FNA Cytology of Metastatic Malignancies of Unknown Primary Site
|
|
|
- Rodger Waters
- 6 years ago
- Views:
Transcription
1 FNA Cytology of Metastatic Malignancies of Unknown Primary Site Tarik M. Elsheikh Jan F. Silverman
2 Pathologic Diagnosis of Metastasis Smaller specimens, less invasive techniques FNA cytology is highly accurate Determine primary site No previous history of malignancy Prior pathology not available Unpredictable pattern of metastasis Accurate Dx modify patient management
3 Metastatic Malignancies of Unknown Primary Site (MUP) 8 th most common malignancy 5-10% of all non-cutaneous malignancies Up to 15% of new referrals to hospital based oncology centers Standard panel of multi-agent chemotherapy Poor prognosis. Median survival 4-12 mo.
4 Metastases of Unknown Primary Site Definition: Bx confirmed. 1º site not found after rigorous, but limited initial clinical and radiographic evaluation careful Hx, physical exam, lab, x-rays, etc..
5 Is Workup of MUP Necessary? Optimal management may be organspecific, and rely on accurate determination of primary site Inability to ID a primary major clinical challenge Patient anxiety:? Inadequate evaluation by physician? Prognosis improved if primary is found
6 Cost Effectiveness of Pathologic Workup Extensive radiological exams & serum tumor markers often unsuccessful in finding 1º site Pathologic evaluation (including extended IHC panel) is more cost effective than clinical workup Clinical tests alone Cost per Success Theoretical costeffectiveness patient rate ratio $ 18,000 * 20 % $ 250,000 IHC panel** $ 2, % $ 2,900 * excluding physician charges ** panel of 6 tests Wick et al 1999
7 Cost Effectiveness of Pathologic Workup 2 Overutilization occurs in individual cases or by individual pathologists Too many Ab s in 30% of cases Unnecessary IHC in 10% of cases
8 FNA Diagnosis of MUP A Clinico-pathologic approach 1. Cytomorphologic features 2. Ancillary studies: IHC 3. Clinical patterns of metastases
9 FNA Diagnosis of MUP 2 A Clinico-pathologic approach 1. Cytomorphologic features Histologic types (specific cell lineage): adenoca, squamous ca, melanoma, etc. Morphologic patterns (non specific cell lineage): small cell, large cell, oncocytic, spindle, etc. 2. Ancillary studies: IHC 3. Clinical patterns of metastases
10 CYTOMORPHOLOGIC PATTERNS OF MUP Specific Cell Lineage Cell Pattern / Type Squamous CA Sarcoma Melanoma Adenocarcinoma Lymphoma Small Cell Oncocytic/Granular Clear Cell Pleomorphic/Giant Cell Spindle cell Polygonal, Large Cell
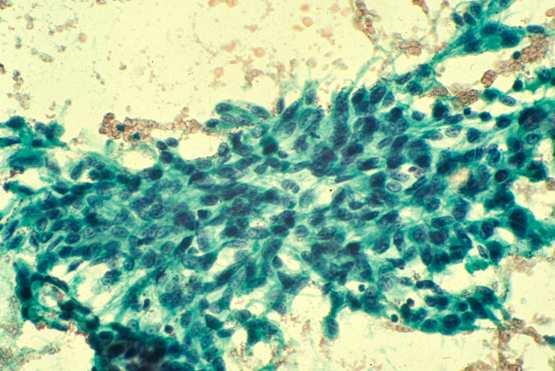
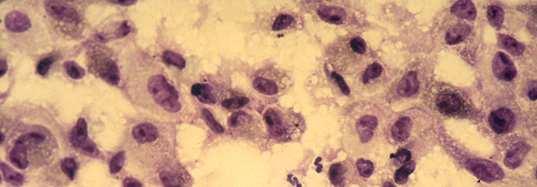
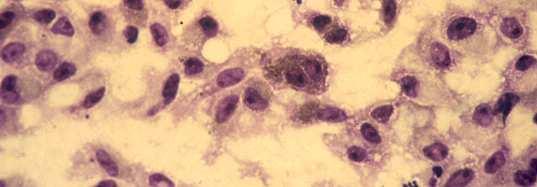
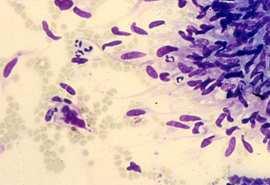
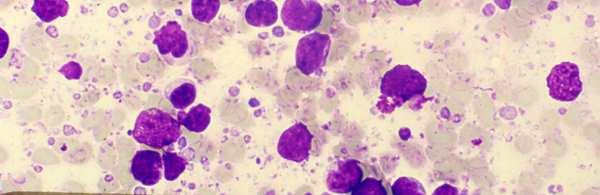
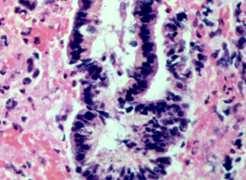
11 Case 1 CT guided FNA biopsy of a kidney mass in a 68 year old woman.
12 Diagnosis: Metastatic adenocarcinoma. A lung primary was subsequently found
13 Adenocarcinoma Most common MUP (60%) W-M differentiated adenocarcinoma median survival 3-6 months Lung & pancreas: most common (40%) GI tract Liver Nonspecific diagnosis 1º vs. MET
14 Morphologic Patterns of Differentiated Adenocarcinoma (W-M) Adenocarcinoma Columnar/ductal Microacinar Mucinous Papillary Low grade Pancreas Bile duct Colon Lung(BAC) Breast Carcinoid Hyperchromatic COLON Endometrioid CA High grade Hypochromatic Lung Pancreas Prostate Bile duct Stomach Prostate NEC Thyroid Granulosa CT Breast Ovary Pancreas GIT Chordoma Thyroid Ovary Kidney Endometrium Breast Lung
15 Adenocarcinoma Columnar/ductal Low grade High grade Hyperchromatic Hypochromatic


16 Adenocarcinoma: Low Grade Columnar/ductal Cohesive clusters and geographic flat sheets
17 Low Grade Columnar/Ductal Uniform cell population with bland appearance Low N/C ratio, finely granular chromatin, small nucleoli Round to elongated nuclei, luminal borders
18 Low Grade Columnar/Ductal Adenocarcinoma Carcinoid Pancreas Breast Bile duct Lung (BAC) Colon Carcinoid Cholangiocarcinoma


19 High Grade Columnar/Ductal Adenocarcinoma Cohesive clusters and flat sheets


20 High Grade Columnar/Ductal Adenocarcinoma Nuclear overlapping, haphazard arrangement, significant pleomorphism. Acinar formation may bee seen.
21 Adenocarcinoma Columnar/ductal Low grade High grade Hyperchromatic Hypochromatic
22 High Grade Columnar/Ductal Adenocarcinoma Hypochromatic Lung Pancreas Bile duct Prostate Stomach

")
23 High Grade Columnar/Ductal Adenocarcinoma Hyperchromatic COLON Endometrioid CA (endometrium, ovary, cervix) Bile duct


24 Columnar/ductal Low grade High grade Hyperchromatic Hypochromatic LUNG PANCREAS COLON Prostate Endometrioid Bile duct Stomach FNA of vertebral body High grade, columnar/ductal Metastatic lung CA to bone
25 Columnar/ductal Low grade Hyperchromatic High grade Hypochromatic COLON Endometrioid LUNG PANCREAS Prostate Bile duct Stomach FNA of liver Metastatic pancreatic CA to liver


26 Columnar/ductal Low grade Hyperchromatic High grade Hypochromatic COLON Endometrioid ca bile duct LUNG PANCREAS Prostate Bile duct Stomach FNA of liver High grade, columnar/ductal Metastatic colon CA to liver
27 CYTOMORPHOLOGIC PATTERNS OF METASTASIS OF UNKNOWN PRIMARY ORGIN Specific Cell Lineage Cell Pattern / Type Squamous CA Sarcoma Melanoma Adenocarcinoma Lymphoma Small Cell Oncocytic/Granular Clear Cell Pleomorphic/Giant Cell Spindle cell Polygonal, Large Cell
28 CARCINOMA Adenocarcinoma (60%) Squamous cell carcinoma (10%) Undifferentiated CA/P.D. Small cell/ne carcinoma Melanoma Modified from DeMay p


29 Squamous Cell Carcinoma
30 MELANOMA Metastasis to unusual sites Mimics other malignancies Primary occult or not apparent by history

31
32 Melan - A
33 Malignant Melanoma Variants Rhabdoid Signet-ring Spindle Myxoid Desmoplastic Ballon Cell Small Cell
34 Signet-Ring Melanoma Ballon Cell Spindle Cell Small Cell MM

