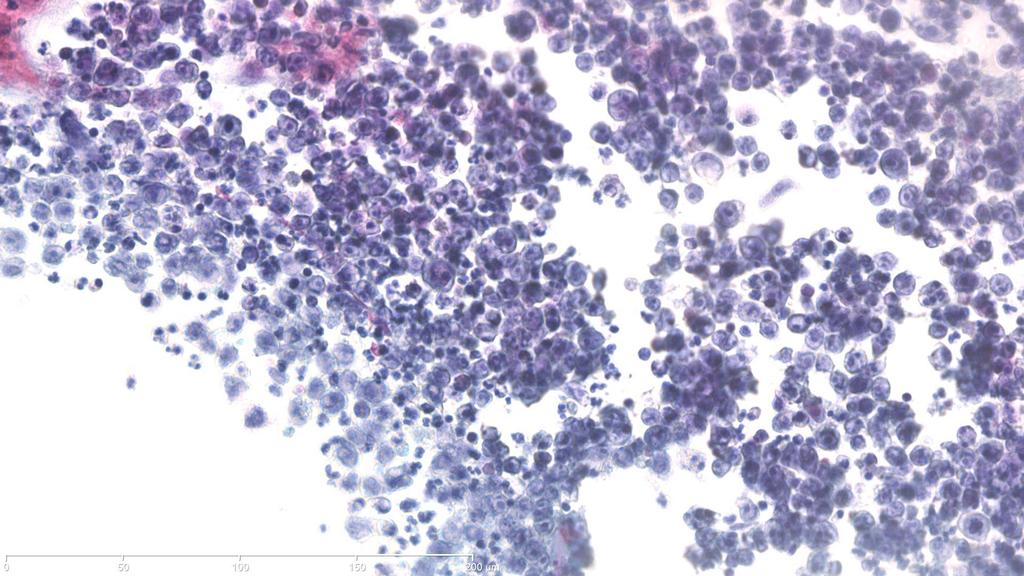
12 Case 2 Respiratory Cytology 60 year old gentleman Enlarged mediastinal lymph nodes and multiple lung nodules EBUS TBNA
13
14
15

16
17
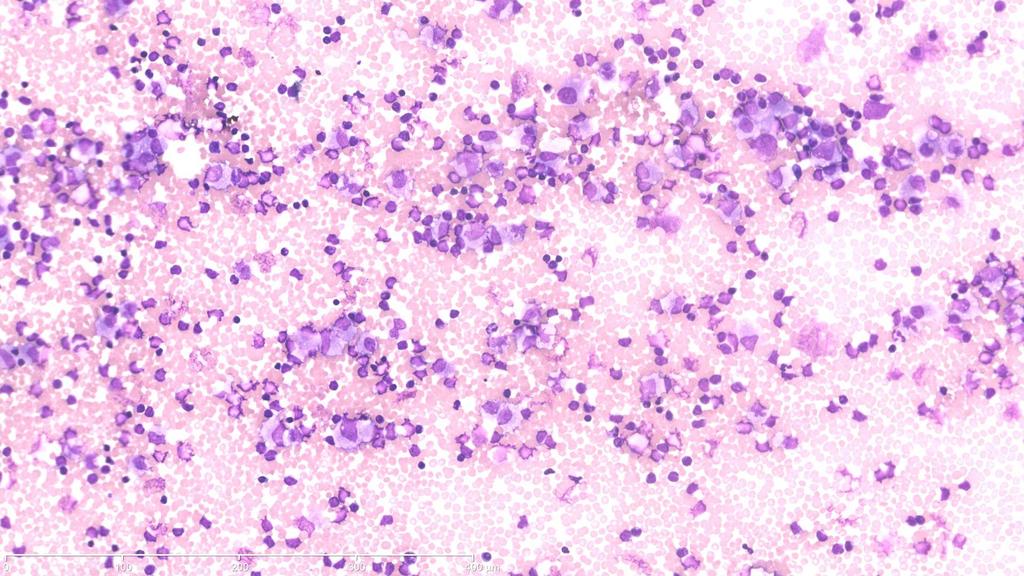
18 Case 2 Respiratory Cytology 60 year old gentleman with enlarged mediastinal lymph nodes and multiple lung nodules EBUS TBNA Differential Diagnosis A. High Grade Lymphoma B. Small Round Blue Cell Tumour C. Adenocarcinoma D. Small Cell Carcinoma
19 DIAGNOSIS
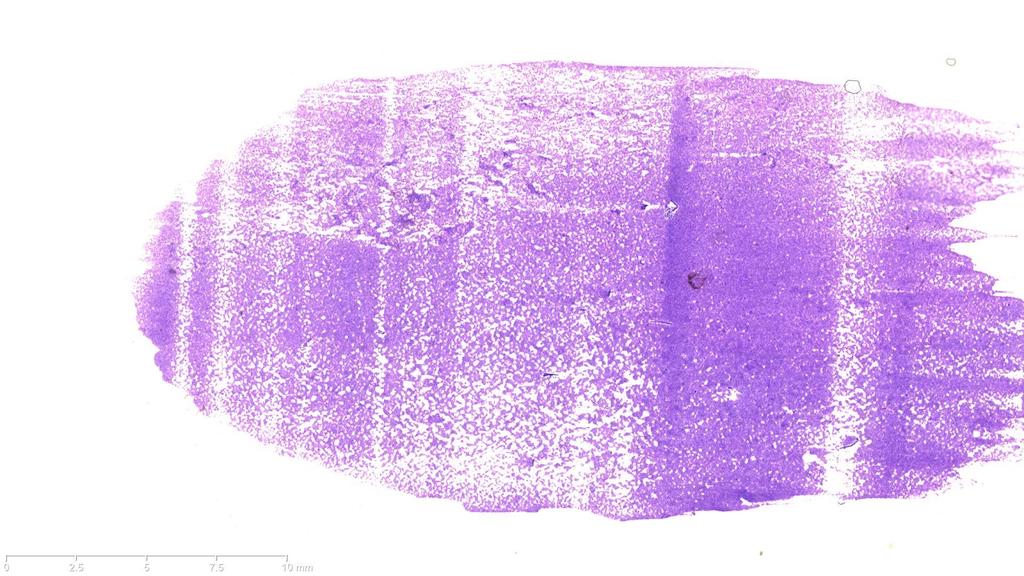
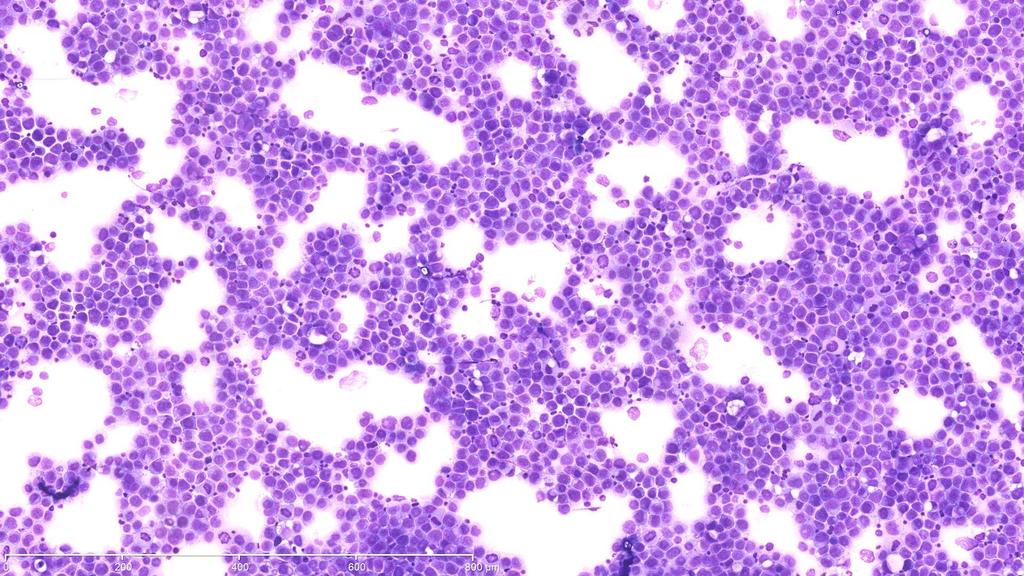
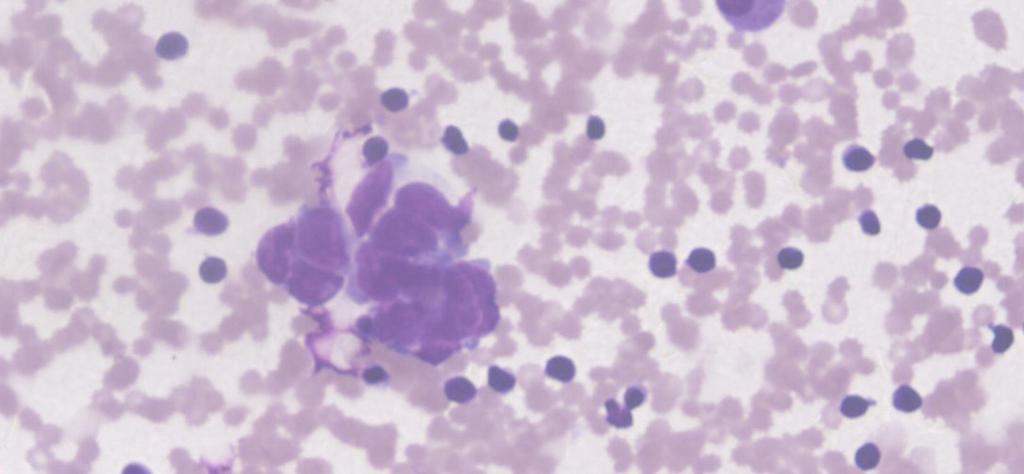
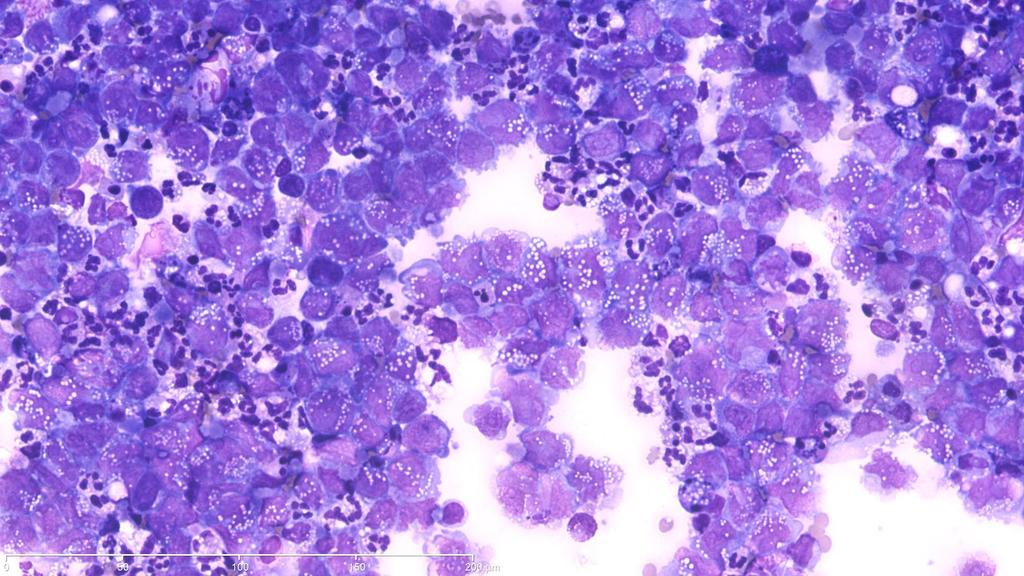
20 Case 3 Respiratory Cytology 22 year old female Mediastinal lymphadenopathy and multiple lung and bone lesions EBUS TBNA
21
22
23
24
25
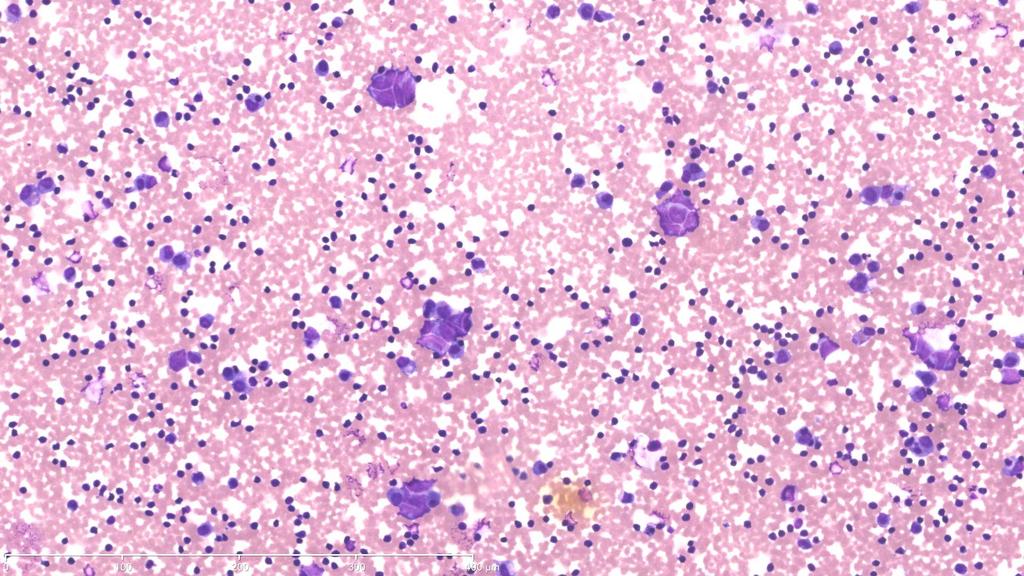
26 Case 3 Respiratory Cytology 22 year old female with mediastinal lymphadenopathy and multiple bone lesions EBUS TBNA Differential Diagnosis A. High Grade Lymphoma B. Adenocarcinoma C. Small Cell Carcinoma D. Nasopharyngeal carcinoma
27 DIAGNOSIS
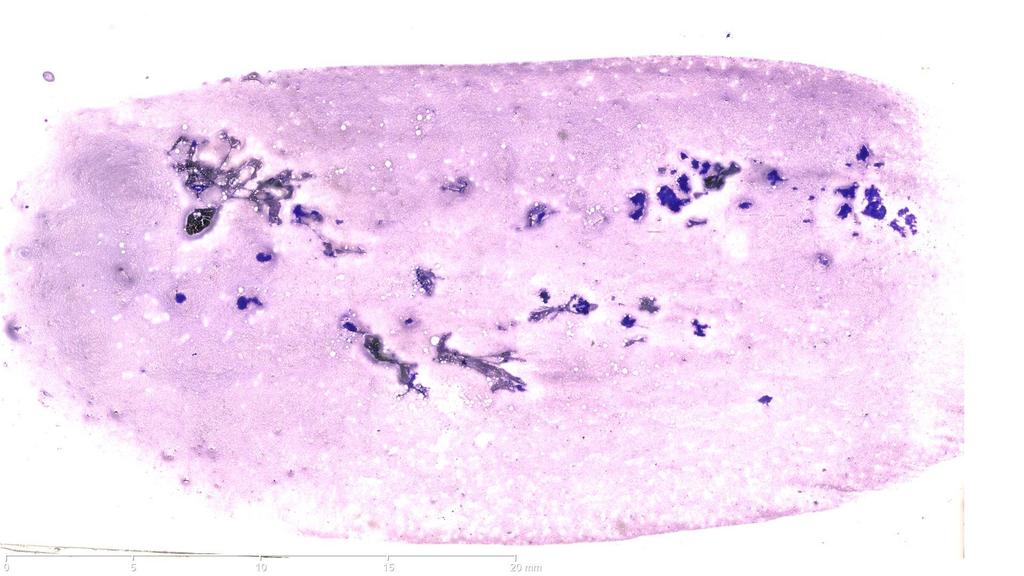
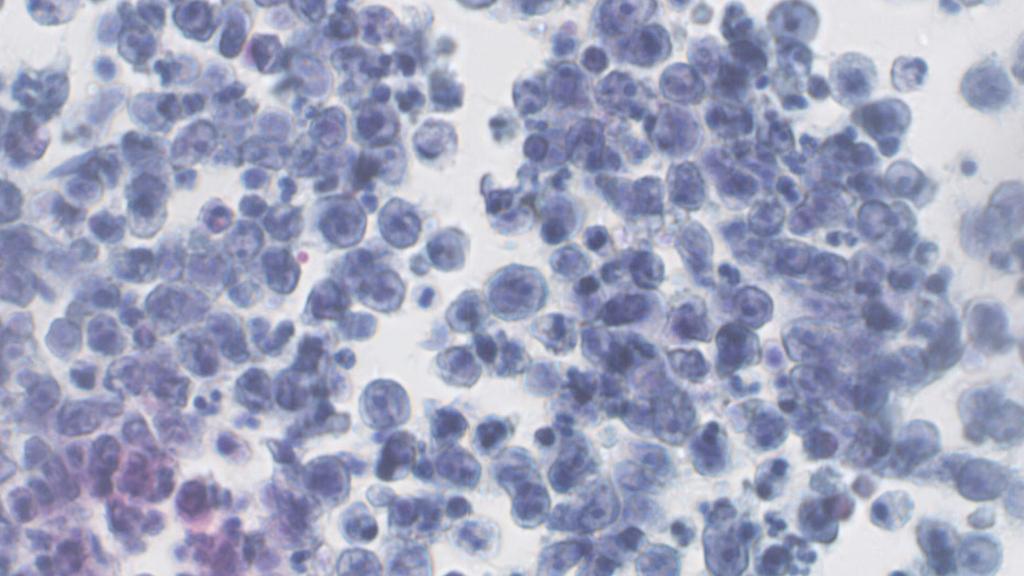
28 Case 4 Respiratory Cytology 65 year old male Loss of sense of smell Cervical and mediastinal lymphadenopathy
29
30
31
32
33
34
35

36
37
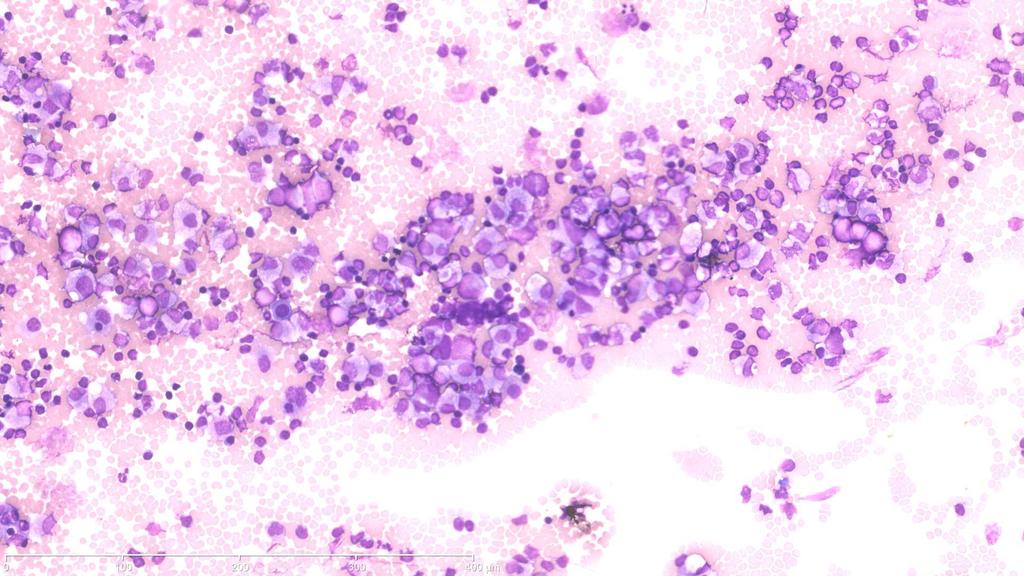
38 Case 4 Respiratory Cytology 65 year old male, loss of sense of smell, cervical and mediastinal lymphadenopathy. EBUS TBNA Differential diagnosis A. High Grade Lymphoma B. Metastatic Olfactory neuroblastoma C. Metastatic Nasopharyngeal carcinoma D. Metastatic Small Cell Carcinoma
39 DIAGNOSIS
40 Case 5 Respiratory Cytology 56 year old gentleman Large hilar mass Superior Vena Cava Obstruction Mediastinal lymphadenopathy EBUS TBNA

41
42
43
44
45
46
47
48 Case 5 Respiratory Cytology 56 year old gentleman, Large hilar mass, SVCO, Mediastinal lymphadenopathy EBUS TBNA Differential diagnosis A. High Grade Lymphoma B. Metastatic Poorly differentiated Non Small Cell Carcinoma C. Metastatic Malignant Melanoma D. Metastatic Small Cell Carcinoma
49 DIAGNOSIS
50 Case 6 Respiratory Cytology 60 year old female 3cm mass and mediastinal lymphadenopathy EBUS FNA
51
52
53
54
55
56 Case 6 Respiratory Cytology 60 year old female with a 3cm mass and mediastinal lymphadenopathy EBUS FNA Differential Diagnosis A. Spindle Cell Squamous Cell Carcinoma B. Granulomatous Inflammation C. Benign Nerve Sheath Tumour D. Malignant Melanoma
57 DIAGNOSIS
58 Case 7 Respiratory Cytology 28 year old male Immunocompromised Respiratory distress and diffuse pulmonary infiltrated on CT scan Bronchoalveolar lavage
59
60
61
62 Case 7 Respiratory Cytology 28 year old male, Immunocompromised, Respiratory distress and diffuse pulmonary infiltrated on CT scan Broncho-alveolar lavage Differential Diagnosis A. Alveolar proteinosis B. Normal C. Pneumocystis jirovecii D. CMV pneumonitis
63 DIAGNOSIS
64 Case 8 Respiratory Cytology 65 year old female Known case of breast cancer Right pleural effusion Pleural effusion cytology
65
66
67
68

69
70
71 Case 8 Respiratory Cytology 65 year old female, Known case of breast cancer, Right pleural effusion. Pleural effusion cytology Differential Diagnosis A. Reactive Effusion B. Malignant Mesothelioma C. Metastatic Breast Carcinoma D. High Grade Lymphoma
72 DIAGNOSIS
73 Case 9 Respiratory Cytology 55 year old male Hilar mass and left sided pleural effusion Pleural effusion cytology
74
75
76
77 Case 9 Respiratory Cytology 55 year old male, Hilar mass and left sided pleural effusion Pleural effusion cytology Differential Diagnosis A. Metastatic Non Small Cell Carcinoma B. Metastatic Small Cell Carcinoma C. Reactive Effusion D. High Grade Lymphoma
78 DIAGNOSIS
79 Case 10 Respiratory Cytology 32 year old gentleman Multiple pulmonary nodules, large mediastinal mass and bilateral pleural effusions Pleural effusion cytology
80
81
82
83
84
85
86 Case 10 Respiratory Cytology 32 year old gentleman, Multiple pulmonary nodules, large mediastinal mass and bilateral pleural effusions Pleural effusion cytology Differential Diagnosis A. Metastatic Non Small Cell Carcinoma B. Metastatic Small Cell Carcinoma C. Malignant Mesothelioma D. High Grade Lymphoma