35 Rhabdoid MM

36 Pigmented dendritic histiocytes
37 SARCOMA Very unusual unknown primary Primary site usually obvious Diff Dx: Sarcomatoid carcinoma / melanoma Spindle, epitheliod, pleomorphic, small cell, myxoid
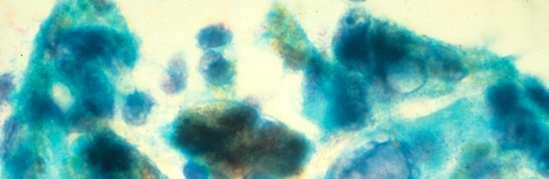
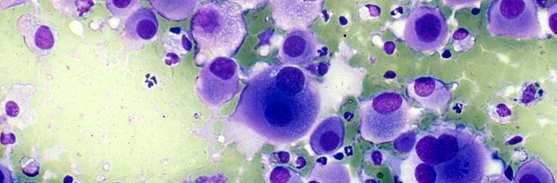
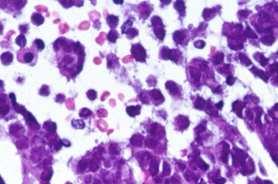
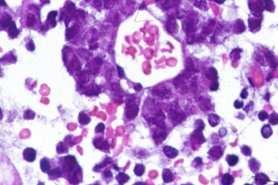
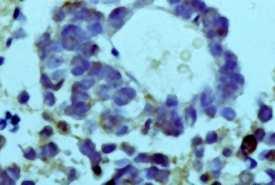
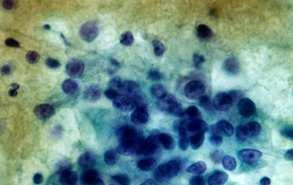
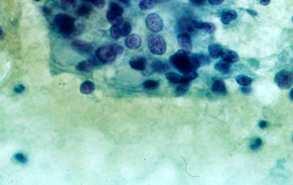
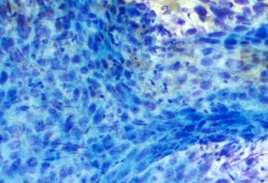
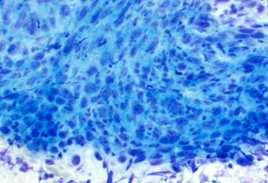
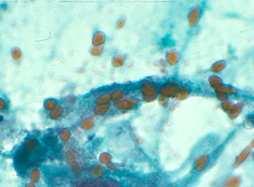
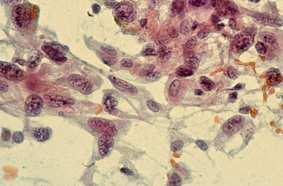
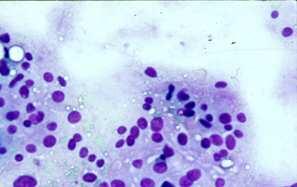
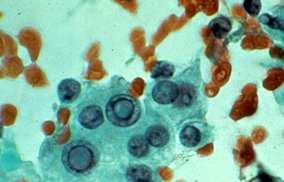
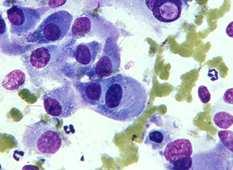
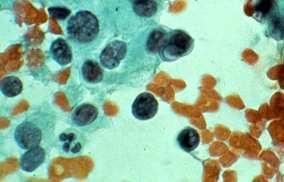
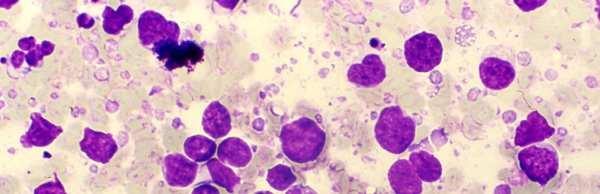
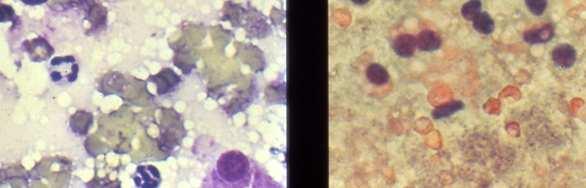
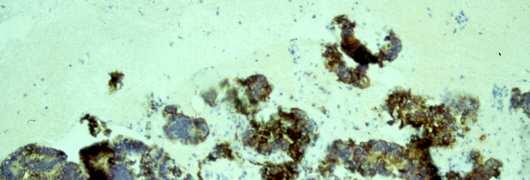
38 Case 2 An 81 year old woman was identified as having a right hilar lung mass. FNA biopsy was performed.
39
40
41 Case 2 DIAGNOSIS Metastatic Hurthle cell carcinoma of the thyroid
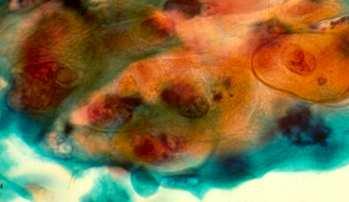
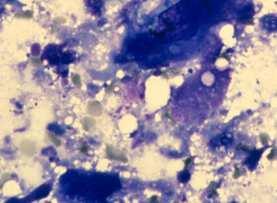
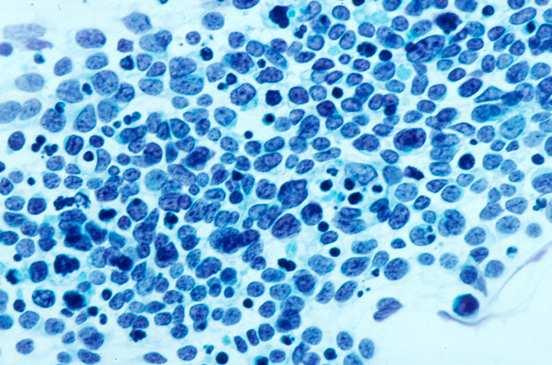
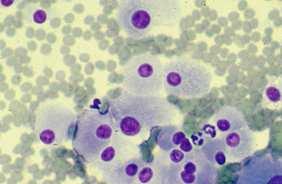
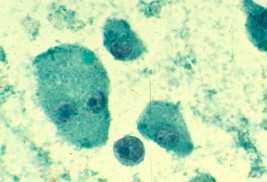
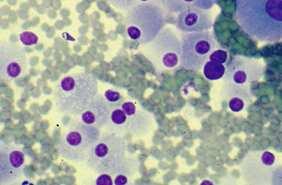
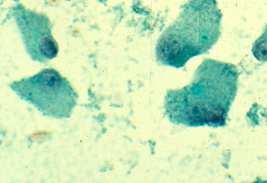
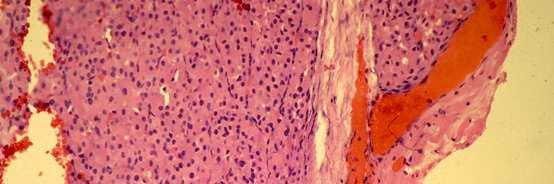
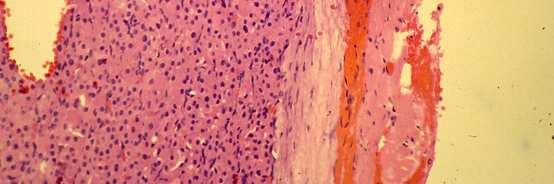
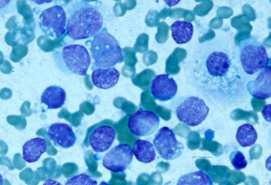
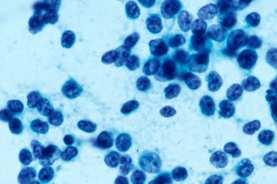
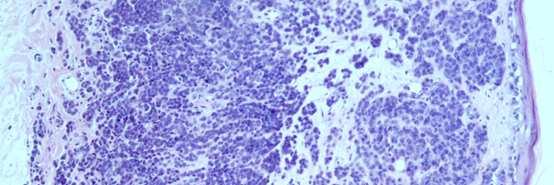
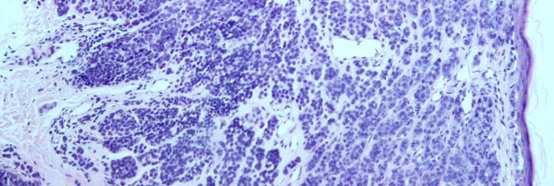
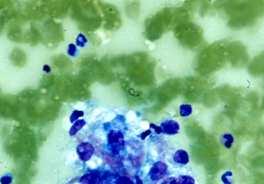
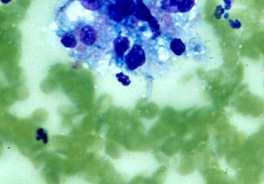
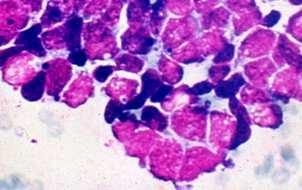
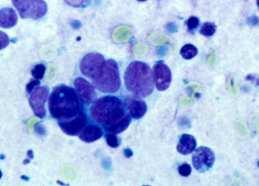
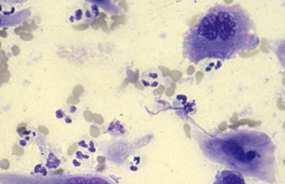
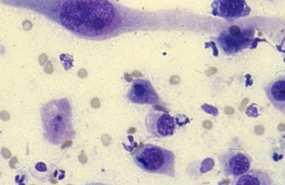
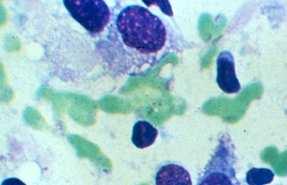
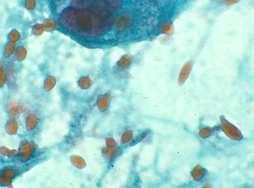
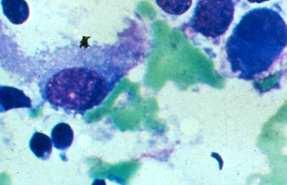
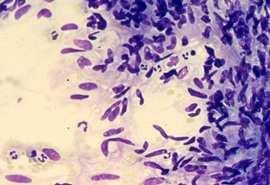
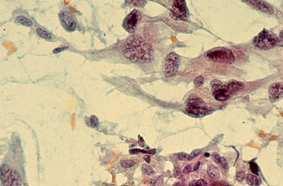
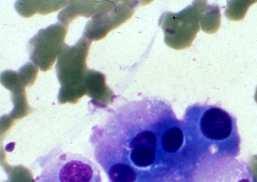
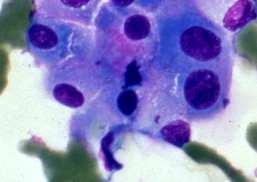
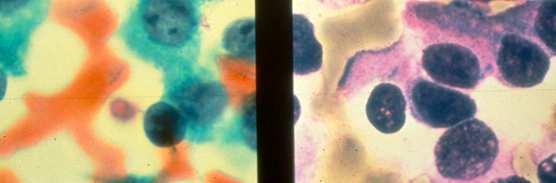
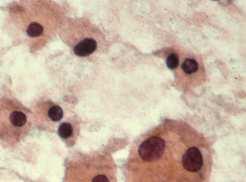
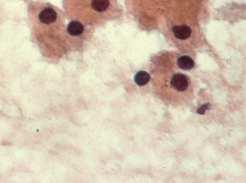
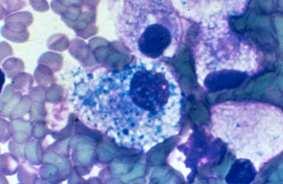
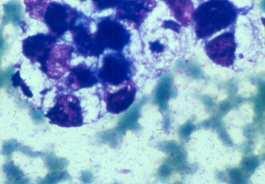
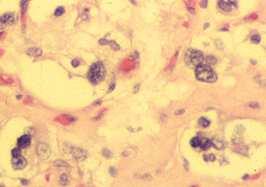
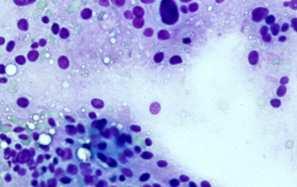
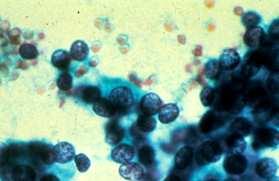
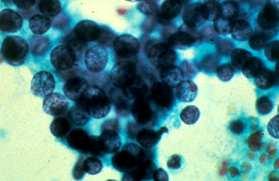
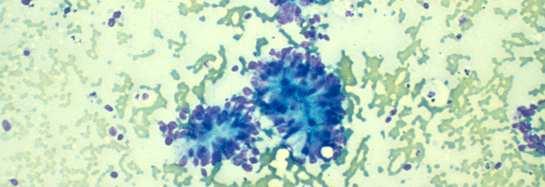
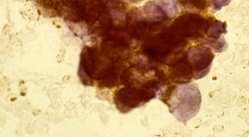
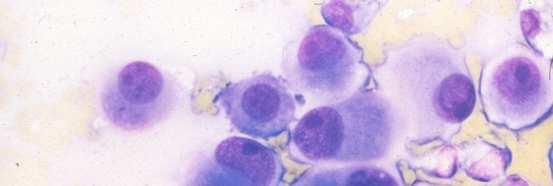
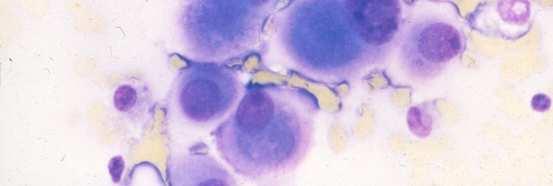
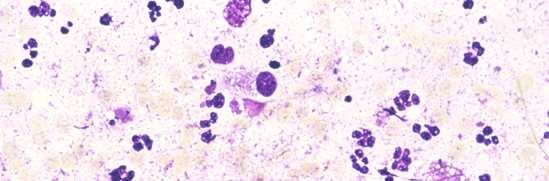
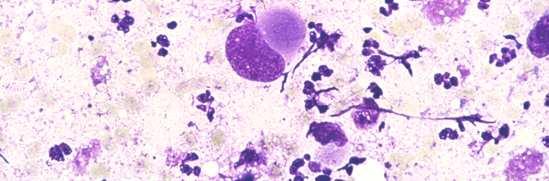
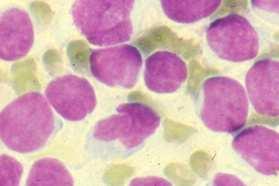
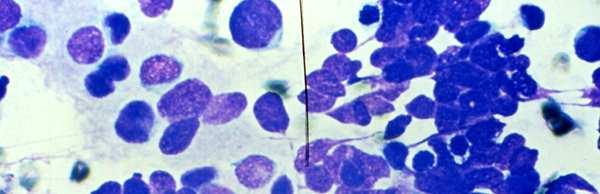
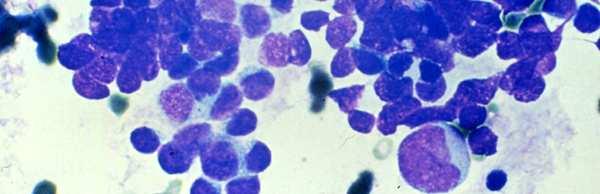
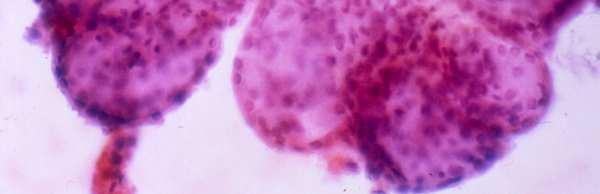
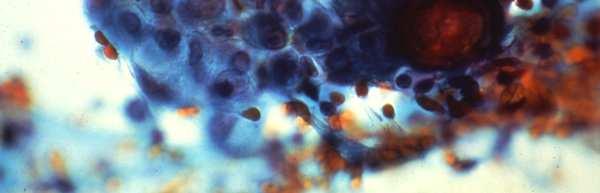
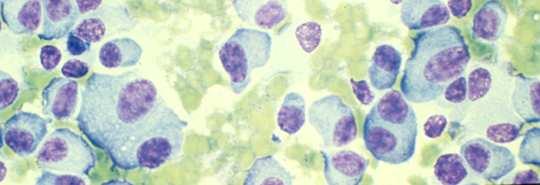
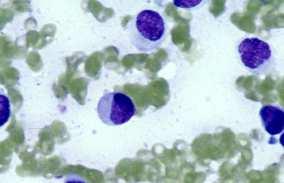
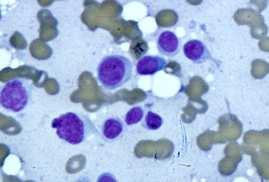
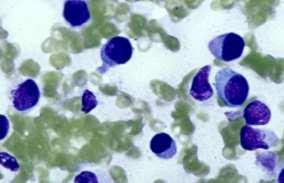
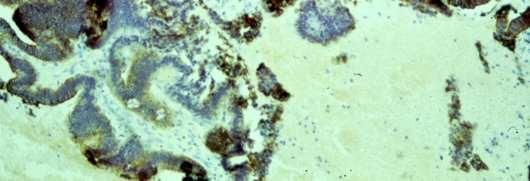
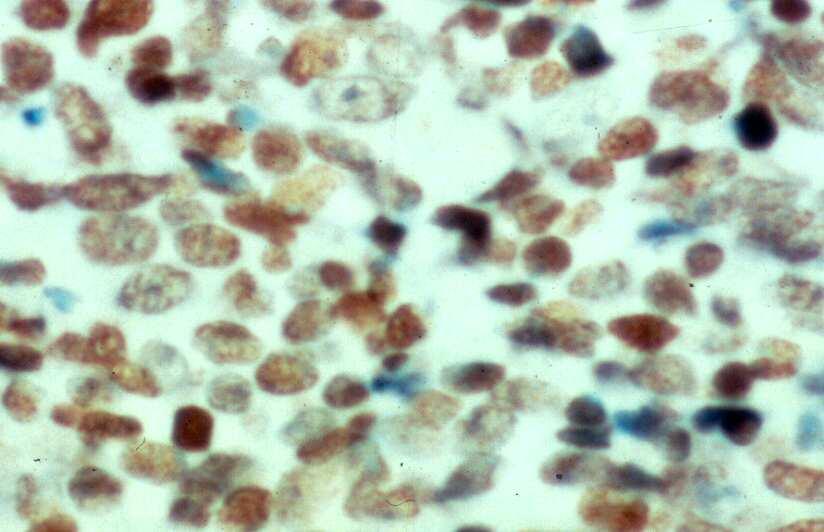
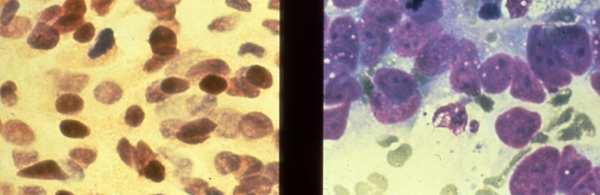
42 Case 3 A CT guided FNA biopsy of a single mass involving the anterior right lobe of liver was performed in a 72 year old female
43
44
45
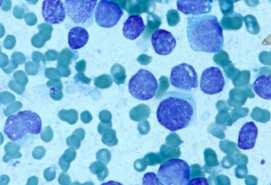
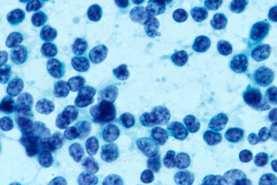
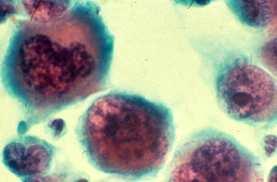
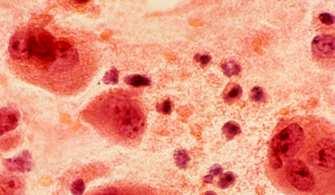
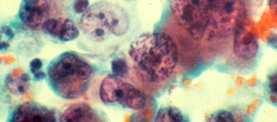
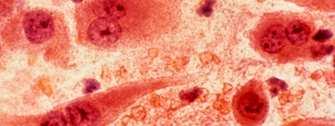
46 Case 3 DIAGNOSIS Metastatic small cell variant of malignant melanoma to the liver
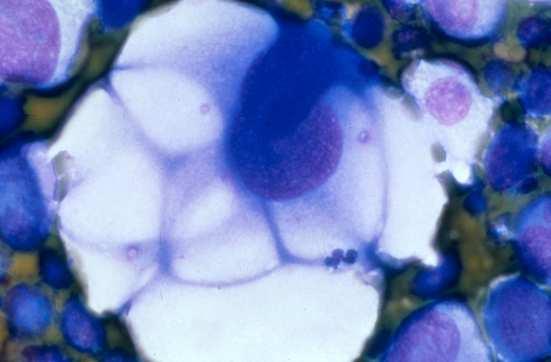
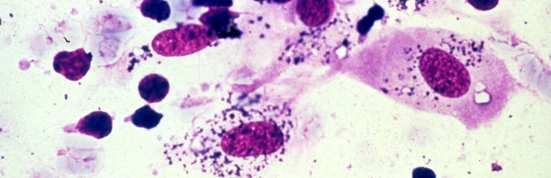
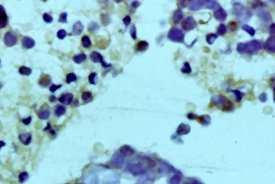
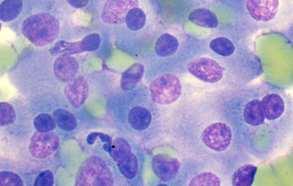
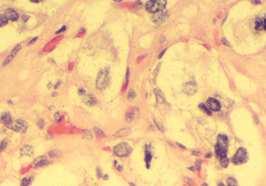
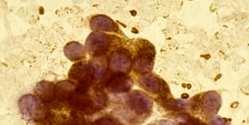
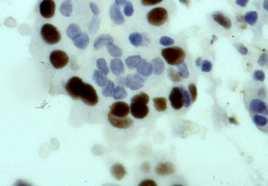
47 Case 4 53 year old male presented with a 6 cm sacral mass and pain in his legs. A FNA biopsy was performed
48

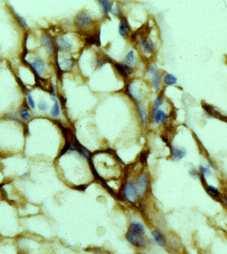
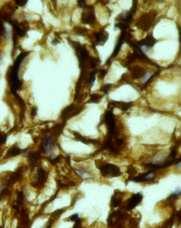
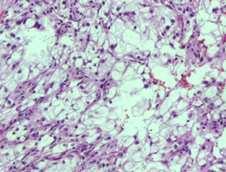
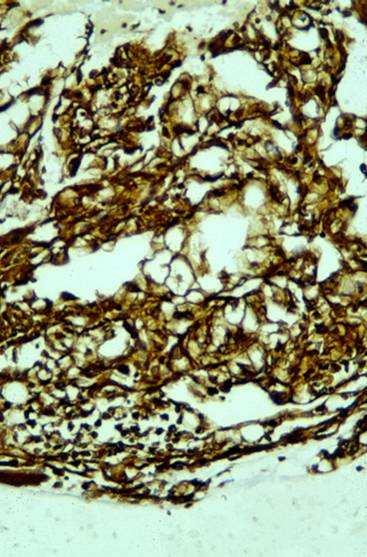
49 Vimentin CAM 5.2 CD 10
50 Case 4 DIAGNOSIS Metastatic conventional clear cell carcinoma of the kidney
51 CYTOMORPHOLOGIC PATTERNS OF METASTASIS OF UNKNOWN PRIMARY ORGIN Cell Pattern / Type Small Cell Oncocytic/Granular Clear Cell Pleomorphic/Giant Cell Spindle cell Polygonal, Large Cell
52 Small Cell Tumors Neuroendocrine tumors Carcinoids / Islet cell tumors, ect. Small cell (neuroendocrine) carcinoma Poorly differentiated carcinomas Squamous Cell Carcinoma Adenocarcinoma Lymphomas Small blue cell tumors of childhood Some sarcomas (synovial) Melanoma variant