87 DIAGNOSIS
88 THANKS
The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL
 The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL Conflict of Interest This presentation is supported by AstraZeneca Two main steps before
The Various Methods to Biopsy the Lung PROF SHITRIT DAVID HEAD, PULMONARY DEPARTMENT MEIR MEDICAL CENTER, ISRAEL Conflict of Interest This presentation is supported by AstraZeneca Two main steps before
Lung Cytology: Lessons Learned from Errors in Practice
 Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Respiratory Cytology and Ancillary diagnostic techniques. Dr Alex Rice Royal Brompton Hospital
 Respiratory Cytology and Ancillary diagnostic techniques Dr Alex Rice Royal Brompton Hospital Overview Specialist Cardiothoracic centre BAL specimens and cell differential counts EBUS Diagnostic pitfalls
Respiratory Cytology and Ancillary diagnostic techniques Dr Alex Rice Royal Brompton Hospital Overview Specialist Cardiothoracic centre BAL specimens and cell differential counts EBUS Diagnostic pitfalls
Icd 10 code for hilar adenopathy lung
 Icd 10 code for hilar adenopathy lung The Borg System is 100 % Icd 10 code for hilar adenopathy lung 14-9-2016 The search textbox has an autosuggest feature. When you enter three or more characters, a
Icd 10 code for hilar adenopathy lung The Borg System is 100 % Icd 10 code for hilar adenopathy lung 14-9-2016 The search textbox has an autosuggest feature. When you enter three or more characters, a
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
GROUP 1: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases. Including: Excluding:
 GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Impact of immunostaining of pulmonary and mediastinal cytology
 Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
SCOPE OF PRACTICE PGY-5
 Recognize normal cytomorphology of cells derived from the respiratory, gastrointestinal, and genitourinary tracts, and body fluid (Cerebrospinal fluid, pleural and peritoneal fluid) Recognize normal cytomorphology