53 Small Cell CA Merkel Cell
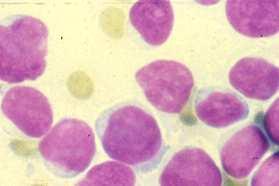
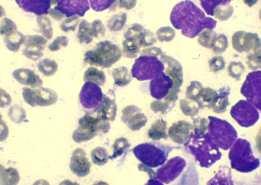
54 Lymphoma


55 CK7/20 -;P63, CK5/6 and K903 + Basaloid Squamous Cell
56 Pleomorphic / Giant Cells Carcinomas Lung, Pancreas, Liver, Thyroid, etc. Sarcomas i.e., Malignant fibrous histiocytoma, etc. Germ cell tumors Choriocarcinoma Neuroendocrine tumors Pheochromocytoma Lymphoreticular neoplasms Anaplastic large cell lymphoma (Ki-1) Melanoma
57 Pleomorphic Large Cell Lung Pancreas - Pleomorphic Giant Cell CA
58 Spindle Cells Sarcomas Fibrosarcoma Sarcomatoid Carcinomas Renal Cell CA; Spindle Squamous CA Pseudosarcomas Nodular fasciitis, fibromatosis, repair, etc. Neuroendocrine tumors Paraganglioma Melanoma
59 Sarcomatoid Squamous Cell CA
60 Melanoma
61 Sarcomatoid Renal Cell
62 Leiomyosarcoma MFH
63 Granular Cell Neoplasms Carcinomas (Adenomas) Kidney, Liver, Salivary Gland, Glassy Cell (cervix) Oncocytic / Hurthle Neoplasms Kidney, Thyroid, etc. Apocrine - Breast, Sweat Gland Neuroendocrine Tumors - Carcinoid, Paraganglioma Soft Tissue Tumors - Granular Cell Tumor Others: Muscle, Alveolar Soft Parts Sarcoma Melanoma Hilar / Leydig Cell Tumor DDX: Nonspecific degeneration Modified from DeMay

64 Hurthle Cell CA Renal Cell CA

65 Islet Cell Tumor
66 Oncocytic Neuroendocrine Warthin s
67 Clear cell Tumors Carcinomas KIDNEY, also Ovary, Liver, Adrenal, Salivary Gland, lung GYN, Thyroid Oncocytic neoplasms Acinic / Acinar Tumors Neuroendocrine Tumors (i.e., paragaglioma) Soft Tissue Tumors (i.e., clear cell sarcoma) Lymphoma - very rare Germ Cell Tumors Melanoma (ballon cells)


68 Clear Cell - Kidney Yolk-Sac CA

69 Paraganglioma
70 Intranuclear Cytoplasmic Inclusions Thyroid Papillary CA, others Lung Bronchioloalveolar CA Liver Favors HCC Melanoma Many others

71 Melanoma Thyroid
72 Microacinar Complexes Prostate Thyroid Carcinoid / Islet (Rosettes) Others - Granulosa cell tumor, other SRCT of childhood
73 Thyroid - Follicular CA Carcinoid

74 PSA + Prostrate CA
75 Hyaline Globules Carcinoma (Rhabdoid) Wide variety, often PD malignancies Sarcomas Lymphoma Melanoma (Rhabdoid) Hepatocellular, renal, ovary
76 Melanoma
77 Pleomorphic Giant Cell - Pancreas
78 Single Cell Adeno CA BREAST Pancreas Stomach Prostate Other Tumors Small Cell CA Mesothelioma Carcinoids Melanoma Hematopoeitic

79 Small Cell CA Merkel
80 Neuroblastoma
81 Non-Hodgkin Lymphoma


82 Gastric CA

83 Adrenal Cortex
84 Papillary Neoplasms Ovary GI Tract, Pancreas Lung (Bronchioloalveolar) Thyroid Renal Others

85 Papillary RC

86 Papillary TC
87 Plasmacytoid Cells Plasma Cells Carcinoid / Islet Melanoma Breast CA Pleomorphic adenoma

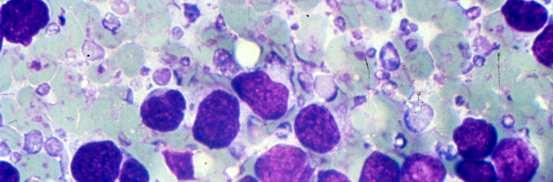
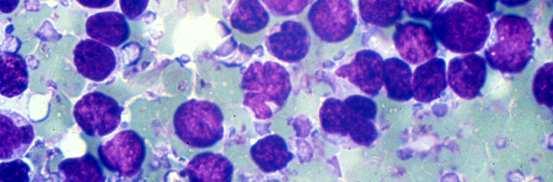
88 Multiple Myeloma

89 Multiple Myeloma Breast CA


90

91
92 Colloid (Mucinous) Neoplasms Colloid Carcinomas GI tract, Breast, Ovary, Pancreas Pseudomyxoma peritonei (appendix) Myxoid sarcomas Melanoma (Rare)

93 Colon - Colloid CA
94 Mucin Positivity excludes: LYMPHOMA / LEUKEMIA SARCOMA (except chordoma) MELANOMA Modified from DeMay
95 Case 5 72 year old male presented with a single lung mass. FNA biopsy was performed

96
97 CK 20
98 Case 5 DIAGNOSIS Metastatic colon cancer to the lung
99 Which Cytokeratin to use? Complex keratin (K903, 34BE12) - Basal cell and squamous cell CK 5/6 - Squamous cell, mesothelium, urothelium CK 7/20 - Adeno CA of unknown primary
100 IHC MARKERS FOR INTESTINAL CA CK 7/20 Villin - Colorectal, pancreas. Occasionally in non - GI i.e. endometrial, RCC (brush border staining) CDX2 - Intestinal tumors, also bladder adeno, ovarian mucinous Strong uniform CDX-2 +/with or without villin - favors colorectal
101 Organ-specific and Organ-associated Markers Antibodies to: Identifying: Also identifies: Prostatic specific antigen (PSA) Prostatic acid phosphatase (PAP) Gross cystic disease fluid protein -15 Thyroglobulin Thyroid transcription factor-1 (TTF-1) Uroplakin Inhibin Hep PAR-1 LCA, B&T Prostrate Carcinoma Prostrate Carcinoma Breast Carcinoma Thyroid carcinoma Thyroid and Lung carcinomas Urothelial carcinomas Adrenal Liver Lymphoid Neuroendocrine carcinomas Salivary gland, sweat gland tumors Rare other carcinomas Sex cord / stromal, granular cell Modified from Pathol case Review 4(6), p254, 1999 Pathol case Review 4(6), p150, 2001


102

103 PSA + Prostrate CA
104 IMMUNOHISTOCHEMICAL DETECTION OF TTF-1 IN LUNG TUMORS Adenocarcinoma 72.5% Squamous carcinoma 10% Large cell carcinoma 25.8% Large cell neuoendocrine carcinoma 75.0% Typical carcinoid 30.5% Atypical carcinoid 100% Small cell carcinoma 94.1% Alveolar adenoma 100% Ordonez, N., Adv Anat Path 7:124, 2000


105 TTF-1 + / Adeno CA TTF-1 + / Small Cell CA
106 NUCLEAR TRANSCRIPTION FACTOR ANTIBODIES MyoD1 and Myogenin - Skeletal Muscle TTF-1 - Lung and Thyroid CDX2 Intestinal Microphthalmia transcription factor (MITF) - Melanoma WT1- Serous CA, Mesothelial Pax8/Pax2- Mullerian, Thyroid Advantages - All or none positive; no false positive, cytoplasmic positive due to biotin, etc.; not related to differentiation
107 Hormone Receptor Expressions in Carcinomas ER and/or PR Positive Carcinomas (Subset) Breast, Ovarian, Endometrial Cervical Skin sweat gland Thyroid Neuroendocrine (e.g., carcinoid ER and/or PR Negative Carcinomas Lung non-small cell (antibody dependent) Colorectal Hepatocellular ER = estrogen receptors; PR = progesterone receptors Pathol Case Review 4(6), p254, 1999