Recognize normal cytomorphology of cells derived from the respiratory, gastrointestinal, and genitourinary tracts, and body fluid (Cerebrospinal fluid, pleural and peritoneal fluid) Recognize normal cytomorphology
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis
 1 Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis Optimal management of Cancer Histological diagnosis & accurate staging at presentation Molecular analysis of primary tumour
1 Assessing the lung and mediastinum in cancer-is tissue the issue? George Santis Optimal management of Cancer Histological diagnosis & accurate staging at presentation Molecular analysis of primary tumour
Diagnostic Value of EBUS-TBNA in Various Lung Diseases (Lymphoma, Tuberculosis, Sarcoidosis)
") Diagnostic Value of EBUS-TBNA in Various Lung Diseases (Lymphoma, Tuberculosis, Sarcoidosis) Sevda Sener Cömert, MD, FCCP. SBU, Kartal Dr.Lütfi Kırdar Training and Research Hospital Department of Pulmonary
Diagnostic Value of EBUS-TBNA in Various Lung Diseases (Lymphoma, Tuberculosis, Sarcoidosis) Sevda Sener Cömert, MD, FCCP. SBU, Kartal Dr.Lütfi Kırdar Training and Research Hospital Department of Pulmonary
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Collecting Cancer Data: Lung
 Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer
 Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Lung Cancer - Suspected
 Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Cancer - Suspected Shared Decision Making Lung Cancer: http://www.enhertsccg.nhs.uk/ Patient presents with abnormal CXR Lung cancer - clinical presentation History and Examination Incidental finding
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Chest Radiology Interpretation: Findings of Tuberculosis
 Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Chest Radiology Interpretation: Findings of Tuberculosis Get out your laptops, smart phones or other devices pollev.com/chestradiology Case #1 1 Plombage Pneumonia Cancer 2 Reading the TB CXR Be systematic!