108 Breast CA / ER +
109 IHC Panel for the Workup of METS X known Primary Cytokeratins: CAM 5.2, CK7, CK20, PAN CK, AE1/3, CK 5/6 EMA, CEA S-100, HMB-45, etc. LCA, etc. Specific-PSA, Thyroglobulin, TTF-1, GCDFP-15, inhibin, Hep par 1, CDX-2 NE markers-nse, Synatophysin, CD56, Chromogranin, MAP-2, etc. Germ Cell-CK, PLAP, Oct 3/4, CD30, C-kit Hormonal (ER/PR)
110 IHC WORKUP OF UNDIFFERENTIATED/POORLY DIFFERENTIATED MALIGNANCY AE-1/3 CD 45 S-100 PLAP Additional markers Carcinoma Differential keratins, EMA Melanoma HMB 45, Melan A Lymphoma CD 20, CD 3, CD 30 etc Germ cell tumor EMA, OCT-4, CD-30
111 Clinical Patterns of Metastasis
112 FNA Workup of MUP A Clinico-pathologic approach 1. Cytomorphologic features 2. Ancillary studies: IHC 3. Clinical patterns of metastases Common metastatic sites Uncommon metastatic sites
113 Metastatic Malignancies Determination of primary site is facilitated by familiarity with cytologic features of the malignancy and selected use of ICC Still, a primary site may not be determined because of non-specific cytologic & IHC features, or an atypical pattern of dissemination
114 Patterns of Metastases Usual patterns of METS to common sites : lung, lymph nodes, liver Cancer may occasionally metastasize to unusual sites: breast, spleen, pancreas This unpredictable pattern of METS may pose diagnostic problems for clinicians and pathologists misdiagnosis as a primary neoplasm Familiarity with variable patterns of metastasis a more specific diagnosis
115 Initial Sites of Metastasis Parallel natural drainage pathways of primary malignancy, i.e. related to anatomic location of tumor Lymphatic: regional lymph nodes head & neck, cervix, melanoma Vascular: venous pathways head & neck, bone, kidney lung pancreas, stomach, colon liver prostate axial skeleton via paravertebral veins
116 Common Sites of Metastasis Most common sites of metastasis: Lymph nodes lung large bones liver Most common primary sites of MUP: Lung Pancreas Colon Liver stomach Reyes 1998, FNA of 116 MUP Most common sites of metastasis Lymph nodes liver Most common primary sources Lung Prostate Kidney colon
117 Lymph Nodes Most common site for metastasis Diagnostic accuracy for metastatic carcinoma is 82-99% Knowledge of exact location of involved lymph node is of prime importance
118 Lymph Node Metastasis Lymph nodes Cervical Common/Probable primary site or malignancy Head and neck, lung, melanoma, breast Right supraclavicular Lung, breast, lymphoma Left supraclavicular Lung, breast, cervix, prostate, lymphoma Axillary Breast, lung, arm, regional trunk, GI tract Inguinal Melanoma, trunk, leg, vulva, prostate, anorectal, bladder


119 Metastatic basaloid squamous cell carcinoma to upper cervical lymph node Hypopharyngeal primary was found
120 METS to Cervical Lymph Nodes Head & neck squamous CA, melanoma : most common Adenocarcinoma Primaries arising in supra-clavicular organs Thyroid Salivary glands Primaries arising in infra-clavicular organs Lung GI tract Breast Ovary Prostate
121 Supraclavicular Lymph Nodes Primary sites involving left SCLN (Virchow s Node) are different from those involving right SCLN Cervin et al 1995, FNA of 96 SCLN Pelvic (16/19) & abdominal (6/6) malignancies LSCLN Thorax, breast, head/neck no difference in metastatic pattern to LSCLN or RSCLN Most common primaries: lung/breast > pelvis/testis > abdomen
122 Case 7. FNA biopsy of left supraclavicular lymph node. The patient is a 65 year old man with a remote previous history of malignancy


123 Diagnosis: Metastatic urothelial carcinoma. The patient had a previous history of bladder CA
124 PD carcinoma may mimic lymphoma Diff Dx: large cell lymphoma, neuroendocrine CA, melanoma Dx: Metastatic large cell CA, lung 1º, involving cervical lymph node
125 Lymphoma may mimic carcinoma DX: Anaplastic large cell lymphoma (Ki-1), involving RSCLN

126 Lung Metastases Breast, GIT- common Any malignancy lung Multiple nodules, most commonly Miliary: Melanoma, kidney, ovary, thyroid medullary CA Cannon ball: Sarcoma, kidney, melanoma, colorectal CA


127 Multiple lung nodules (cannon ball) in 49 yr old woman. No previous malig. CDX2 CK7-, CK20+ CDX2+, TTF1- DX: Metastatic adeno CA c/w colon 1 CK20
128 Lung Metastases (cont.) Diffuse infiltrate or solitary coin lesion (more problematic) rule out primary lung carcinoma Diffuse (6-8 % of pulmonary mets): Lung, breast, GI tract, pancreas Solitary MET (3-9 % of all solitary pulmonary nodules): Melanoma, breast, colon, kidney, sarcoma, non-seminomatous GCT FNA sensitivity =89%, specificity =96%



129 Solitary lung mass, 68y F Hx breast ca X 1 month, SBR I, 0/18 nodes ER/PR IHC: CK 7+, CK 20-, TTF1-, ER+, PR+ Diagnosis: Metastatic breast ca breast
130 Lung 53 year old male presented with a solitary 3 cm lung mass. Patient also had an indistinct kindey mass
131
132 FNA of right lower lobe lung masses may also inadvertently sample benign liver tissue