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
GOALS AND OBJECTIVES FOR THORACIC PATHOLOGY ROTATION
 GOALS AND OBJECTIVES FOR THORACIC PATHOLOGY ROTATION LEVEL: PGY2, PGY3, PGY5 A number of these rotations are introductory in nature, as they are major subspecialties, and are followed by two more blocks
GOALS AND OBJECTIVES FOR THORACIC PATHOLOGY ROTATION LEVEL: PGY2, PGY3, PGY5 A number of these rotations are introductory in nature, as they are major subspecialties, and are followed by two more blocks
American College of Radiology ACR Appropriateness Criteria
 American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
American College of Radiology ACR Criteria Radiologic Management of Thoracic Nodules and Masses Variant 1: Middle-aged patient (35 60 years old) with an incidental 1.5-cm lung nodule. The lesion was smooth.
MEDIASTINAL STAGING surgical pro
 MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
Electromagnetic navigational bronchoscopy in patients with solitary pulmonary nodules
 Original article Electromagnetic navigational bronchoscopy in patients with solitary pulmonary nodules Samuel Copeland MD, Shrinivas Kambali MD, Gilbert Berdine MD, Raed Alalawi MD Abstract Background:
Original article Electromagnetic navigational bronchoscopy in patients with solitary pulmonary nodules Samuel Copeland MD, Shrinivas Kambali MD, Gilbert Berdine MD, Raed Alalawi MD Abstract Background:
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
September 2014 Imaging Case of the Month. Michael B. Gotway, MD. Department of Radiology Mayo Clinic Arizona Scottsdale, AZ
 September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
September 2014 Imaging Case of the Month Michael B. Gotway, MD Department of Radiology Mayo Clinic Arizona Scottsdale, AZ Clinical History: A 57-year-old non-smoking woman presented to her physician as
Cancer of Unknown Primary (CUP) Protocol
 Protocol") 1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Approach to Pulmonary Nodules
 Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
Approach to Pulmonary Nodules Edwin Jackson, Jr., DO Assistant Professor-Clinical Director, James Early Detection Clinic Department of Internal Medicine Division of Pulmonary, Allergy, Critical Care and
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY
 in HEAD & NECK SURGERY") Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Lung Cancer Case Study
 Lung Cancer Case Study Presented by s GP Education Programme 2 Part One Initial presentation 60 year old lady, presents with a 6 week history of right sided chest pain. The pain is like a dull ache, but
Lung Cancer Case Study Presented by s GP Education Programme 2 Part One Initial presentation 60 year old lady, presents with a 6 week history of right sided chest pain. The pain is like a dull ache, but
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Case of the Day Chest
 Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
Case of the Day Chest Darin White MDCM FRCPC Department of Radiology, Mayo Clinic 76 th Annual Scientific Meeting Canadian Association of Radiologists Montreal, QC April 26, 2013 2013 MFMER slide-1 Disclosures
PET CT for Staging Lung Cancer
 PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
Division of Diagnostic Imaging, The University of Texas M.D. Anderson Cancer Center, Houston, Texas, USA
 89 Lymphology 28 (1995) 89-94 Division of Diagnostic Imaging, The University of Texas M.D. Anderson Cancer Center, Houston, Texas, USA ABSTRACT The anatomy of the posterior intercostal lymphatics and lymph
89 Lymphology 28 (1995) 89-94 Division of Diagnostic Imaging, The University of Texas M.D. Anderson Cancer Center, Houston, Texas, USA ABSTRACT The anatomy of the posterior intercostal lymphatics and lymph
Collaborative Stage. Site-Specific Instructions - LUNG
 Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
AJCC-NCRA Education Needs Assessment Results
 AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
Radiology-Pathology Conference
 July 31, 2009 Radiology-Pathology Conference Daniel T Ginat, M.D., M.S. Sharlin Johnykutty,, M.D. Presentation material is for education purposes only. All rights reserved. 2009 URMC Radiology Page 1 of
July 31, 2009 Radiology-Pathology Conference Daniel T Ginat, M.D., M.S. Sharlin Johnykutty,, M.D. Presentation material is for education purposes only. All rights reserved. 2009 URMC Radiology Page 1 of
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
False-Positive Somatostatin Receptor Scintigraphy: Really?
 Logo False-Positive Somatostatin Receptor Scintigraphy: Really? Dr. Augusto Llamas-Olier, Dr. Maria Cristina Martinez, Dr. Emperatriz Angarita, Dr. Amelia De Los Reyes Nuclear medicine department. Instituto
Logo False-Positive Somatostatin Receptor Scintigraphy: Really? Dr. Augusto Llamas-Olier, Dr. Maria Cristina Martinez, Dr. Emperatriz Angarita, Dr. Amelia De Los Reyes Nuclear medicine department. Instituto
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
Case 1: Question. 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule
 HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
HRCT WORK SHOP Case 1 Case 1: Question 1.1 What is the main pattern of this HRCT? 1. Intralobular line 2. Groundglass opacity 3. Perilymphatic nodule Case 1: Question 1.2 What is the diagnosis? 1. Hypersensitivity
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
PLACE LABEL HERE. Radiation Therapy Oncology Group Phase II - SBRT - Medically Inoperable I /II NSCLC Follow-up Form. RTOG Study No.
 Radiation Therapy Oncology Group Phase II - SBRT - Medically Inoperable I /II NSCLC Follow-up Form RTOG Study No. 0813 Case # Name RTOG Patient ID INSTRUCTIONS: Submit this form at the appropriate followup
Radiation Therapy Oncology Group Phase II - SBRT - Medically Inoperable I /II NSCLC Follow-up Form RTOG Study No. 0813 Case # Name RTOG Patient ID INSTRUCTIONS: Submit this form at the appropriate followup
Lung tumors & pleural lesions
 Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
Lung tumors & pleural lesions A brief introduction 95% of lung tumors are carcinomas Among the remaining 5%, we will discuss: -Hamartoma the most common benign lung tumor spherical, coin lesion on x-rays
Mesothelioma: diagnostic challenges from a pathological perspective. Naseema Vorajee August 2016
 Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Video-Mediastinoscopy Thoracoscopy (VATS)
") Surgical techniques Video-Mediastinoscopy Thoracoscopy (VATS) Gunda Leschber Department of Thoracic Surgery ELK Berlin Chest Hospital, Berlin, Germany Teaching Hospital of Charité Universitätsmedizin Berlin
Surgical techniques Video-Mediastinoscopy Thoracoscopy (VATS) Gunda Leschber Department of Thoracic Surgery ELK Berlin Chest Hospital, Berlin, Germany Teaching Hospital of Charité Universitätsmedizin Berlin
PET/CT in lung cancer
 PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
PET/CT in lung cancer Andrei Šamarin North Estonia Medical Centre 3 rd Baltic Congress of Radiology 08.10.2010 Imaging in lung cancer Why do we need PET/CT? CT is routine imaging modality for staging of
Interesting Cases. Pulmonary
 Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
Interesting Cases Pulmonary 54M with prior history of COPD, hep B/C, and possible history of TB presented with acute on chronic dyspnea, and productive cough Hazy opacity overlying the left hemithorax
All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis
 All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis Presenter Disclosure Faculty/Speaker: Dr. Brett Finney BSc MD CCFP Relationships with financial sponsors: Grants/Research
All I Need Is The Air That I Breathe: A Case Study of Immunotherapy and Severe Pneumonitis Presenter Disclosure Faculty/Speaker: Dr. Brett Finney BSc MD CCFP Relationships with financial sponsors: Grants/Research
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
TB Radiology for Nurses Garold O. Minns, MD
 TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TB Nurse Case Management Salina, Kansas March 31-April 1, 2010 TB Radiology for Nurses Garold O. Minns, MD April 1, 2010 TB Radiology for Nurses Highway Patrol Training Center Salina, KS April 1, 2010
TUMOR,NEOPLASM. Pathology Department, Zhejiang University School of Medicine,
 TUMOR,NEOPLASM Pathology Department, Zhejiang University School of Medicine, 马丽琴,maliqin198@zju.edu.cn The points in this chapter What is a neoplasm (conception) Morphology of neoplasm Macroscopy of Neoplasm
TUMOR,NEOPLASM Pathology Department, Zhejiang University School of Medicine, 马丽琴,maliqin198@zju.edu.cn The points in this chapter What is a neoplasm (conception) Morphology of neoplasm Macroscopy of Neoplasm
Metastatic Renal Cell Carcinoma: The Importance of Immunohistochemistry in Differential Diagnosis
 This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
This is an Open Access article licensed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 License (www.karger.com/oa-license), applicable to the online version of the article
* MILIARY MOTTLING --
 * MILIARY MOTTLING -- RARE CAUSE DR ARATHI SRINIVASAN FELLOW IN PEDIATRIC HEMATO ONCOLOGY DR A ANDAL DEPARTMENT OF PEDIATRICS DR JULIUS XAVIER SCOTT DEPARTMENT OF PEDIATRIC HEMATO ONCOLOGY KANCHI KAMAKOTI
* MILIARY MOTTLING -- RARE CAUSE DR ARATHI SRINIVASAN FELLOW IN PEDIATRIC HEMATO ONCOLOGY DR A ANDAL DEPARTMENT OF PEDIATRICS DR JULIUS XAVIER SCOTT DEPARTMENT OF PEDIATRIC HEMATO ONCOLOGY KANCHI KAMAKOTI
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Evaluation of Neck Mass. Disclosure. Learning Objectives 3/24/2014. Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ. Nothing to disclose
 Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
CALGARY ZONE PULMONARY REFERRAL QUICK REFERENCE
 CALGARY ZONE PULMONARY REFERRAL QUICK REFERENCE EMERGENCY (Patient needs to be seen immediately) Hemoptysis (Active & 2 TBSP per day) Hypoxemia (if resting O2 SAT 85%) Pulmonary embolism (Acute - known
CALGARY ZONE PULMONARY REFERRAL QUICK REFERENCE EMERGENCY (Patient needs to be seen immediately) Hemoptysis (Active & 2 TBSP per day) Hypoxemia (if resting O2 SAT 85%) Pulmonary embolism (Acute - known
Malignant Effusions. Anantham Devanand Respiratory and Critical Care Medicine Singapore General Hospital
 Malignant Effusions Anantham Devanand Respiratory and Critical Care Medicine Singapore General Hospital Malignant Effusions Definition: Presence of malignant cells in the pleural space 75% are caused by
Malignant Effusions Anantham Devanand Respiratory and Critical Care Medicine Singapore General Hospital Malignant Effusions Definition: Presence of malignant cells in the pleural space 75% are caused by