133 Lung PAP PSA Multiple lung nodules, 76 y M No previous hx of malignancy 5-10% of PD prostate CA either PSA- or PAP- (best to use both)
134 Unusual Sites of Metastasis Include breast, thyroid, pancreas, kidney, small bones, eye, spleen Uncommonly encountered May pose diagnostic difficulties and lead to confusion with primary neoplasms arising in these sites
135 Mechanisms of Metastasis to Unusual Sites Initial sites of metastasis lymph nodes or venous (lung, liver) Subsequent (2 ) widespread dissemination from initial metastatic site via arterial system brain, endocrine glands, small bones, spleen
136 METS to Thyroid Unusual site of involvement in clinical practice; although autopsy series report 2-26% of patients with malignancy Solitary mass or multiple small nodules Direct extension head & neck squamous cell CA, adenoid cystic CA Kidney > colon, lung, breast > melanoma
137 METS to Thyroid (2) Alien cytology Differential diagnosis: Renal CC, clear cell type vs. thyroid CA with clear cells RCC, granular type vs. Hurthle cell neoplasm RCA, TTF-1, thyroglobulin Plasmacytoma + amyloid vs. Medullary CA (EMA, kappa/lambda, Calcitonin, CEA) Dx of metastasis may prevent inappropriate thyroidectomy
138 FNA right thyroid nodule, 76 year old female. Patient had previous Hx of malignancy X 15 yrs Diagnosis: Metastatic Renal cell CA
139 Summary Cytopathologic Workup of MUP Clinico-pathologic approach 1. Cytomorphologic patterns Cell lineage: adenoca, squamous, etc. Cytomorphologic classification: small cell, large cell, etc. 2. Ancillary studies IHC 3. Clinical patterns of metastasis Common metastatic sites Uncommon metastatic sites
140 Gene Expression Profiling in MUP Confirm existing suspicions or provide new info? - High agreement with already available CP data? superiority to IHC + clinical info in unresolved cases: not helpful (Personal experience w AviaraDx) Cost: $ 3,350-3,750 Prospective studies are needed to assess: - Effect on patient outcome - Which profiling methodology /gene panel is best? IHC remains crucial component of workup. GEP may play supportive role in unresolved cases. Promising future
141 General Principles Considered in Analysis of Suspected Metastasis Familiar with cytologic features of common malignancies originating in a primary site Unusual/alien cytology for a primary site Knowledge of common and unusual metastatic patterns of malignancies & possible diagnostic pitfalls Produce a potential short list of possible primary sites Cytomorphology and IHC can then help arrive at a more specific diagnosis
142 General Principles Considered in Analysis of Suspected Metastasis (2) Clinical history of previous malignancy Review of previous pathology material Tissue confirmation in unresolved cases before definitive treatment
FNA Cytology of Metastatic Malignancies of Unknown Primary Site
 FNA Cytology of Metastatic Malignancies of Unknown Primary Site Tarik M. Elsheikh Cleveland Clinic Jan F. Silverman Alleghany Hospitals Pathologic Diagnosis of Metastasis Smaller specimens, less invasive
FNA Cytology of Metastatic Malignancies of Unknown Primary Site Tarik M. Elsheikh Cleveland Clinic Jan F. Silverman Alleghany Hospitals Pathologic Diagnosis of Metastasis Smaller specimens, less invasive
Cutaneous metastases. Thaddeus Mully. University of California, San Francisco Professor, Departments of Pathology and Dermatology
 Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Cutaneous metastases Thaddeus Mully University of California, San Francisco Professor, Departments of Pathology and Dermatology DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Thaddeus Mully Course C005 Essential
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Differential diagnosis of HCC
 Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
Hepatocellular Carcinoma Quest for an Ideal Immunohistochemical Panel Sanjay Kakar, MD UCSF Differential diagnosis of HCC Hepatocellular lesions Adenoma, FNH, HG dysplasia Adenocarcinoma CholangioCA, metastasis
Effusion Cytology: Diagnostic Challenges
 Effusion Cytology: Diagnostic Challenges Tarik M. Elsheikh, MD Professor and Medical Director, Anatomic Pathology Cleveland Clinic Outside Consult Case 45 year old woman, presented with nausea, dyspnea,
Effusion Cytology: Diagnostic Challenges Tarik M. Elsheikh, MD Professor and Medical Director, Anatomic Pathology Cleveland Clinic Outside Consult Case 45 year old woman, presented with nausea, dyspnea,
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
The clinically challenging entity of liver metastasis from tumors of unknown primary
 The clinically challenging entity of liver metastasis from tumors of unknown primary Xuchen Zhang, MD, PhD Associate Professor of Pathology Department of Pathology Yale University School of Medicine Liver
The clinically challenging entity of liver metastasis from tumors of unknown primary Xuchen Zhang, MD, PhD Associate Professor of Pathology Department of Pathology Yale University School of Medicine Liver
Presentation material is for education purposes only. All rights reserved URMC Radiology Page 1 of 98
 Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Presentation material is for education purposes only. All rights reserved. 2011 URMC Radiology Page 1 of 98 Radiology / Pathology Conference February 2011 Brooke Koltz, Cytopathology Resident Presentation
Ascitic Fluid and Use of Immunocytochemistry. Mercè Jordà, University of Miami
 Ascitic Fluid and Use of Immunocytochemistry Mercè Jordà, University of Miami Is It Malignant? Yes? No Ascitic Fluid Cytomorphologic Useful Findings Tight clusters with smooth borders Cellular and nuclear
Ascitic Fluid and Use of Immunocytochemistry Mercè Jordà, University of Miami Is It Malignant? Yes? No Ascitic Fluid Cytomorphologic Useful Findings Tight clusters with smooth borders Cellular and nuclear
List of Available TMAs in the PRN
 TMA RPCI_BrainCa01 RPCI_BrCa03 RPCI_BrCa04 RPCI_BrCa05 RPCI_BrCa0 RPCI_BrCa07 RPCI_BrCa08 RPCI_BrCa15 RPCI_BrCa1 RPCI_BrCa17 RPCI_BrCa18 RPCI_BrCa19 RPCI_BrCa20 RPCI_BrCa21 RPCI_BrCa24 RPCI_BrCa25 RPCI_BrCa2
TMA RPCI_BrainCa01 RPCI_BrCa03 RPCI_BrCa04 RPCI_BrCa05 RPCI_BrCa0 RPCI_BrCa07 RPCI_BrCa08 RPCI_BrCa15 RPCI_BrCa1 RPCI_BrCa17 RPCI_BrCa18 RPCI_BrCa19 RPCI_BrCa20 RPCI_BrCa21 RPCI_BrCa24 RPCI_BrCa25 RPCI_BrCa2
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Carcinoma of Unknown Primary (CUP)
") Metasta c Carcinoma of Unknown Primary: Diagnos c Approach Using Immunohistochemistry James R. Conner, MD, PhD Mount Sinai Hospital Toronto, ON Carcinoma of Unknown Primary (CUP) 3-5% of all new malignant
Metasta c Carcinoma of Unknown Primary: Diagnos c Approach Using Immunohistochemistry James R. Conner, MD, PhD Mount Sinai Hospital Toronto, ON Carcinoma of Unknown Primary (CUP) 3-5% of all new malignant
The Panel Approach to Diagnostics. Lauren Hopson International Product Specialist Cell Marque Corporation
 The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
Histopathological diagnosis of CUP
 Histopathological diagnosis of CUP Dr Karin Oien karin.oien@glasgow.ac.uk Disclosure slide Dr Karin Oien has no financial interests in any company mentioned in this presentation. Dr Karin Oien is conducting
Histopathological diagnosis of CUP Dr Karin Oien karin.oien@glasgow.ac.uk Disclosure slide Dr Karin Oien has no financial interests in any company mentioned in this presentation. Dr Karin Oien is conducting
Carcinoma of unknown primary origin (CUP) is defined
 is defined") REVIEW ARTICLE Metastatic Carcinoma of Unknown Primary: Diagnostic Approach Using Immunohistochemistry James R. Conner, MD, PhD and Jason L. Hornick, MD, PhD Abstract: Carcinoma of unknown primary origin
REVIEW ARTICLE Metastatic Carcinoma of Unknown Primary: Diagnostic Approach Using Immunohistochemistry James R. Conner, MD, PhD and Jason L. Hornick, MD, PhD Abstract: Carcinoma of unknown primary origin
Neuroendocrine Carcinoma. Lebanon Neuroendocrine Neoplasms of H&N Nov /7/2011. Broad Classification:
 H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
H&N Neuroendocrine Neoplasms: Classification and Diagnostic Considerations Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Broad Classification: A. Epithelial:
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
CARCINOMA OF UNKNOWN PRIMARY: DIAGNOSTIC APPROACH USING IMMUNOHISTOCHEMISTRY
 CARCINOMA OF UNKNOWN PRIMARY: DIAGNOSTIC APPROACH USING IMMUNOHISTOCHEMISTRY Jason L Hornick, MD, PhD Director of Surgical Pathology Director of Immunohistochemistry Brigham and Women s Hospital Associate
CARCINOMA OF UNKNOWN PRIMARY: DIAGNOSTIC APPROACH USING IMMUNOHISTOCHEMISTRY Jason L Hornick, MD, PhD Director of Surgical Pathology Director of Immunohistochemistry Brigham and Women s Hospital Associate
Reporting of carcinoma of unknown primary tumour (CUP)
") Reporting of carcinoma of unknown primary tumour (CUP) Prof John Schofield Kent Oncology Centre with grateful thanks to Dr Karin Oien University of Glasgow Royal College of Pathologists Cancer datasets
Reporting of carcinoma of unknown primary tumour (CUP) Prof John Schofield Kent Oncology Centre with grateful thanks to Dr Karin Oien University of Glasgow Royal College of Pathologists Cancer datasets
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens
 How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
4/12/2018. MUSC Pathology Symposium Kiawah Island April 18, Jesse K. McKenney, MD
 MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
MUSC Pathology Symposium Kiawah Island April 18, 2018 Jesse K. McKenney, MD 1 Urothelial Carcinoma with Alternative Differentiation 2 Urothelial Carcinoma with Alternative Differentiation Recognition as
Mesothelioma: diagnostic challenges from a pathological perspective. Naseema Vorajee August 2016
 Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Mesothelioma: diagnostic challenges from a pathological perspective Naseema Vorajee August 2016 Naseema.vorajee@nhls.ac.za Pleural diseases (whether neoplastic, reactive or infective) may have similar
Lung Tumor Cases: Common Problems and Helpful Hints
 Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Lung Tumor Cases: Common Problems and Helpful Hints Brandon T. Larsen, MD, PhD Senior Associate Consultant Department of Laboratory Medicine and Pathology Mayo Clinic Arizona Arizona Society of Pathologists
Medullary Thyroid Carcinoma. This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands
 Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
FNA of Thyroid. Toward a Uniform Terminology With Management Guidelines. NCI NCI Thyroid FNA State of the Science Conference
 FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
FNA of Thyroid NCI NCI Thyroid FNA State of the Science Conference Toward a Uniform Terminology With Management Guidelines Thyroid Thyroid FNA Cytomorphology NCI Thyroid FNA State of the Science Conference
Diagnostic IHC in lung and pleura pathology
 Diagnostic IHC in lung and pleura pathology Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark WHO 2004 and Web Malignant mesothelioma Epithelioid
Diagnostic IHC in lung and pleura pathology Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark WHO 2004 and Web Malignant mesothelioma Epithelioid
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Pathology Mystery and Surprise
 Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
Pathology Mystery and Surprise Tim Smith, MD Director Anatomic Pathology Medical University of South Carolina Disclosures No conflicts to declare Some problem cases Kidney tumor Scalp tumor Bladder tumor
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics. Mercè Jordà, University of Miami
 Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Cytological Sub-classification of Lung Cancer: Morphologic and Molecular Characteristics Mercè Jordà, University of Miami Mortality Lung cancer is the most frequent cause of cancer incidence and mortality
Case #1 FNA of nodule in left lobe of thyroid in 67 y.o. woman
 Challenging Cases Manon Auger M.D., F.R.C.P. (C) Professor, Department of Pathology McGill University Director, Cytopathology Laboratory McGill University it Health Center Case #1 FNA of nodule in left