Case 1 : Question. 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random
 Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Interesting case Case 1 Case 1 : Question 1.1 What is the intralobular distribution? 1. Centrilobular 2. Perilymphatic 3. Random Case 1: Answer 1.1 What is the intralobular distribution? 1. Centrilobular
Differential Diagnosis in Conventional Radiology
 Differential Diagnosis in Conventional Radiology Bearbeitet von Francis A. Burgener, Martti Kormano, Tomi Pudas Neuausgabe 2007. Buch. 872 S. Hardcover ISBN 978 3 13 656103 4 Format (B x L): 21 x 29,7
Differential Diagnosis in Conventional Radiology Bearbeitet von Francis A. Burgener, Martti Kormano, Tomi Pudas Neuausgabe 2007. Buch. 872 S. Hardcover ISBN 978 3 13 656103 4 Format (B x L): 21 x 29,7
MEDICAL POLICY Gene Expression Profiling for Cancers of Unknown Primary Site
 POLICY: PG0364 ORIGINAL EFFECTIVE: 04/22/16 LAST REVIEW: 07/26/18 MEDICAL POLICY Gene Expression Profiling for Cancers of Unknown Primary Site GUIDELINES This policy does not certify benefits or authorization
POLICY: PG0364 ORIGINAL EFFECTIVE: 04/22/16 LAST REVIEW: 07/26/18 MEDICAL POLICY Gene Expression Profiling for Cancers of Unknown Primary Site GUIDELINES This policy does not certify benefits or authorization
Malignant Cardiac Tumors Rad-Path Correlation
 Malignant Cardiac Tumors Rad-Path Correlation Vincent B. Ho, M.D., M.B.A. 1 Jean Jeudy, M.D. 2 Aletta Ann Frazier, M.D. 2 1 Uniformed Services University of the Health Sciences 2 University of Maryland
Malignant Cardiac Tumors Rad-Path Correlation Vincent B. Ho, M.D., M.B.A. 1 Jean Jeudy, M.D. 2 Aletta Ann Frazier, M.D. 2 1 Uniformed Services University of the Health Sciences 2 University of Maryland
PULMONARY TUBERCULOSIS RADIOLOGY
 PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
PULMONARY TUBERCULOSIS RADIOLOGY RADIOLOGICAL MODALITIES Medical radiophotography Radiography Fluoroscopy Linear (conventional) tomography Computed tomography Pulmonary angiography, bronchography Ultrasonography,
Contents. Basic Ultrasound Principles and Terminology. Ultrasound Nodule Characteristics
 Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
Contents Basic Ultrasound Principles and Terminology Basic Ultrasound Principles... 1 Ultrasound System... 2 Linear Transducer for Superficial Images and Ultrasound-Guided FNA... 3 Scanning Planes... 4
SELECTED DILEMMAS IN RESPIRATORY CYTOPATHOLOGY (2 CASES)
") SELECTED DILEMMAS IN RESPIRATORY CYTOPATHOLOGY (2 CASES) Dr. Mariamma Joseph Professor of Pathology Division Head Cytopathology Department of Pathology and Laboratory Medicine LHSC and Western University
SELECTED DILEMMAS IN RESPIRATORY CYTOPATHOLOGY (2 CASES) Dr. Mariamma Joseph Professor of Pathology Division Head Cytopathology Department of Pathology and Laboratory Medicine LHSC and Western University
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
Fellowship in Cytopathology Department of Pathology. All India Institute of Medical Sciences (AIIMS) Jodhpur, Rajasthan, India
 Jodhpur, Rajasthan, India") Fellowship in Cytopathology Department of Pathology All India Institute of Medical Sciences (AIIMS) Jodhpur, Rajasthan, India Syllabus for Fellowship in Cytopathology: FNAC Direct, Guided, EUS Exfoliative
Fellowship in Cytopathology Department of Pathology All India Institute of Medical Sciences (AIIMS) Jodhpur, Rajasthan, India Syllabus for Fellowship in Cytopathology: FNAC Direct, Guided, EUS Exfoliative
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
FINALIZED SEER SINQ S MAY 2012
 FINALIZED SEER SINQ S MAY 2012 : 20120039 Primary site/heme & Lymphoid Neoplasms: What site do I code this to and what rule applies? How did you arrive at this? Please advise. See discussion. Patient with
FINALIZED SEER SINQ S MAY 2012 : 20120039 Primary site/heme & Lymphoid Neoplasms: What site do I code this to and what rule applies? How did you arrive at this? Please advise. See discussion. Patient with
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Page 28 Oropharynx p16 positive Pathological Stage II,T2 N2 M0 T3 N0,N1 M0 Stage II,T2 N2 M0 T3,T4 N0,N1 M0 Page 61 Oesophagus Adenocarcinoma Pathological
UICC TNM 8 th Edition Errata ions are in italics Page 28 Oropharynx p16 positive Pathological Stage II,T2 N2 M0 T3 N0,N1 M0 Stage II,T2 N2 M0 T3,T4 N0,N1 M0 Page 61 Oesophagus Adenocarcinoma Pathological
Bronchial syndrome. Atelectasis Draining bronchus Bronchiectasis
 Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Bronchial syndrome Atelectasis Draining bronchus Bronchiectasis Etienne Leroy Terquem Pierre L Her SPI / ISP Soutien Pneumologique International / International Support for Pulmonology Atelectasis Consequence
Reparatory system 18 lectures Heyam Awad
 Reparatory system 18 lectures 8-10 Heyam Awad These lectures cover the following topics 1. Diffuse hemorrhagic syndromes 2. Lung tumors important: theses slides are your study source for these lectures.
Reparatory system 18 lectures 8-10 Heyam Awad These lectures cover the following topics 1. Diffuse hemorrhagic syndromes 2. Lung tumors important: theses slides are your study source for these lectures.
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
Pulmonary Sarcoidosis - Radiological Evaluation
 Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
Original Research Article Pulmonary Sarcoidosis - Radiological Evaluation Jayesh Shah 1, Darshan Shah 2*, C. Raychaudhuri 3 1 Associate Professor, 2 1 st Year Resident, 3 Professor and HOD Radiology Department,
PDF created with pdffactory Pro trial version
 Neuroblastoma Tumor derived from neural crest cell that form the sympathetic ganglia&adrenal medulla. Causes *unknown. *familial neuroblastoma has been reported but is rare. * The incidence is 1:100,000
Neuroblastoma Tumor derived from neural crest cell that form the sympathetic ganglia&adrenal medulla. Causes *unknown. *familial neuroblastoma has been reported but is rare. * The incidence is 1:100,000
Mediastinal Incidentalomas
 ORIGINAL ARTICLE Jos A. Stigt, MD,* James E. Boers, MD, PhD, Ad H. Oostdijk, MD, Jan-Willem K. van den Berg, MD, PhD,* and Harry J. M. Groen, MD, PhD Introduction: Incidental mediastinal lymphadenopathy
ORIGINAL ARTICLE Jos A. Stigt, MD,* James E. Boers, MD, PhD, Ad H. Oostdijk, MD, Jan-Willem K. van den Berg, MD, PhD,* and Harry J. M. Groen, MD, PhD Introduction: Incidental mediastinal lymphadenopathy
Pleural effusion as an initial manifestation in a patient with primary pulmonary monoclonal B-cell lymphocyte proliferative disease
 Du et al. Respiratory Research (2018) 19:247 https://doi.org/10.1186/s12931-018-0941-6 LETTER TO THE EDITOR Pleural effusion as an initial manifestation in a patient with primary pulmonary monoclonal B-cell
Du et al. Respiratory Research (2018) 19:247 https://doi.org/10.1186/s12931-018-0941-6 LETTER TO THE EDITOR Pleural effusion as an initial manifestation in a patient with primary pulmonary monoclonal B-cell
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma
 July 2016 New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma Contributed by: Laurel Rose, MD, Resident Physician, Indiana University School of Medicine,
July 2016 New lung lesion in a 55 year-old male treated with chemoradiation for non-small cell lung carcinoma Contributed by: Laurel Rose, MD, Resident Physician, Indiana University School of Medicine,
FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations
 Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Chest XRay interpretation INTERPRETATIONS Identifications: Name & Date Technical evaluation Basic Interpretations TECHNICAL EVALUATION 1. Projection: AP/PA view To differentiate between AP & PA films,
Reparatory system lectures Heyam Awad
 Reparatory system lectures 8-10 Heyam Awad note These lectures cover the following topics 1. Diffuse hemorrhagic syndromes 2. Lung tumors important: theses slides are your study source for these lectures.
Reparatory system lectures 8-10 Heyam Awad note These lectures cover the following topics 1. Diffuse hemorrhagic syndromes 2. Lung tumors important: theses slides are your study source for these lectures.
SCBT-MR 2015 Incidentaloma on Chest CT
 SCBT-MR 2015 Incidentaloma on Chest CT Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report Incidentaloma Pulmonary Nodule Mediastinal Lymph Node Coronary Artery Calcium Incidental
SCBT-MR 2015 Incidentaloma on Chest CT Reginald F. Munden MD, DMD, MBA I have no conflicts of interest to report Incidentaloma Pulmonary Nodule Mediastinal Lymph Node Coronary Artery Calcium Incidental
Tumor Board Discussions: Case 1
 Tumor Board Discussions: Case 1 David S. Ettinger, MD The Alex Grass Professor of Oncology Johns Hopkins University School of Medicine Baltimore, Maryland Case #1 50-year-old Asian female, never smoker
Tumor Board Discussions: Case 1 David S. Ettinger, MD The Alex Grass Professor of Oncology Johns Hopkins University School of Medicine Baltimore, Maryland Case #1 50-year-old Asian female, never smoker
Invasion And Metastasis. Wirsma Arif Harahap Surgical Oncologist Surgery Department Andalas Medical Schoool
 Invasion And Metastasis Wirsma Arif Harahap Surgical Oncologist Surgery Department Andalas Medical Schoool Biology of tumor growth The natural history of malignant tumors can be divided into four phase:
Invasion And Metastasis Wirsma Arif Harahap Surgical Oncologist Surgery Department Andalas Medical Schoool Biology of tumor growth The natural history of malignant tumors can be divided into four phase:
Pathology of the Respiratory System 5: Lung and Thoracic Cavity
 Pathology of the Respiratory System 5: Lung and Thoracic Cavity Shannon Martinson, Jan 2017 http://people.upei.ca/smartinson/ VPM 222 Systemic Pathology DISORDERS OF THE LUNG Congenital Pigmentary deposition
Pathology of the Respiratory System 5: Lung and Thoracic Cavity Shannon Martinson, Jan 2017 http://people.upei.ca/smartinson/ VPM 222 Systemic Pathology DISORDERS OF THE LUNG Congenital Pigmentary deposition
Right infrahilar nodule
 Right infrahilar nodule Search Infrahilar nodule Nov 9, 2015.. CT chest showed a right infrahilar mass 3.5 2.5 cm along with multiple bilateral lung nodules of size 9 to 11 mm. Bronchoscopy. Jun 13, 2015.
Right infrahilar nodule Search Infrahilar nodule Nov 9, 2015.. CT chest showed a right infrahilar mass 3.5 2.5 cm along with multiple bilateral lung nodules of size 9 to 11 mm. Bronchoscopy. Jun 13, 2015.
Damaris Pena, Gilda Diaz-Fuentes, and Sindhaghatta Venkatram
 Hindawi Case Reports in Pulmonology Volume 2017, Article ID 3851849, 5 pages https://doi.org/10.1155/2017/3851849 Case Report Purulent Appearing Material in an Endobronchial Ultrasound-Guided Transbronchial
Hindawi Case Reports in Pulmonology Volume 2017, Article ID 3851849, 5 pages https://doi.org/10.1155/2017/3851849 Case Report Purulent Appearing Material in an Endobronchial Ultrasound-Guided Transbronchial
MRI XR, CT, NM. Principal Modality (2): Case Report # 2. Date accepted: 15 March 2013
: Case Report # 2. Date accepted: 15 March 2013") Radiological Category: Musculoskeletal Principal Modality (1): Principal Modality (2): MRI XR, CT, NM Case Report # 2 Submitted by: Hannah Safia Elamir, D.O. Faculty reviewer: Naga R. Chinapuvvula, M.D.
Radiological Category: Musculoskeletal Principal Modality (1): Principal Modality (2): MRI XR, CT, NM Case Report # 2 Submitted by: Hannah Safia Elamir, D.O. Faculty reviewer: Naga R. Chinapuvvula, M.D.
DIAGNOSIS OF LUNG CANCER. Dr. Sayeed ahmed, Assistant prof, MD,DAA.
 DIAGNOSIS OF LUNG CANCER Dr. Sayeed ahmed, Assistant prof, MD,DAA. Diagnosis of lung cancer can be done by 1) Clinical presentation 2) Investigations a) non invasive b) invasive Clinical Presentation Metastatic
DIAGNOSIS OF LUNG CANCER Dr. Sayeed ahmed, Assistant prof, MD,DAA. Diagnosis of lung cancer can be done by 1) Clinical presentation 2) Investigations a) non invasive b) invasive Clinical Presentation Metastatic
Dr Nick McIvor. Dr John Chaplin. Head & Neck Surgeon Auckland City Hospital Auckland. Auckland Head & Neck Surgeon Gillies Hospital Auckland
 Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00