Challenging Cases Manon Auger M.D., F.R.C.P. (C) Professor, Department of Pathology McGill University Director, Cytopathology Laboratory McGill University it Health Center Case #1 FNA of nodule in left
Breast - ductal carcinoma CK7 ER PR GATA3 Mammaglobin (50-70%) GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2 on all newly diagnosed cases
 GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2 on all newly diagnosed cases") Adrenal cortical carcinoma Inhibin Synap Melan-A Calretinin Vimentin Chromogr CK7 CK20 Breast - ductal carcinoma CK7 ER PR GATA3 Mammaglobin (50-70%) GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2
Adrenal cortical carcinoma Inhibin Synap Melan-A Calretinin Vimentin Chromogr CK7 CK20 Breast - ductal carcinoma CK7 ER PR GATA3 Mammaglobin (50-70%) GCDFP-15 (50-70%) E-cadherin HMWCK CK20 PAX2 ER/PR/HER2
Pancreatic Cytopathology: The Solid Neoplasms
 Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Pancreatic Cytopathology: The Solid Neoplasms Syed Z. Ali, M.D. Professor of Pathology and Radiology Director of Cytopathology The Johns Hopkins Hospital Baltimore, Maryland Pancreatic Cytopathology: Past,
Lung Cytology: Lessons Learned from Errors in Practice
 Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
Lung Cytology: Lessons Learned from Errors in Practice Stephen S. Raab, M.D. Department of Laboratory Medicine Eastern Health and Memorial University of Newfoundland, St. John s, NL and University of Washington,
incidence rate x 100,000/year
 Tier R=rare C=common Cancer Entity European crude and age adjusted incidence by cancer, years of diagnosis 2000 and 2007 Analisys based on 83 population-based cancer registries * applying the European
Tier R=rare C=common Cancer Entity European crude and age adjusted incidence by cancer, years of diagnosis 2000 and 2007 Analisys based on 83 population-based cancer registries * applying the European
Update on Thyroid FNA The Bethesda System. Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center
 Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Update on Thyroid FNA The Bethesda System Shikha Bose M.D. Associate Professor Cedars Sinai Medical Center Thyroid Nodules Frequent occurrence Palpable: 4-7% of adults Ultrasound: 10-31% Majority benign
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
New Developments in Immunohistochemistry for Gynecologic Pathology
 New Developments in Immunohistochemistry for Gynecologic Pathology Michael T. Deavers, M.D. Professor, Departments of Pathology and Gynecologic Oncology Immunohistochemistry in Gynecologic Pathology Majority
New Developments in Immunohistochemistry for Gynecologic Pathology Michael T. Deavers, M.D. Professor, Departments of Pathology and Gynecologic Oncology Immunohistochemistry in Gynecologic Pathology Majority
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH
 FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
FNA OF SALIVARY GLANDS: A PRACTICAL APPROACH FNA of Salivary Glands: Challenges Wide range of neoplastic and non-neoplastic lesions Cytological overlap between the different benign and malignant tumors
Case year female. Routine Pap smear
 Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Case 1 57 year female Routine Pap smear Diagnosis? 1. Atypical glandular cells of unknown significance (AGUS) 2. Endocervical AIS 3. Endocervical adenocarcinoma 4. Endometrial adenocarcinoma 5. Adenocarcinoma
Immunohistochemical classification of lung carcinomas and mesotheliomas. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark
 Immunohistochemical classification of lung carcinomas and mesotheliomas Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Endobronchial ultrasound guided transbronchial needle biopsy
Immunohistochemical classification of lung carcinomas and mesotheliomas Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Endobronchial ultrasound guided transbronchial needle biopsy
Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources
 Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources 1 IHC Identification Targets Specimens Controls 2 Tissue controls Trouble Spots 3 The Key to Description IHC Description 4 Intermediate Filaments
Charles Halsey, DVM, PhD, DACVP Pfizer, Inc. IHC Resources 1 IHC Identification Targets Specimens Controls 2 Tissue controls Trouble Spots 3 The Key to Description IHC Description 4 Intermediate Filaments
4/17/2015. Case 1. A 37 year old man with a 2.2 cm solitary left thyroid mass.
 Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Case 1 A 37 year old man with a 2.2 cm solitary left thyroid mass. Case 1 Case 1 1 Case 1: Diagnosis? A. Benign B. Atypia of undetermined significance/follicular lesion of undetermined significance C.
Case 2. Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset
 Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Case 2 Dr. Sathima Natarajan M.D. Kaiser Permanente Medical Center Sunset History 24 year old male presented with a 3 day history of right flank pain, sharp in nature Denies fever, chills, hematuria or
Other Sites. Table 2 Continued. MPH Rules 11/8/07. NAACCR Webinar Series 1
 MPH s 11/8/07 Other s 1 Table 2 Continued Use this two-page table to select combination histology codes. Compare the terms in the diagnosis to the terms in Columns 1 and 2. If the terms match, code the
MPH s 11/8/07 Other s 1 Table 2 Continued Use this two-page table to select combination histology codes. Compare the terms in the diagnosis to the terms in Columns 1 and 2. If the terms match, code the
Case Hx. Mrs. CP 69 female non smoker Presented with 20 lb weight loss Some changes in bowel habit but no bleeding Upper abdominal discomfort PMH
 Case Hx Mrs. CP 69 female non smoker Presented with 20 lb weight loss Some changes in bowel habit but no bleeding Upper abdominal discomfort PMH HTN, Dyslipidemia, GERD Breast reduction surgery Surgeries
Case Hx Mrs. CP 69 female non smoker Presented with 20 lb weight loss Some changes in bowel habit but no bleeding Upper abdominal discomfort PMH HTN, Dyslipidemia, GERD Breast reduction surgery Surgeries
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000
 Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Impact of immunostaining of pulmonary and mediastinal cytology
 Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
Impact of immunostaining of pulmonary and mediastinal cytology Harman Sekhon MD, PhD Director of Cytopathology Head of Ottawa-site Ontario Tumour Bank June 20, 2014 Disclaimer Pfizer: Honorarium-Advisory
I. Diagnosis of the cancer type in CUP
 Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
Immunohistochemistry in Bone and Soft Tissue Tumors. Sahar Rassi Zankoul, MD
 Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Immunohistochemistry in Bone and Soft Tissue Tumors Sahar Rassi Zankoul, MD Introduction Bone tumors represent a wide variety of tumors of various origins and malignant potentials. These different tumor
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
MEDICAL POLICY Gene Expression Profiling for Cancers of Unknown Primary Site
 POLICY: PG0364 ORIGINAL EFFECTIVE: 04/22/16 LAST REVIEW: 07/26/18 MEDICAL POLICY Gene Expression Profiling for Cancers of Unknown Primary Site GUIDELINES This policy does not certify benefits or authorization
POLICY: PG0364 ORIGINAL EFFECTIVE: 04/22/16 LAST REVIEW: 07/26/18 MEDICAL POLICY Gene Expression Profiling for Cancers of Unknown Primary Site GUIDELINES This policy does not certify benefits or authorization
Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms
 Hindawi Publishing Corporation Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Hindawi Publishing Corporation Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
SCOPE OF PRACTICE PGY-5
 Recognize normal cytomorphology of cells derived from the respiratory, gastrointestinal, and genitourinary tracts, and body fluid (Cerebrospinal fluid, pleural and peritoneal fluid) Recognize normal cytomorphology
Recognize normal cytomorphology of cells derived from the respiratory, gastrointestinal, and genitourinary tracts, and body fluid (Cerebrospinal fluid, pleural and peritoneal fluid) Recognize normal cytomorphology
C.L. Davis Foundation Descriptive Veterinary Pathology Course
 C.L. Davis Foundation 2015 Descriptive Veterinary Pathology Course IHC Resources IHC Identification Targets Antibodies Antibodies 1 Antibodies Specimens Antigen Retrieval Unmasks antigen epitopes Methods
C.L. Davis Foundation 2015 Descriptive Veterinary Pathology Course IHC Resources IHC Identification Targets Antibodies Antibodies 1 Antibodies Specimens Antigen Retrieval Unmasks antigen epitopes Methods
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016
 40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
40th European Congress of Cytology Liverpool, UK, 2-5 th October 2016 EUS FNA of abdominal organs: An approach to reporting and triage for ancillary testing Date and time: Sunday 2 nd October 2016 15.00-16.30
2010 Update. NAACCR Webinar Series 1 4/1/2010. Agenda. Access to 2010 Information. CSv2. Collecting Cancer Data: Soft Tissue Sarcoma
 NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Soft Tissue Sarcoma, Neuroendocrine Tumors (NET) and Gastrointestinal Stromal Tumors (GIST) Agenda Updates Soft Tissue Sarcoma Overview CSv2 MP/H
NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Soft Tissue Sarcoma, Neuroendocrine Tumors (NET) and Gastrointestinal Stromal Tumors (GIST) Agenda Updates Soft Tissue Sarcoma Overview CSv2 MP/H
THYMIC CARCINOMAS AN UPDATE
 THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
THYMIC CARCINOMAS AN UPDATE Mark R. Wick, M.D. University of Virginia Medical Center Charlottesville, VA CARCINOMA OF THE THYMUS General Clinical Features No apparent gender predilection Age range of 35-75
ICD-O Morphology code. R=Rare Tier Tumour ICD-O Topography code C30.0, C31
 R=Rare Tier Tumour ICD-O Topography code ICD-O Morphology code EPITHELIAL TUMOURS OF NASAL CAVITY AND SINUSES R 2 Squamous cell carcinoma with variants of nasal cavity and sinuses C30.0, C3 C30.0, C3 8000,
R=Rare Tier Tumour ICD-O Topography code ICD-O Morphology code EPITHELIAL TUMOURS OF NASAL CAVITY AND SINUSES R 2 Squamous cell carcinoma with variants of nasal cavity and sinuses C30.0, C3 C30.0, C3 8000,
Tumour Markers. For these reasons, only a handful of tumour markers are commonly used by most doctors.
 Tumour Markers What are Tumour Markers? Tumour markers are substances that can be found in the body when cancer is present. They are usually found in the blood or urine. They can be products of cancer
Tumour Markers What are Tumour Markers? Tumour markers are substances that can be found in the body when cancer is present. They are usually found in the blood or urine. They can be products of cancer
Problem 1: Differential of Neuroendocrine Carcinoma 3/23/2017. Disclosure of Relevant Financial Relationships
 Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Differential of Neuroendocrine Carcinoma Alain C. Borczuk,MD Weill Cornell Medicine Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control
Breast cancer: IHC classification. Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
 Breast cancer: IHC classification Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark http://upload.wikimedia.org/wikipedia/commons/1/1a/breast.svg
Breast cancer: IHC classification Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark http://upload.wikimedia.org/wikipedia/commons/1/1a/breast.svg
Liver Specialty Evening Conference. Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle
 Liver Specialty Evening Conference Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle Case History A 65 year-old man presents with abdominal
Liver Specialty Evening Conference Matthew M. Yeh, MD, PhD Professor of Pathology Adjunct Professor of Medicine University of Washington, Seattle Case History A 65 year-old man presents with abdominal
SUPPLEMENTARY INFORMATION
 Supplementary Table 1 trials currently open for patients with pheochromocytoma and/or paraganglima (from trials.gov) www.clinicaltrials.gov; Active PPGL trials Status Of Sunitinib In Patients With Recurrent
Supplementary Table 1 trials currently open for patients with pheochromocytoma and/or paraganglima (from trials.gov) www.clinicaltrials.gov; Active PPGL trials Status Of Sunitinib In Patients With Recurrent
SELECTED DILEMMAS IN RESPIRATORY CYTOPATHOLOGY (2 CASES)
") SELECTED DILEMMAS IN RESPIRATORY CYTOPATHOLOGY (2 CASES) Dr. Mariamma Joseph Professor of Pathology Division Head Cytopathology Department of Pathology and Laboratory Medicine LHSC and Western University
SELECTED DILEMMAS IN RESPIRATORY CYTOPATHOLOGY (2 CASES) Dr. Mariamma Joseph Professor of Pathology Division Head Cytopathology Department of Pathology and Laboratory Medicine LHSC and Western University
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Tumor Markers Yesterday, Today & Tomorrow. Steven E. Zimmerman M.D. Vice President & Chief Medical Director
 Tumor Markers Yesterday, Today & Tomorrow Steven E. Zimmerman M.D. Vice President & Chief Medical Director Tumor Marker - Definition Substances produced by cancer cells or other cells in response to cancer
Tumor Markers Yesterday, Today & Tomorrow Steven E. Zimmerman M.D. Vice President & Chief Medical Director Tumor Marker - Definition Substances produced by cancer cells or other cells in response to cancer
A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy.
 November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
November 2015 Case of the Month A 53 year-old woman with a lung mass, right hilar mass and mediastinal adenopathy. Contributed by: Rasha Salama, M.D., IU Department of Pathology and Laboratory Medicine
Diplomate of the American Board of Pathology in Anatomic and Clinical Pathology
 A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
A 33-year-old male with a left lower leg mass. Contributed by Shaoxiong Chen, MD, PhD Assistant Professor Indiana University School of Medicine/ IU Health Partners Department of Pathology and Laboratory
Case 18. M75. Excision of mass on scalp. Clinically SCC. The best diagnosis is:
 Case 18 M75. Excision of mass on scalp. Clinically SCC. The best diagnosis is: A. Pilomatrical carcinoma B. Adnexal carcinoma NOS C. Metastatic squamous cell carcinoma D.Primary squamous cell carcinoma
Case 18 M75. Excision of mass on scalp. Clinically SCC. The best diagnosis is: A. Pilomatrical carcinoma B. Adnexal carcinoma NOS C. Metastatic squamous cell carcinoma D.Primary squamous cell carcinoma
Oncocytic-Appearing Salivary Gland Tumors. Oncocytic, Cystic, Mucinous, and High Grade Salivary Gland Tumors SALIVARY GLAND FNA: PART II
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital SALIVARY GLAND FNA: PART II Oncocytic,
Adnexal primary or Melanocy+c prolifera+ons in sundamaged metastatic carcinoma?
 Adnexal primary or Melanocy+c prolifera+ons in sundamaged metastatic carcinoma? skin Jane L. Messina, MD Interna0onal Melanoma Pathology Working Group 4 th annual mee0ng Tampa, Florida November 14, 2011
Adnexal primary or Melanocy+c prolifera+ons in sundamaged metastatic carcinoma? skin Jane L. Messina, MD Interna0onal Melanoma Pathology Working Group 4 th annual mee0ng Tampa, Florida November 14, 2011
DIAGNOSTIC DILEMMA. Case Reports Clinical history. Materials and Methods
 DIAGNOSTIC DILEMMA A Metastatic Renal Carcinoid Tumor Presenting as Breast Mass: A Diagnostic Dilemma Farnaz Hasteh, M.D., 1 Robert Pu, M.D., Ph.D., 2 and Claire W. Michael, M.D. 2 * We present clinicopathological
DIAGNOSTIC DILEMMA A Metastatic Renal Carcinoid Tumor Presenting as Breast Mass: A Diagnostic Dilemma Farnaz Hasteh, M.D., 1 Robert Pu, M.D., Ph.D., 2 and Claire W. Michael, M.D. 2 * We present clinicopathological
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix
 The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
The role of immunohistochemistry in surgical pathology of the uterine corpus and cervix Prof. Ben Davidson, MD PhD Department of Pathology, Norwegian Radium Hospital, Oslo University Hospital, Oslo, Norway
SHN-1 Human Digestive Panel Test results
 SHN-1 Human Digestive Panel Test results HN-30 tongue HN-24 salivary gland HN-12 larynx HN-28 esophagus HN-29 stomach HN-20 pancreas HN-13 liver HN-14 gall bladder HN-27-1 duodenum HN-27-2 ileum HN-27-3
SHN-1 Human Digestive Panel Test results HN-30 tongue HN-24 salivary gland HN-12 larynx HN-28 esophagus HN-29 stomach HN-20 pancreas HN-13 liver HN-14 gall bladder HN-27-1 duodenum HN-27-2 ileum HN-27-3
NICHOLAS PAVLIDIS, MD, PhD, FRCP (Edin)
") CANCER OF UNKNOWN PRIMARY A Complex Disease NICHOLAS PAVLIDIS, MD, PhD, FRCP (Edin) PROFESSOR OF MEDICAL ONCOLOGY Bogota, May-June 2016 WHAT IS CANCER OF UNKNOWN PRIMARY (CUP)? Is a clinical disorder where
CANCER OF UNKNOWN PRIMARY A Complex Disease NICHOLAS PAVLIDIS, MD, PhD, FRCP (Edin) PROFESSOR OF MEDICAL ONCOLOGY Bogota, May-June 2016 WHAT IS CANCER OF UNKNOWN PRIMARY (CUP)? Is a clinical disorder where
Tumor Markers & Cytopathology
 Tumor Markers & Cytopathology Objectives: After learning, student should be able to 1. Describe the basic concepts of tumor markers and Asst. Prof. Prasit Suwannalert, Ph.D. (Email: prasit.suw@mahidol.ac.th)
Tumor Markers & Cytopathology Objectives: After learning, student should be able to 1. Describe the basic concepts of tumor markers and Asst. Prof. Prasit Suwannalert, Ph.D. (Email: prasit.suw@mahidol.ac.th)
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms
 Case Reports in Pathology Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Case Reports in Pathology Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Immunohistochemical Evaluation of Necrotic Malignant Melanomas
 Anatomic Pathology / EVALUATION OF NECROTIC MALIGNANT MELANOMAS Immunohistochemical Evaluation of Necrotic Malignant Melanomas Daisuke Nonaka, MD, Jordan Laser, MD, Rachel Tucker, HTL(ASCP), and Jonathan
Anatomic Pathology / EVALUATION OF NECROTIC MALIGNANT MELANOMAS Immunohistochemical Evaluation of Necrotic Malignant Melanomas Daisuke Nonaka, MD, Jordan Laser, MD, Rachel Tucker, HTL(ASCP), and Jonathan
Immunohistochemical classification of the unknown primary tumour (UPT) Part I. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark
 Part I. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark") Immunohistochemical classification of the unknown primary tumour (UPT) Part I Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Tumours of unknown origin: Histology Brain tumour - biopsy
Immunohistochemical classification of the unknown primary tumour (UPT) Part I Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Tumours of unknown origin: Histology Brain tumour - biopsy
Lesions Mimicking Adenoid Cystic Carcinoma. Diagnostic Problems in Salivary Gland Pathology An Update 5/29/2009
 Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Diagnostic Problems in Salivary Gland Pathology An Update Lesions Mimicking Adenoid Cystic Carcinoma Stacey E. Mills, M.D. W.S. Royster Professor of Pathology Director of Surgical and Cytopathology University
Thyroid Cancer: Imaging Techniques (Nuclear Medicine)
") Thyroid Cancer: Imaging Techniques (Nuclear Medicine) Andrei Iagaru, MD MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology Introduction Ø There are
Thyroid Cancer: Imaging Techniques (Nuclear Medicine) Andrei Iagaru, MD MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology Introduction Ø There are
57th Annual HSCP Spring Symposium 4/16/2016
 An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
An Unusual Malignant Spindle Cell Lesion to Involve the Breast Erinn Downs-Kelly, D.O. Associate Professor of Pathology University of Utah & ARUP Laboratories No disclosures Case 39 y/o female with no
What I Learned from 3 Cases and 3 Antibodies
 What I Learned from 3 Cases and 3 Antibodies Melinda Sanders, M.D Vanderbilt University Medical Center Professor of Pathology Consultant in Breast Pathology Disclosure of Relevant Financial Relationships
What I Learned from 3 Cases and 3 Antibodies Melinda Sanders, M.D Vanderbilt University Medical Center Professor of Pathology Consultant in Breast Pathology Disclosure of Relevant Financial Relationships
ISSN X (Print) Original Research Article. DOI: /sjams
 Original Research Article. DOI: /sjams") DOI: 10.21276/sjams.2016.4.7.33 Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2016; 4(7C):2468-2473 Scholars Academic and Scientific Publisher (An International Publisher
DOI: 10.21276/sjams.2016.4.7.33 Scholars Journal of Applied Medical Sciences (SJAMS) Sch. J. App. Med. Sci., 2016; 4(7C):2468-2473 Scholars Academic and Scientific Publisher (An International Publisher
Respiratory Tract Cytology
 Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
Respiratory Tract Cytology 40 th European Congress of Cytology Liverpool, UK Momin T. Siddiqui M.D. Professor of Pathology and Laboratory Medicine Director of Cytopathology Emory University Hospital, Atlanta,
HOSPITAL-BASED CANCER REGISTRY ANNUAL REPORT 2011
 HOSPITAL-BASED CANCER REGISTRY ANNUAL REPORT 2011 SONGKLANAGARIND HOSPITAL FACULTY OF MEDICINE PRINCE OF SONGKLA UNIVERSITY HATYAI SONGKHLA THAILAND EDITOR PARADEE PRECHAWITTAYAKUL, B.Sc. June, 2013 Songklanagarind
HOSPITAL-BASED CANCER REGISTRY ANNUAL REPORT 2011 SONGKLANAGARIND HOSPITAL FACULTY OF MEDICINE PRINCE OF SONGKLA UNIVERSITY HATYAI SONGKHLA THAILAND EDITOR PARADEE PRECHAWITTAYAKUL, B.Sc. June, 2013 Songklanagarind
- Selected Tumors of the Skin Appendages - Primary vs. Metastasis
 - Selected Tumors of the Skin Appendages - Primary vs. Metastasis Napa Valley 2018 Victor G. Prieto, MD, PhD Chair of Pathology UT MD Anderson Cancer Center vprieto@mdanderson.org Napa Valley in May Introduction
- Selected Tumors of the Skin Appendages - Primary vs. Metastasis Napa Valley 2018 Victor G. Prieto, MD, PhD Chair of Pathology UT MD Anderson Cancer Center vprieto@mdanderson.org Napa Valley in May Introduction
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Expression of Cytokeratin 5/6 in Epithelial Neoplasms: An Immunohistochemical Study of 509 Cases
 Expression of Cytokeratin 5/6 in Epithelial Neoplasms: An Immunohistochemical Study of 509 Peiguo G. Chu, M.D., Ph.D., Lawrence M. Weiss, M.D. Department of Pathology, City of Hope National Medical Center,
Expression of Cytokeratin 5/6 in Epithelial Neoplasms: An Immunohistochemical Study of 509 Peiguo G. Chu, M.D., Ph.D., Lawrence M. Weiss, M.D. Department of Pathology, City of Hope National Medical Center,
Dr Sanjiv Manek Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
Dr Sanjiv Manek Oxford Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust Ovarian Endometrial Vulvo-vaginal Cervical Illustration-Cellular Pathology. Oxford
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT?
 POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
POORLY DIFFERENTIATED, HIGH GRADE AND ANAPLASTIC CARCINOMAS: WHAT IS EVERYONE TALKING ABOUT? AGGRESSIVE THYROID CANCERS PAPILLARY CARCINOMA CERTAIN SUBTYPES POORLY DIFFERENTIATED CARCINOMA HIGH GRADE DIFFERENTIATED
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Section 14 Other Cancers. Cancer of Unknown 113 Primary Site INTRODUCTION PATHOLOGIC EVALUATION
 Section 14 Other Cancers Cancer of Unknown 113 Primary Site F. Anthony Greco and John D. Hainsworth INTRODUCTION Cancer of unknown primary (CUP) site is a clinical syndrome that includes many types of
Section 14 Other Cancers Cancer of Unknown 113 Primary Site F. Anthony Greco and John D. Hainsworth INTRODUCTION Cancer of unknown primary (CUP) site is a clinical syndrome that includes many types of
I have nothing to disclose
 A 47 year old female with multiple lung nodules Disclosure of Relevant Financial Relationships Tamar Giorgadze, MD, PhD Professor of Pathology Medical College of Wisconsin Milwaukee, Wisconsin USCAP requires
A 47 year old female with multiple lung nodules Disclosure of Relevant Financial Relationships Tamar Giorgadze, MD, PhD Professor of Pathology Medical College of Wisconsin Milwaukee, Wisconsin USCAP requires
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES
 DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,
DIAGNOSTIC SLIDE SEMINAR: PART 1 RENAL TUMOUR BIOPSY CASES Dr. Andrew J. Evans MD, PhD, FACP, FRCPC Consultant in Genitourinary Pathology University Health Network, Toronto, ON Case 1 43 year-old female,